Child Health Plus Annual Recertification Notice
|
|
|
- Theodore O’Brien’
- 6 years ago
- Views:
Transcription
1 Child Health Plus Annual Recertification Notice Important Information Enclosed Each year, you will be required to recertify your child's coverage by verifying income and residency. Three months prior to your child's annual recertification date, we ask families to complete the Child Health Plus Renewal Form and return by a specified due date. It is important that you recertify on time to ensure that your child's coverage continues. Failure to recertify on time will result in the loss of your child's health insurance and a need to apply for new coverage. HELPFUL HINTS TO COMPLETE THE RENEWAL APPLICATION RECERTIFICATION APPLICATION Please fill in every question completely o List the parent/guardian who is applying for Child Health Plus for their child(ren). o The person listed in Section A must also sign the application in Section E. o The Home Address is where the child lives (it cannot be a Post Office Box). Mailing address can be different than the child s home address. SECTION B About Your Household: o o A Social Security Number (SSN) should be provided for all children recertifying who are U.S. Citizens. If your child s citizenship or immigration status was changed since last year, you may be required to provide proof to process your application. Please see Section G Documents page of the application to determine what forms/documents are acceptable. SECTION C Household Income Information: Current household income MUST be declared for all parents or responsible adults listed in Section B, even if the person does not receive any income. If no income is received you must check the box stating person does not receive income. You have two options to give proof of your income: o You can provide a Social Security Number for each individual who receives income. If you provide a Social Security Number, you do NOT have to provide any income documents with this form. However, all boxes must be completed for all adults living in the household (including children) who receive income. Exact amount must be listed. o You can provide proof of your income for each type of income listed. See the documentation checklist for acceptable proof of income.
2 SECTION D Household Expenses: o o o List anyone in Section C that pays for the care of a child or disabled adult in order to go to work or school. List anyone in Section C that pays for health insurance or if in the past 12 months a child renewing Child Health Plus coverage enrolled in additional health insurance coverage. If your child(ren) has/have other health insurance, they are NOT eligible for Child Health Plus. SECTION E Signature: The person who applied for the child (person listed in Section A) must sign the Application. Signature must be dated within 30 days of receipt of your recertification PREMIUM There may be a monthly premium for Child Health Plus. If you are required to pay a premium, one month s payment must be submitted with this form. To determine if you need to pay a premium based on your family s month income and household, please refer to the attached table How to Calculate Your Income and Family Income Premium Chart.
3 REVISED YCUN-F001 Tips for Completing: Section B, Question 5 of the Recertification Application State Health Benefit Plans provide health insurance coverage through the New York State Health Insurance Program (NYSHIP). Coverage is offered to employees/retirees of NYS government, the State Legislature and the Unified Court System. Some local government and school districts also elect to participate in NYSHIP. By entering yes in the Public Employees box, you are stating that you or your child are eligible for New York State Health Insurance Program (NYSHIP) or a public agency that pays all or part of the cost. By doing so, you are confirming your child s ineligibility for Child Health Plus Coverage. If you are not sure, check with your employer. DO NOT answer yes in this box if you are receiving Public Assistance from your local department of Social Services as the application could +be declined and or delayed.
4

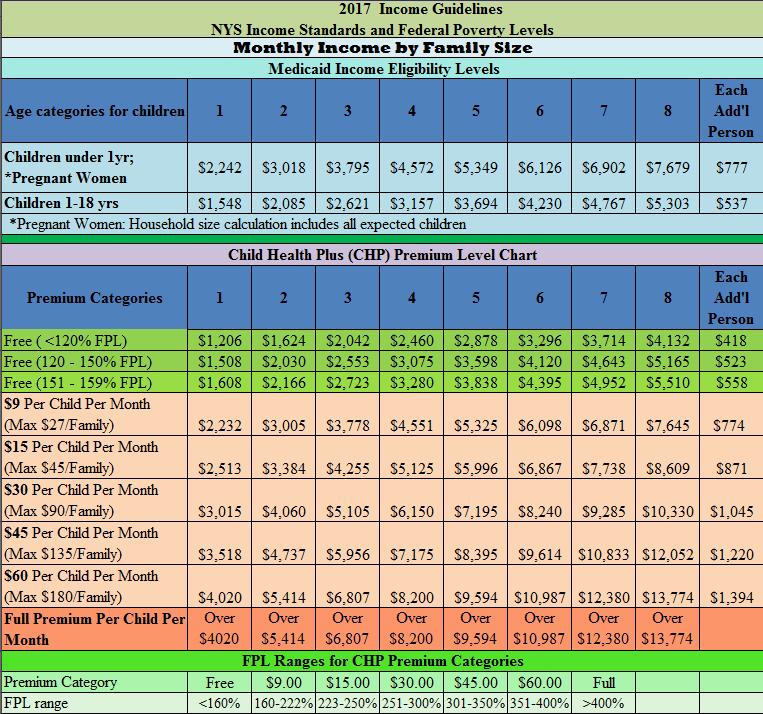
5 In an effort to streamline the enrollment process we developed this worksheet to help you determine if a premium is needed. Please be aware that we cannot process your application without the premium. The application will be returned to you if it is not included. You will need to use your GROSS income - the amount you receive before taxes/deductions are taken out. Also, if you receive TIPS, OVERTIME, or COMMISSION and it shows on your check you MUST count it in your calculations. Please remember that if you have more than one source of income you will have to do this calculation multiple times and combine the amounts to get the total household income amount. WEEKLY If you receive checks weekly use this example. Check 1: $ Check 2: + $ Check 3: Check4 TOTAL: Average: + $ $ $1, / 4 $ x Monthly Income: $1, BI-WEEKLY If you receive checks bi-weekly use this example. Check 1: $ Check 2: + $ TOTAL: Average: $ x Monthly Income: $ $ / 2 TWICE A MONTH If you receive checks on the 15 th and the last day of the month use this example. Check 1: $ Check 2: + $ TOTAL: $ Monthly Income: $ How to Calculate Your Income... MONTHLY If you receive checks once a month. Provide your most recent paystub. Check 1: $ TOTAL: $ Monthly Income: $ Child Health Plus Income Eligibility Effective 04/01/2017 YourCare Health Plan Full Premium $ Federal Poverty Levels for applications received on or after 04/01/2017 Family Size Free $9.00 $15.00 $30.00 $45.00 $60.00 Full Premium 1 $0 - $1,607 $1,608 - $2,232 $2,233 - $2,513 $2,514 - $3,015 $3,016 - $3,518 $3,519 - $4,020 $4,020 or greater 2 $0 - $2,165 $2,166 - $3,005 $3,006 - $3,384 $3,385 - $4,060 $4,061 - $4,737 $4,738 - $5,414 $5,414 or greater 3 $0 - $2,722 $2,723 - $3,778 $3,779 - $4,255 $4,256 - $5,105 $5,106 - $5,956 $5,957 - $6,807 $6,807 or greater 4 $0 - $3,279 $3,280 - $4,551 $4,552 - $5,125 $5,126 - $6,150 $6,151 - $7,175 $7,176 - $8,200 $8,200 or greater 5 $0 - $3,837 $3,838 - $5,325 $5,326 - $5,996 $5,997 - $7,195 $7,196 - $8,395 $8,396 - $ 9,594 $9,594 or greater 6 $0 - $4,394 $4,395 - $6,098 $6,099 - $6,867 $6,868 - $8,240 $8,241 - $9,614 $9,615 - $10,987 $l0,987 or greater Additional Person $558 $774 $871 $1045 $1220 $1394 No Family Contribution $9 Family Contribution $27 max per family per month $15 Family Contribution $45 max per family per month $30 Family Contribution $90 max per family per month $45 Family Contribution $135 max per family per month $60 Family Full Premium Contribution Per Child(ren) $180 max per family Per Month per month REVISED YCUN-C144
's health care coverage will end. Please make sure you answer all the questions on this form or your child(ren) may lose coverage.")
