FINAL CHECK LIST. Immigration Documentation (Resident Alien Cards, Passports, Certificate of Naturalization, I-94, Birth Certificates)
|
|
|
- Warren Bennett
- 6 years ago
- Views:
Transcription
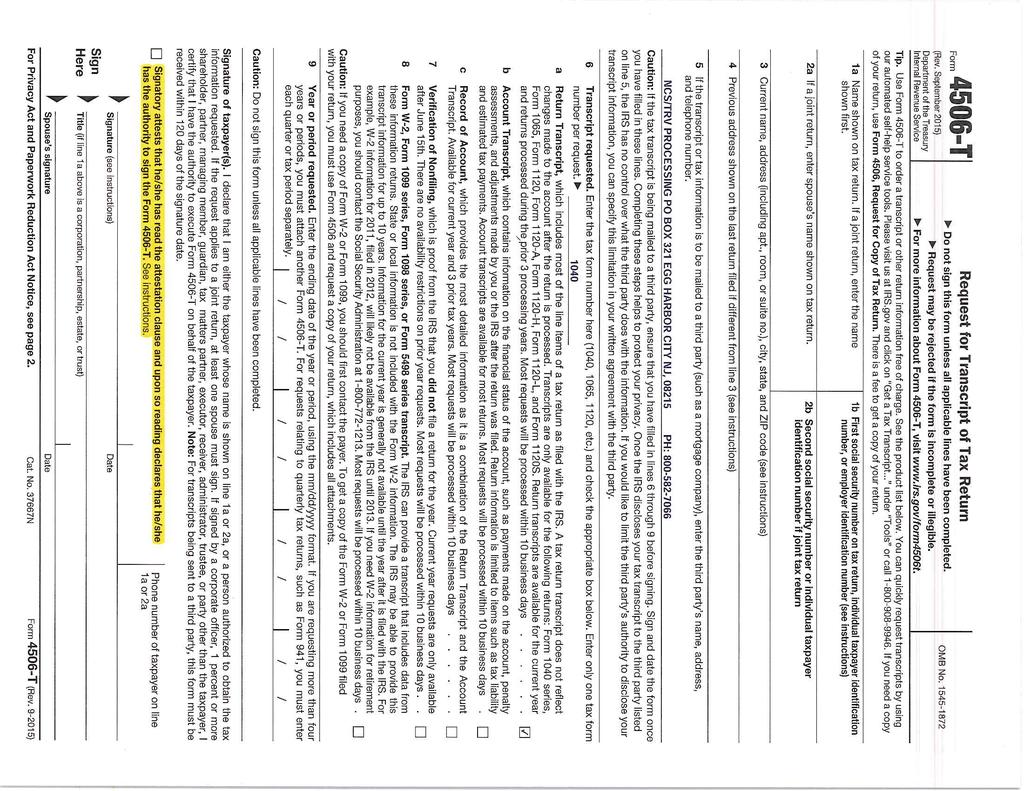
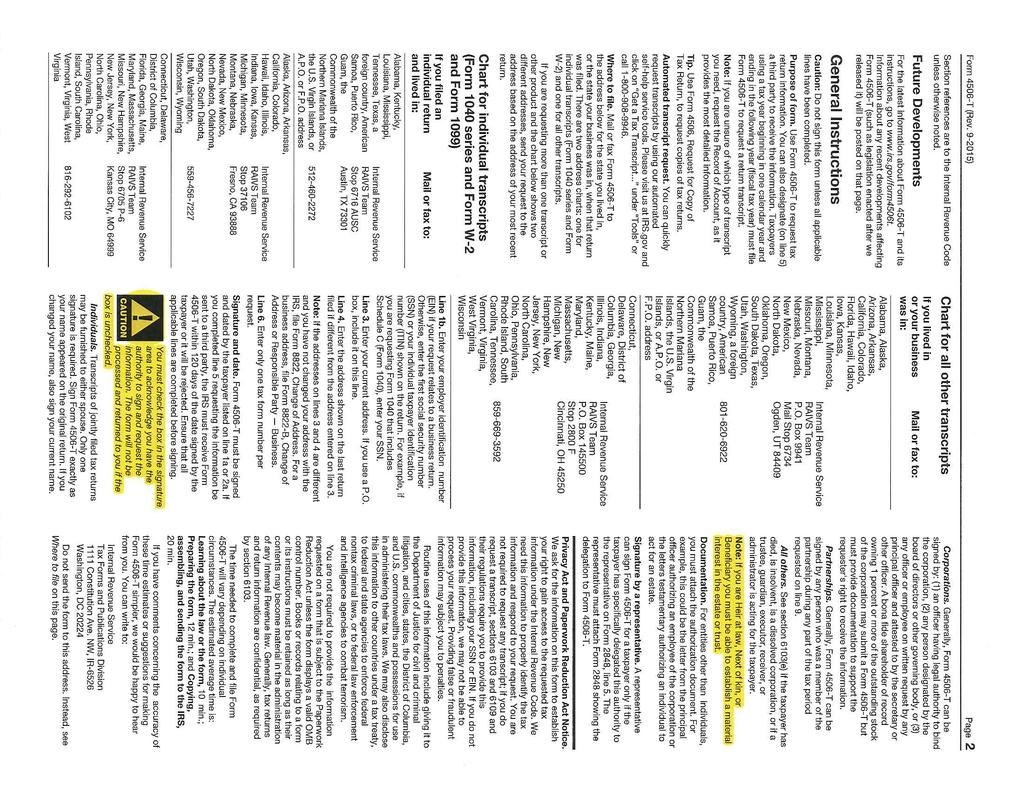
1 Welcome to JPS Health Network. We look forward to providing affordable health care to you and your family. The purpose of the JPS Connection program is to create a healthier community by providing discount health services to Tarrant County residents. Connection members have the benefit of a medical home meaning you have a physician or nurse practitioner assigned to you and your family. You get access to preventative care such as physicals and screenings that will help keep you healthy and out of the emergency room. Inside this packet you will find the application and the documentation requirements for our JPS Connection program. All items on the application must be completed. If not applicable, place either a 0 or N/A in each box. Bring the completed application and required documentation per the final checklist below with you to any of the financial screening locations throughout Tarrant County between the hours of 8:00 a.m. and 4:30 p.m. You may call our Eligibility Center at (817) should you need assistance. Our staff members are happy to answer any questions you may have. Applications can also be acceptable by fax or Enroll@JPSHealth.org. Thank you for choosing JPS and we look forward to providing quality healthcare to you and your family. Regards, Kade Rutherford Executive Director, Revenue Cycle FINAL CHECK LIST Picture ID for all applicants (Government Issued, School, and Work) Immigration Documentation (Resident Alien Cards, Passports, Certificate of Naturalization, I-94, Birth Certificates) Birth Certificates for all child dependents Shelter Letter, Approved Agency Residence Letter or Valid Homeless Scan Card Agency award letters (Food Stamps, TANF, Housing, CHIP/Medicaid, RSDI, SSI, etc.) Completed Application (Incomplete applications are not accepted) Application signed and dated by applicant and spouse Complete and sign form 4506T Review, initial, and sign the Membership Responsibility Form Homeowners, self-employed, or clients receiving Social Security must provide a current 30 day bank statement for all accounts Days proof of Income for all household members (check stubs, award letters, financial aid refund, selfemployment forms, etc.) *Valid/Current Documentation Required* **More information may be requested at time of interview** Revised 09/23/15

2 Eligibility & Enrollment Centers Eligibility & Enrollment Center (Location with largest number of specialists) 1325 S. Main Street Fort Worth, Texas JPS Health Center South Campus 2500 Circle Drive Fort Worth, TX JPS Health Center Stop Six/Walter B. Barbour 3301 Stalcup Road Fort Worth, TX Healing Wings 1350 S. Main St. Suite 1600 Fort Worth, TX JPS Health Center - Northwest/Iona Reed 401 Stribling Dr. Azle, TX * Wednesdays Only JPS Health Center Viola M. Pitts/Como 4701 Bryant Irvin Road North Fort Worth, TX JPS Eligibility Center Arlington 1030 Arkansas Lane Ste 214 Arlington, TX JPS Health Center Diamond Hill 3308 Deen Road Fort Worth, TX JPS Health Center Northeast 837 Brown Trail Bedford, TX Center for Cancer Care 601 W. Terrell Ave Fort Worth, TX JPS Health Center Gerturde Tarpley/Watauga 6601 Watauga Rd # 124 Watauga, TX 76148
3 JPS Health Network Application for JPS Connection Program 10/01/15 Name: Maiden Name: (Last) (First) (MI) Live w/ someone Rent Home #: Address: Own Cell#: (Street) (Apt. #) (City) (State) (Zip) (County) Please check primary contact phone Address: Homeless / Scan Card Primary Language: English Spanish Vietnamese Other Marital Status: Single Sepa Divorce Widowe Married (If married, spouse s signature also is required) Ethnicity: Caucasian African-American Hispanic Native American Other List the names of each person living in household (attach additional sheets as necessary) Must provide copies of identification documents such as a state issued driver s license/id, birth certificates (for children under 18) & Immigration cards. Full Name of Household Members: Relationship to applicant: Self Spouse Child Child Child Sex: Date of Birth Place of Birth Check one: Social Security # Is this person applying for coverage? (Circle One) Male Female US Citizen Legal Permanent Resident Refugee/Asylee Undocumented Male Female US Citizen Legal Permanent Resident Refugee/Asylee Undocumented Male Female US Citizen Legal Permanent Resident Refugee/Asylee Undocumented Male Female US Citizen Legal Permanent Resident Refugee/Asylee Undocumented Male Female US Citizen Legal Permanent Resident Refugee/Asylee Undocumented First time applying? Is this person pregnant? (Circle One) Does this person currently have medical coverage? (Check box) Does this person receive school financial aid? Does this person receive Veteran Benefits? (Circle One) Does this person receive any government assistance**? (Check all that apply) Medicaid/CHIP Medicare A Only Medicare A&B Marketplace Private Through Employer Or Self VA None Medicaid/CHIP Medicare A Only Medicare A&B Marketplace Private Through Employer VA None Medicaid/CHIP Medicare A Only Medicare A&B Marketplace Private Through Employer VA None Medicaid/CHIP Medicare A Only Medicare A&B Marketplace Private Through Employer VA None Medicaid/CHIP Medicare A Only Medicare A&B Marketplace Private Through Employer VA None Food Stamps Housing TANF None Food Stamps Housing TANF None Food Stamps Housing TANF None Food Stamps Housing TANF None Food Stamps Housing TANF None **Must provide a copy of current award letters if, a member of your household receives TANF, Food Stamps and/or Housing assistance.
