PAYING FOR VALUE Implications for Rural Hospitals
|
|
|
- Alison Wells
- 5 years ago
- Views:
Transcription
1 PAYING FOR VALUE Implications for Rural Hospitals Harold D. Miller President and CEO Center for Healthcare Quality and Payment Reform
2 Concern Continues to Grow About Rising Healthcare Costs $ TOTAL HEALTH CARE SPENDING TOTAL HEALTH CARE SPENDING TOTAL HEALTH CARE SPENDING TOTAL HEALTH CARE SPENDING TIME 2
3 Typical Solution #1: Cut Provider Fees for Services $ TOTAL HEALTH CARE SPENDING TOTAL HEALTH CARE SPENDING TOTAL HEALTH CARE SPENDING SAVINGS Cut Provider Fees TOTAL HEALTH CARE SPENDING BY PAYERS 3
4 Typical Solution #2: Shift Costs to Patients $ SAVINGS TOTAL HEALTH CARE SPENDING TOTAL HEALTH CARE SPENDING TOTAL HEALTH CARE SPENDING TOTAL HEALTH CARE SPENDING BY PAYERS Higher Cost-Share & Deductibles 4
5 Typical Solution #3: Delay or Deny Care to Patients $ SAVINGS TOTAL HEALTH CARE SPENDING TOTAL HEALTH CARE SPENDING TOTAL HEALTH CARE SPENDING TOTAL HEALTH CARE SPENDING BY PAYERS Lack of Needed Care 5
6 Results of These Win-Lose Strategies Small physician practices and hospitals forced out of business or forced to consolidate with large systems that can demand higher prices Hard-to-treat patients can t get the care they need Deferral of needed services and delivery of unnecessary services results in more serious problems and more expensive care in the future Health insurance costs continue to rise and access to insurance coverage and healthcare services decreases 6
7 Health Insurance Premiums Continue to Grow U.S. Family Premiums Inflation 7
8 WA Premiums $6,000 More Expensive Than 12-Year Inflation Washington State Family Premiums $6,119 Inflation 8
9 Health Insurance Premiums Are Equal to 35% of Avg. Annual Pay 9

10 Health Insurance Premiums Are Equal to 35% of Avg. Annual Pay If insurance premiums in Washington State had increased at the same rate as inflation from 2002 to 2014, Washington employers could have increased wages by 11% or hired 11% more workers 10
11 Medicare Isn t Doing Any Better Medicare Will Be Insolvent by

12 Medicare Spending Is the Biggest Driver of Federal Deficits 46% of Spending Growth is Healthcare Source: CBO Budget Outlook August
13 Is There a Better Way?


14 Institute of Medicine Estimate: 30% of Spending is Avoidable 14

15 5-17% of Hospital Admissions Are Potentially Preventable Source: AHRQ HCUP 15
16 Millions of Preventable Events Harm Patients and Increase Costs Medical Error # Errors (2008) Cost Per Error Total U.S. Cost Pressure Ulcers 374,964 $10,288 $3,857,629,632 Postoperative Infection 252,695 $14,548 $3,676,000,000 Complications of Implanted Device 60,380 $18,771 $1,133,392,980 Infection Following Injection 8,855 $78,083 $691,424,965 Pneumothorax 25,559 $24,132 $616,789,788 Central Venous Catheter Infection 7,062 $83,365 $588,723,630 Others 773,808 $11,640 $9,007,039,005 TOTAL 1,503,323 $13,019 $19,571,000,000 3 Adverse Events Every Minute Source: The Economic Measurement of Medical Errors, Milliman and the Society of Actuaries,


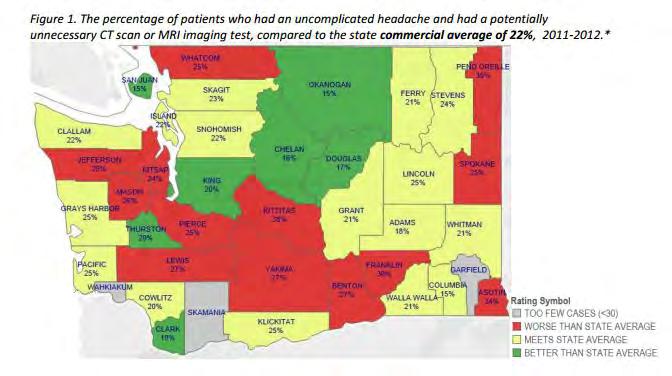
17 Many Tests & Services Are Unnecessary & May Be Harmful 17
18 20-50% Non-Adherence to Choosing Wisely Criteria 18
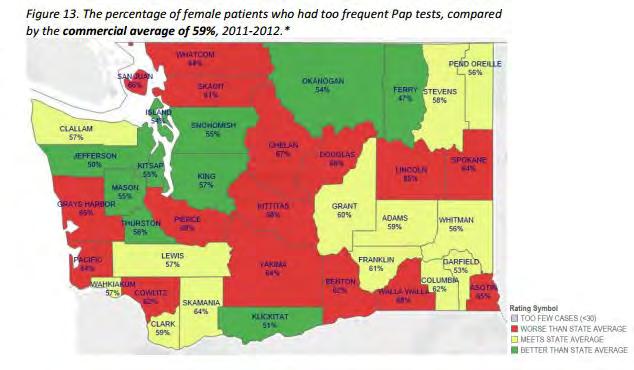
19 Significant Variation in Avoidable Spending in WA 19
20 The Right Focus: Spending That is Unnecessary or Avoidable $ AVOIDABLE SPENDING AVOIDABLE SPENDING AVOIDABLE SPENDING AVOIDABLE SPENDING NECESSARY SPENDING NECESSARY SPENDING NECESSARY SPENDING NECESSARY SPENDING TIME 20
21 The Right Goal: Less Avoidable $, $ AVOIDABLE SPENDING AVOIDABLE SPENDING AVOIDABLE SPENDING AVOIDABLE SPENDING NECESSARY SPENDING TIME 21
22 The Right Goal: Less Avoidable $, More Necessary $ $ AVOIDABLE SPENDING AVOIDABLE SPENDING AVOIDABLE SPENDING AVOIDABLE SPENDING NECESSARY SPENDING NECESSARY SPENDING NECESSARY SPENDING NECESSARY SPENDING TIME 22
23 The Hoped-For Result: Win-Win for Patients & Payers $ AVOIDABLE SPENDING SAVINGS AVOIDABLE SPENDING SAVINGS AVOIDABLE SPENDING SAVINGS AVOIDABLE SPENDING Lower Spending for Payers NECESSARY SPENDING NECESSARY SPENDING NECESSARY SPENDING NECESSARY SPENDING Better Care for Patients TIME 23
24 Payer Efforts to Promote Value Rather Than Volume of Services Value-Based Purchasing Value-Based Payment 24
25 Private Value-Based Purchasing = Using High-Value Providers Patients High-Value Providers Low-Value Providers 25
26 How Do You Define High Value? Patients High-Value Providers Low-Value Providers 26
27 Is This How to Define Value? VALUE = QUALITY COST 27
28 Which Oncologist Would You Use to Treat Your Cancer? VALUE = QUALITY COST ONCOLOGIST #1 7 Year Survival $5,000/patient ONCOLOGIST #2 10 Year Survival $10,000/patient 28
29 Oncologist #2 Rates Worse on the Standard Measure of Value VALUE = QUALITY COST ONCOLOGIST #1 7 Year Survival $5,000/patient 0.51 days of life per dollar > > ONCOLOGIST #2 10 Year Survival $10,000/patient 0.37 days of life per dollar 29
30 Assessing Value is a Lot Harder Than This VALUE = QUALITY COST 30
31 All Too Often, High-Value Means Willing to Accept Discounted Fee High-Value Providers (i.e., discounts) Low-Value Providers 31
32 Step 2: Reward High-Value Providers With More Patients More Patients High-Value Providers (i.e., discounts) Low-Value Providers 32
33 But Wait: Weren t We Going to Stop Rewarding Volume??? More Patients High-Value Providers (i.e., discounts) Low-Value Providers Volume Value 33
34 What if the Network is Already Narrow? More? Patients One Provider in the Community (Rural Area, Consolidated System, Etc.) 34
35 National Narrow Networks: Centers of Excellence More Patients High-Value Providers in Other Cities One Provider in the local Community 35
36 Walmart, Lowes, and Others Using Centers of Excellence Virginia Mason Mayo Clinic Cleveland Clinic Geisinger Mercy Mayo Clinic Scott & White Mayo Clinic 36
37 Will Every Cancer Patient Have to Go to Minnesota? 37
38 Critical Access Hospitals Could Be Harmed by Value-Based Purchasing CAHs don t have published data on quality CAHs will not be able to underbid large hospitals Patients going to hospitals in other cities for treatment would reduce volumes in the CAH, making it more difficult to maintain high quality care in the CAH, creating a downward spiral 38
39 Paying Based on Value Rather Than Volume of Services Value-Based Purchasing Value-Based Payment 39
40 Value-Based Payment Provides Incentives for Higher Value Care $ Bonus Penalty Pay for Performance ( P4P ) Based on Quality and Cost Measures Fee for Service 40
41 Hospital Value-Based Payment Hospital Readmission Penalties Hospital-Acquired Condition Penalties Hospital Value-Based Purchasing 41
42 Hospital Readmission Penalties $ Current Payment & High Readmit Rate Revenue from High Readmit Rate Reduce Readmissions OR Revenue from Admissions Payments for All Admissions Will Be Cut 42
43 $ The Hope: Hospitals Will Reduce Readmissions to Avoid Penalties Current Payment & High Readmit Rate Revenue from High Readmit Rate Lower Readmits & No Payment Cut Revenue from Average Readmit Rate Revenue from Admissions Revenue from Admissions w/ no Change in Payment Rate 43
44 $ The Myth: Hospitals Control All of the Reasons for Readmissions Current Payment & High Readmit Rate Revenue from High Readmit Rate Poor Access to Primary Care Low Quality of Post-Acute Care Patients w/o Capacity for Self-Care or Inadequate Home Support Lower Readmits & No Payment Cut Revenue from Average Readmit Rate Revenue from Admissions Revenue from Admissions w/ no Change in Payment Rate 44


