Acknowledgement. Employee Signature. Printed Name. Job Title
|
|
|
- Erika Hall
- 6 years ago
- Views:
Transcription
1 Acknowledgement I have read this job description and fully understand the requirements set forth therein. I understand that this is to be used as a guide and that I will be responsible for performing other duties as assigned. I further understand that this job description does not constitute an employment contract with Premier Therapy. Employee Signature Date Printed Name Job Title 11/7/2013
2 RESIDENTS RIGHTS POLICY Policy: Each of the residents at this facility has a right to a dignified existence, self-determination and communication with and access to individuals and services inside and outside of facility. We promote and protect THE RIGHT OF EACH INDIVIDUAL RESIDENT TO: 1. Safe, clean living environment. 2. Be free from physical, verbal, mental and emotional abuse and to be treated with courtesy, respect and full recognition of dignity and individuality. 3. Adequate and appropriate medical treatment, nursing care and other services that comprise necessary and appropriate care consistent with the program for which the resident contracted. This care shall be provided without regard to race, color, religion, national origin, age or source of payment. 4. Have all reasonable requests and inquiries responded to promptly. 5. Have clothes and bed sheets changed as the need arises to insure comfort and sanitation. 6. Obtain a specialty of any physician or other person responsible for resident s care or for the coordination of care. 7. Select a staff physician of choice or obtain own physician outside the home. 8. Participate in decisions that affect your life; to participate in plan of care meetings; and participate in planning care in treatment and in changes in care and treatment, have access to information on medical record; give or withhold informed consent; refuse treatment. 9. Withhold payment to physician if physician did not visit. 10. Confidential treatment of personal and medical records: refuse release of medical record to any individual outside the home except as required by law we transfer to another facility, or as required by a third-party payment contract. 11. Privacy during medical examination or treatment and personal care. 12. Refuse to serve as medical research subject. 13. Be free from any physical or chemical restraints or prolonged isolation imposed for the purpose of discipline or convenience and not required to protect residents or others from injury unless ordered by the physician. (Chemical restraint is defined as that which alters the functioning of the central nervous system in a manner that limits physical and cognitive functioning to the degree that the resident cannot attain his or her highest practical physical, mental and psychological well being.) 14. Obtain pharmacist of choice and pay fair market price for drugs. 15. Exercise all civil rights unless adjudicated incompetent: Right to Vote. 16. Have access to opportunities that enable resident, at his/her expense or at the expense of a third-party payer, to achieve fullest potential in education, vocation, social, recreation and rehabilitation. 17. Consume a reasonable amount of alcoholic beverage, at his/her expense, unless contraindicated by attended physician. 18. To be informed, prior to admission, that this is a non-smoking facility. I, have read and understand the above (printed name) noted Resident s Rights and will adhere and abide by them accordingly. Signature Date

3

4
5

6

7

8

9


10
11
12 EMPLOYEE HANDBOOK ACKNOWLEDGMENT PAGE I ACKNOWLEDGE THAT I HAVE (please check one): received a printed copy viewed an electronic version* of the Premier Therapy Employee Handbook dated April 1, I understand that I am expected to read and comply with the Handbook. I ALSO UNDERSTAND THE FOLLOWING: The Employee Handbook outlines certain standards, policies, procedures, programs and benefits, but they are not all-inclusive and I am responsible for consulting with my supervisor, the next level of management or the Corporate Office regarding questions not addressed in the Handbook. The Employee Handbook is not intended to be, nor should I construe it as an express or implied contract of employment or a guarantee of employment for any specific period of time. It also is not intended to guarantee to me any specific terms or benefits of employment. The Employee Handbook is subject to change at the sole discretion of the Company and without prior notice. The Company may deviate from its standards, policies, procedures, programs and benefits, including those discussed in the Handbook, when it deems necessary in its sole discretion. This Employee Handbook supersedes and replaces all prior employee handbooks, manuals, or policies issued by the Company or any predecessor owner or operator. My employment with the Company is at-will, meaning that either the Company or I can terminate my employment at any time and for any reason and with or without cause or notice. No written materials may be distributed or oral representations made to me, which contradict the employment at-will standard. Please sign, date and fax this form to or mail to Premier Therapy, 701 Sharon Road, Beaver, PA Printed Name Employee s Signature Date *An electronic version is available via the company's intranet "Resources" link accessible from your therapy department.
13 EMPLOYMENT APPLICATION Today s Date: Premier Therapy and its affiliate, Atlas Rehab and Wellness, (the "Company") is an equal opportunity/affirmative action employer. All qualified applicants will be considered without regard to age, race, color, sex, religion, nation origin, marital status, ancestry, citizenship, veteran status, sexual orientation or preference, or ph ysical or mental disability. Rev. 5/1/13 Have you previously worked for Premier Therapy or Atlas Rehab & Wellness? PERSONAL If so, when and in what capacity? Last Name First Initial Social Security # Street Address Home Telephone # ( ) City State Zip Business Telephone # ( ) address Cell Telephone # ( ) Position Applied For Referred By Hourly Rate Desired EDUCATION Circle Highest Grade Completed: High School College, Trade or Business Graduate Studies School Name of School City and State Degree, Diploma, License/Certificate Date Graduated High School College/University Vocational, Business, Other List Any Professional Designations EMPLOYMENT HISTORY LIST ALL EMPLOYMENTS FOR THE PAST 10 YEARS, STARTING WITH THE MOST RECENT POSITION.ALL INFORMATION MUST BE COMPLETED.YOU MAY ATTACH A RESUME, BUT NOT IN PLACE OF COMPLETING THE REQUIRED INFORMATION. Employed From / / Employed Until / / Job Title Duties & Responsibilities Employer Name Supervisor Name Starting Salary Employer Address Supervisor Phone # Ending Salary Reason for Leaving Employed From / / Employed Until / / Job Title Employer Name Supervisor Name Starting Salary Employer Address Supervisor Phone # Ending Salary Reason for Leaving Duties & Responsibilities 1
14 REFERENCES (LIST THREE BUSINESS ASSOCIATED REFERENCES) Name Name Name Business Relationship/Years Acquainted Business Relationship/Years Acquainted Business Relationship/Years Acquainted Phone Phone Phone GENERAL Yes No If hired, will you be able to work rotating weekend and holiday coverage and overtime in accordance with Premier Therapy policy? Can you perform the essential functions of the position for which you are applying, with or without reasonable accommodation? If no, please explain. (If you have any question as to what functions are applicable to the position for which you are applying, please ask the interviewer before you answer the question.) Have you ever been convicted of a crime, including a sex abuse or child abuse-related crime, excluding misdemeanors and summary offenses, which has not been annulled, expunged or sealed by court? (A yes response does not automatically disqualify your application.) If yes, please explain. Have you ever had your professional license suspended, revoked, and/or are you currently under a disciplinary action status with the state licensing board? (A "yes" response does not automatically disqualify your application.) If yes, please explain. CERTIFICATION &AUTHORIZATION The above information is true and correct. I understand that, in the event of my employment by the Company, I shall be subject to dismissal if any information that I have given in this application is false or misleading or if I have failed to give any information herein requested, regardless of the time elapsed after discovery. I authorize the Company to inquire into my educational, professional and past employment history references as needed to research my qualifications for this position. I hereby give my consent to any former employer to provide employment-related information about me to the Company and will hold the Company and my former employer harmless from any claim made on the basis that such information about me was provided or that any employment decision was made on the basis of such information. I understand that nothing in this employment application, the granting of an interview or my subsequent employment with the Company is intended to create an employment contract between myself and the Company under which my employment could be terminated only for cause. On the contrary, I understand and agree that, if hired, my employment will be terminable at will and may be terminated by the Company or me at any time and for any reason. I understand that no person has any authority to enter into any agreement contrary to the foregoing. If employed, I will be required to provide original documents, which verify my identity and right to work in the United States under the Immigration Reform and Control Act (IRCA) of The document(s) provided will be used for completion of Form I-9. Resignation Without Notice Policy While we hope both you and Premier Therapy will mutually benefit from continued employment, we realize it may become necessary for you to leave your job with Premier. If you anticipate having to resign your position, you are expected to submit your written notice at least three (3) weeks in advance of the date you must leave and work all of your final schedule. In this regard, failure by an employee to comply with our Resignation Without Notice Policy will result in the employee being paid minimum wage for hours worked in any unissued paycheck and forfeiting any accrued paid time off. This policy helps Premier Therapy maintain the best quality care for our residents while avoiding interruptions. If an application for employment is going to be processed, the applicant must sign accordingly, signifying they understand this policy. For further information, ask your interviewer to show you the Resignation Without Notice Policy in the Premier Therapy Employee Handbook. I hereby acknowledge that I have read and agree to the above statements. Printed Name Signature Date 2 Please fax both pages to: or mail to: Premier Therapy 701 Sharon Rd. Beaver, PA 15009
15 Electronic Signature Form Signature will be uploaded to therapy software for use on electronic patient documentation and therapy records. PLEASE PRINT First Name: Middle Initial: Last Name: Discipline: * Date of Birth: / / OTs and OTAs: If you are NBCOT certified, your credentials will be OTR/L or COTA/L after your signature below. If you are not NBCOT certified, your credentials would be OTA/L or OT/L. PTs and PTAs: Please include PT or PTA after your signature below. Speech Therapists: Please include "CCC/SLP" or "CFY/SLP" following your signature below. Please keep entire signature AND CREDENTIALS within the box and DO NOT TOUCH THE LINES. Sign Here: Today's Date: Please sign, date, and fax this form to or mail to: Premier Therapy 701 Sharon Road Beaver, PA /16/13
