IMPLEMENTATION COMPLETION AND RESULTS REPORT (IDA-41410) A CREDIT IN THE AMOUNT OF SDR 24.2 MILLION (US$35.0 MILLION EQUIVALENT) TO THE
|
|
|
- Octavia Paul
- 5 years ago
- Views:
Transcription
1 Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Document of The World Bank IMPLEMENTATION COMPLETION AND RESULTS REPORT (IDA-41410) ON A CREDIT IN THE AMOUNT OF SDR 24.2 MILLION (US$35.0 MILLION EQUIVALENT) TO THE REPUBLIC OF NIGER FOR AN Report No: ICR2146 INSTITUTIONAL STRENGTHENING AND HEALTH SECTOR SUPPORT PROGRAM Human Development Sector Health, Nutrition and Population (AFTHE) Country Department AFCF2 Africa Region DECEMBER 19, 2011
2 CURRENCY EQUIVALENTS (Exchange Rate Effective October 2005) Currency Unit = CFA Franc (FCFA) 1US$ = 545 FCFA FISCAL YEAR January 1 December 31 ABBREVIATIONS AND ACRONYMS AAP / PAA Annual Action Plan MoU Memorandum of Understanding AIDS Acquired Immune Deficiency MTEF / Medium Term Expenditure Framework Syndrome CDMT AFD Agence Française de MTR Mid-Term Review Développement ARV Anti retroviral drugs NSI / INS National Statistics Institute CAS Country Assistance Strategy NGO Non-Governmental Organization CSR Country Status Report DCA Development Credit Agreement PAD Project Appraisal Document DHS / EDS Demographic and Health Survey PCN Project Concept Note DM Decision Meeting PDO Project Development Objective DPL Development Program Lending PEMFAR Public Expenditure Management Report DSRP / PRSP Poverty Reduction Strategy Paper PER / RDP Public Expenditure Review PHRD Policy and Human Resources Development Fund EA Environmental Assessment PNC / CPN Pre natal consultation EMP Environmental Management Plan PPF Project Preparation Facility EU European Union PRODEM Population Project PRSC / RSRC Poverty Reduction Strategy Credit FM Financial Management PRSP / DRSP Poverty Reduction Strategy Paper FMR/RSF Financial Monitoring Report QAG Quality Assurance Group GAVI GAVI Alliance QER Quality Enhancement Review GDP Gross Domestic Product SDR Special Drawing Rights HDP / PDS Health Development Plan SIL Sector Investment Loan HIPC Highly Indebted Poor Country SIM Sector Investment Maintenance Initiative HIV Human Immune Deficiency Virus SOE Statement of Expenditure HR Human resources STI Sexually Transmitted Infections SWAp Sector-wide Approach ICR Implementation Completion and Results Report IDA International Development TA Technical Assistance Association IEG Internal Evaluation Group TF Trust Fund IMCI Integrated management of TFP Technical & Financial Partners
3 childhood illnesses IO Intermediate outcome indicators TOR Terms of Reference ISR Implementation Status Report TTL Task Team Leader KPI Key Performance Indicators UN United Nations UNICEF United Nations Children s Fund MAP Multi-Sectoral AIDS Program UNFPA United Nations Population Fund MBB Marginal Budgeting for Bottlenecks USAID United States Agency for International Development MDG Millennium Development Goals USD US Dollar M&E Monitoring and Evaluation MIS / SNIS Management Information System WHO World Health Organization MHP Minimum Health Package MOH / MSP Ministry of Health Vice President : Obiageli K. Ezekwesili Country Director : Ousmane Diagana Sector Manager : Jean-Jacques De St. Antoine Project Team Leader : Djibrilla Karamoko ICR Team Leader : Jean-Jacques de Saint Antoine
4
5 NIGER INSTITUTIONAL STRENGTHENING AND HEALTH SECTOR SUPPORT PROGRAM Table of Contents A. Basic Information i B. Key Dates i C. Ratings Summary i D. Sector and Theme Codes ii E. Bank Staff ii F. Results Framework Analysis ii G. Ratings of Project Performance in ISRs vii H. Restructuring (if any) vii I. Disbursement Profile vii 1. Project Context, Development Objectives and Design Context at Appraisal Original Project Development Objectives (PDO) and Key Indicators (as approved) Original Components Revised Components Other significant changes 4 2. Key Factors Affecting Implementation and Outcomes Project Preparation, Design and Quality at Entry Implementation Monitoring and Evaluation (M&E) Design, Implementation and Utilization Safeguard and Fiduciary Compliance Post-completion Operation/Next Phase Relevance of Objectives, Design and Implementation Achievement of Project Development Objectives Efficiency Justification of Overall Outcome Rating Overarching Themes, Other Outcomes and Impacts 19
6 3.6 Summary of Findings of Beneficiary Survey and/or Stakeholder Workshops Assessment of Risk to Development Outcome Assessment of Bank and Borrower Performance Bank Performance Borrower Performance Lessons Learned Comments on Issues Raised by Borrower/Implementing Agencies/Partners 24 Annex 1: Project Costs and Financing 26 Annex 2: Descriptive summary of project outputs 27 Annex 3: Economic and Financial Analysis 30 Annex 4: Bank Lending and Implementation Support/Supervision Processes 32 Annex 5: Beneficiary Survey Results 34 Annex 6: Stakeholder Workshop Report and Results 35 Annex 7: Summary of Borrower's ICR and/or Comments on Draft ICR 36 Annex 8: Comments of Co-financing partners and Other Partners/Stakeholders 38 Annex 9: List of Supporting Documents 39 MAP
7 A. Basic Information Country: Niger Project Name: Instit. Strengthening & Health Sector Support Program (ISHSSP) Project ID: P L/C/TF Number(s): IDA ICR Date: 12/19/2011 ICR Type: Core ICR Lending Instrument: SIM Borrower: Original Total Commitment: Revised Amount: XDR 24.20M Environmental Category: B NIGER Ministry of Finance and Economy XDR 24.20M Disbursed Amount: XDR 23.90M Implementing Agencies: Ministry of Health Cofinanciers and Other External Partners: SPAIN GAVI United Nations International Children's Education Fund (UNICEF) Agence Française de développement B. Key Dates Process Date Process Original Date Revised / Actual Date(s) Concept Review: 05/06/2004 Effectiveness: 07/20/ /20/2006 Appraisal: 06/14/2005 Restructuring(s): Approval: 01/05/2006 Mid-term Review: Closing: 06/30/ /30/2011 C. Ratings Summary C.1 Performance Rating by ICR Outcomes: Risk to Development Outcome: Bank Performance: Borrower Performance: Satisfactory Substantial Satisfactory Satisfactory C.2 Detailed Ratings of Bank and Borrower Performance (by ICR) Bank Ratings Borrower Ratings Quality at Entry: Satisfactory Government: Moderately Satisfactory Quality of Supervision: Moderately Satisfactory Implementing Agency/Agencies: Satisfactory Overall Bank Satisfactory Overall Borrower Satisfactory i
8 Performance: Performance: C.3 Quality at Entry and Implementation Performance Indicators Implementation QAG Assessments (if Indicators Performance any) Potential Problem Project at any time (Yes/No): Problem Project at any time (Yes/No): DO rating before Closing/Inactive status: Yes No D. Sector and Theme Codes Satisfactory Sector Code (as % of total Bank financing) Quality at Entry (QEA): None Quality of Supervision (QSA): Central government administration 13 Health 65 Other social services 15 Sub-national government administration 7 Original None Rating Actual Theme Code (as % of total Bank financing) Child health 14 Health system performance 29 Malaria 14 Participation and civic engagement 14 Population and reproductive health 29 E. Bank Staff Positions At ICR At Approval Vice President: Obiageli Katryn Ezekwesili Gobind T. Nankani Country Director: Ousmane Diagana Madani M. Tall Sector Manager: Jean J. De St Antoine Alexandre V. Abrantes Project Team Leader: Djibrilla Karamoko Djibrilla Karamoko ICR Team Leader: ICR Primary Author: Jean J. De St Antoine Peter D. Bachrach F. Results Framework Analysis ii
9 Project Development Objectives (from Project Appraisal Document) The PDO aims at improving sector capacity, effectiveness and efficiency in the provision of essential health care in Niger and in monitoring Infant Mortality Rates over time. The project will contribute to the provision of a minimum package of essential health services targeted at the poor, women and children. Revised Project Development Objectives (as approved by original approving authority) (a) PDO Indicator(s) Indicator Original Target Values (from Baseline Value approval documents) Infant mortality rate (per thousand) PAD: DHS-MICS (2006): 81.0 Formally Actual Value Achieved at Revised Target Completion or Target Years Values Indicator 1 : Value (Quantitative PAD: or Qualitative) Date achieved DHS-MICS 2006 Child survival/mortality survey (2010) Comments (incl. % With the DHS-MICS (2006) result of 81.0 as baseline, the actual value achieved of 63.2 is a achievement) 22.0% reduction in infant mortality Indicator 2 : Under five mortality rate (per thousand) Value (Quantitative PAD: PAD: or Qualitative) DHS-MICS (2006): Date achieved DHS-MICS 2006 Child survival/mortality survey (2010). Comments (incl. % With the DHS-MICS 2006 result of as baseline, the actual value achieved of is a achievement) 34.1% reduction in the under-five mortality rate Indicator 3 : Maternal mortality ratio (per 100,000) Value (Quantitative PAD: 700 PAD: or Qualitative) DHS-MICS (2006): 648 Date achieved DHS-MICS 2006 Child survival/mortality survey (2010). With the DHS-MICS (2006) result as baseline, the actual value achieved of is a 14.5% Comments (incl. % reduction in the maternal mortality ratio; the project target (probably too ambitious) was achieved achievement) at 89% Indicator 4 : Contraceptive prevalence (modern methods) (percent) Value (Quantitative PAD: 4.0% PAD: 15.0% 16.0% or Qualitative) DHS-MICS (2006): 5.0% Date achieved DHS-MICS 2006 Contraceptive prevalence survey (2010) Comments (incl. % achievement) With the DHS-MICS (2006) result as baseline, the utilization rate more than tripled. The original target was achieved at 107% NB: The PAD was prepared on the basis of data in the National Health Development Plan prior to the final publication of the DHS-MICS, resulting in some anomalies in the target values. See also Section 2.3. iii
10 (b) Intermediate Outcome Indicator(s) PDO 1: Contribute to the reduction of maternal and infant mortality Original Target Values Indicator Baseline Value (from approval documents) iv Formally Revised Target Values Actual Value Achieved at Completion or Target Years Indicator 1 : Percentage of population with access to health facilities/outreach offering minimum health package Value (Quantitative 41.5% 80.0% 49.4% or Qualitative) Date achieved 31 December 2005 Statistical Directory (2005) 31 December 2010 Statistical Directory (2010) Comments (incl. % The target was achieved at 62%. achievement) Indicator 2 : Percentage of health facilities carrying out outreach activities Value (Quantitative 68.0% 75.0% 89.8% or Qualitative) Date achieved 31 December 2006 Statistical Directory (2006) 31 December 2010 Statistical Directory (2010) Comments (incl. % achievement) Taking the 2006 Statistical Directory result of 68.0% as baseline, the actual value achieved of 89.8% is an increase of 32%. The project target was achieved at 120%. Indicator 3 : Outpatient visits per capita Value (Quantitative or Qualitative) Date achieved 31 December 2005 Statistical Directory (2005) 31 December 2010 Statistical Directory (2010) Comments (incl. % achievement) Between 2005 and 2010, the number of outpatient visits per capita more than doubled. The target was achieved at 114%. Indicator 4 : Assisted delivery by skilled attendant (percent) Value (Quantitative 25.0% or Qualitative) PAD: 16.0% Stat Dir. (2005): 10.9% DHS-MICS (2006): 17.2% Stat Dir. (2010): 20.5% Child survival/mortality survey (2010): 30.9% Date achieved 31 December December 2010 Based on the annual statistical directories, assisted deliveries increased by 188%; the target was Comments (incl. % achieved at 82%. Based on the formulation in the national surveys (2006 and 2010), assisted deliveries achievement) increased by 180% increase; the target was achieved at 124%. Indicator 5 : Percentage of health district centers offering Basic Emergency Obstetric Care Value (Quantitative 27.3% 70.0% 81.3% or Qualitative) Date achieved 31 December 2006 Statistical Directory (2006) 31 December 2010 Statistical Directory (2010) Comments (incl. % achievement) Comparing the results from 2006 and 2010, the proportion of health centers tripled; the target was achieved at 116%. Indicator 6 : Percentage Ante Natal care coverage Value (Quantitative 46.4% 70.0% 95.7% or Qualitative) Date achieved DHS-MICS (2006) Child survival/mortality survey (2010) Comments (incl. % With the DHS-MICS (2006) result as baseline, ante-natal coverage more than doubled. The original