45 Hospitals May Be Penalized for Having Patients With Higher Needs JAMA Intern Med. Published online September 14, doi: /jamainternmed
46 $ Under Current Pmt System, Fewer Readmissions = Lower Margins Current Payment & High Readmit Rate Revenue from High Readmit Rate Margin Lower Readmits & No Payment Cut Losses Revenue from Average Readmit Rate Revenue from Admissions Hospital Costs Revenue from Admissions w/ no Change in Payment Rate Hospital Costs (Don t Decrease in Proportion to Revenues) 46
47 $ So Hospitals Are Hurt Financially Current Payment & High Readmit Rate Losses Revenue from High Readmit Rate One Way or the Other Lower Readmits & No Payment Cut Losses Revenue from Average Readmit Rate Reduced Revenue from Admissions Due to Readmission Penalties Hospital Costs Revenue from Admissions w/ no Change in Payment Rate Hospital Costs (Don t Decrease in Proportion to Revenues) 47
48 Hospital Value-Based Payment Hospital Readmission Penalties Hospital-Acquired Condition Penalties Hospital Value-Based Purchasing Payment levels are cut across the board Hospitals have to earn back the cuts based on quality measures and resource use measures Medicare Spending Per Beneficiary measure calculates cost of all services that occur up to 30 days after discharge Hospital is penalized if costs are higher than other hospitals for similar patients 48
49 Impact of VBP on Critical Access Hospitals CAHs not subject directly to Value-Based Purchasing Affordable Care Act required a demonstration project to do this but CMS has not implemented one Resource Use measures for IPPS hospitals could discourage use of CAHs If CAH SNF cost per day is high or if patient is readmitted to the CAH, IPPS hospitals could avoid using the CAH for post-acute care services 49
50 Most Value-Based Payment for Docs Has Been Quality Bonuses $ P4P+ QUALITY MEASURES Mammograms Colon Cancer Screening HbA1c Control LDL FFS 50
51 P4P Hasn t Worked Terribly Well $ P4P+ FFS QUALITY MEASURES Mammograms Colon Cancer Screening HbA1c Control LDL A small bonus may not be enough to pay for the added costs of improving quality A small bonus may not be enough to offset loss of fee-for-service revenue from healthier patients or lower utilization A small bonus may not be enough to offset the costs of collecting and reporting the quality data LOSSES/ UNPAID SVCS 51
52 Over-Emphasis on Narrow Quality Measures Can Harm Patients Hypoglycemia 1 Yr Mortality: 19.9% 30 Day Readmits: 16.3% Hyperglycemia 1 Yr Mortality: 17.1% 30 Day Readmits: 15.3% Source: National Trends in US Hospital Admissions for Hyperglycemia and Hypoglycemia Among Medicare Beneficiaries, 1999 to 2011 JAMA Internal Medicine May 17,
53 Solution? Add More Measures $ P4P+ QUALITY MEASURES Mammograms Colon Cancer Screening HbA1c Control LDL P4P+ QUALITY MEASURES Mammograms Colon Cancer Screening Flu Vaccine Tobacco Counseling Hypertension Control HbA1c Control LDL Eye Exams Aspirin Use FFS FFS LOSSES/ UNPAID SVCS LOSSES/ UNPAID SVCS 53
54 When That Didn t Work, Bonuses Were Converted Into Penalties $ P4P+ QUALITY MEASURES Mammograms Colon Cancer Screening HbA1c Control LDL P4P+ QUALITY MEASURES Mammograms Colon Cancer Screening Flu Vaccine Tobacco Counseling Hypertension Control HbA1c Control LDL Eye Exams Aspirin Use P4P- QUALITY MEASURES Mammograms Colon Cancer Screening Flu Vaccine BMI Screens Tobacco Counseling Fall Risk Assessment Hypertension Control HbA1c Control LDL Eye Exams Aspirin Use FFS FFS FFS LOSSES/ UNPAID SVCS LOSSES/ UNPAID SVCS LOSSES/ UNPAID SVCS 54
55 The End of Collaboration? In the CMS Value-Based Payment Modifier, bonuses are only paid to physicians who have above average quality if penalties are assessed on other physicians with below average quality To maintain budget neutrality, the size of bonuses depends on the size of penalties Under this system, why would high-performing physicians want to help under-performing physicians to improve? 55
56 MACRA MACRA (Medicare Access and CHIP Reauthorization Act) repealed the Sustainable Growth Rate (SGR) formula that was threatening to cut physician payment every year MACRA created two optional replacements MIPS (Merit-Based Incentive Payment System) APMs (Alternative Payment Models) 56
57 MIPS is P4P on Steroids $ +x% -4.5% +x% -6% +x% -9% +x% -10% +4% -4% +5% -5% +7% -7% +9% -9% +9% -9% +9% -9% FFS + PQRS + MU + VBM FFS + PQRS + MU + VBM FFS + PQRS + MU + VBM FFS + PQRS + MU + VBM FFS + MIPS FFS + MIPS FFS + MIPS FFS + MIPS FFS + MIPS FFS + MIPS MIPS Merit-Based Incentive Payment System Quality Resource Use Clinical Practice Improvement Activities EHR Meaningful Use 50% -> 30% 10% -> 30% 15% 25% 57
58 Docs Will Be Rewarded for Using Fewer and Lower-Cost Services $ +x% -4.5% +x% -6% +x% -9% +x% -10% +4% -4% +5% -5% +7% -7% +9% -9% +9% -9% +9% -9% FFS + PQRS + MU + VBM FFS + PQRS + MU + VBM FFS + PQRS + MU + VBM FFS + PQRS + MU + VBM FFS + MIPS FFS + MIPS FFS + MIPS FFS + MIPS FFS + MIPS FFS + MIPS Physicians Pay Will Be Based on Total Cost of Care For their Patients Quality Resource Use Clinical Practice Improvement Activities EHR Meaningful Use 50% -> 30% 10% -> 30% 15% 25% 58
59 Quality Measures Critical Access Hospitals Could Be Harmed by MIPS Small volumes of patients and safety net services could make quality measures for physicians look poor compared to those at other hospitals Resource Use Measures Surgeons will be penalized if their patients use higher-cost post-acute care services Primary care physicians will be penalized if their patients are hospitalized at higher-cost hospitals If CAH cost per day or cost per admission is higher than other hospitals, physicians could avoid using the CAH for admissions or post-acute care services 59
60 MACRA Encourages APMs MACRA (Medicare Access and CHIP Reauthorization Act) repealed the Sustainable Growth Rate (SGR) formula that was threatening to cut physician payment every year MACRA created two optional replacements MIPS (Merit-Based Incentive Payment System) APMs (Alternative Payment Models) 60
61 HHS Announced Goal to Move Away From VBP & FFS+P4P Value-Based Purchasing HHS Goal for 2018 FFS No payment for services that will benefit patients Lower revenues from reducing avoidable costs P4P FFS No payment for services that will benefit patients Lower revenues from reducing avoidable costs Alternative Payment Models Built on a FFS Architecture P4P FFS 61
62 HHS Announced Goal to Move Away From VBP & FFS+P4P Value-Based Purchasing HHS Goal for 2018 FFS No payment for services that will benefit patients Lower revenues from reducing avoidable costs P4P FFS No payment for services that will benefit patients Lower revenues from reducing avoidable costs Alternative Payment Models Built on a FFS Architecture P4P FFS What the heck is an Alternative Payment Model Built on FFS Architecture? And is that better than FFS+P4P? 62
63 CMS Alternative Payment Models Announced To Date TYPE OF PROVIDER CMS PROGRAM PAYMENT STRUCTURE Health Systems, Multi-Specialty Groups, PHOs, and IPAs Primary Care Specialty Care Hospitals and Post-Acute Care Accountable Care Organizations (MSSP & Pioneer) Comprehensive Primary Care Initiative Oncology Care Model Comprehensive Care for Joint Replacement FFS + Shared Savings on Attributed Total Spending FFS + PMPM $ for Attributed Patients + Shared Savings on Attributed Total Spending (for State or Region) FFS + PMPM $ for Attributed Patients + Shared Savings on Attributed Total Spending (for 6-month window) FFS + Bonuses/Penalties on Attributed Total Spending 63
64 CMS Alternative Payment Models Don t Change Current Payments TYPE OF PROVIDER CMS PROGRAM PAYMENT STRUCTURE Health Systems, Multi-Specialty Groups, PHOs, and IPAs Primary Care Specialty Care Hospitals and Post-Acute Care Accountable Care Organizations (MSSP & Pioneer) Comprehensive Primary Care Initiative Oncology Care Model Comprehensive Care for Joint Replacement FFS + Shared Savings on Attributed Total Spending FFS + PMPM $ for Attributed Patients + Shared Savings on Attributed Total Spending (for State or Region) FFS + PMPM $ for Attributed Patients + Shared Savings on Attributed Total Spending (for 6-month window) FFS + Hospital Bonuses/Penalties for Attributed Total Spending 64
65 Some Provide Additional Upfront Resources to Physicians TYPE OF PROVIDER CMS PROGRAM PAYMENT STRUCTURE Health Systems, Multi-Specialty Groups, PHOs, and IPAs Primary Care Specialty Care Hospitals and Post-Acute Care Accountable Care Organizations (MSSP & Pioneer) Comprehensive Primary Care Initiative Oncology Care Model Comprehensive Care for Joint Replacement FFS + Shared Savings on Attributed Total Spending FFS + PMPM $ for Attributed Patients + Shared Savings on Attributed Total Spending (for State or Region) FFS + PMPM $ for Attributed Patients + Shared Savings on Attributed Total Spending (for 6-month window) FFS + Hospital Bonuses/Penalties for Attributed Total Spending 65
66 Most Only Provide More $ After Other Spending is Reduced TYPE OF PROVIDER CMS PROGRAM PAYMENT STRUCTURE Health Systems, Multi-Specialty Groups, PHOs, and IPAs Primary Care Specialty Care Hospitals and Post-Acute Care Accountable Care Organizations (MSSP & Pioneer) Comprehensive Primary Care Initiative Oncology Care Model Comprehensive Care for Joint Replacement FFS + Shared Savings on Attributed Total Spending FFS + PMPM $ for Attributed Patients + Shared Savings on Attributed Total Spending (for State or Region) FFS + PMPM $ for Attributed Patients + Shared Savings on Attributed Total Spending (for 6-month window) FFS + Hospital Bonuses/Penalties for Attributed Total Spending 66
67 How Shared Savings Works Hospitals, physicians, skilled nursing facilities, etc. all get paid the same way they do today. CMS adds up all of your spending and compares it to what you spent the previous year to calculate the increase CMS compares your increase to the increase in spending for other providers treating supposedly similar patients If your increase is less than the other providers, CMS makes an additional payment to you next year based on a percentage of the difference between your increase and other providers increases (i.e., a share of the savings) One-sided risk means you can get an additional payment if your increase is lower than others, but no penalty if your increase is higher Two-sided risk means you also have to pay money back to CMS if your increase is higher 67
68 Problems With Shared Savings Providers receive no upfront resources to improve care management for patients Already efficient providers receive little or no additional revenue and may be forced out of business Providers who have been practicing inefficiently or inappropriately are paid more than others Providers could be rewarded for denying needed care as well as by reducing overuse Providers are placed at risk for costs they cannot control and random variation in spending 68
69 In Most ACOs, Physicians/Hospitals Are Paid the Same As Today Fee-for-Service Payment MEDICARE, MEDICAID HEALTH PLAN PATIENTS Heart Disease ACO Diabetes Back Pain Hospitals Pregnancy Primary Care Cardiology Endocrinology Neurosurgery OB/GYN 69
70 Most ACOs Spend a Lot on IT and Nurse Care Managers Fee-for-Service Payment MEDICARE, MEDICAID HEALTH PLAN PATIENTS Heart Disease Expensive IT Systems ACO Nurse Care Managers Diabetes Back Pain Hospitals Pregnancy Primary Care Cardiology Endocrinology Neurosurgery OB/GYN 70
71 Possible Future Shared Savings Doesn t Support Better Care Today Fee-for-Service Payment MEDICARE, MEDICAID HEALTH PLAN Shared Savings Payment??? PATIENTS Heart Disease Diabetes Back Pain Pregnancy Primary Care Cardiology Expensive IT Systems ACO Hospitals Endocrinology Nurse Care Managers Share of Shared Savings $?? Neurosurgery OB/GYN 71
72 Medicare ACOs Aren t Succeeding Due to Flaws in Payment Model 2013 Results for Medicare Shared Savings ACOs 46% of ACOs (102/220) increased Medicare spending Only one-fourth (52/220) received shared savings payments After making shared savings payments, Medicare spent more than it saved 2014 Results for Medicare Shared Savings ACOs 45% of ACOs (152/333) increased Medicare spending Only one-fourth (86/333) received shared savings payments After making shared savings payments, Medicare spent more than it saved 72


73 Private Shared Savings ACOs Are Also Floundering 73
74 Most Alternative Payment Models Are Just FFS + P4P Value-Based Purchasing P4P APMs Built on FFS Architecture Shared Savings PMPM FFS No payment for services that will benefit patients Lower revenues from reducing avoidable costs FFS No payment for services that will benefit patients Lower revenues from reducing avoidable costs FFS No payment for services that will benefit patients Lower revenues from reducing avoidable costs 74
75 Is There a Better Way? Value-Based Purchasing APMs Built on FFS Architecture P4P Shared Savings PMPM FFS No payment for services that will benefit patients Lower revenues from reducing avoidable costs FFS No payment for services that will benefit patients Lower revenues from reducing avoidable costs FFS No payment for services that will benefit patients Lower revenues from reducing avoidable costs? 75
76 What If We Paid for Cars the Way We Pay for Care? 76
77 What If We Paid for Cars the Way We Pay for Care? ACA Affordable Car Act 77
78 What If We Paid for Cars the Way We Pay for Care? ACA Affordable Car Act Goal: Every citizen should have affordable transportation 78
79 What If We Paid for Cars the Way We Pay for Care? ACA Affordable Car Act Goal: Every citizen should have affordable transportation Method for Achieving the Goal: Give all citizens insurance that would cover the cost of new automobiles and repairs when needed 79
80 How to Control Spending on Cars If Insurance Is Paying For Them? 80
81 Should the Government Set Fees for Each Car Part HCPCS Codes (Hierarchical Car Parts Compensation System) 81

 AMA")

82 And Pay Auto Workers Based On How Many Parts They Installed? HCPCS Codes (Hierarchical Car Parts Compensation System) AMA Automobile Manufacturing Association CPT System (Car Parts Tokens) 82
83 The Result for Drivers If We Paid That Way 83





84 The Result for Drivers If We Paid Cars would get many unnecessary parts That Way 84

85 The Result for Drivers If We Paid Cars would get many unnecessary parts That Way Cars would be readmitted to the factory frequently to correct malfunctions 85
86 Spending on Cars Would Grow Rapidly 86

87 Spending on Cars Would Grow Rapidly 87
88 What to Do? 88
89 What to Do? Cut Fees for Parts & Assembly Cut Fees for Parts & Assembly 89
90 What to Do? Cut Fees for Parts & Assembly Cut Fees for Parts & Assembly More Parts Used 90
91 What to Do? Cut Fees for Parts & Assembly Cut Fees for Parts & Assembly More Parts Used $ Factories Merge to Resist Fee Cuts $ $ 91
92 What to Do? Managed Cars 92
93 Waiting for Prior Authorization to Buy a New Car What to Do? Managed Cars 93


