MHS Prior Authorization 0317.PR.P.PP
|
|
|
- Jeremy Parrish
- 6 years ago
- Views:
Transcription

1 MHS Prior Authorization 0317.PR.P.PP
2 Prior Authorization (PA) PA requirements Recent Updates Helpful Tips Web Telephone Fax Referrals Appeals Process Need to Know Questions and Answers Agenda MHS Prior Authorization 101 MHS Prior Authorization
3 Prior Authorization Prior Authorization (Medical Services) Prior Authorization is an approval from MHS to provide services designated as needing approval before treatment and/or payment Inpatient authorizations = IP + 10 digits Outpatient authorizations = OP + 10 digits Emergent = Symptoms suggesting imminent, life-threatening condition. No PA required, but notification requested within two business days Urgent concurrent = Emergent inpatient admission. Determination timeline within 24 hours of receipt of request Pre-service non urgent = Elective procedures. Determination within 15 calendar days Benefit limitations apply 3
4 Prior Authorization MHS Medical Management will review state guidelines and all available clinical documentation and seek Medical Director input as needed PA for observation level of care (up to 72 hours) and for diagnostic services do not require an authorization for contracted facilities. For non-diagnostic services, authorization requirements remain the same If the provider requests an inpatient level of care for a covered/eligible condition, or procedure and documentation supports an outpatient/observation level of care, we will send the case for Medical Director review 4
5 Outpatient Services Prior Authorization All elective procedures must have prior authorization from MHS at least two business days prior to the date of service All urgent and emergent services do not require prior authorization, but must be called in to MHS within two business days following the admit. Prior Authorizations are not a guarantee of payment Members must be Medicaid Eligible on the date of service *Failure to obtain prior authorization will result in a denial for related claims 5
6 Prior Authorization Transfers MHS requires notification and approval for all transfers at least two business days in advance MHS requires notification within two business days following all emergent transfers Transfers include, but are not limited to: Facility to facility Level of care changes 6
7 Prior Authorization Services that require prior authorization regardless of contract status: Injectable drugs (see mhsindiana.com/provider-guides for up-to-date list of codes) Nutritional counseling (unless diabetic) Pain management programs, including epidural, facet and trigger point injections PET, MRI, MRA and Nuclear Cardiology/SPECT scans Cardiac rehabilitation Hearing aids and devices Home and Institutional hospice (benefit limitations apply) In-home infusion therapy Orthopedic footwear Orthotics and prosthetics, if cost is greater than $250 Respiratory therapy services Pulmonary rehabilitation 7
8 Prior Authorization Is Prior Authorization Needed? MHS website mhsindiana.com Quick reference guide Non-contracted provider services require prior authorization 8

9 Are services being performed in the Emergency Department or Urgent Care Center or are these family planning services billed with a contraceptive management diagnosis? 9
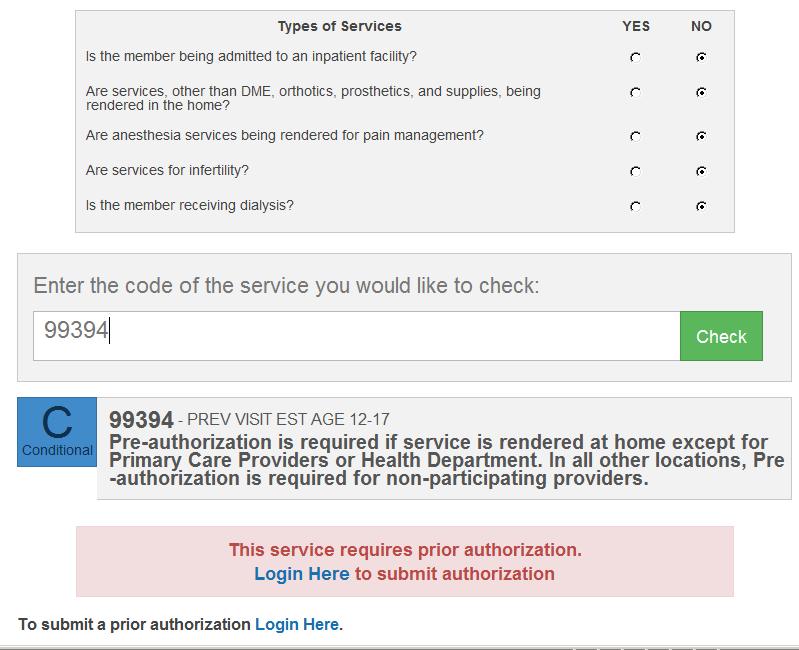
10 10
11 Information Needed to Complete All PAs: Member s Name, RID, and Date of Birth Type of service needed (e.g. office visit, outpatient surgery, DME, inpatient admission, testing, physical therapy, occupational therapy, speech therapy etc.) Date(s) of service Ordering Physician with NPI number Servicing Physician with NPI number HCPCS/CPT codes requested for approval Diagnosis code Prior Authorization Contact person, including phone and fax numbers Clinical information to support medical necessity Including current (within three months) clinical that is pertinent to the requested service, history of symptoms, previous treatment and results, physician rationale for ordering treatments and/or testing (MD exam notes) Providers must request updates to prior authorizations within 30 days from the original date of service before claim submission 11
12 Recent PA Updates 12
13 Therapy Services - (Speech, Occupational, Physical Therapy) 10/1/17 authorization is no longer required Benefit limitations are applicable Must follow billing guidelines (GP, GN, GO modifiers) National Imaging Associates, Inc. (NIA) will conduct retrospective review to evaluate medical necessity If requested, medical records can be uploaded to or faxed to NIA at Medical necessity appeals will be conducted by NIA Follow steps outlined in denial notification NIA Customer Care Associates are available to assist providers at
14 Durable & Home Medical Equipment Members and referring providers will no longer need to search for a DME provider or provider of medical supplies to service their needs Order is submitted directly to MHS, coordinated by Medline and delivered to the member Availability via Medline s web portal to submit orders and track delivery Prior authorization required by the ordering physician for all non-participating DME providers Does not apply to items provided by and billed by physician office Exclusions applicable to specific hospital based DME/HME vendors ALL requests should be initiated via MHS secure portal Web Portal: Simply go to mhsindiana.com, log into the provider portal, and click on Create Authorization. Choose DME and you will be directed to the Medline portal for order entry 14
15 Helpful Tips when requesting PA 15
16 DME PA Requests Completed certificate of medical necessity with current (from within three months) information and MD signature from within the year Medical Clearance Form These forms are on the IHCP provider website go to quick links on the right side and click forms. The form is under medical clearance forms and certifications of medical necessity. (There are also hospice forms, prior authorization forms) Physician s order Whether request is for authorization of purchase or rental Power wheelchairs must have home evaluation Enteral/Formula: Current height/weight, growth charts, nutrition history, previous testing/imaging/surgeries, current MD office visit notes related to the request 16
17 Additional Information Needed Bariatric Surgery Must include cardiac workup, pulmonary workup, diet and exercise logs, current lab reports, and psychologist report Pain Management Must have documentation of at least six weeks of therapy on area receiving treatment Include previous procedures/surgeries, medications, description of pain, any contraindications or imaging studies Include prior injection test results for injection series Home Health Physician s orders, including most recent MD notes about the issue at hand Home care plan, including home exercise program Progress notes for medical necessity determination 17
18 Outpatient Radiology PA Requests MHS partners with NIA for outpatient Radiology PA Process PA requests can be submitted NIA Web site at Not applicable for ER and Observation requests 18
19 Pharmacy PA Requests Envolve Pharmacy Solutions Preferred Drug Lists and authorization forms are available at mhsindiana.com/provider/pharmacy PA requests Phone Fax non specialty drugs Specialty drugs Pharmacy.envolvehealth.com Formulary integrated into many EHR solutions Online PA submission available through CoverMyMeds covermymeds.com Online PA forms for Specialty Drugs on mhsindiana.com 19

20 Web Portal 20
21 Web Authorization Providers can submit Prior Authorizations online via the MHS Secure Provider Portal at mhsindiana.com/login When using the portal, providers can upload supporting documentation directly Exceptions: Must submit hospice, home health and biopharmacy PA requests via fax Providers also can check authorization status on the portal 21

