Blue Cross Blue Shield of Kansas Blue Choice Comprehensive Major Medical Program
|
|
|
- Amelia Robbins
- 5 years ago
- Views:
Transcription
662-3490 Stephanie.")
1 Blue Cross Blue Shield of Kansas Blue Choice Comprehensive Major Medical Program ESSDACK HEALTH INSURANCE GROUP Stephanie Buckman Group Enrollment Representative One North Main, Suite 301 Hutchinson, Kansas (620)
2 ESSDACK Health Insurance Plan Blue Choice Comprehensive Major Medical - Triple Option October 1, 2012 September 30, 2013 EXISTING MEMBER DISTRICTS - GRANDFATHERED $500 Deductible $1,000 Deductible $1,500 Deductible Deductible $500 per person $1,000 per family Coinsurance 80 / 20 (Plan pays 80%; individual pays 20% to coinsurance maximum) Coinsurance $1,000 per person Maximum $2,000 per family Deductible plus $1,500 per person Coinsurance Out $3,000 per family of Pocket Totals* Patient uses local BC/BS pharmacy and receives medication immediately. Blue Rx Mail Order (Prim ) Prim Pharmacy mails medications to your home. Dependent Coverage $1,000 per person $2,000 per family 80 / 20 (Plan pays 80%; individual pays 20% to coinsurance maximum) $2,000 per person $4,000 per family $3,000 per person $6,000 per family $1,500 per person $3,000 per family 80 / 20 (Plan pays 80%; individual pays 20% to coinsurance maximum) $2,500 per person $5,000 per family $4,000 per person $8,000 per family Chiropractic Subject to deductible and coinsurance Subject to deductible and coinsurance Subject to deductible and coinsurance Accidental Injuries Subject to deductible and coinsurance Subject to deductible and coinsurance Subject to deductible and coinsurance Blue Rx Card $15 Generic Copay $15 Generic Copay $15 Generic Copay $40 Name Brand Copay when no $40 Name Brand Copay when no $40 Name Brand Copay when no Generic is available, Generic is available, Generic is available, $40 Plus Cost Difference for Name $40 Plus Cost Difference for Name $40 Plus Cost Difference for Name Brand when Generic is available. Brand when Generic is available. Brand when Generic is available. Maximum supply: 30 days Maximum supply: 30 days Maximum supply: 30 days $35 Generic Copay $90 Name Brand Copay when no Generic is available, $90 Plus Cost Difference for Name Brand when Generic is available. Maximum supply: 90 days Eligible children covered to age 26, unless eligible through own employer $35 Generic Copay $90 Name Brand Copay when no Generic is available, $90 Plus Cost Difference for Name Brand when Generic is available. Maximum supply: 90 days Eligible children covered to age 26, unless eligible through own employer $35 Generic Copay $90 Name Brand Copay when no Generic is available, $90 Plus Cost Difference for Name Brand when Generic is available. Maximum supply: 90 days Eligible children covered to age 26, unless eligible through own employer Lifetime Maximum Unlimited Unlimited Unlimited Pre-admission certification is required on all planned inpatient admissions. * Deductible Plus Coinsurance Out of Pocket Totals do not include excess charges of non-contracting providers, additional coinsurance for using non-blue Choice providers, outpatient prescription drug costs or copays, etc. Some step therapy, quantity limits and prior authorization may be required on certain drugs. Refer to carriers Summary Plan Descriptions for more benefit details. MONTHLY PREMIUMS with Grandfathered Contingency $500 Deductible $1,000 Deductible $1,500 Deductible Single Family Single Family Single Family Current Rates 10/1/11-9/30/12 $ $1, $ $ $ $ Renewal Rates 10/1/12-9/30/13 $ $ $ $ $ $ Monthly $ INCREASE ($6.00) ($15.00) $0 ($6.00) $0 ($5.00) Monthly % INCREASE -1.4% -1.5% 0% -.7% 0% -.6% Employees can move one deductible level at open enrollment. For example: If you are enrolled in the $500 Option today, you can move to the $1,000 on 10/1/12. If you are enrolled in the $1,000 Option today, you can move to either the $500 or $1,500 on 10/1/12. If you are on the $1,500 Option today, you can move to the $1,000 on 10/1/12. CONTINGENCY ON RATES: On June 17, 2010, the Interim Final Rules regarding "Grandfathered" Group Health Plans under The Patient Protection and Affordable Care Act (PPACA) were issued. These rates are firm for districts that attest to maintaining their Grandfathered status. Grandfathered Plans cannot decrease the percent of premiums the employer pays by more than 5 percentage points as compared to the contribution percent at March 23, All Member Districts will be required to provide the data necessary to make this determination. If a member district is not in compliance, the ESSDACK Health Insurance Group will work with the district to come under compliance. If a member district is not able to come under compliance, a one-time exception to the Statement of Assurances will be made to allow a non-compliant district to withdraw from the ESSDACK Health Insurance Plan effective September 30, 2012 and pursue a contract directly with BC/BS or another insurance company. We reserve the right to re-rate should enrollment effective 10/1/2012 vary by + or 10% within each option. 4/17/2012 GBS kr
3 Benefit Summary for ESSDACK Health Insurance Plan Triple Option Comprehensive Major Medical Program Effective October 1, 2012 September 30, 2013 Maximum benefits are available when services are received from Blue Choice providers. Your financial responsibility is based on the provider network you select. Non-Blue Choice & Non-CAP: Difference between the payment allowance and provider charge, additional 20% coinsurance amount, deductible, coinsurance or copay amount CAP (Non-Blue Choice): Additional 20% coinsurance amount,* deductible, coinsurance or copay amount Blue Choice: Deductible, coinsurance or copay amount *Limited to a combined $2,000 per person, $4,000 two-or-more persons each benefit period. Member Pays Triple Option $500 Deductible $1,000 Deductible $1,500 Deductible Coinsurance (Member portion for most services) $500 Deductible $1,000 Deductible $1,500 Deductible Annual Out-of-Pocket Maximum (includes deductible and coinsurance) Copays do not apply to the annual out-of-pocket amount. Employees can move one deductible level at open enrollment. $500/$1,000 individual/two-or-more persons $1,000/$2,000 individual/two-or-more persons $1,500/$3,000 individual/two-or-more persons 20% of allowed amounts after deductible has been met; up to $1,000/$2,000 individual/two-or-more persons $2,000/$4,000 individual/two-or-more persons $2,500/$5,000 individual/two-or-more persons $500 Deductible: $1,500/$3,000 individual/two-or-more persons $1,000 Deductible: $3,000/$6,000 individual/two-or-more persons $1,500 Deductible: $4,000/$8,000 individual/two-or-more persons After the annual out-of-pocket amount has been reached (ded/coins), eligible benefits will be paid at 100% of the allowed amount for the remainder of the benefit period. Unlimited Lifetime Benefit. Eligible children covered to age 26. Covered Services Medical Services Doctor Visits home/office (including hearing and eye exam) Surgery inpatient and outpatient Maternity Care Well Child & Well Baby Office Visit Immunizations up to age 72 months Immunizations over 72 months Well Women Annual Check Up Office Visit Mammogram Pap Smear Routine Physicals Annual Check Up Office Visit Injections Outpatient Radiology and Lab Service Inpatient Hospital Pre-admission certification required for all planned inpatient admissions at Accidental Injury Services Ambulance Services Outpatient Hospital Covers 100% of maximum allowance MC284c GF TO 09/10
4 Covered Services Emergency Room Services Private Duty Nursing Freestanding Outpatient Facilities (Examples: surgery, renal dialysis) Medical Equipment/Disposable Supplies Chiropractic Short-term Therapies Physical, Speech and Occupational, Respiratory and Cardiac Subject to the deductible and/or coinsurance Eligible covered nursing services in the home would be subject to pre-certification for medical necessity Mental Illness & Substance Use Disorders Inpatient Services Requires pre-admission certification from New Directions Behavioral Health at Outpatient Services Prescription Drugs Blue Rx Card Retail Blue Rx Mail (90-day supply) $15 Generic Copay $40 Name Brand Copay when no Generic is available, $40 Plus Cost Difference for Name Brand when Generic is available Maximum supply: 30 days $35 Generic copay $90 Name Brand Copay when no Generic is available, $90 Plus Cost Difference for Name Brand when Generic is available. Maximum supply: 90 days (Note: prior authorization and quantity limits may apply) Exclusions: The following procedures and all related services and supplies are not covered under this program. Services provided directly for or relative to diseases or injuries caused by or arising out of acts of war, insurrection, rebellion, armed invasion, or aggression; duplicate benefits provided under federal, state or local laws, regulations or programs, except Medicaid; cosmetic or reconstructive surgery (except as stated in the certificate); any keratotomy procedures; charges for personal items; convalescent or custodial/maintenance care or rest cures; blood or payments to donors of blood; any service or supply related to the medical management of obesity; charges for services by immediate relatives or by members of your household; acupuncture and admissions for acupuncture; services related to temporomandibular joint dysfunction syndrome over the amount specified in the certificate; services or supplies related to sex changes, sexual dysfunctions or inadequacies; any medically-aided insemination procedure; services related to the reversal of sterilization procedures; mental illness or substance use disorder services provided by a non-eligible provider; hearing aids; eyeglasses or contact lenses (except after the removal of cataracts); unnecessary services and admissions; services or supplies which are experimental or investigative in nature; services not specifically listed as benefits in the certificate; services covered and payable by any medical expense payment provision of any automobile insurance policy. This is a brief summary of the coverage available under this program. It is not a legal document. The exact provisions of the benefits and exclusions are contained in the certificate.