16 Form W-4 (2014) Purpose. Complete Form W-4 so that your employer can withhold the correct federal income tax from your pay. Consider completing a new Form W-4 each year and when your personal or financial situation changes. Exemption from withholding. If you are exempt, complete only lines 1, 2, 3, 4, and 7 and sign the form to validate it. Your exemption for 2014 expires February 17, See Pub. 505, Tax Withholding and Estimated Tax. Note. If another person can claim you as a dependent on his or her tax return, you cannot claim exemption from withholding if your income exceeds $1,000 and includes more than $350 of unearned income (for example, interest and dividends). Exceptions. An employee may be able to claim exemption from withholding even if the employee is a dependent, if the employee: Is age 65 or older, Is blind, or Will claim adjustments to income; tax credits; or itemized deductions, on his or her tax return. The exceptions do not apply to supplemental wages greater than $1,000,000. Basic instructions. If you are not exempt, complete the Personal Allowances Worksheet below. The worksheets on page 2 further adjust your withholding allowances based on itemized deductions, certain credits, adjustments to income, or two-earners/multiple jobs situations. Complete all worksheets that apply. However, you may claim fewer (or zero) allowances. For regular wages, withholding must be based on allowances you claimed and may not be a flat amount or percentage of wages. Head of household. Generally, you can claim head of household filing status on your tax return only if you are unmarried and pay more than 50% of the costs of keeping up a home for yourself and your dependent(s) or other qualifying individuals. See Pub. 501, Exemptions, Standard Deduction, and Filing Information, for information. Tax credits. You can take projected tax credits into account in figuring your allowable number of withholding allowances. Credits for child or dependent care expenses and the child tax credit may be claimed using the Personal Allowances Worksheet below. See Pub. 505 for information on converting your other credits into withholding allowances. Nonwage income. If you have a large amount of nonwage income, such as interest or dividends, consider making estimated tax payments using Form 1040-ES, Estimated Tax for Individuals. Otherwise, you may owe additional tax. If you have pension or annuity iincome, see Pub. 505 to find out if you should adjust your withholding on Form W-4 or W-4P. Two earners or multiple jobs. If you have a working spouse or more than one job, figure the total number of allowances you are entitled to claim on all jobs using worksheets from only one Form W-4. Your withholding usually will be most accurate when all allowances are claimed on the Form W-4 for the highest paying job and zero allowances are claimed on the others. See Pub. 505 for details. Nonresident alien. If you are a nonresident alien, see Notice 1392, Supplemental Form W-4 Instructions for Nonresident Aliens, before completing this form. Check your withholding. After your Form W-4 takes effect, use Pub. 505 to see how the amount you are having withheld compares to your projected total tax for See Pub. 505, especially if your earnings exceed $130,000 (Single) or $180,000 (Married). Future developments. Information about any future developments affecting Form W-4 (such as legislation enacted after we release it) will be posted at Personal Allowances Worksheet (Keep for your records.) A Enter 1 for yourself if no one else can claim you as a dependent A You are single and have only one job; or B Enter 1 if: { You are married, have only one job, and your spouse does not work; or... B Your wages from a second job or your spouse s wages (or the total of both) are $1,500 or less. C Enter 1 for your spouse. But, you may choose to enter -0- if you are married and have either a working spouse or more than one job. (Entering -0- may help you avoid having too little tax withheld.) C D Enter number of dependents (other than your spouse or yourself) you will claim on your tax return D E Enter 1 if you will file as head of household on your tax return (see conditions under Head of household above).. E F Enter 1 if you have at least $2,000 of child or dependent care expenses for which you plan to claim a credit... F (Note. Do not include child support payments. See Pub. 503, Child and Dependent Care Expenses, for details.) G Child Tax Credit (including additional child tax credit). See Pub. 972, Child Tax Credit, for more information. If your total income will be less than $65,000 ($95,000 if married), enter 2 for each eligible child; then less 1 if you have three to six eligible children or less 2 if you have seven or more eligible children. If your total income will be between $65,000 and $84,000 ($95,000 and $119,000 if married), enter 1 for each eligible child... G H Add lines A through G and enter total here. (Note. This may be different from the number of exemptions you claim on your tax return.) H { If you plan to itemize or claim adjustments to income and want to reduce your withholding, see the Deductions For accuracy, and Adjustments Worksheet on page 2. complete all If you are single and have more than one job or are married and you and your spouse both work and the combined worksheets earnings from all jobs exceed $50,000 ($20,000 if married), see the Two-Earners/Multiple Jobs Worksheet on page 2 to that apply. avoid having too little tax withheld. If neither of the above situations applies, stop here and enter the number from line H on line 5 of Form W-4 below. Form W-4 Department of the Treasury Internal Revenue Service Separate here and give Form W-4 to your employer. Keep the top part for your records. Employee's Withholding Allowance Certificate Whether you are entitled to claim a certain number of allowances or exemption from withholding is subject to review by the IRS. Your employer may be required to send a copy of this form to the IRS. 1 Your first name and middle initial Last name OMB No Your social security number Home address (number and street or rural route) 3 Single Married Married, but withhold at higher Single rate. Note. If married, but legally separated, or spouse is a nonresident alien, check the Single box. City or town, state, and ZIP code 4 If your last name differs from that shown on your social security card, check here. You must call for a replacement card. 5 Total number of allowances you are claiming (from line H above or from the applicable worksheet on page 2) 5 6 Additional amount, if any, you want withheld from each paycheck $ 7 I claim exemption from withholding for 2014, and I certify that I meet both of the following conditions for exemption. Last year I had a right to a refund of all federal income tax withheld because I had no tax liability, and This year I expect a refund of all federal income tax withheld because I expect to have no tax liability. If you meet both conditions, write Exempt here Under penalties of perjury, I declare that I have examined this certificate and, to the best of my knowledge and belief, it is true, correct, and complete. Employee s signature (This form is not valid unless you sign it.) Date 8 Employer s name and address (Employer: Complete lines 8 and 10 only if sending to the IRS.) 9 Office code (optional) 10 Employer identification number (EIN) For Privacy Act and Paperwork Reduction Act Notice, see page 2. Cat. No Q Form W-4 (2014)
17 Form W-4 (2014) Page 2 Deductions and Adjustments Worksheet Note. Use this worksheet only if you plan to itemize deductions or claim certain credits or adjustments to income. 1 Enter an estimate of your 2014 itemized deductions. These include qualifying home mortgage interest, charitable contributions, state and local taxes, medical expenses in excess of 10% (7.5% if either you or your spouse was born before January 2, 1950) of your income, and miscellaneous deductions. For 2014, you may have to reduce your itemized deductions if your income is over $305,050 and you are married filing jointly or are a qualifying widow(er); $279,650 if you are head of household; $254,200 if you are single and not head of household or a qualifying widow(er); or $152,525 if you are married filing separately. See Pub. 505 for details $ $12,400 if married filing jointly or qualifying widow(er) 2 Enter: { $9,100 if head of household } $ $6,200 if single or married filing separately 3 Subtract line 2 from line 1. If zero or less, enter $ 4 Enter an estimate of your 2014 adjustments to income and any additional standard deduction (see Pub. 505) 4 $ 5 Add lines 3 and 4 and enter the total. (Include any amount for credits from the Converting Credits to Withholding Allowances for 2014 Form W-4 worksheet in Pub. 505.) $ 6 Enter an estimate of your 2014 nonwage income (such as dividends or interest) $ 7 Subtract line 6 from line 5. If zero or less, enter $ 8 Divide the amount on line 7 by $3,950 and enter the result here. Drop any fraction Enter the number from the Personal Allowances Worksheet, line H, page Add lines 8 and 9 and enter the total here. If you plan to use the Two-Earners/Multiple Jobs Worksheet, also enter this total on line 1 below. Otherwise, stop here and enter this total on Form W-4, line 5, page 1 10 Two-Earners/Multiple Jobs Worksheet (See Two earners or multiple jobs on page 1.) Note. Use this worksheet only if the instructions under line H on page 1 direct you here. 1 Enter the number from line H, page 1 (or from line 10 above if you used the Deductions and Adjustments Worksheet) 1 2 Find the number in Table 1 below that applies to the LOWEST paying job and enter it here. However, if you are married filing jointly and wages from the highest paying job are $65,000 or less, do not enter more than If line 1 is more than or equal to line 2, subtract line 2 from line 1. Enter the result here (if zero, enter -0- ) and on Form W-4, line 5, page 1. Do not use the rest of this worksheet Note. If line 1 is less than line 2, enter -0- on Form W-4, line 5, page 1. Complete lines 4 through 9 below to figure the additional withholding amount necessary to avoid a year-end tax bill. 4 Enter the number from line 2 of this worksheet Enter the number from line 1 of this worksheet Subtract line 5 from line Find the amount in Table 2 below that applies to the HIGHEST paying job and enter it here $ 8 Multiply line 7 by line 6 and enter the result here. This is the additional annual withholding needed.. 8 $ 9 Divide line 8 by the number of pay periods remaining in For example, divide by 25 if you are paid every two weeks and you complete this form on a date in January when there are 25 pay periods remaining in Enter the result here and on Form W-4, line 6, page 1. This is the additional amount to be withheld from each paycheck 9 $ Table 1 Table 2 Married Filing Jointly All Others Married Filing Jointly All Others If wages from LOWEST paying job are Enter on line 2 above $0 - $6, ,001-13, ,001-24, ,001-26, ,001-33, ,001-43, ,001-49, ,001-60, ,001-75, ,001-80, , , , , , , , , , , ,001 and over 15 If wages from LOWEST paying job are Enter on line 2 above $0 - $6, ,001-16, ,001-25, ,001-34, ,001-43, ,001-70, ,001-85, , , , , , , ,001 and over 10 Privacy Act and Paperwork Reduction Act Notice. We ask for the information on this form to carry out the Internal Revenue laws of the United States. Internal Revenue Code sections 3402(f)(2) and 6109 and their regulations require you to provide this information; your employer uses it to determine your federal income tax withholding. Failure to provide a properly completed form will result in your being treated as a single person who claims no withholding allowances; providing fraudulent information may subject you to penalties. Routine uses of this information include giving it to the Department of Justice for civil and criminal litigation; to cities, states, the District of Columbia, and U.S. commonwealths and possessions for use in administering their tax laws; and to the Department of Health and Human Services for use in the National Directory of New Hires. We may also disclose this information to other countries under a tax treaty, to federal and state agencies to enforce federal nontax criminal laws, or to federal law enforcement and intelligence agencies to combat terrorism. If wages from HIGHEST paying job are Enter on line 7 above $0 - $74,000 $590 74, , , ,000 1, , ,000 1, , ,000 1, ,001 and over 1,560 If wages from HIGHEST paying job are Enter on line 7 above $0 - $37,000 $590 37,001-80, , ,000 1, , ,000 1, ,001 and over 1,560 You are not required to provide the information requested on a form that is subject to the Paperwork Reduction Act unless the form displays a valid OMB control number. Books or records relating to a form or its instructions must be retained as long as their contents may become material in the administration of any Internal Revenue law. Generally, tax returns and return information are confidential, as required by Code section The average time and expenses required to complete and file this form will vary depending on individual circumstances. For estimated averages, see the instructions for your income tax return. If you have suggestions for making this form simpler, we would be happy to hear from you. See the instructions for your income tax return.
