NEW HIRE EMPLOYEE INFORMATION FORM
|
|
|
- Jack Carson
- 6 years ago
- Views:
Transcription
1 NEW HIRE EMPLOYEE INFORMATION FORM Employee s Name: Social Security Number: Street Address: Birth Date: Apt / PO Box: City: State: Zip: Primary Phone: Name: Emergency Contact Information Relationship: Contact Phone Number (Daytime): I agree that the information listed above is accurate and correct. I understand and agree that it is my responsibility to complete, sign and submit all applicable re-hire forms including, but not limited to, the W-4, I-9, bank direct deposit, employee handbook receipts and other documents deemed appropriate within the required time in order to continue my employment. Employee Signature: Date: Company Name: Information below to be completed by an Authorized Company Representative Department: Job Title: Start Date: Pay Information: RATE $ Hourly Salary Exempt Salary Non-Exempt Normally Scheduled Hours: to Primary Assigned Shift: First Second Third Average Hours Per Week: Full-Time (30+ hrs/wk) Part-Time (20-29 hrs/wk) On-Call (<20 hrs/wk) Seasonal/Temporary Eligible for benefits after probationary period? Yes No Signature of Authorized Company Representative Date Attach the completed document along with W-4/State tax forms, direct deposit information and I-9 form. Send immediately to ensure timely processing.
2

3
4
5
6 Form MO W-4 Missouri Department of Revenue Employee s Withholding Allowance Certificate This certificate is for income tax withholding and child support enforcement purposes only. Type or print. Full Name Social Security Number Filing Status Single r Married r Head of Household r Home Address (Number and Street or Rural Route) City or Town State ZIP Code 1. Allowance For Yourself: Enter 1 for yourself if your filing status is single, married, or head of household... 1 Employee Signature 2. Allowance For Your Spouse: Does your spouse work? r Yes r No If yes, enter 0. If no, enter 1 for your spouse Allowance For Dependents: Enter the number of dependents you will claim on your tax return. Do not claim yourself or your spouse or dependents that your spouse has already claimed on his or her Form MO W Additional Allowances: You may claim additional allowances if you itemize your deductions or have other state tax deductions or credits that lower your tax. Enter the number of additional allowances you would like to claim Total Number Of Allowances You Are Claiming: Add Lines 1 through 4 and enter total here Additional Withholding: If you expect to have a balance due (as a result of interest income, dividends, income from a part-time job, etc.) on your tax return, you may request your employer to withhold an additional amount of tax from each pay period. To calculate the amount needed, divide the amount of the expected balance due by the number of pay periods in a year. Enter the additional amount to be withheld each pay period here... 6 $ 7. Exempt Status: If you had a right to a refund of all of your Missouri income tax withheld last year because you had no tax liability and this year you expect a refund of all Missouri income tax withheld because you expect to have no tax liability, write Exempt on Line 7. See information below If you meet the conditions set forth under the Servicemember Civil Relief Act, as amended by the Military Spouses Residency Relief Act and have no Missouri tax liability, write Exempt on line 8. See information below If income earned as a member of any active duty component of the Armed Forces of the United State is eligible for the military income deduction write exempt on Line Under penalties of perjury, I certify that I am entitled to the number of withholding allowances claimed on this certificate, or I am entitled to claim exempt status. Employee s Signature (Form is not valid unless you sign it) Date (MM/DD/YYYY) / / Employer s Name Employer s Address Employer City State ZIP Code Date Services for Pay First Performed by Employee (MM/DD/YYYY) Federal Employer I.D. Number Missouri Tax Identification Number / / Notice To Employer: Within 20 days of hiring a new employee, send a copy of Form MO W-4 to the Missouri Department of Revenue, P.O. Box 3340, Jefferson City, MO or fax to (573) Employee Information You Do Not Pay Missouri Income Tax on all of the Income You Earn! Visit to try our online withholding calculator. Form MO W-4 is completed so you can have as much take-home pay as possible without an income tax liability due to the state of Missouri when you file your return. Deductions and exemptions reduce the amount of your taxable income. If your income is less than the total of your personal exemption plus your standard deduction, you should mark Exempt on Line 7 above. The following amounts of your annual Missouri adjusted gross income will not be taxed by the state of Missouri when you file your individual income tax return. Single $2,100 personal exemption $6,350 standard deduction $8,450 Total + $1,200 for each dependent + up to $5,000 for federal tax Married Filing Combined $ 4,200 personal exemption $12,700 standard deduction $16,900 Combined Total (For both spouses) + $1,200 for each dependent + up to $10,000 for federal tax If your filing status is married filing combined and your spouse works, do not claim an exemption on Form MO W-4 for your spouse. If you and your spouse have dependents, please be sure only one of you claim the dependents on your Form MO W-4. If both spouses claim the dependents as an allowance on Form MO W-4, it may cause you to owe additional Missouri income tax when you file your return. If you have more than one employer, you should claim a smaller number or no allowances on each Form MO W-4 filed with employers other than your principal employer so the amount withheld will be closer to your amount of total tax. If you itemize your deductions, instead of using the standard deduction, the amount not taxed by Missouri may be a greater or lesser amount. Items to Remember: Head of Household $ 3,500 personal exemption $ 9,350 standard deduction $12,850 Total + $1,200 for each dependent + up to $5,000 for federal tax If you are claiming an Exempt status due to the Military Spouses Residency Relief Act you must provide one of the following to your employer: Leave and Earnings Statement of the non-resident military servicemember, Form W-2 issued to the nonresident military servicemember, a military identification card, or specific military orders received by the servicemember. You must also provide verification of residency such as a copy of your state income tax return filed in your state of residence, a property tax receipt from the state of residence, a current drivers license, vehicle registration or voter ID card. Mail to: Taxation Division Phone: (573) P.O. Box 3340 Fax: (573) Jefferson City, MO Form MO W-4 (Revised ) Visit for additional information regarding new hire reporting.
7 DIRECT DEPOSIT AGREEMENT EMPLOYEE NAME: SSN: COMPANY NAME: DEPOSIT #1 Financial Institution: Route/Transit Number: Account Number: Account Type: CHECKING SAVINGS GLOBAL Debit Card Rtg# Deposit Entire Amount Deposit $ Deposit % DEPOSIT #2 Financial Institution: Route/Transit Number: Account Number: Account Type: CHECKING SAVINGS GLOBAL Debit Card Rtg# Deposit Balance Deposit $ Deposit % We cannot process your direct deposit without the supporting documentation from your financial institution. Attach a voided check, letter from your financial institution or other supporting documentation. Do not attach a deposit slip! If you don't provide supporting documentation, you will receive a live check while your direct deposit account information is being verified. I hereby authorize ContinuumHR to initiate automatic deposits to my account(s) at the financial institution(s) named above. Further, I agree not to hold ContinuumHR responsible for any delay or loss of funds due to incorrect or incomplete information supplied by me or my financial institution or due to an error on the part of my financial institution in depositing funds to my account. I hereby authorize and request ContinuumHR to deduct from my salary or wages and pay to the named financial institution as indicated above. By signing this form I authorize ContinuumHR to initiate credits and to make adjustments, if necessary, for any entry made in error without express written authorization. I shall look solely to the above named financial institution for any information regarding my account. This agreement will remain in effect until ContinuumHR receives a written notice of cancellation from me or my financial institution, or until I submit a new direct deposit form to the Payroll Department. EMPLOYEE SIGNATURE: DATE: CM/NH 01/2017
8 Employment Eligibility Verification Department of Homeland Security U.S. Citizenship and Immigration Services USCIS Form I-9 OMB No Expires 08/31/2019 START HERE: Read instructions carefully before completing this form. The instructions must be available, either in paper or electronically, during completion of this form. Employers are liable for errors in the completion of this form. ANTI-DISCRIMINATION NOTICE: It is illegal to discriminate against work-authorized individuals. Employers CANNOT specify which document(s) an employee may present to establish employment authorization and identity. The refusal to hire or continue to employ an individual because the documentation presented has a future expiration date may also constitute illegal discrimination. Section 1. Employee Information and Attestation (Employees must complete and sign Section 1 of Form I-9 no later than the first day of employment, but not before accepting a job offer.) Last Name (Family Name) First Name (Given Name) Middle Initial Other Last Names Used (if any) Address (Street Number and Name) Apt. Number City or Town State ZIP Code Date of Birth (mm/dd/yyyy) U.S. Social Security Number - - Employee's Address Employee's Telephone Number I am aware that federal law provides for imprisonment and/or fines for false statements or use of false documents in connection with the completion of this form. I attest, under penalty of perjury, that I am (check one of the following boxes): 1. A citizen of the United States 2. A noncitizen national of the United States (See instructions) 3. A lawful permanent resident (Alien Registration Number/USCIS Number): 4. An alien authorized to work until (expiration date, if applicable, mm/dd/yyyy): Some aliens may write "N/A" in the expiration date field. (See instructions) Aliens authorized to work must provide only one of the following document numbers to complete Form I-9: An Alien Registration Number/USCIS Number OR Form I-94 Admission Number OR Foreign Passport Number. QR Code - Section 1 Do Not Write In This Space 1. Alien Registration Number/USCIS Number: OR 2. Form I-94 Admission Number: OR 3. Foreign Passport Number: Country of Issuance: Signature of Employee Today's Date (mm/dd/yyyy) Preparer and/or Translator Certification (check one): I did not use a preparer or translator. A preparer(s) and/or translator(s) assisted the employee in completing Section 1. (Fields below must be completed and signed when preparers and/or translators assist an employee in completing Section 1.) I attest, under penalty of perjury, that I have assisted in the completion of Section 1 of this form and that to the best of my knowledge the information is true and correct. Signature of Preparer or Translator Today's Date (mm/dd/yyyy) Last Name (Family Name) First Name (Given Name) Address (Street Number and Name) City or Town State ZIP Code Employer Completes Next Page Form I-9 07/17/17 N Page 1 of 3

