NEW EMPLOYEE PACK STATUS: MANAGERS/SUPERVISORS. For questions or additional assistance with completing your paperwork, please reach out to:
|
|
|
- Anne Simon
- 6 years ago
- Views:
Transcription

1 NEW EMPLOYEE PACK STATUS: MANAGERS/SUPERVISORS For questions or additional assistance with completing your paperwork, please reach out to: Alice Paul, HR Assistant x a p a u a i m n t l s. c o m DIGITAL DOCS COMPLETE PAPERWORK ONLINE, SAVE TIME & INSTANTLY SUBMIT! You can request a link to the forms from your recruiter anytime. UPLOAD YOUR IDs You can submit your identification for your IRS tax forms digitally too! No need to bring those sensitive documents to work with you! You can send us copies of your driver s license, medical card, social security card, birth certificate and/or passport. The secured upload portal can be used with your computer, tablet or smart phone. p o r t a l. t e n s t r e e t. c o m / a i m n a t i o n a l A I M T R A N S P O R T A T I O N S O L U T I O N S A I M L e a s i n g C o m p a n y A I M I n t e g r a t e d L o g i s t i c s A I M S e r v i c e s C o m p a n y
2 A I M N E W E M P L O Y E E P A C K STATUS: MANAGERS/SUPERVISORS Notes/Questions sheet Government Forms Federal I-9 form Federal W-4 form State Tax form (if applicable) Health & Benefits Forms Anthem Medical, Dental & Vision Enrollment Spouse Eligibility Form Bravo Wellness Questionnaire Dearborn Life Insurance Enrollment 401(K) Beneficiary Designation Form Affordable Health Care notice New Employee Forms Direct Deposit Authorization Form ADP Pay Stub Viewing Instructions Voluntary Self Identification Form Company Communication & Emergency Contact Form AIM Photo & Video Release Form AIM Substance Form and Drug Free Workplace Policy DDTA HIPAA Release Certificate of Violations for Annual Reviews Certificate of Driver s License Compliance AIM Protective Eyewear Policy AIM Accident & Injury Reporting Procedures Company & Driver Policy Handbook OSHA Hazard Standard Rule OSHA Hazard GHS Booklet OSHA Hazard Quiz Reasonable Suspicion Checklist Reasonable Suspicion Quiz A I M T R A N S P O R T A T I O N S O L U T I O N S A I M L e a s i n g C o m p a n y A I M I n t e g r a t e d L o g i s t i c s A I M S e r v i c e s C o m p a n y

3 Employment Eligibility Verification Department of Homeland Security U.S. Citizenship and Immigration Services USCIS Form I-9 OMB No Expires 08/31/2019 START HERE: Read instructions carefully before completing this form. The instructions must be available, either in paper or electronically, during completion of this form. Employers are liable for errors in the completion of this form. ANTI-DISCRIMINATION NOTICE: It is illegal to discriminate against work-authorized individuals. Employers CANNOT specify which document(s) an employee may present to establish employment authorization and identity. The refusal to hire or continue to employ an individual because the documentation presented has a future expiration date may also constitute illegal discrimination. Section 1. Employee Information and Attestation (Employees must complete and sign Section 1 of Form I-9 no later than the first day of employment, but not before accepting a job offer.) Last Name (Family Name) First Name (Given Name) Middle Initial Other Last Names Used (if any) Address (Street Number and Name) Apt. Number City or Town State ZIP Code Date of Birth (mm/dd/yyyy) U.S. Social Security Number Employee's Address Employee's Telephone Number - - I am aware that federal law provides for imprisonment and/or fines for false statements or use of false documents in connection with the completion of this form. I attest, under penalty of perjury, that I am (check one of the following boxes): 1. A citizen of the United States 2. A noncitizen national of the United States (See instructions) 3. A lawful permanent resident (Alien Registration Number/USCIS Number): 4. An alien authorized to work until (expiration date, if applicable, mm/dd/yyyy): Some aliens may write "N/A" in the expiration date field. (See instructions) Aliens authorized to work must provide only one of the following document numbers to complete Form I-9: An Alien Registration Number/USCIS Number OR Form I-94 Admission Number OR Foreign Passport Number. QR Code - Section 1 Do Not Write In This Space 1. Alien Registration Number/USCIS Number: OR 2. Form I-94 Admission Number: OR 3. Foreign Passport Number: Country of Issuance: Signature of Employee Today's Date (mm/dd/yyyy) Preparer and/or Translator Certification (check one): I did not use a preparer or translator. A preparer(s) and/or translator(s) assisted the employee in completing Section 1. (Fields below must be completed and signed when preparers and/or translators assist an employee in completing Section 1.) I attest, under penalty of perjury, that I have assisted in the completion of Section 1 of this form and that to the best of my knowledge the information is true and correct. Signature of Preparer or Translator Today's Date (mm/dd/yyyy) Last Name (Family Name) First Name (Given Name) Address (Street Number and Name) City or Town State ZIP Code Employer Completes Next Page Form I-9 07/17/17 N Page 1 of 3
4 Employment Eligibility Verification Department of Homeland Security U.S. Citizenship and Immigration Services USCIS Form I-9 OMB No Expires 08/31/2019 Section 2. Employer or Authorized Representative Review and Verification (Employers or their authorized representative must complete and sign Section 2 within 3 business days of the employee's first day of employment. You must physically examine one document from List A OR a combination of one document from List B and one document from List C as listed on the "Lists of Acceptable Documents.") Employee Info from Section 1 Last Name (Family Name) First Name (Given Name) M.I. Citizenship/Immigration Status List A OR List B AND List C Identity and Employment Authorization Identity Employment Authorization Document Title Document Title Document Title Issuing Authority Document Number Issuing Authority Document Number Issuing Authority Document Number Expiration Date (if any)(mm/dd/yyyy) Expiration Date (if any)(mm/dd/yyyy) Expiration Date (if any)(mm/dd/yyyy) Document Title Issuing Authority Document Number Additional Information QR Code - Sections 2 & 3 Do Not Write In This Space Expiration Date (if any)(mm/dd/yyyy) Document Title Issuing Authority Document Number Expiration Date (if any)(mm/dd/yyyy) Certification: I attest, under penalty of perjury, that (1) I have examined the document(s) presented by the above-named employee, (2) the above-listed document(s) appear to be genuine and to relate to the employee named, and (3) to the best of my knowledge the employee is authorized to work in the United States. The employee's first day of employment (mm/dd/yyyy): (See instructions for exemptions) Signature of Employer or Authorized Representative Today's Date (mm/dd/yyyy) Title of Employer or Authorized Representative Last Name of Employer or Authorized Representative First Name of Employer or Authorized Representative Employer's Business or Organization Name Employer's Business or Organization Address (Street Number and Name) City or Town State ZIP Code Section 3. Reverification and Rehires (To be completed and signed by employer or authorized representative.) A. New Name (if applicable) B. Date of Rehire (if applicable) Last Name (Family Name) First Name (Given Name) Middle Initial Date (mm/dd/yyyy) C. If the employee's previous grant of employment authorization has expired, provide the information for the document or receipt that establishes continuing employment authorization in the space provided below. Document Title Document Number Expiration Date (if any) (mm/dd/yyyy) I attest, under penalty of perjury, that to the best of my knowledge, this employee is authorized to work in the United States, and if the employee presented document(s), the document(s) I have examined appear to be genuine and to relate to the individual. Signature of Employer or Authorized Representative Today's Date (mm/dd/yyyy) Name of Employer or Authorized Representative Form I-9 07/17/17 N Page 2 of 3
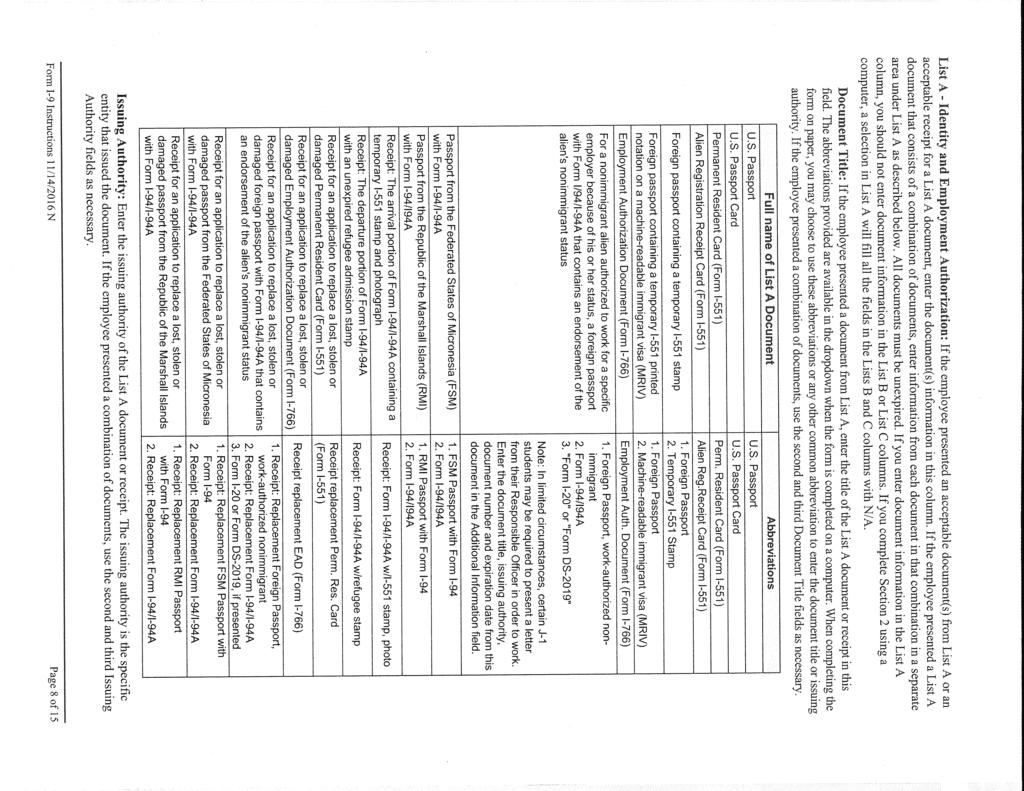
5 LISTS OF ACCEPTABLE DOCUMENTS All documents must be UNEXPIRED Employees may present one selection from List A or a combination of one selection from List B and one selection from List C. LIST A Documents that Establish Both Identity and Employment Authorization LIST B LIST C Documents that Establish Employment Authorization OR Documents that Establish Identity AND 1. U.S. Passport or U.S. Passport Card 2. Permanent Resident Card or Alien Registration Receipt Card (Form I-551) 3. Foreign passport that contains a temporary I-551 stamp or temporary I-551 printed notation on a machinereadable immigrant visa 4. Employment Authorization Document that contains a photograph (Form I-766) 5. For a nonimmigrant alien authorized to work for a specific employer because of his or her status: a. Foreign passport; and b. Form I-94 or Form I-94A that has the following: (1) The same name as the passport; and (2) An endorsement of the alien's nonimmigrant status as long as that period of endorsement has not yet expired and the proposed employment is not in conflict with any restrictions or limitations identified on the form. 6. Passport from the Federated States of Micronesia (FSM) or the Republic of the Marshall Islands (RMI) with Form I-94 or Form I-94A indicating nonimmigrant admission under the Compact of Free Association Between the United States and the FSM or RMI 1. Driver's license or ID card issued by a State or outlying possession of the United States provided it contains a photograph or information such as name, date of birth, gender, height, eye color, and address 2. ID card issued by federal, state or local government agencies or entities, provided it contains a photograph or information such as name, date of birth, gender, height, eye color, and address 3. School ID card with a photograph 4. Voter's registration card 5. U.S. Military card or draft record 6. Military dependent's ID card 7. U.S. Coast Guard Merchant Mariner Card 8. Native American tribal document 9. Driver's license issued by a Canadian government authority For persons under age 18 who are unable to present a document listed above: 10. School record or report card 11. Clinic, doctor, or hospital record 12. Day-care or nursery school record 1. A Social Security Account Number card, unless the card includes one of the following restrictions: (1) NOT VALID FOR EMPLOYMENT (2) VALID FOR WORK ONLY WITH INS AUTHORIZATION (3) VALID FOR WORK ONLY WITH DHS AUTHORIZATION 2. Certification of report of birth issued by the Department of State (Forms DS-1350, FS-545, FS-240) 3. Original or certified copy of birth certificate issued by a State, county, municipal authority, or territory of the United States bearing an official seal 4. Native American tribal document 5. U.S. Citizen ID Card (Form I-197) 6. Identification Card for Use of Resident Citizen in the United States (Form I-179) 7. Employment authorization document issued by the Department of Homeland Security Examples of many of these documents appear in Part 13 of the Handbook for Employers (M-274). Refer to the instructions for more information about acceptable receipts. Form I-9 07/17/17 N Page 3 of 3