18 IT 4 Rev. 5/07 Notice to Employee 1. For state purposes, an individual may claim only natural dependency exemptions. This includes the taxpayer, spouse and each dependent. Dependents are the same as defined in the Internal Revenue Code and as claimed in the taxpayer s federal income tax return for the taxable year for which the taxpayer would have been permitted to claim had the taxpayer filed such a return. 2. You may file a new certificate at any time if the number of your exemptions increases. You must file a new certificate within 10 days if the number of exemptions previously claimed by you decreases because: (a) Your spouse for whom you have been claiming exemption is divorced or legally separated, or claims her (or his) own exemption on a separate certificate. (b) The support of a dependent for whom you claimed exemption is taken over by someone else. (c) You find that a dependent for whom you claimed exemption must be dropped for federal purposes. The death of a spouse or a dependent does not affect your withholding until the next year but requires the filing of a new certificate. If possible, file a new certificate by Dec. 1st of the year in which the death occurs. For further information, consult the Ohio Department of Taxation, Personal and School District Income Tax Division, or your employer. 3. If you expect to owe more Ohio income tax than will be withheld, you may claim a smaller number of exemptions; or under an agreement with your employer, you may have an additional amount withheld each pay period. 4. A married couple with both spouses working and filing a joint return will, in many cases, be required to file an individual estimated income tax form IT 1040ES even though Ohio income tax is being withheld from their wages. This result may occur because the tax on their combined income will be greater than the sum of the taxes withheld from the husband s wages and the wife s wages. This requirement to file an individual estimated income tax form IT 1040ES may also apply to an individual who has two jobs, both of which are subject to withholding. In lieu of filing the individual estimated income tax form IT 1040ES, the individual may provide for additional withholding with his employer by using line 5. please detach here Employee s Withholding Exemption Certificate IT 4 Rev. 5/07 Print full name Social Security number Home address and ZIP code Public school district of residence (See The Finder at tax.ohio.gov.) School district no. 1. Personal exemption for yourself, enter 1 if claimed If married, personal exemption for your spouse if not separately claimed (enter 1 if claimed) Exemptions for dependents Add the exemptions that you have claimed above and enter total Additional withholding per pay period under agreement with employer... $ Under the penalties of perjury, I certify that the number of exemptions claimed on this certificate does not exceed the number to which I am entitled. Signature Date
19 IT 4 NR! please detach here Employee s Statement of Residency in a Reciprocity State IT 4NR Rev. 12/00 Print full name Social security number Home address and ZIP code Ohio Employers: You are required to have a copy of this form on file for each employee who is a resident of Indiana, Kentucky, West Virginia, Michigan or Pennsylvania receiving compensation paid in Ohio and who claims exemption from withholding of Ohio income tax under the reciprocal agreements between Ohio and these other states. Employees residing outside Ohio and in a state with whom Ohio has reciprocity: If you are a resident of a state with whom Ohio has reciprocity, you may claim exemption from withholding of Ohio income tax by completing this form and filing it with your employer, under the reciprocal withholding agreements between Ohio and these states. Note: If you change your residence from the state specified herein to any other state, you must notify your employer within10 days. I hereby declare, under penalties of perjury, that I am a resident of the state of and that, pursuant to an agreement existing between that state and the state of Ohio, I claim exemption from withholding of Ohio income tax on compensation paid to me in the state of Ohio. Signature Date
20 CLGS-32-6 (8-11) FOR ALL EMPLOYEES WORKING IN PENNSYLVANIA REGARDLESS OF THEIR STATE OF RESIDENCY. RESIDENCY CERTIFICATION FORM Local Earned Income Tax Withholding TO EMPLOYERS/TAXPAYERS: This form is to be used by employers and/or taxpayers to report essential information for the collection and distribution of Local Earned Income Taxes. This form must be utilized by employers when a new employee is hired or when a current employee notifies employer of a name and/or address change. NAME (Last Name, First Name, Middle Initial) EMPLOYEE INFORMATION - RESIDENCE LOCATION SOCIAL SECURITY NUMBER STREET ADDRESS (No PO Box, RD or RR) SECOND LINE OF ADDRESS CITY STATE ZIP CODE DAYTIME PHONE NUMBER MUNICIPALITY (City, Borough or Township) COUNTY RESIDENT PSD CODE TOTAL RESIDENT EIT RATE EMPLOYER INFORMATION - EMPLOYMENT LOCATION EMPLOYER BUSINESS NAME (Use Federal ID Name) EMPLOYER FEIN Premier Therapy STREET ADDRESS WHERE ABOVE EMPLOYEE REPORTS TO WORK (No PO Box, RD or RR) SECOND LINE OF ADDRESS CITY STATE ZIP CODE PHONE NUMBER MUNICIPALITY (City, Borough or Township) COUNTY WORK LOCATION PSD CODE WORK LOCATION NON-RESIDENT EIT RATE SIGNATURE OF EMPLOYEE CERTIFICATION Under penalties of perjury, I (we) declare that I (we) have examined this information, including all accompanying schedules and statements and to the best of my (our) belief, they are true, correct and complete. DATE (MM/DD/YYYY) PHONE NUMBER ADDRESS For information on obtaining the appropriate MUNICIPALITY (City, Borough, Township), PSD CODES and EIT (Earned Income Tax) RATES, please refer to the Pennsylvania Department of Community & Economic Development website:
21 WORKERS COMPENSATION INFORMATION In Pennsylvania, the workers compensation law provides wage loss and medical benefits to employees who cannot work, or who need medical care, because of a work-related injury. Benefits are required to be paid by your employer when self-insured, or through insurance provided by your employer. Your employer is required to post the name of the company responsible for paying workers compensation benefits at its primary place of business and at its sites of employment in a prominent and easily accessible place, including, without limitation, areas used for the treatment of injured employees or for the administration of first-aid. You should report immediately any injury or work-related illness to your employer. Your benefits could be delayed or denied if you do not notify your employer immediately. If your claim is denied by your employer, you have the right to request a hearing before a workers compensation judge. The Bureau of Workers Compensation cannot provide legal advice; however, you may contact them for additional general information at: Bureau of Workers Compensation 1171 South Cameron Street, Room 103 Harrisburg, Pennsylvania Telephone number within Pennsylvania (800) Telephone number outside of this Commonwealth (717) TTY (800) (for hearing and speech impaired only) PA Keyword: workers comp. ACKNOWLEDGEMENT I,, employee of Premier Employee name (please print) Therapy, hereby certify that I was provided with the above statement on / /. (date) Employee Signature Auxiliary aids and services are available upon request to individuals with disabilities. Equal Opportunity Employer/Program
22 PHYSICAL STATEMENT I have reviewed the following (job description title) job description for. (employee name - please print) I have examined this employee and find him/her to be physically capable of performing all essential functions of the position. Comments: Physician Printed Name: Physician Signature: Street Address: (Date) Employees: This form can be used as an alternative to your physician s standard format, if necessary.
23 Additional Items Needed #1 TB Test Results (Mantoux) #2 Professional Licensure (current) #3 CPR Certification (ONLY if providing Home Health Services) #4 Drivers' License (ONLY if providing Home Health Services) #5 Automobile Insurance Certificate (ONLY if providing Home Health Services) May 1, 2013

24 EMERGENCY CONTACT INFORMATION EMPLOYEE NAME: IN CASE OF AN EMERGENCY, PLEASE CONTACT: PRIMARY CONTACT: NAME: PHONE: ADDRESS: RELATIONSHIP: ALTERNATE CONTACT: NAME: PHONE: ADDRESS: RELATIONSHIP:
25 VOLUNTARY SELF IDENTIFICATION The Equal Employment Opportunity Commission (EEOC) requires organizations with 100 or more employees to complete an EEO 1 report each year. The EEOC has recently announced several changes to the job categories and rearranged its race and ethnicity groupings. Therefore, we are asking employees to complete a new voluntary self identification sheet below so that we can properly update our records according to these new report requirements. Completion of this data is voluntary and will not affect your opportunity for employment or terms or conditions of employment. This form will be used for EEO 1 reporting purposes only and will be kept separate from all other personnel records only accessed by Human Resources Department. Please return completed forms to the Human Resources Department. PLEASE PRINT: Name: Job Title: GENDER: Male Female RACE/ETHNICITY: (Please check one of the descriptions below corresponding to the ethnic group with which you identify.) White (Not Hispanic or Latino) A person having origins in any of the original peoples of Europe, the Middle East or North Africa. Black or African American (Not Hispanic or Latino) A person having origins in any of the black racial groups of Africa. Hispanic or Latino A person of Cuban, Mexican, Puerto Rican, South or Central American, or other Spanish culture or origin regardless of race. Asian (Not Hispanic or Latino) A person having origins in any of the original peoples of the Far East, Southeast Asia or the Indian Subcontinent, including, for example, Cambodia, China, India, Japan, Korea, Malaysia, Pakistan, the Philippine Islands, Thailand and Vietnam. American Indian or Alaska Native (Not Hispanic or Latino) A person having origins in any of the original peoples of North and South America (including Central America) and who maintain tribal affiliation or community attachment. Native Hawaiian or Other Pacific Islander (Not Hispanic or Latino) A person having origins in any of the peoples of Hawaii, Guam, Samoa or other Pacific Islands. Two or More Races (Not Hispanic or Latino) All persons who identify with more than one of the above five races. Date completed: PLEASE RETURN FORM TO HUMAN RESOURCES DEPARTMENT AT Jan. 23, 2012 rev.
