ENROLLMENT FORMS FOR SELF-DIRECTED DROP PLAN
|
|
|
- Elvin Wheeler
- 5 years ago
- Views:
Transcription

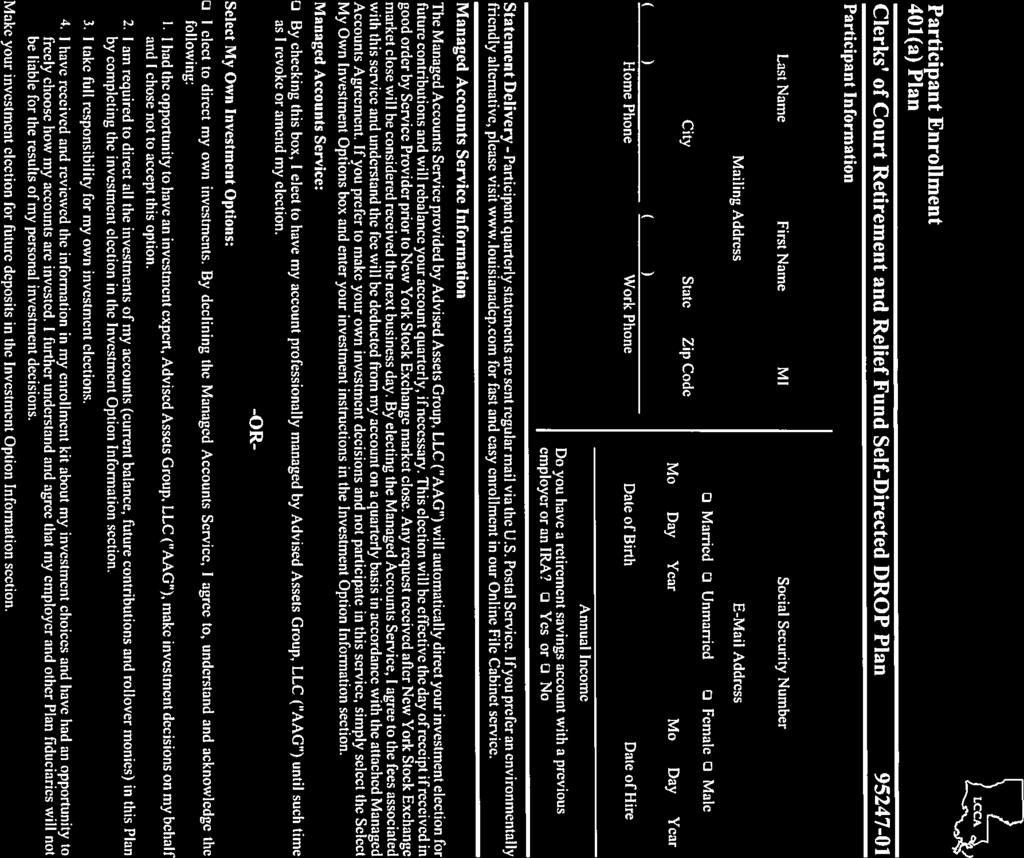
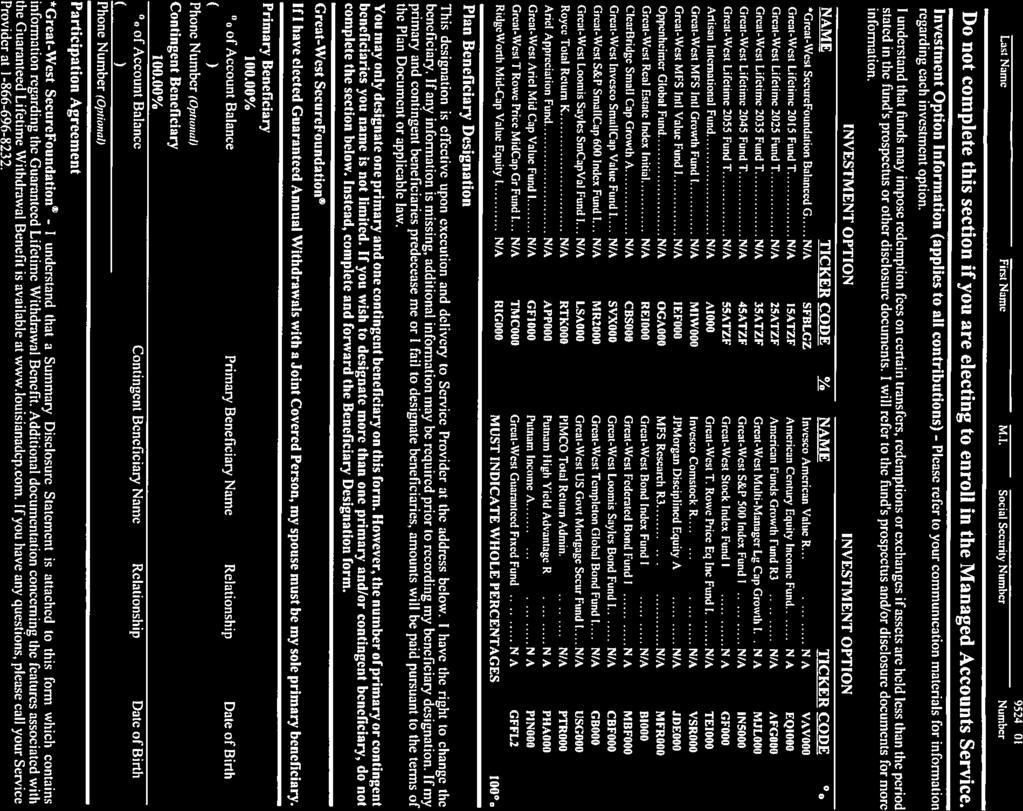
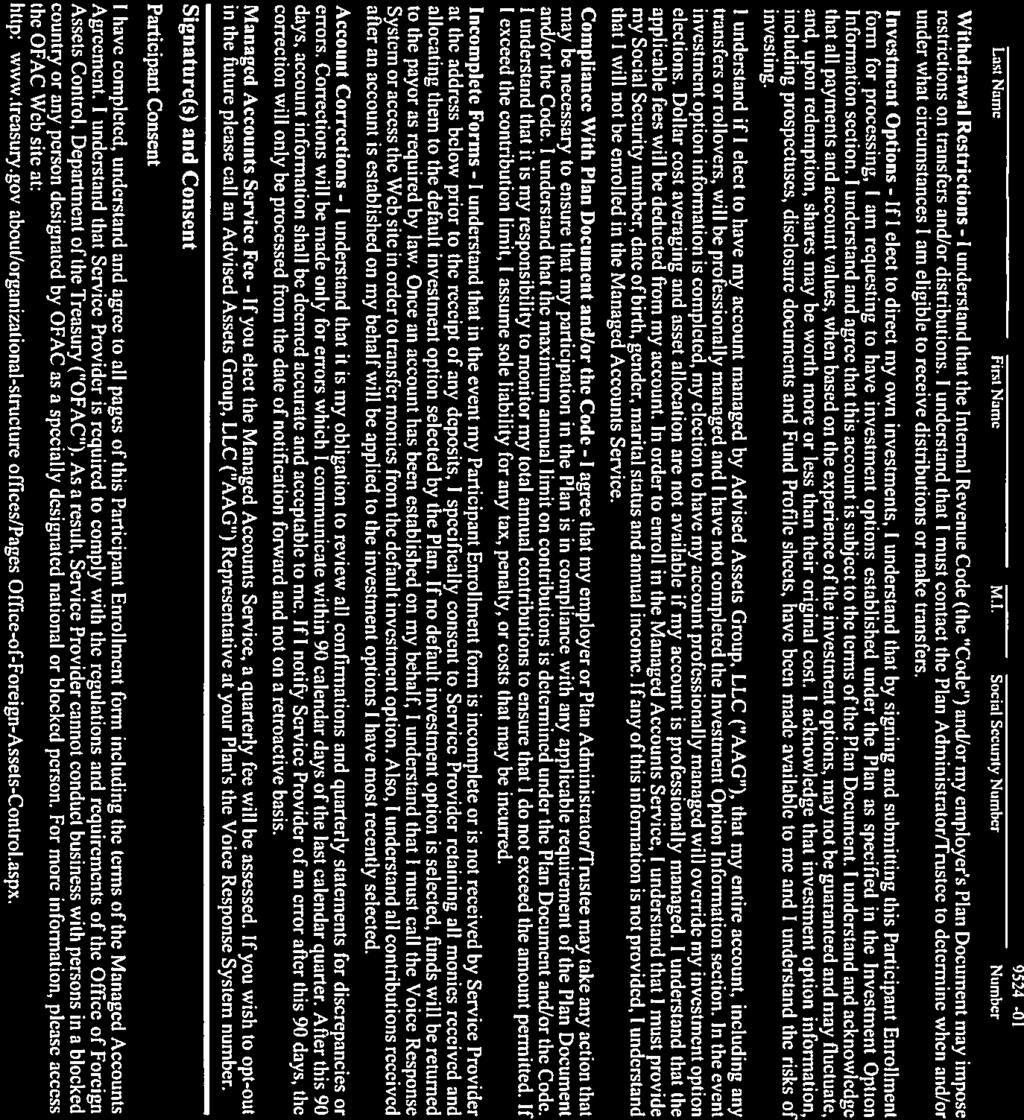
1 LOUISIANA CLERKS OF COURT RETIREMENT AND RELIEF FUND Jefferson Highway, Building A Suite B-1 Baton Rouge, Louisiana TELEPHONE (225) (800) FACSIMILE (225) DEBBIE D. HUDNALL EXECUTIVE DIRECTOR ENROLLMENT FORMS FOR SELF-DIRECTED DROP PLAN EMPOWER RETIREMENT SERVICES FORMS MUST BE COMPLETED AND RETURNED TO: LA CLERKS OF COURT RETIREMENT & RELIEF FUND JEFFERSON HIGHWAY, BUILDING A BATON ROUGE, LA 70809
2 LOUISIANA CLERKS OF COURT RETIREMENT AND RELIEF FUND IRREVOCABLE WAIVER **Member must initial each paragraph for Irrevocable Waiver to be valid** I,, acknowledge that I have certain rights regarding the interest earned on my Deferred Retirement Option Plan (DROP) account which are protected by Article X, Section 29 of the Louisiana Constitution. I understand that I am waiving my right to be in the Clerks of Court Retirement and Relief Fund ( LCCR ) traditional DROP account. I understand that by choosing to participate in the Self-Directed Plan (SDP), I must move 100% of my balance from the traditional DROP account to the SDP. I acknowledge my right to have my DROP account earn interest at money market investment rates guaranteed to be no less than zero if I choose not to sign this election and waiver. I make this irrevocable waiver of my constitutional rights as set forth in Article X, Section 29(A) and (B) of the Louisiana Constitution as it relates to my subaccount in the SDP, including, but not necessarily limited to, as regards the interest earnings on my DROP account. I understand that the word irrevocable means that I will not at any time be able to change my mind after I sign this waiver. I acknowledge that, by choosing to participate in the SDP, the benefits payable to me are not the obligations of the state or the system, and that any returns and other rights of the plan are the sole liability and responsibility of myself and Great-West Retirement Services. I understand that by choosing to sign this document and electing to participate in the SDP, I can elect a beneficiary other than my spouse without my spouse s signature. I understand that by signing this waiver, then the Clerks Retirement and Relief Fund shall no longer monitor any of my beneficiary designations. I agree that Great-West Retirement Services and I shall be responsible for complying with all applicable provisions of the Internal Revenue Code. I agree that if any violation of the Internal Revenue Code occurs as a result of my participation in Great-West Retirement Services, it shall be the sole responsibility and liability of me and Great-West Retirement Services, not the state or LCCR. I understand that there shall be no liability on the part of and no cause of action of any nature shall arise against the state, LCCR, or its agents or employees, for any action taken by me for choices I make in relationship to the funds in which I choose to place my subaccount balance once I move to Great-West Retirement Services. I understand that by signing this waiver, my DROP account balance will not be protected by the Louisiana Constitution. My DROP, account balance will earn interest as returned by my self-directed DROP account with Great-West Retirement Services. I fully understand the risks involved in electing this option and do hereby knowingly assume this risk. I understand that, by signing this waiver, the amount of money in my DROP account will be reduced if the return on my self-directed DROP account is negative. I acknowledge that I may call the retirement system office and ask questions or seek additional information prior to signing this waiver. Signed in,,, 20. (City) (State) (Month/Day) (Year) (First Witness Signature) (Member s Signature) (Second Witness Signature) MAIL FORMS TO: Clerks of Court Retirement and Relief Fund Jefferson Highway, Building A Baton Rouge, LA 70809
3
4
5
6
7
8

9
10
11
12
13
14
15
16
17
ENROLLMENT FORMS FOR SELF-DIRECTED DROP PLAN GREAT-WEST RETIREMENT SERVICES
 LOUISIANA CLERKS OF COURT RETIREMENT AND RELIEF FUND 11745 Bricksome Avenue Suite B-1 Baton Rouge, Louisiana 70816 TELEPHONE (225) 293-1162 (800) 256-6660 FACSIMILE (225) 291-7859 DEBBIE D. HUDNALL EXECUTIVE
LOUISIANA CLERKS OF COURT RETIREMENT AND RELIEF FUND 11745 Bricksome Avenue Suite B-1 Baton Rouge, Louisiana 70816 TELEPHONE (225) 293-1162 (800) 256-6660 FACSIMILE (225) 291-7859 DEBBIE D. HUDNALL EXECUTIVE
Welcome! Retiree Workshop July 26, 2017
 Welcome! Retiree Workshop July 26, 2017 MEET THE RED TEAM Retirement Education Department JANET HARRIS WENDY DEMOUY CARLOS JONES CHARLES WOOD Retirement Benefits Specialist Retirement Benefits Educator
Welcome! Retiree Workshop July 26, 2017 MEET THE RED TEAM Retirement Education Department JANET HARRIS WENDY DEMOUY CARLOS JONES CHARLES WOOD Retirement Benefits Specialist Retirement Benefits Educator
I HAVE RECEIVED AND READ THE ENCLOSED 9-PAGE SPECIAL TAX NOTICE:
 I HAVE RECEIVED AND READ THE ENCLOSED 9-PAGE SPECIAL TAX NOTICE: Date: Member s Signature Print Name Note: Please return ONLY this page to: Louisiana Sheriffs Pension & Relief Fund 1225 Nicholson Drive
I HAVE RECEIVED AND READ THE ENCLOSED 9-PAGE SPECIAL TAX NOTICE: Date: Member s Signature Print Name Note: Please return ONLY this page to: Louisiana Sheriffs Pension & Relief Fund 1225 Nicholson Drive
PLAN A MONTHLY REPORT OF EARNINGS AND CONTRIBUTIONS RATES EFFECTIVE 7/01/17 THROUGH 6/30/18 REPORT DUE BY 10TH OF MONTH SAMPLE
 PLAN A Municipal Employees' Retirement System of LA (MERS) 7937 Office Park Boulevard Baton Rouge, LA 70809 Phone: 225-925-4810 * Toll Free: 800-820-1137 * Fax: 225-925-4816 3 MONTHLY REPORT OF EARNINGS
PLAN A Municipal Employees' Retirement System of LA (MERS) 7937 Office Park Boulevard Baton Rouge, LA 70809 Phone: 225-925-4810 * Toll Free: 800-820-1137 * Fax: 225-925-4816 3 MONTHLY REPORT OF EARNINGS
REQUEST FOR DROP/BACK-DROP DISTRIBUTION
 REQUEST FOR DROP/BACK-DROP DISTRIBUTION LOUISIANA DISTRICT ATTORNEYS RETIREMENT SYSTEM 1645 NICHOLSON DRIVE BATON ROUGE, LOUISIANA 70802 (225)267-4824 IMPORTANT: Before completing this form, please read
REQUEST FOR DROP/BACK-DROP DISTRIBUTION LOUISIANA DISTRICT ATTORNEYS RETIREMENT SYSTEM 1645 NICHOLSON DRIVE BATON ROUGE, LOUISIANA 70802 (225)267-4824 IMPORTANT: Before completing this form, please read