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22 Form W-4 (2017) Purpose. Complete Form W-4 so that your employer can withhold the correct federal income tax from your pay. Consider completing a new Form W-4 each year and when your personal or financial situation changes. Exemption from withholding. If you are exempt, complete only lines 1, 2, 3, 4, and 7 and sign the form to validate it. Your exemption for 2017 expires February 15, See Pub. 505, Tax Withholding and Estimated Tax. Note: If another person can claim you as a dependent on his or her tax return, you can t claim exemption from withholding if your total income exceeds $1,050 and includes more than $350 of unearned income (for example, interest and dividends). Exceptions. An employee may be able to claim exemption from withholding even if the employee is a dependent, if the employee: Is age 65 or older, Is blind, or Will claim adjustments to income; tax credits; or itemized deductions, on his or her tax return. The exceptions don t apply to supplemental wages greater than $1,000,000. Basic instructions. If you aren t exempt, complete the Personal Allowances Worksheet below. The worksheets on page 2 further adjust your withholding allowances based on itemized deductions, certain credits, adjustments to income, or two-earners/multiple jobs situations. Complete all worksheets that apply. However, you may claim fewer (or zero) allowances. For regular wages, withholding must be based on allowances you claimed and may not be a flat amount or percentage of wages. Head of household. Generally, you can claim head of household filing status on your tax return only if you are unmarried and pay more than 50% of the costs of keeping up a home for yourself and your dependent(s) or other qualifying individuals. See Pub. 501, Exemptions, Standard Deduction, and Filing Information, for information. Tax credits. You can take projected tax credits into account in figuring your allowable number of withholding allowances. Credits for child or dependent care expenses and the child tax credit may be claimed using the Personal Allowances Worksheet below. See Pub. 505 for information on converting your other credits into withholding allowances. Nonwage income. If you have a large amount of nonwage income, such as interest or dividends, consider making estimated tax payments using Form 1040-ES, Estimated Tax for Individuals. Otherwise, you may owe additional tax. If you have pension or annuity income, see Pub. 505 to find out if you should adjust your withholding on Form W-4 or W-4P. Two earners or multiple jobs. If you have a working spouse or more than one job, figure the total number of allowances you are entitled to claim on all jobs using worksheets from only one Form W-4. Your withholding usually will be most accurate when all allowances are claimed on the Form W-4 for the highest paying job and zero allowances are claimed on the others. See Pub. 505 for details. Nonresident alien. If you are a nonresident alien, see Notice 1392, Supplemental Form W-4 Instructions for Nonresident Aliens, before completing this form. Check your withholding. After your Form W-4 takes effect, use Pub. 505 to see how the amount you are having withheld compares to your projected total tax for See Pub. 505, especially if your earnings exceed $130,000 (Single) or $180,000 (Married). Future developments. Information about any future developments affecting Form W-4 (such as legislation enacted after we release it) will be posted at Personal Allowances Worksheet (Keep for your records.) A Enter 1 for yourself if no one else can claim you as a dependent A You re single and have only one job; or B Enter 1 if: You re married, have only one job, and your spouse doesn t work; or... B { } Your wages from a second job or your spouse s wages (or the total of both) are $1,500 or less. C Enter 1 for your spouse. But, you may choose to enter -0- if you are married and have either a working spouse or more than one job. (Entering -0- may help you avoid having too little tax withheld.) C D Enter number of dependents (other than your spouse or yourself) you will claim on your tax return D E Enter 1 if you will file as head of household on your tax return (see conditions under Head of household above).. E F Enter 1 if you have at least $2,000 of child or dependent care expenses for which you plan to claim a credit... F (Note: Do not include child support payments. See Pub. 503, Child and Dependent Care Expenses, for details.) G Child Tax Credit (including additional child tax credit). See Pub. 972, Child Tax Credit, for more information. If your total income will be less than $70,000 ($100,000 if married), enter 2 for each eligible child; then less 1 if you have two to four eligible children or less 2 if you have five or more eligible children. If your total income will be between $70,000 and $84,000 ($100,000 and $119,000 if married), enter 1 for each eligible child. G H Add lines A through G and enter total here. (Note: This may be different from the number of exemptions you claim on your tax return.) H { If you plan to itemize or claim adjustments to income and want to reduce your withholding, see the Deductions For accuracy, and Adjustments Worksheet on page 2. complete all If you are single and have more than one job or are married and you and your spouse both work and the combined worksheets earnings from all jobs exceed $50,000 ($20,000 if married), see the Two-Earners/Multiple Jobs Worksheet on page 2 that apply. to avoid having too little tax withheld. If neither of the above situations applies, stop here and enter the number from line H on line 5 of Form W-4 below. Separate here and give Form W-4 to your employer. Keep the top part for your records. Employee s Withholding Allowance Certificate Form W-4 Department of the Treasury Whether you are entitled to claim a certain number of allowances or exemption from withholding is Internal Revenue Service subject to review by the IRS. Your employer may be required to send a copy of this form to the IRS. 1 Your first name and middle initial Last name OMB No Your social security number Home address (number and street or rural route) 3 Single Married Married, but withhold at higher Single rate. Note: If married, but legally separated, or spouse is a nonresident alien, check the Single box. City or town, state, and ZIP code 4 If your last name differs from that shown on your social security card, check here. You must call for a replacement card. 5 Total number of allowances you are claiming (from line H above or from the applicable worksheet on page 2) 5 6 Additional amount, if any, you want withheld from each paycheck $ 7 I claim exemption from withholding for 2017, and I certify that I meet both of the following conditions for exemption. Last year I had a right to a refund of all federal income tax withheld because I had no tax liability, and This year I expect a refund of all federal income tax withheld because I expect to have no tax liability. If you meet both conditions, write Exempt here Under penalties of perjury, I declare that I have examined this certificate and, to the best of my knowledge and belief, it is true, correct, and complete. Employee s signature (This form is not valid unless you sign it.) Date 8 Employer s name and address (Employer: Complete lines 8 and 10 only if sending to the IRS.) 9 Office code (optional) 10 Employer identification number (EIN) For Privacy Act and Paperwork Reduction Act Notice, see page 2. Cat. No Q Form W-4 (2017)
23 Form W-4 (2017) Page 2 Deductions and Adjustments Worksheet Note: Use this worksheet only if you plan to itemize deductions or claim certain credits or adjustments to income. 1 Enter an estimate of your 2017 itemized deductions. These include qualifying home mortgage interest, charitable contributions, state and local taxes, medical expenses in excess of 10% of your income, and miscellaneous deductions. For 2017, you may have to reduce your itemized deductions if your income is over $313,800 and you re married filing jointly or you re a qualifying widow(er); $287,650 if you re head of household; $261,500 if you re single, not head of household and not a qualifying widow(er); or $156,900 if you re married filing separately. See Pub. 505 for details $ $12,700 if married filing jointly or qualifying widow(er) 2 Enter: $9,350 if head of household $ { } $6,350 if single or married filing separately 3 Subtract line 2 from line 1. If zero or less, enter $ 4 Enter an estimate of your 2017 adjustments to income and any additional standard deduction (see Pub. 505) 4 $ 5 Add lines 3 and 4 and enter the total. (Include any amount for credits from the Converting Credits to Withholding Allowances for 2017 Form W-4 worksheet in Pub. 505.) $ 6 Enter an estimate of your 2017 nonwage income (such as dividends or interest) $ 7 Subtract line 6 from line 5. If zero or less, enter $ 8 Divide the amount on line 7 by $4,050 and enter the result here. Drop any fraction Enter the number from the Personal Allowances Worksheet, line H, page Add lines 8 and 9 and enter the total here. If you plan to use the Two-Earners/Multiple Jobs Worksheet, also enter this total on line 1 below. Otherwise, stop here and enter this total on Form W-4, line 5, page 1 10 Two-Earners/Multiple Jobs Worksheet (See Two earners or multiple jobs on page 1.) Note: Use this worksheet only if the instructions under line H on page 1 direct you here. 1 Enter the number from line H, page 1 (or from line 10 above if you used the Deductions and Adjustments Worksheet) 1 2 Find the number in Table 1 below that applies to the LOWEST paying job and enter it here. However, if you are married filing jointly and wages from the highest paying job are $65,000 or less, do not enter more than If line 1 is more than or equal to line 2, subtract line 2 from line 1. Enter the result here (if zero, enter -0- ) and on Form W-4, line 5, page 1. Do not use the rest of this worksheet Note: If line 1 is less than line 2, enter -0- on Form W-4, line 5, page 1. Complete lines 4 through 9 below to figure the additional withholding amount necessary to avoid a year-end tax bill. 4 Enter the number from line 2 of this worksheet Enter the number from line 1 of this worksheet Subtract line 5 from line Find the amount in Table 2 below that applies to the HIGHEST paying job and enter it here $ 8 Multiply line 7 by line 6 and enter the result here. This is the additional annual withholding needed.. 8 $ 9 Divide line 8 by the number of pay periods remaining in For example, divide by 25 if you are paid every two weeks and you complete this form on a date in January when there are 25 pay periods remaining in Enter the result here and on Form W-4, line 6, page 1. This is the additional amount to be withheld from each paycheck 9 $ Table 1 Table 2 Married Filing Jointly All Others Married Filing Jointly All Others If wages from LOWEST paying job are Enter on line 2 above $0 - $7, ,001-14, ,001-22, ,001-27, ,001-35, ,001-44, ,001-55, ,001-65, ,001-75, ,001-80, ,001-95, , , , , , , , , ,001 and over 15 If wages from LOWEST paying job are Enter on line 2 above $0 - $8, ,001-16, ,001-26, ,001-34, ,001-44, ,001-70, ,001-85, , , , , , , ,001 and over 10 Privacy Act and Paperwork Reduction Act Notice. We ask for the information on this form to carry out the Internal Revenue laws of the United States. Internal Revenue Code sections 3402(f)(2) and 6109 and their regulations require you to provide this information; your employer uses it to determine your federal income tax withholding. Failure to provide a properly completed form will result in your being treated as a single person who claims no withholding allowances; providing fraudulent information may subject you to penalties. Routine uses of this information include giving it to the Department of Justice for civil and criminal litigation; to cities, states, the District of Columbia, and U.S. commonwealths and possessions for use in administering their tax laws; and to the Department of Health and Human Services for use in the National Directory of New Hires. We may also disclose this information to other countries under a tax treaty, to federal and state agencies to enforce federal nontax criminal laws, or to federal law enforcement and intelligence agencies to combat terrorism. If wages from HIGHEST paying job are Enter on line 7 above $0 - $75,000 $610 75, ,000 1, , ,000 1, , ,000 1, , ,000 1, ,001 and over 1,600 If wages from HIGHEST paying job are Enter on line 7 above $0 - $38,000 $610 38,001-85,000 1,010 85, ,000 1, , ,000 1, ,001 and over 1,600 You are not required to provide the information requested on a form that is subject to the Paperwork Reduction Act unless the form displays a valid OMB control number. Books or records relating to a form or its instructions must be retained as long as their contents may become material in the administration of any Internal Revenue law. Generally, tax returns and return information are confidential, as required by Code section The average time and expenses required to complete and file this form will vary depending on individual circumstances. For estimated averages, see the instructions for your income tax return. If you have suggestions for making this form simpler, we would be happy to hear from you. See the instructions for your income tax return.
