BACKGROUND CLEARANCE INSTRUCTIONS STUDENT APPLICANT
|
|
|
- Madeline Sutton
- 6 years ago
- Views:
Transcription
1 BACKGROUND CLEARANCE INSTRUCTIONS STUDENT APPLICANT The amended Child Protective Services Law, effective December 31, 2014, and accompanying policies; PASSHE Board of Governors A (Protection of Minors) and Bloomsburg University s PRP 2410 (Background Screening, Protection of Minors and Volunteerism) requires all university employees to successfully complete background clearances every three (3) years. Specifically, all employees are required to successfully complete the Pennsylvania Child Abuse History Clearance, Pennsylvania State Police Criminal Record Check, and FBI Federal Criminal History Record. Please complete the actions listed below in order to comply. 1. Complete the form entitled BLOOMSBURG UNIVERSITY OF PENNSYLVANIA APPLICANT ACKNOWLEDGMENT AND CONSENT FOR CRIMINAL BACKGROUND CHECK. 2. Go to to obtain your one time use payment code for completing the Pennsylvania Child Abuse History Clearance. You must use your Husky ID and password. Copy or print the code to proceed with the next step. 3. Go to to complete your Pennsylvania Child Abuse Clearance electronically utilizing the payment code obtained in the previous step. a. Select CREATE A NEW ACCOUNT to create a Keystone ID, which is a username. Please retain this information for future access. b. If you have previously created a Keystone ID, LOGIN with your Keystone ID and password. Additional Instructions for registering and completing the online form are available under USERS GUIDES CWIS CITIZENS ACCOUNT at: Completion of this step will take approximately thirty (30) minutes. You will receive an original report, for your records, via . Forward a copy of the registration confirmation to Ellen Sudbury (esudbury@bloomu.edu), Compliance Coordinator, Rm 104B, Waller Administration Building. 4. Apply for the FBI Federal Criminal History Record at: This link will direct you to registration for the Department of Human Services (formerly DPW). a. Select Register Online. b. Go to Payment Type and Select AGENCY. c. Go to Agency ID and enter ABID #: PALS20954 d. Go to Billing Password and enter ABID Password: P (BU employees only) e. Select EMPLOYMENT WITH SIGNIFICANT LIKELIHOOD OF REGULAR CONTACT WITH CHILDREN as Reason Fingerprinted. f. Make two (2) copies of the registration. i. Present one copy at the FBI fingerprint site. ii. Forward one copy to Ellen Sudbury (esudbury@bloomu.edu), Compliance Coordinator. 5. Present your registration confirmation and photo ID at a Cogent FBI fingerprint site. The Bloomsburg University Store is an authorized fingerprint collection location. The store may be contacted at (570) for inquiries. Other authorized locations are listed on the registration website. 6. Return the following documents to, Ellen Sudbury (esudbury@bloomu.edu), Compliance Coordinator, Waller Administration Building, Room 104B. ( ) a. BLOOMSBURG UNIVERSITY OF PENNSYLVANIA APPLICANT ACKNOWLEDGMENT AND CONSENT FOR CRIMINAL BACKGROUND CHECK. Return this document immediately upon completion. b. Forwarded of Pennsylvania Child Abuse History confirmation. Return this document immediately upon completion. c. Forwarded copy of FBI fingerprint confirmation. Return this document immediately upon completion. d. Original Results of FBI Fingerprint background clearance once received at your registration address. The current lead time for receipt of this document is ten (10) to fourteen (14) days.

2 BLOOMSBURG UNIVERSITY OF PENNSYLVANIA APPLICANT ACKNOWLEDGEMENT AND CONSENT FOR CRIMINAL BACKGROUND CHECK 1. hereby acknowledge and consent to the following: (PRINT NAME) 2. I have applied for a position with Bloomsburg University and have been advised that all university employees are required to satisfy the requirements of the Pennsylvania Child Protective Services Law (CPSL). 3. I acknowledge that CPSL requires a Pennsylvania State Police Criminal History Report, Pennsylvania Department of Human Services Child Abuse History Clearance and a Federal Bureau of Investigation Criminal History Report. 4. I further acknowledge that I will provide the original Federal Bureau of Investigation Criminal History Report (fingerprint report) to Human Resources at Bloomsburg University. 5. I will use the provided payment code to submit my Pennsylvania Department of Human Services Child Abuse History Clearance report electronically, which will allow Bloomsburg University access to the final report. 6. I understand that Human Resources at Bloomsburg University will run the Pennsylvania State Police Criminal History report (e-patch) on my behalf and I am providing the following information for them to do so. Full Name (print) Date of Birth Full Social Security Number Aliases and/or Maiden Name Race Race is a required field in the Pennsylvania State Police application for the Criminal History Report. Failure to provide race on this form will result in race being reported as unknown to the Pennsylvania State Police. 7. I understand that CPSL permits (but does not require) Bloomsburg University to hire me on a provisional basis for an approved time period not to exceed ninety (90) days. 8. I understand that during any authorized period of provisional employment/participation, I will not be permitted to work alone with children and must work in the immediate vicinity of a permanent Bloomsburg University employee. 9. I understand that Bloomsburg University may immediately terminate my provisional employment/participation should the Pennsylvania State Police, Pennsylvania Department of Human Services and/or the Federal Bureau of Investigation be unable to provide the required reports within the approved provisional period. SIGNATURE DATE ADDRESS TELEPHONE NUMBER APPLICANT FOR: FACULTY STAFF STUDENT EMPLOYMENT VOLUNTEER DEPARTMENT: Approved by University Legal Counsel April 13, 2015
3 ADDITIONAL INFORMATION/SUGGESTIONS FOR COMPLETING THE BACKGROUND CLEARANCES 1. COMPLETING THE BLOOMSBURG UNIVERSITY OF PENNSYLVANIA APPLICANT ACKNOWLEDGEMENT AND CONSENT FOR CRIMINAL BACKGROUND CHECK FORM a. Write legibly (we need to be able to read your SS# and DOB to enter them correctly for your PA State Police clearance. b. Race does not need to be filled in. If it is left blank, we will enter unknown in the required field for the PA State Police background clearance. c. Be sure to fill in your department and all contact information 2. OBTAINING YOUR PAYMENT CODE a. When obtaining your payment code from the BloomU portal, please copy and paste it to avoid confusing the O and 0 or the I and 1. b. If you forget or lose your code, log back in and the site will give you the same code again. The code is linked to your BU login. 3. COMPLETING THE CHILD ABUSE HISTORY CLEARANCE a. Use Internet Explorer b. Your Keystone ID is another name for your login (that you create). Do not use your BU login or the payment code in this field. c. Write down your Keystone ID, password and the answers to your security questions so you can log in to retrieve your results d. If you have already created an account in the past, you will need to log in using those credentials. If you can t remember them, contact the CWIS support center. e. When prompted, enter your Social Security number. Your clearance will clear much quicker (sometimes immediately). Without your Social Security number your clearance will take days longer to process. f. Use your home address (not your BU address) on your clearance. g. Use School Employee NOT governed by the Public School code as your Application Purpose. 4. FBI FEDERAL CRIMINAL HISTORY CLEARANCE a. Register under the Department of Public Welfare/Human Services not with the Department of Education. b. Use the address where you will be living in 2 weeks as your mailing address. The original report will be mailed to that address and you must bring the original report in to HR before you are approved to work. c. If you make a mistake on your registration, you can cancel it and re-register. Don t continue with your fingerprinting if you spelled your name wrong or typed in the wrong SS#. We will require you to have the clearance repeated. d. Use lotion on your hands prior to going to have your prints taken. It reduces the risk of having your prints rejected. e. The results will be mailed to you in a white business envelope from the Commonwealth of Pennsylvania, Department of Public Welfare, on blue marbled paper.
