SUMMARY OF MATERIAL MODIFICATION TO THE SUMMARY PLAN DESCRIPTION OF THE MEDICAL BENEFITS UNDER THE UTICA COLLEGE HEALTH BENEFITS PLAN
|
|
|
- Lorena Morgan
- 5 years ago
- Views:
Transcription
1 SUMMARY OF MATERIAL MODIFICATION TO THE SUMMARY PLAN DESCRIPTION OF THE MEDICAL BENEFITS UNDER THE UTICA COLLEGE HEALTH BENEFITS PLAN This Summary of Material Modification describes changes, to the Summary Plan Description of the Medical Benefits under the Utica College Health Benefits Plan (the Plan ). After reading it, you should attach it to your copy of the Summary Plan Description. 1. Effective as of January 1, 2017, the Excellus BluePPO Plan, Excellus BluePPO Plan Signature Deduct 3 No Deductible Preventative Rx, and Excellus BluePPO Plan Signature Deduct 3 plans are offered. See the attached Benefit Summaries. 2. Effective as of January 1, 2017, the Answer to Question 4 in the Summary Plan Description What are the special enrollment periods? is changed as follows: Generally, the special enrollment periods allow employees who satisfy the eligibility requirements explained in the Answer to Question 1 to enroll in Plan coverage in the following situations: The employee initially declined Plan coverage because he had other health care coverage, but he later loses that other coverage through no fault of his own. The employee can enroll himself, his spouse (or eligible domestic partner) and eligible children. He must complete the enrollment form within thirty (30) days after losing the other health care coverage. Note, in order for this special enrollment rule to apply, at the time the employee initially declines Plan coverage he must provide, in writing, his reason for declining it. The employee initially declined Plan coverage because he had other health care coverage from another employer, but that employer stops contributing toward the cost of that other coverage. The employee can enroll himself, his spouse (or eligible domestic partner) and eligible children. The employee must complete the enrollment form within thirty (30) days after that employer stops contributing toward the cost of the other coverage. Note, in order for this special enrollment rule to apply, at the time he initially declines Plan coverage he must provide, in writing, his reason for declining it. 1 Copyright 2017 Lifetime Benefit Solutions, Inc.
2 The employee declined Plan coverage and he later acquires a new spouse (or eligible domestic partner) or a new eligible child (through birth or adoption of a child). The employee can enroll himself, his spouse (or eligible domestic partner) and eligible children. The employee must complete the enrollment form within thirty (30) days after the marriage, birth, adoption or placement for adoption. The employee, his spouse (or eligible domestic partner) or eligible children lose eligibility for Medicaid coverage or coverage under a State Children s Health Insurance Program. The employee must complete the enrollment form within sixty (60) days after the loss of that coverage. The employee, his spouse (or eligible domestic partner) or eligible children become eligible to participate in a premium assistance program under Medicaid or a State Children s Health Insurance Program. The employee must complete the enrollment form within sixty (60) days after that eligibility determination. 3. Effective as of January 1, 2017, the answer to Question and Answer 5 in the Summary Plan Description How much must participants pay for Plan coverage? is changed as follows. If there are ordinary increases or decreases in the premium, your payroll deductions will automatically be adjusted to reflect any change in your cost. Following is the current cost for this coverage. The Employer will provide participants with advance written notice of any changes to their cost. Medical Option Monthly Rate Employee Cost Employer Share Excellus PPO Single $1, $ $ Employee + 1 $2, $ $1, Family $2, $ $2, HealthyBlue Single $ $ $ Employee + 1 $1, $ $ Family $1, $ $1, Copyright 2017 Lifetime Benefit Solutions, Inc.
3 Medical Option Monthly Rate Employee Cost Employer Share Single $ $ $ Employee + 1 $1, $ $1, Family $1, $ $1, The explanation of COBRA Continuation Coverage beginning on page 22 of the Summary Plan Description in the Answer to Question 17 What additional rights does a participant have? is changed as follows: COBRA Continuation Coverage This section has important information about your right to COBRA continuation coverage, which is a temporary extension of coverage under the Plan. It explains COBRA continuation coverage, when it may become available to you and your family, and what you need to do to protect your right to get it. When you become eligible for COBRA, you may also become eligible for other coverage options that may cost less than COBRA continuation coverage. The right to COBRA continuation coverage was created by a federal law, the Consolidated Omnibus Budget Reconciliation Act of 1985 (COBRA). COBRA continuation coverage can become available to you and other members of your family when group health coverage would otherwise end. For more information about your rights and obligations under the Plan and under federal law contact the Plan Administrator. You may have other options available to you when you lose group health coverage. For example, you may be eligible to buy an individual plan through the Health Insurance Marketplace. By enrolling in coverage through the Marketplace, you may qualify for lower costs on your monthly premiums and lower out-ofpocket costs. Additionally, you may qualify for a 30-day special enrollment period for another group health plan for which you are eligible (such as a spouse s plan), even if that plan generally doesn t accept late enrollees. What is COBRA continuation coverage? COBRA continuation coverage is a continuation of Plan coverage when it would otherwise end because of a life event. This is also called a qualifying event. Specific qualifying events are listed below. After a qualifying event, COBRA continuation coverage must be offered to each person who is a qualified beneficiary. You, your spouse, and your dependent children could become 3 Copyright 2017 Lifetime Benefit Solutions, Inc.
4 qualified beneficiaries if coverage under the Plan is lost because of the qualifying event. Under the Plan, qualified beneficiaries who elect COBRA continuation coverage must pay for COBRA continuation coverage. If you re an employee, you ll become a qualified beneficiary if you lose your coverage under the Plan because of the following qualifying events: (1) Your hours of employment are reduced; or (2) Your employment ends for any reason other than your gross misconduct. If you re the spouse of an employee, you ll become a qualified beneficiary if you lose your coverage under the Plan because of the following qualifying events: (1) Your spouse dies; (2) Your spouse's hours of employment are reduced; (3) Your spouse's employment ends for any reason other than his or her gross misconduct; (4) Your spouse becomes enrolled in Medicare (Part A, Part B, or both); or (5) You become divorced or legally separated from your spouse. Your dependent children will become qualified beneficiaries if they lose coverage under the Plan because of the following qualifying events: (1) The parent-employee dies; (2) The parent-employee's hours of employment are reduced; (3) The parent-employee's employment ends for any reason other than his or her gross misconduct; (4) The parent-employee becomes enrolled in Medicare (Part A, Part B, or both); (5) The parents become divorced or legally separated; or (6) The child stops being eligible for coverage under the Plan as a dependent child. Sometimes, filing a proceeding in bankruptcy under title 11 of the United States Code can be a qualifying event. If a proceeding in bankruptcy is filed with respect to the Employer and that bankruptcy results in the loss of any retired employee s coverage under the Plan, the retired employee is a qualified beneficiary. The retired employee's spouse, surviving spouse, and dependent children will also be qualified beneficiaries if bankruptcy results in the loss of their coverage under the Plan. 4 Copyright 2017 Lifetime Benefit Solutions, Inc.
5 When is COBRA continuation coverage available? The Plan will offer COBRA continuation coverage to qualified beneficiaries only after the Plan Administrator has been notified that a qualifying event has occurred. The Employer must notify the Plan Administrator of the following qualifying events. The end of employment or reduction of hours of employment; Death of the employee; Commencement of a proceeding in bankruptcy with respect to the employer; or The employee s becoming entitled to Medicare benefits (under Part A, Part B, or both). For all other qualifying events (divorce or legal separation of the employee and spouse or a child's losing eligibility for coverage as a dependent child), you must notify the Plan Administrator within 60 days after the qualifying event occurs. You must provide this notice to: Benefits Coordinator, Utica College, 1600 Burrstone Road, Utica, New York, The notice must be in writing, and must contain your name and address, the name and address of any affected persons, a description of the qualifying event, and the date of the qualifying event. You may be asked to provide additional documentation or information after you have submitted the notice. How is COBRA continuation coverage provided? Once the Plan Administrator receives notice that a qualifying event has occurred, COBRA continuation coverage will be offered to each qualified beneficiary. Each qualified beneficiary will have an independent right to elect COBRA continuation coverage. Covered employees may elect COBRA continuation coverage on behalf of their spouses, and parents may elect COBRA continuation coverage on behalf of their children. COBRA continuation coverage is a temporary continuation of coverage that generally lasts for 18 months due to employment termination or reduction of hours of work. Certain qualifying events, or a second qualifying event during the initial period of coverage, may permit a beneficiary to receive a maximum of 36 months of coverage. 5 Copyright 2017 Lifetime Benefit Solutions, Inc.
6 There are also ways in which this 18-month period of COBRA continuation coverage can be extended: Disability extension of 18-month period of continuation coverage If you or anyone in your family covered under the Plan is determined by the Social Security Administration ( SSA ) to be disabled and you provide proper and timely notice of the SSA determination, you and your entire family may be entitled to get up to an additional 11 months of COBRA coverage, for a maximum of 29 months. The disability would have to have started at some time before the 60th day of COBRA continuation coverage and must last at least until the end of the 18-month period of COBRA continuation coverage. You must provide this notice to the Benefits Coordinator, Utica College, 1600 Burrstone Road, Utica, New York, within 60 days of the date of the SSA determination and before the end of the 18-month period of COBRA continuation coverage. The notice must be in writing, and must contain your name and address, the name and address of the disabled qualified beneficiary, and the date the disability was determined to have begun. You must also attach a copy of the SSA determination. You may be asked to provide additional documentation or information after you have submitted the notice. Second qualifying event extension of 18-month period of continuation coverage If your family experiences another qualifying event during the 18 months of COBRA continuation coverage, the spouse and dependent children in your family can get up to 18 additional months of COBRA continuation coverage, for a maximum of 36 months, if the Plan is properly notified of the second qualifying event. This extension may be available to the spouse and any dependent children getting COBRA continuation coverage if the employee or former employee dies, becomes entitled to Medicare benefits (under Part A, Part B, or both); gets divorced or legally separated; or if the child stops being eligible under the Plan as a dependent child. This extension is only available if the second qualifying event would have caused the spouse or dependent child to lose coverage under the Plan had the first qualifying event not occurred. You must provide this notice to the Benefits Coordinator, Utica College, 1600 Burrstone Road, Utica, New York, within 60 days after the second qualifying event. The notice must be in writing, and must contain your name and address, the name and address of any affected persons, a description of the second qualifying event, and the date of the second qualifying event. You may be asked to provide additional documentation or information after you have submitted the notice. 6 Copyright 2017 Lifetime Benefit Solutions, Inc.
7 Are there other coverage options besides COBRA continuation coverage? Yes. Instead of enrolling in COBRA continuation coverage, there may be other coverage options for you and your family through the Health Insurance Marketplace, Medicaid, or other group health plan coverage options (such as a spouse s plan) through what is called a special enrollment period. Some of these options may cost less than COBRA continuation coverage. You can learn more about many of these options at If You Have Questions Questions concerning your Plan or your COBRA continuation coverage rights should be addressed to the contact or contacts identified below. For more information about your rights under the Employee Retirement Income Security Act (ERISA), including COBRA, the Patient Protection and Affordable Care Act, and other laws affecting group health plans, contact the nearest Regional or District Office of the U.S. Department of Labor's Employee Benefits Security Administration (EBSA) in your area or visit (Addresses and phone numbers of Regional and District EBSA Offices are available through EBSA's website.) For more information about the Marketplace, visit Keep your Plan informed of address changes To protect your family's rights, let the Plan Administrator know about any changes in the addresses of family members. You should also keep a copy, for your records, of any notices you send to the Plan Administrator. Plan contact information Information about the Plan and COBRA continuation coverage can be obtained from: Utica College Health Benefits Plan Benefits Coordinator Utica College 1600 Burrstone Road Utica, New York (315) Copyright 2017 Lifetime Benefit Solutions, Inc.