26 AUTHORIZATION AGREEMENT FOR AUTOMATIC DIRECT DEPOSITS EFFECTIVE JANUARY 1, 2013 DIRECT DEPOSIT IS MANDATORY FOR ALL EXISTING AND NEW EMPLOYEES IF YOU DON T HAVE A BANK ACCOUNT, A PAY CARD WILL BE ISSUED. YOU MUST COMPLETE A SEPARATE FORM FOR EACH ACCOUNT YOU ARE ADDING OR CHANGING. If this is a new account: 1. The account must be established and active at your bank before you request direct deposit. 2. Confirm the bank accepts direct deposits and verify the transit routing and account numbers. 3. For savings account, you MUST confirm the transit routing number with your bank. 4. Notify the bank that you are going to set up direct deposit though payroll. Please check the appropriate box and complete: Canceling account (Item C below.) Payroll must cancel direct deposit BEFORE you cancel account. Direct deposit already set up, changing dollar amount only (C through E below.) A new account (A though E below.) A new account to replace an existing direct deposit (A through E below.) Account number you are replacing (REQUIRED): A. Bank Name B. Bank Transit Routing Number. C. Bank Account Number. D. Checking Savings E. Full Deposit Partial Deposit (amount per paydate) $ Please fax this completed form along with a voided check for checking, or a deposit slip for savings accounts to 724/ (Payroll Department). Each new account will go through a pre-note process that will take one payroll period. I authorize CTR and the bank listed above to deposit my net pay or portion thereof as indicated into my account each paydate. If funds to which I am not entitled are deposited to my account, I authorize CTR to direct the bank to return said funds to CTR. I understand that my deposit may not be credited to my account until 5:00 PM on the paydate indicated on the check voucher. Employee Name (Print): Employee Signature: Date:
27 Global Cash Card Pay Card Enrollment Form AUTHORIZATION FORM The undersigned, by evidence of their signature below and provision of the necessary information hereby authorizes Premier Therapy to process a pay period ACH transaction (Debit Card) Employee for the express purpose of payroll deposit and services provided by CTR to the Customer. The undersigned, by evidence of their signature below hereby acknowledges that they are authorizing ACH (Debit Card) for payroll deposit. Signature Title Printed name Date If you are enrolling in the Pay Card payroll feature, please complete this form and fax to or mail to: ATTN: Payroll Department Premier Therapy 701 Sharon Road Beaver, PA 15009
Separate here and give Form W-4 to your employer. Keep the top part for your records. Employee s Withholding Allowance Certificate
 Form W-4 (2017) Purpose. Complete Form W-4 so that your employer can withhold the correct federal income tax from your pay. Consider completing a new Form W-4 each year and when your personal or financial
Form W-4 (2017) Purpose. Complete Form W-4 so that your employer can withhold the correct federal income tax from your pay. Consider completing a new Form W-4 each year and when your personal or financial
Separate here and give Form W-4 to your employer. Keep the top part for your records. Employee s Withholding Allowance Certificate
 Form W-4 (2017) Purpose. Complete Form W-4 so that your employer can withhold the correct federal income tax from your pay. Consider completing a new Form W-4 each year and when your personal or financial
Form W-4 (2017) Purpose. Complete Form W-4 so that your employer can withhold the correct federal income tax from your pay. Consider completing a new Form W-4 each year and when your personal or financial
XXXXXX NON-UNION VOUCHER. White - Payroll Company Yellow - Accounting Department Pink - Employee TIME CLOCK RATE ALLOWANCES SPECIAL COMPENSATIONS
 XXXXXX NON-UNION VOUCHER DATE PRODUCTION & PROJECT NAME 1 2 3 LAST NAME FIRST NAME MI STREET ADDRESS CITY STATE ZIP DATE OF BIRTH: IF MINOR PHONE IF NEW IF NEW EMPLOYEE ADDRESS SOCIAL SECURITY NUMBER WORK
XXXXXX NON-UNION VOUCHER DATE PRODUCTION & PROJECT NAME 1 2 3 LAST NAME FIRST NAME MI STREET ADDRESS CITY STATE ZIP DATE OF BIRTH: IF MINOR PHONE IF NEW IF NEW EMPLOYEE ADDRESS SOCIAL SECURITY NUMBER WORK
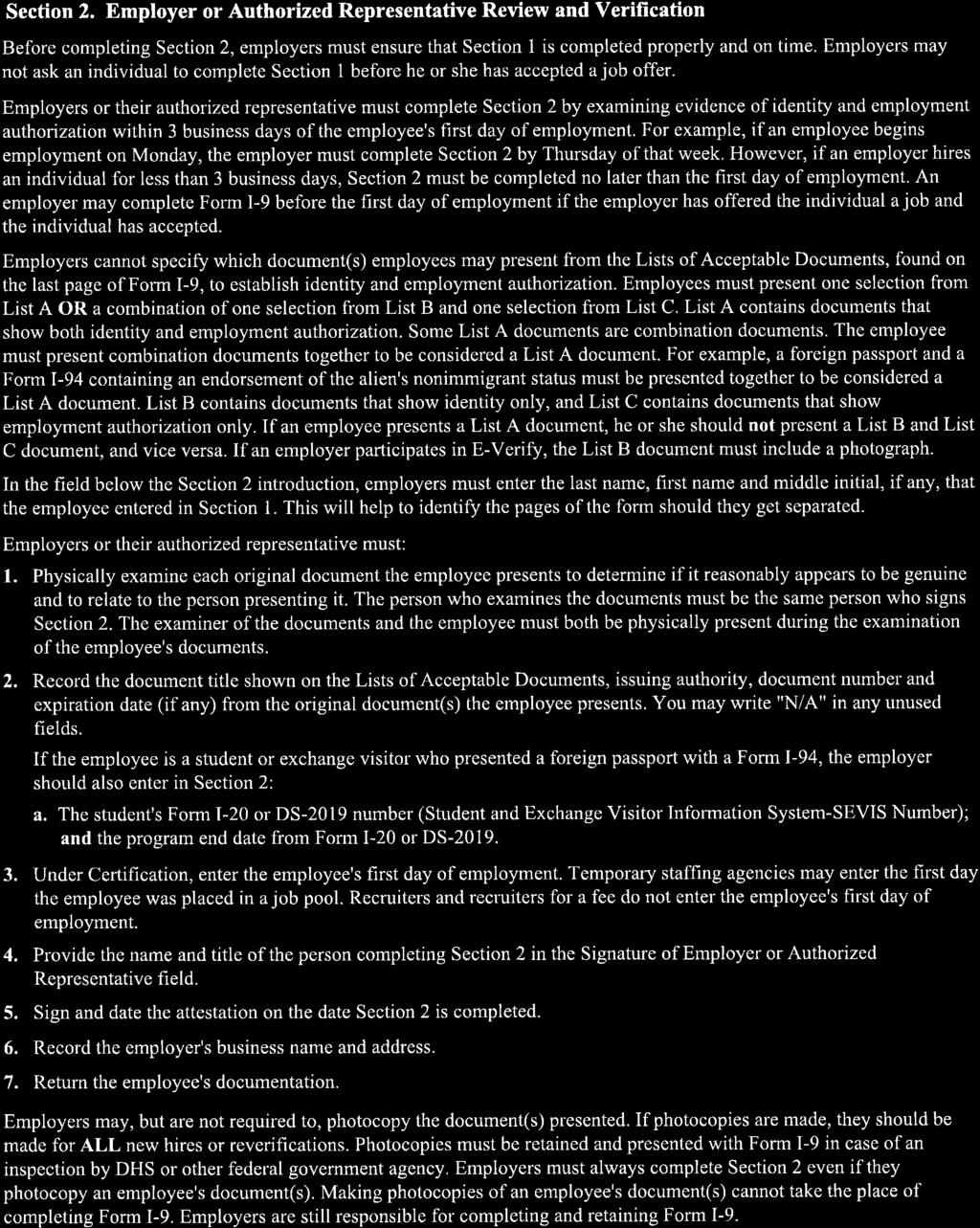
Employment Eligibility Verification
 Employment Eligibility Verification Department of Homeland Security U.S. Citizenship and Immigration Services USCIS Form I-9 OMB No. 1615-0047 Expires 08/31/2019 START HERE: Read instructions carefully
Employment Eligibility Verification Department of Homeland Security U.S. Citizenship and Immigration Services USCIS Form I-9 OMB No. 1615-0047 Expires 08/31/2019 START HERE: Read instructions carefully
Separate here and give Form W-4 to your employer. Keep the top part for your records. Employee s Withholding Allowance Certificate
 Form W-4 (2017) Purpose. Complete Form W-4 so that your employer can withhold the correct federal income tax from your pay. Consider completing a new Form W-4 each year and when your personal or financial
Form W-4 (2017) Purpose. Complete Form W-4 so that your employer can withhold the correct federal income tax from your pay. Consider completing a new Form W-4 each year and when your personal or financial
Missouri Department of Revenue Employee s Withholding Allowance Certificate
 Form MO W-4 Missouri Department of Revenue Employee s Withholding Allowance Certificate This certificate is for income tax withholding and child support enforcement purposes only. Type or print. Full Name
Form MO W-4 Missouri Department of Revenue Employee s Withholding Allowance Certificate This certificate is for income tax withholding and child support enforcement purposes only. Type or print. Full Name
Please complete and sign all forms in the PRE-EMPLOYMENT FORMS section.
 NATIONAL HOME HEALTH SERVICES EMPLOYMENT FORMS 5811 Dempster St Morton Grove, IL 60053 Phone: (847) 329-9933 Fax: (847) 930-0375 APPLICANT NAME POSITION APPLYING FOR DATE Please complete and sign all forms
NATIONAL HOME HEALTH SERVICES EMPLOYMENT FORMS 5811 Dempster St Morton Grove, IL 60053 Phone: (847) 329-9933 Fax: (847) 930-0375 APPLICANT NAME POSITION APPLYING FOR DATE Please complete and sign all forms
A - EMPLOYEE INFORMATION SUBMISSION AND CERTIFICATION
 Office/Client Number New Employee Packet Employer Information: Choose your option for submitting employee information. For detailed instructions for these options, refer to the PEO New Employee Packet
Office/Client Number New Employee Packet Employer Information: Choose your option for submitting employee information. For detailed instructions for these options, refer to the PEO New Employee Packet
New Employee Welcome Letter and Orientation Checklist
 Lafayette DQ Restaurants P.O. Box 302 Delphi, IN 46923 Phone: (765) 447-1089 Fax: (765) 535-5001 New Employee Welcome Letter and Orientation Checklist Welcome to the DQ family! In order to start training
Lafayette DQ Restaurants P.O. Box 302 Delphi, IN 46923 Phone: (765) 447-1089 Fax: (765) 535-5001 New Employee Welcome Letter and Orientation Checklist Welcome to the DQ family! In order to start training
EMPLOYEE INFORMATION SHEET
 EMPLOYEE INFORMATION SHEET PLEASE PRINT CLEARLY COMPANY: EMPLOYEE #: SOCIAL SECURITY NUMBER: - - NAME: First MI LAST STREET: CITY: AS APPEARS ON SOCIAL SECURITY CARD STATE: ZIP CODE: TELEPHONE NUMBER:
EMPLOYEE INFORMATION SHEET PLEASE PRINT CLEARLY COMPANY: EMPLOYEE #: SOCIAL SECURITY NUMBER: - - NAME: First MI LAST STREET: CITY: AS APPEARS ON SOCIAL SECURITY CARD STATE: ZIP CODE: TELEPHONE NUMBER:
Last Name First Name Middle Initial ADDRESS Street City County State Zip
 APPLICATION FOR EMPLOYMENT Kolberg-Pioneer, Inc. An Equal Opportunity Employer (HRF-002-03 01/16) This application is valid for the calendar year of 2018. Kolberg-Pioneer, Inc. will provide the Social
APPLICATION FOR EMPLOYMENT Kolberg-Pioneer, Inc. An Equal Opportunity Employer (HRF-002-03 01/16) This application is valid for the calendar year of 2018. Kolberg-Pioneer, Inc. will provide the Social
Employee Data Form. [ ] ] ] [ ] ] [ ] _] _]_ ] Home Address Apt City State Zip Code County. Ethnicity: Are you Hispanic/Latino?