4 STUDENT EMPLOYMENT CHECKLIST Supervisor s Responsibility: For already enrolled students: Please check the Active Student List on the S Drive: under BU documents, under Payroll/Active Student List and write the PERSONNEL # of the student on the placement card. If you do not find the Personnel #, then attach the completed forms listed below (Checklist for New Students). All forms are available on the S Drive: under the folders BU documents/ Payroll; also at (Please save this link as a favorite). Please return this checklist along with all completed forms to Student Payroll, WAB-121. Ensure that both you and the student sign all applicable paperwork. PACKETS MISSING ANY OF THE FIRST FIVE (5) FORMS WILL BE RETURNED TO THE APPROPRIATE STUDENT SUPERVISOR. Please do not hesitate to contact Nikki Black, Student Payroll Coordinator, with questions. Thank you! Checklist for New Student Employee paperwork to be completed for Payroll processing - Placement Card - I-9 Form- Signed and dated by both student and supervisor. A student is not LEGALLY eligible to begin employment until they have provided the ORIGINAL DOCUMENTS required to complete the I-9 and they have signed and dated the I-9. This should be done by the first day of employment. The supervisor has until the third day of employment to complete the form. Regardless of the documents used to complete the I-9, you must include a copy of the student s social security card. - Local Earned Income Tax Residency Certification Form - W4 Form - Direct Deposit Form Student Voluntary Self-Identification Survey Form. Declaration is voluntary; however, the form must be signed and dated. Local Service Tax Form Please complete this form only if: You expect to make less than $12,000 annually, or You work multiple jobs and have this tax deducted from another employer (Please provide a copy of proof of the LST payment from your other employer). Background check & clearance forms complete. Please refer to checklist. Student Supervisor (please print) Date Student Payroll Checklist Revised 1/2017
5
6
7
8 DCED-CLGS-06 (1-11) LOCAL EARNED INCOME TAX RESIDENCY CERTIFICATION FORM COMMONWEALTH OF PENNSYLVANIA DEPARTMENT OF COMMUNITY & ECONOMIC DEVELOPMENT GOVERNOR S CENTER FOR LOCAL GOVERMENT SERVICES TO EMPLOYERS/TAXPAYERS: This form is to be used by employers and/or taxpayers to report essential information for the collection and distribution of Local Earned Income Taxes. This form must be utilized by employers when a new employee is hired or when a current employee notifies employer of a name and/or address change. NAME (Last, FIrst, Middle Initial) EMPLOYEE INFORMATION - RESIDENCE LOCATION FIRST LINE OF ADDRESS (If PO Box, please include actual street address) SECOND LINE OF ADDRESS CITY STATE ZIP CODE DAYTIME PHONE NUMBER MUNICIPALITY (City, Borough, Township) COUNTY PSD CODE TOTAL RESIDENT EIT RATE EMPLOYER NAME (Use Federal ID Name) EMPLOYER INFORMATION - EMPLOYMENT LOCATION EMPLOYER FEIN FIRST LINE OF ADDRESS ( I If PO Box, please include actual street address) SECOND LINE OF ADDRESS CITY STATE ZIP CODE PHONE NUMBER MUNICIPALITY (City, Borough, Township) COUNTY PSD CODE MUNICIPAL NON-RESIDENT EIT RATE SIGNATURE OF EMPLOYEE CERTIFICATION DATE PHONE NUMBER ADDRESS For information on obtaining the appropriate MUNICIPALITY (City, Borough, Township), PSD CODES and EIT (Earned Income Tax) RATES, please refer to the Pennsylvania Department of Community & Economic Development website: Select Get Local Gov Support, >Municipal Statistics
9
10
11 Return to: Student Payroll Waller Administration Bldg. STATE SYSTEM of HIGHER EDUCATION DIRECT DEPOSIT AUTHORIZATION Name Social Security OR Personnel Number address (Please Print) I hereby authorize the Pennsylvania State System of Higher Education to (check one) I hereby decline direct deposit (Complete section 2 below) START STOP CHANGE Total bi weekly payroll deduction to the Financial Institution shown below. You may designate any bank, savings and loan association, or credit union in the U.S. that (1) is a member of the Federal Reserve System and (2) accepts electronic funds transfer. Payroll will notify you if the institution you choose does not qualify. Financial Institution s Name Transit Routing Number Account Number Type of Account (Checking or Savings) Deduction Amount (Dollar Amount or Net) Effective with pay date of I have an established account at the Financial Institution indicated above, and authorize the State System of Higher Education to initiate credit entries and to initiate debit entries and adjustments for any credit entries in error to my (our) account (s) indicated above. I have provided a copy of a voided check or a deposit slip (see attached) solely for the purpose of verifying my account number and the Financial Institution s routing number. My authorization will remain in effect until revoked by me in writing or I terminate my employment with the State System of Higher Education. Signature Date Section 2-Declining Direct Deposit- By declining direct deposit of my pay, I will be required to pick up my paycheck in the Student Payroll Office, 2 nd Floor, Waller Administration Bldg, each biweekly payday between 9:00am to 11:30am. If I have not picked up my check by 11:30am, the check will be mailed to the address stated on my check. CHECKS CAN ONLY BE DISTRIBUTED ON PAY DAY Signature Date
12 Voluntary Self-Identification Survey In order for Bloomsburg University to comply with Equal Employment Opportunity laws and regulations and to assess our recruitment and retention efforts, we solicit the ethnicity and gender of all employees. Our affirmative action/social equity efforts would be greatly enhanced by providing this information. We would appreciate your completion of this form. Please return to Student Payroll, Waller Administration Building. Please be advised that this request is optional. Refusal to provide this information will not subject you to discharge or any adverse treatment. Any information obtained will only be used in compliance with the foregoing statutes and regulations issued thereunder. Also, information obtained concerning individuals shall be kept confidential, except that (1) supervisors and managers may be informed regarding restrictions on the work or duties of individuals with disabilities and disabled veterans, regarding necessary accommodations; (2) first aid and safety personnel may be informed, when and to the extent appropriate, if the condition may require emergency treatment; and (3) government officials investigating compliance with the above laws may be informed. Last Name: First Name: Address: Gender: (Circle one) Male Female 1) What is your ethnicity (Do you consider yourself to be Hispanic/Latino/Spanish)? Hispanic or Latino: Persons of Cuban, Mexican, Puerto Rican, South or Central America or other Spanish culture or origin, regardless of race. Not Hispanic or Latino 2) What is your race (In addition, select one or more of the following racial categories to describe yourself)? Hispanic of any race For non-hispanics only: American Indian or Alaskan Native: Persons having origins in any of the original peoples of North America, and who maintain cultural identification through tribal affiliation or community recognition. Asian: Persons having origins in any of the original peoples of the Far East, Southeast Asia, or the Indian subcontinent, including, for example, Cambodia, China, India, Japan, Korea, Malaysia. Pakistan, the Philippine Islands, Thailand, and Vietnam. Black or African American: Persons having origins in any of the black racial groups of Africa. Native Hawaiian or Pacific Islander: Persons having origins in any of the peoples of Hawaii, Guam, Samoa, or other Pacific Islands. White/Caucasian (Not of Hispanic origin): Persons having origins in any of the original peoples of Europe, North Africa, or the Middle East. Two or more races Race and/or ethnicity unknown Non-resident alien How do you classify yourself? (if applicable)
13 Special Disabled Veteran: means (1) a veteran who is entitled to compensation (or who but for the receipt of military retired pay would be entitled to compensation) under laws administered by the Department of Veterans Affairs for a disability (a) rated at 30 percent or more, or (b) rated at 10 or 20 percent in the case of a veteran who has been determined under Section 1506 of Title 38, USC to have a serious employment handicap or (2) a person who was discharged or released from active duty because of a service-connected disability. Veteran of the Vietnam-Era: means a person who: (1) served on active duty for a period of more than 180 days, and was discharged or released therefrom with other than a dishonorable discharge, if any part of such active duty occurred: (a) in the Republic of Vietnam between February 28, 1961, and May 7, 1975; or (b) between August 5, 1964 and May 7, 1965, in all other cases; (2) was discharged or released from active duty for a service-connected disability if any part of such active duty was performed (a) in the Republic of Vietnam between February 28, 1961, and May 7, 1975; or (b) between August 5, 1964 and May 7, 1965, in all other cases. Other Veteran: means a veteran who served on active duty during a way or in a campaign or expedition for which a campaign badge has been authorized. To identify the campaigns or expeditions that meet this criterion, contact the Office of Personnel Management (OPM) and ask for the OPM VETS Guide, Appendix B. A local OPM telephone number may be found in the telephone book under nearest OPM location. For those with Internet access, the information required to make this determination is available at Individual with a disability: means a person who: has a physical or mental impairment that substantially limits one or more major life activities; has a record of such an impairment; or is regarded as having such an impairment. Do you have a mobility concern that would prevent you from evacuating a building in an emergency? (Circle one) Yes No If you have been self-identified as an individual with a disability or as a special disabled veteran, please describe your disability: Have accommodations for your disability been made to aid you in performing your job?: (Circle one) Yes No If yes, please describe such accommodations: If you feel that accommodations for your disability would aid you in performing your job, please describe: Signature Date Bloomsburg University of Pennsylvania is committed to affirmative action by way of providing equal educational and employment opportunities for all persons without regard to race, religion, age, gender, ancestry, lifestyle, or disability.