9 Employment Eligibility Verification Department of Homeland Security U.S. Citizenship and Immigration Services USCIS Form I-9 OMB No Expires 08/31/2019 Section 2. Employer or Authorized Representative Review and Verification (Employers or their authorized representative must complete and sign Section 2 within 3 business days of the employee's first day of employment. You must physically examine one document from List A OR a combination of one document from List B and one document from List C as listed on the "Lists of Acceptable Documents.") Employee Info from Section 1 Last Name (Family Name) First Name (Given Name) M.I. Citizenship/Immigration Status List A OR List B AND List C Identity and Employment Authorization Identity Employment Authorization Document Title Document Title Document Title Issuing Authority Document Number Issuing Authority Document Number Issuing Authority Document Number Expiration Date (if any)(mm/dd/yyyy) Expiration Date (if any)(mm/dd/yyyy) Expiration Date (if any)(mm/dd/yyyy) Document Title Issuing Authority Document Number Additional Information QR Code - Sections 2 & 3 Do Not Write In This Space Expiration Date (if any)(mm/dd/yyyy) Document Title Issuing Authority Document Number Expiration Date (if any)(mm/dd/yyyy) Certification: I attest, under penalty of perjury, that (1) I have examined the document(s) presented by the above-named employee, (2) the above-listed document(s) appear to be genuine and to relate to the employee named, and (3) to the best of my knowledge the employee is authorized to work in the United States. The employee's first day of employment (mm/dd/yyyy): (See instructions for exemptions) Signature of Employer or Authorized Representative Today's Date (mm/dd/yyyy) Title of Employer or Authorized Representative Last Name of Employer or Authorized Representative First Name of Employer or Authorized Representative Employer's Business or Organization Name Employer's Business or Organization Address (Street Number and Name) City or Town State ZIP Code Section 3. Reverification and Rehires (To be completed and signed by employer or authorized representative.) A. New Name (if applicable) B. Date of Rehire (if applicable) Last Name (Family Name) First Name (Given Name) Middle Initial Date (mm/dd/yyyy) C. If the employee's previous grant of employment authorization has expired, provide the information for the document or receipt that establishes continuing employment authorization in the space provided below. Document Title Document Number Expiration Date (if any) (mm/dd/yyyy) I attest, under penalty of perjury, that to the best of my knowledge, this employee is authorized to work in the United States, and if the employee presented document(s), the document(s) I have examined appear to be genuine and to relate to the individual. Signature of Employer or Authorized Representative Today's Date (mm/dd/yyyy) Name of Employer or Authorized Representative Form I-9 07/17/17 N Page 2 of 3
10 LISTS OF ACCEPTABLE DOCUMENTS All documents must be UNEXPIRED Employees may present one selection from List A or a combination of one selection from List B and one selection from List C. LIST A Documents that Establish Both Identity and Employment Authorization LIST B LIST C Documents that Establish Employment Authorization OR Documents that Establish Identity AND 1. U.S. Passport or U.S. Passport Card 2. Permanent Resident Card or Alien Registration Receipt Card (Form I-551) 3. Foreign passport that contains a temporary I-551 stamp or temporary I-551 printed notation on a machinereadable immigrant visa 4. Employment Authorization Document that contains a photograph (Form I-766) 5. For a nonimmigrant alien authorized to work for a specific employer because of his or her status: a. Foreign passport; and b. Form I-94 or Form I-94A that has the following: (1) The same name as the passport; and (2) An endorsement of the alien's nonimmigrant status as long as that period of endorsement has not yet expired and the proposed employment is not in conflict with any restrictions or limitations identified on the form. 6. Passport from the Federated States of Micronesia (FSM) or the Republic of the Marshall Islands (RMI) with Form I-94 or Form I-94A indicating nonimmigrant admission under the Compact of Free Association Between the United States and the FSM or RMI 1. Driver's license or ID card issued by a State or outlying possession of the United States provided it contains a photograph or information such as name, date of birth, gender, height, eye color, and address 2. ID card issued by federal, state or local government agencies or entities, provided it contains a photograph or information such as name, date of birth, gender, height, eye color, and address 3. School ID card with a photograph 4. Voter's registration card 5. U.S. Military card or draft record 6. Military dependent's ID card 7. U.S. Coast Guard Merchant Mariner Card 8. Native American tribal document 9. Driver's license issued by a Canadian government authority For persons under age 18 who are unable to present a document listed above: 10. School record or report card 11. Clinic, doctor, or hospital record 12. Day-care or nursery school record 1. A Social Security Account Number card, unless the card includes one of the following restrictions: (1) NOT VALID FOR EMPLOYMENT (2) VALID FOR WORK ONLY WITH INS AUTHORIZATION (3) VALID FOR WORK ONLY WITH DHS AUTHORIZATION 2. Certification of report of birth issued by the Department of State (Forms DS-1350, FS-545, FS-240) 3. Original or certified copy of birth certificate issued by a State, county, municipal authority, or territory of the United States bearing an official seal 4. Native American tribal document 5. U.S. Citizen ID Card (Form I-197) 6. Identification Card for Use of Resident Citizen in the United States (Form I-179) 7. Employment authorization document issued by the Department of Homeland Security Examples of many of these documents appear in Part 13 of the Handbook for Employers (M-274). Refer to the instructions for more information about acceptable receipts. Form I-9 07/17/17 N Page 3 of 3


11 IF YOU HAVE THE RIGHT TO WORK Don t let anyone take it away. There are laws to protect you from discrimination in the workplace. You should know that In most cases, employers cannot deny you a job or fire you because of your national origin or citizenship status or refuse to accept your legally acceptable documents. Employers cannot reject documents because they have a future expiration date. Employers cannot terminate you because of E-Verify without giving you an opportunity to resolve the problem. Contact IER For assistance in your own language Phone: TTY: us IER@usdoj.gov Or write to U.S. Department of Justice CRT Immigrant and Employee Rights NYA 950 Pennsylvania Ave., NW Washington, DC If any of these things happen to you, contact the Immigrant and Employee Rights Section (IER). In most cases, employers cannot require you to be a U.S. citizen or a lawful permanent resident. Immigrant and Employee Rights Section U.S. Department of Justice, Civil Rights Division


12 SI USTED TIENE DERECHO A TRABAJAR No deje que nadie se lo quite. Existen leyes que lo protegen contra la discriminación en el trabajo. Usted debe saber que En la mayoría de los casos, los empleadores no pueden negarle un empleo o despedirlo debido a su nacionalidad de origen o estatus de ciudadanía, ni tampoco negarse a aceptar sus documentos válidos y legales. Los empleadores no pueden rechazar documentos porque tengan una fecha de vencimiento futura. Los empleadores no pueden despedirlo debido a E-Verify sin darle una oportunidad de resolver el problema Comuníquese con la IER Para ayuda en su propio idioma: Teléfono: TTY: Mándenos un correo: IER@usdoj.gov O escríbanos a: U.S. Department of Justice CRT Immigrant and Employee Rights NYA 950 Pennsylvania Ave., NW Washington, DC Si alguna de estas cosas le ha sucedido, comuníquese con la Sección de Derechos de Inmigrantes y Empleados (IER, por sus siglas en inglés) En la mayoría de los casos, los empleadores no pueden exigir que usted sea ciudadano estadounidense o residente legal permanente. Sección de Derechos de Inmigrantes y Empleados Departamento de Justica de los EE. UU., División de Derechos Civiles
13 Acknowledgements of Co-Employment Relationship EMPLOYEE ACKNOWLEDGEMENTS & AGREEMENTS I acknowledge and agree that 1) I have been hired as an at-will employee of ContinuumHR which is an employee leasing company, 2) there is no contract of employment which exists between me and the client to which I have been assigned (hereafter my company ); and 3) there is no contract of employment between ContinuumHR and me; and 4) ContinuumHR has no liability with regard to any employment agreement. I further understand and agree that my company, ContinuumHR or I can terminate our employment relationship at any time as I am an at-will employee. I also agree that while I am a leased employee of ContinuumHR, if ContinuumHR does not receive payment from my company for services which I perform as a leased employee, ContinuumHR will still pay me the applicable minimum wage (or the legally required minimum salary) for any such pay period, and I agree to this method of compensation. I understand and agree that ContinuumHR has no obligation to pay me any other compensation or benefit unless ContinuumHR has specifically, in a written agreement with me, adopted the company s obligation to pay me such compensation or benefit. I understand that my company at all times remains obligated to pay me my regular hourly rate of pay if I am a non-exempt employee and to pay me my full salary if I am an exempt employee even if ContinuumHR is not paid by my company. I understand and agree that ContinuumHR does not assume responsibility for payment of bonuses, commissions, severance pay, deferred compensation, profit sharing, vacation, sick or other paid time off pay, or for any other payment where payment for such items has not yet been received by ContinuumHR from my company. I have been informed and I agree that if my assignment with my company or any ContinuumHR client to which I am assigned ends for any reason, I must report back to ContinuumHR within seventy two (72) hours for possible reassignment and that unemployment benefits may be denied if I fail to do so. Employment-At-Will Acknowledgement I acknowledge and agree that my employment with ContinuumHR is that of an employee-at-will and as such is entered into voluntarily. What this means is that my company, ContinuumHR and I are free to end the employment relationship at any time, for any reason, with or without cause or advance notice. I further understand and agree that the employment-at-will status with ContinuumHR may be altered only with the written authorization of the President of ContinuumHR. No one other than the President of ContinuumHR has the authority to bind ContinuumHR to any employment contract for any specified period of time with