Provider Orientation. Or togethercchp.org
|
|
|
- Marjory Pearson
- 6 years ago
- Views:
Transcription

1 Provider Orientation Or togethercchp.org
2 What is Together with Children s Community Health Plan? A local health plan for individuals and families Affiliated with Children s Hospital of Wisconsin Plans for Everyone not just kids Coverage sold On Exchange and Off Exchange Offers access to high-quality health care in Southeast Wisconsin An Exclusive Provider Organization (EPO)

3 Service Area Together with CCHP is offered in the following counties: Milwaukee Washington Ozaukee Waukesha Kenosha Racine
4 Infrastructure/Operations Administrative Services Agreement with UPMC Health Plan for provider service and claims. Why UPMC Health Plan they are provider owned, experience with coverage on and off Exchange.
5 Infrastructure/Operations CCHP is responsible for: Credentialing Case Management Complaints and Appeals Provider Contracting & Relations Quality Improvement Sales and Broker support Utilization Management

6 Provider Network Please note that the Together with CCHP provider network is different from our Medicaid provider network

7 Together ID Card - front

8 Together ID Card - back

9 Together Plan Designs
10 Together Benefits Bronze, Silver, Silver Standard and Gold Plans Preventive Care Coverage Pediatric Routine Vision Prescription Drug Coverage Healthy Mom, Health Baby Provider Incentive Referrals to in-network Specialists not required Care outside of the provider network is not covered with the exception of urgent and emergency care Members receive an Evidence of Coverage which is located on our web site under Members tab
11 Pediatric Vision Avesis (Pediatric Vision only) Annual eye exam included with no cost sharing Benefit includes lenses (contacts or glasses) and frames Customer Service:


12 Prescription Drug Benefits Express Scripts Broad network of pharmacies to choose from, including Walgreens and CVS Prescription drug formulary available online Mandatory generic drug substitution Convenient mail order available $0 preventive prescriptions
13 Prescription Drug Benefits To see if the drug being prescribed is covered, pharmacists and clinical staff can: Call Together with CCHP Pharmacy Services at Refer to the Together with CCHP Pharmacy Benefit Guide which can be found on the web site at togethercchp.org/formulary

14 Together Pharmacy Benefit Guide
15 Notifications/Prior Authorization Prior authorization list available at Must submit a prior authorization request online Use your current CCHP login No retro authorizations Call with questions or refer to the Provider Manual

16

17 Provider Portal
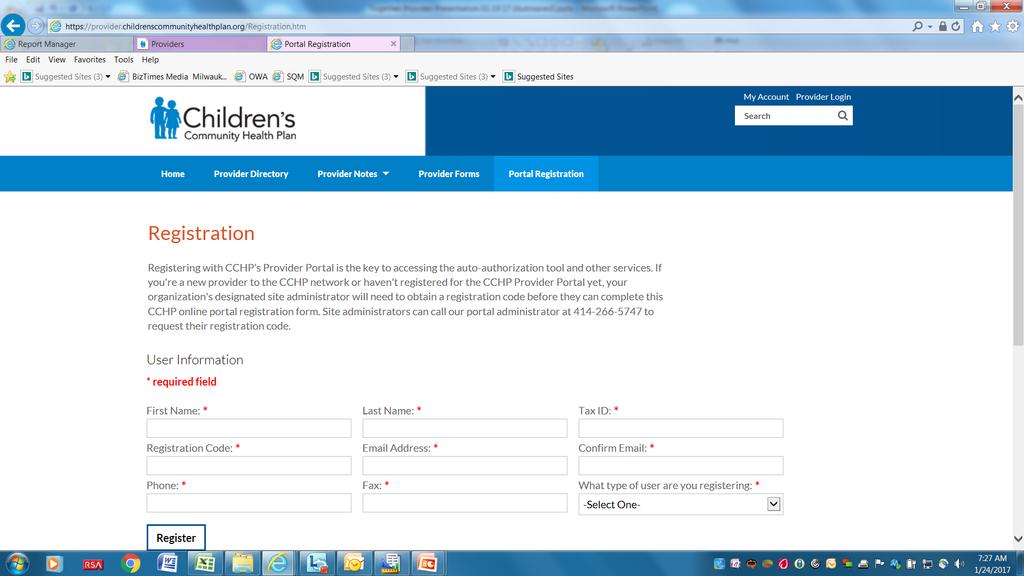
18 Registration Page

19 Provider Portal Login Page

20 Provider Portal

21 Together Provider Portal

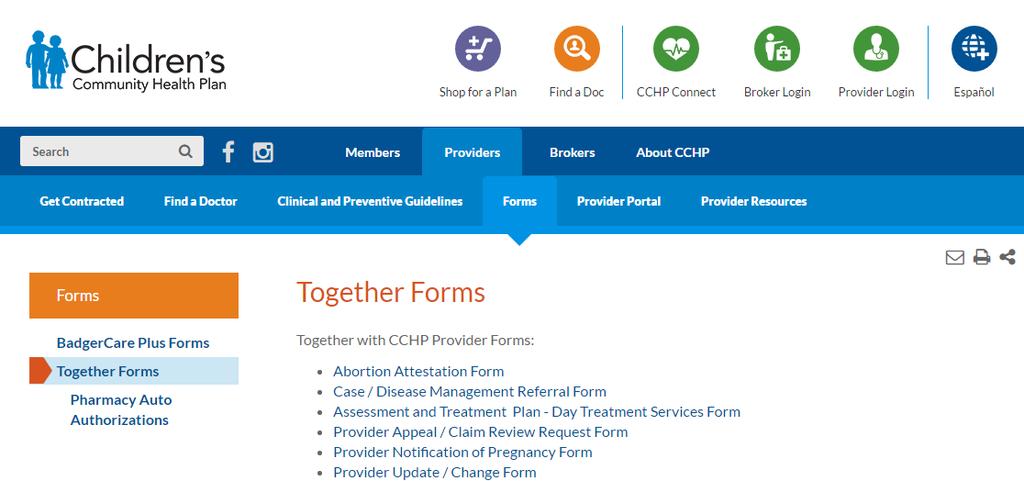
22 Provider Forms
23
24 Claim Submission File claims timely Bill on appropriate claim forms Payment made within 30 days on clean claims Hand written claims not accepted
25 Claims Submission Electronic Claims Preferred: Please submit claims electronically to Together with CCHP EDI Payer ID#: 251CC Electronic Remittance Advice (ERA) and Electronic Fund Transfers (EFT) are available forms available on web site Paper Claims: Mailing Address: Together with CCHP P.O. Box Pittsburgh, PA
26 Where to call with claims questions? For questions regarding claims and Explanation of Payment (EOP), please contact Together with CCHP Provider Service at
27 Claim Appeals Please call Provider Services to discuss claim denials prior to submitting a written appeal. To file a written appeal: Complete the Together with CCHP Provider Appeal Form, which is available on the Provider Forms page at togethercchp.org Submit the form, along with copies of any supporting documentation to: Together with CCHP ATTN: Appeals Department P.O. Box 1997, MS 6280 Milwaukee, WI
28 Grace Period If member is terminated due to lack of payment Claims are paid for days 1-30 Claims paid during days days will be recouped
29 Provider Updates For Provider demographic changes complete the Provider Update/Change Form available on our web site. Examples: TIN change Address change Billing address change

