Itemized Statement of Charges
|
|
|
- Antony Hodge
- 5 years ago
- Views:
Transcription
1
2
3 MR JOHN DOE Itemized Statement of Charges Patient's Name Mayo Clinic Number Visit Number Dates of Service /02/02-01/03/02 Please refer to patient's name, Mayo Clinic number and visit number on all correspondence. Billing Account Number: Statement Date: January 21, 2002 Addressee Services Provided By MR JOHN DOE MAYO CLINIC ROCHESTER 520 PLEASANT STREET 200 FIRST STREET SW ANYTOWN, MN ROCHESTER, MN THIS IS NOT A BILL THIS IS FOR YOUR INFORMATION ONLY Important Information to Assist You 1. This Itemized Statement of Charges is for your information only. You will be receiving a Monthly Statement of Account (your bill) reflecting your financial responsibility. The visit number above will help you identify this specific visit on your Monthly Statement of Account. 2. Please review this statement carefully. If you have questions, please contact Patient Account Services: Mayo Clinic Telephone RO-HA-04-ACCT 8:00 AM to 5:00 PM CST 200 First Street SW Monday through Friday Rochester, MN We have generated a claim for the following insurance company(ies): ABC Insurance ** Verify the insurance is correct and notify us of any changes ** 4. Retain this Itemized Statement of Charges for your records. PAGE 1 Mayo Clinic IRS No Mayo Hospice IRS No Mayo Clinic Outreach Service IRS No Please see reverse for important information. MC /R0202
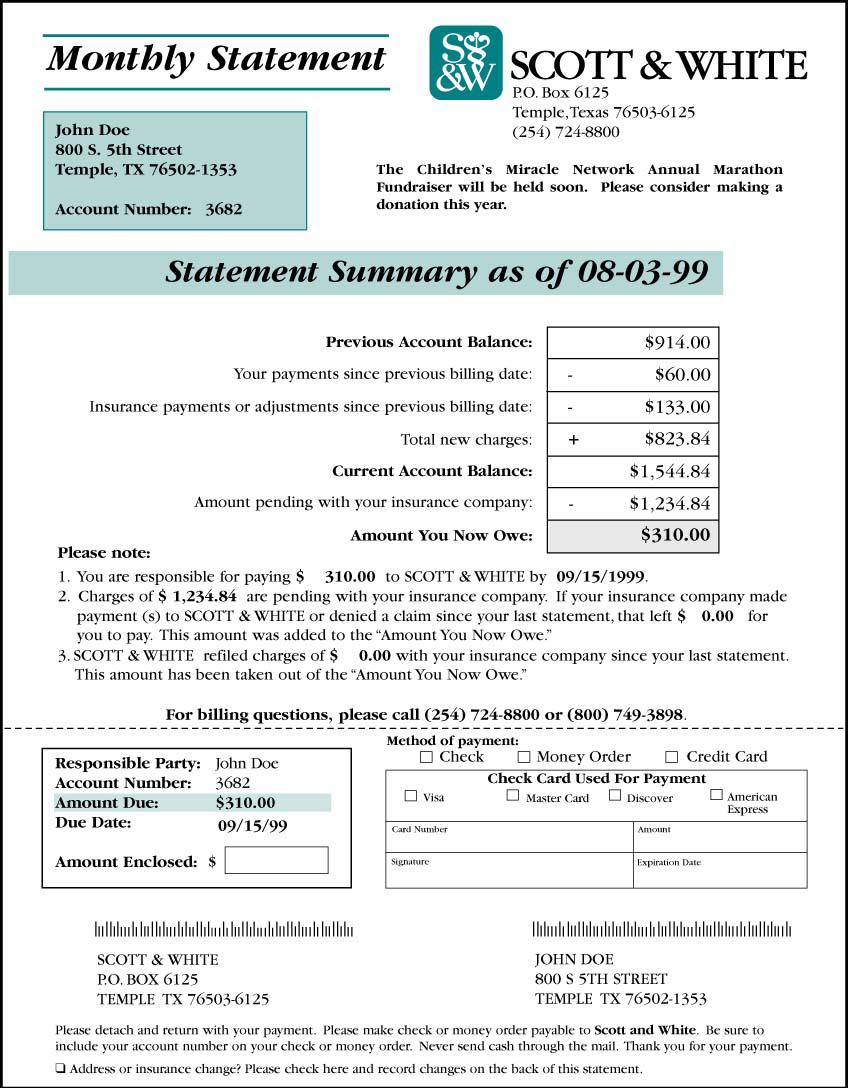
4 Monthly Statement of Account Page 1 MR JOHN DOE Billing Account Number: PLEASANT STREET Statement Date: February 4, 2002 ANYTOWN, MN Customer Service: Messages: Thank you for choosing Mayo Clinic. Thank you for your payment. You are currently responsible for paying $65.85 to Mayo Clinic. PLEASE NOTE: Charges totaling $ are pending with your insurance. You will be responsible for the portion not covered. If you have questions about insurance claims or payments, contact your insurance representative. Account Summary: Previous Account Balance $ as of 01/04/02 New Charges $ Payment/Adjustments $ Current Account Balance $ Insurance Claims Pending $ CURRENT AMOUNT DUE: $ To help us process your payment, please return the lower portion of this statement with your payment. Do not send currency. Billing Addressee Billing Account Number Date Due Amount Due Amount Enclosed DOE, JOHN Upon Receipt $ Check here if your address has changed. Please indicate changes on back. To pay by check or money order: Make payable to MAYO CLINIC. Write your billing account number on the front of your check or money order and mail in the enclosed envelope to: To pay by credit/debit card: Please indicate credit/debit card preference. Provide the account information and sign below, or call Visa Mastercard Discover American Express Diners Club Card Account No.: MAYO CLINIC P.O. BOX 4003 ROCHESTER, MN Card Holder Name: Authorized Signature: Expiration Date: Amount: MC2323/R0202
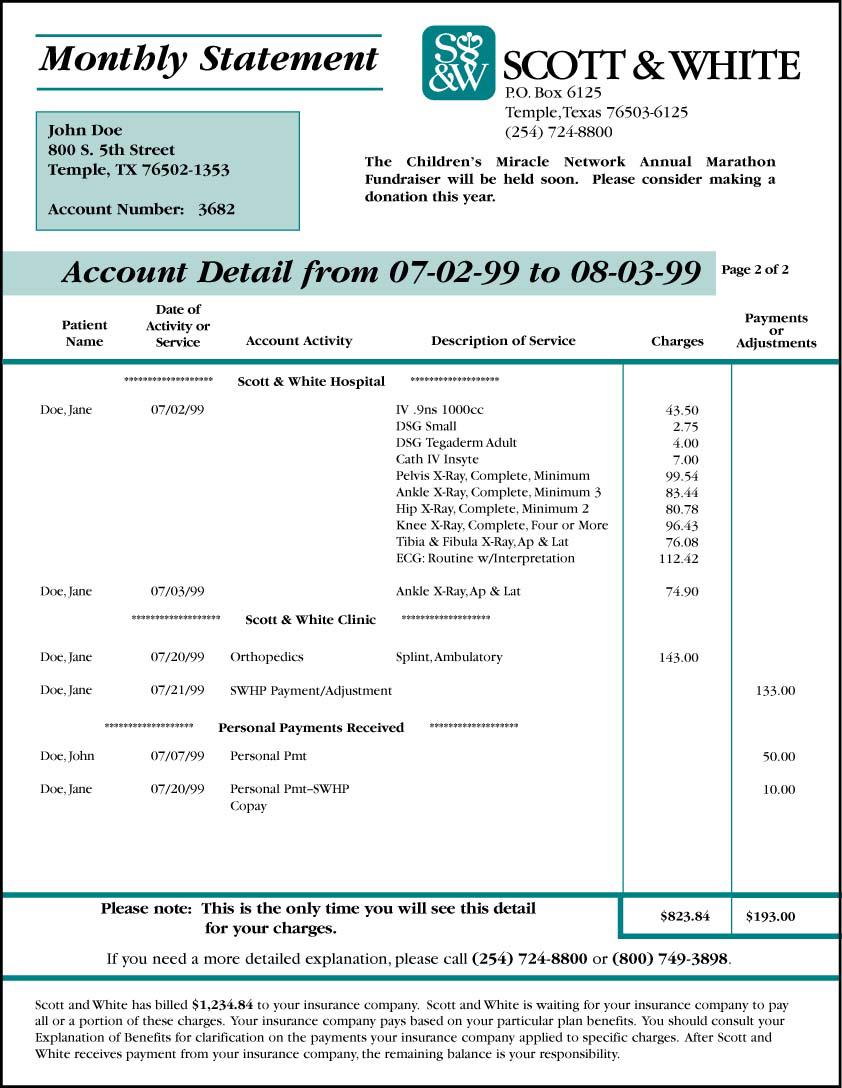
5 Monthly Statement of Account Page 2 Patient Name Mayo Clinic Number/Visit Number Dates of Service Place of Service Transaction Detail/Description Insurance Account Claims Personal Activity Pending Responsibility DOE, JOHN Visit /08/ /08/2001 St. Marys Hospital Previous Balance $ /19/01 Personal Payment $ Visit Balance $ 0.00 Insurance Pending $ 0.00 Amount Due $ 0.00 DOE, JOHN Visit /06/ /08/2001 Mayo Clinic Rochester Previous Balance $ /19/01 ABC Insurance payment $ Visit Balance $ Insurance Pending $ 0.00 Amount Due $ DOE, JANE Visit /18/ /18/2001 Rochester Methodist Hospital New Charges $ /27/01 Insurance Claim Filed/ABC Insurance Visit Balance $ Insurance Pending $ Amount Due $ 0.00 DOE, JANE Visit /18/ /19/2001 Mayo Clinic Rochester New Charges $ /22/01 Insurance Claim Filed/ABC Insurance Visit Balance $ Insurance Pending $ Amount Due $ 0.00 MC2323-A/R0202 Current Account Balance $ Insurance Claims Pending $ Current Amount Due $ 65.85
6 Payment Policy Even though you may have insurance, you are responsible for payment of your Mayo Clinic accounts. You will receive a statement each month your account has a balance. If payment is not received for any claims pending with your insurance company within 45 days, we will look to you for full payment. Billing Inquiries Please review this statement carefully. We welcome any questions you may have about your account, and invite you to contact Patient Account Services by telephone, Monday through Friday, 8:00 a.m. to 5:00 p.m. CST, or by letter. We will make every attempt to answer your questions concerning your account. Patient Account Services For international billing inquiries: Mayo Clinic International Financial Services RO-HA-04-ACCT Mayo Clinic 200 First Street SW 200 First Street SW Rochester, MN Rochester, MN Telephone Telephone Glossary of Terms Adjustments: A credit or debit transaction applied to the account. Billing Account Number: The account number of the person assigned to receive the bill. Refer to this number when contacting Mayo Clinic with questions. Billing Addressee: The person designated to receive the monthly billing statements. This person can coordinate the billing, payment and insurance coverage for the account. Contract Adjustment: A credit or debit applied to the account due to the contractual agreement between Mayo Clinic and the insurance company. Insurance Claims Pending: Charges filed to insurance company; Mayo Clinic has not received a determination of the benefits. Mayo Clinic Number: The patient s personal identification number. New Charges: Charges billed by Mayo Clinic since the previous monthly statement. These are detailed on your Itemized Statement of Charges. Visit Balance: The current balance of each episode of care. Visit Number: A number assigned to identify each episode of care. The number is used to track services and payments. Address/Telephone Change Name Address City State Zip Telephone