any employee. If the contractual co-employment relationship between ContinuumHR and my company ends, I will no longer be a co-employee of ContinuumHR, however my relationship with my company will not change because of the termination of the co-employment agreement. Employee Policies Agreement I understand and agree that the Employee Policies describe important information about ContinuumHR and my company. ContinuumHR and my company have the sole discretion to alter these policies from time to time, with or without prior notice. ContinuumHR reserves the right to revise, supplement and rescind or deviate from any policy or provision of the handbook from time to time, with or without notice, as its sole and absolute discretion consistent with all applicable federal and state laws. I also understand that the revisions to these policies may supersede or eliminate existing policies and that such changes will be communicated through official notices when possible. While every attempt has been made to ensure that these policies are consistent with federal, state and local laws, if any questions occur, the policy will be enforced consistent with the applicable law. These policies are not a legal document or an employment contract and may be revised with or without notice. None of these Employee Policies or any individual policies, related practices or guidelines are to be construed as any guarantee of employment, employment contract, or part of any employment contract. I agree and I have received the Employee Policies. I further understand and agree that it is my responsibility to read the Employee Policies and any subsequent additions or revisions and to abide by the rules, policies and standards set forth in the book. The Employee Policies contains representative summary information about employment policies and practices and not all of the ContinuumHR policies are set forth in this book. Nothing in these Employee Policies alters the fact that all employee of ContinuumHR are employed for an indefinite period and that such employment may be terminated at any time, with or without cause or notice, at the will of either the employee or the Employer. CM NH/0715 Employee Acknowledgements and Agreements 1
14 Prohibition Against Discrimination & Harassment Agreement I also agree that is at any time during my employment I am subjected to any type of discrimination because of race, sex, age, religion, color, retaliation, national origin, handicap, disability or marital status, or if I am subjected to any type of harassment including sexual harassment; I will immediately contact an appropriate person of my company, the president or owner of the company and/or my supervisor. I understand and agree that my company and ContinuumHR are responsible for investigating my complaint and taking appropriate action. I further acknowledge and agree that ContinuumHR does not have actual control over my workplace and as such, is not in a position to end or remediate any discrimination, harassment, or retaliation which may be occurring. The responsibility to end such inappropriate conduct rests with my company. Problem/Complaint Resolution Acknowledgement I understand and agree that I have an affirmative obligation to report any workplace harassment or discrimination to my supervisor or my company management staff or a member of the ContinuumHR Human Resources team. ContinuumHR and my company will listen to my problem or concern, investigate it and to the extent possible, settle the matter. I understand that not all matters will be resolved to my satisfaction; however, decisions will be communicated to me in a timely manner. I further agree that the decision of the president of my company and, where applicable, ContinuumHR is final. Complaints will be kept confidential as possible, consistent with the conduct of a full and fair investigation. I also understand that violating confidentiality may be subject to immediate discipline. I further acknowledge that the registering of a valid complaint will no way be used against me, nor will it have an adverse impact on my employment status, unless such accusation is shown to be intentionally false. Safety Rules Agreement I agree to obey the safety rules and to exercise caution in all work activities. In addition, I will comply with all occupational safety and health standards and regulations established by the Occupational Safety and Health Act and state and local regulations. I will immediately report any unsafe condition to the appropriate supervisor and/or ContinuumHR Human Resources professional. I understand that violating safety standards, causing hazardous or dangerous situations, or failing to report or where appropriate, remedy such situations, may be considered sufficient cause for disciplinary action, up to an including suspension or termination of employment. Workers Compensation/On-the Job Injury or Illness Acknowledgement In recognition of the fact that any work related injuries which might be sustained by me are covered by state workers compensation statutes, and to avoid the circumvention of such state statutes which may result from suits against the customers or clients of ContinuumHR or against ContinuumHR based on the same injury or injuries and to the extent permitted by law. I hereby waive and forever release any rights I might have to make claims or bring suit against any client or customer of ContinuumHR or against ContinuumHR for damages based upon injuries which are covered under such workers compensation statutes. I also agree to comply with any drug testing policy which my company or ContinuumHR may adopt, and I specifically agree to post-accident drug testing in any situation where it is allowed by law. I understand and agree that is I am accepted as a leased employee of ContinuumHR, I am expressly prohibited from performing any work outside the state in which I currently reside in, for any client during my status as a leased employee except as may be allowed in writing by ContinuumHR and ContinuumHR s workers compensation carrier. I understand that I will not be a leased employee of ContinuumHR and will not be provided workers compensation benefits through ContinuumHR or ContinuumHR s workers compensation carrier. My leased employment with ContinuumHR will be considered immediately terminated upon commencement of my trip outside of my current state to perform work for a client where prior written approval has not been received from ContinuumHR and its workers compensation carrier. Agreement I have read, understand and agree to all the provisions contained in this Employment Acknowledgements and Agreements. I understand and agree to all terms and conditions herein stated as a condition of my employment. I hereby certify that all the information given on this document or any supporting documents is true and correct, and I understand that any misrepresentations of this information may result in immediate termination of employment. Print Name Employee Signature Date CM NH/0715 Employee Acknowledgements and Agreements 2




15 Welcome to PerkSpot! PerkSpot is a one-stop-shop for exclusive discounts at some of your favorite national and local merchants! TRAVEL COMPUTERS MOVIES CELL PHONES FOOD Start by signing up or logging in at chr.perkspot.com Access PerkSpot at work, home, or on the go & browse through thousands of discounts! Keep an eye out for new featured discounts in PerkSpot s weekly . Hundreds of great merchants like... and many more! CHR.PERKSPOT.COM
NEW HIRE EMPLOYEE INFORMATION FORM
 NEW HIRE EMPLOYEE INFORMATION FORM Employee s Name: Social Security Number: Street Address: Birth Date: Apt / PO Box: City: State: Zip: Primary Phone: Name: Email: Emergency Contact Information Relationship:
NEW HIRE EMPLOYEE INFORMATION FORM Employee s Name: Social Security Number: Street Address: Birth Date: Apt / PO Box: City: State: Zip: Primary Phone: Name: Email: Emergency Contact Information Relationship:
NEW HIRE EMPLOYEE INFORMATION FORM
 NEW HIRE EMPLOYEE INFORMATION FORM Employee s Name: Social Security Number: Street Address: Birth Date: Apt / PO Box: City: State: Zip: Primary Phone: Name: Email: Emergency Contact Information Relationship:
NEW HIRE EMPLOYEE INFORMATION FORM Employee s Name: Social Security Number: Street Address: Birth Date: Apt / PO Box: City: State: Zip: Primary Phone: Name: Email: Emergency Contact Information Relationship:
NEW HIRE EMPLOYEE INFORMATION FORM
 NEW HIRE EMPLOYEE INFORMATION FORM Employee s Name: Social Security Number: Street Address: Birth Date: Apt / PO Box: City: State: Zip: Primary Phone: Name: Email: Emergency Contact Information Relationship:
NEW HIRE EMPLOYEE INFORMATION FORM Employee s Name: Social Security Number: Street Address: Birth Date: Apt / PO Box: City: State: Zip: Primary Phone: Name: Email: Emergency Contact Information Relationship:
NEW HIRE EMPLOYEE INFORMATION FORM
 NEW HIRE EMPLOYEE INFORMATION FORM Employee s Name: Social Security Number: Street Address: Birth Date: Apt / PO Box: City: State: Zip: Primary Phone: Name: Email: Emergency Contact Information Relationship:
NEW HIRE EMPLOYEE INFORMATION FORM Employee s Name: Social Security Number: Street Address: Birth Date: Apt / PO Box: City: State: Zip: Primary Phone: Name: Email: Emergency Contact Information Relationship:
EMPLOYEE PORTAL PASSWORD SET UP
 EMPLOYEE PORTAL PASSWORD SET UP Here are some helpful tips to make sure you have access to paystubs and W2 s. Please be sure you include an email address in your new hire paperwork. The first page titled
EMPLOYEE PORTAL PASSWORD SET UP Here are some helpful tips to make sure you have access to paystubs and W2 s. Please be sure you include an email address in your new hire paperwork. The first page titled
Employment Eligibility Verification
 Employment Eligibility Verification Department of Homeland Security U.S. Citizenship and Immigration Services USCIS Form I-9 OMB No. 1615-0047 Expires 08/31/2019 START HERE: Read instructions carefully
Employment Eligibility Verification Department of Homeland Security U.S. Citizenship and Immigration Services USCIS Form I-9 OMB No. 1615-0047 Expires 08/31/2019 START HERE: Read instructions carefully
Separate here and give Form W-4 to your employer. Keep the top part for your records. Employee s Withholding Allowance Certificate
 Form W-4 (2017) Purpose. Complete Form W-4 so that your employer can withhold the correct federal income tax from your pay. Consider completing a new Form W-4 each year and when your personal or financial
Form W-4 (2017) Purpose. Complete Form W-4 so that your employer can withhold the correct federal income tax from your pay. Consider completing a new Form W-4 each year and when your personal or financial
Employment Eligibility Verification
 Employment Eligibility Verification Department of Homeland Security U.S. Citizenship and Immigration Services USCIS Form I-9 OMB No. 1615-0047 Expires 08/31/2019 START HERE: Read instructions carefully
Employment Eligibility Verification Department of Homeland Security U.S. Citizenship and Immigration Services USCIS Form I-9 OMB No. 1615-0047 Expires 08/31/2019 START HERE: Read instructions carefully
Southeast ID#: Name: SSN: PREVIOUS CIVIL OR COLLEGE DISCIPLINE