5




6

7
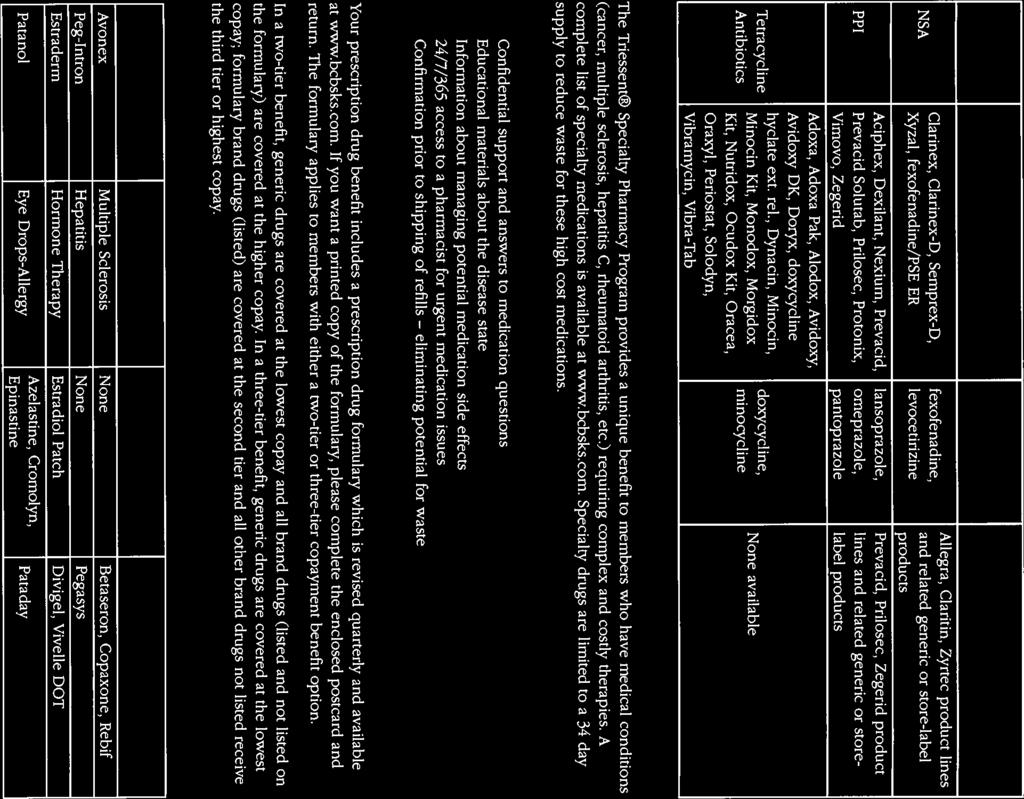
8 ESSDACK Health Insurance Group Mandatory Generic Option How the Option Works When a brand name drug is dispensed and there is an appropriate generic substitute available, the insured s responsibility will be the difference between the allowance for the brand drug and the generic substitute, plus the brand deductible. Generic allowances are determined by the maximum allowable cost (MAC) for the generic drug. In some situations, the difference between the brand and the generic substitute, plus brand deductible, will be greater than the allowed charge for the brand drug. In this situation, the insured will only be responsible for the allowed charge of the brand drug. The availability of a generic substitute is determined by the FDA. The generic must be determined to be bio equivalent to the brand drug. There are some drugs which are available in the same strength and dosage form as the brand, but are not considered bio equivalent. The insured will only be responsible for the brand drug deductible when the brand is dispensed for these drugs. If the pharmacy indicates that the generic is not available in the marketplace, or if state law prohibits generic substitution, the brand drug will be treated as a single source brand. The insured s responsibility will be the brand deductible. If the pharmacy indicates that the brand drug is being used as a generic, the brand will be reimbursed at the generic allowance and the insured will only be responsible for the generic deductible. If the brand drug is required by the doctor and cannot be substituted with a generic equivalent, the insured will be required to pay the difference between the brand allowance and the generic allowance, plus the brand deductible. If the pharmacy does not stock the generic and the brand drug is dispensed, the insured will be required to pay the difference between the brand allowance and the generic allowance, plus the brand deductible. Sometimes your doctor may prescribe a medication to be dispensed as written when there is a formulary preferred brand or generic alternative drug. To help your benefit plan save money, the pharmacist may, on occasion, discuss with your doctor whether an alternative drug might be appropriate for you. Let your doctor know if you have a question about a change in prescription or prefer the original prescription. Your doctor always makes the final decision on your drug.
9 General Notice of Pre-existing Condition Exclusion Note: The Affordable Care Act of 2010 eliminates pre-existing requirements and is being phased in during two separate time periods. Children under the age of 19 with a pre-existing condition can not be denied insurance at plan anniversaries on or after Sept. 23, This protection is extended to all other people with pre-existing conditions at plan anniversaries on or after Jan. 1, This plan imposes a pre-existing condition exclusion. This means that if you have a medical condition before coming to our plan, you might have to wait days before this plan will provide coverage for that condition. This exclusion applies only to conditions for which medical advice, diagnosis, care or treatment was recommended or received within the -day period prior to your date of employment. The pre-existing condition exclusion does not apply to pregnancy, children under the age of 19 or a child enrolled in the plan within 63 days of adoption or placement for adoption. The length of this pre-existing condition exclusion will be reduced by the number of days of your prior creditable coverage. Most prior health coverage is creditable coverage and can be used to reduce the pre-existing condition waiting period if you have not experienced a gap in coverage of 63 or more days. Certificate of Creditable Coverage To reduce the pre-existing condition exclusion by your creditable coverage, you should give your employer a copy of any certificates of creditable coverage you have. If you do not have a certificate, but you have had prior health coverage, you may obtain one from your prior plan or issuer. Questions? All questions about the pre-existing condition exclusion and creditable coverage should be directed to Blue Cross and Blue Shield of Kansas, Customer Service Department, 1133 Topeka Blvd., Topeka, KS You may also call BCBSKS at , in Topeka or , toll-free. Pre-existing Notice 04/11 An Independent Licensee of the Blue Cross and Blue Shield Association
10 CONTINUATION COVERAGE RIGHTS UNDER COBRA Introduction For employees eligible for coverage under the Unified School District #405 Insurance Plan (the Plan), this notice contains important information about your right to COBRA continuation coverage which is a temporary extension of coverage under the Plan. The right to COBRA continuation coverage was created by a federal law, the Consolidated Omnibus Budget Reconciliation Act of 1985 (COBRA). COBRA continuation coverage can become available to you and to other members of your family who are covered under the Plan when you would otherwise lose your group health coverage. This notice generally explains COBRA continuation coverage, when it may become available to you and your family, and what you need to do to protect the right to receive it. This notice gives only a summary of your COBRA continuation coverage rights. For more information about your rights and obligations under the Plan and under federal law, you should either review the Plan s Summary Plan Description or get a copy of the Plan Document from the Group Leader. COBRA continuation coverage for the Plan is administered by: Marsha S. Huggans, Group Leader Frisbie Education Center 800 South Workman Lyons, KS (620) COBRA Continuation Coverage COBRA continuation coverage is a continuation of Plan coverage when coverage would otherwise end because of a life event known as a qualifying event. Specific qualifying events are listed later in this notice. COBRA continuation coverage must be offered to each person who is a qualified beneficiary. A qualified beneficiary is someone who will lose coverage under the Plan because of a qualifying event. Depending on the type of qualifying event, employees, spouses of employees, and dependent children of employees may be qualified beneficiaries. Under the Plan, qualified beneficiaries who elect COBRA continuation coverage must pay for COBRA continuation coverage. If you are an employee, you will become a qualified beneficiary if you will lose your coverage under the Plan because either one of the following qualifying events happens: (1) Your hours of employment are reduced, or (2) Your employment ends for any reason other than your gross misconduct. If you are the spouse of an employee, you will become a qualified beneficiary if you will lose your coverage under the Plan because any of the following qualifying events happens: (1) Your spouse dies; (2) Your spouse s hours of employment are reduced; (3) Your spouse s employment ends for any reason other than his or her gross misconduct; (4) Your spouse becomes enrolled in Medicare (Part A, Part B, or both); or (5) You become divorced or legally separated from your spouse.