![Employee Data Form. [ ] ] ] [ ] ] [ ] _] _]_ ] Home Address Apt City State Zip Code County. Ethnicity: Are you Hispanic/Latino?](/thumbs/79/79502522.jpg "Employee Data Form. [ ] ] ] [ ] ] [ ] _] _]_ ] Home Address Apt City State Zip Code County. Ethnicity: Are you Hispanic/Latino?") Employee Data Form Baltimore City Public Schools Office Of Human Capital 200 E. North Avenue, Room 110 Baltimore, Maryland 21202 www. s New /Rehire employees are required to complete this form as part
Employee Data Form Baltimore City Public Schools Office Of Human Capital 200 E. North Avenue, Room 110 Baltimore, Maryland 21202 www. s New /Rehire employees are required to complete this form as part
EMPLOYER INFORMATION SHEET
 General EMPLOYER INFORMATION SHEET Business Name: Business Address: City, State, Zip: Filing Name (if different): Filing Address (if different): City, State, Zip: Contact Name: Phone: Fax: Email: Company
General EMPLOYER INFORMATION SHEET Business Name: Business Address: City, State, Zip: Filing Name (if different): Filing Address (if different): City, State, Zip: Contact Name: Phone: Fax: Email: Company
Application for Employment
 Position Sought: Community Transit of Delaware County, Inc. 206 Eddystone Avenue Suite 200 Eddystone, PA 19022-1594 Application for Employment Date: (Last) (First) (Middle Name) (Street Address) (City)
Position Sought: Community Transit of Delaware County, Inc. 206 Eddystone Avenue Suite 200 Eddystone, PA 19022-1594 Application for Employment Date: (Last) (First) (Middle Name) (Street Address) (City)
New Employment & Sign-up Checklist for Managers and Departmental Representatives
 FLORIDA A&M UNIVERSITY New Employment & Sign-up Checklist for Managers and Departmental Representatives Executive Service A&P USPS OPS Faculty (Please complete Section II Only) Employee Name: Class Title:
FLORIDA A&M UNIVERSITY New Employment & Sign-up Checklist for Managers and Departmental Representatives Executive Service A&P USPS OPS Faculty (Please complete Section II Only) Employee Name: Class Title:
YOU DO NOT NEED TO PRINT THIS PAGE. Substitute Records Requirements. Social Security Card (copies not accepted)
") YOU DO NOT NEED TO PRINT THIS PAGE. Appointment Date & Time: Name: Date: Substitute Records Requirements I-9 (only complete page 1) W-4 Social Security Card (copies not accepted) Driver s License Direct
YOU DO NOT NEED TO PRINT THIS PAGE. Appointment Date & Time: Name: Date: Substitute Records Requirements I-9 (only complete page 1) W-4 Social Security Card (copies not accepted) Driver s License Direct
Western States Office and Professional Employees Pension Fund
 Western States Office and Professional Employees Pension Fund FEDERAL INCOME TAX WITHHOLDING TAX WITHHOLDING ELECTION Please complete the attached W-4P Withholding Certificate for Pension or Annuity Payments.
Western States Office and Professional Employees Pension Fund FEDERAL INCOME TAX WITHHOLDING TAX WITHHOLDING ELECTION Please complete the attached W-4P Withholding Certificate for Pension or Annuity Payments.
Employment Application
 P.O. Box 643 Benavides, Tx 78341 (361) 256-4726 Office (361) 256-4728 Fax Scorp1144@yahoo.com Scorpion Exploration & Production, Inc. Full Name Mailing Address Employment Application Applicant Information
P.O. Box 643 Benavides, Tx 78341 (361) 256-4726 Office (361) 256-4728 Fax Scorp1144@yahoo.com Scorpion Exploration & Production, Inc. Full Name Mailing Address Employment Application Applicant Information
Villanova University New Employee Personal Information Form
 Villanova University New Employee Personal Infmation Fm Employee Name (as it appears on your social security card): Department: of Birth: Gender: US Citizen? If no, Visa status/permanent resident #: of
Villanova University New Employee Personal Infmation Fm Employee Name (as it appears on your social security card): Department: of Birth: Gender: US Citizen? If no, Visa status/permanent resident #: of
DIVERSIFIED Edgewood Road, NE Cedar Rapids, IA
 DIVERSIFIED --------------------- 4443 Edgewood Road, NE Cedar Rapids, IA 52499 800-755-5801 www.divinvest.com Federal Tax Withholding Election Form Instructions To change your federal income tax withholding,
DIVERSIFIED --------------------- 4443 Edgewood Road, NE Cedar Rapids, IA 52499 800-755-5801 www.divinvest.com Federal Tax Withholding Election Form Instructions To change your federal income tax withholding,
Separate here and give Form W-4 to your employer. Keep the top part for your records. Employee's Withholding Allowance Certificate
 Form W-4 (2015) Purpose. Complete Form W-4 so that your employer can withhold the correct federal income tax from your pay. Consider completing a new Form W-4 each year and when your personal or financial
Form W-4 (2015) Purpose. Complete Form W-4 so that your employer can withhold the correct federal income tax from your pay. Consider completing a new Form W-4 each year and when your personal or financial
Decatur County Schools
 Decatur County Schools 100 West Street Bainbridge, Georgia 39817 (229) 248-2200 Fax (229) 248-2252 This application will remain active for one year from date received unless requested to reactivate after
Decatur County Schools 100 West Street Bainbridge, Georgia 39817 (229) 248-2200 Fax (229) 248-2252 This application will remain active for one year from date received unless requested to reactivate after
State Employees Credit Union Application for Employment
 State Employees Credit Union Application for Employment Note: Application must be handwritten. Do not type. We appreciate your interest in our organization. Please complete the application as fully as
State Employees Credit Union Application for Employment Note: Application must be handwritten. Do not type. We appreciate your interest in our organization. Please complete the application as fully as
Employment Application
 Employment Application To Applicant Instructions We appreciate your interest in our company and we are interested in reviewing your qualifications for our current open positions. To make this the best
Employment Application To Applicant Instructions We appreciate your interest in our company and we are interested in reviewing your qualifications for our current open positions. To make this the best
SURRENDER REQUEST FORM. Policy Number: Insured:
 SURRENDER REQUEST FORM Section A Policy Information (You Must Complete This Section) Policy Number: Insured: (First Name) (Last Name) Sec tion B Surrender Request and Withholding Election (You Must Complete
SURRENDER REQUEST FORM Section A Policy Information (You Must Complete This Section) Policy Number: Insured: (First Name) (Last Name) Sec tion B Surrender Request and Withholding Election (You Must Complete
We (The Jeffrey Corporation) are making you a contingent job offer to work at Burger King Store #.
 are making you a contingent job offer to work at Burger King Store #.") Date Dear Applicant, We (The Jeffrey Corporation) are making you a contingent job offer to work at Burger King Store #. Part of the hiring/re-hiring process requires that we verify your eligibility to
Date Dear Applicant, We (The Jeffrey Corporation) are making you a contingent job offer to work at Burger King Store #. Part of the hiring/re-hiring process requires that we verify your eligibility to
CITY OF CALISTOGA DOWN PAYMENT ASSISTANCE PROGRAM LOAN APPLICATION
 DOWN PAYMENT ASSISTANCE PROGRAM LOAN APPLICATION Date Applicant s Name Phone Residence Address Home City, State, Zip Code Phone Mailing Address (If different) FAMILY INFORMATION Applicant or Co-Applicant
DOWN PAYMENT ASSISTANCE PROGRAM LOAN APPLICATION Date Applicant s Name Phone Residence Address Home City, State, Zip Code Phone Mailing Address (If different) FAMILY INFORMATION Applicant or Co-Applicant
To determine your eligibility for the program, the following documentation must be completed and submitted:
 Dear Applicant, As a participating jurisdiction in the St. Charles Urban County, the City of St. Peters will administer a St. Peters Urban County Home Improvement Loan Program (H.I.L.P) once federal funding
Dear Applicant, As a participating jurisdiction in the St. Charles Urban County, the City of St. Peters will administer a St. Peters Urban County Home Improvement Loan Program (H.I.L.P) once federal funding
EMPLOYER WITH EMPLOYEES - PAYROLL INTAKE FORM
 EMPLOYER WITH EMPLOYEES - PAYROLL INTAKE FORM CONTACT INFORMATION Payroll Client (First, Last): Phone #: ( ) - Legal Business Name: Business DBA (If Applicable): Business Type: LLC Partnership Corp S-Corp
EMPLOYER WITH EMPLOYEES - PAYROLL INTAKE FORM CONTACT INFORMATION Payroll Client (First, Last): Phone #: ( ) - Legal Business Name: Business DBA (If Applicable): Business Type: LLC Partnership Corp S-Corp
Preliminary Rental Application
 OP 241 For Office Use Only Rec d Time Rec d Initials Preliminary Rental Application Please note that this is a preliminary application and gives no lease or rent rights. Community Office ( ) Unit Size
OP 241 For Office Use Only Rec d Time Rec d Initials Preliminary Rental Application Please note that this is a preliminary application and gives no lease or rent rights. Community Office ( ) Unit Size
INSTRUCTIONS FOR PAPERWORK ALL FORMS MUST BE SIGNED AND DATED PLEASE PRINT ONE-SIDED SHEETS
 INSTRUCTIONS FOR PAPERWORK ALL FORMS MUST BE SIGNED AND DATED PLEASE PRINT ONE-SIDED SHEETS CFISD EMPLOYEE INFORMATION SHEET Must be LEGIBLE Fill in all blanks You MUST bubble an answer for Part 1-Ethnicity
INSTRUCTIONS FOR PAPERWORK ALL FORMS MUST BE SIGNED AND DATED PLEASE PRINT ONE-SIDED SHEETS CFISD EMPLOYEE INFORMATION SHEET Must be LEGIBLE Fill in all blanks You MUST bubble an answer for Part 1-Ethnicity
Personal Information: *Please complete all information. Use ink and print clearly, so we can get to know you! Last Name:
 In order to be hired, you must be willing to submit to a physical and urinalysis screening. Application is valid for thirty (30) days from Date Received Today s Date: Bausch-American Towers Attn: HR Manager,
In order to be hired, you must be willing to submit to a physical and urinalysis screening. Application is valid for thirty (30) days from Date Received Today s Date: Bausch-American Towers Attn: HR Manager,
Employment Eligibility Verification
 Employment Eligibility Verification Department of Homeland Security U.S. Citizenship and Immigration Services USCIS Form I-9 OMB No. 1615-0047 Expires 08/31/2019 START HERE: Read instructions carefully
Employment Eligibility Verification Department of Homeland Security U.S. Citizenship and Immigration Services USCIS Form I-9 OMB No. 1615-0047 Expires 08/31/2019 START HERE: Read instructions carefully
MASSACHUSETTS WATER RESOURCES AUTHORITY Employment Application
 MASSACHUSETTS WATER RESOURCES AUTHORITY Employment Application Massachusetts Water Resources Authority is an Equal Opportunity/Affirmative Action Employer. MWRA does not discriminate on the basis of race,
MASSACHUSETTS WATER RESOURCES AUTHORITY Employment Application Massachusetts Water Resources Authority is an Equal Opportunity/Affirmative Action Employer. MWRA does not discriminate on the basis of race,
Mobiloil Federal Credit Union Employment Application
 Mobiloil Federal Credit Union Employment Application It is our policy to provide equal employment opportunity to all qualified persons without regard to race, creed, color, religious belief, sex, age,
Mobiloil Federal Credit Union Employment Application It is our policy to provide equal employment opportunity to all qualified persons without regard to race, creed, color, religious belief, sex, age,
WAITLIST APPLICATION CHECK LIST
 3550 VILLA LANE NAPA, CALIFORNIA 94558-3436 (707) 251-8077 WAITLIST APPLICATION CHECK LIST Thank you for your interest in Silverado Creek rental housing. For your convenience we ve summarized below the
3550 VILLA LANE NAPA, CALIFORNIA 94558-3436 (707) 251-8077 WAITLIST APPLICATION CHECK LIST Thank you for your interest in Silverado Creek rental housing. For your convenience we ve summarized below the
Southeast ID#: Name: SSN: PREVIOUS CIVIL OR COLLEGE DISCIPLINE
 /Student Employment Work Referral Southeast ID#: Name: SSN: STUDENT EMPLOYEE ELIGIBILITY AND RESPONSIBILITIES 1. You must complete, and have on file with Student Financial Services, employment eligibility
/Student Employment Work Referral Southeast ID#: Name: SSN: STUDENT EMPLOYEE ELIGIBILITY AND RESPONSIBILITIES 1. You must complete, and have on file with Student Financial Services, employment eligibility
Exact title of the position for which you are applying. Applications will only be processed for current vacancy. (Last) (First) (Middle)
 (First) (Middle)") EFFINGHAM COUNTY BOARD OF COMMISSIONERS Employment Application 601 North Laurel Street Springfield, Georgia 31329 hr@effinghamcounty.org Telephone: 912-754-2104 Fax: 912-754-8402 We are an equal opportunity/drug
EFFINGHAM COUNTY BOARD OF COMMISSIONERS Employment Application 601 North Laurel Street Springfield, Georgia 31329 hr@effinghamcounty.org Telephone: 912-754-2104 Fax: 912-754-8402 We are an equal opportunity/drug
What s In My Paycheck? compensation package: all of the wages (salary, bonus, commission) and benefits provided by an employer. What s In My Paycheck?