94 Waiting for Prior Authorization to Buy a New Car What to Do? Managed Cars Requirements to Try Lower-Cost Services First 94
95 STEP 1 Continue Paying Factories & Workers Based on Parts What to Do? Shared Savings Program 95
96 What to Do? Shared Savings Program STEP 1 Continue Paying Factories & Workers Based on Parts STEP 2 After Cars Are Built & Sold, Compare Total Cost of Parts and Award Shared Savings # of Parts x Cost of Parts < # of Parts x Cost of Parts 96
97 What to Do? Shared Savings Program STEP 1 Continue Paying Factories & Workers Based on Parts STEP 2 After Cars Are Built & Sold, Compare Total Cost of Parts and Award Shared Savings # of Parts x Cost of Parts < # of Parts x Cost of Parts + Give Factory 0-50% of Difference in Cost of Parts Compared to Other Cars If Minimum Savings Threshold and Quality Targets Were Met 97
98 What to Do? Shared Savings Program STEP 1 Continue Paying Factories & Workers Based on Parts STEP 2 After Cars Are Built & Sold, Compare Total Cost of Parts and Award Shared Savings RESULT # of Parts x Cost of Parts < # of Parts x Cost of Parts + Give Factory 0-50% of Difference in Cost of Parts Compared to Other Cars If Minimum Savings Threshold and Quality Targets Were Met 98
99 What to Do? Shared Savings Program STEP 1 Continue Paying Factories & Workers Based on Parts STEP 2 After Cars Are Built & Sold, Compare Total Cost of Parts and Award Shared Savings # of Parts x Cost of Parts < # of Parts x Cost of Parts + Give Factory 0-50% of Difference in Cost of Parts Compared to Other Cars If Minimum Savings Threshold and Quality Targets Were Met RESULT Some factories would reduce parts, but not enough to get shared savings 99
100 What to Do? Shared Savings Program STEP 1 Continue Paying Factories & Workers Based on Parts STEP 2 After Cars Are Built & Sold, Compare Total Cost of Parts and Award Shared Savings # of Parts x Cost of Parts < # of Parts x Cost of Parts + Give Factory 0-50% of Difference in Cost of Parts Compared to Other Cars If Minimum Savings Threshold and Quality Targets Were Met RESULT Some factories would reduce parts, but not enough to get shared savings Some factories would spend more to meet quality targets than they receive in shared savings 100
101 What to Do? Shared Savings Program STEP 1 Continue Paying Factories & Workers Based on Parts STEP 2 After Cars Are Built & Sold, Compare Total Cost of Parts and Award Shared Savings # of Parts x Cost of Parts < # of Parts x Cost of Parts + Give Factory 0-50% of Difference in Cost of Parts Compared to Other Cars If Minimum Savings Threshold and Quality Targets Were Met RESULT Some factories would reduce parts, but not enough to get shared savings Some factories would spend more to meet quality targets than they receive in shared savings Some factories would leave out parts where there were no quality measures 101
102 What to Do? Shared Savings Program STEP 1 Continue Paying Factories & Workers Based on Parts STEP 2 After Cars Are Built & Sold, Compare Total Cost of Parts and Award Shared Savings # of Parts x Cost of Parts < # of Parts x Cost of Parts + Give Factory 0-50% of Difference in Cost of Parts Compared to Other Cars If Minimum Savings Threshold and Quality Targets Were Met RESULT Some factories would reduce parts, but not enough to get shared savings Some factories would spend more to meet quality targets than they receive in shared savings Some factories would leave out parts where there were no quality measures Most factories and workers would lose money and go back to business as usual 102
103 The Way We Actually Pay for Cars Is Much Better

104 Pay for Complete Cars With Warranties, Not Parts & Repairs 104
105 True Value-Based APMs Pay for Comprehensive Services Value-Based Purchasing APMs Built on FFS Architecture P4P Shared Savings PMPM Condition- Based Payments FFS No payment for services that will benefit patients Lower revenues from reducing avoidable costs FFS No payment for services that will benefit patients Lower revenues from reducing avoidable costs FFS No payment for services that will benefit patients Lower revenues from reducing avoidable costs Bundled/ Warrantied Payments Primary Care Medical Home Payments 105
106 Examples of How Good APMs Can Work Value-Based Purchasing APMs Built on FFS Architecture P4P Shared Savings PMPM Condition- Based Payments FFS No payment for services that will benefit patients Lower revenues from reducing avoidable costs FFS No payment for services that will benefit patients Lower revenues from reducing avoidable costs FFS No payment for services that will benefit patients Lower revenues from reducing avoidable costs Bundled/ Warrantied Payments Primary Care Medical Home Payments 106
107 A Hypothetical Case of Surgery COST TYPE TODAY Physician Fee $2,000 Hospital Cost $20,900 Hosp. Margin (5%) $ 1,100 Total Hospital Pmt $22,000 Total Cost to Payer $24,
108 Most of the Money Is Not Going to the Physician COST TYPE TODAY Physician Fee $2,000 Physician receives 8% of total spending Hospital Cost $20,900 Hosp. Margin (5%) $ 1,100 Total Hospital Pmt $22,000 Total Cost to Payer $24,
109 What if the Surgeon Could Reduce The Hospital s Costs? COST TYPE TODAY CHANGE Physician Fee $2,000 Hospital Cost $20,900-3% ($630) Hosp. Margin (5%) $ 1,100 Total Hospital Pmt $22,000 Total Cost to Payer $24,
110 Today: All Savings Goes to the Hospital, No Reward for Physician COST TYPE TODAY CHANGE SPLIT Physician Fee $2, % Hospital Cost $20,900-3% ($630) Hosp. Margin (5%) $ 1, % ($630) Total Hospital Pmt $22,000 Total Cost to Payer $24,000-0% 110
111 Bundling Eliminates Boundary Between Hospital & Physician Pmt COST TYPE TODAY Physician Fee $ 2,000 Hospital Cost $20,900 Hospital Margin $ 1,100 Total Cost to Payer $24,
112 Bundling Allows Savings Split Among Docs, Hospitals, Payers COST TYPE TODAY CHANGE SPLIT Physician Fee $ 2, % ($200) Hospital Cost $20,900-3% ($630) Hospital Margin $ 1, % ($200) Total Cost to Payer $24,000-1% ($230) 112
113 So Price of Surgery is Lower But More Profitable COST TYPE TODAY CHANGE SPLIT NEW Physician Fee $ 2, % ($200) $ 2,200 Hospital Cost $20,900-3% ($630) $20,270 Hospital Margin $ 1, % ($200) $ 1,300 Total Cost to Payer $24,000-1% ($230) $23,
114 Opportunities to Reduce Hospital Costs Use of lower-cost medical devices and equipment, or negotiating for better prices on devices Better scheduling of scarce resources (e.g., surgery suites) to reduce both underutilization & overtime Coordination among multiple physicians and departments to avoid duplication and conflicts in scheduling Standardization of equipment and supplies to facilitate bulk purchasing Less wastage of expensive supplies Reduced length of stay Etc. 114
115 Medicare Acute Care Episode (ACE) Demonstration Bundled Medicare Part A (hospital) and Part B (physician) payments together for cardiac and orthopedic (hips & knees) procedures Total Medicare payment was 1%-8% lower than what the standard Medicare DRG + physician fee would have been Payment was made to a Physician-Hospital Organization, which then divided the payment between hospital and surgeon Surgeon could receive up to 25% above Medicare fee Patient cost-sharing reduced by up to 50% of Medicare s savings CMS waived Stark rules for gainsharing Implemented in 2009/2010 in five hospital systems based on competitive bids: Hillcrest Medical Center, Oklahoma (cardiac + orthopedic procedures) Baptist Health System, Texas (cardiac + orthopedic procedures) Oklahoma Heart Hospital, Oklahoma (cardiac procedures) Lovelace Health System, New Mexico (cardiac + orthopedic procedures) Exempla Saint Joseph Hospital, Colorado (cardiac procedures) Most hospitals achieved significant savings, and physicians received increases in payment for procedures 115