30 Together with CCHP Reference Guide
31 & Contact Information Send us your and contact information for future updates and news. Send s to
32 Questions?
Prior Authorization All non-emergent services rendered by non-contracted providers require prior authorization, unless specified otherwise.
 Prior Authorization All non-emergent services rendered by non-contracted providers require prior authorization, unless specified otherwise. Abortions, Hysterectomies and Sterilizations Ambulance Emergency
Prior Authorization All non-emergent services rendered by non-contracted providers require prior authorization, unless specified otherwise. Abortions, Hysterectomies and Sterilizations Ambulance Emergency
UnitedHealthcare Community Plan of Missouri
 UnitedHealthcare Community Plan of Missouri Agenda UnitedHealthcare Community Plan of Missouri Member Eligibility and Benefits Notification and Prior Authorization Claims Management Care Provider Resources
UnitedHealthcare Community Plan of Missouri Agenda UnitedHealthcare Community Plan of Missouri Member Eligibility and Benefits Notification and Prior Authorization Claims Management Care Provider Resources
Plan Year 2020 Medical Plan Comparison
 Plan Year 2020 Medical Plan Comparison MEDICAL Service Areas Global Global Statewide Urgent and Emergent Statewide Urgent and Emergent Annual (medical and prescription combined) $1,500 Individual $3,000
Plan Year 2020 Medical Plan Comparison MEDICAL Service Areas Global Global Statewide Urgent and Emergent Statewide Urgent and Emergent Annual (medical and prescription combined) $1,500 Individual $3,000
Prior Authorization All non-emergent services rendered by non-contracted providers require prior authorization, unless specified otherwise.
 Prior Authorization All non-emergent services rendered by non-contracted providers require prior authorization, unless specified otherwise. Abortions, Hysterectomies and Sterilizations Ambulance Emergency
Prior Authorization All non-emergent services rendered by non-contracted providers require prior authorization, unless specified otherwise. Abortions, Hysterectomies and Sterilizations Ambulance Emergency
Housekeeping. Link Participant ID with Audio. Mute your line UNMUTED. Raise your hand with questions
 Housekeeping Link Participant ID with Audio If your Participant ID has not been entered, dial #ParticipantID#. EXAMPLE: Participant ID is 16, then enter #16#. Mute your line UNMUTED MUTED OTHER MUTE OPTIONS
Housekeeping Link Participant ID with Audio If your Participant ID has not been entered, dial #ParticipantID#. EXAMPLE: Participant ID is 16, then enter #16#. Mute your line UNMUTED MUTED OTHER MUTE OPTIONS
Douglas County Community Provider Outreach January 2018
 Douglas County Community Provider Outreach January 2018 Douglas County Gold Rx Plan Changes Description 2017 In-Network / Out-of-Network 2018 In-Network / Out-of-Network Gold Rx Premium $180 $189 Ambulance
Douglas County Community Provider Outreach January 2018 Douglas County Gold Rx Plan Changes Description 2017 In-Network / Out-of-Network 2018 In-Network / Out-of-Network Gold Rx Premium $180 $189 Ambulance
DEAN ADVANTAGE MANUAL
 DEAN ADVANTAGE MANUAL Dean Health Plan Dean Advantage Manual Revised 12/2017 1 TABLE OF CONTENTS WHAT IS DEAN ADVANTAGE?... 2 SUMMARY OF EXCLUSIONS... 3 AUTOMATIC ASSIGNMENT OF PRIMARY CARE PRACTITIONER...
DEAN ADVANTAGE MANUAL Dean Health Plan Dean Advantage Manual Revised 12/2017 1 TABLE OF CONTENTS WHAT IS DEAN ADVANTAGE?... 2 SUMMARY OF EXCLUSIONS... 3 AUTOMATIC ASSIGNMENT OF PRIMARY CARE PRACTITIONER...
Medicaid Modernization: How to Build a Relationship with an MCO
 Medicaid Modernization: How to Build a Relationship with an MCO 2015/2016 Agenda Building a positive relationship with providers is critical to a smooth transition to managed care. We are here to help
Medicaid Modernization: How to Build a Relationship with an MCO 2015/2016 Agenda Building a positive relationship with providers is critical to a smooth transition to managed care. We are here to help
Rocky Mountain View 2015 INDIVIDUAL & FAMILY PLANS. MK645-A-R11/13/14þ
 Rocky Mountain View 2015 INDIVIDUAL & FAMILY PLANS MK645-A-R11/13/14þ WE UNDERSTAND COLORADO. WE UNDERSTAND YOU. Rocky Mountain Health Plans, a Colorado-based, t-for-profit health plan, understands the
Rocky Mountain View 2015 INDIVIDUAL & FAMILY PLANS MK645-A-R11/13/14þ WE UNDERSTAND COLORADO. WE UNDERSTAND YOU. Rocky Mountain Health Plans, a Colorado-based, t-for-profit health plan, understands the
Klamath County Community Provider Outreach January 2018
 Klamath County Community Provider Outreach January 2018 Klamath County Gold Rx Plan Changes (In-network/Out-of-network) Description 2017 2018 Gold Rx Premium $180 $189 Ambulance $100 $150 Emergency $65
Klamath County Community Provider Outreach January 2018 Klamath County Gold Rx Plan Changes (In-network/Out-of-network) Description 2017 2018 Gold Rx Premium $180 $189 Ambulance $100 $150 Emergency $65
Cenpatico South Carolina Frequently Asked Questions (FAQ)
") Cenpatico South Carolina Frequently Asked Questions (FAQ) GENERAL Who is Cenpatico? Cenpatico, a division of Centene Corporation, is one of the nation s most experienced behavioral health companies providing
Cenpatico South Carolina Frequently Asked Questions (FAQ) GENERAL Who is Cenpatico? Cenpatico, a division of Centene Corporation, is one of the nation s most experienced behavioral health companies providing
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services. Coverage Period: Beginning On or After 1/1/2019
 Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: Beginning On or After 1/1/2019 Silver 70 Off Exchange Trio HMO Coverage for: Individual + Family
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: Beginning On or After 1/1/2019 Silver 70 Off Exchange Trio HMO Coverage for: Individual + Family
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services. Coverage Period: Beginning On or After 1/1/2018
 Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: Beginning On or After 1/1/2018 Silver Full PPO 1700/55 OffEx Coverage for: Individual + Family
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: Beginning On or After 1/1/2018 Silver Full PPO 1700/55 OffEx Coverage for: Individual + Family
Caring for Your Small Business Small Group Plans for Groups with 1 to 100 Employees
 Caring for Your Small Business 2019 Small Group Plans for Groups with 1 to 100 Employees EmblemHealth offers small group plans with the needs and budgets of small businesses in mind. Each plan offers quality
Caring for Your Small Business 2019 Small Group Plans for Groups with 1 to 100 Employees EmblemHealth offers small group plans with the needs and budgets of small businesses in mind. Each plan offers quality
Introduction to UnitedHealthcare Community Plan of California/Medi-Cal
 Introduction to UnitedHealthcare Community Plan of California/Medi-Cal Welcome/Agenda: Mission/Vision UnitedHealthcare Community Plan of California/Medi-Cal Member Eligibility and Benefits Notification
Introduction to UnitedHealthcare Community Plan of California/Medi-Cal Welcome/Agenda: Mission/Vision UnitedHealthcare Community Plan of California/Medi-Cal Member Eligibility and Benefits Notification
For non-preferred providers: $14,300 Person/$28,600 Family. Doesn t apply to preventive care services or glasses for children.
 WPS Preferred Plan: Bronze 7150 Coverage Period: 1/1/2017 12/31/2017 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Single/Family Plan Type: PPO This is only a summary.
WPS Preferred Plan: Bronze 7150 Coverage Period: 1/1/2017 12/31/2017 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Single/Family Plan Type: PPO This is only a summary.
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services. Coverage Period: Beginning On or After 1/1/2018
 Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: Beginning On or After 1/1/2018 Bronze Full PPO Savings 4300/40% OffEx Coverage for: Individual
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: Beginning On or After 1/1/2018 Bronze Full PPO Savings 4300/40% OffEx Coverage for: Individual
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services. Coverage Period: Beginning On or After 1/1/2018
 Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: Beginning On or After 1/1/2018 Gold Trio HMO 500/35 OffEx Coverage for: Individual + Family
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: Beginning On or After 1/1/2018 Gold Trio HMO 500/35 OffEx Coverage for: Individual + Family
Paramount Advantage. Facility Orientation
 Paramount Advantage Facility Orientation Overview Paramount Advantage Toledo-based Ohio Managed Care Plan (MCP) Established 1993 Provides health care coverage to Covered Families and Children (CFC) Aged,
Paramount Advantage Facility Orientation Overview Paramount Advantage Toledo-based Ohio Managed Care Plan (MCP) Established 1993 Provides health care coverage to Covered Families and Children (CFC) Aged,
$1,500 Individual/$3,000 Family for participating providers. $3,000 Individual/$6,000. Important Questions Answers Why this Matters:
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.calcpahealth.com or by calling 1-877-480-7923. Important
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.calcpahealth.com or by calling 1-877-480-7923. Important
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services. Coverage Period: Beginning On or After 1/1/2018
 Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: Beginning On or After 1/1/2018 Blue Shield Gold 80 PPO 0/25 + Child Dental Coverage for: Individual
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: Beginning On or After 1/1/2018 Blue Shield Gold 80 PPO 0/25 + Child Dental Coverage for: Individual
CARING FOR YOUR SMALL BUSINESS. Off-Exchange 2018 Plans and Services for Groups With Up to 100 Employees
 CARING FOR YOUR SMALL BUSINESS Off-Exchange 2018 Plans and Services for Groups With Up to 100 Employees SMALL GROUP PLANS AT A GLANCE EmblemHealth offers small group plans with the needs and budgets of
CARING FOR YOUR SMALL BUSINESS Off-Exchange 2018 Plans and Services for Groups With Up to 100 Employees SMALL GROUP PLANS AT A GLANCE EmblemHealth offers small group plans with the needs and budgets of
ElevateHealth Gold 1000 Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services
 New Hampshire ElevateHealth Gold 1000 Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/2018 12/31/2018 Coverage for: Individual + Family
New Hampshire ElevateHealth Gold 1000 Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/2018 12/31/2018 Coverage for: Individual + Family
For non-participating providers: $11,000 Person/$22,000 Family. Doesn t apply to preventive care. Are there other deductibles for specific services?
 Arise Health Plan: POS HDHP Bronze 5500 Coverage Period: 1/1/2017 12/31/2017 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Single/Family Plan Type: POS This is only
Arise Health Plan: POS HDHP Bronze 5500 Coverage Period: 1/1/2017 12/31/2017 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Single/Family Plan Type: POS This is only
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services
 Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: Beginning On or After 1/1/2018 Gold 80 HMO Trio Coverage for: Individual + Family Plan Type:
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: Beginning On or After 1/1/2018 Gold 80 HMO Trio Coverage for: Individual + Family Plan Type:
Ambetter of Arkansas. Arkansas Medical Society 12 th Annual Insurance Conference October 1, /5/2015
 Ambetter of Arkansas Arkansas Medical Society 12 th Annual Insurance Conference October 1, 2015 AGENDA 1. Verification of Eligibility 2. Prior Authorization 3. Claims Submission 4. PaySpan 5. Ambetter
Ambetter of Arkansas Arkansas Medical Society 12 th Annual Insurance Conference October 1, 2015 AGENDA 1. Verification of Eligibility 2. Prior Authorization 3. Claims Submission 4. PaySpan 5. Ambetter