11 achievement) target was achieved at 137%. The annual statistical directory shows an increase from 50.1% in 2005 to 90.6% in Indicator 7 : Percentage of children under five sleeping under simple or impregnated bed nets Value (Quantitative 23.5% 40.0% 83.0% or Qualitative) Date achieved DHS-MICS (2006) Child survival/mortality survey (2010) With the DHS-MICS (2006) result as baseline, the percentage of children using bed nets more than Comments (incl. % tripled. The original target was achieved at 208%. The project procured 250,000 impregnated bed achievement) nets to complement the 2.8 million procured by the GF Indicator 8 : Proportion of women who receive intermittent treatment for malaria during the last pregnancy Value (Quantitative or Qualitative) PAD: 17.0% Stat Dir (2005): 46.9% DHS-MICS (2006): 47.6% 40.0% Stat Dir (2010):73.7% Date achieved 31 December December 2010 Statistical Directory (2010) Comparing the results from the 2005 and 2010 Statistical Directories, the proportion of women Comments (incl. % receiving intermittent treatment for malaria increased by more than 60%. The original target was achievement) achieved at 184%. Indicator 9 : Percentage of children having received full vaccination coverage (under five years old) for Measles Value (Quantitative or Qualitative) PAD: 60.0% Stat Dir (2005): 80.0% DHS-MICS (2006): 47.0% 70.0% Stat Dir (2010) : 88.8% Child survival/mortality survey (2010): 68.6% Date achieved 31 December 2005 National child survival and mortality survey (2010) Comments (incl. % achievement) With the DHS-MICS result of 2006 as baseline, the actual value achieved of 68.6% represents an increase of almost 50% in measles vaccination. The original target was achieved at 98%. Indicator 10 : Malnutrition of children under five years old (percentage of cases treated) Value (Quantitative PAD: 17.0% 50.0% or Qualitative) Stat Dir (2005): 27.0% Stat Dir (2010): 120.8% Date achieved 31 December December 2010 Statistical Directory results ( ) differ (56.7% and 120.8%), due perhaps to the 2010 food Comments (incl. % crisis and multiple child visits. Regular nutritional surveys show a consistent range of child achievement) malnutrition (weight-age) from 44.4% in 2006 to 40.6% in 2010 PDO 2: support the Borrower s Program to improve efficiency and quality of care in the health system Indicator 11 : Average length (in days) of shortage of stocks of the 6 most essential molecules Value (Quantitative PAD: 21 days 0 or Qualitative) Stat Dir (2006): 5.1% Stat Dir (2010): 1.6% Date achieved 31 December December 2010 Comments (incl. % achievement) Comparing the results from the 2006 and 2010 Statistical Directories, the stockout rate for the 6 most essential drugs declined from 5.1% to 1.6%, a reduction of 70%. The original target was not achieved. Indicator 12 : Portion of Government budget allocated to the health sector Value (Quantitative PAD: 7.27% 15.0% or Qualitative) Stat Dir (2005): 5.96% Stat Dir (2010): 7.85% v
12 Date achieved 31 December December 2010 The health budget reached 10.17% (2008) before declining to 7.85%. The Abuja target was achieved Comments (incl. % at 52%. Between , budgets almost doubled in absolute terms (26 to 50 billion Fcfa) and actual achievement) expenditures more than doubled (16 to 40 billion Fcfa) Indicator 13 : Portion of the health budget allocated and transferred to regions and health districts Value (Quantitative 20.0% 60.0% 72.7% or Qualitative) Date achieved 31 December 2005 Statistical Directory (2005) 31 December 2010 Statistical Directory (2010) Comments (incl. % The original target was achieved at 121%. achievement) Indicator 14 : Percentage of health centers and hospital with available resource to manage health care waste Value (Quantitative PAD: 20.0% 100.0% or Qualitative) Stat Dir (2006): 27.5% Stat Dir (2010): 58.8% Date achieved 31 December December 2010 Comments (incl. % achievement) Over the project period, the proportion of health facilities able to manage health care waste more than doubled; the original target was achieved at 59%. Indicator 15 : Percentage of health centers staffed in accordance with agreed standard staffing norms Value (Quantitative or Qualitative) CSI (335/578): 58.0% HD (5/23): 20.0% CHR (7/8): 85.0% Global (347/609): 57.0% CSI (549/578): 95.0% HD (23/23): 100% CHR (8/8): 100% Global (580/609): 95.2% CSI: 59% HD: 70% CHR: 86% Global: 70.5% Date achieved 21 July December 2010 Statistical Directory (2010) Comments (incl. % achievement) Indicator 16 : Value (Quantitative or Qualitative) Date achieved Because the indicator was not monitored in a disaggregated manner, the PAD baseline value and original target were recalculated. The original target was achieved at 74%. The Government has recruited 1600 health staff for deployment during Number of new staff trained per annum and by specialties TBD TBD Paramedical staff: 328 Medical staff: 219 Report on specialized training ( ) Over the period , 425 paramedical and 340 medical staff were expected to receive specialized Comments (incl. % training; 547 (72%) were trained during the period to ; approximately 10% of these achievement) were trained by the project. Indicator 17 : Number of recruited staff (contractual and civil servants) compared with the needs estimated Value (Quantitative PAD: nd TBD or Qualitative) Stat Dir (2005): 30.4% Stat Dir (2010): 63.4% Date achieved 31 December December 2010 Comments (incl. % Between , the proportion recruited staff compared with estimated needs more than doubled (to achievement) 63.4%). For the entire period, of the 8065 staff requested, 4323 (53.4%) were recruited. Indicator 18 : Percentage of functioning health management committees per district Value (Quantitative PAD: 20.0% 80.0% or Qualitative) Stat Dir (2005): 78.4% Stat Dir (2010): 85.7% Date achieved 31 December December 2010 Comments (incl. % At the end of the period, 85.7% of the committees were functioning; the indicator was achieved at achievement) 107%. Indicator 19 : Percentage of health centers under the performance based management system Value (Quantitative 0.0% 100.0% Unknown vi
13 or Qualitative) Date achieved 21 July 2006 Comments (incl. % achievement) Data collected on this indicator cannot be reliably analyzed. Between , regions used various numerators and denominators. Beginning in 2009, the Ministry used the number of managerial personnel having signed a performance contract, but this was not the PAD indicator and there was no real follow-up on performance. G. Ratings of Project Performance in ISRs No. Date ISR Actual Disbursements DO IP Archived (USD millions) 1 09/22/2006 Satisfactory Moderately Satisfactory /28/2007 Satisfactory Moderately Satisfactory /28/2007 Satisfactory Moderately Satisfactory /28/2008 Moderately Satisfactory Satisfactory /24/2008 Moderately Satisfactory Satisfactory /22/2008 Moderately Satisfactory Satisfactory /09/2008 Moderately Satisfactory Satisfactory /16/2009 Moderately Satisfactory Moderately Satisfactory /09/2009 Moderately Satisfactory Moderately Satisfactory /17/2010 Moderately Satisfactory Moderately Satisfactory /01/2010 Moderately Satisfactory Moderately Satisfactory /05/2011 Satisfactory Moderately Satisfactory /28/2011 Satisfactory Moderately Satisfactory H. Restructuring (if any) Not Applicable I. Disbursement Profile vii
14 viii
15 1. Project Context, Development Objectives and Design 1.1 Context at Appraisal 1. Country context. The Country Status Report (CSR) of 2002 described Niger as one of the world's poorest countries with extremely limited prospects resulting from: (i) explosive population growth; (ii) a lack of natural resources and a highly degraded natural environment; and (iii) very limited international competitiveness due to low human and institutional capacity. The CSR also pointed to the years of poor governance and the country s location in a potentially volatile subregion as further handicaps. 2. Despite these daunting challenges, the 2003 CAS described: (i) improved macroeconomic performance over the preceding years; (ii) increased flows of donor support and interim debt relief since attaining the enhanced Heavily Indebted Poor Country (HIPC) Decision Point in December 2000; and (iii) a strong poverty reduction framework to achieve significant progress towards the Millennium Development Goals (MDGs). To maximize the effectiveness of the available resources, the CAS emphasized strengthening government capacity to: (i) build consensus around sectoral strategies and expenditure programs; (ii) plan, coordinate (with its partners), and manage development programs; and (iii) decentralize the delivery of basic services. 3. Health situation. While noting the contribution of negative factors to the extreme vulnerability of poor Nigeriens, particularly women and children, the CSR also described Niger s progress in improving its health indicators over the previous decade. It cautioned, however, that as a HIPC country, Niger would need to: (i) rapidly meet several human development targets agreed on in the 2002 Poverty Reduction Strategy Paper (PRSP) to remain on track for the debt initiative; and (ii) make measurable progress toward achieving the Millennium Development Goals (MDGs). Among the principal obstacles faced by the country were: its poverty, with an annual gross national income per capita of only US$180 placing it among the world s poorest countries; its population growth, with one of the highest population growth rates in the world at 3.1%, a total fertility ratio of 7.5 children per woman, and the prospect of reaching 53 million people by 2050 and becoming the second highest populated West African country after Nigeria; and its significant gaps in the results achieved in rural (where 80% of the population live) and urban areas and among various socio-economic groups The Project Appraisal Document (PAD) summarized the key issues in the health sector in terms of: (i) inequitable access with only 28% of rural populations (as opposed to 99% of urban populations) within 5km of basic health services and fees (especially for hospital services) representing significant barriers to health seeking behavior, particularly for infants and young children; (ii) insufficient quality of existing health services resulting from inadequate human resources and periodic stock-outs of drugs and consumables; (iii) chronic underfunding of the health sector contributing to imbalances (between investment and recurrent costs) and poor allocation of sector resources; and (iv) inadequate capacity to carry out basic sector management functions (for health policy and regulation, program planning and implementation, resource mobilization and 1 As an example, the Demographic Health Survey (DHS) of 1998 showed a modern contraceptive prevalence rate of only 2.1% in rural areas as opposed to 18.6% in urban areas. 1
16 disbursement, etc.), exacerbated by a lack of coordination among the different technical and financial development partners. 5. Country Assistance Strategy and Rationale for Bank Involvement. As noted in the Poverty Reduction Strategy (2002), the Bank and the Government agreed that: (i) continued progress on the health reform agenda was of fundamental importance; and (ii) a progressive shift towards consolidated programmatic lending (ie. Development Program Lending) would be the preferred lending instrument to maximize the development impact of Bank support. As part of its existing or planned portfolio, the Bank was also involved in three other operations in health-related areas: HIV/AIDS (MAP); Population Project (PRODEM), and the budget support project (RSRC-2) which included a number of reform measures in health and population as triggers for tranche releases. Sector work was also planned in nutrition. 6. The project s objectives were in line with most recent Country Assistance Strategy (of January 21, 2003), particularly with respect to the CAS pillars for: (i) improving the access of the poor to quality social services; and (ii) strengthening institutional and individual capacity both within and outside the Government. More specifically, the CAS directly targeted human development deficiencies and the vulnerabilities resulting from them and sought to: (i) support the Government in developing and implementing an appropriate strategy on population; (ii) intensify the fight against HIV/AIDS; (iii) improve the delivery of basic education; and (iv) make water infrastructure accessible to the poor. 7. The Bank intended to support the implementation of the Health Development Plan ( ) with a focus on policy dialogue and areas where IDA could best exercise its leverage, experience, and expertise. These included two significant innovations for which the Bank had an important comparative advantage: (i) emphasizing capacity building within MOH at all levels, which had not been done previously; and (ii) introducing a Sector-Wide Approach (SWAp), with donors agreeing to work jointly on project preparation and implementation and to carry out joint annual reviews of work plans and sector performance. Noting the Bank s strong support of SWAps (with generally good results) in the health sector in several African and Asian countries, the Government and other development partners recognized the Bank s experience in providing technical input to build the requisite capacity and in helping to bridge the identified financial gaps. 1.2 Original Project Development Objectives (PDO) and Key Indicators (as approved) 8. The PAD presents the PDO as follows: to improve sector capacity, effectiveness and efficiency in the provision of essential health care in Niger and contribute to the reduction of maternal and child mortality by providing a minimum package of essential health services targeted at the poor, women and children. The Development Credit Agreement (DCA) phrases the PDO somewhat differently: to support the Borrower s Program to improve efficiency and quality of care in the health system and contribute to the reduction of maternal and child mortality Revised PDO (as approved by original approving authority) and Key Indicators, and reasons/justification 9. Concerned with the ambition of the PDO and KPI, management urged the team to consider revisions immediately after effectiveness, at mid-term, and during the final year of project implementation; restructuring documents were even prepared in the final instance. In the end, the PDO and KPI were not revised for two reasons: (i) the Government preferred to maintain PDO 2 The Task Team preferred the DCA presentation of the PDO. 2
