SPORT CLIPS PAYROLL INFORMATION FORM CLIENT NAME: TO BE COMPLETED BY EMPLOYEE: Employee Name: Employee
|
|
|
- Madlyn Morton
- 6 years ago
- Views:
Transcription

1 SPORT CLIPS PAYROLL INFORMATION FORM CLIENT NAME: TO BE COMPLETED BY EMPLOYEE: Employee Name: Employee Local Tax (IF APPLICABLE): SSN: City or County Township or Borough School District PA EMST: if already paid for current year, please provide receipt. VOLUNTARY INFORMATION (Used for EEOC reporting only) AFFIRMATIVE ACTION/EEO INFORMATION: Gender: Female Male Race: Hispanic or Latino Asian White American Indian or Alaskan Native Black or African American Two or More Races (not Hispanic or Native Hawaiian or Pacific Islander Latino) Please check the appropriate box and write in name, etc. Where was the New Team Member previously? Other Chain: Name Private Salon Name Beauty School Name Moved to the area. From: How did the New Team Member come to Sport Clips? Classified Ad: Which paper? Post Card Friend or Family: Who? Walk-by TV or radio Ad: Which one? Beauty School Presentation: Which school? Other (Explain) TO BE COMPLETED BY CLIENT COMPANY: 1. Hire Date: Rehire Date: (Requires current W-4) 2. Pay Frequency: Weekly Bi-Weekly Semi-monthly Monthly 3. Job Status: Full-time Part-time 4. Salary Rate OR Hourly Rate 5. Job Description/Title Department (if applicable) 6. Workers Comp Code PPEOC USE ONLY Payroll Information Form Employee Information Form W-4 I-9 Verified by State Withholding Form (If Applicable) Voluntary Substance Testing Form Statement of Understanding Date
2 PINNACLE PEO EMPLOYEE INFORMATION FORM Pinnacle PEO Corp. is an at-will employer INSTRUCTIONS: 1. Please read NOTE below 3. Continue on the back if more space is needed to complete any question. 2. Complete all questions 4. Print clearly. Incomplete or illegible applications will not be processed. Date: Name: Social Security Number: Last First Middle Initial Maiden Home Phone: Work Phone: Current Address: Prior Address: Emergency Contact: Phone: NOTE: Please answer all appropriate questions completely and to the best of your ability. False or misleading statements are grounds for refusal or termination of employment and benefits. Federal law provides penalties for false statements or documents related to United States employment eligibility. All qualified applicants will receive consideration without discrimination because of sex, marital status, race, age, creed, national origin or the presence of non job-related handicaps, and such information may be omitted from this form. A felony conviction will not necessarily bar the applicant from employment. Affirmative action hiring of handicapped individuals, disabled or Vietnam-era veterans, minorities and women may be requested by qualified applicants. Additional testing of job-related skills, mental/physical condition and for the presence of drugs in your body may be required before employment. AVAILABILITY: For which position are you applying? EXPERIENCE: Please put most recent employer first. Most Recent Employer: Name of Employer Name of Employer Address Address Address City, State, Zip City, State, Zip City, State, Zip Telephone Telephone Telephone Supervisor May We Contact? Supervisor May We Contact? Supervisor May We Contact? Date Employed Salary/Pay Rate Date Employed Salary/Pay Rate Date Employed Salary/Pay Rate Start End Start End Start End Start End Start End Start End Position/Duties: Warehouse Helper Position/Duties: Position/Duties: SECURITY: In which states have you lived in the past seven years? Have you used another name(s) or social security number other than those on this form? Have you been convicted, or pled guilty or no contest to a felony? Yes No Do you regularly take any prescription medication or drugs which may affect your job performance or safety? Yes No Have you ever been injured on the job or received workers compensation benefits? Yes No (Will not be used for purposes of discrimination) Please provide details REFERENCES: Include only individuals familiar with your work ability. Do not include relatives. Name Address/Phone Years Known/Relationship CERTIFICATION AND RELEASE: I certify that I have read and understand the note on this page and that the answers given by me to the foregoing questions and statements made by me are complete and true to the best of my knowledge and belief. I understand that any false information, omissions or misrepresentations of facts called for in this application may result in rejection of my application or discharge at any time during my employment. I authorize the company and its agents including consumer reporting bureaus to verify any of this information including, but not limited to, criminal history and motor vehicle records. I authorize all persons, schools, companies and law enforcement authorities to release any information concerning my background and hereby release any said persons, schools, companies and law enforcement authorities from any liabilities for any damage whatsoever for issuing this information. I also understand that the use of illegal drugs is prohibited during employment. If company policy requires, I am willing to submit to drug testing to detect the use of illegal drugs before and during employment. Signed Date
3 Form W-4 (2012) Purpose. Complete Form W-4 so that your employer can withhold the correct federal income tax from your pay. Consider completing a new Form W-4 each year and when your personal or financial situation changes. Exemption from withholding. If you are exempt, complete only lines 1, 2, 3, 4, and 7 and sign the form to validate it. Your exemption for 2012 expires February 18, See Pub. 505, Tax Withholding and Estimated Tax. Note. If another person can claim you as a dependent on his or her tax return, you cannot claim exemption from withholding if your income exceeds $950 and includes more than $300 of unearned income (for example, interest and dividends). Basic instructions. If you are not exempt, complete the Personal Allowances Worksheet below. The worksheets on page 2 further adjust your withholding allowances based on itemized deductions, certain credits, adjustments to income, or two-earners/multiple jobs situations. Complete all worksheets that apply. However, you may claim fewer (or zero) allowances. For regular wages, withholding must be based on allowances you claimed and may not be a flat amount or percentage of wages. Head of household. Generally, you can claim head of household filing status on your tax return only if you are unmarried and pay more than 50% of the costs of keeping up a home for yourself and your dependent(s) or other qualifying individuals. See Pub. 501, Exemptions, Standard Deduction, and Filing Information, for information. Tax credits. You can take projected tax credits into account in figuring your allowable number of withholding allowances. Credits for child or dependent care expenses and the child tax credit may be claimed using the Personal Allowances Worksheet below. See Pub. 505 for information on converting your other credits into withholding allowances. Nonwage income. If you have a large amount of nonwage income, such as interest or dividends, consider making estimated tax payments using Form 1040-ES, Estimated Tax for Individuals. Otherwise, you may owe additional tax. If you have pension or annuity income, see Pub. 505 to find out if you should adjust your withholding on Form W-4 or W-4P. Two earners or multiple jobs. If you have a working spouse or more than one job, figure the total number of allowances you are entitled to claim on all jobs using worksheets from only one Form W-4. Your withholding usually will be most accurate when all allowances are claimed on the Form W-4 for the highest paying job and zero allowances are claimed on the others. See Pub. 505 for details. Nonresident alien. If you are a nonresident alien, see Notice 1392, Supplemental Form W-4 Instructions for Nonresident Aliens, before completing this form. Check your withholding. After your Form W-4 takes effect, use Pub. 505 to see how the amount you are having withheld compares to your projected total tax for See Pub. 505, especially if your earnings exceed $130,000 (Single) or $180,000 (Married). Future developments. The IRS has created a page on IRS.gov for information about Form W-4, at Information about any future developments affecting Form W-4 (such as legislation enacted after we release it) will be posted on that page. Personal Allowances Worksheet (Keep for your records.) A Enter 1 for yourself if no one else can claim you as a dependent A You are single and have only one job; or B Enter 1 if: { You are married, have only one job, and your spouse does not work; or... B Your wages from a second job or your spouse s wages (or the total of both) are $1,500 or less. C Enter 1 for your spouse. But, you may choose to enter -0- if you are married and have either a working spouse or more than one job. (Entering -0- may help you avoid having too little tax withheld.) C D Enter number of dependents (other than your spouse or yourself) you will claim on your tax return D E Enter 1 if you will file as head of household on your tax return (see conditions under Head of household above).. E F Enter 1 if you have at least $1,900 of child or dependent care expenses for which you plan to claim a credit... F (Note. Do not include child support payments. See Pub. 503, Child and Dependent Care Expenses, for details.) G Child Tax Credit (including additional child tax credit). See Pub. 972, Child Tax Credit, for more information. If your total income will be less than $61,000 ($90,000 if married), enter 2 for each eligible child; then less 1 if you have three to seven eligible children or less 2 if you have eight or more eligible children. If your total income will be between $61,000 and $84,000 ($90,000 and $119,000 if married), enter 1 for each eligible child... G H Add lines A through G and enter total here. (Note. This may be different from the number of exemptions you claim on your tax return.) H { If you plan to itemize or claim adjustments to income and want to reduce your withholding, see the Deductions For accuracy, and Adjustments Worksheet on page 2. complete all If you are single and have more than one job or are married and you and your spouse both work and the combined worksheets earnings from all jobs exceed $40,000 ($10,000 if married), see the Two-Earners/Multiple Jobs Worksheet on page 2 to that apply. avoid having too little tax withheld. If neither of the above situations applies, stop here and enter the number from line H on line 5 of Form W-4 below. Form W-4 Department of the Treasury Internal Revenue Service Separate here and give Form W-4 to your employer. Keep the top part for your records. Employee's Withholding Allowance Certificate Whether you are entitled to claim a certain number of allowances or exemption from withholding is subject to review by the IRS. Your employer may be required to send a copy of this form to the IRS. 1 Your first name and middle initial Last name OMB No Your social security number Home address (number and street or rural route) 3 Single Married Married, but withhold at higher Single rate. Note. If married, but legally separated, or spouse is a nonresident alien, check the Single box. City or town, state, and ZIP code 4 If your last name differs from that shown on your social security card, check here. You must call for a replacement card. 5 Total number of allowances you are claiming (from line H above or from the applicable worksheet on page 2) 5 6 Additional amount, if any, you want withheld from each paycheck $ 7 I claim exemption from withholding for 2012, and I certify that I meet both of the following conditions for exemption. Last year I had a right to a refund of all federal income tax withheld because I had no tax liability, and This year I expect a refund of all federal income tax withheld because I expect to have no tax liability. If you meet both conditions, write Exempt here Under penalties of perjury, I declare that I have examined this certificate and, to the best of my knowledge and belief, it is true, correct, and complete. Employee s signature (This form is not valid unless you sign it.) Date 8 Employer s name and address (Employer: Complete lines 8 and 10 only if sending to the IRS.) 9 Office code (optional) 10 Employer identification number (EIN) For Privacy Act and Paperwork Reduction Act Notice, see page 2. Cat. No Q Form W-4 (2012)