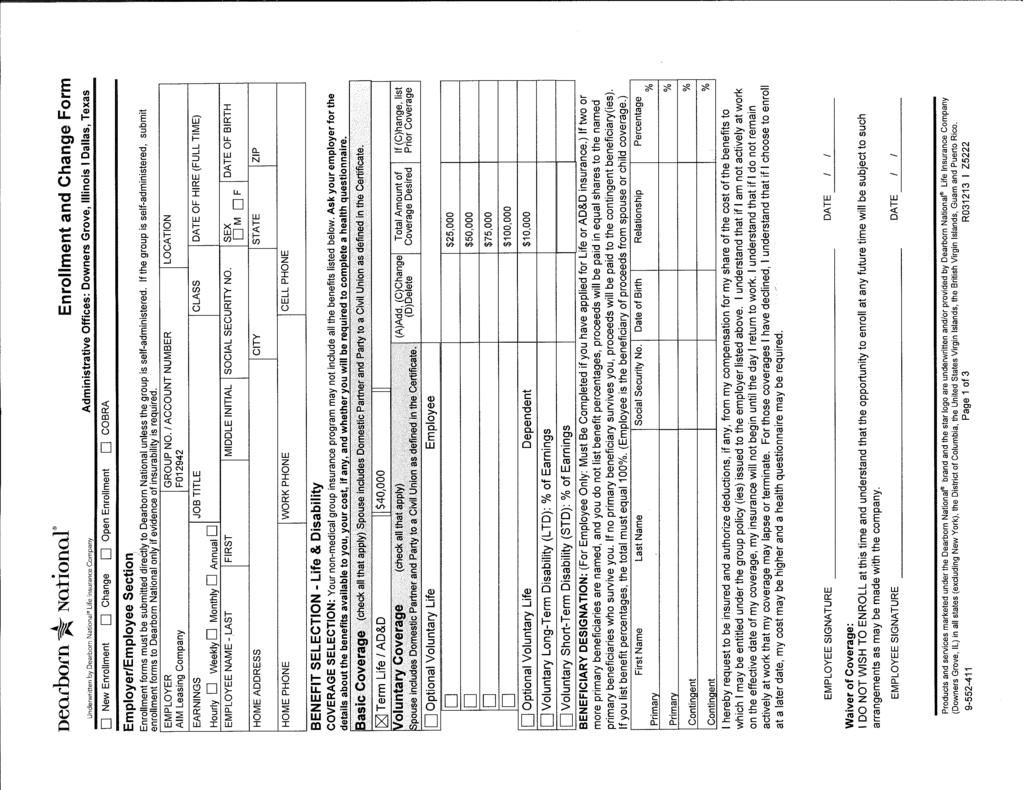
24 Employee Enrollment Application Your Anthem enrollment application is inside. It is essential that you read it carefully and complete all necessary sections. If you are a new enrollee }} Applying for health, vision and/or dental benefits, please complete Sections 1, 3, 4, 5, 6, 7, 8 and 9. Your signature is required in Section 9. }} Waiving any or all benefits, please complete Sections 1, 4, and 10. Your signature is required in Section 10. If you are adding a dependent(s) Complete Section 2 in addition to the above. It is important that you read and understand the Significant Terms, Conditions and Authorizations in Section 9. Thank you for choosing Anthem Blue Cross and Blue Shield. Note: You may be required to supply additional information. Anthem provides administrative claims payment services only, and does not assume any financial risk or obligation with respect to claims. A-77 LG-ASO Rev. 12/10 Anthem Blue Cross and Blue Shield is the trade name of: In Indiana: Anthem Insurance Companies, Inc. In Kentucky: Anthem Health Plans of Kentucky, Inc. In Missouri (excluding 30 counties in the Kansas City area): RightCHOICE Managed Care, Inc. (RIT), Healthy Alliance Life Insurance Company (HALIC), and HMO Missouri, Inc. RIT and certain affiliates administer non-hmo benefits underwritten by HALIC and HMO benefits underwritten by HMO Missouri, Inc. RIT and certain affiliates only provide administrative services for self-funded plans and do not underwrite benefits. In Ohio: Community Insurance Company. In Wisconsin: Blue Cross Blue Shield of Wisconsin ( BCBSWi ), which underwrites or administers the PPO and indemnity policies; Compcare Health Services Insurance Corporation ( Compcare ), which underwrites or administers the HMO policies; and Compcare and BCBSWi collectively, which underwrite or administer the POS policies. Independent licensees of the Blue Cross and Blue Shield Association. ANTHEM is a registered trademark of Anthem Insurance Companies, Inc. The Blue Cross and Blue Shield names and symbols are the registered marks of the Blue Cross and Blue Shield Association. Page 1 of 5
25 Enrollment Application Anthem provides administrative claims payment services only, and does not assume any financial risk or obligation with respect to claims. Please complete this form in ink and return to your employer. Use extra sheets of paper if necessary. All information given should apply to this employer. Anthem s Primary Care Physician (PCP) listings, for HMO/POS products can be obtained through EMPLOYER USE ONLY Group no. Sub-group no. Applicant no./dept. name Request effective date (MM/DD/YYYY) Employer name Address (please include suite no., city, state, ZIP code) ANTHEM USE ONLY Plan PCP COB m Yes m No m Yes m No Health effective date (MM/DD/YYYY) Dental effective date (MM/DD/YYYY) Vision effective date (MM/DD/YYYY) Pre-ex date (MM/DD/YYYY) Section 1. REASON FOR APPLICATION m New enrollment m Waiver m Add dependent (see Section 2) m Rehire (event date) m New hire m Annual open enrollment m COBRA Qualifying event m Conversion (event date) Section 2. STATUS CHANGE/EVENT m Event date (MM/DD/YYYY) m Marriage m Birth m Adoption* m Legal guardianship* m Other *Include legal documentation. Section 3. TYPE OF COVERAGE/PLAN Health coverage Dental coverage Vision coverage m HMO* 1 (except Ohio) m EPO (Ohio only) m PPO m POS m Blue Traditional m Anthem Essential SM Choice PPO m Blue Access SM Hospital Surgical PPO (IN, KY, OH only) m Blue Access SM Choice Hospital Surgical PPO (MO only) m Blue Preferred ASO/EPO m Lumenos Health Savings Account m Lumenos Health Reimbursement Account m Lumenos Health Incentive Account m Lumenos Health Incentive Account Plus m Anthem Essential SM PPO m Anthem Essential SM Select (MO only) m Blue Access SM Hospital Surgical PPO (MO only) m Blue Preferred Select (MO only) m Blue Preferred Plus Hospital Surgical POS (WI only) 1 Ohio only-a health insuring corporation product or HIC Anthem will facilitate the opening of a Health Savings Account in your name, if directed by your Employer. m PPO m Traditional (IN, OH only) m Dental Blue 100/200/300 m Dental Blue 100 m Vision m Employee only m Employee and spouse m Employee and child(ren) m Family coverage m No coverage m Employee only m Employee and spouse m Employee and child(ren) m Family coverage m No coverage m Employee only m Employee and spouse m Employee and child(ren) m Family coverage m No coverage Section 4. EMPLOYEE INFORMATION (*Only complete Primary Care Physician (PCP) information when enrolling in HMO or POS products.) Social security no. (required) Last name First name M.I. Age Date of birth (MM/DD/YYYY) Home address (street, city, state, ZIP code) County (KY residents include municipality) m Single m Divorced m Married Sex m M m F Home phone Work phone address Are you retired? Are you disabled? Are you hospitalized? m Yes m No m Yes m No m Yes m No Occupation Full-time hire date (MM/DD/YYYY) Income reported by Hours working per week m W2 m 1099 m Other Anthem PCP name* Anthem PCP address* Anthem PCP ID no.* New patient?* A-77 LG-ASO Rev. 12/10 m Yes m No Page 2 of 5
26 Policyholder name Policyholder social security no. Section 5. FAMILY INFORMATION Spouse and dependents to be enrolled. Attach a separate sheet if necessary. Please read the Genetic Information Non-discrimination Act (GINA) information under Significant Terms, Conditions and Authorizations section, prior to answering questions below. 1 Relationship to employee: m Spouse m Domestic Partner (DP) Dependent name (last name, first name, M.I.) Social security no. (required for spouse or DP) Sex Date of birth Is dependent s address different than applicant s address? m Yes m No If yes, please provide full address m M m F Court ordered health care benefits? m Yes m No (If Yes, include legal documentation) Currently hospitalized or disabled? m Yes m No (If Yes, give reason) Anthem PCP name* Anthem PCP address* Anthem PCP ID no.* New patient?* 2 Relationship to employee: m Son m Daughter m Other Dependent name (last name, first name, M.I.) Social security no. Sex Date of birth Is dependent s address different than applicant s address? m Yes m No If yes, please provide full address m M m F Court ordered health care benefits? m Yes m No (If Yes, include legal documentation) m Yes m No Currently hospitalized or disabled? m Yes m No (If Yes, give reason) Anthem PCP name* Anthem PCP address* Anthem PCP ID no.* New patient?* 3 Relationship to employee: m Son m Daughter m Other Dependent name (last name, first name, M.I.) Social security no. Sex Date of birth Is dependent s address different than applicant s address? m Yes m No If yes, please provide full address m M m F Court ordered health care benefits? m Yes m No (If Yes, include legal documentation) m Yes m No Currently hospitalized or disabled? m Yes m No (If Yes, give reason) Anthem PCP name* Anthem PCP address* Anthem PCP ID no.* New patient?* Section 6. OTHER HEALTH COVERAGE Please check one: Yes (complete below) No On the day your coverage begins, list family members, including yourself, who will be covered by any other health coverage. Name of person(s) covered Relationship to employee Name of the HMO or insurance company Policy/certificate no. m Self m Spouse m Child(ren) m Yes m No Address of the HMO or insurance company Phone no. of HMO or insurance company Effective date (MM/DD/YYYY) Policyholder name Policyholder social security no. Policyholder date of birth Section 7. MEDICARE COVERAGE If you or your dependents are enrolled in Medicare or Medicaid, complete the following. 1 Name of enrollee (last name, first name, M.I.) Medicare Part A effective date Medicare Part B effective date Medicare/Medicaid ID no. ESRD onset date Medicare Part D ID no. Medicare Part D carrier Reason for Medicare entitlement Medicare Part D effective date Medicare Part D term date m Age m Disability m End stage renal disease (ESRD) m ESRD and disability 2 Name of enrollee (last name, first name, M.I.) Medicare Part A effective date Medicare Part B effective date Medicare/Medicaid ID no. ESRD onset date Medicare Part D ID no. Medicare Part D carrier Reason for Medicare entitlement Medicare Part D effective date Medicare Part D term date m Age m Disability m End stage renal disease (ESRD) m ESRD and disability *Only complete Primary Care Physician (PCP) information for HMO or POS products. A-77 LG-ASO Rev. 12/10 Page 3 of 5
27 Policyholder name Policyholder social security no. Section 8. PRIOR HEALTH COVERAGE. Please check one: Yes (complete below) No Have you been covered by Anthem within the past two (2) years? m Yes m No Group name/id no. Dates policy in effect Policy/Certificate no. Have you and/or your dependents had prior coverage with another carrier(s) in the past two (2) years? m Yes m No Section 9. SIGNIFICANT TERMS, CONDITIONS AND AUTHORIZATION (TERMS) Genetic Information Non-discrimination Act (GINA): When answering questions on this enrollment application, the information provided for each individual should include only information about that individual, and should not include any genetic information. Genetic information includes family medical history and information related to the individual s genetic testing, genetic services, genetic counseling, or genetic diseases for which the individual may be at risk. All responses pertaining to an individual will only be considered and applied to the individual in question. Health Savings Account Notice: Except as otherwise provided in any agreement between me and the financial custodian, the custodian of my Health Savings Account (HSA), I understand that my authorization is required before the financial custodian may provide Anthem Blue Cross and Blue Shield with information regarding my HSA. I hereby authorize the financial custodian to provide Anthem Blue Cross and Blue Shield with information about my HSA, including account number, account balance and information, regarding account activity. I also understand that I may provide Anthem Blue Cross and Blue Shield with a written request to revoke my authorization at any time. Please read this section carefully before signing the application. 1. I may not assign any payment under my Anthem Blue Cross and Blue Shield administered benefit plan. 2. I authorize deduction from my wages/pension, if necessary for the required payment for the benefit for which I, or any dependents have applied. 3. I am applying for the benefit selected on this application. If I select a coverage, or combination of coverages, not available to me and/or a class for which I am not eligible, I agree that my selection(s) is hereby automatically amended to be consistent with the employer s application. 4. I understand that, to the extent permitted by law, Anthem reserves the right to accept or decline this application and that no right whatsoever is created by this application. I also understand that this coverage, if approved, may exclude for pre-existing conditions. 5. I am responsible to timely notify my employer of any change that would make me or any dependent ineligible for benefits. 6. By signing this application, I agree and consent to the recording and/or monitoring of any telephone conversation between Anthem and myself. I acknowledge that I have read the Significant Terms, Conditions and Authorizations, and I accept such provisions as a condition of enrollment. I represent that the answers given to all questions on this application are true and accurate to the best of my knowledge and I understand they are being relied on by Anthem in accepting this application. I understand that any misstatements or failure to report new medical information prior to my effective date may result in a material change to benefits or rates. Any material misrepresentation or significant omission found in this application may result to denial of benefits or rescission or cancellation of my benefits. Ohio: Any person who, with intent to defraud or knowing that he or she is facilitating a fraud against an insurer, submits an application or files a claim containing false or deceptive statement is guilty of insurance fraud. Kentucky: Any person who knowingly and with intent to defraud any insurance company, health maintenance organization, self-insured plan, or other person, files an application for insurance or other form of health care coverage containing any materially false information or conceals, for the purpose of misleading, information concerning any fact material thereto commits a fraudulent insurance act, which is a crime. I give this authorization for and on behalf of any eligible dependents and myself if covered by the Plan. I am acting as their agent and representative. Your health benefit plan will be administered by one of the following companies based upon the state in which your employer is located: In Indiana: Anthem Blue Cross and Blue Shield is the trade name of Anthem Insurance Companies, Inc. In Kentucky: Anthem Blue Cross and Blue Shield is the trade name of Anthem Health Plans of Kentucky, Inc. In Missouri: Anthem Blue Cross and Blue Shield is the trade name of RightCHOICE Managed Care, Inc. (RIT), Healthy Alliance Life Insurance Company (HALIC), and HMO Missouri, Inc. RIT and certain affiliates administer non-hmo benefits underwritten by HALIC and HMO benefits underwritten by HMO Missouri, Inc. In Ohio: Anthem Blue Cross and Blue Shield is the trade name of Community Insurance Company. In WIsconsin: Anthem Blue Cross and Blue Shield is the trade name of Blue Cross Blue Shield of Wisconsin ( BCBSWi ), which underwrites or administers the PPO and indemnity policies; Compcare Health Services Insurance Corporation ( Compcare ), which underwrites or administers the HMO policies; and Compcare and BCBSWi collectively, which underwrite or administer the POS policies. Thank you for choosing Anthem Blue Cross and Blue Shield. List prior carrier(s) Dates policy in effect Please check the type of prior coverage: m Employee only m Employee and spouse m Employee and child(ren) m Employee/spouse/child(ren) Termination reason: m Divorce/legal separation m Death of spouse m COBRA coverage exhausted m Group plan terminated m Employer/group contribution ceased m Employment terminated m Other Read the TERMS section above carefully before signing. Please review your application for errors or omissions. By signing this, I am indicating that I have read and understand the language in the TERMS section of this application and agree to all of its terms. Applicant signature X A-77 LG-ASO Rev. 12/10 Date Page 4 of 5