 /Student Employment Work Referral Southeast ID#: Name: SSN: STUDENT EMPLOYEE ELIGIBILITY AND RESPONSIBILITIES 1. You must complete, and have on file with Student Financial Services, employment eligibility
/Student Employment Work Referral Southeast ID#: Name: SSN: STUDENT EMPLOYEE ELIGIBILITY AND RESPONSIBILITIES 1. You must complete, and have on file with Student Financial Services, employment eligibility
RAYMOND CENTRAL PUBLIC SCHOOLS SUBSTITUTE TEACHER DATA SHEET
 RAYMOND CENTRAL PUBLIC SCHOOLS SUBSTITUTE TEACHER DATA SHEET PLEASE NOTE: We need a voided check for payment by Direct Deposit and we must have an email address. Thank you. W-4 Form I-9 Form - 2 forms
RAYMOND CENTRAL PUBLIC SCHOOLS SUBSTITUTE TEACHER DATA SHEET PLEASE NOTE: We need a voided check for payment by Direct Deposit and we must have an email address. Thank you. W-4 Form I-9 Form - 2 forms
NEW EMPLOYEE DATA SHEET HOUSING CORPORATE. Mailing Address: City: State: Zip: Phone Number: ( ) -
 -") EMPLOYEE SECTION: NEW EMPLOYEE DATA SHEET HOUSING CORPORATE Name: Please Print (as shown on Social Security Card) Mailing Address: City: State: Zip: Phone Number: ( ) - Social Security #: - - Date of Birth:
EMPLOYEE SECTION: NEW EMPLOYEE DATA SHEET HOUSING CORPORATE Name: Please Print (as shown on Social Security Card) Mailing Address: City: State: Zip: Phone Number: ( ) - Social Security #: - - Date of Birth:
December, Following is an overview of the payroll tax rates and other payroll related information in effect in 2019:
 1 December, 2018 It s time again for the annual payroll letter. The following pages include payroll and other miscellaneous information that may be helpful in fulfilling your payroll and related reporting
1 December, 2018 It s time again for the annual payroll letter. The following pages include payroll and other miscellaneous information that may be helpful in fulfilling your payroll and related reporting
Separate here and give Form W-4 to your employer. Keep the top part for your records. Employee s Withholding Allowance Certificate
 Form W-4 (2017) Purpose. Complete Form W-4 so that your employer can withhold the correct federal income tax from your pay. Consider completing a new Form W-4 each year and when your personal or financial
Form W-4 (2017) Purpose. Complete Form W-4 so that your employer can withhold the correct federal income tax from your pay. Consider completing a new Form W-4 each year and when your personal or financial
YOU DO NOT NEED TO PRINT THIS PAGE. Substitute Records Requirements. Social Security Card (copies not accepted)
") YOU DO NOT NEED TO PRINT THIS PAGE. Appointment Date & Time: Name: Date: Substitute Records Requirements I-9 (only complete page 1) W-4 Social Security Card (copies not accepted) Driver s License Direct
YOU DO NOT NEED TO PRINT THIS PAGE. Appointment Date & Time: Name: Date: Substitute Records Requirements I-9 (only complete page 1) W-4 Social Security Card (copies not accepted) Driver s License Direct
New Employee Information
 HOUSTON S PREMIER POKER DESTINATION New Employee Information Before you will be scheduled the following MUST be completed: 1. Your new hire packet must be filled out completely and correctly and handed
HOUSTON S PREMIER POKER DESTINATION New Employee Information Before you will be scheduled the following MUST be completed: 1. Your new hire packet must be filled out completely and correctly and handed
New Employment & Sign-up Checklist for Managers and Departmental Representatives
 FLORIDA A&M UNIVERSITY New Employment & Sign-up Checklist for Managers and Departmental Representatives Executive Service A&P USPS OPS Faculty (Please complete Section II Only) Employee Name: Class Title:
FLORIDA A&M UNIVERSITY New Employment & Sign-up Checklist for Managers and Departmental Representatives Executive Service A&P USPS OPS Faculty (Please complete Section II Only) Employee Name: Class Title:
Graveyard Productions, LLC
 Graveyard Productions, LLC Check here if you are under 18 years old Recruitment Application- 2018 PLEASE PRINT LEGIBLY Applicant Information Full Name: Date: Last First M.I. Address: Street Address Apartment/Unit
Graveyard Productions, LLC Check here if you are under 18 years old Recruitment Application- 2018 PLEASE PRINT LEGIBLY Applicant Information Full Name: Date: Last First M.I. Address: Street Address Apartment/Unit
YOU DO NOT NEED TO PRINT THIS PAGE. Substitute Records Requirements. Social Security Card (copies not accepted)
") YOU DO NOT NEED TO PRINT THIS PAGE. Appointment Date & Time: Name: Date: Substitute Records Requirements I-9 (only complete page 1) W-4 Social Security Card (copies not accepted) Driver s License Direct
YOU DO NOT NEED TO PRINT THIS PAGE. Appointment Date & Time: Name: Date: Substitute Records Requirements I-9 (only complete page 1) W-4 Social Security Card (copies not accepted) Driver s License Direct
EMPLOYEE INFORMATION SHEET
 EMPLOYEE INFORMATION SHEET PLEASE PRINT CLEARLY COMPANY: EMPLOYEE #: SOCIAL SECURITY NUMBER: - - NAME: First MI LAST STREET: CITY: AS APPEARS ON SOCIAL SECURITY CARD STATE: ZIP CODE: TELEPHONE NUMBER:
EMPLOYEE INFORMATION SHEET PLEASE PRINT CLEARLY COMPANY: EMPLOYEE #: SOCIAL SECURITY NUMBER: - - NAME: First MI LAST STREET: CITY: AS APPEARS ON SOCIAL SECURITY CARD STATE: ZIP CODE: TELEPHONE NUMBER:
Branson Public Schools
 Branson Public Schools Dr. Don Forrest, Assistant Superintendent of Business Services 1756 Bee Creek Rd Branson, MO 65616 Phone: 417.334.6541 uww.branson.k12.mo.us Fax: 417.332.2510 Amy Mulvaney, Administrative
Branson Public Schools Dr. Don Forrest, Assistant Superintendent of Business Services 1756 Bee Creek Rd Branson, MO 65616 Phone: 417.334.6541 uww.branson.k12.mo.us Fax: 417.332.2510 Amy Mulvaney, Administrative
EMP NAME: DEPT CODE LOCATION: B/G CHK: N/A COMPLETED START DATE: PAY RATE: TAX CODES: ( FILLED BY OFFICE ONLY ) LIVE IN WORK IN LST
 LIVE IN WORK IN LST") APPLICATION MGR: EMP # EMP NAME: DEPT CODE LOCATION: B/G CHK: N/A COMPLETED START DATE: PAY RATE: DAYS TO WORK: Mon Tues Wed Thurs Fri Sat Sun SCHEDULED HOURS: - PART TIME FULL TIME (30 hours or more )
APPLICATION MGR: EMP # EMP NAME: DEPT CODE LOCATION: B/G CHK: N/A COMPLETED START DATE: PAY RATE: DAYS TO WORK: Mon Tues Wed Thurs Fri Sat Sun SCHEDULED HOURS: - PART TIME FULL TIME (30 hours or more )
2019 English Applica on
 2019 English Applica on (Please Print) Date: First Name Last Name Social Security Address Apt. City State Zip Code Home Phone Cell Phone E-Mail Please place a check by your response or provide the appropriate
2019 English Applica on (Please Print) Date: First Name Last Name Social Security Address Apt. City State Zip Code Home Phone Cell Phone E-Mail Please place a check by your response or provide the appropriate
LS Contracting Group, Inc. General Contractor & Specialty Restoration
 LS Contracting Group, Inc. General Contractor & Specialty Restoration 5660 N. Elston Ave. Chicago, IL 60646 p: (773) 774-1122 f: (773) 774-5660 lscontracting.com EMPLOYMENT APPLICATION CHECKLIST Name:
LS Contracting Group, Inc. General Contractor & Specialty Restoration 5660 N. Elston Ave. Chicago, IL 60646 p: (773) 774-1122 f: (773) 774-5660 lscontracting.com EMPLOYMENT APPLICATION CHECKLIST Name:
Employment Application
 P.O. Box 643 Benavides, Tx 78341 (361) 256-4726 Office (361) 256-4728 Fax Scorp1144@yahoo.com Scorpion Exploration & Production, Inc. Full Name Mailing Address Employment Application Applicant Information
P.O. Box 643 Benavides, Tx 78341 (361) 256-4726 Office (361) 256-4728 Fax Scorp1144@yahoo.com Scorpion Exploration & Production, Inc. Full Name Mailing Address Employment Application Applicant Information
Packet A - Forms. If you have any questions, please contact Human Resources at
 Packet A - Forms 2018 TEMPORARY NEW HIRE PAPERWORK Welcome to Union College! This packet contains new hire forms necessary for you to become established as a Union College employee. Please fill out and
Packet A - Forms 2018 TEMPORARY NEW HIRE PAPERWORK Welcome to Union College! This packet contains new hire forms necessary for you to become established as a Union College employee. Please fill out and
INSTRUCTIONS FOR PAPERWORK ALL FORMS MUST BE SIGNED AND DATED PLEASE PRINT ONE-SIDED SHEETS
 INSTRUCTIONS FOR PAPERWORK ALL FORMS MUST BE SIGNED AND DATED PLEASE PRINT ONE-SIDED SHEETS CFISD EMPLOYEE INFORMATION SHEET Must be LEGIBLE Fill in all blanks You MUST bubble an answer for Part 1-Ethnicity
INSTRUCTIONS FOR PAPERWORK ALL FORMS MUST BE SIGNED AND DATED PLEASE PRINT ONE-SIDED SHEETS CFISD EMPLOYEE INFORMATION SHEET Must be LEGIBLE Fill in all blanks You MUST bubble an answer for Part 1-Ethnicity
Separate here and give Form W-4 to your employer. Keep the top part for your records. Employee's Withholding Allowance Certificate
 Form W-4 (2015) Purpose. Complete Form W-4 so that your employer can withhold the correct federal income tax from your pay. Consider completing a new Form W-4 each year and when your personal or financial
Form W-4 (2015) Purpose. Complete Form W-4 so that your employer can withhold the correct federal income tax from your pay. Consider completing a new Form W-4 each year and when your personal or financial
On Call Staffing On - Boarding Checklist
 On Call Staffing On - Boarding Checklist Please note that we will need ALL of the items below completed and returned to our office. Documents can be returned in person, via fax, or mail. Completed Application
On Call Staffing On - Boarding Checklist Please note that we will need ALL of the items below completed and returned to our office. Documents can be returned in person, via fax, or mail. Completed Application
Jersey Assistance for Community Caregiving (JACC) Program PEP Enrollment Packet
 Program PEP Enrollment Packet") Public Partnerships Jersey Assistance for Community Caregiving (JACC) Program Phone: 1-866-239-2778 Paperwork Fax: 1-866-547-2481 Paperwork E-mail: njpplfax@pcgus.com Website: www.publicpartnerships.com
Public Partnerships Jersey Assistance for Community Caregiving (JACC) Program Phone: 1-866-239-2778 Paperwork Fax: 1-866-547-2481 Paperwork E-mail: njpplfax@pcgus.com Website: www.publicpartnerships.com
MAYOR BYRON W. BROWN S SUMMER YOUTH INTERNSHIP PROGRAM APPLICATION
 MAYOR BYRON W. BROWN S SUMMER YOUTH INTERNSHIP PROGRAM February 1, 2018 Dear Applicant: Thank you for your interest in applying for my 2018 Summer Youth Internship Program. This is truly a wonderful opportunity
MAYOR BYRON W. BROWN S SUMMER YOUTH INTERNSHIP PROGRAM February 1, 2018 Dear Applicant: Thank you for your interest in applying for my 2018 Summer Youth Internship Program. This is truly a wonderful opportunity
Commonwealth of Virginia
 Commonwealth of Virginia Virginia Employment Commission NOTICE TO WORKERS Every day many unemployed workers tell us that unemployment insurance is due them "because they have paid for it." This is not
Commonwealth of Virginia Virginia Employment Commission NOTICE TO WORKERS Every day many unemployed workers tell us that unemployment insurance is due them "because they have paid for it." This is not
Warrick County School Corporation
 Warrick County School Corporation SUPERINTENDENT S OFFICE P.O. Box 809/Boonville, Indiana 47601/812-897-0400 Welcome to the Warrick County School Corporation Welcome to the one of the best school corporations
