Critical Access Hospital (CAH) ND Critical Access Hospital Board Boot Camp April 13, 2018
|
|
|
- Aldous Carpenter
- 5 years ago
- Views:
Transcription
1 Critical Access Hospital (CAH) Financial Analysis 2016, ND CAH ACO Experiences, Plans and Possibilities ND Critical Access Hospital Board Boot Camp April 13, Support for the Financial Analysis The CAH Financial Reporting project is supported by funding from the North Dakota Medicare Rural Hospital Flexibility Program, administered by the Center for Rural Health at the UND School of Medicine and Health Sciences. Funding is provided through the Federal Office of Rural Health Policy by the U.S. Department of Health and Human Services. 2 1
2 North Dakota CAH Financial Analysis Agenda CAH Financials for All 36 North Dakota CAHs Eastern/Western ND CAH Financial Analysis 27 Original ND CAHs Reporting for 10 Years Accountable Care Organizations (ACO) 3 ND CAH Financial Analysis All 36 North Dakota CAHs Calendar


3 North Dakota CAH Financial Analysis Definition of Terms Used Operating Revenue Revenue generated from healthcare related services provided Contractual Deductions The difference between what is charged for services and what is allowed/paid Bad Debt/Charity Care Uncompensated care provided by facilities Expenses Expenses incurred Operating Margin Operating revenue less contractual deductions and expense Non-operating Revenue Revenue realized from non operational sources such as donations, foundation, investments, government subsidies, etc. Net Margin Net Margin realized from all sources of revenue and expense 6 3
4 North Dakota CAH Financial Analysis Calendar 2016 Observations 10 th year of the CAH Financial Analysis 36 CAHs have reported financials since Licensed CAH Hospital beds 32 of 36 Facilities Own/Operate a Clinic 32 Facilities Who Own/Operate Clinics, Operate 53 Clinics 42 of the 53 Clinics Are Rural Health Clinics (RHCs) 13 of 36 Facilities Own/Operate a Nursing Home (585 beds) 6 Facilities Operate Basic Care (132 beds) 8 Facilities Operate Assisted Living (136 apartments) 8 Facilities Own and Operate the Local Ambulance 2 Facilities Own/Operate Home Care (some provide RHC visiting nurse) 7 ND CAH Acute/Swing Bed Occupancy (Patient Census) Survey Snapshot at a Point in Time August 2016 and Prior Years Licensed Beds & Occupancy for 36 Facilities CAH Licensed Beds 1,439 1, Acute Patients Skilled Swing Bed Patients Non Skilled Swing Bed
5 North Dakota CAH Financial Analysis 2016 Observations (continued) CAHs had 104,261 ER Visits CAHs reported 367,565 Clinic Visits Hospital and Clinic Revenue 36 CAHs Orig. 27 $304,993,808 Medicare revenue (39%) (46%) $218,106,179 BCBS revenue (28%) (23%) $117,902,582 Other revenue (15%) (11%) $ 65,534,194 Medicaid revenue (8%) (9%) $ 46,839,671 Self Pay revenue (6%) (7%) $ 27,481,023 Medicaid Expansion (4%) (3%) $780,857,457 TOTAL $780,857,457 $247,414,013 9 North Dakota Critical Access Hospitals 2016 Hospital/Clinic Patient Revenue By Payer 45% 40% 35% 30% 25% 20% 39% 15% 28% 10% 15% 5% 0% 8% 6% 4% Medicare Medicaid Medicaid Expansion BCBS Self Pay Other Medicare Medicaid Medicaid Expansion BCBS Self Pay Other 10 5
6 North Dakota 2016 CAH Financial Analysis 36 CAH Observations Description CAHs with Positive Operating Margin Mean Operating Margin -3.5% -4.5% 0.1% 0.2% Median Operating Margin -2.3% -5.1% -1.5%.03% CAHs with Positive Net Margin Mean Net Margin 0.6% 2.1% 2.7% 3.8% Median Net Margin 0.2% -0.3% 3.1% 2.6% 11 North Dakota Critical Access Hospitals Statement of Operations, Comparing 2010 to Facilities 36 Facilities Variance % 2010 Total 2016 Total Operating Revenue * $537,401,689 $871,543, % Contractual Deductions -$156,390,822 -$267,966, % Bad Debt/Charity Expense - $15,981,219 - $32,517, % Net Revenue $365,029,648 $571,058, % *(Other operating revenue grew 123%) $13,007,817 $29,661,790 Expenses $368,653,823 $570,889, % Operating Margin -$3,624, , % Operating Margin Mean% -0.7% 0.03% Operating Margin Median% - 1.4% 0.2% Non Operating Rev. - $ 2,639,921 $21,639, % NET Income/Loss - $ 6,264,096 $21,809, % Net Margin Mean % -1.2% 3.8% Net Margin Median % -0.7% 2.6% 12 6
7 North Dakota Critical Access Hospitals Statement of Operations, Comparing 2014 to Facilities 36 Facilities Variance % 2014 Total 2016 Total Operating Revenue * $708,815,428 $871,543, % Contractual Deductions -$188,777,096 -$267,966, % Bad Debt/Charity Expense - $37,740,043 - $32,517, % Net Revenue $483,298,288 $571,058, % *(Other operating revenue grew 61%) $18,538,618 $29,661,790 Expenses $505,107,418 $570,889, % Operating Margin -$21,809,130 $169, % Operating Margin Mean % -4.5% 0.03% Operating Margin Median % - 5.1% 0.2% Non Operating Rev. $31,768,771 $21,639, % NET Income/Loss $ 9,959,642 $21,809, % Net Margin Mean % 2.1% 3.8% Net Margin Median % -0.3% 2.6% 13 North Dakota Critical Access Hospitals 2016 Operating Margins 30% 24% 20% Operating Margin 10% 0% -10% -12% -13% -7% -5% -5% -4% -4% -4% -4% -3% -3% -2% -1% -1% 0% 0% 1% 1% 1% 2% 2% 3% 4% 5% 5% 5% 5% 6% 7% 8% 9% 10% 0.25% 0.03% -20% -20% -30% -28% -28% -40% West of HWY 83 East of HWY 83 Median (0.25%) Mean (.03%) 14 7
8 30.0% North Dakota Critical Access Hospitals 2014, 2015, 2016 Operating Margins 20.0% 10.0% Operating Margin 0.0% -10.0% % -30.0% -40.0% 2014 Operating Margins 2015 Operating Margins 2016 Operating Margins 15 50% North Dakota Critical Access Hospitals 2016 Net Margins 46% 40% 30% 24% 31% 20% 17% Net Margin 10% 0% 8% 8% 9% 9% 9% 6% 7% 7% 5% 5% 5% 0% 1% 1% 1% 1% 2% 2% 3% 3% 3% 3% 2.6% 3.8% -10% -10% -1% -2% -2% -6% -5% -5%-4% -20% -17% -22% -30% West of HWY 83 East of HWY 83 Median (2.6%) Mean (3.8%) 16 8
9 50.0% North Dakota Critical Access Hospitals 2014, 2015, 2016 Net Margins 40.0% 30.0% 20.0% Net Margin 10.0% 0.0% % -20.0% -30.0% 2014 Net Margins 2015 Net Margins 2016 Net Margins 17 NORTH DAKOTA 36 CRITICAL ACCESS HOSPITALS OPERATING REVENUE Inpatient Outpatient Clinic Other 95,671,000 90,949, ,715,148 84,008,509 79,383,746 89,933, ,997,022 REVENUE 78,894,415 86,319,651 70,204,748 77,427, ,374, ,907,110 58,665, ,209, ,437, ,106, ,236, ,270, ,847, ,498, ,727, ,759, ,751, ,519, ,782, ,492, ,285,
10 North Dakota 36 Critical Access Hospitals Bad Debt Expense % Inpatient, Outpatient, Clinic, Swing Bed Revenue 7.00% 6.00% 5.00% Bad Debt Percentage 4.00% 3.00% 2.00% 3.44% 4.73% 5.62% 5.79% 6.03% 5.42% 4.19% 1.00% 0.00% ND CAH Financial Analysis Comparison East of Highway 83 & West of Highway
11 North Dakota Critical Access Hospitals Statement of Operations Analysis 24 CAHs 12 CAHS East of 83 West of Total 2016 Total Operating Revenue $438,887,567 $432,655,995 Contractual Deductions -$120,889,412 -$147,077,587 Bad Debt/Charity Care -$11,765,587 -$20,752,103 Net Operating Revenue $306,232,569 $264,826,306 Expenses $297,363,112 $273,526,282 Operating Margin $8,869,457 - $8,699,976 Operating Margin Mean % 2.9% -3.3% Operating Margin Median % 0.9% -3.9% Non Operating Rev. $14,445,840 $7,193,977 NET Income/Loss $23,315,297 - $1,506,000 Net Margin % Mean 7.6% -0.6% Net Margin % Median 3.8% 1.2% 21 North Dakota Critical Access Hospitals Statement of Operations Analysis West of 83 West of Total Total Variance % Operating Revenue $336,128,051 $432,655, % Contractual Deductions -$94,438,111 -$147,077, % Bad Debt/Charity Expense -$25,507,865 -$20,752, % Net Revenue $216,182,076 $264,826, % Expenses $229,229,085 $273,526, % Operating Margin -$13,047,010 -$8,699, % Operating Margin Mean % -6.0% -3.3% Operating Margin Median % -6.9% -3.9% Non Operating Rev. $14,237,473 $7,193, % NET Income/Loss $1,190,463-1,506, % Net Margin % Mean 0.6% -0.6% Net Margin % Median 2.9% 1.2% 22 11
12 15.0 ND Critical Access Hospitals Operating Margin Calendar Year 2016 The CAHs West of Highway Percentages West of HWY 83 Median (-3.9%) Mean (-3.3%) 23 North Dakota Critical Access Hospitals West of Hwy 83 Revenue 450,000, ,000,000 28,005, ,000,000 26,072,513 83,260, ,000,000 23,932,947 27,774,366 74,316,302 Revenue 250,000, ,000,000 26,431,524 43,236,513 24,212,751 47,262,256 65,940,086 70,647, ,608, ,791, ,000, ,000, ,091, ,309, ,220, ,238,738 50,000,000 47,711,857 51,417,318 49,777,532 53,313,734 69,244,663 79,296, Inpatient Outpatient Clinic Other 24 12
13 North Dakota Critical Access Hospitals Bad Debt Percentage of Revenue, East Vs West of Hwy Bad Debt Percentage of Hospital Inp, Outpt, Swingbed, Clinic Revenue % 7.14% 4.02% 7.70% 3.85% 8.27% 5.22% 5.22% 3.11% 3.11% East West Original CAHs in the Analysis Calendar
 Mean (-2.")