11 Your dependent children will become qualified beneficiaries if they will lose coverage under the Plan because any of the following qualifying events happens: (1) The parent-employee dies; (2) The parent-employee s hours of employment are reduced; (3) The parent-employee s employment ends for any reason other than his or her gross misconduct; (4) The parent-employee becomes enrolled in Medicare (Part A, Part B, or both); (5) The parents become divorced or legally separated; or (6) The child stops being eligible for coverage under the plan as a dependent child. Sometimes, filing a proceeding in bankruptcy under title 11 of the United States Code can be a qualifying event. If a proceeding in bankruptcy is filed with respect to Unified School District #405, and that bankruptcy results in the loss of coverage of any retired employee covered under the Plan, the retired employee is a qualified beneficiary with respect to the bankruptcy. The retired employee s spouse, surviving spouse, and dependent children will also be qualified beneficiaries if bankruptcy results in the loss of their coverage under the Plan. The Plan will offer COBRA continuation coverage to qualified beneficiaries only after the Group Leader has been notified that a qualifying event has occurred. When the qualifying event is the end of employment or reduction of hours of employment, death of the employee, commencement of a proceeding in bankruptcy with respect to the employer, or enrollment of the employee in Medicare (Part A, Part B or both), the employer must notify the Group Leader of the qualifying event within 30 days of any of these events. For the other qualifying events (divorce or legal separation of the employee and spouse or a dependent child s losing eligibility for coverage as a dependent child), you must notify the Group Leader. The Plan requires you to notify the Group Leader within 60 days after the qualifying event occurs. Once the Group Leader receives notice that a qualifying event has occurred, COBRA continuation coverage will be offered to each of the qualified beneficiaries. For each qualified beneficiary who elects COBRA continuation coverage, COBRA continuation coverage will begin on the date that Plan coverage would otherwise have been lost. COBRA continuation coverage is a temporary continuation of coverage. When the qualifying event is the death of the employee, enrollment of the employee in Medicare (Part A, Part B, or both), your divorce or legal separation, or a dependent child losing eligibility as a dependent child, COBRA continuation coverage lasts up for up to 36 months. When the qualifying event is the end of employment or reduction of the employee s hours of employment, COBRA continuation coverage lasts for up to 18 months. There are two ways in which this 18-month period of COBRA continuation coverage can be extended.
12 Disability extension of 18-month period of continuation coverage If you or anyone in your family covered under the Plan is determined by the Social Security Administration to be disabled at any time during the first 60 days of COBRA continuation coverage and you notify the Group Leader in a timely fashion, you and your entire family can receive up to an additional 11 months of COBRA continuation coverage, for a total maximum of 29 months. You must make sure that the Group Leader is notified of the Social Security Administration s determination within 60 days of the date of the determination and before the end of the 18-month period of COBRA continuation coverage. Second qualifying event extension of 18-month period of continuation coverage If your family experiences another qualifying event while receiving COBRA continuation coverage, the spouse and dependent children in your family can get additional months of COBRA continuation coverage, up to a maximum of 36 months. This extension is available to a dependent child when that child stops being eligible under the Plan as a dependent child. In all these cases, you must make sure that the Group Leader is notified of the second qualifying event within 60 days of the second qualifying event. If You Have Questions If you have questions about your COBRA continuation coverage, you should contact Marsha S. Huggans, Group Leader or you may contact the nearest Regional or District Office of the U.S. Department of Labor s Employee Benefits Security Administration (EBSA). Addresses and phone numbers of Regional and District EBSA Offices are available through EBSA s website at Keep Your Plan Informed of Address Changes In order to protect your family s rights, you should keep the Group Leader informed of any changes in the addresses of family members. You should also keep a copy, for your records, of any notices you send to the Group Leader.
13

14
Blue Cross Blue Shield of Kansas Blue Choice Comprehensive Major Medical Program
 Blue Cross Blue Shield of Kansas Blue Choice Comprehensive Major Medical Program ESSDACK HEALTH INSURANCE GROUP Effective October 1, 2010 through September 30, 2011 Stephanie Buckman Group Enrollment Representative
Blue Cross Blue Shield of Kansas Blue Choice Comprehensive Major Medical Program ESSDACK HEALTH INSURANCE GROUP Effective October 1, 2010 through September 30, 2011 Stephanie Buckman Group Enrollment Representative
SUMMARY OF MATERIAL MODIFICATION TO THE SUMMARY PLAN DESCRIPTION OF THE MEDICAL BENEFITS UNDER THE UTICA COLLEGE HEALTH BENEFITS PLAN
 SUMMARY OF MATERIAL MODIFICATION TO THE SUMMARY PLAN DESCRIPTION OF THE MEDICAL BENEFITS UNDER THE UTICA COLLEGE HEALTH BENEFITS PLAN This Summary of Material Modification describes changes, to the Summary
SUMMARY OF MATERIAL MODIFICATION TO THE SUMMARY PLAN DESCRIPTION OF THE MEDICAL BENEFITS UNDER THE UTICA COLLEGE HEALTH BENEFITS PLAN This Summary of Material Modification describes changes, to the Summary
PLAN DESIGN AND BENEFITS MC Open Access Plan 1913
 PLAN FEATURES PREFERRED CARE NON-PREFERRED CARE Deductible (per calendar year) $1,500 Individual $4,500 Family $4,000 Individual $12,000 Family Unless otherwise indicated, the Deductible must be met prior
PLAN FEATURES PREFERRED CARE NON-PREFERRED CARE Deductible (per calendar year) $1,500 Individual $4,500 Family $4,000 Individual $12,000 Family Unless otherwise indicated, the Deductible must be met prior
California Small Group MC Aetna Life Insurance Company
 PLAN FEATURES Deductible (per calendar year) $5,000 Individual $10,000 Family Unless otherwise indicated, the Deductible must be met prior to benefits being payable. All covered expenses accumulate toward
PLAN FEATURES Deductible (per calendar year) $5,000 Individual $10,000 Family Unless otherwise indicated, the Deductible must be met prior to benefits being payable. All covered expenses accumulate toward
Not applicable. Immunizations 1 exam per 12 months for members age 18 to age 65; 1 exam per 12 months for adults age 65 and older.
 PLAN FEATURES NON- Deductible (per calendar year) $300 Employee $600 Employee $900 Family $1,800 Family Unless otherwise indicated, the Deductible must be met prior to benefits being payable. Once Family
PLAN FEATURES NON- Deductible (per calendar year) $300 Employee $600 Employee $900 Family $1,800 Family Unless otherwise indicated, the Deductible must be met prior to benefits being payable. Once Family
California Small Group MC Aetna Life Insurance Company NETWORK CARE
 PLAN FEATURES Deductible (per calendar year) Unless otherwise indicated, the Deductible must be met prior to benefits being payable. All covered expenses accumulate toward the preferred and non-preferred
PLAN FEATURES Deductible (per calendar year) Unless otherwise indicated, the Deductible must be met prior to benefits being payable. All covered expenses accumulate toward the preferred and non-preferred
Florida Open Access Managed Choice Aetna Life Insurance Company Plan Effective Date: 03/01/2012. PLAN DESIGN AND BENEFITS MC OA Plan A-50
 Florida 2-100 Open Access Managed Choice Aetna Life Insurance Company Plan Effective Date: 03/01/2012 PLAN DESIGN AND BENEFITS MC OA Plan 12-3000A-50 PLAN FEATURES PREFERRED PROVIDERS NON-PREFERRED PROVIDERS
Florida 2-100 Open Access Managed Choice Aetna Life Insurance Company Plan Effective Date: 03/01/2012 PLAN DESIGN AND BENEFITS MC OA Plan 12-3000A-50 PLAN FEATURES PREFERRED PROVIDERS NON-PREFERRED PROVIDERS
Florida Health Network Option (POS Open Access) Aetna Life Insurance Company Plan Effective Date: 03/01/2012
 Aetna Life Insurance Company Plan Effective Date: 03/01/2012") Florida 2-100 Health Network Option (POS Open Access) Aetna Life Insurance Company Plan Effective Date: 03/01/2012 PLAN DESIGN AND BENEFITS HNOption Plan 12-2000-70 PLAN FEATURES PARTICIPATING PROVIDERS
Florida 2-100 Health Network Option (POS Open Access) Aetna Life Insurance Company Plan Effective Date: 03/01/2012 PLAN DESIGN AND BENEFITS HNOption Plan 12-2000-70 PLAN FEATURES PARTICIPATING PROVIDERS
Florida Open Access Managed Choice Aetna Life Insurance Company Plan Effective Date: 03/01/2012
 Florida 2-100 Open Access Managed Choice Aetna Life Insurance Company Plan Effective Date: 03/01/2012 PLAN FEATURES PREFERRED PROVIDERS NON-PREFERRED PROVIDERS Deductible (per calendar year) PLAN DESIGN
Florida 2-100 Open Access Managed Choice Aetna Life Insurance Company Plan Effective Date: 03/01/2012 PLAN FEATURES PREFERRED PROVIDERS NON-PREFERRED PROVIDERS Deductible (per calendar year) PLAN DESIGN
PLAN DESIGN AND BENEFITS - IN MANAGED CHOICE POS OPEN ACCESS 90/60/60 $1,000 PREFERRED CARE
 PLAN FEATURES NON- Deductible (per calendar year) $1,000 Individual $2,000 Individual $2,000 Family $4,000 Family Unless otherwise indicated, the Deductible must be met prior to benefits being payable.
PLAN FEATURES NON- Deductible (per calendar year) $1,000 Individual $2,000 Individual $2,000 Family $4,000 Family Unless otherwise indicated, the Deductible must be met prior to benefits being payable.