Warrick County School Corporation SUPERINTENDENT S OFFICE P.O. Box 809/Boonville, Indiana 47601/812-897-0400 Welcome to the Warrick County School Corporation Welcome to the one of the best school corporations
TENNESSEE CONSOLIDATED RETIREMENT SYSTEM 502 Deaderick Street Nashville, Tennessee
 Retirement Application for Service or Early Retirement Benefits TENNESSEE CONSOLIDATED RETIREMENT SYSTEM 502 Deaderick Street Nashville, Tennessee 37243-0201 1-800-770-8277 http://tcrs.tn.gov Refer to
Retirement Application for Service or Early Retirement Benefits TENNESSEE CONSOLIDATED RETIREMENT SYSTEM 502 Deaderick Street Nashville, Tennessee 37243-0201 1-800-770-8277 http://tcrs.tn.gov Refer to
Dedicated to Providing the Highest Level of Public Safety Services to our Community
 FIRE CHIEF Lonnie E. Click Dedicated to Providing the Highest Level of Public Safety Services to our Community COMMISSIONERS Earl W. Bill Houchin Jerry F. Morris Gerald D. Sleater INTRODUCTION Thank you
FIRE CHIEF Lonnie E. Click Dedicated to Providing the Highest Level of Public Safety Services to our Community COMMISSIONERS Earl W. Bill Houchin Jerry F. Morris Gerald D. Sleater INTRODUCTION Thank you
Employee Packet Forms
 Welcome!! Outreach Health Services looks forward to working with you. This Employee Packet has the forms and information you need to become an employee. The participant, who is your employer, can help
Welcome!! Outreach Health Services looks forward to working with you. This Employee Packet has the forms and information you need to become an employee. The participant, who is your employer, can help
TENNESSEE CONSOLIDATED RETIREMENT SYSTEM 502 Deaderick Street Nashville, Tennessee (615)
") Retirement Application for Disability Benefits TENNESSEE CONSOLIDATED RETIREMENT SYSTEM 502 Deaderick Street Nashville, Tennessee 37243-0201 1-800-770-8277 (615) 253-8693 http://tcrs.tn.gov Refer to pages
Retirement Application for Disability Benefits TENNESSEE CONSOLIDATED RETIREMENT SYSTEM 502 Deaderick Street Nashville, Tennessee 37243-0201 1-800-770-8277 (615) 253-8693 http://tcrs.tn.gov Refer to pages
Blank Forms (Volume 1)
") Blank Forms (Volume 1) These forms are provided for congregational use and may be copied. Payroll Congregational Payroll Information Employment Eligibility Verification (I-9) Payroll Authorization Form
Blank Forms (Volume 1) These forms are provided for congregational use and may be copied. Payroll Congregational Payroll Information Employment Eligibility Verification (I-9) Payroll Authorization Form
Employee Data Sheet NAME. Title: Dr. Mr. Ms. Mrs. Miss First: Middle: Last: Suffix: CONTACT INFORMATION
 Employee Data Sheet Social Security #: Today s Date: NAME Title: Dr. Mr. Ms. Mrs. Miss First: Middle: Last: Suffix: CONTACT INFORMATION Address: Apt/Unit #: City: State: Zip Code: County: Home Phone (include
Employee Data Sheet Social Security #: Today s Date: NAME Title: Dr. Mr. Ms. Mrs. Miss First: Middle: Last: Suffix: CONTACT INFORMATION Address: Apt/Unit #: City: State: Zip Code: County: Home Phone (include
City of Becker Employment Application
 Date Received: Received By: City of Becker Employment Application Return to: Becker Community Center PO Box 250 Becker, MN 55308 Ph: 763-200-4271 Fax: 763-261-2018 Applicant Name: Last First Middle Initial
Date Received: Received By: City of Becker Employment Application Return to: Becker Community Center PO Box 250 Becker, MN 55308 Ph: 763-200-4271 Fax: 763-261-2018 Applicant Name: Last First Middle Initial
Personal Fact Sheet (This information is not to be requested before employment)
") Personal Fact Sheet (This information is not to be requested before employment) Self-disclosure of this information is requested for Affirmative Action, insurance and other purposes. It will not in any
Personal Fact Sheet (This information is not to be requested before employment) Self-disclosure of this information is requested for Affirmative Action, insurance and other purposes. It will not in any
Store# Name (First, Middle, Last) SSN # Date of Birth. City State Zip. Hire Date Position Rate of pay/annual Salary. Select... Rehire.
 SSN # Date of Birth. City State Zip. Hire Date Position Rate of pay/annual Salary. Select... Rehire.") Store# Name (First, Middle, Last) SSN # Date of Birth Address Apt/Lot City State Zip Hire Date Position Rate of pay/annual Salary Rehire nmlkj Yes nmlkj No Select... Native American If yes, please list
Store# Name (First, Middle, Last) SSN # Date of Birth Address Apt/Lot City State Zip Hire Date Position Rate of pay/annual Salary Rehire nmlkj Yes nmlkj No Select... Native American If yes, please list
TTC Form T3-107) ct Deposit (TTC Form T3-21)
 ct Deposit (TTC Form T3-21)") TO: Adjunct Instructor FROM: Human Resources, Fredric Yeadon (843-574-6825) RE: Adjunct Instructor Packet Welcome to Trident Technical College! Please complete the following paperwork before reporting
TO: Adjunct Instructor FROM: Human Resources, Fredric Yeadon (843-574-6825) RE: Adjunct Instructor Packet Welcome to Trident Technical College! Please complete the following paperwork before reporting
FORMS TO BE COMPLETED AND SUBMITTED TO HUMAN RESOURCES. The College requires all Employees complete and submit the following documents:
 FORMS TO BE COMPLETED AND SUBMITTED TO HUMAN RESOURCES The College requires all Employees complete and submit the following documents: 1. I-9 Employment Eligibility Verification: Complete the I-9 Form
FORMS TO BE COMPLETED AND SUBMITTED TO HUMAN RESOURCES The College requires all Employees complete and submit the following documents: 1. I-9 Employment Eligibility Verification: Complete the I-9 Form
Employee (Caregiver) Packet (Keep this folder for your records)
 Packet (Keep this folder for your records)") Employee (Caregiver) Packet (Keep this folder for your records) You will need to complete the following steps in order to hire an employee. Enrollment forms to enroll and hire a Support Broker can be found
Employee (Caregiver) Packet (Keep this folder for your records) You will need to complete the following steps in order to hire an employee. Enrollment forms to enroll and hire a Support Broker can be found
NO CONFLICT ATTESTATION. In order to qualify to act as the Personal Assistant for this Consumer, I attest to the ALL of following:
 NO CONFLICT ATTESTATION In order to qualify to act as the Personal Assistant for this Consumer, I attest to the ALL of following: 1. I am NOT the Consumer s Designated Representative. 2. The Consumer is
NO CONFLICT ATTESTATION In order to qualify to act as the Personal Assistant for this Consumer, I attest to the ALL of following: 1. I am NOT the Consumer s Designated Representative. 2. The Consumer is
Missouri Department of Revenue Employee s Withholding Allowance Certificate
 Form MO W-4 Missouri Department of Revenue Employee s Withholding Allowance Certificate This certificate is for income tax withholding and child support enforcement purposes only. Type or print. Full Name
Form MO W-4 Missouri Department of Revenue Employee s Withholding Allowance Certificate This certificate is for income tax withholding and child support enforcement purposes only. Type or print. Full Name
Application for Service or Early Retirement Benefits
 Application for Service or Early Retirement Benefits Tennessee Consolidated Retirement System 502 Deaderick Street Nashville, Tennessee 37243-0201 1-800-922-7772 RetireReadyTN.gov Do NOT complete this
Application for Service or Early Retirement Benefits Tennessee Consolidated Retirement System 502 Deaderick Street Nashville, Tennessee 37243-0201 1-800-922-7772 RetireReadyTN.gov Do NOT complete this
BRIDGEWATER STATE UNIVERSITY. Preferred Name*: (if applicable)
") BRIDGEWATER STATE UNIVERSITY First Name: Last Name: ------ --+----------------------~ Middle Name: Preferred Name*: (if applicable) -------- Date of Birth: Social Security Number: ------J ' Marital status:
BRIDGEWATER STATE UNIVERSITY First Name: Last Name: ------ --+----------------------~ Middle Name: Preferred Name*: (if applicable) -------- Date of Birth: Social Security Number: ------J ' Marital status:
COLCHESTER SCHOOL DISTRICT
 COLCHESTER SCHOOL DISTRICT APPLICATION FOR SUBSTITUTING Administrative Offices, 125 Laker Lane P.O. Box 27, Colchester, VT 05446-0027 Phone (802) 264-5999 Fax (802) 863-4774 Name: Telephone No.: Mailing
COLCHESTER SCHOOL DISTRICT APPLICATION FOR SUBSTITUTING Administrative Offices, 125 Laker Lane P.O. Box 27, Colchester, VT 05446-0027 Phone (802) 264-5999 Fax (802) 863-4774 Name: Telephone No.: Mailing
Employee Data Sheet NAME. Title: Dr. Mr. Ms. Mrs. Miss First: Middle: Last: Suffix: CONTACT INFORMATION
 Employee Data Sheet Social Security #: Today s Date: NAME Title: Dr. Mr. Ms. Mrs. Miss First: Middle: Last: Suffix: CONTACT INFORMATION Address: Apt/Unit #: City: State: Zip Code: County: Home Phone (include
Employee Data Sheet Social Security #: Today s Date: NAME Title: Dr. Mr. Ms. Mrs. Miss First: Middle: Last: Suffix: CONTACT INFORMATION Address: Apt/Unit #: City: State: Zip Code: County: Home Phone (include
Personal Data Form. UIN#: Dr. Mr. Mrs. Ms. Last Name: First Name: Middle Initial:
 Personal Data Form UIN#: Dr. Mr. Mrs. Ms. Last Name: First Name: Middle Initial: Preferred Name (if different than above): Social Security Number: Mailing Address (same as W4): City: Zip/Postal Code: Permanent
Personal Data Form UIN#: Dr. Mr. Mrs. Ms. Last Name: First Name: Middle Initial: Preferred Name (if different than above): Social Security Number: Mailing Address (same as W4): City: Zip/Postal Code: Permanent
Personal Data Form. UIN#: Dr. Mr. Mrs. Ms. Last Name: First Name: Middle Initial:
 Personal Data Form UIN#: Dr. Mr. Mrs. Ms. Last Name: First Name: Middle Initial: Preferred Name (if different than above): Social Security Number: Mailing Address (same as W4): City: Zip/Postal Code: Permanent
Personal Data Form UIN#: Dr. Mr. Mrs. Ms. Last Name: First Name: Middle Initial: Preferred Name (if different than above): Social Security Number: Mailing Address (same as W4): City: Zip/Postal Code: Permanent
Name: MCO (circle one): AG UHC VSHP (Blue Care) Worker Training Checklist. I-9 Criminal Attestation Tax Exempt W-4. Additional Comments:
: AG UHC VSHP (Blue Care) Worker Training Checklist. I-9 Criminal Attestation Tax Exempt W-4. Additional Comments:") 414 Union ST, Ste 1100 Nashville, TN 37219 Fax - Worker United Health Care Fax: 877.432.4103 (FOR DOCUMENTS ONLY. NO TIMESHEETS TO THIS NUMBER) Customer Service: 888.866.1154 To: Fax: Phone: Member Name:
414 Union ST, Ste 1100 Nashville, TN 37219 Fax - Worker United Health Care Fax: 877.432.4103 (FOR DOCUMENTS ONLY. NO TIMESHEETS TO THIS NUMBER) Customer Service: 888.866.1154 To: Fax: Phone: Member Name:
Personal Data Form. UIN#: Dr. Mr. Mrs. Ms. Last Name: First Name: Middle Initial:
 Personal Data Form UIN#: Dr. Mr. Mrs. Ms. Last Name: First Name: Middle Initial: Preferred Name (if different than above): Social Security Number: Mailing Address (same as W4): City: Zip/Postal Code: Permanent
Personal Data Form UIN#: Dr. Mr. Mrs. Ms. Last Name: First Name: Middle Initial: Preferred Name (if different than above): Social Security Number: Mailing Address (same as W4): City: Zip/Postal Code: Permanent
Bring all completed forms to your paperwork session. Any questions that you may have about the forms, we will be happy to address at the session.
