Name: MCO (circle one): AG UHC VSHP (Blue Care) Worker Training Checklist. I-9 Criminal Attestation Tax Exempt W-4. Additional Comments:
|
|
|
- Morris Wright
- 5 years ago
- Views:
Transcription
1 414 Union ST, Ste 1100 Nashville, TN Fax - Worker United Health Care Fax: (FOR DOCUMENTS ONLY. NO TIMESHEETS TO THIS NUMBER) Customer Service: To: Fax: Phone: Member Name: From: Pages: Date Sent: Rep/EOR Name: Worker Name: Do you provide care for another member? (circle one) YES NO If yes, please list the other member s name and MCO: Name: MCO (circle one): AG UHC VSHP (Blue Care) Circle all documents included on this fax: Worker Application/ Demographics CPR/First Aid Certification Worker Training Checklist Service Agreement I-9 Criminal Attestation Tax Exempt W-4 Name Change Fraud Form EFT Worker Driver s License/ Social Security Card Additional Comments:
2
3 Public Partnerships, LLC Financial Administrator One Cabot RD, STE 102 Medford, MA Toll Free Numbers Phone: TTY: Administrative Fax: Employment Packet Introduction to PPL Information for Workers Dear Worker: CHOICES Consumer Direction Program Employment Packet Welcome aboard! You have received this packet because a member in the CHOICES Consumer Direction Program has selected you to provide services. TennCare and the managed care organizations participating in the CHOICES program have contracted with Public Partnerships, LLC (PPL) to act as the Fiscal Employer Agent (FEA) for CHOICES Consumer Direction members. PPL will make payments on behalf of members who employ workers. Below you will see three lists of forms. The forms in the list Forms Required for All Workers must be completed and submitted to PPL as soon as possible so that PPL can pay you. The forms in the list Optional Forms are not required by PPL, but may be useful to you. If they are, submit these forms to PPL. Keep the forms in the list Forms to Keep You Will Use These for the Program. You must complete a separate employment packet for each member who employs you. PPL cannot pay for any services until a completed packet is received and we receive documentation that you have completed all required training. PPL will issue paychecks to you based on properly submitted time. These paychecks will reflect tax withholdings. If you have any questions, please call us toll free at Thank you. Forms Required For All Workers 1. USCIS Form I-9. Department of Homeland Security - Employment Eligibility Verification 2. IRS Form W-4. Employee s Withholding Allowance Certificate 3. CHOICES Provider Application 4. Service Agreement 5. Employer/Worker Relationship Federal Tax Exemption Information Form Forms to Keep You Will Use These for the Program 1. Payroll Schedule 2. PPL Customer Service 3. Worker Training and Certification Requirements 4. Required Worker Training 5. Consumer Direction in the CHOICES Program Worker Training 6. CHOICES Worker Training Checklist for Consumer Direction NEED HELP? CALL TOLL FREE AT Worker Letter Page 1 of 2
4 1. EFT Instructions and Application 2. Change of Address/Name Form Optional Forms Before you are eligible to provide services to a CHOICES member, you must: Complete and submit to PPL all forms listed on page 1 of this packet. Complete and successfully pass a Criminal Background Check and Registry Checks. Complete First Aid and CPR Certification. Complete required training. After you start working for a CHOICES member, you will: Use the EVV call-in, call-out system to record the time worked. Complete daily notes for each shift. Receive a W-2 Wage Statement from PPL every year, on behalf of your employer. What is the U.S. Citizenship and Immigration Services (USCIS) Form I-9? The USCIS Form I-9 is your employment eligibility verification. You must bring this form, and the documents listed on the I-9 to your employer, the CHOICES member. Your employer will review the documents, confirm your identity and verify your identity by signing this form. Federal law requires that all employers and workers complete this form. What taxes will be withheld? Will I see them on my paycheck stub? PPL will withhold Social Security, Medicare (FICA), and federal income taxes from your paycheck as applicable. A summary of all tax withholdings will appear on your paycheck stub throughout the calendar year. PPL also will mail you a W-2 form each January. You will need this W-2 form to file your individual tax return by April of each year. Your employer will receive regular reports from PPL about your total hours worked. PPL encourages you to call us toll free at if you have any questions. TTY users please dial toll free at PPL staff is available to help walk you through the forms over the phone. We look forward to working with you. NEED HELP? CALL TOLL FREE AT Worker Letter Page 2 of 2
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22