4 List the names of each person living in household (attach additional sheets as necessary) Do not leave blank spaces if it does not apply put a -0- or N/A Application will be returned if boxes are left unanswered. Full Name of Household Members: Relationship to applicant: Self Spouse Child Child Child If you and/or a member of the household work for yourself, do odd jobs or work for someone but do not have taxes withheld from your wages then you or that household member are self-employed. Is this person Self Employed? (Circle one) Monthly Income after deductions from Self Employment $ $ $ $ $ Do you and/or a member of the household work? Is this person Employed? (Circle one) Employer Name: Employer Street Address: Employer State, City, Zip: Employer Phone: Monthly Income before deductions from Employment $ $ $ $ $ If you and/or a member of your household have a 2 nd Employer please list below: 2 nd Employer Name: Monthly Income before deductions from Employment $ $ $ $ $ Do you and/or a member of your household have the following other monthly income and/or financial aid refund? Unemployment $ $ $ $ $ Workers Compensation $ $ $ $ $ Child Support $ $ $ $ $ Pensions/Retirement $ $ $ $ $ Social Security Retirement $ SSI Disability $ $ $ $ $ VA Benefits $ $ $ $ $ Oil/Royalties $ $ $ $ $ School Financial Aid Refund $ $ $ $ $ Money received from family and friends $ $ $ $ $ Other (List Below): The last year an Income Tax Return was filed $ Year Year Year Year Year 2 of 3
5 List all assets owned by members of your household (attach additional sheets if necessary) Assets and Bank Accounts: Bank name Bank account type: (Circle All that Apply) Balance for all bank accounts $ Bank name Bank account type: (Circle All that Apply) Balance for all bank accounts $ Retirement Accounts: Bank or Company Name Account type: (Circle All that Apply) Current Cash Value for all accounts $ CD and Investment Accounts: Bank or Company Name Account type: (Circle All that Apply) Current Cash Value for all accounts $ Checking Savings Business Accounts Checking Savings Business Accounts IRA 401(k) 403(b) Other: CD Stocks Mutual Funds Other: "I understand that anyone who knowingly lies or misrepresents the truth or arranges for someone to knowingly lie or misrepresent the truth in the completion of this application is committing a crime which can be punished under federal law and/or state law. Everything on this application is the truth as best I know it." If at any time false information is discovered, penalties will include, but are not limited to, loss of household benefits and the inability to reapply for the JPS Connection Program for no less than a period of ninety (90) days. I authorize JPS Health Network to obtain electronic records for the purpose of making a determination of whether I meet the eligibility requirements for the JPS Connection Program. I also understand that any approval will be conditional based on the information reviewed in my records. Signature of Applicant: Date: Signature of Co-Applicant/Spouse: Date: Spouse s signature is required to complete screening even if spouse is not requesting assistance at this time. For Office Use Only: This application is good for 30 days from the date above. If someone helped you to complete this form, please give his or her name. Name (please print): Telephone number: 3 of 3
6 JPS Health Network Verification of Assistance and Residency for JPS Connection Program This form only needs to be completed if the applicant is being assisted by another individual. I, verify that Name of person providing assistance Applicant(s) full name Patient s MR# and/or Social Security # lives at Applicant(s) Address City/Zip Code Financial Assistance: I provide financial assistance to the applicant. Yes No This individual is claimed as a dependent on my most recent filed income tax return. Yes No Does the applicant have a job? If yes, provide employer name Does the applicant have another income source? If yes, how much I provide applicant with the following: Food Personal items Transportation Cash/Check $ per Week or Month Other Do you pay rent or other bills for this applicant? If yes, how much and how often? Residency Assistance (check all that apply): The applicant(s) resides at my Tarrant County residence. The applicant(s) does not pay rent to me. The applicant(s) pays to help toward the rent and utilities. How long has the applicant(s) resided at your address? Does the applicant(s) have another residence? If yes, where Relationship of Person Providing the Assistance to the Applicant(s): I certify that the above information is true and correct. "I understand that anyone who knowingly lies or misrepresents the truth or arranges for someone to knowingly lie or misrepresent the truth in the completion of this application is committing a crime which can be punished under federal law and/or state law. Everything on this application is the truth as best I know it. Signature of the Person Providing the Assistance: Address, City, State, Zip: Phone Number: Date signed: Revised Date
7 JPS Health Network Statement of Self-Employment for JPS Connection Indigent Healthcare Program List your business income and expenses for the past 3 months (one form per month) *Important: receipts, invoices, or other verifying papers may be requested Name of Person Having Self-Employment Income: Describe what you did to earn this money: Business Expenses Write in the dates you paid the expenses and the amount of each expense. Expenses are your costs of doing business. Ex: supplies, repairs, rent, utilities, seed, feed, business insurance, licenses, fees, your social security contribution for people who worked for you, and labor (not salaries you pay yourself). Business Income List dates income was received and the amount for each date. Income includes money from sales, commissions, leases, tips, or whatever you do or sell for money. Ex: babysitting, contract/sub-contract work, landscaping, day labor, panhandling, hairdressers and manicurist Date Type of Expense Amount Date Type of Income Amount Total Self Employment Income $ Enter Expenses & Subtract Here -0 Total Self-Employment Expenses $ Net Self-Employment Income $ "I understand that anyone who knowingly lies or misrepresents the truth or arranges for someone to knowingly lie or misrepresent the truth in the completion of this application is committing a crime which can be punished under Federal law, State law, or both. Everything on this application is the truth as best I know it." If at any time false information is discovered penalties will include, but are not limited to, loss of my membership benefits and the inability to reapply for the JPS Connection Indigent Healthcare Program for no less than a period of ninety (90) days. Signature of Applicant: 10/01/15 Date:
8 JPS Health Network Membership Responsibilities for JPS Connection Indigent Healthcare Program JPS Connection is a tax-supported medical program offered to eligible Tarrant County residents. JPS Connection offers low cost medical care available only through JPS Health Network facilities. I understand that JPS Connection is not an insurance company or an insurance plan. I understand that the JPS Connection does not cover all of the services provided at JPS Health Network including, but not limited to dental, cosmetic procedures, maternity services, assisted reproductive technology, and transplants. Motor vehicle accidents are not covered by JPS Connection when there is the presence of other insurance. JPS Connection remains the payor of last resort for all services. I understand that if I am deemed eligible for state or federal assistance, pharmaceutical assistance programs, or insurance, I must comply with seeking that assistance before receiving any assistance from the JPS Connection Program. This includes any third party commercial insurance, Medicaid, VA benefits and/or parts AB&D of Medicare. Failure to do so will make me ineligible for JPS Connection. Documentation provided to JPS Health Network will be used to apply for any coverage for which I may be potentially eligible. I authorize the Tarrant County Hospital District of Fort Worth to release any demographic and financial information requested by representatives, agents or intermediaries of local, state, or federal agencies; insurance companies; pharmaceutical assistance programs; or other organizations or entities as may be required by said representative for payment of claims arising from services provided under the JPS Connection Program. As a JPS Connection member, I understand I am responsible for the co-payments for services rendered. I have been provided a copy of the JPS Connection Co-pay Schedule. I am aware that when JPS Connection is used supplemental to another payor, I am responsible for all physician/professional fees, co-payments and any deductibles related to professional services rendered. This includes, but not limited to, Acclaim, UNT, Sheridan, RadCare, IES or any other professional group you may receive bills from. As a JPS Connection member, I understand that I have an obligation to notify the Financial Screening department of JPS Health Network of any changes. I agree to inform the Financial Screening department of the JPS Health Network immediately of any changes in my Tarrant County residence, household income, family size and insurance coverage. Failure to do so, may result in loss of membership benefits. I understand that the JPS Connection membership privileges are on a limited time basis. In order to continue receiving a discount on medical services, through the JPS Connection program, it will be necessary to complete another financial screening at the end of my enrollment period. I understand I will be expected to pay all charges incurred after eligibility has expired. I acknowledge that should the JPS Health Network receive returned mail, from the mailing address I provided, that my JPS Connection membership privileges will be suspended pending further review. I understand that I am responsible for providing true and accurate documentation. If at any time false information is discovered penalties may include, but not limited to, loss of my membership benefits and the inability to reapply for the JPS Connection Indigent Healthcare Program for no less than a period of ninety (90) days. "I understand that anyone who knowingly lies or misrepresents the truth or arranges for someone to knowingly lie or misrepresent the truth in the completion of this application is committing a crime which can be punished under Federal law, State law, or both. Everything on this application is the truth as best I know it." Signature of Applicant: Date: Signature of Co-Applicant: Date:
9
10
Nebraska Ryan White Program
 For office use only: Date Received: MR#: Nebraska Ryan White Program Application Information Date: Check all the programs applying for: Part B Part C Part D ADAP ADAP co-payment assistance Wait list If
For office use only: Date Received: MR#: Nebraska Ryan White Program Application Information Date: Check all the programs applying for: Part B Part C Part D ADAP ADAP co-payment assistance Wait list If
ATTENTION: NEW PATIENTS Please allow 4 to 6 weeks to receive your FIRST fill on your prescriptions.