22 Secure Portal Registration or Login 22


23 Registration The Registration is complete and the Secure Portal homepage will be visible! Please allow hours for your account to be verified. An will be sent once access to the portal tools have been granted to the respective account. 23

24 Authorizations View, create and filter group authorizations 24

25 Create a New Authorization New Authorization Click Create Authorization Enter Member ID or Last Name and Birthdate 25


26 Creating a New Authorization Select a Service Type 26

27 Creating a New Authorization Select Provider NPI Add Primary Diagnosis 27

28 Creating a New Authorization If required Add Additional Procedures 28

29 Creating a New Authorization Service Line Details Provider Request will appear on the left side of the screen Update Servicing Provider - Check box if same as Requesting Provider - Update Servicing Provider information if not the same Update Start Date and End Date Update Total Units/Visits/Days Update Primary Procedure - Code lookup provided Add any additional procedures Add additional Service Line if applicable - All service lines added will appear on the left side of the screen 29


30 Creating a New Authorization Submit a new Authorization Confirmation Number 30

31 Telephonic 31
32 Telephone Authorization Providers can initiate Prior Authorization through the MHS referral line by calling Monday - Friday 8 a.m. to 5 p.m. (Closed for lunch from noon to 1 p.m.) After hours, MHS 24-hour nurse line available to take emergent requests. The PA process begins at MHS by speaking with the MHS non-clinical referral staff For procedures requiring additional review, we will transfer providers to a live nurse line to facilitate the PA process Please have all clinical information ready at time of call 32

33 Fax Authorization 33

34 Fax Authorization MHS Medical Management Department Member RID, name, and DOB required. Diagnosis code(s) required Check service category 34