6 It is time to renew your child(ren)'s Child Health Plus (CHP) coverage! Please read this entire renewal form before you begin filling out the form. If you do not complete this form on time, your child(ren)'s health care coverage will end. Please make sure you answer all the questions on this form or your child(ren) may lose coverage. If you have questions about what is needed to renew your child(ren)'s coverage or need help completing this form, contact us at: Return Form to: YourCare Health Plan PO Box Eagan, MN Do not use this renewal form to add a new child to Child Health Plus. This form can only be used to renew coverage for children already enrolled in CHP who are under the age of 19 and to evaluate existing CHP members for Medicaid eligibility. If you would like to add a new child to CHP, please contact your health plan or a facilitated enroller to complete a new Access NY Health Care application for that child. * Child Health Plus Premium - There may be a monthly premium for Child Health Plus. If you are required to pay a premium, one month's payment must be submitted with this form. Please refer to the information on page 6 about family premium contributions to determine the amount of your monthly premium based upon your family's income and household size. If you have any questions or need to know where to mail your premium, please call YourCare Health Plan at: Important Information About Your Rights - You have the option of changing your Child Health Plus health plan at any time, but you will have to complete a new application on the New York State of Health Marketplace. You cannot use this renewal form to switch your Child Health Plus health plan. If your child is disabled or has a chronic illness, he/she may be eligible for Medicaid programs and services. To receive information about changing health plans or to learn about programs for special needs families, call SECTION A: CONTACT INFORMATION This section should be completed by a parent, guardian, or person renewing coverage on behalf of the child(ren). Tell us who you are and how to contact you. Legal First Name of Person Completing this Form Middle Initial Legal Last Name What Language Do You Primary Phone Number Another Phone Number Speak? Address Read? What type of number is this? Home Cell Work Other What type of number is this? Home Cell Work Other Do you want to receive information from your health plan via ? Yes No If known, please provide your child(ren) s health plan identification number(s): Home Address of the Children Renewing Health Insurance Street Address Did your address change in the past 12 months? Yes No Apartment Number City State Zip Code County Mailing Address if Different from the Home Address Street Address Apartment Number City State Zip Code County REVISED CHRU03 04/12
7 SECTION B: ABOUT YOUR HOUSEHOLD Page 2 of 6 (04/2012) You must answer all of the questions and check all appropriate boxes for each person listed. DO NOT LEAVE A BOX IN THE ROW BLANK. List information about yourself in the first row of boxes. In the other rows, list the name of all the children in the household, spouses, parents, step-parents, and any other children under 21 living with them. You may also list other household members at your option; however, they may not be added to your family size. This information helps us determine the size of your family and which program your child is eligible for. 1. Enter the full legal name of each person living in your household. List yourself in row Indicate how each person listed in this section is related to you (example: spouse, child, step-child, niece, etc.) 3. Give the date of birth for each person listed. 4. Write yes or no to indicate if this person is renewing CHP coverage. You must write no for all family members who are not renewing CHP coverage. 5. Write yes or no if this person is a Public Employee who can get health insurance coverage through a State Health Benefits Plan or the New York State Health Insurance Program (NYSHIP). NYSHIP is offered to employees/retirees of NYS government, the State Legislature and the Unified Court System. Some local government agencies and school districts also elect to participate with NYSHIP. If you are not sure, check with your employer or benefit administrator. If your child has access to a State Health Benefits Plan through NYSHIP, he/she will be ineligible for Child Health Plus coverage. 6. Indicate if this person is male or female. 7. Answer if anyone is pregnant in the household by writing yes or no. You will need to provide proof of pregnancy for anyone that is pregnant (see page 6). 8. Identify whether or not this person is a full time student by writing yes or no. 9. A Social Security Number (SSN) should be provided for any child renewing coverage or household member if they have one. Write Not Applicable (N/A) if this person does not have a Social Security Number. 10. Almost all children are eligible for either CHP or Medicaid, regardless of citizenship or immigration status, if they are New York State residents and do not have other health insurance. Please list every child's citizenship and immigration status to help us determine their program eligibility. If your child s immigration status has changed since the last application, you must provide proof of the change for each child (see page 6 for examples of acceptable proof) and give the date the child s immigration status changed. No proof is needed if your child s status has not changed in the last year Public Is this Citizenship or Immigration Category Relationship Renewing Employee with Person Full Social (Check a Box) to Person Date CHP State Health Sex Pregnant? Time Security Number Only enter a date of status if you check the Legal Name in Box 01 of Birth Coverage? Benefits? (Male or (Yes/No) Student? (If you have one) immigrant box (DOS: mm/dd/yy) (First, Middle Initial, Last) (Spouse, Child) (mm/dd/yy) (Yes/No) (Yes/No) Female) SEND PROOF (Yes/No) (XXX-XX-XXXX) ONLY SEND PROOF OF A CHANGE Self Revised CHRU04 04/12
8 SECTION C: HOUSEHOLD INCOME Page 3 of 6 (04/2012) Complete all of the following boxes for all adults living in the household as well as anyone else in the household (including children) who receive income. For each person, indicate what type(s) of income they receive, how much before taxes, and how often (weekly, every 2 weeks, monthly, or annually). If the person is not regularly employed throughout the year, or if the person's income goes up and down every month, write the amount the person expects to receive this calendar year. Do not use an income range or approximations. If there is No Income coming into the household, check the box below each person s name and indicate below how the renewing child(ren) are financially supported. Here is a list of different types of income that you may be receiving and we need to know about: * Earnings from Work: Gross Wages, Salaries, Commissions, Tips, Overtime, and Self- Employment before taxes * Unearned Income: Social Security Benefits (SSB), Disability Payments (SSD), Unemployment Payments, Interest and Dividends, Veteran's Benefits, Workers Compensation, Child Support/Alimony, Rental Income, and Pension * Contributions/Other: Income (money) from Relatives, Friends, Roomers and Boarders (include money that anyone gives to help meet living expenses), Temporary (Cash) Assistance, Supplemental Security Income (SSI), Student Grants, or Loans Name of ALL Adult(s) in Section B and Other Household Members, Including Children, Who Receive Income Social Security Number (XXX-XX-XXXX) You have two options to give proof of your income. 1. You can provide a Social Security Number for each individual who receives income for us to check (verify). If you provide a Social Security Number, you do NOT have to provide any income documents with this form. You must still complete all of the questions in this section. -OR- 2. You can provide proof of your income for each type of income listed. See page 6 for a list of documents you will need to provide as proof of your income. The proof submitted must be dated within one month prior to the date you sign this form and include the name of the person who gets the income. Type of Income (Either write your Social Security Number or You Must Send Proof of Your Household Income) Earnings from Work Unearned Income List Type : $ Do you receive Child Support? Yes No $ Check if this person does not receive income. Contributions/Other List Type: $ Earnings from Work Unearned Income List Type : $ Do you receive Child Support? Yes No $ Check if this person does not receive income. Contributions/Other List Type: $ Earnings from Work Unearned Income List Type : $ Do you receive Child Support? Yes No $ Check if this person does not receive income. Contributions/Other List Type: $ Earnings from Work Unearned Income List Type : $ Do you receive Child Support? Yes No $ Check if this person does not receive income. Contributions/Other List Type: $ How Much? (Before Taxes) How Often? (Ex: Monthly) NO INCOME: If there is no money coming into the household, explain below how the children renewing coverage are being supported. For example, the children are living with a friend/relative who is paying for their living expenses (room and/or board). If someone is paying your living expenses, you must supply a letter from the person providing support that they have signed and dated. The letter must include their name, address, telephone number and the amount they give you or the children for living expenses as well as how often. Explanation: REVISED CHRU05 04/12
9 SECTION D: HOUSEHOLD EXPENSES Page 4 of 6 (04/2012) Dependent Care Complete if anyone listed in Section C pays for the care of a child or a disabled adult in order to go to work or school. Child care/dependent care costs are how much a parent or other adult in the household pays another person to take care of child(ren) or dependent adult(s) while they are working or going to school. Some of this amount may be subtracted from the household's monthly income and will help us determine for which program the child(ren) are eligible. Please note that proof of these costs may be requested if your child appears eligible for the Medicaid program. Name of Person Being Cared For Amount Paid How Often $ Weekly Every 2 Weeks Monthly $ Weekly Every 2 Weeks Monthly $ Weekly Every 2 Weeks Monthly Health Insurance Complete if anyone listed in Section C pays for health insurance or if in the past 12 months a child renewing CHP coverage enrolled in additional health insurance coverage. If the applying children have other health insurance, you must provide proof of the other policy so we can determine if they are eligible (see page 6). Indicate your monthly cost (how much a parent or adult pays per month for their premium) and what type of coverage is provided under this health insurance policy. If you have a health insurance deduction taken from your paycheck stub, please indicate in this section the name of the policy holder and who the policy covers. Name of Policy Holder Person(s) Covered Insurance Company Name Monthly Cost Coverage Type $ $ $ Comprehensive Other: Comprehensive Other: Comprehensive Other: SEND PROOF Dental Only Dental Only Dental Only Vision Only Vision Only Vision Only SECTION E: SIGNATURE You must sign and date the application. Your application cannot be processed without your signature. By signing this application, I agree to have the information on this application shared only among Child Health Plus and Medicaid, my health plan, the local social services district, and the facilitated enrollment organization providing application assistance. I also consent to sharing this information with any school-based health center that provides services to the applicant(s). I understand this information is being shared for the purposes of determining eligibility of those individuals applying for Child Health Plus or Medicaid or to evaluate the success of these programs. If you do NOT want any information on this application shared for purposes of making an eligibility determination for Medicaid, please check this box: I agree that any licensed doctor, hospital, or other health care provider may give my health plan information about medical services enrolled members of my family have received, as requested, and to such an extent as may be responsible and necessary for the operation and regulation of the plan. This information will be kept confidential. I understand that each person renewing/applying for Child Health Plus or Medicaid will be enrolled in the appropriate program, if eligible. I understand that if my child is found eligible for Child Health Plus, he/she will be re-enrolled in the plan listed on page one of this application. I also understand that if my child is found eligible for Medicaid instead of Child Health Plus, he/she will be enrolled in that same managed care health plan unless that health plan does not participate in Medicaid managed care. If my child s plan does not participate in Medicaid managed care, my child will be enrolled in another health plan. If my child lives in a county that does not require enrollees to be in a Medicaid managed care health plan, my child will still be enrolled in a health plan unless I notify my local social services department, in writing, that I do not want him/her to be in a plan. I have also read and understand the Terms, Rights and Responsibilities included with this form (see page 5). I certify under penalty of perjury that everything on this form is the truth as best I know Signature of the Person Listed in Section A: _ Date: REVISED CHRU6 04/12