28 Policyholder name Policyholder social security no. Section 10. WAIVER OF COVERAGE For employee and/or any eligible dependent not enrolling. Check all that apply: Waiving: m Health m Dental m Vision m Life m All Name of person waiving Already protected by coverage of: m Spouse m Parent m None Employer name Carrier: m Anthem (give certificate/policy no.) m Other carrier (give name, ID no.) Check all that apply: Waiving: m Health m Dental m Vision m Life m All Name of person waiving Already protected by coverage of: m Spouse m Parent m None Employer name Carrier: m Anthem (give certificate/policy no.) m Other carrier (give name, ID no.) Check all that apply: Waiving: m Health m Dental m Vision m Life m All Name of person waiving Already protected by coverage of: m Spouse m Parent m None Employer name Carrier: m Anthem (give certificate/policy no.) m Other carrier (give name, ID no.) Check all that apply: Waiving: m Health m Dental m Vision m Life m All Name of person waiving Already protected by coverage of: m Spouse m Parent m None Employer name Carrier: m Anthem (give certificate/policy no.) m Other carrier (give name, ID no.) Check all that apply: Waiving: m Health m Dental m Vision m Life m All Name of person waiving Already protected by coverage of: m Spouse m Parent m None Employer name Carrier: m Anthem (give certificate/policy no.) m Other carrier (give name, ID no.) I certify that I have been given an opportunity to apply for the employer s health benefits plan, and after careful consideration, have decided not to take advantage of this offer. In the event I wish to apply for such benefits hereafter, I may do so, subject to established procedures. If I am declining enrollment for myself or my dependents (including my spouse) because of other health insurance coverage, I may in the future be able to enroll myself or my dependents in this plan, provided that enrollment is requested within 31 days after other coverage ends. My dependent(s) or I may be subject to pre-existing condition restrictions or waiting periods specified in the group benefit booklet, if a dependent or I are late enrollees. The pre-existing exclusion may not apply to a dependent who is enrolled in the plan prior to his/her 19 th Birthday. In addition, if I have a dependent as a result of marriage, birth, adoption or placement for adoption. I may be able to enroll myself and my dependents provided that I request enrollment within 31 days after the marriage, birth, adoption or placement of adoption. I also understand that my dependents and I may enroll under two additional circumstances: }} Either my or my dependent s Medicaid or Children s Health Insurance Program (CHIP) coverage is terminated as a result of loss of eligibility; or }} My dependent or I become eligible for a subsidy (state premium assistance program). In these cases, I may be able to enroll myself and my dependents provided that I request enrollment within 60 days of the loss of Medicaid/CHIP or of the eligibility determination. Applicant signature X A-77 LG-ASO Rev. 12/10 Date Page 5 of 5
29 Spouse Eligibility Certification for Aim NationaLease/Aim Integrated Logistics Employees As a result of the recently negotiated Aim NationaLease/Aim Integrated Logistics agreement, each employee who has spousal coverage is required to return the attached form completed in its entirety. The Spouse Eligibility section must be completed by you and your spouse (front). The Spouse Insurance Verification Form (back) must be completed by your spouse s employer. The entire form, front & back, must be completed, signed, and returned to Human Resources by your eligibility date. I do not have a spouse. I carry family coverage for myself and my dependents. PLEASE STOP, SIGN ON THE REVERSE SIDE AND RETURN FORM. My Spouse is: Employed Not Employed Is group medical insurance available to your spouse through his/her employment? Yes No I HEREBY ELECT HEALTH COVERAGE FOR MY SPOUSE AS FOLLOWS: My spouse WILL enroll in his/her employer s health benefit plan. My Spouse WILL NOT enroll in his/her employer s health benefit plan. I understand my spouse will remain as a covered dependent under the Aim NationaLease/Aim Integrated Logistics plan and that I will pay $ per month by payroll deduction for my spouse s coverage. My spouse WILL enroll in my health plan since he/she is not employed or has benefits available to him/her (employer must complete the back if employed). I HEREBY CERTIFY THAT THE EMPLOYEE AND SPOUSE INFORMATION ON THIS FORM IS CORRECT, and understand that, to ensure benefits are coordinated properly between employers and plans Aim NationaLease/Aim Integrated Logistics will verify the accuracy of information by conducting audits, contacting me, and contacting my spouse s employer. I further certify my election and authorization above. I FURTHER CERTIFY that if my spouse s status changes, I understand I must notify Aim NationaLease/Aim Integrated Logistics within 30 days of that change. If an employee or dependent, or anyone acting on behalf of either, makes a false statement or withholds relevant information that results in providing coverage or payment in claim, Aim NationaLease/Aim Integrated Logistics and/or its insurer may recover any amounts wrongfully paid, including legal fees. Employees Signature Date Aim NationaLease Human Resources Department 1500 Trumbull Avenue Girard, OH Fax: (330)
30 Spouse Insurance Verification Form TO BE COMPLETED BY THE EMPLOYER OF THE SPOUSE OF THE AIM NATIONALEASE/AIM INTEGRATED LOGISTICS EMPLOYEE (Aim NationaLease/Aim Integrated Logistics employee name) SPOUSE S EMPLOYER INFORMATION EMPLOYEE S NAME (Spouse of Aim NationaLease/Aim Integrated Logistics Employee) SOCIAL SECURITY NUMBER: DATE OF BIRTH: MAILING ADDRESS: BELOW THIS LINE TO BE FILLED OUT BY THE EMPLOYER Do you offer employer-sponsored group medical insurance to employee? Yes No If your answer is YES, please have your employer complete ALL applicable sections below. MEDICAL INSURANCE PLAN INFORMATION PLAN/GROUP # CONTRACT YEAR: From: To: DATE OF OPEN ENROLLMENT PERIOD: FOR EFFECTIVE DATE OF INSURANCE COMPANY NAME: MAILING ADDRESS I HEREBY CERTIFY THAT THE ABOVE EMPLOYER AND PLAN INFORMATION IS CORRECT Spouse s Employer Title Area Code/Phone Administrator Signature Aim NationaLease Human Resources Department 1500 Trumbull Avenue Girard, OH Fax: (330)
 within the last 12 months: o Yes o No Once enrolled in the Anthem Blue Cross Blue Shield plan, I will participate in the online Health Risk Assessment that Anthem")
31 The following questionnaire will determine how many wellness credits you will receive. See the Benefits Compensation Book for further details. I have used nicotine product(s) within the last 12 months: o Yes o No Once enrolled in the Anthem Blue Cross Blue Shield plan, I will participate in the online Health Risk Assessment that Anthem provides at o Yes o No Name Signature Date This form must be turned in with your Anthem BCBS application in order to accurately adjust your contribution level.
32
33
34
35 Beneficiary Designation 401(k) Plan Use black or blue ink when completing this form. For questions regarding this form, contact Service Center at Aim Leasing Company 401(k) Plan A Participant Information Account extension identifies funds transferred to a beneficiary due to death, alternate payee due to divorce Social Security Number Account Extension or a participant with multiple accounts. / / Last Name First Name M.I. Date of Birth ( ) Street Address Personal Phone Number ( ) City State Zip Code Work Phone Number Address Married Unmarried B Primary Beneficiary Designation (Attach an additional sheet to name additional beneficiaries.) If I am married, my Plan requires my spouse as primary beneficiary for 100% or my spouse consents to my beneficiary designation. % / / % of Account Balance Primary Beneficiary Name Relationship Social Security Number Date of Birth Street Address City State Zip Code % / / % of Account Balance Primary Beneficiary Name Relationship Social Security Number Date of Birth Street Address City State Zip Code % / / % of Account Balance Primary Beneficiary Name Relationship Social Security Number Date of Birth Street Address City State Zip Code Contingent Beneficiary Designation % / / % of Account Balance Contingent Beneficiary Name Relationship Social Security Number Date of Birth Street Address City State Zip Code % / / % of Account Balance Contingent Beneficiary Name Relationship Social Security Number Date of Birth Street Address City State Zip Code % / / % of Account Balance Contingent Beneficiary Name Relationship Social Security Number Date of Birth Street Address City State Zip Code C Signatures and Consent Participant Consent I have completed, understand and agree to all pages of this Beneficiary Designation form. Subject to and in accordance with the terms of the Plan, I am making the above beneficiary designations for my vested account in the event of my death. If I have more than one primary beneficiary, the account will be divided as specified. If a primary beneficiary predeceases me, his or her benefit will be allocated to the surviving primary beneficiaries. Contingent beneficiaries will receive a benefit only if there is no surviving primary beneficiary, as specified. If a contingent beneficiary predeceases me, his or her benefit will be allocated to the surviving contingent beneficiaries. If I fail to designate beneficiaries, amounts will be paid pursuant to the terms of the Plan or applicable law. This designation is effective upon execution and delivery to Plan Administrator/Trustee. If any information is missing, additional information may be required prior to recording my designation. This designation supersedes all prior designations. Beneficiaries will share equally if percentages are not provided and any amounts unpaid upon death will be divided equally. Primary and contingent beneficiaries must separately total 100% in whole percentages. ][STD FBENED ][06/09/14 ][Page 1 of 2 ][B01: ][MITA/
36 Last Name First Name M.I. Social Security Number Number Important Notice: In accordance with ERISA and/or Plan Document, if I am married and I elect a primary beneficiary other than my spouse or in addition to my spouse, my spouse must consent by signing the Spousal Consent section of this form. Any person who presents false or fraudulent information is subject to criminal and civil penalties. Participant Signature Spousal Consent Dates of the participant s spouse signature and notarization must match. Date (Required) I, (name of spouse), the current spouse of the participant, hereby voluntarily consent to the participant s primary beneficiary designation above and understand its effect. I understand that my spouse s beneficiary designation means that I will not receive 100% of his or her vested account balance under the Plan and that my spouse s election is not valid unless I consent to it. I understand that by consenting to the beneficiary designation, I give up my right to a qualified survivor annuity. I hereby voluntarily consent to the primary beneficiary(ies) named on the previous page. I understand that my consent is irrevocable unless my spouse revokes the waiver election, changes the beneficiary designation, or designates me to receive 100% of his or her vested account balance. Spouse Signature Witness of Spouse s Signature Date (Required) The spouse s signature must be witnessed by a Notary Public. Statement of Notary NOTE: Notary seal must be visible. State of ) The consent to this request was subscribed and sworn (or affirmed) to before me on this day of, year, by )ss. (name of spouse) proved to me on the basis of satisfactory evidence to be the person who County of ) appeared before me, who affirmed that such consent represents his/her free and voluntary act. SEAL Notary Public Signature My commission expires D Mailing Instructions Participant forward to Employer Employer DO NOT send this form to the Service Center as beneficiary records are not maintained. Please retain this for your records. ][STD FBENED ][06/09/14 ][Page 2 of 2 ][B01: ][MITA/
37 Tartan Insurance or info@tartanagency.com
38 3. Employer nam e 4. Employer Identification Num ber (EIN) Aim Leasing Company Employer address 6. Em ployer phone num ber 1500 Trumbull Ave C ity 8. State 9. ZIP cod e Girard OH W ho can w e contact about employee health coverage at this job? Tartan Insurance Agency 11. Phone number (if different from above) 12. Em ail address info@tartanagency.com Current full time employees who satisfied the company's probationary period. Spouse, natural children, adopted children, stepchildren, spouse's children and anyone under legal guardianship.
39 PF 4 Rev 1/16 DIRECT DEPOSIT AUTHORIZATION I hereby authorize AIM (hereinafter called Company ), to initiate credit entries and to initiate, if necessary, debit entry adjustments for any credit entries in error to my account indicated below and to the depository name below (hereinafter call Depository ), to credit and/or debit the same to such account. DEPOSITORY NAME/BRANCH CITY, STATE, ZIP CODE CHECKING Routing Number NET CHECK Account Number $ SAVINGS Routing Number NET CHECK Account Number $ Through our payroll system, you can have funds directly deposited into a maximum of 3 accounts and any combination of checking and savings accounts however, PLEASE USE ONE FORM PER ACCOUNT. This authorization is to remain in full force and effect until the Company has received written notification from me of its termination in such time and in such manner as to afford Company and Depository a reasonable opportunity to act on it. In addition, should your employment with the company terminated, all direct deposits will be cancelled. Once the authorization form is received by the Company, the information will be verified (pre-noted) before the program is initiated. For accuracy, the Company will run two trial transactions with the Company s financial institution and your designated financial institution. It will take approximately three weeks for the first direct deposit to your account. PRINT NAME SIGNATURE DATE Attach a voided or cancelled check here it is required for processing. Photocopies of either one will due also. NO DEPOSIT SLIPS.