17 which were consistent with the National Health Development Plan; and (ii) the DHS results (which became available after effectiveness) suggested that a number of the indicators could be achieved during the project. Data on the key outcome and intermediate outcome indicators are presented in Section F of the Data Sheet and discussed in more detail in Section 3.2 and Annex Main Beneficiaries and Benefits 10. A beneficiary assessment, conducted in rural communities on poverty issues (2003), highlighted: (i) the importance of health status as a leading cause and consequence of poverty; and (ii) the challenge of sustaining the demand for health care from poor and rural populations. With a focus on the poor and other vulnerable groups (primarily women and children), the project was expected to improve the health status of these beneficiaries by increasing the affordability of, accessibility to, and quality of public health services. By addressing the broader issues of poverty reduction, gender and equity, and the increased involvement of communities in managing health services, the project was also expected to sustain demand for services. 11. Among the benefits envisioned by the programmatic lending, the project expected to initiate a phased approach to: (i) rationalize investments by coordinating donor inputs and maintaining the focus on outcomes and results; (ii) harmonize planning and fiduciary management procedures based on improved capacity and national systems satisfactory to all the development partners working in the sector; and (iii) introduce sector budget support or eventual full budget support. 1.5 Original Components 12. Component 1: Strengthening human resources development and management (US$ 10 million) 3. The objectives were to improve efficiency and equity of the health system by optimizing the distribution and enhancing the performance of human resources through: (i) modernizing human resource management (including the revision of HR norms, the development of career plans, and the implementation of training activities both for basic and continuing education); and (ii) implementing incentive systems to encourage redeployment of personnel in rural areas and reward individual s and or unit s performance in achieving set objectives in their respective annual work plan. 13. Component 2: Expansion of services and delivery of minimum health package (MHP) (US$ 20 million). The objectives were to: increase the availability of essential drugs and medical supplies in all public health facilities and avoid inventory shortages of a selected list of the most essential drugs (including measures to strengthen financing, procurement, and distribution as well as increasing private and traditional sector participation in distribution and decreasing opportunities for illicit drug distribution); strengthen health programs and improve the quality of services (to address the major causes of morbidity and mortality of children less than five years old; to implement a sound reproductive health strategy with improved protocols for antenatal and post natal care; to promote modern family planning methods by integrating services into the Minimum Health Package and expanding community based distribution of contraceptives and social marketing; to strengthen the integrated management of childhood illnesses (IMCI) at community and health facility levels; to develop behavior 3 Technically, because of the nature of the project, no component costs were identified; these indicative amounts are from the ISRs. 3
18 change strategies and financial and non-financial incentives to increase utilization of essential services; and to expand Malaria Subprograms; and promote demand and improve geographical access (of the poor) to essential health services provided at the primary level by promoting outreach strategies, revising of the cost-recovery policy, and adopting measures for the exemption of payment of certain services for the poor. 14. Component 3: Strengthening governance and institutional capacity (US$ 5 million). The objectives were to: Strengthen health system management and institutional capacity to assume the responsibilities and tasks defined in the institutional reform framework, comprising policy development and analysis, performance monitoring, and evaluation (e.g., sector decentralization, district development, and strengthening of personnel capacity); strengthening of the infrastructure and equipment management including the rationalization of health investments according to a health map; hospital reform; and strengthening of the National Health Information System; Ensure equitability by improving access to a Minimum Health Package for the whole population by increasing resources, developing a redistributive budget allocation mechanism to balance regional and district-level disparities, and establishing financial protection systems; and Improve community participation to strengthen responsibility for administering resource mobilization strategies, improving the responsiveness and accountability of the health system, and promoting community-based health care. 15. Component 4: Monitoring and evaluation (US$ million). The objectives were to: implement appropriate monitoring and evaluation mechanisms regarding Subprograms performance and ensure good coordination of the monitoring and evaluation activities of the Technical and Financial Partners. 1.6 Revised Components 16. The project components were not revised. 1.7 Other significant changes 17. Though discussions about restructuring the PDO were conducted just after effectiveness, at the time of the mid-term review, and in the final year of project implementation, the project was never restructured. A single amendment to the Development Credit Agreement was approved in 2010 to reallocate the proceeds of the project. 2. Key Factors Affecting Implementation and Outcomes 2.1 Project Preparation, Design and Quality at Entry 18. From the beginning, the project was conceived as a SWAp with the objectives of rationalizing investment and donor coordination, focusing on the results established in the Health Development Plan , and assisting MOH in the transition to full-budgetary support for longterm nature capacity building in the health sector. While in line with Government intentions and Bank strategy, the design was clearly ambitious, and the project preparation process and design features reflected the challenges of realizing the sector-wide approach. 4
19 19. Project preparation. Project preparation was initiated in February 2004, with a joint identification mission comprising the Bank, other international agencies (WHO, UNFPA, UNICEF), and key donors (European Union, Belgian Cooperation, French Cooperation, Canadian IDA, Japan, etc). A number of these agencies were already assisting the ministry in: (i) updating the Health Development Plan (HDP); (ii) examining institutional issues at central, regional, and district levels; and (iii) analyzing core bottlenecks, using the Marginal Budgeting for Bottlenecks (MBB) approach to formulate the Medium Term Expenditure Framework (MTEF). 20. It was expected that the partnership would be maintained throughout the preparation, with all donors endorsing the approach, participating in the preparation process (with technical assistance in their areas of competence), and pledging to coordinate their interventions within the revised HDP. The Bank committed financial resources through a PHRD grant and a PPF to support the background analysis: Submitted in April and approved in July 2004, PHRD financing (TF ) in the amount of US$ 470,899 was used to carry out studies in the areas of: (i) human resources (census, training, planning and managing, incentives); (ii) health service quality assessment; (iii) institutional, fiduciary, and management change; and (iv) promotion of the private sector. The PHRD grant was closed in September 2005 (with a balance of US$ 75,000). At PHRD closing, a Project Preparation Facility (Q4950-NIR) in the amount of US$ 600,000 was approved to continue activities initiated under the PHRD, including: (i) implementing institutional changes within the Ministry of Health, especially in the area of human resource development; (ii) organizing the preparation of annual action plans for 2006 (at central, regional and district levels); and (iii) strengthening project coordination and implementation tools and capabilities. The refinancing date of the PPF was subsequently extended from February to May 2006 and then to August 2006 and was closed with project effectiveness in July A Project Concept Note (PCN) was reviewed in May 2004, and the proposed project was endorsed as a potentially effective response to the challenges hindering sector development, namely: (i) lack of capacity within the sector; (ii) insufficient funding; and (iii) uncertainty and lack of coordination in donor assistance. An important concern at this stage was the impact of the cost recovery policy, seen as a major constraint on health service utilization by the poor and needing revision, for which a study was under way with preliminary conclusions expected in June By the completion of the pre-appraisal mission of September 2004, substantial progress had been made on the basic elements of the project comprising agreements on: the objectives of the Health Development Plan, the institutional arrangements and reforms (and particularly human resource and financial management), and the budgetary framework (MTEF) so as to have a coherent package for analysis in an integrated manner for discussion with MOH, the Ministry of Finance, and the Civil Service Ministry; the core principles for financing with priority to: (i) ensuring (and then maintaining) the functionality of existing health facilities before rehabilitating or building new ones; (ii) favoring the extremely poor and disadvantaged regions during the budget allocation process; and (iii) ensuring proper resource transfer to cost centers at the district level; and the substance of the draft letter of understanding which would link the various participants in the organization and financing of the sector-wide approach. 5
20 23. Subsequently, three key issues emerged. First, there were political uncertainties related to: (i) the pending legislative and presidential elections implying the need to re-establish consensus following any political changes; and (ii) the Ministry of Finance s reluctance to confirm the financial projections underlying the financing projections of the HDP implying the need to revise downward the initial goals and objectives. Second, the challenge of limiting the population s contribution to health expenditures (estimated by the national health accounts study at 55% of total health expenditures) became evident, triggering discussions about the need to urgently define an exemption policy to allow the poor to have access to a minimum package of services. 24. Third, the unavailability of IDA funds contributed to a delay in project processing, which was used by the team to conduct a quality enhancement review (February 2005) and to make progress on several key implementation readiness areas, including donor coordination and sector financing, fiduciary arrangements, and a program of reforms within the HDP. These included proposed measures to: (i) encourage (using incentives) the deployment of more health staff to rural areas; (ii) exonerate certain groups (poor), products (contraceptives), and services (prenatal care) from cost recovery; (iii) reform the national drug importing and distribution system; and (iv) introduce performance based management. 25. The decision meeting and appraisal mission were conducted in June 2005, negotiations were held in November 2005, and the project was approved by the Board in December Project design. The proposed project was the third operation in the health sector in Niger, following: (i) the Health Development Project ( ; US$27.8 million); and (ii) the Health Sector Development Project ( ; US$40 million), which contributed to the implementation of the HDP ( ). Both projects emphasized sector reform (to organize and finance the sector; strengthen the management of human resources, pharmaceuticals; improve service delivery; etc.) but were ultimately considered unsatisfactory for having failed to effectively strengthen institutional capacity and human resources as a prelude to addressing the key systemic issues The option of a third standard project to finance specific activities was briefly considered, but it was rejected as inadequate given: (i) the existing strategic framework (the MDGs, PRSP, and HDP); (ii) the sector s systemic and management issues and the ongoing RSRC 2 (DPL2) intended to address key policy bottlenecks in the health sector (e.g., budget allocation and execution, human resource management, implementation of selected, fully subsidized services, etc.); and (iii) the need to quickly develop and align health sector implementation capacity with the PRSC approach. 28. The ICR of the previous project had discussed lessons learned particularly with respect to: (i) being realistic about the scope and speed of health sector reform; (ii) ensuring that the indicators chosen are really appropriate and reasonable; (iii) being ready for implementation; and (iv) defining what improved quality really means to stakeholders, especially the rural poor. But, as the Quality Enhancement Review (QER) comments suggest, the SWAp design did not easily allow the team to incorporate these lessons. 29. First, the identification mission optimistically envisioned a two-phased approach with early testing followed by extensive pooling after the mid-term review; but the PCN described a SWAp which would almost certainly be a hybrid and modest in its ambitions, given the limited national capacity and number of participating partners. The QER urged the team to be more explicit and candid about the project approach (SIL or SIM) and indicate strengths (using performance-based support to achieve certain objectives) and weaknesses (indicating that it will make progress towards a SWAp at some undefined time in the future). The project was ultimately 6