116 Yes, a Health Care Provider Can Offer a Warranty Geisinger Health System ProvenCare SM A single payment for an ENTIRE 90 day period including: ALL related pre-admission care ALL inpatient physician and hospital services ALL related post-acute care ALL care for any related complications or readmissions Types of conditions/treatments currently offered: Cardiac Bypass Surgery Cardiac Stents Cataract Surgery Total Hip Replacement Bariatric Surgery Perinatal Care Low Back Pain Treatment of Chronic Kidney Disease 116
117 Payment + Process Improvement = Better Outcomes, Lower Costs 117
118 Readmission Reduction: 44% 118
119 119
120 It Can Be Done By Physicians, Not Just Large Health Systems In 1987, an orthopedic surgeon in Lansing, Michigan and the local hospital, Ingham Medical Center, offered: a fixed total price for surgical services for shoulder and knee problems a warranty for any subsequent services needed for a two-year period, including repeat visits, imaging, rehospitalization and additional surgery Results: Health insurer paid 40% less than otherwise Surgeon received over 80% more in payment than otherwise Hospital received 13% more than otherwise, despite fewer rehospitalizations Method: Reducing unnecessary auxiliary services such as radiography and physical therapy Reducing the length of stay in the hospital Reducing complications and readmissions. Johnson LL, Becker RL. An alternative health-care reimbursement system application of arthroscopy and financial warranty: results of a two-year pilot study. Arthroscopy Aug;10(4):
121 A Warranty is Not an Outcome Guarantee Offering a warranty on care does not imply that you are guaranteeing a cure or a good outcome It merely means that you are agreeing to correct avoidable problems at no (additional) charge Most warranties are limited warranties, in the sense that they agree to pay to correct some problems, but not all 121
122 Prices for Warrantied Care Will Likely Be Higher 122
123 Prices for Warrantied Care Will Likely Be Higher Q: Why should we pay more to get good-quality care?? A: In most industries, warrantied products cost more, but they re desirable because TOTAL spending on the product (repairs & replacement) is lower than without the warranty 123
124 Cost of Success Example: $5,000 Procedure, Added Cost of Readmit 20% Readmission Rate Rate of Readmits $5,000 $5,000 20% 124
125 Cost of Success Average Payment for Procedure is Higher than the Official Price Added Cost of Readmit Rate of Readmits Average Total Cost $5,000 $5,000 20% $6,
126 Cost of Success Average Payment for Procedure is Higher than the Official Price Added Cost of Readmit Rate of Readmits Average Total Cost $5,000 $5,000 20% $6,000 So how much should you charge to offer this same procedure with a warranty? 126
127 Cost of Success Starting Point for Warranty Price: Actual Current Average Payment Added Cost of Readmit Rate of Readmits Average Total Cost Price Charged Net Margin $5,000 $5,000 20% $6,000 $6,000 $ 0 127
128 Cost of Success Limited Warranty Gives Financial Incentive to Improve Quality Added Cost of Readmit Rate of Readmits Average Total Cost Price Charged Net Margin $5,000 $5,000 20% $6,000 $6,000 $ 0 $5,000 $5,000 15% $5,750 $6,000 $250 Reducing Adverse Events...Reduces Costs... Improves The Bottom Line 128
129 Cost of Success Higher-Quality Provider Can Charge Less, Attract Patients Added Cost of Readmit Rate of Readmits Average Total Cost Price Charged Net Margin $5,000 $5,000 20% $6,000 $6,000 $ 0 $5,000 $5,000 15% $5,750 $6,000 $250 $5,000 $5,000 15% $5,750 $5,900 $ 150 Enables Lower Prices Still With Better Margin 129
130 Cost of Success A Virtuous Cycle of Quality Improvement & Cost Reduction Added Cost of Readmit Rate of Readmits Average Total Cost Price Charged Net Margin $5,000 $5,000 20% $6,000 $6,000 $ 0 $5,000 $5,000 15% $5,750 $6,000 $250 $5,000 $5,000 15% $5,750 $5,900 $150 $5,000 $5,000 10% $5,500 $5,900 $400 Reducing Adverse Events...Reduces Costs... Improves The Bottom Line 130
131 Cost of Success Win-Win-Win Through Appropriate Payment & Pricing Added Cost of Readmit Rate of Readmits Average Total Cost Price Charged Net Margin $5,000 $5,000 20% $6,000 $6,000 $ 0 $5,000 $5,000 15% $5,750 $6,000 $250 $5,000 $5,000 15% $5,750 $5,900 $150 $5,000 $5,000 10% $5,500 $5,900 $400 $5,000 $5,000 10% $5,500 $5,700 $200 $5,000 $5,000 5% $5,250 $5,700 $450 Quality is Better......Cost is Lower......Providers More Profitable 131
132 Cost of Success In Contrast, Non-Payment Alone Creates Financial Losses Added Cost of Readmit Rate of Readmits Average Total Cost Payment Net Margin $5,000 $5,000 20% $6,000 $6,000 $ 0 $5,000 $5,000 20% $6,000 $5,000 -$1,000 $5,000 $5,000 10% $5,500 $5,000 -$ 500 $5,000 $5,000 0% $5,000 $5,000 $0 Non- Payment for Readmits Causes Losses While Improving 132
133 Many Variations Possible in Combining Bundles and Warranties 133
134 Starting with a Hospital Procedure PATIENT Procedure Hospital DRG Physician Fee 134
135 Simplest Bundle, Already Working SINGLE PMT in CMS Demonstrations PATIENT Procedure Hospital DRG Physician Fee 135
136 Bundling All Physicians Promotes SINGLE PMT More Care Coordination PATIENT Procedure Hospital DRG Lead Doc. Fee Consultant Fee Consultant Fee 136
137 Not All Care Providers Are Inside the Hospital Walls SINGLE PMT PATIENT Procedure Hospital DRG Lead Doc. Fee Consultant Fee Consultant Fee Post-Acute Rehab Home Health PCP Specialist PROBLEM: No incentive to reduce unnecessary use of expensive post-acute care 137
138 Bundling Inpatient and Post-Acute Care Promotes Coordination SINGLE PAYMENT PATIENT Procedure Hospital DRG Lead Doc. Fee Consultant Fee Consultant Fee Post-Acute Rehab Home Health PCP Specialist 138
139 Does the Bundle Stop When Things Go Bad in the Hospital? SINGLE PAYMENT PATIENT Procedure Hospital DRG Lead Doc. Fee Consultant Fee Consultant Fee Complication DRG/Outlier Lead Doc. Fee Consultant Fee Consultant Fee Post-Acute Rehab Home Health PCP Specialist PROBLEM: Hospital and physicians are paid more to treat expensive infections and complications 139
140 Including a Warranty for Complications in the Bundle SINGLE PAYMENT PATIENT Procedure Hospital DRG Lead Doc. Fee Consultant Fee Consultant Fee Complication DRG/Outlier Lead Doc. Fee Consultant Fee Consultant Fee Post-Acute Rehab Home Health PCP Specialist 140
141 Including a Warranty for Post-Discharge Problems SINGLE PAYMENT PATIENT Procedure Hospital DRG Lead Doc. Fee Consultant Fee Consultant Fee Complication DRG/Outlier Lead Doc. Fee Consultant Fee Consultant Fee Post-Acute Rehab Home Health PCP Specialist Readmission Hospital DRG Lead Doc. Fee Consultant Fee Consultant Fee Days Post-Discharge
142 Episode Payments Are Bundles Over a Full Course of Treatment SINGLE PAYMENT PATIENT Procedure Hospital DRG Lead Doc. Fee Consultant Fee Consultant Fee Complication DRG/Outlier Lead Doc. Fee Consultant Fee Consultant Fee Post-Acute Rehab Home Health PCP Specialist Readmission Hospital DRG Lead Doc. Fee Consultant Fee Consultant Fee Days Post-Discharge
143 What If The Procedure Could Be Done Outside the Hospital? SINGLE PAYMENT PATIENT Procedure Hospital DRG Lead Doc. Fee Consultant Fee Consultant Fee Complication DRG/Outlier Lead Doc. Fee Consultant Fee Consultant Fee Post-Acute Rehab Home Health PCP Specialist Readmission Hospital DRG Lead Doc. Fee Consultant Fee Consultant Fee Alternate Setting Facility Fee Physician Fee PROBLEM: No incentive to use lowercost setting, since payer gains all savings from lower facility fees 143
144 A Facility-Independent Episode SINGLE PAYMENT PATIENT Procedure Hospital DRG Lead Doc. Fee Consultant Fee Consultant Fee Complication DRG/Outlier Lead Doc. Fee Consultant Fee Consultant Fee Post-Acute Rehab Home Health PCP Specialist Readmission Hospital DRG Lead Doc. Fee Consultant Fee Consultant Fee Alternate Setting Facility Fee Physician Fee SOLUTION: Providers keep some of the savings from moving procedures to lower-cost settings 144
145 What if An Alternative Procedure Would Be Better or Cheaper? SINGLE PAYMENT PATIENT Procedure Hospital DRG Lead Doc. Fee Consultant Fee Consultant Fee Complication DRG/Outlier Lead Doc. Fee Consultant Fee Consultant Fee Post-Acute Rehab Home Health PCP Specialist Readmission Hospital DRG Lead Doc. Fee Consultant Fee Consultant Fee Alternate Setting Facility Fee Physician Fee Alternate Procedure Facility Fee Prof. Fee PROBLEM: No incentive to use lower-cost procedures (or to use no procedure at all) 145
146 A Condition-Based (Not Procedure-Based) Payment SINGLE PAYMENT PATIENT Procedure Hospital DRG Lead Doc. Fee Consultant Fee Consultant Fee Complication DRG/Outlier Lead Doc. Fee Consultant Fee Consultant Fee Post-Acute Rehab Home Health PCP Specialist Readmission Hospital DRG Lead Doc. Fee Consultant Fee Consultant Fee Alternate Setting Facility Fee Physician Fee Alternate Procedure Facility Fee Prof. Fee SOLUTION: Provider keeps some of the savings from using lower-cost procedures 146
147 Opportunities for Lower-Cost Care for Many Conditions Knee Osteoarthritis Home-based rehab instead of facility-based rehab Physical therapy instead of surgery Maternity Care Vaginal delivery instead of C-Section Term delivery instead of early elective delivery Delivery in birth center instead of hospital Chest Pain Non-invasive imaging instead of invasive imaging Medical management instead of invasive treatment Chronic Disease Management Improved education and self-management support Avoiding hospitalizations for exacerbations 147
148 Opportunities for Lower-Cost Care for Many Conditions Knee Osteoarthritis Home-based rehab instead of facility-based rehab Physical therapy instead of surgery Maternity Care Vaginal delivery instead of C-Section Term delivery instead of early elective delivery Delivery in birth center instead of hospital TODAY Savings for Payers = Lower Margins for Hospitals Chest Pain Non-invasive imaging instead of invasive imaging Medical management instead of invasive treatment Chronic Disease Management Improved education and self-management support Avoiding hospitalizations for exacerbations 148
149 Opportunities for Lower-Cost Care for Many Conditions Knee Osteoarthritis Home-based rehab instead of facility-based rehab Physical therapy instead of surgery Maternity Care Vaginal delivery instead of C-Section Term delivery instead of early elective delivery Delivery in birth center instead of hospital Chest Pain Non-invasive imaging instead of invasive imaging Medical management instead of invasive treatment Chronic Disease Management Improved education and self-management support Avoiding hospitalizations for exacerbations TODAY Savings for Payers = Lower Margins for Hospitals CONDITION-BASED PAYMENT Savings for Payers = Higher Margins for Hospitals 149

150 What About Transparency? 150
151 Current Transparency Efforts Are Focused on Procedure Price Payment for Procedure Provider 1: $25,000 dded Provider 2: $23,000-8% 151
152 Payment for Procedure Provider 1: What Hidden Costs Accompany the Lower Price? Payment and Rate of Complications $25,000 $30,000 2% Provider 2: $23,000 $30,000 10% -8% 152
153 Payment for Procedure Provider 1: Total Spending May Be Higher With the Lower Price Provider Payment and Rate of Complications Average Total Payment $25,000 $30,000 2% $25,600 Provider 2: $23,000 $30,000 10% $26,000-8% +2% Provider 2 has a lower starting price, but is more expensive when lower quality is factored in 153
154 Bundled/Warrantied Pmts Allow Comparing Apples to Apples Payment for Procedure Provider 1: Provider 2: Payment and Rate of Complications Bundled/ Episode Payment 2% $25,600 10% $26,000 +2% Bundled prices show that Provider 1 is the higher-value provider 154
155 True Value-Based Alternative Payment Models Value-Based Purchasing APMs Built on FFS Architecture P4P Shared Savings PMPM Condition- Based Payments FFS No payment for services that will benefit patients Lower revenues from reducing avoidable costs FFS No payment for services that will benefit patients Lower revenues from reducing avoidable costs FFS No payment for services that will benefit patients Lower revenues from reducing avoidable costs Bundled/ Warrantied Payments Primary Care Medical Home Payments 155
156 Can Create Win-Win-Wins for Patients, Payers, & Hospitals Value-Based Purchasing APMs Built on FFS Architecture P4P Shared Savings PMPM Better Care for Patients FFS No payment for services that will benefit patients Lower revenues from reducing avoidable costs FFS No payment for services that will benefit patients Lower revenues from reducing avoidable costs FFS No payment for services that will benefit patients Lower revenues from reducing avoidable costs Lower Spending for Payers Financially Viable Physician Practices & Hospitals 156
157 Can Create Win-Win-Wins for Patients, Payers, & Hospitals Value-Based Purchasing APMs Built on FFS Architecture FFS No payment for services that will benefit patients Lower revenues from reducing avoidable costs P4P FFS No payment for services that will benefit patients Lower revenues from reducing avoidable costs Shared Savings PMPM FFS No payment for services that will benefit patients Lower revenues from reducing avoidable costs Better Care for Patients BUT Lower ONLY Spending IF THEY RE for Payers DESIGNED Financially THE Viable RIGHT Physician WAY Practices & Hospitals 157
158 CMS Comprehensive Care for Joint Replacement EPISODE PAYMENT FOR SURGERIES PATIENT Hospital Costs for Surgery Readmits Post-Acute Care (IRF, SNF, HH) 158
159 Principal Goal of CMS Proposal Is Reducing Post-Acute Care Cost EPISODE PAYMENT FOR SURGERIES PATIENT Hospital Costs for Surgery Readmits Post-Acute Care (IRF, SNF, HH) Hospital Costs for Surgery Readmits Post-Acute Care SAVINGS 159
160 Proposed Structure Encourages Lower Spending, Not Better Care EPISODE PAYMENT FOR SURGERIES PATIENT Hospital Costs for Surgery Readmits Post-Acute Care (IRF, SNF, HH) Hospital Costs for Surgery Readmits Post-Acute Care SAVINGS No risk adjustment target spending amount is the same for high-risk, poor functional status patients as low-risk patients No flexibility to deliver different types of post-acute care or to be paid differently no change in current payment systems 160
161 Hospitals at Risk for Total Cost With Everyone Still Paid the Same EPISODE PAYMENT FOR SURGERIES PATIENT Hospital Costs for Surgery Readmits Post-Acute Care (IRF, SNF, HH) Hospital Costs for Surgery Readmits Post-Acute Care SAVINGS CMS No risk adjustment target spending amount is the same for high-risk, poor functional status patients as low-risk patients No flexibility to deliver different types of post-acute care or to be paid differently no change in current payment systems Hospital is at risk for higher post-acute care spending Hospital Physicians and Post-Acute Care 161
162 Over Time, CMS Keeps More of the Savings, If There Are Any EPISODE PAYMENT FOR SURGERIES PATIENT Hospital Costs for Surgery Readmits Post-Acute Care (IRF, SNF, HH) Hospital Costs for Surgery Readmits Post-Acute Care SAVINGS CMS No risk adjustment target spending amount is the same for high-risk, poor functional status patients as low-risk patients No flexibility to deliver different types of post-acute care or to be paid differently no change in current payment systems Hospital is at risk for higher post-acute care spending Target spending is reduced every year to match lower FFS spending Hospital Physicians and Post-Acute Care 162
163 If There Are Fewer Surgeries, CMS Keeps ALL of the Savings EPISODE PAYMENT FOR SURGERIES PATIENT Hospital Costs for Surgery Readmits Post-Acute Care (IRF, SNF, HH) Hospital Costs for Surgery Readmits Post-Acute Care SAVINGS CMS Hospital Non-Surg. Treatment SAVINGS Physicians and Post-Acute Care 163
164 Critical Access Hospitals Could Be Harmed by CJR Hospitals will be penalized if their patients use higher-cost post-acute care services If CAH cost per SNF/swing day is higher than other hospitals, CJR hospitals could avoid using the CAH for post-acute care services 164
165 Good Ways and Bad Ways to Define Alternative Payment Models HOW PAYMENT REFORMS ARE DESIGNED TODAY Medicare and Health Plans Define Payment Systems Providers Have To Change Care to Align With Payment Systems Patients and Providers May Not Come Out Ahead THE RIGHT WAY TO DESIGN PAYMENT REFORMS Providers Redesign Care and Identify Payment Barriers Payers Change Payment to Support Redesigned Care Patients Get Better Care and Providers Stay Financially Viable 165
166 Three Paths to the Future PAY FOR PERFORMANCE ( Value-Based Payment/Purchasing ) ( Merit-Based Incentive Payment System ) CURRENT PAYMENT SYSTEMS PAYER-DESIGNED ALTERNATIVE PAYMENT MODELS (APMs) PROVIDER-DESIGNED ALTERNATIVE PAYMENT MODELS (APMs) 166