14 ND Critical Access Hospitals Operating Margin Calendar Year Original Facilities 15% 10% 5% 0% 8% 9% 4% 5% 5% 6% 7% 2% 2% 1% 1% 1% Percentages -5% -10% -4% -4% -4% -3% -3% -2% -1% -1% -7% -6% -1.3% -2.9% -15% -12% -13% -20% -20% -25% -28% -28% -30% West of HWY 83 East of HWY 83 Median (-1.3%) Mean (-2.9%) 28 14
15 ND CAH Original 27 Facilities Statement of Operations Analysis 27 Facilities 27 Facilities Total Total Variance % Operating Revenue $194,605,635 $326,227, % Bad Debt/Charity Care - $ 3,522,554 -$9,980, % Other Deductions -$35,571,417 -$46,086, % Net Patient Revenue $155,511,664 $270,161, % (Other operating revenue grew 520%) Expenses $161,465,871 $278,009, % Operating Margin - $5,954,207 - $ 7,848,777-31% Operating Margin Mean % -3.8% -2.9% Operating Margin Median % -3.0% -1.3% Non Operating Rev. $4,112,571 $ 9,994, % NET Income/Loss -$ 249,444 $ 2,095,749 Net Margin % Mean -0.2% 0.8% Net Margin % Median -1.7% 1.7% Original North Dakota Critical Access Hospitals Revenue 300,000,000 Revenue 250,000, ,000, ,000,000 56,662,419 57,816,522 23,112,679 61,940,518 65,747,351 23,450,801 23,215,516 73,110,951 32,360,823 72,721,678 36,290,658 70,252,628 37,929,952 77,671,504 40,344,028 78,132,424 44,654,891 80,699,556 48,730,168 20,417, ,000,000 82,825,552 93,034, ,634, ,004, ,324, ,930, ,929, ,277, ,274, ,969,771 50,000,000 31,578,867 33,974,027 32,852,204 30,692,375 28,343,736 26,532,438 26,527,212 24,961,299 26,055,987 24,029, Inpatient Outpatient Clinic Other 30 15
16 North Dakota CAH Financial Analysis Observations Of the 27 Reporting in all 10 years 5 Had Operating Losses all 10 years 8 Had Operating Losses in 9 of 10 Years Of the 27 Reporting in all 10 Years Facilities With Positive Operating Margin CAH Financials Thoughts Inpatient utilization at the smaller CAHs continues to decline Outpatient and Clinic Revenue continues to experience growth in CAHs Medicaid Expansion accounted for $27 million or 4% of patient revenue Bad debt/charity care expense has continued to stabilize and decline Decreased 14% or $5 million from 2015 to 2016 The 340b program accounted for $7.5 million in (other operating) revenue Half of CAHs participated in 340b program CAHs incurred $16 million in contract nursing expense in 2016 $3 million more than in 2015 Operating margins continued to improve 18 facilities had a positive operating margin in of those utilized the 340b program Net margins continued a positive trend Volume to value transition and MIPS will impact us in the future 32 16
?")

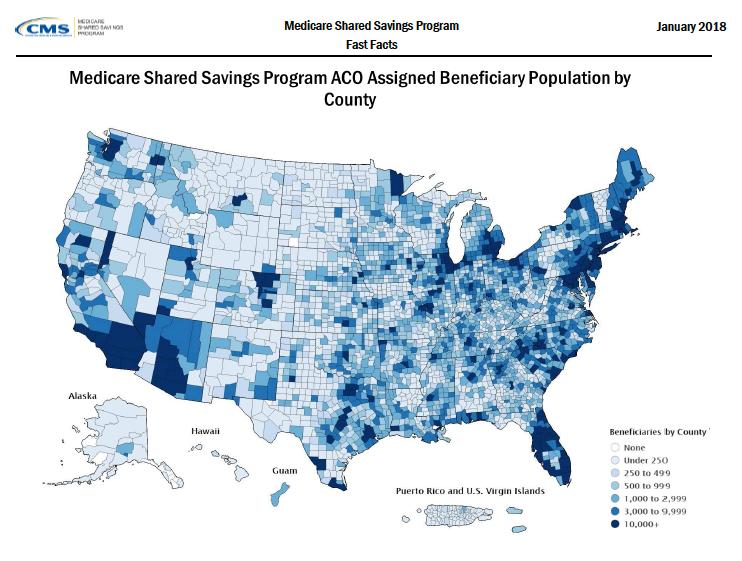
17 Accountable Care Organization (ACO)??? 33 Projected Change in Medicare Enrollment 17
18 Projected Medicare Spending Medicare Spending in Billions $1,100 $1,000 $900 $800 $700 $600 $586 $597 $615 $671 $695 $722 $794 $849 $911 $1,018 $1,064 $ Medicare Part A Trust Fund Balance % of Annual Expenditures In billions: 100% 80% 60% 40% 20% 0%
 A group of health care providers who come together to coordinate the quality and cost of care provided to patients attributed to the ACO Types of ACOs Pioneer ACO, Next Generation,")
19 Medicare Spending 37 Accountable Care Organization ACO Guidelines Established in the Affordable Care Act (ACA) CMS Initiative to Shift from Volume to Value Based Payment Accountable Care Organization (ACO) A group of health care providers who come together to coordinate the quality and cost of care provided to patients attributed to the ACO Types of ACOs Pioneer ACO, Next Generation, Medicare/Medicaid ACO, Medicare Shared Savings (MSSP) MSSP Models One-Sided (Share in Savings) Two-Sided (Share in Savings and Losses) Both models incorporate quality metrics Patient experience, care coordination, population health 38 19

20 39 Accountable Care Organization Separate Organization Legal structure and governance Can Include Hospitals, Clinics, Physicians Attribution of at least 5,000 lives How is it done Annual Wellness Visit Care Coordination Transitions of Care Advanced Care Planning Data, Data Data Quadruple AIM Improve Health Outcomes Improve how we Deliver Care Reduce Cost Improve Satisfaction 40 20
21 Clinical Quality Measures o Examples of Quality Outcomes Ø Potentially Preventable ER visits Ø Potentially Preventable Admissions Ø Patient Satisfaction Surveys Ø Claims Data Ø Health Outcomes ü ü ü ü ü At risk population Chronic disease management Preventative health screens and services Immunizations throughout the lifespan Wellness promotion for all Data Analytics o Data Analytics Medicare Claims Data Ø Cost by type of service provided Ø Acute, ER, Nursing Home, Hospice, Clinic Ø Cost by provider organization Ø Local Provider, Tertiary, Nursing Home, Etc. Ø Encounters by provider Ø Physician Primary Care, Specialist Ø Encounter data by Diagnosis 21
22 North Dakota Medicare ACO High Sierras Northern Plains ACO Submitted applications in 2015 Started January 1, 2016 North Dakota and California providers grouped to meet attribution One sided risk Medicare Shared Savings (MSSP) Received CMS AIM Funding ACO Investment Model (AIM) Prepaid Shared Savings Encouraged rural participation in the ACO model Board of Directors that manage the ACO ACO Champions that lead the ACO work 43 High Sierras Northern Plains ACO North Dakota Participants First Care Health Center Park River Heart of America Medical Center Rugby McKenzie County Healthcare Systems Watford City Sakakawea Medical Center/CCCHC Beulah/Hazen Southwest Healthcare Services Bowman California Participants Barton Health, Mammoth Hospital, Ridgecrest Regional Hospital, Truckee Tahoe Medical Group Arizona Participants Gila Health Resources 44 22

23 Example of ACO info 45 CMS Shift from Volume to Value 46 23

24 47 24

25 What does the future hold Federal deficit will continue to be a challenge Medicare Trust Fund will be of continued concern CMS is continuing the shift from volume to value Future CMS value based initiatives may not be called ACO s, but the transition to value will continue Patients will expect more quality and outcome based results Commercial insurers are also transitioning to value based payment BCBS Blue Alliance Many states have Medicaid managed care 2019 CMS ACO applications due in summer of Thanks for Listening! Questions? Darrold Bertsch Sakakawea Medical Center Coal Country Community Health Center dbertsch@smcnd.org Cell
CAH Metrics and Financial Measures
 acumen CAH Metrics and Financial Measures Presented by Ann King White, CPA BKD, LLP August 5, 2015 AZ Rural Flex Program 2015 Performance Improvement Summit Financial Indicators and Comparison Benchmarks
acumen CAH Metrics and Financial Measures Presented by Ann King White, CPA BKD, LLP August 5, 2015 AZ Rural Flex Program 2015 Performance Improvement Summit Financial Indicators and Comparison Benchmarks
The Case For Value ACA to MACRA to MIPS
 The Case For Value ACA to MACRA to MIPS 2016-2019 Robert E Nesse M.D. Professor of Family Medicine Mayo Medical School Senior Director of Health Care Policy and Payment Reform nesse.robert@mayo.edu What
The Case For Value ACA to MACRA to MIPS 2016-2019 Robert E Nesse M.D. Professor of Family Medicine Mayo Medical School Senior Director of Health Care Policy and Payment Reform nesse.robert@mayo.edu What
MultiCare Health System Year End 2012 Results December 31, 2012