14 LOCAL SERVICES TAX EXEMPTION CERTIFICATE Tax Year APPLICATION FOR EXEMPTION FROM LOCAL SERVICES TAX A copy of this application for exemption from the Local Services Tax (LST), and all necessary supporting documents, must be completed and presented to your employer AND to the political subdivision levying the Local Services Tax where you are principally employed. This application for exemption from the Local Services Tax must be signed and dated. No exemption will be approved until proper documentation has been received. Name: Address: City/State: Soc Sec #: Phone #: Zip: REASON FOR EXEMPTION 1. MULTIPLE EMPLOYERS: Attach a copy of a current pay statement from your principal employer that shows the name of the employer, the length of the payroll period and the amount of Local Services Tax withheld. List all employers on the reverse side of this form. You must notify your other employers of a change in principal place of employment within two weeks of the change. 2. EXPECTED TOTAL EARNED INCOME AND NET PROFITS FROM ALL SOURCES WITHIN (municipality or school district) WILL BE LESS THAN $ : Attach copies of your last pay statements or your W-2 for the year prior. If you are self-employed, please attach a copy of your PA Schedule C, F, or RK-1 for the prior year. 3. ACTIVE DUTY MILITARY EXEMPTION: Please attach a copy of your orders directing you to active duty status. Annual training is not eligible for exemption. You are required to advise the tax office when you are discharged from active duty status. 4. MILITARY DISABILITY EXEMPTION: Please attach copy of your discharge orders and a statement from the United States Veterans Administrator documenting your disability. Only 100% permanent disabilities are recognized for this exemption. EMPLOYER: Once you receive this Exemption Certificate, you shall not withhold the Local Services Tax for the portion of the calendar year for which this certificate applies, unless you are otherwise notified or instructed by the tax collector to withhold the tax. Tax Office: Address: City/State: Phone #: Zip: IMPORTANT NOTE TO EMPLOYERS 1. The municipality is required by law to exempt from the LST employees whose earned income from all sources (employers and self-employment) in their municipality is less than $12,000 when the levied rate exceeds $ The school district for the municipality in which your worksite(s) is located may or may not levy an LST. If it does, the income exemption provided may differ from the municipality and can be anywhere from $0 to $11, Contact the tax office where your business worksites are located to obtain this information. LST Exemption 10-07
15 Employment Information: List all places of employment for the applicable tax year. Please list your PRIMARY EMPLOYER under #1 below and your secondary employers under the other columns. If self employed, write SELF under Employer Name column. Employer Name Address Address 2 City, State Zip Municipality Phone Start Date End Date Status (FT or PT) Gross Earnings 1. PRIMARY EMPLOYER Employer Name Address Address 2 City, State Zip Municipality Phone Start Date End Date Status (FT or PT) Gross Earnings PLEASE NOTE: All information received by the Tax Collector is considered to be CONFIDENTIAL and is only used for official purposes relating to the collection, administration and enforcement of the LOCAL SERVICES TAX. I DECLARE UNDER PENALTY OF LAW THAT THE INFORMATION STATED ON AND ATTACHED TO THIS FORM IS TRUE AND CORRECT: SIGNATURE: DATE: LST Exemption 10-07
16 Student Name: Student ID#: State of Understanding of Privacy Act Provisions I understand that by virtue of my employment with the Bloomsburg University Office I may have access to records which contain individually identifiable information, the disclosure of which is prohibited by the Privacy Act of I understand that I should only view information in any form paper, electronic or otherwise that is necessary for the performance of my job responsibilities. I understand that I should only access this information on computer systems during the times which I am working. I acknowledge that I fully understand that the willful or intentional disclosure by me of this information to any unauthorized person, could subject me to criminal and civil penalties imposed by the law. I further acknowledge that such willful or intentional unauthorized disclosure also violates the school s policy and could constitute just cause for disciplinary action including termination of my employment regardless of whether criminal or civil penalties are imposed. Student Signature Date Witness Date Department
Last Name First Name Middle Initial ADDRESS Street City County State Zip
 APPLICATION FOR EMPLOYMENT Kolberg-Pioneer, Inc. An Equal Opportunity Employer (HRF-002-03 01/16) This application is valid for the calendar year of 2018. Kolberg-Pioneer, Inc. will provide the Social
APPLICATION FOR EMPLOYMENT Kolberg-Pioneer, Inc. An Equal Opportunity Employer (HRF-002-03 01/16) This application is valid for the calendar year of 2018. Kolberg-Pioneer, Inc. will provide the Social
Application for Employment
 Position Sought: Community Transit of Delaware County, Inc. 206 Eddystone Avenue Suite 200 Eddystone, PA 19022-1594 Application for Employment Date: (Last) (First) (Middle Name) (Street Address) (City)
Position Sought: Community Transit of Delaware County, Inc. 206 Eddystone Avenue Suite 200 Eddystone, PA 19022-1594 Application for Employment Date: (Last) (First) (Middle Name) (Street Address) (City)
CITY OF CALISTOGA DOWN PAYMENT ASSISTANCE PROGRAM LOAN APPLICATION
 DOWN PAYMENT ASSISTANCE PROGRAM LOAN APPLICATION Date Applicant s Name Phone Residence Address Home City, State, Zip Code Phone Mailing Address (If different) FAMILY INFORMATION Applicant or Co-Applicant
DOWN PAYMENT ASSISTANCE PROGRAM LOAN APPLICATION Date Applicant s Name Phone Residence Address Home City, State, Zip Code Phone Mailing Address (If different) FAMILY INFORMATION Applicant or Co-Applicant
Mobiloil Federal Credit Union Employment Application
 Mobiloil Federal Credit Union Employment Application It is our policy to provide equal employment opportunity to all qualified persons without regard to race, creed, color, religious belief, sex, age,
Mobiloil Federal Credit Union Employment Application It is our policy to provide equal employment opportunity to all qualified persons without regard to race, creed, color, religious belief, sex, age,
Employment Application
 Employment Application To Applicant Instructions We appreciate your interest in our company and we are interested in reviewing your qualifications for our current open positions. To make this the best
Employment Application To Applicant Instructions We appreciate your interest in our company and we are interested in reviewing your qualifications for our current open positions. To make this the best
State Employees Credit Union Application for Employment
 State Employees Credit Union Application for Employment Note: Application must be handwritten. Do not type. We appreciate your interest in our organization. Please complete the application as fully as
State Employees Credit Union Application for Employment Note: Application must be handwritten. Do not type. We appreciate your interest in our organization. Please complete the application as fully as
To determine your eligibility for the program, the following documentation must be completed and submitted:
 Dear Applicant, As a participating jurisdiction in the St. Charles Urban County, the City of St. Peters will administer a St. Peters Urban County Home Improvement Loan Program (H.I.L.P) once federal funding
Dear Applicant, As a participating jurisdiction in the St. Charles Urban County, the City of St. Peters will administer a St. Peters Urban County Home Improvement Loan Program (H.I.L.P) once federal funding
Voluntary Information for Equal Employment Opportunity Purposes
 Voluntary Information for Equal Employment Opportunity Purposes Below is a Voluntary Information Sheet that we would like you to complete. It will be used for Equal Opportunity purposes only. The requested
Voluntary Information for Equal Employment Opportunity Purposes Below is a Voluntary Information Sheet that we would like you to complete. It will be used for Equal Opportunity purposes only. The requested
Exact title of the position for which you are applying. Applications will only be processed for current vacancy. (Last) (First) (Middle)
 (First) (Middle)") EFFINGHAM COUNTY BOARD OF COMMISSIONERS Employment Application 601 North Laurel Street Springfield, Georgia 31329 hr@effinghamcounty.org Telephone: 912-754-2104 Fax: 912-754-8402 We are an equal opportunity/drug
EFFINGHAM COUNTY BOARD OF COMMISSIONERS Employment Application 601 North Laurel Street Springfield, Georgia 31329 hr@effinghamcounty.org Telephone: 912-754-2104 Fax: 912-754-8402 We are an equal opportunity/drug