10 SECTION F: TERMS, RIGHTS and RESPONSIBILITIES Page 5 of 6 (04/2012) By completing and signing this form, I am renewing Child Health Plus. I understand that this form, notices, and other supporting information will be sent to the program(s) for which I want to renew. I agree to the release of personal and financial information from this form and any other information needed to determine eligibility for these programs. I understand that I may be asked for more information; I agree to immediately report any changes to the information on this form. I understand that I must provide the information needed to prove eligibility for each program. If I have been unable to get the information for Medicaid, I will tell the social services district. The social services district may be able to help in getting information. I understand that workers from the programs for which family members or I have applied may check the information given by me for this form. The agencies that run these programs will keep this information confidential according to 42 U.S.C. 1396a (a) (7) and 42 CFR and any federal and state laws and regulations. By applying for CHP, I agree to pay the applicable premium contribution not paid by New York State. I understand that CHP and Medicaid will not pay medical expenses that insurance or another person is supposed to pay, and that if I am applying for Medicaid, I am giving to the Medicaid agency all of my rights to receive medical support from a spouse or parents of persons under 21 years old and my right to third party payments for the entire time I am on Medicaid. I understand that I have the right to claim good cause not to cooperate in using health insurance if its use could cause harm to my health or safety or to the health and safety of someone I am legally responsible for. I understand that my eligibility for these programs will not be affected by my race, color, or national origin. I also understand that depending on the requirements of these individual programs, my age, sex, or disability status may be a factor in whether or not I am eligible. I understand that anyone who knowingly lies or hides the truth in order to receive services under these programs is committing a crime and subject to federal and state penalties and may have to repay the amount of benefits received and pay civil penalties. The New York State Department of Tax and Finance has the right to review income information on this form. SSNs are not required to enroll in CHP. If available, I will include it for children renewing/applying for Medicaid. SSNs are not required for pregnant Medicaid applicants or non-qualified aliens. SSNs are not required for legally responsible adults or any other person residing in the Medicaid applicant's household who is not applying for Medicaid. SSNs are required for Medicaid applicants who are not pregnant. I understand that this is required by Federal law at 42 U.S.C. 1320B-7 (a) and by Medicaid regulations at 42 CFR The Medicaid agency and the CHP program will use the SSN to verify my income, eligibility and the amount of medical assistance payments made on my behalf. The information may be matched with the records in other agencies, such as the Social Security Administration, Internal Revenue Service or State Department of Taxation and Finance. I give permission to the Local Department of Social Services and New York State to obtain any information regarding the educational records of my child(ren), herein named, necessary for claiming Medicaid reimbursement for health-related educational services, and to provide the appropriate federal government agency access to this information for the sole purposes of audit. I consent to the release of any medical information about me and any members of my family for whom I can give consent: (1) by my PCP, any health care provider or the New York State Department of Health (SDOH) to my health plan and any health care providers involved in caring for me or my family, as reasonably necessary for my health plan or my providers to carry out treatment, payment or health care operations; (2) by health plan and any health care providers to SDOH and other authorized federal, state and local agencies for purposes of administration of Medicaid, Child Health Plus and Family Health Plus programs; and (3) by my health plan to other persons or organizations, as reasonably necessary for my health plan to carry out treatment, payment or health care operations. I also agree that the information released may include HIV, mental health or alcohol and substance abuse information about me and members of my family, to the extent permitted by law. FOR OFFICE USE ONLY To be completed by the person assisting with the application. Signature of Person who Obtained Eligibility Information: Employed By: Health Plan Social Services District Provider Agency Community-Based Facilitated Enrolment Agency. Specify: To be completed by Facilitated Enrollers: Facilitated Enroller Name: Lead Agency: Lead Org. ID: Application Start Date (mm/dd/yy): Application Sequence Number: Application Completion Date (mm/dd/yy): Enter Code of Applying Child(ren): Medicaid CHP REVISED CHRU7 04/12
11 SECTION G: DOCUMENTATION Page 6 of 6 (04/2012) Proof of Household Income: If you do not provide your SSN, you must provide ONE proof for each type of income you have. The proof must be dated and received within the last four weeks of the application signature date, whether you get paid weekly, bi-weekly, or monthly. Wages and Salary Paycheck stubs (4 consecutive weeks) Signed and dated letter from employer on company letterhead with phone # Current signed and dated income tax return and all schedules* Business/payroll records Self-Employment Current signed and dated income tax return and all schedules* Records of earnings and expenses/business records Unemployment Benefits Award letter/certificate Monthly benefit statement from the NYS Department of Labor Print out of the recipients account information from the NYS Department of Labor s website - A copy of the direct payment card with printout Correspondence from NYS Department of Labor Social Security Award letter/certificate Annual benefit statement Correspondence from Social Security Administration Child Support/Alimony Letter from person providing support that is signed, dated, and gives contact information Letter from court Child support/alimony check stub A copy of the New York Eppicard with printout A copy of the child support account information from the following website Copy of the bank statement showing direct deposit Income from Rent or Room/Board Letter from roomer, boarder, tenant Check stub Interest/Dividends or Royalties Recent statement from bank, credit union, or financial institution Letter from broker or agent 1099 or tax return (if no other documentation is available) Support from other Family Members Statement or letter from family member that is signed, dated, and gives contact information Military Pay * Income tax Award letter or Check stub returns for other Veteran s Benefits than self employed Award letter or Benefit check stub must be for Correspondence from Veterans Administration applications prior to Private Pension/Annuities April of the Statement from pension/annuity following year. Worker s Compensation Award letter or Check stub CHRU08 04/12 Proof of Pregnancy (Provide one of the following): Presumptive Eligibility Screening Worksheet completed by Qualified Provider that gives your expected date of delivery Statement from Medical Professional with expected date of delivery WIC Medical Referral Form that gives your expected date of delivery Proof of Other Health Insurance (Provide all that apply): Premium Insurance Policy Certificate of Insurance Insurance Card Proof of Identity, U.S. Citizenship and/or Immigration Status: You are only required to provide proof of your child s citizenship or immigration status if there was a change since last year. The United States Citizenship and Immigration Services (USCIS) has said that enrollment in CHPlus CANNOT affect your child's ability to get a green card, become a citizen, sponsor a family member or travel in and out of the country. The state will not report any of the information on this form to the USCIS. Provide ONE of the following documents to prove both Citizenship, Identity, and your Date of Birth: U.S. Passport Book/Card OR Certificate of Naturalization (DHS Forms N-550 or N-570) OR Certificate of US Citizenship (DHS Forms N-560 or N-561) OR NYS Enhanced Driver s License (EDL). If one of the above documents is not available, you must provide ONE document from EACH LIST - Citizenship AND Identity: Citizenship U.S. Birth Certificate* Certificate of Birth Abroad (Form FS-545)* Native American Tribal Document* Certificate of Report of Birth (Form DS-1350)* U.S. National ID Card (Form I-197 or I-179) Religious/School Records* Official military record of service showing US Place of Birth Evidence of qualifying for U.S. citizenship under the Child Citizenship Act of 2000 Final adoption decree Identity State Driver s license or ID card with photo* ID card issued by a federal, state, or local government agency U.S. Military card or draft record or U.S. Coast Guard Merchant Mariner Card School ID card with a photo Verified School, Nursery or Daycare records (for children under 16) Clinic, Doctor or Hospital records (for children under 16)* Certificate of Degree of Indian blood or other Native American/Alaska native tribal document with photo These lists are not all inclusive. Documents with a * next to it also show Date of Birth. If you are not a U.S. Citizen: The list below contains some of the most common United States Citizenship and Immigration Services (USCIS) forms used to show your immigration status. This list is not all inclusive. If you do not have one of these documents, please call: Immigration Status You can use ONE of the following documents to prove both Immigration Status, Identity and Date of Birth: I-551 Permanent Resident Card ( Green Card ) I-688B or I-766 Employment Authorization Card Other documents that may show your Immigration Status, but require an additional Identity document are: I-94 Arrival/Departure Record* USCIS Form I-797 Notice of Action Evidence of Continuous U.S. Residence prior to 1/1/1972. Family Premium Contribution: There may be a monthly premium for Child Health Plus. If you are required to pay a premium, one month s payment must be submitted with this form. There are no premiums for Medicaid. To determine if you need to pay a premium based on your family s monthly income and household size, use the attached table. If you need help understanding your expected CHPlus premium, call or The full premium varies, depending upon the health plan you choose. Income eligibility levels change at least annually. You may contact your CHPlus plan or visit NY State Department of Health s website at for an updated premium and income eligibility table.
Health Insurance APPLICATION. for Children, Adults and Families
 Health Insurance APPLICATION for Children, Adults and Families INSTRUCTIONS CONFIDENTIALITY STATEMENT All of the information you provide on this application will remain confidential. The only people who
Health Insurance APPLICATION for Children, Adults and Families INSTRUCTIONS CONFIDENTIALITY STATEMENT All of the information you provide on this application will remain confidential. The only people who
APPLICATION PACKET. Please read pages 1 through 6 for some important things you ll need to know before you apply.