 ATTENTION: NEW PATIENTS Please allow 4 to 6 weeks to receive your FIRST fill on your prescriptions. Regional Healthcare does not control shipments of medication. The pharmaceutical company which supplies
ATTENTION: NEW PATIENTS Please allow 4 to 6 weeks to receive your FIRST fill on your prescriptions. Regional Healthcare does not control shipments of medication. The pharmaceutical company which supplies
HealthyCare Card Application
 HealthyCare Card Application This is an application for the HealthyCare Card, a program of Healthy Community Network. The HealthyCare Card (HCC) is a community program which provides discounts to care
HealthyCare Card Application This is an application for the HealthyCare Card, a program of Healthy Community Network. The HealthyCare Card (HCC) is a community program which provides discounts to care
Rx for Oklahoma P.O. Box 603 Jay, OK Phone: ext 34 or 29 Fax:
 Rx for Oklahoma P.O. Box 603 Jay, OK 74346 Phone: 918-253-4683 ext 34 or 29 Fax: 918-253-6059 Email: lindaely@neocaa.org Email: lrutherford@neocaa.org Serving Craig, Delaware and Ottawa Counties Thank
Rx for Oklahoma P.O. Box 603 Jay, OK 74346 Phone: 918-253-4683 ext 34 or 29 Fax: 918-253-6059 Email: lindaely@neocaa.org Email: lrutherford@neocaa.org Serving Craig, Delaware and Ottawa Counties Thank
FINANCIAL ASSISTANCE APPLICATION: COVER LETTER
 FINANCIAL ASSISTANCE APPLICATION: COVER LETTER Thank you for choosing Children s of Alabama to provide for the healthcare needs of your child. Please find attached the forms you must complete in order
FINANCIAL ASSISTANCE APPLICATION: COVER LETTER Thank you for choosing Children s of Alabama to provide for the healthcare needs of your child. Please find attached the forms you must complete in order
SUPPLEMENTAL INFORMATION. Spouse Information Form
 SUPPLEMENTAL INFORMATION Spouse Information Form NJ FamilyCare Aged, Blind, Disabled Programs SECTION 1 Applicant 2 (Spouse) STATE of NEW JERSEY Department of Human Services Division of Medical Assistance
SUPPLEMENTAL INFORMATION Spouse Information Form NJ FamilyCare Aged, Blind, Disabled Programs SECTION 1 Applicant 2 (Spouse) STATE of NEW JERSEY Department of Human Services Division of Medical Assistance
Application Adult & Dislocated Worker Programs
 Application Adult & Dislocated Worker Programs Workforce Innovation and Opportunity Act (WIOA) FORM WIOA I-B 1.1 For Adult and Dislocated Worker Programs If you are age 18 or older and need help in obtaining
Application Adult & Dislocated Worker Programs Workforce Innovation and Opportunity Act (WIOA) FORM WIOA I-B 1.1 For Adult and Dislocated Worker Programs If you are age 18 or older and need help in obtaining
Health Care Coverage APPLICATION FOR. Health Care in Pennsylvania. Easy, affordable protection for your family
 Important information about health care benefits. Ask someone to read this to you. APPLICATION FOR Health Care Coverage This application may be used by families with children or by pregnant women who apply
Important information about health care benefits. Ask someone to read this to you. APPLICATION FOR Health Care Coverage This application may be used by families with children or by pregnant women who apply
Acceptable Dependent Verification Items (Including Spouse as a Dependent)
") BILLING EXHIBIT A: APPROVED DOCUMENT LIST We will review and consider household financial income for possible discounted services. Qualification for Financial Assistance depends upon a number of things
BILLING EXHIBIT A: APPROVED DOCUMENT LIST We will review and consider household financial income for possible discounted services. Qualification for Financial Assistance depends upon a number of things
P E N N S Y L V A N I A Application for Payment of Medicare Premiums, Coinsurance and Deductibles
 P E N N S Y L V A N I A Application for Payment of Medicare Premiums, Coinsurance and Deductibles If you have a disability and need this form in large print or another format, please call our helpline
P E N N S Y L V A N I A Application for Payment of Medicare Premiums, Coinsurance and Deductibles If you have a disability and need this form in large print or another format, please call our helpline
Application for Legal Assistance
 Application for Legal Assistance 1. What Brought You Here. (Please print clearly). Date: Briefly state your legal issue: Are you (or have you been) represented by an attorney in this matter? If so, who?
Application for Legal Assistance 1. What Brought You Here. (Please print clearly). Date: Briefly state your legal issue: Are you (or have you been) represented by an attorney in this matter? If so, who?
Affordable Homeownership Program Application: Instructions
 Affordable Homeownership Program Application: Instructions Habitat reviews applications on a first come, first served basis. Please expect the entire application process to take between 1 3 months. Instructions
Affordable Homeownership Program Application: Instructions Habitat reviews applications on a first come, first served basis. Please expect the entire application process to take between 1 3 months. Instructions
PATIENT REGISTRATION FORM
 Patient Information PATIENT REGISTRATION FORM (Name) First: M.I. Last: Address: City: State: Zip: D.O.B. Email: (Phones) Home: Cell: Work: Fill out both above and below section with patient information,
Patient Information PATIENT REGISTRATION FORM (Name) First: M.I. Last: Address: City: State: Zip: D.O.B. Email: (Phones) Home: Cell: Work: Fill out both above and below section with patient information,
Patient Financial Assistance Application
 This application is used to evaluate your eligibility for the University of Texas MD Anderson Cancer Center s Patient Financial Assistance Program. To ensure prompt review of your application, please complete
This application is used to evaluate your eligibility for the University of Texas MD Anderson Cancer Center s Patient Financial Assistance Program. To ensure prompt review of your application, please complete
Tri-County Community Council, Inc PO Box 1210 Bonifay, Florida 32425
 Tri-County Community Council, Inc PO Box 1210 Bonifay, Florida 32425 ***PROOF OF ALL HOUSEHOLD INCOME (LAST 30 DAYS), ELECTRIC OR GAS BILL, CURRENT PICTURE ID ON APPLICANT, AND SOCIAL SECURITY CARDS ON
Tri-County Community Council, Inc PO Box 1210 Bonifay, Florida 32425 ***PROOF OF ALL HOUSEHOLD INCOME (LAST 30 DAYS), ELECTRIC OR GAS BILL, CURRENT PICTURE ID ON APPLICANT, AND SOCIAL SECURITY CARDS ON
DO NOT LEAVE ANY PART BLANK, WRITE NO or NA (Not Applicable) Head of Household Last Name First Name Middle Initial
 Head of Household Last Name First Name Middle Initial") Lake County Housing Authority 33928 North US Highway 45 Grayslake, IL 60030 PERSONAL DECLARATION This Form MUST be completely filled out personally by the head of the household. You must use the correct
Lake County Housing Authority 33928 North US Highway 45 Grayslake, IL 60030 PERSONAL DECLARATION This Form MUST be completely filled out personally by the head of the household. You must use the correct
Child Health Plus Annual Recertification Notice
 Child Health Plus Annual Recertification Notice Important Information Enclosed Each year, you will be required to recertify your child's coverage by verifying income and residency. Three months prior to
Child Health Plus Annual Recertification Notice Important Information Enclosed Each year, you will be required to recertify your child's coverage by verifying income and residency. Three months prior to
APPLICATION PACKET. Please read pages 1 through 6 for some important things you ll need to know before you apply.