THIRD QUARTER 2018 SMALL GROUP PRODUCT PORTFOLIO
 THIRD QUARTER 2018 SMALL GROUP PRODUCT PORTFOLIO A 1 2 Benefi ts of BlueShield Innovative plan designs Expanded (EX) network plans Enhanced network access with POS locally and PPO for out-of-area Available
THIRD QUARTER 2018 SMALL GROUP PRODUCT PORTFOLIO A 1 2 Benefi ts of BlueShield Innovative plan designs Expanded (EX) network plans Enhanced network access with POS locally and PPO for out-of-area Available
Coverage for: Individual + Family Plan Type: PPO
 Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 09/01/2018-12/31/2018 Venezia Transport Service: High Plan Coverage for: Individual + Family
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 09/01/2018-12/31/2018 Venezia Transport Service: High Plan Coverage for: Individual + Family
Important Questions Answers Why this Matters:
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.crystalrunhp.com or by calling 1-844-638-6506. Important
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.crystalrunhp.com or by calling 1-844-638-6506. Important
2016 COPAY AND DEDUCTIBLE PLANS
 2016 COPAY AND DEDUCTIBLE PLANS Health Insurance for Individuals & Families Welcome to PreferredOne PreferredOne.com Your Health, Your Choice, Many Options At PreferredOne, our name says it all you and
2016 COPAY AND DEDUCTIBLE PLANS Health Insurance for Individuals & Families Welcome to PreferredOne PreferredOne.com Your Health, Your Choice, Many Options At PreferredOne, our name says it all you and
FIRST QUARTER 2018 SMALL GROUP PRODUCT PORTFOLIO
 FIRST QUARTER 2018 SMALL GROUP PRODUCT PORTFOLIO Benefits of BlueShield Innovative plan designs Expanded (EX) network plans Enhanced network access with POS locally and PPO for out-of-area Available for
FIRST QUARTER 2018 SMALL GROUP PRODUCT PORTFOLIO Benefits of BlueShield Innovative plan designs Expanded (EX) network plans Enhanced network access with POS locally and PPO for out-of-area Available for
Johns Hopkins HealthCare LLC
 Johns Hopkins HealthCare LLC Johns Hopkins Employer Health Programs (EHP) Presented by: by: Johns Hopkins HealthCare Provider Relations Department 11/14/2018 Agenda Welcome About JHHC Provider Website
Johns Hopkins HealthCare LLC Johns Hopkins Employer Health Programs (EHP) Presented by: by: Johns Hopkins HealthCare Provider Relations Department 11/14/2018 Agenda Welcome About JHHC Provider Website
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services. Coverage Period: Beginning On or After 1/1/2018
 Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: Beginning On or After 1/1/2018 Platinum Full PPO 0/10 OffEx Coverage for: Individual + Family
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: Beginning On or After 1/1/2018 Platinum Full PPO 0/10 OffEx Coverage for: Individual + Family
$ 0 Does not apply to Vision benefit. Important Questions Answers Why this Matters: What is the overall deductible?
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.vsp.com or by calling 1-800-877-7195. Important Questions
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.vsp.com or by calling 1-800-877-7195. Important Questions
Medicare Advantage HMO plans
 2018 Medicare Advantage HMO plans Promise Rx (HMO-POS) Surety Rx (HMO-POS) Medicare coverage that works with and for you Y0117_MC-778-2822-C-10-17 approved Why choose a plan from Security Health Plan?
2018 Medicare Advantage HMO plans Promise Rx (HMO-POS) Surety Rx (HMO-POS) Medicare coverage that works with and for you Y0117_MC-778-2822-C-10-17 approved Why choose a plan from Security Health Plan?
Frequently Asked Questions
 Frequently Asked Questions Q. What is an Open Delivery System? A. An Open Delivery System provides access to a host of affiliated providers with admitting privileges at various HAP-contracted hospitals
Frequently Asked Questions Q. What is an Open Delivery System? A. An Open Delivery System provides access to a host of affiliated providers with admitting privileges at various HAP-contracted hospitals
Standard Bronze Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services
 Massachusetts Standard Bronze Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/2018 12/31/2018 Coverage for: Individual + Family Plan Type:
Massachusetts Standard Bronze Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/2018 12/31/2018 Coverage for: Individual + Family Plan Type:
You don t have to meet deductibles for specific services.
 Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/2019 12/31/2019 Highmark Delaware: Health Savings Embedded Blue EPO Silver 4450 HSA Coverage
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/2019 12/31/2019 Highmark Delaware: Health Savings Embedded Blue EPO Silver 4450 HSA Coverage
Plan Comparison Checklist
 Plan Comparison Checklist Date: The chart below should serve as a comprehensive guide for users when comparing health insurance plans during open enrollment. This chart is also used by Compass case managers
Plan Comparison Checklist Date: The chart below should serve as a comprehensive guide for users when comparing health insurance plans during open enrollment. This chart is also used by Compass case managers
Rocky Mountain View INDIVIDUAL & FAMILY PLANS
 Rocky Mountain View INDIVIDUAL & FAMILY PLANS WHEN IT COMES TO HEALTH INSURANCE, WE KNOW WHAT MATTERS MOST: YOU. No one plans to be sick or injured, but if something happens, we want you to remain in control
Rocky Mountain View INDIVIDUAL & FAMILY PLANS WHEN IT COMES TO HEALTH INSURANCE, WE KNOW WHAT MATTERS MOST: YOU. No one plans to be sick or injured, but if something happens, we want you to remain in control
Summary of Benefits. January 1, 2018 December 31, Providence Medicare Harbor + RX (HMO) Providence Medicare Summit + RX (HMO-POS)
 Providence Medicare Summit + RX (HMO-POS)") Summary of Benefits January 1, 2018 December 31, 2018 These Plans are available in Snohomish and King Counties in Washington. 2018 Advantage Plans is an HMO, HMO-POS, and HMO SNP plan with a Medicare and