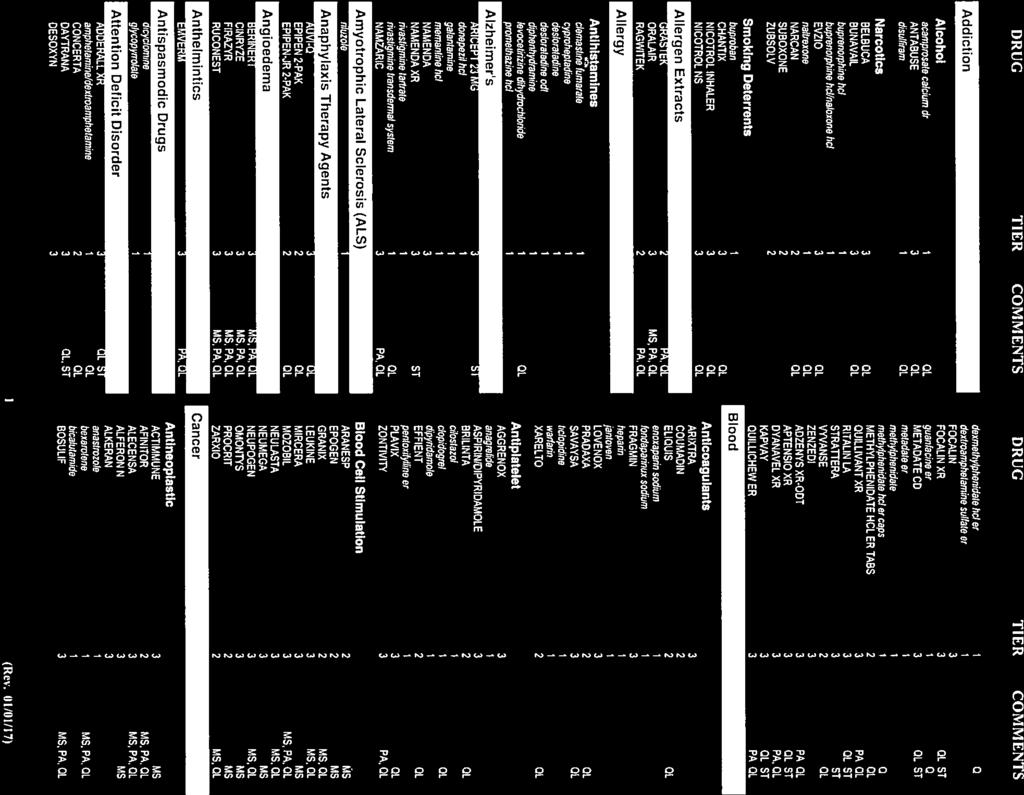
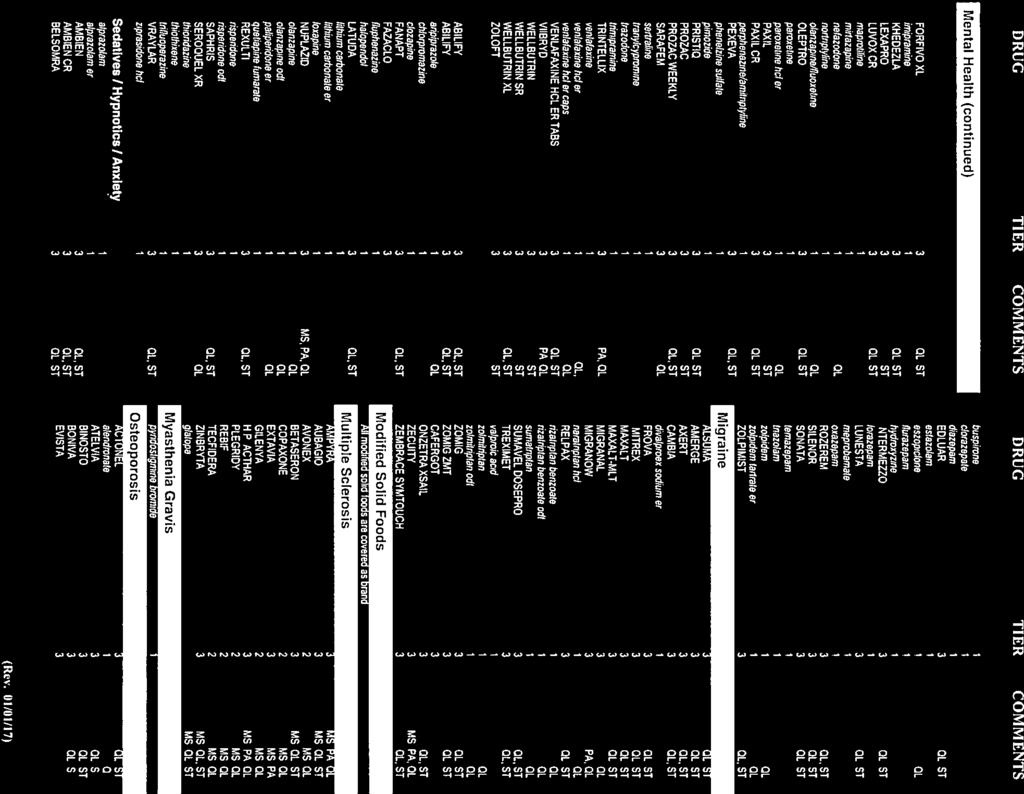
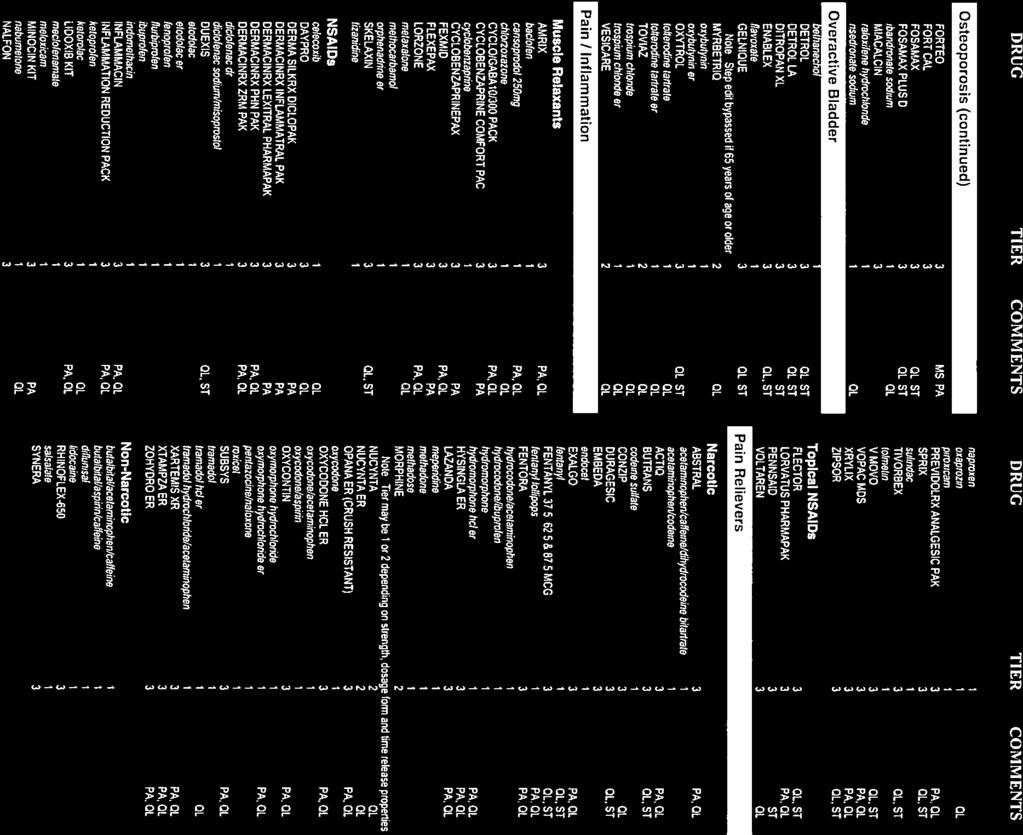
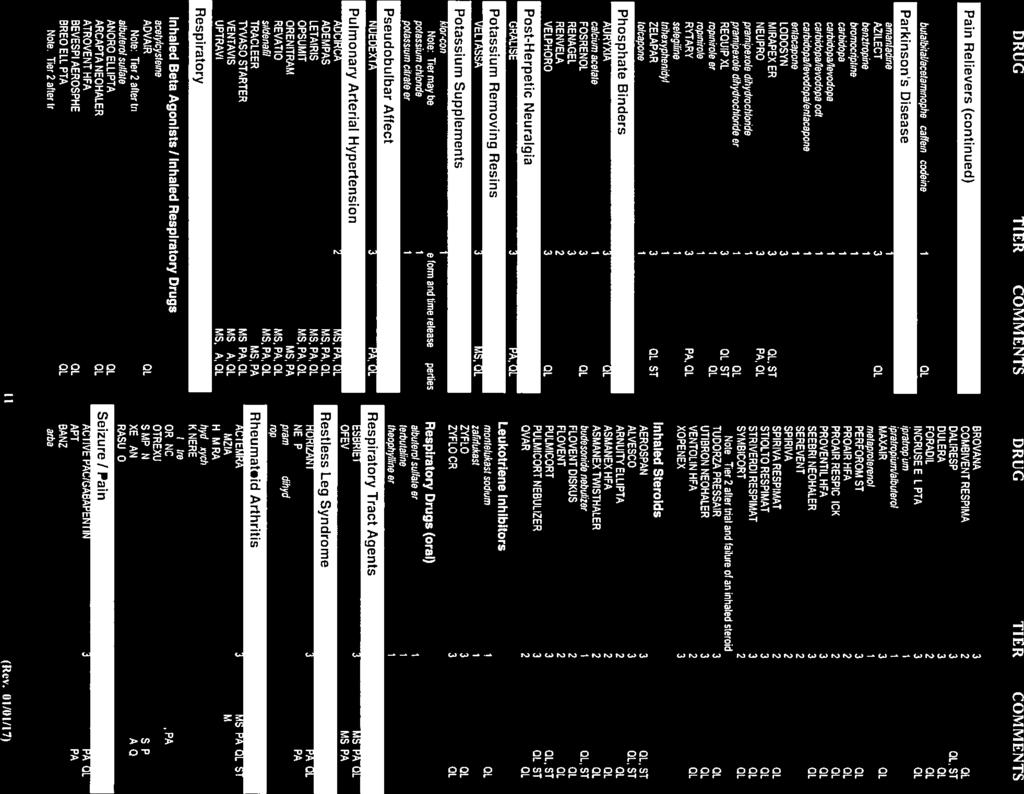
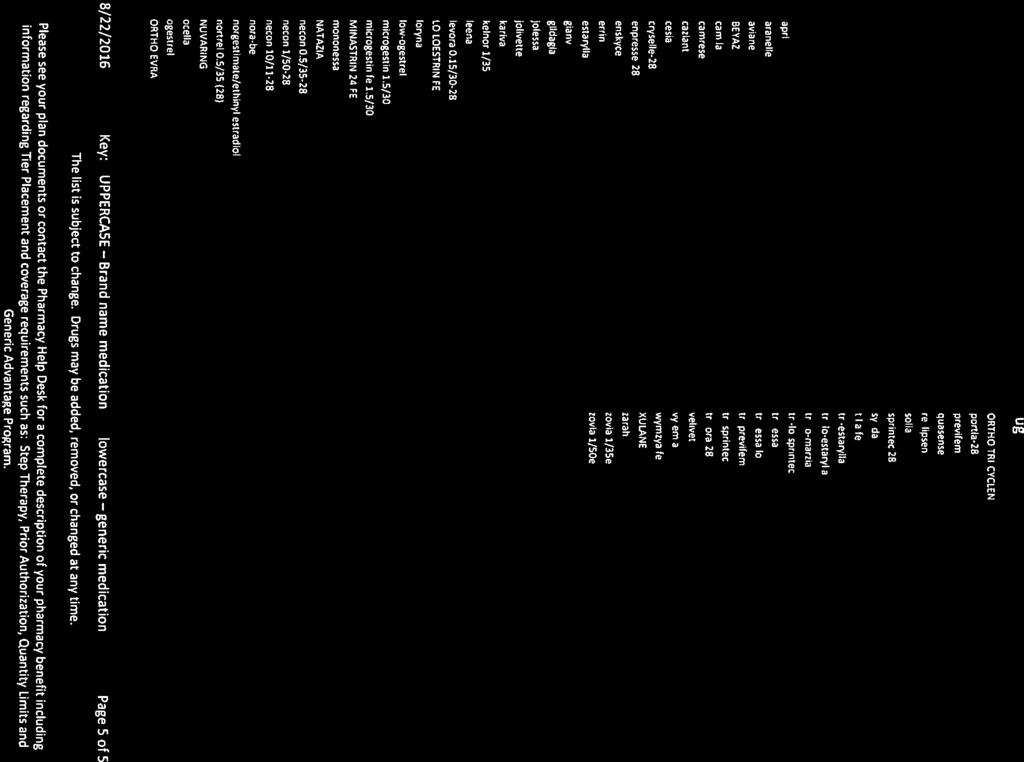
8 Refer to the attached 2017 Excellus BlueCross BlueShield 3-Tier Formulary Guide and Preventative Drug List. To access current Participating Provider information (free of charge), go to the following website: Excellus BlueCross BlueShield Upon request, copies of the provider lists will be furnished to you, without charge, as a separate document. 8 Copyright 2017 Lifetime Benefit Solutions, Inc.