L O U I S I A N A I N S U R A N C E G U A R A N T Y A S S O C I A T I O N
 L O U I S I A N A I N S U R A N C E G U A R A N T Y A S S O C I A T I O N LIGA To be completed by all persons making claims against the Louisiana Insurance Guaranty Association ( LIGA ) pursuant to the
L O U I S I A N A I N S U R A N C E G U A R A N T Y A S S O C I A T I O N LIGA To be completed by all persons making claims against the Louisiana Insurance Guaranty Association ( LIGA ) pursuant to the
BENEFIT ENROLLMENT FORM
 EMPLOYEE INFORMATION BENEFIT ENROLLMENT FORM Name: Address: City: State: Zip: Phone # SSN#: G-ID#: Birth : Gender: Male Female Primary Care Physician: PCP Code: BENEFIT ELECTIONS (see Medical Rates Sheet
EMPLOYEE INFORMATION BENEFIT ENROLLMENT FORM Name: Address: City: State: Zip: Phone # SSN#: G-ID#: Birth : Gender: Male Female Primary Care Physician: PCP Code: BENEFIT ELECTIONS (see Medical Rates Sheet
TRANSMITTAL INFORMATION For All Business Filings
 JAY DARDENNE SECRETARY OF STATE STATE OF LOUISIANA SECRETARY OF STATE Commercial (225) 925-4704 (225) 922-0435 Fax Administrative Services (225) 925-4704 (225) 925-4726 Fax Uniform Commercial Code (225)
JAY DARDENNE SECRETARY OF STATE STATE OF LOUISIANA SECRETARY OF STATE Commercial (225) 925-4704 (225) 922-0435 Fax Administrative Services (225) 925-4704 (225) 925-4726 Fax Uniform Commercial Code (225)
BOARD OF TAX APPEALS STATE OF LOUISIANA
 BOARD OF TAX APPEALS STATE OF LOUISIANA, B.T.A. DOCKET NO. Petitioner versus KIMBERLY L. ROBINSON, SECRETARY, DEPARTMENT OF REVENUE, STATE OF LOUISIANA Respondent PETITION TO REVIEW DENIAL OF REFUND/CREDIT
BOARD OF TAX APPEALS STATE OF LOUISIANA, B.T.A. DOCKET NO. Petitioner versus KIMBERLY L. ROBINSON, SECRETARY, DEPARTMENT OF REVENUE, STATE OF LOUISIANA Respondent PETITION TO REVIEW DENIAL OF REFUND/CREDIT
Spouse's Consent to Waive a Qualified Joint and Survivor Annuity
 Spouse's Consent to Waive a Qualified Joint and Survivor Annuity Instruction: The sample language does not address the one-year-of-marriage rule under section 417(d); if a plan applies the one-year rule,
Spouse's Consent to Waive a Qualified Joint and Survivor Annuity Instruction: The sample language does not address the one-year-of-marriage rule under section 417(d); if a plan applies the one-year rule,
DESIGNATION OF BENEFICIARY FORM FOR PRE-RETIREMENT DEATH BENEFITS ONLY
 DESIGNATION OF BENEFICIARY FORM FOR PRE-RETIREMENT DEATH BENEFITS ONLY Please read these instructions before completing the form. Use this form to designate or change a beneficiary only for Pre-Retirement
DESIGNATION OF BENEFICIARY FORM FOR PRE-RETIREMENT DEATH BENEFITS ONLY Please read these instructions before completing the form. Use this form to designate or change a beneficiary only for Pre-Retirement
NOTICE OF BENEFIT WITHDRAWAL (Complete Entire Set of Forms and Return)
") NOTICE OF BENEFIT WITHDRAWAL (Complete Entire Set of Forms and Return) TO: SSN: On, your account balance in the Southwestern Illinois Laborers Annuity Fund was. Normally, the Trustee will compute the value
NOTICE OF BENEFIT WITHDRAWAL (Complete Entire Set of Forms and Return) TO: SSN: On, your account balance in the Southwestern Illinois Laborers Annuity Fund was. Normally, the Trustee will compute the value
CITY OF HOLLYWOOD NOTICE OF INTENT AND AGREEMENT TO PARTICIPATE IN THE PLANNED RETIREMENT BENEFIT
 CITY OF HOLLYWOOD NOTICE OF INTENT AND AGREEMENT TO PARTICIPATE IN THE PLANNED RETIREMENT BENEFIT Employee's Name:. Employee's Normal Retirement Date:. Maximum Number of Years Employee May Participate
CITY OF HOLLYWOOD NOTICE OF INTENT AND AGREEMENT TO PARTICIPATE IN THE PLANNED RETIREMENT BENEFIT Employee's Name:. Employee's Normal Retirement Date:. Maximum Number of Years Employee May Participate
Paul Hastings LLP Defined Contribution Retirement Plan (401k) Beneficiary Designation Form
 Beneficiary Designation Form") Paul Hastings LLP Defined Contribution Retirement Plan (401k) Beneficiary Designation Form Print Name: Job Title: Social Security Number: (Optional) I understand that benefits are paid out in a lump sum.
Paul Hastings LLP Defined Contribution Retirement Plan (401k) Beneficiary Designation Form Print Name: Job Title: Social Security Number: (Optional) I understand that benefits are paid out in a lump sum.
Southern California Pipe Trades
 Southern California Pipe Trades LO56050514 (Retired) Defined Contribution Fund Retirement/Disability/Termination Distribution LO56050517 (Disabled) Application Complete all applicable sections and return
Southern California Pipe Trades LO56050514 (Retired) Defined Contribution Fund Retirement/Disability/Termination Distribution LO56050517 (Disabled) Application Complete all applicable sections and return
FORM 6. PENSION PARTNER WAIVER ON TRANSFER to a LIF, DC RIA OR ANNUITY
 FINANCE Superintendent of Pensions FORM 6 PENSION PARTNER WAIVER ON TRANSFER to a LIF, DC RIA OR ANNUITY Part 1 Waiver of Up to 50% Unlocking, Minimum 60% Joint Life Pension/Retirement Income I,, am a
FINANCE Superintendent of Pensions FORM 6 PENSION PARTNER WAIVER ON TRANSFER to a LIF, DC RIA OR ANNUITY Part 1 Waiver of Up to 50% Unlocking, Minimum 60% Joint Life Pension/Retirement Income I,, am a
Beneficiary Designation
 Beneficiary Designation INSTRUCTIONS To designate a beneficiary or to change your existing beneficiary designation on your plan, complete all applicable sections of this form, obtain any required signatures,
Beneficiary Designation INSTRUCTIONS To designate a beneficiary or to change your existing beneficiary designation on your plan, complete all applicable sections of this form, obtain any required signatures,
Louisiana Clerks of Court Retirement & Relief Fund REQUEST FOR PROPOSAL INVESTMENT CONSULTING SERVICES
 Louisiana Clerks of Court Retirement & Relief Fund REQUEST FOR PROPOSAL INVESTMENT CONSULTING SERVICES 2018 SECTION I OVERVIEW A. Purpose The Louisiana Clerks of Court Retirement and Relief Fund ( LCCR
Louisiana Clerks of Court Retirement & Relief Fund REQUEST FOR PROPOSAL INVESTMENT CONSULTING SERVICES 2018 SECTION I OVERVIEW A. Purpose The Louisiana Clerks of Court Retirement and Relief Fund ( LCCR
Southern California Pipe Trades
 Southern California Pipe Trades LO56050514 (Retired) Defined Contribution Fund Retirement/Disability/Termination Distribution LO56050517 (Disabled) Application Complete all applicable sections and return