35 Fax Authorization Enter the referring provider s information Enter the rendering provider s individual NPI#. 35
36 Fax Authorization 36
37 Exceptions to prior authorization requirements Members can see these specialists and get these services without a direct referral from their PMP: Podiatrist Chiropractor Family planning Immunizations Routine vision care Routine dental care Behavioral health by type and specialty HIV/AIDS case management Diabetes self management *Benefit limitations apply Self-referral Services 37
38 Prior Authorization Denial and Appeal Process 38
39 PA Denial and Appeal Process If MHS denies the requested service: And the member is still receiving services, the provider has the right to an expedited appeal. The attending physician must request this And the member already has been discharged, the attending physician must submit an appeal in writing within 33 days of the denial The attending physician has the right to a peer-to-peer discussion with an MHS physician Providers initiate peer-to-peer discussions and expedited appeals by calling an MHS appeals coordinator at They must request peer-to-peer within 10 days of the adverse determination *Prior authorization appeals are also known as medical necessity appeals 39
40 PA Denial and Appeal Process Send Prior Authorization/Medical Necessity Appeals to: Managed Health Services Attn: Appeals Coordinator 550 North Meridian Street, Suite 101 Indianapolis, IN Providers must initiate appeals within 33 days of the receipt of the denial letter for MHS to consider We will communicate determination to the provider within 20 business days of receipt A prior authorization appeal is different than a claim appeal request Applicable to members and non-contracted providers 40
41 Need to Know 41
42 Providers can update previously approved PAs within 30 days of the original date of service prior to claim denial for changes in: Dates of service CPT/HCPCS codes Physician Prior Authorization (PA) Request *Providers may make corrections to the existing PA as long as the claim has not been submitted 42 42
43 Prior Authorization (PA) Request MHS strives to return a decision on all PA requests within two business days of request Reasons for a delayed decision may include: Lack of information or incomplete request Illegible faxed copies of PA forms e.g. handwriting is illegible or fax is otherwise not readable Request requiring Medical Director review MHS has up to seven days to render PA decisions 43
44 Prior Authorization (PA) Request PA approval requires the need for medical necessity If your claim is denied, please contact Provider Services at to determine the cause of the denial Medical Management does not verify eligibility or benefit limitations Provider is responsible for eligibility and benefit verification 44
45 Continuity of Care PA Request MHS will honor pre-existing authorizations from any other Medicaid program during the first 30 days of enrollment or up to the expiration date of the previous authorization, whichever occurs first, and upon notification to MHS Reference: MHS Provider Manual Chapter 6 45
46 MHS Provider Relations Team Candace Ervin Envolve Dental Indiana Provider Relations ext Chad Pratt Provider Relations Specialist Northeast Region ext Tawanna Danzie Provider Relations Specialist Northwest Region ext Jennifer Garner Provider Relations Specialist Southeast Region ext Taneya Wagaman Provider Relations Specialist Central Region ext Katherine Gibson Provider Relations Specialist North Central Region ext Esther Cervantes Provider Relations Specialist South West Region ext Mary Schermer Behavioral Health Provider Relations Specialist - West Region ext mary.schermer@envolvehealth.com LaKisha Browder Behavioral Health Provider Relations Specialist - East Region ext lakisha.browder@envolvehealth.com
47 Review Learned about the PA process and timelines Highlighted the recent change regarding DME/HME and Therapy PA requirements Reviewed PA submission options Reviewed the Appeals Process 47
48 Questions Thank you for partnering with MHS 48
MHS CMS 1500 Tips and Billing Guidelines
 MHS CMS 1500 Tips and Billing Guidelines AGENDA Creating Claim on MHS Web Portal Claim Process Claim Rejection Claim Denial Claim Adjustment Dispute Resolution Taxonomy Eligibility Reviewing Claims DME
MHS CMS 1500 Tips and Billing Guidelines AGENDA Creating Claim on MHS Web Portal Claim Process Claim Rejection Claim Denial Claim Adjustment Dispute Resolution Taxonomy Eligibility Reviewing Claims DME
MHS Secure Provider Web Portal Overview 0718.MA.P.PP 8/18
 MHS Secure Provider Web Portal Overview 0718.MA.P.PP 8/18 Agenda Save Time by Utilizing the MHS Secure Web Portal: Administration Quality Reports Eligibility Member Record Patient List Authorizations Claims
MHS Secure Provider Web Portal Overview 0718.MA.P.PP 8/18 Agenda Save Time by Utilizing the MHS Secure Web Portal: Administration Quality Reports Eligibility Member Record Patient List Authorizations Claims
MHS UB Tips and Billing Guidelines 0418.PR.P.PP 5/18
 MHS UB 04 2018 Tips and Billing Guidelines 0418.PR.P.PP 5/18 Agenda Claim Process Claim Process Common Claim Rejections Common Claim Denials Claim Adjustments Claims Dispute Resolution Prior Authorization
MHS UB 04 2018 Tips and Billing Guidelines 0418.PR.P.PP 5/18 Agenda Claim Process Claim Process Common Claim Rejections Common Claim Denials Claim Adjustments Claims Dispute Resolution Prior Authorization
0518.PR.P.PP.2 7/18. The Ins and Outs of CMS 1500 Billing
 0518.PR.P.PP.2 7/18 The Ins and Outs of CMS 1500 Billing AGENDA Claim Process Creating Claim on MHS Web Portal Reviewing Claims Claim Denial Claim Adjustment Dispute Resolution Taxonomy Allwell Information
0518.PR.P.PP.2 7/18 The Ins and Outs of CMS 1500 Billing AGENDA Claim Process Creating Claim on MHS Web Portal Reviewing Claims Claim Denial Claim Adjustment Dispute Resolution Taxonomy Allwell Information
MHS UB-04 Billing and Claim Processing Tips and Billing Guidelines
 MHS UB-04 Billing and Claim Processing Tips and Billing Guidelines 1 1015.PR.P.PP 10/15 Agenda Who is MHS? Claim Process Filing Process Common Claim Rejections Common Claim Denials Claim Adjustments Claims
MHS UB-04 Billing and Claim Processing Tips and Billing Guidelines 1 1015.PR.P.PP 10/15 Agenda Who is MHS? Claim Process Filing Process Common Claim Rejections Common Claim Denials Claim Adjustments Claims
Welcome to Managed Health Services (MHS) 0717.PR.P.PP 10/17
 0717.PR.P.PP 10/17") Welcome to Managed Health Services (MHS) 0717.PR.P.PP 10/17 Agenda MHS Overview Health Programs Claim Process Prior Authorization Process HEDIS Coordinated Care Programs MHS Partnership Ambetter Questions
Welcome to Managed Health Services (MHS) 0717.PR.P.PP 10/17 Agenda MHS Overview Health Programs Claim Process Prior Authorization Process HEDIS Coordinated Care Programs MHS Partnership Ambetter Questions
MHS Updates Summer PR.P.PP
 MHS Updates Summer 2017 0517.PR.P.PP Updates Important to You Prior Authorization (PA) Updates DME Changes Therapy Authorization Process MHS Prior Authorization 101 Home Health MHS Occurrence Prior Authorization
MHS Updates Summer 2017 0517.PR.P.PP Updates Important to You Prior Authorization (PA) Updates DME Changes Therapy Authorization Process MHS Prior Authorization 101 Home Health MHS Occurrence Prior Authorization
Calendar Year Medical Deductible Calendar Year Out-of-Pocket Maximum $2,000 per individual / $4,000 per family Lifetime Benefit Maximum
 An independent member of the Blue Shield Association Access+HMO Per Admit 20-500 Benefit Summary (For groups of 101 and above) (Uniform Health Plan Benefits and Coverage Matrix) Blue Shield of California
An independent member of the Blue Shield Association Access+HMO Per Admit 20-500 Benefit Summary (For groups of 101 and above) (Uniform Health Plan Benefits and Coverage Matrix) Blue Shield of California
Secure Provider Web Portal Overview 0917.MA.P.PP
 Secure Provider Web Portal Overview 0917.MA.P.PP Agenda Secure Web Portal Administration Quality Reports Eligibility Member Record Patient List Authorizations Claims Review Claims Secure Messaging Administration
Secure Provider Web Portal Overview 0917.MA.P.PP Agenda Secure Web Portal Administration Quality Reports Eligibility Member Record Patient List Authorizations Claims Review Claims Secure Messaging Administration
Full PPO Combined Deductible /60 Benefit Summary (For groups of 101 and above) (Uniform Health Plan Benefits and Coverage Matrix)
 (Uniform Health Plan Benefits and Coverage Matrix)") An independent member of the Blue Shield Association Full PPO Combined Deductible 25-250 90/60 Benefit Summary (For groups of 101 and above) (Uniform Health Plan Benefits and Coverage Matrix) Blue Shield
An independent member of the Blue Shield Association Full PPO Combined Deductible 25-250 90/60 Benefit Summary (For groups of 101 and above) (Uniform Health Plan Benefits and Coverage Matrix) Blue Shield