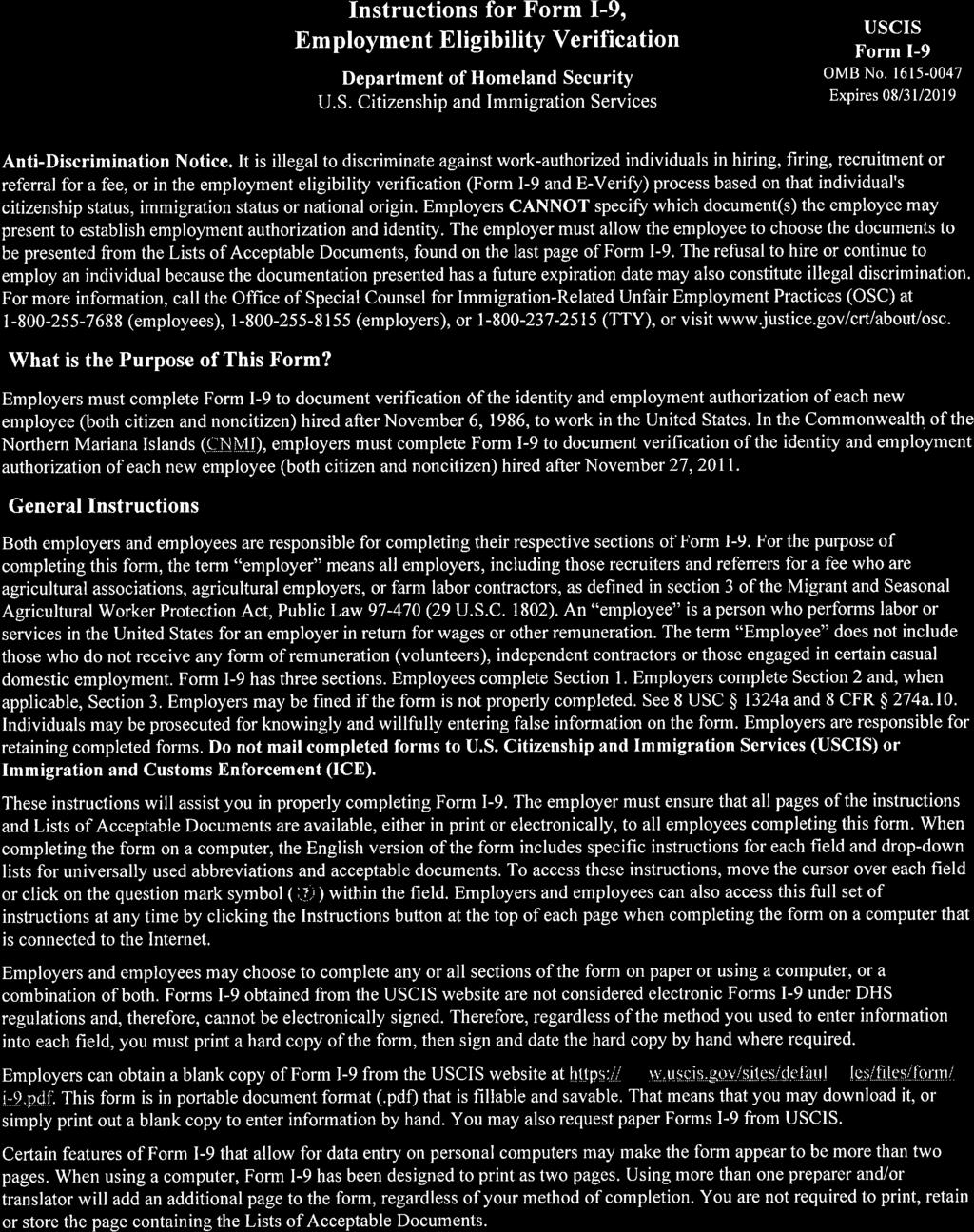
23 Employment Eligibility Verification Department of Homeland Security U.S. Citizenship and Immigration Services USCIS Form I-9 OMB No Expires 08/31/2019 START HERE: Read instructions carefully before completing this form. The instructions must be available, either in paper or electronically, during completion of this form. Employers are liable for errors in the completion of this form. ANTI-DISCRIMINATION NOTICE:It is illegal to discriminate against work-authorized individuals. Employers CANNOT specify which document(s) an employee may present to establish employment authorization and identity. The refusal to hire or continue to employ an individual because the documentation presented has a future expiration date may also constitute illegal discrimination. Section 1. Employee Information and Attestation (Employees must complete and sign Section 1 of Form I-9 no later than the first day of employment, but not before accepting a job offer.) Last Name (Family Name) First Name (Given Name) Middle Initial Other Last Names Used (if any) Address (Street Number and Name) Apt. Number City or Town State ZIP Code Date of Birth (mm/dd/yyyy) U.S. Social Security Number Employee's Address Employee's Telephone Number - - I am aware that federal law provides for imprisonment and/or fines for false statements or use of false documents in connection with the completion of this form. I attest, under penalty of perjury, that I am (check one of the following boxes): 1. A citizen of the United States 2. A noncitizen national of the United States (See instructions) 3. A lawful permanent resident (Alien Registration Number/USCIS Number): 4. An alien authorized to work until (expiration date, if applicable, mm/dd/yyyy): Some aliens may write "N/A" in the expiration date field. (See instructions) Aliens authorized to work must provide only one of the following document numbers to complete Form I-9: An Alien Registration Number/USCIS Number OR Form I-94 Admission Number OR Foreign Passport Number. QR Code - Section 1 Do Not Write In This Space 1. Alien Registration Number/USCIS Number: OR 2. Form I-94 Admission Number: OR 3. Foreign Passport Number: Country of Issuance: Signature of Employee Today's Date (mm/dd/yyyy) Preparer and/or Translator Certification (check one): I did not use a preparer or translator. A preparer(s) and/or translator(s) assisted the employee in completing Section 1. (Fields below must be completed and signed when preparers and/or translators assist an employee in completing Section 1.) I attest, under penalty of perjury, that I have assisted in the completion of Section 1 of this form and that to the best of my knowledge the information is true and correct. Signature of Preparer or Translator Today's Date (mm/dd/yyyy) Last Name (Family Name) First Name (Given Name) Address (Street Number and Name) City or Town State ZIP Code Employer Completes Next Page Form I-9 07/17/17 N Page 1 of 3
24
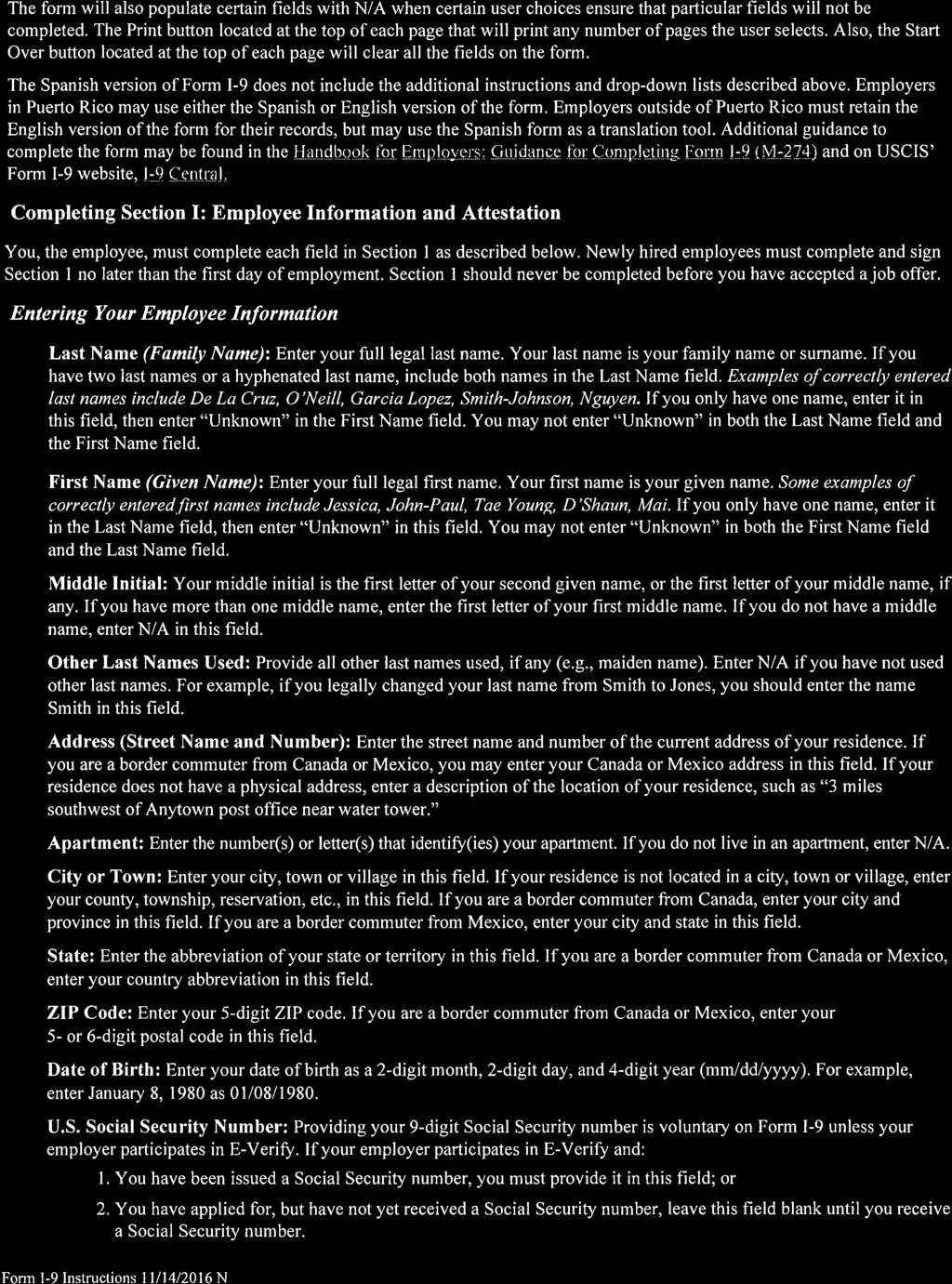
25 Employment Eligibility Verification Department of Homeland Security U.S. Citizenship and Immigration Services USCIS Form I-9 OMB No Expires 08/31/2019 Section 2. Employer or Authorized Representative Review and Verification (Employers or their authorized representative must complete and sign Section 2 within 3 business days of the employee's first day of employment. You must physically examine one document from List A OR a combination of one document from List B and one document from List C as listed on the "Lists of Acceptable Documents.") Employee info from Section 1 Last Name (Family Name) First Name (Given Name) M.I. Citizenship/Immigration Status List A A Identity and Employment Authorization Document Title ORR List B ANDD List C Identity Employment Authorization Document Title Document Title Issuing Authority Document Number Issuing Authority Document Number Issuing Authority Document Number Expiration Date (if any)(mm/dd/yyyy) Expiration Date (if any)(mm/dd/yyyy) Expiration Date (if any)(mm/dd/yyyy) Document Title Issuing Authority Document Number Additional Information QR Code - Sections 2 & 3 Do Not Write In This Space Expiration Date (if any)(mm/dd/yyyy) Document Title Issuing Authority Document Number Expiration Date (if any)(mm/dd/yyyy) Certification: I attest, under penalty of perjury, that (1) I have examined the document(s) presented by the above-named employee, (2) the above-listed document(s) appear to be genuine and to relate to the employee named, and (3) to the best of my knowledge the employee is authorized to work in the United States. The employee's first day of employment (mm/dd/yyyy): (See instructions for exemptions) Signature of Employer or Authorized Representative Today's Date (mm/dd/yyyy) Title of Employer or Authorized Representative Last Name of Employer or Authorized Representative First Name of Employer or Authorized Representative Employer's Business or Organization Name Employer's Business or Organization Address (Street Number and Name) City or Town State ZIP Code Section 3. Reverification and Rehires (To be completed and signed by employer or authorized representative.) A. New Name (if applicable) B. Date of Rehire (if applicable) Last Name (Family Name) First Name (Given Name) Middle Initial Date (mm/dd/yyyy) C. If the employee's previous grant of employment authorization has expired, provide the information for the document or receipt that establishes continuing employment authorization in the space provided below. Document Title Document Number Expiration Date (if any) (mm/dd/yyyy) I attest, under penalty of perjury, that to the best of my knowledge, this employee is authorized to work in the United States, and if the employee presented document(s), the document(s), I have examined appear to be genuine and to relate to the individual. Signature of Employer or Authorized Representative Today's Date (mm/dd/yyyy) Name of Employer or Authorized Representative Form I-9 07/17/17 N Page 2 of 3
26
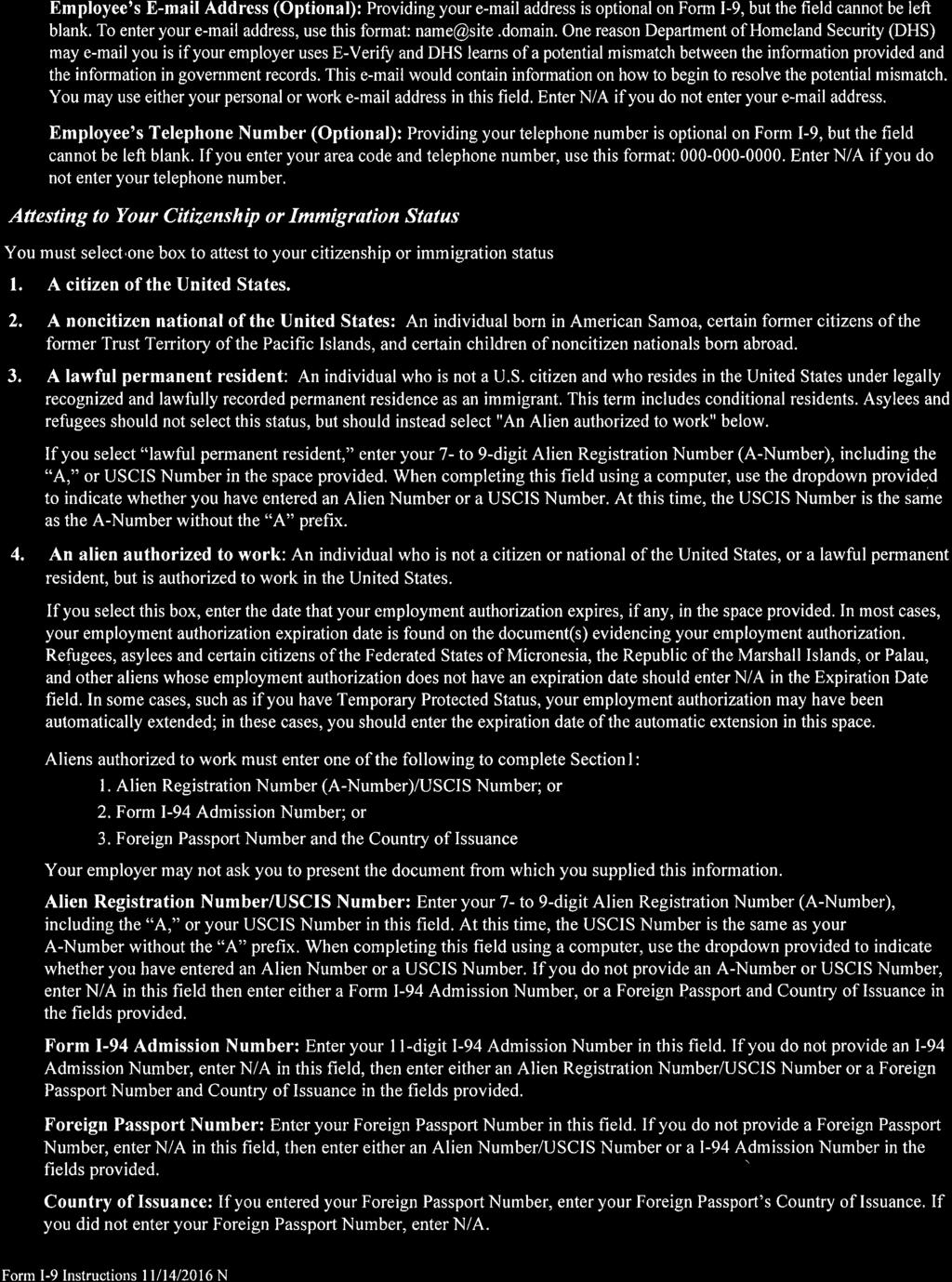
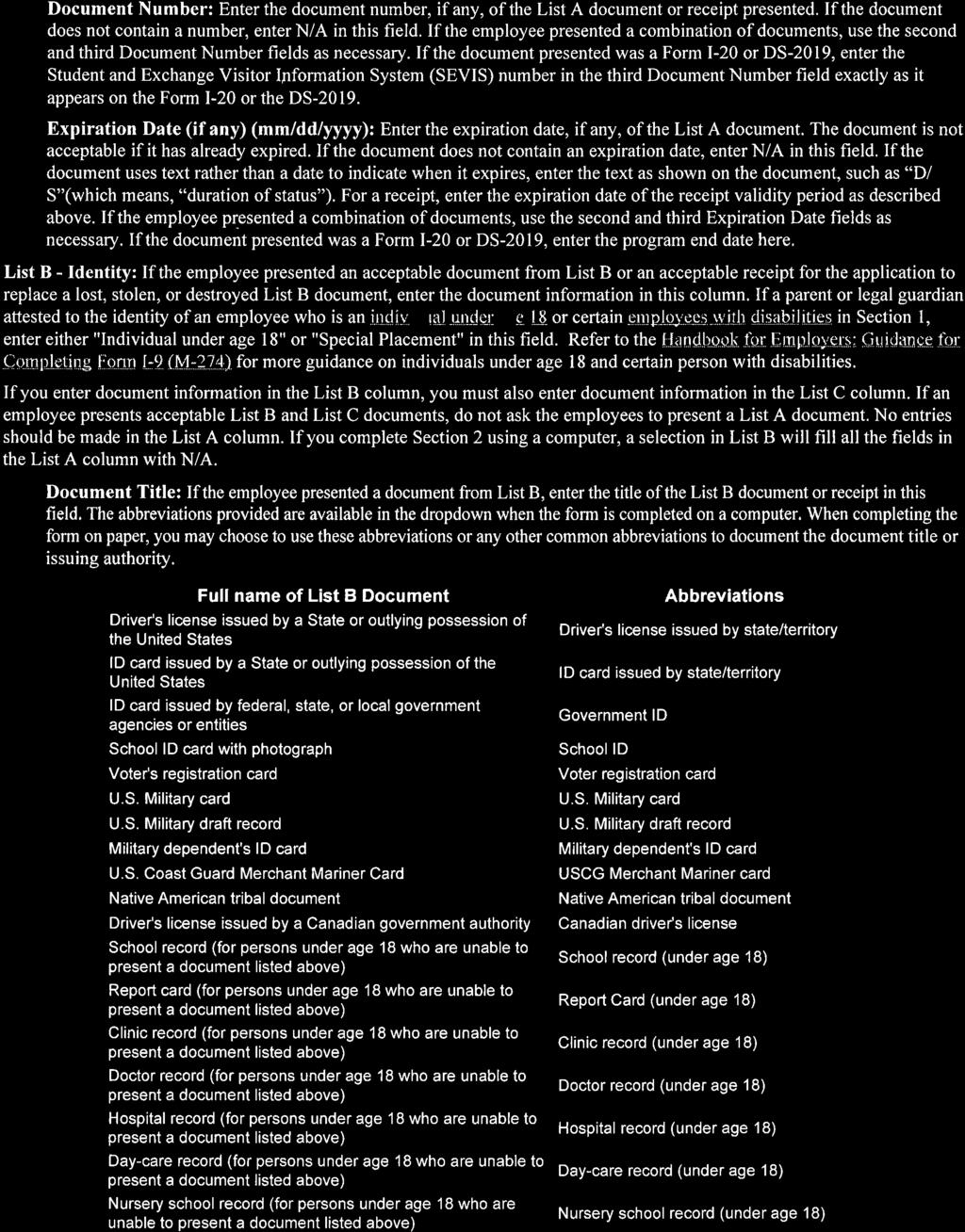
27 LISTS OF ACCEPTABLE DOCUMENTS All documents must be UNEXPIREDD Employees may present one selection from List A or a combination of one selection from List B and one selection from List C. LIST A LIST BT B Documents that Establish Identity LIST C Documents that Establish Employment Authorization Documents that Establish Both Identity and Employment Authorization OR AND 1. U.S. Passport or U.S. Passport Card 2. Permanent Resident Card or Alien Registration Receipt Card (Form I-551) 3. Foreign passport that contains a temporary I-551 stamp or temporary I-551 printed notation on a machinereadable immigrant visa 4. Employment Authorization Document that contains a photograph (Form I-766) 5. For a nonimmigrant alien authorized to work for a specific employer because of his or her status: a. Foreign passport; and b. Form I-94 or Form I-94A that has the following: (1) The same name as the passport; and (2) An endorsement of the alien's nonimmigrant status as long as that period of endorsement has not yet expired and the proposed employment is not in conflict with any restrictions or limitations identified on the form. 6. Passport from the Federated States of Micronesia (FSM) or the Republic of the Marshall Islands (RMI) with Form I-94 or Form I-94A indicating nonimmigrant admission under the Compact of Free Association Between the United States and the FSM or RMI 1. Driver's license or ID card issued by a State or outlying possession of the United States provided it contains a photograph or information such as name, date of birth, gender, height, eye color, and address 2. ID card issued by federal, state or local government agencies or entities, provided it contains a photograph or information such as name, date of birth, gender, height, eye color, and address 3. School ID card with a photograph 4. Voter's registration card 5. U.S. Military card or draft record 6. Military dependent's ID card 7. U.S. Coast Guard Merchant Mariner Card 8. Native American tribal document 9. Driver's license issued by a Canadian government authority For persons under age 18 who are unable to present a document listed above: 10. School record or report card 11. Clinic, doctor, or hospital record 12. Day-care or nursery school record 1. A Social Security Account Number card, unless the card includes one of the following restrictions: (1) NOT VALID FOR EMPLOYMENT (2) VALID FOR WORK ONLY WITH INS AUTHORIZATION (3) VALID FOR WORK ONLY WITH DHS AUTHORIZATION 2. Certification of report of birth issued by the Department of State (Forms DS-1350, FS-545, FS-240) 3. Original or certified copy of birth certificate issued by a State, county, municipal authority, or territory of the United States bearing an official seal 4. Native American tribal document 5. U.S. Citizen ID Card (Form I-197) 6. Identification Card for Use of Resident Citizen in the United States (Form I-179) 7. Employment authorization document issued by the Department of Homeland Security Examples of many of these documents appear in Part 13 of the Handbook for Employers (M-274). Refer to the instructions for more information about acceptable receipts. Form I-9 07/17/17 N Page 3 of 3
28
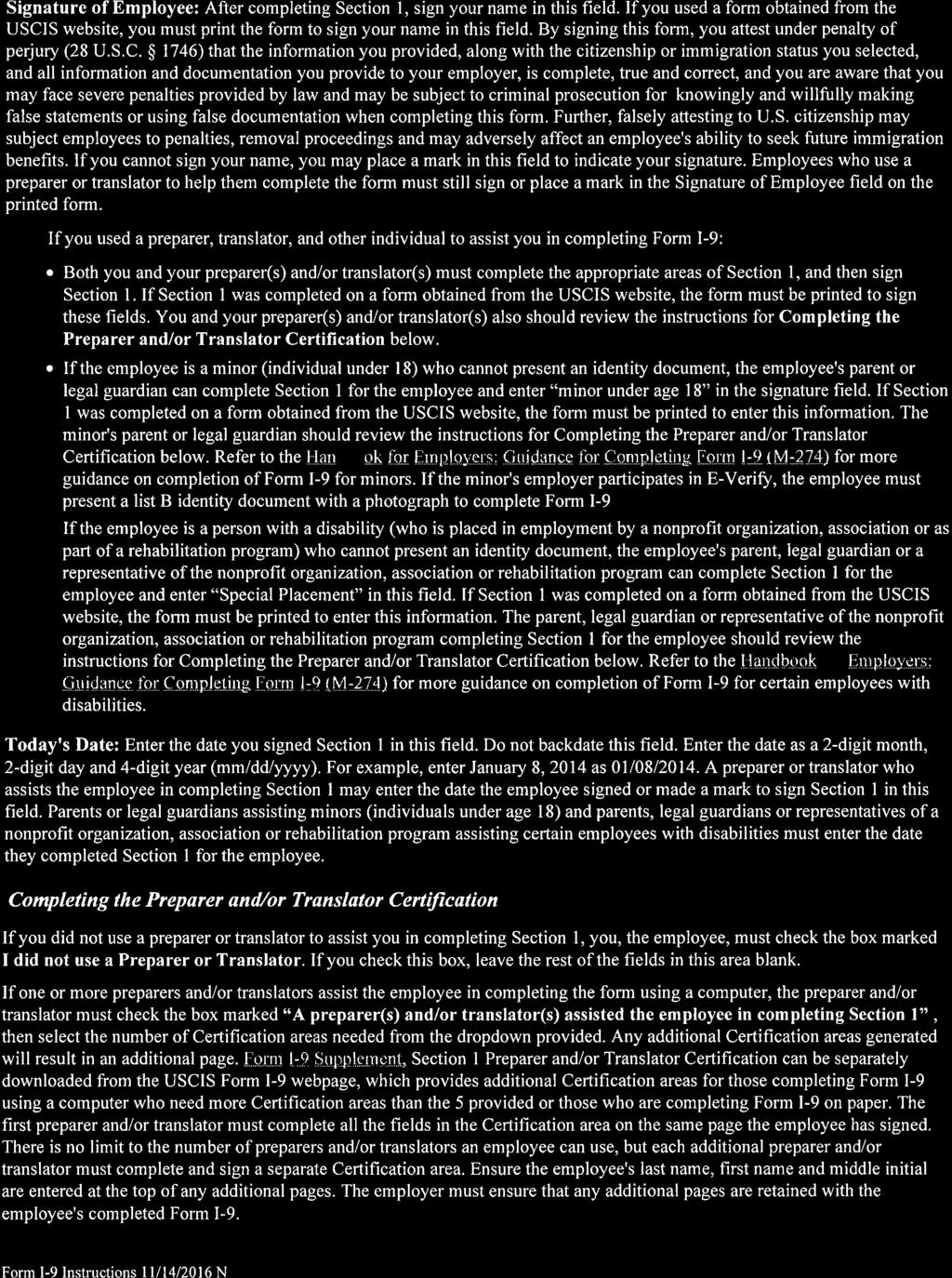
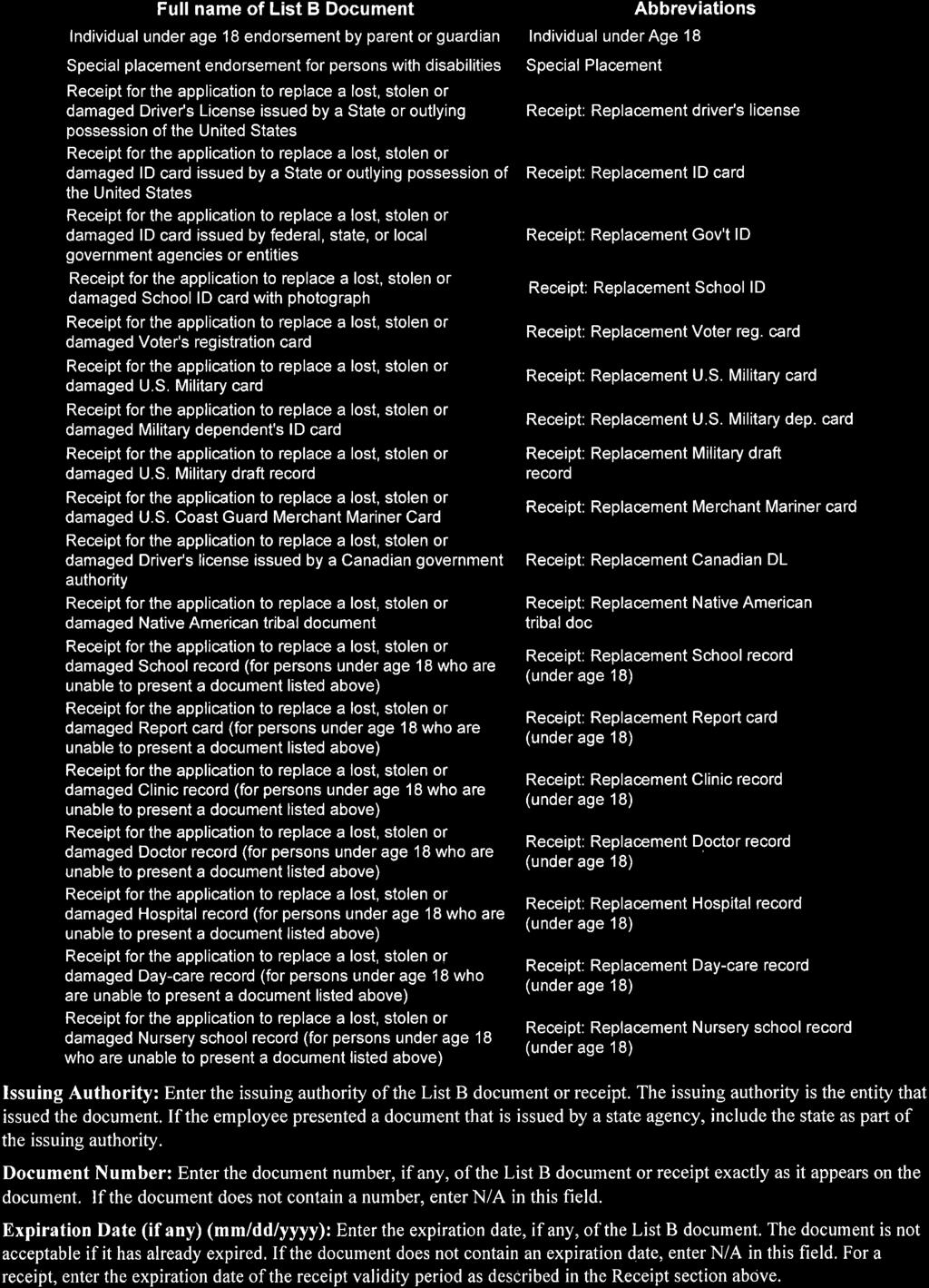
29 Form W-4 (2017) Purpose. Complete Form W-4 so that your employer can withhold the correct federal income tax from your pay. Consider completing a new Form W-4 each year and when your personal or financial situation changes. Exemption from withholding. If you are exempt, complete only lines 1, 2, 3, 4, and 7 and sign the form to validate it. Your exemption for 2017 expires February 15, See Pub. 505, Tax Withholding and Estimated Tax. Note: If another person can claim you as a dependent on his or her tax return, you can t claim exemption from withholding if your total income exceeds $1,050 and includes more than $350 of unearned income (for example, interest and dividends). Exceptions. An employee may be able to claim exemption from withholding even if the employee is a dependent, if the employee: Is age 65 or older, Is blind, or Will claim adjustments to income; tax credits; or itemized deductions, on his or her tax return. The exceptions don t apply to supplemental wages greater than $1,000,000. Basic instructions. If you aren t exempt, complete the Personal Allowances Worksheet below. The worksheets on page 2 further adjust your withholding allowances based on itemized deductions, certain credits, adjustments to income, or two-earners/multiple jobs situations. Complete all worksheets that apply. However, you may claim fewer (or zero) allowances. For regular wages, withholding must be based on allowances you claimed and may not be a flat amount or percentage of wages. Head of household. Generally, you can claim head of household filing status on your tax return only if you are unmarried and pay more than 50% of the costs of keeping up a home for yourself and your dependent(s) or other qualifying individuals. See Pub. 501, Exemptions, Standard Deduction, and Filing Information, for information. Tax credits. You can take projected tax credits into account in figuring your allowable number of withholding allowances. Credits for child or dependent care expenses and the child tax credit may be claimed using the Personal Allowances Worksheet below. See Pub. 505 for information on converting your other credits into withholding allowances. Nonwage income. If you have a large amount of nonwage income, such as interest or dividends, consider making estimated tax payments using Form 1040-ES, Estimated Tax for Individuals. Otherwise, you may owe additional tax. If you have pension or annuity income, see Pub. 505 to find out if you should adjust your withholding on Form W-4 or W-4P. Two earners or multiple jobs. If you have a working spouse or more than one job, figure the total number of allowances you are entitled to claim on all jobs using worksheets from only one Form W-4. Your withholding usually will be most accurate when all allowances are claimed on the Form W-4 for the highest paying job and zero allowances are claimed on the others. See Pub. 505 for details. Nonresident alien. If you are a nonresident alien, see Notice 1392, Supplemental Form W-4 Instructions for Nonresident Aliens, before completing this form. Check your withholding. After your Form W-4 takes effect, use Pub. 505 to see how the amount you are having withheld compares to your projected total tax for See Pub. 505, especially if your earnings exceed $130,000 (Single) or $180,000 (Married). Future developments. Information about any future developments affecting Form W-4 (such as legislation enacted after we release it) will be posted at Personal Allowances Worksheet (Keep for your records.) A Enter 1 for yourself if no one else can claim you as a dependent A You re single and have only one job; or B Enter 1 if: You re married, have only one job, and your spouse doesn t work; or... B { } Your wages from a second job or your spouse s wages (or the total of both) are $1,500 or less. C Enter 1 for your spouse. But, you may choose to enter -0- if you are married and have either a working spouse or more than one job. (Entering -0- may help you avoid having too little tax withheld.) C D Enter number of dependents (other than your spouse or yourself) you will claim on your tax return D E Enter 1 if you will file as head of household on your tax return (see conditions under Head of household above).. E F Enter 1 if you have at least $2,000 of child or dependent care expenses for which you plan to claim a credit... F (Note: Do not include child support payments. See Pub. 503, Child and Dependent Care Expenses, for details.) G Child Tax Credit (including additional child tax credit). See Pub. 972, Child Tax Credit, for more information. If your total income will be less than $70,000 ($100,000 if married), enter 2 for each eligible child; then less 1 if you have two to four eligible children or less 2 if you have five or more eligible children. If your total income will be between $70,000 and $84,000 ($100,000 and $119,000 if married), enter 1 for each eligible child. G H Add lines A through G and enter total here. (Note: This may be different from the number of exemptions you claim on your tax return.) H { If you plan to itemize or claim adjustments to income and want to reduce your withholding, see the Deductions For accuracy, and Adjustments Worksheet on page 2. complete all If you are single and have more than one job or are married and you and your spouse both work and the combined worksheets earnings from all jobs exceed $50,000 ($20,000 if married), see the Two-Earners/Multiple Jobs Worksheet on page 2 that apply. to avoid having too little tax withheld. If neither of the above situations applies, stop here and enter the number from line H on line 5 of Form W-4 below. Separate here and give Form W-4 to your employer. Keep the top part for your records. Employee s Withholding Allowance Certificate Form W-4 Department of the Treasury Whether you are entitled to claim a certain number of allowances or exemption from withholding is Internal Revenue Service subject to review by the IRS. Your employer may be required to send a copy of this form to the IRS. 1 Your first name and middle initial Last name OMB No Your social security number Home address (number and street or rural route) 3 Single Married Married, but withhold at higher Single rate. Note: If married, but legally separated, or spouse is a nonresident alien, check the Single box. City or town, state, and ZIP code 4 If your last name differs from that shown on your social security card, check here. You must call for a replacement card. 5 Total number of allowances you are claiming (from line H above or from the applicable worksheet on page 2) 5 6 Additional amount, if any, you want withheld from each paycheck $ 7 I claim exemption from withholding for 2017, and I certify that I meet both of the following conditions for exemption. Last year I had a right to a refund of all federal income tax withheld because I had no tax liability, and This year I expect a refund of all federal income tax withheld because I expect to have no tax liability. If you meet both conditions, write Exempt here Under penalties of perjury, I declare that I have examined this certificate and, to the best of my knowledge and belief, it is true, correct, and complete. Employee s signature (This form is not valid unless you sign it.) Date 8 Employer s name and address (Employer: Complete lines 8 and 10 only if sending to the IRS.) 9 Office code (optional) 10 Employer identification number (EIN) For Privacy Act and Paperwork Reduction Act Notice, see page 2. Cat. No Q Form W-4 (2017)
30
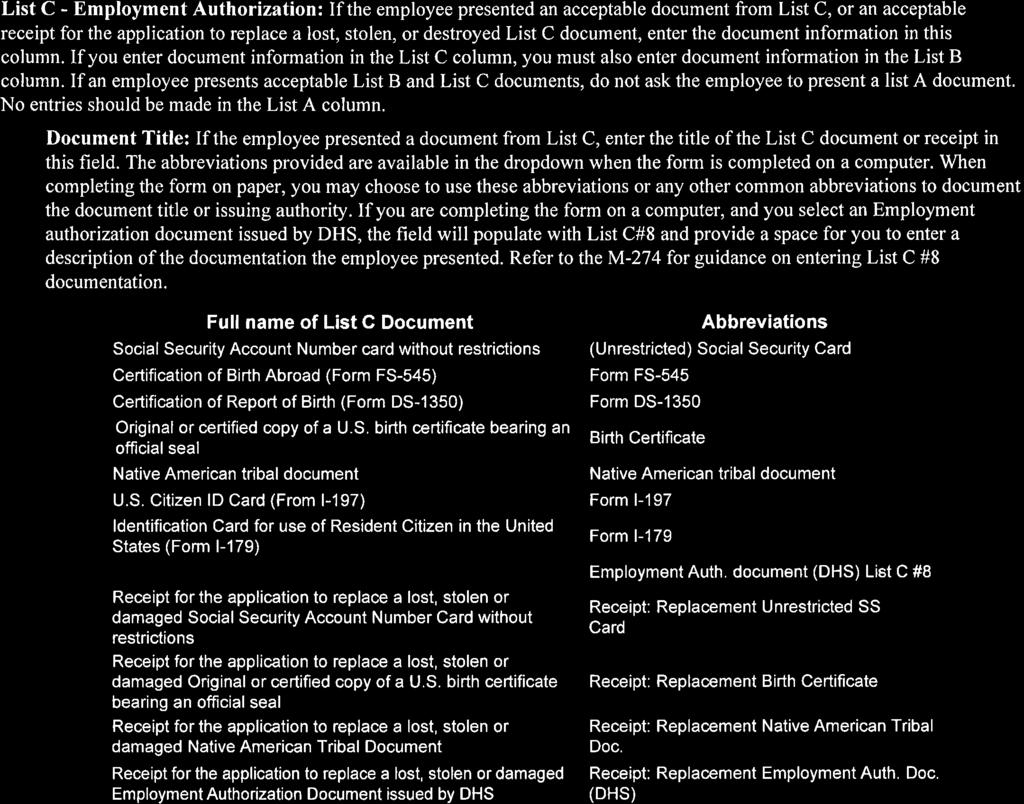
31 Form W-4 (2017) Page 2 Deductions and Adjustments Worksheet Note: Use this worksheet only if you plan to itemize deductions or claim certain credits or adjustments to income. 1 Enter an estimate of your 2017 itemized deductions. These include qualifying home mortgage interest, charitable contributions, state and local taxes, medical expenses in excess of 10% of your income, and miscellaneous deductions. For 2017, you may have to reduce your itemized deductions if your income is over $313,800 and you re married filing jointly or you re a qualifying widow(er); $287,650 if you re head of household; $261,500 if you re single, not head of household and not a qualifying widow(er); or $156,900 if you re married filing separately. See Pub. 505 for details $ $12,700 if married filing jointly or qualifying widow(er) 2 Enter: $9,350 if head of household $ { } $6,350 if single or married filing separately 3 Subtract line 2 from line 1. If zero or less, enter $ 4 Enter an estimate of your 2017 adjustments to income and any additional standard deduction (see Pub. 505) 4 $ 5 Add lines 3 and 4 and enter the total. (Include any amount for credits from the Converting Credits to Withholding Allowances for 2017 Form W-4 worksheet in Pub. 505.) $ 6 Enter an estimate of your 2017 nonwage income (such as dividends or interest) $ 7 Subtract line 6 from line 5. If zero or less, enter $ 8 Divide the amount on line 7 by $4,050 and enter the result here. Drop any fraction Enter the number from the Personal Allowances Worksheet, line H, page Add lines 8 and 9 and enter the total here. If you plan to use the Two-Earners/Multiple Jobs Worksheet, also enter this total on line 1 below. Otherwise, stop here and enter this total on Form W-4, line 5, page 1 10 Two-Earners/Multiple Jobs Worksheet (See Two earners or multiple jobs on page 1.) Note: Use this worksheet only if the instructions under line H on page 1 direct you here. 1 Enter the number from line H, page 1 (or from line 10 above if you used the Deductions and Adjustments Worksheet) 1 2 Find the number in Table 1 below that applies to the LOWEST paying job and enter it here. However, if you are married filing jointly and wages from the highest paying job are $65,000 or less, do not enter more than If line 1 is more than or equal to line 2, subtract line 2 from line 1. Enter the result here (if zero, enter -0- ) and on Form W-4, line 5, page 1. Do not use the rest of this worksheet Note: If line 1 is less than line 2, enter -0- on Form W-4, line 5, page 1. Complete lines 4 through 9 below to figure the additional withholding amount necessary to avoid a year-end tax bill. 4 Enter the number from line 2 of this worksheet Enter the number from line 1 of this worksheet Subtract line 5 from line Find the amount in Table 2 below that applies to the HIGHEST paying job and enter it here $ 8 Multiply line 7 by line 6 and enter the result here. This is the additional annual withholding needed.. 8 $ 9 Divide line 8 by the number of pay periods remaining in For example, divide by 25 if you are paid every two weeks and you complete this form on a date in January when there are 25 pay periods remaining in Enter the result here and on Form W-4, line 6, page 1. This is the additional amount to be withheld from each paycheck 9 $ Table 1 Table 2 Married Filing Jointly All Others Married Filing Jointly All Others If wages from LOWEST paying job are Enter on line 2 above $0 - $7, ,001-14, ,001-22, ,001-27, ,001-35, ,001-44, ,001-55, ,001-65, ,001-75, ,001-80, ,001-95, , , , , , , , , ,001 and over 15 If wages from LOWEST paying job are Enter on line 2 above $0 - $8, ,001-16, ,001-26, ,001-34, ,001-44, ,001-70, ,001-85, , , , , , , ,001 and over 10 Privacy Act and Paperwork Reduction Act Notice. We ask for the information on this form to carry out the Internal Revenue laws of the United States. Internal Revenue Code sections 3402(f)(2) and 6109 and their regulations require you to provide this information; your employer uses it to determine your federal income tax withholding. Failure to provide a properly completed form will result in your being treated as a single person who claims no withholding allowances; providing fraudulent information may subject you to penalties. Routine uses of this information include giving it to the Department of Justice for civil and criminal litigation; to cities, states, the District of Columbia, and U.S. commonwealths and possessions for use in administering their tax laws; and to the Department of Health and Human Services for use in the National Directory of New Hires. We may also disclose this information to other countries under a tax treaty, to federal and state agencies to enforce federal nontax criminal laws, or to federal law enforcement and intelligence agencies to combat terrorism. If wages from HIGHEST paying job are Enter on line 7 above $0 - $75,000 $610 75, ,000 1, , ,000 1, , ,000 1, , ,000 1, ,001 and over 1,600 If wages from HIGHEST paying job are Enter on line 7 above $0 - $38,000 $610 38,001-85,000 1,010 85, ,000 1, , ,000 1, ,001 and over 1,600 You are not required to provide the information requested on a form that is subject to the Paperwork Reduction Act unless the form displays a valid OMB control number. Books or records relating to a form or its instructions must be retained as long as their contents may become material in the administration of any Internal Revenue law. Generally, tax returns and return information are confidential, as required by Code section The average time and expenses required to complete and file this form will vary depending on individual circumstances. For estimated averages, see the instructions for your income tax return. If you have suggestions for making this form simpler, we would be happy to hear from you. See the instructions for your income tax return.
32
33 CHOICES PROVIDER APPLICATION As a potential employee in the Tennessee CHOICES Consumer-Direction program, you are required to complete this application and submit it to Public Partnerships, LLC (PPL) with your Employment Paperwork. PPL will conduct a criminal background and abuse registry check on you before submitting the completed Provider Agreement to TennCare. All incomplete applications will be returned to the address listed on your application. Original signature is required for all documents. If you have any questions regarding this application please contact TennCare at You will need to complete and sign both of the attached pages. 1. Application services and demographic page 2. Criminal Attestation / Disclosure page Note: Exceptions to background results may be granted at the member s discretion and only if all of the following conditions are met: Offense is a misdemeanor; Offense occurred more than five (5) years ago; Offense is not related to physical or sexual or emotional abuse of another person; Offense does not involve violence against another person or the manufacture, sale, or distribution of drugs; and There is only one disqualifying offense. CHOICES Provider Application: Page 1 of 4
34
35 TENNESSEE DEPARTMENT OF FINANCE AND ADMINISTRATION CHOICES HCBS Consumer-Direction Individual Provider Application (Check All That Apply) New Enrollment Reactivation Services you will to provide to CHOICES Consumer-Directed Participant: (Check All That Apply) Personal Care Visits Attendant Services In-Home Respite Companion Care Demographic Information Legal First Name: Legal Last Name: Address: City: State: Zip Code: Telephone Number ( _ ) - Alternate Number: ( ) - Address (if applicable): Social Security Number: - - Date of Birth: / / Application Surety Statement: I certify that the information provided on this application is complete and correct to the best of my knowledge. Signature: (Original signature of provider) Date: / / Printed Name: CHOICES Provider Application: Page 2 of 4
36
37 Disclosure Criminal Attestation Legal First Name: Provider Type: Individual Legal Last Name: Please answer the following questions as of the current date: 1. Have you personally been convicted of fraud related to Medicare, Medicaid or Title XX programs? NO YES If you answered YES, please provide details: 2. Have you personally been convicted of a criminal offense related to Medicare, Medicaid or Title XX programs? NO YES If you answered YES, please provide details: You will be required to submit to a background check to be completed in accordance with TCA Any offer of employment is contingent upon successfully passing the criminal background check. To pass the background check, you must not have a case of abuse, neglect, mistreatment or exploitation in your background. Furthermore, per TCA , you must list any prior conviction by any local, state, federal or military court of any felony or any other conviction involving sexual crimes, including but not limited to rape, sexual assault, sexual battery, exhibitionism, voyeurism, or any attempt to commit any of such sexual crimes: homicide or attempted homicide; felonious assault or attempted felonious assault; unlawful breaking or entering; robbery; burglary; theft; or arson. Also, if you are required to register, or have registered with the registry of sexual offenders in accordance with TCA , you must disclose such information. Please list any prior convictions or information regarding the registry of sexual offenders below: Choices Provider Application Page 3 of 4
38
39 Disclosure Criminal Attestation APPLICANT S STATEMENT I certify that all answers given herein are true and complete to the best of my knowledge. I authorize investigation of all matters contained in this application and I understand that misrepresentations, omissions of fact or incomplete information requested in this application may remove me from further consideration for employment. Applicant Signature: Date: It is the policy of the Department of Finance and Administration to ensure compliance with Title VI of the Civil Rights Act of 1964; 49 CFR Part 26, related statutes and regulations to the end that no person shall be excluded from participation in or be denied the benefits of, or be subjected to discrimination under any program or activity receiving federal financial assistance on the grounds of race, color, or national origin. BACKGROUND AND REGISTRY CHECKS COMPLETED BY PPL PPL conducts checks of all registries listed below on the Provider applicant. Tennessee Sexual Offender Registry National Sexual Offender Registry Tennessee Felony Offender Registry Tennessee Health Abuse Registry OIG List of Excluded Individuals/Entities Kroll Criminal Background Check Choices Provider Application Page 4 of 4
40
41 Consumer Direction SERVICE AGREEMENT I. Parties to the Agreement is a CHOICES member who has signed up to be in Consumer Direction. [Complete if applicable:] is his/her Representative for Consumer Direction. If the member does not have a representative, the member is the Employer in this agreement. If the member has a representative, the representative is the Employer in this agreement. is the Worker in this agreement. The Worker will be employed to provide consumer directed care for the member in the CHOICES program. This is an agreement between the Employer and the Worker. This agreement describes the responsibilities that the Employer and the Worker agree to perform. It sets out rules that the Employer and Worker agree to follow. It also describes certain rights that each party has. Public Partnerships Limited, LLC (PPL) is not a party to this agreement. However, both the Employer and the Worker agree to use PPL s services in carrying out this agreement. II. Terms of Agreement Services and Rate of Pay Services the Worker will provide to the member, the rate of pay for each service, and the tasks to be performed are: Services paid based on a hourly wage Personal care visits $. per hour ($. per 15 minutes) Tasks to be performed: In-home respite Tasks to be performed: $. per hour ($. per 15 minutes) Attendant care Tasks to be performed: $. per hour ($. per 15 minutes) Member/Representative Initials for changes / / Date Worker Initial for changes / / Date 1
42
43 Back-up Care The Worker wants to serve as back-up if other Workers are sick or unable to provide care. The Worker does not want to serve as back-up if other Workers are sick or unable to provide care. Services paid based on a monthly fee Companion care $. per month Tasks to be performed: Back-up Companion Care ONLY paid based on a daily rate* Companion care $. per day Tasks to be performed: * Note: This daily rate for Companion Care service can be paid ONLY for back-up care. This is care provided when the regular Companion is sick or unexpectedly not able to work. This daily rate can t be paid as part of ongoing Companion Care services. Self-Direction of Health Care Tasks If the Worker will also help the member with medicine, check this box. Be sure it s a kind of medicine that can be self-directed. (This doesn t include medicine that must be injected.) Be sure that giving medicine is included in the Tasks to be performed for that service. BEFORE the Worker can help with medicine, the member or representative must talk with the member s doctor to be sure it s OK. If the doctor says it s OK, the member or representative must train the Worker on how to give the medicine. The Employer must provide a list of medicine to be given by the Worker, the dosage, and the time it should be given. The Worker must write down all medicine that s given, the dosage and the time it s given. This could be in a medication log or in the daily service notes kept in the member s home. If the Worker doesn t give the right kind and amount of medicine at the scheduled time, they must report it to the member s Care Coordinator right away. This is called a medication error. The Employer will not ask, and the Worker will not perform any other health care tasks besides helping the member with medicine unless the Worker is permitted to perform those tasks under the Tennessee Nurse Practice Act. That s the State law which says what kinds of care must be performed by a Registered or Licensed Nurse and when there are exceptions. Member/Representative Initials for changes / / Date Worker Initial for changes / / Date 2
44
45 Transportation If the Worker will accompany the member into the community, check this box. If the Worker will transport the member into the community, check this box. o If this box is checked, whose car will the Worker drive? o If the Worker will drive his or her own car, will the member or Employer reimburse mileage? Yes No (Mileage is not covered by TennCare.) o If Yes, explain how (fixed amount per mile please specify, reimburse cost of gas, etc.) Accompanying or transporting the member must fit within the definition of the service being provided. And, it must be listed as one of the Tasks to be performed for that service. If it is, the time spent doing those things can be paid through CHOICES Consumer Direction as part of the hourly wage for that service. The cost of travel back and forth (including gas) cannot. No additional hours of service will be approved in order to accompany or transport a member. And, no additional payment will be made through CHOICES. The Employer and the Worker understand that the cost of transportation is not covered for services provided through Consumer Direction. Approval of Services Delivered through Consumer Direction The Employer will schedule, and the Worker will provide ONLY those services (including the type and amount of services) the member is approved to receive. Services the member is approved to receive are listed in the member s Plan of Care. The Employer will not ask the Worker to perform, and the Worker will not provide care that s not covered under the CHOICES program. This includes, but is not limited to: Any service the member is not approved to receive; More of any service than a member is approved to receive; Any service provided after the member s TennCare ends, or after the member is no longer in Consumer Direction or the CHOICES program. Care or household tasks (including washing dishes or laundry, fixing meals, or shopping) for anyone other than the member, even if they live in the same household; Yard work; or Care of non-service related pets and animals. This includes feeding, walking, bathing, or cleaning up after pets. The Employer agrees to tell the Worker right away if the member is no longer in Consumer Direction or the CHOICES program. The Employer agrees to pay the Worker for any care he asks the Worker to give that s not covered under the CHOICES program. Payment through CHOICES will not be made for services not approved in the member s Plan of Care. This includes the kind of service, amount of service, and the schedule at which care is to be provided. Member/Representative Initials for changes / / Date Worker Initial for changes / / Date 3
46