Southern California Pipe Trades LO56050514 (Retired) Defined Contribution Fund Retirement/Disability/Termination Distribution LO56050517 (Disabled) Application Complete all applicable sections and return
Southern California Pipe Trades
 Southern California Pipe Trades LO56050516 Defined Contribution Fund Special Employer Account [401(a)] Withdrawal Application Complete all applicable sections and return pages 1-3 to: Southern California
Southern California Pipe Trades LO56050516 Defined Contribution Fund Special Employer Account [401(a)] Withdrawal Application Complete all applicable sections and return pages 1-3 to: Southern California
PROVIDER TYPE SPECIFIC PACKET/CHECKLIST. (Louisiana Medicaid) ENVIRONMENTAL ACCESSIBILITY ADAPTATIONS (EAA) (Environmental Modifications) CONTRACTOR
 ENVIRONMENTAL ACCESSIBILITY ADAPTATIONS (EAA) (Environmental Modifications) CONTRACTOR") PROVIDER TYPE SPECIFIC PACKET/CHECKLIST (Louisiana Medicaid) ENVIRONMENTAL ACCESSIBILITY ADAPTATIONS (EAA) (Environmental Modifications) CONTRACTOR (Enrollment packet is subject to change without notice)
PROVIDER TYPE SPECIFIC PACKET/CHECKLIST (Louisiana Medicaid) ENVIRONMENTAL ACCESSIBILITY ADAPTATIONS (EAA) (Environmental Modifications) CONTRACTOR (Enrollment packet is subject to change without notice)
IBEW LOCAL NO. 812 ANNUITY PLAN QUALIFIED PRE-RETIREMENT SURVIVOR ANNUITY NOTICE. Participant s Name: Date:
 s Name: Date: IBEW LOCAL NO. 812 ANNUITY PLAN QUALIFIED PRE-RETIREMENT SURVIVOR ANNUITY NOTICE This notice explains the Qualified Pre-Retirement Survivor Annuity under the IBEW Local No. 812 Annuity Plan
s Name: Date: IBEW LOCAL NO. 812 ANNUITY PLAN QUALIFIED PRE-RETIREMENT SURVIVOR ANNUITY NOTICE This notice explains the Qualified Pre-Retirement Survivor Annuity under the IBEW Local No. 812 Annuity Plan
Health Care FSA COBRA ELECTION NOTICE for the Health Care FSA offered through the Office of Group Benefits
 Health Care FSA COBRA ELECTION NOTICE for the Health Care FSA offered through the Office of Group Benefits Date July 4, 2014 Dear: DEPENDENT OF NAME ADDRESS ANY CITY, LA 99999 Introduction This notice
Health Care FSA COBRA ELECTION NOTICE for the Health Care FSA offered through the Office of Group Benefits Date July 4, 2014 Dear: DEPENDENT OF NAME ADDRESS ANY CITY, LA 99999 Introduction This notice
Southern California Pipe Trades
 Southern California Pipe Trades LO56050514 (Retired) Defined Contribution Fund Retirement/Disability/Termination Distribution LO56050517 (Disabled) Application Complete all applicable sections and return
Southern California Pipe Trades LO56050514 (Retired) Defined Contribution Fund Retirement/Disability/Termination Distribution LO56050517 (Disabled) Application Complete all applicable sections and return
Form 1 [Subclause 29.1(4)(b)(ii)] SPOUSE S CONSENT TO TRANSFER TO A REGISTERED RETIREMENT INCOME FUND CONTRACT
![Form 1 [Subclause 29.1(4)(b)(ii)] SPOUSE S CONSENT TO TRANSFER TO A REGISTERED RETIREMENT INCOME FUND CONTRACT](/thumbs/85/92230754.jpg "Form 1 [Subclause 29.1(4)(b)(ii)] SPOUSE S CONSENT TO TRANSFER TO A REGISTERED RETIREMENT INCOME FUND CONTRACT") Saskatchewan Justice Pension Benefits Form 1 [Subclause 29.1(4)(b)(ii)] SPOUSE S CONSENT TO TRANSFER TO A REGISTERED RETIREMENT INCOME FUND CONTRACT I, (print or type full name of spouse) certify that
Saskatchewan Justice Pension Benefits Form 1 [Subclause 29.1(4)(b)(ii)] SPOUSE S CONSENT TO TRANSFER TO A REGISTERED RETIREMENT INCOME FUND CONTRACT I, (print or type full name of spouse) certify that
Southern California Pipe Trades
 Southern California Pipe Trades LO56050505 Defined Contribution Fund Hardship Withdrawal Application Complete all applicable sections and return pages 1-4 to: Southern California Pipe Trades Administrative
Southern California Pipe Trades LO56050505 Defined Contribution Fund Hardship Withdrawal Application Complete all applicable sections and return pages 1-4 to: Southern California Pipe Trades Administrative
FIRST ASSURANCE LIFE OF AMERICA PO DRAWER BATON ROUGE, LA PROOF OF DEATH CREDITOR INSURANCE CLAIM FORM
 PROOF OF DEATH CREDITOR INSURANCE CLAIM FORM INSTRUCTIONS FOR FILING A CLAIM FOR DEATH BENEFITS THIS CLAIM FORM IS USED FOR FILING A DEATH CLAIM WITH. THE CLAIM FORM MUST BE COMPLETED FULLY AND CORRECTLY
PROOF OF DEATH CREDITOR INSURANCE CLAIM FORM INSTRUCTIONS FOR FILING A CLAIM FOR DEATH BENEFITS THIS CLAIM FORM IS USED FOR FILING A DEATH CLAIM WITH. THE CLAIM FORM MUST BE COMPLETED FULLY AND CORRECTLY
PROMISSORY NOTE. 2.1 Payments. During the term of this Note, Borrower shall pay to Lender as follows:
 PROMISSORY NOTE $41,500.00, 2017 FOR VALUE RECEIVED, without defalcation, and intending to be legally bound hereby, CHARLES A MELTON ARTS & EDUCATION CENTER, a Pennsylvania nonprofit corporation, with
PROMISSORY NOTE $41,500.00, 2017 FOR VALUE RECEIVED, without defalcation, and intending to be legally bound hereby, CHARLES A MELTON ARTS & EDUCATION CENTER, a Pennsylvania nonprofit corporation, with
LSU. For Classified July, Agricultural Center. System. their system chart below. of the. of the applicable
 LSU Agricultural Center Retirement Incentive Program For Classified Employees July, 2009 Section 1. Eligibility To be eligible to participate in the LSU Agricultural Center Retirement Incentive Program,
LSU Agricultural Center Retirement Incentive Program For Classified Employees July, 2009 Section 1. Eligibility To be eligible to participate in the LSU Agricultural Center Retirement Incentive Program,
Employee Information Name (Last, First, Initial) Please Print: Address: Gender (M/F): Date of Birth (MM/DD/YYYY): Phone Number: Address:
 Please Print: Address: Gender (M/F): Date of Birth (MM/DD/YYYY): Phone Number: Address:") Employee (Last, First, Initial) Please Print: Address: : (MM/DD/YYYY): Phone Number: E-mail Address: Marital Status: Single Married Widowed Divorced Date of Hire/Change to Eligible Status (MM/DD/YYY):
Employee (Last, First, Initial) Please Print: Address: : (MM/DD/YYYY): Phone Number: E-mail Address: Marital Status: Single Married Widowed Divorced Date of Hire/Change to Eligible Status (MM/DD/YYY):
ADOPT-A-PARK AGREEMENT
 ADOPT-A-PARK AGREEMENT The City of Perth Amboy Adopt-A-Park program is designed to increase community involvement in preserving our City parks. The program is voluntary and is designed for organizations,