 MultiCare Health System Year End 2012 Results December 31, 2012 MultiCare Health System (MHS), a Washington nonprofit corporation, is an integrated healthcare delivery system providing inpatient, outpatient,
MultiCare Health System Year End 2012 Results December 31, 2012 MultiCare Health System (MHS), a Washington nonprofit corporation, is an integrated healthcare delivery system providing inpatient, outpatient,
NANTICOKE HEALTH SERVICES OBLIGATED GROUP COMBINING BALANCE SHEET September 30, Nanticoke Alternative Care
 Nanticoke Memorial Hospital Assets Current Assets: Cash 1,463,123 Patient Receivables, Net 12,747,937 Other Receivables 1,205,107 Inventories 1,933,790 Prepaid Expenses 841,766 Intercompany Receivables
Nanticoke Memorial Hospital Assets Current Assets: Cash 1,463,123 Patient Receivables, Net 12,747,937 Other Receivables 1,205,107 Inventories 1,933,790 Prepaid Expenses 841,766 Intercompany Receivables
WASHINGTON RURAL HEALTH ACCESS PRESERVATION. Enabling Rural Hospitals in Washington State To Survive and Thrive
 WASHINGTON RURAL HEALTH ACCESS PRESERVATION Enabling Rural s in State To Survive and Thrive Origin and Goals of WRHAP Project WSHA/DOH New Blue H Project Identified issues threatening sustainability of
WASHINGTON RURAL HEALTH ACCESS PRESERVATION Enabling Rural s in State To Survive and Thrive Origin and Goals of WRHAP Project WSHA/DOH New Blue H Project Identified issues threatening sustainability of
SARASOTA COUNTY PUBLIC HOSPITAL DISTRICT
 FINANCIAL STATEMENTS (UNAUDITED) AS OF, AND FOR THE THREE MONTHS ENDED DECEMBER 31, 2008 MANAGEMENT S DISCUSSION AND ANALYSIS FOR THE THREE MONTHS ENDED DECEMBER 31, 2008 For the three months ended December
FINANCIAL STATEMENTS (UNAUDITED) AS OF, AND FOR THE THREE MONTHS ENDED DECEMBER 31, 2008 MANAGEMENT S DISCUSSION AND ANALYSIS FOR THE THREE MONTHS ENDED DECEMBER 31, 2008 For the three months ended December
A Primer on Ratio Analysis and the CAH Financial Indicators Report
 A Primer on Ratio Analysis and the CAH Financial Indicators Report CAH Financial Indicators Report Team North Carolina Rural Health Research and Policy Analysis Center Cecil G. Sheps Center for Health
A Primer on Ratio Analysis and the CAH Financial Indicators Report CAH Financial Indicators Report Team North Carolina Rural Health Research and Policy Analysis Center Cecil G. Sheps Center for Health
Chart 4.1: Percentage of Hospitals with Negative Total and Operating Margins,
 Chart 4.1: Percentage of Hospitals with Negative Total and Operating Margins, 1995 2014 45% 40% 35% Negative Operating Margin 30% 25% 20% 15% Negative Total Margin 10% 5% 0% 95 96 97 98 99 00 01 02 03
Chart 4.1: Percentage of Hospitals with Negative Total and Operating Margins, 1995 2014 45% 40% 35% Negative Operating Margin 30% 25% 20% 15% Negative Total Margin 10% 5% 0% 95 96 97 98 99 00 01 02 03
Medicare Reimbursement Update and Financial Improvement Tools for Rural Hospitals
 acumen Medicare Reimbursement Update and Financial Improvement Tools for Rural Hospitals Presented by Ann King White, CPA BKD, LLP June 15, 2017 insight ideas attention reach expertise depth agility talent
acumen Medicare Reimbursement Update and Financial Improvement Tools for Rural Hospitals Presented by Ann King White, CPA BKD, LLP June 15, 2017 insight ideas attention reach expertise depth agility talent
THE FUTURE OF HEALTHCARE: TRENDS THAT WILL AFFECT YOUR PROFESSIONAL AND PERSONAL LIFE
 THE FUTURE OF HEALTHCARE: TRENDS THAT WILL AFFECT YOUR PROFESSIONAL AND PERSONAL LIFE Dr. Keith Hornberger, BSRT, MBA, DHA, FACHE 1 The Future Direction of Healthcare Healthcare Reform will catalyze a
THE FUTURE OF HEALTHCARE: TRENDS THAT WILL AFFECT YOUR PROFESSIONAL AND PERSONAL LIFE Dr. Keith Hornberger, BSRT, MBA, DHA, FACHE 1 The Future Direction of Healthcare Healthcare Reform will catalyze a
Daniels Memorial Health Care Center
 Daniels Memorial Health Care Center Presentation to the Board of Directors November 19, 2015 Financial Date Statements or subtitle For the Year Ended June 30, 2015 www.wipfli.com 1 Table of Contents Required
Daniels Memorial Health Care Center Presentation to the Board of Directors November 19, 2015 Financial Date Statements or subtitle For the Year Ended June 30, 2015 www.wipfli.com 1 Table of Contents Required
Inventory of Supplies $ 1,397,336 $ 990 $ - Total Current Assets $ 18,373,272 $ 1,420,650 $ 172,240 $ - $ 19,966,162. Assets Limited Use : $ - $ - $ -
 NANTICOKE HEALTH SERVICES, INC. OBLIGATED GROUP BALANCE SHEET DECEMBER 31, 2008 NMH LCLP DUAL ELIMINATIONS OBLIGATED GROUP Current Assets: Cash & Cash Equivalents 1,685,947 325,869 165,154 2,176,970 Patient
NANTICOKE HEALTH SERVICES, INC. OBLIGATED GROUP BALANCE SHEET DECEMBER 31, 2008 NMH LCLP DUAL ELIMINATIONS OBLIGATED GROUP Current Assets: Cash & Cash Equivalents 1,685,947 325,869 165,154 2,176,970 Patient
Advancing Risk Capability in 2015: Medicare Shared Savings Program and ACO Investment Model. March 23, 2015 // 12:00 P.M. 1:00 P.M.
 Advancing Risk Capability in 2015: Medicare Shared Savings Program and ACO Investment Model March 23, 2015 // 12:00 P.M. 1:00 P.M. EST CENTER FOR INDUSTRY TRANSFORMATION The DHG Healthcare Center for Industry
Advancing Risk Capability in 2015: Medicare Shared Savings Program and ACO Investment Model March 23, 2015 // 12:00 P.M. 1:00 P.M. EST CENTER FOR INDUSTRY TRANSFORMATION The DHG Healthcare Center for Industry
4012 FORM CMS
 4012 FORM CMS-2552-10 09-17 4012. Worksheet S-10 - Hospital Uncompensated and Indigent Care Data--Section 112(b) of the Balanced Budget Refinement Act (BBRA) requires that short-term acute care hospitals
4012 FORM CMS-2552-10 09-17 4012. Worksheet S-10 - Hospital Uncompensated and Indigent Care Data--Section 112(b) of the Balanced Budget Refinement Act (BBRA) requires that short-term acute care hospitals
Coverage Expansion [Sections 310, 323, 324, 341, 342, 343, 344, and 1701]
![Coverage Expansion [Sections 310, 323, 324, 341, 342, 343, 344, and 1701]](/thumbs/87/96500790.jpg "Coverage Expansion [Sections 310, 323, 324, 341, 342, 343, 344, and 1701]") Summary of the U.S. House of Representatives Health Reform Bill October 2009 The following summarizes the major hospital and health system provisions included in the U.S. House of Representatives health
Summary of the U.S. House of Representatives Health Reform Bill October 2009 The following summarizes the major hospital and health system provisions included in the U.S. House of Representatives health
A Primer on Financial Ratio Analysis and CAHMPAS
 A Primer on Financial Ratio Analysis and CAHMPAS CAHMPAS Team North Carolina Rural Health Research and Policy Analysis Center Cecil G. Sheps Center for Health Services Research 725 Martin Luther King,
A Primer on Financial Ratio Analysis and CAHMPAS CAHMPAS Team North Carolina Rural Health Research and Policy Analysis Center Cecil G. Sheps Center for Health Services Research 725 Martin Luther King,
Fact Sheet Medicare Secondary Payer Small Employer Exception
 Fact Sheet Medicare Secondary Payer Small Employer Exception The Episcopal Church Medical Trust (Medical Trust) is providing eligible employers with the option to apply for the Medicare Secondary Payer
Fact Sheet Medicare Secondary Payer Small Employer Exception The Episcopal Church Medical Trust (Medical Trust) is providing eligible employers with the option to apply for the Medicare Secondary Payer
A Practical Discussion of Value and Quality Based Payments What Do I Do Now?