21 identified as a SIM, and the PAD attempted to address the other concerns in the draft Memorandum of Understanding (MoU) included in the PAD (Annex 17). 30. Second, the QER questioned several other design issues related to the feasibility of: (i) linking broad support of the Health Development Plan with targeted assistance in selected areas (human resources management, financial management, institutional and organizational change, and reproductive health interventions); (ii) coordinating formal and informal arrangements to manage the complementarity of sector financing; and (iii) combining managerially challenging initiatives (performance-based results) and ambitious institutional changes (decentralization, direct funds transfers, etc.). The PAD responded to these concerns with additional annexes (Annexes 15, 18, 19, and 21). 31. Third, the QER also focused extensively on Niger s estimated financial needs for the health sector, questioned whether IDA s proposed annual contribution would be sufficient to have an impact, and urged the team to consider disbursing over less than five years (as a faster transition to a SWAp approach) or increasing the size of the IDA credit. The PAD included a lengthy discussions of sector financing (in Annex 1, which also identified other sources of sector financing, Annex 2, and Annex 9), but did not directly address the issue of whether the amount of the credit was sufficient. 32. Finally, though the QER did not focus explicitly on the risk table presented in the PAD, the dozen or so risks (and risk mitigation measures) might have been addressed in more detail. In retrospect, each of the potential risks was correctly identified and accurately assessed, and several were especially prescient, notably the risk of sustaining leadership in the context of rapid organizational and technical change. The decision meeting revisited several of the design features and also expressed concern about the fiduciary capabilities of the ministry. 33. At negotiations, a number of important design features were confirmed, and agreement was reached on the details of the Malaria Booster component. At that point, while all of the partners remained supportive of the approach, but only the French Development Agency (AFD) remained as a formal partner with the Bank in financing the project. 34. Quality at Entry. The QER panel suggested that in addition to the usual implementation readiness items in the fiduciary areas, the task team have in place by negotiations: (i) the MoU with the donors (which had been the intention of the task team); (ii) the first year annual work program for the health sector with full funding secured; and (iii) the clarification of the harmonization/coordination mechanisms. These recommendations were followed but, along with ratification of the credit agreement, delayed effectiveness until July 20, Implementation 35. Already ambitious, the project was implemented in an evolving national context characterized by: (i) initial overall political stability (which was subsequently followed by periods of political instability); (ii) the introduction of autonomy for governing at the local community level; and (iii) key reforms in the areas of public financial management and public procurement. Project implementation within the health sector context was marked by: (i) the expected difficulties of implementing a sector-wide approach 4 ; and (ii) the introduction of free health services for specific groups as part of the President s Special Program. The result was a project implemented at two different speeds, with modest advances in implementing the SWAp accompanied by often 4 See Denise Vaillancourt, Do Health Sector-Wide Approaches Achieve Results? IEG Working Paper 2009/4. 7
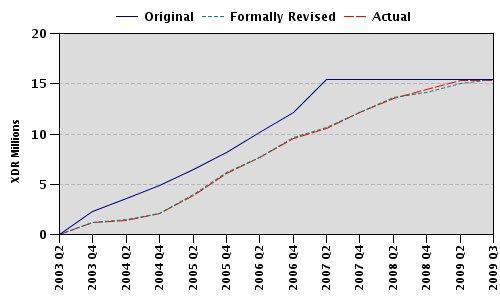
22 substantial advances in results. 36. Project disbursement. The original Development Credit Agreement (Cr 4141-NIR) in the amount of SDR 24.2 million (US$35.0 million equivalent) was signed on February 16, 2006 and became effective on July 20, Financing agreements to participate in the pooled account (or Common Fund) were subsequently reached with the French Development Agency (as a condition of effectiveness), the Spanish Development Agency, GAVI, and UNICEF. Initially, it was expected that the Common Fund would: (i) receive funds from IDA and AFD based on periodic Financial Monitoring Reports (FMRs) 5 ; and (ii) disburse funds directly against an agreed-to annual action plan (AAP). A summary of the cumulative disbursements into the Common Fund (by source) and the expenditures of the Common Fund (by category) is presented below. 6 Table 1: Cumulative financing and expenditures of the Common Fund (in CFA million) Ressources / Emplois (at 30/06) Financing (by source) Direct participants IDA AFD AECID GAVI UNICEF Other sources AFD / AT UNFPA Expenditures (by category) Central level Regional level Malaria The project had early disbursement delays (only 43% of the proceeds had been disbursed as of June 2009), resulting from the ministry s limited administrative and technical capacity in implementing the report-based disbursement process. The pace of disbursements increased rapidly thereafter, due in large measure to improved training of fiduciary staff and a series of sizeable procurements for works (ministry expansion and hospital/health center rehabilitation) and goods (ARVs and malaria drugs and supplies). 38. Project implementation. Project success was predicated on implementing reforms, strengthening partnerships, and enhancing the effectiveness and efficiency of the sector, which would together contribute to the achievement of the PDO. In the end, project implementation took a somewhat different path with: (i) impressive progress on most of the key performance indicators; and with considerable investments of time and money, and (ii) slow (but positive) movement on the reforms, partnerships, and ways of doing business. Throughout project implementation, achievement of the PDO, implementation progress, and the different components were all consistently rated Satisfactory or Moderately Satisfactory. Progress on the key performance 5 Subsequently, believing that the FMRs did not provide sufficient information, AFD added the results of the annual audit as a condition for its second tranche release. 6 The disbursement profile is presented in Section I of the Data Sheet. 8
23 indicators is treated in a subsequent section; progress on implementing several of the SWAp elements mentioned by the IEG study are discussed below. 39. Reforms: Though intended to enhance the reform process 7, the project s progress was (as might be expected) uneven, with advances in some areas and setbacks in others; some examples: (i) the ministerial reorganization recognized the crucial importance of human resources and nutrition and established national directorates, but modified the Directorate of Reproductive Health to be the Directorate for Mother and Child Health; (ii) the development of health financing policy recognized the importance of reducing the burden imposed by cost recovery did not find a sustainable means to ensure free health services and strengthen supply chain management for drugs and other consumables; and (iii) the management of human resources (including the use of performance contracts) accomplished a number of important actions (HR management systems, HR planning, curriculum reform and training, etc.), but effective change in deployment, motivation, career development, etc. (necessarily involving the Ministries of Finance and Civil Service) was difficult to achieve. 40. Partnerships: The quality and functionality of partnerships varied between government and: (i) its partners (and among the partners); and (ii) the Bank and AFD as the principal partners in the Common Fund. Government and its partners: As in most developing countries, the multilateral, bilateral, and NGO agencies follow their own institutional mandates, agendas, and procedures, though most have aligned their technical interventions (at Government insistence) with the Health Development Plan. Relationships are (mostly) cordial with frequent (at least 4-5 times a year) meetings between the Ministry and its partners and, with Ministry agreement, partners were encouraged to meet and harmonize their viewpoints for discussion. However, while several additional partners were attracted to the Common Fund, there does not seem to have been a concerted effort to encourage and/or recruit other partners, even on partial or limited terms. Common Fund partners: While AFD, the Bank, and the Government have generally agreed on procedures, these have involved numerous documents: legal (credit agreement and convention), procedural (procedures manual), and interpretational (memorandum of understanding-lettre d entente and a memorandum of operational procedures-note de conduite) which have not in every case resolved all of the issues to the satisfaction of the three parties. In addition, while the different parties agreed on the basic program documents (MTEF, Annual Action Plans and Budgets, Biannual progress reports, etc.), they were not uniformly in agreement on a number of issues including the timing and alignment of document submission and the criteria for the periodic disbursements into the Common Fund. 41. Ways of doing business: The SWAp sought to: (i) enhance efficiency with increased predictability, flow, and use of sector financial resources; and (ii) strengthen program effectiveness with improved tools and processes to plan, budget and manage funds, and measure results. From a financing perspective, the sector suffered and has continued to suffer from chronic underfunding from domestic resources. This has become particularly critical as the government has fallen behind in its commitment to provide health facilities with the funds lost through the removal of user fees for targeted populations. 7 In addition to the project, several of the PRSC triggers involved health sector reform measures for financing, HR, sector management, etc. 9
IMPLEMENTATION COMPLETION AND RESULTS REPORT (IDA TF-58152) ON A CREDIT IN THE AMOUNT OF SDR6.7 MILLION (US$ 10 MILLION EQUIVALENT) TO THE
 ON A CREDIT IN THE AMOUNT OF SDR6.7 MILLION (US$ 10 MILLION EQUIVALENT) TO THE") Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized AFTHE AFCS1 Africa Region Document of The World Bank Report No: ICR00001497 IMPLEMENTATION
Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized AFTHE AFCS1 Africa Region Document of The World Bank Report No: ICR00001497 IMPLEMENTATION
Actual Project Name : Madagascar Sustainable Health System Development Project Country: Madagascar. Project Costs (US$M US$M):
:") Public Disclosure Authorized IEG ICR Review Independent Evaluation Group 1. Project Data: Date Posted : 03/17/2011 Report Number : ICRR13456 Public Disclosure Authorized PROJ ID : P103606 Appraisal Actual
Public Disclosure Authorized IEG ICR Review Independent Evaluation Group 1. Project Data: Date Posted : 03/17/2011 Report Number : ICRR13456 Public Disclosure Authorized PROJ ID : P103606 Appraisal Actual
FOR OFFICIAL USE ONLY
 Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Document of The World Bank FOR OFFICIAL USE ONLY PROJECT PAPER ON A PROPOSED ADDITIONAL
Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Document of The World Bank FOR OFFICIAL USE ONLY PROJECT PAPER ON A PROPOSED ADDITIONAL
PROJECT INFORMATION DOCUMENT (PID) CONCEPT STAGE. Health Service Delivery Project (HSDP) Region
 CONCEPT STAGE. Health Service Delivery Project (HSDP) Region") PROJECT INFORMATION DOCUMENT (PID) CONCEPT STAGE Project Name Health Service Delivery Project (HSDP) Region AFRICA Sector Health (100%) Project ID P111840 Borrower(s) GOVERNMENT OF ANGOLA Implementing
PROJECT INFORMATION DOCUMENT (PID) CONCEPT STAGE Project Name Health Service Delivery Project (HSDP) Region AFRICA Sector Health (100%) Project ID P111840 Borrower(s) GOVERNMENT OF ANGOLA Implementing
Sector-wide Health System and Social Development Support Project Region
 PROJECT INFORMATION DOCUMENT (PID) CONCEPT STAGE Report No.: AB1473 Country Mali Prpoject ID P093689 Project Name Sector-wide Health System and Social Development Support Project Region AFRICA Sector Health
PROJECT INFORMATION DOCUMENT (PID) CONCEPT STAGE Report No.: AB1473 Country Mali Prpoject ID P093689 Project Name Sector-wide Health System and Social Development Support Project Region AFRICA Sector Health
RESTRUCTURING PAPER ON A PROPOSED PROJECT RESTRUCTURING OF CAMEROON HEALTH SECTOR SUPPORT INVESTMENT PROJECT CREDIT: 4478-CM TO THE
 Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized 1 Document of The World Bank RESTRUCTURING PAPER ON A PROPOSED PROJECT RESTRUCTURING
Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized 1 Document of The World Bank RESTRUCTURING PAPER ON A PROPOSED PROJECT RESTRUCTURING
Institutionalization of National Health Accounts: The Experience of Madagascar. Paper prepared for the World Bank NHA Initiative.