 Directions for completing the New Hire Paperwork On-Line: Please print all pages (12 forms) 1-Employment Eligibility Verification Form: complete and sign/date Section 1. If your social security card states
Directions for completing the New Hire Paperwork On-Line: Please print all pages (12 forms) 1-Employment Eligibility Verification Form: complete and sign/date Section 1. If your social security card states
Bring all completed forms to your paperwork session. Any questions that you may have about the forms, we will be happy to address at the session.
 Directions for completing the New Hire Paperwork On-Line: Please print all pages (12 forms) 1-Employment Eligibility Verification Form: complete and sign/date Section 1. If your social security card states
Directions for completing the New Hire Paperwork On-Line: Please print all pages (12 forms) 1-Employment Eligibility Verification Form: complete and sign/date Section 1. If your social security card states
The New Hire Orientation Packet
 The New Hire Orientation Packet www.beesteelinc.com Workplace Conduct Policy Policy Statement Bee Steel is committed to providing a healthy and safe working environment. Bee Steel believes that is employees,
The New Hire Orientation Packet www.beesteelinc.com Workplace Conduct Policy Policy Statement Bee Steel is committed to providing a healthy and safe working environment. Bee Steel believes that is employees,
BACKGROUND SCREENING & PRE-EMPLOYMENT REQUIREMENTS
 BACKGROUND SCREENING & PRE-EMPLOYMENT REQUIREMENTS REQUIREMENT DUE DATE DETAILS/INSTRUCTIONS HR administers fingerprinting at the Great Hearts office. Fingerprint Clearance Status Form: Consent to Conduct
BACKGROUND SCREENING & PRE-EMPLOYMENT REQUIREMENTS REQUIREMENT DUE DATE DETAILS/INSTRUCTIONS HR administers fingerprinting at the Great Hearts office. Fingerprint Clearance Status Form: Consent to Conduct
2017 New Hire Forms Directions & Resources
 2017 New Hire Forms Directions & Resources Federal W4 Forms Complete form; filling in all spaces in sections 1-7, remembering to sign and date form. State W4 Forms Complete Employee Withholding Allowance
2017 New Hire Forms Directions & Resources Federal W4 Forms Complete form; filling in all spaces in sections 1-7, remembering to sign and date form. State W4 Forms Complete Employee Withholding Allowance
P E N N S Y L V A N I A Application for Payment of Medicare Premiums, Coinsurance and Deductibles
 P E N N S Y L V A N I A Application for Payment of Medicare Premiums, Coinsurance and Deductibles If you have a disability and need this form in large print or another format, please call our helpline
P E N N S Y L V A N I A Application for Payment of Medicare Premiums, Coinsurance and Deductibles If you have a disability and need this form in large print or another format, please call our helpline
OCCUPATIONAL TAX CERTIFICATE
 CITY OF JONESBORO 124 North Avenue Jonesboro, Georgia 30236 City Hall: (770) 478-3800 Fax: (770) 478-3775 www.jonesboroga.com OCCUPATIONAL TAX CERTIFICATE APPLICATION ATTACH ADDITIONAL PAGES IF NECCESSARY.
CITY OF JONESBORO 124 North Avenue Jonesboro, Georgia 30236 City Hall: (770) 478-3800 Fax: (770) 478-3775 www.jonesboroga.com OCCUPATIONAL TAX CERTIFICATE APPLICATION ATTACH ADDITIONAL PAGES IF NECCESSARY.
E V A N S N E T W O R K O F C O M P A N I E S
 E V A N S N E T W O R K O F C O M P A N I E S AGENT: Scan ALL forms and documents except as noted below in red. Driver Application Part 1 (Pre-Qualification) Application and PSP Disclosure and Authorization
E V A N S N E T W O R K O F C O M P A N I E S AGENT: Scan ALL forms and documents except as noted below in red. Driver Application Part 1 (Pre-Qualification) Application and PSP Disclosure and Authorization
INSTRUCTIONS FOR COMPLETING NEW HIRE PAPERWORK
 INSTRUCTIONS FOR COMPLETING NEW HIRE PAPERWORK **DO NOT PRINT DOUBLE SIDED ** USE BLUE OR BLACK INK ONLY 1. ADDITIONAL INFORMATION SHEET: Must be LEGIBLE. PLEASE PRINT. Make sure that you have checked
INSTRUCTIONS FOR COMPLETING NEW HIRE PAPERWORK **DO NOT PRINT DOUBLE SIDED ** USE BLUE OR BLACK INK ONLY 1. ADDITIONAL INFORMATION SHEET: Must be LEGIBLE. PLEASE PRINT. Make sure that you have checked
Personal Data Form. UIN#: Dr. Mr. Mrs. Ms. Last Name: First Name: Middle Initial:
 Personal Data Form UIN#: Dr. Mr. Mrs. Ms. Last Name: First Name: Middle Initial: Preferred Name (if different than above): Social Security Number: Mailing Address (same as W4): City: Zip/Postal Code: Permanent
Personal Data Form UIN#: Dr. Mr. Mrs. Ms. Last Name: First Name: Middle Initial: Preferred Name (if different than above): Social Security Number: Mailing Address (same as W4): City: Zip/Postal Code: Permanent
Separate here and give Form W-4 to your employer. Keep the worksheet(s) for your records. Employee s Withholding Allowance Certificate
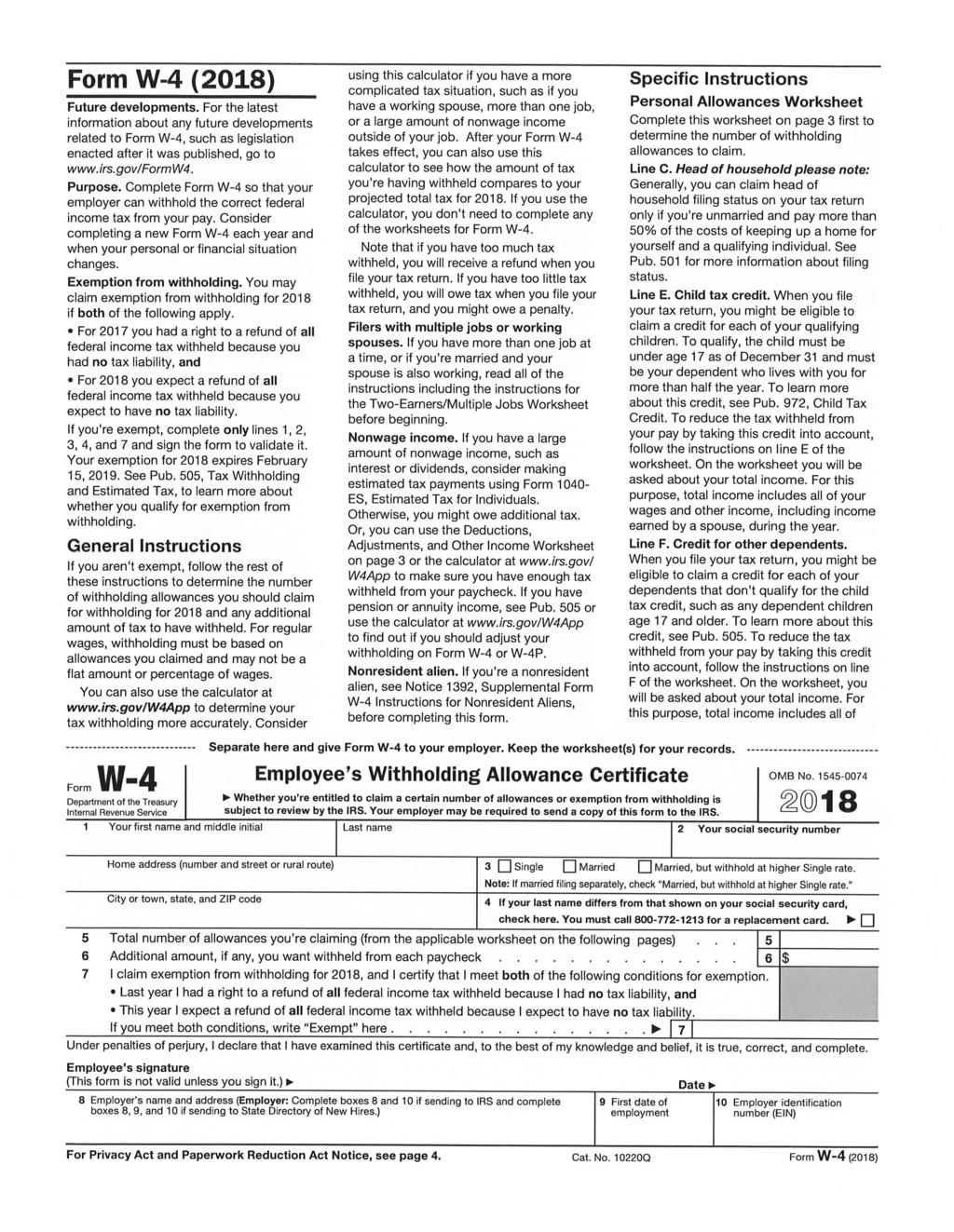
 for your records. Employee s Withholding Allowance Certificate") Form W-4 (2018) Future developments. For the latest information about any future developments related to Form W-4, such as legislation enacted after it was published, go to www.irs.gov/formw4. Purpose.