47 Schedule of Services Services must be given as described in the member s plan of care, including the schedule at which care is needed. Care should be given at the time it s needed by the member. The Employer will decide when each Worker will deliver care, based on the schedule in the member s Plan of Care. A Worker should sign this agreement ONLY if he will be able to give care at the time it s needed by the member. If the member s needs change the member needs a different kind of care or needs the care at a different time the Employer must tell the member s Care Coordinator so the plan of care can be updated. If care will be needed at a different time, the Employer should give the Worker as much advance notice as possible. The Employer must make sure the Worker will be able to give the care at the new time it s needed. If not, the Employer will have to find another Worker to give care at the time it s needed by the member. The Worker must notify the Employer as soon as possible if he will not be able to provide care as scheduled. (This includes when the Worker can t provide care at all, will be late arriving, or must leave early). This will allow the Employer to arrange back-up care so the member s needs are met. Repeated problems providing care as scheduled may affect the Worker s employment in Consumer Direction. If care is provided at a different schedule than listed in the plan of care, the Worker may not be paid for the care. The Employer and Worker must work with PPL to get the schedule change approved before the Worker can be paid. Not all schedule changes can be approved. Talk with PPL right away if the schedule needs to be changed. Recording time worked The Worker agrees to log in at the beginning and end of each service to log their time. The Worker will log into the electronic visit verification (EVV) system used by the member s MCO. If the Worker forgets to log in or out at a visit or provides care at a different time than it was scheduled, the Worker agrees to contact PPL right away. The Worker agrees to work with the Employer and PPL to resolve any problems with time that has been logged. The Worker understands that he may not be paid for services if he fails to log in or out at each visit, or provides care at a different time than it was scheduled to be given, unless the problem can be resolved. If for any reason, the electronic visit verification (EVV) system is not available, the worker agrees to record the hours worked in the manner requested by PPL. Member/Representative Initials for changes / / Date Worker Initial for changes / / Date 4
48
49 Payment for Approved Services This Agreement does not guarantee the Worker a minimum number of hours or a minimum amount of income each pay period. The Worker will be paid for services approved in the Plan of Care that is actually provided to the member. The Worker s pay will be based on the total hours of approved care provided, minus deductions for the employee s share of federal taxes. The Worker agrees to be paid on a twice-monthly schedule by direct deposit to a checking or savings account, or by paper check. The Worker understands that he will not be paid: For services not approved in the Plan of Care; For services provided at a different schedule than listed in the Plan of Care; For services not provided or time not worked; While a member is hospitalized, in a nursing facility or Community-Based Residential Alternative facility (like an Assisted Living or an Adult Care Home); or To provide care at the same time a member is receiving Adult Day Care services. The Worker cannot log or bill and will not be paid for time to travel to and from work at the member s home. Benefits The Worker will not receive insurance or other benefits under this agreement, or participate in any pension or retirement plan. The Worker understands that the Employer is not required to have Worker s compensation insurance. Additional Employer Responsibilities 1. The Employer agrees to define the Worker s job duties and develop a job description for the Worker. 2. The Employer agrees to train the Worker to deliver care based on the member s needs and preferences. 3. If the Worker will perform any self-directed health care tasks, the Employer will train the Worker on how to perform those tasks. 4. The Employer will provide a safe working environment. 5. The Employer will make sure the Worker provides only as much care as the member is approved to receive. 6. The Employer will make sure that the Worker provides care only as scheduled in the Plan of Care. 7. The Employer will make sure the Worker doesn t give more than 40 hours of care in a week for all hourly wage services combined (they can t work overtime). 8. The Employer agrees to supervise the Worker, evaluate the Worker s job performance, and address problems or concerns with the Worker s performance. This may include firing the worker, if needed. Member/Representative Initials for changes / / Date Worker Initial for changes / / Date 5
50
51 9. The Employer agrees to decide how much the Worker will be paid (from a range of rates set by the State). 10. The Employer agrees to review the time the Worker reports to be sure it s right. 11. The Employer agrees to ensure the Worker is keeping good notes in the home about the care the Worker provides. 12. The Employer agrees to develop a back-up plan to address times that a scheduled Worker doesn t show up (the member can t decide to just go without services), and to activate the back-up plan when needed. 13. The Employer agrees to report any suspected abuse, neglect or exploitation to Adult Protective Services. 14. The Employer agrees to notify the member s Care Coordinator of any significant changes in the member s condition or needs. This includes (but is not limited to) any time the member is admitted to a hospital or nursing home, or stops receiving care (even temporarily) for any reason. 15. The Employer agrees to report all critical incidents to the member s Care Coordinator in a timely manner and to cooperate with all investigations. 16. The Employer agrees to inform PPL of any changes in mailing address or phone number. Employer Responsibility for Hiring Decisions The Employer can choose to hire a Worker who fails the background check through the exception process listed in TennCare rules. The Employer understands that this decision and any consequences that may result are the Employer s sole responsibility. In making any and all hiring decisions, the Employer agrees to hold harmless, release, and forever discharge the State of Tennessee, the Bureau of TennCare, the member s MCO, PPL and any and all of their employees and agents from any claims and/or damages that may arise. Worker Qualifications By signing this Agreement, the Worker attests that he meets minimum qualifications to be a Worker in the CHOICES Consumer Direction program. The Worker: Is 18 years of age or older. Is not the member s Representative for Consumer Direction. Is not the member s spouse, legal guardian or Power of Attorney. Is able to perform all of the services (including tasks) needed by the member. Is able to provide care at the schedule needed by the member. Has basic reading and writing skills. Has a valid Social Security number and is authorized to work in the United States. Has passed a criminal record check or been granted an exception and doesn t appear on the abuse and sexual offender registries. Has completed all required training. Has completed all required paperwork to provide care through Consumer Direction. Has signed a Medicaid Agreement for a Medicaid Provider ID number. Has provided a valid driver s license and proof of insurance (if transporting the member). Member/Representative Initials for changes / / Date Worker Initial for changes / / Date 6
52
53 Additional Worker Responsibilities The Worker understands that he or she works for the Employer, and not for PPL, the member s MCO, or the State of Tennessee. 1. The Worker agrees to provide all of the services listed in this agreement. 2. The Worker agrees to perform all of the tasks needed by the member that are part of that service. 3. The Worker agrees to give the care when it s needed by the member, at the schedule set in the Plan of Care. If the worker provides care outside of the plan of care and the schedule change is not approved by the care coordinator, the Worker understands that he or she may not be paid for that care that was provided at a different time. 4. The Worker understands that if the schedule change is approved after the care has been provided, payment for those services may be delayed. 5. The Worker will not provide care that s not approved by the member s MCO or not covered by TennCare. 6. The Worker may refuse to provide care or perform a task that: Might be adverse to the member s health. The Worker believes poses a danger to his/her own health. The Worker believes they have not been adequately trained to perform. Is not part of this Agreement. 7. Unless the Worker is providing Companion Care, the Worker will not provide more than 40 hours of care per week to the member. No hourly wage Worker will be approved to work overtime in the CHOICES Consumer Direction program. 8. The Worker agrees to be on time, and neatly and appropriately dressed. 9. If the Worker is sick or has an emergency and cannot provide care as scheduled, he or she agrees to tell the Employer right away so that back-up care can be arranged. 10. The Worker agrees to participate in any and all training that s required, and all training requested by the Employer. 11. The Worker agrees to provide safe care as directed by the Employer. 12. The Worker agrees to use Universal Precautions. 13. The Worker agrees to call 911 if there s an emergency. 14. The Worker agrees to report any suspected abuse, neglect or exploitation to Adult Protective Services. 15. The Worker agrees to notify the member s Care Coordinator of any significant changes in the member s condition or needs. This includes (but is not limited to) any time the member is admitted to a hospital or nursing home, or stops receiving care (even temporarily) for any reason. 16. The Worker agrees to report all critical incidents to the member s Care Coordinator in a immediately and to cooperate with all investigations. 17. The Worker agrees to inform PPL of any changes in mailing address or phone number. 18. The Worker agrees to treat the member with dignity and respect. This includes respecting the member s beliefs, choices, culture, religion, privacy, and personal property, and behaving respectfully toward the member s family, friends and guests. 19. The Worker agrees to communicate effectively with the member. If the member has a preferred communication method or device, it should be respected and utilized. Member/Representative Initials for changes / / Date Worker Initial for changes / / Date 7
54
55 20. The Worker agrees to keep good notes about the services delivered and the tasks performed for each service. This includes all medicine that s given to the member (if the member or his representative is self-directing health care tasks). Notes about service delivery will be kept in the member s home. This is in addition to information that may be logged into the electronic visit verification (EVV) system. 21. The Worker agrees to keep all information about the member and his or her family private. This includes information about the member s needs and the care provided by the Worker for the member. 22. The Worker agrees to have the employee s share of required federal taxes withheld from his or her wages. This includes Social Security, Medicare, and Federal income taxes. 23. The Worker agrees to cooperate with the Employer and with PPL in providing information needed to comply with all labor and tax laws and regulations. 24. The Worker understands that he or she cannot use member s property unless the member and his/her Representative say it s OK. This should only be when it s part of giving the member s care. This includes the member s telephone. 25. The Worker agrees to not make or accept personal phone calls, or send or receive text messages or s while providing care through Consumer Direction. Conditions of Agreement The Employer and the Worker agree to use the help provided by PPL for CHOICES members in Consumer Direction. This includes (but is not limited to) paying Workers, and filing Employer payroll taxes and forms. It also includes having a Supports Broker. Complying with State and Federal Laws The Employer and the Worker agree to follow all of TennCare s rules for Consumer Direction in the CHOICES program. The Employer and the Worker agree to comply with all State and Federal laws, including labor and tax laws. The Employer and the Worker understand that: State and Federal Medicaid funds will be used to pay for services delivered by the Worker through Consumer Direction. Billing for care that wasn t given (or billing for more care than was given) is against the law. A person who knows the care wasn t given and allows the bill to be paid is also responsible. Any intentional act or failure to act that results in payment of State or Federal funds that should not have been paid is an act of fraud under the State s TennCare program and title XIX of the federal Social Security Act. Fraudulent acts include, but are not limited to misrepresenting the time that s worked, the services performed, or the person giving the care. Under the Tennessee Medicaid False Claims Act, any person that causes a claim for payment to be submitted under the TennCare program that s false or fraudulent is subject to Federal and State civil and criminal penalties. A member, representative or Worker who fails to follow all State and Federal rules cannot be part of Consumer Direction in the CHOICES program. Member/Representative Initials for changes / / Date Worker Initial for changes / / Date 8
56
57 Duration of Agreement This agreement is effective when it s signed by both parties. The agreement will be in effect until either party informs the other party that they want to end the agreement. Notice may be provided verbally or in writing. Whenever possible, notice should be given at least two (2) weeks before the agreement will end. The Employer may not give two (2) weeks notice if there are serious problems with the care provided. This agreement will also end immediately if the member loses TennCare, or is no longer in Consumer Direction or the CHOICES program. Changing the Agreement This agreement can be changed only by agreement of both parties. Any changes to this Agreement must be made in writing. Both parties must sign the revised Agreement to show that they agree to any changes that are made. A copy of the revised agreement must be given to PPL after it is signed by both parties. Holding Others Harmless (Indemnification) The parties agree to hold harmless, release, and forever discharge the State of Tennessee, the Bureau of TennCare, the member s MCO, PPL and any and all of their employees and agents from any claims and/or damages that may arise out of any decision, act or omission by the member, Employer or Worker. By signing below, both parties affirm that they understand and agree with this information, and promise to abide by this agreement, carry out all of their responsibilities, and follow the rules for CHOICES Consumer Direction. Employer Signs Here Worker Signs Here / / Date / / Date Member/Representative Initials for changes / / Date Worker Initial for changes / / Date 9
58
59 Application for Tax Exemptions Based on Age, Student Status, and Family Relationship State Worked: Program: Participant Name: Employer Name: Employee Name: Employee Date of Birth: / / Employees providing domestic services, such as personal assistance, may be exempt from paying certain federal and state taxes based on the employee s age, student status, or family relationship to the employer. In some cases, the employer may also be exempt based on the employee s status. If you and your employer qualify for these exemptions you must take them. PCG Public Partnerships will determine the tax exemptions that apply to you and to your employer (see enclosed guidelines). Employee Please answer all the following questions based on your age, student status, and relationship to the employer: 1. Are you a non-resident alien temporarily in the United States on an F-1, J-1, M-1, or Q-1 visa admitted to the US for the purpose of providing domestic services? Yes, that description fits my status. No, that description does not fit my status. 2. Are you the child of the employer (includes adopted children)? Yes, my employer is my parent (mother or father). No, my employer is not my parent. 3. Are you the spouse of the employer? Yes, my employer is my spouse (husband, wife). No, my employer is not my spouse. 4. Are you the parent of the employer (includes adopted children)? Yes, my employer is my child (son or daughter). No, my employer is not my child. 5. If you answered Yes to Question 4, check any of the following that apply. If you answered No, proceed to Question 6. Yes, I also provide care for my grandchild or step-grandchild in my child s home. Yes, my grandchild or step-grandchild is under age 18, or has a physical or mental condition that requires personal care of an adult for at least four continuous weeks during the calendar quarter in which services are performed. Yes, my child (son or daughter) is widowed or divorced and not remarried, or living with a spouse who has a mental or physical condition which prohibits the spouse from caring for my grandchild for at least four continuous weeks during the calendar quarter in which services are performed. 6. Are you under the age of 18 or do you turn 18 this calendar year? Yes, I am under 18 or am turning 18 this calendar year. No, I am over 18. If you answered Yes to Question 6, answer the following question. If you answered No, skip this section. Is the job of performing household services (personal assistance) your principal occupation? Note: Do not answer Yes if you are a student. Yes, performing household services is my principal occupation. No, performing household services is not my principle occupation, or I am a student. IMPORTANT: You must notify PCG Public Partnerships if your status changes. Employee Signature: Date: / / Submit to: Revised: 6/1/12 Form TE 20 PCG Public Partnerships, LLC Financial Administrator One Cabot RD, 5STE 102 Medford, MA 0215
60
61 Guide to Tax Exemptions Based on Age, Student Status, and Family Relationship Employee Copy Keep for your records Employees providing domestic services such as personal assistance may be exempt from paying certain federal and state taxes based on the employee s age, student status or family relationship to the employer. In some cases, the employer may also be exempt from paying certain taxes based on the employee s status. IMPORTANT: Please see IRS Publication: #926 Household Employer s Tax Guide, and IRS website article: Foreign Student Liability for Social Security and Medicare Taxes for additional information. IMPORTANT: These exemptions are not optional. If the employee and employer qualify for these tax exemptions they must be taken. If the employee s earnings are exempt from these taxes, the employee may not qualify for the related benefits, such as retirement benefits and unemployment compensation. The questions regarding family relationship refer to the relationship between the employee and the employer of record (common law employer). In some cases, the program participant is the employer of record. In other cases, the employer of record may be someone other than the program participant. Check program rules. Program rules may prohibit some types of employees. For example, most Medicaid-funded programs do not permit a spouse to be paid as an employee for providing services to a spouse. Check program rules. PCG Public Partnerships will determine the tax exemptions that apply to the employee and employer based on the information provided by the employee. PCG Public Partnerships cannot provide tax advice. Tax Exemptions for Non-Resident Students For a non-resident student in the United States on an F-1, J-1, M-1, or Q-1 visa admitted to the US for the purpose of providing domestic services, the employer and employee are exempt from paying FICA (Social Security and Medicare taxes) and the employer is exempt from paying FUTA (Federal Unemployment Tax) on wages paid to this employee. The employer may also be exempt from paying State Unemployment Insurance, depending on the rules in the state. Tax Exemptions for Children Employed by Parent For a child under 21 employed by his or her parent, the employer and employee are exempt from paying FICA (Social Security and Medicare taxes) and the employer is exempt from paying FUTA (Federal Unemployment Tax) on wages paid to this employee until the child (employee) turns 21 years of age. The employer may also be exempt from paying State Unemployment Insurance, depending on the rules in the state. Tax Exemptions for Spouses Employed Spouses For a spouse (husband, wife, or domestic partner in some states) employed by his or her spouse, the employer and employee are exempt from paying FICA (Social Security and Medicare taxes) and the employer is exempt from paying FUTA (Federal Unemployment Tax) on wages paid to this employee. The employer may also be exempt from paying State Unemployment Insurance, depending on the rules in the state. Revised: 6/1/12 Form TE 20 PCG Public Partnerships, LLC Financial Administrator One Cabot RD, 5STE 102 Medford, MA 0215
 and the employer is exempt from paying FUTA (Federal Unemployment Tax) on wages paid to")
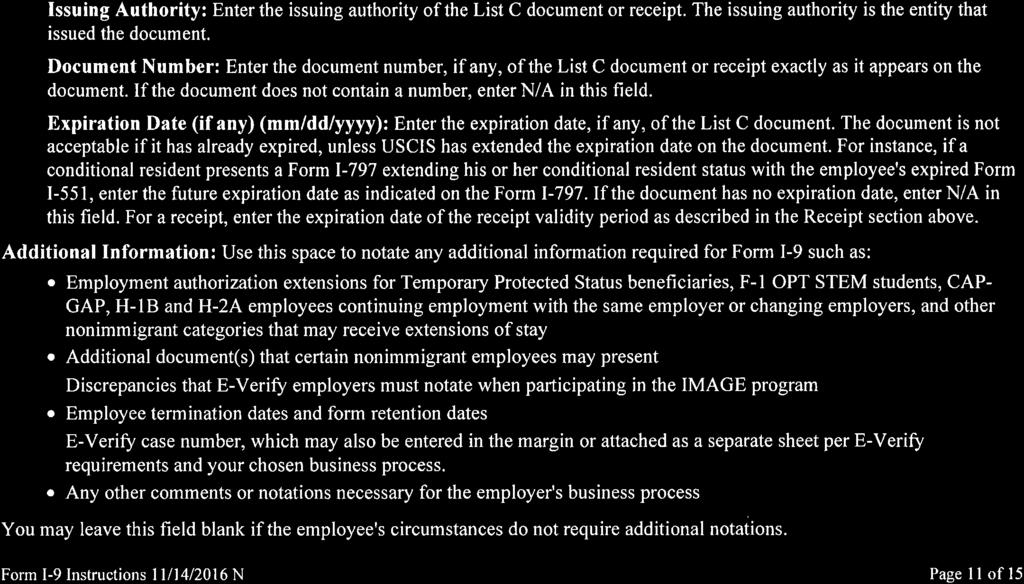
62 Tax Exemptions for Parents Employed by Children For a parent employed by his or her child and answering No to any of the additional questions under Question #6 regarding caring for a grandchild or step grandchild, the employer and employee are exempt from paying FICA (Social Security and Medicare taxes) and the employer is exempt from paying FUTA (Federal Unemployment Tax) on wages paid to this employee. The employer may also be exempt from paying State Unemployment Insurance, depending on the rules in the state. For a parent employed by his or her child and answering Yes to all of the additional questions regarding caring for a grandchild or step grandchild, the employer is exempt from paying Federal Unemployment Tax (FUTA) on wages paid to this employee. The employer may also be exempt from paying State Unemployment Insurance, depending on the rules in the state. Tax Exemptions for Employee under Age 18 For employees under the age of 18 or turning 18 in the calendar year: If the employee is a student, domestic services are deemed not to be the employee s principle occupation and the employer and employee are exempt from paying FICA (Social Security and Medicare taxes). Employment Relationship Status Foreign Student on VISA in US for Purpose of Providing Domestic Service Child Employed by Parent Federal Insurance Contributions Act - Social Security and Medicare Taxes Federal Unemployment Tax Act State Unemployment Insurance (FICA) (FUTA) (SUI) FICA exempt FUTA exempt See footnote (1) FICA exempt only until 21 st birthday FUTA exempt only until 21 st birthday See footnote (2) Spouse Employed by Spouse FICA exempt FUTA exempt SUI exempt (3) Parent Employed by Child Employee Under 18 or Turning Age 18 in Calendar Year FICA exempt only if not also caring for dependent child of the employer (employee s grandchild) FICA exempt through year of 18 th birthday only if enrolled as a fulltime student FUTA exempt Not Applicable SUI exempt except in NY and WA. See footnote (4) Not Applicable (1) Foreign student in the United States on F-1/J-1 VISA is exempt from SUI in the following states: PA, WA. (2) Child under 18 employed by parent is SUI exempt in the following states: CA, IL, MA, ME, NJ, NV, OH, OR, PA, SC, TN, WA, WV. Child under 21 employed by parent is SUI exempt in the following states: AZ, GA, IN, KS, NY, OK, VA, WY, and District of Columbia. (3) For California only, a registered domestic partner employed by his/her registered domestic partner is SUI exempt. (4) Parent employed by child is SUI exempt in all states and the District of Columbia with the exception of NY and WA. Revised: 6/1/12 Form TE 20 PCG Public Partnerships, LLC Financial Administrator One Cabot RD, 5STE 102 Medford, MA 0215
63 CONSUMER DIRECTION FRAUD FORM Employee A member in the CHOICES Consumer Direction Program has selected you to provide caregiver services. Before you begin, it is important that you understand there are certain things you are not allowed to do as a caregiver in CHOICES Consumer Direction, and that if you knowingly do those things you could be charged with TennCare fraud. Please read this form carefully, sign at the bottom, and send this form back to PPL with your other employment paperwork. If you have any questions about the information in this form, contact PPL at Providing Care In CHOICES Consumer Direction There are certain circumstances under which you are not allowed to be paid for care you provide in Consumer Direction. CHOICES only pays for care to meet needs that can t be met by family members or others who help the member. CHOICES does not pay you to provide care that you would have given for free. You can t provide care to a member receiving Consumer Direction if you are their spouse, Representative for Consumer Direction, legal guardian, or Power of Attorney. You can t provide Personal Care Visits, Attendant Care, or In-Home Respite Care if you live with the member. You can t provide Companion Care (Only available to members who are enrolled in CHOICES Group 2) for: An immediate family member (spouse, parent, grandparent, child, grandchild, sibling, mother-in-law, father-in-law, sister-in-law, brother-in-law, daughter-in-law, or son-in-law including adopted or step family members) Anyone you live with (or that you have lived within the last 5 years) Service Agreement: You must sign a Service Agreement with the CHOICES member and/or their Representative. It s like a contract that sets out what each of you agree to do. The Service Agreement must include: The services you will provide, The rate you will be paid, and Any self-directed health care tasks you will perform while giving care to the member. The services listed in the Service Agreement must be provided to the CHOICES member only; workers cannot provide services to the CHOICES member s family or friends. AND, workers cannot be paid for services 1 P a g e
64
65 provided while the member is in the hospital, a Nursing Facility, or at a doctor s appointment accompanied by unpaid support. What is TennCare Fraud or Abuse? The Tennessee Office of Inspector General (OIG) or the Tennessee Bureau of Investigation Medicaid Fraud Control Unit (MFCU) may investigate suspected fraud and abuse of the TennCare program, including CHOICES Consumer Direction. Fraud is an intentional deception or misrepresentation made by a person with the knowledge that the deception could result in some unauthorized benefit to himself or some other person. It includes any act that that constitutes fraud under applicable Federal or State law (see 42 CFR 455.2). Abuse is provider practices that are inconsistent with sound fiscal, business, or medical practices, and result in an unnecessary cost to the Medicaid program, or in reimbursement for services that are not medically necessary or that fail to meet professional recognized standards for health care. It also includes recipient practices that result in unnecessary cost to the Medicaid program (see 42 CFR 455.2). Fraud includes knowingly being paid for care that you did not or are not allowed to provide. It also includes, but is not limited to, the following: Misrepresenting the hours you work/falsifying time sheets Using someone else s identity to work Helping someone else commit fraud If a member or employer asks you to do something and you re not sure if you are allowed to do it, contact PPL at If you believe the member/employer is knowingly committing TennCare fraud, you can also contact the OIG via hotline ( ) or report fraud online at By agreeing to participate in Consumer Direction, you acknowledge that you have received the following information: You cannot provide hourly services to a CHOICES member who lives with you. You cannot provide companion care to a CHOICES member if you are an immediate family member (spouse, parent, grandparent, child, grandchild, sibling, mother-in-law, father-in-law, sister-in-law, brother-in-law, daughter-in-law, or son-in-law including adopted or step family members), or if you have lived with them during the last five years. You cannot perform services for family or other household members of the CHOICES member. You cannot perform services while the CHOICES member is in the hospital, nursing facility, or at a doctor s appointment accompanied by unpaid support. You cannot report that you have worked hours that you did not work for the CHOICES member. You cannot use someone else s identity to work for a CHOICES member. You cannot help someone else commit fraud by making false statements (written or verbal) for them, or falsifying documents. Does the worker currently live with the member? YES NO Have you lived with the member in the last 5 years? (for companion care workers only) YES NO N/A 2 P a g e
66
67 Are you related to OR legal guardian of the member? YES NO Adopted, In-laws and step family members are included. If yes, what is your relationship? Parent Child Sibling Grandparent Aunt/Uncle Cousin Legally Appointed Guardian Spouse Grandchild Niece/Nephew Violation in any of these areas is considered fraud and could lead to an investigation by the Office of Inspector General (OIG) or the Tennessee Bureau of Investigation Medicaid Fraud Control Unit (MFCU) and potentially criminal charges. I acknowledge that I have read and understand the information provided in this form: Worker Signature Witness Signature / / Date / / Date 3 P a g e
68
69 Forms to Keep The following forms are documents you should keep. They provide important information about the pay schedule, PPL Customer Service, and required certifications and trainings. 1. Payroll Schedule (1 page) Use this to track when you will be paid. 2. PPL Customer Service (1 page) This form provides you with information about our customer service center and complaint system. 3. Worker Training and Certification Requirements (3 pages) This document lists all of the training and certifications you will need to be a provider in this program. 4. Required Worker Training (1 page) This document provides information on the Consumer Direction in the CHOICES Program Worker Training. 5. Consumer Direction in the CHOICES Program Worker Training Presentation (14 pages) This document contains the PowerPoint slides presented during the Worker Training. You will want to have these during the presentation. 6. Choices Worker Training Checklist for Consumer Direction (2 pages) This checklist includes all of the sections that will be covered during the Worker Training Presentation. Please fax or mail to PPL upon completion: FAX: MAIL: PPL Nashville 414 Union ST, Ste 1100 Nashville, TN NEED HELP? CALL TOLL FREE AT Forms To Keep: Page 1 of 1
70
71 Customer Service: TN TennCare - UHC Timesheet Fax: Payment Schedule choices.achoice@pcgus.com Public Partnerships, LLC One Cabot Road, Suite 102 Medford, MA ALL TIMESHEETS DUE BY 4PM CST (5PM EASTERN TIME) Pay Period Starts: December 3, 2017 December 16, 2017 December 17, 2017 December 18, 2017 January 2, 2018 December 17, 2017 December 30, 2017 December 31, 2017 January 1, 2018 January 16, 2018 December 31, 2017 January 13, 2018 January 14, 2018 January 15, 2018 January 14, 2018 January 28, 2018 February 11, 2018 February 25, 2018 March 11, 2018 March 25, 2018 April 8, 2018 April 22, 2018 May 6, 2018 May 20, 2018 June 3, 2018 June 17, 2018 July 1, 2018 July 15, 2018 July 29, 2018 August 12, 2018 August 26, 2018 September 9, 2018 Pay Period Ends: January 27, 2018 January 28, 2018 January 29, 2018 February 12, 2018 February 10, 2018 February 24, 2018 February 25, 2018 February 26, 2018 March 12, 2018 March 10, 2018 March 11, 2018 March 12, 2018 March 26, 2018 March 24, 2018 March 25, 2018 March 26, 2018 April 9, 2018 April 7, 2018 July 14, 2018 July 28, 2018 August 11, 2018 August 25, 2018 September 8, 2018 September 22, 2018 February 11, 2018 April 8, 2018 July 15, 2018 July 29, 2018 August 12, 2018 August 26, 2018 September 9, 2018 September 23, 2018 April 9, 2018 April 23, 2018 April 21, 2018 April 22, 2018 April 23, 2018 May 7, 2018 May 5, 2018 May 6, 2018 May 7, 2018 May 21, 2018 May 19, 2018 May 20, 2018 May 21, 2018 June 4, 2018 June 2, 2018 June 3, 2018 June 16, 2018 June 17, 2018 June 18, 2018 July 2, 2018 June 30, 2018 Faxed/Mailed Timesheets Due*: July 1, 2018 Electronic Timesheets Due: June 4, 2018 July 2, 2018 July 16, 2018 July 30, 2018 August 13, 2018 August 27, 2018 September 10, 2018 September 24, 2018 Checks/EFT Sent**: January 29, 2018 February 12, 2018 February 26, 2018 June 18, 2018 July 16, 2018 July 30, 2018 August 13, 2018 August 27, 2018 September 10, 2018 September 24, 2018 October 9, 2018 September 23, 2018 October 6, 2018 October 7, 2018 October 8, 2018 October 22, 2018 October 7, 2018 October 20, 2018 October 21, 2018 October 22, 2018 November 5, 2018 October 21, 2018 November 3, 2018 November 4, 2018 November 5, 2018 November 19, 2018 November 4, 2018 November 17, 2018 November 18, 2018 November 19, 2018 December 3, 2018 November 18, 2018 December 1, 2018 December 2, 2018 December 3, 2018 December 17, 2018 December 2, 2018 December 15, 2018 December 16, 2018 December 17, 2018 December 31, 2018 December 16, 2018 December 29, 2018 December 30, 2018 December 31, 2018 January 14, 2019 December 30, 2018 January 12, 2019 January 13, 2019 January 14, 2019 January 28, 2019 *Faxed or mailed paper timesheets are due one day earlier than electronic timesheets to allow for the manual processing required by paper timesheet submission. **Please note that the date the "Checks/EFT Sent" column shows the date the checks will be postmarked or sent to our bank. This is not the date that workers will receive their checks.
72 Public Partnerships, LLC Fiscal/Employer Agent One Cabot RD, Ste 102 Medford, MA Toll Free Numbers Phone: TTY: Administrative Fax: PPL CUSTOMER SERVICE PPL has a Customer Service Center. This is for consumers, employees and Support Brokers. The Customer Service Center can be reached by calling toll-free at Dedicated Customer Service Specialists will answer this number. The Customer Service Center is open between 9:00AM and 5:00 PM EST, Monday through Friday. PPL has a separate phone line ( ) that connects callers to our TTY system. This is for people with hearing and/or speech impairments who use text telephones. We also have a tollfree fax number ( ) and project specific address (choices.achoice@pcgus.com). Our Customer Service Center telephone system has voice mail. This is used as a back up during business hours. It is also used on nights, weekends and holidays. PPL will return any calls left on voice mail during business hours within one business day of the message. PPL s Customer Service Center has experienced Customer Service Specialists. They are trained to communicate with a diverse group of people. Over half of our Customer Service Specialists speak both Spanish and English. We also have access to translation services through our Language Line. This is used to help people who speak other languages. PPL does not charge callers for translation services. PPL enters all calls received, including complaints, into our computer system. We identify the consumer, the complaint and the date it was made. We also track how we addressed the issue, and date it was resolved. Please call us at if you have any questions. TTY users please dial We look forward to serving you. Customer Service: Page 1 of 1