 Emerging Challenges in Primary Care: 2016 A Practical Discussion of Value and Quality Based Payments What Do I Do Now? Modified from AHLA Physicians and Hospitals Law Institute 2016 Faculty Ellie Bane
Emerging Challenges in Primary Care: 2016 A Practical Discussion of Value and Quality Based Payments What Do I Do Now? Modified from AHLA Physicians and Hospitals Law Institute 2016 Faculty Ellie Bane
The Guthrie Clinic Financial Highlights for the Three and Six Months Ended December 31, 2017
 Financial Highlights for the Three and Six Months Ended December 31, 2017 I. Introduction In accordance with the provisions of the Master Indenture relating to the 2011 and 2007 Guthrie Health Bonds, enclosed
Financial Highlights for the Three and Six Months Ended December 31, 2017 I. Introduction In accordance with the provisions of the Master Indenture relating to the 2011 and 2007 Guthrie Health Bonds, enclosed
21% Total Medicare Beneficiaries (2017): 58 million
: 58 million") About 1 in 5 Medicare beneficiaries are receiving care from ACOs or medical home models in 2017 Medicare Advantage: 19 million beneficiaries 33% 21% ACOs and Medical Homes 12 million beneficiaries Traditional
About 1 in 5 Medicare beneficiaries are receiving care from ACOs or medical home models in 2017 Medicare Advantage: 19 million beneficiaries 33% 21% ACOs and Medical Homes 12 million beneficiaries Traditional
Growth and Success of Accountable Care Organizations (ACOs) in the US from Dennis Horrigan June 2016
 in the US from Dennis Horrigan June 2016") Growth and Success of Accountable Care Organizations (ACOs) in the US from 2010-2016 Dennis Horrigan June 2016 Introducing Dennis Horrigan Dennis R. Horrigan President and Chief Executive Officer Catholic
Growth and Success of Accountable Care Organizations (ACOs) in the US from 2010-2016 Dennis Horrigan June 2016 Introducing Dennis Horrigan Dennis R. Horrigan President and Chief Executive Officer Catholic
Next Generation Accountable Care Organization (ACO) Model Overview
 Model Overview") The Physicians Advocacy Institute s Medicare Quality Payment Program (QPP) Physician Education Initiative Next Generation Accountable Care Organization (ACO) Model Overview Ad 1 P a g e MEDICARE QPP PHYSICIAN
The Physicians Advocacy Institute s Medicare Quality Payment Program (QPP) Physician Education Initiative Next Generation Accountable Care Organization (ACO) Model Overview Ad 1 P a g e MEDICARE QPP PHYSICIAN
Predictive Qualifying Alternative Payment Model (APM) Participants (QPs) Methodology Fact Sheet What is the Predictive QP Status Analysis?
 Participants (QPs) Methodology Fact Sheet What is the Predictive QP Status Analysis?") Predictive Qualifying Alternative Payment Model (APM) Participants (QPs) Methodology Fact Sheet What is the Predictive QP Status Analysis? One of the Quality Payment Program s goals is to be clear about
Predictive Qualifying Alternative Payment Model (APM) Participants (QPs) Methodology Fact Sheet What is the Predictive QP Status Analysis? One of the Quality Payment Program s goals is to be clear about
Member Fact Sheet Medicare Secondary Payer Small Employer Exception
 Member Fact Sheet Medicare Secondary Payer Small Employer Exception The Episcopal Church Medical Trust (Medical Trust) is providing eligible employers with the option to apply for the Medicare Secondary
Member Fact Sheet Medicare Secondary Payer Small Employer Exception The Episcopal Church Medical Trust (Medical Trust) is providing eligible employers with the option to apply for the Medicare Secondary
Population Health and Wellness: 2 Stories from Cleveland Clinic. Elizabeth Sump Senior Director, Health Policy Cleveland Clinic
 Population Health and Wellness: 2 Stories from Cleveland Clinic Elizabeth Sump Senior Director, Health Policy Cleveland Clinic 1 2 population health stories Cleveland Clinic Employee Health Plan Cleveland
Population Health and Wellness: 2 Stories from Cleveland Clinic Elizabeth Sump Senior Director, Health Policy Cleveland Clinic 1 2 population health stories Cleveland Clinic Employee Health Plan Cleveland
Rev. 12 FORM CMS ( ) (INSTRUCTIONS FOR THIS WORKSHEET ARE PUBLISHED IN CMS PUB. 15-2, SECTION )
 (INSTRUCTIONS FOR THIS WORKSHEET ARE PUBLISHED IN CMS PUB. 15-2, SECTION )") COMPLEX IDENTIFICATION DATA FROM PART I Hospital and Hospital Health Care Complex Address: 1 Street: P.O. Box: 1 2 City: State: ZIP Code: County: 2 Hospital and Hospital-Based Component Identification:
COMPLEX IDENTIFICATION DATA FROM PART I Hospital and Hospital Health Care Complex Address: 1 Street: P.O. Box: 1 2 City: State: ZIP Code: County: 2 Hospital and Hospital-Based Component Identification:
SDMGMA Third Party Payer Day. Lori Lawson, Deputy Medicaid Director
 SDMGMA Third Party Payer Day Lori Lawson, Deputy Medicaid Director 1 Agenda Medicaid Overview TPL ARSD How to report TPL on 1500 form How to report TPL on UB form Common TPL Errors ICD-10 update a. Readiness
SDMGMA Third Party Payer Day Lori Lawson, Deputy Medicaid Director 1 Agenda Medicaid Overview TPL ARSD How to report TPL on 1500 form How to report TPL on UB form Common TPL Errors ICD-10 update a. Readiness
Glossary. Adults: Individuals ages 19 through 64. Allowed amounts: See prices paid. Allowed costs: See prices paid.