Form W-4 (2018) Future developments. For the latest information about any future developments related to Form W-4, such as legislation enacted after it was published, go to www.irs.gov/formw4. Purpose.
APPLICATION PACKET. Please read pages 1 through 6 for some important things you ll need to know before you apply.
 DEPARTMENT OF HEALTH AND FAMILY SERVICES Division of Health Care Access and Accountability HCF 10182 (02/08) STATE OF WISCONSIN APPLICATION PACKET Please read pages 1 through 6 for some important things
DEPARTMENT OF HEALTH AND FAMILY SERVICES Division of Health Care Access and Accountability HCF 10182 (02/08) STATE OF WISCONSIN APPLICATION PACKET Please read pages 1 through 6 for some important things
Louisiana LABOR LAW POSTINGS
 Louisiana LABOR LAW POSTINGS Louisiana Labor Law Postings Thank you for using GovDocs! This file contains the following state postings: Name of Posting Posting Code Posting Requirements Agency Responsible
Louisiana LABOR LAW POSTINGS Louisiana Labor Law Postings Thank you for using GovDocs! This file contains the following state postings: Name of Posting Posting Code Posting Requirements Agency Responsible
Human Resources Department Mary Lou Glaesmann, Asst. Supt. for HR
 Human Resources Department Mary Lou Glaesmann, Asst. Supt. for HR Welcome! This document contains the paperwork you will be required to complete and bring to your HR orientation. Below are some helpful
Human Resources Department Mary Lou Glaesmann, Asst. Supt. for HR Welcome! This document contains the paperwork you will be required to complete and bring to your HR orientation. Below are some helpful
Please complete and sign all forms in the PRE-EMPLOYMENT FORMS section.
 NATIONAL HOME HEALTH SERVICES EMPLOYMENT FORMS 5811 Dempster St Morton Grove, IL 60053 Phone: (847) 329-9933 Fax: (847) 930-0375 APPLICANT NAME POSITION APPLYING FOR DATE Please complete and sign all forms
NATIONAL HOME HEALTH SERVICES EMPLOYMENT FORMS 5811 Dempster St Morton Grove, IL 60053 Phone: (847) 329-9933 Fax: (847) 930-0375 APPLICANT NAME POSITION APPLYING FOR DATE Please complete and sign all forms
SUNCHASE AT LONGWOOD & THE GREENS AT SUNCHASE RENTAL CRITERIA
 SUNCHASE AT LONGWOOD & THE GREENS AT SUNCHASE RENTAL CRITERIA Management Services Corporation strongly supports the applicable Federal and State Fair Housing laws in both spirit and actual practice. All
SUNCHASE AT LONGWOOD & THE GREENS AT SUNCHASE RENTAL CRITERIA Management Services Corporation strongly supports the applicable Federal and State Fair Housing laws in both spirit and actual practice. All
We (The Jeffrey Corporation) are making you a contingent job offer to work at Burger King Store #.
 are making you a contingent job offer to work at Burger King Store #.") Date Dear Applicant, We (The Jeffrey Corporation) are making you a contingent job offer to work at Burger King Store #. Part of the hiring/re-hiring process requires that we verify your eligibility to
Date Dear Applicant, We (The Jeffrey Corporation) are making you a contingent job offer to work at Burger King Store #. Part of the hiring/re-hiring process requires that we verify your eligibility to
New Employee Welcome Letter and Orientation Checklist
 Lafayette DQ Restaurants P.O. Box 302 Delphi, IN 46923 Phone: (765) 447-1089 Fax: (765) 535-5001 New Employee Welcome Letter and Orientation Checklist Welcome to the DQ family! In order to start training
Lafayette DQ Restaurants P.O. Box 302 Delphi, IN 46923 Phone: (765) 447-1089 Fax: (765) 535-5001 New Employee Welcome Letter and Orientation Checklist Welcome to the DQ family! In order to start training
Person ID Name. Job Code
 REQUEST FOR PERSONNEL ACTION ACTION REQUESTED FOR POSITION (Please check the box to the left of the action you are requesting): New Position Modify (Change) Position Continue Current Position Delimit Assignment
REQUEST FOR PERSONNEL ACTION ACTION REQUESTED FOR POSITION (Please check the box to the left of the action you are requesting): New Position Modify (Change) Position Continue Current Position Delimit Assignment
Personal Data Form. UIN#: Dr. Mr. Mrs. Ms. Last Name: First Name: Middle Initial:
 Personal Data Form UIN#: Dr. Mr. Mrs. Ms. Last Name: First Name: Middle Initial: Preferred Name (if different than above): Social Security Number: Mailing Address (same as W4): City: Zip/Postal Code: Permanent
Personal Data Form UIN#: Dr. Mr. Mrs. Ms. Last Name: First Name: Middle Initial: Preferred Name (if different than above): Social Security Number: Mailing Address (same as W4): City: Zip/Postal Code: Permanent
Colorado LABOR LAW POSTINGS
 Colorado LABOR LAW POSTINGS Colorado Labor Law Postings Thank you for using GovDocs! This file contains the following state postings: Name of Posting Posting Code Posting Requirements Agency Responsible
Colorado LABOR LAW POSTINGS Colorado Labor Law Postings Thank you for using GovDocs! This file contains the following state postings: Name of Posting Posting Code Posting Requirements Agency Responsible
Mailing Address (Street) (Apt) Telephone Numbers: Work: ( ) - Home: ( ) - (City) (State) (Zip Code) Other: ( ) -
 (Apt) Telephone Numbers: Work: ( ) - Home: ( ) - (City) (State) (Zip Code) Other: ( ) -") CITY OF ORANGE CITY HUMAN RESOURCES AN EQUAL OPPORTUNITY EMPLOYER 205 EAST GRAVES AVENUE ORANGE CITY, FL 32763 (386-775-5457) THE CITY OF ORANGE CITY ONLY ACCEPTS APPLICATIONS FOR OPEN POSITIONS Instructions:
CITY OF ORANGE CITY HUMAN RESOURCES AN EQUAL OPPORTUNITY EMPLOYER 205 EAST GRAVES AVENUE ORANGE CITY, FL 32763 (386-775-5457) THE CITY OF ORANGE CITY ONLY ACCEPTS APPLICATIONS FOR OPEN POSITIONS Instructions:
CDL DRIVER NEW EMPLOYEE PACK
 CDL DRIVER NEW EMPLOYEE PACK For questions or additional assistance with completing your paperwork, please reach out to: Alice Paul, HR Assistant 8 0 0-8 7 3-5 0 5 9 x 1 8 9 a p a u l @ a i m n t l s.
CDL DRIVER NEW EMPLOYEE PACK For questions or additional assistance with completing your paperwork, please reach out to: Alice Paul, HR Assistant 8 0 0-8 7 3-5 0 5 9 x 1 8 9 a p a u l @ a i m n t l s.