Dental, Vision & Hearing
 INSURANCE COMPANY Dental, Vision & Hearing Application Booklet Insurance Agency: Producer/Agent Name: Producer/Agent Phone Number: 34 112 1050 0915 MT Welcome! Thank you for choosing Medico Insurance Company
INSURANCE COMPANY Dental, Vision & Hearing Application Booklet Insurance Agency: Producer/Agent Name: Producer/Agent Phone Number: 34 112 1050 0915 MT Welcome! Thank you for choosing Medico Insurance Company
BB&T Association Services Online Payment System Sample Screens Revised 08/02/2012
 BB&T Association Services Online Payment System Sample Screens Revised 08/02/2012 Associations can accept payments from our website through BB&T Association Services optional Online Payment System. Our
BB&T Association Services Online Payment System Sample Screens Revised 08/02/2012 Associations can accept payments from our website through BB&T Association Services optional Online Payment System. Our
Making One-Time E-Check and Card Payments 1,2 Quick Reference Guide
 H O M E O W N E R S ASS O C I A T I O N SER V I C E S Making One-Time E-Check and Card Payments 1,2 Quick Reference Guide This guide walks you through making quick one-time payments using an e-check or
H O M E O W N E R S ASS O C I A T I O N SER V I C E S Making One-Time E-Check and Card Payments 1,2 Quick Reference Guide This guide walks you through making quick one-time payments using an e-check or
Vantage 100 (HMO-POS) $ per month
 $ per month") 2019 Medicare Advantage Enrollment Election Form Vantage Medicare Advantage Vantage Health Plan, Inc. 130 DeSiard Street, Suite 300 Monroe, LA 71201 (318) 361-0900 TTY (318) 361-2131 (866) 704-0109 TTY
2019 Medicare Advantage Enrollment Election Form Vantage Medicare Advantage Vantage Health Plan, Inc. 130 DeSiard Street, Suite 300 Monroe, LA 71201 (318) 361-0900 TTY (318) 361-2131 (866) 704-0109 TTY
Action Financial Services, LLC Recurring Payment Authorization Form
 Sign and complete this form to authorize Action Financial Services, LLC to make a debit from your account listed below. By signing below, I authorize Action Financial Services, LLC. to charge the account
Sign and complete this form to authorize Action Financial Services, LLC to make a debit from your account listed below. By signing below, I authorize Action Financial Services, LLC. to charge the account
For Preview Only - Please Do Not Copy
 Information about filing fees, filing documents by facsimile transmission and a filing letter to the Secretary of State s office for the certificate of formation for a limited partnership Fax filing &
Information about filing fees, filing documents by facsimile transmission and a filing letter to the Secretary of State s office for the certificate of formation for a limited partnership Fax filing &
To learn more about the requirements for your debit card claims, go directly to Section 3, page 4.
 FSA Debit Card Guide IMPORTANT: Please Read There are many misconceptions about debit cards and FSAs. Before you read any further, it s important to understand that using the FSA debit card does NOT eliminate
FSA Debit Card Guide IMPORTANT: Please Read There are many misconceptions about debit cards and FSAs. Before you read any further, it s important to understand that using the FSA debit card does NOT eliminate
Important Information About the Notice on Health Insurance Marketplace Coverage Options and Your Discover Financial Services Benefits
 Statement Date: July 8, 2014 A000001 JANE DOE088200009 DO NOT MAIL RIVERTON UT 84096 myhr Service Center http://resources.hewitt.com/discover myhr Service Center 844-DFS-myHR (844-337-6947) between 8:00
Statement Date: July 8, 2014 A000001 JANE DOE088200009 DO NOT MAIL RIVERTON UT 84096 myhr Service Center http://resources.hewitt.com/discover myhr Service Center 844-DFS-myHR (844-337-6947) between 8:00
Making a One-Time Bill Payment Using MyUHCare
 Making a One-Time Bill Payment Using MyUHCare Follow these instructions to make a one-time payment by credit/debit card or check for all or part of your University Hospitals bill through MyUHCare, your
Making a One-Time Bill Payment Using MyUHCare Follow these instructions to make a one-time payment by credit/debit card or check for all or part of your University Hospitals bill through MyUHCare, your
Individual Enrollment Request Form
 Individual Enrollment Request Form To enroll in VillageHealth, please provide the following information: Please check which plan you want to enroll in: o 001 VillageHealth (HMO-POS SNP) Riverside and San
Individual Enrollment Request Form To enroll in VillageHealth, please provide the following information: Please check which plan you want to enroll in: o 001 VillageHealth (HMO-POS SNP) Riverside and San
Banta Consulting. Financial Strategies for Getting the Dollars Off the Books and Into the Bank!