73 Public Partnerships, LLC Fiscal/Employer Agent One Cabot RD, Ste 102 Medford, MA Toll Free Numbers Phone: TTY: Administrative Fax: WORKER TRAINING AND CERTIFICATION REQUIREMENTS Before you can start providing services to a member in the CHOICES Consumer Direction Program, you must provide PPL with proof that you have completed the required training and have the required certifications. PPL staff or the member s support broker will provide most of the training to you. You must complete all training. You are not paid for training. REQUIRED TRAINING Overview of the CHOICES program and consumer direction of HCBS; Standard caring for elderly and disabled populations; Abuse and neglect identification and reporting; Fraud and abuse prevention and reporting; Critical incident reporting; Use of timesheets for recording time worked and submitting to employer for approval; and Blood borne pathogens Some workers will also receive training from their employers on the administration of specific health care tasks. REQUIRED CERTIFICATIONS You are required to have CPR and First Aid Certification. The certifications must be from the American Red Cross, the American Heart Association, First Responder or the National Safety Council. Other vendors are not approved. Workers must pay for the cost of these certifications. American Red Cross, First Responder or National Safety Council: If we get one of these cards, we must have: Both sides of the card Course title must include the words CPR or AED Holder signature CPR Certification: We can accept: OR American Heart Association: If we get this card, we must have: All sides of the card, including the modules Completed (not filled in) modules must include the words CPR or AED Holder signature Online CPR certification is acceptable but only under these conditions: The course must be from one of the approved agencies listed above that offers online knowledge courses and in person skills demonstrations test. (Card requirements remain the same) Only the knowledge portion of the course may be taken online. WORKER TRAINING AND CERTIFICATION REQUIREMENTS: Page 1 of 3
74 The skills demonstration must be completed in person with a certified instructor who will issue a certification card If a worker has completed a CPR course but does not yet have a card, PPL can accept an original signed letter on the association s letterhead from the instructor of the course detailing the name of the individual being certified and the expiration date of certification for 45 days only. PPL will enter the certification s expiration date as 45 days from the date of the training. The worker must submit the actual card reflecting FA/CPR course completion within the 45 day window to maintain compliance avoid potential pay issues. The worker must renew all certifications prior to expiration date and submit proof of recertification to maintain compliance and avoid potential pay issues. American Red Cross, First Responder or National Safety Council: If we get one of these cards, we must have: Both sides of the card Course title must include the words first aid Holder signature First Aid Certification: We can accept: OR American Heart OR Current medical license for Association: Registered Nurse (RN), Licensed If we get this card, we Practical Nurse (LPN), Certified must have: Nurse Assistant/Aide (CNA) or All sides of the Certified Nurse Technician card, including (CNT): the modules Photocopy of the license Completed (not including an expiration date filled in) modules or: must include the Print out of the provider s licensure words first aid records from Holder signature ex.htm Online First Aid certification is acceptable but only under these conditions: The course must be from one of the approved agencies listed above that offers online knowledge courses and in person skills demonstrations test.(card requirements remain the same.) Only the knowledge portion of the course may be taken online The skills demonstration must be completed in person with a certified instructor who will issue a certification card If a worker has completed a first aid course but does not yet have a card, PPL can accept an original signed letter on the association s letterhead from the instructor of the course detailing the name of the individual being certified and the expiration date of certification for 45 days only. PPL will enter the certification s expiration date as 45 days from the date of the training. The worker must submit the actual card reflecting FA/CPR course completion within the 45 day window to maintain compliance avoid potential pay issues. The worker must renew all certifications prior to expiration date and submit proof of recertification to maintain compliance and avoid potential pay issues. WORKER TRAINING AND CERTIFICATION REQUIREMENTS: Page 2 of 3
75 BACKGROUND AND REGISTRY CHECKS PPL will process a number of registry checks on you. If there is a match on your name, date of birth and, if applicable, SSN, you will not be able to participate in this program. Tennessee Sexual Offender Registry National Sexual Offender Registry Tennessee Felony Offender Registry Tennessee Health Abuse Registry OIG List of Excluded Individuals/Entities Please note that PPL will be checking the OIG List of Excluded Individuals/Entities on a monthly basis. Should we ascertain that you have been added to the list and have continued to provide services to a CHOICES member, we will immediately report you to the Tennessee Bureau of Investigation and the Office of the Inspector General. PPL will also invoice you for any services provided since the last clean run of the OIG List of Excluded Individuals/Entities. PPL will also perform a criminal background check on you. If the background report notes that records were found, you will be notified of the findings and provided a copy of the background results. You will be given 10 days to dispute the results. If you are not able to prove that the results were erroneous within 10 business days, you may be deemed ineligible for employment. The following findings shall disqualify a person from serving as a Worker: 1. Identification on the abuse registry; 2. Identification on the State or national sexual offender registry; 3. Identification that the person has been excluded from participation in Medicare, Medicaid, SCHIP, or any Federal health care programs (as defined in Section 128B(f) of the Social Security Act; 4. Failure to have a required license; and/or 5. Refusal to cooperate with a background check; Exceptions to criminal background disqualifications may be granted at the member's discretion if the background check results are not part of the above mentioned disqualifications. If you fail the background check, you can ask the member to still consider hiring you. The member can decide not to hire you or can approve an exception. Should the Member decide to grant the criminal history exception and hire you, PPL shall notify the Member s MCO and collaborate with that MCO to amend the Member s Risk Agreement to reflect that the Member voluntarily chooses to take on the risk associated with hiring an individual with a criminal history and is solely responsible for any negative consequences stemming from that decision. WORKER TRAINING AND CERTIFICATION REQUIREMENTS: Page 3 of 3
76 REQUIRED WORKER TRAINING Every worker in the CHOICES Consumer Direction Program must complete the required training in order to provide services in this program. This employee packet contains a copy of : Consumer Direction in the Choices Program worker training presentation; and a copy of the Choices Worker Training Checklist for Consumer Direction. You can use the copy of the presentation to follow along during training. After the training is finished, you must fill in the checklist and send it to PPL or give it to the Supports Broker. Training is offered twice each week over the phone. Please pick the best day and time that works for you and plan to call in. It is a toll-free number. TRAINING SESSIONS Training Session 1 Every Tuesday, 9am-10am CST Phone # Participant Code: # Training Session 2 Every Thursday, 5pm-6pm CST Phone # Participant Code: # What to do: 1. Pick a training session. 2. Call the toll free number for that day/time and enter the Participant Code. 3. Stay on the call until training is complete and end of session roll call is finished. (Roll will be taken at the beginning and end of each session). 4. If you are sending the checklist to PPL you can mail or fax it in. Mailing address: FAX Number: Public Partnerships, LLC Attn. Megan Bass 414 Union ST Ste 1100 Nashville, TN Required Working Training: Page 1 of 1
 Role - Financial")
77 Title Consumer Direction in the CHOICES Program Comprehensive Training on CHOICES, Consumer Direction, Financial Administration, and Supports Brokerage Page 1 Title AGENDA CHOICES Overview Consumer Direction Care Coordinator Role & Responsibilities in Consumer Direction Supports Broker Role & Responsibilities Member Role & Responsibilities Public Partnerships, LLC (PPL) Role - Financial Management Services Supporting Older Adults and People who have Disabilities Self-Direction of Health Care Tasks Universal Precautions and Blood Borne Pathogens Reporting Requirements Creating an Account on BetterOnline Completing a Timesheet using BetterOnline, Time4Care, or paper timesheets Questions and Answers Page 2 Version 2-6/3/2016 1