 and benefits provided by an employer. What s In My Paycheck?") compensation package: all of the wages (salary, bonus, commission) and benefits provided by an employer wages: money paid or received for work or services completed, usually by the hour, day, or week hourly
compensation package: all of the wages (salary, bonus, commission) and benefits provided by an employer wages: money paid or received for work or services completed, usually by the hour, day, or week hourly
Employment Application
 Print Name (First, ( M., Last): Employment Application PERSONAL INFORMATION Date: Street Address: Apt. Unit/# Home Phone: City State Zip Cell Phone: Email Address: Are you authorized to work in the U.S.?
Print Name (First, ( M., Last): Employment Application PERSONAL INFORMATION Date: Street Address: Apt. Unit/# Home Phone: City State Zip Cell Phone: Email Address: Are you authorized to work in the U.S.?
NO CONFLICT ATTESTATION. In order to qualify to act as the Personal Assistant for this Consumer, I attest to the ALL of following:
 NO CONFLICT ATTESTATION In order to qualify to act as the Personal Assistant for this Consumer, I attest to the ALL of following: 1. I am NOT the Consumer s Designated Representative. 2. The Consumer is
NO CONFLICT ATTESTATION In order to qualify to act as the Personal Assistant for this Consumer, I attest to the ALL of following: 1. I am NOT the Consumer s Designated Representative. 2. The Consumer is
Student Employee New Hire Packet
 Student Employee New Hire Packet New Hire Checklist: o Authorization to Hire Form o Student Application o Federal W-4 Form o NJ State W-4 Form o I-9 Form o Social Security Card (for Payroll purposes) o
Student Employee New Hire Packet New Hire Checklist: o Authorization to Hire Form o Student Application o Federal W-4 Form o NJ State W-4 Form o I-9 Form o Social Security Card (for Payroll purposes) o
SPORT CLIPS PAYROLL INFORMATION FORM CLIENT NAME: TO BE COMPLETED BY EMPLOYEE: Employee Name: Employee
 SPORT CLIPS PAYROLL INFORMATION FORM CLIENT NAME: TO BE COMPLETED BY EMPLOYEE: Employee Name: Employee Email: Local Tax (IF APPLICABLE): SSN: City or County Township or Borough School District PA EMST:
SPORT CLIPS PAYROLL INFORMATION FORM CLIENT NAME: TO BE COMPLETED BY EMPLOYEE: Employee Name: Employee Email: Local Tax (IF APPLICABLE): SSN: City or County Township or Borough School District PA EMST:
Employment Application Fire & Rescue Department
 Village of Pleasant Prairie 9915 39 th Avenue Pleasant Prairie, WI 53158 (262) 925-6731 Fax (262) 925-6788 Town of Salem 8339 Antioch Road Salem, WI 53168 (262) 298-5630 Fax (262) 298-5649 Employment Application
Village of Pleasant Prairie 9915 39 th Avenue Pleasant Prairie, WI 53158 (262) 925-6731 Fax (262) 925-6788 Town of Salem 8339 Antioch Road Salem, WI 53168 (262) 298-5630 Fax (262) 298-5649 Employment Application
Voluntary Information for Equal Employment Opportunity Purposes
 Voluntary Information for Equal Employment Opportunity Purposes Below is a Voluntary Information Sheet that we would like you to complete. It will be used for Equal Opportunity purposes only. The requested
Voluntary Information for Equal Employment Opportunity Purposes Below is a Voluntary Information Sheet that we would like you to complete. It will be used for Equal Opportunity purposes only. The requested
New Employee Information
 HOUSTON S PREMIER POKER DESTINATION New Employee Information Before you will be scheduled the following MUST be completed: 1. Your new hire packet must be filled out completely and correctly and handed
HOUSTON S PREMIER POKER DESTINATION New Employee Information Before you will be scheduled the following MUST be completed: 1. Your new hire packet must be filled out completely and correctly and handed
MedStart-5. Application for Assistance
 MedStart-5 Application for Assistance Transportation Meals Assistance Utilities Co-Payments Adult Home Care Lab Testing For application help, contact us at 1-888-842-2654 To apply for benefits, follow
MedStart-5 Application for Assistance Transportation Meals Assistance Utilities Co-Payments Adult Home Care Lab Testing For application help, contact us at 1-888-842-2654 To apply for benefits, follow
Ohio Civil Service Application forstateandcountyagencies
 Ohio Civil Service Application forstateandcountyagencies GEN-4268 (REVISED 01/12) 06/08) ThestateofOhioisanEqualOpportunityEmployerandproviderofADAservices. State is an Opportunity Employer and provider
Ohio Civil Service Application forstateandcountyagencies GEN-4268 (REVISED 01/12) 06/08) ThestateofOhioisanEqualOpportunityEmployerandproviderofADAservices. State is an Opportunity Employer and provider
Hardee County Board of County Commissioners Equal Employment Opportunity (EEO) Self-Identification Form (completion of this form is voluntary)
 Self-Identification Form (completion of this form is voluntary)") Please submit to: Hardee County Board of County Commissioners HR Department 205 Hanchey Road, Wauchula, Florida 33873 Phone: (863) 773-2161 Hardee County Board of County Commissioners Equal Employment
Please submit to: Hardee County Board of County Commissioners HR Department 205 Hanchey Road, Wauchula, Florida 33873 Phone: (863) 773-2161 Hardee County Board of County Commissioners Equal Employment
Warrick County School Corporation
 Warrick County School Corporation SUPERINTENDENT S OFFICE P.O. Box 809/Boonville, Indiana 47601/812-897-0400 Welcome to the Warrick County School Corporation Welcome to the one of the best school corporations
Warrick County School Corporation SUPERINTENDENT S OFFICE P.O. Box 809/Boonville, Indiana 47601/812-897-0400 Welcome to the Warrick County School Corporation Welcome to the one of the best school corporations
ESKATON HAZEL SHIRLEY MANOR San Pablo Avenue, El Cerrito, CA PH: (510) FAX: (510) TDD: (800)
 FAX: (510) TDD: (800)") RCVD BY DATE TIME ESKATON HAZEL SHIRLEY MANOR 11025 San Pablo Avenue, El Cerrito, CA 94530 PH: (510) 232-3430 FAX: (510) 232-1056 TDD: (800) 735-2922 www.eskaton.org APPLICATION FOR HOUSING PLEASE PRINT
RCVD BY DATE TIME ESKATON HAZEL SHIRLEY MANOR 11025 San Pablo Avenue, El Cerrito, CA 94530 PH: (510) 232-3430 FAX: (510) 232-1056 TDD: (800) 735-2922 www.eskaton.org APPLICATION FOR HOUSING PLEASE PRINT
 Form W-4 (2018) Future developments. For the latest information about any future developments related to Form W-4, such as legislation enacted after it was published, go to www.irs.gov/formw4. Purpose.
Form W-4 (2018) Future developments. For the latest information about any future developments related to Form W-4, such as legislation enacted after it was published, go to www.irs.gov/formw4. Purpose.
BACKGROUND CLEARANCE INSTRUCTIONS STUDENT APPLICANT
 BACKGROUND CLEARANCE INSTRUCTIONS STUDENT APPLICANT The amended Child Protective Services Law, effective December 31, 2014, and accompanying policies; PASSHE Board of Governors 2014-01-A (Protection of
BACKGROUND CLEARANCE INSTRUCTIONS STUDENT APPLICANT The amended Child Protective Services Law, effective December 31, 2014, and accompanying policies; PASSHE Board of Governors 2014-01-A (Protection of
FORMS TO BE COMPLETED AND SUBMITTED TO HUMAN RESOURCES. The College requires all Employees complete and submit the following documents:
 FORMS TO BE COMPLETED AND SUBMITTED TO HUMAN RESOURCES The College requires all Employees complete and submit the following documents: 1. I-9 Employment Eligibility Verification: Complete the I-9 Form
FORMS TO BE COMPLETED AND SUBMITTED TO HUMAN RESOURCES The College requires all Employees complete and submit the following documents: 1. I-9 Employment Eligibility Verification: Complete the I-9 Form
How Do I Adjust My Tax Withholding?
 Contents Department of the Treasury Internal Revenue Service What s New for 2011... 2 Reminder.... Publication 919 Introduction... 3 Cat. No. 63900P How Do I Adjust My Tax Withholding? Checking Your Withholding...
Contents Department of the Treasury Internal Revenue Service What s New for 2011... 2 Reminder.... Publication 919 Introduction... 3 Cat. No. 63900P How Do I Adjust My Tax Withholding? Checking Your Withholding...