167 Learn More About Win-Win-Win Payment and Delivery Reform 167
168 For More Information: Harold D. Miller President and CEO Center for Healthcare Quality and Payment Reform (412)
WINNING IN ACCOUNTABLE CARE How Hospitals and Health Systems Can Survive and Thrive Under Payment and Delivery Reform
 WINNING IN ACCOUNTABLE CARE How Hospitals and Health Systems Can Survive and Thrive Under Payment and Delivery Reform Harold D. Miller President and CEO Center for Healthcare Quality and Payment Reform
WINNING IN ACCOUNTABLE CARE How Hospitals and Health Systems Can Survive and Thrive Under Payment and Delivery Reform Harold D. Miller President and CEO Center for Healthcare Quality and Payment Reform
DELIVERING HIGHER-VALUE MATERNITY CARE
 DELIVERING HIGHER-VALUE MATERNITY CARE Designing Alternative Payment Models for Better Care, Lower Spending, and Financially Viable Maternity Care Providers Harold D. Miller President and CEO Center for
DELIVERING HIGHER-VALUE MATERNITY CARE Designing Alternative Payment Models for Better Care, Lower Spending, and Financially Viable Maternity Care Providers Harold D. Miller President and CEO Center for
REDESIGNING HEALTH CARE FROM THE BOTTOM UP INSTEAD OF FROM THE TOP DOWN Better Care at Lower Costs Through Patient-Centered Payment
 REDESIGNING HEALTH CARE FROM THE BOTTOM UP INSTEAD OF FROM THE TOP DOWN Better Care at Lower Costs Through Patient-Centered Payment Harold D. Miller President and CEO Center for Healthcare Quality and
REDESIGNING HEALTH CARE FROM THE BOTTOM UP INSTEAD OF FROM THE TOP DOWN Better Care at Lower Costs Through Patient-Centered Payment Harold D. Miller President and CEO Center for Healthcare Quality and
CREATING A PHYSICIAN-LED HEALTHCARE FUTURE Better Care for Patients, Lower Healthcare Spending, & Financially Viable Physician Practices
 CREATING A PHYSICIAN-LED HEALTHCARE FUTURE Better Care for Patients, Lower Healthcare Spending, & Financially Viable Physician Practices Harold D. Miller President and CEO Center for Healthcare Quality
CREATING A PHYSICIAN-LED HEALTHCARE FUTURE Better Care for Patients, Lower Healthcare Spending, & Financially Viable Physician Practices Harold D. Miller President and CEO Center for Healthcare Quality
A Practical Discussion of Value and Quality Based Payments What Do I Do Now?
 Emerging Challenges in Primary Care: 2016 A Practical Discussion of Value and Quality Based Payments What Do I Do Now? Modified from AHLA Physicians and Hospitals Law Institute 2016 Faculty Ellie Bane
Emerging Challenges in Primary Care: 2016 A Practical Discussion of Value and Quality Based Payments What Do I Do Now? Modified from AHLA Physicians and Hospitals Law Institute 2016 Faculty Ellie Bane
Volume to Value The Great Transformation of American Medicine
 Volume to Value The Great Transformation of American Medicine 2010-2020 Richard I. Fogel, MD FHRS Chief Clinical Officer St. Vincent Health October 2015 Fee for Service You get paid for what you do The
Volume to Value The Great Transformation of American Medicine 2010-2020 Richard I. Fogel, MD FHRS Chief Clinical Officer St. Vincent Health October 2015 Fee for Service You get paid for what you do The
CAN HEALTHCARE PROVIDERS BE HAPPIER WITH LESS REVENUE? Finding Win-Win-Win Approaches to Reducing Healthcare Spending
 CAN HEALTHCARE PROVIDERS BE HAPPIER WITH LESS REVENUE? Finding Win-Win-Win Approaches to Reducing Healthcare Spending Harold D. Miller President and CEO Center for Healthcare Quality and Payment Reform
CAN HEALTHCARE PROVIDERS BE HAPPIER WITH LESS REVENUE? Finding Win-Win-Win Approaches to Reducing Healthcare Spending Harold D. Miller President and CEO Center for Healthcare Quality and Payment Reform
REDESIGNING HEALTH CARE FROM THE BOTTOM UP INSTEAD OF FROM THE TOP DOWN
 REDESIGNING HEALTH CARE FROM THE BOTTOM UP INSTEAD OF FROM THE TOP DOWN How Physicians Can be a Disruptive Force for Better Care and Lower Spending Harold D. Miller President and CEO Center for Healthcare
REDESIGNING HEALTH CARE FROM THE BOTTOM UP INSTEAD OF FROM THE TOP DOWN How Physicians Can be a Disruptive Force for Better Care and Lower Spending Harold D. Miller President and CEO Center for Healthcare
The Case For Value ACA to MACRA to MIPS
 The Case For Value ACA to MACRA to MIPS 2016-2019 Robert E Nesse M.D. Professor of Family Medicine Mayo Medical School Senior Director of Health Care Policy and Payment Reform nesse.robert@mayo.edu What
The Case For Value ACA to MACRA to MIPS 2016-2019 Robert E Nesse M.D. Professor of Family Medicine Mayo Medical School Senior Director of Health Care Policy and Payment Reform nesse.robert@mayo.edu What
Prospective vs. Retrospective. Will Bundled Payment Really Be.. Fee For Service
 Fee For Service Episode Based Payment: Are You Ready For Medicare s Next Wave of Provider Payment Reform? Payer Robert Mechanic, MBA The Estes Park Institute January 30, 2012 Hospital Surgeon Specialist
Fee For Service Episode Based Payment: Are You Ready For Medicare s Next Wave of Provider Payment Reform? Payer Robert Mechanic, MBA The Estes Park Institute January 30, 2012 Hospital Surgeon Specialist
4/8/17. The Changing Nature of Physician Payment and Health Care Reform in The AMA A Unifying Voice for Physicians
 The Changing Nature of Physician Payment and Health Care Reform in 2017 U of Mo Family Medicine Update April 7, 2017 David Barbe, MD MHA President-elect American Medical Association VP Regional Operations
The Changing Nature of Physician Payment and Health Care Reform in 2017 U of Mo Family Medicine Update April 7, 2017 David Barbe, MD MHA President-elect American Medical Association VP Regional Operations
Providers involved in the Centers for Medicare & Medicaid Services ACE demonstration project share
 Pursuing Bundled Payments Lessons from the ACE Demonstration Providers involved in the Centers for Medicare & Medicaid Services ACE demonstration project share lessons learned from their experiences in
Pursuing Bundled Payments Lessons from the ACE Demonstration Providers involved in the Centers for Medicare & Medicaid Services ACE demonstration project share lessons learned from their experiences in
Eight Indispensable Financial Considerations of Shifting from Volume to Value Reimbursement
 Eight Indispensable Financial Considerations of Shifting from Volume to Value Reimbursement September 25-26, 2017 Max Reiboldt, CPA President CEO Learning Objectives This session will provide you with
Eight Indispensable Financial Considerations of Shifting from Volume to Value Reimbursement September 25-26, 2017 Max Reiboldt, CPA President CEO Learning Objectives This session will provide you with
Cardiac Bundle (AMI, CABG, and SHFFT), CR and ACO Track 1+ January 11, 2017
, CR and ACO Track 1+ January 11, 2017") To Dial-in: 877.668.4490 or 408.792.6300 Event Number: 669 367 723 Cardiac Bundle (AMI, CABG, and SHFFT), CR and ACO Track 1+ January 11, 2017 CMS Final Rule and Materials Advancing Care Coordination through
To Dial-in: 877.668.4490 or 408.792.6300 Event Number: 669 367 723 Cardiac Bundle (AMI, CABG, and SHFFT), CR and ACO Track 1+ January 11, 2017 CMS Final Rule and Materials Advancing Care Coordination through
First a word about the rising cost of retiree healthcare
 Medicare Trends First a word about the rising cost of retiree healthcare The average 66-year-old couple is expected to spend nearly 60% of their Social Security income on medical bills, according to a
Medicare Trends First a word about the rising cost of retiree healthcare The average 66-year-old couple is expected to spend nearly 60% of their Social Security income on medical bills, according to a
Growth and Success of Accountable Care Organizations (ACOs) in the US from Dennis Horrigan June 2016
 in the US from Dennis Horrigan June 2016") Growth and Success of Accountable Care Organizations (ACOs) in the US from 2010-2016 Dennis Horrigan June 2016 Introducing Dennis Horrigan Dennis R. Horrigan President and Chief Executive Officer Catholic
Growth and Success of Accountable Care Organizations (ACOs) in the US from 2010-2016 Dennis Horrigan June 2016 Introducing Dennis Horrigan Dennis R. Horrigan President and Chief Executive Officer Catholic
MACRA Overview. April 2016
 MACRA Overview April 2016 CMS is Focused on Progression from Volume-Based to Value-Based Payments Hospitals have some value-based payment via Hospital VBP, readmissions, and HAC programs Other provider
MACRA Overview April 2016 CMS is Focused on Progression from Volume-Based to Value-Based Payments Hospitals have some value-based payment via Hospital VBP, readmissions, and HAC programs Other provider
WASHINGTON RURAL HEALTH ACCESS PRESERVATION. Enabling Rural Hospitals in Washington State To Survive and Thrive
 WASHINGTON RURAL HEALTH ACCESS PRESERVATION Enabling Rural s in State To Survive and Thrive Origin and Goals of WRHAP Project WSHA/DOH New Blue H Project Identified issues threatening sustainability of
WASHINGTON RURAL HEALTH ACCESS PRESERVATION Enabling Rural s in State To Survive and Thrive Origin and Goals of WRHAP Project WSHA/DOH New Blue H Project Identified issues threatening sustainability of
Health Care Policy Landscape: Market Trends & Frontline Perspectives
 Health Care Policy Landscape: Market Trends & Frontline Perspectives December 1, 2016 www.leavittpartners.com Post-Election, New Administration Insights Top 10 Health Policy Actions to Watch 1 2 3 4 Substantial
Health Care Policy Landscape: Market Trends & Frontline Perspectives December 1, 2016 www.leavittpartners.com Post-Election, New Administration Insights Top 10 Health Policy Actions to Watch 1 2 3 4 Substantial
FMV Considerations for Bundled Payment Arrangements
 FMV Considerations for Bundled Payment Arrangements Matthew J. Milliron, MBA HealthCare Appraisers, Inc. Becker s CEO + CFO Roundtable November 8, 2016 Today s Roadmap Healthcare Transactions Refresh Bundled
FMV Considerations for Bundled Payment Arrangements Matthew J. Milliron, MBA HealthCare Appraisers, Inc. Becker s CEO + CFO Roundtable November 8, 2016 Today s Roadmap Healthcare Transactions Refresh Bundled
Improving your ASC s performance in 2018
 Improving your ASC s performance in 2018 The ASC guide to major trends that will impact your practice Marilyn Denegre Rumbin, JD MBA Director, Payer & Reimbursement Strategy February 2018 1 Welcome Marilyn
Improving your ASC s performance in 2018 The ASC guide to major trends that will impact your practice Marilyn Denegre Rumbin, JD MBA Director, Payer & Reimbursement Strategy February 2018 1 Welcome Marilyn
AMERICAN COLLEGE OF GASTROENTEROLOGY MAKING $ENSE OF MACRA
 AMERICAN COLLEGE OF GASTROENTEROLOGY 6400 Goldsboro Road, Suite 200, Bethesda, Maryland 20817-5842; P: 301-263-9000; F: 301-263-9025 MAKING $ENSE OF MACRA CMS.SGR MACRA MIPS APMs QCDRs ACOs Why does Washington
AMERICAN COLLEGE OF GASTROENTEROLOGY 6400 Goldsboro Road, Suite 200, Bethesda, Maryland 20817-5842; P: 301-263-9000; F: 301-263-9025 MAKING $ENSE OF MACRA CMS.SGR MACRA MIPS APMs QCDRs ACOs Why does Washington
Designing Value-Based Payments That Support Affordable, High-Quality Healthcare Services. Harold D. Miller
 Designing Value-Based Payments That Support Affordable, High-Quality Healthcare Services Harold D. Miller First Edition December 2018 CONTENTS WHAT IS AN ALTERNATIVE PAYMENT MODEL?... 1 HOW TO CREATE A
Designing Value-Based Payments That Support Affordable, High-Quality Healthcare Services Harold D. Miller First Edition December 2018 CONTENTS WHAT IS AN ALTERNATIVE PAYMENT MODEL?... 1 HOW TO CREATE A
Healthcare Reform and Its Impact on the Care Delivery System
 Healthcare Reform and Its Impact on the Care Delivery System Agenda 1) The Era of Healthcare Reform 2) Healthcare Reform and Post-Acute Care 3) Succeeding in the Reform Era: Managing the Continuum of Health
Healthcare Reform and Its Impact on the Care Delivery System Agenda 1) The Era of Healthcare Reform 2) Healthcare Reform and Post-Acute Care 3) Succeeding in the Reform Era: Managing the Continuum of Health
The Payment Reform GLOSSARY. Definitions and Explanations of the Terminology Used to Describe Methods of Paying for Healthcare Services.