 DEPARTMENT OF HEALTH AND FAMILY SERVICES Division of Health Care Access and Accountability HCF 10182 (02/08) STATE OF WISCONSIN APPLICATION PACKET Please read pages 1 through 6 for some important things
DEPARTMENT OF HEALTH AND FAMILY SERVICES Division of Health Care Access and Accountability HCF 10182 (02/08) STATE OF WISCONSIN APPLICATION PACKET Please read pages 1 through 6 for some important things
Health Care Coverage APPLICATION FOR. Health Care in Pennsylvania. Easy, affordable protection for your family
 Important information about health care benefits. Ask someone to read this to you. APPLICATION FOR Health Care Coverage This application may be used by families with children or by pregnant women who apply
Important information about health care benefits. Ask someone to read this to you. APPLICATION FOR Health Care Coverage This application may be used by families with children or by pregnant women who apply
P E N N S Y L V A N I A Application for Payment of Medicare Premiums, Coinsurance and Deductibles
 P E N N S Y L V A N I A Application for Payment of Medicare Premiums, Coinsurance and Deductibles If you have a disability and need this form in large print or another format, please call our helpline
P E N N S Y L V A N I A Application for Payment of Medicare Premiums, Coinsurance and Deductibles If you have a disability and need this form in large print or another format, please call our helpline
Medicaid. Medicaid SOBRA. ALL Kids. for Low Income Families. Insurance. The Alabama Child Caring. Foundation
 Medicaid for Low Income Families ALL Kids Insurance SOBRA Medicaid The Alabama Child Caring Foundation THIS IS YOUR APPLICATION for free or low cost health care coverage. These programs cover low income
Medicaid for Low Income Families ALL Kids Insurance SOBRA Medicaid The Alabama Child Caring Foundation THIS IS YOUR APPLICATION for free or low cost health care coverage. These programs cover low income
What is CoverKids? $28,725 $38,775 $48,825 $58,875 $68,925 $78,975 $89,025 $99,075 $109,125 $119,175
 What is CoverKids? CoverKids is full health coverage for children and pregnant women who cannot afford employer sponsored insurance or individual insurance and who make too much to be eligible for TennCare.
What is CoverKids? CoverKids is full health coverage for children and pregnant women who cannot afford employer sponsored insurance or individual insurance and who make too much to be eligible for TennCare.
Massachusetts Application for Health and Dental Coverage and Help Paying Costs
 Massachusetts Application for Health and Dental Coverage and Help Paying Costs HOW TO APPLY USE THIS APPLICATION TO SEE WHAT COVERAGE CHOICES YOU MAY QUALIFY FOR. WHO CAN USE THIS APPLICATION? You can
Massachusetts Application for Health and Dental Coverage and Help Paying Costs HOW TO APPLY USE THIS APPLICATION TO SEE WHAT COVERAGE CHOICES YOU MAY QUALIFY FOR. WHO CAN USE THIS APPLICATION? You can
Application for Health Coverage and Help Paying Costs
 Iowa Department of Human Services Application for Health Coverage and Help Paying Costs Use this application to see what coverage choices you qualify for Affordable private health insurance plans that
Iowa Department of Human Services Application for Health Coverage and Help Paying Costs Use this application to see what coverage choices you qualify for Affordable private health insurance plans that
Application for Medical Assistance for the Elderly and Persons with Disabilities
 Application for Medical Assistance for the Elderly and Persons with Disabilities KC1500 Who can use this application? Apply faster online This application is for the elderly and persons with disabilities
Application for Medical Assistance for the Elderly and Persons with Disabilities KC1500 Who can use this application? Apply faster online This application is for the elderly and persons with disabilities
Application for Benefits Medicaid Buy-In for Children
 Texas Health and Human Services Commission Form H1200-MBIC Cover Letter January 2011 Application for Benefits Medicaid Buy-In for Children About this program: Medicaid Buy-In for Children can help pay
Texas Health and Human Services Commission Form H1200-MBIC Cover Letter January 2011 Application for Benefits Medicaid Buy-In for Children About this program: Medicaid Buy-In for Children can help pay
Application for Lifeline Telephone Service
 Important Lifeline Information Lifeline is a service and a government assistance program designed to make phone and internet services more affordable for low-income customers. Assistance is provided in
Important Lifeline Information Lifeline is a service and a government assistance program designed to make phone and internet services more affordable for low-income customers. Assistance is provided in
OTSEGO COUNTY DEPARTMENT OF SOCIAL SERVICES DOCUMENTATION REQUIREMENTS
 - 1 - OTSEGO COUNTY DEPARTMENT OF SOCIAL SERVICES DOCUMENTATION REQUIREMENTS THIS CHART IS A GUIDE ONLY BE SURE TO PROGRAMS ABBREVIATIONS REVIEW ALL 5 PAGES OF INFORMATION TA=Temporary Assistance X Required
- 1 - OTSEGO COUNTY DEPARTMENT OF SOCIAL SERVICES DOCUMENTATION REQUIREMENTS THIS CHART IS A GUIDE ONLY BE SURE TO PROGRAMS ABBREVIATIONS REVIEW ALL 5 PAGES OF INFORMATION TA=Temporary Assistance X Required
SUPPLEMENTAL INFORMATION. Spouse Information Form
 SUPPLEMENTAL INFORMATION Spouse Information Form NJ FamilyCare Aged, Blind, Disabled Programs SECTION 1 Applicant 2 (Spouse) STATE of NEW JERSEY Department of Human Services Division of Medical Assistance
SUPPLEMENTAL INFORMATION Spouse Information Form NJ FamilyCare Aged, Blind, Disabled Programs SECTION 1 Applicant 2 (Spouse) STATE of NEW JERSEY Department of Human Services Division of Medical Assistance
Rights and Responsibilities
 Welcome to the Georgia Division of Family and Children Services! If you need help filling out this application, ask us or call 1-877-423-4746. If you are deaf or hard of hearing, please call GA Relay at
Welcome to the Georgia Division of Family and Children Services! If you need help filling out this application, ask us or call 1-877-423-4746. If you are deaf or hard of hearing, please call GA Relay at
Health Coverage & Help Paying Costs Application for One Person
 THINGS TO KNOW Health Coverage & Help Paying Costs Application for One Person Use this application to see what insurance choices you qualify for Free or low-cost insurance from Medicaid or the Kentucky
THINGS TO KNOW Health Coverage & Help Paying Costs Application for One Person Use this application to see what insurance choices you qualify for Free or low-cost insurance from Medicaid or the Kentucky
Family-Related Medical Assistance Application
 Family-Related Medical Assistance Application Form Approved DCF. CF-ES 2370, Dec 2013 things to know Use this application to see what coverage choices you qualify for Free or low-cost insurance from Medicaid
Family-Related Medical Assistance Application Form Approved DCF. CF-ES 2370, Dec 2013 things to know Use this application to see what coverage choices you qualify for Free or low-cost insurance from Medicaid
Mail-In Application for Medical Benefits (Esta solicitud está disponible en español.) (This application is available in Spanish.)
 (This application is available in Spanish.)") Illinois Department of Human Services Illinois Department of Healthcare and Family Services Mail-In Application for Medical Benefits (Esta solicitud está disponible en español.) (This application is available
Illinois Department of Human Services Illinois Department of Healthcare and Family Services Mail-In Application for Medical Benefits (Esta solicitud está disponible en español.) (This application is available
Application for Health Coverage & Help Paying Costs
 Application for Health Coverage & Help Paying Costs Use this application to see what coverage choices you qualify for Affordable private health insurance plans that offer comprehensive coverage to help
Application for Health Coverage & Help Paying Costs Use this application to see what coverage choices you qualify for Affordable private health insurance plans that offer comprehensive coverage to help
Application for Health Coverage and Help Paying Costs Instructions
 Application for Health Coverage and Help Paying Costs Instructions Commonwealth of Massachusetts EOHHS Please read these instructions before you fill out the application. Apply faster online! Go to: MAhealthconnector.org.
Application for Health Coverage and Help Paying Costs Instructions Commonwealth of Massachusetts EOHHS Please read these instructions before you fill out the application. Apply faster online! Go to: MAhealthconnector.org.
OMB APPROVAL EDITION What is a household? Be honest on this form. You may need to show other documents
 1. About Lifeline Lifeline is a federal benefit that lowers the monthly cost of phone or internet service. Rules If you qualify, your household can get Lifeline for phone or internet service, but not both.
1. About Lifeline Lifeline is a federal benefit that lowers the monthly cost of phone or internet service. Rules If you qualify, your household can get Lifeline for phone or internet service, but not both.
DELAWARE CHILDREN S CARE PLAN
 DELAWARE CHILDREN S CARE PLAN About DCCP Available through Highmark Blue Cross Blue Shield Delaware (Highmark Delaware), the Delaware Children s Care Plan (DCCP) provides comprehensive health benefits
DELAWARE CHILDREN S CARE PLAN About DCCP Available through Highmark Blue Cross Blue Shield Delaware (Highmark Delaware), the Delaware Children s Care Plan (DCCP) provides comprehensive health benefits
MAYOR BYRON W. BROWN S SUMMER YOUTH INTERNSHIP PROGRAM APPLICATION
 MAYOR BYRON W. BROWN S SUMMER YOUTH INTERNSHIP PROGRAM February 1, 2018 Dear Applicant: Thank you for your interest in applying for my 2018 Summer Youth Internship Program. This is truly a wonderful opportunity
MAYOR BYRON W. BROWN S SUMMER YOUTH INTERNSHIP PROGRAM February 1, 2018 Dear Applicant: Thank you for your interest in applying for my 2018 Summer Youth Internship Program. This is truly a wonderful opportunity
Children s National Financial Assistance Application
 Children s National Financial Assistance Application Children s National will offer financial assistance to patients who are unable to pay their hospital and/or clinic bills due to difficult financial
Children s National Financial Assistance Application Children s National will offer financial assistance to patients who are unable to pay their hospital and/or clinic bills due to difficult financial
Brookings School District. = = = = = Dear Parent/Guardian:
 Brookings School District = = = = = Dear Parent/Guardian: Children need healthy meals to learn. The Brookings School District offers healthy meals every day that it is open USDA provides reimbursement
Brookings School District = = = = = Dear Parent/Guardian: Children need healthy meals to learn. The Brookings School District offers healthy meals every day that it is open USDA provides reimbursement
Nebraska Ryan White Program
 For office use only: Date Received: MR#: Nebraska Ryan White Program Application Information Date: Check all the programs applying for: Part B Part C Part D ADAP ADAP co-payment assistance Wait list If
For office use only: Date Received: MR#: Nebraska Ryan White Program Application Information Date: Check all the programs applying for: Part B Part C Part D ADAP ADAP co-payment assistance Wait list If
If you have questions about how much your fee will be, you may stop by or call with your income information before your appointment.