PLAN DESIGN AND BENEFITS - NYC Community Plan SM 6-11 PARTICIPATING PROVIDER REFERRED*
 Aetna Health Inc. for Referred Benefits Plan Effective Date: 10/1/2011 PLAN FEATURES Deductible (per calendar ) $5,000 Individual $15,000 Family Unless otherwise indicated, the Deductible must be met prior
Aetna Health Inc. for Referred Benefits Plan Effective Date: 10/1/2011 PLAN FEATURES Deductible (per calendar ) $5,000 Individual $15,000 Family Unless otherwise indicated, the Deductible must be met prior
Short-Term PPO Plans. Individual and Family Health Care Plans for California
 Short-Term PPO Plans Individual and Family Health Care Plans for California Could This Be You? Our Short-Term Plans are Long on Benefits...for You! You can depend on our experience we ve been helping people
Short-Term PPO Plans Individual and Family Health Care Plans for California Could This Be You? Our Short-Term Plans are Long on Benefits...for You! You can depend on our experience we ve been helping people
NETWORK CARE Managed Choice POS (Open Access)
") PLAN FEATURES Network Primary Care Physician Selection Deductible (per calendar year) Managed Choice POS (Open Access) Unless otherwise indicated, the Deductible must be met prior to benefits being payable.
PLAN FEATURES Network Primary Care Physician Selection Deductible (per calendar year) Managed Choice POS (Open Access) Unless otherwise indicated, the Deductible must be met prior to benefits being payable.
MEMBER COST SHARE. 20% after deductible
 PLAN FEATURES Network Not Applicable Primary Care Physician Selection Not Applicable Deductible (per calendar year) $500 Individual (2-member maximum) Unless otherwise indicated, the Deductible must be
PLAN FEATURES Network Not Applicable Primary Care Physician Selection Not Applicable Deductible (per calendar year) $500 Individual (2-member maximum) Unless otherwise indicated, the Deductible must be
$250 per member. All covered expenses accumulate separately toward the Network and Out-of-network Coinsurance Maximum.
 PLAN FEATURES Network Managed Choice POS (Open Access) OUT-OF- Not Applicable Primary Care Physician Selection Deductible (per calendar year) Not Applicable $250 per member Not Applicable $250 per member
PLAN FEATURES Network Managed Choice POS (Open Access) OUT-OF- Not Applicable Primary Care Physician Selection Deductible (per calendar year) Not Applicable $250 per member Not Applicable $250 per member
PLAN DESIGN AND BENEFITS - New York Open Access MC 3-11 HSA Compatible
 PLAN FEATURES Deductible (per plan year) $3,000 Individual $6,000 Individual $6,000 Family $12,000 Family Unless otherwise indicated, the Deductible must be met prior to benefits being payable. All covered
PLAN FEATURES Deductible (per plan year) $3,000 Individual $6,000 Individual $6,000 Family $12,000 Family Unless otherwise indicated, the Deductible must be met prior to benefits being payable. All covered
All covered expenses accumulate separately toward the Network and Out-of-Network Coinsurance Maximum.
 PLAN FEATURES Network Managed Choice POS (Open Access) Primary Care Physician Selection Not Applicable Deductible (per calendar year) $250 per member (2-member maximum) Unless otherwise indicated, the
PLAN FEATURES Network Managed Choice POS (Open Access) Primary Care Physician Selection Not Applicable Deductible (per calendar year) $250 per member (2-member maximum) Unless otherwise indicated, the
North Carolina Small Group Indemnity Aetna Life Insurance Company Plan Effective Date: 10/01/2010
 PLAN FEATURES [Deductible (per calendar year) $1,000 Individual $3,000 Family Unless otherwise indicated, the Deductible must be met prior to benefits being payable. Member cost sharing for for prescription
PLAN FEATURES [Deductible (per calendar year) $1,000 Individual $3,000 Family Unless otherwise indicated, the Deductible must be met prior to benefits being payable. Member cost sharing for for prescription
NETWORK CARE. $4,500 Individual. (2-member maximum)
") PLAN FEATURES Network Open Choice PPO Primary Care Physician Selection Deductible (per calendar year) Not Applicable $750 per member Not Applicable $750 per member (2-member maximum) (2-member maximum)
PLAN FEATURES Network Open Choice PPO Primary Care Physician Selection Deductible (per calendar year) Not Applicable $750 per member Not Applicable $750 per member (2-member maximum) (2-member maximum)
NETWORK CARE. $250 per member (2-member maximum)
") PLAN FEATURES Network Managed Choice POS (Open Access) Primary Care Physician Selection Not Applicable Deductible (per calendar year) $250 per member (2-member maximum) Unless otherwise indicated, the
PLAN FEATURES Network Managed Choice POS (Open Access) Primary Care Physician Selection Not Applicable Deductible (per calendar year) $250 per member (2-member maximum) Unless otherwise indicated, the
Traditional Choice (Indemnity) (08/12)
 (08/12)") PLAN FEATURES Network Primary Care Physician Selection Deductible (per calendar year) Not Applicable Not Applicable $500 Individual (2-member maximum) Unless otherwise indicated, the Deductible must be
PLAN FEATURES Network Primary Care Physician Selection Deductible (per calendar year) Not Applicable Not Applicable $500 Individual (2-member maximum) Unless otherwise indicated, the Deductible must be
All covered expenses accumulate separately toward the Network and Out-of-Network Coinsurance Maximum.
 PLAN FEATURES Network Managed Choice POS (Open Access) Primary Care Physician Selection Deductible (per calendar year) Not Applicable $500 per member Not Applicable $500 per member (2-member maximum) (2-member
PLAN FEATURES Network Managed Choice POS (Open Access) Primary Care Physician Selection Deductible (per calendar year) Not Applicable $500 per member Not Applicable $500 per member (2-member maximum) (2-member
NETWORK CARE. $4,500 (2-member maximum)
") PLAN FEATURES Network Managed Choice POS (Open Access) Primary Care Physician Selection Not Applicable Deductible (per calendar year) $4,500 (2-member maximum) Unless otherwise indicated, the Deductible
PLAN FEATURES Network Managed Choice POS (Open Access) Primary Care Physician Selection Not Applicable Deductible (per calendar year) $4,500 (2-member maximum) Unless otherwise indicated, the Deductible
Health Care Benefits. Important!
 Health Care Benefits The Major League Baseball Players Welfare Plan (referred to as the Welfare Plan in this section) provides comprehensive health care benefits for you and your eligible dependents. Whether
Health Care Benefits The Major League Baseball Players Welfare Plan (referred to as the Welfare Plan in this section) provides comprehensive health care benefits for you and your eligible dependents. Whether
Basic Fixed indemnity health insurance for individuals and families
 Basic Fixed indemnity health insurance for individuals and families Basic is a group association fixed indemnity health insurance plan underwritten by Madison National Life Insurance Company, Inc., a Wisconsin
Basic Fixed indemnity health insurance for individuals and families Basic is a group association fixed indemnity health insurance plan underwritten by Madison National Life Insurance Company, Inc., a Wisconsin
Florida Health Network Only (HMO Open Access) Aetna Life Insurance Company Plan Effective Date: 03/01/2012
 Aetna Life Insurance Company Plan Effective Date: 03/01/2012") Florida 2-100 Health Network Only (HMO Open Access) Aetna Life Insurance Company Plan Effective Date: 03/01/2012 PLAN DESIGN AND BENEFITS HNOnly Plan 12-1500-Compass PLAN FEATURES Deductible (per calendar
Florida 2-100 Health Network Only (HMO Open Access) Aetna Life Insurance Company Plan Effective Date: 03/01/2012 PLAN DESIGN AND BENEFITS HNOnly Plan 12-1500-Compass PLAN FEATURES Deductible (per calendar
$3,000 Individual $6,000 Family All covered expenses accumulate separately toward the Network and Out-of-Network Coinsurance Maximum.