40 VIEW YOUR PAYSTUBS ONLINE The ADP site is very case sensitive, so please enter and remember information that is capitalized and/or lowercase. How to Register on ADP ipaystatements: 1. Go to 2. Enter registration code: aimleasing-aim 3. First Name, Last Name 4. Select Last 4 Digits of SSN, EIN, or ITIN a. enter last 4 of your SSN b. enter last 4 of your SSN again to verify 5. Enter Birth month and day 6. When the pop up appears, click on Register now 7. Enter your contact information 8. Create your user ID and password 9. Confirm password 10. Enter 3 question and answers 11. Click Register now It will then ask you for your contact information like your , it will then you an activation code that you must retrieve from your and then enter into the screen. Once you enter that code it will give you your sign in information. Once you are complete you will use the same website but you will now hit LOG IN and enter your user name and password. AIMHR ADP

41 PF 6 Rev 7-13 VOLUNTARY SELF IDENTIFICATION NAME DATE OF BIRTH Sex: (Circle) Male Female SOCIAL SEC # XXX XX - POSITION APPLIED FOR / CURRENT POSITION RACE/ETHNICITY: Hispanic or Latino A person of Cuban, Mexican, Puerto Rican, South or Central American, or other Spanish culture of origin regardless of race. White (Not Hispanic or Latino) A person having origins in any of the original peoples of Europe, the Middle East, or North Africa. Black or African American (Not Hispanic or Latino) A person having origins in any of the black racial groups of Africa. Native Hawaiian or Other Pacific Islander (Not Hispanic or Latino) A person having origins in any of the peoples of Hawaii, Guam, Samoa, or other Pacific Islands. Asian (Not Hispanic or Latino) A person having origins in any of the original peoples of the Far East, Southeast Asia, or the Indian Subcontinent, including, for example, Cambodia, China, India, Japan, Korea, Malaysia, Pakistan, the Philippine Islands, Thailand, and Vietnam. American Indian or Alaska Native (Not Hispanic or Latino) A person having origins in any of the original peoples of North and South America (including Central America), and who maintain tribal affiliation or community attachment. Two or More Races (Not Hispanic or Latino) All persons who identify with more than one of the above five races. The employer is subject to certain governmental recordkeeping and reporting requirements for the administration of civil rights laws and regulations. In order to comply with these laws, the employer invites employees to voluntarily self- identify their race and ethnicity. Submission of this information is voluntary and refusal to provide it will not subject you to any adverse treatment. The information obtained will be kept confidential and may only be used in accordance with the provisions of applicable laws, executive orders, and regulations, including those that require the information to be summarized and reported to the federal government for civil rights enforcement. When reported, data will not identify any specific individual. ****************************************************************************** *Note to supervisor: If this form is not completed by the applicant, do a visual identification and make notes here: SUPERVISOR SIGNATURE DATE VETERAN STATUS (please check one): I am not a veteran I am a special disabled veteran I am a veteran of the Vietnam era I am a veteran who served on active duty in the U.S. military during a war or in campaign or expedition for which a campaign badge has been authorized I am a recently separated veteran (veterans within one year from discharge or release from active duty) MUST BE RETURNED TO HUMAN RESOURCES EMPLOYEE SIGNATURE DATE
42 C O M P A N Y C O M M U N I C A T I O N & E M E R G E N C Y N O T I F I C A T I O N F O R M Employee Name: Date of Birth: / / Address: City: State: Zip: Home #: ( ) Mobile #: ( ) FOR INTERNAL COMMUNICATION: company-wide broadcasts, notifications and memos. ie. open enrollment, united way, general social media. Name: Phone#: ( ) Please add my family member to company communication. Name: Relationship: Phone#: ( ) EMERGENCY CONTACT: Name: Relationship: Home #: ( ) Mobile #: ( ) Work #: ( ) ALTERNATE EMERGENCY CONTACT: Name: Relationship: Home #: ( ) Mobile #: ( ) Work #: ( ) PLEASE USE THE BACK OF THE FORM IF YOU WOULD LIKE TO ADD ANY ADDITIONAL CONTACTS. Please complete this form and return it Human Resources in Girard, OH.


43 E M P L O Y E E P H O T O & V I D E O R E L E A S E F O R M I hereby grant AIM Leasing Company the right to use photographs and/or video recordings taken of me by agents or employees of the company for training, promotional or advertising purposes related to AIM Leasing Company. This permission includes, without limitation, the right to reproduce these images and/or video in various printed publications, displays, electronic/online media, broadcast opportunities and other means, where applicable. I understand that all photos and/or video recordings taken are without compensation to me, the undersigned, and are the property of AIM Leasing Company. (Signature) (Date) (Printed or Typed Name) (Phone) (Address) (City, State, Zip)
Separate here and give Form W-4 to your employer. Keep the top part for your records. Employee s Withholding Allowance Certificate
 Form W-4 (2017) Purpose. Complete Form W-4 so that your employer can withhold the correct federal income tax from your pay. Consider completing a new Form W-4 each year and when your personal or financial
Form W-4 (2017) Purpose. Complete Form W-4 so that your employer can withhold the correct federal income tax from your pay. Consider completing a new Form W-4 each year and when your personal or financial
Employment Eligibility Verification
 Employment Eligibility Verification Department of Homeland Security U.S. Citizenship and Immigration Services USCIS Form I-9 OMB No. 1615-0047 Expires 08/31/2019 START HERE: Read instructions carefully
Employment Eligibility Verification Department of Homeland Security U.S. Citizenship and Immigration Services USCIS Form I-9 OMB No. 1615-0047 Expires 08/31/2019 START HERE: Read instructions carefully
Employee Enrollment Application
 Employee Enrollment Application Your Anthem enrollment application is inside. It is essential that you read it carefully and complete all necessary sections. If you are a new enrollee Applying for health,
Employee Enrollment Application Your Anthem enrollment application is inside. It is essential that you read it carefully and complete all necessary sections. If you are a new enrollee Applying for health,
Employment Eligibility Verification
 Employment Eligibility Verification Department of Homeland Security U.S. Citizenship and Immigration Services USCIS Form I-9 OMB No. 1615-0047 Expires 08/31/2019 START HERE: Read instructions carefully
Employment Eligibility Verification Department of Homeland Security U.S. Citizenship and Immigration Services USCIS Form I-9 OMB No. 1615-0047 Expires 08/31/2019 START HERE: Read instructions carefully
CDL DRIVER NEW EMPLOYEE PACK
 CDL DRIVER NEW EMPLOYEE PACK For questions or additional assistance with completing your paperwork, please reach out to: Alice Paul, HR Assistant 8 0 0-8 7 3-5 0 5 9 x 1 8 9 a p a u l @ a i m n t l s.
CDL DRIVER NEW EMPLOYEE PACK For questions or additional assistance with completing your paperwork, please reach out to: Alice Paul, HR Assistant 8 0 0-8 7 3-5 0 5 9 x 1 8 9 a p a u l @ a i m n t l s.
Separate here and give Form W-4 to your employer. Keep the top part for your records. Employee s Withholding Allowance Certificate
 Form W-4 (2017) Purpose. Complete Form W-4 so that your employer can withhold the correct federal income tax from your pay. Consider completing a new Form W-4 each year and when your personal or financial
Form W-4 (2017) Purpose. Complete Form W-4 so that your employer can withhold the correct federal income tax from your pay. Consider completing a new Form W-4 each year and when your personal or financial
New Employment & Sign-up Checklist for Managers and Departmental Representatives
 FLORIDA A&M UNIVERSITY New Employment & Sign-up Checklist for Managers and Departmental Representatives Executive Service A&P USPS OPS Faculty (Please complete Section II Only) Employee Name: Class Title:
FLORIDA A&M UNIVERSITY New Employment & Sign-up Checklist for Managers and Departmental Representatives Executive Service A&P USPS OPS Faculty (Please complete Section II Only) Employee Name: Class Title:
YOU DO NOT NEED TO PRINT THIS PAGE. Substitute Records Requirements. Social Security Card (copies not accepted)
") YOU DO NOT NEED TO PRINT THIS PAGE. Appointment Date & Time: Name: Date: Substitute Records Requirements I-9 (only complete page 1) W-4 Social Security Card (copies not accepted) Driver s License Direct
YOU DO NOT NEED TO PRINT THIS PAGE. Appointment Date & Time: Name: Date: Substitute Records Requirements I-9 (only complete page 1) W-4 Social Security Card (copies not accepted) Driver s License Direct
EMPLOYEE INFORMATION SHEET
 EMPLOYEE INFORMATION SHEET PLEASE PRINT CLEARLY COMPANY: EMPLOYEE #: SOCIAL SECURITY NUMBER: - - NAME: First MI LAST STREET: CITY: AS APPEARS ON SOCIAL SECURITY CARD STATE: ZIP CODE: TELEPHONE NUMBER:
EMPLOYEE INFORMATION SHEET PLEASE PRINT CLEARLY COMPANY: EMPLOYEE #: SOCIAL SECURITY NUMBER: - - NAME: First MI LAST STREET: CITY: AS APPEARS ON SOCIAL SECURITY CARD STATE: ZIP CODE: TELEPHONE NUMBER:
RAYMOND CENTRAL PUBLIC SCHOOLS SUBSTITUTE TEACHER DATA SHEET
 RAYMOND CENTRAL PUBLIC SCHOOLS SUBSTITUTE TEACHER DATA SHEET PLEASE NOTE: We need a voided check for payment by Direct Deposit and we must have an email address. Thank you. W-4 Form I-9 Form - 2 forms
RAYMOND CENTRAL PUBLIC SCHOOLS SUBSTITUTE TEACHER DATA SHEET PLEASE NOTE: We need a voided check for payment by Direct Deposit and we must have an email address. Thank you. W-4 Form I-9 Form - 2 forms
Southeast ID#: Name: SSN: PREVIOUS CIVIL OR COLLEGE DISCIPLINE
 /Student Employment Work Referral Southeast ID#: Name: SSN: STUDENT EMPLOYEE ELIGIBILITY AND RESPONSIBILITIES 1. You must complete, and have on file with Student Financial Services, employment eligibility
/Student Employment Work Referral Southeast ID#: Name: SSN: STUDENT EMPLOYEE ELIGIBILITY AND RESPONSIBILITIES 1. You must complete, and have on file with Student Financial Services, employment eligibility
New Employee Information
 HOUSTON S PREMIER POKER DESTINATION New Employee Information Before you will be scheduled the following MUST be completed: 1. Your new hire packet must be filled out completely and correctly and handed
HOUSTON S PREMIER POKER DESTINATION New Employee Information Before you will be scheduled the following MUST be completed: 1. Your new hire packet must be filled out completely and correctly and handed
Employee Enrollment Application
 Employee Enrollment Application Group Size 51+ Eligible Employees - Medically Underwritten Your Anthem enrollment application is inside. It is essential that you read it carefully and complete all the
Employee Enrollment Application Group Size 51+ Eligible Employees - Medically Underwritten Your Anthem enrollment application is inside. It is essential that you read it carefully and complete all the
Separate here and give Form W-4 to your employer. Keep the top part for your records. Employee s Withholding Allowance Certificate
 Form W-4 (2017) Purpose. Complete Form W-4 so that your employer can withhold the correct federal income tax from your pay. Consider completing a new Form W-4 each year and when your personal or financial
Form W-4 (2017) Purpose. Complete Form W-4 so that your employer can withhold the correct federal income tax from your pay. Consider completing a new Form W-4 each year and when your personal or financial
Graveyard Productions, LLC
 Graveyard Productions, LLC Check here if you are under 18 years old Recruitment Application- 2018 PLEASE PRINT LEGIBLY Applicant Information Full Name: Date: Last First M.I. Address: Street Address Apartment/Unit
Graveyard Productions, LLC Check here if you are under 18 years old Recruitment Application- 2018 PLEASE PRINT LEGIBLY Applicant Information Full Name: Date: Last First M.I. Address: Street Address Apartment/Unit
YOU DO NOT NEED TO PRINT THIS PAGE. Substitute Records Requirements. Social Security Card (copies not accepted)
") YOU DO NOT NEED TO PRINT THIS PAGE. Appointment Date & Time: Name: Date: Substitute Records Requirements I-9 (only complete page 1) W-4 Social Security Card (copies not accepted) Driver s License Direct
YOU DO NOT NEED TO PRINT THIS PAGE. Appointment Date & Time: Name: Date: Substitute Records Requirements I-9 (only complete page 1) W-4 Social Security Card (copies not accepted) Driver s License Direct
EMPLOYEE PORTAL PASSWORD SET UP
 EMPLOYEE PORTAL PASSWORD SET UP Here are some helpful tips to make sure you have access to paystubs and W2 s. Please be sure you include an email address in your new hire paperwork. The first page titled
EMPLOYEE PORTAL PASSWORD SET UP Here are some helpful tips to make sure you have access to paystubs and W2 s. Please be sure you include an email address in your new hire paperwork. The first page titled
December, Following is an overview of the payroll tax rates and other payroll related information in effect in 2019:
 1 December, 2018 It s time again for the annual payroll letter. The following pages include payroll and other miscellaneous information that may be helpful in fulfilling your payroll and related reporting