 DEPARTMENT OF HEALTH AND FAMILY SERVICES Division of Health Care Access and Accountability HCF 10182 (02/08) STATE OF WISCONSIN APPLICATION PACKET Please read pages 1 through 6 for some important things
DEPARTMENT OF HEALTH AND FAMILY SERVICES Division of Health Care Access and Accountability HCF 10182 (02/08) STATE OF WISCONSIN APPLICATION PACKET Please read pages 1 through 6 for some important things
Application for Medical Assistance for the Elderly and Persons with Disabilities
 Application for Medical Assistance for the Elderly and Persons with Disabilities KC1500 Who can use this application? Apply faster online This application is for the elderly and persons with disabilities
Application for Medical Assistance for the Elderly and Persons with Disabilities KC1500 Who can use this application? Apply faster online This application is for the elderly and persons with disabilities
FINANCIAL ASSISTANCE PROGRAM
 Financial Assistance Application FINANCIAL ASSISTANCE PROGRAM As part of our mission, Benefis Health System (including Benefis Hospitals in Great Falls and Benefis Teton Medical Center in Choteau) is committed
Financial Assistance Application FINANCIAL ASSISTANCE PROGRAM As part of our mission, Benefis Health System (including Benefis Hospitals in Great Falls and Benefis Teton Medical Center in Choteau) is committed
We Do Business in Accordance to the Federal Fair Housing Law
 PLEASE COMPLETE IN FULL Housing Authority of the City of Fort Myers Affordable Housing - HORIZONS APARTMENTS 5360 Summerlin Road, Fort Myers, FL 33919 Telephone (239) 936-6760 Fax (239) 936-6761 TDD (239)
PLEASE COMPLETE IN FULL Housing Authority of the City of Fort Myers Affordable Housing - HORIZONS APARTMENTS 5360 Summerlin Road, Fort Myers, FL 33919 Telephone (239) 936-6760 Fax (239) 936-6761 TDD (239)
The Caring Hearts Program covers services which are deemed to be medically necessary as determined by your physician.
 Enclosed please find a Caring Hearts Financial Assistance Application. Please complete the entire application and submit all requested supporting documentation to avoid denial of your application. Caring
Enclosed please find a Caring Hearts Financial Assistance Application. Please complete the entire application and submit all requested supporting documentation to avoid denial of your application. Caring
Application for Legal Assistance
 Application for Legal Assistance 1. What Brought You Here. (Please print clearly). Date: Briefly state your legal issue: Are you (or have you been) represented by an attorney in this matter? If so, who?
Application for Legal Assistance 1. What Brought You Here. (Please print clearly). Date: Briefly state your legal issue: Are you (or have you been) represented by an attorney in this matter? If so, who?
1. APPLICANT INFORMATION. Co-Applicant (spouse must be Co-Applicant) Name Male Female Name Male Female
 Name Male Female Name Male Female") Return by on to: Habitat for Humanity of Greater Plainfield & Middlesex County 2 Randolph Road Plainfield, NJ 07060 Include 25 processing fee in check or money order only. Questions? Call Plainfield Habitat
Return by on to: Habitat for Humanity of Greater Plainfield & Middlesex County 2 Randolph Road Plainfield, NJ 07060 Include 25 processing fee in check or money order only. Questions? Call Plainfield Habitat
If you have any questions prior to mailing or bringing your application in, please feel free to contact our department at
 NJ Hospital Care Assistance Program(NJHCAPS) NJ Hospital Care Assistance Program (formerly known as Charity Care) is available to every patient regardless of whether they are insured or not. Each patient
NJ Hospital Care Assistance Program(NJHCAPS) NJ Hospital Care Assistance Program (formerly known as Charity Care) is available to every patient regardless of whether they are insured or not. Each patient
ST. CLAIR HOSPITAL APPLICATION FOR FINANCIAL ASSISTANCE / CHARITY CARE DEMOGRAPHICS AND SCREENING
 DEMOGRAPHICS AND SCREENING PATIENT DEMOGRAPHIC Patient Name Patient Phone # Patient Address Marital Status: SINGLE MARRIED SEPARATED DIVORCED WIDOWED HOUSEHOLD DEMOGRAPHIC Line Date of Birth Relationship
DEMOGRAPHICS AND SCREENING PATIENT DEMOGRAPHIC Patient Name Patient Phone # Patient Address Marital Status: SINGLE MARRIED SEPARATED DIVORCED WIDOWED HOUSEHOLD DEMOGRAPHIC Line Date of Birth Relationship
MAYOR BYRON W. BROWN S SUMMER YOUTH INTERNSHIP PROGRAM APPLICATION
 MAYOR BYRON W. BROWN S SUMMER YOUTH INTERNSHIP PROGRAM February 1, 2018 Dear Applicant: Thank you for your interest in applying for my 2018 Summer Youth Internship Program. This is truly a wonderful opportunity
MAYOR BYRON W. BROWN S SUMMER YOUTH INTERNSHIP PROGRAM February 1, 2018 Dear Applicant: Thank you for your interest in applying for my 2018 Summer Youth Internship Program. This is truly a wonderful opportunity
Financial Assistance Application
 Financial Assistance Application Please complete the following application to determine eligibility for the Financial Assistance Program. If you have any questions, please call a Financial Counselor. Please
Financial Assistance Application Please complete the following application to determine eligibility for the Financial Assistance Program. If you have any questions, please call a Financial Counselor. Please
If you have questions about how much your fee will be, you may stop by or call with your income information before your appointment.
 238 Arsenal Street, Watertown, NY Family Practice Office: (315) 782-6400 Fax: (315) 782-1330 Adult Office: (315) 782-9903 Fax: (315) 788-0087 Dental Office: (315) 788-9834 Fax: (315) 788-5456 7785 N. State
238 Arsenal Street, Watertown, NY Family Practice Office: (315) 782-6400 Fax: (315) 782-1330 Adult Office: (315) 782-9903 Fax: (315) 788-0087 Dental Office: (315) 788-9834 Fax: (315) 788-5456 7785 N. State
Your Community Health Center If you need help filling out this form, please let us know. PATIENT REGISTRATION FORM (Please Print)
") Your Community Health Center If you need help filling out this form, please let us know. PATIENT REGISTRATION FORM (Please Print) Today s Date: YCHC Medical Provider: YCHC Dental Provider: PATIENT INFORMATION
Your Community Health Center If you need help filling out this form, please let us know. PATIENT REGISTRATION FORM (Please Print) Today s Date: YCHC Medical Provider: YCHC Dental Provider: PATIENT INFORMATION
Pharmaceutical Assistance Program
 Thank you for choosing the Shannon Pharmaceutical Assistance Program to provide service for you. Our goal is to provide medications at a minimal cost for qualifying patients with chronic conditions so
Thank you for choosing the Shannon Pharmaceutical Assistance Program to provide service for you. Our goal is to provide medications at a minimal cost for qualifying patients with chronic conditions so
MEDICATION ASSISTANCE PROGRAM
 1993 Harrison Street Batesville, AR 72501 870.698.9991 (P) 870.698.0022 (F) 1200 South Main Street Searcy, AR 72143 501.268.5000 (P) 501.268.5006 (F) MEDICATION ASSISTANCE PROGRAM Dear Client, Enclosed
1993 Harrison Street Batesville, AR 72501 870.698.9991 (P) 870.698.0022 (F) 1200 South Main Street Searcy, AR 72143 501.268.5000 (P) 501.268.5006 (F) MEDICATION ASSISTANCE PROGRAM Dear Client, Enclosed
APPLICATION FOR SCHOLARSHIP MEMBERSHIP
 APPLICATION FOR SCHOLARSHIP MEMBERSHIP The Skagit Valley Family YMCA provides financial assistance to the extent possible to those in need. Proof of income is required and eligibility is determined by
APPLICATION FOR SCHOLARSHIP MEMBERSHIP The Skagit Valley Family YMCA provides financial assistance to the extent possible to those in need. Proof of income is required and eligibility is determined by
The St Mary Medical Center Financial Assistance program does not cover the cost from all physician offices.