 PLAN FEATURES Network Managed Choice POS (Open Access) OUT-OF- Primary Care Physician Selection Deductible (per calendar year) $3,000 Individual $6,000 Family Unless otherwise indicated, the Deductible
PLAN FEATURES Network Managed Choice POS (Open Access) OUT-OF- Primary Care Physician Selection Deductible (per calendar year) $3,000 Individual $6,000 Family Unless otherwise indicated, the Deductible
NETWORK CARE. $3,500 Individual $7,000 Family
 PLAN FEATURES Network Primary Care Physician Selection Deductible (per calendar year) Managed Choice POS (Open Access) OUT-OF- $2,000 Individual $4,000 Family Unless otherwise indicated, the Deductible
PLAN FEATURES Network Primary Care Physician Selection Deductible (per calendar year) Managed Choice POS (Open Access) OUT-OF- $2,000 Individual $4,000 Family Unless otherwise indicated, the Deductible
Florida Health Network Only (HMO Open Access) Aetna Life Insurance Company Plan Effective Date: 03/01/2012
 Aetna Life Insurance Company Plan Effective Date: 03/01/2012") Florida 2-100 Health Network Only (HMO Open Access) Aetna Life Insurance Company Plan Effective Date: 03/01/2012 PLAN DESIGN AND BENEFITS HNOnly Plan 12-1500-80 HSA PLAN FEATURES Deductible (per calendar
Florida 2-100 Health Network Only (HMO Open Access) Aetna Life Insurance Company Plan Effective Date: 03/01/2012 PLAN DESIGN AND BENEFITS HNOnly Plan 12-1500-80 HSA PLAN FEATURES Deductible (per calendar
ELIGIBILITY INFORMATION YOU NEED TO KNOW
 EMPLOYEE BENEFITS PLAN YEAR 2017-2018 TABLE OF CONTENTS Eligibility Information You Need to Know 3 Medical Benefits / Premiums 4 Deductible Type / Alternative Prescription Drug Program 6 Arkansas Blue
EMPLOYEE BENEFITS PLAN YEAR 2017-2018 TABLE OF CONTENTS Eligibility Information You Need to Know 3 Medical Benefits / Premiums 4 Deductible Type / Alternative Prescription Drug Program 6 Arkansas Blue
Super Blue Plus QHDHP 1 HDHP Non Emb 100%
 Super Blue Plus QHDHP 1 HDHP Non Emb 100% Effective Date December 1, 2018 Benefit Period 2 (used for Deductible and Coinsurances limits and certain Contract Year benefit frequencies.) Note: All Services
Super Blue Plus QHDHP 1 HDHP Non Emb 100% Effective Date December 1, 2018 Benefit Period 2 (used for Deductible and Coinsurances limits and certain Contract Year benefit frequencies.) Note: All Services
QUICK REFERENCE GUIDE
 REFRIGERATION, AIR CONDITIONING & SERVICE DIVISION (UA NJ) WELFARE, PENSION & ANNUITY FUNDS QUICK REFERENCE GUIDE EFFECTIVE: JANUARY 1, 2018 Important Notice: This is an outline of the principal plan provisions
REFRIGERATION, AIR CONDITIONING & SERVICE DIVISION (UA NJ) WELFARE, PENSION & ANNUITY FUNDS QUICK REFERENCE GUIDE EFFECTIVE: JANUARY 1, 2018 Important Notice: This is an outline of the principal plan provisions
NETWORK CARE. $1,000 Individual $2,000 Family
 PLAN FEATURES Network Managed Choice POS (Open Access) Primary Care Physician Selection Not Applicable Deductible (per calendar year) $3,500 Individual $7,000 Family Unless otherwise indicated, the Deductible
PLAN FEATURES Network Managed Choice POS (Open Access) Primary Care Physician Selection Not Applicable Deductible (per calendar year) $3,500 Individual $7,000 Family Unless otherwise indicated, the Deductible
PPO HSA HDHP $2,500 90/50
 PLAN FEATURES Deductible (per calendar year) $2,500 Individual $2,500 Individual $5,000 Family $5,000 Family Unless otherwise indicated, the Deductible must be met prior to benefits being payable. Member
PLAN FEATURES Deductible (per calendar year) $2,500 Individual $2,500 Individual $5,000 Family $5,000 Family Unless otherwise indicated, the Deductible must be met prior to benefits being payable. Member
SUMMARY OF BENEFITS. Alliance Behavioral Healthcare Open Access Plus Plan Effective 7/1/12. Cigna Health and Life Insurance Co.
 SUMMARY OF BENEFITS Cigna Health and Life Insurance Co. Alliance Behavioral Healthcare Effective 7/1/12 Network: GWH/CIGNA Open Access Plus CIGNA has multiple networks. Your plan is paired with the GWH-CIGNA
SUMMARY OF BENEFITS Cigna Health and Life Insurance Co. Alliance Behavioral Healthcare Effective 7/1/12 Network: GWH/CIGNA Open Access Plus CIGNA has multiple networks. Your plan is paired with the GWH-CIGNA
Individual Blue Access Value
 plan BENEFITS GUIDE M I S S O U R I Individual Blue Access Value Blue Access Choice Value Calendar-year deductible Out-of-Pocket Maximum (including deductible) Physician Office Services Preventive Care
plan BENEFITS GUIDE M I S S O U R I Individual Blue Access Value Blue Access Choice Value Calendar-year deductible Out-of-Pocket Maximum (including deductible) Physician Office Services Preventive Care
Not Applicable. $5,000 Individual. All covered expenses accumulate separately toward the Network and Out-of-Network Coinsurance Maximum.
 PLAN FEATURES Network Managed Choice POS (Open Access) Primary Care Physician Selection Deductible (per calendar year) Not Applicable $2,000 per member Not Applicable $2,000 per member (2-member maximum)
PLAN FEATURES Network Managed Choice POS (Open Access) Primary Care Physician Selection Deductible (per calendar year) Not Applicable $2,000 per member Not Applicable $2,000 per member (2-member maximum)
$4,800.00/ individual. $9,600.00/family
 Medical Plans Please note, this brochure provides an overview of certain health care plan provisions under the Adobe Systems Incorporated Group Welfare Plan. It is not intended to be a complete description
Medical Plans Please note, this brochure provides an overview of certain health care plan provisions under the Adobe Systems Incorporated Group Welfare Plan. It is not intended to be a complete description
SUMMARY OF BENEFITS. Montgomery College Open Access Plus Coinsurance Plan. Connecticut General Life Insurance Co. Notice of Grandfathered Plan Status
 SUMMARY OF BENEFITS Connecticut General Life Insurance Co. Notice of Grandfathered Plan Status This plan is being treated as a grandfathered health plan under the Patient Protection and Affordable Care
SUMMARY OF BENEFITS Connecticut General Life Insurance Co. Notice of Grandfathered Plan Status This plan is being treated as a grandfathered health plan under the Patient Protection and Affordable Care
PLAN DESIGN AND BENEFITS - New York Open Access EPO 4-10/10 HSA Compatible
 PLAN FEATURES Deductible (per plan year) $3,500 Individual $7,000 Family Unless otherwise indicated, the Deductible must be met prior to benefits being payable. The Individual Deductible can only be met
PLAN FEATURES Deductible (per plan year) $3,500 Individual $7,000 Family Unless otherwise indicated, the Deductible must be met prior to benefits being payable. The Individual Deductible can only be met
Calendar-year deductible. Home Health Care (Maximum visits per benefit period - 60 visits) Hospice
 Hospice") plan BENEFITS GUIDE K E N T U C K Y Individual Blue Access Value Sí necesita asistencia en español, usted puede solicitarla sin costo adicional contactando a su corredor o agente de cuidados de la salud.
plan BENEFITS GUIDE K E N T U C K Y Individual Blue Access Value Sí necesita asistencia en español, usted puede solicitarla sin costo adicional contactando a su corredor o agente de cuidados de la salud.
Regence Classic Plan Highlights For Groups of /1/2017
 Plan Features Provider choice: Members have direct access to their choice of providers. Coinsurance levels are lowest for In- Network providers. If a member chooses an Out-of-Network provider, the member
Plan Features Provider choice: Members have direct access to their choice of providers. Coinsurance levels are lowest for In- Network providers. If a member chooses an Out-of-Network provider, the member
PLAN DESIGN AND BENEFITS - Tx OAMC 3000 HSA 100% 08 PREFERRED CARE
 Aetna Life Insurance Company Texas Small Group MC Open Access Plan Effective Date: 09/01/2008 PLAN FEATURES NON- Deductible (per calendar year) $3,000 Individual $6,000 Individual $6,000 Family $12,000
Aetna Life Insurance Company Texas Small Group MC Open Access Plan Effective Date: 09/01/2008 PLAN FEATURES NON- Deductible (per calendar year) $3,000 Individual $6,000 Individual $6,000 Family $12,000
WA Bronze PPO Saver /50 (1/14)
") PLAN FEATURES Deductible (per calendar year) Unless otherwise indicated, the Deductible must be met prior to benefits being payable. Member cost sharing for certain services, including member cost sharing
PLAN FEATURES Deductible (per calendar year) Unless otherwise indicated, the Deductible must be met prior to benefits being payable. Member cost sharing for certain services, including member cost sharing
NEW CASTLE COUNTY COMPARISON OF PRE-65 RETIREES/PENSIONERS BENEFITS PLAN YEAR 2019
 Deductible Per Calendar Year (Individual/Family) $200 Individual $400 Family (DME, Prosthetics and Hearing Aids only) $200 per Individual $400 per Family $200 per Individual $400 per Family $200 per Individual
Deductible Per Calendar Year (Individual/Family) $200 Individual $400 Family (DME, Prosthetics and Hearing Aids only) $200 per Individual $400 per Family $200 per Individual $400 per Family $200 per Individual
(30- to 34-day supply) 100% after $40 copay; significant or new therapeutic class drugs: 50%
 100% after $40 copay; significant or new therapeutic class drugs: 50%") C O U N T Y S I N T R A N E T S I T E : H T T P : / / I N T R A N E T. C O. R I V E R S I D E. C A. U S 25 Exclusive Care Select Medicare Coordination Plan Tier 1: Exclusive Care Network Tier 2: Any Provider
C O U N T Y S I N T R A N E T S I T E : H T T P : / / I N T R A N E T. C O. R I V E R S I D E. C A. U S 25 Exclusive Care Select Medicare Coordination Plan Tier 1: Exclusive Care Network Tier 2: Any Provider
PLAN DESIGN AND BENEFITS - Tx OAMC % 08 PREFERRED CARE
 Aetna Life Insurance Company Texas Small Group MC Open Access Plan Effective Date: 11/01/2008 PLAN FEATURES Deductible (per calendar year) $1,000 Individual $3,000 Individual $3,000 3 Individuals per $9,000
Aetna Life Insurance Company Texas Small Group MC Open Access Plan Effective Date: 11/01/2008 PLAN FEATURES Deductible (per calendar year) $1,000 Individual $3,000 Individual $3,000 3 Individuals per $9,000
Your Health Care Benefit Program
 Your Health Care Benefit Program BLUE ADVANTAGE HMO A Blue Cross HMO a product of Blue Cross and Blue Shield of Illinois A message from BLUE CROSS AND BLUE SHIELD Your Group has entered into an agreement
Your Health Care Benefit Program BLUE ADVANTAGE HMO A Blue Cross HMO a product of Blue Cross and Blue Shield of Illinois A message from BLUE CROSS AND BLUE SHIELD Your Group has entered into an agreement
PLAN DESIGN AND BENEFITS - PA POS COST-SHARING 3.4 ($1,500 DED) PARTICIPATING PROVIDERS. $1,500 Individual
 PARTICIPATING PROVIDERS. $1,500 Individual") Plan Coinsurance * Out-of-Pocket Maximum (per calendar year, includes deductible) $3,000 Individual $6,000 Family 50% $6,000 Individual $12,000 Family Amounts over the Recognized Charge, failure to pre-certification
Plan Coinsurance * Out-of-Pocket Maximum (per calendar year, includes deductible) $3,000 Individual $6,000 Family 50% $6,000 Individual $12,000 Family Amounts over the Recognized Charge, failure to pre-certification
SUMMARY OF BENEFITS. Cigna Health and Life Insurance Co. Cornerstone Systems, Inc. Open Access Plus
 SUMMARY OF BENEFITS Cigna Health and Life Insurance Co. Cornerstone Systems, Inc. Open Access Plus General Services In-network Out-of-network Primary care physician You pay $30 copay per visit Physician
SUMMARY OF BENEFITS Cigna Health and Life Insurance Co. Cornerstone Systems, Inc. Open Access Plus General Services In-network Out-of-network Primary care physician You pay $30 copay per visit Physician
10% 30% Not Applicable. Professional: 105% of Medicare Facility: 140% of Medicare Primary Care Physician Selection
 PLAN FEATURES Deductible (per calendar year) $2,000 Individual $2,000 Individual $4,000 Family $4,000 Family All covered expenses accumulate separately toward the preferred or non-preferred Deductible.