4 Form W-4 (2012) Page 2 Deductions and Adjustments Worksheet Note. Use this worksheet only if you plan to itemize deductions or claim certain credits or adjustments to income. 1 Enter an estimate of your 2012 itemized deductions. These include qualifying home mortgage interest, charitable contributions, state and local taxes, medical expenses in excess of 7.5% of your income, and miscellaneous deductions $ $11,900 if married filing jointly or qualifying widow(er) 2 Enter: { $8,700 if head of household } $ $5,950 if single or married filing separately 3 Subtract line 2 from line 1. If zero or less, enter $ 4 Enter an estimate of your 2012 adjustments to income and any additional standard deduction (see Pub. 505) 4 $ 5 Add lines 3 and 4 and enter the total. (Include any amount for credits from the Converting Credits to Withholding Allowances for 2012 Form W-4 worksheet in Pub. 505.) $ 6 Enter an estimate of your 2012 nonwage income (such as dividends or interest) $ 7 Subtract line 6 from line 5. If zero or less, enter $ 8 Divide the amount on line 7 by $3,800 and enter the result here. Drop any fraction Enter the number from the Personal Allowances Worksheet, line H, page Add lines 8 and 9 and enter the total here. If you plan to use the Two-Earners/Multiple Jobs Worksheet, also enter this total on line 1 below. Otherwise, stop here and enter this total on Form W-4, line 5, page 1 10 Two-Earners/Multiple Jobs Worksheet (See Two earners or multiple jobs on page 1.) Note. Use this worksheet only if the instructions under line H on page 1 direct you here. 1 Enter the number from line H, page 1 (or from line 10 above if you used the Deductions and Adjustments Worksheet) 1 2 Find the number in Table 1 below that applies to the LOWEST paying job and enter it here. However, if you are married filing jointly and wages from the highest paying job are $65,000 or less, do not enter more than If line 1 is more than or equal to line 2, subtract line 2 from line 1. Enter the result here (if zero, enter -0- ) and on Form W-4, line 5, page 1. Do not use the rest of this worksheet Note. If line 1 is less than line 2, enter -0- on Form W-4, line 5, page 1. Complete lines 4 through 9 below to figure the additional withholding amount necessary to avoid a year-end tax bill. 4 Enter the number from line 2 of this worksheet Enter the number from line 1 of this worksheet Subtract line 5 from line Find the amount in Table 2 below that applies to the HIGHEST paying job and enter it here $ 8 Multiply line 7 by line 6 and enter the result here. This is the additional annual withholding needed.. 8 $ 9 Divide line 8 by the number of pay periods remaining in For example, divide by 26 if you are paid every two weeks and you complete this form in December Enter the result here and on Form W-4, line 6, page 1. This is the additional amount to be withheld from each paycheck $ Table 1 Table 2 Married Filing Jointly All Others Married Filing Jointly All Others If wages from LOWEST paying job are Enter on line 2 above $0 - $5, ,001-12, ,001-22, ,001-25, ,001-30, ,001-40, ,001-48, ,001-55, ,001-65, ,001-72, ,001-85, ,001-97, , , , , , , ,001 and over 15 If wages from LOWEST paying job are Enter on line 2 above $0 - $8, ,001-15, ,001-25, ,001-30, ,001-40, ,001-50, ,001-65, ,001-80, ,001-95, , , ,001 and over 10 Privacy Act and Paperwork Reduction Act Notice. We ask for the information on this form to carry out the Internal Revenue laws of the United States. Internal Revenue Code sections 3402(f)(2) and 6109 and their regulations require you to provide this information; your employer uses it to determine your federal income tax withholding. Failure to provide a properly completed form will result in your being treated as a single person who claims no withholding allowances; providing fraudulent information may subject you to penalties. Routine uses of this information include giving it to the Department of Justice for civil and criminal litigation; to cities, states, the District of Columbia, and U.S. commonwealths and possessions for use in administering their tax laws; and to the Department of Health and Human Services for use in the National Directory of New Hires. We may also disclose this information to other countries under a tax treaty, to federal and state agencies to enforce federal nontax criminal laws, or to federal law enforcement and intelligence agencies to combat terrorism. If wages from HIGHEST paying job are Enter on line 7 above $0 - $70,000 $570 70, , , ,000 1, , ,000 1, ,001 and over 1,330 If wages from HIGHEST paying job are Enter on line 7 above $0 - $35,000 $570 35,001-90, , ,000 1, , ,000 1, ,001 and over 1,330 You are not required to provide the information requested on a form that is subject to the Paperwork Reduction Act unless the form displays a valid OMB control number. Books or records relating to a form or its instructions must be retained as long as their contents may become material in the administration of any Internal Revenue law. Generally, tax returns and return information are confidential, as required by Code section The average time and expenses required to complete and file this form will vary depending on individual circumstances. For estimated averages, see the instructions for your income tax return. If you have suggestions for making this form simpler, we would be happy to hear from you. See the instructions for your income tax return.
5
6
7 Form 8850 (Rev. January 2012) Department of the Treasury Internal Revenue Service Pre-Screening Notice and Certification Request for the Work Opportunity Credit See separate instructions. Job applicant: Fill in the lines below and check any boxes that apply. Complete only this side. OMB No Your name Social security number Street address where you live City or town, state, and ZIP code County Telephone number If you are under age 40, enter your date of birth (month, day, year) 1 Check here if you received a conditional certification from the state workforce agency (SWA) or a participating local agency for the work opportunity credit. 2 Check here if any of the following statements apply to you. I am a member of a family that has received assistance from Temporary Assistance for Needy Families (TANF) for any 9 months during the past 18 months. I am a veteran and a member of a family that received Supplemental Nutrition Assistance Program (SNAP) benefits (food stamps) for at least a 3-month period during the past 15 months. I was referred here by a rehabilitation agency approved by the state, an employment network under the Ticket to Work program, or the Department of Veterans Affairs. I am at least age 18 but not age 40 or older and I am a member of a family that: a Received SNAP benefits (food stamps) for the past 6 months, or b Received SNAP benefits (food stamps) for at least 3 of the past 5 months, but is no longer eligible to receive them. During the past year, I was convicted of a felony or released from prison for a felony. I received supplemental security income (SSI) benefits for any month ending during the past 60 days. I am a veteran and I was unemployed for a period or periods totaling at least 4 weeks but less than 6 months during the past year. 3 Check here if you are a veteran and you were unemployed for a period or periods totaling at least 6 months during the past year. 4 Check here if you are a veteran entitled to compensation for a service-connected disability and you were discharged or released from active duty in the U.S. Armed Forces during the past year. 5 Check here if you are a veteran entitled to compensation for a service-connected disability and you were unemployed for a period or periods totaling at least 6 months during the past year. 6 Check here if you are a member of a family that: Received TANF payments for at least the past 18 months, or Received TANF payments for any 18 months beginning after August 5, 1997, and the earliest 18-month period beginning after August 5, 1997, ended during the past 2 years, or Stopped being eligible for TANF payments during the past 2 years because federal or state law limited the maximum time those payments could be made. Signature All Applicants Must Sign Under penalties of perjury, I declare that I gave the above information to the employer on or before the day I was offered a job, and it is, to the best of my knowledge, true, correct, and complete. Job applicant s signature For Privacy Act and Paperwork Reduction Act Notice, see page 2. Cat. No L Form 8850 (Rev ) Date
8 Form 8850 (Rev ) Page 2 For Employer s Use Only Employer s name Telephone no. EIN Street address City or town, state, and ZIP code Person to contact, if different from above Telephone no. Street address City or town, state, and ZIP code If, based on the individual s age and home address, he or she is a member of group 4 or 6 (as described under Members of Targeted Groups in the separate instructions), enter that group number (4 or 6) Date applicant: Gave information Was offered job Was hired Started job Under penalties of perjury, I declare that the applicant provided the information on this form on or before the day a job was offered to the applicant and that the information I have furnished is, to the best of my knowledge, true, correct, and complete. Based on the information the job applicant furnished on page 1, I believe the individual is a member of a targeted group. I hereby request a certification that the individual is a member of a targeted group. Employer s signature Title Date Privacy Act and Paperwork Reduction Act Notice Section references are to the Internal Revenue Code. Section 51(d)(13) permits a prospective employer to request the applicant to complete this form and give it to the prospective employer. The information will be used by the employer to complete the employer s federal tax return. Completion of this form is voluntary and may assist members of targeted groups in securing employment. Routine uses of this form include giving it to the state workforce agency (SWA), which will contact appropriate sources to confirm that the applicant is a member of a targeted group. This form may also be given to the Internal Revenue Service for administration of the Internal Revenue laws, to the Department of Justice for civil and criminal litigation, to the Department of Labor for oversight of the certifications performed by the SWA, and to cities, states, and the District of Columbia for use in administering their tax laws. We may also disclose this information to other countries under a tax treaty, to federal and state agencies to enforce federal nontax criminal laws, or to federal law enforcement and intelligence agencies to combat terrorism. You are not required to provide the information requested on a form that is subject to the Paperwork Reduction Act unless the form displays a valid OMB control number. Books or records relating to a form or its instructions must be retained as long as their contents may become material in the administration of any Internal Revenue law. Generally, tax returns and return information are confidential, as required by section The time needed to complete and file this form will vary depending on individual circumstances. The estimated average time is: Recordkeeping.. 6 hr., 27 min. Learning about the law or the form min. Preparing and sending this form to the SWA min. If you have comments concerning the accuracy of these time estimates or suggestions for making this form simpler, we would be happy to hear from you. You can write to the Internal Revenue Service, Tax Products Coordinating Committee, SE:W:CAR:MP:T:M:S, 1111 Constitution Ave. NW, IR-6526, Washington, DC Do not send this form to this address. Instead, see When and Where To File in the separate instructions. Form 8850 (Rev )