CareCore National Musculoskeletal Management Program Physical Medicine and Therapy Frequently Asked Questions
 EVIDENCE-BASED HEALTHCARE SOLUTIONS CareCore National Physical Medicine and Therapy Prepared for December 2, 2014 Table of Contents Introduction to CareCore National... 3 Who is CareCore National?... 3
EVIDENCE-BASED HEALTHCARE SOLUTIONS CareCore National Physical Medicine and Therapy Prepared for December 2, 2014 Table of Contents Introduction to CareCore National... 3 Who is CareCore National?... 3
Benefit modifications for members with Full PPO /60
 An independent licensee of the Blue Shield Association A17436 (01/2017) Benefit modifications for members with Full PPO 250 80/60 Effective January 1, 2017 The Full PPO 250 80/60 plan name will be changed
An independent licensee of the Blue Shield Association A17436 (01/2017) Benefit modifications for members with Full PPO 250 80/60 Effective January 1, 2017 The Full PPO 250 80/60 plan name will be changed
and cardiac diagnostic procedures utilizing nuclear medicine) Bariatric surgery Not Covered Not Covered
 Bariatric surgery Not Covered Not Covered") An independent member of the Blue Shield Association Wesco Aircraft ASO PPO Benefit Summary (For groups of 300 and above) (Uniform Health Plan Benefits and Coverage Matrix) Blue Shield of California Effective:
An independent member of the Blue Shield Association Wesco Aircraft ASO PPO Benefit Summary (For groups of 300 and above) (Uniform Health Plan Benefits and Coverage Matrix) Blue Shield of California Effective:
Frequently Asked Questions Durable Medical Equipment, Prosthetics, Orthotics and Medical Supplies (DMEPOS) Management Program
 Management Program") Frequently Asked Questions Durable Medical Equipment, Prosthetics, Orthotics and Medical Supplies (DMEPOS) Management Program Northwood, Inc. (Northwood) is Well Sense Health Plan s (Well Sense) Durable
Frequently Asked Questions Durable Medical Equipment, Prosthetics, Orthotics and Medical Supplies (DMEPOS) Management Program Northwood, Inc. (Northwood) is Well Sense Health Plan s (Well Sense) Durable
Member Cost Sharing Participating Provider Non-Participating Provider Annual Deductible Individual $250 $750 Family $750 $2,250
 Schedule of Benefits UPMC Business Advantage PPO - Premium Network Deductible: $250 / $750 Coinsurance: 0% Total Annual Out-of-Pocket: $6,350 / $12,700 Primary Care Provider: $20 Copayment per visit Specialist:
Schedule of Benefits UPMC Business Advantage PPO - Premium Network Deductible: $250 / $750 Coinsurance: 0% Total Annual Out-of-Pocket: $6,350 / $12,700 Primary Care Provider: $20 Copayment per visit Specialist:
Medical EPO Plan Schedule of Benefits (Effective January 01, 2019) JHH/JHHSC Non-Union and Union Employees and Eligible Dependents
 JHH/JHHSC Non-Union and Union Employees and Eligible Dependents") Plan Year Deductible Out-of-Pocket Maximum Lifetime Maximum Hopkins Preferred Network Provider EHP Network Provider Individual $500 $500 Family $1000 $1000 Individual $3000 (combined with EHP Network)
Plan Year Deductible Out-of-Pocket Maximum Lifetime Maximum Hopkins Preferred Network Provider EHP Network Provider Individual $500 $500 Family $1000 $1000 Individual $3000 (combined with EHP Network)
Section Eleven. Referrals and Prior Authorization REFERRAL PROCESS. Physician Referrals within Plan Network
 REFERRAL PROCESS Physician Referrals within Plan Network Physicians may refer members to any Specialty Care Physician (Specialist) or ancillary provider within the Fidelis Care network. Except as noted
REFERRAL PROCESS Physician Referrals within Plan Network Physicians may refer members to any Specialty Care Physician (Specialist) or ancillary provider within the Fidelis Care network. Except as noted
Summary of Benefits Custom HMO Zero Admit 10
 Summary of Benefits Custom HMO Zero Admit 10 City of Delano Effective July 1, 2019 HMO Benefit Plan This Summary of Benefits shows the amount you will pay for Covered Services under this Blue Shield of
Summary of Benefits Custom HMO Zero Admit 10 City of Delano Effective July 1, 2019 HMO Benefit Plan This Summary of Benefits shows the amount you will pay for Covered Services under this Blue Shield of
evicore healthcare Utilization management programs Frequently asked questions
 evicore healthcare Utilization management programs Frequently asked questions Who is evicore? evicore is a specialty medical benefits management company that provides utilization management services for
evicore healthcare Utilization management programs Frequently asked questions Who is evicore? evicore is a specialty medical benefits management company that provides utilization management services for
Medical EPO Plan Schedule of Benefits (Effective January 01, 2019) Howard County General Hospital/TCAS Employees and Eligible Dependents
 Howard County General Hospital/TCAS Employees and Eligible Dependents") Plan Year Deductible Out-of-Pocket Maximum Lifetime Maximum Hopkins Affiliated Facility Network (facility charges only) EHP Network Provider Individual $500 $500 Family $1000 $1000 Individual $3000 (combined
Plan Year Deductible Out-of-Pocket Maximum Lifetime Maximum Hopkins Affiliated Facility Network (facility charges only) EHP Network Provider Individual $500 $500 Family $1000 $1000 Individual $3000 (combined
Summary of Benefits. Custom PPO Combined Deductible /60. City of Reedley Effective January 1, 2018 PPO Benefit Plan
 Blue Shield of California is an independent member of the Blue Shield Association Summary of Benefits Custom PPO Combined Deductible 35-500 80/60 City of Reedley Effective January 1, 2018 PPO Benefit Plan
Blue Shield of California is an independent member of the Blue Shield Association Summary of Benefits Custom PPO Combined Deductible 35-500 80/60 City of Reedley Effective January 1, 2018 PPO Benefit Plan
Medical Schedule of Benefits (Effective January 01, 2016) Johns Hopkins Bayview Medical Center Non-Union and Union Employees and Eligible Dependents
 Johns Hopkins Bayview Medical Center Non-Union and Union Employees and Eligible Dependents") Plan Year Deductible Out-of-Pocket Maximum Lifetime Maximum EHP Network Provider Out of Network Provider Hopkins Preferred Network Provider Individual $100 $750 $0 Family $200 $1500 $0 Individual $2000
Plan Year Deductible Out-of-Pocket Maximum Lifetime Maximum EHP Network Provider Out of Network Provider Hopkins Preferred Network Provider Individual $100 $750 $0 Family $200 $1500 $0 Individual $2000
Summary of Benefits City of Santa Monica Custom Trio HMO Per Admit
 Summary of Benefits City of Santa Monica Custom Trio HMO Per Admit 20-100 City of Santa Monica Effective January 1, 2019 HMO Benefit Plan This Summary of Benefits shows the amount you will pay for Covered
Summary of Benefits City of Santa Monica Custom Trio HMO Per Admit 20-100 City of Santa Monica Effective January 1, 2019 HMO Benefit Plan This Summary of Benefits shows the amount you will pay for Covered
Summary of Benefits Access+HMO Zero Admit 20
 Blue Shield of California is an independent member of the Blue Shield Association Summary of Benefits Access+HMO Zero Admit 20 Group Plan HMO Benefit Plan This Summary of Benefits shows the amount you
Blue Shield of California is an independent member of the Blue Shield Association Summary of Benefits Access+HMO Zero Admit 20 Group Plan HMO Benefit Plan This Summary of Benefits shows the amount you
Wesco Aircraft Hardware Corp Effective January 1, 2018 HMO Benefit Plan Wesco Aircraft Custom Access+ HMO Facility Deductible 25-20%/200
 Blue Shield of California is an independent member of the Blue Shield Association Summary of Benefits Wesco Aircraft Hardware Corp Effective January 1, 2018 HMO Benefit Plan Wesco Aircraft Custom Access+
Blue Shield of California is an independent member of the Blue Shield Association Summary of Benefits Wesco Aircraft Hardware Corp Effective January 1, 2018 HMO Benefit Plan Wesco Aircraft Custom Access+
Effective: July 1, Highlights: A description of the prescription drug coverage is provided separately. Participating Providers 1
 High Desert & Inland Trust Custom PPO 3 Benefit Summary (For groups of 300 and above) (Uniform Health Plan Benefits and Coverage Matrix) Blue Shield of California Effective: July 1, 2016 THIS MATRIX IS
High Desert & Inland Trust Custom PPO 3 Benefit Summary (For groups of 300 and above) (Uniform Health Plan Benefits and Coverage Matrix) Blue Shield of California Effective: July 1, 2016 THIS MATRIX IS
Medical PPO Plan Schedule of Benefits (Effective January 01, 2019) Bayview Non-Union and Union Employees and Eligible Dependents
 Bayview Non-Union and Union Employees and Eligible Dependents") Plan Year Deductible Out-of-Pocket Maximum Lifetime Maximum Individual Family Individual Family Hopkins Preferred Network Provider EHP Network Provider Out of Network Provider $150 (under $50K) / $200