Nutrition Services Division DCH 06 (REV. 8/2018) PAGE 1 of 6 MEAL BENEFIT FORM FOR PROVIDERS
 PAGE 1 of 6 MEAL BENEFIT FORM FOR PROVIDERS") PAGE 1 of 6 MEAL BENEFIT FORM FOR PROVIDERS Complete, sign, and return this form to your day care home (DCH) sponsor. If you need assistance completing this form, call: (213) 380-3850 Name of DCH provider:
PAGE 1 of 6 MEAL BENEFIT FORM FOR PROVIDERS Complete, sign, and return this form to your day care home (DCH) sponsor. If you need assistance completing this form, call: (213) 380-3850 Name of DCH provider:
Preliminary Rental Application
 OP 241 For Office Use Only Rec d Time Rec d Initials Preliminary Rental Application Please note that this is a preliminary application and gives no lease or rent rights. Community Office ( ) Unit Size
OP 241 For Office Use Only Rec d Time Rec d Initials Preliminary Rental Application Please note that this is a preliminary application and gives no lease or rent rights. Community Office ( ) Unit Size
MASSACHUSETTS WATER RESOURCES AUTHORITY Employment Application
 MASSACHUSETTS WATER RESOURCES AUTHORITY Employment Application Massachusetts Water Resources Authority is an Equal Opportunity/Affirmative Action Employer. MWRA does not discriminate on the basis of race,
MASSACHUSETTS WATER RESOURCES AUTHORITY Employment Application Massachusetts Water Resources Authority is an Equal Opportunity/Affirmative Action Employer. MWRA does not discriminate on the basis of race,
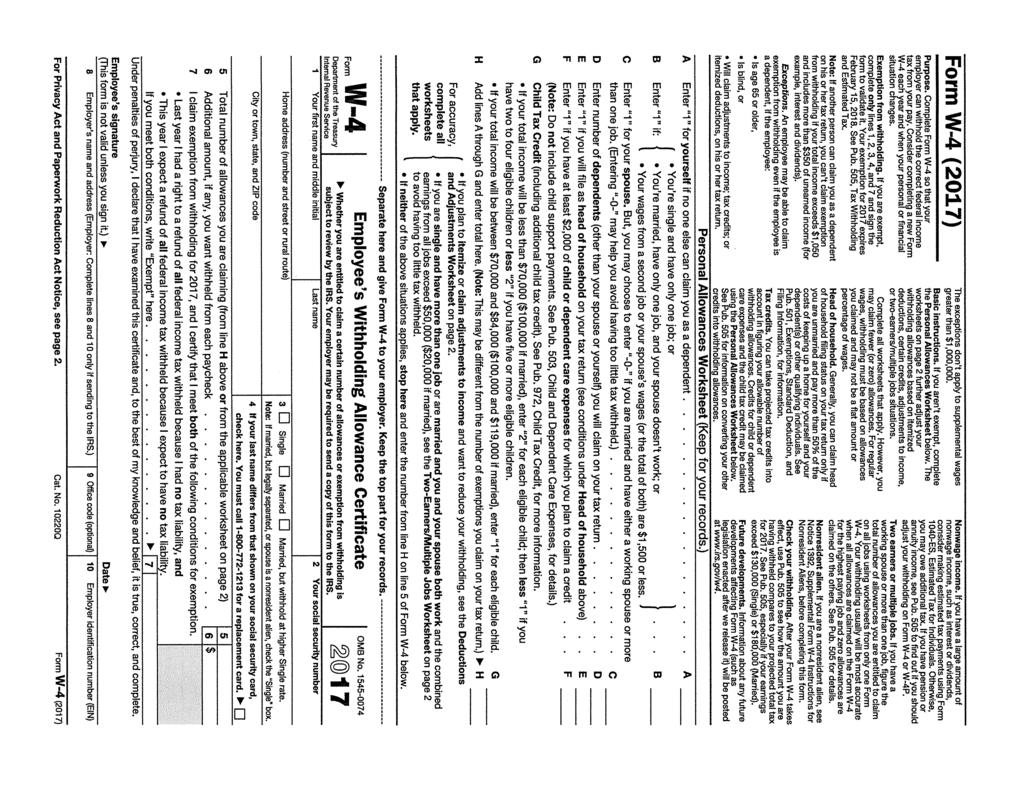
Separate here and give Form W-4 to your employer. Keep the top part for your records. Employee s Withholding Allowance Certificate
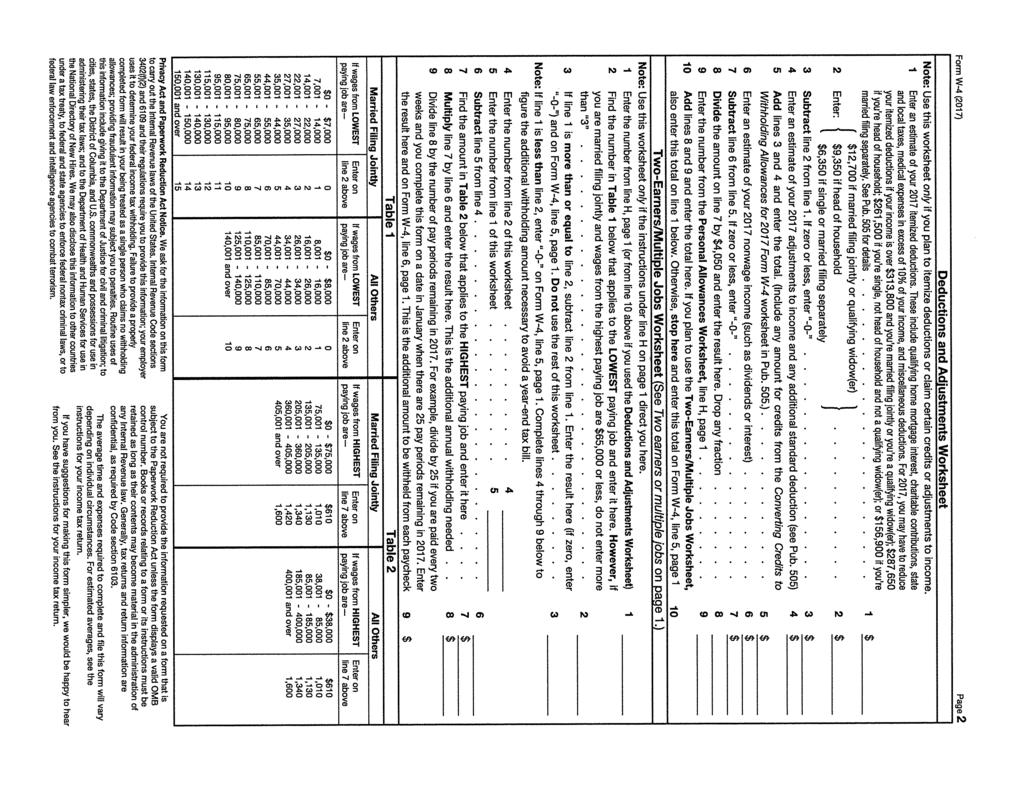
 Form W-4 (2017) Purpose. Complete Form W-4 so that your employer can withhold the correct federal income tax from your pay. Consider completing a new Form W-4 each year and when your personal or financial
Form W-4 (2017) Purpose. Complete Form W-4 so that your employer can withhold the correct federal income tax from your pay. Consider completing a new Form W-4 each year and when your personal or financial
MEAL BENEFIT FORM FOR PROVIDERS
 PAGE 1 of 5 MEAL BENEFIT FORM FOR PROVIDERS Complete, sign, and return this form to your day care home (DCH) sponsor. If you need assistance completing this form, call: Juanita Royal (916) 344-6259 Ext.
PAGE 1 of 5 MEAL BENEFIT FORM FOR PROVIDERS Complete, sign, and return this form to your day care home (DCH) sponsor. If you need assistance completing this form, call: Juanita Royal (916) 344-6259 Ext.
ESKATON HAZEL SHIRLEY MANOR San Pablo Avenue, El Cerrito, CA PH: (510) FAX: (510) TDD: (800)
 FAX: (510) TDD: (800)") RCVD BY DATE TIME ESKATON HAZEL SHIRLEY MANOR 11025 San Pablo Avenue, El Cerrito, CA 94530 PH: (510) 232-3430 FAX: (510) 232-1056 TDD: (800) 735-2922 www.eskaton.org APPLICATION FOR HOUSING PLEASE PRINT
RCVD BY DATE TIME ESKATON HAZEL SHIRLEY MANOR 11025 San Pablo Avenue, El Cerrito, CA 94530 PH: (510) 232-3430 FAX: (510) 232-1056 TDD: (800) 735-2922 www.eskaton.org APPLICATION FOR HOUSING PLEASE PRINT
Personal Information: *Please complete all information. Use ink and print clearly, so we can get to know you! Last Name:
 In order to be hired, you must be willing to submit to a physical and urinalysis screening. Application is valid for thirty (30) days from Date Received Today s Date: Bausch-American Towers Attn: HR Manager,
In order to be hired, you must be willing to submit to a physical and urinalysis screening. Application is valid for thirty (30) days from Date Received Today s Date: Bausch-American Towers Attn: HR Manager,
GEORGIA DEPARTMENT OF EDUCATION (GDOE) Administrative Technology Division. FY 2017 CPI Data Collection Data Elements Glossary
 Administrative Technology Division. FY 2017 CPI Data Collection Data Elements Glossary") GEORGIA DEPARTMENT OF EDUCATION (GDOE) Administrative Technology Division FY 2017 CPI Data Collection Data Elements Glossary CPI DATA ELEMENTS GLOSSARY Glossary ANNUAL CONTRACT SALARY FOR CERTIFIED ANNUAL
GEORGIA DEPARTMENT OF EDUCATION (GDOE) Administrative Technology Division FY 2017 CPI Data Collection Data Elements Glossary CPI DATA ELEMENTS GLOSSARY Glossary ANNUAL CONTRACT SALARY FOR CERTIFIED ANNUAL
AN EQUAL OPPORTUNITY EMPLOYER DATE SOCIAL SECURITY NUMBER CITY CITY IN CASE OF EMERGENCY NOTIFY: NAME RELATIONSHIP TELEPHONE NUMBER ( ) YES NO
 YES NO") Please fill out the application in its entirety FIRST MIDDLE LAST AN EQUAL OPPORTUNITY EMPLOYER DATE SOCIAL SECURITY NUMBER 20 PRESENT STREET CITY STATE ZIP PERSONAL PERMANENT TELEPHONE NUMBER HOME STREET
Please fill out the application in its entirety FIRST MIDDLE LAST AN EQUAL OPPORTUNITY EMPLOYER DATE SOCIAL SECURITY NUMBER 20 PRESENT STREET CITY STATE ZIP PERSONAL PERMANENT TELEPHONE NUMBER HOME STREET
MedStart-5. Application for Assistance
 MedStart-5 Application for Assistance Transportation Meals Assistance Utilities Co-Payments Adult Home Care Lab Testing For application help, contact us at 1-888-842-2654 To apply for benefits, follow
MedStart-5 Application for Assistance Transportation Meals Assistance Utilities Co-Payments Adult Home Care Lab Testing For application help, contact us at 1-888-842-2654 To apply for benefits, follow
July Dear Provider:
 , Inc. Our Mission is to encourage and support the success and well-being of children, families and the child care community... July 2018 Dear Provider: To qualify for tier I reimbursement for meals served
, Inc. Our Mission is to encourage and support the success and well-being of children, families and the child care community... July 2018 Dear Provider: To qualify for tier I reimbursement for meals served
WAITLIST APPLICATION CHECK LIST
 3550 VILLA LANE NAPA, CALIFORNIA 94558-3436 (707) 251-8077 WAITLIST APPLICATION CHECK LIST Thank you for your interest in Silverado Creek rental housing. For your convenience we ve summarized below the
3550 VILLA LANE NAPA, CALIFORNIA 94558-3436 (707) 251-8077 WAITLIST APPLICATION CHECK LIST Thank you for your interest in Silverado Creek rental housing. For your convenience we ve summarized below the
Villanova University New Employee Personal Information Form
 Villanova University New Employee Personal Infmation Fm Employee Name (as it appears on your social security card): Department: of Birth: Gender: US Citizen? If no, Visa status/permanent resident #: of
Villanova University New Employee Personal Infmation Fm Employee Name (as it appears on your social security card): Department: of Birth: Gender: US Citizen? If no, Visa status/permanent resident #: of
Volunteer Driver Application
 Volunteer Driver Application PLEASE PRINT This application will be used to establish your eligibility as a volunteer driver for the Drive to Help program. The information you provide helps us assure you,
Volunteer Driver Application PLEASE PRINT This application will be used to establish your eligibility as a volunteer driver for the Drive to Help program. The information you provide helps us assure you,
Hardee County Board of County Commissioners Equal Employment Opportunity (EEO) Self-Identification Form (completion of this form is voluntary)
 Self-Identification Form (completion of this form is voluntary)") Please submit to: Hardee County Board of County Commissioners HR Department 205 Hanchey Road, Wauchula, Florida 33873 Phone: (863) 773-2161 Hardee County Board of County Commissioners Equal Employment
Please submit to: Hardee County Board of County Commissioners HR Department 205 Hanchey Road, Wauchula, Florida 33873 Phone: (863) 773-2161 Hardee County Board of County Commissioners Equal Employment
REVOLVING LOAN FUND POLICY
 REVOLVING LOAN FUND POLICY The purpose of this policy is to provide guidance regarding loans from a revolving loan fund (RLF) to private and public entities for projects that benefit the community. Nothing
REVOLVING LOAN FUND POLICY The purpose of this policy is to provide guidance regarding loans from a revolving loan fund (RLF) to private and public entities for projects that benefit the community. Nothing
Small Business Enterprise Program
 Small Business Enterprise Program Registration & Roster Enrollment Registration Does NOT Pre-Approve You (The City may use this information to develop bid lists, contract lists and reports. Prime contractors
Small Business Enterprise Program Registration & Roster Enrollment Registration Does NOT Pre-Approve You (The City may use this information to develop bid lists, contract lists and reports. Prime contractors
TRADE ACT PARTICIPANT REPORT
 TRADE ACT PARTICIPANT REPORT REVISED PARTICIPANT RECORD LAYOUT Field Number Field Name Guidelines and Comments Section I: Identification and Characteristics of Applicant 1 I.1. State name Record the full
TRADE ACT PARTICIPANT REPORT REVISED PARTICIPANT RECORD LAYOUT Field Number Field Name Guidelines and Comments Section I: Identification and Characteristics of Applicant 1 I.1. State name Record the full