9 VOLUNTARY SUBSTANCE TESTING I understand to protect myself and my employer, I, voluntarily authorize blood and urine testing for alcohol and/or drug use. I agree to allow such samples and testing be completed at a time and place to be chosen by my employer. I understand should such samples and testing be requested it could be due to suspicion that I am under the influence of alcohol and/or drugs and by being so may endanger myself or others or may affect the product quality of my work. I further authorize the results of samples/testing to be released to my employer. Employee Signature Witnessed by Date Date Title STATEMENT OF UNDERSTANDING I,, fully understand that I am now an employee of Pinnacle PEO Corp. (PPEOC). I understand that I will receive my paycheck from PPEOC each pay period and that all benefits, if applicable, will be administered through them. I understand that they are my employer for the purpose of tax representation, W-2 s, Workers Compensation filing, state and federal unemployment and will represent me in all dealing with the Department of Labor or any other Federal or State agencies. In the event that benefits have been elected, I understand that I will receive appropriate outlines on benefits and services offered to the leased employees of PPEOC, SIGNATURE DATE

10 TO GET PAID Instead of waiting in line to cash your paycheck, have your pay automatically deposited to the Chase Payroll Visa Card. It s safe, fast and easy plus it saves you money! Get cash 24 x 7 at ATMs worldwide Make purchases anywhere Visa debit cards are accepted Shop online, by phone or mail order Eliminate the hassle and costs of cashing a check No lost or stolen checks No credit check required Get your money anywhere, anytime With the Chase Payroll Card, your pay is electronically deposited to your Chase Payroll Card Account each pay period, where your funds are FDIC-insured. You then have immediate and convenient access to your money at over 900,000 automated teller machines (ATMs). You can enjoy surcharge free access at over 40,000 Chase and Allpoint (if your Card carries the Allpoint logo) ATMs in the U.S., and at millions of retail locations worldwide that accept Visa debit cards. Your purchases are protected For the first 90 days from the purchase date, Visa s Purchase Security 1 will replace, repair or reimburse you for eligible items of personal property purchased entirely with your Chase Payroll Visa Card to a maximum of $500 per claim and $50,000 per cardholder. Additionally, Visa s Zero Liability Policy 2 protects you from unauthorized purchases. If your Card is ever lost or stolen, you are automatically protected without losing funds in your Account. 1. This protection is valid in cases of theft, damage due to fire, vandalism, accidentally discharged water or certain weather conditions. Certain restrictions may apply. Enroll in the Chase Payroll Card program today! There is no cost to enroll in the Chase Payroll Card program. Simply complete this enrollment form today and return it to your payroll department. Payroll Card Fee Schedule TRANSACTION Cardholder Fee ATM Withdrawal (U.S.)* Chase or Allpoint ATM Withdrawal (outside U.S.) Point-of-Sale /Signature Transactions Point-Of-Sale Transaction PIN Based Over-the-counter cash withdrawals ATM balance inquiry (U.S.) ATM balance inquiry (outside U.S.) ADDITIONAL SERVICES $1.50 per transaction (after 1 free per deposit) $3.00 per withdrawal FREE Monthly paper statement $1.00 Monthly statements via internet Replace lost/stolen card Expedited card delivery Declined transactions** Copy of statement Negative balance Check to close account Inactivity fee (after 90 days of inactivity) Foreign Exchange conversion rate FREE $5.00 per withdrawal (after 1 free per deposit) $1.00 per inquiry $3.00 per inquiry FREE $15.00 per card $10.00 per card $1.00 per transaction $10.00 per request $15.00 per incident $12.00 per account $5.00 per month 3.5% of the International transaction *Whenever you use any ATM there is a network or ATM withdrawal fee. However your program may allow you a certain number of free ATM withdrawals per month before you are assessed this fee. Additionally non-chase banks may charge you a surcharge typically between $1.00 and $2.00 for using their ATM. You can avoid a surcharge by using a Chase or Allpoint ATM (if your card carries the Allpoint logo). **This fee will assessed if an ATM or Point of Sale transaction is denied due to insufficient funds in your Chase Payroll Card Account. 2. U.S.-issued cards only. The Visa Zero Liability Policy does not apply to commercial card or ATM transactions, or to PIN transactions not processed by Visa or Interlink. See your cardholder agreement for more details. PayAppV04/07 Chase Payroll Visa Cards are issued by JPMorgan Chase Bank, N.A JPMorgan Chase & Co. All rights reserved. JPMorgan Chase Bank, N.A. Member FDIC.
11 Chase Payroll Card Application Important information about procedures for opening a new account To help the government fight the funding of terrorism and money laundering activities, Federal law requires all financial institutions to obtain, verify and record information that identifies each person who opens an account. What this means for you: when you open an account, you will be asked for your name, address, date of birth, and other information that will allow you to be identified. You may also be asked to present your driver s license or other identifying documents. Unless otherwise noted, all fields are required and must be filled in to process this application. I. CARDHOLDER INFORMATION FIRST NAME MI LAST NAME STREET ADDRESS (NO P.O. BOXES) ADDRESS 2 CITY STATE ZIP PRIMARY PHONE SECONDARY PHONE (OPTIONAL) ADDRESS (OPTIONAL) DAT E OF BIRTH (MM/DD/YYYY) MOTHER S MAIDEN NAME U.S. CITIZEN NON-U.S. CITIZEN SSN If you are not a citizen of the United States please provide one or more of the following forms of identification. A. Please select a form of identification SOCIAL SECURITY TAXPAYER ID U.S. ALIEN ID CARD PASSPORT OTHER GOV T ISSUED ID TYPE B. Please fill out the corresponding information COUNTRY OF ISSUANCE NUMBER EXPIRATION DATE (MM / DD / YYYY) Monthly paper statement (optional) - in addition to accessing my Chase Payroll Card transaction activity on-line or via Customer Support, please mail me a monthly payroll card activity statement to the mailing address I have provided above. I understand there is a monthly charge for this statement option, which is disclosed on the Chase Payroll Card enrollment form. II. CARDHOLDER AGREEMENT Return your completed, signed and dated application to your employer. Authorization Agreement for Chase Payroll Card Account will authorize my employer to directly deposit my periodic salary/ compensation payments, net of required tax withholdings, other required withholdings or authorized deductions (a Payroll Payment ) into my Chase Payroll Card Account (the Account ) at JPMorgan Chase Bank, N.A. ( Chase ) and to initiate (if necessary) debit entries and adjustments for any credit entries in error to my Account. I understand that I may withdraw a portion or entire amount of a Payroll Payment deposited by my employer from time to time in cash via an Automated Teller Machine (subject to certain withdrawal limits as discussed in the Program Terms, Conditions and Disclosures), applicable Point-of-Sale (POS) terminals and wherever Visa debit cards are accepted. By signing this application, I hereby authorize Chase to issue a Card to me. I agree that activating my Card shall constitute my agreement to: (1) The Program Terms, Conditions and Disclosures that accompany my Card and (2) changes to, or replacements for, those Program Terms, Conditions or Disclosures that may be sent or made available to me from time to time. I also hereby authorize Chase to debit my Chase Payroll Card Account, without notifying me, for the fees described in the fee schedule that is part of this application, or as such fees may change from time to time. Chase may change those fees at any time. CARDHOLDER S SIGNATURE DATE III. EMPLOYER USE ONLY COMPANY NAME LOCATION PROCESSOR S NAME PROCESSOR S PHONE NUMBER
12 Team Member Handbook Acknowledgment I have read and fully understand the Team Member Handbook ( the Handbook ). I understand the reasons for the policies and procedures, and I agree to abide by the policies and procedures detailed in the handbook in its present form and as it may from time-to-time be modified. I understand that Sport Clips reserves the right to terminate or modify any of its other policies and procedures at any time it deems appropriate in its sole and absolute discretion. THE STATEMENTS AND LANGUAGE IN THE HANDBOOK ARE NOT INTENDED TO CREATE OR CONSTITUTE A CONTRACT BETWEEN SPORT CLIPS AND ANY ONE OR ALL OF ITS TEAM MEMBERS (EMPLOYEES). EMPLOYMENT WITH SPORT CLIPS IS AT THE MUTUAL CONSENT OF THE TEAM MEMBER AND SPORT CLIPS AND IS FOR NO DEFINITE PERIOD. EMPLOYMENT MAY, REGARDLESS OF THE DATE OF PAYMENT OF WAGES AND/OR SALARY, BE TERMINATED AT WILL, ANY TIME, WITH OR WITHOUT CAUSE OR ANY PREVIOUS NOTICE. Please note that you will be working in a Sport Clips store that is a franchise of Sport Clips, Inc. So whenever you see the name Sport Clips, remember that you are working for a business owner who has bought a franchise and the right to do business under the Sport Clips brand name. This franchisee has contracted with Pinnacle PEO Corporation under a Professional Employer Organization agreement, also known as Employee Leasing. Under this type of arrangement, Pinnacle PEO becomes the employer of record and shares employment responsibilities with the franchise owner. I further understand that my continued employment with Sport Clips is based on my compliance with the policies and procedures detailed in the Handbook. Team Member: Date: (Please Print) Signature: (Sign In Ink) Sport Clips #: Witness: Signature: Position: (Please Print) (Sign in Ink) Confidential