PLAN FEATURES Deductible (per calendar year) $2,000 Individual $2,000 Individual $4,000 Family $4,000 Family All covered expenses accumulate separately toward the preferred or non-preferred Deductible.
Aetna Savings Plus plan guide
 Quality health plans & benefits Healthier living Financial well-being Intelligent solutions Aetna Savings Plus plan guide New health plans designed with New Jersey businesses in mind. For businesses with
Quality health plans & benefits Healthier living Financial well-being Intelligent solutions Aetna Savings Plus plan guide New health plans designed with New Jersey businesses in mind. For businesses with
PLAN DESIGN AND BENEFITS - PA POS COST-SHARING NO-REFERRAL 4.4 ($2,000 DED) $2,000 Individual
 $2,000 Individual") Plan Coinsurance * Out-of-Pocket Maximum (per calendar year, includes deductible) $4,000 Individual $8,000 Family 50% $8,000 Individual $16,000 Family Amounts over the Recognized Charge, failure to pre-certification
Plan Coinsurance * Out-of-Pocket Maximum (per calendar year, includes deductible) $4,000 Individual $8,000 Family 50% $8,000 Individual $16,000 Family Amounts over the Recognized Charge, failure to pre-certification
Allen County 2013 Plan Year Employee Benefits Overview
 Allen County 2013 Plan Year Employee Benefits Overview Employee Benefits Allen County recognizes that our employees are our most valuable resource, your benefits program is extremely important to us. Therefore,
Allen County 2013 Plan Year Employee Benefits Overview Employee Benefits Allen County recognizes that our employees are our most valuable resource, your benefits program is extremely important to us. Therefore,
Unlimited/ $1,000,000 per lifetime Primary Care Physician Selection
 PLAN FEATURES Deductible (per calendar year) None Individual None Family Member Coinsurance Out-of-Pocket Maximum $1,500 $3,000 Individual (per calendar year) $3,000 $6,000 Family Member cost sharing for
PLAN FEATURES Deductible (per calendar year) None Individual None Family Member Coinsurance Out-of-Pocket Maximum $1,500 $3,000 Individual (per calendar year) $3,000 $6,000 Family Member cost sharing for
California Natural Products: EPO Option Coverage Period: 01/01/ /31/2017
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.deltahealthsystems.com or by calling 1-209-858-2525 Ext
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.deltahealthsystems.com or by calling 1-209-858-2525 Ext
Lourdes Health System Proposed Effective Date: Aetna Helathfund Aetna Choice POS ll - ASC Salary Band: Less than $21,000 to $41,999
 PROVIDED BY LIFE INSURANCE COMPANY FUND FEATURES HealthFund Amount $750 Employee $1,500 Employee + Spouse $1,500 Employee + Child(ren) $1,500 Family Amount contributed to the Fund by the employer Fund
PROVIDED BY LIFE INSURANCE COMPANY FUND FEATURES HealthFund Amount $750 Employee $1,500 Employee + Spouse $1,500 Employee + Child(ren) $1,500 Family Amount contributed to the Fund by the employer Fund
PLAN DESIGN AND BENEFITS - PA POS HSA COMPATIBLE NO-REFERRAL 2.4 ($2,500 Ded) PARTICIPATING PROVIDERS
 PARTICIPATING PROVIDERS") PLAN FEATURES Deductible (per plan year) $2,500 Individual NON- $5,000 Individual $5,000 Family $10,000 Family Unless otherwise indicated, the Deductible must be met prior to benefits being payable. All
PLAN FEATURES Deductible (per plan year) $2,500 Individual NON- $5,000 Individual $5,000 Family $10,000 Family Unless otherwise indicated, the Deductible must be met prior to benefits being payable. All
B l u e O p t i o n s F o r A d u l t s, F a m i l i e s, a n d C h i l d r e n
 2011 BlueOptions For Adults, Families, and Children BCP2808BR12/10 When choosing a health plan the first thing you want is plenty of choices. While that seems obvious, not every insurance company offers
2011 BlueOptions For Adults, Families, and Children BCP2808BR12/10 When choosing a health plan the first thing you want is plenty of choices. While that seems obvious, not every insurance company offers
Your Summary of Benefits PPO GenRx Plans
 Your Summary of Benefits PPO GenRx Plans Small Group PPO $25 Copay GenRx Plan Effective 10/2010 In addition to dollar and percentage copays, insureds are responsible for deductibles, as described below.
Your Summary of Benefits PPO GenRx Plans Small Group PPO $25 Copay GenRx Plan Effective 10/2010 In addition to dollar and percentage copays, insureds are responsible for deductibles, as described below.
PLAN DESIGN AND BENEFITS - NJ HMO HSA COMPATIBLE NO-REFERRAL 3.1 CALYR (OVR50%/UND50%)
") PLAN FEATURES Deductible (per calendar year) $2,500 Single Subscriber $5,000 Family Unless otherwise indicated, the Deductible must be met prior to benefits being payable. The Single Subscriber Deductible
PLAN FEATURES Deductible (per calendar year) $2,500 Single Subscriber $5,000 Family Unless otherwise indicated, the Deductible must be met prior to benefits being payable. The Single Subscriber Deductible
Covered 100% 20% 1 exam per 12 months for members age 18 and older.