1. PLEASE READ CAREFULLY Applications will be processed in order of date and time received.
 Dear Applicant: Thank you for applying for tenancy at W a t e r s E d g e C r e s c e n t 1 located in Elizabeth, New Jersey 07206. Please complete this application in accordance with the following application
Dear Applicant: Thank you for applying for tenancy at W a t e r s E d g e C r e s c e n t 1 located in Elizabeth, New Jersey 07206. Please complete this application in accordance with the following application
Applications will only be accepted from
 May 2018 Dear Applicant, Thank you for your interest in applying to Pikes Peak Habitat for Humanity! Enclosed you will find the Habitat for Humanity application. Before completing the application, please
May 2018 Dear Applicant, Thank you for your interest in applying to Pikes Peak Habitat for Humanity! Enclosed you will find the Habitat for Humanity application. Before completing the application, please
NAME (FIRST) (MIDDLE) (LAST) SOCIAL SECURITY NO. (OPTIONAL) DATE OF APPLICATION
 (MIDDLE) (LAST) SOCIAL SECURITY NO. (OPTIONAL) DATE OF APPLICATION") Bristol Bay Area Health Corporation P.O. Box 130 Dillingham, Alaska 99576 Phone: 1-907-842-5201 --- In Alaska: 1-800-478-5201 Fax: 1-907-842-9251 --- Email: recruitment@bbahc.org BBAHC enforces a drug
Bristol Bay Area Health Corporation P.O. Box 130 Dillingham, Alaska 99576 Phone: 1-907-842-5201 --- In Alaska: 1-800-478-5201 Fax: 1-907-842-9251 --- Email: recruitment@bbahc.org BBAHC enforces a drug
City of Becker Employment Application
 Date Received: Received By: City of Becker Employment Application Return to: Becker Community Center PO Box 250 Becker, MN 55308 Ph: 763-200-4271 Fax: 763-261-2018 Applicant Name: Last First Middle Initial
Date Received: Received By: City of Becker Employment Application Return to: Becker Community Center PO Box 250 Becker, MN 55308 Ph: 763-200-4271 Fax: 763-261-2018 Applicant Name: Last First Middle Initial
City of Shorewood Application for Employment
 City of Shorewood Application for Employment We welcome you as an applicant for employment with the City of Shorewood. It is the City of Shorewood s policy to provide equal opportunity in employment. The
City of Shorewood Application for Employment We welcome you as an applicant for employment with the City of Shorewood. It is the City of Shorewood s policy to provide equal opportunity in employment. The
Application for Employment
 Application for Employment We welcome you as an applicant for employment with the City of Red Wing. It is the City of Red Wing s policy to provide equal opportunity in employment. The City of Red Wing
Application for Employment We welcome you as an applicant for employment with the City of Red Wing. It is the City of Red Wing s policy to provide equal opportunity in employment. The City of Red Wing
Employment Application Fire & Rescue Department
 Village of Pleasant Prairie 9915 39 th Avenue Pleasant Prairie, WI 53158 (262) 925-6731 Fax (262) 925-6788 Town of Salem 8339 Antioch Road Salem, WI 53168 (262) 298-5630 Fax (262) 298-5649 Employment Application
Village of Pleasant Prairie 9915 39 th Avenue Pleasant Prairie, WI 53158 (262) 925-6731 Fax (262) 925-6788 Town of Salem 8339 Antioch Road Salem, WI 53168 (262) 298-5630 Fax (262) 298-5649 Employment Application
A - EMPLOYEE INFORMATION SUBMISSION AND CERTIFICATION
 Office/Client Number New Employee Packet Employer Information: Choose your option for submitting employee information. For detailed instructions for these options, refer to the PEO New Employee Packet
Office/Client Number New Employee Packet Employer Information: Choose your option for submitting employee information. For detailed instructions for these options, refer to the PEO New Employee Packet
FORMS TO BE COMPLETED AND SUBMITTED TO HUMAN RESOURCES. The College requires all Employees complete and submit the following documents:
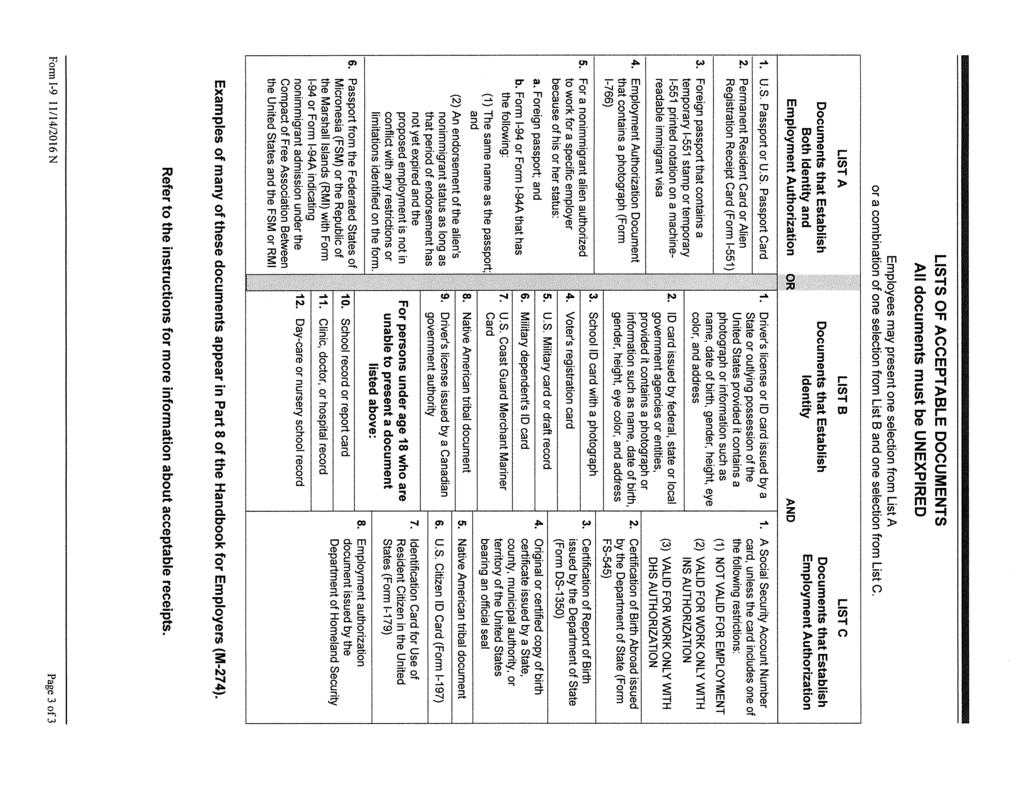
 FORMS TO BE COMPLETED AND SUBMITTED TO HUMAN RESOURCES The College requires all Employees complete and submit the following documents: 1. I-9 Employment Eligibility Verification: Complete the I-9 Form
FORMS TO BE COMPLETED AND SUBMITTED TO HUMAN RESOURCES The College requires all Employees complete and submit the following documents: 1. I-9 Employment Eligibility Verification: Complete the I-9 Form
Last Name First Name Middle Name. Street Address City State Zip Code
 EMPLOYMENT APPLICATION Clean All Services is an equal opportunity employer and affords equal opportunity to all applicants for all positions without regard to race, color, religion, gender, national origin,
EMPLOYMENT APPLICATION Clean All Services is an equal opportunity employer and affords equal opportunity to all applicants for all positions without regard to race, color, religion, gender, national origin,
APPLICATION FOR STATE CERTIFICATION
 APPLICATION FOR STATE CERTIFICATION Thank you for your interest in applying for state certification. We ask that you carefully complete each question. If a question is not applicable, simply answer that
APPLICATION FOR STATE CERTIFICATION Thank you for your interest in applying for state certification. We ask that you carefully complete each question. If a question is not applicable, simply answer that
WELCOME TO TORRANCE MEMORIAL PHYSICIAN NETWORK
 WELCOME TO TORRANCE MEMORIAL PHYSICIAN NETWORK Thank you for choosing us as your healthcare provider. We have enclosed instructions for filling out the paperwork that will be necessary for your first visit.
WELCOME TO TORRANCE MEMORIAL PHYSICIAN NETWORK Thank you for choosing us as your healthcare provider. We have enclosed instructions for filling out the paperwork that will be necessary for your first visit.