Separate here and give Form W-4 to your employer. Keep the top part for your records. Employee s Withholding Allowance Certificate
 Form W-4 (2017) Purpose. Complete Form W-4 so that your employer can withhold the correct federal income tax from your pay. Consider completing a new Form W-4 each year and when your personal or financial
Form W-4 (2017) Purpose. Complete Form W-4 so that your employer can withhold the correct federal income tax from your pay. Consider completing a new Form W-4 each year and when your personal or financial
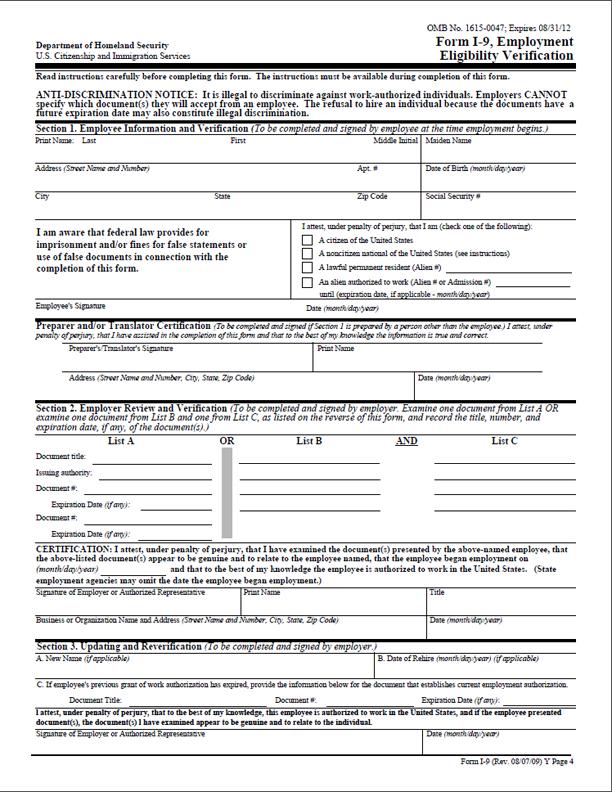
Employment Eligibility Verification
 Employment Eligibility Verification Department of Homeland Security U.S. Citizenship and Immigration Services USCIS Form I-9 OMB No. 1615-0047 Expires 08/31/2019 START HERE: Read instructions carefully
Employment Eligibility Verification Department of Homeland Security U.S. Citizenship and Immigration Services USCIS Form I-9 OMB No. 1615-0047 Expires 08/31/2019 START HERE: Read instructions carefully
Separate here and give Form W-4 to your employer. Keep the top part for your records. Employee s Withholding Allowance Certificate
 Form W-4 (2017) Purpose. Complete Form W-4 so that your employer can withhold the correct federal income tax from your pay. Consider completing a new Form W-4 each year and when your personal or financial
Form W-4 (2017) Purpose. Complete Form W-4 so that your employer can withhold the correct federal income tax from your pay. Consider completing a new Form W-4 each year and when your personal or financial
EMPLOYEE INFORMATION SHEET
 EMPLOYEE INFORMATION SHEET PLEASE PRINT CLEARLY COMPANY: EMPLOYEE #: SOCIAL SECURITY NUMBER: - - NAME: First MI LAST STREET: CITY: AS APPEARS ON SOCIAL SECURITY CARD STATE: ZIP CODE: TELEPHONE NUMBER:
EMPLOYEE INFORMATION SHEET PLEASE PRINT CLEARLY COMPANY: EMPLOYEE #: SOCIAL SECURITY NUMBER: - - NAME: First MI LAST STREET: CITY: AS APPEARS ON SOCIAL SECURITY CARD STATE: ZIP CODE: TELEPHONE NUMBER:
Separate here and give Form W-4 to your employer. Keep the top part for your records. Employee s Withholding Allowance Certificate
 Form W-4 (2017) Purpose. Complete Form W-4 so that your employer can withhold the correct federal income tax from your pay. Consider completing a new Form W-4 each year and when your personal or financial
Form W-4 (2017) Purpose. Complete Form W-4 so that your employer can withhold the correct federal income tax from your pay. Consider completing a new Form W-4 each year and when your personal or financial
XXXXXX NON-UNION VOUCHER. White - Payroll Company Yellow - Accounting Department Pink - Employee TIME CLOCK RATE ALLOWANCES SPECIAL COMPENSATIONS
 XXXXXX NON-UNION VOUCHER DATE PRODUCTION & PROJECT NAME 1 2 3 LAST NAME FIRST NAME MI STREET ADDRESS CITY STATE ZIP DATE OF BIRTH: IF MINOR PHONE IF NEW IF NEW EMPLOYEE ADDRESS SOCIAL SECURITY NUMBER WORK
XXXXXX NON-UNION VOUCHER DATE PRODUCTION & PROJECT NAME 1 2 3 LAST NAME FIRST NAME MI STREET ADDRESS CITY STATE ZIP DATE OF BIRTH: IF MINOR PHONE IF NEW IF NEW EMPLOYEE ADDRESS SOCIAL SECURITY NUMBER WORK
Missouri Department of Revenue Employee s Withholding Allowance Certificate
 Form MO W-4 Missouri Department of Revenue Employee s Withholding Allowance Certificate This certificate is for income tax withholding and child support enforcement purposes only. Type or print. Full Name
Form MO W-4 Missouri Department of Revenue Employee s Withholding Allowance Certificate This certificate is for income tax withholding and child support enforcement purposes only. Type or print. Full Name
New Employee Welcome Letter and Orientation Checklist
 Lafayette DQ Restaurants P.O. Box 302 Delphi, IN 46923 Phone: (765) 447-1089 Fax: (765) 535-5001 New Employee Welcome Letter and Orientation Checklist Welcome to the DQ family! In order to start training
Lafayette DQ Restaurants P.O. Box 302 Delphi, IN 46923 Phone: (765) 447-1089 Fax: (765) 535-5001 New Employee Welcome Letter and Orientation Checklist Welcome to the DQ family! In order to start training
EMPLOYER INFORMATION SHEET
 General EMPLOYER INFORMATION SHEET Business Name: Business Address: City, State, Zip: Filing Name (if different): Filing Address (if different): City, State, Zip: Contact Name: Phone: Fax: Email: Company
General EMPLOYER INFORMATION SHEET Business Name: Business Address: City, State, Zip: Filing Name (if different): Filing Address (if different): City, State, Zip: Contact Name: Phone: Fax: Email: Company
A - EMPLOYEE INFORMATION SUBMISSION AND CERTIFICATION
 Office/Client Number New Employee Packet Employer Information: Choose your option for submitting employee information. For detailed instructions for these options, refer to the PEO New Employee Packet
Office/Client Number New Employee Packet Employer Information: Choose your option for submitting employee information. For detailed instructions for these options, refer to the PEO New Employee Packet
Employment Application
 P.O. Box 643 Benavides, Tx 78341 (361) 256-4726 Office (361) 256-4728 Fax Scorp1144@yahoo.com Scorpion Exploration & Production, Inc. Full Name Mailing Address Employment Application Applicant Information
P.O. Box 643 Benavides, Tx 78341 (361) 256-4726 Office (361) 256-4728 Fax Scorp1144@yahoo.com Scorpion Exploration & Production, Inc. Full Name Mailing Address Employment Application Applicant Information
Last Name First Name Middle Name. Street Address City State Zip Code
 EMPLOYMENT APPLICATION Clean All Services is an equal opportunity employer and affords equal opportunity to all applicants for all positions without regard to race, color, religion, gender, national origin,
EMPLOYMENT APPLICATION Clean All Services is an equal opportunity employer and affords equal opportunity to all applicants for all positions without regard to race, color, religion, gender, national origin,
New Employment & Sign-up Checklist for Managers and Departmental Representatives
 FLORIDA A&M UNIVERSITY New Employment & Sign-up Checklist for Managers and Departmental Representatives Executive Service A&P USPS OPS Faculty (Please complete Section II Only) Employee Name: Class Title:
FLORIDA A&M UNIVERSITY New Employment & Sign-up Checklist for Managers and Departmental Representatives Executive Service A&P USPS OPS Faculty (Please complete Section II Only) Employee Name: Class Title:
Employee Data Form. [ ] ] ] [ ] ] [ ] _] _]_ ] Home Address Apt City State Zip Code County. Ethnicity: Are you Hispanic/Latino?
![Employee Data Form. [ ] ] ] [ ] ] [ ] _] _]_ ] Home Address Apt City State Zip Code County. Ethnicity: Are you Hispanic/Latino?](/thumbs/79/79502522.jpg "Employee Data Form. [ ] ] ] [ ] ] [ ] _] _]_ ] Home Address Apt City State Zip Code County. Ethnicity: Are you Hispanic/Latino?") Employee Data Form Baltimore City Public Schools Office Of Human Capital 200 E. North Avenue, Room 110 Baltimore, Maryland 21202 www. s New /Rehire employees are required to complete this form as part
Employee Data Form Baltimore City Public Schools Office Of Human Capital 200 E. North Avenue, Room 110 Baltimore, Maryland 21202 www. s New /Rehire employees are required to complete this form as part
APPLICATION FOR EMPLOYMENT
 Community Values, Local Choices AN EQUAL OPPORTUNITY EMPLOYER APPLICATION FOR EMPLOYMENT Applicant: We appreciate your interest in C&K Market, Inc. (C&K). A clear understanding of your background and work
Community Values, Local Choices AN EQUAL OPPORTUNITY EMPLOYER APPLICATION FOR EMPLOYMENT Applicant: We appreciate your interest in C&K Market, Inc. (C&K). A clear understanding of your background and work
Western States Office and Professional Employees Pension Fund
 Western States Office and Professional Employees Pension Fund FEDERAL INCOME TAX WITHHOLDING TAX WITHHOLDING ELECTION Please complete the attached W-4P Withholding Certificate for Pension or Annuity Payments.
Western States Office and Professional Employees Pension Fund FEDERAL INCOME TAX WITHHOLDING TAX WITHHOLDING ELECTION Please complete the attached W-4P Withholding Certificate for Pension or Annuity Payments.
Store# Name (First, Middle, Last) SSN # Date of Birth. City State Zip. Hire Date Position Rate of pay/annual Salary. Select... Rehire.
 SSN # Date of Birth. City State Zip. Hire Date Position Rate of pay/annual Salary. Select... Rehire.") Store# Name (First, Middle, Last) SSN # Date of Birth Address Apt/Lot City State Zip Hire Date Position Rate of pay/annual Salary Rehire nmlkj Yes nmlkj No Select... Native American If yes, please list
Store# Name (First, Middle, Last) SSN # Date of Birth Address Apt/Lot City State Zip Hire Date Position Rate of pay/annual Salary Rehire nmlkj Yes nmlkj No Select... Native American If yes, please list
YOU DO NOT NEED TO PRINT THIS PAGE. Substitute Records Requirements. Social Security Card (copies not accepted)
") YOU DO NOT NEED TO PRINT THIS PAGE. Appointment Date & Time: Name: Date: Substitute Records Requirements I-9 (only complete page 1) W-4 Social Security Card (copies not accepted) Driver s License Direct
YOU DO NOT NEED TO PRINT THIS PAGE. Appointment Date & Time: Name: Date: Substitute Records Requirements I-9 (only complete page 1) W-4 Social Security Card (copies not accepted) Driver s License Direct
We (The Jeffrey Corporation) are making you a contingent job offer to work at Burger King Store #.
 are making you a contingent job offer to work at Burger King Store #.") Date Dear Applicant, We (The Jeffrey Corporation) are making you a contingent job offer to work at Burger King Store #. Part of the hiring/re-hiring process requires that we verify your eligibility to
Date Dear Applicant, We (The Jeffrey Corporation) are making you a contingent job offer to work at Burger King Store #. Part of the hiring/re-hiring process requires that we verify your eligibility to
DIVERSIFIED Edgewood Road, NE Cedar Rapids, IA
 DIVERSIFIED --------------------- 4443 Edgewood Road, NE Cedar Rapids, IA 52499 800-755-5801 www.divinvest.com Federal Tax Withholding Election Form Instructions To change your federal income tax withholding,
DIVERSIFIED --------------------- 4443 Edgewood Road, NE Cedar Rapids, IA 52499 800-755-5801 www.divinvest.com Federal Tax Withholding Election Form Instructions To change your federal income tax withholding,
Separate here and give Form W-4 to your employer. Keep the top part for your records. Employee's Withholding Allowance Certificate
 Form W-4 (2015) Purpose. Complete Form W-4 so that your employer can withhold the correct federal income tax from your pay. Consider completing a new Form W-4 each year and when your personal or financial
Form W-4 (2015) Purpose. Complete Form W-4 so that your employer can withhold the correct federal income tax from your pay. Consider completing a new Form W-4 each year and when your personal or financial
Employment Eligibility Verification
 Employment Eligibility Verification Department of Homeland Security U.S. Citizenship and Immigration Services USCIS Form I-9 OMB No. 1615-0047 Expires 08/31/2019 START HERE: Read instructions carefully
Employment Eligibility Verification Department of Homeland Security U.S. Citizenship and Immigration Services USCIS Form I-9 OMB No. 1615-0047 Expires 08/31/2019 START HERE: Read instructions carefully
Please complete and sign all forms in the PRE-EMPLOYMENT FORMS section.