78 Title Overview of CHOICES Definition TennCare CHOICES in LTSS (or CHOICES for short) is TennCare s program for adults (age 21 and older) with a physical disability and seniors (age 65 and older). LTSS offer help doing everyday activities that you may no longer be able to do for yourself as you grow older, or if you have a physical disability, LTSS can assist you with things like bathing, dressing, getting around your home, preparing meals, or doing household chores. LTSS include care in a nursing home, as well as certain services to help a person remain at home or in the community. These are called Home and Community Based Services or HCBS. See more at: History TennCare CHOICES in LTSS services carved out of Managed Care Nursing Facilities Intermediate Care Facilities for persons with intellectual disabilities Home and Community Based Services (HCBS) The Long-Term Care Community Choices Act 2008 Managed Care Organizations now Incentives and focus on prevention and good health Page 3 Title Consumer Direction in CHOICES Consumer Direction (CD) option What it means to direct one s own care Consumer Directed services Personal Care Attendant Services In-home Respite Companion Care Self-direction of Health Care Tasks Provided per the Participant/Member instruction and POC/Service Agreement Page 4 Version 2-6/3/2016 2
79 Title Care Coordinator Role in Consumer Direction Conducts comprehensive Needs Assessment Educates the Member on CHOICES program, including the Consumer Direction option Works with Member and Care Coordination team to develop Plan of Care, which coordinates all aspects of Member s care and determines services Completes Risk Assessment and Risk Agreement Ensures Consumer Direction Back-Up Plan is adequate to meet the Member s needs Authorizes services established in Plan of Care Monitors service provision for quality and appropriateness Receives and reviews all reports submitted by FEA and Supports Broker Maintains monthly phone contact and completes face to face home visits with the members as required by TennCare Page 5 Title Care Coordinator Role in Consumer Direction Additional Roles: Assists the Member/Representative in: Understanding & monitoring individual services Monitoring & evaluating the worker s performance Responding to the member's needs and preferences over time, including: Making changes to Back-up Plan, if needed Making changes to POC based on assessed needs and the person s goals and preferences Assisting the member with identifying a Consumer Direction Representative, if needed, to assist with enrollment and responsibilities of being in the program, and complete the necessary paperwork to appoint a CD Representative with member Page 6 Version 2-6/3/2016 3
80 Title Support Broker Role Provides Training and Support to Members/Representatives in: Understanding CHOICES and Consumer-Direction Fulfilling the responsibilities of being an employer of consumer direction workers Recruiting consumer direction workers Scheduling, training & supervising consumer direction workers Creation of the Initial Consumer Direction Back-Up Plan Fraud and abuse prevention, identification and reporting Abuse and neglect prevention and reporting Page 7 Title Member Role - Being An Employer Hiring Workers Screen, interview and hire Consumer Directed worker(s) Give worker employment packet and instructions for completing Develop job description for worker Employer Responsibilities Train, schedule and supervise worker(s); Evaluate worker s performance Make sure worker(s) keep good, daily notes for each shift on the Activities and Communication Log sheets Monitor schedule and flexibility of hours while ensuring worker does not work over 40 hours per week Review for accuracy and Approve the timesheets for their employee(s) Fire/Hire worker(s) if necessary Self-Direction of Health Care Tasks Train worker(s) to assist with self-directed health care tasks as per member s needs and POC Page 8 Version 2-6/3/2016 4