1 December, 2018 It s time again for the annual payroll letter. The following pages include payroll and other miscellaneous information that may be helpful in fulfilling your payroll and related reporting
Missouri Department of Revenue Employee s Withholding Allowance Certificate
 Form MO W-4 Missouri Department of Revenue Employee s Withholding Allowance Certificate This certificate is for income tax withholding and child support enforcement purposes only. Type or print. Full Name
Form MO W-4 Missouri Department of Revenue Employee s Withholding Allowance Certificate This certificate is for income tax withholding and child support enforcement purposes only. Type or print. Full Name
Separate here and give Form W-4 to your employer. Keep the top part for your records. Employee's Withholding Allowance Certificate
 Form W-4 (2015) Purpose. Complete Form W-4 so that your employer can withhold the correct federal income tax from your pay. Consider completing a new Form W-4 each year and when your personal or financial
Form W-4 (2015) Purpose. Complete Form W-4 so that your employer can withhold the correct federal income tax from your pay. Consider completing a new Form W-4 each year and when your personal or financial
2019 English Applica on
 2019 English Applica on (Please Print) Date: First Name Last Name Social Security Address Apt. City State Zip Code Home Phone Cell Phone E-Mail Please place a check by your response or provide the appropriate
2019 English Applica on (Please Print) Date: First Name Last Name Social Security Address Apt. City State Zip Code Home Phone Cell Phone E-Mail Please place a check by your response or provide the appropriate
LS Contracting Group, Inc. General Contractor & Specialty Restoration
 LS Contracting Group, Inc. General Contractor & Specialty Restoration 5660 N. Elston Ave. Chicago, IL 60646 p: (773) 774-1122 f: (773) 774-5660 lscontracting.com EMPLOYMENT APPLICATION CHECKLIST Name:
LS Contracting Group, Inc. General Contractor & Specialty Restoration 5660 N. Elston Ave. Chicago, IL 60646 p: (773) 774-1122 f: (773) 774-5660 lscontracting.com EMPLOYMENT APPLICATION CHECKLIST Name:
XXXXXX NON-UNION VOUCHER. White - Payroll Company Yellow - Accounting Department Pink - Employee TIME CLOCK RATE ALLOWANCES SPECIAL COMPENSATIONS
 XXXXXX NON-UNION VOUCHER DATE PRODUCTION & PROJECT NAME 1 2 3 LAST NAME FIRST NAME MI STREET ADDRESS CITY STATE ZIP DATE OF BIRTH: IF MINOR PHONE IF NEW IF NEW EMPLOYEE ADDRESS SOCIAL SECURITY NUMBER WORK
XXXXXX NON-UNION VOUCHER DATE PRODUCTION & PROJECT NAME 1 2 3 LAST NAME FIRST NAME MI STREET ADDRESS CITY STATE ZIP DATE OF BIRTH: IF MINOR PHONE IF NEW IF NEW EMPLOYEE ADDRESS SOCIAL SECURITY NUMBER WORK
Branson Public Schools
 Branson Public Schools Dr. Don Forrest, Assistant Superintendent of Business Services 1756 Bee Creek Rd Branson, MO 65616 Phone: 417.334.6541 uww.branson.k12.mo.us Fax: 417.332.2510 Amy Mulvaney, Administrative
Branson Public Schools Dr. Don Forrest, Assistant Superintendent of Business Services 1756 Bee Creek Rd Branson, MO 65616 Phone: 417.334.6541 uww.branson.k12.mo.us Fax: 417.332.2510 Amy Mulvaney, Administrative
Packet A - Forms. If you have any questions, please contact Human Resources at
 Packet A - Forms 2018 TEMPORARY NEW HIRE PAPERWORK Welcome to Union College! This packet contains new hire forms necessary for you to become established as a Union College employee. Please fill out and
Packet A - Forms 2018 TEMPORARY NEW HIRE PAPERWORK Welcome to Union College! This packet contains new hire forms necessary for you to become established as a Union College employee. Please fill out and
New Employee Welcome Letter and Orientation Checklist
 Lafayette DQ Restaurants P.O. Box 302 Delphi, IN 46923 Phone: (765) 447-1089 Fax: (765) 535-5001 New Employee Welcome Letter and Orientation Checklist Welcome to the DQ family! In order to start training
Lafayette DQ Restaurants P.O. Box 302 Delphi, IN 46923 Phone: (765) 447-1089 Fax: (765) 535-5001 New Employee Welcome Letter and Orientation Checklist Welcome to the DQ family! In order to start training
INSTRUCTIONS FOR PAPERWORK ALL FORMS MUST BE SIGNED AND DATED PLEASE PRINT ONE-SIDED SHEETS
 INSTRUCTIONS FOR PAPERWORK ALL FORMS MUST BE SIGNED AND DATED PLEASE PRINT ONE-SIDED SHEETS CFISD EMPLOYEE INFORMATION SHEET Must be LEGIBLE Fill in all blanks You MUST bubble an answer for Part 1-Ethnicity
INSTRUCTIONS FOR PAPERWORK ALL FORMS MUST BE SIGNED AND DATED PLEASE PRINT ONE-SIDED SHEETS CFISD EMPLOYEE INFORMATION SHEET Must be LEGIBLE Fill in all blanks You MUST bubble an answer for Part 1-Ethnicity
Jersey Assistance for Community Caregiving (JACC) Program PEP Enrollment Packet
 Program PEP Enrollment Packet") Public Partnerships Jersey Assistance for Community Caregiving (JACC) Program Phone: 1-866-239-2778 Paperwork Fax: 1-866-547-2481 Paperwork E-mail: njpplfax@pcgus.com Website: www.publicpartnerships.com
Public Partnerships Jersey Assistance for Community Caregiving (JACC) Program Phone: 1-866-239-2778 Paperwork Fax: 1-866-547-2481 Paperwork E-mail: njpplfax@pcgus.com Website: www.publicpartnerships.com
If you want health insurance:
 If you want health insurance: Complete this Anthem application and turn it in to your business manager! If you want a health savings account (and free money!) ollow the directions on page 2. Employer contributions
If you want health insurance: Complete this Anthem application and turn it in to your business manager! If you want a health savings account (and free money!) ollow the directions on page 2. Employer contributions
Please complete in blue or black ink only. Section A: Employee Information Last name First name M.I. Social Security no.
 Employee Enrollment Application For 2 50 Employee Small s Georgia You, the employee, must complete this application. You are solely responsible for its accuracy and completeness. To avoid the possibility
Employee Enrollment Application For 2 50 Employee Small s Georgia You, the employee, must complete this application. You are solely responsible for its accuracy and completeness. To avoid the possibility
Employment Application
 P.O. Box 643 Benavides, Tx 78341 (361) 256-4726 Office (361) 256-4728 Fax Scorp1144@yahoo.com Scorpion Exploration & Production, Inc. Full Name Mailing Address Employment Application Applicant Information
P.O. Box 643 Benavides, Tx 78341 (361) 256-4726 Office (361) 256-4728 Fax Scorp1144@yahoo.com Scorpion Exploration & Production, Inc. Full Name Mailing Address Employment Application Applicant Information
Anthem Health Plans of Kentucky, Inc.
 Employee Enrollment Application For 2 50 Employee Small s Kentucky Anthem Plans of Kentucky, Inc. Anthem Life Insurance Company You, the employee, must complete this application. You are solely responsible
Employee Enrollment Application For 2 50 Employee Small s Kentucky Anthem Plans of Kentucky, Inc. Anthem Life Insurance Company You, the employee, must complete this application. You are solely responsible
EMP NAME: DEPT CODE LOCATION: B/G CHK: N/A COMPLETED START DATE: PAY RATE: TAX CODES: ( FILLED BY OFFICE ONLY ) LIVE IN WORK IN LST
 LIVE IN WORK IN LST") APPLICATION MGR: EMP # EMP NAME: DEPT CODE LOCATION: B/G CHK: N/A COMPLETED START DATE: PAY RATE: DAYS TO WORK: Mon Tues Wed Thurs Fri Sat Sun SCHEDULED HOURS: - PART TIME FULL TIME (30 hours or more )
APPLICATION MGR: EMP # EMP NAME: DEPT CODE LOCATION: B/G CHK: N/A COMPLETED START DATE: PAY RATE: DAYS TO WORK: Mon Tues Wed Thurs Fri Sat Sun SCHEDULED HOURS: - PART TIME FULL TIME (30 hours or more )
EMPLOYER INFORMATION SHEET
 General EMPLOYER INFORMATION SHEET Business Name: Business Address: City, State, Zip: Filing Name (if different): Filing Address (if different): City, State, Zip: Contact Name: Phone: Fax: Email: Company
General EMPLOYER INFORMATION SHEET Business Name: Business Address: City, State, Zip: Filing Name (if different): Filing Address (if different): City, State, Zip: Contact Name: Phone: Fax: Email: Company
Please complete in blue or black ink only. Section A: Employee Information Last name First name M.I. Social Security no.
 Employee Enrollment Application For 1 100 Employee Small s 1 Connecticut You, the employee, must complete this application. You are solely responsible for its accuracy and completeness. To avoid the possibility
Employee Enrollment Application For 1 100 Employee Small s 1 Connecticut You, the employee, must complete this application. You are solely responsible for its accuracy and completeness. To avoid the possibility
Employee Enrollment Application
 Employee Enrollment Application Your Anthem enrollment application is inside. It is essential that you read it carefully and complete all necessary sections. If you are a new enrollee }} Applying for health,
Employee Enrollment Application Your Anthem enrollment application is inside. It is essential that you read it carefully and complete all necessary sections. If you are a new enrollee }} Applying for health,
Warrick County School Corporation
 Warrick County School Corporation SUPERINTENDENT S OFFICE P.O. Box 809/Boonville, Indiana 47601/812-897-0400 Welcome to the Warrick County School Corporation Welcome to the one of the best school corporations
Warrick County School Corporation SUPERINTENDENT S OFFICE P.O. Box 809/Boonville, Indiana 47601/812-897-0400 Welcome to the Warrick County School Corporation Welcome to the one of the best school corporations
Dedicated to Providing the Highest Level of Public Safety Services to our Community
 FIRE CHIEF Lonnie E. Click Dedicated to Providing the Highest Level of Public Safety Services to our Community COMMISSIONERS Earl W. Bill Houchin Jerry F. Morris Gerald D. Sleater INTRODUCTION Thank you
FIRE CHIEF Lonnie E. Click Dedicated to Providing the Highest Level of Public Safety Services to our Community COMMISSIONERS Earl W. Bill Houchin Jerry F. Morris Gerald D. Sleater INTRODUCTION Thank you
NO CONFLICT ATTESTATION. In order to qualify to act as the Personal Assistant for this Consumer, I attest to the ALL of following:
 NO CONFLICT ATTESTATION In order to qualify to act as the Personal Assistant for this Consumer, I attest to the ALL of following: 1. I am NOT the Consumer s Designated Representative. 2. The Consumer is
NO CONFLICT ATTESTATION In order to qualify to act as the Personal Assistant for this Consumer, I attest to the ALL of following: 1. I am NOT the Consumer s Designated Representative. 2. The Consumer is
Please complete in blue or black ink only. Section A: Employee Information Last name First name M.I. Social Security no.
 Employee Enrollment Application For 2 100 Employee Small s Virginia PPO health care plans are insurance products offered by Anthem Blue Cross and Blue Shield; HMO health care plans are health maintenance
Employee Enrollment Application For 2 100 Employee Small s Virginia PPO health care plans are insurance products offered by Anthem Blue Cross and Blue Shield; HMO health care plans are health maintenance
Employee Data Form. [ ] ] ] [ ] ] [ ] _] _]_ ] Home Address Apt City State Zip Code County. Ethnicity: Are you Hispanic/Latino?
![Employee Data Form. [ ] ] ] [ ] ] [ ] _] _]_ ] Home Address Apt City State Zip Code County. Ethnicity: Are you Hispanic/Latino?](/thumbs/79/79502522.jpg "Employee Data Form. [ ] ] ] [ ] ] [ ] _] _]_ ] Home Address Apt City State Zip Code County. Ethnicity: Are you Hispanic/Latino?") Employee Data Form Baltimore City Public Schools Office Of Human Capital 200 E. North Avenue, Room 110 Baltimore, Maryland 21202 www. s New /Rehire employees are required to complete this form as part
Employee Data Form Baltimore City Public Schools Office Of Human Capital 200 E. North Avenue, Room 110 Baltimore, Maryland 21202 www. s New /Rehire employees are required to complete this form as part
ENROLLMENT WORKSHEET. True Life Destinations 4410 Claiborne Sq E # 334 Hampton, Virginia Employee Name: Employee Benefits Worksheet
 True Life Destinations 4410 Claiborne Sq E # 334 Hampton, Virginia 23666 ENROLLMENT WORKSHEET Employee Name: Employee Benefits Worksheet This enrollment worksheet outlines the optioins available to you
True Life Destinations 4410 Claiborne Sq E # 334 Hampton, Virginia 23666 ENROLLMENT WORKSHEET Employee Name: Employee Benefits Worksheet This enrollment worksheet outlines the optioins available to you
Please fill out in blue or black ink only. Section A: Employee Information Last name First name M.I. Social Security no.
 Employee Enrollment Form For Small s New Hampshire You, the employee, must fill out this enrollment form. You must be sure that all the information is correct and that you fill out all the sections that
Employee Enrollment Form For Small s New Hampshire You, the employee, must fill out this enrollment form. You must be sure that all the information is correct and that you fill out all the sections that
New York Small Group Employee Enrollment Application For Groups of (Medical/Vision) For Groups of 1 50 (Dental)
 For Groups of 1 50 (Dental)") New York Small Employee Enrollment Application For s of 1 100 1 (Medical/Vision) For s of 1 50 () You, the employee, must complete this application. You are solely responsible for its accuracy and completeness.
New York Small Employee Enrollment Application For s of 1 100 1 (Medical/Vision) For s of 1 50 () You, the employee, must complete this application. You are solely responsible for its accuracy and completeness.