 Banta Consulting Financial Strategies for Getting the Dollars Off the Books and Into the Bank! Financial Strategies for Getting the Dollars Off the Books And Into the Bank! Lois Banta Banta Consulting,
Banta Consulting Financial Strategies for Getting the Dollars Off the Books and Into the Bank! Financial Strategies for Getting the Dollars Off the Books And Into the Bank! Lois Banta Banta Consulting,
Self Service Payments
 Self Service Payments Before You Begin IMPORTANT: Make sure your browser is setup to 'accept third party cookies'. Please refer to the instructions in the document: How to Enable Third Party Cookies in
Self Service Payments Before You Begin IMPORTANT: Make sure your browser is setup to 'accept third party cookies'. Please refer to the instructions in the document: How to Enable Third Party Cookies in
Sabates Eye Centers P.O. Box Kansas City, MO (913)
") Sabates Eye Centers P.O. Box 26425 Kansas City, MO 64196-6425 (913) 261-2020 Type of Visit: u Routine u Medical Contact Lens Wearer? u Yes u No PATIENT INFORMATION Name (Last, First, Middle Initial) Date
Sabates Eye Centers P.O. Box 26425 Kansas City, MO 64196-6425 (913) 261-2020 Type of Visit: u Routine u Medical Contact Lens Wearer? u Yes u No PATIENT INFORMATION Name (Last, First, Middle Initial) Date
Upgrade My Credit Client Agreement
 Upgrade My Credit Client Agreement 901 W. Bardin Rd. Suite 306 Arlington, Texas 76017 817-886-0302 off. 817-887-0816 fax www.upgrademycredit.com APPLICANT INFORMATION Mr. Mrs. Ms. PLEASE PRINT CLEARLY
Upgrade My Credit Client Agreement 901 W. Bardin Rd. Suite 306 Arlington, Texas 76017 817-886-0302 off. 817-887-0816 fax www.upgrademycredit.com APPLICANT INFORMATION Mr. Mrs. Ms. PLEASE PRINT CLEARLY
Setting up a Bill Payment Plan in MyUHCare
 Setting up a Bill Payment Plan in MyUHCare Follow these instructions to set up a payment plan by credit/debit card or check for your University Hospitals bill through MyUHCare, your secure, online personal
Setting up a Bill Payment Plan in MyUHCare Follow these instructions to set up a payment plan by credit/debit card or check for your University Hospitals bill through MyUHCare, your secure, online personal
2018 Medicare Advantage Prescription Drug Plan Individual Enrollment Request Form
 2018 Medicare Advantage Prescription Drug Plan Individual Enrollment Request Form Please contact SummaCare if you need information in another language or a different format. To enroll in SummaCare, please
2018 Medicare Advantage Prescription Drug Plan Individual Enrollment Request Form Please contact SummaCare if you need information in another language or a different format. To enroll in SummaCare, please
Individual Enrollment Request Form. Please Provide Your Medicare Insurance Information
 MSA Please contact Network Health Medicare Advantage plans if you need information in another language or format (Braille). To Enroll in NetworkPrime (MSA), Please Provide the Following Information. LAST
MSA Please contact Network Health Medicare Advantage plans if you need information in another language or format (Braille). To Enroll in NetworkPrime (MSA), Please Provide the Following Information. LAST
INCOMING ABLE ROLLOVER FORM
 INCOMING ABLE ROLLOVER FORM PLEASE READ THE IMPORTANT INFORMATION BELOW Complete this form to initiate a transfer of funds from another Qualified ABLE Plan (QAP) into an existing STABLE Account, report
INCOMING ABLE ROLLOVER FORM PLEASE READ THE IMPORTANT INFORMATION BELOW Complete this form to initiate a transfer of funds from another Qualified ABLE Plan (QAP) into an existing STABLE Account, report
Welcome to Thomaston Savings Bank
 Welcome to Thomaston Savings Bank Thank you for considering Thomaston Savings Bank for your banking needs. Since 1874, we have been dedicated to providing quality products and exceptional service to our
Welcome to Thomaston Savings Bank Thank you for considering Thomaston Savings Bank for your banking needs. Since 1874, we have been dedicated to providing quality products and exceptional service to our
New Patient Registration
 New Patient Registration 900 Carillon Parkway, Suite 404 Saint Petersburg, Florida 33716 Ph: 727-572-1333 Fax: 727-572-1331 www.spencerdermatology.com Today s : / / Name: (First) (Middle) (Last) (Suffix)
New Patient Registration 900 Carillon Parkway, Suite 404 Saint Petersburg, Florida 33716 Ph: 727-572-1333 Fax: 727-572-1331 www.spencerdermatology.com Today s : / / Name: (First) (Middle) (Last) (Suffix)
Solar Eclipse Credit Card Authorization. Release 9.0.4
 Solar Eclipse Credit Card Authorization Release 9.0.4 i Table Of Contents Disclaimer This document is for informational purposes only and is subject to change without notice. This document and its contents,
Solar Eclipse Credit Card Authorization Release 9.0.4 i Table Of Contents Disclaimer This document is for informational purposes only and is subject to change without notice. This document and its contents,
Christina Agustin, MD Board Certified in Adult Psychiatry 1 Lake Bellevue Drive, Suite 101 Bellevue, WA Phone Fax:
 Christina Agustin, MD Board Certified in Adult Psychiatry 1 Lake Bellevue Drive, Suite 101 Bellevue, WA 98005 Phone 425-301-9869 Fax: 866-546-1618 Welcome to my practice. I look forward to meeting with
Christina Agustin, MD Board Certified in Adult Psychiatry 1 Lake Bellevue Drive, Suite 101 Bellevue, WA 98005 Phone 425-301-9869 Fax: 866-546-1618 Welcome to my practice. I look forward to meeting with
Instructions for Fax or Applications for Service
 845 Galvez Street, Mandeville, LA 70448-4934 985.626.5132 www.h2osystemsinc.com Instructions for Fax or Email Applications for Service To complete your application for water and sewer services via fax
845 Galvez Street, Mandeville, LA 70448-4934 985.626.5132 www.h2osystemsinc.com Instructions for Fax or Email Applications for Service To complete your application for water and sewer services via fax
Individual Enrollment Request Form
 Individual Enrollment Request Form 3800 Kilroy Airport Way, Suite 100 Long Beach, CA 90806 Please contact SCAN Health Plan if you need information in another language or format (Braille). To enroll in
Individual Enrollment Request Form 3800 Kilroy Airport Way, Suite 100 Long Beach, CA 90806 Please contact SCAN Health Plan if you need information in another language or format (Braille). To enroll in
Confinement Waiver Instructions
 Confinement Waiver Instructions Mail or fax completed form to: P.O. Box 1555, Des Moines, IA 50306-1555 Fax: 866 709 3922 Contact us: Annuity Customer Contact Center Tel: 888 266 8489 Athene Annuity and