 238 Arsenal Street, Watertown, NY Family Practice Office: (315) 782-6400 Fax: (315) 782-1330 Adult Office: (315) 782-9903 Fax: (315) 788-0087 Dental Office: (315) 788-9834 Fax: (315) 788-5456 7785 N. State
238 Arsenal Street, Watertown, NY Family Practice Office: (315) 782-6400 Fax: (315) 782-1330 Adult Office: (315) 782-9903 Fax: (315) 788-0087 Dental Office: (315) 788-9834 Fax: (315) 788-5456 7785 N. State
If you have any questions prior to mailing or bringing your application in, please feel free to contact our department at
 NJ Hospital Care Assistance Program(NJHCAPS) NJ Hospital Care Assistance Program (formerly known as Charity Care) is available to every patient regardless of whether they are insured or not. Each patient
NJ Hospital Care Assistance Program(NJHCAPS) NJ Hospital Care Assistance Program (formerly known as Charity Care) is available to every patient regardless of whether they are insured or not. Each patient
Start Overview What You Need to Know When You Apply Former Foster Care Youth (FFCY)
") Start Overview What You Need to Know When You Apply Social Security numbers (SSNs) for applicants who are U.S. citizens. Lawfully present immigrants will also need document information if they are applying
Start Overview What You Need to Know When You Apply Social Security numbers (SSNs) for applicants who are U.S. citizens. Lawfully present immigrants will also need document information if they are applying
EMPLOYEE INFORMATION SHEET
 EMPLOYEE INFORMATION SHEET PLEASE PRINT CLEARLY COMPANY: EMPLOYEE #: SOCIAL SECURITY NUMBER: - - NAME: First MI LAST STREET: CITY: AS APPEARS ON SOCIAL SECURITY CARD STATE: ZIP CODE: TELEPHONE NUMBER:
EMPLOYEE INFORMATION SHEET PLEASE PRINT CLEARLY COMPANY: EMPLOYEE #: SOCIAL SECURITY NUMBER: - - NAME: First MI LAST STREET: CITY: AS APPEARS ON SOCIAL SECURITY CARD STATE: ZIP CODE: TELEPHONE NUMBER:
Eligibility Checklist
 Eligibility Checklist Patient s Name: of Service: /_/ Medical Record #: _ Account Number: _ You are encouraged to apply one week prior to any appointments with proof of appointment and/or referral. In
Eligibility Checklist Patient s Name: of Service: /_/ Medical Record #: _ Account Number: _ You are encouraged to apply one week prior to any appointments with proof of appointment and/or referral. In
Application for Health Coverage & Help Paying Costs
 04.24.13 Application for Health Coverage & Help Paying Costs Use this application to see what coverage choices you qualify for Affordable private health insurance plans that offer comprehensive coverage
04.24.13 Application for Health Coverage & Help Paying Costs Use this application to see what coverage choices you qualify for Affordable private health insurance plans that offer comprehensive coverage
Application for Health Coverage & Help Paying Costs
 Application for Health Coverage & Help Paying Costs Form Approved OMB. 0938-1191 Use this application to see what coverage choices you qualify for Affordable private health insurance plans that offer comprehensive
Application for Health Coverage & Help Paying Costs Form Approved OMB. 0938-1191 Use this application to see what coverage choices you qualify for Affordable private health insurance plans that offer comprehensive
PATIENT REGISTRATION FORM
 Patient Information PATIENT REGISTRATION FORM (Name) First: M.I. Last: Address: City: State: Zip: D.O.B. Email: (Phones) Home: Cell: Work: Fill out both above and below section with patient information,
Patient Information PATIENT REGISTRATION FORM (Name) First: M.I. Last: Address: City: State: Zip: D.O.B. Email: (Phones) Home: Cell: Work: Fill out both above and below section with patient information,
OMB APPROVAL EDITION What is a household? Be honest on this form. You may need to show other documents
 FCC FORM 5629 1. About Lifeline Lifeline is a federal benefit that lowers the monthly cost of phone or internet service. Rules If you qualify, your household can get Lifeline for phone or internet service,
FCC FORM 5629 1. About Lifeline Lifeline is a federal benefit that lowers the monthly cost of phone or internet service. Rules If you qualify, your household can get Lifeline for phone or internet service,
Free and Reduced Price School Meals Information Letter to Households
 Free and Reduced Price School Meals Information Letter to Households Dear Parent/Guardian: Children need healthy meals to learn. Woodland Park School District offers healthy meals every school day. Student
Free and Reduced Price School Meals Information Letter to Households Dear Parent/Guardian: Children need healthy meals to learn. Woodland Park School District offers healthy meals every school day. Student
OMB APPROVAL EDITION What is a household? Be honest on this form. You may need to show other documents
 1. About Lifeline Lifeline is a federal benefit that lowers the monthly cost of phone or internet service. Rules If you qualify, your household can get Lifeline for phone or internet service, but not both.
1. About Lifeline Lifeline is a federal benefit that lowers the monthly cost of phone or internet service. Rules If you qualify, your household can get Lifeline for phone or internet service, but not both.
Southeast ID#: Name: SSN: PREVIOUS CIVIL OR COLLEGE DISCIPLINE
 /Student Employment Work Referral Southeast ID#: Name: SSN: STUDENT EMPLOYEE ELIGIBILITY AND RESPONSIBILITIES 1. You must complete, and have on file with Student Financial Services, employment eligibility
/Student Employment Work Referral Southeast ID#: Name: SSN: STUDENT EMPLOYEE ELIGIBILITY AND RESPONSIBILITIES 1. You must complete, and have on file with Student Financial Services, employment eligibility
Low-Income Telephone and Electric Discount Programs (LITE-UP) Enrollment Form
 Enrollment Form") Low-Income Telephone and Electric Discount Programs (LITE-UP) Enrollment Form The LITE-UP Texas Program can: 1. Provide a discount off your monthly telephone bill. 2. Provide a discount on your electric
Low-Income Telephone and Electric Discount Programs (LITE-UP) Enrollment Form The LITE-UP Texas Program can: 1. Provide a discount off your monthly telephone bill. 2. Provide a discount on your electric
Montana State University MESA Program POTENTIAL PARTICIPANT APPLICATION FORM
 Montana State University MESA Program POTENTIAL PARTICIPANT APPLICATION FORM Date: / / To ensure you qualify for the Matched Education Savings Account (MESA) Program, please read the MESA Frequently Asked
Montana State University MESA Program POTENTIAL PARTICIPANT APPLICATION FORM Date: / / To ensure you qualify for the Matched Education Savings Account (MESA) Program, please read the MESA Frequently Asked
Energy Assistance Attachment Checklist
 Energy Assistance Attachment Checklist Applicant ame: Completed Application, including signature and date on page 4 Signed Release of Information Copy of Current Utility Bill Identification for Bill Holder
Energy Assistance Attachment Checklist Applicant ame: Completed Application, including signature and date on page 4 Signed Release of Information Copy of Current Utility Bill Identification for Bill Holder
Employment Eligibility Verification
 Employment Eligibility Verification Department of Homeland Security U.S. Citizenship and Immigration Services USCIS Form I-9 OMB No. 1615-0047 Expires 08/31/2019 START HERE: Read instructions carefully
Employment Eligibility Verification Department of Homeland Security U.S. Citizenship and Immigration Services USCIS Form I-9 OMB No. 1615-0047 Expires 08/31/2019 START HERE: Read instructions carefully
OMB APPROVAL EDITION What is a household? Be honest on this form. You may need to show other documents
 1. About Lifeline Lifeline is a federal benefit that lowers the monthly cost of phone or internet service. Rules If you qualify, your household can get Lifeline for phone or internet service, but not both.
1. About Lifeline Lifeline is a federal benefit that lowers the monthly cost of phone or internet service. Rules If you qualify, your household can get Lifeline for phone or internet service, but not both.