Last Name First Name Middle Name. Street Address City State Zip Code
 EMPLOYMENT APPLICATION Clean All Services is an equal opportunity employer and affords equal opportunity to all applicants for all positions without regard to race, color, religion, gender, national origin,
EMPLOYMENT APPLICATION Clean All Services is an equal opportunity employer and affords equal opportunity to all applicants for all positions without regard to race, color, religion, gender, national origin,
Small Business Enterprise Program
 Small Business Enterprise Program Registration & Roster Enrollment Registration Does NOT Pre-Approve You (The City may use this information to develop bid lists, contract lists and reports. Prime contractors
Small Business Enterprise Program Registration & Roster Enrollment Registration Does NOT Pre-Approve You (The City may use this information to develop bid lists, contract lists and reports. Prime contractors
APPLICATION FOR EMPLOYMENT
 Community Values, Local Choices AN EQUAL OPPORTUNITY EMPLOYER APPLICATION FOR EMPLOYMENT Applicant: We appreciate your interest in C&K Market, Inc. (C&K). A clear understanding of your background and work
Community Values, Local Choices AN EQUAL OPPORTUNITY EMPLOYER APPLICATION FOR EMPLOYMENT Applicant: We appreciate your interest in C&K Market, Inc. (C&K). A clear understanding of your background and work
RAYMOND CENTRAL PUBLIC SCHOOLS SUBSTITUTE TEACHER DATA SHEET
 RAYMOND CENTRAL PUBLIC SCHOOLS SUBSTITUTE TEACHER DATA SHEET PLEASE NOTE: We need a voided check for payment by Direct Deposit and we must have an email address. Thank you. W-4 Form I-9 Form - 2 forms
RAYMOND CENTRAL PUBLIC SCHOOLS SUBSTITUTE TEACHER DATA SHEET PLEASE NOTE: We need a voided check for payment by Direct Deposit and we must have an email address. Thank you. W-4 Form I-9 Form - 2 forms
APPLICATION FOR EMPLOYMENT
 APPLICATION FOR EMPLOYMENT EDWARDS, Inc. EDWARDS/Greenville, Inc EDWARDS/Wilmington, Inc Employment Desired: Position Desired: This Company Is An Equal Opportunity Employer This company is subject to E-Verify
APPLICATION FOR EMPLOYMENT EDWARDS, Inc. EDWARDS/Greenville, Inc EDWARDS/Wilmington, Inc Employment Desired: Position Desired: This Company Is An Equal Opportunity Employer This company is subject to E-Verify
2019 English Applica on
 2019 English Applica on (Please Print) Date: First Name Last Name Social Security Address Apt. City State Zip Code Home Phone Cell Phone E-Mail Please place a check by your response or provide the appropriate
2019 English Applica on (Please Print) Date: First Name Last Name Social Security Address Apt. City State Zip Code Home Phone Cell Phone E-Mail Please place a check by your response or provide the appropriate
COMMUNITY: PROGRAM: ORIGINAL DATE: TIME: UPDATE: TIME:
 SUBJECT: APPLICANT FOR RESIDENCY TAX CREDIT COMMUNITIES COMMUNITY: PROGRAM: ORIGINAL DATE: TIME: UPDATE: TIME: HOW DID YOU HEAR ABOUT US? APARTMENT SIZE: APPLICANT NAME (FIRST, MIDDLE, LAST): CURRENT ADDRESS:
SUBJECT: APPLICANT FOR RESIDENCY TAX CREDIT COMMUNITIES COMMUNITY: PROGRAM: ORIGINAL DATE: TIME: UPDATE: TIME: HOW DID YOU HEAR ABOUT US? APARTMENT SIZE: APPLICANT NAME (FIRST, MIDDLE, LAST): CURRENT ADDRESS:
APPLICATION FOR EMPLOYMENT
 APPLICATION FOR EMPLOYMENT Morgan-Keller is an equal opportunity employer and does not discriminate on the basis of race, religion, color, national origin, age, sex, gender, disability or any other characteristic
APPLICATION FOR EMPLOYMENT Morgan-Keller is an equal opportunity employer and does not discriminate on the basis of race, religion, color, national origin, age, sex, gender, disability or any other characteristic
To become an Amador Rides Volunteer Driver, you must provide:
 Become an Volunteer Driver! Amador Rides is a collaborative effort from several organizations who want to make sure that Amador County residents can get to their medical, dental, and mental health appointments.
Become an Volunteer Driver! Amador Rides is a collaborative effort from several organizations who want to make sure that Amador County residents can get to their medical, dental, and mental health appointments.
CAREFULLY READ AND FOLLOW INSTRUCTIONS
 PLAINFIELD BOARD OF EDUCATION 1200 Myrtle Avenue Plainfield, NJ 07060 SUBSTITUTE BUS DRIVER CHECK LIST Name: Social Security Number: CAREFULLY READ AND FOLLOW INSTRUCTIONS 1. Go to the State's Website
PLAINFIELD BOARD OF EDUCATION 1200 Myrtle Avenue Plainfield, NJ 07060 SUBSTITUTE BUS DRIVER CHECK LIST Name: Social Security Number: CAREFULLY READ AND FOLLOW INSTRUCTIONS 1. Go to the State's Website
1. PLEASE READ CAREFULLY Applications will be processed in order of date and time received.
 Dear Applicant: Thank you for applying for tenancy at W a t e r s E d g e C r e s c e n t 1 located in Elizabeth, New Jersey 07206. Please complete this application in accordance with the following application
Dear Applicant: Thank you for applying for tenancy at W a t e r s E d g e C r e s c e n t 1 located in Elizabeth, New Jersey 07206. Please complete this application in accordance with the following application
Separate here and give Form W-4 to your employer. Keep the worksheet(s) for your records. Employee s Withholding Allowance Certificate
 for your records. Employee s Withholding Allowance Certificate") Form W-4 (2018) Future developments. For the latest information about any future developments related to Form W-4, such as legislation enacted after it was published, go to www.irs.gov/formw4. Purpose.
Form W-4 (2018) Future developments. For the latest information about any future developments related to Form W-4, such as legislation enacted after it was published, go to www.irs.gov/formw4. Purpose.
Laclede Electric Cooperative Application For Employment
 Laclede Electric Cooperative Application For Employment It is the policy of Laclede Electric Cooperative (LEC) to provide equal opportunity with regard to all terms and conditions of employment. No information
Laclede Electric Cooperative Application For Employment It is the policy of Laclede Electric Cooperative (LEC) to provide equal opportunity with regard to all terms and conditions of employment. No information
NAME (FIRST) (MIDDLE) (LAST) SOCIAL SECURITY NO. (OPTIONAL) DATE OF APPLICATION
 (MIDDLE) (LAST) SOCIAL SECURITY NO. (OPTIONAL) DATE OF APPLICATION") Bristol Bay Area Health Corporation P.O. Box 130 Dillingham, Alaska 99576 Phone: 1-907-842-5201 --- In Alaska: 1-800-478-5201 Fax: 1-907-842-9251 --- Email: recruitment@bbahc.org BBAHC enforces a drug
Bristol Bay Area Health Corporation P.O. Box 130 Dillingham, Alaska 99576 Phone: 1-907-842-5201 --- In Alaska: 1-800-478-5201 Fax: 1-907-842-9251 --- Email: recruitment@bbahc.org BBAHC enforces a drug
Volunteer Driver Application
 Volunteer Driver Application PLEASE PRINT This application will be used to establish your eligibility as a volunteer driver for the Drive to Help program. The information you provide helps us assure you,
Volunteer Driver Application PLEASE PRINT This application will be used to establish your eligibility as a volunteer driver for the Drive to Help program. The information you provide helps us assure you,
State of Connecticut Department of Social Services Application for Medicare Savings Programs (QMB, SLMB, ALMB)
") State of Connecticut Department of Social Services Application for Medicare Savings Programs (QMB, SLMB, ALMB) W-1QMB (Rev 8/16) Use this form to apply for Medicare Savings Program benefits. If you currently
State of Connecticut Department of Social Services Application for Medicare Savings Programs (QMB, SLMB, ALMB) W-1QMB (Rev 8/16) Use this form to apply for Medicare Savings Program benefits. If you currently
AN EQUAL OPPORTUNITY EMPLOYER DATE SOCIAL SECURITY NUMBER CITY CITY IN CASE OF EMERGENCY NOTIFY: NAME RELATIONSHIP TELEPHONE NUMBER ( ) YES NO
 YES NO") Please fill out the application in its entirety FIRST MIDDLE LAST AN EQUAL OPPORTUNITY EMPLOYER DATE SOCIAL SECURITY NUMBER 20 PRESENT STREET CITY STATE ZIP PERSONAL PERMANENT TELEPHONE NUMBER HOME STREET
Please fill out the application in its entirety FIRST MIDDLE LAST AN EQUAL OPPORTUNITY EMPLOYER DATE SOCIAL SECURITY NUMBER 20 PRESENT STREET CITY STATE ZIP PERSONAL PERMANENT TELEPHONE NUMBER HOME STREET
APPLICATION CHECKLIST
 PERF/TRF RETIREMENT APPLICATION State Form 945 (R30 / 2-15) Approved by State Board of Accounts, 2015 INDIANA PUBLIC RETIREMENT SYSTEM Telephone: (888) 286-3544 (Toll-free) Web site: www.inprs.in.gov Use
PERF/TRF RETIREMENT APPLICATION State Form 945 (R30 / 2-15) Approved by State Board of Accounts, 2015 INDIANA PUBLIC RETIREMENT SYSTEM Telephone: (888) 286-3544 (Toll-free) Web site: www.inprs.in.gov Use
WELCOME TO TORRANCE MEMORIAL PHYSICIAN NETWORK
 WELCOME TO TORRANCE MEMORIAL PHYSICIAN NETWORK Thank you for choosing us as your healthcare provider. We have enclosed instructions for filling out the paperwork that will be necessary for your first visit.
WELCOME TO TORRANCE MEMORIAL PHYSICIAN NETWORK Thank you for choosing us as your healthcare provider. We have enclosed instructions for filling out the paperwork that will be necessary for your first visit.