Security Deposit Loan Application 405 SW 6th Street Redmond, Oregon *
 Security Deposit Loan Application 405 SW 6th Street Redmond, Oregon 97756 * 541-923-1018 Thank you for your interest in the Families Forward loan program. Loans are available to Housing Choice Voucher
Security Deposit Loan Application 405 SW 6th Street Redmond, Oregon 97756 * 541-923-1018 Thank you for your interest in the Families Forward loan program. Loans are available to Housing Choice Voucher
Application For Employment Town of Stoughton 10 Pearl Street Stoughton, MA 02072
 Application For Employment Town of Stoughton 10 Pearl Street Stoughton, MA 02072 Please Print Qualified applicants are considered for all positions without regard to race, color, religion, sex, national
Application For Employment Town of Stoughton 10 Pearl Street Stoughton, MA 02072 Please Print Qualified applicants are considered for all positions without regard to race, color, religion, sex, national
Application and Tenant Selection Information
 1277 Shoreline Lane Boise, Idaho 83702 (208) 336-4610 Phone ~ (208) 345-8990 Fax, TDD #1-800-545-1833 Ext. 298 Application and Tenant Selection Information Completed applications for the should be returned
1277 Shoreline Lane Boise, Idaho 83702 (208) 336-4610 Phone ~ (208) 345-8990 Fax, TDD #1-800-545-1833 Ext. 298 Application and Tenant Selection Information Completed applications for the should be returned
YOU MUST MEET THE FOLLOWING BASIC REQUIREMENTS TO BE CONSIDERED FOR SELECTION:
 YOU MUST MEET THE FOLLOWING BASIC REQUIREMENTS TO BE CONSIDERED FOR SELECTION: You must have attended a Homeowner Information Meeting within the past 6 months. You must have lived or worked in Lee or Hendry
YOU MUST MEET THE FOLLOWING BASIC REQUIREMENTS TO BE CONSIDERED FOR SELECTION: You must have attended a Homeowner Information Meeting within the past 6 months. You must have lived or worked in Lee or Hendry
APPLICATION FOR EMPLOYMENT
 APPLICATION FOR EMPLOYMENT Morgan-Keller is an equal opportunity employer and does not discriminate on the basis of race, religion, color, national origin, age, sex, gender, disability or any other characteristic
APPLICATION FOR EMPLOYMENT Morgan-Keller is an equal opportunity employer and does not discriminate on the basis of race, religion, color, national origin, age, sex, gender, disability or any other characteristic
American Academy of Ophthalmology IRIS Registry (Intelligent Research in Sight) Analytics Data Dictionary
 Analytics Data Dictionary") 10/23/2018 American Academy of Ophthalmology IRIS Registry (Intelligent Research in Sight) Analytics Data Dictionary Disclaimer: This data dictionary covers the data elements found within the American
10/23/2018 American Academy of Ophthalmology IRIS Registry (Intelligent Research in Sight) Analytics Data Dictionary Disclaimer: This data dictionary covers the data elements found within the American
To become an Amador Rides Volunteer Driver, you must provide:
 Become an Volunteer Driver! Amador Rides is a collaborative effort from several organizations who want to make sure that Amador County residents can get to their medical, dental, and mental health appointments.
Become an Volunteer Driver! Amador Rides is a collaborative effort from several organizations who want to make sure that Amador County residents can get to their medical, dental, and mental health appointments.
Laclede Electric Cooperative Application For Employment
 Laclede Electric Cooperative Application For Employment It is the policy of Laclede Electric Cooperative (LEC) to provide equal opportunity with regard to all terms and conditions of employment. No information
Laclede Electric Cooperative Application For Employment It is the policy of Laclede Electric Cooperative (LEC) to provide equal opportunity with regard to all terms and conditions of employment. No information
BPO Vendor Packet. Please or fax your completed application back to ISGN:
 BPO Vendor Packet Thank you for your interest in becoming an ISGN Vendor Partner. Please complete the following documents so we may successfully set up your account: 1. Vendor Application 2. Affiliate
BPO Vendor Packet Thank you for your interest in becoming an ISGN Vendor Partner. Please complete the following documents so we may successfully set up your account: 1. Vendor Application 2. Affiliate
Affordable/Income Restricted Housing Lottery Application
 Affordable/Income Restricted Housing Lottery Application Development Name: Weinberg House Development Address: 132 Chestnut Hill Ave, Brighton MA 02135 Deadline to Submit Application: September 7, 2018
Affordable/Income Restricted Housing Lottery Application Development Name: Weinberg House Development Address: 132 Chestnut Hill Ave, Brighton MA 02135 Deadline to Submit Application: September 7, 2018
Rent & Income Chart ACKNOWLEDGMENT OF APPLICATION FOR NEW COMMUNITY HOUSING PROCEDURE:
 Dear Applicant: Thank you for your interest in Marveland Crescent, an affordable community located in the Flanders section of Mt. Olive, New Jersey. Nestled in a park like setting, Marveland Crescent features
Dear Applicant: Thank you for your interest in Marveland Crescent, an affordable community located in the Flanders section of Mt. Olive, New Jersey. Nestled in a park like setting, Marveland Crescent features
CHASE RUN APARTMENTS RENTAL APPLICATION PACKET
 CHASE RUN APARTMENTS RENTAL APPLICATION PACKET Thank you for your interest in Chase Run Apartments. Please feel free to contact our office at 989-772 772-7029 7029 if you have any questions while completing
CHASE RUN APARTMENTS RENTAL APPLICATION PACKET Thank you for your interest in Chase Run Apartments. Please feel free to contact our office at 989-772 772-7029 7029 if you have any questions while completing
LOAN APPLICATION P.O. BOX 1138, HUNTSVILLE, AR OFFICE: FAX:
 LOAN APPLICATION P.O. BOX 1138, HUNTSVILLE, AR 72740 OFFICE: 479.738.1585 FAX: 479.738.6288 FORGE@forgefund.org Please take your time filling out this application. If you need help, please contact FORGE
LOAN APPLICATION P.O. BOX 1138, HUNTSVILLE, AR 72740 OFFICE: 479.738.1585 FAX: 479.738.6288 FORGE@forgefund.org Please take your time filling out this application. If you need help, please contact FORGE
Summer U LEAD Program Application
 Summer U LEAD Program Application U LEAD is offers a summer job internship program for Ramsey County Suburban youth ages 14 to 24. Youth must complete the summer application and complete work readiness
Summer U LEAD Program Application U LEAD is offers a summer job internship program for Ramsey County Suburban youth ages 14 to 24. Youth must complete the summer application and complete work readiness
Name (First) (Middle) (Last) Address. (City) (State) (Zip Code) (Home Phone Number) (Cell Phone Number) ( Address)
 (Middle) (Last) Address. (City) (State) (Zip Code) (Home Phone Number) (Cell Phone Number) ( Address)") Date Name (First) (Middle) (Last) Address (Number) (Street) (City) (State) (Zip Code) (Home Phone Number) (Cell Phone Number) (Email Address) List previous addresses within last 5 years Are you over 18
Date Name (First) (Middle) (Last) Address (Number) (Street) (City) (State) (Zip Code) (Home Phone Number) (Cell Phone Number) (Email Address) List previous addresses within last 5 years Are you over 18
Pleasant Oaks of Stillwater
 Pleasant Oaks of Stillwater 207 East Pleasant Hill Drive Guthrie, OK 73044 Phone: 405-742-7887 Fax: 405-293-9260 Email: Dear Applicant, Thank you for your interest in Pleasant Oaks of Stillwater. We look
Pleasant Oaks of Stillwater 207 East Pleasant Hill Drive Guthrie, OK 73044 Phone: 405-742-7887 Fax: 405-293-9260 Email: Dear Applicant, Thank you for your interest in Pleasant Oaks of Stillwater. We look
California State University Channel Islands Ironwood Hall One University Drive Camarillo, CA (805)
") Division of Business and Financial Affairs Procurement & Logistical Services Service Provider/Contractor/: Thank you for your interest in doing business with California State University Channel Islands
Division of Business and Financial Affairs Procurement & Logistical Services Service Provider/Contractor/: Thank you for your interest in doing business with California State University Channel Islands
K A T L C KENTUCKY Revised June, 2011
 K A T L C KENTUCKY ASSISTIVE TECHNOLOGY LOAN CORPORATION FIFTH THIRD BANK, INC. Providing Financial Loans for Assistive Technology LOAN APPLICATION This Loan Program is Operated Jointly With PLEASE READ
K A T L C KENTUCKY ASSISTIVE TECHNOLOGY LOAN CORPORATION FIFTH THIRD BANK, INC. Providing Financial Loans for Assistive Technology LOAN APPLICATION This Loan Program is Operated Jointly With PLEASE READ
APPLICATION FOR EMPLOYMENT
 APPLICATION FOR EMPLOYMENT PLEASE ANSWER ALL QUESTIONS AND PRINT LEGIBLY. Please complete each section fully and accurately. Please PRINT, except for the signature at the end of this application. To the
APPLICATION FOR EMPLOYMENT PLEASE ANSWER ALL QUESTIONS AND PRINT LEGIBLY. Please complete each section fully and accurately. Please PRINT, except for the signature at the end of this application. To the
Revised Southern California Edison Company Page 1
 Diverse Business Enterprise (DBE) Subcontracting Commitment and Reporting Requirements I. Overview It is Edison s goal to provide diverse business enterprises ( DBEs ), such as women, minority and service-disabled
Diverse Business Enterprise (DBE) Subcontracting Commitment and Reporting Requirements I. Overview It is Edison s goal to provide diverse business enterprises ( DBEs ), such as women, minority and service-disabled
State of Connecticut Department of Social Services Application for Medicare Savings Programs (QMB, SLMB, ALMB)