Confinement Waiver Instructions Mail or fax completed form to: P.O. Box 1555, Des Moines, IA 50306-1555 Fax: 866 709 3922 Contact us: Annuity Customer Contact Center Tel: 888 266 8489 Athene Annuity and
UNIVERSITY MEDICAL CENTER OF PRINCETON AT PLAINSBORO NEW JERSEY HOSPITAL CARE ASSISTANCE PROGRAM REQUIREMENT LIST
 UNIVERSITY MEDICAL CENTER OF PRINCETON AT PLAINSBORO NEW JERSEY HOSPITAL CARE ASSISTANCE PROGRAM REQUIREMENT LIST To further assist us in processing your application for Charity Care, please provide copies
UNIVERSITY MEDICAL CENTER OF PRINCETON AT PLAINSBORO NEW JERSEY HOSPITAL CARE ASSISTANCE PROGRAM REQUIREMENT LIST To further assist us in processing your application for Charity Care, please provide copies
High Impact Communication
 High Impact Communication Please note: This workshop is offered as information only and not as financial, accounting or legal advice. Seminar attendees may make photocopies of these pages for internal
High Impact Communication Please note: This workshop is offered as information only and not as financial, accounting or legal advice. Seminar attendees may make photocopies of these pages for internal
AAA7 Vantage Dual Special Needs (HMO SNP)
") Medicare Advantage Enrollment Election Form Vantage Medicare Advantage Vantage Health Plan, Inc. 130 DeSiard Street, Suite 300 Monroe, LA 71201 (318) 361-0900 TTY (318) 361-2131 (866) 704-0109 TTY (866)
Medicare Advantage Enrollment Election Form Vantage Medicare Advantage Vantage Health Plan, Inc. 130 DeSiard Street, Suite 300 Monroe, LA 71201 (318) 361-0900 TTY (318) 361-2131 (866) 704-0109 TTY (866)
NMCA 2019 ANNUAL CONVENTION April 12 & 13, 2019
 NMCA 2019 ANNUAL CONVENTION April 12 & 13, 2019 EVERYTHING YOU NEED TO REGISTER AS AN EXHIBITOR FOR THE NMCA 2019 CONVENTION IS ENCLOSED!! PLEASE JOIN US!! Enclosed with this letter are a Registration
NMCA 2019 ANNUAL CONVENTION April 12 & 13, 2019 EVERYTHING YOU NEED TO REGISTER AS AN EXHIBITOR FOR THE NMCA 2019 CONVENTION IS ENCLOSED!! PLEASE JOIN US!! Enclosed with this letter are a Registration
Individual Enrollment Request Form
 Individual Enrollment Request Form 3800 Kilroy Airport Way, Suite 100 Long Beach, CA 90806 Please contact SCAN Health Plan if you need information in another language or format (Braille). To enroll in
Individual Enrollment Request Form 3800 Kilroy Airport Way, Suite 100 Long Beach, CA 90806 Please contact SCAN Health Plan if you need information in another language or format (Braille). To enroll in
DATE ISSUED: 3/28/ of 1 LDU CDC(EXHIBIT)-X
-X") The following exhibits are used by the District: Exhibit A: Exhibit B: Report of Gift or Donation 1 page Thank You Letters 2 pages DATE ISSUED: 3/28/2012 1 of 1 EXHIBIT A REPORT OF GIFT OR DONATION DALLAS
The following exhibits are used by the District: Exhibit A: Exhibit B: Report of Gift or Donation 1 page Thank You Letters 2 pages DATE ISSUED: 3/28/2012 1 of 1 EXHIBIT A REPORT OF GIFT OR DONATION DALLAS
HealthPartners Medicare Supplement Outline of Coverage and Disclosure of Information
 HealthPartners Medicare Supplement Outline of Coverage and Disclosure of Information HEALTHPARTNERS EXTENDED BASIC MEDICARE SUPPLEMENT PLAN Use this document to get to know the HealthPartners Extended
HealthPartners Medicare Supplement Outline of Coverage and Disclosure of Information HEALTHPARTNERS EXTENDED BASIC MEDICARE SUPPLEMENT PLAN Use this document to get to know the HealthPartners Extended
Attestation of Eligibility for an Enrollment Period
 301 S. Vine St., Urbana, IL 61801 Attestation of Eligibility for an Enrollment Period Typically, you may enroll in a health plan only during the Open Enrollment Period. There are exceptions that may allow
301 S. Vine St., Urbana, IL 61801 Attestation of Eligibility for an Enrollment Period Typically, you may enroll in a health plan only during the Open Enrollment Period. There are exceptions that may allow
HealthPartners Medicare Supplement Outline of Coverage and Disclosure of Information
 HealthPartners Medicare Supplement Outline of Coverage and Disclosure of Information HEALTHPARTNERS BASIC MEDICARE SUPPLEMENT PLAN Use this document to get to know the HealthPartners Basic Medicare Supplement
HealthPartners Medicare Supplement Outline of Coverage and Disclosure of Information HEALTHPARTNERS BASIC MEDICARE SUPPLEMENT PLAN Use this document to get to know the HealthPartners Basic Medicare Supplement
The Taxpayers Guide to Brooklyn Taxes
 The Taxpayers Guide to Brooklyn Taxes Jocelyne Ruffo - Revenue Collector April Lamothe - Assistant Revenue Collector Telephone # (860) 779-3411, option 5 Fax # 779-7853 Tax Collector PO Box 253 Brooklyn,
The Taxpayers Guide to Brooklyn Taxes Jocelyne Ruffo - Revenue Collector April Lamothe - Assistant Revenue Collector Telephone # (860) 779-3411, option 5 Fax # 779-7853 Tax Collector PO Box 253 Brooklyn,
ambulance cover from under 63 p a week
 2018 ambulance cover from under 6 p a week What does it cost? SINGLE membership of.00 provides cover for a single person only. CHILD membership of 12.00 provides cover for one child up until the end of
2018 ambulance cover from under 6 p a week What does it cost? SINGLE membership of.00 provides cover for a single person only. CHILD membership of 12.00 provides cover for one child up until the end of
INSTANT SAVER 2 ACCOUNT
 INSTANT SAVER 2 ACCOUNT Provided by Scottish Widows Bank SUMMARY BOX PLEASE READ THIS SUMMARY BOX BEFORE YOU COMPLETE THE APPLICATION AND THEN KEEP IT FOR YOUR RECORDS. DON T RETURN IT WITH THE APPLICATION.
INSTANT SAVER 2 ACCOUNT Provided by Scottish Widows Bank SUMMARY BOX PLEASE READ THIS SUMMARY BOX BEFORE YOU COMPLETE THE APPLICATION AND THEN KEEP IT FOR YOUR RECORDS. DON T RETURN IT WITH THE APPLICATION.
Medical Savings Account (MSA)
") 2014 MEDICARE ADVANTAGE Medical Savings Account (MSA) BlueSaver MSA Enrollment Application If you have any questions, we re here to help! www.bsneny.com/msa 1-877-258-SHLD (7453) (TTY 1-877-286-5710) October
2014 MEDICARE ADVANTAGE Medical Savings Account (MSA) BlueSaver MSA Enrollment Application If you have any questions, we re here to help! www.bsneny.com/msa 1-877-258-SHLD (7453) (TTY 1-877-286-5710) October
QUICK TIP: Download a Quick Reference Guide from the Resource Center to help you use the PayFlex member website.
 [Date] Dear DTE Energy Retiree, It s our pleasure to welcome you to PayFlex! You re enrolled in a Retiree Reimbursement Account (RRA). Your RRA comes with some great tools to help you manage your account.
[Date] Dear DTE Energy Retiree, It s our pleasure to welcome you to PayFlex! You re enrolled in a Retiree Reimbursement Account (RRA). Your RRA comes with some great tools to help you manage your account.