Plan Year Deductible Out-of-Pocket Maximum Lifetime Maximum Individual Family Individual Family Hopkins Preferred Network Provider EHP Network Provider Out of Network Provider $150 (under $50K) / $200
CMS-1500 professional providers 2017 annual workshop
 Serving Hoosier Healthwise, Healthy Indiana Plan CMS-1500 professional providers 2017 annual workshop Reminders and updates The (Anthem) Provider Manual was updated in July 2017. The provider manual is
Serving Hoosier Healthwise, Healthy Indiana Plan CMS-1500 professional providers 2017 annual workshop Reminders and updates The (Anthem) Provider Manual was updated in July 2017. The provider manual is
SERVICES WITH A 1 MAY REQUIRE PRIOR AUTHORIZATION
 Monthly Plan Premium YOU PAY $0 You must continue to pay your Medicare Part C Deductible YOU PAY nothing This plan does not have a medical Maximum Out of Pocket $6,000 annually The most you pay for Copayments,
Monthly Plan Premium YOU PAY $0 You must continue to pay your Medicare Part C Deductible YOU PAY nothing This plan does not have a medical Maximum Out of Pocket $6,000 annually The most you pay for Copayments,
Annual Notice of Changes for 2016
 Secure Blue Idaho, (PPO) offered by Blue Cross of Idaho Care Plus, Inc. Annual Notice of Changes for 2016 You are currently enrolled as a member of Secure Blue Idaho (PPO). Next year, there will be some
Secure Blue Idaho, (PPO) offered by Blue Cross of Idaho Care Plus, Inc. Annual Notice of Changes for 2016 You are currently enrolled as a member of Secure Blue Idaho (PPO). Next year, there will be some
Medical Schedule of Benefits (Effective July 01, June 30, 2019) Johns Hopkins Student Health Program
 Johns Hopkins Student Health Program") Plan Year Deductible Out-of-Pocket Maximum Lifetime Maximum EHP Network Provider Out of Network Provider Individual $150 $150 Family $450 $450 Individual $3000 $3000 Family $9000 $9000 Unlimited Acupuncture
Plan Year Deductible Out-of-Pocket Maximum Lifetime Maximum EHP Network Provider Out of Network Provider Individual $150 $150 Family $450 $450 Individual $3000 $3000 Family $9000 $9000 Unlimited Acupuncture
Summary of Benefits Full PPO Savings Two-Tier Embedded Deductible 1500/2700/3000
 Blue Shield of California is an independent member of the Blue Shield Association Summary of Benefits Full PPO Savings Two-Tier Embedded Deductible 1500/2700/3000 Group Plan PPO Savings Benefit Plan This
Blue Shield of California is an independent member of the Blue Shield Association Summary of Benefits Full PPO Savings Two-Tier Embedded Deductible 1500/2700/3000 Group Plan PPO Savings Benefit Plan This
Molina/BMS 2012 Provider Workshops IRG d/b/a APS Healthcare, Inc. Updates. Presented by: Helen C. Snyder, Associate Director
 Molina/BMS 2012 Provider Workshops IRG d/b/a APS Healthcare, Inc. Updates Presented by: Helen C. Snyder, Associate Director Updates Provider Registration with APS v. Molina Medicaid enrollment Eligibility/Provider
Molina/BMS 2012 Provider Workshops IRG d/b/a APS Healthcare, Inc. Updates Presented by: Helen C. Snyder, Associate Director Updates Provider Registration with APS v. Molina Medicaid enrollment Eligibility/Provider
Full PPO Savings Two-Tier Embedded Deductible 2250/2700/4500 Effective January 1, 2019
 Benefit Modification for Members with Full PPO Savings Two-Tier Embedded Deductible 2250/2700/4500 Effective January 1, 2019 This chart is a summary of specific benefit changes to your plan. For a list
Benefit Modification for Members with Full PPO Savings Two-Tier Embedded Deductible 2250/2700/4500 Effective January 1, 2019 This chart is a summary of specific benefit changes to your plan. For a list
Anthem Blue Cross Your Plan: Premier HMO 20/200 admit/100 OP (Essential Formulary $10/$25/$45/30%) Your Network: California Care HMO
 Your Network: California Care HMO") Anthem Blue Cross Your Plan: Premier HMO 20/200 admit/100 OP (Essential Formulary $10/$25/$45/30%) Your Network: California Care HMO This summary of benefits is a brief outline of coverage, designed to
Anthem Blue Cross Your Plan: Premier HMO 20/200 admit/100 OP (Essential Formulary $10/$25/$45/30%) Your Network: California Care HMO This summary of benefits is a brief outline of coverage, designed to
California Small Group MC Aetna Life Insurance Company NETWORK CARE
 PLAN FEATURES Deductible (per calendar year) Unless otherwise indicated, the Deductible must be met prior to benefits being payable. All covered expenses accumulate toward the preferred and non-preferred
PLAN FEATURES Deductible (per calendar year) Unless otherwise indicated, the Deductible must be met prior to benefits being payable. All covered expenses accumulate toward the preferred and non-preferred
Emergency Department: $175 Copayment per visit Coinsurance: 0%
 Schedule of Benefits UPMC Small Business Advantage Primary Care Provider: $25 Copayment per visit Gold PPO $1,000 $25/$50 - Premium Network Specialist: $50 Copayment per visit Deductible: $1,000 / $2,000
Schedule of Benefits UPMC Small Business Advantage Primary Care Provider: $25 Copayment per visit Gold PPO $1,000 $25/$50 - Premium Network Specialist: $50 Copayment per visit Deductible: $1,000 / $2,000
Anthem BlueCross BlueShield Christian Care Communities Blue Access PPO Coverage Period: 01/01/ /31/2015 Summary of Benefits and Coverage:
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.anthem.com or by calling 1-888-650-4047. Important Questions
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.anthem.com or by calling 1-888-650-4047. Important Questions
For more information on your plan, please refer to the final page of this document.
 Schedule of Benefits Panther Blue - General Student Health Plan PPO - Premium Network Deductible: $250 / $500 Coinsurance: 10% Total Annual Out-of-Pocket: $4,200 / $8,400 This document is your Schedule
Schedule of Benefits Panther Blue - General Student Health Plan PPO - Premium Network Deductible: $250 / $500 Coinsurance: 10% Total Annual Out-of-Pocket: $4,200 / $8,400 This document is your Schedule
Medical Schedule of Benefits (Effective January 01, December 31, 2017) Johns Hopkins University Employees and Eligible Dependents
 Johns Hopkins University Employees and Eligible Dependents") Plan Year Deductible Out-of-Pocket Maximum Lifetime Maximum EHP Network Provider Out of Network Provider Individual $250 $500 Family $750 $1500 Individual $2000 $4000 Family $6000 $12000 Unlimited Acupuncture
Plan Year Deductible Out-of-Pocket Maximum Lifetime Maximum EHP Network Provider Out of Network Provider Individual $250 $500 Family $750 $1500 Individual $2000 $4000 Family $6000 $12000 Unlimited Acupuncture
The Deductible is applicable to all covered services except for flat dollar Copayment services.
 PRIORITY HEALTH www.priorityhealth.com/mpsers PRIORITYHMO SM PLUS PLAN MICHIGAN PUBLIC SCHOOL EMPLOYEES RETIREMENT SYSTEM (MPSERS) Effective January 1, 2017 through December 31, 2017 The HMO Plus plan
PRIORITY HEALTH www.priorityhealth.com/mpsers PRIORITYHMO SM PLUS PLAN MICHIGAN PUBLIC SCHOOL EMPLOYEES RETIREMENT SYSTEM (MPSERS) Effective January 1, 2017 through December 31, 2017 The HMO Plus plan
Anthem Blue Cross Your Plan: Premier HMO 10/100% - MUST Trust Your Network: California Care HMO
 Anthem Blue Cross Your Plan: Premier HMO 10/100% - MUST Trust Your Network: California Care HMO This summary of benefits is a brief outline of coverage, designed to help you with the selection process.
Anthem Blue Cross Your Plan: Premier HMO 10/100% - MUST Trust Your Network: California Care HMO This summary of benefits is a brief outline of coverage, designed to help you with the selection process.
Important Questions Answers Why this Matters:
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at https://eoc.anthem.com/eocdps/aso or by calling (855) 333-5735.
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at https://eoc.anthem.com/eocdps/aso or by calling (855) 333-5735.
Annual Notice of Changes for 2016
 True Blue Rx Option I (HMO-POS) offered by Blue Cross of Idaho Care Plus, Inc. Annual Notice of Changes for 2016 You are currently enrolled as a member of True Blue RX Option I (HMO-POS). Next year, there
True Blue Rx Option I (HMO-POS) offered by Blue Cross of Idaho Care Plus, Inc. Annual Notice of Changes for 2016 You are currently enrolled as a member of True Blue RX Option I (HMO-POS). Next year, there
Standard Option Medical Schedule of Benefits (Effective January 01, 2017) Suburban Hospital Employees and Eligible Dependents
 Suburban Hospital Employees and Eligible Dependents") Plan Year Deductible Out-of-Pocket Maximum Lifetime Maximum EHP Network Provider Out of Network Provider Suburban Hospital (facility charges only) Individual $400 $750 $0 Family $800 $1500 $0 Individual
Plan Year Deductible Out-of-Pocket Maximum Lifetime Maximum EHP Network Provider Out of Network Provider Suburban Hospital (facility charges only) Individual $400 $750 $0 Family $800 $1500 $0 Individual
Auxiliary Organizations Association