 The Payment Reform GLOSSARY Definitions and Explanations of the Terminology Used to Describe Methods of Paying for Healthcare Services First Edition INTRODUCTION There is growing national recognition that
The Payment Reform GLOSSARY Definitions and Explanations of the Terminology Used to Describe Methods of Paying for Healthcare Services First Edition INTRODUCTION There is growing national recognition that
AAOS MACRA Proposed Rule Summary (Short)
") AAOS MACRA Proposed Rule Summary (Short) Merit-Based Incentive Payment System (MIPS), Advanced Alternative Payment Model (APM) Incentive, and Criteria for Physician-Focused Payment Models Ref: CMS-5517-P
AAOS MACRA Proposed Rule Summary (Short) Merit-Based Incentive Payment System (MIPS), Advanced Alternative Payment Model (APM) Incentive, and Criteria for Physician-Focused Payment Models Ref: CMS-5517-P
9/23/2016. Our Services. Transitioning from Fee-for-Service to Value-based Reimbursement. Key Trends and Strategies for Rural Health Providers
 Transitioning from Fee-for-Service to Value-based Reimbursement Key Trends and Strategies for Rural Health Providers Paul MacLellan, CEO >> Health care consulting company >> Wholly owned subsidiary of
Transitioning from Fee-for-Service to Value-based Reimbursement Key Trends and Strategies for Rural Health Providers Paul MacLellan, CEO >> Health care consulting company >> Wholly owned subsidiary of
CMS PROPOSES KEY PROVISIONS OF MACRA PHYSICIAN PAYMENT SYSTEM FOR 2019
 Thursday, April 28, 2016 CMS PROPOSES KEY PROVISIONS OF MACRA PHYSICIAN PAYMENT SYSTEM FOR 2019 The Centers for Medicare & Medicaid Services (CMS) late yesterday issued a proposed rule implementing key
Thursday, April 28, 2016 CMS PROPOSES KEY PROVISIONS OF MACRA PHYSICIAN PAYMENT SYSTEM FOR 2019 The Centers for Medicare & Medicaid Services (CMS) late yesterday issued a proposed rule implementing key
The Emergence of Value-Based Care: Present and Future Tense
 The Emergence of Value-Based Care: Present and Future Tense Erik Johnson, Vice President for Value-Based Care May 2016 What Is Value-Based Care? While the concept of value-based care has existed for years,
The Emergence of Value-Based Care: Present and Future Tense Erik Johnson, Vice President for Value-Based Care May 2016 What Is Value-Based Care? While the concept of value-based care has existed for years,
A Path to Accountable Care Organizations: How Do We Get From There to Here? Financial Considerations for Accountable
 A Path to Accountable Care Organizations: How Do We Get From There to Here? Financial Considerations for Accountable Care Entity Engagement Presented by Milliman, Inc. San Francisco, CA susan.pantely@milliman.com
A Path to Accountable Care Organizations: How Do We Get From There to Here? Financial Considerations for Accountable Care Entity Engagement Presented by Milliman, Inc. San Francisco, CA susan.pantely@milliman.com
MACRA: APPLICATIONS & IMPLICATIONS September 13, /13/2016. Mark Blessing, CPA, FHFMA Partner
 MACRA: APPLICATIONS & IMPLICATIONS September 13, 2016 Mark Blessing, CPA, FHFMA Partner mblessing@bkd.com Zach Remmich Managing Consultant zremmich@bkd.com 1 TO RECEIVE CPE CREDIT Participate in entire
MACRA: APPLICATIONS & IMPLICATIONS September 13, 2016 Mark Blessing, CPA, FHFMA Partner mblessing@bkd.com Zach Remmich Managing Consultant zremmich@bkd.com 1 TO RECEIVE CPE CREDIT Participate in entire
Payment Reform in Support of Population Health Management
 Payment Reform in Support of Population Health Management Aligning Forces for Quality Employers - Providers Summit October 25, 2011 Charles Chodroff, MD, MBA, FACP Senior Vice President, Chief Clinical
Payment Reform in Support of Population Health Management Aligning Forces for Quality Employers - Providers Summit October 25, 2011 Charles Chodroff, MD, MBA, FACP Senior Vice President, Chief Clinical
Using Analytics To Transform Your ACO
 Using Analytics To Transform Your ACO How to Develop Effective Cost Reduction Strategies Presented July 2016 Agenda and Presenter External Forces and Market Response Critical Success Factors Analytics
Using Analytics To Transform Your ACO How to Develop Effective Cost Reduction Strategies Presented July 2016 Agenda and Presenter External Forces and Market Response Critical Success Factors Analytics
Delivering Value-Based Care:
 Discussion Summary Delivering Value-Based Care: Episodes of Care Analytics for Health Care Providers, Payers and ACOs July 2015 Interview Featuring: J. Peter Chingos, Senior Industry Consultant, Health
Discussion Summary Delivering Value-Based Care: Episodes of Care Analytics for Health Care Providers, Payers and ACOs July 2015 Interview Featuring: J. Peter Chingos, Senior Industry Consultant, Health
When the Dust Settles-What s Next?
 When the Dust Settles-What s Next? AMA IPPS Conference Robert Nesse M.D. Senior Director of Payment Reform Mayo Clinic nesse.robert@mayo.edu What is Driving the Change in Healthcare? Common Belief: The
When the Dust Settles-What s Next? AMA IPPS Conference Robert Nesse M.D. Senior Director of Payment Reform Mayo Clinic nesse.robert@mayo.edu What is Driving the Change in Healthcare? Common Belief: The
The Future Of Medicare Physician Reimbursement
 Portfolio Media. Inc. 111 West 19 th Street, 5th Floor New York, NY 10011 www.law360.com Phone: +1 646 783 7100 Fax: +1 646 783 7161 customerservice@law360.com The Future Of Medicare Physician Reimbursement
Portfolio Media. Inc. 111 West 19 th Street, 5th Floor New York, NY 10011 www.law360.com Phone: +1 646 783 7100 Fax: +1 646 783 7161 customerservice@law360.com The Future Of Medicare Physician Reimbursement
Designing Value-Based Payments That Support Affordable, High-Quality Healthcare Services. Harold D. Miller
 Designing Value-Based Payments That Support Affordable, High-Quality Healthcare Services Harold D. Miller First Edition December 2018 CONTENTS EXECUTIVE SUMMARY... I I. WHAT IS AN ALTERNATIVE PAYMENT MODEL?...
Designing Value-Based Payments That Support Affordable, High-Quality Healthcare Services Harold D. Miller First Edition December 2018 CONTENTS EXECUTIVE SUMMARY... I I. WHAT IS AN ALTERNATIVE PAYMENT MODEL?...
Opportunities for Orthopedic Specialists in BPCI Advanced
 Opportunities for Orthopedic Specialists in BPCI Advanced January 13 th, 2018 Introduction CMS announced the voluntary Bundled Payment for Care Improvement (BPCI) Advanced program on Tuesday, Jan 9 th
Opportunities for Orthopedic Specialists in BPCI Advanced January 13 th, 2018 Introduction CMS announced the voluntary Bundled Payment for Care Improvement (BPCI) Advanced program on Tuesday, Jan 9 th
CF Health Advisors: Partner Biographies
 The Evolving Healthcare Landscape C F H E A LT H A D V I S O R S S E P T E M B E R, 2 0 1 6 CF Health Advisors: Partner Biographies CHARLENE FRIZZERA President and CEO JEREMY BROWN Managing Partner Former
The Evolving Healthcare Landscape C F H E A LT H A D V I S O R S S E P T E M B E R, 2 0 1 6 CF Health Advisors: Partner Biographies CHARLENE FRIZZERA President and CEO JEREMY BROWN Managing Partner Former
HEALTH POLICY & EDUCATION SERIES
 HEALTH POLICY & PAYMENT EDUCATION SERIES Medicare s Bundled Payment Initiatives The information in this document is based off of policy information available as of August 2016. Updated information may
HEALTH POLICY & PAYMENT EDUCATION SERIES Medicare s Bundled Payment Initiatives The information in this document is based off of policy information available as of August 2016. Updated information may
The MACRA Proposed Rule on MIPS and APMs: Summary and Key Takeaways
 The MACRA Proposed Rule on MIPS and APMs: Summary and Key Takeaways A White Paper May 2016 Impact Advisors LLC 400 E. Diehl Road Suite 190 Naperville IL 60563 1-800- 680-7570 Impact- Advisors.com Executive
The MACRA Proposed Rule on MIPS and APMs: Summary and Key Takeaways A White Paper May 2016 Impact Advisors LLC 400 E. Diehl Road Suite 190 Naperville IL 60563 1-800- 680-7570 Impact- Advisors.com Executive
Medicare Access and CHIP Reauthorization Act of 2015 (HR. 2; MACRA)
") Fact Sheet April 23, 2015 H.R.2 - Medicare Access and CHIP Reauthorization Act of 2015 (MACRA) Background. The Medicare Sustainable Growth Rate formula (SGR), passed by Congress in 1997, was intended to
Fact Sheet April 23, 2015 H.R.2 - Medicare Access and CHIP Reauthorization Act of 2015 (MACRA) Background. The Medicare Sustainable Growth Rate formula (SGR), passed by Congress in 1997, was intended to
HEALTH ECONOMICS AND REIMBURSEMENT
 HEALTH ECONOMICS AND REIMBURSEMENT VASCULAR CY 2016 MEDICARE PHYSICIAN FEE SCHEDULE (PFS) UPDATE Abbott Vascular is pleased to provide you with this summary of the Medicare Physician Fee Schedule (PFS)
HEALTH ECONOMICS AND REIMBURSEMENT VASCULAR CY 2016 MEDICARE PHYSICIAN FEE SCHEDULE (PFS) UPDATE Abbott Vascular is pleased to provide you with this summary of the Medicare Physician Fee Schedule (PFS)
Future of Rural Healthcare Strategies for Success. Iowa Healthcare Collaborative 13 th Annual Conference August 16, 2016 Eric K.
 Future of Rural Healthcare Strategies for Success Iowa Healthcare Collaborative 13 th Annual Conference August 16, 2016 Eric K. Shell, CPA, MBA The Healthcare Environment Has Changed! In the past 36 months,
Future of Rural Healthcare Strategies for Success Iowa Healthcare Collaborative 13 th Annual Conference August 16, 2016 Eric K. Shell, CPA, MBA The Healthcare Environment Has Changed! In the past 36 months,
CMS Cardiac (AMI & CABG), SHFFT and Cardiac Rehab. Demo - Overview. September 13, 2016
, SHFFT and Cardiac Rehab. Demo - Overview. September 13, 2016") CMS Cardiac (AMI & CABG), SHFFT and Cardiac Rehab. Demo - Overview September 13, 2016 Cardiac (AMI & CABG), SHFFT (Surgical Hip/Femur Fracture Treatment) & Cardiac Rehabilitation Demo Why expand Comprehensive
CMS Cardiac (AMI & CABG), SHFFT and Cardiac Rehab. Demo - Overview September 13, 2016 Cardiac (AMI & CABG), SHFFT (Surgical Hip/Femur Fracture Treatment) & Cardiac Rehabilitation Demo Why expand Comprehensive
Coverage Expansion [Sections 310, 323, 324, 341, 342, 343, 344, and 1701]
![Coverage Expansion [Sections 310, 323, 324, 341, 342, 343, 344, and 1701]](/thumbs/87/96500790.jpg "Coverage Expansion [Sections 310, 323, 324, 341, 342, 343, 344, and 1701]") Summary of the U.S. House of Representatives Health Reform Bill October 2009 The following summarizes the major hospital and health system provisions included in the U.S. House of Representatives health
Summary of the U.S. House of Representatives Health Reform Bill October 2009 The following summarizes the major hospital and health system provisions included in the U.S. House of Representatives health
Clinically Integrated Networks and Population Health The next chapter in healthcare
 Clinically Integrated Networks and Population Health The next chapter in healthcare M A T T H E W M A T U S I A K, D H S C, F R I P H ( UK) M T ( A S C P ) Health System Challenges While the Uninsured
Clinically Integrated Networks and Population Health The next chapter in healthcare M A T T H E W M A T U S I A K, D H S C, F R I P H ( UK) M T ( A S C P ) Health System Challenges While the Uninsured
Bundled Payment: Practicalities, Contractual and Governance Issues
 Bundled Payment: Practicalities, Contractual and Governance Issues Alice G. Gosfield Medicare Medicaid Institute American Health Lawyers Association March 22, 2013 c.2013, Alice G. Gosfield Overview Definitions,
Bundled Payment: Practicalities, Contractual and Governance Issues Alice G. Gosfield Medicare Medicaid Institute American Health Lawyers Association March 22, 2013 c.2013, Alice G. Gosfield Overview Definitions,
AMERICAN COLLEGE OF GASTROENTEROLOGY MAKING $ENSE OF MACRA
 AMERICAN COLLEGE OF GASTROENTEROLOGY 6400 Goldsboro Road, Suite 200, Bethesda, Maryland 20817-5842; P: 301-263-9000; F: 301-263-9025 MAKING $ENSE OF MACRA CMS.SGR MACRA MIPS APMs QCDRs ACOs Why does Washington
AMERICAN COLLEGE OF GASTROENTEROLOGY 6400 Goldsboro Road, Suite 200, Bethesda, Maryland 20817-5842; P: 301-263-9000; F: 301-263-9025 MAKING $ENSE OF MACRA CMS.SGR MACRA MIPS APMs QCDRs ACOs Why does Washington
ACOs/Shared Savings Demonstration Project: What Does It All Mean?
 ACOs/Shared Savings Demonstration Project: What Does It All Mean? None Conflicts of Interest Sean P. Roddy, MD Albany, NY Accountable Care Organizations Term introduced in 2006 by Fisher et al. the hospital