Summary of Benefits January 1, 2018 December 31, 2018 These Plans are available in Snohomish and King Counties in Washington. 2018 Advantage Plans is an HMO, HMO-POS, and HMO SNP plan with a Medicare and
Important Questions Answers Why this Matters:
 . Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: On and after 04/01/17 Essential 4000 Alliance C Coverage for: Family Plan Type: PPO The Summary
. Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: On and after 04/01/17 Essential 4000 Alliance C Coverage for: Family Plan Type: PPO The Summary
Provider Manual. ChoiceBenefits. BayCare Health System Medical Plan
 2019 Provider Manual ChoiceBenefits BayCare Health System Medical Plan 1 Table of Contents BayCare... 2 BayCare Exclusive Network... 2 Rules unique to Cigna BayCare Members... 2 Provider Relations Representative...
2019 Provider Manual ChoiceBenefits BayCare Health System Medical Plan 1 Table of Contents BayCare... 2 BayCare Exclusive Network... 2 Rules unique to Cigna BayCare Members... 2 Provider Relations Representative...
Best Buy HMO FLEX Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services
 Massachusetts Best Buy HMO 500 - FLEX Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 04/01/2018 03/31/2019 Coverage for: Individual + Family
Massachusetts Best Buy HMO 500 - FLEX Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 04/01/2018 03/31/2019 Coverage for: Individual + Family
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services. Coverage Period: Beginning On or After 1/1/2018
 Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: Beginning On or After 1/1/2018 Platinum Full PPO 250/15 OffEx Coverage for: Individual + Family
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: Beginning On or After 1/1/2018 Platinum Full PPO 250/15 OffEx Coverage for: Individual + Family
Maine's Choice HSA HMO 5000 Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services
 Maine Maine's Choice HSA HMO 5000 Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/2018 12/31/2018 Coverage for: Individual + Family Plan
Maine Maine's Choice HSA HMO 5000 Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/2018 12/31/2018 Coverage for: Individual + Family Plan
BridgeSpan Health Company: BridgeSpan Bronze Essential 6850 Value PPO
 BridgeSpan Health Company: BridgeSpan Bronze Essential 6850 Value PPO Summary of Benefits and Coverage: What this Plan Covers & What it Costs Questions: Call 1 (855) 857-9943 or visit us at www.bridgespanhealth.com.
BridgeSpan Health Company: BridgeSpan Bronze Essential 6850 Value PPO Summary of Benefits and Coverage: What this Plan Covers & What it Costs Questions: Call 1 (855) 857-9943 or visit us at www.bridgespanhealth.com.
National Elevator Industry: Health Benefit Plan Summary of Benefits and Coverage: What this Plan Covers & What it Costs
 National Elevator Industry: Health Benefit Plan Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage Period: 01/01/2016-12/31/2016 Coverage for: Individual + Family Plan Type:
National Elevator Industry: Health Benefit Plan Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage Period: 01/01/2016-12/31/2016 Coverage for: Individual + Family Plan Type:
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: On and after 01/01/18
 . Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: On and after 01/01/18 EverydayHealth 5000 Alliance Coverage for: Family Plan Type: PPO The
. Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: On and after 01/01/18 EverydayHealth 5000 Alliance Coverage for: Family Plan Type: PPO The
HMO - FLEX Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services
 Massachusetts HMO - FLEX Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/2019 12/31/2019 Coverage for: Individual + Family Plan Type:
Massachusetts HMO - FLEX Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/2019 12/31/2019 Coverage for: Individual + Family Plan Type:
Standard Gold Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services
 Massachusetts Standard Gold Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/2018 12/31/2018 Coverage for: Individual + Family Plan Type:
Massachusetts Standard Gold Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/2018 12/31/2018 Coverage for: Individual + Family Plan Type:
BluePreferred PPO Silver 1500 BlueFund HSA Integrated Deductible
 BluePreferred PPO Silver 1500 BlueFund HSA Integrated Deductible Summary of Benefits Services In-Network You Pay 1 Out-of-Network You Pay 1 FIRSTHELP 24/7 NURSE ADVICE LINE Free advice from a registered
BluePreferred PPO Silver 1500 BlueFund HSA Integrated Deductible Summary of Benefits Services In-Network You Pay 1 Out-of-Network You Pay 1 FIRSTHELP 24/7 NURSE ADVICE LINE Free advice from a registered
Dell Children s Health Plan transition to Amerigroup. Misty Arayata & Emily Rhine Provider Engagement October 2016
 Dell Children s Health Plan transition to Amerigroup Misty Arayata & Emily Rhine Provider Engagement October 2016 TSPEC-0123-16 October 2016 Introduction Effective December 1, 2016 Seton Health Plan will
Dell Children s Health Plan transition to Amerigroup Misty Arayata & Emily Rhine Provider Engagement October 2016 TSPEC-0123-16 October 2016 Introduction Effective December 1, 2016 Seton Health Plan will
2018 Health, Dental and Vision Monthly Contributions
 2018 Health, Dental and Vision Monthly Contributions Benefit Plan Monthly Contributions for Active Regular Full-Time and Part-Time Employees Employee Only Spouse Child(ren) Family Dental: Cigna PPO $ 13
2018 Health, Dental and Vision Monthly Contributions Benefit Plan Monthly Contributions for Active Regular Full-Time and Part-Time Employees Employee Only Spouse Child(ren) Family Dental: Cigna PPO $ 13
this plan begins to pay. If you have other family members on the plan each family member deductible?
 Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: Beginning On or After 1/1/2018 Platinum 90 PPO Coverage for: Individual + Family Plan Type:
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: Beginning On or After 1/1/2018 Platinum 90 PPO Coverage for: Individual + Family Plan Type:
Aetna 1-50 HealthNetworkOnlyOpenAccess NV 01/01/2019
 HealthNetworkOnlyOpenAccess NV 01/01/2019 Plan Name NV Silver HNOnly 3500 70% $40 In Network Deductible (Individual/Family) $3,500/$7,000 Out-of-pocket limit (Individual/Family) $7,500/$15,000 Deductible/out-of-pocket
HealthNetworkOnlyOpenAccess NV 01/01/2019 Plan Name NV Silver HNOnly 3500 70% $40 In Network Deductible (Individual/Family) $3,500/$7,000 Out-of-pocket limit (Individual/Family) $7,500/$15,000 Deductible/out-of-pocket
BE READY FOR ANYTHING
 BE READY FOR ANYTHING Learn What You Need to Know About Your 2019 Highmark Coverage Options Benefit Period: January 1 to December 31, 2019 2019 HEALTH INSURANCE 2 CONNECTING CARE AND COVERAGE * You want
BE READY FOR ANYTHING Learn What You Need to Know About Your 2019 Highmark Coverage Options Benefit Period: January 1 to December 31, 2019 2019 HEALTH INSURANCE 2 CONNECTING CARE AND COVERAGE * You want
COPAY PLANS. PreferredOne.com. Welcome to PreferredOne. Health Insurance for Individuals & Families 2014
 COPAY PLANS Health Insurance for Individuals & Families 2014 Welcome to PreferredOne PreferredOne.com Your Health, Your Choice, Many Options KEY OPEN ENROLLMENT DATES At PreferredOne, our name says it
COPAY PLANS Health Insurance for Individuals & Families 2014 Welcome to PreferredOne PreferredOne.com Your Health, Your Choice, Many Options KEY OPEN ENROLLMENT DATES At PreferredOne, our name says it
BridgeSpan Health Company: BridgeSpan Oregon Standard Silver Plan Value PPO
 BridgeSpan Health Company: BridgeSpan Oregon Standard Silver Plan Value PPO Summary of Benefits and Coverage: What this Plan Covers & What it Costs Questions: Call 1 (855) 857-9943 or visit us at www.bridgespanhealth.com.
BridgeSpan Health Company: BridgeSpan Oregon Standard Silver Plan Value PPO Summary of Benefits and Coverage: What this Plan Covers & What it Costs Questions: Call 1 (855) 857-9943 or visit us at www.bridgespanhealth.com.
BridgeSpan Health Company: BridgeSpan Oregon Standard Silver Plan Coverage Period: 01/01/2015
 BridgeSpan Health Company: BridgeSpan Oregon Standard Silver Plan Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage Period: 01/01/2015 01/01/2015 12/31/2015-12/31/2015 Coverage
BridgeSpan Health Company: BridgeSpan Oregon Standard Silver Plan Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage Period: 01/01/2015 01/01/2015 12/31/2015-12/31/2015 Coverage
PROVIDENCE MEDICARE PRIME + RX (HMO-POS) MEMBER HANDBOOK EVIDENCE OF COVERAGE JAN. 1 DEC. 31, 2016
 MEMBER HANDBOOK EVIDENCE OF COVERAGE JAN. 1 DEC. 31, 2016") PROVIDENCE MEDICARE PRIME + RX (HMO-POS) MEMBER HANDBOOK EVIDENCE OF COVERAGE JAN. 1 DEC. 31, 2016 January 1 December 31, 2016 Evidence of Coverage: Your Medicare Health Benefits and Services and Prescription
PROVIDENCE MEDICARE PRIME + RX (HMO-POS) MEMBER HANDBOOK EVIDENCE OF COVERAGE JAN. 1 DEC. 31, 2016 January 1 December 31, 2016 Evidence of Coverage: Your Medicare Health Benefits and Services and Prescription
Frequently Asked Questions
 Corrected Claims Submissions 1. What is a corrected claim? If a claim was submitted to and accepted by Healthfirst but was later found to have incorrect information, certain data elements on the claim
Corrected Claims Submissions 1. What is a corrected claim? If a claim was submitted to and accepted by Healthfirst but was later found to have incorrect information, certain data elements on the claim
Provider Contacts List
 Common telephone numbers, email addresses and websites for providers and Oregon Health Plan (OHP) members Fax numbers and telephone numbers for prior authorization requests Mailing addresses for claims,
Common telephone numbers, email addresses and websites for providers and Oregon Health Plan (OHP) members Fax numbers and telephone numbers for prior authorization requests Mailing addresses for claims,
BridgeSpan Health Company: BridgeSpan Silver HDHP 2000 MyChoice Northwest
 BridgeSpan Health Company: BridgeSpan Silver HDHP 2000 MyChoice Northwest Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage Period: 01/01/2016 12/31/2016 Coverage for: Individual
BridgeSpan Health Company: BridgeSpan Silver HDHP 2000 MyChoice Northwest Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage Period: 01/01/2016 12/31/2016 Coverage for: Individual
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/ /31/2019
 Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/2019 12/31/2019 Highmark West Virginia: my Blue Access WV EPO Silver 4450 HSA Coverage
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/2019 12/31/2019 Highmark West Virginia: my Blue Access WV EPO Silver 4450 HSA Coverage
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/ /31/2019
 Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/2019 12/31/2019 Highmark West Virginia: my Blue Access WV EPO Bronze 4000 Coverage for:
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/2019 12/31/2019 Highmark West Virginia: my Blue Access WV EPO Bronze 4000 Coverage for:
For preferred providers: $4,350 / Covered. What is the overall deductible? Person or $14,700 / Family; For nonpreferred providers: $14,700 / Covered
 Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/2018 12/31/2018 WI Silver 4350 Coverage for: Individual/Family Plan Type: PPO The Summary
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/2018 12/31/2018 WI Silver 4350 Coverage for: Individual/Family Plan Type: PPO The Summary
DEANCARE GOLD MANUAL
 DEANCARE GOLD MANUAL TABLE OF CONTENTS OVERVIEW OF COVERAGE... 3 COMMUNICATING WITH DEAN HEALTH PLAN... 8 REIMBURSEMENT... 9 CLAIMS AND TIMELY FILING... 9 AUTHORIZATION PROCESS... 10 COMPLAINT/APPEALS
DEANCARE GOLD MANUAL TABLE OF CONTENTS OVERVIEW OF COVERAGE... 3 COMMUNICATING WITH DEAN HEALTH PLAN... 8 REIMBURSEMENT... 9 CLAIMS AND TIMELY FILING... 9 AUTHORIZATION PROCESS... 10 COMPLAINT/APPEALS