Swiftwater/Wildland Application Checklist
 Mountain View Fire and Rescue KING COUNTY FIRE PROTECTION DISTRICT 44 32316 148 AVE SE Auburn, WA 98092 / (253) 735-0284; FAX (253) 735 0287 Swiftwater/Wildland Application Checklist Application complete
Mountain View Fire and Rescue KING COUNTY FIRE PROTECTION DISTRICT 44 32316 148 AVE SE Auburn, WA 98092 / (253) 735-0284; FAX (253) 735 0287 Swiftwater/Wildland Application Checklist Application complete
City of Shorewood Application for Employment
 City of Shorewood Application for Employment We welcome you as an applicant for employment with the City of Shorewood. It is the City of Shorewood s policy to provide equal opportunity in employment. The
City of Shorewood Application for Employment We welcome you as an applicant for employment with the City of Shorewood. It is the City of Shorewood s policy to provide equal opportunity in employment. The
Substitute Paperwork Packet (Revised 10/11/2017)
") www.mresc.org Your Partner in Educational Excellence Substitute Paperwork Packet (Revised 10/11/2017) All substitutes have to be Board approved to be placed on any substitute listing. Please return the
www.mresc.org Your Partner in Educational Excellence Substitute Paperwork Packet (Revised 10/11/2017) All substitutes have to be Board approved to be placed on any substitute listing. Please return the
B and B Maintenance, Inc. Employee Application
 B and B Maintenance, Inc. Employee Application To be completed prior to employment please print clearly B and B Maintenance, Inc. is an equal opportunity employer. Employment is based upon experience and
B and B Maintenance, Inc. Employee Application To be completed prior to employment please print clearly B and B Maintenance, Inc. is an equal opportunity employer. Employment is based upon experience and
INTERNSHIP APPLICATION-LEADERS OF AMERICA
 1 PERSONAL INFORMATION MUST BE COMPLETED IN BLUE OR BLACK INK NO PENCIL INTERNSHIP APPLICATION-LEADERS OF AMERICA 507 E. Mayfield Blvd. San Antonio, Texas 78214 Office: 210-924-0330 Hours: 8:30 am 5:00
1 PERSONAL INFORMATION MUST BE COMPLETED IN BLUE OR BLACK INK NO PENCIL INTERNSHIP APPLICATION-LEADERS OF AMERICA 507 E. Mayfield Blvd. San Antonio, Texas 78214 Office: 210-924-0330 Hours: 8:30 am 5:00
D Job Fair D Community Organization D Employee Referral: D Other: Employment Application Safety Sensitive Positions
 Transit Management of Montgomery 2318 W. Fairview Avenue Montgomery, AL 36108 Fax: 334 262-7366 Employment Application Safety Sensitive Positions Note to Applicant: Please advise us in advance if you require
Transit Management of Montgomery 2318 W. Fairview Avenue Montgomery, AL 36108 Fax: 334 262-7366 Employment Application Safety Sensitive Positions Note to Applicant: Please advise us in advance if you require
Packet A - Forms. If you have any questions, please contact Human Resources at
 Packet A - Forms 2018 TEMPORARY NEW HIRE PAPERWORK Welcome to Union College! This packet contains new hire forms necessary for you to become established as a Union College employee. Please fill out and
Packet A - Forms 2018 TEMPORARY NEW HIRE PAPERWORK Welcome to Union College! This packet contains new hire forms necessary for you to become established as a Union College employee. Please fill out and
Application for Employment
 Application for Employment We welcome you as an applicant for employment with the City of Red Wing. It is the City of Red Wing s policy to provide equal opportunity in employment. The City of Red Wing
Application for Employment We welcome you as an applicant for employment with the City of Red Wing. It is the City of Red Wing s policy to provide equal opportunity in employment. The City of Red Wing
Nutrition Services Division DCH 06 (REV. 8/2018) PAGE 1 of 6 MEAL BENEFIT FORM FOR PROVIDERS
 PAGE 1 of 6 MEAL BENEFIT FORM FOR PROVIDERS") PAGE 1 of 6 MEAL BENEFIT FORM FOR PROVIDERS Complete, sign, and return this form to your day care home (DCH) sponsor. If you need assistance completing this form, call: (213) 380-3850 Name of DCH provider:
PAGE 1 of 6 MEAL BENEFIT FORM FOR PROVIDERS Complete, sign, and return this form to your day care home (DCH) sponsor. If you need assistance completing this form, call: (213) 380-3850 Name of DCH provider:
MINNESOTA CRIME VICTIMS REPARATIONS CLAIM FORM Complete and submit to:
 Date Received: MINNESOTA CRIME VICTIMS REPARATIONS CLAIM FORM Complete and submit to: Claim Number: (Office Use Only) Minnesota Crime Victims Reparations Board 445 Minnesota Street, Suite 2300 St. Paul
Date Received: MINNESOTA CRIME VICTIMS REPARATIONS CLAIM FORM Complete and submit to: Claim Number: (Office Use Only) Minnesota Crime Victims Reparations Board 445 Minnesota Street, Suite 2300 St. Paul
APPLICATION FOR EMPLOYMENT
 APPLICATION FOR EMPLOYMENT Prospective people will receive consideration without discrimination because of race, religion, color, sex, age, national origin, handicap, sexual orientation or veteran status.
APPLICATION FOR EMPLOYMENT Prospective people will receive consideration without discrimination because of race, religion, color, sex, age, national origin, handicap, sexual orientation or veteran status.
**If you have any other questions, please contact us and we will be happy to help.**
 Attention GGRC Public Partnerships, LLC 7776 S Pointe Pkwy W Suite 5 Phoenix, AZ 8544 Worker First name, Last name Worker Mailing Address, Address 2 Worker City, State, Zip Dear Worker This packet includes
Attention GGRC Public Partnerships, LLC 7776 S Pointe Pkwy W Suite 5 Phoenix, AZ 8544 Worker First name, Last name Worker Mailing Address, Address 2 Worker City, State, Zip Dear Worker This packet includes
GEORGIA DEPARTMENT OF EDUCATION (GDOE) Administrative Technology Division. FY 2017 CPI Data Collection Data Elements Glossary
 Administrative Technology Division. FY 2017 CPI Data Collection Data Elements Glossary") GEORGIA DEPARTMENT OF EDUCATION (GDOE) Administrative Technology Division FY 2017 CPI Data Collection Data Elements Glossary CPI DATA ELEMENTS GLOSSARY Glossary ANNUAL CONTRACT SALARY FOR CERTIFIED ANNUAL
GEORGIA DEPARTMENT OF EDUCATION (GDOE) Administrative Technology Division FY 2017 CPI Data Collection Data Elements Glossary CPI DATA ELEMENTS GLOSSARY Glossary ANNUAL CONTRACT SALARY FOR CERTIFIED ANNUAL
Branson Public Schools
 Branson Public Schools Dr. Don Forrest, Assistant Superintendent of Business Services 1756 Bee Creek Rd Branson, MO 65616 Phone: 417.334.6541 uww.branson.k12.mo.us Fax: 417.332.2510 Amy Mulvaney, Administrative
Branson Public Schools Dr. Don Forrest, Assistant Superintendent of Business Services 1756 Bee Creek Rd Branson, MO 65616 Phone: 417.334.6541 uww.branson.k12.mo.us Fax: 417.332.2510 Amy Mulvaney, Administrative
Graveyard Productions, LLC
 Graveyard Productions, LLC Check here if you are under 18 years old Recruitment Application- 2018 PLEASE PRINT LEGIBLY Applicant Information Full Name: Date: Last First M.I. Address: Street Address Apartment/Unit
Graveyard Productions, LLC Check here if you are under 18 years old Recruitment Application- 2018 PLEASE PRINT LEGIBLY Applicant Information Full Name: Date: Last First M.I. Address: Street Address Apartment/Unit
Massachusetts Application for Health and Dental Coverage and Help Paying Costs
 Massachusetts Application for Health and Dental Coverage and Help Paying Costs HOW TO APPLY USE THIS APPLICATION TO SEE WHAT COVERAGE CHOICES YOU MAY QUALIFY FOR. WHO CAN USE THIS APPLICATION? You can
Massachusetts Application for Health and Dental Coverage and Help Paying Costs HOW TO APPLY USE THIS APPLICATION TO SEE WHAT COVERAGE CHOICES YOU MAY QUALIFY FOR. WHO CAN USE THIS APPLICATION? You can
Form1040-ES/V (OCR) Department of the Treasury Internal Revenue Service
 Department of the Treasury Internal Revenue Service") Form1040-ES/V (OCR) Department Treasury Internal Revenue Service Purpose of This Package Use this package to figure and pay your estimated tax. If you are not required to make estimated tax payments for
Form1040-ES/V (OCR) Department Treasury Internal Revenue Service Purpose of This Package Use this package to figure and pay your estimated tax. If you are not required to make estimated tax payments for
Please have the employee complete this Workers Compensation Signature Packet in addition to submission of an injury report using:
 Please have the employee complete this Workers Compensation Signature Packet in addition to submission of an injury report using: Online system link located at http://ohr.psu.edu/workers-compensation/
Please have the employee complete this Workers Compensation Signature Packet in addition to submission of an injury report using: Online system link located at http://ohr.psu.edu/workers-compensation/
Applications will only be accepted from
 May 2018 Dear Applicant, Thank you for your interest in applying to Pikes Peak Habitat for Humanity! Enclosed you will find the Habitat for Humanity application. Before completing the application, please
May 2018 Dear Applicant, Thank you for your interest in applying to Pikes Peak Habitat for Humanity! Enclosed you will find the Habitat for Humanity application. Before completing the application, please
Thomas Transport Delivery: APPLICATION FOR DRIVERS
 Thomas Transport Delivery: APPLICATION FOR DRIVERS You Must answer every question. If any question does not apply to you, answer with Not Applicable (NA). In compliance with local, state, and federal equal
Thomas Transport Delivery: APPLICATION FOR DRIVERS You Must answer every question. If any question does not apply to you, answer with Not Applicable (NA). In compliance with local, state, and federal equal
INDIANA COUNTY Employment Application
 INDIANA COUNTY Employment Application Mailing Address: 825 Philadelphia Street Indiana, PA 15701 Phone: 724-465-3805 Fax: 724-465-3953 Indiana County is an equal opportunity employer, dedicated to a policy
INDIANA COUNTY Employment Application Mailing Address: 825 Philadelphia Street Indiana, PA 15701 Phone: 724-465-3805 Fax: 724-465-3953 Indiana County is an equal opportunity employer, dedicated to a policy
Prisma - Employment Application
 Prisma - Employment Application Prisma is an equal opportunity employer, dedicated to a policy of non- discrimination in employment on any basis including age, sex, color, race, creed, national origin,
Prisma - Employment Application Prisma is an equal opportunity employer, dedicated to a policy of non- discrimination in employment on any basis including age, sex, color, race, creed, national origin,
1. APPLICANT INFORMATION. Co-Applicant (spouse must be Co-Applicant) Name Male Female Name Male Female
 Name Male Female Name Male Female") Return by on to: Habitat for Humanity of Greater Plainfield & Middlesex County 2 Randolph Road Plainfield, NJ 07060 Include 25 processing fee in check or money order only. Questions? Call Plainfield Habitat
Return by on to: Habitat for Humanity of Greater Plainfield & Middlesex County 2 Randolph Road Plainfield, NJ 07060 Include 25 processing fee in check or money order only. Questions? Call Plainfield Habitat
Rent & Income Chart ACKNOWLEDGMENT OF APPLICATION FOR NEW COMMUNITY HOUSING PROCEDURE:
 Dear Applicant: Thank you for your interest in Marveland Crescent, an affordable community located in the Flanders section of Mt. Olive, New Jersey. Nestled in a park like setting, Marveland Crescent features
Dear Applicant: Thank you for your interest in Marveland Crescent, an affordable community located in the Flanders section of Mt. Olive, New Jersey. Nestled in a park like setting, Marveland Crescent features
GREEK CATHOLIC UNION OF THE USA (Herein called GCU)
") GREEK CATHOLIC UNION OF THE USA (Herein called GCU) 5400 TUSCARAWAS ROAD, BEAVER, PENNSYLVANIA 15009-9513 1-800-722-4428 IMMEDIATE ANNUITY APPLICATION (Please print) Is the Proposed Annuitant a member
GREEK CATHOLIC UNION OF THE USA (Herein called GCU) 5400 TUSCARAWAS ROAD, BEAVER, PENNSYLVANIA 15009-9513 1-800-722-4428 IMMEDIATE ANNUITY APPLICATION (Please print) Is the Proposed Annuitant a member
Property Management, Inc.
 EQUAL HOUSING O P P O R T U N I T Y Justus Property Management, Inc. RENTAL APPLICATION Marketing info: How did you hear about the property? Please include a $16.00 fee for each adult household member.
EQUAL HOUSING O P P O R T U N I T Y Justus Property Management, Inc. RENTAL APPLICATION Marketing info: How did you hear about the property? Please include a $16.00 fee for each adult household member.