 Glossary Acute inpatient: A subservice category of the inpatient facility clams that have excluded skilled nursing facilities (SNF), hospice, and ungroupable claims. This subcategory was previously known
Glossary Acute inpatient: A subservice category of the inpatient facility clams that have excluded skilled nursing facilities (SNF), hospice, and ungroupable claims. This subcategory was previously known
McLEOD HEALTH FINANCIAL INFORMATION FOR CONSOLIDATED & OBLIGATED GROUP FOURTH QUARTER REPORT TWELVE MONTHS ENDED SEPTEMBER 30, 2012 AND 2011
 McLEOD HEALTH FINANCIAL INFORMATION FOR CONSOLIDATED & OBLIGATED GROUP FOURTH QUARTER REPORT TWELVE MONTHS ENDED SEPTEMBER 30, 2012 AND 2011 Note: These unaudited financial statements have been prepared
McLEOD HEALTH FINANCIAL INFORMATION FOR CONSOLIDATED & OBLIGATED GROUP FOURTH QUARTER REPORT TWELVE MONTHS ENDED SEPTEMBER 30, 2012 AND 2011 Note: These unaudited financial statements have been prepared
OBLIGATED GROUP MANAGEMENT S DISCUSSION AND ANALYSIS OF RESULTS FOR THE FISCAL YEAR ENDED JUNE 30, 2018
 OBLIGATED GROUP MANAGEMENT S DISCUSSION AND ANALYSIS OF RESULTS FOR THE FISCAL YEAR ENDED JUNE 30, 2018 For additional information please visit www.essentiahealth.org. For past quarterly and annual disclosures
OBLIGATED GROUP MANAGEMENT S DISCUSSION AND ANALYSIS OF RESULTS FOR THE FISCAL YEAR ENDED JUNE 30, 2018 For additional information please visit www.essentiahealth.org. For past quarterly and annual disclosures
Risk Adjusted Episodes as Benchmarks for ACOs: A Society of Actuaries Sponsored Study
 Risk Adjusted Episodes as Benchmarks for ACOs: A Society of Actuaries Sponsored Study Presented by Bill O Brien, FSA, MAAA Consulting Actuary Milliman Houston, TX (832) 878-4078 Preconference I Agenda
Risk Adjusted Episodes as Benchmarks for ACOs: A Society of Actuaries Sponsored Study Presented by Bill O Brien, FSA, MAAA Consulting Actuary Milliman Houston, TX (832) 878-4078 Preconference I Agenda
The Health Insurance Market in Virginia. Maureen Dempsey, MD, MSc, ACC, FAAP Anthem Blue Cross and Blue Shield June 8, 2017
 The Health Insurance Market in Virginia Maureen Dempsey, MD, MSc, ACC, FAAP Anthem Blue Cross and Blue Shield June 8, 2017 Anthem Inc. at a Glance Broad geographic footprint and customer base ` BCBS plans
The Health Insurance Market in Virginia Maureen Dempsey, MD, MSc, ACC, FAAP Anthem Blue Cross and Blue Shield June 8, 2017 Anthem Inc. at a Glance Broad geographic footprint and customer base ` BCBS plans
Clinically Integrated Networks and Population Health The next chapter in healthcare
 Clinically Integrated Networks and Population Health The next chapter in healthcare M A T T H E W M A T U S I A K, D H S C, F R I P H ( UK) M T ( A S C P ) Health System Challenges While the Uninsured
Clinically Integrated Networks and Population Health The next chapter in healthcare M A T T H E W M A T U S I A K, D H S C, F R I P H ( UK) M T ( A S C P ) Health System Challenges While the Uninsured
Common Managed Care Terms & Definitions
 Contact Us: Email: info@emedbiz.com Phone: 561-430-2090 Fax: 561-430-2091 Website: www.emedbiz.com Common Managed Care Terms & Definitions Balance billing: The practice of billing a patient for the amount
Contact Us: Email: info@emedbiz.com Phone: 561-430-2090 Fax: 561-430-2091 Website: www.emedbiz.com Common Managed Care Terms & Definitions Balance billing: The practice of billing a patient for the amount
9/23/2016. Our Services. Transitioning from Fee-for-Service to Value-based Reimbursement. Key Trends and Strategies for Rural Health Providers
 Transitioning from Fee-for-Service to Value-based Reimbursement Key Trends and Strategies for Rural Health Providers Paul MacLellan, CEO >> Health care consulting company >> Wholly owned subsidiary of
Transitioning from Fee-for-Service to Value-based Reimbursement Key Trends and Strategies for Rural Health Providers Paul MacLellan, CEO >> Health care consulting company >> Wholly owned subsidiary of
Medicare Accountable Care Organizations What & Why?
 Medicare Accountable Care Organizations What & Why? Third National Accountable Care Organization Congress David Saÿen, MBA Regional Administrator Centers for Medicare & Medicaid Services San Francisco
Medicare Accountable Care Organizations What & Why? Third National Accountable Care Organization Congress David Saÿen, MBA Regional Administrator Centers for Medicare & Medicaid Services San Francisco
Individual Insurance
 Health Insurance Health Insurance against loss by illness or bodily injury. Health Insurance provides coverage for medicine, visits to the doctor or emergency room, hospital stays and other medical expenses.
Health Insurance Health Insurance against loss by illness or bodily injury. Health Insurance provides coverage for medicine, visits to the doctor or emergency room, hospital stays and other medical expenses.
Owensboro Health 4th Quarter (March May 2016) FY Ending May 31, 2016
 FY Ending May 31, 2016") Owensboro Health 4th Quarter (March May 2016) FY Ending May 31, 2016 Table of Contents Officer s Certificate of Compliance. 3 Management Discussion and Analysis.. 4 Utilization Statistics and Financial
Owensboro Health 4th Quarter (March May 2016) FY Ending May 31, 2016 Table of Contents Officer s Certificate of Compliance. 3 Management Discussion and Analysis.. 4 Utilization Statistics and Financial
NEWLY ENROLLED MEMBERS IN THE INDIVIDUAL HEALTH INSURANCE MARKET AFTER HEALTH CARE REFORM: THE EXPERIENCE FROM 2014 AND 2015
 NEWLY ENROLLED MEMBERS IN THE INDIVIDUAL HEALTH INSURANCE MARKET AFTER HEALTH CARE REFORM: THE EXPERIENCE FROM 2014 AND 2015 Newly Enrolled Members in the Individual Health Insurance Market After Health
NEWLY ENROLLED MEMBERS IN THE INDIVIDUAL HEALTH INSURANCE MARKET AFTER HEALTH CARE REFORM: THE EXPERIENCE FROM 2014 AND 2015 Newly Enrolled Members in the Individual Health Insurance Market After Health
Conway Hospital, Inc., SC
 Conway Hospital, Inc., SC 1 South Carolina Jobs Economic Development Authority, Hospital Revenue Bonds (Conway Hospital, Inc.), Series 2016, $48,405,000, Dated: December 20, 2016 2 South Carolina Jobs
Conway Hospital, Inc., SC 1 South Carolina Jobs Economic Development Authority, Hospital Revenue Bonds (Conway Hospital, Inc.), Series 2016, $48,405,000, Dated: December 20, 2016 2 South Carolina Jobs
PRACTICE TRANSFORMATION. Moving Towards A Future of Team Based Care. Michael A. Kolber, PhD, MD
 PRACTICE TRANSFORMATION Moving Towards A Future of Team Based Care Michael A. Kolber, PhD, MD 1 2 Financial Disclosures: None Thomas Cole, The Voyage of Life: Childhood 4 Medicare Passed into Law 1965
PRACTICE TRANSFORMATION Moving Towards A Future of Team Based Care Michael A. Kolber, PhD, MD 1 2 Financial Disclosures: None Thomas Cole, The Voyage of Life: Childhood 4 Medicare Passed into Law 1965
Gulf Coast and LA HFMA Payer Summit Value-based contracts same healthcare business?
 Gulf Coast and LA HFMA Payer Summit Value-based contracts same healthcare business? Richard R. Vath, MD FMOLHS SVP/Chief Clinical Transformation Officer President Health Leaders Network and Medicare ACO
Gulf Coast and LA HFMA Payer Summit Value-based contracts same healthcare business? Richard R. Vath, MD FMOLHS SVP/Chief Clinical Transformation Officer President Health Leaders Network and Medicare ACO
Medicare Comprehensive ESRD Care (CEC) Initiative
 Initiative") Medicare Comprehensive ESRD Care (CEC) Initiative May 2013 Avalere Health LLC Avalere Health LLC The intersection of business strategy and public policy Background On February 4, 2013, the Center for Medicare
Medicare Comprehensive ESRD Care (CEC) Initiative May 2013 Avalere Health LLC Avalere Health LLC The intersection of business strategy and public policy Background On February 4, 2013, the Center for Medicare
BANNER HEALTH Investor Conference Call
 BANNER HEALTH Investor Conference Call Year Ended December 31, 2012 and Quarter Ended March 31, 2013 May 30, 2013 Dennis Dahlen, Senior Vice President / Chief Financial Officer Banner Health Snapshot 23
BANNER HEALTH Investor Conference Call Year Ended December 31, 2012 and Quarter Ended March 31, 2013 May 30, 2013 Dennis Dahlen, Senior Vice President / Chief Financial Officer Banner Health Snapshot 23