Health Care Renewal Notice
 xxxxxxx * xxxxxxx xxxxxxx xxxxxxx Oct 15, 2017 5:12 PM Health Care Renewal Notice You are getting this notice because it is time to renew coverage for members of your household. This notice tells you the
xxxxxxx * xxxxxxx xxxxxxx xxxxxxx Oct 15, 2017 5:12 PM Health Care Renewal Notice You are getting this notice because it is time to renew coverage for members of your household. This notice tells you the
FREQUENTLY ASKED QUESTIONS ABOUT FREE AND REDUCED-PRICE SCHOOL MEALS. FEDERAL ELIGIBILITY INCOME CHART for School Year: 2017
 FREQUENTLY ASKED QUESTIONS ABOUT FREE AND REDUCED-PRICE SCHOOL MEALS Dear Parent/Guardian: Children need healthy meals to learn. Marietta Public School offers healthy meals every school day. Breakfast
FREQUENTLY ASKED QUESTIONS ABOUT FREE AND REDUCED-PRICE SCHOOL MEALS Dear Parent/Guardian: Children need healthy meals to learn. Marietta Public School offers healthy meals every school day. Breakfast
Application for Energy Assistance
 Office Location: 194 Alimaq Drive Mailing Address: 3449 Rezanof Drive East, Kodiak AK 99615 Phone: (907) 486-9879 Fax: (907) 486-4829 Email: ETSS@kodiakhealthcare.org What is LIHEAP? The Low Income Home
Office Location: 194 Alimaq Drive Mailing Address: 3449 Rezanof Drive East, Kodiak AK 99615 Phone: (907) 486-9879 Fax: (907) 486-4829 Email: ETSS@kodiakhealthcare.org What is LIHEAP? The Low Income Home
Application for Healthy Indiana Plan State Form (R4/12-10) HIP 2515
 HIP 2515") *DFRIHEE01* *This agency is requesting the disclosure of your Social Security Number in accordance with IC 4-1-8-1; disclosure is mandatory and this record cannot be processed without it. Instructions:
*DFRIHEE01* *This agency is requesting the disclosure of your Social Security Number in accordance with IC 4-1-8-1; disclosure is mandatory and this record cannot be processed without it. Instructions:
Massachusetts Application for Health and Dental Coverage and Help Paying Costs
 Massachusetts Application for Health and Dental Coverage and Help Paying Costs Commonwealth of Massachusetts EOHHS THINGS TO KNOW HOW TO APPLY Use this application to see what coverage choices you may
Massachusetts Application for Health and Dental Coverage and Help Paying Costs Commonwealth of Massachusetts EOHHS THINGS TO KNOW HOW TO APPLY Use this application to see what coverage choices you may
FREQUENTLY ASKED QUESTIONS ABOUT FREE AND REDUCED-PRICE SCHOOL MEALS
 FREQUENTLY ASKED QUESTIONS ABOUT FREE AND REDUCED-PRICE SCHOOL MEALS Dear Parent/Guardian: Children need healthy meals to learn. (Name of School/School District) offers healthy meals every school day.
FREQUENTLY ASKED QUESTIONS ABOUT FREE AND REDUCED-PRICE SCHOOL MEALS Dear Parent/Guardian: Children need healthy meals to learn. (Name of School/School District) offers healthy meals every school day.
Last Name First Name Middle. Address Number & Street City State Zip Code. Date of Birth Applicant Co-applicant / / / / Month Day Year Month Day Year
 PARKVIEW APARTMENTS HOUSING APPLICATION Mr. Ms. Miss Date: Mrs. Mr. & Mrs. Last Name First Name Middle Address Number & Street City State Zip Code ( ) ( ) Home Phone Number Alternate Contact Number How
PARKVIEW APARTMENTS HOUSING APPLICATION Mr. Ms. Miss Date: Mrs. Mr. & Mrs. Last Name First Name Middle Address Number & Street City State Zip Code ( ) ( ) Home Phone Number Alternate Contact Number How
Housing Assistance Application Check Sheet
 Housing Assistance Application Check Sheet In order to determine eligibility, the following items are required for all household members: [ ] Application update required annually [ ] Degree of Indian Blood-copy
Housing Assistance Application Check Sheet In order to determine eligibility, the following items are required for all household members: [ ] Application update required annually [ ] Degree of Indian Blood-copy
If your monthly household income meets the guidelines below, we invite you to apply:
 Bringing energy affordability to Michigan. Thank you for your interest in applying for the Consumers Energy CARE Program. CARE is a 2-year affordable payment plan for income-qualified customers of Consumers
Bringing energy affordability to Michigan. Thank you for your interest in applying for the Consumers Energy CARE Program. CARE is a 2-year affordable payment plan for income-qualified customers of Consumers
HCR FAQ. Covered California Individual and Family Coverage. What is Covered California? What is Obamacare? Are they the same?
 HCR FAQ Covered California Individual and Family Coverage What is Covered California? What is Obamacare? Are they the same? Covered California is a new, easy-to-use marketplace established for California
HCR FAQ Covered California Individual and Family Coverage What is Covered California? What is Obamacare? Are they the same? Covered California is a new, easy-to-use marketplace established for California
DO NOT WRITE BELOW THIS LINE FOR SCHOOL USE ONLY
 Date Withdrew Attachment Va F R D 2018-2019 Application for Free and Reduced Price School Meals/Milk To apply for free and reduced price meals for your children, read the instructions on the back, complete
Date Withdrew Attachment Va F R D 2018-2019 Application for Free and Reduced Price School Meals/Milk To apply for free and reduced price meals for your children, read the instructions on the back, complete
Rights and Responsibilities
 Georgia Department of Human Services Rights and Responsibilities Welcome to the Georgia Division of Family and Children Services! We are giving you this information to help you understand your rights and
Georgia Department of Human Services Rights and Responsibilities Welcome to the Georgia Division of Family and Children Services! We are giving you this information to help you understand your rights and
OMB APPROVAL EDITION What is a household? Be honest on this form. You may need to show other documents
 1. About Lifeline Lifeline is a federal benefit that lowers the monthly cost of phone or internet service. Rules If you qualify, your household can get Lifeline for phone or internet service, but not both.
1. About Lifeline Lifeline is a federal benefit that lowers the monthly cost of phone or internet service. Rules If you qualify, your household can get Lifeline for phone or internet service, but not both.
HAWAII COUNTY ECONOMIC OPPORTUNITY COUNCIL
 HAWAII COUNTY ECONOMIC OPPORTUNITY COUNCIL 47 Rainbow Drive Hilo, Hawaii 96720-2013 Sheree Maldonado (MWF 8:30-3:30 PM) Email: smaldonado@hceoc.net 932-2711 FAX: 961-2812 ENERGY CRISIS INTERVENTION (ECI)
HAWAII COUNTY ECONOMIC OPPORTUNITY COUNCIL 47 Rainbow Drive Hilo, Hawaii 96720-2013 Sheree Maldonado (MWF 8:30-3:30 PM) Email: smaldonado@hceoc.net 932-2711 FAX: 961-2812 ENERGY CRISIS INTERVENTION (ECI)
Virginia Individual Development Accounts Candidate Application
 Virginia Individual Development Accounts Candidate Application VIDA candidates must use this application to show that they meet the five criteria below. This form is also used to establish a VIDA savings
Virginia Individual Development Accounts Candidate Application VIDA candidates must use this application to show that they meet the five criteria below. This form is also used to establish a VIDA savings
OMB APPROVAL EDITION What is a household? Be honest on this form. You may need to show other documents
 1. About Lifeline Lifeline is a federal benefit that lowers the monthly cost of phone or internet service. Rules If you qualify, your household can get Lifeline for phone or internet service, but not both.
1. About Lifeline Lifeline is a federal benefit that lowers the monthly cost of phone or internet service. Rules If you qualify, your household can get Lifeline for phone or internet service, but not both.