 PLAN FEATURES NON- Deductible (per calendar year) $1,200 Individual $2,000 Individual $3,600 Family $6,000 Family All covered expenses, excluding prescription drugs, accumulate toward both the preferred
PLAN FEATURES NON- Deductible (per calendar year) $1,200 Individual $2,000 Individual $3,600 Family $6,000 Family All covered expenses, excluding prescription drugs, accumulate toward both the preferred
ROCHESTER INSTITUTE OF TECHNOLOGY Blue PPO (Pre-Medicare) 2019 Benefit Summary
 2019 Benefit Summary") ROCHESTER INSTITUTE OF TECHNOLOGY Blue PPO (Pre-Medicare) 2019 Benefit Summary The Blue PPO is available only to those who live outside the Rochester Area GENERAL INFORMATION Contacting the Carrier Voice:
ROCHESTER INSTITUTE OF TECHNOLOGY Blue PPO (Pre-Medicare) 2019 Benefit Summary The Blue PPO is available only to those who live outside the Rochester Area GENERAL INFORMATION Contacting the Carrier Voice:
PLAN DESIGN AND BENEFITS Standard PPO Plan
 North Carolina PPO (Mandated 1 Life Plan) PLAN DESIGN AND BENEFITS Standard PPO Plan PLAN FEATURES PARTICIPATING Deductible (per plan year) $500 Individual $1,000 Individual $1,500 Family $3,000 Family
North Carolina PPO (Mandated 1 Life Plan) PLAN DESIGN AND BENEFITS Standard PPO Plan PLAN FEATURES PARTICIPATING Deductible (per plan year) $500 Individual $1,000 Individual $1,500 Family $3,000 Family
PARTICIPATING PROVIDERS / REFERRED Deductible (per calendar year)
") Your HMO Plan Primary Care Physician - You choose a Primary Care Physician. The Aetna HMO Deductible provider network gives you access to a wide selection of Primary Care Physicians ( PCP's) and Specialists
Your HMO Plan Primary Care Physician - You choose a Primary Care Physician. The Aetna HMO Deductible provider network gives you access to a wide selection of Primary Care Physicians ( PCP's) and Specialists
PLAN DESIGN & BENEFITS MEDICAL PLAN PROVIDED BY AETNA LIFE INSURANCE COMPANY
 PLAN FEATURES IN-NETWORK OUT-OF-NETWORK Deductible (per calendar year) $500 Individual $1,000 Individual $1,000 Family $2,000 Family All covered expenses accumulate separately toward the preferred or non-preferred
PLAN FEATURES IN-NETWORK OUT-OF-NETWORK Deductible (per calendar year) $500 Individual $1,000 Individual $1,000 Family $2,000 Family All covered expenses accumulate separately toward the preferred or non-preferred
Unlimited except where indicated. Unlimited except where indicated. Primary Care Physician Selection
 PLAN FEATURES Deductible (per calendar year) $500 Individual $1,250 Individual $1,000 Family $2,500 Family All covered expenses excluding prescription drugs accumulate toward both the preferred and non-preferred
PLAN FEATURES Deductible (per calendar year) $500 Individual $1,250 Individual $1,000 Family $2,500 Family All covered expenses excluding prescription drugs accumulate toward both the preferred and non-preferred
Regence Preferred Plan Highlights For Groups of /1/2018
 Regence Preferred Highlights Features Provider choice: Members have direct access to their choice of providers. Coinsurance levels are lowest for Category 1 providers. If a member chooses a Category 3
Regence Preferred Highlights Features Provider choice: Members have direct access to their choice of providers. Coinsurance levels are lowest for Category 1 providers. If a member chooses a Category 3
PLAN COMPARISON (Blue Cross Blue Shield of Massachusetts) For Members Who Are Eligible For Medicare
 For Members Who Are Eligible For Medicare") Quarterly Premium Rate * Per Person $2,215.08 $1,789.50 $618.99 $890.70 Rates effective: 1/1/16 through 12/31/16 1/1/16 through 12/31/16 1/1/16 through 12/31/16 1/1/16 through 12/31/16 Eligibility Service
Quarterly Premium Rate * Per Person $2,215.08 $1,789.50 $618.99 $890.70 Rates effective: 1/1/16 through 12/31/16 1/1/16 through 12/31/16 1/1/16 through 12/31/16 1/1/16 through 12/31/16 Eligibility Service
PLAN COMPARISON (Blue Cross Blue Shield of Massachusetts) For Members Who Are Eligible For Medicare
 For Members Who Are Eligible For Medicare") Quarterly Premium Rate * Per Person $2,358.60 $1,905.33 $658.74 $1,165.11 Rates effective: 1/1/17 through 12/31/17 1/1/17 through 12/31/17 1/1/17 through 12/31/17 1/1/17 through 12/31/17 Eligibility Service
Quarterly Premium Rate * Per Person $2,358.60 $1,905.33 $658.74 $1,165.11 Rates effective: 1/1/17 through 12/31/17 1/1/17 through 12/31/17 1/1/17 through 12/31/17 1/1/17 through 12/31/17 Eligibility Service
Florida - EPO Aetna Select - ASC PLAN DESIGN & BENEFITS ADMINISTERED BY AETNA LIFE INSURANCE COMPANY PLAN FEATURES
 PLAN FEATURES Deductible (per calendar year) $100 Individual $200 Family Unless otherwise indicated, the Deductible must be met prior to benefits being payable. Pharmacy expenses do not apply towards the
PLAN FEATURES Deductible (per calendar year) $100 Individual $200 Family Unless otherwise indicated, the Deductible must be met prior to benefits being payable. Pharmacy expenses do not apply towards the
Your Summary of Benefits PPO Copay Plans
 Your Summary of Benefits PPO Copay Plans Small Group PPO $40 Copay Plan Effective 10/2010 In addition to dollar and percentage copays, members are responsible for deductibles, as described below. Members
Your Summary of Benefits PPO Copay Plans Small Group PPO $40 Copay Plan Effective 10/2010 In addition to dollar and percentage copays, members are responsible for deductibles, as described below. Members
PHYSICIAN SERVICES. $30 copay 1 1 You pay 50% $40 copay. You pay 0% 1 You pay 50% INPATIENT SERVICES OUTPATIENT SERVICES
 BENEFIT IN NETWORK OUT OF NETWORK This plan is intended to comply with the federal Patient Protection and Affordable Care Act. Provisions are subject to change as additional regulatory guidance becomes
BENEFIT IN NETWORK OUT OF NETWORK This plan is intended to comply with the federal Patient Protection and Affordable Care Act. Provisions are subject to change as additional regulatory guidance becomes
PLAN DESIGN & BENEFITS. $100 Individual/$200 Family $500 Individual/$1000 Family
 PLAN FEATURES Deductible (per calendar year) Provider None $1000 Individual/$2000 Family Deductible (per calendar year) Facility Level A: Level B: $100 Individual/$200 Family $500 Individual/$1000 Family
PLAN FEATURES Deductible (per calendar year) Provider None $1000 Individual/$2000 Family Deductible (per calendar year) Facility Level A: Level B: $100 Individual/$200 Family $500 Individual/$1000 Family
CA HMO Deductible $1,500 70%
 Your HMO Plan Primary Care Physician - You choose a Primary Care Physician. The Aetna HMO Deductible provider network gives you access to a wide selection of Primary Care Physicians ( PCP's) and Specialists
Your HMO Plan Primary Care Physician - You choose a Primary Care Physician. The Aetna HMO Deductible provider network gives you access to a wide selection of Primary Care Physicians ( PCP's) and Specialists
Preferred Personal Care Short-Term Health Insurance Stay Covered.
 Preferred Personal Care Short-Term Health Insurance Stay Covered. Administered by Preferred Personal Care Short-Term Health Insurance There are times when you need a health plan to fill in the gap: If
Preferred Personal Care Short-Term Health Insurance Stay Covered. Administered by Preferred Personal Care Short-Term Health Insurance There are times when you need a health plan to fill in the gap: If
Regence BluePoint Benefit Highlights
 Benefit Highlights 's features: Groups can choose from one of the following four networks for benefits: Participating Network, Preferred BlueOption Network, Preferred ValueCare Network, or Preferred FocalPoint
Benefit Highlights 's features: Groups can choose from one of the following four networks for benefits: Participating Network, Preferred BlueOption Network, Preferred ValueCare Network, or Preferred FocalPoint
IL Small Group MC Open Access Aetna Life Insurance Company Plan Effective Date: 04/01/2009 PLAN DESIGN AND BENEFITS- MC $1,500 80/50/50 (04/09)
") PLAN FEATURES Deductible (per calendar ) $1,500 Individual $3,000 Individual $4,500 Family $9,000 Family Unless otherwise indicated, the Deductible must be met prior to benefits being payable. All covered
PLAN FEATURES Deductible (per calendar ) $1,500 Individual $3,000 Individual $4,500 Family $9,000 Family Unless otherwise indicated, the Deductible must be met prior to benefits being payable. All covered
IMPORTANT NOTICE. Please read this information carefully and contact us at if you have any questions.
 PO Box 1090 Great Bend, KS 67530 Fax: (620) 793-1199 www.wship.org Questions? Call 1-800-877-5187 Preguntas? Teléfono 1-800-877-5187 November 2017 IMPORTANT NOTICE Re: - Basic Plan Premium Rate Change
PO Box 1090 Great Bend, KS 67530 Fax: (620) 793-1199 www.wship.org Questions? Call 1-800-877-5187 Preguntas? Teléfono 1-800-877-5187 November 2017 IMPORTANT NOTICE Re: - Basic Plan Premium Rate Change
OVERVIEW OF YOUR BENEFITS
 OVERVIEW OF YOUR BENEFITS 9 IMPORTANT PHONE NUMBERS Rochester Benefit Fund Office (585) 244-0830 For questions about eligibility, Coordination of Benefits, your 1199SEIU Health Benefits ID card, prescription
OVERVIEW OF YOUR BENEFITS 9 IMPORTANT PHONE NUMBERS Rochester Benefit Fund Office (585) 244-0830 For questions about eligibility, Coordination of Benefits, your 1199SEIU Health Benefits ID card, prescription
Regence ActiveCare Plan Highlights For Groups 51+ 1/1/17
 Plan Features Subscribers choose their Coordinated Network. Coordinated Network means a network of providers who integrate clinically in managing members' care. Ambulatory Surgical Center: While many surgical
Plan Features Subscribers choose their Coordinated Network. Coordinated Network means a network of providers who integrate clinically in managing members' care. Ambulatory Surgical Center: While many surgical
OPERATING ENGINEERS LOCAL324 Community Blue PPO Effective Date: 01/01/2016
 OPERATING ENGINEERS LOCAL324 Community Blue PPO 007005154 Effective Date: 01/01/2016 This is intended as an easy-to-read summary and provides only a general overview of your benefits. It is not a contract.
OPERATING ENGINEERS LOCAL324 Community Blue PPO 007005154 Effective Date: 01/01/2016 This is intended as an easy-to-read summary and provides only a general overview of your benefits. It is not a contract.