ACOs/Shared Savings Demonstration Project: What Does It All Mean? None Conflicts of Interest Sean P. Roddy, MD Albany, NY Accountable Care Organizations Term introduced in 2006 by Fisher et al. the hospital
Case Study Background Reading Strategic Management - Banks
 Case Study Background Reading Strategic Management - Banks The CEO of St. Sebastian Health System, a moderate-sized hospital system in a mid-sized, Midwest city has hired you to help turn things around.
Case Study Background Reading Strategic Management - Banks The CEO of St. Sebastian Health System, a moderate-sized hospital system in a mid-sized, Midwest city has hired you to help turn things around.
MACRA Final Rule Summary
 MACRA Final Rule Summary On October 14, 2016, the Centers for Medicare and Medicaid Services (CMS) released its final rule implementing the Medicare Access and CHIP Reauthorization Act of 2015 (MACRA),
MACRA Final Rule Summary On October 14, 2016, the Centers for Medicare and Medicaid Services (CMS) released its final rule implementing the Medicare Access and CHIP Reauthorization Act of 2015 (MACRA),
Fee for Service: Paying for Volume, Not Value
 Payment Reform 1 Fee for Service: Paying for Volume, Not Value Most healthcare services are reimbursed with a fee-for-service model. Pay regardless of quality, outcomes Pay for every test and procedure
Payment Reform 1 Fee for Service: Paying for Volume, Not Value Most healthcare services are reimbursed with a fee-for-service model. Pay regardless of quality, outcomes Pay for every test and procedure
The Road to Value. Aric R. Sharp, MHA, CMPE, FACHE Vice President Accountable Care UnityPoint Health February 3, 2017
 The Road to Value Aric R. Sharp, MHA, CMPE, FACHE Vice President Accountable Care UnityPoint Health February 3, 2017 1,500 Physicians UnityPoint Clinic 17 hospitals + 15 rural network hospitals 35,000
The Road to Value Aric R. Sharp, MHA, CMPE, FACHE Vice President Accountable Care UnityPoint Health February 3, 2017 1,500 Physicians UnityPoint Clinic 17 hospitals + 15 rural network hospitals 35,000
Key Financial and Operational Impacts from the Proposed Rule to Implement MACRA:
 Key Financial and Operational Impacts from the Proposed Rule to Implement MACRA: The proposed rule implementing Access and CHIP Reauthorization Act of 2015 (MACRA) was made available on May 9, 2016. A
Key Financial and Operational Impacts from the Proposed Rule to Implement MACRA: The proposed rule implementing Access and CHIP Reauthorization Act of 2015 (MACRA) was made available on May 9, 2016. A
AMGA MIPS Collaborative. June 21, 2017
 AMGA MIPS Collaborative June 21, 2017 Calculating the MIPS score The MIPS composite performance score will include four weighted categories: MIPS Composite Performance Score Quality Cost Improvement activities
AMGA MIPS Collaborative June 21, 2017 Calculating the MIPS score The MIPS composite performance score will include four weighted categories: MIPS Composite Performance Score Quality Cost Improvement activities
Strategic Purchasing of Medical Devices
 Strategic Purchasing of Medical Devices James C. Robinson Leonard D. Schaeffer Professor of Health Economics Director, Berkeley Center for Health Technology University of California, Berkeley Overview
Strategic Purchasing of Medical Devices James C. Robinson Leonard D. Schaeffer Professor of Health Economics Director, Berkeley Center for Health Technology University of California, Berkeley Overview
Medicare Quality Payment Program Overview (MACRA)
") Medicare Quality Payment Program Overview (MACRA) December 2016 Rev. 12/1/16 Some general observations MACRA is complex More than a replacement for the SGR Many of the new requirements are revisions to
Medicare Quality Payment Program Overview (MACRA) December 2016 Rev. 12/1/16 Some general observations MACRA is complex More than a replacement for the SGR Many of the new requirements are revisions to
Final Rule Summary. Medicare Advancing Care Coordination through Episode Payment Models Program Years: October 1, December 31, 2021
 Final Rule Summary Medicare Advancing Care Coordination through Episode Payment Models Program Years: October 1, 2017- December 31, 2021 April 2017 1 TABLE OF CONTENTS Overview and Resources... 3 Model
Final Rule Summary Medicare Advancing Care Coordination through Episode Payment Models Program Years: October 1, 2017- December 31, 2021 April 2017 1 TABLE OF CONTENTS Overview and Resources... 3 Model
MACRA: New Medicare Reimbursement Models Sharp HealthCare
 MACRA: New Medicare Reimbursement Models Sharp HealthCare August 15, 2016 Nathan M. Bays, Esq. General Counsel, The Health Management Academy Executive Director, Advisors Caitlin Greenbaum, MPH Director,
MACRA: New Medicare Reimbursement Models Sharp HealthCare August 15, 2016 Nathan M. Bays, Esq. General Counsel, The Health Management Academy Executive Director, Advisors Caitlin Greenbaum, MPH Director,
Integrating Population Health Analytics and the EHR Environment Session 87, March 6, 2018
 Integrating Population Health Analytics and the EHR Environment Session 87, March 6, 2018 Nina M. Taggart, MD, Senior Medical Director, Population Health and Payer Relations, Lehigh Valley Health Network
Integrating Population Health Analytics and the EHR Environment Session 87, March 6, 2018 Nina M. Taggart, MD, Senior Medical Director, Population Health and Payer Relations, Lehigh Valley Health Network
2018 Merit-based Incentive Payment System (MIPS) Cost Performance Category Fact Sheet
 Cost Performance Category Fact Sheet") 2018 Merit-based Incentive Payment System (MIPS) Cost Performance Category Fact Sheet What is the Quality Payment Program? The Medicare Access and CHIP Reauthorization Act of 2015 (MACRA) ended the Sustainable
2018 Merit-based Incentive Payment System (MIPS) Cost Performance Category Fact Sheet What is the Quality Payment Program? The Medicare Access and CHIP Reauthorization Act of 2015 (MACRA) ended the Sustainable
The HPfHR 3-Tier System
 The HPfHR 3-Tier System The basic level (Tier 1) of the new healthcare system would cover the entire population- from cradle to grave and would include, based on evidenced based data, all medical, surgical
The HPfHR 3-Tier System The basic level (Tier 1) of the new healthcare system would cover the entire population- from cradle to grave and would include, based on evidenced based data, all medical, surgical
Value-Based Reimbursement Contracting: Strategies for Payer-Provider Success
 Value-Based Reimbursement Contracting: Strategies for Payer-Provider Success Presented by: Jim Wright Vice President, xg Health Solutions Agenda Key Considerations for Value Based Contracting Keys for
Value-Based Reimbursement Contracting: Strategies for Payer-Provider Success Presented by: Jim Wright Vice President, xg Health Solutions Agenda Key Considerations for Value Based Contracting Keys for
FUNDS FLOW METHODOLOGY FOR RISK-BASED CONTRACTS
 CENTER FOR INDUSTRY TRANSFORMATION MAY 2015 FUNDS FLOW METHODOLOGY FOR RISK-BASED CONTRACTS Authors Amy Bibby Partner, DHG Healthcare amy.bibby@dhgllp.com Matthew Fadel Manager, DHG Healthcare matt.fadel@dhgllp.com
CENTER FOR INDUSTRY TRANSFORMATION MAY 2015 FUNDS FLOW METHODOLOGY FOR RISK-BASED CONTRACTS Authors Amy Bibby Partner, DHG Healthcare amy.bibby@dhgllp.com Matthew Fadel Manager, DHG Healthcare matt.fadel@dhgllp.com
FAQs: Accountable Care Organizations (ACOs)
") FAQs: Accountable Care Organizations (ACOs) ACOs are groups of doctors, hospitals, and other health care providers who voluntarily form partnerships to collaborate and share accountability for the quality
FAQs: Accountable Care Organizations (ACOs) ACOs are groups of doctors, hospitals, and other health care providers who voluntarily form partnerships to collaborate and share accountability for the quality
Prepare Your Lab for PAMA: Understand How Your Costs Compare to New Reimbursements! Brad Brimhall, MD, MPH March 21, 2017
 Prepare Your Lab for PAMA: Understand How Your Costs Compare to New Reimbursements! Brad Brimhall, MD, MPH March 21, 2017 Financial Center Schizophrenia in the Lab Revenue Center Inpatient Expense/Cost
Prepare Your Lab for PAMA: Understand How Your Costs Compare to New Reimbursements! Brad Brimhall, MD, MPH March 21, 2017 Financial Center Schizophrenia in the Lab Revenue Center Inpatient Expense/Cost
CNYCC Joint Board and Finance Committee Forum
 1 CNYCC Joint Board and Finance Committee Forum December 1, 2015 Michael Bailit Bailit Health 2 Meeting Agenda 1. Value-Based Payment Overview Environmental Context New York State Roadmap DSRIP Payment
1 CNYCC Joint Board and Finance Committee Forum December 1, 2015 Michael Bailit Bailit Health 2 Meeting Agenda 1. Value-Based Payment Overview Environmental Context New York State Roadmap DSRIP Payment
2018 Merit-Based Incentive Payment System (MIPS) Scoring Overview
 Scoring Overview") The Physicians Advocacy Institute s Medicare Quality Payment Program (QPP) Physician Education Initiative 2018 Merit-Based Incentive Payment System (MIPS) Scoring Overview 1 P a g e MEDICARE QPP PHYSICIAN
The Physicians Advocacy Institute s Medicare Quality Payment Program (QPP) Physician Education Initiative 2018 Merit-Based Incentive Payment System (MIPS) Scoring Overview 1 P a g e MEDICARE QPP PHYSICIAN
9/7/17. MACRA: The Knowns and the Unknowns. Disclosures. Goals and Objectives
 MACRA: The Knowns and the Unknowns Sharon K. Merrick, M.S., CCS-P Director of Payment and Practice Management American Society of Anesthesiologists Wisconsin Society of Anesthesiologists September 10,
MACRA: The Knowns and the Unknowns Sharon K. Merrick, M.S., CCS-P Director of Payment and Practice Management American Society of Anesthesiologists Wisconsin Society of Anesthesiologists September 10,
Bundled Payment: Practicalities, Contractual and Governance Issues
 Bundled Payment: Practicalities, Contractual and Governance Issues Alice G. Gosfield Physicians and Physician Organizations Law Institute Hospitals and Health Systems Law Institute February 12, 2013 c.2013,
Bundled Payment: Practicalities, Contractual and Governance Issues Alice G. Gosfield Physicians and Physician Organizations Law Institute Hospitals and Health Systems Law Institute February 12, 2013 c.2013,
Future Healthcare Payment Models An Overview
 Future Healthcare Payment Models An Overview Carter Dredge THERE IS A CRITICAL NEED TO TRANSFORM HEALTHCARE DELIVERY & PAYMENT 2 Significant Variation in Population Utilization Spine Surgeries per 1,000
Future Healthcare Payment Models An Overview Carter Dredge THERE IS A CRITICAL NEED TO TRANSFORM HEALTHCARE DELIVERY & PAYMENT 2 Significant Variation in Population Utilization Spine Surgeries per 1,000
Evidence-Based Program Reimbursement Strategies. Timothy P. McNeill, RN, MPH
 Evidence-Based Program Reimbursement Strategies Timothy P. McNeill, RN, MPH 1 Medicare & Value Based Purchasing 2 Medicare Advantage Changes 3 DSMT Requirements 4 CDSME Tip Sheet Opportunities for EB Programs
Evidence-Based Program Reimbursement Strategies Timothy P. McNeill, RN, MPH 1 Medicare & Value Based Purchasing 2 Medicare Advantage Changes 3 DSMT Requirements 4 CDSME Tip Sheet Opportunities for EB Programs
Physician Compensation In Today s Changing Market
 Physician Compensation In Today s Changing Market PRESENTED BY: STEVE RICE, AREA PRESIDENT, INTEGRATED HEALTHCARE STRATEGIES STEVE MCCAMY, PRESIDENT AND CEO OF COVENANT MEDICAL GROUP NOVEMBER 9, 2016 Agenda
Physician Compensation In Today s Changing Market PRESENTED BY: STEVE RICE, AREA PRESIDENT, INTEGRATED HEALTHCARE STRATEGIES STEVE MCCAMY, PRESIDENT AND CEO OF COVENANT MEDICAL GROUP NOVEMBER 9, 2016 Agenda
I. Recommendations Related to the Definition of More Than Nominal Risk in Alternative Payment Models
 320 Ft. Duquesne Boulevard Suite 20-J Pittsburgh, PA 15222 Voice: (412) 803-3650 Fax: (412) 803-3651 www.chqpr.org August 21, 2017 Seema Verma Administrator Centers for & Medicaid Services U.S. Department
320 Ft. Duquesne Boulevard Suite 20-J Pittsburgh, PA 15222 Voice: (412) 803-3650 Fax: (412) 803-3651 www.chqpr.org August 21, 2017 Seema Verma Administrator Centers for & Medicaid Services U.S. Department