Employment Eligibility Verification
 Employment Eligibility Verification Department of Homeland Security U.S. Citizenship and Immigration Services USCIS Form I-9 OMB No. 1615-0047 Expires 08/31/2019 START HERE: Read instructions carefully
Employment Eligibility Verification Department of Homeland Security U.S. Citizenship and Immigration Services USCIS Form I-9 OMB No. 1615-0047 Expires 08/31/2019 START HERE: Read instructions carefully
Application for health care coverage
 www.chipcoverspakids.com Keystone Health Plan East HMO Health Coverage Provided to Eligible Children Application for health care coverage If you would like a copy of this application in Spanish, please
www.chipcoverspakids.com Keystone Health Plan East HMO Health Coverage Provided to Eligible Children Application for health care coverage If you would like a copy of this application in Spanish, please
Free and Reduced Price School Breakfast & Lunch
 ROSLYN UNION FREE SCHOOL DISTRICT BOX 367 ROSLYN, NEW YORK 11576 Free and Reduced Price School Breakfast & Lunch Information & Application 2017-2018 August 2017 Dear Parent/Guardian: The Roslyn Union Free
ROSLYN UNION FREE SCHOOL DISTRICT BOX 367 ROSLYN, NEW YORK 11576 Free and Reduced Price School Breakfast & Lunch Information & Application 2017-2018 August 2017 Dear Parent/Guardian: The Roslyn Union Free
Separate here and give Form W-4 to your employer. Keep the top part for your records. Employee s Withholding Allowance Certificate
 Form W-4 (2017) Purpose. Complete Form W-4 so that your employer can withhold the correct federal income tax from your pay. Consider completing a new Form W-4 each year and when your personal or financial
Form W-4 (2017) Purpose. Complete Form W-4 so that your employer can withhold the correct federal income tax from your pay. Consider completing a new Form W-4 each year and when your personal or financial
Request for Benefits. For use with Forms 08MP002E and 08MP003E
 *PS1 * Date: Case name: Case number: County number. Supervisor/worker number: / Request for Benefits For use with Forms 08MP002E and 08MP003E What you need to do to get started: Read the following descriptions
*PS1 * Date: Case name: Case number: County number. Supervisor/worker number: / Request for Benefits For use with Forms 08MP002E and 08MP003E What you need to do to get started: Read the following descriptions
Letter to Parents for School Meal Programs
 Letter to Parents for School Meal Programs Dear Parent/Guardian: Children need healthy meals to learn. Dundee CSD offers healthy meals every school day. Breakfast costs $1.75; Lunch costs $2.05 Grades
Letter to Parents for School Meal Programs Dear Parent/Guardian: Children need healthy meals to learn. Dundee CSD offers healthy meals every school day. Breakfast costs $1.75; Lunch costs $2.05 Grades
Your Texas Benefits: Getting Started
 Your Texas Benefits: Getting Started SNAP Food Benefits (This used to be called Food Stamps.) Helps buy food for good health. Some people might get help the next work day. TANF Cash Help for Families TANF:
Your Texas Benefits: Getting Started SNAP Food Benefits (This used to be called Food Stamps.) Helps buy food for good health. Some people might get help the next work day. TANF Cash Help for Families TANF:
Application Adult & Dislocated Worker Programs
 Application Adult & Dislocated Worker Programs Workforce Innovation and Opportunity Act (WIOA) FORM WIOA I-B 1.1 For Adult and Dislocated Worker Programs If you are age 18 or older and need help in obtaining
Application Adult & Dislocated Worker Programs Workforce Innovation and Opportunity Act (WIOA) FORM WIOA I-B 1.1 For Adult and Dislocated Worker Programs If you are age 18 or older and need help in obtaining
FREQUENTLY ASKED QUESTIONS ABOUT FREE AND REDUCED PRICE SCHOOL MEALS FOR SCHOOL YEAR
 FREQUENTLY ASKED QUESTIONS ABOUT FREE AND REDUCED PRICE SCHOOL MEALS FOR SCHOOL YEAR 2018 19 Dear Parent/Guardian: Children need healthy meals to learn. Fennimore Community Schools offers healthy meals
FREQUENTLY ASKED QUESTIONS ABOUT FREE AND REDUCED PRICE SCHOOL MEALS FOR SCHOOL YEAR 2018 19 Dear Parent/Guardian: Children need healthy meals to learn. Fennimore Community Schools offers healthy meals
FREQUENTLY ASKED QUESTIONS ABOUT FREE AND REDUCED-PRICE SCHOOL MEALS. FEDERAL ELIGIBILITY INCOME CHART for School Year: 2019
 FREQUENTLY ASKED QUESTIONS ABOUT FREE AND REDUCED-PRICE SCHOOL MEALS Dear Parent/Guardian: Children need healthy meals to learn Crescent Public Schools offers healthy meals every school day. Breakfast
FREQUENTLY ASKED QUESTIONS ABOUT FREE AND REDUCED-PRICE SCHOOL MEALS Dear Parent/Guardian: Children need healthy meals to learn Crescent Public Schools offers healthy meals every school day. Breakfast
FREQUENTLY ASKED QUESTIONS ABOUT FREE AND REDUCED-PRICE SCHOOL MEALS. FEDERAL ELIGIBILITY INCOME CHART for School Year: 2018
 FREQUENTLY ASKED QUESTIONS ABOUT FREE AND REDUCED-PRICE SCHOOL MEALS Dear Parent/Guardian: Children need healthy meals to learn. Name of School/School District offers healthy meals every school day. Breakfast
FREQUENTLY ASKED QUESTIONS ABOUT FREE AND REDUCED-PRICE SCHOOL MEALS Dear Parent/Guardian: Children need healthy meals to learn. Name of School/School District offers healthy meals every school day. Breakfast
YANKTON SCHOOL DISTRICT APPLICATION FOR FREE AND REDUCED PRICE SCHOOL MEALS
 YANKTON SCHOOL DISTRICT 63-3 2017-2018 APPLICATION FOR FREE AND REDUCED PRICE SCHOOL MEALS Dear Parent/Guardian: Children need healthy meals to learn. The Yankton School District 63-3 offers healthy meals
YANKTON SCHOOL DISTRICT 63-3 2017-2018 APPLICATION FOR FREE AND REDUCED PRICE SCHOOL MEALS Dear Parent/Guardian: Children need healthy meals to learn. The Yankton School District 63-3 offers healthy meals
Draft Not for Reproduction 05/18/2016
 Instructions for Request for Reduced Fee Department of Homeland Security U.S. Citizenship and Immigration Services USCIS Form I-942 OMB No. 1615-0116 Expires 05/31/2015 What Is the Purpose of Form I-942?
Instructions for Request for Reduced Fee Department of Homeland Security U.S. Citizenship and Immigration Services USCIS Form I-942 OMB No. 1615-0116 Expires 05/31/2015 What Is the Purpose of Form I-942?
FREQUENTLY ASKED QUESTIONS ABOUT FREE AND REDUCED PRICE SCHOOL MEALS
 FREQUENTLY ASKED QUESTIONS ABOUT FREE AND REDUCED PRICE SCHOOL MEALS Dear Parent/Guardian: Children need healthy meals to learn. Rogers School District offers healthy meals every school day. Your children
FREQUENTLY ASKED QUESTIONS ABOUT FREE AND REDUCED PRICE SCHOOL MEALS Dear Parent/Guardian: Children need healthy meals to learn. Rogers School District offers healthy meals every school day. Your children
Household Application for Free and Reduced Price School Meals Complete one application per household. Please use a pen (not a pencil).
.") 2017-2018 Household Application for Free and Reduced Price School Meals Complete one application per household. Please use a pen (not a pencil). Apply online: STEP 1 List ALL Household Members who are
2017-2018 Household Application for Free and Reduced Price School Meals Complete one application per household. Please use a pen (not a pencil). Apply online: STEP 1 List ALL Household Members who are
FREE/REDUCED LUNCH PACKET
 FREE/REDUCED LUNCH PACKET CHILD S NAME ( PLEASE PRINT ) PLEASE FILL OUT ONE APPLICATION PER FAMILY. You DO NOT have to fill out more than one application. If you have already completed an application,
FREE/REDUCED LUNCH PACKET CHILD S NAME ( PLEASE PRINT ) PLEASE FILL OUT ONE APPLICATION PER FAMILY. You DO NOT have to fill out more than one application. If you have already completed an application,
LEOMINSTER PUBLIC SCHOOLS
 LEOMINSTER PUBLIC SCHOOLS 24 Church Street, Leominster, MA 01453 Telephone: 978.534.7700 Fax: 978.534.7775 Anthony J. Bent Ed.D. Interim Superintendent of Schools Maryann Perry Deputy Superintendent Dear
LEOMINSTER PUBLIC SCHOOLS 24 Church Street, Leominster, MA 01453 Telephone: 978.534.7700 Fax: 978.534.7775 Anthony J. Bent Ed.D. Interim Superintendent of Schools Maryann Perry Deputy Superintendent Dear
FINANCIAL ASSISTANCE APPLICATION: COVER LETTER
 FINANCIAL ASSISTANCE APPLICATION: COVER LETTER Thank you for choosing Children s of Alabama to provide for the healthcare needs of your child. Please find attached the forms you must complete in order
FINANCIAL ASSISTANCE APPLICATION: COVER LETTER Thank you for choosing Children s of Alabama to provide for the healthcare needs of your child. Please find attached the forms you must complete in order
Application for Health Coverage & Help Paying Costs
 09/2014 Application for Health Coverage & Help Paying Costs Form Approved OMB No. 0938-1191 Apply faster online Use this application to see what coverage you qualify for Who can use this application? What
09/2014 Application for Health Coverage & Help Paying Costs Form Approved OMB No. 0938-1191 Apply faster online Use this application to see what coverage you qualify for Who can use this application? What
Uninsured? Interested in finding out what free or low cost health insurance options are available for you? Easy ways to find out:
 Uninsured? Interested in finding out what free or low cost health insurance options are available for you? Easy ways to find out: In Person. Group enrollment sessions are available daily by calling Lynn
Uninsured? Interested in finding out what free or low cost health insurance options are available for you? Easy ways to find out: In Person. Group enrollment sessions are available daily by calling Lynn
Frequently Asked Questions
 Arlington Public Schools Food Service Program 869 Massachusetts Ave Arlington, MA 02476 Phone: 781-316-3643 Fax: 781-316-3644 Dear Parent/Guardian: Children need healthy meals to learn. The Arlington Public
Arlington Public Schools Food Service Program 869 Massachusetts Ave Arlington, MA 02476 Phone: 781-316-3643 Fax: 781-316-3644 Dear Parent/Guardian: Children need healthy meals to learn. The Arlington Public
Instructions for Request for Reduced Fee
 Instructions for Request for Reduced Fee Department of Homeland Security U.S. Citizenship and Immigration Services USCIS Form I-942 OMB No. 1615-0133 Expires 11/30/2018 What Is the Purpose of Form I-942?
Instructions for Request for Reduced Fee Department of Homeland Security U.S. Citizenship and Immigration Services USCIS Form I-942 OMB No. 1615-0133 Expires 11/30/2018 What Is the Purpose of Form I-942?