 Institutionalization of National Health Accounts: The Experience of Madagascar Paper prepared for the World Bank NHA Initiative March 11, 2009 1 List of Abbreviations CRESAN DEP ETIMCNS INSTAT MoH MTEF
Institutionalization of National Health Accounts: The Experience of Madagascar Paper prepared for the World Bank NHA Initiative March 11, 2009 1 List of Abbreviations CRESAN DEP ETIMCNS INSTAT MoH MTEF
Ownership, Capacity, Results Focus and Accountability:
 NIGER Ownership, Capacity, Results Focus and Accountability: Lessons for Enhancing the Bank s Program Approach to Health and Population Report No. 106254 JUNE 28, 2016 2016 International Bank for Reconstruction
NIGER Ownership, Capacity, Results Focus and Accountability: Lessons for Enhancing the Bank s Program Approach to Health and Population Report No. 106254 JUNE 28, 2016 2016 International Bank for Reconstruction
Implementation Status & Results Samoa SAMOA HEALTH SECTOR MANAGEMENT PROGRAM SUPPORT PROJECT (P086313)
") Public Disclosure Authorized Public Disclosure Authorized The World Bank Implementation Status & Results Samoa SAMOA HEALTH SECTOR MANAGEMENT PROGRAM SUPPORT PROJECT (P086313) Operation Name: SAMOA HEALTH
Public Disclosure Authorized Public Disclosure Authorized The World Bank Implementation Status & Results Samoa SAMOA HEALTH SECTOR MANAGEMENT PROGRAM SUPPORT PROJECT (P086313) Operation Name: SAMOA HEALTH
THE INTERNATIONAL MONETARY FUND AND INTERNATIONAL DEVELOPMENT ASSOCIATION NIGER
 THE INTERNATIONAL MONETARY FUND AND INTERNATIONAL DEVELOPMENT ASSOCIATION NIGER Poverty Reduction Strategy Paper Progress Report Joint Staff Advisory Note Prepared by the Staffs of the International Monetary
THE INTERNATIONAL MONETARY FUND AND INTERNATIONAL DEVELOPMENT ASSOCIATION NIGER Poverty Reduction Strategy Paper Progress Report Joint Staff Advisory Note Prepared by the Staffs of the International Monetary
Document of The World Bank
 Document of The World Bank PROJECT COMPLETION NOTE OF A LEARNING AND INNOVATION LOAN IN THE AMOUNT OF SDR 2.7 MILLION (US$4 MILLION EQUIVALENT) TO THE REPUBLIC OF MALAWI FOR A DEVELOPMENT LEARNING CENTER
Document of The World Bank PROJECT COMPLETION NOTE OF A LEARNING AND INNOVATION LOAN IN THE AMOUNT OF SDR 2.7 MILLION (US$4 MILLION EQUIVALENT) TO THE REPUBLIC OF MALAWI FOR A DEVELOPMENT LEARNING CENTER
IMPLEMENTATION COMPLETION AND RESULTS REPORT (IDA-H2620) (IDA-4520) (IDA-46610) (IDA-47750) ON A GRANT AND THREE CREDITS
 (IDA-4520) (IDA-46610) (IDA-47750) ON A GRANT AND THREE CREDITS") Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Document of The World Bank IMPLEMENTATION COMPLETION AND RESULTS REPORT (IDA-H2620) (IDA-4520)
Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Document of The World Bank IMPLEMENTATION COMPLETION AND RESULTS REPORT (IDA-H2620) (IDA-4520)
Project development objective/outcomes
 Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized THE SAINT VINCENT & THE GRENADINES HIV/AIDS PREVENTION AND CONTROL PROJECT PE-PO76799
Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized THE SAINT VINCENT & THE GRENADINES HIV/AIDS PREVENTION AND CONTROL PROJECT PE-PO76799
L/C/TF Number(s) Closing Date (Original) Total Financing (USD) IBRD Jun ,000,000.00
 Closing Date (Original) Total Financing (USD) IBRD Jun ,000,000.00") Public Disclosure Authorized 1. Project Data Report Number : ICRR0021272 Public Disclosure Authorized Public Disclosure Authorized Operation ID P159774 Country Fiji Operation Name Fiji Post-Cyclone Winston
Public Disclosure Authorized 1. Project Data Report Number : ICRR0021272 Public Disclosure Authorized Public Disclosure Authorized Operation ID P159774 Country Fiji Operation Name Fiji Post-Cyclone Winston
PROJECT INFORMATION DOCUMENT (PID) CONCEPT STAGE
 CONCEPT STAGE") Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Project Name PROJECT INFORMATION DOCUMENT (PID) CONCEPT STAGE Health Sector Support Project
Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Project Name PROJECT INFORMATION DOCUMENT (PID) CONCEPT STAGE Health Sector Support Project
IMPLEMENTATION COMPLETION AND RESULTS REPORT PROGRAMMATIC CREDITS IN THE AMOUNT OF SDR 54.8 MILLION (US$80 MILLION EQUIVALENT) THE REPUBLIC OF SENEGAL
 THE REPUBLIC OF SENEGAL") Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Document of The World Bank IMPLEMENTATION COMPLETION AND RESULTS REPORT ON PROGRAMMATIC
Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Document of The World Bank IMPLEMENTATION COMPLETION AND RESULTS REPORT ON PROGRAMMATIC
Section 1: Understanding the specific financial nature of your commitment better
 PMNCH 2011 REPORT ON COMMITMENTS TO THE GLOBAL STRATEGY FOR WOMEN S AND CHILDREN S HEALTH QUESTIONNAIRE Norway Completed questionnaire received on September 7 th, 2011 Section 1: Understanding the specific
PMNCH 2011 REPORT ON COMMITMENTS TO THE GLOBAL STRATEGY FOR WOMEN S AND CHILDREN S HEALTH QUESTIONNAIRE Norway Completed questionnaire received on September 7 th, 2011 Section 1: Understanding the specific
IMPLEMENTATION COMPLETION AND RESULTS REPORT (IDA-H0430 IDA-H2060 IDA-H3840) GRANTS IN THE AMOUNT OF SDR 76.9 MILLION (US$ MILLION EQUIVALENT)
 GRANTS IN THE AMOUNT OF SDR 76.9 MILLION (US$ MILLION EQUIVALENT)") Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Document of The World Bank Report No: ICR00001294 IMPLEMENTATION COMPLETION AND RESULTS
Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Document of The World Bank Report No: ICR00001294 IMPLEMENTATION COMPLETION AND RESULTS
Document of The World Bank IMPLEMENTATION COMPLETION AND RESULTS REPORT (IBRD-47320) ON A LOAN IN THE AMOUNT OF US$ 9.
 ON A LOAN IN THE AMOUNT OF US$ 9.") Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Document of The World Bank Report No: ICR00002035 IMPLEMENTATION COMPLETION AND RESULTS
Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Document of The World Bank Report No: ICR00002035 IMPLEMENTATION COMPLETION AND RESULTS
Document of The World Bank IMPLEMENTATION COMPLETION AND RESULTS REPORT (IDA-4072 GUI) ON A CREDIT
 ON A CREDIT") Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Document of The World Bank IMPLEMENTATION COMPLETION AND RESULTS REPORT (IDA-4072 GUI)
Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Document of The World Bank IMPLEMENTATION COMPLETION AND RESULTS REPORT (IDA-4072 GUI)
Implementation Status & Results Mozambique Health Commodity Security Project (P121060)
") Public Disclosure Authorized Public Disclosure Authorized The World Bank Implementation Status & Results Mozambique Health Commodity Security Project (P121060) Operation Name: Health Commodity Security
Public Disclosure Authorized Public Disclosure Authorized The World Bank Implementation Status & Results Mozambique Health Commodity Security Project (P121060) Operation Name: Health Commodity Security
FOR OFFICIAL USE ONLY RESTRUCTURING PAPER ON A PROPOSED PROJECT RESTRUCTURING THE INFORMAL SETTLEMENTS IMPROVEMENT PROJECT CREDIT 4873-KE
 Public Disclosure Authorized Document of The World Bank FOR OFFICIAL USE ONLY Report No: 104604 Public Disclosure Authorized Public Disclosure Authorized RESTRUCTURING PAPER ON A PROPOSED PROJECT RESTRUCTURING
Public Disclosure Authorized Document of The World Bank FOR OFFICIAL USE ONLY Report No: 104604 Public Disclosure Authorized Public Disclosure Authorized RESTRUCTURING PAPER ON A PROPOSED PROJECT RESTRUCTURING
CTF-SCF/TFC.4/Inf.2 March 13, Joint Meeting of the CTF and SCF Trust Fund Committees Manila, Philippines March 16, 2010
 CTF-SCF/TFC.4/Inf.2 March 13, 2010 Joint Meeting of the CTF and SCF Trust Fund Committees Manila, Philippines March 16, 2010 BENCHMARKING CIF'S ADMINISTRATIVE COSTS 2 Background 1. The Joint Trust Fund
CTF-SCF/TFC.4/Inf.2 March 13, 2010 Joint Meeting of the CTF and SCF Trust Fund Committees Manila, Philippines March 16, 2010 BENCHMARKING CIF'S ADMINISTRATIVE COSTS 2 Background 1. The Joint Trust Fund
US$M): Sector Board : ED Cofinancing (US$M US$M): Loan/Credit (US$M Sector(s): US$M):
: Sector Board : ED Cofinancing (US$M US$M): Loan/Credit (US$M Sector(s): US$M):") IEG ICR Review Independent Evaluation Group 1. Project Data: Date Posted : 11/19/2007 Report Number : ICRR12797 PROJ ID : P006204 Project Name : Bo- Education Quality Project Appraisal Actual Project Costs
IEG ICR Review Independent Evaluation Group 1. Project Data: Date Posted : 11/19/2007 Report Number : ICRR12797 PROJ ID : P006204 Project Name : Bo- Education Quality Project Appraisal Actual Project Costs
US$M): Sector Board : Social Development Cofinancing (US$M (US$M US$M): US$M):
: Sector Board : Social Development Cofinancing (US$M (US$M US$M): US$M):") Public Disclosure Authorized IEG ICR Review Independent Evaluation Group Report Number : ICRR14437 1. Project Data: Date Posted : 09/22/2014 Public Disclosure Authorized Public Disclosure Authorized Country:
Public Disclosure Authorized IEG ICR Review Independent Evaluation Group Report Number : ICRR14437 1. Project Data: Date Posted : 09/22/2014 Public Disclosure Authorized Public Disclosure Authorized Country:
Country Practice Area(Lead) Additional Financing Tanzania Health, Nutrition & Population P147991
 Additional Financing Tanzania Health, Nutrition & Population P147991") Public Disclosure Authorized Independent Evaluation Group (IEG) 1. Project Data Report Number : ICRR0020727 Public Disclosure Authorized Public Disclosure Authorized Project ID P125740 Project Name TZ-Basic
Public Disclosure Authorized Independent Evaluation Group (IEG) 1. Project Data Report Number : ICRR0020727 Public Disclosure Authorized Public Disclosure Authorized Project ID P125740 Project Name TZ-Basic
Booklet C.2: Estimating future financial resource needs
 Booklet C.2: Estimating future financial resource needs This booklet describes how managers can use cost information to estimate future financial resource needs. Often health sector budgets are based on
Booklet C.2: Estimating future financial resource needs This booklet describes how managers can use cost information to estimate future financial resource needs. Often health sector budgets are based on
AFRICAN DEVELOPMENT BANK GROUP MADAGASCAR: HIPC APPROVAL DOCUMENT COMPLETION POINT UNDER THE ENHANCED FRAMEWORK
 AFRICAN DEVELOPMENT BANK GROUP MADAGASCAR: HIPC APPROVAL DOCUMENT COMPLETION POINT UNDER THE ENHANCED FRAMEWORK March 2005 TABLE OF CONTENTS Page I Introduction... 1 II Madagascar s Qualification for the
AFRICAN DEVELOPMENT BANK GROUP MADAGASCAR: HIPC APPROVAL DOCUMENT COMPLETION POINT UNDER THE ENHANCED FRAMEWORK March 2005 TABLE OF CONTENTS Page I Introduction... 1 II Madagascar s Qualification for the
IMPLEMENTATION COMPLETION AND RESULTS REPORT (4410-NE) ON A CREDIT IN THE AMOUNT OF SDR 14.4 MILLION (US$23.7 MILLION EQUIVALENT) TO THE
 ON A CREDIT IN THE AMOUNT OF SDR 14.4 MILLION (US$23.7 MILLION EQUIVALENT) TO THE") Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Document of The World Bank IMPLEMENTATION COMPLETION AND RESULTS REPORT (4410-NE) ON
Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Document of The World Bank IMPLEMENTATION COMPLETION AND RESULTS REPORT (4410-NE) ON
INTERNATIONAL MONETARY FUND AND INTERNATIONAL DEVELOPMENT ASSOCIATION BENIN. Second Poverty Reduction Strategy Paper Joint Staff Advisory Note
 INTERNATIONAL MONETARY FUND AND INTERNATIONAL DEVELOPMENT ASSOCIATION BENIN Second Poverty Reduction Strategy Paper Joint Staff Advisory Note Prepared by the Staffs of the International Monetary Fund (IMF)
INTERNATIONAL MONETARY FUND AND INTERNATIONAL DEVELOPMENT ASSOCIATION BENIN Second Poverty Reduction Strategy Paper Joint Staff Advisory Note Prepared by the Staffs of the International Monetary Fund (IMF)
Document of The World Bank FOR OFFICIAL USE ONLY IMPLEMENTATION COMPLETION AND RESULTS REPORT (IDA-H4630 TF TF-96083) ON AN
 ON AN") Public Disclosure Authorized Document of The World Bank FOR OFFICIAL USE ONLY Report No: ICR00003680 Public Disclosure Authorized IMPLEMENTATION COMPLETION AND RESULTS REPORT (IDA-H4630 TF-92396 TF-96083)
Public Disclosure Authorized Document of The World Bank FOR OFFICIAL USE ONLY Report No: ICR00003680 Public Disclosure Authorized IMPLEMENTATION COMPLETION AND RESULTS REPORT (IDA-H4630 TF-92396 TF-96083)
L/C/TF Number(s) Closing Date (Original) Total Financing (USD) TF Dec ,580,000.00
 Closing Date (Original) Total Financing (USD) TF Dec ,580,000.00") Public Disclosure Authorized Independent Evaluation Group (IEG) 1. Project Data Report Number : ICRR0020620 Public Disclosure Authorized Public Disclosure Authorized Operation ID P147166 Country Haiti