 Auxiliary Organizations Association Your Plan: Modified Premier HMO 20/200 admit/100 OP (Modified RX $5/$20/$60/20%) Your Network: California Care HMO This summary of benefits is a brief outline of coverage,
Auxiliary Organizations Association Your Plan: Modified Premier HMO 20/200 admit/100 OP (Modified RX $5/$20/$60/20%) Your Network: California Care HMO This summary of benefits is a brief outline of coverage,
Standard Option Medical Schedule of Benefits (Effective January 01, 2018) Suburban Hospital Employees and Eligible Dependents
 Suburban Hospital Employees and Eligible Dependents") Plan Year Deductible Out-of-Pocket Maximum Lifetime Maximum EHP Network Provider Out of Network Provider Suburban Hospital (facility charges only) Individual $400 $750 $0 Family $800 $1500 $0 Individual
Plan Year Deductible Out-of-Pocket Maximum Lifetime Maximum EHP Network Provider Out of Network Provider Suburban Hospital (facility charges only) Individual $400 $750 $0 Family $800 $1500 $0 Individual
Schedule of Benefits. Plan Information Participating Provider Non-Participating Provider. Deductible: $250 / $750 Rx: $10/$25/$40/$40 Coinsurance: 0%
 Schedule of Benefits UPMC Business Advantage PPO - Premium Network Primary Care Provider: $20 Copayment per visit Specialist: $20 Copayment per visit Deductible: $250 / $750 Rx: $10/$25/$40/$40 Coinsurance:
Schedule of Benefits UPMC Business Advantage PPO - Premium Network Primary Care Provider: $20 Copayment per visit Specialist: $20 Copayment per visit Deductible: $250 / $750 Rx: $10/$25/$40/$40 Coinsurance:
Cost if you use a Non-Network Provider. Cost if you use an In-Network Provider. Covered Medical Benefits
 Anthem Blue Cross California State University Risk Management Authority Your Plan: Custom Premier HMO 20/200 admit/100 OP (Custom Rx $5/$20/$60/20%) Your Network: California Care HMO This summary of benefits
Anthem Blue Cross California State University Risk Management Authority Your Plan: Custom Premier HMO 20/200 admit/100 OP (Custom Rx $5/$20/$60/20%) Your Network: California Care HMO This summary of benefits
Anthem Blue Cross Your Plan: Classic HMO 20/40/250 Admit /125 OP Your Network: Select HMO
 Anthem Blue Cross Your Plan: Classic HMO 20/40/250 Admit /125 OP Your Network: Select HMO This summary of benefits is a brief outline of coverage, designed to help you with the selection process. This
Anthem Blue Cross Your Plan: Classic HMO 20/40/250 Admit /125 OP Your Network: Select HMO This summary of benefits is a brief outline of coverage, designed to help you with the selection process. This
Medical Schedule of Benefits (Effective July 01, June 30, 2018) Johns Hopkins Student Health Program
 Johns Hopkins Student Health Program") Plan Year Deductible Out-of-Pocket Maximum Lifetime Maximum EHP Network Provider Out of Network Provider Individual $150 $150 Family $450 $450 Individual $3000 $3000 Family $9000 $9000 Unlimited Acupuncture
Plan Year Deductible Out-of-Pocket Maximum Lifetime Maximum EHP Network Provider Out of Network Provider Individual $150 $150 Family $450 $450 Individual $3000 $3000 Family $9000 $9000 Unlimited Acupuncture
2015 Benefits Overview
 2015 Benefits Overview ASPIRE HEALTH ADVANTAGE VALUE (HMO) BENEFIT Monthly Plan Premium Out-of-Pocket Limit (In-Network Medicare-covered benefits) Annual Part C Deductible (all services except for Prescription
2015 Benefits Overview ASPIRE HEALTH ADVANTAGE VALUE (HMO) BENEFIT Monthly Plan Premium Out-of-Pocket Limit (In-Network Medicare-covered benefits) Annual Part C Deductible (all services except for Prescription
California Small Group MC Aetna Life Insurance Company
 PLAN FEATURES Deductible (per calendar year) $5,000 Individual $10,000 Family Unless otherwise indicated, the Deductible must be met prior to benefits being payable. All covered expenses accumulate toward
PLAN FEATURES Deductible (per calendar year) $5,000 Individual $10,000 Family Unless otherwise indicated, the Deductible must be met prior to benefits being payable. All covered expenses accumulate toward
Important Questions Answers Why this Matters:
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at https://eoc.anthem.com/eocdps/fi or by calling (855) 333-5735.
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at https://eoc.anthem.com/eocdps/fi or by calling (855) 333-5735.
Your Plan: 2018 HMO Plan (2940) Your Network: California Care HMO
 Your Network: California Care HMO") Anthem Blue Cross Your Plan: 2018 HMO Plan (2940) Your : California Care HMO ACWA JPIA C00361 This summary of benefits is a brief outline of coverage, designed to help you with the selection process. This
Anthem Blue Cross Your Plan: 2018 HMO Plan (2940) Your : California Care HMO ACWA JPIA C00361 This summary of benefits is a brief outline of coverage, designed to help you with the selection process. This
All covered expenses accumulate separately toward the Network and Out-of-Network Coinsurance Maximum.
 PLAN FEATURES Network Managed Choice POS (Open Access) Primary Care Physician Selection Not Applicable Deductible (per calendar year) $250 per member (2-member maximum) Unless otherwise indicated, the
PLAN FEATURES Network Managed Choice POS (Open Access) Primary Care Physician Selection Not Applicable Deductible (per calendar year) $250 per member (2-member maximum) Unless otherwise indicated, the
NETWORK CARE. $4,500 Individual. (2-member maximum)
") PLAN FEATURES Network Open Choice PPO Primary Care Physician Selection Deductible (per calendar year) Not Applicable $750 per member Not Applicable $750 per member (2-member maximum) (2-member maximum)
PLAN FEATURES Network Open Choice PPO Primary Care Physician Selection Deductible (per calendar year) Not Applicable $750 per member Not Applicable $750 per member (2-member maximum) (2-member maximum)
Version: 15/02/2017 [ TPID: ] Page 1
![Version: 15/02/2017 [ TPID: ] Page 1](/thumbs/88/117441870.jpg "Version: 15/02/2017 [ TPID: ] Page 1") PLAN FEATURES NETWORK CARE OUT-OF-NETWORK CARE Primary Care Physician Selection Not required Not required Deductible (per calendar year) $1,500 Individual $3,000 Family $3,000 Individual $9,000 Family
PLAN FEATURES NETWORK CARE OUT-OF-NETWORK CARE Primary Care Physician Selection Not required Not required Deductible (per calendar year) $1,500 Individual $3,000 Family $3,000 Individual $9,000 Family
NIA Frequently Asked Questions (FAQ s) For Dean Health Plan Providers
 For Dean Health Plan Providers") Question GENERAL Why does Dean Health Plan utilize an outpatient imaging program? Why did select National Imaging Associates, Inc. (NIA) to manage its outpatient advanced imaging NIA Frequently Asked Questions
Question GENERAL Why does Dean Health Plan utilize an outpatient imaging program? Why did select National Imaging Associates, Inc. (NIA) to manage its outpatient advanced imaging NIA Frequently Asked Questions
PLAN DESIGN AND BENEFITS - Tx OAMC % 08 PREFERRED CARE
 Aetna Life Insurance Company Texas Small Group MC Open Access Plan Effective Date: 11/01/2008 PLAN FEATURES Deductible (per calendar year) $1,000 Individual $3,000 Individual $3,000 3 Individuals per $9,000
Aetna Life Insurance Company Texas Small Group MC Open Access Plan Effective Date: 11/01/2008 PLAN FEATURES Deductible (per calendar year) $1,000 Individual $3,000 Individual $3,000 3 Individuals per $9,000
Your Plan: 2017 HMO Value Plan (0KGJ) Your Network: California Care HMO
 Your Network: California Care HMO") Anthem Blue Cross Your Plan: 2017 HMO Value Plan (0KGJ) Your : California Care HMO ACWA JPIA C00361 This summary of benefits is a brief outline of coverage, designed to help you with the selection process.
Anthem Blue Cross Your Plan: 2017 HMO Value Plan (0KGJ) Your : California Care HMO ACWA JPIA C00361 This summary of benefits is a brief outline of coverage, designed to help you with the selection process.
Prior Authorizations on the Provider Portal. July 2017
 Prior Authorizations on the Provider Portal July 2017 2 Disclaimer The information provided is current as of June 2017 and is subject to change. Stay current with up-to-date information on the OHCA public
Prior Authorizations on the Provider Portal July 2017 2 Disclaimer The information provided is current as of June 2017 and is subject to change. Stay current with up-to-date information on the OHCA public
Frequently Asked Questions Radiology Prior Authorization Program for the UnitedHealthcare Community Plan, Arizona
 Doc #: UHC1782m_20120305 Frequently Asked Questions Radiology Prior Authorization Program for the UnitedHealthcare Community Plan, Arizona 1. What is the UnitedHealthcare Radiology Prior Authorization
Doc #: UHC1782m_20120305 Frequently Asked Questions Radiology Prior Authorization Program for the UnitedHealthcare Community Plan, Arizona 1. What is the UnitedHealthcare Radiology Prior Authorization
NETWORK CARE Managed Choice POS (Open Access)