ADOPT-A-PARK AGREEMENT The City of Perth Amboy Adopt-A-Park program is designed to increase community involvement in preserving our City parks. The program is voluntary and is designed for organizations,
Western Washington U.A. Supplemental Pension Plan In-service Withdrawal Request Form
 Western Washington U.A. Supplemental Pension Plan In-service Withdrawal Request Form PERSONAL INFORMATION My Name (if new, must include documentation of name change) Social Security number Mailing Address
Western Washington U.A. Supplemental Pension Plan In-service Withdrawal Request Form PERSONAL INFORMATION My Name (if new, must include documentation of name change) Social Security number Mailing Address
Preparation for Individual Counseling. Rank-and-File Members
 Preparation for Individual Counseling Rank-and-File Members Questions to Consider Are you eligible to retire? What type of retirement is best for you? Which retirement option should you select? What should
Preparation for Individual Counseling Rank-and-File Members Questions to Consider Are you eligible to retire? What type of retirement is best for you? Which retirement option should you select? What should
Salary Reduction Contributions Enrollment Form
 Salary Reduction Contributions Enrollment Form Employee Information Employer Name Employee Name (Last, First, Middle) Employee Street Address Department - - Social Security Number / to / (mm/dd) Plan Year
Salary Reduction Contributions Enrollment Form Employee Information Employer Name Employee Name (Last, First, Middle) Employee Street Address Department - - Social Security Number / to / (mm/dd) Plan Year
MEDICAID LOUISIANA PRE ENROLLMENT INSTRUCTIONS MCDLA
 MEDICAID LOUISIANA PRE ENROLLMENT INSTRUCTIONS MCDLA HOW LONG DOES PRE ENROLLMENT TAKE? Standard processing time is 3 weeks. WHERE SHOULD I SEND THE FORMS? Mail the form to: Unisys Provider Enrollment
MEDICAID LOUISIANA PRE ENROLLMENT INSTRUCTIONS MCDLA HOW LONG DOES PRE ENROLLMENT TAKE? Standard processing time is 3 weeks. WHERE SHOULD I SEND THE FORMS? Mail the form to: Unisys Provider Enrollment
Western Washington U.A. Supplemental Pension Plan Request for Distribution Form
 PERSONAL INFORMATION Western Washington U.A. Supplemental Pension Plan Request for Distribution Form Participant Name (if new, must include documentation of name change) Social Security number Mailing
PERSONAL INFORMATION Western Washington U.A. Supplemental Pension Plan Request for Distribution Form Participant Name (if new, must include documentation of name change) Social Security number Mailing
Investor Qualification Section A ALL INDIVIDUAL INVESTORS MUST INITIAL AT LEAST ONE OF THE FOLLOWING:
 THIS IS NOT AN OFFER TO SELL SECURITIES. THE PURPOSE OF THIS QUESTIONAIRE IS TO ESTABLISH A PRE-EXISTING RELATIONSHIP AND TO VERIFY THAT YOU ARE QUALIFIED TO INVEST IF WE HAVE ANY AVAILABLE OFFERINGS IN
THIS IS NOT AN OFFER TO SELL SECURITIES. THE PURPOSE OF THIS QUESTIONAIRE IS TO ESTABLISH A PRE-EXISTING RELATIONSHIP AND TO VERIFY THAT YOU ARE QUALIFIED TO INVEST IF WE HAVE ANY AVAILABLE OFFERINGS IN
Consolidated Public Retirement Board
 Consolidated Public Retirement Board 4101 MacCorkle Avenue, SE Charleston, WV 25304 304-558-3570 or 800-654-4406 www.wvretirement.com PRE-RETIREMENT BENEFICIARY DESIGNATION PUBLIC EMPLOYEES RETIREMENT
Consolidated Public Retirement Board 4101 MacCorkle Avenue, SE Charleston, WV 25304 304-558-3570 or 800-654-4406 www.wvretirement.com PRE-RETIREMENT BENEFICIARY DESIGNATION PUBLIC EMPLOYEES RETIREMENT
General Instructions For Completing This Joinder Agreement
 General Instructions For Completing This Joinder Agreement An Important Note to Grantors: Please read the entire Joinder Agreement carefully, including all of the exhibits. Some of the exhibits require
General Instructions For Completing This Joinder Agreement An Important Note to Grantors: Please read the entire Joinder Agreement carefully, including all of the exhibits. Some of the exhibits require
WISCONSIN NECA-IBEW RETIREMENT PLAN # Instructions for Benefit Payment Election Form- Members under age 60 INSTRUCTIONS
 WISCONSIN NECA-IBEW RETIREMENT PLAN #766870 Instructions for Benefit Payment Election Form- Members under age 60 Participant: Date: I hereby make application for a distribution of your benefits under the
WISCONSIN NECA-IBEW RETIREMENT PLAN #766870 Instructions for Benefit Payment Election Form- Members under age 60 Participant: Date: I hereby make application for a distribution of your benefits under the
Life Event Change (Retirees, Survivors & Inactive Plan Members)
") Life Event Change (Retirees, Survivors & Inactive Plan Members) Please print, complete, and mail, fax, or email this form to the Board of Pensions. Use this form to report life events (such as getting
Life Event Change (Retirees, Survivors & Inactive Plan Members) Please print, complete, and mail, fax, or email this form to the Board of Pensions. Use this form to report life events (such as getting
E. J. Bourgeois, Constable Jefferson Parish 6th Justice Court
 E. J. Bourgeois, Constable Jefferson Parish 6th Justice Court Compiled Financial Statements and Supplementary Information William D. Mercer, CPA A PROFESSIONAL ACCOUNTING CORPORATION CONTENTS Accountant's
E. J. Bourgeois, Constable Jefferson Parish 6th Justice Court Compiled Financial Statements and Supplementary Information William D. Mercer, CPA A PROFESSIONAL ACCOUNTING CORPORATION CONTENTS Accountant's
STATEWIDE HYBRID PLAN IRREVOCABLE ELECTION TO PARTICIPATE IN THE DEFERRED RETIREMENT OPTION PLAN (DROP) AND RESIGNATION FROM EMPLOYMENT
 AND RESIGNATION FROM EMPLOYMENT") FPPA Fire and Police Pension Association 5290 DTC Parkway, Greenwood Village, CO 80111-2721 (303) 770-3772 Toll Free 1(800) 332-3772 www.fppaco.org STATEWIDE HYBRID PLAN IRREVOCABLE ELECTION TO PARTICIPATE
FPPA Fire and Police Pension Association 5290 DTC Parkway, Greenwood Village, CO 80111-2721 (303) 770-3772 Toll Free 1(800) 332-3772 www.fppaco.org STATEWIDE HYBRID PLAN IRREVOCABLE ELECTION TO PARTICIPATE
Distribution Election Form Application & Authorization
 Landscape, Irrigation & Lawn Sprinkler Industry Trusts Defined Contribution Pension Trust c/o Southern California Pipe Trades Administrative Corporation 501 Shatto Place, 5 th Floor, Los Angeles, California
Landscape, Irrigation & Lawn Sprinkler Industry Trusts Defined Contribution Pension Trust c/o Southern California Pipe Trades Administrative Corporation 501 Shatto Place, 5 th Floor, Los Angeles, California