Low-Income Home Energy Assistance Program (LIHEAP)
") Orutsararmiut Native Council LIHEAP Program 117 Alex Hately Drive PO Box 927 Bethel, Alaska 99559-0927 Phone: (907) 543-2608 Fax: (907) 543-2639 Low-Income Home Energy Assistance Program (LIHEAP) LIHEAP
Orutsararmiut Native Council LIHEAP Program 117 Alex Hately Drive PO Box 927 Bethel, Alaska 99559-0927 Phone: (907) 543-2608 Fax: (907) 543-2639 Low-Income Home Energy Assistance Program (LIHEAP) LIHEAP
Massachusetts Application for Free and Reduced Price School Meals
 Grade STEP 1 2016-2017 Massachusetts Application for Free and Reduced Price School Meals If you have received a Notice of Direct Certification from the school district for free meals, do not complete this
Grade STEP 1 2016-2017 Massachusetts Application for Free and Reduced Price School Meals If you have received a Notice of Direct Certification from the school district for free meals, do not complete this
Bellevue Public Schools
 Bellevue Public Schools 2820 Arboretum Drive Bellevue, Nebraska 68005 Telephone: (402) 293-5032 Bellevue Public Schools Application for Free and Reduced Meals-Effective July 2017 Children need healthy
Bellevue Public Schools 2820 Arboretum Drive Bellevue, Nebraska 68005 Telephone: (402) 293-5032 Bellevue Public Schools Application for Free and Reduced Meals-Effective July 2017 Children need healthy
LETTER TO HOUSEHOLDS - CHARGE. Dear Parent or Guardian:
 LETTER TO HOUSEHOLDS - CHARGE Dear Parent or Guardian: Children need healthy meals to learn. McClusky Public School offers healthy meals every school day. Breakfast costs 1.55 and lunch costs 2.80 for
LETTER TO HOUSEHOLDS - CHARGE Dear Parent or Guardian: Children need healthy meals to learn. McClusky Public School offers healthy meals every school day. Breakfast costs 1.55 and lunch costs 2.80 for
Hanover Public Schools
 Hanover Public Schools Dear Parent/Guardian: FREQUENTLY ASKED QUESTIONS ABOUT FREE AND REDUCED PRICE SCHOOL MEALS Children need healthy meals to learn. Hanover Public Schools offers healthy meals every
Hanover Public Schools Dear Parent/Guardian: FREQUENTLY ASKED QUESTIONS ABOUT FREE AND REDUCED PRICE SCHOOL MEALS Children need healthy meals to learn. Hanover Public Schools offers healthy meals every
Social Security Number (SSN) of applying member. Date of Birth
 of applying member. Date of Birth") LDSS-4826 (11/02) Page 1 NEW YORK STATE OFFICE OF TEMPORARY AND DISABILITY ASSISTANCE FOOD STAMP BENEFITS APPLICATION Application Date Interview Date Center/Office Unit Worker Case Type Case Number Registry
LDSS-4826 (11/02) Page 1 NEW YORK STATE OFFICE OF TEMPORARY AND DISABILITY ASSISTANCE FOOD STAMP BENEFITS APPLICATION Application Date Interview Date Center/Office Unit Worker Case Type Case Number Registry
M. David Blackburn, Superintendent. Free and Reduced Price School Meals Information Letter to Households
 SALIDA SCHOOL DISTRICT R-32-J BOARD OF EDUCATION Kyle Earhart, President Jennifer Visitation, Vice-President, Cheri Post, Treasurer Directors: Jeannie Peters, Joel McBride, Joe Smith, Penny Wilken M. David
SALIDA SCHOOL DISTRICT R-32-J BOARD OF EDUCATION Kyle Earhart, President Jennifer Visitation, Vice-President, Cheri Post, Treasurer Directors: Jeannie Peters, Joel McBride, Joe Smith, Penny Wilken M. David
SHELTER PLUS CARE REFERRAL/APPLICATION PACKET
 SHELTER PLUS CARE REFERRAL/APPLICATION PACKET Applicant s Name: Date: Referral Source: Referral Source Contact Person: Contact Phone #: Eastpointe is committed to delivering a continuum of services to
SHELTER PLUS CARE REFERRAL/APPLICATION PACKET Applicant s Name: Date: Referral Source: Referral Source Contact Person: Contact Phone #: Eastpointe is committed to delivering a continuum of services to
Wamego Public Schools
 1008 8 th Street Wamego, KS 66547 Wamego Public Schools Ph: 785 456 7643 Fax: 785 456 8125 www.usd320.com Dear Parent/Guardian: Children need healthy meals to learn. USD 320 offers healthy meals every
1008 8 th Street Wamego, KS 66547 Wamego Public Schools Ph: 785 456 7643 Fax: 785 456 8125 www.usd320.com Dear Parent/Guardian: Children need healthy meals to learn. USD 320 offers healthy meals every
A new application must be submitted each year.
 HUNTINGTON UNION FREE SCHOOL DISTRICT A Tradition of Excellence Since 1657 Kathleen Acker Assistant Superintendent (631) 673-2111 Finance and Management Services August 2017 A new application must be submitted
HUNTINGTON UNION FREE SCHOOL DISTRICT A Tradition of Excellence Since 1657 Kathleen Acker Assistant Superintendent (631) 673-2111 Finance and Management Services August 2017 A new application must be submitted
ATTENTION: NEW PATIENTS Please allow 4 to 6 weeks to receive your FIRST fill on your prescriptions.
 ATTENTION: NEW PATIENTS Please allow 4 to 6 weeks to receive your FIRST fill on your prescriptions. Regional Healthcare does not control shipments of medication. The pharmaceutical company which supplies
ATTENTION: NEW PATIENTS Please allow 4 to 6 weeks to receive your FIRST fill on your prescriptions. Regional Healthcare does not control shipments of medication. The pharmaceutical company which supplies
IMPORTANT INFORMATION - READ and KEEP THESE 3 PAGES! DO NOT hand them in with your application.
 2018 SUMMER YOUTH EMPLOYMENT PROGRAM (SYEP) Allegany County Employment & Training, 7 Wells Lane, Belmont, NY 14813 (585) 268-9445 weiricsb@alleganyco.com What is SYEP 2018? IMPORTANT INFORMATION - READ
2018 SUMMER YOUTH EMPLOYMENT PROGRAM (SYEP) Allegany County Employment & Training, 7 Wells Lane, Belmont, NY 14813 (585) 268-9445 weiricsb@alleganyco.com What is SYEP 2018? IMPORTANT INFORMATION - READ
Apartment Application For Buffalo Municipal Housing Authority Your Choice for Rental Housing
 BMHA manages over 3900 subsidized public housing apartments spread throughout the City of Buffalo. We have apartments for seniors and families. Apartments for disabled, and apartments that are handicap
BMHA manages over 3900 subsidized public housing apartments spread throughout the City of Buffalo. We have apartments for seniors and families. Apartments for disabled, and apartments that are handicap
FINAL CHECK LIST. Immigration Documentation (Resident Alien Cards, Passports, Certificate of Naturalization, I-94, Birth Certificates)
") Welcome to JPS Health Network. We look forward to providing affordable health care to you and your family. The purpose of the JPS Connection program is to create a healthier community by providing discount
Welcome to JPS Health Network. We look forward to providing affordable health care to you and your family. The purpose of the JPS Connection program is to create a healthier community by providing discount
2019 Health Insurance Application
 1515 North Saint Joseph Avenue PO Box 8000 Marshfield, WI 54449-8000 1.844.293.9624 715.221.9258 TTY: 711 Fax: 715.221.9500 Individual and Family 2019 Health Insurance Application FOR STAFF/AGENT/BROKER
1515 North Saint Joseph Avenue PO Box 8000 Marshfield, WI 54449-8000 1.844.293.9624 715.221.9258 TTY: 711 Fax: 715.221.9500 Individual and Family 2019 Health Insurance Application FOR STAFF/AGENT/BROKER
Child s First Name MI Child s Last Name Grade
 2017-2018 Prototype Household Application for Free and Reduced Price School Meals Complete one application per household. Please use a pen (not a pencil). Apply online: on Infinite Campus STEP 1 Definition
2017-2018 Prototype Household Application for Free and Reduced Price School Meals Complete one application per household. Please use a pen (not a pencil). Apply online: on Infinite Campus STEP 1 Definition
USD 250 PITTSBURG COMMUNITY SCHOOLS
 USD 250 PITTSBURG COMMUNITY SCHOOLS Dear Parent/Guardian: Children need healthy meals to learn. USD 250 offers healthy meals every school day. Your children may qualify for free meals or for reduced price
USD 250 PITTSBURG COMMUNITY SCHOOLS Dear Parent/Guardian: Children need healthy meals to learn. USD 250 offers healthy meals every school day. Your children may qualify for free meals or for reduced price
HealthyCare Card Application
 HealthyCare Card Application This is an application for the HealthyCare Card, a program of Healthy Community Network. The HealthyCare Card (HCC) is a community program which provides discounts to care
HealthyCare Card Application This is an application for the HealthyCare Card, a program of Healthy Community Network. The HealthyCare Card (HCC) is a community program which provides discounts to care
Low-Income Telephone/Broadband Discount Program (Texas Lifeline) Enrollment Form
 Enrollment Form") Low-Income Telephone/Broadband Discount Program (Texas Lifeline) Enrollment Form The Texas Lifeline Program can provide a discount off your monthly telephone/broadband bill. What should I send in along
Low-Income Telephone/Broadband Discount Program (Texas Lifeline) Enrollment Form The Texas Lifeline Program can provide a discount off your monthly telephone/broadband bill. What should I send in along
Acceptable Dependent Verification Items (Including Spouse as a Dependent)
") BILLING EXHIBIT A: APPROVED DOCUMENT LIST We will review and consider household financial income for possible discounted services. Qualification for Financial Assistance depends upon a number of things
BILLING EXHIBIT A: APPROVED DOCUMENT LIST We will review and consider household financial income for possible discounted services. Qualification for Financial Assistance depends upon a number of things