Public Disclosure Authorized Independent Evaluation Group (IEG) 1. Project Data Report Number : ICRR0020620 Public Disclosure Authorized Public Disclosure Authorized Operation ID P147166 Country Haiti
SECTOR ASSESSMENT (SUMMARY): PUBLIC SECTOR MANAGEMENT (PUBLIC EXPENDITURE AND FISCAL MANAGEMENT) Sector Performance, Problems, and Opportunities
: PUBLIC SECTOR MANAGEMENT (PUBLIC EXPENDITURE AND FISCAL MANAGEMENT) Sector Performance, Problems, and Opportunities") Improving Public Expenditure Quality Program, SP1 (RRP VIE 50051-001) SECTOR ASSESSMENT (SUMMARY): PUBLIC SECTOR MANAGEMENT (PUBLIC EXPENDITURE AND FISCAL MANAGEMENT) 1 Sector Road Map 1. Sector Performance,
Improving Public Expenditure Quality Program, SP1 (RRP VIE 50051-001) SECTOR ASSESSMENT (SUMMARY): PUBLIC SECTOR MANAGEMENT (PUBLIC EXPENDITURE AND FISCAL MANAGEMENT) 1 Sector Road Map 1. Sector Performance,
Zambia s poverty-reduction strategy paper (PRSP) has been generally accepted
 has been generally accepted") 15 ZAMBIA The survey sought to measure objective evidence of progress against 13 key indicators on harmonisation and alignment (see Foreword). A four-point scaling system was used for all of the Yes/No
15 ZAMBIA The survey sought to measure objective evidence of progress against 13 key indicators on harmonisation and alignment (see Foreword). A four-point scaling system was used for all of the Yes/No
THE INTERNATIONAL MONETARY FUND AND THE INTERNATIONAL DEVELOPMENT ASSOCIATION REPUBLIC OF DJIBOUTI
 THE INTERNATIONAL MONETARY FUND AND THE INTERNATIONAL DEVELOPMENT ASSOCIATION REPUBLIC OF DJIBOUTI Interim Poverty Reduction Strategy Paper Joint Staff Assessment Prepared by the Staff of the International
THE INTERNATIONAL MONETARY FUND AND THE INTERNATIONAL DEVELOPMENT ASSOCIATION REPUBLIC OF DJIBOUTI Interim Poverty Reduction Strategy Paper Joint Staff Assessment Prepared by the Staff of the International
Liberia Reconstruction Trust Fund Implementation Manual
 Liberia Reconstruction Trust Fund Implementation Manual Updated November 2009 2011-02-28 LRTF Implementation Manual 1 I. Background... 3 II. Coverage... 3 III. General Principles... 4 IV. Project Development
Liberia Reconstruction Trust Fund Implementation Manual Updated November 2009 2011-02-28 LRTF Implementation Manual 1 I. Background... 3 II. Coverage... 3 III. General Principles... 4 IV. Project Development
Project Costs (US$M):
:") Public Disclosure Authorized IEG ICR Review Independent Evaluation Group 1. Project Data: Date Posted: 10/05/2015 Report Number: ICRR14849 Public Disclosure Authorized Public Disclosure Authorized Public
Public Disclosure Authorized IEG ICR Review Independent Evaluation Group 1. Project Data: Date Posted: 10/05/2015 Report Number: ICRR14849 Public Disclosure Authorized Public Disclosure Authorized Public
RESTRUCTURING PAPER ON A PROPOSED PROJECT RESTRUCTURING OF URBAN III - PHASE II PROJECT GRANT IDA-H3300 APPROVED ON JULY 9, 2007
 Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Document of The World Bank RESTRUCTURING PAPER ON A PROPOSED PROJECT RESTRUCTURING OF
Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Document of The World Bank RESTRUCTURING PAPER ON A PROPOSED PROJECT RESTRUCTURING OF
UNICEF s equity approach: from the 2010 Narrowing the Gaps study via equity focused programming and monitoring to a Narrowing the Gaps+5 study &
 UNICEF s equity approach: from the 2010 Narrowing the Gaps study via equity focused programming and monitoring to a Narrowing the Gaps+5 study & EQUIST Narrowing the Gaps: Right in Principle, Right in
UNICEF s equity approach: from the 2010 Narrowing the Gaps study via equity focused programming and monitoring to a Narrowing the Gaps+5 study & EQUIST Narrowing the Gaps: Right in Principle, Right in
IMPLEMENTATION COMPLETION AND RESULTS REPORT (IDA IDA IDA-47610) ON A CREDIT
 ON A CREDIT") Public Disclosure Authorized Document of The World Bank Report No: ICR2482 Public Disclosure Authorized IMPLEMENTATION COMPLETION AND RESULTS REPORT (IDA-0 IDA-1 IDA-47610) ON A CREDIT Public Disclosure
Public Disclosure Authorized Document of The World Bank Report No: ICR2482 Public Disclosure Authorized IMPLEMENTATION COMPLETION AND RESULTS REPORT (IDA-0 IDA-1 IDA-47610) ON A CREDIT Public Disclosure
GUIDELINES FOR PREPARING A NATIONAL IMMUNIZATION PROGRAM FINANCIAL SUSTAINABILITY PLAN
 GUIDELINES FOR PREPARING A NATIONAL IMMUNIZATION PROGRAM FINANCIAL SUSTAINABILITY PLAN Prepared by: The Financing Task Force of the Global Alliance for Vaccines and Immunization April 2004 Contents Importance
GUIDELINES FOR PREPARING A NATIONAL IMMUNIZATION PROGRAM FINANCIAL SUSTAINABILITY PLAN Prepared by: The Financing Task Force of the Global Alliance for Vaccines and Immunization April 2004 Contents Importance
Acronyms List. AIDS CCM GFATM/GF HIV HR HSS IP M&E MDG MoH NGO PLHIV/PLH PR SR TA UN UNAIDS UNDP UNESCO UNFPA UNICEF WG WHO NSP NPA MEC
 Acronyms List AIDS CCM GFATM/GF HIV HR HSS IP M&E MDG MoH NGO PLHIV/PLH PR SR TA UN UNAIDS UNDP UNESCO UNFPA UNICEF WG WHO NSP NPA MEC Acquired immunodeficiency syndrome Country Coordinating Mechanism,
Acronyms List AIDS CCM GFATM/GF HIV HR HSS IP M&E MDG MoH NGO PLHIV/PLH PR SR TA UN UNAIDS UNDP UNESCO UNFPA UNICEF WG WHO NSP NPA MEC Acquired immunodeficiency syndrome Country Coordinating Mechanism,
Health System Strengthening
 Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Health System Strengthening Issues Note The World Bank Group 36114 Moscow Washington
Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Health System Strengthening Issues Note The World Bank Group 36114 Moscow Washington
Country Practice Area(Lead) Additional Financing Croatia Finance & Markets P129220
 Additional Financing Croatia Finance & Markets P129220") Public Disclosure Authorized Independent Evaluation Group (IEG) 1. Project Data Report Number : ICRR0020731 Public Disclosure Authorized Public Disclosure Authorized Project ID P116080 Project Name EXPORT
Public Disclosure Authorized Independent Evaluation Group (IEG) 1. Project Data Report Number : ICRR0020731 Public Disclosure Authorized Public Disclosure Authorized Project ID P116080 Project Name EXPORT
Issues paper: Proposed Methodology for the Assessment of the BPoA. Draft July Susanna Wolf
 Issues paper: Proposed Methodology for the Assessment of the BPoA Draft July 2010 Susanna Wolf Introduction The Fourth United Nations Conference on the Least Developed Countries (UNLDC IV) will have among
Issues paper: Proposed Methodology for the Assessment of the BPoA Draft July 2010 Susanna Wolf Introduction The Fourth United Nations Conference on the Least Developed Countries (UNLDC IV) will have among
Health Planning Cycle
 Health Planning Cycle Moazzam Ali Department of Reproductive Health and Research WHO In today's presentation Definitions Rationale for health planning Health planning cycle outline Step by step introduction
Health Planning Cycle Moazzam Ali Department of Reproductive Health and Research WHO In today's presentation Definitions Rationale for health planning Health planning cycle outline Step by step introduction
FOR OFFICIAL USE ONLY
 Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Document of The World Bank FOR OFFICIAL USE ONLY FOOD PRICE CRISIS RESPONSE TRUST FUND
Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Document of The World Bank FOR OFFICIAL USE ONLY FOOD PRICE CRISIS RESPONSE TRUST FUND
IMPLEMENTATION COMPLETION AND RESULTS REPORT (IDA TF-92459) ON A CREDIT IN THE AMOUNT OF SDR MILLION (US$30.00 MILLION EQUIVALENT) TO THE
 ON A CREDIT IN THE AMOUNT OF SDR MILLION (US$30.00 MILLION EQUIVALENT) TO THE") Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Document of The World Bank IMPLEMENTATION COMPLETION AND RESULTS REPORT (IDA-42570 TF-92459)
Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Document of The World Bank IMPLEMENTATION COMPLETION AND RESULTS REPORT (IDA-42570 TF-92459)
Accelerator Discussion Frame Accelerator 1. Sustainable Financing
 Accelerator Discussion Frame Accelerator 1. Sustainable Financing Why is an accelerator on sustainable financing needed? One of the most effective ways to reach the SDG3 targets is to rapidly improve the
Accelerator Discussion Frame Accelerator 1. Sustainable Financing Why is an accelerator on sustainable financing needed? One of the most effective ways to reach the SDG3 targets is to rapidly improve the
BOTSWANA BUDGET BRIEF 2018 Health
 BOTSWANA BUDGET BRIEF 2018 Health Highlights Botswana s National Health Policy and Integrated Health Service Plan for 20102020 (IHSP) are child-sensitive and include specific commitments to reducing infant,
BOTSWANA BUDGET BRIEF 2018 Health Highlights Botswana s National Health Policy and Integrated Health Service Plan for 20102020 (IHSP) are child-sensitive and include specific commitments to reducing infant,
L/C/TF Number(s) Closing Date (Original) Total Project Cost (USD) IBRD Dec ,000, Original Commitment 400,000,
 Closing Date (Original) Total Project Cost (USD) IBRD Dec ,000, Original Commitment 400,000,") Public Disclosure Authorized Independent Evaluation Group (IEG) 1. Project Data Report Number : ICRR0020001 Public Disclosure Authorized Project ID P100580 Country Ukraine Project Name ROADS & SAFETY IMPROVEMENT
Public Disclosure Authorized Independent Evaluation Group (IEG) 1. Project Data Report Number : ICRR0020001 Public Disclosure Authorized Project ID P100580 Country Ukraine Project Name ROADS & SAFETY IMPROVEMENT
Document of The World Bank IMPLEMENTATION COMPLETION AND RESULTS REPORT (IDA-H2190) ON A GRANT
 ON A GRANT") Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Document of The World Bank Report No: ICR0000567 IMPLEMENTATION COMPLETION AND RESULTS
Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Document of The World Bank Report No: ICR0000567 IMPLEMENTATION COMPLETION AND RESULTS
Actual Project Name : Social Insurance. US$9.7 US$9.4 Technical Assistance Project (SITAP) Country: Bosnia and US$M): Project Costs (US$M
 Country: Bosnia and US$M): Project Costs (US$M") IEG ICR Review Independent Evaluation Group 1. Project Data: Date Posted : 10/22/2008 Report Number : ICRR12969 PROJ ID : P071004 Appraisal Actual Project Name : Social Insurance Project Costs (US$M US$M):
IEG ICR Review Independent Evaluation Group 1. Project Data: Date Posted : 10/22/2008 Report Number : ICRR12969 PROJ ID : P071004 Appraisal Actual Project Name : Social Insurance Project Costs (US$M US$M):
Rwanda. UNICEF/Till Muellenmeister. Health Budget Brief
 Rwanda UNICEF/Till Muellenmeister Health Budget Brief Investing in children s health in Rwanda 217/218 Health Budget Brief: Investing in children s health in Rwanda 217/218 United Nations Children s Fund
Rwanda UNICEF/Till Muellenmeister Health Budget Brief Investing in children s health in Rwanda 217/218 Health Budget Brief: Investing in children s health in Rwanda 217/218 United Nations Children s Fund
ONE WASH NATIONAL PROGRAMME (OWNP)
") ONE WASH NATIONAL PROGRAMME (OWNP) ONE Plan ONE Budget ONE Report planning with linked strategic and annual WASH plans at each level budgeting re ecting all WASH-related investments and expenditures financial
ONE WASH NATIONAL PROGRAMME (OWNP) ONE Plan ONE Budget ONE Report planning with linked strategic and annual WASH plans at each level budgeting re ecting all WASH-related investments and expenditures financial
INTEGRATED SAFEGUARDS DATASHEET APPRAISAL STAGE
 Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized I. Basic Information Date prepared/updated: 05/10/2007 INTEGRATED SAFEGUARDS DATASHEET
Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized I. Basic Information Date prepared/updated: 05/10/2007 INTEGRATED SAFEGUARDS DATASHEET
Document of The World Bank
 Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Document of The World Bank IMPLEMENTATION COMPLETION AND RESULTS REPORT (IDA-35380 IDA-35381)
Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Document of The World Bank IMPLEMENTATION COMPLETION AND RESULTS REPORT (IDA-35380 IDA-35381)
AFRICAN DEVELOPMENT BANK GROUP SENEGAL : HIPC APPROVAL DOCUMENT COMPLETION POINT UNDER THE ENHANCED FRAMEWORK
 AFRICAN DEVELOPMENT BANK GROUP SENEGAL : HIPC APPROVAL DOCUMENT COMPLETION POINT UNDER THE ENHANCED FRAMEWORK October 2004 TABLE OF CONTENTS Page I Introduction 1 II HIPC Qualification 1 III HIPC Costs