81 Title Member Role Consumer Direction paperwork Develop the Initial Back-Up Plan with the Support Broker Implement Back-Up Plan when necessary Protection Report to Care Coordinator any fraud, mistreatment, neglect or injury that occurs Contact Care Coordinator with any concerns regarding worker or his/her ability to provide services Page 9 Title PPL s Role - Financial Management Services Support Brokerage Receives referrals from MCOs; assigns support broker for enrollment assistance and training on CD program Processes all employment (hiring) packets, including processing criminal background checks on all workers National, state, and registry checks Track receipt of all workers First Aid and CPR certifications All Workers have to be FA/CPR certified through American Red Cross, American Heart Association, First Responder, National Safety Council; must stay current on certifications No online classes Rosters are not acceptable; need copy of signed card Letter from instructor acceptable for 45 days from date of the class Must not let FA/CPR expire; cannot work if FA/CPR expire Pays workers on behalf of CHOICES Consumer Direction participants Based on approved timesheets from employer and available authorizations from MCO Withholds and deposits taxes, and files tax and labor reports on behalf of CHOICES Consumer-Direction participants Provides the Members/Representatives, Supports Brokers and Care Coordinators with regular reports (Family Friendly Reports) that show how authorized units have been spent and the amount of taxes paid Responds to questions from Members/Representatives and workers Customer Service line, open between 9:00AM and 5:00 PM EST, Monday through Friday. Page 10 Version 2-6/3/2016 5

82 Title PPL s Role Provides Training and Support to Workers in: Understanding CHOICES and Consumer-Direction Supporting Older Adults and People who have Disabilities Fraud and abuse prevention, identification and reporting for Consumer Direction members Abuse and neglect prevention and reporting for Consumer Direction members Universal precautions and blood-borne pathogens Critical incident reporting How to use Timesheets Page 11 Title Supporting Older Adults and People who have Disabilities CHOICES is a person-centered program. Your role goes beyond care - it is to support the member to live their chosen lifestyle and to be as independent as possible. Physical and Emotional Needs Get to know the person you are supporting and make sure service delivery is driven by the person so it meets their basic needs and preferences, while also encouraging independence and self-respect Feeling important and worthwhile Meaningful Relationships Engagement in the person s community Feeling a sense of accomplishment and success Basic human needs: food, water, sleep, physical activity Safety and security Things to look out for Poor appetite Anger Depression Insomnia/restlessness Psychological Aspects It s important to understand why someone is acting or behaving a certain way and be sensitive to those realizations Loss of income, loss of independence, illness, loss of sense of security Page 12 Version 2-6/3/2016 6


83 Title Supporting Older Adults and People who have Disabilities The most important resource for workers is the member s plan of care, which outlines the member s needs and preferences. Promote self-care and independence Assure safety and comfort Always maintain dignity and self-respect for the Member Ask the member about preferences about privacy Always provide privacy for necessary activities Things to consider when supporting someone new: How does the member communicate? Are there language barriers to consider, or assistive devices? Does the person have a legal representative or a primary unpaid caregiver who is important to the member s decision making and/or support needs? Does the person use special equipment? If you provide physical assistance to transfer the person you support: Ask for specific training from Member/Representative Practice with another person in the room Use proper body mechanics to avoid injury Ask the member or the member s appointed representative for assistance, as needed. You can also request assistance from the Care Coordinator. Page 13 Title Self-Direction of Health Care Tasks What can workers do if assisting with Self-Directed Health Care Tasks? Apply topical medications as per Member s instructions Assist with oral and inhaled medications as per Member s instructions. May include: Getting the medications ready Having a drink prepared for them to take medications with Storing the medications properly Document on Daily Communication and Activities Log workers ARE NOT allowed to assist with any intrusive tasks. Intrusive tasks include: finger pricks, shots, trachea tubes, feeding tubes, catheterization, colostomy bags, or packing wounds. Page 14 Version 2-6/3/2016 7

84 Title Universal Precautions and Blood-borne Pathogens Universal Precautions are a Way to Prevent Spreading Infection Blood borne pathogens are spread when a person comes into direct contact with infected blood or body fluid How to protect yourself and the person you support Wear gloves Practice proper hygiene Use appropriate cleaning materials and keep surfaces clean Disinfect contaminated surfaces and objects WASH YOUR HANDS! This is the most effective way to prevent the spread of infection Wash your hands before and/or after Preparing food Assisting with eating Assisting with toileting Handling medications Giving first aid Handling animals Coming in contact with blood or body fluids Removing gloves Using the restroom Page 15 Title Reporting Problems with Consumer Direction Anytime you have an issue or a question, you can contact PPL customer service or the member s support broker TennCare has requirements for reporting three specific types of problems: 1. Fraud and Abuse 2. Abuse and Neglect 3. Critical Incidents All three have a reporting timeline requirement the member s Care Coordinator must be contacted within 24 hours from the time the incident occurs the Care Coordinator is required to complete a Critical Incident Form within 48 hours from the time the incident occurs ALL abuse, neglect and exploitation incidents must be reported to APS Page 16 Version 2-6/3/2016 8
85 Title Definitions & Examples of Required Problems to be Reported Fraud and Abuse : An intentional deception or misrepresentation made by a person with the knowledge that the deception could result in some unauthorized benefit to himself or some other person. It includes any act that constitutes fraud under applicable Federal or State Law. Provider practices that are inconsistent with sound fiscal, business, or medical practices, and result in an unnecessary cost to the Medicaid program, or in reimbursement of services that are not medically necessary or that fail to meet professionally recognized standards for health care. It also includes recipient practices that result in unnecessary cost to the Medicaid/TennCare/Cover TN Program. (as per the OIG) Examples: Worker records time worked and receives a paycheck but does not provide the service while in the home Worker falsifies hours on a timesheet; employer approves of falsified hours Worker records time worked and receives a paycheck but worker and Member engage in non authorized activities during that time period Page 17 Title Definitions & Examples of Required Problems to be Reported Abuse : The knowing infliction of injury, unreasonable confinement, intimidation or punishment with resulting physical harm, pain or mental anguish Examples: Member is overmedicated or over sedated Worker hits Member Worker yells at Member to hurry up or do things differently Neglect : Failure to provide goods or services necessary to avoid physical harm, mental anguish or mental illness, which results in injury or probable risk of serious harm Examples: Member becomes dehydrated because worker is not tending to her needs Worker does not keep Member s personal dwelling free from hazards, i.e. pests, clutter, holes in floor or walls (could also be self neglect) Worker leaves Member with balance problems alone in the bathroom Page 18 Version 2-6/3/2016 9

86 Title Definitions & Examples of Required Problems to be Reported Exploitation: The deliberate misplacement, misappropriation or wrongful, temporary, or permanent use of belongings or money with or without consent Examples Worker reads or withholds Member s mail Worker having the Member make purchases for him and does not repay the Member Worker uses relationship with Member to manipulate items from her, i.e., jewelry, money, other valuable personal belongings. Critical Incident: Any occurrence that causes harm to a Member or puts the Member at risk for abuse, neglect or exploitation These are just a few examples of things to avoid and look out for. Page 19 Title Critical Incidents When to Contact APS Critical Incidents that require APS involvement Death of a CHOICES member due to abuse or neglect Suspected physical or mental abuse of a CHOICES member Theft or financial exploitation of a CHOICES member Severe injury sustained by a CHOICES member Sexual abuse and/or suspected abuse and neglect of a CHOICES member Critical Incidents that do not require APS involvement Accidental and minor injury of a CHOICES member Death of a CHOICES member due to natural causes Medication error involving a CHOICES member self-directing medication administration Remember to ALWAYS call the Care Coordinator within 24 hours of the incident occurring! Page 20 Version 2-6/3/
87 Title Contacting APS For Abuse, Neglect, or Exploitation Reports call: Adult Protective Services: (APS-TENN) Local Numbers Knoxville: Chattanooga: Nashville: Memphis: Callers will give: Name of individual Address Age Phone number Specifics of abuse Page 21 Title APS Reports Critical incidents requiring APS investigation can involve workers or Representatives If the critical incident involves a worker, Worker must be released from providing service until an investigation can be completed Member must implement the back-up plan to ensure services are provided as scheduled Unsubstantiated claim = Member s choice whether or not to keep that person as worker Substantiated claim = Member will have to choose a new worker. Failure to do so may result in involuntary termination from Consumer-Direction If the critical incident involves a member s Representative, Representative must be released from duties until investigation is complete and the Care Coordinator needs to assist member to find temporary replacement Unsubstantiated claim = Member s choice whether or not to keep that person as their Representative Substantiated claim = Member will have to choose a new Representative. Failure to do so may result in involuntary termination from Consumer-Direction. Page 22 Version 2-6/3/

88 Title APS Reports You need to report all cases of suspected abuse, neglect and exploitation because it is the law! Adults - TCA Failure to report suspected fraud, abuse, neglect or exploitation is a Class A misdemeanor and may result in criminal and/or civil liability. Coordinate and collaborate with APS or other investigative entities during and after investigations occur You must report issues within specific timelines: 24 hours verbal report to the Care Coordinator 48 hours Critical Incident Report Form completed by Care Coordinator Page 23 Title Working for your Member/Participant When will you start working? How will you know? When PPL has received and processed all the member s paperwork, all of your paperwork, your background check has come back as passed, and your FA/CPR certs have been received; PPL send notice to the MCO that the member is ready to being services. The MCO will then give an PPL authorized date for services to start. The member s Support Broker will call the member & you with this start date. What s your schedule? You ll need to discuss the schedule with your employer. The member has a recommended number hours of care per week based on the Plan of Care. Your member can determine when you work based on their needs. How will you be paid? Payroll is every two weeks, please reference payroll calendar in your worker packets PPL must have valid authorizations from the MCO and an approved timesheet from the employer in order to pay you. Timesheets can be completed one of 3 different ways, you ll need to discuss with your employer which method they want you to use: 1. the BetterOnline Web Portal 2. the Time4Care mobile app 3. Paper timesheet Page 24 Version 2-6/3/

 and clicking Sign Up Page 25 Title Using the BetterOnline website and Time4Care mobile app Step 1 - Choose the State Step 3 - Choose the Role, then click Next Step 2 - Choose the")
89 Title Using the BetterOnline website and Time4Care mobile app BetterOnline and Time4Care are PPL s timesheet processing system. They are connected to each other. So, an worker could use the mobile app, their employer could use the website, and they will each see the same information. First step is creating an account by using the BetterOnline website (fms.publicpartnerships.com) and clicking Sign Up Page 25 Title Using the BetterOnline website and Time4Care mobile app Step 1 - Choose the State Step 3 - Choose the Role, then click Next Step 2 - Choose the program The program will be TennCare TNAC, TennCare TNAG, or TennCare TNVSHP Step 4 - Enter Credentials your last name, your mailing zip code, your social security number Page 26 Version 2-6/3/
 Answer the 3 security questions Keep this information secure and do not allow anyone else to use your login information.")