Your Plan: Anthem Silver PPO 3400/0%/3400 w/hsa Your Network: Anthem PPO
 Your Plan: Anthem Silver PPO 3400/0%/3400 w/hsa Your Network: Anthem PPO This summary of benefits is a brief outline of coverage, designed to help you with the selection process. This summary does not
Your Plan: Anthem Silver PPO 3400/0%/3400 w/hsa Your Network: Anthem PPO This summary of benefits is a brief outline of coverage, designed to help you with the selection process. This summary does not
ARUP Laboratories, Inc. EPO Medical 750 Plan Coverage Period: 01/01/ /31/2017
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.uhealthplan.utah.edu/aruplabs/ or by calling 1-888-271-5870.
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.uhealthplan.utah.edu/aruplabs/ or by calling 1-888-271-5870.
Covered 100%; deductible waived 40%; after deductible
 PLAN FEATURES IN-NETWORK OUT-OF-NETWORK Deductible (per calendar year) $500 Individual $1,000 Individual $1,500 Family $3,000 Family All covered expenses accumulate simultaneously toward both the preferred
PLAN FEATURES IN-NETWORK OUT-OF-NETWORK Deductible (per calendar year) $500 Individual $1,000 Individual $1,500 Family $3,000 Family All covered expenses accumulate simultaneously toward both the preferred
PLAN DESIGN & BENEFITS PROVIDED BY AETNA HEALTH INC. AND AETNA HEALTH INSURANCE COMPANY
 PLAN FEATURES IN-NETWORK OUT-OF-NETWORK Deductible $2,500 Individual $5,000 Individual (per calendar year) $5,000 Family $10,000 Family Unless otherwise indicated, the deductible must be met prior to benefits
PLAN FEATURES IN-NETWORK OUT-OF-NETWORK Deductible $2,500 Individual $5,000 Individual (per calendar year) $5,000 Family $10,000 Family Unless otherwise indicated, the deductible must be met prior to benefits
Model General Notice of COBRA Continuation Coverage Rights
 Model General Notice of COBRA Continuation Coverage Rights Introduction You re getting this notice because you recently gained coverage under a group health plan (the Plan). This notice has important information
Model General Notice of COBRA Continuation Coverage Rights Introduction You re getting this notice because you recently gained coverage under a group health plan (the Plan). This notice has important information
SUMMARY OF BENEFITS Fisk University Open Access Plus -BUY-UP PLAN Effective 10/1/2015 Customer Service:
 SUMMARY OF BENEFITS Fisk University Open Access Plus -BUY-UP PLAN Effective www.mycigna.com Customer Service: 866-494-2111 Cigna Health and Life Insurance Co. General Services In-Network Out-of-Network
SUMMARY OF BENEFITS Fisk University Open Access Plus -BUY-UP PLAN Effective www.mycigna.com Customer Service: 866-494-2111 Cigna Health and Life Insurance Co. General Services In-Network Out-of-Network
PrimeCare Physicians Plan - OAMC POS 3.2 (04/13) Easily locate PrimeCare participating providers at LEVEL 1:
 Easily locate PrimeCare participating providers at LEVEL 1:") PLAN FEATURES Network Easily locate PrimeCare participating providers at www.aetna.com/docfind/primecare ALL OTHER PrimeCare Physicians Plan NA Designated OAMC Network Providers Primary Care Physician
PLAN FEATURES Network Easily locate PrimeCare participating providers at www.aetna.com/docfind/primecare ALL OTHER PrimeCare Physicians Plan NA Designated OAMC Network Providers Primary Care Physician
General Notice of COBRA Continuation Coverage Rights. **Continuation Coverage Rights Under COBRA**
 General Notice of COBRA Continuation Coverage Rights **Continuation Coverage Rights Under COBRA** Introduction You are getting this notice because you recently gained coverage under The Vanguard Group,
General Notice of COBRA Continuation Coverage Rights **Continuation Coverage Rights Under COBRA** Introduction You are getting this notice because you recently gained coverage under The Vanguard Group,
DUKE UNIVERSITY DURHAM NC
 DUKE UNIVERSITY DURHAM NC Health Benefit Summary Plan Description 7670-00-140114 Revised 01-01-2017 BENEFITS ADMINISTERED BY Table of Contents INTRODUCTION... 1 PLAN INFORMATION... 2 SCHEDULE OF BENEFITS...
DUKE UNIVERSITY DURHAM NC Health Benefit Summary Plan Description 7670-00-140114 Revised 01-01-2017 BENEFITS ADMINISTERED BY Table of Contents INTRODUCTION... 1 PLAN INFORMATION... 2 SCHEDULE OF BENEFITS...
PLAN DESIGN AND BENEFITS AETNA LIFE INSURANCE COMPANY - Insured
 PLAN FEATURES Deductible (per calendar year) Individual $1,500 Family $3,000 All covered expenses accumulate simultaneously toward both the preferred and non-preferred Deductible. Unless otherwise indicated,
PLAN FEATURES Deductible (per calendar year) Individual $1,500 Family $3,000 All covered expenses accumulate simultaneously toward both the preferred and non-preferred Deductible. Unless otherwise indicated,
Aetna Health Inc. New Jersey Small Group QPOS Open Access
 PLAN FEATURES NETWORK Deductible (per calendar year) Not Applicable $1,000 Individual $2,000 Family Deductible applies to all covered expenses unless otherwise indicated. Once the Family Deductible is
PLAN FEATURES NETWORK Deductible (per calendar year) Not Applicable $1,000 Individual $2,000 Family Deductible applies to all covered expenses unless otherwise indicated. Once the Family Deductible is
Southern Healthcare Agency Field Employees Summary of Benefits Blue Cross Blue Shield of MS
 Southern Healthcare Agency Field Employees Summary of Benefits Blue Cross Blue Shield of MS Dual Option #1 Plan: Network Blue Deductible: $5000 Coinsurance: 70% Network/50% Non-Network Out of Pocket: $6450
Southern Healthcare Agency Field Employees Summary of Benefits Blue Cross Blue Shield of MS Dual Option #1 Plan: Network Blue Deductible: $5000 Coinsurance: 70% Network/50% Non-Network Out of Pocket: $6450
Version: 15/02/2017 [ TPID: ] Page 1
![Version: 15/02/2017 [ TPID: ] Page 1](/thumbs/88/117441870.jpg "Version: 15/02/2017 [ TPID: ] Page 1") PLAN FEATURES NETWORK CARE OUT-OF-NETWORK CARE Primary Care Physician Selection Not required Not required Deductible (per calendar year) $1,500 Individual $3,000 Family $3,000 Individual $9,000 Family
PLAN FEATURES NETWORK CARE OUT-OF-NETWORK CARE Primary Care Physician Selection Not required Not required Deductible (per calendar year) $1,500 Individual $3,000 Family $3,000 Individual $9,000 Family
Annual deductibles and maximums In-network Out-of-network Lifetime maximum
 SUMMARY OF BENEFITS City of Richmond & Richmond Public Schools (Plan B) Connecticut General Life Insurance Co. Annual deductibles and maximums Lifetime maximum Unlimited per individual Pre-Existing Condition
SUMMARY OF BENEFITS City of Richmond & Richmond Public Schools (Plan B) Connecticut General Life Insurance Co. Annual deductibles and maximums Lifetime maximum Unlimited per individual Pre-Existing Condition
Regence BluePoint 20/40 Plan Highlights For Groups of /1/2016
 Plan Features Provider choice: Members have direct access to their choice of providers. Coinsurance levels are lowest for In- Network providers. If a member chooses an Out-of-Network provider, the member
Plan Features Provider choice: Members have direct access to their choice of providers. Coinsurance levels are lowest for In- Network providers. If a member chooses an Out-of-Network provider, the member
Quote Effective: 04/01/ /30/2019 Version Updated: 01/07/2019
 Quote Effective: 04/01/2019-06/30/2019 Version Updated: 01/07/2019 Print Package: HIOS ID (Enrollment Code) 78124NY1000265-00 (SON5) Plan Name: Rating Region: Rate Rochester For the Benefits described
Quote Effective: 04/01/2019-06/30/2019 Version Updated: 01/07/2019 Print Package: HIOS ID (Enrollment Code) 78124NY1000265-00 (SON5) Plan Name: Rating Region: Rate Rochester For the Benefits described
Regence Innova Plan Highlights For Groups of /1/2016
 Regence Innova Highlights Features Provider choice: Members have direct access to their choice of providers. Coinsurance levels are lowest for providers. If a member chooses a Category 3 provider, the
Regence Innova Highlights Features Provider choice: Members have direct access to their choice of providers. Coinsurance levels are lowest for providers. If a member chooses a Category 3 provider, the
PLAN DESIGN & BENEFITS ADMINISTERED BY AETNA LIFE INSURANCE COMPANY - SELF FUNDED
 PLAN FEATURES IN-NETWORK ( OUT-OF-NETWORK (Non- Deductible (per plan year) $350 Individual $800 Individual $1,050 Family $2,400 Family All covered expenses accumulate separately toward the preferred or
PLAN FEATURES IN-NETWORK ( OUT-OF-NETWORK (Non- Deductible (per plan year) $350 Individual $800 Individual $1,050 Family $2,400 Family All covered expenses accumulate separately toward the preferred or