New Jersey Department of Human Services Division of Aging Services
 New Jersey Department of Human Services Division of Aging Services GLOBAL OPTIONS FOR LONG-TERM CARE MEDICAID WAIVER PROGRAM In order to promote the health and independence of the elderly and physically
New Jersey Department of Human Services Division of Aging Services GLOBAL OPTIONS FOR LONG-TERM CARE MEDICAID WAIVER PROGRAM In order to promote the health and independence of the elderly and physically
Please accept this as my request to unlock a portion of my account as noted below: Name and LIRA Account Number. Name and LRIF Account Number
 To: RBC Direct Investing Inc. REQUEST TO UNLOCK ALBERTA LIRA/LIF/LRIF Please accept this as my request to unlock a portion of my account as noted below: Name and LIRA Account Number Name and LRIF Account
To: RBC Direct Investing Inc. REQUEST TO UNLOCK ALBERTA LIRA/LIF/LRIF Please accept this as my request to unlock a portion of my account as noted below: Name and LIRA Account Number Name and LRIF Account
APPLICATION FOR GROUP COVERAGE
 Blue Cross and Blue Shield of Louisiana HMO Louisiana Southern National Life APPLICATION FOR GROUP COVERAGE SECTION A - COVERAGE SELECTION Blue Cross and Blue Shield of Louisiana GroupCare PPO (Plan) BlueSaver
Blue Cross and Blue Shield of Louisiana HMO Louisiana Southern National Life APPLICATION FOR GROUP COVERAGE SECTION A - COVERAGE SELECTION Blue Cross and Blue Shield of Louisiana GroupCare PPO (Plan) BlueSaver
consisting of 100% of your vested account balance to your surviving spouse (if any) as beneficiary.
 as beneficiary.") Instructions and PESP Rules for Beneficiary Designations RETAIN FOR YOUR RECORDS Participant s Federal law provides certain rights and death benefits to spouses of participants in qualified retirement
Instructions and PESP Rules for Beneficiary Designations RETAIN FOR YOUR RECORDS Participant s Federal law provides certain rights and death benefits to spouses of participants in qualified retirement
Sample COBRA Notice. ABC Company c/o The COBRA Administrator s Name 1234 South St City, State and Zip 06/10/2008
 ABC Company c/o The COBRA Administrator s Name 06/10/2008 PQB Name: Spouse Name: Street Address Street Address This notice contains important information about your right to continue your health care coverage
ABC Company c/o The COBRA Administrator s Name 06/10/2008 PQB Name: Spouse Name: Street Address Street Address This notice contains important information about your right to continue your health care coverage
Louisiana Family Assistance Rebate Program
 Louisiana Family Assistance Rebate Program Overview The Louisiana Family Assistance Rebate Program is designed to ensure that tbe average Louisiana family and individual receives a net benefit under the
Louisiana Family Assistance Rebate Program Overview The Louisiana Family Assistance Rebate Program is designed to ensure that tbe average Louisiana family and individual receives a net benefit under the
CAPITAL CREDIT ACCOUNT REFUND PACKET AGE
 CAPITAL CREDIT ACCOUNT REFUND PACKET AGE Copy of Driver s License or Birth Certificate.Page 2 Agreement to Terms and Conditions for Payment Of Capital Credits Prior to the Time Such Capital Would Otherwise
CAPITAL CREDIT ACCOUNT REFUND PACKET AGE Copy of Driver s License or Birth Certificate.Page 2 Agreement to Terms and Conditions for Payment Of Capital Credits Prior to the Time Such Capital Would Otherwise
Louisiana Sheriffs Pension and Relief Fund
 BENEFICIARY DESIGNATION FOR REFUNDS MEMBER S NAME: ADDRESS: PARISH: MARITAL STATUS: Married Divorced Single Louisiana law permits you to designate a beneficiary for your employee contributions if you die
BENEFICIARY DESIGNATION FOR REFUNDS MEMBER S NAME: ADDRESS: PARISH: MARITAL STATUS: Married Divorced Single Louisiana law permits you to designate a beneficiary for your employee contributions if you die
HEALTH CARE FSA GENERAL NOTICE OF CONTINUATION COVERAGE RIGHTS UNDER COBRA
 HEALTH CARE FSA GENERAL NOTICE OF CONTINUATION COVERAGE RIGHTS UNDER COBRA 001001 NAME ADDRESS ADDRESS July 4, 2014 Introduction You are receiving this notice because you are covered under the Health Care
HEALTH CARE FSA GENERAL NOTICE OF CONTINUATION COVERAGE RIGHTS UNDER COBRA 001001 NAME ADDRESS ADDRESS July 4, 2014 Introduction You are receiving this notice because you are covered under the Health Care
New Orleans Employers - International Longshoremen s Association, AFL-CIO Pension Plan ( Plan )
") New Orleans Employers - International Longshoremen s Association, AFL-CIO Pension Plan ( Plan ) NOTICE OF PRERETIREMENT SURVIVOR ANNUITY TO: PLAN PARTICIPANTS Preretirement Survivor Annuity For Married
New Orleans Employers - International Longshoremen s Association, AFL-CIO Pension Plan ( Plan ) NOTICE OF PRERETIREMENT SURVIVOR ANNUITY TO: PLAN PARTICIPANTS Preretirement Survivor Annuity For Married
COUNTY OF SAN DIEGO TERMINAL PAY PLAN
 COUNTY OF SAN DIEGO COUNTY OF SAN DIEGO TERMINAL PAY PLAN ABOUT THE PLAN The Terminal Pay Plan (TPP) is a retirement benefit program implemented to provide eligible employees who separate from County service
COUNTY OF SAN DIEGO COUNTY OF SAN DIEGO TERMINAL PAY PLAN ABOUT THE PLAN The Terminal Pay Plan (TPP) is a retirement benefit program implemented to provide eligible employees who separate from County service
Loan Reduction Assistance Program
 Loan Reduction Assistance Program >>> LOAN REDUCTION ASSISTANCE APPLICATION
Loan Reduction Assistance Program >>> LOAN REDUCTION ASSISTANCE APPLICATION
*XXXXXXXXXXXXXX *
 Vanguard Retirement Plan Enrollment and Change Form for 403(b) Custodial Accounts Columbia University Voluntary Retirement Savings Plan Plan # 096141 1. Account Information Check one: New Enrollment Re-Enrollment
Vanguard Retirement Plan Enrollment and Change Form for 403(b) Custodial Accounts Columbia University Voluntary Retirement Savings Plan Plan # 096141 1. Account Information Check one: New Enrollment Re-Enrollment
ADAM H. PUTNAM COMMISSIONER
 FLORIDA DEPARTMENT OF AGRICULTURE AND CONSUMER SERVICES ADAM H. PUTNAM COMMISSIONER PAWNBROKING REGISTRATION APPLICATION Chapter 539.001, Florida Statutes Rule 5J13.002, Florida Administrative Code Florida
FLORIDA DEPARTMENT OF AGRICULTURE AND CONSUMER SERVICES ADAM H. PUTNAM COMMISSIONER PAWNBROKING REGISTRATION APPLICATION Chapter 539.001, Florida Statutes Rule 5J13.002, Florida Administrative Code Florida