Bipartisan Budget Act of 2013
 Summary of Medicare and Medicaid Provisions included in the Bipartisan Budget Act of 2013 and the Pathway for SGR Reform Act of 2013, as passed by the House (12/12/13) and the Senate (12/18/13) On December
Summary of Medicare and Medicaid Provisions included in the Bipartisan Budget Act of 2013 and the Pathway for SGR Reform Act of 2013, as passed by the House (12/12/13) and the Senate (12/18/13) On December
TOTAL CURRENT ASSETS 104,960 50,062 12,049 7, ,582 10,615 (3,270) 181,927
 181,927") NORTHERN ARIZONA HEALTHCARE CONSOLIDATED BALANCE SHEET DECEMBER 2017 FMC VVMC NAH NAHOSC Group NAHPG ELIMINATIONS CONSOLIDATED CURRENT ASSETS Cash and Cash Equivalents 12,809 23,907 7,307 5,274 49,297
NORTHERN ARIZONA HEALTHCARE CONSOLIDATED BALANCE SHEET DECEMBER 2017 FMC VVMC NAH NAHOSC Group NAHPG ELIMINATIONS CONSOLIDATED CURRENT ASSETS Cash and Cash Equivalents 12,809 23,907 7,307 5,274 49,297
Evidence-Based Program Reimbursement Strategies. Timothy P. McNeill, RN, MPH
 Evidence-Based Program Reimbursement Strategies Timothy P. McNeill, RN, MPH 1 Medicare & Value Based Purchasing 2 Medicare Advantage Changes 3 DSMT Requirements 4 CDSME Tip Sheet Opportunities for EB Programs
Evidence-Based Program Reimbursement Strategies Timothy P. McNeill, RN, MPH 1 Medicare & Value Based Purchasing 2 Medicare Advantage Changes 3 DSMT Requirements 4 CDSME Tip Sheet Opportunities for EB Programs
CENTEGRA HEALTH SYSTEM AND AFFILIATES CONSOLIDATING STATEMENT OF REVENUE AND EXPENSES FOR THE TWELVE MONTHS ENDED JUNE 30, 2017 Unaudited
 CONSOLIDATING STATEMENT OF REVENUE AND EXPENSES FOR THE TWELVE MONTHS ENDED JUNE 30, 2017 HOSPITAL THE CENTEGRA HEALTH BRIDGE CLINICAL CHWN GROUP FOUNDATION NIMED COMBINED LAB CMS CPC COMBINED CIS ELIMINATIONS
CONSOLIDATING STATEMENT OF REVENUE AND EXPENSES FOR THE TWELVE MONTHS ENDED JUNE 30, 2017 HOSPITAL THE CENTEGRA HEALTH BRIDGE CLINICAL CHWN GROUP FOUNDATION NIMED COMBINED LAB CMS CPC COMBINED CIS ELIMINATIONS
Presentation by Kevin Stone Senior Consultant and Principal Helms & Company Concord NH
 Presentation by Kevin Stone Senior Consultant and Principal Helms & Company Concord NH Medicaid is Largest Payer- covers 1/3 of entire population Vt. funded Medicaid Expansion program pre- ACA (VHAP; Catamount)
Presentation by Kevin Stone Senior Consultant and Principal Helms & Company Concord NH Medicaid is Largest Payer- covers 1/3 of entire population Vt. funded Medicaid Expansion program pre- ACA (VHAP; Catamount)
In This Issue (click to jump):
:") May 7, 2014 In This Issue (click to jump): Analysis of Trends in Health Spending 2013 2014 Spotlight on Medicare Advantage Enrollment Oncology Drug Trend Report S&P Predicts Shift from Job-Based Coverage
May 7, 2014 In This Issue (click to jump): Analysis of Trends in Health Spending 2013 2014 Spotlight on Medicare Advantage Enrollment Oncology Drug Trend Report S&P Predicts Shift from Job-Based Coverage
American Indian Health System. Donald Warne, MD, MPH Oglala Lakota
 American Indian Health System Donald Warne, MD, MPH Oglala Lakota Overview of: OBJECTIVES Issues in Health Law & Policy AI Health & Resource Disparities Social Justice and Indian Health Role of ACA on
American Indian Health System Donald Warne, MD, MPH Oglala Lakota Overview of: OBJECTIVES Issues in Health Law & Policy AI Health & Resource Disparities Social Justice and Indian Health Role of ACA on
The UNC Health Care System & BlueCross BlueShield of North Carolina Model Medical Practice: A Blueprint for Successful Collaboration
 The UNC Health Care System & BlueCross BlueShield of North Carolina Model Medical Practice: A Blueprint for Successful Collaboration Session Overview Many forward-thinking organizations are forging ahead
The UNC Health Care System & BlueCross BlueShield of North Carolina Model Medical Practice: A Blueprint for Successful Collaboration Session Overview Many forward-thinking organizations are forging ahead
North Shore-Long Island Jewish Health System, Inc. (North Shore-LIJ)
") North Shore-Long Island Jewish Health System, Inc. (North Shore-LIJ) ANNUAL FINANCIAL INFORMATION AND OPERATING DATA FOR THE YEAR ENDED DECEMBER 31, 2013 Contents Management s Discussion and Analysis of
North Shore-Long Island Jewish Health System, Inc. (North Shore-LIJ) ANNUAL FINANCIAL INFORMATION AND OPERATING DATA FOR THE YEAR ENDED DECEMBER 31, 2013 Contents Management s Discussion and Analysis of
The Future of Healthcare from a Public Health System Perspective. George V. Masi President and Chief Executive Officer
 The Future of Healthcare from a Public Health System Perspective George V. Masi President and Chief Executive Officer Mission: We improve our community s health by delivering high-quality healthcare to
The Future of Healthcare from a Public Health System Perspective George V. Masi President and Chief Executive Officer Mission: We improve our community s health by delivering high-quality healthcare to
Banner Health Management s Discussion and Analysis of Results of Operations and Financial Position
 Banner Health Management s Discussion and Analysis of Results of Operations and Financial Position The preparation of financial statements in conformity with accounting principles generally accepted in
Banner Health Management s Discussion and Analysis of Results of Operations and Financial Position The preparation of financial statements in conformity with accounting principles generally accepted in
Impact of ACOs on Care Coordination
 Impact of ACOs on Care Coordination Presented by: Michelle L. Templin Vice President Legislative Affairs and Business Development MHA ACO Network March 2, 2017 Agenda Agenda Key Regulatory Drivers Accountable
Impact of ACOs on Care Coordination Presented by: Michelle L. Templin Vice President Legislative Affairs and Business Development MHA ACO Network March 2, 2017 Agenda Agenda Key Regulatory Drivers Accountable
The Financial Effects of Critical Access Hospital Conversion
 The Financial Effects of Critical Access Hospital Conversion July 23, 2003 Richard Donkle, CPA Dale Gullickson, FHFMA Rural Wisconsin Health Cooperative INTRODUCTION The Balanced Budget Act of 1997 established
The Financial Effects of Critical Access Hospital Conversion July 23, 2003 Richard Donkle, CPA Dale Gullickson, FHFMA Rural Wisconsin Health Cooperative INTRODUCTION The Balanced Budget Act of 1997 established
S E C T I O N. National health care and Medicare spending
 S E C T I O N National health care and Medicare spending Chart 6-1. Medicare made up about one-fifth of spending on personal health care in 2002 Total = $1.34 trillion Other private 4% a Medicare 19%
S E C T I O N National health care and Medicare spending Chart 6-1. Medicare made up about one-fifth of spending on personal health care in 2002 Total = $1.34 trillion Other private 4% a Medicare 19%
MANAGEMENT S DISCUSSION OF FINANCIAL AND OPERATING PERFORMANCE
 MANAGEMENT S DISCUSSION OF FINANCIAL AND OPERATING PERFORMANCE Utilization Trends The Corporation has experienced an increase in utilization from the end of 2015 through fiscal year 2017. Occupancy of
MANAGEMENT S DISCUSSION OF FINANCIAL AND OPERATING PERFORMANCE Utilization Trends The Corporation has experienced an increase in utilization from the end of 2015 through fiscal year 2017. Occupancy of
An Introduction to Value Based Care. Evan Richards Product Leader Value Based Care Solutions May 2016
 An Introduction to Value Based Care Evan Richards Product Leader Value Based Care Solutions May 2016 2016 General Electric Company All rights reserved. This does not constitute a representation or warranty
An Introduction to Value Based Care Evan Richards Product Leader Value Based Care Solutions May 2016 2016 General Electric Company All rights reserved. This does not constitute a representation or warranty
news FOR IMMEDIATE RELEASE
 news FOR IMMEDIATE RELEASE INVESTOR CONTACT: MEDIA CONTACT: Mark Kimbrough Ed Fishbough 615-344-2688 615-344-2810 HCA Reports First Quarter 2018 Results Nashville, Tenn., May 1, 2018 HCA Healthcare, Inc.
news FOR IMMEDIATE RELEASE INVESTOR CONTACT: MEDIA CONTACT: Mark Kimbrough Ed Fishbough 615-344-2688 615-344-2810 HCA Reports First Quarter 2018 Results Nashville, Tenn., May 1, 2018 HCA Healthcare, Inc.