Building a healthier world
 Building a healthier world Improving health care with accountable care John Stockton April 6, 2017 51.25.913.1 (12/16) The current system isn t working It isn t working for our country It isn t working
Building a healthier world Improving health care with accountable care John Stockton April 6, 2017 51.25.913.1 (12/16) The current system isn t working It isn t working for our country It isn t working
March 1, Chairman Lamar Alexander United States Senate Committee on Health, Education, Labor, and Pensions Washington, DC 20510
 March 1, 2019 Chairman Lamar Alexander United States Senate Committee on Health, Education, Labor, and Pensions Washington, DC 20510 Dear Chairman Alexander: On behalf of AMGA and our members, I appreciate
March 1, 2019 Chairman Lamar Alexander United States Senate Committee on Health, Education, Labor, and Pensions Washington, DC 20510 Dear Chairman Alexander: On behalf of AMGA and our members, I appreciate
Impact of ACOs on Care Coordination
 Impact of ACOs on Care Coordination Presented by: Michelle L. Templin Vice President Legislative Affairs and Business Development MHA ACO Network March 2, 2017 Agenda Agenda Key Regulatory Drivers Accountable
Impact of ACOs on Care Coordination Presented by: Michelle L. Templin Vice President Legislative Affairs and Business Development MHA ACO Network March 2, 2017 Agenda Agenda Key Regulatory Drivers Accountable
Medicare Program; Medicare Shared Savings Program: Accountable Care Organizations Proposed Rule
 701 Pennsylvania Ave., NW, Suite 800 Washington, DC 20004-2654 Tel: 202 783 8700 Fax: 202 783 8750 www.advamed.org February 6, 2015 Marilyn Tavenner, Administrator Centers for Medicare & Medicaid Services
701 Pennsylvania Ave., NW, Suite 800 Washington, DC 20004-2654 Tel: 202 783 8700 Fax: 202 783 8750 www.advamed.org February 6, 2015 Marilyn Tavenner, Administrator Centers for Medicare & Medicaid Services
04/12/2016 C H A L L E N G E S F A C I N G U N I T E D S T A T E S H E A L T H C A R E S Y S T E M
 M I C H A E L J. S E E L, M. D. I M P L E M E N T I N G C H A L L E N G E S F A C I N G U N I T E D S T A T E S H E A L T H C A R E S Y S T E M Emphasis on Health care, not Health Fragmented Delivery and
M I C H A E L J. S E E L, M. D. I M P L E M E N T I N G C H A L L E N G E S F A C I N G U N I T E D S T A T E S H E A L T H C A R E S Y S T E M Emphasis on Health care, not Health Fragmented Delivery and
Affordable Care Act Update: Implementing Medicare Costs Savings
 Affordable Care Act Update: Implementing Medicare Costs Savings This new law recognizes that Medicare isn t just something that you re entitled to when you reach 65; it s something that you ve earned.
Affordable Care Act Update: Implementing Medicare Costs Savings This new law recognizes that Medicare isn t just something that you re entitled to when you reach 65; it s something that you ve earned.
No change from proposed rule. healthcare providers and suppliers of services (e.g.,
 American College of Physicians Medicare Shared Savings/Accountable Care Organization (ACO) Final Rule Summary Analysis Category Final Rule Summary Change from Proposed Rule and Comments ACO refers to a
American College of Physicians Medicare Shared Savings/Accountable Care Organization (ACO) Final Rule Summary Analysis Category Final Rule Summary Change from Proposed Rule and Comments ACO refers to a
Medicare at 50. R. B. Drennan, PhD Associate Professor Fox School of Business Temple University 28 January 2016
 Medicare at 50 R. B. Drennan, PhD Associate Professor Fox School of Business Temple University 28 January 2016 Medicare: Beginnings Universal National Health Insurance for all Americans Early Attempts
Medicare at 50 R. B. Drennan, PhD Associate Professor Fox School of Business Temple University 28 January 2016 Medicare: Beginnings Universal National Health Insurance for all Americans Early Attempts
2015 ANNUAL QUALITY AND RESOURCE USE REPORT
 Download Your Report to: --> PDF 508 Compliance CSV 2015 ANNUAL QUALITY AND RESOURCE USE REPORT AND THE 2017 VALUE-BASED PAYMENT MODIFIER SOUTHEAST TEXAS MEDICAL ASSOCIATES LLP LAST FOUR DIGITS OF YOUR
Download Your Report to: --> PDF 508 Compliance CSV 2015 ANNUAL QUALITY AND RESOURCE USE REPORT AND THE 2017 VALUE-BASED PAYMENT MODIFIER SOUTHEAST TEXAS MEDICAL ASSOCIATES LLP LAST FOUR DIGITS OF YOUR
CMS 1701 P UnityPoint Health. October 16, 2018
 CMS 1701 P UnityPoint Health 1776 West Lakes Parkway, Suite 400 West Des Moines, IA 50266 unitypoint.org October 16, 2018 Seema Verma, Administrator Centers for Medicare & Medicaid Services Department
CMS 1701 P UnityPoint Health 1776 West Lakes Parkway, Suite 400 West Des Moines, IA 50266 unitypoint.org October 16, 2018 Seema Verma, Administrator Centers for Medicare & Medicaid Services Department
Bright Health Plan. Confirmed Complaints: N/A. Quality Overview. How Often Do Members Complain About This Company? Accreditation Exchange Product
 Quality Overview Plan Accreditation Exchange Product Accrediting Organization: Accreditation Status: URAC Health Plan Accreditation (Marketplace ) Pending Full: Organization demonstrates full compliance
Quality Overview Plan Accreditation Exchange Product Accrediting Organization: Accreditation Status: URAC Health Plan Accreditation (Marketplace ) Pending Full: Organization demonstrates full compliance
Current State of Medicare. Robert Roth & John Hellow Hooper, Lundy & Bookman, PC
 Current State of Medicare Robert Roth & John Hellow Hooper, Lundy & Bookman, PC Rule for FY 2016 A. FY 2017 Final Rule Released Aug. 2, 2016 (printed in Federal Register Aug. 22, 2016) B. FY 2018 Proposed
Current State of Medicare Robert Roth & John Hellow Hooper, Lundy & Bookman, PC Rule for FY 2016 A. FY 2017 Final Rule Released Aug. 2, 2016 (printed in Federal Register Aug. 22, 2016) B. FY 2018 Proposed
Current State of Medicare
 Current State of Medicare Robert Roth & John Hellow Hooper, Lundy & Bookman, PC Rule for FY 2016 A. FY 2017 Final Rule Released Aug. 2, 2016 (printed in Federal Register Aug. 22, 2016) B. FY 2018 Proposed
Current State of Medicare Robert Roth & John Hellow Hooper, Lundy & Bookman, PC Rule for FY 2016 A. FY 2017 Final Rule Released Aug. 2, 2016 (printed in Federal Register Aug. 22, 2016) B. FY 2018 Proposed
Scripps Health ACO Update
 June 2016 Scripps Health ACO Update Marc Reynolds Senior Vice President, Payer Relations Scripps Health Anil N. Keswani, MD Corporate Vice President, Population Health Management Scripps Health 10 Key
June 2016 Scripps Health ACO Update Marc Reynolds Senior Vice President, Payer Relations Scripps Health Anil N. Keswani, MD Corporate Vice President, Population Health Management Scripps Health 10 Key
Embracing the Future of Care Delivery: What have we learned?
 Embracing the Future of Care Delivery: What have we learned? Robert Nesse, M.D. Senior Advisor for Healthcare Policy and Payment Reform CEO, Mayo Clinic Health System 2010-2015 2014 MFMER slide-1 Fundamental
Embracing the Future of Care Delivery: What have we learned? Robert Nesse, M.D. Senior Advisor for Healthcare Policy and Payment Reform CEO, Mayo Clinic Health System 2010-2015 2014 MFMER slide-1 Fundamental
PRIMER: MACRA and the Merit-based Incentive Payment System (MIPS) Tara O Neill Hayes January 31, 2016
 Tara O Neill Hayes January 31, 2016") PRIMER: MACRA and the Merit-based Incentive Payment System (MIPS) Tara O Neill Hayes January 31, 2016 Background On April 16, 2015, the Medicare Access and CHIP Reauthorization Act (MACRA) was signed into
PRIMER: MACRA and the Merit-based Incentive Payment System (MIPS) Tara O Neill Hayes January 31, 2016 Background On April 16, 2015, the Medicare Access and CHIP Reauthorization Act (MACRA) was signed into
MACRA Medicare Payment Reform and the Implications to Medicare Advantage Plans
 BEYOND THE NUMBERS MACRA Medicare Payment Reform and the Implications to Medicare Advantage Plans True BUSINESS PowerPoint Presentation Template November 2018 PRESENTED BY Bob Moné, FSA, MAAA Liz Myers,
BEYOND THE NUMBERS MACRA Medicare Payment Reform and the Implications to Medicare Advantage Plans True BUSINESS PowerPoint Presentation Template November 2018 PRESENTED BY Bob Moné, FSA, MAAA Liz Myers,
The Health Insurance Market in Virginia. Maureen Dempsey, MD, MSc, ACC, FAAP Anthem Blue Cross and Blue Shield June 8, 2017
 The Health Insurance Market in Virginia Maureen Dempsey, MD, MSc, ACC, FAAP Anthem Blue Cross and Blue Shield June 8, 2017 Anthem Inc. at a Glance Broad geographic footprint and customer base ` BCBS plans
The Health Insurance Market in Virginia Maureen Dempsey, MD, MSc, ACC, FAAP Anthem Blue Cross and Blue Shield June 8, 2017 Anthem Inc. at a Glance Broad geographic footprint and customer base ` BCBS plans
Elevate by Denver Health Medical Plan
 Quality Overview by Denver Health Medical Plan Accreditation Exchange Product Accrediting Organization: Accreditation Status: NCQA Health Plan Accreditation (Marketplace HMO) Accredited* Excellent: Organization
Quality Overview by Denver Health Medical Plan Accreditation Exchange Product Accrediting Organization: Accreditation Status: NCQA Health Plan Accreditation (Marketplace HMO) Accredited* Excellent: Organization
Healthcare Value Purchasing: Perspectives from Employers, Facilities and Consumers
 Healthcare Value Purchasing: Perspectives from Employers, Facilities and Consumers Montana Chamber of Commerce Healthcare Forum November 29-30, 2016 Shane Wolverton SVP CORPORATE DEVELOPMENT, QUANTROS
Healthcare Value Purchasing: Perspectives from Employers, Facilities and Consumers Montana Chamber of Commerce Healthcare Forum November 29-30, 2016 Shane Wolverton SVP CORPORATE DEVELOPMENT, QUANTROS
HIGHLIGHTS. CMS estimates that the net market basket update would increase Medicare SNF payments by approximately $390 million in FY 2018.
 Summary of 2018 Skilled Nursing Center Prospective Payment System Proposed Rule and Pre-Rule on Possible New Payment System Our rates increase 1.0 percent starting October 1, 2017 April 27, 2017 Today,
Summary of 2018 Skilled Nursing Center Prospective Payment System Proposed Rule and Pre-Rule on Possible New Payment System Our rates increase 1.0 percent starting October 1, 2017 April 27, 2017 Today,
AHLA. V. Complex Contracting in the 21st Century between Payers and Providers
 AHLA V. Complex Contracting in the 21st Century between Payers and Providers Lisa A. Hathaway Vice President and Chief Medicare Counsel Aetna Bethesda, MD Alan E. Schabes Benesch Friedlander Coplan & Aronoff
AHLA V. Complex Contracting in the 21st Century between Payers and Providers Lisa A. Hathaway Vice President and Chief Medicare Counsel Aetna Bethesda, MD Alan E. Schabes Benesch Friedlander Coplan & Aronoff
Medicare payment policy and its impact on program spending
 Medicare payment policy and its impact on program spending James E. Mathews, Ph.D. Deputy Director, Medicare Payment Advisory Commission February 8, 2013 Outline of today s presentation Brief background
Medicare payment policy and its impact on program spending James E. Mathews, Ph.D. Deputy Director, Medicare Payment Advisory Commission February 8, 2013 Outline of today s presentation Brief background
MACRA: Redefining How CMS Pays Doctors. White Paper ELLIS MAC KNIGHT, MD DAN KIEHL, JD CONTACT. Senior Vice President/CMO. Associate Consultant
 MACRA: Redefining How CMS Pays Doctors White Paper ELLIS MAC KNIGHT, MD Senior Vice President/CMO DAN KIEHL, JD Associate Consultant June 2016 CONTACT For further information about Coker Group and how
MACRA: Redefining How CMS Pays Doctors White Paper ELLIS MAC KNIGHT, MD Senior Vice President/CMO DAN KIEHL, JD Associate Consultant June 2016 CONTACT For further information about Coker Group and how
Healthcare Finance Trends and Perspectives
 Healthcare Finance Trends and Perspectives AONE Annual Conference, Fort Worth, TX April 2 nd, 2016 Chuck Alsdurf, MAcc, CPA Director, Healthcare Finance Policy, Operational Initiatives Healthcare Financial
Healthcare Finance Trends and Perspectives AONE Annual Conference, Fort Worth, TX April 2 nd, 2016 Chuck Alsdurf, MAcc, CPA Director, Healthcare Finance Policy, Operational Initiatives Healthcare Financial