1. GENERAL INSTRUCTIONS
 Fidelity Investments Enrollment Form and Beneficiary Designation for the Evangelical Presbyterian Church 403(b)(9) Plan Account 1. GENERAL INSTRUCTIONS Opening a new account: Please complete this form
Fidelity Investments Enrollment Form and Beneficiary Designation for the Evangelical Presbyterian Church 403(b)(9) Plan Account 1. GENERAL INSTRUCTIONS Opening a new account: Please complete this form
Preferred Adult Dental Plan Application For Individuals and Families Effective January 1, 2017
 Preferred Adult Dental Plan Application For Individuals and Families Effective January 1, 2017 Use this application if you are currently enrolled on a Premera Blue Cross Blue Shield of Alaska (Premera)
Preferred Adult Dental Plan Application For Individuals and Families Effective January 1, 2017 Use this application if you are currently enrolled on a Premera Blue Cross Blue Shield of Alaska (Premera)
TRANSFERRING PENSION CONTRIBUTIONS
 TRANSFERRING PENSION CONTRIBUTIONS When you work outside the jurisdiction of the North Central States Regional Council of Carpenters Pension Fund, your Employer may pay required pension contributions to
TRANSFERRING PENSION CONTRIBUTIONS When you work outside the jurisdiction of the North Central States Regional Council of Carpenters Pension Fund, your Employer may pay required pension contributions to
BENEFICIARY DESIGNATION FORM for AMERICAN AIRLINES, INC.
 BENEFICIARY DESIGNATION FORM for AMERICAN AIRLINES, INC. INSTRUCTIONS Please print clearly in CAPITAL LETTERS, using only blue or black ink. Do not use correction fluid. If you need to change information
BENEFICIARY DESIGNATION FORM for AMERICAN AIRLINES, INC. INSTRUCTIONS Please print clearly in CAPITAL LETTERS, using only blue or black ink. Do not use correction fluid. If you need to change information
CARRIER ENTERPRISE NORTHEAST, LLC ( CE ) (PLEASE PRINT CLEARLY) Credit Agreement
 (PLEASE PRINT CLEARLY) Credit Agreement") CARRIER ENTERPRISE NORTHEAST, LLC ( CE ) Date Credit Agreement (PLEASE PRINT CLEARLY) Company Name of Applicant (If applicant is a corporation or LLC, give name as it appears in the ARTICLES OF INCORPORATION)
CARRIER ENTERPRISE NORTHEAST, LLC ( CE ) Date Credit Agreement (PLEASE PRINT CLEARLY) Company Name of Applicant (If applicant is a corporation or LLC, give name as it appears in the ARTICLES OF INCORPORATION)
Country Club of Culpeper Application for Membership PERSONAL
 Application for Membership PERSONAL Name Mr. Mrs. Ms. Street Address City State ZipCode Telephone Home: Work: Email: Date of Birth Social Security No. Spouse s Name Mr. Mrs. Ms. Date of Birth Social Security
Application for Membership PERSONAL Name Mr. Mrs. Ms. Street Address City State ZipCode Telephone Home: Work: Email: Date of Birth Social Security No. Spouse s Name Mr. Mrs. Ms. Date of Birth Social Security
Voluntary Life Insurance
 Voluntary Life Insurance Benefit Highlights for CAJON VALLEY UNION SD What is voluntary life insurance? Voluntary life insurance is coverage that you pay for. Voluntary life insurance pays your beneficiary
Voluntary Life Insurance Benefit Highlights for CAJON VALLEY UNION SD What is voluntary life insurance? Voluntary life insurance is coverage that you pay for. Voluntary life insurance pays your beneficiary
CONSUMER CREDIT CARD AGREEMENT AND DISCLOSURE
 CONSUMER CREDIT CARD AGREEMENT AND DISCLOSURE VISA SIGNATURE CONNECT REWARDS/CONNECT This Consumer Credit Card Agreement and Disclosure together with the Account Opening Disclosure and any other Account
CONSUMER CREDIT CARD AGREEMENT AND DISCLOSURE VISA SIGNATURE CONNECT REWARDS/CONNECT This Consumer Credit Card Agreement and Disclosure together with the Account Opening Disclosure and any other Account
* * Beneficiary Designation With Restricted Payout (for Annuity Contracts Only)
") Mail or fax completed form to: P.O. Box 1555, Des Moines, IA 50306-1555 Fax: 866 709 3922 Contact us: Annuity Customer Contact Center - Tel: 888 266 8489 Athene Annuity and Life Company 7700 Mills Civic
Mail or fax completed form to: P.O. Box 1555, Des Moines, IA 50306-1555 Fax: 866 709 3922 Contact us: Annuity Customer Contact Center - Tel: 888 266 8489 Athene Annuity and Life Company 7700 Mills Civic
New York Public Employee Retirement System Special Durable Power of Attorney (Rev. 6/18)
") Office of the New York State Comptroller 110 State Street, Albany, New York 12244-0001 Received New York Public Employee Retirement System Special Durable Power of Attorney (Rev. 6/18) This is a Public
Office of the New York State Comptroller 110 State Street, Albany, New York 12244-0001 Received New York Public Employee Retirement System Special Durable Power of Attorney (Rev. 6/18) This is a Public
Name Address City, State and Zip Code Social Security Number Telephone ( ) Date of request
 Date of request") *HYBRID-MANDATORY* GENERAL RETIREMENT SYSTEM OF THE CITY OF DETROIT REQUEST FOR WITHDRAWAL OF MANDATORY EMPLOYEE CONTRIBUTIONS FROM THE COMPONENT I PLAN AND DISTRIBUTION DESIGNATION Name Address City,
*HYBRID-MANDATORY* GENERAL RETIREMENT SYSTEM OF THE CITY OF DETROIT REQUEST FOR WITHDRAWAL OF MANDATORY EMPLOYEE CONTRIBUTIONS FROM THE COMPONENT I PLAN AND DISTRIBUTION DESIGNATION Name Address City,
Chapter 12: Deferred Retirement Option Plan
 Content Overview What is the Deferred Retirement Option Plan? Types of DROP Accounts Entering DROP The Application Process gmembers gemployers Calculating a DROP Benefit Ending DROP and Retiring The Retirement
Content Overview What is the Deferred Retirement Option Plan? Types of DROP Accounts Entering DROP The Application Process gmembers gemployers Calculating a DROP Benefit Ending DROP and Retiring The Retirement
ilinkblue Institutional Provider Service Agreement
 An independent licensee of the Blue Cross and Blue Shield Association. ilinkblue Institutional Provider Service Agreement STATE of LOUISIANA PARISH of THIS AGREEMENT, made and entered into as of the day
An independent licensee of the Blue Cross and Blue Shield Association. ilinkblue Institutional Provider Service Agreement STATE of LOUISIANA PARISH of THIS AGREEMENT, made and entered into as of the day
JOINDER AGREEMENT For THE GEORGIA COMMUNITY TRUST MASTER TRUST AGREEMENT. A. This Sub-account is funded with those assets listed in Schedule B hereto.