9 Excellus BluePPO $5/$15/$30 Benefit Time Period: 01/01/ /31/2017 UTICA COLLEGE General Information Cost Sharing Expenses Deductible - Single $0 $750 Deductible - Family $0 $2,250 Each individual does not exceed the single deductible. 0% 30% Annual Out of Pocket Maximum - Single $4,200 $4,200 Annual Out of Pocket Maximum - Family $12,600 $12,600 Out-of-pocket maximums accumulate coinsurance, copays and the deductible. Out-ofpocket maximums exclude balances over allowable expense and non-covered services. Out-of-pocket maximums accumulate coinsurance, copays and the deductible. Out-ofpocket maximums exclude balances over allowable expense and non-covered services. Office Visit Cost Shares Cost Share - Primary Care Cost Share - Specialist $20 Copayment $20 Copayment Plan Limits Plan/Calendar Year Diabetic Preauthorization and Step Therapy Calendar Year Benefits Yes Who is Covered Domestic Partner Coverage Covered 1 of /29/ :12:38
10 Inpatient Services Inpatient Facility Inpatient Hospital Services Mental Health Care Substance Use Detoxification Skilled Nursing Facility Covered in Covered in Covered in Covered in Physical Rehabilitation Covered in Covered in Maternity Care Covered in 45 Days Per Year Limits are combined INN and OON. 60 Days per year Limits are combined INN and OON. Inpatient Professional Services Inpatient Hospital Surgery Anesthesia Includes anesthesia rendered for Inpatient, Outpatient, Office Visit, and Maternity services. Anesthesia does not require a preauth or referral. Outpatient Facility Services Outpatient Facility Services SurgiCenters and Freestanding Ambulatory Centers Surgical Care Diagnostic X-ray Diagnostic Laboratory and Pathology Radiation Therapy Chemotherapy $20 Copayment $20 Copayment Covered in Covered in Covered in Infusion Therapy Inclusive of Primary Service Inclusive of Primary Service Dialysis Mental Health Care Substance Use Care Covered in $20 Copayment $20 Copayment Advanced Imaging Services includes PET scans, MRI, nuclear medicine, and CAT scans. Is inclusive in the Home Care benefit and not covered as a separate benefit. Includes Partial Hospitalization Includes Partial Hospitalization Home and Hospice Care Home Care Home Care Covered in 25% Subject to $50 Deductible Limits are combined INN and OON. 2 of /29/ :12:38
11 Hospice Care Hospice Care Inpatient Covered in Outpatient and Office Professional Services Professional Services Office Surgery Diagnostic X-ray Diagnostic Laboratory and Pathology Radiation Therapy Chemotherapy Infusion Therapy Dialysis Mental Health Care Maternity Care TeleMedicine Program Chiropractic Care Allergy Testing Allergy Treatment Including Serum Hearing Evaluations Routine PCP/Specialist - $20 Copayment PCP/Specialist - $20 Copayment PCP/Specialist - Inclusive of Primary Service PCP/Specialist - $20 Copayment PCP/Specialist - $10 Copayment PCP/Specialist - $20 Copayment PCP/Specialist - $20 Copayment Inclusive of Primary Service Not Covered PCP/Specialist - Not Covered Not Covered Is inclusive in the Home Care benefit and not covered as a separate benefit. Covers online internet consultations between the member and the providers who participate in our telemedicine program for medical conditions that are not an emergency condition. Allergy Testing includes injections and scratch and prick tests. Includes desensitization treatments (injections & serums). Not Covered Limits are combined INN and OON. Rehab and Habilitation Outpatient Facility Physical Rehabilitation Occupational Rehabilitation Speech Rehabilitation $20 Copayment $20 Copayment $20 Copayment 45 Visits per year Includes aggregate of visits for INN and OON and professional and facility covered services for physical, speech, and occupational therapy. 45 Visits per year 45 Visits per year 3 of /29/ :12:38
12 Outpatient Professional Services Physical Rehabilitation Occupational Rehabilitation Speech Rehabilitation PCP/Specialist - $20 Copayment PCP/Specialist - $20 Copayment PCP/Specialist - $20 Copayment 45 Visits per year Includes aggregate of visits for INN and OON and professional and facility covered services for physical, speech, and occupational therapy. 45 Visits per year 45 Visits per year Preventive Services Preventive Professional Services Meeting Federal Guidelines* Adult Physical Examination Adult Immunizations Well Child Visits and Immunizations Routine GYN Visit Pre/Post-Natal Care Mammography Screening Professional Colonoscopy Screening Professional Bone Density Screening Professional Not Covered Covered in 1 Exam per year Preventive Facility Services Meeting Federal Guidelines* Cervical Cytology Preventative Mammography Screening Facility Colonoscopy Screening Facility Bone Density Screening Facility Covered in Covered in Covered in Covered in Preventive services in addition to those required under Federal Guidelines - Professional Prostate Cancer Screening Mammography Screening Professional Colonoscopy Screening Professional Bone Density Screening Professional PCP/Specialist - $20 Copayment PCP/Specialist - $20 Copayment 4 of /29/ :12:38
13 Preventive services in addition to those required under Federal Guidelines - Facility Mammography Screening Facility Colonoscopy Screening Facility Bone Density Screening Facility Covered in $20 Copayment $20 Copayment Other Benefits Additional Benefits Treatment of Diabetes Insulin and Supplies Diabetic Equipment Durable Medical Equipment (DME) Medical Supplies Acupuncture PCP/Specialist - $20 Copayment PCP/Specialist - $20 Copayment PCP/Specialist - 20% PCP/Specialist - 20% PCP/Specialist - Not Covered Not Covered Private Duty Nursing PCP/Specialist - Not Covered Not Covered Not Covered Limited to a 30 day supply for retail pharmacy or a 90 day supply for mail order pharmacy. Not Covered Limits combined INN and OON. Emergency Services ER Facility Facility Emergency Room Visit $50 Copayment $50 Copayment Prior Authorization may not apply to any emergency care services. Emergency services are covered worldwide if provided by a hospital facility. Transportation Prehospital Emergency and Transportation - Ground or Water $20 Copayment $20 Copayment Urgent Care Urgent Care Center Facility Visit $25 Copayment 5 of /29/ :12:38
14 Ancillary Benefits Vision Adult Eye Exams - Routine $20 Copayment Adult Eyewear - Routine Not Covered Not Covered Pediatric Eye Exams - Routine $20 Copayment Pediatric Eyewear - Routine Not Covered Not Covered 1 Exam per calendar year Limits are combined INN and OON. Not Covered Includes Frames/Lenses or Contact Lenses 1 Exam per calendar year Limits are combined INN and OON. Not Covered Includes Frames/Lenses or Contact Lenses Rx Benefits Rx Plan Rx Plan $5/$15/$30 Rx Benefits Days Supply Per Retail Order 30 Days Supply Per Mail Order 90 Copays Per Mail Order Supply 2 This document is not a contract. It is only intended to highlight the coverage of this program. Benefits are determined by the terms of the contract. Any inconsistencies between this document and the contract shall be resolved in favor of the contract in effect at the time services are rendered. All benefits are subject to medical necessity. All day and visit limits are combined limits for both in and out of network benefits. * For non-grandfathered groups, Preventive Services coverage required by the Patient Protection and Affordable Care Act are not quoted herein. Please refer to the United States Preventive Services Task Force list of items and services rated "A" or "B" that are covered pursuant to the Patient Protection and Affordable Care Act requirements. 6 of /29/ :12:38
15 Excellus BluePPO Signature Deduct 3 $5/$35/$70, $0 gen for kids Integrated Rx, No Ded Prev Rx Benefit Time Period: 01/01/ /31/2017 UTICA COLLEGE General Information Cost Sharing Expenses Deductible - Single $1,800 $3,600 Deductible - Family $3,600 $7,200 10% 20% Annual Out of Pocket Maximum - Single $3,600 $7,200 Annual Out of Pocket Maximum - Family $7,200 $14,400 Annual Out of Pocket Maximum - Per Person Cap $6,550 $14,400 Out-of-pocket maximums accumulate coinsurance, copays and the deductible. Out-ofpocket maximums exclude balances over allowable expense and non-covered services. Out-of-pocket maximums accumulate coinsurance, copays and the deductible. Out-ofpocket maximums exclude balances over allowable expense and non-covered services. The Out-of-Pocket Maximum Per Person Cap includes deductible, coinsurance, copays and prescription drugs. If a member under a family contract meets the Out-Of-Pocket Maximum Per Person Cap amount, the individual will no longer pay for covered services and claims will be paid at 100% of the allowable amount by the Health Plan for the remainder of the plan year. The remaining annual out-of-pocket maximum still needs to be met by any combination of family members on the contract before claims are paid at 100% for the whole family. Office Visit Cost Shares Cost Share - Primary Care Cost Share - Specialist Plan Limits Plan/Calendar Year Diabetic Preauthorization and Step Therapy Calendar Year Benefits Yes Who is Covered Domestic Partner Coverage Covered 1 of /02/ :46:36
16 Inpatient Services Inpatient Facility Inpatient Hospital Services Mental Health Care Substance Use Detoxification Skilled Nursing Facility Physical Rehabilitation Maternity Care 45 Days per contract year Limits are combined INN and OON. 60 Days per year Limits are combined INN and OON. Inpatient Professional Services Inpatient Hospital Surgery Anesthesia Subject to $1,800 Deductible Includes anesthesia rendered for Inpatient, Outpatient, Office Visit, and Maternity services. Anesthesia does not require a preauth or referral. Outpatient Facility Services Outpatient Facility Services SurgiCenters and Freestanding Ambulatory Centers Surgical Care Diagnostic X-ray Diagnostic Laboratory and Pathology Radiation Therapy Chemotherapy Infusion Therapy Inclusive of Primary Service Inclusive of Primary Service Dialysis Mental Health Care Substance Use Care Is inclusive in the Home Care benefit and not covered as a separate benefit. Includes Partial Hospitalization Includes Partial Hospitalization Home and Hospice Care Home Care Home Care Hospice Care 2 of /02/ :46:36
17 Hospice Care Inpatient Outpatient and Office Professional Services Professional Services Office Surgery Diagnostic X-ray Diagnostic Laboratory and Pathology Radiation Therapy Chemotherapy Infusion Therapy Dialysis Mental Health Care Maternity Care TeleMedicine Program Chiropractic Care Allergy Testing Allergy Treatment Including Serum Hearing Evaluations Routine PCP/Specialist - Inclusive of Primary Service Inclusive of Primary Service Not Covered Is inclusive in the Home Care benefit and not covered as a separate benefit. Covers online internet consultations between the member and the providers who participate in our telemedicine program for medical conditions that are not an emergency condition. Allergy Testing includes injections and scratch and prick tests. Includes desensitization treatments (injections & serums). 1 Exam per contract year Limits are combined INN and OON. 3 of /02/ :46:36