 Dear St. Mary Medical Center is committed to providing high quality care to all in our community. We may be able to assist you with your medical bills if you are not able to afford them. Please read the
Dear St. Mary Medical Center is committed to providing high quality care to all in our community. We may be able to assist you with your medical bills if you are not able to afford them. Please read the
RENTAL APPLICATION CHECKLIST
 RENTAL APPLICATION CHECKLIST Please note: The application will not be accepted with incomplete information and missing documentation. All documents requested must be provided. Name: Date & Time: Applicant(s)
RENTAL APPLICATION CHECKLIST Please note: The application will not be accepted with incomplete information and missing documentation. All documents requested must be provided. Name: Date & Time: Applicant(s)
Arapahoe Housing Authority
 Arapahoe Housing Authority 208 Sixth Street, Box 0 Arapahoe, NE 68922 Telephone: (308) 962-7669 Fax: (308) 962-3669 Email: araphous@atcjet.net Office Use Only: Date of Application: Time of Application:
Arapahoe Housing Authority 208 Sixth Street, Box 0 Arapahoe, NE 68922 Telephone: (308) 962-7669 Fax: (308) 962-3669 Email: araphous@atcjet.net Office Use Only: Date of Application: Time of Application:
DEMOGRAPHICS. Last (Please Print) First MI. Street/Avenue (Please Print)
 First MI. Street/Avenue (Please Print)") Application Date: DEMOGRAPHICS County Office: Social Security #: Birth Date: / / Gender: [ ] Male [ ] Female Last & First Name: Last (Please Print) First MI Maiden Name: (If applicable) Current Address:
Application Date: DEMOGRAPHICS County Office: Social Security #: Birth Date: / / Gender: [ ] Male [ ] Female Last & First Name: Last (Please Print) First MI Maiden Name: (If applicable) Current Address:
Virginia Individual Development Accounts Candidate Application
 Virginia Individual Development Accounts Candidate Application VIDA candidates must use this application to show that they meet the five criteria below. This form is also used to establish a VIDA savings
Virginia Individual Development Accounts Candidate Application VIDA candidates must use this application to show that they meet the five criteria below. This form is also used to establish a VIDA savings
Finance Division Revenue Cycle Operational Policy Page 1 of 6. Financial Assistance Program
 Finance Division Revenue Cycle Operational Policy Page 1 of 6 Financial Assistance Program I. POLICY STATEMENT Origination Date: Revision Date: 2/4/09 4/15/09, 8/3/09, 2/15/11, 3/14, 1/16, 11/16 Grady
Finance Division Revenue Cycle Operational Policy Page 1 of 6 Financial Assistance Program I. POLICY STATEMENT Origination Date: Revision Date: 2/4/09 4/15/09, 8/3/09, 2/15/11, 3/14, 1/16, 11/16 Grady
Medicaid. Medicaid SOBRA. ALL Kids. for Low Income Families. Insurance. The Alabama Child Caring. Foundation
 Medicaid for Low Income Families ALL Kids Insurance SOBRA Medicaid The Alabama Child Caring Foundation THIS IS YOUR APPLICATION for free or low cost health care coverage. These programs cover low income
Medicaid for Low Income Families ALL Kids Insurance SOBRA Medicaid The Alabama Child Caring Foundation THIS IS YOUR APPLICATION for free or low cost health care coverage. These programs cover low income
FIRST TIME HOMEBUYER (FTHB) ASSISTANCE PROGRAM. City of Kenner Community Development Department PROGRAM INSTRUCTIONS & APPLICATION
 ASSISTANCE PROGRAM. City of Kenner Community Development Department PROGRAM INSTRUCTIONS & APPLICATION") Dear Applicant: City of Kenner Community Development Department PROGRAM INSTRUCTIONS & APPLICATION Thank you for your interest in the City of Kenner s First time Homebuyers Assistance Program (FTHB). Attached
Dear Applicant: City of Kenner Community Development Department PROGRAM INSTRUCTIONS & APPLICATION Thank you for your interest in the City of Kenner s First time Homebuyers Assistance Program (FTHB). Attached
HOMEOWNERSHIP APPLICATION (Rev. 3/16/17) = Submit a copy of each requested item to the application
 = Submit a copy of each requested item to the application") PART 1: Applicant(s) Information HOMEOWNERSHIP APPLICATION (Rev. 3/16/17) = Submit a copy of each requested item to the application Application deadline: no exceptions APPLICANT (Head of Household owner
PART 1: Applicant(s) Information HOMEOWNERSHIP APPLICATION (Rev. 3/16/17) = Submit a copy of each requested item to the application Application deadline: no exceptions APPLICANT (Head of Household owner
APPLICANT PLEASE DO NOT WRITE ON THIS SHEET FOR OFFICE USE ONLY
 Date received: Staff initials: Dear Applicant, Thank you for considering Coburn Place Safe Haven s transitional housing program for your new beginning! Coburn Place Safe Haven is a two year transitional
Date received: Staff initials: Dear Applicant, Thank you for considering Coburn Place Safe Haven s transitional housing program for your new beginning! Coburn Place Safe Haven is a two year transitional
Rural Housing, Inc. 1
 Rural Housing, Inc. 1 Application for Assistance: Property Taxes General Guidelines: Must be under 50% County Median Income by family size, call for specific $ limit Housing costs must be affordable, less
Rural Housing, Inc. 1 Application for Assistance: Property Taxes General Guidelines: Must be under 50% County Median Income by family size, call for specific $ limit Housing costs must be affordable, less
Application for health care coverage
 www.chipcoverspakids.com Keystone Health Plan East HMO Health Coverage Provided to Eligible Children Application for health care coverage If you would like a copy of this application in Spanish, please
www.chipcoverspakids.com Keystone Health Plan East HMO Health Coverage Provided to Eligible Children Application for health care coverage If you would like a copy of this application in Spanish, please
SENIOR HOME REPAIR GRANT (SHRG) Application Package
 Application Package") SENIOR HOME REPAIR GRANT (SHRG) Application Package 5555 Arlington Ave. Riverside, CA 92504 951-343-5469 Updated 10/22/12 Application Submission Checklist APPLICATION PACKAGE SUBMISSION CHECKLIST Participation
SENIOR HOME REPAIR GRANT (SHRG) Application Package 5555 Arlington Ave. Riverside, CA 92504 951-343-5469 Updated 10/22/12 Application Submission Checklist APPLICATION PACKAGE SUBMISSION CHECKLIST Participation
Massachusetts Application for Health and Dental Coverage and Help Paying Costs
 Massachusetts Application for Health and Dental Coverage and Help Paying Costs HOW TO APPLY USE THIS APPLICATION TO SEE WHAT COVERAGE CHOICES YOU MAY QUALIFY FOR. WHO CAN USE THIS APPLICATION? You can
Massachusetts Application for Health and Dental Coverage and Help Paying Costs HOW TO APPLY USE THIS APPLICATION TO SEE WHAT COVERAGE CHOICES YOU MAY QUALIFY FOR. WHO CAN USE THIS APPLICATION? You can
Welcome to Pine Grove Apartments. Thank you for your interest in our community.
 PINE GROVE APARTMENTS 600 Carlton Rd., #111 Palmetto, Georgia 30268 Tel 770-463-2107 Fax 770-463-5952 TDD # 800-255-0135 Visit our website: apartmentspalmetto.com TO ALL PROSPECTIVE RESIDENTS: Welcome
PINE GROVE APARTMENTS 600 Carlton Rd., #111 Palmetto, Georgia 30268 Tel 770-463-2107 Fax 770-463-5952 TDD # 800-255-0135 Visit our website: apartmentspalmetto.com TO ALL PROSPECTIVE RESIDENTS: Welcome
We Do Business in Accordance to the Federal Fair Housing Law
 PLEASE COMPLETE IN FULL SW Florida Affordable Choice Foundation, Inc. Application for Covington Meadows Covington Meadows Circle, Lehigh Acres, FL 33936 Telephone (239) 344-3220 Fax (239) 344-3273 TDD
PLEASE COMPLETE IN FULL SW Florida Affordable Choice Foundation, Inc. Application for Covington Meadows Covington Meadows Circle, Lehigh Acres, FL 33936 Telephone (239) 344-3220 Fax (239) 344-3273 TDD
The application must be completed in the handwriting of the head of household. Incomplete applications will not be processed.