 JOINDER AGREEMENT For THE GEORGIA COMMUNITY TRUST MASTER TRUST AGREEMENT 1. The undersigned hereby enrolls in and adopts The Georgia Community Trust Master Trust Agreement dated Aug. 25, 2015 which Agreement
JOINDER AGREEMENT For THE GEORGIA COMMUNITY TRUST MASTER TRUST AGREEMENT 1. The undersigned hereby enrolls in and adopts The Georgia Community Trust Master Trust Agreement dated Aug. 25, 2015 which Agreement
FILED: NEW YORK COUNTY CLERK 07/28/ :23 PM INDEX NO /2015 NYSCEF DOC. NO. 56 RECEIVED NYSCEF: 07/28/2015 EXHIBIT 30
 FILED: NEW YORK COUNTY CLERK 07/28/2015 05:23 PM INDEX NO. 651841/2015 NYSCEF DOC. NO. 56 RECEIVED NYSCEF: 07/28/2015 EXHIBIT 30 STANDSTILL AGREEMENT THIS STANDSTILL AGREEMENT (this Agreement ) is dated
FILED: NEW YORK COUNTY CLERK 07/28/2015 05:23 PM INDEX NO. 651841/2015 NYSCEF DOC. NO. 56 RECEIVED NYSCEF: 07/28/2015 EXHIBIT 30 STANDSTILL AGREEMENT THIS STANDSTILL AGREEMENT (this Agreement ) is dated
ADDENDUM TO THE RETIREMENT SAVINGS PLAN DECLARATION OF TRUST ESTABLISHING A LOCKED-IN RETIREMENT ACCOUNT. Saskatchewan (LIRA)
") ADDENDUM TO THE RETIREMENT SAVINGS PLAN DECLARATION OF TRUST ESTABLISHING A LOCKED-IN RETIREMENT ACCOUNT Saskatchewan (LIRA) 1. What the Words Mean: Please remember that in this Addendum, I, me and my
ADDENDUM TO THE RETIREMENT SAVINGS PLAN DECLARATION OF TRUST ESTABLISHING A LOCKED-IN RETIREMENT ACCOUNT Saskatchewan (LIRA) 1. What the Words Mean: Please remember that in this Addendum, I, me and my
ADDENDUM TO THE REGISTERED RETIREMENT INCOME FUND DECLARATION OF TRUST. Saskatchewan (PRIF)
") ADDENDUM TO THE REGISTERED RETIREMENT INCOME FUND DECLARATION OF TRUST Saskatchewan (PRIF) 1. What the Words Mean: Please remember that in this Addendum, I, me and my mean the individual who has signed
ADDENDUM TO THE REGISTERED RETIREMENT INCOME FUND DECLARATION OF TRUST Saskatchewan (PRIF) 1. What the Words Mean: Please remember that in this Addendum, I, me and my mean the individual who has signed
X Member s Signature. Social Security #: Address: Jurisdiction: Survivor Information: Name of Survivor: Address: City: State: Zip:
 WRS-A5 Application-Judicial Page 1 of 2 (Revised 5/11) Judicial Plan Application for Retirement Member Information: Name: Social Security#: Phone #: Email: Check box if new address Final Date of Employment:
WRS-A5 Application-Judicial Page 1 of 2 (Revised 5/11) Judicial Plan Application for Retirement Member Information: Name: Social Security#: Phone #: Email: Check box if new address Final Date of Employment:
Case CSS Doc 856 Filed 12/06/18 Page 1 of 9 IN THE UNITED STATES BANKRUPTCY COURT FOR THE DISTRICT OF DELAWARE
 Case 17-12906-CSS Doc 856 Filed 12/06/18 Page 1 of 9 IN THE UNITED STATES BANKRUPTCY COURT FOR THE DISTRICT OF DELAWARE In re: Chapter 11 CHARMING CHARLIE HOLDINGS INC., et al., 1 Case No. 17-12906 (CSS
Case 17-12906-CSS Doc 856 Filed 12/06/18 Page 1 of 9 IN THE UNITED STATES BANKRUPTCY COURT FOR THE DISTRICT OF DELAWARE In re: Chapter 11 CHARMING CHARLIE HOLDINGS INC., et al., 1 Case No. 17-12906 (CSS
FORM LETTER OF CREDIT. Bank. (address) IRREVOCABLE STANDBY LETTER OF CREDIT FOR INTERNAL IDENTIFICATION PURPOSES ONLY
 IRREVOCABLE STANDBY LETTER OF CREDIT FOR INTERNAL IDENTIFICATION PURPOSES ONLY") FORM LETTER OF CREDIT Bank (address) IRREVOCABLE STANDBY LETTER OF CREDIT DATE: AMOUNT U.S. $ FOR INTERNAL IDENTIFICATION PURPOSES ONLY Our Number: Beneficiary: Applicant: Attn: At the request of: Ref:
FORM LETTER OF CREDIT Bank (address) IRREVOCABLE STANDBY LETTER OF CREDIT DATE: AMOUNT U.S. $ FOR INTERNAL IDENTIFICATION PURPOSES ONLY Our Number: Beneficiary: Applicant: Attn: At the request of: Ref:
In-Service Withdrawal Form PLEASE TYPE OR PRINT Signature Required
 In-Service Withdrawal Form PLEASE TYPE OR PRINT Signature Required Company Name: PARTICIPANT INFORMATION Employee Name: Employee Address: Date of Birth: (Street) (City) (State) (Zip) Social Security Number:
In-Service Withdrawal Form PLEASE TYPE OR PRINT Signature Required Company Name: PARTICIPANT INFORMATION Employee Name: Employee Address: Date of Birth: (Street) (City) (State) (Zip) Social Security Number:
The Union Lincoln Regional Water Supply Initiative. Financial Statements. For The Year Ended December 31,2008
 7^/3 The Union Lincoln Regional Water Supply Initiative Financial Statements Under provisions of state law, this report is a public documenl Acopy of the report has been submitted to the entity and other
7^/3 The Union Lincoln Regional Water Supply Initiative Financial Statements Under provisions of state law, this report is a public documenl Acopy of the report has been submitted to the entity and other
Westhollow Village Homeowners Association, Inc. Swimming Pool Use Acknowledge of Risk Waiver and Release of Liability
 Westhollow Village Homeowners Association, Inc. Swimming Pool Use Acknowledge of Risk Waiver and Release of Liability In consideration of my use of Westhollow Village s swimming pools, I hereby forever
Westhollow Village Homeowners Association, Inc. Swimming Pool Use Acknowledge of Risk Waiver and Release of Liability In consideration of my use of Westhollow Village s swimming pools, I hereby forever
Last name First name MI. Apt / Suite / PO box number Gender m Female m Male Language of choice m English m Spanish City State Zip code County / Parish
 Large group employee enrollment form The offering company(ies) listed on the signature page, severally or collectively, as the content may require, are referred to in this application as Humana. Print
Large group employee enrollment form The offering company(ies) listed on the signature page, severally or collectively, as the content may require, are referred to in this application as Humana. Print
ARTICLES OF INCORPORATION OF LOUISIANA ASSOCIATION OF COLLEGIATE REGISTRARS AND ADMISSIONS OFFICERS, INC. (A LOUISIANA NONPROFIT CORPORATION)
") ARTICLES OF INCORPORATION OF LOUISIANA ASSOCIATION OF COLLEGIATE REGISTRARS AND ADMISSIONS OFFICERS, INC. (A LOUISIANA NONPROFIT CORPORATION) The undersigned, acting pursuant to the Nonprofit Corporation
ARTICLES OF INCORPORATION OF LOUISIANA ASSOCIATION OF COLLEGIATE REGISTRARS AND ADMISSIONS OFFICERS, INC. (A LOUISIANA NONPROFIT CORPORATION) The undersigned, acting pursuant to the Nonprofit Corporation
Louisiana Conference Benefits Office 527 North Blvd, Baton Rouge, LA
 Louisiana Conference Benefits Office 527 North Blvd, Baton Rouge, LA 70802 225-346-1646 Moving Costs - Clergy Income Tax AND Conference Reporting Requirements Revised: 5.22.18 Z:/Finance Files/District
Louisiana Conference Benefits Office 527 North Blvd, Baton Rouge, LA 70802 225-346-1646 Moving Costs - Clergy Income Tax AND Conference Reporting Requirements Revised: 5.22.18 Z:/Finance Files/District
Annuity Contract Scheduled Systematic Withdrawal
 Annuity Contract Scheduled Systematic Withdrawal Questions? Call our National Service Center at 1-800-888-2461. Instructions Please type or print. Use this form to establish or change a Scheduled Systematic
Annuity Contract Scheduled Systematic Withdrawal Questions? Call our National Service Center at 1-800-888-2461. Instructions Please type or print. Use this form to establish or change a Scheduled Systematic
A Personal Representative s Guide to Probate
 A longer title for this article would be What does it mean for you to be the personal representative and for me to be your lawyer? This guide addresses our respective responsibilities assuming that you
A longer title for this article would be What does it mean for you to be the personal representative and for me to be your lawyer? This guide addresses our respective responsibilities assuming that you
Life Investors Insurance Company
 Life Investors Insurance Company Appointment Requirements: Complete Application for Appointment Agreement Complete and Sign Fair Credit Reporting Act Disclosure Review and Sign Appointment Agreement Review
Life Investors Insurance Company Appointment Requirements: Complete Application for Appointment Agreement Complete and Sign Fair Credit Reporting Act Disclosure Review and Sign Appointment Agreement Review
DECLARATION OF THIRD PARTY SUPPLEMENTAL NEEDS TRUST THIS IS A BINDING LEGAL DOCUMENT. YOU ARE ADVISED TO OBTAIN PROFESSIONAL ADVICE BEFORE SIGNING.