ACO Contracting Guide for SNFs
 ACO Contracting Guide for SNFs Part 2: Preparing for and Contracting with ACOs Updated December 2016 About the Author Alexis Finkelberg Bortniker Alexis F. Bortniker is Senior Counsel with Foley & Lardner
ACO Contracting Guide for SNFs Part 2: Preparing for and Contracting with ACOs Updated December 2016 About the Author Alexis Finkelberg Bortniker Alexis F. Bortniker is Senior Counsel with Foley & Lardner
April 10, THN Approval Council: Compliance and Integrity Committee
 Policy Title: 3-Day SNF Rule Waiver Benefit Enhancement Department Responsible: Compliance and Integrity Policy Number: 1.95 THN s Effective Date: April 10, 2017 Next Review/Revision Date: April 2018 Title
Policy Title: 3-Day SNF Rule Waiver Benefit Enhancement Department Responsible: Compliance and Integrity Policy Number: 1.95 THN s Effective Date: April 10, 2017 Next Review/Revision Date: April 2018 Title
Presentation to the IOM Committee on Core Metrics Tom Williams, Dr PH, President & CEO, IHA January 7, 2014, Irvine, California
 Presentation to the IOM Committee on Core Metrics Tom Williams, Dr PH, President & CEO, IHA January 7, 2014, Irvine, California Organization: California multi-sector healthcare leadership group Mission:
Presentation to the IOM Committee on Core Metrics Tom Williams, Dr PH, President & CEO, IHA January 7, 2014, Irvine, California Organization: California multi-sector healthcare leadership group Mission:
CABINET FOR HEALTH AND FAMILY SERVICES DEPARTMENT FOR MEDICAID SERVICES
 Steven L. Beshear Governor CABINET FOR HEALTH AND FAMILY SERVICES DEPARTMENT FOR MEDICAID SERVICES 275 E. Main Street, 6W-A Frankfort, KY 40621 P: 502.564.4321 F: 502.564.0509 www.chfs.ky.gov Janie Miller
Steven L. Beshear Governor CABINET FOR HEALTH AND FAMILY SERVICES DEPARTMENT FOR MEDICAID SERVICES 275 E. Main Street, 6W-A Frankfort, KY 40621 P: 502.564.4321 F: 502.564.0509 www.chfs.ky.gov Janie Miller
ACO Essentials Series
 ACO Essentials Series How to Use Health Endeavors Technology January, 2017 1/11/2017 1 Agenda Day 1&2 Interactive Analytic Tools Define ACO Goals- Success Plan Organizational Structure Executive TIN and
ACO Essentials Series How to Use Health Endeavors Technology January, 2017 1/11/2017 1 Agenda Day 1&2 Interactive Analytic Tools Define ACO Goals- Success Plan Organizational Structure Executive TIN and
17 th Annual Citi Not-for-Profit Health Care Investor Conference Partnering and Collaborating to Drive Value and Innovation May 18, 2016
 17 th Annual Citi Not-for-Profit Health Care Investor Conference Partnering and Collaborating to Drive Value and Innovation May 18, 2016 Presenters: Richard P. Miller President and Chief Executive Officer
17 th Annual Citi Not-for-Profit Health Care Investor Conference Partnering and Collaborating to Drive Value and Innovation May 18, 2016 Presenters: Richard P. Miller President and Chief Executive Officer
1 st Quarter FY2013. Senior Management. David J. Kilarski Chief Executive Officer
 Senior Management David J. Kilarski Chief Executive Officer 910-715-1442 dkilarski@firsthealth.org Executive Summary Lynn DeJaco Chief Financial Officer 910-715-1568 ldejaco@firsthealth.org FirstHealth
Senior Management David J. Kilarski Chief Executive Officer 910-715-1442 dkilarski@firsthealth.org Executive Summary Lynn DeJaco Chief Financial Officer 910-715-1568 ldejaco@firsthealth.org FirstHealth
Investor Presentation. August 2007
 Investor Presentation August 2007 Forward-Looking Statement This presentation should be considered forward-looking and is subject to various risk factors and uncertainties. For more information on those
Investor Presentation August 2007 Forward-Looking Statement This presentation should be considered forward-looking and is subject to various risk factors and uncertainties. For more information on those
Kit Carson County Health Service District Rooted in excellence. Growing in trust.
 Rooted in excellence. Growing in trust. FINANCIAL STATEMENT SUMMARY Income Statement Summary Kit Carson County Health Service District (KCCHSD) had a net loss of $4,041 for the month and a net profit of
Rooted in excellence. Growing in trust. FINANCIAL STATEMENT SUMMARY Income Statement Summary Kit Carson County Health Service District (KCCHSD) had a net loss of $4,041 for the month and a net profit of
Assessing ACO Performance
 Assessing ACO Performance David V. Axene, FSA, FCA, CERA, MAAA As more health plans utilize Accountable Care Organizations (i.e., ACOs) as part of their network operations, ACO performance assessment is
Assessing ACO Performance David V. Axene, FSA, FCA, CERA, MAAA As more health plans utilize Accountable Care Organizations (i.e., ACOs) as part of their network operations, ACO performance assessment is
Volume to Value The Great Transformation of American Medicine
 Volume to Value The Great Transformation of American Medicine 2010-2020 Richard I. Fogel, MD FHRS Chief Clinical Officer St. Vincent Health October 2015 Fee for Service You get paid for what you do The
Volume to Value The Great Transformation of American Medicine 2010-2020 Richard I. Fogel, MD FHRS Chief Clinical Officer St. Vincent Health October 2015 Fee for Service You get paid for what you do The
Financial Statements. Kit Carson County Health Service District. October 2018
 Financial Statements Kit Carson County Health Service District Kit Carson County Health Service District Rooted in excellence. Growing in trust. FINANCIAL STATEMENT SUMMARY Income Statement Summary Kit
Financial Statements Kit Carson County Health Service District Kit Carson County Health Service District Rooted in excellence. Growing in trust. FINANCIAL STATEMENT SUMMARY Income Statement Summary Kit
Medicare Spending Per Beneficiary (MSPB) Measure
 Measure") Medicare Spending Per Beneficiary (MSPB) Measure Audio for this event is available via INTERNET STREAMING. No telephone line is required. Computer speakers or headphones are necessary to listen to streaming
Medicare Spending Per Beneficiary (MSPB) Measure Audio for this event is available via INTERNET STREAMING. No telephone line is required. Computer speakers or headphones are necessary to listen to streaming
Population-Based Healthcare: Structural Models and Options
 Population-Based Healthcare: Structural Models and Options George Choriatis, Esq. Rivkin Radler LLP Presented at: Annual Fall Meeting New York State Bar Association Health Law Section Albany, New York
Population-Based Healthcare: Structural Models and Options George Choriatis, Esq. Rivkin Radler LLP Presented at: Annual Fall Meeting New York State Bar Association Health Law Section Albany, New York
Health Care Reform in the United States
 Health Care Reform in the United States 4 Corners MGMA Conference April 2014 Karl Rebay, MBA, FHFMA Director, Health Care Consulting 1 The material appearing in this presentation is for informational purposes
Health Care Reform in the United States 4 Corners MGMA Conference April 2014 Karl Rebay, MBA, FHFMA Director, Health Care Consulting 1 The material appearing in this presentation is for informational purposes
2018 Merit-based Incentive Payment System (MIPS) Cost Performance Category Fact Sheet
 Cost Performance Category Fact Sheet") 2018 Merit-based Incentive Payment System (MIPS) Cost Performance Category Fact Sheet What is the Quality Payment Program? The Medicare Access and CHIP Reauthorization Act of 2015 (MACRA) ended the Sustainable
2018 Merit-based Incentive Payment System (MIPS) Cost Performance Category Fact Sheet What is the Quality Payment Program? The Medicare Access and CHIP Reauthorization Act of 2015 (MACRA) ended the Sustainable
ACOs/Shared Savings Demonstration Project: What Does It All Mean?
 ACOs/Shared Savings Demonstration Project: What Does It All Mean? None Conflicts of Interest Sean P. Roddy, MD Albany, NY Accountable Care Organizations Term introduced in 2006 by Fisher et al. the hospital
ACOs/Shared Savings Demonstration Project: What Does It All Mean? None Conflicts of Interest Sean P. Roddy, MD Albany, NY Accountable Care Organizations Term introduced in 2006 by Fisher et al. the hospital
COMMUNITY HEALTH NETWORK, INC. & AFFILIATED ENTITIES
 COMMUNITY HEALTH NETWORK, INC. & AFFILIATED ENTITIES Unaudited Consolidated Financial Statements As of and for the Quarter Ended March 31, 2012 and A-1 Quarterly Financial Information Community Health
COMMUNITY HEALTH NETWORK, INC. & AFFILIATED ENTITIES Unaudited Consolidated Financial Statements As of and for the Quarter Ended March 31, 2012 and A-1 Quarterly Financial Information Community Health
LAHEY HEALTH SYSTEM F i n a n c i a l S t a t e m e n t D i s c u s s i o n a n d A n a l y s i s. For the Six Months Ended March 31, 2017
 LAHEY HEALTH SYSTEM F i n a n c i a l S t a t e m e n t D i s c u s s i o n a n d A n a l y s i s For the Six Months Ended March 31, 2017 Introduction The attached combined financial statements of Lahey
LAHEY HEALTH SYSTEM F i n a n c i a l S t a t e m e n t D i s c u s s i o n a n d A n a l y s i s For the Six Months Ended March 31, 2017 Introduction The attached combined financial statements of Lahey
The Emergence of Value-Based Care: Present and Future Tense
 The Emergence of Value-Based Care: Present and Future Tense Erik Johnson, Vice President for Value-Based Care May 2016 What Is Value-Based Care? While the concept of value-based care has existed for years,