 Important Information Please read this carefully before completing the application form If you or anyone in your family is a person with disabilities, and you require a specific accommodation in order
Important Information Please read this carefully before completing the application form If you or anyone in your family is a person with disabilities, and you require a specific accommodation in order
Moffitt Cancer. Policy: Charity Care/Financial Assistance. Policy Statement. Purpose. Scope. Procedures. Effective: 04/2018 Page 1 of 10
 Responsible Office: Business Office Category: Finance Authorized: Vice President, Revenue Cycle Policy Number: ADM-C032 Management Review Frequency: 3 years Effective: 04/2018 Policy Statement This Policy
Responsible Office: Business Office Category: Finance Authorized: Vice President, Revenue Cycle Policy Number: ADM-C032 Management Review Frequency: 3 years Effective: 04/2018 Policy Statement This Policy
Memorial Hermann Advantage (PPO)
") Memorial Hermann Advantage (PPO) 2016 Enrollment Form Follow these easy steps to enroll in a Memorial Hermann Advantage Preferred Provider Organization (PPO). 1. Each applicant must fill out a separate
Memorial Hermann Advantage (PPO) 2016 Enrollment Form Follow these easy steps to enroll in a Memorial Hermann Advantage Preferred Provider Organization (PPO). 1. Each applicant must fill out a separate
Application for Health Coverage and Help Paying Costs
 Iowa Department of Human Services Application for Health Coverage and Help Paying Costs Use this application to see what coverage choices you qualify for Affordable private health insurance plans that
Iowa Department of Human Services Application for Health Coverage and Help Paying Costs Use this application to see what coverage choices you qualify for Affordable private health insurance plans that
Post-Doc, Post-Doc Trainee & Instructor
 Post-Doc, Post-Doc Trainee & Instructor NEW-HIRE DOCUMENTS: Emergency Contact Information Form New Employee Disclosure Form Release of Reference Form Request for Verification of Prior State Service Form
Post-Doc, Post-Doc Trainee & Instructor NEW-HIRE DOCUMENTS: Emergency Contact Information Form New Employee Disclosure Form Release of Reference Form Request for Verification of Prior State Service Form
Memorial Hermann Advantage (HMO)
") Memorial Hermann Advantage (HMO) 2017 Enrollment Form Follow these easy steps to enroll in a Memorial Hermann Advantage Health Maintenance Organization (HMO). 1. Each applicant must fill out a separate
Memorial Hermann Advantage (HMO) 2017 Enrollment Form Follow these easy steps to enroll in a Memorial Hermann Advantage Health Maintenance Organization (HMO). 1. Each applicant must fill out a separate
ST. LAWRENCE COUNTY OFFICE OF INDIGENT DEFENSE 48 Court Street, Canton, New York Telephone:
 ST. LAWRENCE COUNTY OFFICE OF INDIGENT DEFENSE 48 Court Street, Canton, New York 13617-1169 Telephone: 315-379-2401 APPLICATION FOR ATTORNEY SERVICES Instruction Sheet You must submit ALL of the following
ST. LAWRENCE COUNTY OFFICE OF INDIGENT DEFENSE 48 Court Street, Canton, New York 13617-1169 Telephone: 315-379-2401 APPLICATION FOR ATTORNEY SERVICES Instruction Sheet You must submit ALL of the following
Independent Household Resources Verification Worksheet
 Independent Household Resources Verification Worksheet 2015-2016 Your 2015 2016 Free Application for Federal Student Aid (FAFSA) was selected for review in a process called verification. Federal regulations
Independent Household Resources Verification Worksheet 2015-2016 Your 2015 2016 Free Application for Federal Student Aid (FAFSA) was selected for review in a process called verification. Federal regulations
VETERANS ASSISTANCE PROGRAM ELIGIBILITY CERTIFICATION
 VETERANS ASSISTANCE PROGRAM ELIGIBILITY CERTIFICATION Assistance requested: Rent: Veteran must have rental agreement and/or eviction notice. Number of bedrooms Utilities: Veteran must have a disconnect/final
VETERANS ASSISTANCE PROGRAM ELIGIBILITY CERTIFICATION Assistance requested: Rent: Veteran must have rental agreement and/or eviction notice. Number of bedrooms Utilities: Veteran must have a disconnect/final
Agent Mailing Address City State Zip Code. Agent Address
 Application Medicare-Eligible Basic Plan Questions? Call 1-800-877-5187 Please type or PRINT in black ink All sections must be filled out completely Your premium and required documents should be included
Application Medicare-Eligible Basic Plan Questions? Call 1-800-877-5187 Please type or PRINT in black ink All sections must be filled out completely Your premium and required documents should be included
OTSEGO COUNTY DEPARTMENT OF SOCIAL SERVICES DOCUMENTATION REQUIREMENTS
 - 1 - OTSEGO COUNTY DEPARTMENT OF SOCIAL SERVICES DOCUMENTATION REQUIREMENTS THIS CHART IS A GUIDE ONLY BE SURE TO PROGRAMS ABBREVIATIONS REVIEW ALL 5 PAGES OF INFORMATION TA=Temporary Assistance X Required
- 1 - OTSEGO COUNTY DEPARTMENT OF SOCIAL SERVICES DOCUMENTATION REQUIREMENTS THIS CHART IS A GUIDE ONLY BE SURE TO PROGRAMS ABBREVIATIONS REVIEW ALL 5 PAGES OF INFORMATION TA=Temporary Assistance X Required
Eligibility Checklist
 Eligibility Checklist Patient s Name: of Service: /_/ Medical Record #: _ Account Number: _ You are encouraged to apply one week prior to any appointments with proof of appointment and/or referral. In
Eligibility Checklist Patient s Name: of Service: /_/ Medical Record #: _ Account Number: _ You are encouraged to apply one week prior to any appointments with proof of appointment and/or referral. In
Asian American Health Coalition - Hope Clinic 7001 Corporate Drive, Ste 120 Houston, Texas Phone (713) ~ Fax (713)
 ~ Fax (713)") PATIENT REGISTRATION Staff: Today s : of Birth: Last Name: First Name: Middle Name Gender: Female Male Social Security # : - - Address: Apt: City: State: Zip Code: Home Phone #: Cell Phone #: Can we leave
PATIENT REGISTRATION Staff: Today s : of Birth: Last Name: First Name: Middle Name Gender: Female Male Social Security # : - - Address: Apt: City: State: Zip Code: Home Phone #: Cell Phone #: Can we leave
1) NOTE: There is only one rental unit in this program. It is a single-family, threebedroom house, suitable for a family size of up to five people.
 NOTE: There is only one rental unit in this program. It is a single-family, threebedroom house, suitable for a family size of up to five people.") SUDBURY HOUSING AUTHORITY LOCAL PROGRAM Pre-Application 2016 1) NOTE: There is only one rental unit in this program. It is a single-family, threebedroom house, suitable for a family size of up to five
SUDBURY HOUSING AUTHORITY LOCAL PROGRAM Pre-Application 2016 1) NOTE: There is only one rental unit in this program. It is a single-family, threebedroom house, suitable for a family size of up to five
CAN T AFFORD THE FULL COST OF AN ITEM YOU NEED TO MAINTAIN OR INCREASE INDEPENDENCE? APPLY FOR A LOAN TO BREAK DOWN THE COST INTO MONTHLY PAYMENTS!