PPO Enrollment Application
 PPO Enrollment Application Welcome to Anthem Blue Cross and Blue Shield (Anthem). This is your Enrollment Application and Form. Because we are dedicated to making the enrollment process easy for you, this
PPO Enrollment Application Welcome to Anthem Blue Cross and Blue Shield (Anthem). This is your Enrollment Application and Form. Because we are dedicated to making the enrollment process easy for you, this
Employee last name Employee first name M.I. Employee Social Security no.* (required)
") Employee Form For 1 100 Employee Small Groups California Instructions: If you are cancelling coverage for a dependent or changing a name, please provide a reason in the designated sections. Complete electronically,
Employee Form For 1 100 Employee Small Groups California Instructions: If you are cancelling coverage for a dependent or changing a name, please provide a reason in the designated sections. Complete electronically,
APPLICATION CHECKLIST
 PERF/TRF RETIREMENT APPLICATION State Form 945 (R30 / 2-15) Approved by State Board of Accounts, 2015 INDIANA PUBLIC RETIREMENT SYSTEM Telephone: (888) 286-3544 (Toll-free) Web site: www.inprs.in.gov Use
PERF/TRF RETIREMENT APPLICATION State Form 945 (R30 / 2-15) Approved by State Board of Accounts, 2015 INDIANA PUBLIC RETIREMENT SYSTEM Telephone: (888) 286-3544 (Toll-free) Web site: www.inprs.in.gov Use
Personal Fact Sheet (This information is not to be requested before employment)
") Personal Fact Sheet (This information is not to be requested before employment) Self-disclosure of this information is requested for Affirmative Action, insurance and other purposes. It will not in any
Personal Fact Sheet (This information is not to be requested before employment) Self-disclosure of this information is requested for Affirmative Action, insurance and other purposes. It will not in any
SMALL GROUP ENROLLMENT/CHANGE FORM COMPLETE THIS APPLICATION IN ITS ENTIRETY IN BLUE OR BLACK INK. DO NOT USE PENCIL OR HIGHLIGHTER.
 22259 SMALL GROUP ENROLLMENT/CHANGE FORM COMPLETE THIS APPLICATION IN ITS ENTIRETY IN BLUE OR BLACK INK. DO NOT USE PENCIL OR HIGHLIGHTER. q ENROLLING (Complete sections I, II, IV, and V) q WAIVING (Complete
22259 SMALL GROUP ENROLLMENT/CHANGE FORM COMPLETE THIS APPLICATION IN ITS ENTIRETY IN BLUE OR BLACK INK. DO NOT USE PENCIL OR HIGHLIGHTER. q ENROLLING (Complete sections I, II, IV, and V) q WAIVING (Complete
FORMS TO BE COMPLETED AND SUBMITTED TO HUMAN RESOURCES. The College requires all Employees complete and submit the following documents:
 FORMS TO BE COMPLETED AND SUBMITTED TO HUMAN RESOURCES The College requires all Employees complete and submit the following documents: 1. I-9 Employment Eligibility Verification: Complete the I-9 Form
FORMS TO BE COMPLETED AND SUBMITTED TO HUMAN RESOURCES The College requires all Employees complete and submit the following documents: 1. I-9 Employment Eligibility Verification: Complete the I-9 Form
City State ZIP code. Single Married Domestic Partner. Date waiting period begins (MM/DD/YYYY)
") Employee Enrollment Application For 1 100 Employee Small s California care plans offered by Anthem Blue Cross (Anthem). Insurance plans offered by Anthem Blue Cross Life and Insurance Company. You, the
Employee Enrollment Application For 1 100 Employee Small s California care plans offered by Anthem Blue Cross (Anthem). Insurance plans offered by Anthem Blue Cross Life and Insurance Company. You, the
SURRENDER REQUEST FORM. Policy Number: Insured:
 SURRENDER REQUEST FORM Section A Policy Information (You Must Complete This Section) Policy Number: Insured: (First Name) (Last Name) Sec tion B Surrender Request and Withholding Election (You Must Complete
SURRENDER REQUEST FORM Section A Policy Information (You Must Complete This Section) Policy Number: Insured: (First Name) (Last Name) Sec tion B Surrender Request and Withholding Election (You Must Complete
Step by Step Guide to Anthem Blue Cross Enrollment Application. FOR Adding/Dropping Dependents for Anthem Medical
 Step by Step Guide to Anthem Blue Cross Enrollment Application FOR ing/dropping Dependents for Anthem Medical For members of the California Association of REALTORS Use this form to: or drop dependents
Step by Step Guide to Anthem Blue Cross Enrollment Application FOR ing/dropping Dependents for Anthem Medical For members of the California Association of REALTORS Use this form to: or drop dependents
Please fill out in blue or black ink only. Section A: Employee Information Last name First name M.I. Social Security no.
 Employee Enrollment Form For 1-50 Employee Small s 1 New Hampshire You, the employee, must fill out this enrollment form. You must be sure that all the information is correct and that you fill out all
Employee Enrollment Form For 1-50 Employee Small s 1 New Hampshire You, the employee, must fill out this enrollment form. You must be sure that all the information is correct and that you fill out all
Human Resources Department Mary Lou Glaesmann, Asst. Supt. for HR
 Human Resources Department Mary Lou Glaesmann, Asst. Supt. for HR Welcome! This document contains the paperwork you will be required to complete and bring to your HR orientation. Below are some helpful
Human Resources Department Mary Lou Glaesmann, Asst. Supt. for HR Welcome! This document contains the paperwork you will be required to complete and bring to your HR orientation. Below are some helpful
Group Membership Change Form for Small Business ACA Plans (1-50)
") Complete the following information Group Name Group Contact Group Number ( ) Group Phone Number Employee Name (First, Last) Group Membership Change Form for Small Business ACA Plans (1-50) Please submit
Complete the following information Group Name Group Contact Group Number ( ) Group Phone Number Employee Name (First, Last) Group Membership Change Form for Small Business ACA Plans (1-50) Please submit
A - EMPLOYEE INFORMATION SUBMISSION AND CERTIFICATION
 Office/Client Number New Employee Packet Employer Information: Choose your option for submitting employee information. For detailed instructions for these options, refer to the PEO New Employee Packet
Office/Client Number New Employee Packet Employer Information: Choose your option for submitting employee information. For detailed instructions for these options, refer to the PEO New Employee Packet
Western States Office and Professional Employees Pension Fund
 Western States Office and Professional Employees Pension Fund FEDERAL INCOME TAX WITHHOLDING TAX WITHHOLDING ELECTION Please complete the attached W-4P Withholding Certificate for Pension or Annuity Payments.
Western States Office and Professional Employees Pension Fund FEDERAL INCOME TAX WITHHOLDING TAX WITHHOLDING ELECTION Please complete the attached W-4P Withholding Certificate for Pension or Annuity Payments.
**If you have any other questions, please contact us and we will be happy to help.**
 Attention GGRC Public Partnerships, LLC 7776 S Pointe Pkwy W Suite 5 Phoenix, AZ 8544 Worker First name, Last name Worker Mailing Address, Address 2 Worker City, State, Zip Dear Worker This packet includes
Attention GGRC Public Partnerships, LLC 7776 S Pointe Pkwy W Suite 5 Phoenix, AZ 8544 Worker First name, Last name Worker Mailing Address, Address 2 Worker City, State, Zip Dear Worker This packet includes
Employee Packet Forms
 Welcome!! Outreach Health Services looks forward to working with you. This Employee Packet has the forms and information you need to become an employee. The participant, who is your employer, can help
Welcome!! Outreach Health Services looks forward to working with you. This Employee Packet has the forms and information you need to become an employee. The participant, who is your employer, can help
Missouri Individual Enrollment Application
 Missouri Individual Enrollment Application IMPORTANT: If you are a new applicant, a separate premium payment is required to be submitted with each application. If you are a current Individual policyholder
Missouri Individual Enrollment Application IMPORTANT: If you are a new applicant, a separate premium payment is required to be submitted with each application. If you are a current Individual policyholder
Bring all completed forms to your paperwork session. Any questions that you may have about the forms, we will be happy to address at the session.
 Directions for completing the New Hire Paperwork On-Line: Please print all pages (12 forms) 1-Employment Eligibility Verification Form: complete and sign/date Section 1. If your social security card states
Directions for completing the New Hire Paperwork On-Line: Please print all pages (12 forms) 1-Employment Eligibility Verification Form: complete and sign/date Section 1. If your social security card states
Bring all completed forms to your paperwork session. Any questions that you may have about the forms, we will be happy to address at the session.
 Directions for completing the New Hire Paperwork On-Line: Please print all pages (12 forms) 1-Employment Eligibility Verification Form: complete and sign/date Section 1. If your social security card states
Directions for completing the New Hire Paperwork On-Line: Please print all pages (12 forms) 1-Employment Eligibility Verification Form: complete and sign/date Section 1. If your social security card states
Missouri Individual Enrollment Application
 Missouri Individual Enrollment Application IMPORTANT: If you are a new applicant, a separate premium payment is required to be submitted with each application. If you are a current Individual policyholder
Missouri Individual Enrollment Application IMPORTANT: If you are a new applicant, a separate premium payment is required to be submitted with each application. If you are a current Individual policyholder
Group Enrollment Application Change Form
 Group Enrollment Application Change Form Please read the instructions on the inside thoroughly before completing this enrollment application/change form. Blue Cross and Blue Shield of Texas, a Division
Group Enrollment Application Change Form Please read the instructions on the inside thoroughly before completing this enrollment application/change form. Blue Cross and Blue Shield of Texas, a Division
Please complete and sign all forms in the PRE-EMPLOYMENT FORMS section.
 NATIONAL HOME HEALTH SERVICES EMPLOYMENT FORMS 5811 Dempster St Morton Grove, IL 60053 Phone: (847) 329-9933 Fax: (847) 930-0375 APPLICANT NAME POSITION APPLYING FOR DATE Please complete and sign all forms
NATIONAL HOME HEALTH SERVICES EMPLOYMENT FORMS 5811 Dempster St Morton Grove, IL 60053 Phone: (847) 329-9933 Fax: (847) 930-0375 APPLICANT NAME POSITION APPLYING FOR DATE Please complete and sign all forms
Group Enrollment Application Change Form
 Group Enrollment Application Change Form Please read the instructions on the inside thoroughly before completing this enrollment application/change form. Blue Cross and Blue Shield of Illinois, a Division
Group Enrollment Application Change Form Please read the instructions on the inside thoroughly before completing this enrollment application/change form. Blue Cross and Blue Shield of Illinois, a Division
Employment Application
 Print Name (First, ( M., Last): Employment Application PERSONAL INFORMATION Date: Street Address: Apt. Unit/# Home Phone: City State Zip Cell Phone: Email Address: Are you authorized to work in the U.S.?
Print Name (First, ( M., Last): Employment Application PERSONAL INFORMATION Date: Street Address: Apt. Unit/# Home Phone: City State Zip Cell Phone: Email Address: Are you authorized to work in the U.S.?
2017 New Hire Forms Directions & Resources
 2017 New Hire Forms Directions & Resources Federal W4 Forms Complete form; filling in all spaces in sections 1-7, remembering to sign and date form. State W4 Forms Complete Employee Withholding Allowance
2017 New Hire Forms Directions & Resources Federal W4 Forms Complete form; filling in all spaces in sections 1-7, remembering to sign and date form. State W4 Forms Complete Employee Withholding Allowance
DIVERSIFIED Edgewood Road, NE Cedar Rapids, IA
 DIVERSIFIED --------------------- 4443 Edgewood Road, NE Cedar Rapids, IA 52499 800-755-5801 www.divinvest.com Federal Tax Withholding Election Form Instructions To change your federal income tax withholding,
DIVERSIFIED --------------------- 4443 Edgewood Road, NE Cedar Rapids, IA 52499 800-755-5801 www.divinvest.com Federal Tax Withholding Election Form Instructions To change your federal income tax withholding,
Group Enrollment Application Change Form
 Small Group Group Enrollment Application Change Form Please read the instructions on the inside thoroughly before completing this enrollment application/change form. Blue Cross and Blue Shield of Montana,
Small Group Group Enrollment Application Change Form Please read the instructions on the inside thoroughly before completing this enrollment application/change form. Blue Cross and Blue Shield of Montana,
SPECIAL ENROLLMENT PERIOD FORM
 SPECIAL ENROLLMENT PERIOD FORM A Special Enrollment Period (SEP) is defined as a period during which you and your family have a right to sign up for new or make changes to existing health insurance coverage.
SPECIAL ENROLLMENT PERIOD FORM A Special Enrollment Period (SEP) is defined as a period during which you and your family have a right to sign up for new or make changes to existing health insurance coverage.