 NATIONAL HOME HEALTH SERVICES EMPLOYMENT FORMS 5811 Dempster St Morton Grove, IL 60053 Phone: (847) 329-9933 Fax: (847) 930-0375 APPLICANT NAME POSITION APPLYING FOR DATE Please complete and sign all forms
NATIONAL HOME HEALTH SERVICES EMPLOYMENT FORMS 5811 Dempster St Morton Grove, IL 60053 Phone: (847) 329-9933 Fax: (847) 930-0375 APPLICANT NAME POSITION APPLYING FOR DATE Please complete and sign all forms
Decatur County Schools
 Decatur County Schools 100 West Street Bainbridge, Georgia 39817 (229) 248-2200 Fax (229) 248-2252 This application will remain active for one year from date received unless requested to reactivate after
Decatur County Schools 100 West Street Bainbridge, Georgia 39817 (229) 248-2200 Fax (229) 248-2252 This application will remain active for one year from date received unless requested to reactivate after
Southeast ID#: Name: SSN: PREVIOUS CIVIL OR COLLEGE DISCIPLINE
 /Student Employment Work Referral Southeast ID#: Name: SSN: STUDENT EMPLOYEE ELIGIBILITY AND RESPONSIBILITIES 1. You must complete, and have on file with Student Financial Services, employment eligibility
/Student Employment Work Referral Southeast ID#: Name: SSN: STUDENT EMPLOYEE ELIGIBILITY AND RESPONSIBILITIES 1. You must complete, and have on file with Student Financial Services, employment eligibility
EMPLOYER WITH EMPLOYEES - PAYROLL INTAKE FORM
 EMPLOYER WITH EMPLOYEES - PAYROLL INTAKE FORM CONTACT INFORMATION Payroll Client (First, Last): Phone #: ( ) - Legal Business Name: Business DBA (If Applicable): Business Type: LLC Partnership Corp S-Corp
EMPLOYER WITH EMPLOYEES - PAYROLL INTAKE FORM CONTACT INFORMATION Payroll Client (First, Last): Phone #: ( ) - Legal Business Name: Business DBA (If Applicable): Business Type: LLC Partnership Corp S-Corp
What s In My Paycheck? compensation package: all of the wages (salary, bonus, commission) and benefits provided by an employer. What s In My Paycheck?
 and benefits provided by an employer. What s In My Paycheck?") compensation package: all of the wages (salary, bonus, commission) and benefits provided by an employer wages: money paid or received for work or services completed, usually by the hour, day, or week hourly
compensation package: all of the wages (salary, bonus, commission) and benefits provided by an employer wages: money paid or received for work or services completed, usually by the hour, day, or week hourly
SURRENDER REQUEST FORM. Policy Number: Insured:
 SURRENDER REQUEST FORM Section A Policy Information (You Must Complete This Section) Policy Number: Insured: (First Name) (Last Name) Sec tion B Surrender Request and Withholding Election (You Must Complete
SURRENDER REQUEST FORM Section A Policy Information (You Must Complete This Section) Policy Number: Insured: (First Name) (Last Name) Sec tion B Surrender Request and Withholding Election (You Must Complete
Employment Application
 Print Name (First, ( M., Last): Employment Application PERSONAL INFORMATION Date: Street Address: Apt. Unit/# Home Phone: City State Zip Cell Phone: Email Address: Are you authorized to work in the U.S.?
Print Name (First, ( M., Last): Employment Application PERSONAL INFORMATION Date: Street Address: Apt. Unit/# Home Phone: City State Zip Cell Phone: Email Address: Are you authorized to work in the U.S.?
COMMUNITY: PROGRAM: ORIGINAL DATE: TIME: UPDATE: TIME:
 SUBJECT: APPLICANT FOR RESIDENCY TAX CREDIT COMMUNITIES COMMUNITY: PROGRAM: ORIGINAL DATE: TIME: UPDATE: TIME: HOW DID YOU HEAR ABOUT US? APARTMENT SIZE: APPLICANT NAME (FIRST, MIDDLE, LAST): CURRENT ADDRESS:
SUBJECT: APPLICANT FOR RESIDENCY TAX CREDIT COMMUNITIES COMMUNITY: PROGRAM: ORIGINAL DATE: TIME: UPDATE: TIME: HOW DID YOU HEAR ABOUT US? APARTMENT SIZE: APPLICANT NAME (FIRST, MIDDLE, LAST): CURRENT ADDRESS:
How Do I Adjust My Tax Withholding?
 Contents Department of the Treasury Internal Revenue Service What s New for 2011... 2 Reminder.... Publication 919 Introduction... 3 Cat. No. 63900P How Do I Adjust My Tax Withholding? Checking Your Withholding...
Contents Department of the Treasury Internal Revenue Service What s New for 2011... 2 Reminder.... Publication 919 Introduction... 3 Cat. No. 63900P How Do I Adjust My Tax Withholding? Checking Your Withholding...
RAYMOND CENTRAL PUBLIC SCHOOLS SUBSTITUTE TEACHER DATA SHEET
 RAYMOND CENTRAL PUBLIC SCHOOLS SUBSTITUTE TEACHER DATA SHEET PLEASE NOTE: We need a voided check for payment by Direct Deposit and we must have an email address. Thank you. W-4 Form I-9 Form - 2 forms
RAYMOND CENTRAL PUBLIC SCHOOLS SUBSTITUTE TEACHER DATA SHEET PLEASE NOTE: We need a voided check for payment by Direct Deposit and we must have an email address. Thank you. W-4 Form I-9 Form - 2 forms
Student Employee New Hire Packet
 Student Employee New Hire Packet New Hire Checklist: o Authorization to Hire Form o Student Application o Federal W-4 Form o NJ State W-4 Form o I-9 Form o Social Security Card (for Payroll purposes) o
Student Employee New Hire Packet New Hire Checklist: o Authorization to Hire Form o Student Application o Federal W-4 Form o NJ State W-4 Form o I-9 Form o Social Security Card (for Payroll purposes) o
New Employee Information
 HOUSTON S PREMIER POKER DESTINATION New Employee Information Before you will be scheduled the following MUST be completed: 1. Your new hire packet must be filled out completely and correctly and handed
HOUSTON S PREMIER POKER DESTINATION New Employee Information Before you will be scheduled the following MUST be completed: 1. Your new hire packet must be filled out completely and correctly and handed
Instructions. Please complete the top section. Please check each box in questions 1 through 6 that apply to you. Please sign and date at the bottom.
 Instructions Thank you for taking the time to complete the two forms in this PDF. While the forms ask for sensitive information, that information is critical to the success of this project and we will
Instructions Thank you for taking the time to complete the two forms in this PDF. While the forms ask for sensitive information, that information is critical to the success of this project and we will
 Form W-4 (2018) Future developments. For the latest information about any future developments related to Form W-4, such as legislation enacted after it was published, go to www.irs.gov/formw4. Purpose.
Form W-4 (2018) Future developments. For the latest information about any future developments related to Form W-4, such as legislation enacted after it was published, go to www.irs.gov/formw4. Purpose.
NO CONFLICT ATTESTATION. In order to qualify to act as the Personal Assistant for this Consumer, I attest to the ALL of following:
 NO CONFLICT ATTESTATION In order to qualify to act as the Personal Assistant for this Consumer, I attest to the ALL of following: 1. I am NOT the Consumer s Designated Representative. 2. The Consumer is
NO CONFLICT ATTESTATION In order to qualify to act as the Personal Assistant for this Consumer, I attest to the ALL of following: 1. I am NOT the Consumer s Designated Representative. 2. The Consumer is
Instructions. Please complete the top section. Please check each box in questions 1 through 7 that apply to you. Please sign and date at the bottom.
 Instructions Thank you for taking the time to complete the two forms in this PDF. While the forms ask for sensitive information, that information is critical to the success of this project and we will
Instructions Thank you for taking the time to complete the two forms in this PDF. While the forms ask for sensitive information, that information is critical to the success of this project and we will
Separate here and give Form W-4 to your employer. Keep the worksheet(s) for your records. Employee s Withholding Allowance Certificate
 for your records. Employee s Withholding Allowance Certificate") Form W-4 (2018) Future developments. For the latest information about any future developments related to Form W-4, such as legislation enacted after it was published, go to www.irs.gov/formw4. Purpose.
Form W-4 (2018) Future developments. For the latest information about any future developments related to Form W-4, such as legislation enacted after it was published, go to www.irs.gov/formw4. Purpose.