 CAN T AFFORD THE FULL COST OF AN ITEM YOU NEED TO MAINTAIN OR INCREASE INDEPENDENCE? APPLY FOR A LOAN TO BREAK DOWN THE COST INTO MONTHLY PAYMENTS! INTERESTED? WHAT TO DO NEXT: 1. Determine the item that
CAN T AFFORD THE FULL COST OF AN ITEM YOU NEED TO MAINTAIN OR INCREASE INDEPENDENCE? APPLY FOR A LOAN TO BREAK DOWN THE COST INTO MONTHLY PAYMENTS! INTERESTED? WHAT TO DO NEXT: 1. Determine the item that
INFORMATION UPDATE FOR HOUSING BRING COMPLETED APPLICATION TO YOUR APPOINTMENT FOR OFFICE USE ONLY: Application Annual Mover
 IMPORTANT TE: If you or anyone in your family is a person with disabilities, and you require a specific accommodation in order to fully utilize our programs and/or services, please contact the Housing
IMPORTANT TE: If you or anyone in your family is a person with disabilities, and you require a specific accommodation in order to fully utilize our programs and/or services, please contact the Housing
Application for Benefits Medicaid Buy-In for Children
 Texas Health and Human Services Commission Form H1200-MBIC Cover Letter January 2011 Application for Benefits Medicaid Buy-In for Children About this program: Medicaid Buy-In for Children can help pay
Texas Health and Human Services Commission Form H1200-MBIC Cover Letter January 2011 Application for Benefits Medicaid Buy-In for Children About this program: Medicaid Buy-In for Children can help pay
Applications will only be accepted from
 May 2018 Dear Applicant, Thank you for your interest in applying to Pikes Peak Habitat for Humanity! Enclosed you will find the Habitat for Humanity application. Before completing the application, please
May 2018 Dear Applicant, Thank you for your interest in applying to Pikes Peak Habitat for Humanity! Enclosed you will find the Habitat for Humanity application. Before completing the application, please
TOWN OF TUFTONBORO PO BOX 98, 240 MIDDLE ROAD CENTER TUFTONBORO, NH Telephone (603) Fax (603)
 Fax (603)") TOWN OF TUFTONBORO PO BOX 98, 240 MIDDLE ROAD CENTER TUFTONBORO, NH 03816 Telephone (603) 569-4539 Fax (603) 569-4328 APPLICATION FOR GENERAL ASSISTANCE Date of Application Referred by: Name Street Address
TOWN OF TUFTONBORO PO BOX 98, 240 MIDDLE ROAD CENTER TUFTONBORO, NH 03816 Telephone (603) 569-4539 Fax (603) 569-4328 APPLICATION FOR GENERAL ASSISTANCE Date of Application Referred by: Name Street Address
FAMILY ASSETS FOR INDEPENDENCE IN MINNESOTA (FAIM) FAIM New Participant Application Form AGENCY USE ONLY : Agency Name:
 FAIM New Participant Application Form AGENCY USE ONLY : Agency Name:") FAMILY ASSETS FOR INDEPENDENCE IN MINNESOTA (FAIM) AGENCY USE ONLY : FAIM New Participant Application Form Revised 05/23/14 Agency Name: Bank Account Number of 1 st Deposit Asset Grant First Name MI Last
FAMILY ASSETS FOR INDEPENDENCE IN MINNESOTA (FAIM) AGENCY USE ONLY : FAIM New Participant Application Form Revised 05/23/14 Agency Name: Bank Account Number of 1 st Deposit Asset Grant First Name MI Last
Administrative and Operational Policies and Procedures
 Policy 1.10 Original Date 01/15/2013 Number: Issued: Section: Finance Date Reviewed: 04/29/2013 Title: Financial Assistance Policy Date Revised: 01/01/2014 11/01/2016 08/01/2018 Regulatory Agency: Department
Policy 1.10 Original Date 01/15/2013 Number: Issued: Section: Finance Date Reviewed: 04/29/2013 Title: Financial Assistance Policy Date Revised: 01/01/2014 11/01/2016 08/01/2018 Regulatory Agency: Department
Our Mission. Promoting Independence by Providing Car Care
 Please Submit the Following: Our Mission Check List Douglas County Residents Only Promoting Independence by Providing Car Care FOR ALL APPLICANTS Fill out application completely and sign Sign the attached
Please Submit the Following: Our Mission Check List Douglas County Residents Only Promoting Independence by Providing Car Care FOR ALL APPLICANTS Fill out application completely and sign Sign the attached
Please check the type of assistance you are requesting: Rent Deposit Utility Medication Food Bus Passes ID Dental Medical COBRA Other
 Last Name IC New Case # For office use only Application for County Assistance Primary language Do you need an Interpreter? Y N Please check the type of assistance you are requesting: Rent Deposit Utility
Last Name IC New Case # For office use only Application for County Assistance Primary language Do you need an Interpreter? Y N Please check the type of assistance you are requesting: Rent Deposit Utility
Application for Transitional Housing
 United Ministries, Inc. EARLS PLACE 1400 E. Lombard Street Baltimore, Maryland 21231 Application for Transitional Housing Today s Date: General Information How did you hear about Earl s Place? First Name:
United Ministries, Inc. EARLS PLACE 1400 E. Lombard Street Baltimore, Maryland 21231 Application for Transitional Housing Today s Date: General Information How did you hear about Earl s Place? First Name:
Jane Place Neighborhood Sustainability Initiative! Application:! Palmyra Apartments!
 Thank you for contacting Jane Place Neighborhood Sustainability Initiative regarding rental availabilities at 2739 Palmyra Street. The first step in the process is to complete the enclosed application."
Thank you for contacting Jane Place Neighborhood Sustainability Initiative regarding rental availabilities at 2739 Palmyra Street. The first step in the process is to complete the enclosed application."
COMMUNITY FINANCIAL ASSISTANCE APPLICATION
 COMMUNITY FINANCIAL ASSISTANCE APPLICATION Attached is Mary Free Bed Rehabilitation Hospital s Community Financial Assistance Application Form (CFA-3). If you are interested in applying for financial assistance
COMMUNITY FINANCIAL ASSISTANCE APPLICATION Attached is Mary Free Bed Rehabilitation Hospital s Community Financial Assistance Application Form (CFA-3). If you are interested in applying for financial assistance
Hough Heritage. Application Instructions. 2. Use only black or blue ink. Colored inks, markers or pencil are not permitted.
 Hough Heritage Application Instructions 1. Please print all answers. 2. Use only black or blue ink. Colored inks, markers or pencil are not permitted. 3. If a question does not apply, please write N/A
Hough Heritage Application Instructions 1. Please print all answers. 2. Use only black or blue ink. Colored inks, markers or pencil are not permitted. 3. If a question does not apply, please write N/A
BASED ON INCOME FROM 2017
 BASED ON INCOME FROM 2017 Tax Year 2018 Renewal Form Assessment Year 2017 Property Tax Exemption for Senior Citizens and Disabled Persons Chapter 84.36 RCW and Chapter 458-16A WAC You are receiving a reduction
BASED ON INCOME FROM 2017 Tax Year 2018 Renewal Form Assessment Year 2017 Property Tax Exemption for Senior Citizens and Disabled Persons Chapter 84.36 RCW and Chapter 458-16A WAC You are receiving a reduction
Submit your application by fax or mail to: Ray of Hope Cancer Foundation 3455 Ringsby Court #111 Denver, CO Fax:
 This application is for both organizations. Please send a copy to each individual organization to which you are applying. Eligibility varies between organizations, so carefully confirm your eligibility
This application is for both organizations. Please send a copy to each individual organization to which you are applying. Eligibility varies between organizations, so carefully confirm your eligibility
Before your appointment:
 Call the Receptionist @ (270) 467-7120 To Schedule an Appointment with SHAWN SALES Thank you for your interest in applying for residency at the Housing Authority of Bowling Green. Enclosed is the declaration,
Call the Receptionist @ (270) 467-7120 To Schedule an Appointment with SHAWN SALES Thank you for your interest in applying for residency at the Housing Authority of Bowling Green. Enclosed is the declaration,
Enrollment INSTRUCTIONS
 Enrollment INSTRUCTIONS UnitedHealthcare Group Medicare Advantage (PPO) is a Medicare Advantage Plan. UnitedHealthcare RxSupplement TM is an Outpatient Prescription Drug Plan that works together with your
Enrollment INSTRUCTIONS UnitedHealthcare Group Medicare Advantage (PPO) is a Medicare Advantage Plan. UnitedHealthcare RxSupplement TM is an Outpatient Prescription Drug Plan that works together with your
- Please return this packet with the needed information found on the second page. - DON T forget anything or it will delay the application!