") State of Connecticut Department of Social Services Application for Medicare Savings Programs (QMB, SLMB, ALMB) W-1QMB (Rev 8/16) Use this form to apply for Medicare Savings Program benefits. If you currently
State of Connecticut Department of Social Services Application for Medicare Savings Programs (QMB, SLMB, ALMB) W-1QMB (Rev 8/16) Use this form to apply for Medicare Savings Program benefits. If you currently
Employment Eligibility Verification
 Employment Eligibility Verification Department of Homeland Security U.S. Citizenship and Immigration Services USCIS Form I-9 OMB No. 1615-0047 Expires 08/31/2019 START HERE: Read instructions carefully
Employment Eligibility Verification Department of Homeland Security U.S. Citizenship and Immigration Services USCIS Form I-9 OMB No. 1615-0047 Expires 08/31/2019 START HERE: Read instructions carefully
Application for Benefits Medicaid Buy-In for Children
 Texas Health and Human Services Commission Form H1200-MBIC Cover Letter January 2011 Application for Benefits Medicaid Buy-In for Children About this program: Medicaid Buy-In for Children can help pay
Texas Health and Human Services Commission Form H1200-MBIC Cover Letter January 2011 Application for Benefits Medicaid Buy-In for Children About this program: Medicaid Buy-In for Children can help pay
MARYLAND HOSPITAL CREDENTIALING APPLICATION
 Error! Name STATE OF MARYLAND DHMH MARYLAND HOSPITAL CREDENTIALING APPLICATION Please type or print. Incomplete or illegible applications will not be processed. I. PERSONAL INFORMATION Name (Last, First,
Error! Name STATE OF MARYLAND DHMH MARYLAND HOSPITAL CREDENTIALING APPLICATION Please type or print. Incomplete or illegible applications will not be processed. I. PERSONAL INFORMATION Name (Last, First,
Rental Application for New Horizons 20 Benson Avenue Worcester, MA (508) / TTY (978)
 / TTY (978)") For Internal Use Only Rental Application for New Horizons 20 Benson Avenue Worcester, MA 01605 (508) 852-2711 / TTY (978) 630-6754 Date Received Time Received If you have a disability and as a result of
For Internal Use Only Rental Application for New Horizons 20 Benson Avenue Worcester, MA 01605 (508) 852-2711 / TTY (978) 630-6754 Date Received Time Received If you have a disability and as a result of
Subject: Referral Response: Berkeley Municipal Code Section Amendment Related to Commissioners
 Page 1 of 7 Office of the City Manager CONSENT CALENDAR July 25, 2017 To: From: Honorable Mayor and Members of the City Council Dee Williams-Ridley, City Manager Submitted by: Mark Numainville, City Clerk
Page 1 of 7 Office of the City Manager CONSENT CALENDAR July 25, 2017 To: From: Honorable Mayor and Members of the City Council Dee Williams-Ridley, City Manager Submitted by: Mark Numainville, City Clerk
Ohio Civil Service Application forstateandcountyagencies
 Ohio Civil Service Application forstateandcountyagencies GEN-4268 (REVISED 01/12) 06/08) ThestateofOhioisanEqualOpportunityEmployerandproviderofADAservices. State is an Opportunity Employer and provider
Ohio Civil Service Application forstateandcountyagencies GEN-4268 (REVISED 01/12) 06/08) ThestateofOhioisanEqualOpportunityEmployerandproviderofADAservices. State is an Opportunity Employer and provider
COMMUNITY: PROGRAM: ORIGINAL DATE: TIME: UPDATE: TIME:
 SUBJECT: APPLICANT FOR RESIDENCY TAX CREDIT COMMUNITIES COMMUNITY: PROGRAM: ORIGINAL DATE: TIME: UPDATE: TIME: HOW DID YOU HEAR ABOUT US? APARTMENT SIZE: APPLICANT NAME (FIRST, MIDDLE, LAST): CURRENT ADDRESS:
SUBJECT: APPLICANT FOR RESIDENCY TAX CREDIT COMMUNITIES COMMUNITY: PROGRAM: ORIGINAL DATE: TIME: UPDATE: TIME: HOW DID YOU HEAR ABOUT US? APARTMENT SIZE: APPLICANT NAME (FIRST, MIDDLE, LAST): CURRENT ADDRESS:
P E N N S Y L V A N I A Application for Payment of Medicare Premiums, Coinsurance and Deductibles
 P E N N S Y L V A N I A Application for Payment of Medicare Premiums, Coinsurance and Deductibles If you have a disability and need this form in large print or another format, please call our helpline
P E N N S Y L V A N I A Application for Payment of Medicare Premiums, Coinsurance and Deductibles If you have a disability and need this form in large print or another format, please call our helpline
SOUTH TEXAS HEROES HOUSING ASSISTANCE (STHHA) APPLICATION
 APPLICATION") APPLICANT CO-APPLICANT Rental Emergency Asst. Utility Pmt. Supportive Services SOCIAL SECURITY NUMBER SOCIAL SECURITY NUMBER HA HP DV/SA RELOCATION EVICTION OTHER CURRENT ADDRESS APT OR LOT # TELEPHONE
APPLICANT CO-APPLICANT Rental Emergency Asst. Utility Pmt. Supportive Services SOCIAL SECURITY NUMBER SOCIAL SECURITY NUMBER HA HP DV/SA RELOCATION EVICTION OTHER CURRENT ADDRESS APT OR LOT # TELEPHONE
New Employee Welcome Letter and Orientation Checklist
 Lafayette DQ Restaurants P.O. Box 302 Delphi, IN 46923 Phone: (765) 447-1089 Fax: (765) 535-5001 New Employee Welcome Letter and Orientation Checklist Welcome to the DQ family! In order to start training
Lafayette DQ Restaurants P.O. Box 302 Delphi, IN 46923 Phone: (765) 447-1089 Fax: (765) 535-5001 New Employee Welcome Letter and Orientation Checklist Welcome to the DQ family! In order to start training
Name Last First M.I. Head of Household
 PROGRAM APPLICATION Name First Last M.I. Street Address Apt. # City State Zip Phone Cell Email: Household Composition Name Last First M.I. Relationship Head of Household of Birth Age Social Security #
PROGRAM APPLICATION Name First Last M.I. Street Address Apt. # City State Zip Phone Cell Email: Household Composition Name Last First M.I. Relationship Head of Household of Birth Age Social Security #
Employment Application
 Employment Application Name: Home Address: Today s date Home Phone: Back-up Phone: Email Address: Are you 18 years of age or older? Yes No Other names under which you have worked or attended school: Are
Employment Application Name: Home Address: Today s date Home Phone: Back-up Phone: Email Address: Are you 18 years of age or older? Yes No Other names under which you have worked or attended school: Are
Application for Employment
 Application for Employment 221 E. Clark St. Albert Lea, MN 56007 We welcome you as an applicant for employment with the City of Albert Lea. It is the City s policy to provide equal opportunity in employment.
Application for Employment 221 E. Clark St. Albert Lea, MN 56007 We welcome you as an applicant for employment with the City of Albert Lea. It is the City s policy to provide equal opportunity in employment.
Please make sure your application has all of the items listed in the boxed area complete before turning it into YNHA Weatherization Program.
 Applicant Name: YAKAMA NATION HOUSING AUTHORITY Weatherization Application 701 South Camas Avenue - - P.O. Box 156 Wapato, WA 98951-1499 Phone: (509) 877-6171 Ext. 1105 or 1102 Fax: (509) 877-6317 Toll
Applicant Name: YAKAMA NATION HOUSING AUTHORITY Weatherization Application 701 South Camas Avenue - - P.O. Box 156 Wapato, WA 98951-1499 Phone: (509) 877-6171 Ext. 1105 or 1102 Fax: (509) 877-6317 Toll
City of Modesto Homeowner Rehabilitation Program
 City of Modesto Homeowner Rehabilitation Program Overview The City of Modesto s (City) Homeowner Rehabilitation Program is designed to repair or eliminate health and safety hazards in residential properties,
City of Modesto Homeowner Rehabilitation Program Overview The City of Modesto s (City) Homeowner Rehabilitation Program is designed to repair or eliminate health and safety hazards in residential properties,
Dear Prospective Homeowner,
 Dear Prospective Homeowner, Thank you for expressing an interest in partnering with Habitat for Humanity to help build and occupy a new home. The application process of our homeownership program is detailed
Dear Prospective Homeowner, Thank you for expressing an interest in partnering with Habitat for Humanity to help build and occupy a new home. The application process of our homeownership program is detailed
CATHOLICS FOR HOUSING, INC. (CFH) CFH NOVA DPA APPLICATION CHECK LIST JANUARY 2017
 CFH NOVA DPA APPLICATION CHECK LIST JANUARY 2017") CFH NOVA DPA APPLICATION CHECK LIST JANUARY 2017 Application Package Application completed and signed Authorization to Release Information First Time Homebuyer Affidavit Employment / Income Verification
CFH NOVA DPA APPLICATION CHECK LIST JANUARY 2017 Application Package Application completed and signed Authorization to Release Information First Time Homebuyer Affidavit Employment / Income Verification
City of Modesto Homebuyer Assistance Program
 City of Modesto Homebuyer Assistance Program Overview The City of Modesto s (City) Homebuyer Assistance Program provides deferred-payment; lowinterest loans to assist low income families purchase a qualified
City of Modesto Homebuyer Assistance Program Overview The City of Modesto s (City) Homebuyer Assistance Program provides deferred-payment; lowinterest loans to assist low income families purchase a qualified
Health Coverage & Help Paying Costs Application for One Person
 THINGS TO KNOW Health Coverage & Help Paying Costs Application for One Person Use this application to see what insurance choices you qualify for Free or low-cost insurance from Medicaid or the Kentucky
THINGS TO KNOW Health Coverage & Help Paying Costs Application for One Person Use this application to see what insurance choices you qualify for Free or low-cost insurance from Medicaid or the Kentucky
Massachusetts Application for Health and Dental Coverage and Help Paying Costs
 Massachusetts Application for Health and Dental Coverage and Help Paying Costs HOW TO APPLY USE THIS APPLICATION TO SEE WHAT COVERAGE CHOICES YOU MAY QUALIFY FOR. WHO CAN USE THIS APPLICATION? You can