P E N N S Y L V A N I A Application for Payment of Medicare Premiums, Coinsurance and Deductibles
 P E N N S Y L V A N I A Application for Payment of Medicare Premiums, Coinsurance and Deductibles If you have a disability and need this form in large print or another format, please call our helpline
P E N N S Y L V A N I A Application for Payment of Medicare Premiums, Coinsurance and Deductibles If you have a disability and need this form in large print or another format, please call our helpline
Last Name First Name Middle Initial ADDRESS Street City County State Zip
 APPLICATION FOR EMPLOYMENT Kolberg-Pioneer, Inc. An Equal Opportunity Employer (HRF-002-03 01/16) This application is valid for the calendar year of 2018. Kolberg-Pioneer, Inc. will provide the Social
APPLICATION FOR EMPLOYMENT Kolberg-Pioneer, Inc. An Equal Opportunity Employer (HRF-002-03 01/16) This application is valid for the calendar year of 2018. Kolberg-Pioneer, Inc. will provide the Social
Swiftwater/Wildland Application Checklist
 Mountain View Fire and Rescue KING COUNTY FIRE PROTECTION DISTRICT 44 32316 148 AVE SE Auburn, WA 98092 / (253) 735-0284; FAX (253) 735 0287 Swiftwater/Wildland Application Checklist Application complete
Mountain View Fire and Rescue KING COUNTY FIRE PROTECTION DISTRICT 44 32316 148 AVE SE Auburn, WA 98092 / (253) 735-0284; FAX (253) 735 0287 Swiftwater/Wildland Application Checklist Application complete
APPLICATION CHECKLIST
 PERF/TRF RETIREMENT APPLICATION State Form 945 (R30 / 2-15) Approved by State Board of Accounts, 2015 INDIANA PUBLIC RETIREMENT SYSTEM Telephone: (888) 286-3544 (Toll-free) Web site: www.inprs.in.gov Use
PERF/TRF RETIREMENT APPLICATION State Form 945 (R30 / 2-15) Approved by State Board of Accounts, 2015 INDIANA PUBLIC RETIREMENT SYSTEM Telephone: (888) 286-3544 (Toll-free) Web site: www.inprs.in.gov Use
Social Security Number (SSN) of applying member. Date of Birth
 of applying member. Date of Birth") LDSS-4826 (11/02) Page 1 NEW YORK STATE OFFICE OF TEMPORARY AND DISABILITY ASSISTANCE FOOD STAMP BENEFITS APPLICATION Application Date Interview Date Center/Office Unit Worker Case Type Case Number Registry
LDSS-4826 (11/02) Page 1 NEW YORK STATE OFFICE OF TEMPORARY AND DISABILITY ASSISTANCE FOOD STAMP BENEFITS APPLICATION Application Date Interview Date Center/Office Unit Worker Case Type Case Number Registry
INSTRUCTIONS FOR PAPERWORK ALL FORMS MUST BE SIGNED AND DATED PLEASE PRINT ONE-SIDED SHEETS
 INSTRUCTIONS FOR PAPERWORK ALL FORMS MUST BE SIGNED AND DATED PLEASE PRINT ONE-SIDED SHEETS CFISD EMPLOYEE INFORMATION SHEET Must be LEGIBLE Fill in all blanks You MUST bubble an answer for Part 1-Ethnicity
INSTRUCTIONS FOR PAPERWORK ALL FORMS MUST BE SIGNED AND DATED PLEASE PRINT ONE-SIDED SHEETS CFISD EMPLOYEE INFORMATION SHEET Must be LEGIBLE Fill in all blanks You MUST bubble an answer for Part 1-Ethnicity
Instructions for Form 990-BL
 Instructions for Form 990-BL (Rev. December 2008) Information and Initial Excise Tax Return for Black Lung Benefit Trusts and Certain Related Persons Department of the Treasury Internal Revenue Service
Instructions for Form 990-BL (Rev. December 2008) Information and Initial Excise Tax Return for Black Lung Benefit Trusts and Certain Related Persons Department of the Treasury Internal Revenue Service
Packet A - Forms. If you have any questions, please contact Human Resources at
 Packet A - Forms 2018 TEMPORARY NEW HIRE PAPERWORK Welcome to Union College! This packet contains new hire forms necessary for you to become established as a Union College employee. Please fill out and
Packet A - Forms 2018 TEMPORARY NEW HIRE PAPERWORK Welcome to Union College! This packet contains new hire forms necessary for you to become established as a Union College employee. Please fill out and
Graveyard Productions, LLC
 Graveyard Productions, LLC Check here if you are under 18 years old Recruitment Application- 2018 PLEASE PRINT LEGIBLY Applicant Information Full Name: Date: Last First M.I. Address: Street Address Apartment/Unit
Graveyard Productions, LLC Check here if you are under 18 years old Recruitment Application- 2018 PLEASE PRINT LEGIBLY Applicant Information Full Name: Date: Last First M.I. Address: Street Address Apartment/Unit
CAREFULLY READ AND FOLLOW INSTRUCTIONS
 PLAINFIELD BOARD OF EDUCATION 1200 Myrtle Avenue Plainfield, NJ 07060 SUBSTITUTE BUS DRIVER CHECK LIST Name: Social Security Number: CAREFULLY READ AND FOLLOW INSTRUCTIONS 1. Go to the State's Website
PLAINFIELD BOARD OF EDUCATION 1200 Myrtle Avenue Plainfield, NJ 07060 SUBSTITUTE BUS DRIVER CHECK LIST Name: Social Security Number: CAREFULLY READ AND FOLLOW INSTRUCTIONS 1. Go to the State's Website
The Housing Authority of the City Of New Albany 300 Erni Avenue New Albany IN 47150
 The Housing Authority of the City Of New Albany 300 Erni Avenue New Albany IN 47150 Public Housing: GENERAL INFORMATION We do not have emergency housing. Emergency housing is available only through a shelter.
The Housing Authority of the City Of New Albany 300 Erni Avenue New Albany IN 47150 Public Housing: GENERAL INFORMATION We do not have emergency housing. Emergency housing is available only through a shelter.
When Can You Start? Days/Hours Name Street Address/City/State/Zip:
 Application DATE: POSITION APPLIED FOR: Management Driver In-Store Restaurant Full Time Part Time When Can You Start? Days/Hours Name Street Address/City/State/Zip: Phone: Are you under 18? Yes No Email:
Application DATE: POSITION APPLIED FOR: Management Driver In-Store Restaurant Full Time Part Time When Can You Start? Days/Hours Name Street Address/City/State/Zip: Phone: Are you under 18? Yes No Email:
Applications will only be accepted from
 May 2018 Dear Applicant, Thank you for your interest in applying to Pikes Peak Habitat for Humanity! Enclosed you will find the Habitat for Humanity application. Before completing the application, please
May 2018 Dear Applicant, Thank you for your interest in applying to Pikes Peak Habitat for Humanity! Enclosed you will find the Habitat for Humanity application. Before completing the application, please
WELLFLEET APARTMENTS HOUSING APPLICATION PLEASE PRINT
 Three Main Street Mercantile Unit # 7 Eastham, MA 02642 Tel: 508-240-7873, ext 17 *TDD #1-800-439-0183 Fax: 508-240-1511 WELLFLEET APARTMENTS HOUSING APPLICATION PLEASE PRINT This is an application for
Three Main Street Mercantile Unit # 7 Eastham, MA 02642 Tel: 508-240-7873, ext 17 *TDD #1-800-439-0183 Fax: 508-240-1511 WELLFLEET APARTMENTS HOUSING APPLICATION PLEASE PRINT This is an application for
Your Premier Service Provider
 FVC Frenchman Valley Coop fvcoop.com Your Premier Service Provider 202 Broadway St., PO Box 578 Imperial, NE 69033 Updated 04/30/2013 Application for Employment Prospective employees will receive consideration
FVC Frenchman Valley Coop fvcoop.com Your Premier Service Provider 202 Broadway St., PO Box 578 Imperial, NE 69033 Updated 04/30/2013 Application for Employment Prospective employees will receive consideration
Property Management, Inc.
 EQUAL HOUSING O P P O R T U N I T Y Justus Property Management, Inc. RENTAL APPLICATION Marketing info: How did you hear about the property? Please include a $16.00 fee for each adult household member.
EQUAL HOUSING O P P O R T U N I T Y Justus Property Management, Inc. RENTAL APPLICATION Marketing info: How did you hear about the property? Please include a $16.00 fee for each adult household member.
2019 English Applica on
 2019 English Applica on (Please Print) Date: First Name Last Name Social Security Address Apt. City State Zip Code Home Phone Cell Phone E-Mail Please place a check by your response or provide the appropriate
2019 English Applica on (Please Print) Date: First Name Last Name Social Security Address Apt. City State Zip Code Home Phone Cell Phone E-Mail Please place a check by your response or provide the appropriate
Dear Prospective Homeowner,
 Dear Prospective Homeowner, Thank you for expressing an interest in partnering with Habitat for Humanity to help build and occupy a new home. The application process of our homeownership program is detailed
Dear Prospective Homeowner, Thank you for expressing an interest in partnering with Habitat for Humanity to help build and occupy a new home. The application process of our homeownership program is detailed
GREEK CATHOLIC UNION OF THE USA (Herein called GCU)
") GREEK CATHOLIC UNION OF THE USA (Herein called GCU) 5400 TUSCARAWAS ROAD, BEAVER, PENNSYLVANIA 15009-9513 1-800-722-4428 IMMEDIATE ANNUITY APPLICATION (Please print) Is the Proposed Annuitant a member
GREEK CATHOLIC UNION OF THE USA (Herein called GCU) 5400 TUSCARAWAS ROAD, BEAVER, PENNSYLVANIA 15009-9513 1-800-722-4428 IMMEDIATE ANNUITY APPLICATION (Please print) Is the Proposed Annuitant a member
**If you have any other questions, please contact us and we will be happy to help.**
 Attention GGRC Public Partnerships, LLC 7776 S Pointe Pkwy W Suite 5 Phoenix, AZ 8544 Worker First name, Last name Worker Mailing Address, Address 2 Worker City, State, Zip Dear Worker This packet includes
Attention GGRC Public Partnerships, LLC 7776 S Pointe Pkwy W Suite 5 Phoenix, AZ 8544 Worker First name, Last name Worker Mailing Address, Address 2 Worker City, State, Zip Dear Worker This packet includes
APPLICATION FOR OCCUPANCY
 Equal OFFICE USE ONLY /Time Received: Housing Opportunity Erskine Community Homes APPLICATION FOR OCCUPANCY PLEASE PRINT - RETURN COMPLETED APPLICATION TO: GREATER MINNESOTA MANAGEMENT 210 GARFIELD AVENUE,
Equal OFFICE USE ONLY /Time Received: Housing Opportunity Erskine Community Homes APPLICATION FOR OCCUPANCY PLEASE PRINT - RETURN COMPLETED APPLICATION TO: GREATER MINNESOTA MANAGEMENT 210 GARFIELD AVENUE,
(see instructions) 9 City 10 State 11 ZIP code 12 Country (if not U.S.) 13 Occupation, profession, or business Bloomsburg P A accountant
 9 City 10 State 11 ZIP code 12 Country (if not U.S.) 13 Occupation, profession, or business Bloomsburg P A accountant") IRS Form 8300 (Rev. July 2012) OMB No. 1545-0892 Department of the Treasury Internal Revenue Service Report of Cash Payments Over $10,000 Received in a Trade or Business See instructions for definition
IRS Form 8300 (Rev. July 2012) OMB No. 1545-0892 Department of the Treasury Internal Revenue Service Report of Cash Payments Over $10,000 Received in a Trade or Business See instructions for definition
3. Mailing address Apt # City State ZIP code
 Form 13614-C (October 2018) You will need: Tax Information such as Forms W-2, 1099, 1098, 1095. Social security cards or ITIN letters for all persons on your tax return. Picture ID (such as valid driver's
Form 13614-C (October 2018) You will need: Tax Information such as Forms W-2, 1099, 1098, 1095. Social security cards or ITIN letters for all persons on your tax return. Picture ID (such as valid driver's
Branson Public Schools
 Branson Public Schools Dr. Don Forrest, Assistant Superintendent of Business Services 1756 Bee Creek Rd Branson, MO 65616 Phone: 417.334.6541 uww.branson.k12.mo.us Fax: 417.332.2510 Amy Mulvaney, Administrative
Branson Public Schools Dr. Don Forrest, Assistant Superintendent of Business Services 1756 Bee Creek Rd Branson, MO 65616 Phone: 417.334.6541 uww.branson.k12.mo.us Fax: 417.332.2510 Amy Mulvaney, Administrative
APPLICATION FOR APARTMENTS. NAME: Last First Middle. ADDRESS: Street City State Zip Code TELEPHONE #: HOME WORK MESSAGE. * Social Security #
 1 APPLICATION FOR APARTMENTS NAME: Last First Middle ADDRESS: Street City State Zip Code TELEPHONE #: HOME WORK MESSAGE APARTMENT SIZE REQUESTED Directions to Applicant: Answer all questions on this application.