AFRICAN DEVELOPMENT BANK GROUP SENEGAL : HIPC APPROVAL DOCUMENT COMPLETION POINT UNDER THE ENHANCED FRAMEWORK October 2004 TABLE OF CONTENTS Page I Introduction 1 II HIPC Qualification 1 III HIPC Costs
Actual Project Name : Mn - Sustainable Livelihoods Country: Mongolia US$M): Project Costs (US$M
: Project Costs (US$M") IEG ICR Review Independent Evaluation Group 1. Project Data: Date Posted : 10/29/2008 Report Number : ICRR12989 PROJ ID : P067770 Appraisal Actual Project Name : Mn - Sustainable Project Costs (US$M US$M):
IEG ICR Review Independent Evaluation Group 1. Project Data: Date Posted : 10/29/2008 Report Number : ICRR12989 PROJ ID : P067770 Appraisal Actual Project Name : Mn - Sustainable Project Costs (US$M US$M):
L/C/TF Number(s) Closing Date (Original) Total Project Cost (USD) IBRD Sep ,000, Original Commitment 50,000,
 Closing Date (Original) Total Project Cost (USD) IBRD Sep ,000, Original Commitment 50,000,") Public Disclosure Authorized Independent Evaluation Group (IEG) 1. Project Data Report Number : ICRR0020276 Public Disclosure Authorized Project ID P102299 Project Name BW-HIV/AIDS Project SIL (FY09) Country
Public Disclosure Authorized Independent Evaluation Group (IEG) 1. Project Data Report Number : ICRR0020276 Public Disclosure Authorized Project ID P102299 Project Name BW-HIV/AIDS Project SIL (FY09) Country
Document of The World Bank IMPLEMENTATION COMPLETION AND RESULTS REPORT (IBRD TF-57202) ON A LOAN IN THE AMOUNT OF 20.0 MILLION US$ EQUIVALENT)
 ON A LOAN IN THE AMOUNT OF 20.0 MILLION US$ EQUIVALENT)") Public Disclosure Authorized Document of The World Bank Report No: ICR00002536 Public Disclosure Authorized IMPLEMENTATION COMPLETION AND RESULTS REPORT (IBRD-48200 TF-57202) ON A LOAN IN THE AMOUNT OF
Public Disclosure Authorized Document of The World Bank Report No: ICR00002536 Public Disclosure Authorized IMPLEMENTATION COMPLETION AND RESULTS REPORT (IBRD-48200 TF-57202) ON A LOAN IN THE AMOUNT OF
INTERNATIONAL DEVELOPMENT ASSOCIATION AND INTERNATIONAL MONETARY FUND REPUBLIC OF ARMENIA
 INTERNATIONAL DEVELOPMENT ASSOCIATION AND INTERNATIONAL MONETARY FUND REPUBLIC OF ARMENIA Poverty Reduction Strategy Paper Second Progress Report Joint Staff Advisory Note Prepared by the Staffs of the
INTERNATIONAL DEVELOPMENT ASSOCIATION AND INTERNATIONAL MONETARY FUND REPUBLIC OF ARMENIA Poverty Reduction Strategy Paper Second Progress Report Joint Staff Advisory Note Prepared by the Staffs of the
PROJECT INFORMATION DOCUMENT (PID) CONCEPT STAGE Report No.: AB2560 Project Name. Bahia Integrated Water Management Region
 CONCEPT STAGE Report No.: AB2560 Project Name. Bahia Integrated Water Management Region") Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized PROJECT INFORMATION DOCUMENT (PID) CONCEPT STAGE Report No.: AB2560 Project Name Bahia
Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized PROJECT INFORMATION DOCUMENT (PID) CONCEPT STAGE Report No.: AB2560 Project Name Bahia
BENIN: COUNTRY FINANCING PARAMETERS
 BENIN: COUNTRY FINANCING PARAMETERS BENIN: COUNTRY FINANCING PARAMETERS May 5, 2005 Summary 1. This note provides the supporting analysis and background for the country financing parameters under the new
BENIN: COUNTRY FINANCING PARAMETERS BENIN: COUNTRY FINANCING PARAMETERS May 5, 2005 Summary 1. This note provides the supporting analysis and background for the country financing parameters under the new
L/C/TF Number(s) Closing Date (Original) Total Financing (USD) TF-A Jun ,000,000.00
 Closing Date (Original) Total Financing (USD) TF-A Jun ,000,000.00") Public Disclosure Authorized Independent Evaluation Group (IEG) 1. Project Data Report Number : ICRR0020814 Public Disclosure Authorized Public Disclosure Authorized Operation ID P156865 Country West Bank
Public Disclosure Authorized Independent Evaluation Group (IEG) 1. Project Data Report Number : ICRR0020814 Public Disclosure Authorized Public Disclosure Authorized Operation ID P156865 Country West Bank
Document of The World Bank. IMPLEMENTATION COMPLETION AND RESULTS REPORT (IDA UNI and UNI) CREDITS IN THE AMOUNTS OF
 CREDITS IN THE AMOUNTS OF") Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Document of The World Bank IMPLEMENTATION COMPLETION AND RESULTS REPORT (IDA-36530 UNI
Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Document of The World Bank IMPLEMENTATION COMPLETION AND RESULTS REPORT (IDA-36530 UNI
Nigeria - Program to Support Saving One Million Lives (P146583)
") Public Disclosure Authorized AFRICA Nigeria Health, Nutrition & Population Global Practice Requesting Unit: AFCW2 Responsible Unit: GHN07 IBRD/IDA Program-for-Results FY 2015 Team Leader(s): Benjamin P.
Public Disclosure Authorized AFRICA Nigeria Health, Nutrition & Population Global Practice Requesting Unit: AFCW2 Responsible Unit: GHN07 IBRD/IDA Program-for-Results FY 2015 Team Leader(s): Benjamin P.
INTERNATIONAL DEVELOPMENT ASSOCIATION AND INTERNATIONAL MONETARY FUND REPUBLIC OF SIERRA LEONE
 INTERNATIONAL DEVELOPMENT ASSOCIATION AND INTERNATIONAL MONETARY FUND REPUBLIC OF SIERRA LEONE Poverty Reduction Strategy Paper Joint Staff Advisory Note Prepared by the Staffs of the International Development
INTERNATIONAL DEVELOPMENT ASSOCIATION AND INTERNATIONAL MONETARY FUND REPUBLIC OF SIERRA LEONE Poverty Reduction Strategy Paper Joint Staff Advisory Note Prepared by the Staffs of the International Development
IMPLEMENTATION COMPLETION AND RESULTS REPORT (IDA-H2770, IDA-H6880, IDA-49520) A GRANT IN THE AMOUNT OF SDR 10 MILLION (US$15.00 MILLION EQUIVALENT),
 A GRANT IN THE AMOUNT OF SDR 10 MILLION (US$15.00 MILLION EQUIVALENT),") Public Disclosure Authorized Document of The World Bank Report No: ICR00003583 Public Disclosure Authorized IMPLEMENTATION COMPLETION AND RESULTS REPORT (IDA-H2770, IDA-H6880, IDA-49520) ON A GRANT IN
Public Disclosure Authorized Document of The World Bank Report No: ICR00003583 Public Disclosure Authorized IMPLEMENTATION COMPLETION AND RESULTS REPORT (IDA-H2770, IDA-H6880, IDA-49520) ON A GRANT IN
Tanzania Health Sector Development APL II Region
 PROJECT INFORMATION DOCUMENT (PID) CONCEPT STAGE Report No.: AB5049 Project Name Tanzania Health Sector Development APL II Region Africa Sector Health (80%), Non-compulsory health finance (10%), Central
PROJECT INFORMATION DOCUMENT (PID) CONCEPT STAGE Report No.: AB5049 Project Name Tanzania Health Sector Development APL II Region Africa Sector Health (80%), Non-compulsory health finance (10%), Central
L/C/TF Number(s) Closing Date (Original) Total Project Cost (USD) IDA Jun ,300, Original Commitment 30,400,
 Closing Date (Original) Total Project Cost (USD) IDA Jun ,300, Original Commitment 30,400,") Public Disclosure Authorized Independent Evaluation Group (IEG) 1. Project Data Report Number : ICRR0020110 Public Disclosure Authorized Project ID P107311 Country Mozambique Project Name MZ-Nat'l Dec
Public Disclosure Authorized Independent Evaluation Group (IEG) 1. Project Data Report Number : ICRR0020110 Public Disclosure Authorized Project ID P107311 Country Mozambique Project Name MZ-Nat'l Dec
ASIAN DEVELOPMENT BANK
 ASIAN DEVELOPMENT BANK TAR: INO 34149 TECHNICAL ASSISTANCE (Financed from the Japan Special Fund) TO THE REPUBLIC OF INDONESIA FOR PREPARING THE SECOND DECENTRALIZED HEALTH SERVICES PROJECT November 2001
ASIAN DEVELOPMENT BANK TAR: INO 34149 TECHNICAL ASSISTANCE (Financed from the Japan Special Fund) TO THE REPUBLIC OF INDONESIA FOR PREPARING THE SECOND DECENTRALIZED HEALTH SERVICES PROJECT November 2001
Cofinancing (US$M): c. Policy Areas: The policy areas included into the Program Document of the FIRM DPL were the following:
: c. Policy Areas: The policy areas included into the Program Document of the FIRM DPL were the following:") Public Disclosure Authorized IEG ICR Review Independent Evaluation Group 1. Project Data: Date Posted: 03/25/2015 Report Number: ICRR14675 Public Disclosure Authorized Public Disclosure Authorized Public
Public Disclosure Authorized IEG ICR Review Independent Evaluation Group 1. Project Data: Date Posted: 03/25/2015 Report Number: ICRR14675 Public Disclosure Authorized Public Disclosure Authorized Public
IMPLEMENTATION COMPLETION AND RESULTS REPORT. A CREDIT (IDA-46110) and A GRANT (IDA-H6940)
 and A GRANT (IDA-H6940)") Public Disclosure Authorized Document of The World Bank Report No: ICR00003458 Public Disclosure Authorized Public Disclosure Authorized IMPLEMENTATION COMPLETION AND RESULTS REPORT ON A CREDIT (IDA-46110)
Public Disclosure Authorized Document of The World Bank Report No: ICR00003458 Public Disclosure Authorized Public Disclosure Authorized IMPLEMENTATION COMPLETION AND RESULTS REPORT ON A CREDIT (IDA-46110)
IMPLEMENTATION COMPLETION AND RESULTS REPORT (IBRD-48650) ON A LOAN IN THE AMOUNT OF EURO 90.0 MILLION (US$ MILLION EQUIVALENT) TO THE
 ON A LOAN IN THE AMOUNT OF EURO 90.0 MILLION (US$ MILLION EQUIVALENT) TO THE") Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Document of The World Bank IMPLEMENTATION COMPLETION AND RESULTS REPORT (IBRD-48650)
Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Document of The World Bank IMPLEMENTATION COMPLETION AND RESULTS REPORT (IBRD-48650)
Document of The World Bank IMPLEMENTATION COMPLETION AND RESULTS REPORT (IDA IDA IDA-H0400) ON A CREDIT
 ON A CREDIT") Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Document of The World Bank IMPLEMENTATION COMPLETION AND RESULTS REPORT (IDA-37720 IDA-37721
Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Document of The World Bank IMPLEMENTATION COMPLETION AND RESULTS REPORT (IDA-37720 IDA-37721
IMPLEMENTATION COMPLETION AND RESULTS REPORT (IDA-43460) ON A CREDIT IN THE AMOUNT OF SDR 16.4 MILLION (US$ 25.0 MILLION EQUIVALENT) TO THE
 ON A CREDIT IN THE AMOUNT OF SDR 16.4 MILLION (US$ 25.0 MILLION EQUIVALENT) TO THE") Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Document of The World Bank Report No: ICR00002710 IMPLEMENTATION COMPLETION AND RESULTS
Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Document of The World Bank Report No: ICR00002710 IMPLEMENTATION COMPLETION AND RESULTS
Council conclusions on the EU role in Global Health. 3011th FOREIGN AFFAIRS Council meeting Brussels, 10 May 2010
 COUNCIL OF THE EUROPEAN UNION Council conclusions on the EU role in Global Health 3011th FOREIGN AFFAIRS Council meeting Brussels, 10 May 2010 The Council adopted the following conclusions: 1. The Council
COUNCIL OF THE EUROPEAN UNION Council conclusions on the EU role in Global Health 3011th FOREIGN AFFAIRS Council meeting Brussels, 10 May 2010 The Council adopted the following conclusions: 1. The Council
L/C/TF Number(s) Closing Date (Original) Total Project Cost (USD) IBRD Dec ,000,000.00
 Closing Date (Original) Total Project Cost (USD) IBRD Dec ,000,000.00") Public Disclosure Authorized Independent Evaluation Group (IEG) 1. Project Data Report Number : ICRR0020665 Public Disclosure Authorized Public Disclosure Authorized Project ID P117440 Country El Salvador
Public Disclosure Authorized Independent Evaluation Group (IEG) 1. Project Data Report Number : ICRR0020665 Public Disclosure Authorized Public Disclosure Authorized Project ID P117440 Country El Salvador
RESTRUCTURING PAPER ON A PROPOSED PROJECT RESTRUCTURING OF THE SECOND ADDITIONAL FINANCING (CREDIT 4987-CM) BOARD APPROVAL DATE: JUNE 23, 2011
 BOARD APPROVAL DATE: JUNE 23, 2011") Public Disclosure Authorized Document of The World Bank Report No: 65071-CM Public Disclosure Authorized Public Disclosure Authorized RESTRUCTURING PAPER ON A PROPOSED PROJECT RESTRUCTURING OF THE SECOND
Public Disclosure Authorized Document of The World Bank Report No: 65071-CM Public Disclosure Authorized Public Disclosure Authorized RESTRUCTURING PAPER ON A PROPOSED PROJECT RESTRUCTURING OF THE SECOND
US$M): Sector Board : Public Sector (US$M US$M): Cofinancing (US$M. ICR Review
: Sector Board : Public Sector (US$M US$M): Cofinancing (US$M. ICR Review") Public Disclosure Authorized IEG ICR Review Independent Evaluation Group Report Number : ICRR14400 1. Project Data: Date Posted : 07/24/2014 Public Disclosure Authorized Public Disclosure Authorized Public
Public Disclosure Authorized IEG ICR Review Independent Evaluation Group Report Number : ICRR14400 1. Project Data: Date Posted : 07/24/2014 Public Disclosure Authorized Public Disclosure Authorized Public
RESTRUCTURING PAPER ON A PROPOSED PROJECT RESTRUCTURING OF THE TRANSPARENCY AND ACCOUNTABILITY CAPACITY BUILDING PROJECT (CREDIT NO.
 Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Document of The World Bank RESTRUCTURING PAPER ON A PROPOSED PROJECT RESTRUCTURING OF
Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Document of The World Bank RESTRUCTURING PAPER ON A PROPOSED PROJECT RESTRUCTURING OF
The World Bank. Key Dates. Project Development Objectives. Components. Overall Ratings. Implementation Status and Key Decisions
 Public Disclosure Authorized Public Disclosure Copy AFRICA South Sudan Health, Nutrition & Population Global Practice Special Financing Emergency Recovery Loan FY 2012 Seq No: 7 ARCHIVED on 23-Dec-2015
Public Disclosure Authorized Public Disclosure Copy AFRICA South Sudan Health, Nutrition & Population Global Practice Special Financing Emergency Recovery Loan FY 2012 Seq No: 7 ARCHIVED on 23-Dec-2015
IMPLEMENTATION COMPLETION AND RESULTS REPORT (TF056601) ON A MULTI DONOR TRUST FUND TF IN THE AMOUNT OF US$ MILLION EQUIVALENT TO THE
 ON A MULTI DONOR TRUST FUND TF IN THE AMOUNT OF US$ MILLION EQUIVALENT TO THE") Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Document of The World Bank IMPLEMENTATION COMPLETION AND RESULTS REPORT (TF056601) ON
Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Document of The World Bank IMPLEMENTATION COMPLETION AND RESULTS REPORT (TF056601) ON
Year end report (2016 activities, related expected results and objectives)
") Year end report (2016 activities, related expected results and objectives) Country: LIBERIA EU-Lux-WHO UHC Partnership Date: December 31st, 2016 Prepared by: WHO Liberia country office Reporting Period:
Year end report (2016 activities, related expected results and objectives) Country: LIBERIA EU-Lux-WHO UHC Partnership Date: December 31st, 2016 Prepared by: WHO Liberia country office Reporting Period:
INTERNATIONAL MONETARY FUND AND INTERNATIONAL DEVELOPMENT ASSOCIATION ETHIOPIA
 INTERNATIONAL MONETARY FUND AND INTERNATIONAL DEVELOPMENT ASSOCIATION ETHIOPIA Poverty Reduction Strategy Paper Annual Progress Report Joint Staff Assessment Prepared by the Staffs of the IMF and IDA Approved
INTERNATIONAL MONETARY FUND AND INTERNATIONAL DEVELOPMENT ASSOCIATION ETHIOPIA Poverty Reduction Strategy Paper Annual Progress Report Joint Staff Assessment Prepared by the Staffs of the IMF and IDA Approved
Annex 1: The One UN Programme in Ethiopia
 Annex 1: The One UN Programme in Ethiopia Introduction. 1. This One Programme document sets out how the UN in Ethiopia will use a One UN Fund to support coordinated efforts in the second half of the current
Annex 1: The One UN Programme in Ethiopia Introduction. 1. This One Programme document sets out how the UN in Ethiopia will use a One UN Fund to support coordinated efforts in the second half of the current
CONSULTATIVE GROUP MEETING FOR KENYA. Nairobi, November 24-25, Joint Statement of the Government of the Republic of Kenya and the World Bank
 CONSULTATIVE GROUP MEETING FOR KENYA Nairobi, November 24-25, 2003 Joint Statement of the Government of the Republic of Kenya and the World Bank The Government of the Republic of Kenya held a Consultative
CONSULTATIVE GROUP MEETING FOR KENYA Nairobi, November 24-25, 2003 Joint Statement of the Government of the Republic of Kenya and the World Bank The Government of the Republic of Kenya held a Consultative
TARGETING MECHANISMS OF THE SOCIAL SAFETY NET SYSTEMS IN THE COMCEC REGION COUNTRY EXPERIENCE: CAMEROUN
 TARGETING MECHANISMS OF THE SOCIAL SAFETY NET SYSTEMS IN THE COMCEC REGION COUNTRY EXPERIENCE: CAMEROUN I- INTRODUCTION With a surface area of 475,000 km2 and a population of around 22 million people,
TARGETING MECHANISMS OF THE SOCIAL SAFETY NET SYSTEMS IN THE COMCEC REGION COUNTRY EXPERIENCE: CAMEROUN I- INTRODUCTION With a surface area of 475,000 km2 and a population of around 22 million people,
PROJECT INFORMATION DOCUMENT (PID) APPRAISAL STAGE Report No.: AB5681 STRENGTHENING HEALTH ACTIVITY FOR THE RURAL POOR PROJECT Region
 APPRAISAL STAGE Report No.: AB5681 STRENGTHENING HEALTH ACTIVITY FOR THE RURAL POOR PROJECT Region") Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Project Name PROJECT INFORMATION DOCUMENT (PID) APPRAISAL STAGE Report No.: AB5681 STRENGTHENING
Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Project Name PROJECT INFORMATION DOCUMENT (PID) APPRAISAL STAGE Report No.: AB5681 STRENGTHENING
US$M): Sector Board : FPD Cofinancing (US$M US$M): (US$M US$M):
: Sector Board : FPD Cofinancing (US$M US$M): (US$M US$M):") Public Disclosure Authorized IEG ICR Review Independent Evaluation Group Report Number : ICRR13644 1. Project Data: Date Posted : 07/14/2011 Public Disclosure Authorized Public Disclosure Authorized Public
Public Disclosure Authorized IEG ICR Review Independent Evaluation Group Report Number : ICRR13644 1. Project Data: Date Posted : 07/14/2011 Public Disclosure Authorized Public Disclosure Authorized Public
INTERNATIONAL MONETARY FUND AND INTERNATIONAL DEVELOPMENT ASSOCIATION REPUBLIC OF BENIN
 INTERNATIONAL MONETARY FUND AND INTERNATIONAL DEVELOPMENT ASSOCIATION REPUBLIC OF BENIN Annual Progress Report of the Poverty Reduction Strategy Joint Staff Advisory Note Prepared by the Staffs of the
INTERNATIONAL MONETARY FUND AND INTERNATIONAL DEVELOPMENT ASSOCIATION REPUBLIC OF BENIN Annual Progress Report of the Poverty Reduction Strategy Joint Staff Advisory Note Prepared by the Staffs of the
9644/10 YML/ln 1 DG E II
 COUNCIL OF THE EUROPEAN UNION Brussels, 10 May 2010 9644/10 DEVGEN 154 ACP 142 PTOM 21 FIN 192 RELEX 418 SAN 107 NOTE from: General Secretariat dated: 10 May 2010 No. prev. doc.: 9505/10 Subject: Council
COUNCIL OF THE EUROPEAN UNION Brussels, 10 May 2010 9644/10 DEVGEN 154 ACP 142 PTOM 21 FIN 192 RELEX 418 SAN 107 NOTE from: General Secretariat dated: 10 May 2010 No. prev. doc.: 9505/10 Subject: Council
How many operations were planned for the
 Public Disclosure Authorized IEG ICR Review Independent Evaluation Group 1. Project Data: Date Posted: 01/20/2016 Report Number: ICRR14887 Public Disclosure Authorized Public Disclosure Authorized Public
Public Disclosure Authorized IEG ICR Review Independent Evaluation Group 1. Project Data: Date Posted: 01/20/2016 Report Number: ICRR14887 Public Disclosure Authorized Public Disclosure Authorized Public
The World Bank Land Husbandry, Water Harvesting and Hillside Irrigation (P114931)
") Public Disclosure Authorized Public Disclosure Authorized The World Bank RESTRUCTURING PAPER ON A PROPOSED PROJECT RESTRUCTURING OF LAND HUSBANDRY, WATER HARVESTING AND HILLSIDE IRRIGATION PROJECT APPROVED
Public Disclosure Authorized Public Disclosure Authorized The World Bank RESTRUCTURING PAPER ON A PROPOSED PROJECT RESTRUCTURING OF LAND HUSBANDRY, WATER HARVESTING AND HILLSIDE IRRIGATION PROJECT APPROVED
Poverty Profile Executive Summary. Azerbaijan Republic
 Poverty Profile Executive Summary Azerbaijan Republic December 2001 Japan Bank for International Cooperation 1. POVERTY AND INEQUALITY IN AZERBAIJAN 1.1. Poverty and Inequality Measurement Poverty Line
Poverty Profile Executive Summary Azerbaijan Republic December 2001 Japan Bank for International Cooperation 1. POVERTY AND INEQUALITY IN AZERBAIJAN 1.1. Poverty and Inequality Measurement Poverty Line
FOR OFFICIAL USE ONLY
 Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Document of The World Bank FOR OFFICIAL USE ONLY PROJECT PAPER ON A PROPOSED ADDITIONAL
Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Document of The World Bank FOR OFFICIAL USE ONLY PROJECT PAPER ON A PROPOSED ADDITIONAL
UN BHUTAN COUNTRY FUND
 UN BHUTAN COUNTRY FUND Terms of Reference Introduction: 1. The UN system in Bhutan is implementing the One Programme 2014-2018. The One Programme is the result of a highly consultative and participatory
UN BHUTAN COUNTRY FUND Terms of Reference Introduction: 1. The UN system in Bhutan is implementing the One Programme 2014-2018. The One Programme is the result of a highly consultative and participatory
Ex-Ante Evaluation (for Japanese ODA Loan)
") Japanese ODA Loan Ex-Ante Evaluation (for Japanese ODA Loan) 1. Name of the Project Country: The Republic of Kenya Project: Health Sector Policy Loan for Attainment of the Universal Health Coverage Loan
Japanese ODA Loan Ex-Ante Evaluation (for Japanese ODA Loan) 1. Name of the Project Country: The Republic of Kenya Project: Health Sector Policy Loan for Attainment of the Universal Health Coverage Loan
Rwanda. Till Muellenmeister. Health Budget Brief
 Rwanda Till Muellenmeister Health Budget Brief Investing in children s health in Rwanda 217/218 Health Budget Brief: Investing in children s health in Rwanda 217/218 United Nations Children s Fund (UNICEF)
Rwanda Till Muellenmeister Health Budget Brief Investing in children s health in Rwanda 217/218 Health Budget Brief: Investing in children s health in Rwanda 217/218 United Nations Children s Fund (UNICEF)