Cardiology Consultants of Atlanta, P.C N. Decatur Rd. Suite 395, Decatur GA, (404) phone (678) fax
 phone (678) fax") OFFICE POLICIES AND PROCEDURES Thank you for choosing Cardiology Consultants of Atlanta for your cardiovascular care. We realize that you have a choice in medical providers and are pleased that you have
OFFICE POLICIES AND PROCEDURES Thank you for choosing Cardiology Consultants of Atlanta for your cardiovascular care. We realize that you have a choice in medical providers and are pleased that you have
STUDENT LOAN STATEMENT
 STUDENT LOAN STATEMENT 100 Global Drive Suite 800 Warrendale PA 15086 1 Go paperless! Sign up for E-bill or Automated Payments at heartlandecsinet STATEMENT ENCLOSED 107001234561234567891234578901 John
STUDENT LOAN STATEMENT 100 Global Drive Suite 800 Warrendale PA 15086 1 Go paperless! Sign up for E-bill or Automated Payments at heartlandecsinet STATEMENT ENCLOSED 107001234561234567891234578901 John
Tulsa Pediatric Urgent Care Clinic Patient Information Sheet
 Tulsa Pediatric Urgent Care Clinic Patient Information Sheet Please read carefully and fill out form completely Date: Patient (Last) (First) (MI) Date of Birth: Male or Female Home/ Mailing Address: (City)
Tulsa Pediatric Urgent Care Clinic Patient Information Sheet Please read carefully and fill out form completely Date: Patient (Last) (First) (MI) Date of Birth: Male or Female Home/ Mailing Address: (City)
Xofigo (radium Ra 223 dichloride) Injection Access Support for Patients
 Injection Access Support for Patients") Xofigo (radium Ra 223 dichloride) Injection Access Support for Patients Bayer is committed to supporting patient access to Xofigo Xofigo Access Services provides a variety of services to support your access
Xofigo (radium Ra 223 dichloride) Injection Access Support for Patients Bayer is committed to supporting patient access to Xofigo Xofigo Access Services provides a variety of services to support your access
Electronic Funds Transfer - Your Rights and Responsibilities ELECTRONIC FUND TRANSFER AGREEMENT AND DISCLOSURE
 Marblehead Bank 21 Atlantic Avenue - 1 Humphrey Street Marblehead MA 01945 100 Cummings Center - Suite 101-F Beverly MA 01915 781-631-5500 customercare@marblebank.com marblebank.com Electronic Funds Transfer
Marblehead Bank 21 Atlantic Avenue - 1 Humphrey Street Marblehead MA 01945 100 Cummings Center - Suite 101-F Beverly MA 01915 781-631-5500 customercare@marblebank.com marblebank.com Electronic Funds Transfer
Welcome Home! Valid state issued photo identification and a social security card.
 Welcome Home! In order for us to process your application in the quickest manner possible, we will need the following items when you submit your application. Two most recent pay stubs. Income must be equal
Welcome Home! In order for us to process your application in the quickest manner possible, we will need the following items when you submit your application. Two most recent pay stubs. Income must be equal
Health Benefits Simplified
 Health Benefits Simplified What you need to do: What s inside: Review this benefit overview Benefit Highlights 3. 4. Turn in all completed paper forms to your Human Resources Department. Complete the HealthEZpay
Health Benefits Simplified What you need to do: What s inside: Review this benefit overview Benefit Highlights 3. 4. Turn in all completed paper forms to your Human Resources Department. Complete the HealthEZpay
Test card guide. Document version 1.5
 Test card guide mpay24 2.7 Document version 1.5 Contents 1. HISTORY OF THE DOCUMENT... 3 2. GETTING IN TOUCH WITH TECHNICAL SUPPORT...4 3. CHOOSING A TEST CARD...5 4. CARRY OUT A TEST PAYMENT...7 1. HISTORY
Test card guide mpay24 2.7 Document version 1.5 Contents 1. HISTORY OF THE DOCUMENT... 3 2. GETTING IN TOUCH WITH TECHNICAL SUPPORT...4 3. CHOOSING A TEST CARD...5 4. CARRY OUT A TEST PAYMENT...7 1. HISTORY
To enroll in Vantage Medicare Advantage, please provide the following information:
 Medicare Advantage Enrollment Election Form Vantage Medicare Advantage Vantage Health Plan, Inc. 130 DeSiard Street, Suite 300 Monroe, LA 71201 (318) 361-0900 TTY (318) 361-2131 (866) 704-0109 TTY (866)
Medicare Advantage Enrollment Election Form Vantage Medicare Advantage Vantage Health Plan, Inc. 130 DeSiard Street, Suite 300 Monroe, LA 71201 (318) 361-0900 TTY (318) 361-2131 (866) 704-0109 TTY (866)
GlobalHealth Medicare Advantage Plans
 GlobalHealth Medicare Advantage Plans Individual Enrollment Request Form Please contact GlobalHealth if you need information in another language or format. To Enroll in a GlobalHealth Medicare Advantage
GlobalHealth Medicare Advantage Plans Individual Enrollment Request Form Please contact GlobalHealth if you need information in another language or format. To Enroll in a GlobalHealth Medicare Advantage
State Bank Financial State Bank Shelby 4020 Mormon Coulee Road La Crosse WI ELECTRONIC FUND TRANSFER AGREEMENT AND DISCLOSURE
 State Bank Financial State Bank Shelby 4020 Mormon Coulee Road 608.788.0400 ELECTRONIC FUND TRANSFER AGREEMENT AND DISCLOSURE For purposes of this disclosure and agreement the terms "we", "us" and "our"
State Bank Financial State Bank Shelby 4020 Mormon Coulee Road 608.788.0400 ELECTRONIC FUND TRANSFER AGREEMENT AND DISCLOSURE For purposes of this disclosure and agreement the terms "we", "us" and "our"
Standard Insurance Company. SI CTAdp 1 of 49 (5/14)
") Administration Guide for District-Paid Group Insurance Plans Endorsed by California Educators Insurance Plan (CEIP) for California Teachers Association (CTA) Standard Insurance Company SI 14724-CTAdp 1
Administration Guide for District-Paid Group Insurance Plans Endorsed by California Educators Insurance Plan (CEIP) for California Teachers Association (CTA) Standard Insurance Company SI 14724-CTAdp 1
PATIENT REGISTRATION (Please Print) Social Security # Address City State Zip. Address
 Social Security # Address City State Zip. Address") PATIENT REGISTRATION (Please Print) Date Name (Last) (First) (MI) Clinician Social Security # Address City State Zip Email Address Home Phone ( ) Mobile/Alt. Phone ( ) Work Phone ( ) PLEASE IDENTIFY WHICH
PATIENT REGISTRATION (Please Print) Date Name (Last) (First) (MI) Clinician Social Security # Address City State Zip Email Address Home Phone ( ) Mobile/Alt. Phone ( ) Work Phone ( ) PLEASE IDENTIFY WHICH
The Nineteenth Pennsylvania Drilling and Blasting Conference November 14 and 15, 2019
 EXHIBITOR REGISTRATION FORM The Nineteenth Pennsylvania Drilling and Blasting Conference November 14 and 15, 2019 We hereby contract for an exhibit booth at the Nineteenth Pennsylvania Drilling and Blasting
EXHIBITOR REGISTRATION FORM The Nineteenth Pennsylvania Drilling and Blasting Conference November 14 and 15, 2019 We hereby contract for an exhibit booth at the Nineteenth Pennsylvania Drilling and Blasting
The Office of Student Accounts. We re here to help!