What s In My Paycheck? compensation package: all of the wages (salary, bonus, commission) and benefits provided by an employer. What s In My Paycheck?
 and benefits provided by an employer. What s In My Paycheck?") compensation package: all of the wages (salary, bonus, commission) and benefits provided by an employer wages: money paid or received for work or services completed, usually by the hour, day, or week hourly
compensation package: all of the wages (salary, bonus, commission) and benefits provided by an employer wages: money paid or received for work or services completed, usually by the hour, day, or week hourly
Name: MCO (circle one): AG UHC VSHP (Blue Care) Worker Training Checklist. I-9 Criminal Attestation Tax Exempt W-4. Additional Comments:
: AG UHC VSHP (Blue Care) Worker Training Checklist. I-9 Criminal Attestation Tax Exempt W-4. Additional Comments:") 414 Union ST, Ste 1100 Nashville, TN 37219 Fax - Worker United Health Care Fax: 877.432.4103 (FOR DOCUMENTS ONLY. NO TIMESHEETS TO THIS NUMBER) Customer Service: 888.866.1154 To: Fax: Phone: Member Name:
414 Union ST, Ste 1100 Nashville, TN 37219 Fax - Worker United Health Care Fax: 877.432.4103 (FOR DOCUMENTS ONLY. NO TIMESHEETS TO THIS NUMBER) Customer Service: 888.866.1154 To: Fax: Phone: Member Name:
Summary Plan Description for Employees of URS Federal Services Effective January 1, 2014 Medical Section
 Summary Plan Description for Employees of URS Federal Services Effective January 1, 2014 Medical Section Date Revised: January 2014 YOUR MEDICAL PLAN COVERAGE... 1 Mental Health and Substance Abuse and
Summary Plan Description for Employees of URS Federal Services Effective January 1, 2014 Medical Section Date Revised: January 2014 YOUR MEDICAL PLAN COVERAGE... 1 Mental Health and Substance Abuse and
EMPLOYER WITH EMPLOYEES - PAYROLL INTAKE FORM
 EMPLOYER WITH EMPLOYEES - PAYROLL INTAKE FORM CONTACT INFORMATION Payroll Client (First, Last): Phone #: ( ) - Legal Business Name: Business DBA (If Applicable): Business Type: LLC Partnership Corp S-Corp
EMPLOYER WITH EMPLOYEES - PAYROLL INTAKE FORM CONTACT INFORMATION Payroll Client (First, Last): Phone #: ( ) - Legal Business Name: Business DBA (If Applicable): Business Type: LLC Partnership Corp S-Corp
Student Employee New Hire Packet
 Student Employee New Hire Packet New Hire Checklist: o Authorization to Hire Form o Student Application o Federal W-4 Form o NJ State W-4 Form o I-9 Form o Social Security Card (for Payroll purposes) o
Student Employee New Hire Packet New Hire Checklist: o Authorization to Hire Form o Student Application o Federal W-4 Form o NJ State W-4 Form o I-9 Form o Social Security Card (for Payroll purposes) o
New Business New Hire New Renewal New COBRA Qualifying/Triggering Event. Address. Spouse/Domestic Partner Child 1 Child 2 Child 3
 721 South Parker, Suite 200, Orange, CA 92868 (800) 558-8003 www.calchoice.com / / Life / Enrollment Application Select one A Personal Information Company Name COMPLETE WAIVER SECTION ON PAGE 4 IF YOU
721 South Parker, Suite 200, Orange, CA 92868 (800) 558-8003 www.calchoice.com / / Life / Enrollment Application Select one A Personal Information Company Name COMPLETE WAIVER SECTION ON PAGE 4 IF YOU
Limited-purpose Health FSA Frequently Asked Questions
 What is a limited-purpose flexible spending account? A limited-purpose health flexible spending account (referred to as a limited-purpose FSA) is part of your benefits package. This account lets you use
What is a limited-purpose flexible spending account? A limited-purpose health flexible spending account (referred to as a limited-purpose FSA) is part of your benefits package. This account lets you use
COLCHESTER SCHOOL DISTRICT
 COLCHESTER SCHOOL DISTRICT APPLICATION FOR SUBSTITUTING Administrative Offices, 125 Laker Lane P.O. Box 27, Colchester, VT 05446-0027 Phone (802) 264-5999 Fax (802) 863-4774 Name: Telephone No.: Mailing
COLCHESTER SCHOOL DISTRICT APPLICATION FOR SUBSTITUTING Administrative Offices, 125 Laker Lane P.O. Box 27, Colchester, VT 05446-0027 Phone (802) 264-5999 Fax (802) 863-4774 Name: Telephone No.: Mailing
Last name First name M.I. Social Security no.* (required) City State ZIP code. Single Married Domestic Partner
 City State ZIP code. Single Married Domestic Partner") Employee Enrollment Application For 1 100 Employee Small Groups California Health care plans offered by Anthem Blue Cross. Insurance plans offered by Anthem Blue Cross Life and Health Insurance Company.
Employee Enrollment Application For 1 100 Employee Small Groups California Health care plans offered by Anthem Blue Cross. Insurance plans offered by Anthem Blue Cross Life and Health Insurance Company.
New Group Checklist. 30 days prior to the effective date, the following Group information is required:
 New Group Checklist 30 days prior to the effective date, the following Group information is required: Group Policy Application completed and signed. Enrollment forms; be sure to complete any applicable
New Group Checklist 30 days prior to the effective date, the following Group information is required: Group Policy Application completed and signed. Enrollment forms; be sure to complete any applicable
TENNESSEE CONSOLIDATED RETIREMENT SYSTEM 502 Deaderick Street Nashville, Tennessee
 Retirement Application for Service or Early Retirement Benefits TENNESSEE CONSOLIDATED RETIREMENT SYSTEM 502 Deaderick Street Nashville, Tennessee 37243-0201 1-800-770-8277 http://tcrs.tn.gov Refer to
Retirement Application for Service or Early Retirement Benefits TENNESSEE CONSOLIDATED RETIREMENT SYSTEM 502 Deaderick Street Nashville, Tennessee 37243-0201 1-800-770-8277 http://tcrs.tn.gov Refer to
Enrollment/Change Form
 Enrollment/Change Form Thank you for choosing Empire. Please fill out all items in order for us to quickly and accurately process your enrollment. Once you ve completed this form, please sign in the space
Enrollment/Change Form Thank you for choosing Empire. Please fill out all items in order for us to quickly and accurately process your enrollment. Once you ve completed this form, please sign in the space
Blank Forms (Volume 1)
") Blank Forms (Volume 1) These forms are provided for congregational use and may be copied. Payroll Congregational Payroll Information Employment Eligibility Verification (I-9) Payroll Authorization Form
Blank Forms (Volume 1) These forms are provided for congregational use and may be copied. Payroll Congregational Payroll Information Employment Eligibility Verification (I-9) Payroll Authorization Form
Group Enrollment Application Change Form
 Group Enrollment Application Change Form Please read the instructions on the inside thoroughly before completing this enrollment application/change form. GHS Health Maintenance Organization, Inc. d/b/a
Group Enrollment Application Change Form Please read the instructions on the inside thoroughly before completing this enrollment application/change form. GHS Health Maintenance Organization, Inc. d/b/a
Employee Data Sheet NAME. Title: Dr. Mr. Ms. Mrs. Miss First: Middle: Last: Suffix: CONTACT INFORMATION
 Employee Data Sheet Social Security #: Today s Date: NAME Title: Dr. Mr. Ms. Mrs. Miss First: Middle: Last: Suffix: CONTACT INFORMATION Address: Apt/Unit #: City: State: Zip Code: County: Home Phone (include
Employee Data Sheet Social Security #: Today s Date: NAME Title: Dr. Mr. Ms. Mrs. Miss First: Middle: Last: Suffix: CONTACT INFORMATION Address: Apt/Unit #: City: State: Zip Code: County: Home Phone (include
TENNESSEE CONSOLIDATED RETIREMENT SYSTEM 502 Deaderick Street Nashville, Tennessee (615)
") Retirement Application for Disability Benefits TENNESSEE CONSOLIDATED RETIREMENT SYSTEM 502 Deaderick Street Nashville, Tennessee 37243-0201 1-800-770-8277 (615) 253-8693 http://tcrs.tn.gov Refer to pages
Retirement Application for Disability Benefits TENNESSEE CONSOLIDATED RETIREMENT SYSTEM 502 Deaderick Street Nashville, Tennessee 37243-0201 1-800-770-8277 (615) 253-8693 http://tcrs.tn.gov Refer to pages
TTC Form T3-107) ct Deposit (TTC Form T3-21)
 ct Deposit (TTC Form T3-21)") TO: Adjunct Instructor FROM: Human Resources, Fredric Yeadon (843-574-6825) RE: Adjunct Instructor Packet Welcome to Trident Technical College! Please complete the following paperwork before reporting
TO: Adjunct Instructor FROM: Human Resources, Fredric Yeadon (843-574-6825) RE: Adjunct Instructor Packet Welcome to Trident Technical College! Please complete the following paperwork before reporting
Store# Name (First, Middle, Last) SSN # Date of Birth. City State Zip. Hire Date Position Rate of pay/annual Salary. Select... Rehire.
 SSN # Date of Birth. City State Zip. Hire Date Position Rate of pay/annual Salary. Select... Rehire.") Store# Name (First, Middle, Last) SSN # Date of Birth Address Apt/Lot City State Zip Hire Date Position Rate of pay/annual Salary Rehire nmlkj Yes nmlkj No Select... Native American If yes, please list
Store# Name (First, Middle, Last) SSN # Date of Birth Address Apt/Lot City State Zip Hire Date Position Rate of pay/annual Salary Rehire nmlkj Yes nmlkj No Select... Native American If yes, please list
Salary Reduction Contributions Enrollment Form
 Salary Reduction Contributions Enrollment Form Employee Information Employer Name Employee Name (Last, First, Middle) Employee Street Address Department - - Social Security Number / to / (mm/dd) Plan Year
Salary Reduction Contributions Enrollment Form Employee Information Employer Name Employee Name (Last, First, Middle) Employee Street Address Department - - Social Security Number / to / (mm/dd) Plan Year
Child Resident Street Address (required - a PO Box will not be accepted) City County State Zip. Mailing address (if different) City County State Zip
 City County State Zip. Mailing address (if different) City County State Zip") PO Box 339 400 Warren Avenue Bremerton, WA 98337 APPLICATION FOR INDIVIDUAL/FAMILY PLAN COVERAGE KPS is a health care service contractor licensed and marketing in all of Washington State Please review
PO Box 339 400 Warren Avenue Bremerton, WA 98337 APPLICATION FOR INDIVIDUAL/FAMILY PLAN COVERAGE KPS is a health care service contractor licensed and marketing in all of Washington State Please review
HOW TO ENROLL WITH TIAA-CREF
 HOW TO ENROLL WITH TIAA-CREF To enroll, you must complete your Enrollment Form and Plan Contribution Allocation Administrative Form, and sign the notice on prospectuses and documents. There is also one
HOW TO ENROLL WITH TIAA-CREF To enroll, you must complete your Enrollment Form and Plan Contribution Allocation Administrative Form, and sign the notice on prospectuses and documents. There is also one
Coordination of Benefits (COB)
") Page 1 of 5 Advanced Search Contact Us Employer Home Health & Wellness Plans & Benefits Answers@Anthem Communications Request a Quote Benefits Manager Services Click the Login button to View Group Information,
Page 1 of 5 Advanced Search Contact Us Employer Home Health & Wellness Plans & Benefits Answers@Anthem Communications Request a Quote Benefits Manager Services Click the Login button to View Group Information,
Personal Data Form. UIN#: Dr. Mr. Mrs. Ms. Last Name: First Name: Middle Initial:
 Personal Data Form UIN#: Dr. Mr. Mrs. Ms. Last Name: First Name: Middle Initial: Preferred Name (if different than above): Social Security Number: Mailing Address (same as W4): City: Zip/Postal Code: Permanent
Personal Data Form UIN#: Dr. Mr. Mrs. Ms. Last Name: First Name: Middle Initial: Preferred Name (if different than above): Social Security Number: Mailing Address (same as W4): City: Zip/Postal Code: Permanent
Personal Data Form. UIN#: Dr. Mr. Mrs. Ms. Last Name: First Name: Middle Initial:
 Personal Data Form UIN#: Dr. Mr. Mrs. Ms. Last Name: First Name: Middle Initial: Preferred Name (if different than above): Social Security Number: Mailing Address (same as W4): City: Zip/Postal Code: Permanent
Personal Data Form UIN#: Dr. Mr. Mrs. Ms. Last Name: First Name: Middle Initial: Preferred Name (if different than above): Social Security Number: Mailing Address (same as W4): City: Zip/Postal Code: Permanent
Personal Data Form. UIN#: Dr. Mr. Mrs. Ms. Last Name: First Name: Middle Initial:
 Personal Data Form UIN#: Dr. Mr. Mrs. Ms. Last Name: First Name: Middle Initial: Preferred Name (if different than above): Social Security Number: Mailing Address (same as W4): City: Zip/Postal Code: Permanent
Personal Data Form UIN#: Dr. Mr. Mrs. Ms. Last Name: First Name: Middle Initial: Preferred Name (if different than above): Social Security Number: Mailing Address (same as W4): City: Zip/Postal Code: Permanent
Member Enrollment Application (Group size 100+)
") Member Enrollment Application (Group size 100+) Please print in ink and return to your employer. Use extra sheets if necessary. Employee Social Security No. BlueChoice Healthcare Plan (HMO), Blue Open
Member Enrollment Application (Group size 100+) Please print in ink and return to your employer. Use extra sheets if necessary. Employee Social Security No. BlueChoice Healthcare Plan (HMO), Blue Open
American Heritage Life Insurance Company 1776 American Heritage Life Drive Jacksonville, Florida
 CLAIM FORM If you have any questions regarding benefits available, or how to file your claim, or if you would like to appeal any determination, please contact our customer service department at 1-800-348-4489
CLAIM FORM If you have any questions regarding benefits available, or how to file your claim, or if you would like to appeal any determination, please contact our customer service department at 1-800-348-4489
RE: Pension Application Member ID #: XXX-XX. Dear Participant,
 2357 59 th Street St. Louis, MO 63110 (314) 644-2777 ext. 3 1-800-489-0228 Fax: (314) 645-6226 RE: Pension Application Member ID #: XXX-XX Dear Participant, Congratulations! Our office was recently notified
2357 59 th Street St. Louis, MO 63110 (314) 644-2777 ext. 3 1-800-489-0228 Fax: (314) 645-6226 RE: Pension Application Member ID #: XXX-XX Dear Participant, Congratulations! Our office was recently notified