90 Title Using the BetterOnline website and Time4Care mobile app Step 5 User Information Create a username Create a password - must be 8+ characters long, must include lower and uppercase letters, at least one number, at least one unique character (?!$%) Answer the 3 security questions Keep this information secure and do not allow anyone else to use your login information. Page 27 Title Using the BetterOnline website and Time4Care mobile app Once your account is created, you can continue using the BetterOnline website OR you can download the Time4Care mobile app The Time4Care app is a free download that can be found in the Apple App Store, Google Play Store, or Amazon Fire Store and can be used on any smartphone or tablet device. Search TIME4CARE in the store. You should see the icon below once the app is downloaded. Open the app and login with your account information that your created on the BetterOnline website Page 28 Version 2-6/3/


91 Title Creating a Timesheet on the BetterOnline website Log onto the website to create a new timesheet; click the create timesheet link Choose create timesheet to the right of the member s name If you work for more than one member, you will see each member listed here and be able to choose which member s profile you need to create a timesheet under Smith, Jane C Nashville 03/03/1933 JANE SMITH Page 29 Title Creating a Timesheet on the BetterOnline website Click on the Calendar to select the date A timesheet for the date range you selected will open, you will be able to enter the service, the time in and time out, and add additional hours for days you worked. Once you ve entered all the hours you need to enter on this timesheet, scroll down and click Next By clicking There are more hours you can add additional shifts to the same date Be specific on your hours! Page 30 Version 2-6/3/

92 Title Creating a Timesheet on the BetterOnline website After clicking next you ll be able to see your timesheet. If you need to add more hours, click save my work and your timesheet will be saved for you to go back and edit at a later date. If you re done with your timesheet, check the box near the statement I understand that payment and satisfaction of this claim will be from federal and state funds, and that any false claims, statements, documents, or concealment of a material fact, may be prosecuted under applicable federal and/or state laws. and click Submit Page 31 Title Creating a Timesheet on the BetterOnline website When you ve submitted your timesheet, your employer will be able to see the completed timesheet, review it for accuracy, and approve it for payment If your employer sees an issue with your timesheet, your employer can reject the timesheet. The timesheet will then be available to you to edit and correct to reflect the correct time. If you saved your timesheet, you can click on the Timesheets header, then Search Timesheets and in the Timesheet Status field choose Saved and click Search Your saved timesheet will show on the page, and you ll be able to choose the edit button on the left to edit your timesheet and add additional hours Page 32 Version 2-6/3/


93 Title Creating a Timesheet on the Time4Care app Open the app and log in You can choose to Clock In or Clock Out if you re entering time for the current shift you re working OR you can choose Enter Time in a Timesheet if you re entering time for a shift/day that has already passed If you want to access a timesheet you have previously saved either on the website or on the app, choose Enter Time in a Timesheet Page 33 Title Creating a Timesheet on the Time4Care app If you choose Clock In or Clock Out You ll see the current date and time listed. If you have location services turned on, it will also show you in the same location at the member s household You ll be able to choose the member you re working for, the service you re working, and click Clock In Now When you finish your shift, you ll need to remember to access the app again and click Clock Out Now to make sure the system reflects the correct end time of your shift Page 34 Version 2-6/3/



94 Title Creating a Timesheet on the Time4Care app If you choose Enter Time in a Timesheet You ll see the month for the current pay period You ll be able see all timesheets in the month, and the status of those timesheets You can select the member name on the Saved timesheet to edit the timesheet Jane Smith Jane Smith Jane Smith Jane Smith Page 35 Title Creating a Timesheet on the Time4Care app When you click on the saved timesheet, you can: Jane Smith Edit the time already entered on the timesheet by clicking on the service Add an additional entry to a date by clicking Add Entry Add a new entry to a date by clicking Add Entry Clicking Add Entry from the timesheet page, will allow you to select the service code, your time in, and time out. Click Add Entry again to save the information on your timesheet. Page 36 Version 2-6/3/

95 Title Using Paper Timesheets Your name, worker number, service code, and your signature must be on the timesheet The name of the member you help, the member number, and the EOR s signature must be on the timesheet. Include pay period start and end dates, fill in the AM/PM bubbles, write clearly and neatly Be careful when faxing a paper timesheet. Make sure to look at the instructions on the fax machine. Some fax machines need the document to be placed Face Up and some need the document to be placed Face Down. If you do not do this right it can delay your payment, because PPL may receive a blank page. A coversheet is not needed. If you make a mistake on a paper timesheet, you will need to create a new timesheet and present to your employer for approval. Timesheets must be faxed prior to the 5:00 PM EST Sunday payroll deadline for timely payroll processing. If your timesheet is faxed after the deadline, it will be processed the following week. Faxed or mailed paper timesheets are due one day earlier than electronic timesheets to allow for the manual processing required by paper timesheet submission. Page 37 Title Using Paper Timesheets Special Situations When you work overnight, you must enter one line for work you did before midnight and a line the next day for work you did after midnight. For example: Worker s shift is 10 pm to 7am. The time worked from 10 pm until 11:59 pm is one line item on timesheet. Time from Midnight to 7 am the following day and is entered as another line item on the time sheet. When using a paper timesheet if you work multiple times in one day, enter each start time on a new line. For example: Start work at 9:00 AM and leave work at 10:30 AM. This will be one line item. Return to work at 12:00 PM and leave work again at 2:00 PM. This will be your second line item for the day. When using a paper timesheet if you work multiple services in one day, enter each service on a new timesheet. For example: Work personal care at 9:00 AM and leave work at 10:30 AM. This will be one timesheet. Return to work in-home respite a at 6:00 PM and leave work again at 10:00 PM. This will be on a second timesheet. Use AM and PM correctly. AM Starts at Midnight and goes until 1 minute before Noon. (12:00am 11:59pm) PM starts at Noon and goes until 1 minute before Midnight. (12:00pm 11:59pm) Page 38 Version 2-6/3/
 Page 39")

96 Title Paper Timesheet (example) Page 39 Title Questions? Page 40 Version 2-6/3/
97
98 CHOICES WORKER TRAINING CHECKLIST FOR CONSUMER DIRECTION Please utilize this form to indicate if training in all areas for workers has been completed. Remember to submit all tests to PPL and keep a copy for your records. Employee Name: Training topic to be covered Yes 1. Overview of CHOICES and Consumer Direction program 2. Understanding the role of members and representatives in Consumer Direction 3. Understanding the role of the care coordinator, the supports broker and the FEA 4. Understanding the role of the worker in Consumer Direction 5. CPR/First Aid 6. Caring for the elderly and disabled populations 7. Abuse and neglect prevention and reporting 8. Fraud and abuse prevention and reporting 9. Critical Incident Reporting 10. Understanding the requirements for specialized training for workers regarding member s individualized service needs and preferences 11. Understanding that if the member elects to self-direct health care tasks that the member/representative will provide training specific to the member s needs 12. General training on blood-borne pathogens 13. Understanding that the worker can request additional training on any of these items from the supports broker. 14. Understanding that the member, care coordinator or supports broker can require additional and refresher training on any of these items. 15. Understanding the timing for the authorization process, what authorizations are and that worker will not be paid for working hours that are not authorized 16. Understanding the member/ representative will set a worker s rate of pay and determine the schedule of workers. CHOICES Worker Training Checklist: Page 1 of 2
99

100 17. Use of the BetterOnline and Time4Care electronic timesheet systems, and use of paper timesheets. Understanding timesheets will be used for capturing worker time and that workers will be paid based on Employer approved timesheets. 18. Understanding that worker is responsible for accurate recording of time worked on timesheets (electronic or paper) and submitting the completed timesheet to Employer for approval by pay period deadline date. 19. Understanding of the daily notes requirement CHOICES worker Signature CHOICES worker Printed Name Date CHOICES Worker Training Checklist: Page 2 of 2
101
 This form is used to establish direct deposit of your paycheck from PPL to your bank account. We encourage workers to use direct deposit. 2.")
102 Optional Forms The following forms are not required by PPL If they are useful to you however, please complete and submit to PPL 1. EFT Instructions and Application (2 pages) This form is used to establish direct deposit of your paycheck from PPL to your bank account. We encourage workers to use direct deposit. 2. Change of Address/Name Form (1 page) Please submit this form directly to PPL if you change your mailing address or name. If you change your name, you must submit this form, along with a copy of your updated Social Security Card with your new name. PPL needs this information to pay your withheld taxes to the IRS and State and mail your W-2 at the end of the year. NEED HELP? CALL TOLL FREE AT Optional Forms: Page 1 of 1
103
 or Vendor would like their payments made via Direct Deposit, they may fill out and submit this form to Public Partnerships, LLC (PPL). How do I complete this form?")