 The Office of Student Accounts We re here to help! 2014-2015 Total Undergraduate Direct Cost In State Fall 14 Spring 15 Year Tuition $ 5,281.05 $ 5,281.05 $ 10,562.10 Fees $ 2,231.05 $ 2,231.05* $ 4,462.10
The Office of Student Accounts We re here to help! 2014-2015 Total Undergraduate Direct Cost In State Fall 14 Spring 15 Year Tuition $ 5,281.05 $ 5,281.05 $ 10,562.10 Fees $ 2,231.05 $ 2,231.05* $ 4,462.10
Enrollment Request Form Please contact Stanford Health Care Advantage if you need information in another language or format (Braille).
.") Filling out and returning the enrollment request form is your first step to becoming a Stanford Health Care Advantage (HMO) member. If you and your spouse are both applying, you ll each need to fill out
Filling out and returning the enrollment request form is your first step to becoming a Stanford Health Care Advantage (HMO) member. If you and your spouse are both applying, you ll each need to fill out
IT IS NOT A FREE LEGAL SERVICE.
 Dear Potential Qualified-Income Legal Team (QUILT) Program Client: Using the guidelines presented on the enclosed QUILT Information Sheet, you may determine whether you are eligible to request representation
Dear Potential Qualified-Income Legal Team (QUILT) Program Client: Using the guidelines presented on the enclosed QUILT Information Sheet, you may determine whether you are eligible to request representation
REQUEST FOR PROPOSALS (RFP) Section 125 Flexible Benefits Plan Proposals
 Section 125 Flexible Benefits Plan Proposals") REQUEST FOR PROPOSALS (RFP) Section 125 Flexible Benefits Plan Proposals TITLE: Section 125 Cafeteria Plan Proposals ISSUE DATE: April 18, 2014 DUE DATE: May 9, 2014 DELIVER TO: Erica Setzer, Finance Officer
REQUEST FOR PROPOSALS (RFP) Section 125 Flexible Benefits Plan Proposals TITLE: Section 125 Cafeteria Plan Proposals ISSUE DATE: April 18, 2014 DUE DATE: May 9, 2014 DELIVER TO: Erica Setzer, Finance Officer
Kids R.O.C.K. Summer 2019 Registration Packet
 City of Inver Grove Heights Parks and Recreation Department Kids R.O.C.K. Summer 2019 Registration Packet Please carefully complete all of the following pages. Your child s registration will not be processed
City of Inver Grove Heights Parks and Recreation Department Kids R.O.C.K. Summer 2019 Registration Packet Please carefully complete all of the following pages. Your child s registration will not be processed
Interactive Voice Response (IVR) System
 System") Interactive Voice Response (IVR) System HOME HEALTH & HOSPICE USER GUIDE Table of Contents Introduction 2 Required Information 2 Menu Options 2 Claim Status and Redetermination Status Information 2 NPI,
Interactive Voice Response (IVR) System HOME HEALTH & HOSPICE USER GUIDE Table of Contents Introduction 2 Required Information 2 Menu Options 2 Claim Status and Redetermination Status Information 2 NPI,
BRETT P. TERRIEN, LMHC
 617.470.5404 BRETT@TERRIENLMHC.COM INTAKE INFORMATION Name Date Street Address City/State/Zip Email Marital Status Date of Birth Referred By Phone Work Phone Preferred contact: Phone Work Phone Email Insurance
617.470.5404 BRETT@TERRIENLMHC.COM INTAKE INFORMATION Name Date Street Address City/State/Zip Email Marital Status Date of Birth Referred By Phone Work Phone Preferred contact: Phone Work Phone Email Insurance
COMMISSIONER OF TAXATION CITY OF MAUMEE 400 CONANT STREET PHONE:
 00 CONANT ST. MAUMEE OH 7-00 HOURS MONDAY FRIDAY 8:00 AM :0 PM TELEPHONE: (9) 897-70 FAX: (9) 897-89 WWW.MAUMEE.ORG EMAIL: TAX@MAUMEE.ORG EMPLOYER S MUNICIPAL INCOME TAX WITHHOLDING FORMS FORM MW (MONTHLY
00 CONANT ST. MAUMEE OH 7-00 HOURS MONDAY FRIDAY 8:00 AM :0 PM TELEPHONE: (9) 897-70 FAX: (9) 897-89 WWW.MAUMEE.ORG EMAIL: TAX@MAUMEE.ORG EMPLOYER S MUNICIPAL INCOME TAX WITHHOLDING FORMS FORM MW (MONTHLY
Assurant Clarity SM. Questions about your plan? Benefits Guide. Time Insurance Company John Alden Life Insurance Company. Finally, Original Thinking
 Assurant Clarity SM Benefits Guide Finally, Original Thinking Questions about your plan? Call your Front Desk team at 888.345.6007 Time Insurance Company John Alden Life Insurance Company Assurant Health
Assurant Clarity SM Benefits Guide Finally, Original Thinking Questions about your plan? Call your Front Desk team at 888.345.6007 Time Insurance Company John Alden Life Insurance Company Assurant Health
DDA / DBA CHANGE FORM
 DDA / DBA CHANGE FORM Thank you for notifying us of the recent change to your business. We re happy to process the DDA / DBA change you requested for your payment processing account. The information below
DDA / DBA CHANGE FORM Thank you for notifying us of the recent change to your business. We re happy to process the DDA / DBA change you requested for your payment processing account. The information below
Memorial Hermann Advantage (HMO)
") 2015 APPLICATION Memorial Hermann Advantage (HMO) Memorial Hermann Advantage (HMO) plan Individual Enrollment Form Be sure to read the important disclosures listed on the back before completing this application.
2015 APPLICATION Memorial Hermann Advantage (HMO) Memorial Hermann Advantage (HMO) plan Individual Enrollment Form Be sure to read the important disclosures listed on the back before completing this application.
Instructions for Fax or Applications for Service
 845 Galvez Street, Mandeville, LA 70448-4934 985.626.5132 www.h2osystemsinc.com Instructions for Fax or Email Applications for Service To complete your application for water and sewer services via fax
845 Galvez Street, Mandeville, LA 70448-4934 985.626.5132 www.h2osystemsinc.com Instructions for Fax or Email Applications for Service To complete your application for water and sewer services via fax
THE GEORGE WASHINGTON UNIVERSITY STUDENT ACCOUNT EBILL SOLUTION TERMS AND CONDITIONS
 THE GEORGE WASHINGTON UNIVERSITY STUDENT ACCOUNT EBILL SOLUTION TERMS AND CONDITIONS These Terms and Conditions are designed to provide you with information related to the George Washington University
THE GEORGE WASHINGTON UNIVERSITY STUDENT ACCOUNT EBILL SOLUTION TERMS AND CONDITIONS These Terms and Conditions are designed to provide you with information related to the George Washington University
Helpful Tips to Sign Up Parents
 Helpful Tips to Sign Up Parents Helpful Tips to Sign Up Parents 1. Present EZ-EFT as the expected way to pay. Present EZ-EFT to your customers, not as an option, but as the norm. If EZ-EFT is positioned
Helpful Tips to Sign Up Parents Helpful Tips to Sign Up Parents 1. Present EZ-EFT as the expected way to pay. Present EZ-EFT to your customers, not as an option, but as the norm. If EZ-EFT is positioned
PATIENT INFORMATION Patient Name: Last First Middle Initial. Address. Street or P.O. Box City, State Zip
 PATIENT INFORMATION - 2018 Patient Name: Last First Middle Initial Address: Street or P.O. Box City, State Zip of Birth: / / Race: Gender: Male Female Social Security #: Marital Status: Single Married
PATIENT INFORMATION - 2018 Patient Name: Last First Middle Initial Address: Street or P.O. Box City, State Zip of Birth: / / Race: Gender: Male Female Social Security #: Marital Status: Single Married
BCN Advantage HMO-POS Application
 BCN Advantage HMO-POS Application 2018 Employer Group/Union Enrollment Form (Coverage effective 2018) 1 Complete the following information to enroll in BCN Advantage HMO-POS. Name of employer group/union
BCN Advantage HMO-POS Application 2018 Employer Group/Union Enrollment Form (Coverage effective 2018) 1 Complete the following information to enroll in BCN Advantage HMO-POS. Name of employer group/union
The best way to bank just got better.