18 Rehab and Habilitation Outpatient Facility Physical Rehabilitation Occupational Rehabilitation Speech Rehabilitation 45 Visits per contract year Includes aggregate of visits for INN and OON and professional and facility covered services for physical, speech, and occupational therapy. 45 Visits per contract year 45 Visits per contract year Outpatient Professional Services Physical Rehabilitation Occupational Rehabilitation Speech Rehabilitation 45 Visits per contract year Includes aggregate of visits for INN and OON and professional and facility covered services for physical, speech, and occupational therapy. 45 Visits per contract year 45 Visits per contract year Preventive Services Preventive Professional Services Meeting Federal Guidelines* Adult Physical Examination Adult Immunizations Well Child Visits and Immunizations Routine GYN Visit Pre/Post-Natal Care Mammography Screening Professional Colonoscopy Screening Professional Bone Density Screening Professional Covered in 1 Exam per year Preventive Facility Services Meeting Federal Guidelines* Cervical Cytology Preventative Mammography Screening Facility Colonoscopy Screening Facility Covered in Covered in Covered in 4 of /02/ :46:36
19 Bone Density Screening Facility Covered in Preventive services in addition to those required under Federal Guidelines - Professional Prostate Cancer Screening Mammography Screening Professional Colonoscopy Screening Professional Bone Density Screening Professional Preventive services in addition to those required under Federal Guidelines - Facility Mammography Screening Facility Colonoscopy Screening Facility Bone Density Screening Facility Covered in Covered in Other Benefits Additional Benefits Treatment of Diabetes Insulin and Supplies Diabetic Equipment Durable Medical Equipment (DME) Medical Supplies Acupuncture PCP/Specialist - Not Covered Not Covered Not Covered Private Duty Nursing PCP/Specialist - Not Covered Not Covered Not Covered Limited to a 90 day supply for retail pharmacy or a 90 day supply for mail order pharmacy. Emergency Services ER Facility Facility Emergency Room Visit Subject to $1,800 Deductible Prior Authorization may not apply to any Emergency services are covered worldwide if provided by a hospital facility. 5 of /02/ :46:36
20 Transportation Prehospital Emergency and Transportation - Ground or Water Subject to $1,800 Deductible Urgent Care Urgent Care Center Facility Visit Ancillary Benefits Vision Adult Eye Exams - Routine 1 exam per contract year Adult Eyewear - Routine Not Covered Not Covered Not Covered Pediatric Eye Exams - Routine 1 exam per contract year Pediatric Eyewear - Routine Not Covered Not Covered Not Covered Rx Benefits Rx Plan Rx Plan $5/$35/$70, $0 gen for kids Integrated Rx, No Ded Prev Rx Rx Benefits Days Supply Per Retail Order 30 Days Supply Per Mail Order 90 Copays Per Mail Order Supply 2 This document is not a contract. It is only intended to highlight the coverage of this program. Benefits are determined by the terms of the contract. Any inconsistencies between this document and the contract shall be resolved in favor of the contract in effect at the time services are rendered. All benefits are subject to medical necessity. All day and visit limits are combined limits for both in and out of network benefits. * For non-grandfathered groups, Preventive Services coverage required by the Patient Protection and Affordable Care Act are not quoted herein. Please refer to the United States Preventive Services Task Force list of items and services rated "A" or "B" that are covered pursuant to the Patient Protection and Affordable Care Act requirements. 6 of /02/ :46:36
21 Excellus BluePPO Signature Deduct 3 $5/$35/$70, $0 gen for kids Integrated Rx Benefit Time Period: 01/01/ /31/2017 Utica College General Information Cost Sharing Expenses Deductible - Single $1,800 $3,600 Deductible - Family $3,600 $7,200 10% 20% Annual Out of Pocket Maximum - Single $3,600 $7,200 Annual Out of Pocket Maximum - Family $7,200 $14,400 Annual Out of Pocket Maximum - Per Person Cap $6,550 $14,400 Out-of-pocket maximums accumulate coinsurance, copays and the deductible. Out-ofpocket maximums exclude balances over allowable expense and non-covered services. Out-of-pocket maximums accumulate coinsurance, copays and the deductible. Out-ofpocket maximums exclude balances over allowable expense and non-covered services. The Out-of-Pocket Maximum Per Person Cap includes deductible, coinsurance, copays and prescription drugs. If a member under a family contract meets the Out-Of-Pocket Maximum Per Person Cap amount, the individual will no longer pay for covered services and claims will be paid at 100% of the allowable amount by the Health Plan for the remainder of the plan year. The remaining annual out-of-pocket maximum still needs to be met by any combination of family members on the contract before claims are paid at 100% for the whole family. Office Visit Cost Shares Cost Share - Primary Care Cost Share - Specialist Plan Limits Plan/Calendar Year Diabetic Preauthorization and Step Therapy Calendar Year Benefits Yes Who is Covered Domestic Partner Coverage Covered 1 of /04/ :13:18
22 Inpatient Services Inpatient Facility Inpatient Hospital Services Mental Health Care Substance Use Detoxification Skilled Nursing Facility Physical Rehabilitation Maternity Care 45 Days per contract year Limits are combined INN and OON. 60 Days per year Limits are combined INN and OON. Inpatient Professional Services Inpatient Hospital Surgery Anesthesia Subject to $1,800 Deductible Includes anesthesia rendered for Inpatient, Outpatient, Office Visit, and Maternity services. Anesthesia does not require a preauth or referral. Outpatient Facility Services Outpatient Facility Services SurgiCenters and Freestanding Ambulatory Centers Surgical Care Diagnostic X-ray Diagnostic Laboratory and Pathology Radiation Therapy Chemotherapy Infusion Therapy Inclusive of Primary Service Inclusive of Primary Service Dialysis Mental Health Care Substance Use Care Is inclusive in the Home Care benefit and not covered as a separate benefit. Includes Partial Hospitalization Includes Partial Hospitalization Home and Hospice Care Home Care Home Care Hospice Care 2 of /04/ :13:18
23 Hospice Care Inpatient Outpatient and Office Professional Services Professional Services Office Surgery Diagnostic X-ray Diagnostic Laboratory and Pathology Radiation Therapy Chemotherapy Infusion Therapy Dialysis Mental Health Care Maternity Care TeleMedicine Program Chiropractic Care Allergy Testing Allergy Treatment Including Serum Hearing Evaluations Routine PCP/Specialist - Inclusive of Primary Service Inclusive of Primary Service Not Covered Is inclusive in the Home Care benefit and not covered as a separate benefit. Covers online internet consultations between the member and the providers who participate in our telemedicine program for medical conditions that are not an emergency condition. Allergy Testing includes injections and scratch and prick tests. Includes desensitization treatments (injections & serums). 1 Exam per contract year Limits are combined INN and OON. 3 of /04/ :13:18
24 Rehab and Habilitation Outpatient Facility Physical Rehabilitation Occupational Rehabilitation Speech Rehabilitation 45 Visits per contract year Includes aggregate of visits for INN and OON and professional and facility covered services for physical, speech, and occupational therapy. 45 Visits per contract year 45 Visits per contract year Outpatient Professional Services Physical Rehabilitation Occupational Rehabilitation Speech Rehabilitation 45 Visits per contract year Includes aggregate of visits for INN and OON and professional and facility covered services for physical, speech, and occupational therapy. 45 Visits per contract year 45 Visits per contract year Preventive Services Preventive Professional Services Meeting Federal Guidelines* Adult Physical Examination Adult Immunizations Well Child Visits and Immunizations Routine GYN Visit Pre/Post-Natal Care Mammography Screening Professional Colonoscopy Screening Professional Bone Density Screening Professional Covered in 1 Exam per year Preventive Facility Services Meeting Federal Guidelines* Cervical Cytology Preventative Mammography Screening Facility Colonoscopy Screening Facility Covered in Covered in Covered in 4 of /04/ :13:18
25 Bone Density Screening Facility Covered in Preventive services in addition to those required under Federal Guidelines - Professional Prostate Cancer Screening Mammography Screening Professional Colonoscopy Screening Professional Bone Density Screening Professional Preventive services in addition to those required under Federal Guidelines - Facility Mammography Screening Facility Colonoscopy Screening Facility Bone Density Screening Facility Covered in Covered in Other Benefits Additional Benefits Treatment of Diabetes Insulin and Supplies Diabetic Equipment Durable Medical Equipment (DME) Medical Supplies Limited to a 90 day supply for retail pharmacy or a 90 day supply for mail order pharmacy. Acupuncture PCP/Specialist - Not Covered Not Covered Private Duty Nursing PCP/Specialist - Not Covered Not Covered Not Covered Emergency Services ER Facility Facility Emergency Room Visit Subject to $1,800 Deductible Prior Authorization may not apply to any Emergency services are covered worldwide if provided by a hospital facility. 5 of /04/ :13:18
26 Transportation Prehospital Emergency and Transportation - Ground or Water Subject to $1,800 Deductible Urgent Care Urgent Care Center Facility Visit Ancillary Benefits Vision Adult Eye Exams - Routine 1 exam per contract year Adult Eyewear - Routine Not Covered Not Covered Not Covered Pediatric Eye Exams - Routine 1 exam per contract year Pediatric Eyewear - Routine Not Covered Not Covered Not Covered Rx Benefits Rx Plan Rx Plan $5/$35/$70, $0 gen for kids Integrated Rx Rx Benefits Days Supply Per Retail Order 30 Days Supply Per Mail Order 90 Copays Per Mail Order Supply 2 This document is not a contract. It is only intended to highlight the coverage of this program. Benefits are determined by the terms of the contract. Any inconsistencies between this document and the contract shall be resolved in favor of the contract in effect at the time services are rendered. All benefits are subject to medical necessity. All day and visit limits are combined limits for both in and out of network benefits. * For non-grandfathered groups, Preventive Services coverage required by the Patient Protection and Affordable Care Act are not quoted herein. Please refer to the United States Preventive Services Task Force list of items and services rated "A" or "B" that are covered pursuant to the Patient Protection and Affordable Care Act requirements. 6 of /04/ :13:18
27
28
29
30
31
32
33
34
35
36
37
38
39
40
41
42
43

44
45
46
47

48
49
50
51
52

53
54

55

56
57
58
59
Simply Blue HDHP. General Information ROCHESTER REGIONAL HEALTH SYSTEM. Cost Sharing Expenses
 ROCHESTER REGIONAL HEALTH SYSTEM Simply Blue HDHP $10/$30/$50 Subj. to Ded. Dom. $25/$50/$90 Subj. to Ded, No Ded Prev Rx Benefit Time Period: 01/01/2019-12/31/2019 General Cost Sharing Expenses Deductible
ROCHESTER REGIONAL HEALTH SYSTEM Simply Blue HDHP $10/$30/$50 Subj. to Ded. Dom. $25/$50/$90 Subj. to Ded, No Ded Prev Rx Benefit Time Period: 01/01/2019-12/31/2019 General Cost Sharing Expenses Deductible
Quote Effective: 04/01/ /30/2019 Version Updated: 01/07/2019
 Quote Effective: 04/01/2019-06/30/2019 Version Updated: 01/07/2019 Print Package: HIOS ID (Enrollment Code) 78124NY1000265-00 (SON5) Plan Name: Rating Region: Rate Rochester For the Benefits described
Quote Effective: 04/01/2019-06/30/2019 Version Updated: 01/07/2019 Print Package: HIOS ID (Enrollment Code) 78124NY1000265-00 (SON5) Plan Name: Rating Region: Rate Rochester For the Benefits described
Important Questions Answers Why this Matters: What is the overall deductible? Are there other deductibles for specific services?