") PLAN FEATURES Network Primary Care Physician Selection Deductible (per calendar year) Managed Choice POS (Open Access) Unless otherwise indicated, the Deductible must be met prior to benefits being payable.
PLAN FEATURES Network Primary Care Physician Selection Deductible (per calendar year) Managed Choice POS (Open Access) Unless otherwise indicated, the Deductible must be met prior to benefits being payable.
Important Questions Answers Why this Matters:
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.anthem.com or by calling 1-800-843-6447. Important Questions
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.anthem.com or by calling 1-800-843-6447. Important Questions
CMS 1450 (UB-04) institutional providers
 institutional providers") Serving Hoosier Healthwise, Healthy Indiana Plan CMS 1450 (UB-04) institutional providers 2017 Annual Workshop Reminders and updates The provider manual was updated in July 2017. The provider manual is
Serving Hoosier Healthwise, Healthy Indiana Plan CMS 1450 (UB-04) institutional providers 2017 Annual Workshop Reminders and updates The provider manual was updated in July 2017. The provider manual is
2019 Summary of Benefits
 Your health. Our focus. 2019 Summary of Benefits Health Partners Medicare Special (HMO SNP) 2019 Summary of Benefits Health Partners Medicare (H9207) Health Partners Medicare Special (HMO SNP) (plan 004)
Your health. Our focus. 2019 Summary of Benefits Health Partners Medicare Special (HMO SNP) 2019 Summary of Benefits Health Partners Medicare (H9207) Health Partners Medicare Special (HMO SNP) (plan 004)
North Carolina Small Group Indemnity Aetna Life Insurance Company Plan Effective Date: 10/01/2010
 PLAN FEATURES [Deductible (per calendar year) $1,000 Individual $3,000 Family Unless otherwise indicated, the Deductible must be met prior to benefits being payable. Member cost sharing for for prescription
PLAN FEATURES [Deductible (per calendar year) $1,000 Individual $3,000 Family Unless otherwise indicated, the Deductible must be met prior to benefits being payable. Member cost sharing for for prescription
MEMBER COST SHARE. 20% after deductible
 PLAN FEATURES Network Not Applicable Primary Care Physician Selection Not Applicable Deductible (per calendar year) $500 Individual (2-member maximum) Unless otherwise indicated, the Deductible must be
PLAN FEATURES Network Not Applicable Primary Care Physician Selection Not Applicable Deductible (per calendar year) $500 Individual (2-member maximum) Unless otherwise indicated, the Deductible must be
Your Plan: 2018 Classic PPO Plan (1122 and ZOJZ) Your Network: Prudent Buyer PPO
 Your Network: Prudent Buyer PPO") Anthem Blue Cross Your Plan: 2018 Classic PPO Plan (1122 and ZOJZ) Your : Prudent Buyer PPO ACWA JPIA C00361 This summary of benefits is a brief outline of coverage, designed to help you with the selection
Anthem Blue Cross Your Plan: 2018 Classic PPO Plan (1122 and ZOJZ) Your : Prudent Buyer PPO ACWA JPIA C00361 This summary of benefits is a brief outline of coverage, designed to help you with the selection
Schedule of Benefits. Plan Information Participating Provider Non-Participating Provider
 Schedule of Benefits Panther Basic HSA PPO - Premium Network Deductible: $1,500 / $3,000 Coinsurance: 30% Total Annual Out-of-Pocket: $5,000 / $10,000 Primary Care Provider: 30% after Deductible Specialist:
Schedule of Benefits Panther Basic HSA PPO - Premium Network Deductible: $1,500 / $3,000 Coinsurance: 30% Total Annual Out-of-Pocket: $5,000 / $10,000 Primary Care Provider: 30% after Deductible Specialist:
Your Plan: 2018 Advantage PPO Plan (S828 and Z0KC) Your Network: Prudent Buyer PPO
 Your Network: Prudent Buyer PPO") Anthem Blue Cross Your Plan: 2018 Advantage PPO Plan (S828 and Z0KC) Your : Prudent Buyer PPO ACWA JPIA C00361 This summary of benefits is a brief outline of coverage, designed to help you with the selection
Anthem Blue Cross Your Plan: 2018 Advantage PPO Plan (S828 and Z0KC) Your : Prudent Buyer PPO ACWA JPIA C00361 This summary of benefits is a brief outline of coverage, designed to help you with the selection
Johns Hopkins HealthCare LLC
 Johns Hopkins HealthCare LLC Johns Hopkins Employer Health Programs (EHP) Presented by: by: Johns Hopkins HealthCare Provider Relations Department 11/14/2018 Agenda Welcome About JHHC Provider Website
Johns Hopkins HealthCare LLC Johns Hopkins Employer Health Programs (EHP) Presented by: by: Johns Hopkins HealthCare Provider Relations Department 11/14/2018 Agenda Welcome About JHHC Provider Website
2019 Summary of Benefits Medicare Advantage Plans with Part D Prescription Drug Coverage
 2019 Summary of Benefits Medicare Advantage Plans with Part D Prescription Drug Coverage Plus H1035-002 H1035-006 H1035-014 January 1, 2019 December 31, 2019 The plan's service area includes: Flagler and
2019 Summary of Benefits Medicare Advantage Plans with Part D Prescription Drug Coverage Plus H1035-002 H1035-006 H1035-014 January 1, 2019 December 31, 2019 The plan's service area includes: Flagler and
Schedule of Benefits. Plan Information. Primary Care Provider: $10 Copayment per visit
 Schedule of Benefits PPO IA - Premium Network Deductible: $500 / $1,000 Coinsurance: 0% Total Annual Out-of-Pocket: $6,450 / $12,900 Primary Care : $10 Copayment per visit Specialist: $30 Copayment per
Schedule of Benefits PPO IA - Premium Network Deductible: $500 / $1,000 Coinsurance: 0% Total Annual Out-of-Pocket: $6,450 / $12,900 Primary Care : $10 Copayment per visit Specialist: $30 Copayment per
Anthem Blue Cross Your Plan: Modified Premier HMO 15/100% (Essential formulary $5/$15/$25/$45/30%) Your Network: California Care HMO
 Your Network: California Care HMO") Anthem Blue Cross Your Plan: Modified Premier HMO 15/100% (Essential formulary $5/$15/$25/$45/30%) Your Network: California Care HMO This summary of benefits is a brief outline of coverage, designed to
Anthem Blue Cross Your Plan: Modified Premier HMO 15/100% (Essential formulary $5/$15/$25/$45/30%) Your Network: California Care HMO This summary of benefits is a brief outline of coverage, designed to
I. PLAN DESCRIPTIONS. A. POS Point of Service
 I. PLAN DESCRIPTIONS A. POS Point of Service The Partnership Plan offers a single point of service plan to provide healthcare services both within and outside a defined network of Providers. No referrals
I. PLAN DESCRIPTIONS A. POS Point of Service The Partnership Plan offers a single point of service plan to provide healthcare services both within and outside a defined network of Providers. No referrals
Summary of Benefits. Calendar Year Deductibles (CYD) 2. Calendar Year Out-of-Pocket Maximum 4. No Lifetime Benefit Maximum
 2. Calendar Year Out-of-Pocket Maximum 4. No Lifetime Benefit Maximum") Summary of Benefits Superior Court of California, County of San Bernardino Effective January 1, 2019 HMO Benefit Plan Superior Court of California, San Bernardino Custom Access+ HMO Zero Admit 10 This
Summary of Benefits Superior Court of California, County of San Bernardino Effective January 1, 2019 HMO Benefit Plan Superior Court of California, San Bernardino Custom Access+ HMO Zero Admit 10 This
Medicare PPO Blue (PPO)
") Benefits Overview 2016 Drug Copayments $10 $20 $35 Medicare PPO Blue (PPO) Medicare PPO Blue (PPO) is a Medicare Advantage plan from Blue Cross and Blue Shield of Massachusetts HMO Blue, Inc. Blue Cross
Benefits Overview 2016 Drug Copayments $10 $20 $35 Medicare PPO Blue (PPO) Medicare PPO Blue (PPO) is a Medicare Advantage plan from Blue Cross and Blue Shield of Massachusetts HMO Blue, Inc. Blue Cross
You have from October 15 until December 7 to make changes to your Medicare coverage for next year.
 Explorer Rx 7 (PPO) offered by PacificSource Medicare Annual Notice of Changes for 2018 You are currently enrolled as a member of Explorer Rx 7 (PPO). Next year, there will be some changes to the plan
Explorer Rx 7 (PPO) offered by PacificSource Medicare Annual Notice of Changes for 2018 You are currently enrolled as a member of Explorer Rx 7 (PPO). Next year, there will be some changes to the plan
2018 NMRHCA Benefits Presentation Presbyterian Senior Care (HMO-POS) Plan I and Plan II
 Plan I and Plan II") 2018 NMRHCA Benefits Presentation Presbyterian Senior Care (HMO-POS) Plan I and Plan II Who we are Started in 1908 as a Tuberculosis Sanatorium Presbyterian Today Locally owned, nonprofit healthcare system
2018 NMRHCA Benefits Presentation Presbyterian Senior Care (HMO-POS) Plan I and Plan II Who we are Started in 1908 as a Tuberculosis Sanatorium Presbyterian Today Locally owned, nonprofit healthcare system
GENERAL BENEFIT INFORMATION
 Authorization Policy The following policy applies to Tufts Health Plan contracted providers rendering outpatient and inpatient services. This policy applies to Commercial 1 products (including Tufts Health
Authorization Policy The following policy applies to Tufts Health Plan contracted providers rendering outpatient and inpatient services. This policy applies to Commercial 1 products (including Tufts Health