Massachusetts Application for Health and Dental Coverage and Help Paying Costs HOW TO APPLY USE THIS APPLICATION TO SEE WHAT COVERAGE CHOICES YOU MAY QUALIFY FOR. WHO CAN USE THIS APPLICATION? You can
(Please Print using Black or Blue Ink) SEX: GENDER IDENTITY: MARITAL STATUS: SINGLE MARRIED OTHER
 SEX: GENDER IDENTITY: MARITAL STATUS: SINGLE MARRIED OTHER") PATIENT INFORMATION (Please Print using Black or Blue Ink) LAST NAME: FIRST NAME: MIDDLE INITIAL: ADDRESS: CITY: STATE: ZIP: SEX: GENDER IDENTITY: MARITAL STATUS: SINGLE MARRIED OTHER RACE (OPTIONAL):
PATIENT INFORMATION (Please Print using Black or Blue Ink) LAST NAME: FIRST NAME: MIDDLE INITIAL: ADDRESS: CITY: STATE: ZIP: SEX: GENDER IDENTITY: MARITAL STATUS: SINGLE MARRIED OTHER RACE (OPTIONAL):
EMPLOYMENT APPLICATION
 EMPLOYMENT APPLICATION POSITION APPLYING FOR: APPLICATION DATE: PERSONAL LAST NAME FIRST NAME MI PRIOR NAME(S), IF APPLICABLE MAILING ADDRESS CITY STATE ZIP WORK PHONE HOME PHONE CELL PHONE EMAIL ADDRESS
EMPLOYMENT APPLICATION POSITION APPLYING FOR: APPLICATION DATE: PERSONAL LAST NAME FIRST NAME MI PRIOR NAME(S), IF APPLICABLE MAILING ADDRESS CITY STATE ZIP WORK PHONE HOME PHONE CELL PHONE EMAIL ADDRESS
Jackson Municipal Airport Authority Certified Police Officer
 Jackson Municipal Airport Authority Certified Police Officer This is a certified law enforcement officer position. Successful candidates will perform a variety of duties in the enforcement of laws, rules
Jackson Municipal Airport Authority Certified Police Officer This is a certified law enforcement officer position. Successful candidates will perform a variety of duties in the enforcement of laws, rules
**ATTN: SOME PAGES NEED TO BE FILLED OUT ON BOTH SIDES**
 **ATTN: SOME PAGES NEED TO BE FILLED OUT ON BOTH SIDES** APPLICANT FLOW DATA Applicants are considered without regard to race, color, creed, national origin, religion, sex, disability, age, marital status,
**ATTN: SOME PAGES NEED TO BE FILLED OUT ON BOTH SIDES** APPLICANT FLOW DATA Applicants are considered without regard to race, color, creed, national origin, religion, sex, disability, age, marital status,
Date Position Applied For. Full Name. Last First Middle. Social Security No. Home Phone ( ) Cell Phone ( ) Present Address
 Cell Phone ( ) Present Address") APPLICATION FOR EMPLOYMENT PLEASE READ CAREFULLY AND ANSWER ALL QUESTIONS. Return completed application to: HR Dept. / 16243 Highway 216 / Brookwood, AL 35444 (Attach a separate sheet if additional space
APPLICATION FOR EMPLOYMENT PLEASE READ CAREFULLY AND ANSWER ALL QUESTIONS. Return completed application to: HR Dept. / 16243 Highway 216 / Brookwood, AL 35444 (Attach a separate sheet if additional space
Application Instructions
 Colorado CLT Application Instructions You must submit a completed application with all the required documentation prior to signing a contract for purchase. To ensure your application is complete, please
Colorado CLT Application Instructions You must submit a completed application with all the required documentation prior to signing a contract for purchase. To ensure your application is complete, please
ANTI-DISCRIMINATION POLICY of the SCHOOL DISTRICT OF PHILADELPHIA ADOPTED NOVEMBER 14, 2007
 ANTI-DISCRIMINATION POLICY of the SCHOOL DISTRICT OF PHILADELPHIA ADOPTED NOVEMBER 14, 2007 SECTION 1. THE POLICY It is the policy of the School District of Philadelphia (the "District") acting through
ANTI-DISCRIMINATION POLICY of the SCHOOL DISTRICT OF PHILADELPHIA ADOPTED NOVEMBER 14, 2007 SECTION 1. THE POLICY It is the policy of the School District of Philadelphia (the "District") acting through
Employment Application
 Personal Information Name (Last, First, MI) Date Email Position Applying For? What pay rate are you looking to make? How did you hear about the position? Position Specifications and Work Certifications
Personal Information Name (Last, First, MI) Date Email Position Applying For? What pay rate are you looking to make? How did you hear about the position? Position Specifications and Work Certifications
APPLICATION FOR EMPLOYMENT
 For Office Use Only 1 2 3 IN TERVIEWS SCH ED ULED Date Time Interviewer APPLICATION FOR EMPLOYMENT Date: / _/ _ PLEASE TYPE OR PRINT. In order to be considered for employment, this application must be
For Office Use Only 1 2 3 IN TERVIEWS SCH ED ULED Date Time Interviewer APPLICATION FOR EMPLOYMENT Date: / _/ _ PLEASE TYPE OR PRINT. In order to be considered for employment, this application must be
Property Management, Inc.
 EQUAL HOUSING O P P O R T U N I T Y Justus Property Management, Inc. RENTAL APPLICATION Marketing info: How did you hear about the property? Please include a $16.00 fee for each adult household member.
EQUAL HOUSING O P P O R T U N I T Y Justus Property Management, Inc. RENTAL APPLICATION Marketing info: How did you hear about the property? Please include a $16.00 fee for each adult household member.
Patient Name: DOB: Sex: Male/Female. Primary Address: Home Phone: Mobile Phone: Address: Emergency Contact Name and Phone Number:
 Patient Registration Patient Name: DOB: Sex: Male/Female Primary Address: Home Phone: Mobile Phone: Email Address: Emergency Contact Name and Phone Number: Primary Language: Race(s): (Circle all that applies)
Patient Registration Patient Name: DOB: Sex: Male/Female Primary Address: Home Phone: Mobile Phone: Email Address: Emergency Contact Name and Phone Number: Primary Language: Race(s): (Circle all that applies)
APPLICATION FOR APARTMENTS. NAME: Last First Middle. ADDRESS: Street City State Zip Code TELEPHONE #: HOME WORK MESSAGE. * Social Security #
 1 APPLICATION FOR APARTMENTS NAME: Last First Middle ADDRESS: Street City State Zip Code TELEPHONE #: HOME WORK MESSAGE APARTMENT SIZE REQUESTED Directions to Applicant: Answer all questions on this application.
1 APPLICATION FOR APARTMENTS NAME: Last First Middle ADDRESS: Street City State Zip Code TELEPHONE #: HOME WORK MESSAGE APARTMENT SIZE REQUESTED Directions to Applicant: Answer all questions on this application.
GENERAL INFORMATION (complete for all programs)
") FINANCIAL SELF-RELIANCE DEPARTMENT REQUEST FOR SERVICES I am interested in: Home Ownership Home Buyer s Certificate Foreclosure Prevention/Loss Mitigation Credit Counseling Other: GENERAL INFORMATION (complete
FINANCIAL SELF-RELIANCE DEPARTMENT REQUEST FOR SERVICES I am interested in: Home Ownership Home Buyer s Certificate Foreclosure Prevention/Loss Mitigation Credit Counseling Other: GENERAL INFORMATION (complete
Assist family members due to another family member s active military duty or impending active duty abroad
 Applying For Paid Family Leave To Use Paid Family Leave To: Bond with a newborn, a newly adopted or fostered child Complete Form PFL -1 Complete PFL-1, Part A Provide PFL-1 to employer Employer completes
Applying For Paid Family Leave To Use Paid Family Leave To: Bond with a newborn, a newly adopted or fostered child Complete Form PFL -1 Complete PFL-1, Part A Provide PFL-1 to employer Employer completes
Acknowledgement. Employee Signature. Printed Name. Job Title
 Acknowledgement I have read this job description and fully understand the requirements set forth therein. I understand that this is to be used as a guide and that I will be responsible for performing other
Acknowledgement I have read this job description and fully understand the requirements set forth therein. I understand that this is to be used as a guide and that I will be responsible for performing other
APPLICATION FOR APARTMENT
 For Office Use Only. Application ID: APPLICATION FOR APARTMENT INSTRUCTIONS: 1. SUBMIT ONLY ONE APPLICATION PER HOUSEHOLD. You may be disqualified if more than one application is received per lottery for
For Office Use Only. Application ID: APPLICATION FOR APARTMENT INSTRUCTIONS: 1. SUBMIT ONLY ONE APPLICATION PER HOUSEHOLD. You may be disqualified if more than one application is received per lottery for
CITY OF BOCA RATON SHIP APPLICATION PACKAGE WE ARE ACCEPTING SHIP APPLICATIONS ON AN ONGOING BASIS, UNTIL FURTHER NOTICE.
 Courtesy of http://www.downpaymentsolutions.com CITY OF BOCA RATON SHIP APPLICATION PACKAGE WE ARE ACCEPTING SHIP APPLICATIONS ON AN ONGOING BASIS, UNTIL FURTHER NOTICE. BEFORE SUBMITTING YOUR APPLICATION,
Courtesy of http://www.downpaymentsolutions.com CITY OF BOCA RATON SHIP APPLICATION PACKAGE WE ARE ACCEPTING SHIP APPLICATIONS ON AN ONGOING BASIS, UNTIL FURTHER NOTICE. BEFORE SUBMITTING YOUR APPLICATION,
 California Department of Education, May 2016 School Year 2016-2017 Sunrise Middle School Application for Free and Reduced-Price Meals: State Meal Program Complete one application per household. Read the
California Department of Education, May 2016 School Year 2016-2017 Sunrise Middle School Application for Free and Reduced-Price Meals: State Meal Program Complete one application per household. Read the
Optum SLCO Provider Biller s Training. Updated June 15, 2017 Optum Salt Lake County
 Optum SLCO Provider Biller s Training Updated June 15, 2017 Optum Salt Lake County Overview Provider Connect Search Window Enhancement Discharge Form MHER Updates Claim Submissions Emergency indicator
Optum SLCO Provider Biller s Training Updated June 15, 2017 Optum Salt Lake County Overview Provider Connect Search Window Enhancement Discharge Form MHER Updates Claim Submissions Emergency indicator
West River Revolving Loan Fund. Application Information
 West River Revolving Loan Fund Application Information Revised 2/17/2011 West River Revolving Loan Fund Application Information The West River Foundation, Inc., a private non-profit corporation, governs
West River Revolving Loan Fund Application Information Revised 2/17/2011 West River Revolving Loan Fund Application Information The West River Foundation, Inc., a private non-profit corporation, governs