1 APPLICATION FOR APARTMENTS NAME: Last First Middle ADDRESS: Street City State Zip Code TELEPHONE #: HOME WORK MESSAGE APARTMENT SIZE REQUESTED Directions to Applicant: Answer all questions on this application.
CDBG HOME OWNER REPAIR PROGRAM APPLICATION CHECKLIST
 CDBG HOME OWNER REPAIR PROGRAM APPLICATION CHECKLIST City of LaPorte Office of Community Development & Planning 801 Michigan Ave., LaPorte, IN 46350 Phone: (219) 362-8260 FAX: (219) 325-0656 CDBG Home
CDBG HOME OWNER REPAIR PROGRAM APPLICATION CHECKLIST City of LaPorte Office of Community Development & Planning 801 Michigan Ave., LaPorte, IN 46350 Phone: (219) 362-8260 FAX: (219) 325-0656 CDBG Home
Birth date (month/day/year) Place of birth Your Medicare claim number (if any)
 Place of birth Your Medicare claim number (if any)") State of Maine Department of Health and Human Services (DHHS) Application For MaineCare, Food Supplement and Other Benefits Application for: MaineCare Full Benefits Low Cost Drugs (DEL) / MaineRx Plus
State of Maine Department of Health and Human Services (DHHS) Application For MaineCare, Food Supplement and Other Benefits Application for: MaineCare Full Benefits Low Cost Drugs (DEL) / MaineRx Plus
RECEIVED BY THE HRA Date: Time: APPLICATION FOR PUBLIC AND SECTION 8 NEW CONSTRUCTION HOUSING ASSISTANCE Equal Housing Opportunity
 RECEIVED BY THE HRA Date: Time: APPLICATION FOR PUBLIC AND SECTION 8 NEW CONSTRUCTION HOUSING ASSISTANCE Equal Housing Opportunity Applicant Name: First Middle Initial Last Co-Applicant: First Middle Initial
RECEIVED BY THE HRA Date: Time: APPLICATION FOR PUBLIC AND SECTION 8 NEW CONSTRUCTION HOUSING ASSISTANCE Equal Housing Opportunity Applicant Name: First Middle Initial Last Co-Applicant: First Middle Initial
Application and Tenant Selection Information
 1277 Shoreline Lane Boise, Idaho 83702 (208) 336-4610 Phone ~ (208) 345-8990 Fax, TDD #1-800-545-1833 Ext. 298 Application and Tenant Selection Information Completed applications for the should be returned
1277 Shoreline Lane Boise, Idaho 83702 (208) 336-4610 Phone ~ (208) 345-8990 Fax, TDD #1-800-545-1833 Ext. 298 Application and Tenant Selection Information Completed applications for the should be returned
EMP NAME: DEPT CODE LOCATION: B/G CHK: N/A COMPLETED START DATE: PAY RATE: TAX CODES: ( FILLED BY OFFICE ONLY ) LIVE IN WORK IN LST
 LIVE IN WORK IN LST") APPLICATION MGR: EMP # EMP NAME: DEPT CODE LOCATION: B/G CHK: N/A COMPLETED START DATE: PAY RATE: DAYS TO WORK: Mon Tues Wed Thurs Fri Sat Sun SCHEDULED HOURS: - PART TIME FULL TIME (30 hours or more )
APPLICATION MGR: EMP # EMP NAME: DEPT CODE LOCATION: B/G CHK: N/A COMPLETED START DATE: PAY RATE: DAYS TO WORK: Mon Tues Wed Thurs Fri Sat Sun SCHEDULED HOURS: - PART TIME FULL TIME (30 hours or more )
Mailing Address (Street) (Apt) Telephone Numbers: Work: ( ) - Home: ( ) - (City) (State) (Zip Code) Other: ( ) -
 (Apt) Telephone Numbers: Work: ( ) - Home: ( ) - (City) (State) (Zip Code) Other: ( ) -") CITY OF ORANGE CITY HUMAN RESOURCES AN EQUAL OPPORTUNITY EMPLOYER 205 EAST GRAVES AVENUE ORANGE CITY, FL 32763 (386-775-5457) THE CITY OF ORANGE CITY ONLY ACCEPTS APPLICATIONS FOR OPEN POSITIONS Instructions:
CITY OF ORANGE CITY HUMAN RESOURCES AN EQUAL OPPORTUNITY EMPLOYER 205 EAST GRAVES AVENUE ORANGE CITY, FL 32763 (386-775-5457) THE CITY OF ORANGE CITY ONLY ACCEPTS APPLICATIONS FOR OPEN POSITIONS Instructions:
Frequently Asked Questions
 Arlington Public Schools Food Service Program 869 Massachusetts Ave Arlington, MA 02476 Phone: 781-316-3643 Fax: 781-316-3644 Dear Parent/Guardian: Children need healthy meals to learn. The Arlington Public
Arlington Public Schools Food Service Program 869 Massachusetts Ave Arlington, MA 02476 Phone: 781-316-3643 Fax: 781-316-3644 Dear Parent/Guardian: Children need healthy meals to learn. The Arlington Public
Certificate of Foreign Status of Beneficial Owner for United States Tax Withholding
 Form W-8BEN Certificate of Foreign Status of Beneficial Owner for United States Tax Withholding (Rev. February 2006) OMB No. 1545-1621 Department of the Treasury Section references are to the Internal
Form W-8BEN Certificate of Foreign Status of Beneficial Owner for United States Tax Withholding (Rev. February 2006) OMB No. 1545-1621 Department of the Treasury Section references are to the Internal
1) To be eligible for this property, you must be at least 55 years of age to qualify. Income limits do apply.
 To be eligible for this property, you must be at least 55 years of age to qualify. Income limits do apply.") INSTRUCTIONS FOR COMPLETING THE APPLICATION FOR THE INN AT CITY HALL: Thank you for your interest. The following instructions, if followed properly, will ensure timely processing of your application and
INSTRUCTIONS FOR COMPLETING THE APPLICATION FOR THE INN AT CITY HALL: Thank you for your interest. The following instructions, if followed properly, will ensure timely processing of your application and
APPLICATION FOR EMPLOYMENT
 APPLICATION FOR EMPLOYMENT EDWARDS, Inc. EDWARDS/Greenville, Inc EDWARDS/Wilmington, Inc Employment Desired: Position Desired: This Company Is An Equal Opportunity Employer This company is subject to E-Verify
APPLICATION FOR EMPLOYMENT EDWARDS, Inc. EDWARDS/Greenville, Inc EDWARDS/Wilmington, Inc Employment Desired: Position Desired: This Company Is An Equal Opportunity Employer This company is subject to E-Verify
DISTRIBUTION /DIRECT ROLLOVER/TRANSFER REQUEST 401(a) Plan Refer to the Participant Distribution Instructions while completing this form.
 Plan Refer to the Participant Distribution Instructions while completing this form.") DISTRIBUTION /DIRECT ROLLOVER/TRANSFER REQUEST 401(a) Plan Refer to the Participant Distribution Instructions while completing this form. Virginia Cash Match Plan 650272 If still employed, refer to Section
DISTRIBUTION /DIRECT ROLLOVER/TRANSFER REQUEST 401(a) Plan Refer to the Participant Distribution Instructions while completing this form. Virginia Cash Match Plan 650272 If still employed, refer to Section
HOMEOWNERSHIP APPLICATION (Rev. 3/16/17) = Submit a copy of each requested item to the application
 = Submit a copy of each requested item to the application") PART 1: Applicant(s) Information HOMEOWNERSHIP APPLICATION (Rev. 3/16/17) = Submit a copy of each requested item to the application Application deadline: no exceptions APPLICANT (Head of Household owner
PART 1: Applicant(s) Information HOMEOWNERSHIP APPLICATION (Rev. 3/16/17) = Submit a copy of each requested item to the application Application deadline: no exceptions APPLICANT (Head of Household owner
Please scan or take a picture of documents below.