ALCOHOL LICENSE APPLICATION FOR LIQUOR, BEER, OR WINE RETAIL AND BROWN BAGGING. Identification Section 1 Name of licensee: Social security no:
 ALCOHOL LICENSE APPLICATION FOR LIQUOR, BEER, OR WINE RETAIL AND BROWN BAGGING Identification Section 1 Name of licensee: Social security no: 2 Is licensee a corporation? Yes No If yes, name and address
ALCOHOL LICENSE APPLICATION FOR LIQUOR, BEER, OR WINE RETAIL AND BROWN BAGGING Identification Section 1 Name of licensee: Social security no: 2 Is licensee a corporation? Yes No If yes, name and address
NEW EMPLOYEE PACK STATUS: MANAGERS/SUPERVISORS. For questions or additional assistance with completing your paperwork, please reach out to:
 NEW EMPLOYEE PACK STATUS: MANAGERS/SUPERVISORS For questions or additional assistance with completing your paperwork, please reach out to: Alice Paul, HR Assistant 8 0 0-8 7 3-5 0 5 9 x 1 8 9 a p a u l
NEW EMPLOYEE PACK STATUS: MANAGERS/SUPERVISORS For questions or additional assistance with completing your paperwork, please reach out to: Alice Paul, HR Assistant 8 0 0-8 7 3-5 0 5 9 x 1 8 9 a p a u l
**If you have any other questions, please contact us and we will be happy to help.**
 Attention GGRC Public Partnerships, LLC 7776 S Pointe Pkwy W Suite 5 Phoenix, AZ 8544 Worker First name, Last name Worker Mailing Address, Address 2 Worker City, State, Zip Dear Worker This packet includes
Attention GGRC Public Partnerships, LLC 7776 S Pointe Pkwy W Suite 5 Phoenix, AZ 8544 Worker First name, Last name Worker Mailing Address, Address 2 Worker City, State, Zip Dear Worker This packet includes
ALCOHOL LICENSE APPLICATION. Identification Section 1 Name of licensee: Social security no:
 ALCOHOL LICENSE APPLICATION Identification Section 1 Name of licensee: Social security no: 2 Is licensee a corporation? Yes No If yes, name and address of registered agent 3 Legal business name, address
ALCOHOL LICENSE APPLICATION Identification Section 1 Name of licensee: Social security no: 2 Is licensee a corporation? Yes No If yes, name and address of registered agent 3 Legal business name, address
MANAGEMENT SERVICES RENTAL CRITERIA FOR THE WOODS, WOODLANE, WOODRIDGE, LINDEN LANE, BRANDYWINE WOODSLODGE, TURTLE CREEK AND BURNET ON ELLIOTT
 MANAGEMENT SERVICES RENTAL CRITERIA FOR THE WOODS, WOODLANE, WOODRIDGE, LINDEN LANE, BRANDYWINE WOODSLODGE, TURTLE CREEK AND BURNET ON ELLIOTT Management Services Corporation strongly supports the applicable
MANAGEMENT SERVICES RENTAL CRITERIA FOR THE WOODS, WOODLANE, WOODRIDGE, LINDEN LANE, BRANDYWINE WOODSLODGE, TURTLE CREEK AND BURNET ON ELLIOTT Management Services Corporation strongly supports the applicable
City of Staples Application for Employment
 City of Staples Application for Employment We consider applicants for all positions without regard to race, color, religion, sex, national origin, age, marital or veteran status, the presence of a non-job-related
City of Staples Application for Employment We consider applicants for all positions without regard to race, color, religion, sex, national origin, age, marital or veteran status, the presence of a non-job-related
DEPARTMENT OF HUMAN RESOURCES FAMILY INVESTMENT ADMINISTRATION Assistance Request
 DEPARTMENT OF HUMAN RESOURCES FAMILY INVESTMENT ADMINISTRATION Assistance Request The Family Investment Administration is committed to providing access, and reasonable accommodation in its services, programs,
DEPARTMENT OF HUMAN RESOURCES FAMILY INVESTMENT ADMINISTRATION Assistance Request The Family Investment Administration is committed to providing access, and reasonable accommodation in its services, programs,
Medical Assistance (Medicaid) Financial Eligibility Application for Long Term Care, Supports and Services
 Financial Eligibility Application for Long Term Care, Supports and Services") Check any that you are applying for: Medical Assistance (Medicaid) Financial Eligibility Application for Long Term Care, Supports and Services You may also apply online at www.compass.state.pa.us Care
Check any that you are applying for: Medical Assistance (Medicaid) Financial Eligibility Application for Long Term Care, Supports and Services You may also apply online at www.compass.state.pa.us Care
APPLICATION FOR BUSINESS LICENSE INCLUDING SALES AND USE TAX AND OCCUPATIONAL PRIVILEGE TAX REGISTRATION
 City of Aurora Tax and Licensing 15151 E. Alameda Parkway, Suite 1100 Aurora, CO 80012 (303) 739-7057 www.auroragov.org REGISTRATION/LICENSE FEE: $50.00 PAYABLE TO CITY OF AURORA APPLY ONLINE AND SAVE
City of Aurora Tax and Licensing 15151 E. Alameda Parkway, Suite 1100 Aurora, CO 80012 (303) 739-7057 www.auroragov.org REGISTRATION/LICENSE FEE: $50.00 PAYABLE TO CITY OF AURORA APPLY ONLINE AND SAVE
Medical Assistance (Medicaid) Financial Eligibility Application for Long Term Care, Supports and Services
 Financial Eligibility Application for Long Term Care, Supports and Services") Medical Assistance (Medicaid) Financial Eligibility Application for Long Term Care, Supports and Services You may also apply online at www.compass.state.pa.us Check any that you are applying for: Care
Medical Assistance (Medicaid) Financial Eligibility Application for Long Term Care, Supports and Services You may also apply online at www.compass.state.pa.us Check any that you are applying for: Care
APPLICATION FOR EMPLOYMENT
 APPLICATION FOR EMPLOYMENT EDWARDS, Inc. EDWARDS/Greenville, Inc EDWARDS/Wilmington, Inc Employment Desired: Position Desired: This Company Is An Equal Opportunity Employer This company is subject to E-Verify
APPLICATION FOR EMPLOYMENT EDWARDS, Inc. EDWARDS/Greenville, Inc EDWARDS/Wilmington, Inc Employment Desired: Position Desired: This Company Is An Equal Opportunity Employer This company is subject to E-Verify
INSTRUCTIONS FOR COMPLETING NEW HIRE PAPERWORK
 INSTRUCTIONS FOR COMPLETING NEW HIRE PAPERWORK ADDITIONAL INFORMATION SHEET: Must be LEGIBLE, PLEASE PRINT, Make sure that you have checked the "CAN" or "CANNOT" be given to the public box at the bottom
INSTRUCTIONS FOR COMPLETING NEW HIRE PAPERWORK ADDITIONAL INFORMATION SHEET: Must be LEGIBLE, PLEASE PRINT, Make sure that you have checked the "CAN" or "CANNOT" be given to the public box at the bottom
FACTS YOU SHOULD KNOW ABOUT APPLYING FOR TEMPORARY CASH ASSISTANCE, FOOD SUPPLEMENT PROGRAM (FORMERLY FOOD STAMPS), AND MEDICAL ASSISTANCE
, AND MEDICAL ASSISTANCE") Your Rights and Responsibilities FACTS YOU SHOULD KNOW ABOUT APPLYING FOR TEMPORARY CASH ASSISTANCE, FOOD SUPPLEMENT PROGRAM (FORMERLY FOOD STAMPS), AND MEDICAL ASSISTANCE Social Security Numbers You must
Your Rights and Responsibilities FACTS YOU SHOULD KNOW ABOUT APPLYING FOR TEMPORARY CASH ASSISTANCE, FOOD SUPPLEMENT PROGRAM (FORMERLY FOOD STAMPS), AND MEDICAL ASSISTANCE Social Security Numbers You must
*NEWACCT* BUSINESS ACCOUNT APPLICATION Institutional Advisor Services. General Instructions
 General Instructions By completing and signing this application the account owner is establishing an account subject to the terms and conditions made available by your advisor and at trustamerica.com/tca
General Instructions By completing and signing this application the account owner is establishing an account subject to the terms and conditions made available by your advisor and at trustamerica.com/tca
LOYALTY OATH. (H.B OK Leg.)
") Printed name of Employee Social Security Number Position LOYALTY OATH (H.B. 918-1968 OK Leg.) I do solemnly swear (or affirm) that I will support the Constitution and the Laws of the United States of America
Printed name of Employee Social Security Number Position LOYALTY OATH (H.B. 918-1968 OK Leg.) I do solemnly swear (or affirm) that I will support the Constitution and the Laws of the United States of America
2018 GAPP CPP/FPC Study Group
 2018 GAPP CPP/FPC Study Group SECTION 1: THE EMPLOYER-EMPLOYEE RELATIONSHIP THE EMPLOYER EMPLOYEE RELATIONSHIP Classification - Employee vs. Independent Contractor Employer's Obligation Penalties For Misclassification
2018 GAPP CPP/FPC Study Group SECTION 1: THE EMPLOYER-EMPLOYEE RELATIONSHIP THE EMPLOYER EMPLOYEE RELATIONSHIP Classification - Employee vs. Independent Contractor Employer's Obligation Penalties For Misclassification
Assurance Company. Term Life Eligibility. Child Term Life Insurance. Member Term Life Insurance LIFE INSURANCE
 Assurance Company Voluntary Term Life and Short Term Disability Insurance Term Life Eligibility If you are a member and work at least 40 hours per month, you are eligible to apply for member Voluntary
Assurance Company Voluntary Term Life and Short Term Disability Insurance Term Life Eligibility If you are a member and work at least 40 hours per month, you are eligible to apply for member Voluntary
Moda Health HMO. Individual enrollment election form. To enroll in Moda Health HMO plan, please provide the following information:
 Moda Health HMO Individual enrollment election form Moda Health Plan, Inc. Attn: Medicare Billing & Eligibility P.O. Box 40384 Portland, OR 97240-0384 503-265-4762 1-877-299-9062 TTY: 711 Fax: 503-224-1975
Moda Health HMO Individual enrollment election form Moda Health Plan, Inc. Attn: Medicare Billing & Eligibility P.O. Box 40384 Portland, OR 97240-0384 503-265-4762 1-877-299-9062 TTY: 711 Fax: 503-224-1975
APPLICATION FOR STATE EMERGENCY RELIEF Michigan Department of Human Services
 APPLICATION FOR STATE EMERGENCY RELIEF Michigan Department of Human Services Case Name: Case Number: Date: DHS Office: Specialist: Phone: Fax: Specialist ID: Client ID: I hereby make application for the
APPLICATION FOR STATE EMERGENCY RELIEF Michigan Department of Human Services Case Name: Case Number: Date: DHS Office: Specialist: Phone: Fax: Specialist ID: Client ID: I hereby make application for the
2016 GAPP CPP/FPC Study Group SECTION 1: THE EMPLOYER-EMPLOYEE RELATIONSHIP
 2016 GAPP CPP/FPC Study Group SECTION 1: THE EMPLOYER-EMPLOYEE RELATIONSHIP THE EMPLOYER EMPLOYEE RELATIONSHIP Employee vs. Independent Contractor Employer's Obligation Penalties For Misclassification
2016 GAPP CPP/FPC Study Group SECTION 1: THE EMPLOYER-EMPLOYEE RELATIONSHIP THE EMPLOYER EMPLOYEE RELATIONSHIP Employee vs. Independent Contractor Employer's Obligation Penalties For Misclassification
USE THIS FORM AS YOUR RETURN FAX COVER PAGE
 Innovative, Inc. 5501 LBJ Freeway Suite 108 Dallas, Texas 75240 (972) 392-1144 (800) 859-1615 Fax (972) 392-1196 (Secure Fax Line) Email: payroll@stadiumpeople.com (Secure Email Address) Attn: Payroll
Innovative, Inc. 5501 LBJ Freeway Suite 108 Dallas, Texas 75240 (972) 392-1144 (800) 859-1615 Fax (972) 392-1196 (Secure Fax Line) Email: payroll@stadiumpeople.com (Secure Email Address) Attn: Payroll
International Student and Scholar Services Middle Tennessee State University. J-1 Visitor s Handbook
 International Student and Scholar Services Middle Tennessee State University J-1 Visitor s Handbook Table of Contents Important Documents and Acronyms...1 Your Activities as a J-1 Visitor...3 Time Limits...4
International Student and Scholar Services Middle Tennessee State University J-1 Visitor s Handbook Table of Contents Important Documents and Acronyms...1 Your Activities as a J-1 Visitor...3 Time Limits...4
CDS Participant's New Attendant Check List
 CDS Participant's New Attendant Check List Participant : The person receiving care through the Medicaid-funded program Consumer Directed Services (CDS). This person is the employer of the attendant. May
CDS Participant's New Attendant Check List Participant : The person receiving care through the Medicaid-funded program Consumer Directed Services (CDS). This person is the employer of the attendant. May