 DECLARATION OF THIRD PARTY SUPPLEMENTAL NEEDS TRUST THIS IS A BINDING LEGAL DOCUMENT. YOU ARE ADVISED TO OBTAIN PROFESSIONAL ADVICE BEFORE SIGNING. This Declaration of Third Party Supplemental Needs Trust
DECLARATION OF THIRD PARTY SUPPLEMENTAL NEEDS TRUST THIS IS A BINDING LEGAL DOCUMENT. YOU ARE ADVISED TO OBTAIN PROFESSIONAL ADVICE BEFORE SIGNING. This Declaration of Third Party Supplemental Needs Trust
POLICY NO. 2 THE BOARD OF THE UBCP RETIREMENT BENEFITS SOCIETY
 POLICY NO. 2 THE BOARD OF THE UBCP RETIREMENT BENEFITS SOCIETY FINANCIAL HARDSHIP WITHDRAWAL POLICY adopted October 16, 2007 updated May 25, 2010 Reviewed February 2014 Producer retirement contributions
POLICY NO. 2 THE BOARD OF THE UBCP RETIREMENT BENEFITS SOCIETY FINANCIAL HARDSHIP WITHDRAWAL POLICY adopted October 16, 2007 updated May 25, 2010 Reviewed February 2014 Producer retirement contributions
GOTHENBURG PUBLIC SCHOOLS TEMPORARY EARLY RETIREMENT INCENTIVE PROGRAM
 A. PURPOSE GOTHENBURG PUBLIC SCHOOLS The purpose of this program is to encourage eligible Certificated Employees who are considering an early-leaving decision to accelerate their retirement plans. Objectives
A. PURPOSE GOTHENBURG PUBLIC SCHOOLS The purpose of this program is to encourage eligible Certificated Employees who are considering an early-leaving decision to accelerate their retirement plans. Objectives
Annuitant s Name (Please print) Social Insurance Number RIF Account Number
 Social Insurance Number RIF Account Number") PRESCRIBED RETIREMENT INCOME FUND (RIF) ADDENDUM PROVINCE OF MANITOBA Steadyhand Investment Funds Inc. 1747 West 3 rd Avenue Vancouver, BC V6J 1K7 www.steadyhand.com 1-888-888-3147 Annuitant s Name (Please
PRESCRIBED RETIREMENT INCOME FUND (RIF) ADDENDUM PROVINCE OF MANITOBA Steadyhand Investment Funds Inc. 1747 West 3 rd Avenue Vancouver, BC V6J 1K7 www.steadyhand.com 1-888-888-3147 Annuitant s Name (Please
GUARDIAN POOLED TRUST JOINDER AGREEMENT
 Trust sub-account number: Acceptance Date: These Blanks to be Completed by the Trustee version 3.3 GUARDIAN POOLED TRUST JOINDER AGREEMENT This is a legal document. You are encouraged to seek independent,
Trust sub-account number: Acceptance Date: These Blanks to be Completed by the Trustee version 3.3 GUARDIAN POOLED TRUST JOINDER AGREEMENT This is a legal document. You are encouraged to seek independent,
LOUISIANA DELTA COMMUNITY COLLEGE LOUISIANA COMMUNITY AND TECHNICAL COLLEGE SYSTEM STATE OF LOUISIANA Monroe, Louisiana
 Monroe, Louisiana Basic Financial Statements and Independent Auditor's Reports As of and for the Years Ended June 30, 2003 and 2002 January 28, 2004 DIRECTOR OF FINANCIAL AND COMPLIANCE AUDIT Albert J.
Monroe, Louisiana Basic Financial Statements and Independent Auditor's Reports As of and for the Years Ended June 30, 2003 and 2002 January 28, 2004 DIRECTOR OF FINANCIAL AND COMPLIANCE AUDIT Albert J.
INSTRUCTIONS FOR PROVIDER'S ELECTION TO EMPLOY ELECTRONIC DATA INTERCHANGE OF CLAIMS FOR PROCESSING IN THE LOUISIANA MEDICAL ASSISTANCE PROGRAM
 Individual Louisiana s Medicaid Program INSTRUCTIONS FOR PROVIDER'S ELECTION TO EMPLOY ELECTRONIC DATA INTERCHANGE OF CLAIMS FOR PROCESSING IN THE LOUISIANA MEDICAL ASSISTANCE PROGRAM Prior to submitting
Individual Louisiana s Medicaid Program INSTRUCTIONS FOR PROVIDER'S ELECTION TO EMPLOY ELECTRONIC DATA INTERCHANGE OF CLAIMS FOR PROCESSING IN THE LOUISIANA MEDICAL ASSISTANCE PROGRAM Prior to submitting
Addendum To Retirement Savings Plan Declaration Of Trust For Locked-In Pension Transfers To A Locked-In Retirement Account (ONTARIO LIRA)
") Addendum To Retirement Savings Plan Declaration Of Trust For Locked-In Pension Transfers To A Locked-In Retirement Account (ONTARIO LIRA) Fidelity Investments Retirement Savings Plan (RSP 521-049) (the
Addendum To Retirement Savings Plan Declaration Of Trust For Locked-In Pension Transfers To A Locked-In Retirement Account (ONTARIO LIRA) Fidelity Investments Retirement Savings Plan (RSP 521-049) (the
3608 West 26 th Street Erie, PA (814) Fax (814) Application Information
 Fax (814) Application Information") 3608 West 26 th Street Erie, PA 16506 (814) 836-8677 Fax (814) 836-9747 Position Applied For: (Check all that apply) EMT ( ) Fulltime ( ) Paramedic ( ) Part-time ( ) Wheelchair Van Driver ( ) Office (
3608 West 26 th Street Erie, PA 16506 (814) 836-8677 Fax (814) 836-9747 Position Applied For: (Check all that apply) EMT ( ) Fulltime ( ) Paramedic ( ) Part-time ( ) Wheelchair Van Driver ( ) Office (
COMMONWEALTH OF VIRGINIA DEPARTMENT OF EDUCATION P. O. BOX 2120 RICHMOND, VIRGINIA
 COMMONWEALTH OF VIRGINIA DEPARTMENT OF EDUCATION P. O. BOX 2120 RICHMOND, VIRGINIA 23218-2120 VIRGINIA TEACHING SCHOLARSHIP LOAN PROGRAM PROMISSORY NOTE 2017-2018 MAKER S FULL NAME: SOCIAL SECURITY NUMBER:
COMMONWEALTH OF VIRGINIA DEPARTMENT OF EDUCATION P. O. BOX 2120 RICHMOND, VIRGINIA 23218-2120 VIRGINIA TEACHING SCHOLARSHIP LOAN PROGRAM PROMISSORY NOTE 2017-2018 MAKER S FULL NAME: SOCIAL SECURITY NUMBER:
SMALL GROUP ENROLLMENT/CHANGE FORM COMPLETE THIS APPLICATION IN ITS ENTIRETY IN BLUE OR BLACK INK. DO NOT USE PENCIL OR HIGHLIGHTER.
 22259 SMALL GROUP ENROLLMENT/CHANGE FORM COMPLETE THIS APPLICATION IN ITS ENTIRETY IN BLUE OR BLACK INK. DO NOT USE PENCIL OR HIGHLIGHTER. q ENROLLING (Complete sections I, II, IV, and V) q WAIVING (Complete
22259 SMALL GROUP ENROLLMENT/CHANGE FORM COMPLETE THIS APPLICATION IN ITS ENTIRETY IN BLUE OR BLACK INK. DO NOT USE PENCIL OR HIGHLIGHTER. q ENROLLING (Complete sections I, II, IV, and V) q WAIVING (Complete
COMPLETING THIS FORM TO APPOINT A REPRESENTATIVE
 COMPLETING THIS FORM TO APPOINT A REPRESENTATIVE Choosing to be Represented You can choose to have a representative help you when you do business with Social Security. We will work with your representative,
COMPLETING THIS FORM TO APPOINT A REPRESENTATIVE Choosing to be Represented You can choose to have a representative help you when you do business with Social Security. We will work with your representative,
Anthem Health Plans of Kentucky, Inc.
 Employee Enrollment Application For 2 50 Employee Small s Kentucky Anthem Plans of Kentucky, Inc. Anthem Life Insurance Company You, the employee, must complete this application. You are solely responsible
Employee Enrollment Application For 2 50 Employee Small s Kentucky Anthem Plans of Kentucky, Inc. Anthem Life Insurance Company You, the employee, must complete this application. You are solely responsible