 The best way to bank just got better. New, enhanced mobile and online banking services are coming. Details inside. customersbank.com 2 A letter from our President & COO Dear Neighbor: We are always striving
The best way to bank just got better. New, enhanced mobile and online banking services are coming. Details inside. customersbank.com 2 A letter from our President & COO Dear Neighbor: We are always striving
Patient Guide to Billing and Insurance
 Patient Guide to Billing and Insurance Patient Account Payment Policies December 2017 Lexington Clinic Central Business Office Payment Policies Customer service...2 Check-in...2 Plan participation, network
Patient Guide to Billing and Insurance Patient Account Payment Policies December 2017 Lexington Clinic Central Business Office Payment Policies Customer service...2 Check-in...2 Plan participation, network
2017 Medicare Advantage Prescription Drug Plan (MAPD) Individual Enrollment Form
 Individual Enrollment Form") 2017 Medicare Advantage Prescription Drug Plan (MAPD) Individual Enrollment Form Please contact SummaCare if you need information in a different format. To enroll in SummaCare, please provide the following
2017 Medicare Advantage Prescription Drug Plan (MAPD) Individual Enrollment Form Please contact SummaCare if you need information in a different format. To enroll in SummaCare, please provide the following
NC Independent Living Attendant Sample Forms Packet
 NC Independent Living Attendant Sample Forms Packet Contents: Attendant Sample Forms Checklist Attendant Sample Forms Please use the enclosed sample forms to fill out the forms in the Attendant Packet.
NC Independent Living Attendant Sample Forms Packet Contents: Attendant Sample Forms Checklist Attendant Sample Forms Please use the enclosed sample forms to fill out the forms in the Attendant Packet.
Entity Account Application US High Yield Corporate Bond Fund
 >> Mail to: Muzinich Funds c/o U.S. Bank Global Fund Services PO Box 701 Entity Account Application US High Yield Corporate Bond Fund Overnight Express Mail To: Muzinich Funds c/o U.S. Bank Global Fund
>> Mail to: Muzinich Funds c/o U.S. Bank Global Fund Services PO Box 701 Entity Account Application US High Yield Corporate Bond Fund Overnight Express Mail To: Muzinich Funds c/o U.S. Bank Global Fund
Entity Account Application Please do not use this form for IRA accounts
 Entity Account Application Please do not use this form for IRA accounts >> Mail to: Steben Managed Futures Strategy Fund c/o U.S. Bank Global Fund Services P.O. Box 701 Milwaukee, WI 53201-0701 In compliance
Entity Account Application Please do not use this form for IRA accounts >> Mail to: Steben Managed Futures Strategy Fund c/o U.S. Bank Global Fund Services P.O. Box 701 Milwaukee, WI 53201-0701 In compliance
ELECTRONIC FUND TRANSFER DISCLOSURE AND AGREEMENT. Martha's Vineyard Savings Bank 78 Main Street Edgartown, MA
 ELECTRONIC FUND TRANSFER DISCLOSURE AND AGREEMENT Martha's Vineyard Savings Bank 78 Main Street 508-627-4266 For purposes of this disclosure and agreement the terms "we", "us" and "our" refer to Martha's
ELECTRONIC FUND TRANSFER DISCLOSURE AND AGREEMENT Martha's Vineyard Savings Bank 78 Main Street 508-627-4266 For purposes of this disclosure and agreement the terms "we", "us" and "our" refer to Martha's
Reinier Van Coevorden, M.D. RVC Medical th Ave NW, suite 204 Issaquah, WA 98027
 Reinier Van Coevorden, M.D. RVC Medical 1301 4 th Ave NW, suite 204 Issaquah, WA 98027 Concierge Practice Patient Agreement You have decided to participate in concierge practice with Dr. Van Coevorden
Reinier Van Coevorden, M.D. RVC Medical 1301 4 th Ave NW, suite 204 Issaquah, WA 98027 Concierge Practice Patient Agreement You have decided to participate in concierge practice with Dr. Van Coevorden
Car Spa, Inc. Fleet Account Application
 Car Spa, Inc. Fleet Account Application Enclosed: Program Info Application Frequently Asked Questions Sample Reports Instructions: 1. Please read all information regarding the Fleet Account 2. Fill out
Car Spa, Inc. Fleet Account Application Enclosed: Program Info Application Frequently Asked Questions Sample Reports Instructions: 1. Please read all information regarding the Fleet Account 2. Fill out
NexPoint Real Estate Strategies Fund
 To establish an account, the minimum initial investment is $500. Once your account is established, the minimum for additional investments is $50. If you have any questions or need any help filling out
To establish an account, the minimum initial investment is $500. Once your account is established, the minimum for additional investments is $50. If you have any questions or need any help filling out
Activity Summary. New Balance $ Minimum Payment Due $ Payment Due Date 02/03/2016. Reward Points. January 2016 Statement
 Page 1 of 4 Open Date: 12/08/2015 Closing Date: 01/07/2016 Account: 4798 5100 5300 3857 Visa Business Bonus Rewards Card BATTLE ROCK CHARTER New Balance $117.31 Minimum Payment Due $17.00 Payment Due Date
Page 1 of 4 Open Date: 12/08/2015 Closing Date: 01/07/2016 Account: 4798 5100 5300 3857 Visa Business Bonus Rewards Card BATTLE ROCK CHARTER New Balance $117.31 Minimum Payment Due $17.00 Payment Due Date
Government Transaction Dispute Office Guide
 Government Transaction Dispute Office Guide Treasury and Trade Solutions Government Transaction Dispute Office Guide Table of Contents Table of Contents I. General Overview...2 V. Electronic Access System...7
Government Transaction Dispute Office Guide Treasury and Trade Solutions Government Transaction Dispute Office Guide Table of Contents Table of Contents I. General Overview...2 V. Electronic Access System...7
SCHOOL EASYPAY FEE PAYMENT OPTIONS & PAYMENT METHODS
 SCHOOL EASYPAY FEE PAYMENT OPTIONS & PAYMENT METHODS After much thought and consideration in regards to the school fees procedure, we are excited to provide you with some information about the mutually
SCHOOL EASYPAY FEE PAYMENT OPTIONS & PAYMENT METHODS After much thought and consideration in regards to the school fees procedure, we are excited to provide you with some information about the mutually
Individual Enrollment Request Form
 SE Please contact Network Health Medicare Advantage Plans To Enroll in a Network Health Medicare Advantage Plan, Please Provide the Following Information. Please check which plan you want to enroll in.
SE Please contact Network Health Medicare Advantage Plans To Enroll in a Network Health Medicare Advantage Plan, Please Provide the Following Information. Please check which plan you want to enroll in.
ELECTRONIC FUND TRANSFERS YOUR RIGHTS AND RESPONSIBILITIES
 ELECTRONIC FUND TRANSFERS YOUR RIGHTS AND RESPONSIBILITIES The Electronic Fund Transfers we are capable of handling for consumers are indicated below, some of which may not apply to your account. Some
ELECTRONIC FUND TRANSFERS YOUR RIGHTS AND RESPONSIBILITIES The Electronic Fund Transfers we are capable of handling for consumers are indicated below, some of which may not apply to your account. Some
Aetna Group Medicare Advantage Frequently Asked Questions
 Aetna Group Medicare Advantage Frequently Asked Questions Providers & the Aetna Network 1. How do I find out if my providers are in the Aetna Medicare Advantage Network or if they accept the Aetna plan?