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.empireblue.com or by calling 1-800-342-9816. Important
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.empireblue.com or by calling 1-800-342-9816. Important
Group Name. South Seneca School District
 Group Name South Seneca School District Excellus BlueCross BlueShield makes finding the information and support you need easier resources, savings, and tools are available online 24/7. Find a doctor or
Group Name South Seneca School District Excellus BlueCross BlueShield makes finding the information and support you need easier resources, savings, and tools are available online 24/7. Find a doctor or
SUPRO: 2018 SCHEDULE OF BENEFITS - EMPLOYEE COST SHARING
 SU Pro (In- and Out-of-) In - Out -of- Cost Sharing Definitions Annual Deductible 1 Coinsurance Annual Out-of-Pocket Maximum 2 $200 per individual with a maximum of $400 for a family 5% of allowable amount
SU Pro (In- and Out-of-) In - Out -of- Cost Sharing Definitions Annual Deductible 1 Coinsurance Annual Out-of-Pocket Maximum 2 $200 per individual with a maximum of $400 for a family 5% of allowable amount
ROCHESTER INSTITUTE OF TECHNOLOGY Blue PPO (Pre-Medicare) 2019 Benefit Summary
 2019 Benefit Summary") ROCHESTER INSTITUTE OF TECHNOLOGY Blue PPO (Pre-Medicare) 2019 Benefit Summary The Blue PPO is available only to those who live outside the Rochester Area GENERAL INFORMATION Contacting the Carrier Voice:
ROCHESTER INSTITUTE OF TECHNOLOGY Blue PPO (Pre-Medicare) 2019 Benefit Summary The Blue PPO is available only to those who live outside the Rochester Area GENERAL INFORMATION Contacting the Carrier Voice:
$15 copay $25 copay. - Silver&Fit copays are not included in the Annual Out-Of- Pocket Maximum
 Prepared for Dundee Central School Effective: 01/01/2018 Plan Feature Highlights Annual deductible None $250 Annual out-of-pocket maximum (medical services only, does not include prescription drugs) $1,250
Prepared for Dundee Central School Effective: 01/01/2018 Plan Feature Highlights Annual deductible None $250 Annual out-of-pocket maximum (medical services only, does not include prescription drugs) $1,250
SUBLUE AND SUORANGE: 2018 SCHEDULE OF BENEFITS -EMPLOYEE COST SHARING
 Cost Sharing Definitions Annual Deductible 1 (amounts are not cumulative across levels) $100 per individual with a maximum of $250 for a family $300 per individual with a maximum of $1,000 for a family
Cost Sharing Definitions Annual Deductible 1 (amounts are not cumulative across levels) $100 per individual with a maximum of $250 for a family $300 per individual with a maximum of $1,000 for a family
Healthy New York Summary of Benefits
 Healthy New York Summary of Benefits Services Hospital Services Skilled Nursing Facility Surgery Anesthesia Diagnostic X-ray Diagnostic Laboratory and Pathology Chemotherapy Radiation Therapy Surgical
Healthy New York Summary of Benefits Services Hospital Services Skilled Nursing Facility Surgery Anesthesia Diagnostic X-ray Diagnostic Laboratory and Pathology Chemotherapy Radiation Therapy Surgical
Table of Contents. Health Benefit Plans. Staying Healthy. Family & Money Matters. Employee Discounts. Monthly Resident Rates
 House Staff 2014 Loyola benefits Table of Contents Health Benefit Plans Your Health Care Plan Options...2 Eligibility...3-4 COBRA...5-9 Staying Healthy Medical Plans... 10-21 Prescription Drug Benefit...22
House Staff 2014 Loyola benefits Table of Contents Health Benefit Plans Your Health Care Plan Options...2 Eligibility...3-4 COBRA...5-9 Staying Healthy Medical Plans... 10-21 Prescription Drug Benefit...22
$15 copay $25 copay. in a specialist office. - Silver&Fit copays are not included in the Annual Out-Of- Pocket Maximum
 Prepared for Genesee Area Healthcare Plan Effective: 01/01/2019 Plan Feature Highlights Annual deductible None $250 Annual out-of-pocket maximum (medical services only, does not include prescription drugs)
Prepared for Genesee Area Healthcare Plan Effective: 01/01/2019 Plan Feature Highlights Annual deductible None $250 Annual out-of-pocket maximum (medical services only, does not include prescription drugs)
Trinity Health - Syracuse HSA - Ind Excellus BCBS: Excellus BluePPO Signature Deduct 3
 Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Trinity Health - Syracuse HSA - Ind Excellus BCBS: Excellus BluePPO Signature Deduct 3 Coverage Period: 01/01/2019-12/31/2019
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Trinity Health - Syracuse HSA - Ind Excellus BCBS: Excellus BluePPO Signature Deduct 3 Coverage Period: 01/01/2019-12/31/2019
Medical EPO Plan Schedule of Benefits (Effective January 01, 2019) JHH/JHHSC Non-Union and Union Employees and Eligible Dependents
 JHH/JHHSC Non-Union and Union Employees and Eligible Dependents") Plan Year Deductible Out-of-Pocket Maximum Lifetime Maximum Hopkins Preferred Network Provider EHP Network Provider Individual $500 $500 Family $1000 $1000 Individual $3000 (combined with EHP Network)
Plan Year Deductible Out-of-Pocket Maximum Lifetime Maximum Hopkins Preferred Network Provider EHP Network Provider Individual $500 $500 Family $1000 $1000 Individual $3000 (combined with EHP Network)
Medical PPO Plan Schedule of Benefits (Effective January 01, 2019) Bayview Non-Union and Union Employees and Eligible Dependents
 Bayview Non-Union and Union Employees and Eligible Dependents") Plan Year Deductible Out-of-Pocket Maximum Lifetime Maximum Individual Family Individual Family Hopkins Preferred Network Provider EHP Network Provider Out of Network Provider $150 (under $50K) / $200
Plan Year Deductible Out-of-Pocket Maximum Lifetime Maximum Individual Family Individual Family Hopkins Preferred Network Provider EHP Network Provider Out of Network Provider $150 (under $50K) / $200
Empire BlueCross WSWHE Counties Health Insurance Consortium Trust: HRA Coverage Period: 07/01/ /30/2015
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.empireblue.com or by calling 1-800-342-9816. * Health
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.empireblue.com or by calling 1-800-342-9816. * Health
Even though you pay these expenses, they don t count toward the out-ofpocket limit.
 Anthem HealthKeepers Premier POS: Henrico County General Government and Public Schools Coverage Period: 1/1/2017-12/31/2017 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage
Anthem HealthKeepers Premier POS: Henrico County General Government and Public Schools Coverage Period: 1/1/2017-12/31/2017 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage
You don't have to meet deductibles for specific services.
 Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Excellus BCBS: Excellus BluePPO A nonprofit independent licensee of the BlueCross BlueShield Association The
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Excellus BCBS: Excellus BluePPO A nonprofit independent licensee of the BlueCross BlueShield Association The
Medical Schedule of Benefits (Effective January 01, 2016) Johns Hopkins Bayview Medical Center Non-Union and Union Employees and Eligible Dependents
 Johns Hopkins Bayview Medical Center Non-Union and Union Employees and Eligible Dependents") Plan Year Deductible Out-of-Pocket Maximum Lifetime Maximum EHP Network Provider Out of Network Provider Hopkins Preferred Network Provider Individual $100 $750 $0 Family $200 $1500 $0 Individual $2000
Plan Year Deductible Out-of-Pocket Maximum Lifetime Maximum EHP Network Provider Out of Network Provider Hopkins Preferred Network Provider Individual $100 $750 $0 Family $200 $1500 $0 Individual $2000
PEIA PPB Plan A Benefits At a Glance
 PEIA PPB Plan A Benefits At a Glance Benefit Description PEIA PPB Plan A In-Network PEIA PPB Plan A Out-of-Network Annual deductible Varies by salary and employer type. See premium charts. Twice the in-network
PEIA PPB Plan A Benefits At a Glance Benefit Description PEIA PPB Plan A In-Network PEIA PPB Plan A Out-of-Network Annual deductible Varies by salary and employer type. See premium charts. Twice the in-network
Trinity Health - Syracuse Essential Excellus BCBS: Signature Hybrid 5
 Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Trinity Health - Syracuse Essential Excellus BCBS: Signature Hybrid 5 Coverage Period: 01/01/2019-12/31/2019
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Trinity Health - Syracuse Essential Excellus BCBS: Signature Hybrid 5 Coverage Period: 01/01/2019-12/31/2019
Health care benefits for your on demand life.