 9027 Blewett Road Beaumont, TX 77705 409-794-3833 (Office) 409-794-9989 (Fax) Please scan or take a picture of documents below. Driver s License/ ID Card (Required for employment) Social Security Card
9027 Blewett Road Beaumont, TX 77705 409-794-3833 (Office) 409-794-9989 (Fax) Please scan or take a picture of documents below. Driver s License/ ID Card (Required for employment) Social Security Card
Introducing CashPay. The payroll card that delivers convenience and purchasing power. CashPay Card Guide
 Introducing CashPay The payroll card that delivers convenience and purchasing power CashPay Card Guide Get started with CashPay card convenience now When you enroll to have your pay direct deposited to
Introducing CashPay The payroll card that delivers convenience and purchasing power CashPay Card Guide Get started with CashPay card convenience now When you enroll to have your pay direct deposited to
Employment Application
 Personal Information Name (Last, First, MI) Date Email Position Applying For? What pay rate are you looking to make? How did you hear about the position? Position Specifications and Work Certifications
Personal Information Name (Last, First, MI) Date Email Position Applying For? What pay rate are you looking to make? How did you hear about the position? Position Specifications and Work Certifications
Housing Authority for the City of Amery 300 North Harriman Avenue Amery, WI (phone) (fax)
 (fax)") Housing Authority for the City of Amery 300 North Harriman Avenue Amery, WI 54001 715-268-2500 (phone) 715-268-7700 (fax) aha@amerytel.net Office Use Only: (/Time stamp) Programs Applying For: (Check all
Housing Authority for the City of Amery 300 North Harriman Avenue Amery, WI 54001 715-268-2500 (phone) 715-268-7700 (fax) aha@amerytel.net Office Use Only: (/Time stamp) Programs Applying For: (Check all
Application for Benefits Medicaid Buy-In for Children
 Texas Health and Human Services Commission Form H1200-MBIC Cover Letter January 2011 Application for Benefits Medicaid Buy-In for Children About this program: Medicaid Buy-In for Children can help pay
Texas Health and Human Services Commission Form H1200-MBIC Cover Letter January 2011 Application for Benefits Medicaid Buy-In for Children About this program: Medicaid Buy-In for Children can help pay
1. APPLICANT INFORMATION. Co-Applicant (spouse must be Co-Applicant) Name Male Female Name Male Female
 Name Male Female Name Male Female") Return by on to: Habitat for Humanity of Greater Plainfield & Middlesex County 2 Randolph Road Plainfield, NJ 07060 Include 25 processing fee in check or money order only. Questions? Call Plainfield Habitat
Return by on to: Habitat for Humanity of Greater Plainfield & Middlesex County 2 Randolph Road Plainfield, NJ 07060 Include 25 processing fee in check or money order only. Questions? Call Plainfield Habitat
Name (First) (Middle) (Last) Address. (City) (State) (Zip Code) (Home Phone Number) (Cell Phone Number) ( Address)
 (Middle) (Last) Address. (City) (State) (Zip Code) (Home Phone Number) (Cell Phone Number) ( Address)") Date Name (First) (Middle) (Last) Address (Number) (Street) (City) (State) (Zip Code) (Home Phone Number) (Cell Phone Number) (Email Address) List previous addresses within last 5 years Are you over 18
Date Name (First) (Middle) (Last) Address (Number) (Street) (City) (State) (Zip Code) (Home Phone Number) (Cell Phone Number) (Email Address) List previous addresses within last 5 years Are you over 18
APPLICATION FOR RESIDENCY
 Please note: Each adult 18 years of age and older needs to complete a separate application unless a married couple. APPLICANT INFORMATION Name: Spouse: Current Address: Telephone: Email: Bedroom Size Requested:
Please note: Each adult 18 years of age and older needs to complete a separate application unless a married couple. APPLICANT INFORMATION Name: Spouse: Current Address: Telephone: Email: Bedroom Size Requested:
Hanover Public Schools
 Hanover Public Schools Dear Parent/Guardian: FREQUENTLY ASKED QUESTIONS ABOUT FREE AND REDUCED PRICE SCHOOL MEALS Children need healthy meals to learn. Hanover Public Schools offers healthy meals every
Hanover Public Schools Dear Parent/Guardian: FREQUENTLY ASKED QUESTIONS ABOUT FREE AND REDUCED PRICE SCHOOL MEALS Children need healthy meals to learn. Hanover Public Schools offers healthy meals every
What is a household? Be honest on this form
 1. About Lifeline Lifeline is a federal benefit that lowers the monthly cost of phone or internet service. Rules If you qualify, your household can get Lifeline for phone or internet service, but not both.
1. About Lifeline Lifeline is a federal benefit that lowers the monthly cost of phone or internet service. Rules If you qualify, your household can get Lifeline for phone or internet service, but not both.
YOU MUST MEET THE FOLLOWING BASIC REQUIREMENTS TO BE CONSIDERED FOR SELECTION:
 YOU MUST MEET THE FOLLOWING BASIC REQUIREMENTS TO BE CONSIDERED FOR SELECTION: You must have attended a Homeowner Information Meeting within the past 6 months. You must have lived or worked in Lee or Hendry
YOU MUST MEET THE FOLLOWING BASIC REQUIREMENTS TO BE CONSIDERED FOR SELECTION: You must have attended a Homeowner Information Meeting within the past 6 months. You must have lived or worked in Lee or Hendry
Pleasant Oaks of Stillwater
 Pleasant Oaks of Stillwater 207 East Pleasant Hill Drive Guthrie, OK 73044 Phone: 405-742-7887 Fax: 405-293-9260 Email: Dear Applicant, Thank you for your interest in Pleasant Oaks of Stillwater. We look
Pleasant Oaks of Stillwater 207 East Pleasant Hill Drive Guthrie, OK 73044 Phone: 405-742-7887 Fax: 405-293-9260 Email: Dear Applicant, Thank you for your interest in Pleasant Oaks of Stillwater. We look
MAYOR BYRON W. BROWN S SUMMER YOUTH INTERNSHIP PROGRAM APPLICATION
 MAYOR BYRON W. BROWN S SUMMER YOUTH INTERNSHIP PROGRAM February 1, 2018 Dear Applicant: Thank you for your interest in applying for my 2018 Summer Youth Internship Program. This is truly a wonderful opportunity
MAYOR BYRON W. BROWN S SUMMER YOUTH INTERNSHIP PROGRAM February 1, 2018 Dear Applicant: Thank you for your interest in applying for my 2018 Summer Youth Internship Program. This is truly a wonderful opportunity
OMB APPROVAL EDITION What is a household? Be honest on this form. You may need to show other documents
 1. About Lifeline Lifeline is a federal benefit that lowers the monthly cost of phone or internet service. Rules If you qualify, your household can get Lifeline for phone or internet service, but not both.
1. About Lifeline Lifeline is a federal benefit that lowers the monthly cost of phone or internet service. Rules If you qualify, your household can get Lifeline for phone or internet service, but not both.
Preliminary Rental Application
 OP 241 For Office Use Only Rec d Time Rec d Initials Preliminary Rental Application Please note that this is a preliminary application and gives no lease or rent rights. Community Office ( ) Unit Size
OP 241 For Office Use Only Rec d Time Rec d Initials Preliminary Rental Application Please note that this is a preliminary application and gives no lease or rent rights. Community Office ( ) Unit Size
Application Adult & Dislocated Worker Programs
 Application Adult & Dislocated Worker Programs Workforce Innovation and Opportunity Act (WIOA) FORM WIOA I-B 1.1 For Adult and Dislocated Worker Programs If you are age 18 or older and need help in obtaining
Application Adult & Dislocated Worker Programs Workforce Innovation and Opportunity Act (WIOA) FORM WIOA I-B 1.1 For Adult and Dislocated Worker Programs If you are age 18 or older and need help in obtaining
In order to process your application, we find it necessary to charge an application fee. The fee is $17 for one adult or $34 for two or more adults.
 Dear Applicant: In order to process your application, we find it necessary to charge an application fee. The fee is $17 for one adult or $34 for two or more adults. This is a NON-REFUNDABLE FEE, even if
Dear Applicant: In order to process your application, we find it necessary to charge an application fee. The fee is $17 for one adult or $34 for two or more adults. This is a NON-REFUNDABLE FEE, even if
Prototype Application for Free and Reduced-price School Meals or Free Milk
 2015-2016 Prototype Application for Free and Reduced-price School Meals or Free Milk Complete one application per household. Please use a pen (not a pencil). Apply online at www.abcdefgh.edu Application
2015-2016 Prototype Application for Free and Reduced-price School Meals or Free Milk Complete one application per household. Please use a pen (not a pencil). Apply online at www.abcdefgh.edu Application
PRE-EMPLOYMENT CHECKLIST
 PRE-EMPLOYMENT CHECKLIST MANAGER TO COMPLETE THIS FORM NOT EMPLOYEE New Hire/Re-Hire Employment Forms Employee Name. Position Store # First day of work Pay Rate. Send to the Payroll Department for all
PRE-EMPLOYMENT CHECKLIST MANAGER TO COMPLETE THIS FORM NOT EMPLOYEE New Hire/Re-Hire Employment Forms Employee Name. Position Store # First day of work Pay Rate. Send to the Payroll Department for all
HOW TO APPLY FOR FREE AND REDUCED PRICE SCHOOL MEALS
 HOW TO APPLY FOR FREE AND REDUCED PRICE SCHOOL MEALS Please use these instructions to help you fill out the application for free or reduced price school meals. You only need to submit one application per
HOW TO APPLY FOR FREE AND REDUCED PRICE SCHOOL MEALS Please use these instructions to help you fill out the application for free or reduced price school meals. You only need to submit one application per
EMPLOYMENT APPLICATION
 EMPLOYMENT APPLICATION POSITION APPLYING FOR: APPLICATION DATE: PERSONAL LAST NAME FIRST NAME MI PRIOR NAME(S), IF APPLICABLE MAILING ADDRESS CITY STATE ZIP WORK PHONE HOME PHONE CELL PHONE EMAIL ADDRESS
EMPLOYMENT APPLICATION POSITION APPLYING FOR: APPLICATION DATE: PERSONAL LAST NAME FIRST NAME MI PRIOR NAME(S), IF APPLICABLE MAILING ADDRESS CITY STATE ZIP WORK PHONE HOME PHONE CELL PHONE EMAIL ADDRESS
Laclede Electric Cooperative Application For Employment
 Laclede Electric Cooperative Application For Employment It is the policy of Laclede Electric Cooperative (LEC) to provide equal opportunity with regard to all terms and conditions of employment. No information
Laclede Electric Cooperative Application For Employment It is the policy of Laclede Electric Cooperative (LEC) to provide equal opportunity with regard to all terms and conditions of employment. No information
Massachusetts Application for Free and Reduced Price School Meals
 Grade STEP 1 2016-2017 Massachusetts Application for Free and Reduced Price School Meals If you have received a Notice of Direct Certification from the school district for free meals, do not complete this
Grade STEP 1 2016-2017 Massachusetts Application for Free and Reduced Price School Meals If you have received a Notice of Direct Certification from the school district for free meals, do not complete this
OMB APPROVAL EDITION What is a household? Be honest on this form. You may need to show other documents
 1. About Lifeline Lifeline is a federal benefit that lowers the monthly cost of phone or internet service. Rules If you qualify, your household can get Lifeline for phone or internet service, but not both.
1. About Lifeline Lifeline is a federal benefit that lowers the monthly cost of phone or internet service. Rules If you qualify, your household can get Lifeline for phone or internet service, but not both.