All covered expenses accumulate separately toward the Network and Out-of-Network Coinsurance Maximum.
 PLAN FEATURES Network Managed Choice POS (Open Access) Primary Care Physician Selection Deductible (per calendar year) Not Applicable $500 per member Not Applicable $500 per member (2-member maximum) (2-member
PLAN FEATURES Network Managed Choice POS (Open Access) Primary Care Physician Selection Deductible (per calendar year) Not Applicable $500 per member Not Applicable $500 per member (2-member maximum) (2-member
NETWORK CARE. $250 per member (2-member maximum)
") PLAN FEATURES Network Managed Choice POS (Open Access) Primary Care Physician Selection Not Applicable Deductible (per calendar year) $250 per member (2-member maximum) Unless otherwise indicated, the
PLAN FEATURES Network Managed Choice POS (Open Access) Primary Care Physician Selection Not Applicable Deductible (per calendar year) $250 per member (2-member maximum) Unless otherwise indicated, the
NETWORK CARE. $4,500 (2-member maximum)
") PLAN FEATURES Network Managed Choice POS (Open Access) Primary Care Physician Selection Not Applicable Deductible (per calendar year) $4,500 (2-member maximum) Unless otherwise indicated, the Deductible
PLAN FEATURES Network Managed Choice POS (Open Access) Primary Care Physician Selection Not Applicable Deductible (per calendar year) $4,500 (2-member maximum) Unless otherwise indicated, the Deductible
BCBSM provides administrative claims services only. Your employer or plan sponsor is financially responsible for claims.
 GRPS Simply Blue Option C $500/$1000 deductible, $20, $40, $80 rx Eligible Groups: Support Non Exempt, Exempt/Professional Admin. Western Michigan Health Insurance Pool Group Number: 71565 Package Code(s):
GRPS Simply Blue Option C $500/$1000 deductible, $20, $40, $80 rx Eligible Groups: Support Non Exempt, Exempt/Professional Admin. Western Michigan Health Insurance Pool Group Number: 71565 Package Code(s):
PLAN DESIGN AND BENEFITS MC Open Access Plan 1913
 PLAN FEATURES PREFERRED CARE NON-PREFERRED CARE Deductible (per calendar year) $1,500 Individual $4,500 Family $4,000 Individual $12,000 Family Unless otherwise indicated, the Deductible must be met prior
PLAN FEATURES PREFERRED CARE NON-PREFERRED CARE Deductible (per calendar year) $1,500 Individual $4,500 Family $4,000 Individual $12,000 Family Unless otherwise indicated, the Deductible must be met prior
2017 NMRHCA Benefits Presentation
 2017 NMRHCA Benefits Presentation Presbyterian Senior Care (HMO-POS) Plan I and Plan II _[code]_[mmddyyyy] Who we are Started in 1908 as a Tuberculosis Sanatorium Presbyterian Today Locally owned, nonprofit
2017 NMRHCA Benefits Presentation Presbyterian Senior Care (HMO-POS) Plan I and Plan II _[code]_[mmddyyyy] Who we are Started in 1908 as a Tuberculosis Sanatorium Presbyterian Today Locally owned, nonprofit
PLAN DESIGN AND BENEFITS - Tx OAMC 3000 HSA 100% 08 PREFERRED CARE
 Aetna Life Insurance Company Texas Small Group MC Open Access Plan Effective Date: 09/01/2008 PLAN FEATURES NON- Deductible (per calendar year) $3,000 Individual $6,000 Individual $6,000 Family $12,000
Aetna Life Insurance Company Texas Small Group MC Open Access Plan Effective Date: 09/01/2008 PLAN FEATURES NON- Deductible (per calendar year) $3,000 Individual $6,000 Individual $6,000 Family $12,000
Lee s Summit School District
 Plan Type Plan Description (Visit our website at www.bluekc.com to receive a complete listing of network hospitals and physicians) Lee s Summit School District Effective Date: 1/1/16 Health Benefit Plan
Plan Type Plan Description (Visit our website at www.bluekc.com to receive a complete listing of network hospitals and physicians) Lee s Summit School District Effective Date: 1/1/16 Health Benefit Plan
Benefits Summary SelectHC IV
 Benefits Summary SelectHC IV An Embedded Deductible, High Deductible Health Plan (HDHP) This chart only summarizes covered benefits. Please refer to the Policy for coverage details including exclusions
Benefits Summary SelectHC IV An Embedded Deductible, High Deductible Health Plan (HDHP) This chart only summarizes covered benefits. Please refer to the Policy for coverage details including exclusions
For Large Groups Lower Premium Health Benefit Plan 03900
 Summary of Benefits for Services In-Network Out-of-Network Financial Features (DED 1 ) (PBP 2 ) $2,000 $4,500 (DED is the amount the member is responsible for before Florida Blue pays) Coinsurance (Coinsurance
Summary of Benefits for Services In-Network Out-of-Network Financial Features (DED 1 ) (PBP 2 ) $2,000 $4,500 (DED is the amount the member is responsible for before Florida Blue pays) Coinsurance (Coinsurance
40% (Not subject to the Calendar-Year Deductible) CT scans, MRIs, MRAs, PET scans, and cardiac diagnostic
 CT scans, MRIs, MRAs, PET scans, and cardiac diagnostic") An independent member of the Blue Shield Association P.C. Specialists dba Technology Integration Group Custom Shield PPO Combined Deductible 30-1250 90/60 Benefit Summary (For groups of 300 and above)
An independent member of the Blue Shield Association P.C. Specialists dba Technology Integration Group Custom Shield PPO Combined Deductible 30-1250 90/60 Benefit Summary (For groups of 300 and above)
$250 per member. All covered expenses accumulate separately toward the Network and Out-of-network Coinsurance Maximum.
 PLAN FEATURES Network Managed Choice POS (Open Access) OUT-OF- Not Applicable Primary Care Physician Selection Deductible (per calendar year) Not Applicable $250 per member Not Applicable $250 per member
PLAN FEATURES Network Managed Choice POS (Open Access) OUT-OF- Not Applicable Primary Care Physician Selection Deductible (per calendar year) Not Applicable $250 per member Not Applicable $250 per member
Anthem Blue Cross Your Plan: Classic HMO 20/40/250 Admit /125 OP ($5/$15/$30/$50/30%) Your Network: California Care HMO
 Your Network: California Care HMO") Anthem Blue Cross Your Plan: Classic HMO 20/40/250 Admit /125 OP ($5/$15/$30/$50/30%) Your Network: California Care HMO This summary of benefits is a brief outline of coverage, designed to help you with
Anthem Blue Cross Your Plan: Classic HMO 20/40/250 Admit /125 OP ($5/$15/$30/$50/30%) Your Network: California Care HMO This summary of benefits is a brief outline of coverage, designed to help you with
An Overview of Your Health and Dental Benefits
 An Overview of Your Health and Dental Benefits Educators Health Alliance Direct Bill Plan 2 \ EDUCATORS HEALTH ALLIANCE HEALTH AND DENTAL PLAN OPTIONS Exclusively for Educators Health Alliance Direct Bill
An Overview of Your Health and Dental Benefits Educators Health Alliance Direct Bill Plan 2 \ EDUCATORS HEALTH ALLIANCE HEALTH AND DENTAL PLAN OPTIONS Exclusively for Educators Health Alliance Direct Bill
Anthem Blue Cross Your Plan: Value HMO 30/40/30% Your Network: California Care HMO
 Anthem Blue Cross Your Plan: Value HMO 30/40/30% Your : California Care HMO This summary of benefits is a brief outline of coverage, designed to help you with the selection process. This summary does not
Anthem Blue Cross Your Plan: Value HMO 30/40/30% Your : California Care HMO This summary of benefits is a brief outline of coverage, designed to help you with the selection process. This summary does not
Anthem Blue Cross Your Plan: CSEBO HMO 10 (Custom Premier HMO 10/100%) Your Network: California Care HMO
 Your Network: California Care HMO") Anthem Blue Cross Your Plan: CSEBO HMO 10 (Custom Premier HMO 10/100%) Your Network: California Care HMO This summary of benefits is a brief outline of coverage, designed to help you with the selection
Anthem Blue Cross Your Plan: CSEBO HMO 10 (Custom Premier HMO 10/100%) Your Network: California Care HMO This summary of benefits is a brief outline of coverage, designed to help you with the selection
Anthem Blue Cross Your Plan: Anthem Elements Choice HMO 1500 (Essential Formulary $5/$20/$50/$65/30% $500 Deductible) Your Network: Select HMO
 Your Network: Select HMO") Anthem Blue Cross Your Plan: Anthem Elements Choice HMO 1500 (Essential Formulary $5/$20/$50/$65/30% $500 Deductible) Your Network: Select HMO This summary of benefits is a brief outline of coverage, designed
Anthem Blue Cross Your Plan: Anthem Elements Choice HMO 1500 (Essential Formulary $5/$20/$50/$65/30% $500 Deductible) Your Network: Select HMO This summary of benefits is a brief outline of coverage, designed
SUBLUE AND SUORANGE: 2018 SCHEDULE OF BENEFITS -EMPLOYEE COST SHARING
 Cost Sharing Definitions Annual Deductible 1 (amounts are not cumulative across levels) $100 per individual with a maximum of $250 for a family $300 per individual with a maximum of $1,000 for a family
Cost Sharing Definitions Annual Deductible 1 (amounts are not cumulative across levels) $100 per individual with a maximum of $250 for a family $300 per individual with a maximum of $1,000 for a family