104 Public Partnerships, LLC TennCare UHC Consumer Direction 7776 S Pointe Pkwy W, Suite 150 Phoenix, AZ Instructions for Direct Deposit Setup What is the purpose of this form? If a Support Service Worker (SSW) or Vendor would like their payments made via Direct Deposit, they may fill out and submit this form to Public Partnerships, LLC (PPL). How do I complete this form? Fill in your Name, PPL ID (if known), and Social Security Number in the blanks at the top of the page. Check off the appropriate box indicating if the Direct Deposit is going to a Checking Account, Savings Account, or a Pay Card. Attach a Voided Check to the form OR submit documentation from your financial entity confirming the account number and routing number of the account you wish the funds to be deposited into. Sign and Date the bottom of the form. Where to send the form? Fax Mail choices.achoice@pcgus.com Public Partnerships, LLC TennCare UHC Consumer Direction 7776 S Pointe Pkwy W, Suite 150 Phoenix, AZ Direct Deposit Setup Instructions
Separate here and give Form W-4 to your employer. Keep the top part for your records. Employee s Withholding Allowance Certificate
 Form W-4 (2017) Purpose. Complete Form W-4 so that your employer can withhold the correct federal income tax from your pay. Consider completing a new Form W-4 each year and when your personal or financial
Form W-4 (2017) Purpose. Complete Form W-4 so that your employer can withhold the correct federal income tax from your pay. Consider completing a new Form W-4 each year and when your personal or financial
Employment Eligibility Verification
 Employment Eligibility Verification Department of Homeland Security U.S. Citizenship and Immigration Services USCIS Form I-9 OMB No. 1615-0047 Expires 08/31/2019 START HERE: Read instructions carefully
Employment Eligibility Verification Department of Homeland Security U.S. Citizenship and Immigration Services USCIS Form I-9 OMB No. 1615-0047 Expires 08/31/2019 START HERE: Read instructions carefully
Employment Eligibility Verification
 Employment Eligibility Verification Department of Homeland Security U.S. Citizenship and Immigration Services USCIS Form I-9 OMB No. 1615-0047 Expires 08/31/2019 START HERE: Read instructions carefully
Employment Eligibility Verification Department of Homeland Security U.S. Citizenship and Immigration Services USCIS Form I-9 OMB No. 1615-0047 Expires 08/31/2019 START HERE: Read instructions carefully
Name: MCO (circle one): AG UHC VSHP (Blue Care) Worker Training Checklist. I-9 Criminal Attestation Tax Exempt W-4. Additional Comments:
: AG UHC VSHP (Blue Care) Worker Training Checklist. I-9 Criminal Attestation Tax Exempt W-4. Additional Comments:") 414 Union ST, Ste 1100 Nashville, TN 37219 Fax - Worker United Health Care Fax: 877.432.4103 (FOR DOCUMENTS ONLY. NO TIMESHEETS TO THIS NUMBER) Customer Service: 888.866.1154 To: Fax: Phone: Member Name:
414 Union ST, Ste 1100 Nashville, TN 37219 Fax - Worker United Health Care Fax: 877.432.4103 (FOR DOCUMENTS ONLY. NO TIMESHEETS TO THIS NUMBER) Customer Service: 888.866.1154 To: Fax: Phone: Member Name:
Separate here and give Form W-4 to your employer. Keep the top part for your records. Employee s Withholding Allowance Certificate
 Form W-4 (2017) Purpose. Complete Form W-4 so that your employer can withhold the correct federal income tax from your pay. Consider completing a new Form W-4 each year and when your personal or financial
Form W-4 (2017) Purpose. Complete Form W-4 so that your employer can withhold the correct federal income tax from your pay. Consider completing a new Form W-4 each year and when your personal or financial
New Employment & Sign-up Checklist for Managers and Departmental Representatives
 FLORIDA A&M UNIVERSITY New Employment & Sign-up Checklist for Managers and Departmental Representatives Executive Service A&P USPS OPS Faculty (Please complete Section II Only) Employee Name: Class Title:
FLORIDA A&M UNIVERSITY New Employment & Sign-up Checklist for Managers and Departmental Representatives Executive Service A&P USPS OPS Faculty (Please complete Section II Only) Employee Name: Class Title:
RAYMOND CENTRAL PUBLIC SCHOOLS SUBSTITUTE TEACHER DATA SHEET
 RAYMOND CENTRAL PUBLIC SCHOOLS SUBSTITUTE TEACHER DATA SHEET PLEASE NOTE: We need a voided check for payment by Direct Deposit and we must have an email address. Thank you. W-4 Form I-9 Form - 2 forms
RAYMOND CENTRAL PUBLIC SCHOOLS SUBSTITUTE TEACHER DATA SHEET PLEASE NOTE: We need a voided check for payment by Direct Deposit and we must have an email address. Thank you. W-4 Form I-9 Form - 2 forms
EMPLOYEE INFORMATION SHEET
 EMPLOYEE INFORMATION SHEET PLEASE PRINT CLEARLY COMPANY: EMPLOYEE #: SOCIAL SECURITY NUMBER: - - NAME: First MI LAST STREET: CITY: AS APPEARS ON SOCIAL SECURITY CARD STATE: ZIP CODE: TELEPHONE NUMBER:
EMPLOYEE INFORMATION SHEET PLEASE PRINT CLEARLY COMPANY: EMPLOYEE #: SOCIAL SECURITY NUMBER: - - NAME: First MI LAST STREET: CITY: AS APPEARS ON SOCIAL SECURITY CARD STATE: ZIP CODE: TELEPHONE NUMBER:
Southeast ID#: Name: SSN: PREVIOUS CIVIL OR COLLEGE DISCIPLINE
 /Student Employment Work Referral Southeast ID#: Name: SSN: STUDENT EMPLOYEE ELIGIBILITY AND RESPONSIBILITIES 1. You must complete, and have on file with Student Financial Services, employment eligibility
/Student Employment Work Referral Southeast ID#: Name: SSN: STUDENT EMPLOYEE ELIGIBILITY AND RESPONSIBILITIES 1. You must complete, and have on file with Student Financial Services, employment eligibility
YOU DO NOT NEED TO PRINT THIS PAGE. Substitute Records Requirements. Social Security Card (copies not accepted)
") YOU DO NOT NEED TO PRINT THIS PAGE. Appointment Date & Time: Name: Date: Substitute Records Requirements I-9 (only complete page 1) W-4 Social Security Card (copies not accepted) Driver s License Direct
YOU DO NOT NEED TO PRINT THIS PAGE. Appointment Date & Time: Name: Date: Substitute Records Requirements I-9 (only complete page 1) W-4 Social Security Card (copies not accepted) Driver s License Direct
New Employee Information
 HOUSTON S PREMIER POKER DESTINATION New Employee Information Before you will be scheduled the following MUST be completed: 1. Your new hire packet must be filled out completely and correctly and handed
HOUSTON S PREMIER POKER DESTINATION New Employee Information Before you will be scheduled the following MUST be completed: 1. Your new hire packet must be filled out completely and correctly and handed
Separate here and give Form W-4 to your employer. Keep the top part for your records. Employee s Withholding Allowance Certificate
 Form W-4 (2017) Purpose. Complete Form W-4 so that your employer can withhold the correct federal income tax from your pay. Consider completing a new Form W-4 each year and when your personal or financial
Form W-4 (2017) Purpose. Complete Form W-4 so that your employer can withhold the correct federal income tax from your pay. Consider completing a new Form W-4 each year and when your personal or financial
Graveyard Productions, LLC
 Graveyard Productions, LLC Check here if you are under 18 years old Recruitment Application- 2018 PLEASE PRINT LEGIBLY Applicant Information Full Name: Date: Last First M.I. Address: Street Address Apartment/Unit
Graveyard Productions, LLC Check here if you are under 18 years old Recruitment Application- 2018 PLEASE PRINT LEGIBLY Applicant Information Full Name: Date: Last First M.I. Address: Street Address Apartment/Unit
December, Following is an overview of the payroll tax rates and other payroll related information in effect in 2019:
 1 December, 2018 It s time again for the annual payroll letter. The following pages include payroll and other miscellaneous information that may be helpful in fulfilling your payroll and related reporting
1 December, 2018 It s time again for the annual payroll letter. The following pages include payroll and other miscellaneous information that may be helpful in fulfilling your payroll and related reporting
EMPLOYEE PORTAL PASSWORD SET UP
 EMPLOYEE PORTAL PASSWORD SET UP Here are some helpful tips to make sure you have access to paystubs and W2 s. Please be sure you include an email address in your new hire paperwork. The first page titled
EMPLOYEE PORTAL PASSWORD SET UP Here are some helpful tips to make sure you have access to paystubs and W2 s. Please be sure you include an email address in your new hire paperwork. The first page titled
YOU DO NOT NEED TO PRINT THIS PAGE. Substitute Records Requirements. Social Security Card (copies not accepted)
") YOU DO NOT NEED TO PRINT THIS PAGE. Appointment Date & Time: Name: Date: Substitute Records Requirements I-9 (only complete page 1) W-4 Social Security Card (copies not accepted) Driver s License Direct
YOU DO NOT NEED TO PRINT THIS PAGE. Appointment Date & Time: Name: Date: Substitute Records Requirements I-9 (only complete page 1) W-4 Social Security Card (copies not accepted) Driver s License Direct
Separate here and give Form W-4 to your employer. Keep the top part for your records. Employee's Withholding Allowance Certificate
 Form W-4 (2015) Purpose. Complete Form W-4 so that your employer can withhold the correct federal income tax from your pay. Consider completing a new Form W-4 each year and when your personal or financial
Form W-4 (2015) Purpose. Complete Form W-4 so that your employer can withhold the correct federal income tax from your pay. Consider completing a new Form W-4 each year and when your personal or financial
New Employee Welcome Letter and Orientation Checklist
 Lafayette DQ Restaurants P.O. Box 302 Delphi, IN 46923 Phone: (765) 447-1089 Fax: (765) 535-5001 New Employee Welcome Letter and Orientation Checklist Welcome to the DQ family! In order to start training
Lafayette DQ Restaurants P.O. Box 302 Delphi, IN 46923 Phone: (765) 447-1089 Fax: (765) 535-5001 New Employee Welcome Letter and Orientation Checklist Welcome to the DQ family! In order to start training
Missouri Department of Revenue Employee s Withholding Allowance Certificate
 Form MO W-4 Missouri Department of Revenue Employee s Withholding Allowance Certificate This certificate is for income tax withholding and child support enforcement purposes only. Type or print. Full Name
Form MO W-4 Missouri Department of Revenue Employee s Withholding Allowance Certificate This certificate is for income tax withholding and child support enforcement purposes only. Type or print. Full Name
EMP NAME: DEPT CODE LOCATION: B/G CHK: N/A COMPLETED START DATE: PAY RATE: TAX CODES: ( FILLED BY OFFICE ONLY ) LIVE IN WORK IN LST
 LIVE IN WORK IN LST") APPLICATION MGR: EMP # EMP NAME: DEPT CODE LOCATION: B/G CHK: N/A COMPLETED START DATE: PAY RATE: DAYS TO WORK: Mon Tues Wed Thurs Fri Sat Sun SCHEDULED HOURS: - PART TIME FULL TIME (30 hours or more )
APPLICATION MGR: EMP # EMP NAME: DEPT CODE LOCATION: B/G CHK: N/A COMPLETED START DATE: PAY RATE: DAYS TO WORK: Mon Tues Wed Thurs Fri Sat Sun SCHEDULED HOURS: - PART TIME FULL TIME (30 hours or more )
Jersey Assistance for Community Caregiving (JACC) Program PEP Enrollment Packet
 Program PEP Enrollment Packet") Public Partnerships Jersey Assistance for Community Caregiving (JACC) Program Phone: 1-866-239-2778 Paperwork Fax: 1-866-547-2481 Paperwork E-mail: njpplfax@pcgus.com Website: www.publicpartnerships.com
Public Partnerships Jersey Assistance for Community Caregiving (JACC) Program Phone: 1-866-239-2778 Paperwork Fax: 1-866-547-2481 Paperwork E-mail: njpplfax@pcgus.com Website: www.publicpartnerships.com
2019 English Applica on
 2019 English Applica on (Please Print) Date: First Name Last Name Social Security Address Apt. City State Zip Code Home Phone Cell Phone E-Mail Please place a check by your response or provide the appropriate
2019 English Applica on (Please Print) Date: First Name Last Name Social Security Address Apt. City State Zip Code Home Phone Cell Phone E-Mail Please place a check by your response or provide the appropriate
Packet A - Forms. If you have any questions, please contact Human Resources at
 Packet A - Forms 2018 TEMPORARY NEW HIRE PAPERWORK Welcome to Union College! This packet contains new hire forms necessary for you to become established as a Union College employee. Please fill out and
Packet A - Forms 2018 TEMPORARY NEW HIRE PAPERWORK Welcome to Union College! This packet contains new hire forms necessary for you to become established as a Union College employee. Please fill out and
XXXXXX NON-UNION VOUCHER. White - Payroll Company Yellow - Accounting Department Pink - Employee TIME CLOCK RATE ALLOWANCES SPECIAL COMPENSATIONS
 XXXXXX NON-UNION VOUCHER DATE PRODUCTION & PROJECT NAME 1 2 3 LAST NAME FIRST NAME MI STREET ADDRESS CITY STATE ZIP DATE OF BIRTH: IF MINOR PHONE IF NEW IF NEW EMPLOYEE ADDRESS SOCIAL SECURITY NUMBER WORK
XXXXXX NON-UNION VOUCHER DATE PRODUCTION & PROJECT NAME 1 2 3 LAST NAME FIRST NAME MI STREET ADDRESS CITY STATE ZIP DATE OF BIRTH: IF MINOR PHONE IF NEW IF NEW EMPLOYEE ADDRESS SOCIAL SECURITY NUMBER WORK
INSTRUCTIONS FOR PAPERWORK ALL FORMS MUST BE SIGNED AND DATED PLEASE PRINT ONE-SIDED SHEETS
 INSTRUCTIONS FOR PAPERWORK ALL FORMS MUST BE SIGNED AND DATED PLEASE PRINT ONE-SIDED SHEETS CFISD EMPLOYEE INFORMATION SHEET Must be LEGIBLE Fill in all blanks You MUST bubble an answer for Part 1-Ethnicity
INSTRUCTIONS FOR PAPERWORK ALL FORMS MUST BE SIGNED AND DATED PLEASE PRINT ONE-SIDED SHEETS CFISD EMPLOYEE INFORMATION SHEET Must be LEGIBLE Fill in all blanks You MUST bubble an answer for Part 1-Ethnicity
EMPLOYER INFORMATION SHEET
 General EMPLOYER INFORMATION SHEET Business Name: Business Address: City, State, Zip: Filing Name (if different): Filing Address (if different): City, State, Zip: Contact Name: Phone: Fax: Email: Company
General EMPLOYER INFORMATION SHEET Business Name: Business Address: City, State, Zip: Filing Name (if different): Filing Address (if different): City, State, Zip: Contact Name: Phone: Fax: Email: Company
LS Contracting Group, Inc. General Contractor & Specialty Restoration
 LS Contracting Group, Inc. General Contractor & Specialty Restoration 5660 N. Elston Ave. Chicago, IL 60646 p: (773) 774-1122 f: (773) 774-5660 lscontracting.com EMPLOYMENT APPLICATION CHECKLIST Name:
LS Contracting Group, Inc. General Contractor & Specialty Restoration 5660 N. Elston Ave. Chicago, IL 60646 p: (773) 774-1122 f: (773) 774-5660 lscontracting.com EMPLOYMENT APPLICATION CHECKLIST Name:
Warrick County School Corporation
 Warrick County School Corporation SUPERINTENDENT S OFFICE P.O. Box 809/Boonville, Indiana 47601/812-897-0400 Welcome to the Warrick County School Corporation Welcome to the one of the best school corporations
Warrick County School Corporation SUPERINTENDENT S OFFICE P.O. Box 809/Boonville, Indiana 47601/812-897-0400 Welcome to the Warrick County School Corporation Welcome to the one of the best school corporations
**If you have any other questions, please contact us and we will be happy to help.**
 Attention GGRC Public Partnerships, LLC 7776 S Pointe Pkwy W Suite 5 Phoenix, AZ 8544 Worker First name, Last name Worker Mailing Address, Address 2 Worker City, State, Zip Dear Worker This packet includes
Attention GGRC Public Partnerships, LLC 7776 S Pointe Pkwy W Suite 5 Phoenix, AZ 8544 Worker First name, Last name Worker Mailing Address, Address 2 Worker City, State, Zip Dear Worker This packet includes
NO CONFLICT ATTESTATION. In order to qualify to act as the Personal Assistant for this Consumer, I attest to the ALL of following:
 NO CONFLICT ATTESTATION In order to qualify to act as the Personal Assistant for this Consumer, I attest to the ALL of following: 1. I am NOT the Consumer s Designated Representative. 2. The Consumer is
NO CONFLICT ATTESTATION In order to qualify to act as the Personal Assistant for this Consumer, I attest to the ALL of following: 1. I am NOT the Consumer s Designated Representative. 2. The Consumer is
Employment Application
 P.O. Box 643 Benavides, Tx 78341 (361) 256-4726 Office (361) 256-4728 Fax Scorp1144@yahoo.com Scorpion Exploration & Production, Inc. Full Name Mailing Address Employment Application Applicant Information
P.O. Box 643 Benavides, Tx 78341 (361) 256-4726 Office (361) 256-4728 Fax Scorp1144@yahoo.com Scorpion Exploration & Production, Inc. Full Name Mailing Address Employment Application Applicant Information
Branson Public Schools
 Branson Public Schools Dr. Don Forrest, Assistant Superintendent of Business Services 1756 Bee Creek Rd Branson, MO 65616 Phone: 417.334.6541 uww.branson.k12.mo.us Fax: 417.332.2510 Amy Mulvaney, Administrative
Branson Public Schools Dr. Don Forrest, Assistant Superintendent of Business Services 1756 Bee Creek Rd Branson, MO 65616 Phone: 417.334.6541 uww.branson.k12.mo.us Fax: 417.332.2510 Amy Mulvaney, Administrative
Dedicated to Providing the Highest Level of Public Safety Services to our Community
 FIRE CHIEF Lonnie E. Click Dedicated to Providing the Highest Level of Public Safety Services to our Community COMMISSIONERS Earl W. Bill Houchin Jerry F. Morris Gerald D. Sleater INTRODUCTION Thank you
FIRE CHIEF Lonnie E. Click Dedicated to Providing the Highest Level of Public Safety Services to our Community COMMISSIONERS Earl W. Bill Houchin Jerry F. Morris Gerald D. Sleater INTRODUCTION Thank you
Employee Packet Forms
 Welcome!! Outreach Health Services looks forward to working with you. This Employee Packet has the forms and information you need to become an employee. The participant, who is your employer, can help
Welcome!! Outreach Health Services looks forward to working with you. This Employee Packet has the forms and information you need to become an employee. The participant, who is your employer, can help
Please complete and sign all forms in the PRE-EMPLOYMENT FORMS section.
 NATIONAL HOME HEALTH SERVICES EMPLOYMENT FORMS 5811 Dempster St Morton Grove, IL 60053 Phone: (847) 329-9933 Fax: (847) 930-0375 APPLICANT NAME POSITION APPLYING FOR DATE Please complete and sign all forms
NATIONAL HOME HEALTH SERVICES EMPLOYMENT FORMS 5811 Dempster St Morton Grove, IL 60053 Phone: (847) 329-9933 Fax: (847) 930-0375 APPLICANT NAME POSITION APPLYING FOR DATE Please complete and sign all forms
FORMS TO BE COMPLETED AND SUBMITTED TO HUMAN RESOURCES. The College requires all Employees complete and submit the following documents:
 FORMS TO BE COMPLETED AND SUBMITTED TO HUMAN RESOURCES The College requires all Employees complete and submit the following documents: 1. I-9 Employment Eligibility Verification: Complete the I-9 Form
FORMS TO BE COMPLETED AND SUBMITTED TO HUMAN RESOURCES The College requires all Employees complete and submit the following documents: 1. I-9 Employment Eligibility Verification: Complete the I-9 Form
Personal Fact Sheet (This information is not to be requested before employment)
") Personal Fact Sheet (This information is not to be requested before employment) Self-disclosure of this information is requested for Affirmative Action, insurance and other purposes. It will not in any
Personal Fact Sheet (This information is not to be requested before employment) Self-disclosure of this information is requested for Affirmative Action, insurance and other purposes. It will not in any
What s In My Paycheck? compensation package: all of the wages (salary, bonus, commission) and benefits provided by an employer. What s In My Paycheck?
 and benefits provided by an employer. What s In My Paycheck?") compensation package: all of the wages (salary, bonus, commission) and benefits provided by an employer wages: money paid or received for work or services completed, usually by the hour, day, or week hourly
compensation package: all of the wages (salary, bonus, commission) and benefits provided by an employer wages: money paid or received for work or services completed, usually by the hour, day, or week hourly
Western States Office and Professional Employees Pension Fund
 Western States Office and Professional Employees Pension Fund FEDERAL INCOME TAX WITHHOLDING TAX WITHHOLDING ELECTION Please complete the attached W-4P Withholding Certificate for Pension or Annuity Payments.
Western States Office and Professional Employees Pension Fund FEDERAL INCOME TAX WITHHOLDING TAX WITHHOLDING ELECTION Please complete the attached W-4P Withholding Certificate for Pension or Annuity Payments.
Human Resources Department Mary Lou Glaesmann, Asst. Supt. for HR
 Human Resources Department Mary Lou Glaesmann, Asst. Supt. for HR Welcome! This document contains the paperwork you will be required to complete and bring to your HR orientation. Below are some helpful
Human Resources Department Mary Lou Glaesmann, Asst. Supt. for HR Welcome! This document contains the paperwork you will be required to complete and bring to your HR orientation. Below are some helpful
COLCHESTER SCHOOL DISTRICT
 COLCHESTER SCHOOL DISTRICT APPLICATION FOR SUBSTITUTING Administrative Offices, 125 Laker Lane P.O. Box 27, Colchester, VT 05446-0027 Phone (802) 264-5999 Fax (802) 863-4774 Name: Telephone No.: Mailing
COLCHESTER SCHOOL DISTRICT APPLICATION FOR SUBSTITUTING Administrative Offices, 125 Laker Lane P.O. Box 27, Colchester, VT 05446-0027 Phone (802) 264-5999 Fax (802) 863-4774 Name: Telephone No.: Mailing
Employee (Caregiver) Packet (Keep this folder for your records)
 Packet (Keep this folder for your records)") Employee (Caregiver) Packet (Keep this folder for your records) You will need to complete the following steps in order to hire an employee. Enrollment forms to enroll and hire a Support Broker can be found
Employee (Caregiver) Packet (Keep this folder for your records) You will need to complete the following steps in order to hire an employee. Enrollment forms to enroll and hire a Support Broker can be found
Employee Data Form. [ ] ] ] [ ] ] [ ] _] _]_ ] Home Address Apt City State Zip Code County. Ethnicity: Are you Hispanic/Latino?
![Employee Data Form. [ ] ] ] [ ] ] [ ] _] _]_ ] Home Address Apt City State Zip Code County. Ethnicity: Are you Hispanic/Latino?](/thumbs/79/79502522.jpg "Employee Data Form. [ ] ] ] [ ] ] [ ] _] _]_ ] Home Address Apt City State Zip Code County. Ethnicity: Are you Hispanic/Latino?") Employee Data Form Baltimore City Public Schools Office Of Human Capital 200 E. North Avenue, Room 110 Baltimore, Maryland 21202 www. s New /Rehire employees are required to complete this form as part
Employee Data Form Baltimore City Public Schools Office Of Human Capital 200 E. North Avenue, Room 110 Baltimore, Maryland 21202 www. s New /Rehire employees are required to complete this form as part
DIVERSIFIED Edgewood Road, NE Cedar Rapids, IA
 DIVERSIFIED --------------------- 4443 Edgewood Road, NE Cedar Rapids, IA 52499 800-755-5801 www.divinvest.com Federal Tax Withholding Election Form Instructions To change your federal income tax withholding,
DIVERSIFIED --------------------- 4443 Edgewood Road, NE Cedar Rapids, IA 52499 800-755-5801 www.divinvest.com Federal Tax Withholding Election Form Instructions To change your federal income tax withholding,
Bring all completed forms to your paperwork session. Any questions that you may have about the forms, we will be happy to address at the session.
 Directions for completing the New Hire Paperwork On-Line: Please print all pages (12 forms) 1-Employment Eligibility Verification Form: complete and sign/date Section 1. If your social security card states
Directions for completing the New Hire Paperwork On-Line: Please print all pages (12 forms) 1-Employment Eligibility Verification Form: complete and sign/date Section 1. If your social security card states
Bring all completed forms to your paperwork session. Any questions that you may have about the forms, we will be happy to address at the session.
 Directions for completing the New Hire Paperwork On-Line: Please print all pages (12 forms) 1-Employment Eligibility Verification Form: complete and sign/date Section 1. If your social security card states
Directions for completing the New Hire Paperwork On-Line: Please print all pages (12 forms) 1-Employment Eligibility Verification Form: complete and sign/date Section 1. If your social security card states
Student Employee New Hire Packet
 Student Employee New Hire Packet New Hire Checklist: o Authorization to Hire Form o Student Application o Federal W-4 Form o NJ State W-4 Form o I-9 Form o Social Security Card (for Payroll purposes) o
Student Employee New Hire Packet New Hire Checklist: o Authorization to Hire Form o Student Application o Federal W-4 Form o NJ State W-4 Form o I-9 Form o Social Security Card (for Payroll purposes) o
On Call Staffing On - Boarding Checklist
 On Call Staffing On - Boarding Checklist Please note that we will need ALL of the items below completed and returned to our office. Documents can be returned in person, via fax, or mail. Completed Application
On Call Staffing On - Boarding Checklist Please note that we will need ALL of the items below completed and returned to our office. Documents can be returned in person, via fax, or mail. Completed Application
EMPLOYER WITH EMPLOYEES - PAYROLL INTAKE FORM
 EMPLOYER WITH EMPLOYEES - PAYROLL INTAKE FORM CONTACT INFORMATION Payroll Client (First, Last): Phone #: ( ) - Legal Business Name: Business DBA (If Applicable): Business Type: LLC Partnership Corp S-Corp
EMPLOYER WITH EMPLOYEES - PAYROLL INTAKE FORM CONTACT INFORMATION Payroll Client (First, Last): Phone #: ( ) - Legal Business Name: Business DBA (If Applicable): Business Type: LLC Partnership Corp S-Corp
Employment Application
 Print Name (First, ( M., Last): Employment Application PERSONAL INFORMATION Date: Street Address: Apt. Unit/# Home Phone: City State Zip Cell Phone: Email Address: Are you authorized to work in the U.S.?
Print Name (First, ( M., Last): Employment Application PERSONAL INFORMATION Date: Street Address: Apt. Unit/# Home Phone: City State Zip Cell Phone: Email Address: Are you authorized to work in the U.S.?
TTC Form T3-107) ct Deposit (TTC Form T3-21)
 ct Deposit (TTC Form T3-21)") TO: Adjunct Instructor FROM: Human Resources, Fredric Yeadon (843-574-6825) RE: Adjunct Instructor Packet Welcome to Trident Technical College! Please complete the following paperwork before reporting
TO: Adjunct Instructor FROM: Human Resources, Fredric Yeadon (843-574-6825) RE: Adjunct Instructor Packet Welcome to Trident Technical College! Please complete the following paperwork before reporting
Personal Data Form. UIN#: Dr. Mr. Mrs. Ms. Last Name: First Name: Middle Initial:
 Personal Data Form UIN#: Dr. Mr. Mrs. Ms. Last Name: First Name: Middle Initial: Preferred Name (if different than above): Social Security Number: Mailing Address (same as W4): City: Zip/Postal Code: Permanent
Personal Data Form UIN#: Dr. Mr. Mrs. Ms. Last Name: First Name: Middle Initial: Preferred Name (if different than above): Social Security Number: Mailing Address (same as W4): City: Zip/Postal Code: Permanent
Personal Data Form. UIN#: Dr. Mr. Mrs. Ms. Last Name: First Name: Middle Initial:
 Personal Data Form UIN#: Dr. Mr. Mrs. Ms. Last Name: First Name: Middle Initial: Preferred Name (if different than above): Social Security Number: Mailing Address (same as W4): City: Zip/Postal Code: Permanent
Personal Data Form UIN#: Dr. Mr. Mrs. Ms. Last Name: First Name: Middle Initial: Preferred Name (if different than above): Social Security Number: Mailing Address (same as W4): City: Zip/Postal Code: Permanent
 Form W-4 (2018) Future developments. For the latest information about any future developments related to Form W-4, such as legislation enacted after it was published, go to www.irs.gov/formw4. Purpose.
Form W-4 (2018) Future developments. For the latest information about any future developments related to Form W-4, such as legislation enacted after it was published, go to www.irs.gov/formw4. Purpose.
Personal Data Form. UIN#: Dr. Mr. Mrs. Ms. Last Name: First Name: Middle Initial:
 Personal Data Form UIN#: Dr. Mr. Mrs. Ms. Last Name: First Name: Middle Initial: Preferred Name (if different than above): Social Security Number: Mailing Address (same as W4): City: Zip/Postal Code: Permanent
Personal Data Form UIN#: Dr. Mr. Mrs. Ms. Last Name: First Name: Middle Initial: Preferred Name (if different than above): Social Security Number: Mailing Address (same as W4): City: Zip/Postal Code: Permanent
A - EMPLOYEE INFORMATION SUBMISSION AND CERTIFICATION
 Office/Client Number New Employee Packet Employer Information: Choose your option for submitting employee information. For detailed instructions for these options, refer to the PEO New Employee Packet
Office/Client Number New Employee Packet Employer Information: Choose your option for submitting employee information. For detailed instructions for these options, refer to the PEO New Employee Packet
Blank Forms (Volume 1)
") Blank Forms (Volume 1) These forms are provided for congregational use and may be copied. Payroll Congregational Payroll Information Employment Eligibility Verification (I-9) Payroll Authorization Form
Blank Forms (Volume 1) These forms are provided for congregational use and may be copied. Payroll Congregational Payroll Information Employment Eligibility Verification (I-9) Payroll Authorization Form
CDS Participant's New Attendant Check List
 CDS Participant's New Attendant Check List Participant : The person receiving care through the Medicaid-funded program Consumer Directed Services (CDS). This person is the employer of the attendant. May
CDS Participant's New Attendant Check List Participant : The person receiving care through the Medicaid-funded program Consumer Directed Services (CDS). This person is the employer of the attendant. May
We (The Jeffrey Corporation) are making you a contingent job offer to work at Burger King Store #.
 are making you a contingent job offer to work at Burger King Store #.") Date Dear Applicant, We (The Jeffrey Corporation) are making you a contingent job offer to work at Burger King Store #. Part of the hiring/re-hiring process requires that we verify your eligibility to
Date Dear Applicant, We (The Jeffrey Corporation) are making you a contingent job offer to work at Burger King Store #. Part of the hiring/re-hiring process requires that we verify your eligibility to
INSTRUCTIONS FOR COMPLETING NEW HIRE PAPERWORK
 INSTRUCTIONS FOR COMPLETING NEW HIRE PAPERWORK **DO NOT PRINT DOUBLE SIDED ** USE BLUE OR BLACK INK ONLY 1. ADDITIONAL INFORMATION SHEET: Must be LEGIBLE. PLEASE PRINT. Make sure that you have checked
INSTRUCTIONS FOR COMPLETING NEW HIRE PAPERWORK **DO NOT PRINT DOUBLE SIDED ** USE BLUE OR BLACK INK ONLY 1. ADDITIONAL INFORMATION SHEET: Must be LEGIBLE. PLEASE PRINT. Make sure that you have checked
Store# Name (First, Middle, Last) SSN # Date of Birth. City State Zip. Hire Date Position Rate of pay/annual Salary. Select... Rehire.
 SSN # Date of Birth. City State Zip. Hire Date Position Rate of pay/annual Salary. Select... Rehire.") Store# Name (First, Middle, Last) SSN # Date of Birth Address Apt/Lot City State Zip Hire Date Position Rate of pay/annual Salary Rehire nmlkj Yes nmlkj No Select... Native American If yes, please list
Store# Name (First, Middle, Last) SSN # Date of Birth Address Apt/Lot City State Zip Hire Date Position Rate of pay/annual Salary Rehire nmlkj Yes nmlkj No Select... Native American If yes, please list
SURRENDER REQUEST FORM. Policy Number: Insured:
 SURRENDER REQUEST FORM Section A Policy Information (You Must Complete This Section) Policy Number: Insured: (First Name) (Last Name) Sec tion B Surrender Request and Withholding Election (You Must Complete
SURRENDER REQUEST FORM Section A Policy Information (You Must Complete This Section) Policy Number: Insured: (First Name) (Last Name) Sec tion B Surrender Request and Withholding Election (You Must Complete
How Do I Adjust My Tax Withholding?
 Contents Department of the Treasury Internal Revenue Service What s New for 2011... 2 Reminder.... Publication 919 Introduction... 3 Cat. No. 63900P How Do I Adjust My Tax Withholding? Checking Your Withholding...
Contents Department of the Treasury Internal Revenue Service What s New for 2011... 2 Reminder.... Publication 919 Introduction... 3 Cat. No. 63900P How Do I Adjust My Tax Withholding? Checking Your Withholding...
2017 New Hire Forms Directions & Resources
 2017 New Hire Forms Directions & Resources Federal W4 Forms Complete form; filling in all spaces in sections 1-7, remembering to sign and date form. State W4 Forms Complete Employee Withholding Allowance
2017 New Hire Forms Directions & Resources Federal W4 Forms Complete form; filling in all spaces in sections 1-7, remembering to sign and date form. State W4 Forms Complete Employee Withholding Allowance
TYPE OF APPLICATION (select one): PERSONAL ASSISTANT COMMUNITY SPECIALIST SUPPORT BROKER
: PERSONAL ASSISTANT COMMUNITY SPECIALIST SUPPORT BROKER") Missouri Self-Directed Supports EMPLOYEE APPLICATION Based on the pre-employment information you provided, we have pre-populated this application and most of the forms included in your enrollment packet.
Missouri Self-Directed Supports EMPLOYEE APPLICATION Based on the pre-employment information you provided, we have pre-populated this application and most of the forms included in your enrollment packet.
BRIDGEWATER STATE UNIVERSITY. Preferred Name*: (if applicable)
") BRIDGEWATER STATE UNIVERSITY First Name: Last Name: ------ --+----------------------~ Middle Name: Preferred Name*: (if applicable) -------- Date of Birth: Social Security Number: ------J ' Marital status:
BRIDGEWATER STATE UNIVERSITY First Name: Last Name: ------ --+----------------------~ Middle Name: Preferred Name*: (if applicable) -------- Date of Birth: Social Security Number: ------J ' Marital status:
MAYOR BYRON W. BROWN S SUMMER YOUTH INTERNSHIP PROGRAM APPLICATION
 MAYOR BYRON W. BROWN S SUMMER YOUTH INTERNSHIP PROGRAM February 1, 2018 Dear Applicant: Thank you for your interest in applying for my 2018 Summer Youth Internship Program. This is truly a wonderful opportunity
MAYOR BYRON W. BROWN S SUMMER YOUTH INTERNSHIP PROGRAM February 1, 2018 Dear Applicant: Thank you for your interest in applying for my 2018 Summer Youth Internship Program. This is truly a wonderful opportunity
Personal Data Form. UIN#: Dr. Mr. Mrs. Ms. Last Name: First Name: Middle Initial:
 Personal Data Form UIN#: Dr. Mr. Mrs. Ms. Last Name: First Name: Middle Initial: Preferred Name (if different than above): Social Security Number: Mailing Address (same as W4): City: Zip/Postal Code: Permanent
Personal Data Form UIN#: Dr. Mr. Mrs. Ms. Last Name: First Name: Middle Initial: Preferred Name (if different than above): Social Security Number: Mailing Address (same as W4): City: Zip/Postal Code: Permanent
Separate here and give Form W-4 to your employer. Keep the worksheet(s) for your records. Employee s Withholding Allowance Certificate
 for your records. Employee s Withholding Allowance Certificate") Form W-4 (2018) Future developments. For the latest information about any future developments related to Form W-4, such as legislation enacted after it was published, go to www.irs.gov/formw4. Purpose.
Form W-4 (2018) Future developments. For the latest information about any future developments related to Form W-4, such as legislation enacted after it was published, go to www.irs.gov/formw4. Purpose.
P E N N S Y L V A N I A Application for Payment of Medicare Premiums, Coinsurance and Deductibles
 P E N N S Y L V A N I A Application for Payment of Medicare Premiums, Coinsurance and Deductibles If you have a disability and need this form in large print or another format, please call our helpline
P E N N S Y L V A N I A Application for Payment of Medicare Premiums, Coinsurance and Deductibles If you have a disability and need this form in large print or another format, please call our helpline
Decatur County Schools
 Decatur County Schools 100 West Street Bainbridge, Georgia 39817 (229) 248-2200 Fax (229) 248-2252 This application will remain active for one year from date received unless requested to reactivate after
Decatur County Schools 100 West Street Bainbridge, Georgia 39817 (229) 248-2200 Fax (229) 248-2252 This application will remain active for one year from date received unless requested to reactivate after
TENNESSEE CONSOLIDATED RETIREMENT SYSTEM 502 Deaderick Street Nashville, Tennessee
 Retirement Application for Service or Early Retirement Benefits TENNESSEE CONSOLIDATED RETIREMENT SYSTEM 502 Deaderick Street Nashville, Tennessee 37243-0201 1-800-770-8277 http://tcrs.tn.gov Refer to
Retirement Application for Service or Early Retirement Benefits TENNESSEE CONSOLIDATED RETIREMENT SYSTEM 502 Deaderick Street Nashville, Tennessee 37243-0201 1-800-770-8277 http://tcrs.tn.gov Refer to
The New Hire Orientation Packet
 The New Hire Orientation Packet www.beesteelinc.com Workplace Conduct Policy Policy Statement Bee Steel is committed to providing a healthy and safe working environment. Bee Steel believes that is employees,
The New Hire Orientation Packet www.beesteelinc.com Workplace Conduct Policy Policy Statement Bee Steel is committed to providing a healthy and safe working environment. Bee Steel believes that is employees,
OCCUPATIONAL TAX CERTIFICATE
 CITY OF JONESBORO 124 North Avenue Jonesboro, Georgia 30236 City Hall: (770) 478-3800 Fax: (770) 478-3775 www.jonesboroga.com OCCUPATIONAL TAX CERTIFICATE APPLICATION ATTACH ADDITIONAL PAGES IF NECCESSARY.
CITY OF JONESBORO 124 North Avenue Jonesboro, Georgia 30236 City Hall: (770) 478-3800 Fax: (770) 478-3775 www.jonesboroga.com OCCUPATIONAL TAX CERTIFICATE APPLICATION ATTACH ADDITIONAL PAGES IF NECCESSARY.
Employee Data Sheet NAME. Title: Dr. Mr. Ms. Mrs. Miss First: Middle: Last: Suffix: CONTACT INFORMATION
 Employee Data Sheet Social Security #: Today s Date: NAME Title: Dr. Mr. Ms. Mrs. Miss First: Middle: Last: Suffix: CONTACT INFORMATION Address: Apt/Unit #: City: State: Zip Code: County: Home Phone (include
Employee Data Sheet Social Security #: Today s Date: NAME Title: Dr. Mr. Ms. Mrs. Miss First: Middle: Last: Suffix: CONTACT INFORMATION Address: Apt/Unit #: City: State: Zip Code: County: Home Phone (include
SUPPLEMENTAL INFORMATION. Spouse Information Form
 SUPPLEMENTAL INFORMATION Spouse Information Form NJ FamilyCare Aged, Blind, Disabled Programs SECTION 1 Applicant 2 (Spouse) STATE of NEW JERSEY Department of Human Services Division of Medical Assistance
SUPPLEMENTAL INFORMATION Spouse Information Form NJ FamilyCare Aged, Blind, Disabled Programs SECTION 1 Applicant 2 (Spouse) STATE of NEW JERSEY Department of Human Services Division of Medical Assistance
Personal Data Form. UIN#: Dr. Mr. Mrs. Ms. Last Name: First Name: Middle Initial:
 Personal Data Form UIN#: Dr. Mr. Mrs. Ms. Last Name: First Name: Middle Initial: Preferred Name (if different than above): Social Security Number: Mailing Address (same as W4): City: Zip/Postal Code: Permanent
Personal Data Form UIN#: Dr. Mr. Mrs. Ms. Last Name: First Name: Middle Initial: Preferred Name (if different than above): Social Security Number: Mailing Address (same as W4): City: Zip/Postal Code: Permanent
TENNESSEE CONSOLIDATED RETIREMENT SYSTEM 502 Deaderick Street Nashville, Tennessee (615)
") Retirement Application for Disability Benefits TENNESSEE CONSOLIDATED RETIREMENT SYSTEM 502 Deaderick Street Nashville, Tennessee 37243-0201 1-800-770-8277 (615) 253-8693 http://tcrs.tn.gov Refer to pages
Retirement Application for Disability Benefits TENNESSEE CONSOLIDATED RETIREMENT SYSTEM 502 Deaderick Street Nashville, Tennessee 37243-0201 1-800-770-8277 (615) 253-8693 http://tcrs.tn.gov Refer to pages
Chapter 7: Payroll and Other Information Returns
 Chapter 7: Payroll and Other Information Returns INTRODUCTION 100 Characteristics of Employees/Self-Employed 105 Status of Congregational Workers 110 Employee s File 115 Minister of the Gospel 120 CAFETERIA
Chapter 7: Payroll and Other Information Returns INTRODUCTION 100 Characteristics of Employees/Self-Employed 105 Status of Congregational Workers 110 Employee s File 115 Minister of the Gospel 120 CAFETERIA
APPLICATION SCREENING COVER NOTICE
 APPLICATION SCREENING COVER NOTICE An application fee of $25.00 is charged per person. NO CASH PLEASE (check or money order only). The application fee covers the cost of checking landlord, credit, employment
APPLICATION SCREENING COVER NOTICE An application fee of $25.00 is charged per person. NO CASH PLEASE (check or money order only). The application fee covers the cost of checking landlord, credit, employment
SPORT CLIPS PAYROLL INFORMATION FORM CLIENT NAME: TO BE COMPLETED BY EMPLOYEE: Employee Name: Employee
 SPORT CLIPS PAYROLL INFORMATION FORM CLIENT NAME: TO BE COMPLETED BY EMPLOYEE: Employee Name: Employee Email: Local Tax (IF APPLICABLE): SSN: City or County Township or Borough School District PA EMST:
SPORT CLIPS PAYROLL INFORMATION FORM CLIENT NAME: TO BE COMPLETED BY EMPLOYEE: Employee Name: Employee Email: Local Tax (IF APPLICABLE): SSN: City or County Township or Borough School District PA EMST:
Person ID Name. Job Code
 REQUEST FOR PERSONNEL ACTION ACTION REQUESTED FOR POSITION (Please check the box to the left of the action you are requesting): New Position Modify (Change) Position Continue Current Position Delimit Assignment
REQUEST FOR PERSONNEL ACTION ACTION REQUESTED FOR POSITION (Please check the box to the left of the action you are requesting): New Position Modify (Change) Position Continue Current Position Delimit Assignment
CDL DRIVER NEW EMPLOYEE PACK
 CDL DRIVER NEW EMPLOYEE PACK For questions or additional assistance with completing your paperwork, please reach out to: Alice Paul, HR Assistant 8 0 0-8 7 3-5 0 5 9 x 1 8 9 a p a u l @ a i m n t l s.
CDL DRIVER NEW EMPLOYEE PACK For questions or additional assistance with completing your paperwork, please reach out to: Alice Paul, HR Assistant 8 0 0-8 7 3-5 0 5 9 x 1 8 9 a p a u l @ a i m n t l s.
APPLICATION PACKET. Please read pages 1 through 6 for some important things you ll need to know before you apply.
 DEPARTMENT OF HEALTH AND FAMILY SERVICES Division of Health Care Access and Accountability HCF 10182 (02/08) STATE OF WISCONSIN APPLICATION PACKET Please read pages 1 through 6 for some important things
DEPARTMENT OF HEALTH AND FAMILY SERVICES Division of Health Care Access and Accountability HCF 10182 (02/08) STATE OF WISCONSIN APPLICATION PACKET Please read pages 1 through 6 for some important things
Application for Service or Early Retirement Benefits
 Application for Service or Early Retirement Benefits Tennessee Consolidated Retirement System 502 Deaderick Street Nashville, Tennessee 37243-0201 1-800-922-7772 RetireReadyTN.gov Do NOT complete this
Application for Service or Early Retirement Benefits Tennessee Consolidated Retirement System 502 Deaderick Street Nashville, Tennessee 37243-0201 1-800-922-7772 RetireReadyTN.gov Do NOT complete this
NEW EMPLOYEE PACK STATUS: MANAGERS/SUPERVISORS. For questions or additional assistance with completing your paperwork, please reach out to:
 NEW EMPLOYEE PACK STATUS: MANAGERS/SUPERVISORS For questions or additional assistance with completing your paperwork, please reach out to: Alice Paul, HR Assistant 8 0 0-8 7 3-5 0 5 9 x 1 8 9 a p a u l
NEW EMPLOYEE PACK STATUS: MANAGERS/SUPERVISORS For questions or additional assistance with completing your paperwork, please reach out to: Alice Paul, HR Assistant 8 0 0-8 7 3-5 0 5 9 x 1 8 9 a p a u l
Employee Data Sheet NAME. Title: Dr. Mr. Ms. Mrs. Miss First: Middle: Last: Suffix: CONTACT INFORMATION
 Employee Data Sheet Social Security #: Today s Date: NAME Title: Dr. Mr. Ms. Mrs. Miss First: Middle: Last: Suffix: CONTACT INFORMATION Address: Apt/Unit #: City: State: Zip Code: County: Home Phone (include
Employee Data Sheet Social Security #: Today s Date: NAME Title: Dr. Mr. Ms. Mrs. Miss First: Middle: Last: Suffix: CONTACT INFORMATION Address: Apt/Unit #: City: State: Zip Code: County: Home Phone (include
APPLICATION CHECKLIST
 PERF/TRF RETIREMENT APPLICATION State Form 945 (R30 / 2-15) Approved by State Board of Accounts, 2015 INDIANA PUBLIC RETIREMENT SYSTEM Telephone: (888) 286-3544 (Toll-free) Web site: www.inprs.in.gov Use
PERF/TRF RETIREMENT APPLICATION State Form 945 (R30 / 2-15) Approved by State Board of Accounts, 2015 INDIANA PUBLIC RETIREMENT SYSTEM Telephone: (888) 286-3544 (Toll-free) Web site: www.inprs.in.gov Use
PERSONAL INFORMATION: You may have someone help you complete this application. Address. Birthdate Sex Race U.S. Citizen (Yes or No)
") Georgia Application for Medicaid & Medicare Savings for Qualified Beneficiaries (QMB - payment of premiums, coinsurance, and deductibles; SLMB - payment of Part B premium; and QI-1 - payment of Part B
Georgia Application for Medicaid & Medicare Savings for Qualified Beneficiaries (QMB - payment of premiums, coinsurance, and deductibles; SLMB - payment of Part B premium; and QI-1 - payment of Part B
HS-0169 revised 01/13
 Tennessee Department of Human Services Family Assistance Application THIS BOX DHS USE ONLY Case #: Date received: County: We will take your application with only your name, address, and signature. However,
Tennessee Department of Human Services Family Assistance Application THIS BOX DHS USE ONLY Case #: Date received: County: We will take your application with only your name, address, and signature. However,
Medical Assistance (Medicaid) Financial Eligibility Application for Long Term Care, Supports and Services
 Financial Eligibility Application for Long Term Care, Supports and Services") Check any that you are applying for: Medical Assistance (Medicaid) Financial Eligibility Application for Long Term Care, Supports and Services You may also apply online at www.compass.state.pa.us Care
Check any that you are applying for: Medical Assistance (Medicaid) Financial Eligibility Application for Long Term Care, Supports and Services You may also apply online at www.compass.state.pa.us Care
LONG-TERM RENTAL APPLICATION
 p LONG-TERM RENTAL APPLICATION For approval on APCHA-managed units, W2 s, 1099 s and/or Employment History Report from the Social Security Office may be required. THE FOLLOWING MUST BE SUBMITTED FOR ANYONE
p LONG-TERM RENTAL APPLICATION For approval on APCHA-managed units, W2 s, 1099 s and/or Employment History Report from the Social Security Office may be required. THE FOLLOWING MUST BE SUBMITTED FOR ANYONE
PPL s Payroll Service- MA DDS Autism Waiver Program
 Public Partnerships, LLC (PPL) Agency Payroll Department One Cabot rd. STE 102 Medford, MA 02155 Phone 1-866-315-3740 Admin Fax 1-866-578-0533 TS Fax 1-866-578-0536 STEP ONE - SETTING UP AN EMPLOYER ACCOUNT
Public Partnerships, LLC (PPL) Agency Payroll Department One Cabot rd. STE 102 Medford, MA 02155 Phone 1-866-315-3740 Admin Fax 1-866-578-0533 TS Fax 1-866-578-0536 STEP ONE - SETTING UP AN EMPLOYER ACCOUNT
Instructions for Contract Between Sponsor and Household Member
 Instructions for Contract Between Sponsor and Household Member Department of Homeland Security U.S. Citizenship and Immigration Services USCIS Form I-864A OMB No. 1615-0075 Expires 03/31/2020 What Is the
Instructions for Contract Between Sponsor and Household Member Department of Homeland Security U.S. Citizenship and Immigration Services USCIS Form I-864A OMB No. 1615-0075 Expires 03/31/2020 What Is the
Medical Assistance (Medicaid) Financial Eligibility Application for Long Term Care, Supports and Services
 Financial Eligibility Application for Long Term Care, Supports and Services") Medical Assistance (Medicaid) Financial Eligibility Application for Long Term Care, Supports and Services You may also apply online at www.compass.state.pa.us Check any that you are applying for: Care
Medical Assistance (Medicaid) Financial Eligibility Application for Long Term Care, Supports and Services You may also apply online at www.compass.state.pa.us Check any that you are applying for: Care
DEPARTMENT OF HUMAN RESOURCES FAMILY INVESTMENT ADMINISTRATION Assistance Request
 DEPARTMENT OF HUMAN RESOURCES FAMILY INVESTMENT ADMINISTRATION Assistance Request The Family Investment Administration is committed to providing access, and reasonable accommodation in its services, programs,
DEPARTMENT OF HUMAN RESOURCES FAMILY INVESTMENT ADMINISTRATION Assistance Request The Family Investment Administration is committed to providing access, and reasonable accommodation in its services, programs,
Last Name First Name Middle. Address Number & Street City State Zip Code. Date of Birth Applicant Co-applicant / / / / Month Day Year Month Day Year
 PARKVIEW APARTMENTS HOUSING APPLICATION Mr. Ms. Miss Date: Mrs. Mr. & Mrs. Last Name First Name Middle Address Number & Street City State Zip Code ( ) ( ) Home Phone Number Alternate Contact Number How
PARKVIEW APARTMENTS HOUSING APPLICATION Mr. Ms. Miss Date: Mrs. Mr. & Mrs. Last Name First Name Middle Address Number & Street City State Zip Code ( ) ( ) Home Phone Number Alternate Contact Number How
ONLINE APPLICATION. After receiving your application, what is the best way for us to contact you?
 ONLINE APPLICATION To apply for a new apartment home at Park Trace, please fill out the application and credit card authorization. You may print, sign and send it to our office via: Fax: (770) 242-9018
ONLINE APPLICATION To apply for a new apartment home at Park Trace, please fill out the application and credit card authorization. You may print, sign and send it to our office via: Fax: (770) 242-9018
Swiftwater/Wildland Application Checklist
 Mountain View Fire and Rescue KING COUNTY FIRE PROTECTION DISTRICT 44 32316 148 AVE SE Auburn, WA 98092 / (253) 735-0284; FAX (253) 735 0287 Swiftwater/Wildland Application Checklist Application complete
Mountain View Fire and Rescue KING COUNTY FIRE PROTECTION DISTRICT 44 32316 148 AVE SE Auburn, WA 98092 / (253) 735-0284; FAX (253) 735 0287 Swiftwater/Wildland Application Checklist Application complete
INSTRUCTIONS FOR COMPLETING NEW HIRE PAPERWORK
 INSTRUCTIONS FOR COMPLETING NEW HIRE PAPERWORK 1. EMPLOYMENT AFTER RETIREMENT ACKNOWLEDGEMENT FORM o Please read and sign the acknowledgment form agreeing to read the Teacher Retirement System of Texas
INSTRUCTIONS FOR COMPLETING NEW HIRE PAPERWORK 1. EMPLOYMENT AFTER RETIREMENT ACKNOWLEDGEMENT FORM o Please read and sign the acknowledgment form agreeing to read the Teacher Retirement System of Texas