Summary of Benefits January 1, 2019 December 31, 2019
 Summary of Benefits January 1, 2019 December 31, 2019 Providence Medicare Extra + RX (HMO) This Plan is available in Clackamas, Columbia, Lane, Marion, Multnomah, Polk, Washington and Yamhill counties
Summary of Benefits January 1, 2019 December 31, 2019 Providence Medicare Extra + RX (HMO) This Plan is available in Clackamas, Columbia, Lane, Marion, Multnomah, Polk, Washington and Yamhill counties
2016 COPAY AND DEDUCTIBLE PLANS
 2016 COPAY AND DEDUCTIBLE PLANS Health Insurance for Individuals & Families Welcome to PreferredOne PreferredOne.com Your Health, Your Choice, Many Options At PreferredOne, our name says it all you and
2016 COPAY AND DEDUCTIBLE PLANS Health Insurance for Individuals & Families Welcome to PreferredOne PreferredOne.com Your Health, Your Choice, Many Options At PreferredOne, our name says it all you and
BluePreferred PPO HSA/HRA 5500 ON/ OFF SHOP Integrated Deductible
 BluePreferred PPO HSA/HRA 5500 ON/ OFF SHOP Integrated Deductible Summary of Benefits Services In-Network You Pay 1 Out-of-Network You Pay 1 FIRSTHELP 24/7 NURSE ADVICE LINE Free advice from a registered
BluePreferred PPO HSA/HRA 5500 ON/ OFF SHOP Integrated Deductible Summary of Benefits Services In-Network You Pay 1 Out-of-Network You Pay 1 FIRSTHELP 24/7 NURSE ADVICE LINE Free advice from a registered
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: On and after 01/01/18
 . Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: On and after 01/01/18 EverydayHealth 6500 Neighborhood Coverage for: Family Plan Type: HMO
. Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: On and after 01/01/18 EverydayHealth 6500 Neighborhood Coverage for: Family Plan Type: HMO
Coverage for: Individual + Family Plan Type: PPO
 Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/2019-12/31/2019 Chestnut Hill College: PPO 2 Coverage for: Individual + Family Plan Type:
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/2019-12/31/2019 Chestnut Hill College: PPO 2 Coverage for: Individual + Family Plan Type:
Ensuring your health Health Plans for Oregon Individuals and Families
 Ensuring your health 2019 Health Plans for Oregon Individuals and Families At your service The PacificSource difference is our exceptional customer service. We re focused on making health insurance easier
Ensuring your health 2019 Health Plans for Oregon Individuals and Families At your service The PacificSource difference is our exceptional customer service. We re focused on making health insurance easier
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: On and after 04/01/17
 . Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: On and after 04/01/17 EverydayHealth 6000 Statewide C Coverage for: Family Plan Type: PPO
. Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: On and after 04/01/17 EverydayHealth 6000 Statewide C Coverage for: Family Plan Type: PPO
Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage Period: 01/01/ /31/2018
 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage Period: 01/01/2018 12/31/2018 Highmark Delaware: Shared Cost Blue EPO 6950 Coverage for: Individual/Family Plan Type: EPO
Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage Period: 01/01/2018 12/31/2018 Highmark Delaware: Shared Cost Blue EPO 6950 Coverage for: Individual/Family Plan Type: EPO
Important Questions Answers Why this Matters:
 Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: On and after 01/01/18 Portfolio 3250 Alliance Coverage for: Family Plan Type: HSA-qualified
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: On and after 01/01/18 Portfolio 3250 Alliance Coverage for: Family Plan Type: HSA-qualified
LVAIC-Muhlenberg College: Lehigh Valley Flex Blue PPO Coverage Period: 01/01/ /31/2017
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.highmarkblueshield.com or by calling 1-800-345-3806.
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.highmarkblueshield.com or by calling 1-800-345-3806.
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: On and after 01/01/18
 . Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: On and after 01/01/18 EverydayHealth 6500 Statewide HMO Coverage for: Family Plan Type: HMO
. Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: On and after 01/01/18 EverydayHealth 6500 Statewide HMO Coverage for: Family Plan Type: HMO
Important Questions Answers Why this Matters:
 . Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: On and after 01/01/18 Portfolio 6650 Alliance Coverage for: Family Plan Type: HSA-qualified
. Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: On and after 01/01/18 Portfolio 6650 Alliance Coverage for: Family Plan Type: HSA-qualified
Important Questions Answers Why this Matters:
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.anthem.com/ca or by calling 1-855-333-5730. Important
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.anthem.com/ca or by calling 1-855-333-5730. Important
2018 INDIVIDUAL AND FAMILY PLANS
 2018 INDIVIDUAL AND FAMILY PLANS 2018 Individual Plans 2018 PLATINUM PLAN Platinum Standard Individual $815.03 Monthly premium individual/family Individual and child(ren) $1,385.55 Individual and spouse/domestic
2018 INDIVIDUAL AND FAMILY PLANS 2018 Individual Plans 2018 PLATINUM PLAN Platinum Standard Individual $815.03 Monthly premium individual/family Individual and child(ren) $1,385.55 Individual and spouse/domestic
2018 Medical Plan Comparison Key Highlights
 2018 Medical Plan Comparison Key Highlights A reference to assist you in selecting the medical plan which best meets your family needs. The choices you make for where you seek care and services will have
2018 Medical Plan Comparison Key Highlights A reference to assist you in selecting the medical plan which best meets your family needs. The choices you make for where you seek care and services will have