The Emergence of Value-Based Care: Present and Future Tense Erik Johnson, Vice President for Value-Based Care May 2016 What Is Value-Based Care? While the concept of value-based care has existed for years,
The distribution of the Health Care System s licensed bed complement and beds in service as of December 31, 2013 was as follows:
 THE CARLE FOUNDATION OBLIGATED GROUP ANNUAL OPERATING INFORMATION Year Ended December 31, 2013 INTRODUCTION The Carle Health Care System (the Health Care System or System ) consists of The Carle Foundation
THE CARLE FOUNDATION OBLIGATED GROUP ANNUAL OPERATING INFORMATION Year Ended December 31, 2013 INTRODUCTION The Carle Health Care System (the Health Care System or System ) consists of The Carle Foundation
Fiscal Management for Rural Hospital Department Managers Webinar Series
 Fiscal Management for Rural Hospital Department Managers Webinar Series November 11, 2011 November 18, 2011 December 9, 2011 December 16, 2011 Health Education and Learning Program (HELP) Webinar Series
Fiscal Management for Rural Hospital Department Managers Webinar Series November 11, 2011 November 18, 2011 December 9, 2011 December 16, 2011 Health Education and Learning Program (HELP) Webinar Series
The Road to Value. Aric R. Sharp, MHA, CMPE, FACHE Vice President Accountable Care UnityPoint Health February 3, 2017
 The Road to Value Aric R. Sharp, MHA, CMPE, FACHE Vice President Accountable Care UnityPoint Health February 3, 2017 1,500 Physicians UnityPoint Clinic 17 hospitals + 15 rural network hospitals 35,000
The Road to Value Aric R. Sharp, MHA, CMPE, FACHE Vice President Accountable Care UnityPoint Health February 3, 2017 1,500 Physicians UnityPoint Clinic 17 hospitals + 15 rural network hospitals 35,000
Implementing Revenue Recognition for Health Care Organizations M A R C H 1 8,
 Implementing Revenue Recognition for Health Care Organizations M A R C H 1 8, 2 0 1 8 Background & Key Principles ASU 2014-09 REVENUE FROM CONTRACTS WITH CUSTOMERS Effective for Public Business Entities
Implementing Revenue Recognition for Health Care Organizations M A R C H 1 8, 2 0 1 8 Background & Key Principles ASU 2014-09 REVENUE FROM CONTRACTS WITH CUSTOMERS Effective for Public Business Entities
MANAGEMENT S DISCUSSION AND ANALYSIS OF FINANCIAL CONDITION AND RESULTS OF OPERATIONS FOR ASCENSION
 MANAGEMENT S DISCUSSION AND ANALYSIS OF FINANCIAL CONDITION AND RESULTS OF OPERATIONS FOR ASCENSION As of and for the six months ended December 31, 2014 and 2013 The following information should be read
MANAGEMENT S DISCUSSION AND ANALYSIS OF FINANCIAL CONDITION AND RESULTS OF OPERATIONS FOR ASCENSION As of and for the six months ended December 31, 2014 and 2013 The following information should be read
Evaluation of the Low-Income Pool Program Using Milestone Data: SFY
 Evaluation of the Low-Income Pool Program Using Milestone Data: SFY 2008 09 Niccie McKay, PhD Prepared by the Department of Health Services Research, Management and Policy at the University of Florida
Evaluation of the Low-Income Pool Program Using Milestone Data: SFY 2008 09 Niccie McKay, PhD Prepared by the Department of Health Services Research, Management and Policy at the University of Florida
How Bundled Payments Create Value in New Product Designs Cognizant
 How Bundled Payments Create Value in New Product Designs 1 About Cognizant 2 This Will Not Take Long. 3 What is a Health Insurance Product? 4 Understanding Product Design Commercial Insurance One specific
How Bundled Payments Create Value in New Product Designs 1 About Cognizant 2 This Will Not Take Long. 3 What is a Health Insurance Product? 4 Understanding Product Design Commercial Insurance One specific
MANAGEMENT S DISCUSSION AND ANALYSIS
 450 Brookline Avenue, Boston, MA 02215-5450 617.632.3000 617.632.5330 TDD This document is dated as of March 12, 2018 SPECIAL NOTE CONCERNING FORWARD-LOOKING STATEMENTS. Certain of the discussions included
450 Brookline Avenue, Boston, MA 02215-5450 617.632.3000 617.632.5330 TDD This document is dated as of March 12, 2018 SPECIAL NOTE CONCERNING FORWARD-LOOKING STATEMENTS. Certain of the discussions included
Making the most of Medicare
 & BCBS Nebraska Sponsor Making the most of Medicare NOT FDIC INSURED ı MAY LOSE VALUE ı NO BANK GUARANTEE NOT A DEPOSIT ı NOT INSURED BY ANY FEDERAL GOVERNMENT AGENCY First Westroads Bank, Inc. is not
& BCBS Nebraska Sponsor Making the most of Medicare NOT FDIC INSURED ı MAY LOSE VALUE ı NO BANK GUARANTEE NOT A DEPOSIT ı NOT INSURED BY ANY FEDERAL GOVERNMENT AGENCY First Westroads Bank, Inc. is not
2012 Children s Health Insurance Program Annual Report
 2012 Children s Health Insurance Program Annual Report Table of Contents Executive Summary... 1 Services... 2 Eligibility... 2 Costs and Contributions... 3 Insurance Contractors... 4 Outreach... 4 Enrollment...
2012 Children s Health Insurance Program Annual Report Table of Contents Executive Summary... 1 Services... 2 Eligibility... 2 Costs and Contributions... 3 Insurance Contractors... 4 Outreach... 4 Enrollment...
SUMMA HEALTH SYSTEM OBLIGATED GROUP CONTINUING DISCLOSURE FOR THE THREE MONTHS ENDED MARCH 31, 2012
 SUMMA HEALTH SYSTEM OBLIGATED GROUP CONTINUING DISCLOSURE FOR THE THREE MONTHS ENDED MARCH 31, 2012 MANAGEMENT S DISCUSSION AND ANALYSIS OF THE RESULTS OF OPERATIONS AND FINANCIAL POSITION SUMMA HEALTH
SUMMA HEALTH SYSTEM OBLIGATED GROUP CONTINUING DISCLOSURE FOR THE THREE MONTHS ENDED MARCH 31, 2012 MANAGEMENT S DISCUSSION AND ANALYSIS OF THE RESULTS OF OPERATIONS AND FINANCIAL POSITION SUMMA HEALTH
Deferred inflows of resources Deferred gain on debt refunding 11,668 12,578
 Shands Teaching Hospital and Clinics, Inc. and Subsidiaries Consolidated Basic Statements of Net Position (Unaudited) As of June 30, 2014 and 2013 (Amounts in Thousands) 2014 2013 Assets Current assets
Shands Teaching Hospital and Clinics, Inc. and Subsidiaries Consolidated Basic Statements of Net Position (Unaudited) As of June 30, 2014 and 2013 (Amounts in Thousands) 2014 2013 Assets Current assets
No change from proposed rule. healthcare providers and suppliers of services (e.g.,
 American College of Physicians Medicare Shared Savings/Accountable Care Organization (ACO) Final Rule Summary Analysis Category Final Rule Summary Change from Proposed Rule and Comments ACO refers to a
American College of Physicians Medicare Shared Savings/Accountable Care Organization (ACO) Final Rule Summary Analysis Category Final Rule Summary Change from Proposed Rule and Comments ACO refers to a
Alabama Medicaid. APHCA Compliance Academy and Networking Forum. May 24, 2018
 Alabama Medicaid APHCA Compliance Academy and Networking Forum May 24, 2018 ROBERT MOON, MD CHIEF MEDICAL OFFICER ALABAMA MEDICAID AGENCY 1 AGENDA Medicaid Overview Political Environment Pivot Plan Questions
Alabama Medicaid APHCA Compliance Academy and Networking Forum May 24, 2018 ROBERT MOON, MD CHIEF MEDICAL OFFICER ALABAMA MEDICAID AGENCY 1 AGENDA Medicaid Overview Political Environment Pivot Plan Questions
Spectrum Health System and Affiliates Consolidated Financial Statements. March 31, 2018
 Spectrum Health System and Affiliates Consolidated Financial Statements March 31, 2018 CHIEF FINANCIAL OFFICER S REPORT The enclosed package represents the consolidated financial statements for Spectrum
Spectrum Health System and Affiliates Consolidated Financial Statements March 31, 2018 CHIEF FINANCIAL OFFICER S REPORT The enclosed package represents the consolidated financial statements for Spectrum
KanCare All MCO Training FQHC s & RHC s Spring 2018
 KanCare All MCO Training FQHC s & RHC s Spring 2018 Welcome Introductions Welcome, Introductions & Agenda Agenda Encounter Rates Place of Service (POS) Secondary Claims Credentialing Issues How to avoid
KanCare All MCO Training FQHC s & RHC s Spring 2018 Welcome Introductions Welcome, Introductions & Agenda Agenda Encounter Rates Place of Service (POS) Secondary Claims Credentialing Issues How to avoid
First Quarter Fiscal Year Financial Report (Unaudited Statements)
") Bond Long Term Rating Standard and Poor s AA/Negative FITCH Investors Service AA/Stable First Quarter Fiscal Year Financial Report (Unaudited Statements) Cone Health is an integrated health care delivery
Bond Long Term Rating Standard and Poor s AA/Negative FITCH Investors Service AA/Stable First Quarter Fiscal Year Financial Report (Unaudited Statements) Cone Health is an integrated health care delivery
Balance Sheet Benefis Health System For month Ended September
 Montana Facility Finance Authority Hospital Revenue Series 2007 Bonds - $125 Million Benefis Health System Continuing Disclosure Quarterly Report (Quarter ended 9/30/2009) The accompanying unaudited balance
Montana Facility Finance Authority Hospital Revenue Series 2007 Bonds - $125 Million Benefis Health System Continuing Disclosure Quarterly Report (Quarter ended 9/30/2009) The accompanying unaudited balance
Disclosure of Hospital Financial and Statistical Data: Fiscal Year 2015
 Disclosure of Hospital Financial and Statistical Data: Fiscal Year 2015 Issued August 3, 2016 Updated August 31, 2016 Health Services Cost Review Commission 4160 Patterson Avenue Baltimore, Maryland 21215
Disclosure of Hospital Financial and Statistical Data: Fiscal Year 2015 Issued August 3, 2016 Updated August 31, 2016 Health Services Cost Review Commission 4160 Patterson Avenue Baltimore, Maryland 21215