Aetna Group Medicare Advantage Frequently Asked Questions Providers & the Aetna Network 1. How do I find out if my providers are in the Aetna Medicare Advantage Network or if they accept the Aetna plan?
National Multiple Sclerosis Society Marathon Strides Against MS (MSAMS) 2010 Boston Marathon Charity Program
 2010 Boston Marathon Charity Program") Send completed applications to: Nancy Dlugoenski National MS Society 60 Federal Street Millers Falls, MA 01349 National Multiple Sclerosis Society Marathon Strides Against MS (MSAMS) 2010 Boston Marathon
Send completed applications to: Nancy Dlugoenski National MS Society 60 Federal Street Millers Falls, MA 01349 National Multiple Sclerosis Society Marathon Strides Against MS (MSAMS) 2010 Boston Marathon
Entity Account Application Please do not use this form for IRA accounts
 Entity Account Application Please do not use this form for IRA accounts >> Mail to: Bridges Investment Fund c/o U.S. Bank Global Fund Services PO Box 701 Milwaukee, WI 53201-0701 Milwaukee, WI 53202-5207
Entity Account Application Please do not use this form for IRA accounts >> Mail to: Bridges Investment Fund c/o U.S. Bank Global Fund Services PO Box 701 Milwaukee, WI 53201-0701 Milwaukee, WI 53202-5207
ADVANTAGE PLAN MEMBERSHIP Enrollment Form
 Return Form to: Your Nearest Urgent Clinics Medical Care Location or Email: franklin@ihcadvantage.com Phone: 832-661-2022 www.ihcadvantage.com ADVANTAGE PLAN MEMBERSHIP Enrollment Form Primary Member:
Return Form to: Your Nearest Urgent Clinics Medical Care Location or Email: franklin@ihcadvantage.com Phone: 832-661-2022 www.ihcadvantage.com ADVANTAGE PLAN MEMBERSHIP Enrollment Form Primary Member:
County: State: ZIP: Address: Billing Address for Premium Notices (complete only if different from above).
.") Application Form Complete and sign the application. A-425 P.O. Box 6170, Columbia, SC 29260-6170 Blue Option benefits are provided in network only. No benefits are provided for services received out of
Application Form Complete and sign the application. A-425 P.O. Box 6170, Columbia, SC 29260-6170 Blue Option benefits are provided in network only. No benefits are provided for services received out of
Champaign-U rbana, Illinois
 PRESENTS 2019 Health & Fitness E X P O Thursday, April 25, 2019 4:00 p.m. 8:00 p.m. Friday, April 26, 2019 10:00 a.m. 7:00 p.m. Activities and Recreation Center, University of Illinois Campus SPONSORED
PRESENTS 2019 Health & Fitness E X P O Thursday, April 25, 2019 4:00 p.m. 8:00 p.m. Friday, April 26, 2019 10:00 a.m. 7:00 p.m. Activities and Recreation Center, University of Illinois Campus SPONSORED
2018 HEALTH CARE FSA PROGRAM WITH PAYFLEX (AETNA)
") 2018 HEALTH CARE FSA PROGRAM WITH PAYFLEX (AETNA) Whether you are newly enrolling for 2018 or re-enrolling for 2018, you ll find the information here very helpful in understanding your FSA plan and the
2018 HEALTH CARE FSA PROGRAM WITH PAYFLEX (AETNA) Whether you are newly enrolling for 2018 or re-enrolling for 2018, you ll find the information here very helpful in understanding your FSA plan and the
Financial Policy Guidelines
 Financial Policy Guidelines Welcome to The Women s Group of Northwestern. We strive to provide you with excellent medical care and our goal is to make your visit as convenient as possible. Please read
Financial Policy Guidelines Welcome to The Women s Group of Northwestern. We strive to provide you with excellent medical care and our goal is to make your visit as convenient as possible. Please read
Entity Account Application
 >> Mail to: Nicholas Funds c/o U.S. Bank Global Fund Services PO Box 701 Milwaukee, WI 53201-0701 Entity Account Application Please do not use this form for IRA accounts In compliance with the USA PATRIOT
>> Mail to: Nicholas Funds c/o U.S. Bank Global Fund Services PO Box 701 Milwaukee, WI 53201-0701 Entity Account Application Please do not use this form for IRA accounts In compliance with the USA PATRIOT
Checklist. New Employee Payroll Packet Print pages which require responses AND the I-9 for completion and submission
 New Employee Payroll Packet Student Workers, Work Study, and Temporary Employees Welcome to Great Falls College Montana State University! Listed below is a checklist with items that need to be completed
New Employee Payroll Packet Student Workers, Work Study, and Temporary Employees Welcome to Great Falls College Montana State University! Listed below is a checklist with items that need to be completed
* * Billing Notice. Total Amount Due $ Statement Date: July 10, OneUSG Connect - Benefits connect-benefits.usg.
 Statement Date: July 10, 2017 V000001 TEST L. DBP BILL 01 DO NOT MAIL JACKSON GA 30233 OneUSG Connect - Benefits connect-benefits.usg.edu OneUSG Connect - Benefits Call Center 1-844-5USGBEN (587-4236)
Statement Date: July 10, 2017 V000001 TEST L. DBP BILL 01 DO NOT MAIL JACKSON GA 30233 OneUSG Connect - Benefits connect-benefits.usg.edu OneUSG Connect - Benefits Call Center 1-844-5USGBEN (587-4236)
Return Stock Transfer forms and Account Information Change Forms to Mastercard Shareholder Services at the following addresses:
 Dear Mastercard Class B Stockholder: Enclosed is the form you requested. Please complete the form in its entirety and return as directed below: Return Stock Transfer forms and Account Information Change
Dear Mastercard Class B Stockholder: Enclosed is the form you requested. Please complete the form in its entirety and return as directed below: Return Stock Transfer forms and Account Information Change
Dr. Sarah Y. Vinson s Practice Policies
 Dr. Sarah Y. Vinson s Practice Policies FEE SCHEDULE: $230 50 minute psychotherapy and/or psychopharmacology appt. $450 2 hour initial intake appt. $155 30 minute phone, Skype or in-person appt.; $125
Dr. Sarah Y. Vinson s Practice Policies FEE SCHEDULE: $230 50 minute psychotherapy and/or psychopharmacology appt. $450 2 hour initial intake appt. $155 30 minute phone, Skype or in-person appt.; $125
Customized Delivery Solutions Mail Order
 Mail Order Welcome to Apogee Bio Pharm s Mail Order Service! Our program is designed for members who are taking medications on an ongoing basis, such as medication to reduce blood pressure or to treat
Mail Order Welcome to Apogee Bio Pharm s Mail Order Service! Our program is designed for members who are taking medications on an ongoing basis, such as medication to reduce blood pressure or to treat
STUDENT FINANCIALS 101 MONEY MATTERS
 STUDENT FINANCIALS 101 MONEY MATTERS STUDENT FINANCIAL AGREEMENT Before a student can register, the student must e-sign a Student Financial Agreement. This is, in general, a promise to pay for all charges
STUDENT FINANCIALS 101 MONEY MATTERS STUDENT FINANCIAL AGREEMENT Before a student can register, the student must e-sign a Student Financial Agreement. This is, in general, a promise to pay for all charges
Regular Mailing Address Third Avenue Funds. P. O. Box 9802 Providence, RI
 THIRD AVENUE FUNDS Please send your signed and completed application to Third Avenue Funds in the enclosed postage-paid business reply envelope. Please call 1-800-443-1021 with any questions, Monday through
THIRD AVENUE FUNDS Please send your signed and completed application to Third Avenue Funds in the enclosed postage-paid business reply envelope. Please call 1-800-443-1021 with any questions, Monday through