 Health care benefits for your on demand life. Classic Blue BTD Broome Boces Plan features Primary Care Physician (PCP) and coinsurance Referrals Not required Out of network benefits Covered Out of area
Health care benefits for your on demand life. Classic Blue BTD Broome Boces Plan features Primary Care Physician (PCP) and coinsurance Referrals Not required Out of network benefits Covered Out of area
Model General Notice of COBRA Continuation Coverage Rights
 Model General Notice of COBRA Continuation Coverage Rights Introduction You re getting this notice because you recently gained coverage under a group health plan (the Plan). This notice has important information
Model General Notice of COBRA Continuation Coverage Rights Introduction You re getting this notice because you recently gained coverage under a group health plan (the Plan). This notice has important information
Medical EPO Plan Schedule of Benefits (Effective January 01, 2019) Howard County General Hospital/TCAS Employees and Eligible Dependents
 Howard County General Hospital/TCAS Employees and Eligible Dependents") Plan Year Deductible Out-of-Pocket Maximum Lifetime Maximum Hopkins Affiliated Facility Network (facility charges only) EHP Network Provider Individual $500 $500 Family $1000 $1000 Individual $3000 (combined
Plan Year Deductible Out-of-Pocket Maximum Lifetime Maximum Hopkins Affiliated Facility Network (facility charges only) EHP Network Provider Individual $500 $500 Family $1000 $1000 Individual $3000 (combined
Schedule of Benefits (GR-9N-S DE)
") Schedule of Benefits (GR-9N-S-01-001-01 DE) Plan Sponsor: The Church of Jesus Christ of Latter-Day Saints-Senior Missionaries Group Policy Number: 840232 Issue Date: June 3, 2013 Effective Date: August
Schedule of Benefits (GR-9N-S-01-001-01 DE) Plan Sponsor: The Church of Jesus Christ of Latter-Day Saints-Senior Missionaries Group Policy Number: 840232 Issue Date: June 3, 2013 Effective Date: August
Medical Schedule of Benefits (Effective January 01, December 31, 2017) Johns Hopkins University Employees and Eligible Dependents
 Johns Hopkins University Employees and Eligible Dependents") Plan Year Deductible Out-of-Pocket Maximum Lifetime Maximum EHP Network Provider Out of Network Provider Individual $250 $500 Family $750 $1500 Individual $2000 $4000 Family $6000 $12000 Unlimited Acupuncture
Plan Year Deductible Out-of-Pocket Maximum Lifetime Maximum EHP Network Provider Out of Network Provider Individual $250 $500 Family $750 $1500 Individual $2000 $4000 Family $6000 $12000 Unlimited Acupuncture
PLAN DESIGN AND BENEFITS - IN MANAGED CHOICE POS OPEN ACCESS 90/60/60 $1,000 PREFERRED CARE
 PLAN FEATURES NON- Deductible (per calendar year) $1,000 Individual $2,000 Individual $2,000 Family $4,000 Family Unless otherwise indicated, the Deductible must be met prior to benefits being payable.
PLAN FEATURES NON- Deductible (per calendar year) $1,000 Individual $2,000 Individual $2,000 Family $4,000 Family Unless otherwise indicated, the Deductible must be met prior to benefits being payable.
Important Questions Answers Why This Matters:
 Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/2018 12/31/2018 : Roper St. Francis Flex Plan Coverage for: Individual or Family Plan
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/2018 12/31/2018 : Roper St. Francis Flex Plan Coverage for: Individual or Family Plan
SCHEDULE OF BENEFITS UNIVERSITY OF PITTSBURGH PPO PLAN - Applies to PA Child Welfare Resource Center
 SCHEDULE OF BENEFITS UNIVERSITY OF PITTSBURGH PPO PLAN - Applies to PA Child Welfare Resource Center The following Schedule of Benefits is part of your Certificate of Coverage. It sets forth benefit limits
SCHEDULE OF BENEFITS UNIVERSITY OF PITTSBURGH PPO PLAN - Applies to PA Child Welfare Resource Center The following Schedule of Benefits is part of your Certificate of Coverage. It sets forth benefit limits
Benefits Summary Direct HMO / HMO For Groups with 2-50 Eligible Employees (Eff. 10/01/10, Pending NYS Dept. of Insurance Approval)
") Copayment Options 1 Inpatient Copayment Primary (PCP) Copayment Specialist Copayment ER Copayment Option 12 copayment* copayment 1 $50 copayment 1 $150 copayment *Per admission/maximum per calendar year
Copayment Options 1 Inpatient Copayment Primary (PCP) Copayment Specialist Copayment ER Copayment Option 12 copayment* copayment 1 $50 copayment 1 $150 copayment *Per admission/maximum per calendar year
CROUSE HOSPITAL - Select Plan Excellus BCBS: Excellus BluePPO
 Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services CROUSE HOSPITAL - Select Plan Excellus BCBS: Excellus BluePPO Coverage Period: 01/01/2019-12/31/2019 A nonprofit
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services CROUSE HOSPITAL - Select Plan Excellus BCBS: Excellus BluePPO Coverage Period: 01/01/2019-12/31/2019 A nonprofit
Standard Option Medical Schedule of Benefits (Effective January 01, 2018) Suburban Hospital Employees and Eligible Dependents
 Suburban Hospital Employees and Eligible Dependents") Plan Year Deductible Out-of-Pocket Maximum Lifetime Maximum EHP Network Provider Out of Network Provider Suburban Hospital (facility charges only) Individual $400 $750 $0 Family $800 $1500 $0 Individual
Plan Year Deductible Out-of-Pocket Maximum Lifetime Maximum EHP Network Provider Out of Network Provider Suburban Hospital (facility charges only) Individual $400 $750 $0 Family $800 $1500 $0 Individual
Schedule of Benefits. Plan Information. Member Cost Sharing
 Schedule of Benefits Panther Gold Plan - Enhanced Access HMO Applies to Bradford, Johnstown and Greensburg campuses only HMO Deductible: $0 / $0 Coinsurance: 0% Total Annual Out-of-Pocket: $1,800 / $3,600
Schedule of Benefits Panther Gold Plan - Enhanced Access HMO Applies to Bradford, Johnstown and Greensburg campuses only HMO Deductible: $0 / $0 Coinsurance: 0% Total Annual Out-of-Pocket: $1,800 / $3,600
SCHEDULE OF BENEFITS ADVANTAGE PANTHER GOLD PLAN Enhanced Access HMO Applies to Oakland, Johnstown, and Titusville campuses
 SCHEDULE OF BENEFITS ADVANTAGE PANTHER GOLD PLAN Enhanced Access HMO Applies to Oakland, Johnstown, and Titusville campuses This document is called a Schedule of Benefits. It is part of your Certificate
SCHEDULE OF BENEFITS ADVANTAGE PANTHER GOLD PLAN Enhanced Access HMO Applies to Oakland, Johnstown, and Titusville campuses This document is called a Schedule of Benefits. It is part of your Certificate
Coverage for: Individual Plan Type: PPO. Important Questions Answers Why this Matters:
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.mypomco.com or by calling 1-888-201-5150. Includes amendments
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.mypomco.com or by calling 1-888-201-5150. Includes amendments
Important Questions Answers Why this Matters:
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document by calling 1-585-343-0055 ext. 6415. Important Questions Answers
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document by calling 1-585-343-0055 ext. 6415. Important Questions Answers
Medical Benefits Comparison Book 2018 Medicare Retirees in the Rochester Area
 Medical Benefits Comparison Book 2018 Medicare Retirees in the Rochester Area Human Resources Finance & Administration Rochester Institute of Technology Medical Benefit Comparison This information provides
Medical Benefits Comparison Book 2018 Medicare Retirees in the Rochester Area Human Resources Finance & Administration Rochester Institute of Technology Medical Benefit Comparison This information provides
Medical Schedule of Benefits (Effective July 01, June 30, 2019) Johns Hopkins Student Health Program
 Johns Hopkins Student Health Program") Plan Year Deductible Out-of-Pocket Maximum Lifetime Maximum EHP Network Provider Out of Network Provider Individual $150 $150 Family $450 $450 Individual $3000 $3000 Family $9000 $9000 Unlimited Acupuncture
Plan Year Deductible Out-of-Pocket Maximum Lifetime Maximum EHP Network Provider Out of Network Provider Individual $150 $150 Family $450 $450 Individual $3000 $3000 Family $9000 $9000 Unlimited Acupuncture
Blue Cross Blue Shield of Kansas Blue Choice Comprehensive Major Medical Program
 Blue Cross Blue Shield of Kansas Blue Choice Comprehensive Major Medical Program ESSDACK HEALTH INSURANCE GROUP Effective October 1, 2010 through September 30, 2011 Stephanie Buckman Group Enrollment Representative
Blue Cross Blue Shield of Kansas Blue Choice Comprehensive Major Medical Program ESSDACK HEALTH INSURANCE GROUP Effective October 1, 2010 through September 30, 2011 Stephanie Buckman Group Enrollment Representative
Standard Option Medical Schedule of Benefits (Effective January 01, 2017) Suburban Hospital Employees and Eligible Dependents
 Suburban Hospital Employees and Eligible Dependents") Plan Year Deductible Out-of-Pocket Maximum Lifetime Maximum EHP Network Provider Out of Network Provider Suburban Hospital (facility charges only) Individual $400 $750 $0 Family $800 $1500 $0 Individual
Plan Year Deductible Out-of-Pocket Maximum Lifetime Maximum EHP Network Provider Out of Network Provider Suburban Hospital (facility charges only) Individual $400 $750 $0 Family $800 $1500 $0 Individual
Medical Schedule of Benefits (Effective July 01, June 30, 2018) Johns Hopkins Student Health Program
 Johns Hopkins Student Health Program") Plan Year Deductible Out-of-Pocket Maximum Lifetime Maximum EHP Network Provider Out of Network Provider Individual $150 $150 Family $450 $450 Individual $3000 $3000 Family $9000 $9000 Unlimited Acupuncture
Plan Year Deductible Out-of-Pocket Maximum Lifetime Maximum EHP Network Provider Out of Network Provider Individual $150 $150 Family $450 $450 Individual $3000 $3000 Family $9000 $9000 Unlimited Acupuncture
Important Questions Answers Why this Matters:
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.anthem.com or by calling 1-855-603-7982. Important Questions
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.anthem.com or by calling 1-855-603-7982. Important Questions
Other Participating UPMC Facilities Level 2 Benefit Period
 Schedule of Benefits Advantage Panther Gold Plan - Enhanced Access HMO Applies to Oakland and Titusville campuses HMO Deductible: $0 / $0 Coinsurance: 0% Total Annual Out-of-Pocket: $1,800 / $3,600 Primary
Schedule of Benefits Advantage Panther Gold Plan - Enhanced Access HMO Applies to Oakland and Titusville campuses HMO Deductible: $0 / $0 Coinsurance: 0% Total Annual Out-of-Pocket: $1,800 / $3,600 Primary
HOW THE MEDICAL PLANS COMPARE
 HOW THE MEDICAL PLANS COMPARE FEATURE Cigna and UPMC High Deductible Health Plans (HDHP) Cigna Open Access Plus (OAP) UPMC Health Plan Organization (EPO) Type of Plan With a High Deductible Health Plan/Health
HOW THE MEDICAL PLANS COMPARE FEATURE Cigna and UPMC High Deductible Health Plans (HDHP) Cigna Open Access Plus (OAP) UPMC Health Plan Organization (EPO) Type of Plan With a High Deductible Health Plan/Health
Important Questions Answers Why this Matters:
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.soundhealthwellness.com or by calling 1-800-225-7620.