 IU Health La Porte Community Health Center IU Health La Porte Dental Center 400 Teegarden Street, Suite B 400 Teegarden Street, Suite A La Porte, Indiana 46350 La Porte, Indiana 46350 Phone (219) 326-0043
IU Health La Porte Community Health Center IU Health La Porte Dental Center 400 Teegarden Street, Suite B 400 Teegarden Street, Suite A La Porte, Indiana 46350 La Porte, Indiana 46350 Phone (219) 326-0043
APPLICATION FOR STERN CENTER/CONGREGATE TRUMBULL HOUSING AUTHORITY 210 Hedgehog Circle Daisy Torres
 CONGREGATE LIVING Updated August 15, 2017 About the Congregate: THE CONGREGATE IS A SMOKE-FREE BUILDING By definition, the Congregate is a non-institutional, independent group living environment that integrates
CONGREGATE LIVING Updated August 15, 2017 About the Congregate: THE CONGREGATE IS A SMOKE-FREE BUILDING By definition, the Congregate is a non-institutional, independent group living environment that integrates
HFM/CASCADE DENTAL PLAN APPLICATION ADULT APPLICANT (age 18 and over)
") HFM/CASCADE DENTAL PLAN APPLICATION ADULT APPLICANT (age 18 and over) SECTION 1: INSTRUCTIONS 1. This form is for use by adults wishing to apply for Delta Dental benefits through the HFM/Cascade Dental
HFM/CASCADE DENTAL PLAN APPLICATION ADULT APPLICANT (age 18 and over) SECTION 1: INSTRUCTIONS 1. This form is for use by adults wishing to apply for Delta Dental benefits through the HFM/Cascade Dental
Prairie Harvest Mental Health Occupancy Application **IMPORTANT INFORMATION** READ & KEEP THIS PAGE
 Prairie Harvest Mental Health Occupancy Application 1 An Equal Housing Opportunity Provider To qualify for housing from Prairie Harvest Mental Health, the applicant must meet the following criteria: Applicants
Prairie Harvest Mental Health Occupancy Application 1 An Equal Housing Opportunity Provider To qualify for housing from Prairie Harvest Mental Health, the applicant must meet the following criteria: Applicants
**Keep in mind that you do not need to mail this print-out to your local agency.**
 **Keep in mind that you do not need to mail this print-out to your local agency.** Thank you for using MI Bridges to apply for benefits! Jackson, your application was sent to the following address on May
**Keep in mind that you do not need to mail this print-out to your local agency.** Thank you for using MI Bridges to apply for benefits! Jackson, your application was sent to the following address on May
Financial Assistance/Charity Care Application Form Instructions
 Financial Assistance/Charity Care Application Form Instructions This is an application for financial assistance (also known as charity care) at Seattle Cancer Care Alliance (SCCA). Washington State requires
Financial Assistance/Charity Care Application Form Instructions This is an application for financial assistance (also known as charity care) at Seattle Cancer Care Alliance (SCCA). Washington State requires
Request for Benefits. For use with Forms 08MP002E and 08MP003E
 *PS1 * Date: Case name: Case number: County number. Supervisor/worker number: / Request for Benefits For use with Forms 08MP002E and 08MP003E What you need to do to get started: Read the following descriptions
*PS1 * Date: Case name: Case number: County number. Supervisor/worker number: / Request for Benefits For use with Forms 08MP002E and 08MP003E What you need to do to get started: Read the following descriptions
UNIVERSITY MEDICAL CENTER OF PRINCETON AT PLAINSBORO NEW JERSEY HOSPITAL CARE ASSISTANCE PROGRAM REQUIREMENT LIST
 UNIVERSITY MEDICAL CENTER OF PRINCETON AT PLAINSBORO NEW JERSEY HOSPITAL CARE ASSISTANCE PROGRAM REQUIREMENT LIST To further assist us in processing your application for Charity Care, please provide copies
UNIVERSITY MEDICAL CENTER OF PRINCETON AT PLAINSBORO NEW JERSEY HOSPITAL CARE ASSISTANCE PROGRAM REQUIREMENT LIST To further assist us in processing your application for Charity Care, please provide copies
DELAWARE CHILDREN S CARE PLAN
 DELAWARE CHILDREN S CARE PLAN About DCCP Available through Highmark Blue Cross Blue Shield Delaware (Highmark Delaware), the Delaware Children s Care Plan (DCCP) provides comprehensive health benefits
DELAWARE CHILDREN S CARE PLAN About DCCP Available through Highmark Blue Cross Blue Shield Delaware (Highmark Delaware), the Delaware Children s Care Plan (DCCP) provides comprehensive health benefits
Security Deposit Loan Application 405 SW 6th Street Redmond, Oregon *
 Security Deposit Loan Application 405 SW 6th Street Redmond, Oregon 97756 * 541-923-1018 Thank you for your interest in the Families Forward loan program. Loans are available to Housing Choice Voucher
Security Deposit Loan Application 405 SW 6th Street Redmond, Oregon 97756 * 541-923-1018 Thank you for your interest in the Families Forward loan program. Loans are available to Housing Choice Voucher
Medical Assistance (Medicaid) Financial Eligibility Application for Long Term Care, Supports and Services
 Financial Eligibility Application for Long Term Care, Supports and Services") Check any that you are applying for: Medical Assistance (Medicaid) Financial Eligibility Application for Long Term Care, Supports and Services You may also apply online at www.compass.state.pa.us Care
Check any that you are applying for: Medical Assistance (Medicaid) Financial Eligibility Application for Long Term Care, Supports and Services You may also apply online at www.compass.state.pa.us Care
Sliding Fee Program. Gwinn 135 East M-35 Gwinn, MI (906) Iron River 1500 W. Ice Lake Rd. Iron River, MI (906)
 Iron River 1500 W. Ice Lake Rd. Iron River, MI (906)") Sliding Fee Program What is the Sliding Fee Program? The Sliding Fee Program is a federally funded program that provides a discount to patients who are uninsured or underinsured. This program allows qualifying
Sliding Fee Program What is the Sliding Fee Program? The Sliding Fee Program is a federally funded program that provides a discount to patients who are uninsured or underinsured. This program allows qualifying
ACADEMIC YEAR To: EMPLID: Date: / / From:
 2017-2018 ACADEMIC YEAR To: EMPLID: Date: / / From: Please submit photocopies of the required documentation for calendar year 2015. DOCUMENTS MUST BE SUBMITTED AND ALL PROBLEMS WITH YOUR FAFSA MUST BE
2017-2018 ACADEMIC YEAR To: EMPLID: Date: / / From: Please submit photocopies of the required documentation for calendar year 2015. DOCUMENTS MUST BE SUBMITTED AND ALL PROBLEMS WITH YOUR FAFSA MUST BE
Application for Healthy Indiana Plan State Form (R4/12-10) HIP 2515
 HIP 2515") *DFRIHEE01* *This agency is requesting the disclosure of your Social Security Number in accordance with IC 4-1-8-1; disclosure is mandatory and this record cannot be processed without it. Instructions:
*DFRIHEE01* *This agency is requesting the disclosure of your Social Security Number in accordance with IC 4-1-8-1; disclosure is mandatory and this record cannot be processed without it. Instructions:
Medical Assistance (Medicaid) Financial Eligibility Application for Long Term Care, Supports and Services
 Financial Eligibility Application for Long Term Care, Supports and Services") Medical Assistance (Medicaid) Financial Eligibility Application for Long Term Care, Supports and Services You may also apply online at www.compass.state.pa.us Check any that you are applying for: Care
Medical Assistance (Medicaid) Financial Eligibility Application for Long Term Care, Supports and Services You may also apply online at www.compass.state.pa.us Check any that you are applying for: Care
Household Resources Verification Worksheet (V6) Independent Student
 Independent Student") 2014-2015 Household Resources Verification Worksheet (V6) Independent Student Your 2014 2015 Free Application for Federal Student Aid (FAFSA) was selected for review in a process called verification. The
2014-2015 Household Resources Verification Worksheet (V6) Independent Student Your 2014 2015 Free Application for Federal Student Aid (FAFSA) was selected for review in a process called verification. The
Application Letter. Once approved both medically and financially, the applicant may be admitted to Stella Maris pending appropriate bed availability.
 Application Letter The long term care application process at Stella Maris is twofold, involving both a medical and a financial review. Long term care is generally paid for either privately or by Maryland
Application Letter The long term care application process at Stella Maris is twofold, involving both a medical and a financial review. Long term care is generally paid for either privately or by Maryland
Phone Home Work Cell. Other Emergency Contacts Name Name Phone Home Phone Home
 FLORIDA HOSPITAL TRANSPLANT CENTER CLINIC DEMOGRAPHIC INFORMATION This application MUST be filled out completely. ALL incomplete applications will be returned to sender Name (First) (MI) (Last) (Maiden)
FLORIDA HOSPITAL TRANSPLANT CENTER CLINIC DEMOGRAPHIC INFORMATION This application MUST be filled out completely. ALL incomplete applications will be returned to sender Name (First) (MI) (Last) (Maiden)
Application for Legal Assistance
 Application for Legal Assistance Apply in person at Government Plaza, 205 Government St., Room 427 Check VLP voicemail or website to get current days & times to apply in person To return completed application:
Application for Legal Assistance Apply in person at Government Plaza, 205 Government St., Room 427 Check VLP voicemail or website to get current days & times to apply in person To return completed application:
POMERENE HOSPITAL CHARITY CARE PROGRAM REQUIREMENT LIST
 POMERENE HOSPITAL CHARITY CARE PROGRAM REQUIREMENT LIST Name of Patient: Date of Service: Account Number: Dear Applicant, Enclosed please find an application for the Pomerene Hospital Charity Care program.
POMERENE HOSPITAL CHARITY CARE PROGRAM REQUIREMENT LIST Name of Patient: Date of Service: Account Number: Dear Applicant, Enclosed please find an application for the Pomerene Hospital Charity Care program.