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.soundhealthwellness.com or by calling 1-800-225-7620.
OVERVIEW OF YOUR BENEFITS
 OVERVIEW OF YOUR BENEFITS 9 IMPORTANT PHONE NUMBERS Rochester Benefit Fund Office (585) 244-0830 For questions about eligibility, Coordination of Benefits, your 1199SEIU Health Benefits ID card, prescription
OVERVIEW OF YOUR BENEFITS 9 IMPORTANT PHONE NUMBERS Rochester Benefit Fund Office (585) 244-0830 For questions about eligibility, Coordination of Benefits, your 1199SEIU Health Benefits ID card, prescription
What is the overall deductible?
 Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 7/1/2018 6/30/2019 WEA Trust Essential Health Plan: Kenosha School District Coverage for: Individual/Family
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 7/1/2018 6/30/2019 WEA Trust Essential Health Plan: Kenosha School District Coverage for: Individual/Family
University of Cincinnati Medical Plan Summary and Comparison Non AAUP - Effective January 1- December 31, 2018
 Annual Deductible Annual Health Savings Account Funding (UC) $1500 individual $3,000 family Varies by Annual Base Pay as of 1/1/18 $3,000 per person $6,000 family Varies by Annual Base Pay as of 1/1/18
Annual Deductible Annual Health Savings Account Funding (UC) $1500 individual $3,000 family Varies by Annual Base Pay as of 1/1/18 $3,000 per person $6,000 family Varies by Annual Base Pay as of 1/1/18
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: Beginning on or after 1/1/2019
 Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: Beginning on or after 1/1/2019 Kalamazoo College, G-1013: Orange Plan Coverage for: Covered
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: Beginning on or after 1/1/2019 Kalamazoo College, G-1013: Orange Plan Coverage for: Covered
SCHEDULE OF BENEFITS UPMC HEALTH PLAN PA CHILD WELFARE RESOURCE PPO
 SCHEDULE OF BENEFITS UPMC HEALTH PLAN PA CHILD WELFARE RESOURCE PPO This document is called a Schedule of Benefits. It is part of your Certificate of Coverage or your Summary Plan Description. Your Schedule
SCHEDULE OF BENEFITS UPMC HEALTH PLAN PA CHILD WELFARE RESOURCE PPO This document is called a Schedule of Benefits. It is part of your Certificate of Coverage or your Summary Plan Description. Your Schedule
Important Questions Answers Why this Matters:
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at https://eoc.empireblue.com/eocdps/fi or by calling 1-855-220-3341.
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at https://eoc.empireblue.com/eocdps/fi or by calling 1-855-220-3341.
Schedule of Benefits. Plan Information Participating Provider Non-Participating Provider
 Schedule of Benefits Panther Basic HSA PPO - Premium Network Deductible: $1,500 / $3,000 Coinsurance: 30% Total Annual Out-of-Pocket: $5,000 / $10,000 Primary Care Provider: 30% after Deductible Specialist:
Schedule of Benefits Panther Basic HSA PPO - Premium Network Deductible: $1,500 / $3,000 Coinsurance: 30% Total Annual Out-of-Pocket: $5,000 / $10,000 Primary Care Provider: 30% after Deductible Specialist:
You don t have to meet deductibles for specific services, but see the chart starting on page 2 for other costs for services this plan covers.
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document by calling 1-866-497-5711. Important Questions Answers Why this
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document by calling 1-866-497-5711. Important Questions Answers Why this
2018 Employee Benefits Overview
 2018 Employee Benefits Overview www.ncmmhcbenefits.info Employee Benefits We recognize that our employees are our most valuable resource and your benefits program is extremely important to North Central
2018 Employee Benefits Overview www.ncmmhcbenefits.info Employee Benefits We recognize that our employees are our most valuable resource and your benefits program is extremely important to North Central
General Notice of COBRA Continuation Coverage Rights. ** Continuation Coverage Rights Under COBRA**
 General Notice of COBRA Continuation Coverage Rights ** Continuation Coverage Rights Under COBRA** Introduction You re getting this notice because you recently gained coverage under a group health plan
General Notice of COBRA Continuation Coverage Rights ** Continuation Coverage Rights Under COBRA** Introduction You re getting this notice because you recently gained coverage under a group health plan
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 1/1/19 12/31/19
 Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 1/1/19 12/31/19 Toledo Electrical Welfare Fund : Plan M Medicare Supplement Coverage for: Individual/Family
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 1/1/19 12/31/19 Toledo Electrical Welfare Fund : Plan M Medicare Supplement Coverage for: Individual/Family
Coverage Period: 01/01/ /31/2018 A nonprofit independent licensee of the BlueCross BlueShield Association
 Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Excellus BCBS: Essential Plan 2 Coverage Period: 01/01/2018-12/31/2018 A nonprofit independent licensee of the
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Excellus BCBS: Essential Plan 2 Coverage Period: 01/01/2018-12/31/2018 A nonprofit independent licensee of the
Marsh and McLennan: Anthem Blue Cross and Blue Shield $2,850 Deductible Plan Coverage Period: 01/01/ /31/2017
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at https://eoc.anthem.com/eocdps/aso or by calling (855) 570-1150.
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at https://eoc.anthem.com/eocdps/aso or by calling (855) 570-1150.
Maine's Choice HSA HMO 5000 Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services
 Maine Maine's Choice HSA HMO 5000 Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/2018 12/31/2018 Coverage for: Individual + Family Plan
Maine Maine's Choice HSA HMO 5000 Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/2018 12/31/2018 Coverage for: Individual + Family Plan
Important Questions Answers Why this Matters:
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.summacare.com or by calling 1-800-996-8701. Important
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.summacare.com or by calling 1-800-996-8701. Important
California Small Group MC Aetna Life Insurance Company NETWORK CARE
 PLAN FEATURES Deductible (per calendar year) Unless otherwise indicated, the Deductible must be met prior to benefits being payable. All covered expenses accumulate toward the preferred and non-preferred
PLAN FEATURES Deductible (per calendar year) Unless otherwise indicated, the Deductible must be met prior to benefits being payable. All covered expenses accumulate toward the preferred and non-preferred
01/01/ /31/2019 UMR: PALO PINTO GENERAL HOSPITAL:
 Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/2019 12/31/2019 UMR: PALO PINTO GENERAL HOSPITAL: 7670-00-160036 001 Coverage for: Individual
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/2019 12/31/2019 UMR: PALO PINTO GENERAL HOSPITAL: 7670-00-160036 001 Coverage for: Individual
Super Blue Plus QHDHP HDHP Non Emb 100%
 Super Blue Plus QHDHP 1 2017 HDHP Non Emb 100% Effective Date April 1, 2018 to November 31, 2018, then restart December 1, 2018. Benefit Period (used for Deductible and Coinsurances limits and certain
Super Blue Plus QHDHP 1 2017 HDHP Non Emb 100% Effective Date April 1, 2018 to November 31, 2018, then restart December 1, 2018. Benefit Period (used for Deductible and Coinsurances limits and certain
Super Blue Plus QHDHP 1 HDHP Non Emb 100%
 Super Blue Plus QHDHP 1 HDHP Non Emb 100% Effective Date December 1, 2018 Benefit Period 2 (used for Deductible and Coinsurances limits and certain Contract Year benefit frequencies.) Note: All Services
Super Blue Plus QHDHP 1 HDHP Non Emb 100% Effective Date December 1, 2018 Benefit Period 2 (used for Deductible and Coinsurances limits and certain Contract Year benefit frequencies.) Note: All Services
California Natural Products: EPO Option Coverage Period: 01/01/ /31/2017
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.deltahealthsystems.com or by calling 1-209-858-2525 Ext
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.deltahealthsystems.com or by calling 1-209-858-2525 Ext
Important Questions Answers Why this Matters:
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.arcsvs.com or by calling 1-877-309-2955. Important Questions
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.arcsvs.com or by calling 1-877-309-2955. Important Questions
NETWORK CARE. $4,500 Individual. (2-member maximum)
") PLAN FEATURES Network Open Choice PPO Primary Care Physician Selection Deductible (per calendar year) Not Applicable $750 per member Not Applicable $750 per member (2-member maximum) (2-member maximum)
PLAN FEATURES Network Open Choice PPO Primary Care Physician Selection Deductible (per calendar year) Not Applicable $750 per member Not Applicable $750 per member (2-member maximum) (2-member maximum)
Coverage for: Single Enrollee Plan Type: TRAD/PPO. Important Questions Answers Why This Matters: $2,500/single Network $5,000/single Non-Network
 Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/2018-12/31/2018 STRS OHIO : Basic Plan with Medicare Part B Only Coverage for: Single
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/2018-12/31/2018 STRS OHIO : Basic Plan with Medicare Part B Only Coverage for: Single
Premium, balance-billed charges, penalties for not obtaining pre-authorization (pre-auth) for services, and health care this plan doesn't cover.
 for services, and health care this plan doesn't cover.") This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.assuranthealth.com or by calling 1-800-553-7654. Important
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.assuranthealth.com or by calling 1-800-553-7654. Important
Blue Cross Blue Shield of Kansas Blue Choice Comprehensive Major Medical Program
 Blue Cross Blue Shield of Kansas Blue Choice Comprehensive Major Medical Program ESSDACK HEALTH INSURANCE GROUP Stephanie Buckman Group Enrollment Representative One North Main, Suite 301 Hutchinson, Kansas
Blue Cross Blue Shield of Kansas Blue Choice Comprehensive Major Medical Program ESSDACK HEALTH INSURANCE GROUP Stephanie Buckman Group Enrollment Representative One North Main, Suite 301 Hutchinson, Kansas
Health Care Benefits. Important!
 Health Care Benefits The Major League Baseball Players Welfare Plan (referred to as the Welfare Plan in this section) provides comprehensive health care benefits for you and your eligible dependents. Whether
Health Care Benefits The Major League Baseball Players Welfare Plan (referred to as the Welfare Plan in this section) provides comprehensive health care benefits for you and your eligible dependents. Whether
Coverage for: Individual/Family Plan Type: PPO
 The Summary of Benefits and Coverage (SBC) document will help you choose a health plan. The SBC shows you how you and the plan would share the cost for covered health care services. NOTE: Information about
The Summary of Benefits and Coverage (SBC) document will help you choose a health plan. The SBC shows you how you and the plan would share the cost for covered health care services. NOTE: Information about
Even though you pay these expenses, they don t count toward the out-ofpocket limit.
 CEBCO: Champaign County Plan 1a Blue Access (PPO) Coverage Period: 01/01/2016-12/31/2016 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual/Family Plan Type:
CEBCO: Champaign County Plan 1a Blue Access (PPO) Coverage Period: 01/01/2016-12/31/2016 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual/Family Plan Type:
Important Questions Answers Why this Matters:
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.anthem.com or by calling 1-877-309-2955. Important Questions
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.anthem.com or by calling 1-877-309-2955. Important Questions
Important Questions Answers Why this Matters:
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at https://eoc.anthem.com/eocdps/fi or by calling 1-800-542-9402.
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at https://eoc.anthem.com/eocdps/fi or by calling 1-800-542-9402.
For: 80/20 Plan for Retired Employees Over Age 65 and Dependents
 Schedule of Benefits Employer: Cornell University ASC: 397366 Issue Date: September 1, 2010 Effective Date: September 1, 2010 Schedule: 11A Booklet Base: 11 For: 80/20 Plan for Retired Employees Over Age
Schedule of Benefits Employer: Cornell University ASC: 397366 Issue Date: September 1, 2010 Effective Date: September 1, 2010 Schedule: 11A Booklet Base: 11 For: 80/20 Plan for Retired Employees Over Age
The Harvard Pilgrim PPO Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services
 Massachusetts The Harvard Pilgrim PPO Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 12/01/2017 11/30/2018 Coverage for: Individual + Family
Massachusetts The Harvard Pilgrim PPO Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 12/01/2017 11/30/2018 Coverage for: Individual + Family
$ 600 individual / $ 1,200 family Does not apply to prescription drugs or exercise facility reimbursements. $ 4,000 individual / $ 8,000 family
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.metroplus.org or by calling 1-855-809-4073. Important
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.metroplus.org or by calling 1-855-809-4073. Important
Yes, written or oral approval is required, based upon medical policies.
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.uhc.com/calpers or by calling 1-877-359-3714. Important
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.uhc.com/calpers or by calling 1-877-359-3714. Important
COVERAGE INFORMATION. $2,400 Person/$4,800 Family - Aggregate As Noted Below $2,400 Person/$4,800 Family - Aggregate 0% coinsurance* 0% coinsurance*
 Vermont VM: Plan Name: MVP VT Gold 3 HDHP Plus 2400 Plan Form: FRVT-HMOH-G-003-N (2018) Plan Status: Active MVP VT Gold 3 HDHP Plus 2400 Plan Cost-Sharing Highlights Annual Deductible Coinsurance Annual
Vermont VM: Plan Name: MVP VT Gold 3 HDHP Plus 2400 Plan Form: FRVT-HMOH-G-003-N (2018) Plan Status: Active MVP VT Gold 3 HDHP Plus 2400 Plan Cost-Sharing Highlights Annual Deductible Coinsurance Annual
ELIGIBILITY INFORMATION YOU NEED TO KNOW
 EMPLOYEE BENEFITS PLAN YEAR 2017-2018 TABLE OF CONTENTS Eligibility Information You Need to Know 3 Medical Benefits / Premiums 4 Deductible Type / Alternative Prescription Drug Program 6 Arkansas Blue
EMPLOYEE BENEFITS PLAN YEAR 2017-2018 TABLE OF CONTENTS Eligibility Information You Need to Know 3 Medical Benefits / Premiums 4 Deductible Type / Alternative Prescription Drug Program 6 Arkansas Blue
Coverage for: Individual/Family Plan Type: PPO
 The Summary of Benefits and Coverage (SBC) document will help you choose a health plan. The SBC shows you how you and the plan would share the cost for covered health care services. NOTE: Information about
The Summary of Benefits and Coverage (SBC) document will help you choose a health plan. The SBC shows you how you and the plan would share the cost for covered health care services. NOTE: Information about
Are there services covered before you meet your deductible? Yes. Preventive care is covered before you meet your deductible.
 Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/2018-12/31/2018 Horizon BCBSNJ: MIDDLESEX COUNTY ROOSEVELT CARE CENTER Coverage for: All
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/2018-12/31/2018 Horizon BCBSNJ: MIDDLESEX COUNTY ROOSEVELT CARE CENTER Coverage for: All
PacificSource: BALANCE PSN _20 S4 Coverage Period: 09/20/ /19/2016
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at PacificSource.com or by calling 1-888-977-9299 Important
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at PacificSource.com or by calling 1-888-977-9299 Important
Anthem BlueCross BlueShield PPO $1,000 B What this Plan Covers & What it Costs Coverage Period: 10/01/ /30/2013 Individual/Family PPO
 Anthem BlueCross BlueShield PPO $1,000 B What this Plan Covers & What it Costs Coverage Period: 10/01/2012-09/30/2013 Individual/Family PPO This is only a summary. If you want more detail about your coverage
Anthem BlueCross BlueShield PPO $1,000 B What this Plan Covers & What it Costs Coverage Period: 10/01/2012-09/30/2013 Individual/Family PPO This is only a summary. If you want more detail about your coverage
BMC HealthNet Plan: Bronze Saver/Bronze Low Coverage Period: 08/01/ /31/2013 Summary of Benefits and Coverage:
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.bmchp.org or by calling 1-877-492-6967. Important Questions
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.bmchp.org or by calling 1-877-492-6967. Important Questions
SCHEDULE OF BENEFITS UPMC HEALTH PLAN PANTHER PREMIER PPO
 SCHEDULE OF BENEFITS UPMC HEALTH PLAN PANTHER PREMIER PPO This document is called a Schedule of Benefits. It is part of your Certificate of Coverage or your Summary Plan Description. Your Schedule of Benefits
SCHEDULE OF BENEFITS UPMC HEALTH PLAN PANTHER PREMIER PPO This document is called a Schedule of Benefits. It is part of your Certificate of Coverage or your Summary Plan Description. Your Schedule of Benefits
For more information on your plan, please refer to the final page of this document.
 Schedule of Benefits Panther Blue - General Student Health Plan PPO - Premium Network Deductible: $250 / $500 Coinsurance: 10% Total Annual Out-of-Pocket: $4,200 / $8,400 This document is your Schedule
Schedule of Benefits Panther Blue - General Student Health Plan PPO - Premium Network Deductible: $250 / $500 Coinsurance: 10% Total Annual Out-of-Pocket: $4,200 / $8,400 This document is your Schedule
University of Cincinnati Medical Plan Summary and Comparison Effective January 1- December 31, 2018-AAUP only
 Annual Deductible Annual Health Savings Account Funding (UC) $1500 individual $3,000 family Varies by Annual Base Pay as of 1/1/2018 $3,000 per person $6,000 family Varies by Annual Base Pay as of 1/1/2018
Annual Deductible Annual Health Savings Account Funding (UC) $1500 individual $3,000 family Varies by Annual Base Pay as of 1/1/2018 $3,000 per person $6,000 family Varies by Annual Base Pay as of 1/1/2018
Emergency Department: $175 Copayment per visit Coinsurance: 0%
 Schedule of Benefits UPMC Small Business Advantage Primary Care Provider: $25 Copayment per visit Gold PPO $1,000 $25/$50 - Premium Network Specialist: $50 Copayment per visit Deductible: $1,000 / $2,000
Schedule of Benefits UPMC Small Business Advantage Primary Care Provider: $25 Copayment per visit Gold PPO $1,000 $25/$50 - Premium Network Specialist: $50 Copayment per visit Deductible: $1,000 / $2,000
Coverage for: Individual/Family Plan Type: PPO
 The Summary of Benefits and Coverage (SBC) document will help you choose a health plan. The SBC shows you how you and the plan would share the cost for covered health care services. NOTE: Information about
The Summary of Benefits and Coverage (SBC) document will help you choose a health plan. The SBC shows you how you and the plan would share the cost for covered health care services. NOTE: Information about
All covered expenses accumulate separately toward the Network and Out-of-Network Coinsurance Maximum.
 PLAN FEATURES Network Managed Choice POS (Open Access) Primary Care Physician Selection Not Applicable Deductible (per calendar year) $250 per member (2-member maximum) Unless otherwise indicated, the
PLAN FEATURES Network Managed Choice POS (Open Access) Primary Care Physician Selection Not Applicable Deductible (per calendar year) $250 per member (2-member maximum) Unless otherwise indicated, the
Important Questions Answers Why this Matters:
 Anthem BlueCross BlueShield Anthem KeyCare 25 / $10/$30/$50/20% Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage Period: 11/01/2015-10/31/2016 Coverage For: Individual/Family
Anthem BlueCross BlueShield Anthem KeyCare 25 / $10/$30/$50/20% Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage Period: 11/01/2015-10/31/2016 Coverage For: Individual/Family
Attachment C - Schedule of Benefits. PremierBlue Plan A52
 - Schedule of Benefits PremierBlue Benefit percentages apply to the BCBST Maximum Allowable Charge. Network level applies to services received from Network Providers and Non-Contracted Providers. Out-of-Network
- Schedule of Benefits PremierBlue Benefit percentages apply to the BCBST Maximum Allowable Charge. Network level applies to services received from Network Providers and Non-Contracted Providers. Out-of-Network
Model COBRA Continuation Coverage General Notice Instructions
 Model COBRA Continuation Coverage General Notice Instructions The Department of Labor has developed a model Consolidated Omnibus Budget Reconciliation Act of 1985 (COBRA) continuation coverage general
Model COBRA Continuation Coverage General Notice Instructions The Department of Labor has developed a model Consolidated Omnibus Budget Reconciliation Act of 1985 (COBRA) continuation coverage general
IU Health Plans: Southern Indiana Physicians HSA Medical Saver Plan Coverage Period: 01/01/ /31/2018 Summary of Benefits and Coverage:
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.myiuhealthplans.com or by calling 1.866.895.5975. Important
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.myiuhealthplans.com or by calling 1.866.895.5975. Important
You don t have to meet deductibles for specific services.
 Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/2019-12/31/2019 Highmark Blue Cross Blue Shield: BlueCare Custom PPO Coverage for: Individual/Family
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/2019-12/31/2019 Highmark Blue Cross Blue Shield: BlueCare Custom PPO Coverage for: Individual/Family
Coverage for: Individual/Family Plan Type: PPO
 The Summary of Benefits and Coverage (SBC) document will help you choose a health plan. The SBC shows you how you and the plan would share the cost for covered health care services. NOTE: Information about
The Summary of Benefits and Coverage (SBC) document will help you choose a health plan. The SBC shows you how you and the plan would share the cost for covered health care services. NOTE: Information about
All covered expenses accumulate separately toward the Network and Out-of-Network Coinsurance Maximum.
 PLAN FEATURES Network Managed Choice POS (Open Access) Primary Care Physician Selection Deductible (per calendar year) Not Applicable $500 per member Not Applicable $500 per member (2-member maximum) (2-member
PLAN FEATURES Network Managed Choice POS (Open Access) Primary Care Physician Selection Deductible (per calendar year) Not Applicable $500 per member Not Applicable $500 per member (2-member maximum) (2-member
NETWORK CARE. $4,500 (2-member maximum)
") PLAN FEATURES Network Managed Choice POS (Open Access) Primary Care Physician Selection Not Applicable Deductible (per calendar year) $4,500 (2-member maximum) Unless otherwise indicated, the Deductible
PLAN FEATURES Network Managed Choice POS (Open Access) Primary Care Physician Selection Not Applicable Deductible (per calendar year) $4,500 (2-member maximum) Unless otherwise indicated, the Deductible
NETWORK CARE. $250 per member (2-member maximum)
") PLAN FEATURES Network Managed Choice POS (Open Access) Primary Care Physician Selection Not Applicable Deductible (per calendar year) $250 per member (2-member maximum) Unless otherwise indicated, the
PLAN FEATURES Network Managed Choice POS (Open Access) Primary Care Physician Selection Not Applicable Deductible (per calendar year) $250 per member (2-member maximum) Unless otherwise indicated, the