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/ /31/2019
 Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/2019 12/31/2019 Highmark West Virginia: my Blue Access WV EPO Silver 3500-2 Free PCP Visits
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/2019 12/31/2019 Highmark West Virginia: my Blue Access WV EPO Silver 3500-2 Free PCP Visits
Medicare Advantage HMO plans
 2018 Medicare Advantage HMO plans Essence (HMO-POS) Essence Rx (HMO-POS) Esteem Rx (HMO-POS) Spirit (HMO-POS) Spirit Rx (HMO-POS) Medicare coverage that works with and for you Y0117_MC-778-2820-C-10-17
2018 Medicare Advantage HMO plans Essence (HMO-POS) Essence Rx (HMO-POS) Esteem Rx (HMO-POS) Spirit (HMO-POS) Spirit Rx (HMO-POS) Medicare coverage that works with and for you Y0117_MC-778-2820-C-10-17
Summary of Benefits and Coverage:
 Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: Beginning on or after 01/01/2018 Community Preferred (Silver) Employer Coverage for: Individual
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: Beginning on or after 01/01/2018 Community Preferred (Silver) Employer Coverage for: Individual
2018 ConnectiCare SOLO. Individual plans
 2018 ConnectiCare SOLO Individual plans Welcome to ConnectiCare This guide includes information about ConnectiCare s 2018 SOLO plans. We re pleased to offer you a range of plan options, giving you the
2018 ConnectiCare SOLO Individual plans Welcome to ConnectiCare This guide includes information about ConnectiCare s 2018 SOLO plans. We re pleased to offer you a range of plan options, giving you the
Bronze 60 HMO. Individual & Family Plan Summary of Benefits and Coverage
 Bronze 60 HMO Individual & Family Plan Summary of Benefits and Coverage DMHC Approved Date 08/25/2017 Rev. 04/03/2018 Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered
Bronze 60 HMO Individual & Family Plan Summary of Benefits and Coverage DMHC Approved Date 08/25/2017 Rev. 04/03/2018 Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered
Bronze 60 HMO. Employer Group Summary of Benefits and Coverage
 Bronze 60 HMO Employer Group Summary of Benefits and Coverage DMHC Approved Date 08/25/2017 Rev. 04/03/2018 Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage
Bronze 60 HMO Employer Group Summary of Benefits and Coverage DMHC Approved Date 08/25/2017 Rev. 04/03/2018 Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage
Coverage Period: Beginning on or after 01/01/2018 Coverage for: Individual + Family Plan Type: PPO
 Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services S.PIC.7350.100.50 (Silver) Coverage Period: Beginning on or after 01/01/2018 Coverage for: Individual + Family
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services S.PIC.7350.100.50 (Silver) Coverage Period: Beginning on or after 01/01/2018 Coverage for: Individual + Family
EverydayHealth 5000/100 Alliance Summary of Benefits and Coverage: What this Plan Covers & What it Costs
 EverydayHealth 5000/100 Alliance Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage Period: On and after 10/18/16 Coverage for: Individual Plan Type: PPO This is only a summary.
EverydayHealth 5000/100 Alliance Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage Period: On and after 10/18/16 Coverage for: Individual Plan Type: PPO This is only a summary.
2018 Community Blue Medicare PPO Summary of Benefits
 2018 Community Blue Medicare PPO Summary of Benefits Residents of the following counties: Allegheny, Beaver, Butler, Erie, Greene, Fayette, Washington, Westmoreland, please click here. Residents of the
2018 Community Blue Medicare PPO Summary of Benefits Residents of the following counties: Allegheny, Beaver, Butler, Erie, Greene, Fayette, Washington, Westmoreland, please click here. Residents of the
Getting Started with Medicare
 Getting Started with Medicare TABLE OF CONTENTS 2 What is Medicare? 3 Original Medicare Parts A and B 5 Medicare Part C Medicare Advantage Plans 6 Medicare Part D Prescription Drug Coverage 8 How to Enroll
Getting Started with Medicare TABLE OF CONTENTS 2 What is Medicare? 3 Original Medicare Parts A and B 5 Medicare Part C Medicare Advantage Plans 6 Medicare Part D Prescription Drug Coverage 8 How to Enroll
Innovation Health At-A-Glance
 Innovation Health At-A-Glance A quick reference guide for health care professionals 71.02.801.1 A (3/15) innovation-health.com A guide for doing business with Innovation Health Getting started with Innovation
Innovation Health At-A-Glance A quick reference guide for health care professionals 71.02.801.1 A (3/15) innovation-health.com A guide for doing business with Innovation Health Getting started with Innovation
2017 South Dakota Day with the Payers
 2017 South Dakota Day with the Payers HealthPartners, Inc. Founded in 1957 as a cooperative Largest consumer-governed non-profit health plan in the country We serve more than 1.5 million medical and dental
2017 South Dakota Day with the Payers HealthPartners, Inc. Founded in 1957 as a cooperative Largest consumer-governed non-profit health plan in the country We serve more than 1.5 million medical and dental
The Harvard Pilgrim Best Buy HMO Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services
 Massachusetts The Harvard Pilgrim Best Buy HMO Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 12/01/2017 11/30/2018 Coverage for: Individual
Massachusetts The Harvard Pilgrim Best Buy HMO Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 12/01/2017 11/30/2018 Coverage for: Individual
Silver 70 HMO. Individual & Family Plan Summary of Benefits and Coverage
 Silver 70 HMO Individual & Family Plan Summary of Benefits and Coverage DMHC Approved Date 08/25/2017 Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage
Silver 70 HMO Individual & Family Plan Summary of Benefits and Coverage DMHC Approved Date 08/25/2017 Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage
Prepared By: 600 West 5 th Street, Suite 200 Austin, TX Toll Free: O: (512) F: (512) Hours 8:30 to 5:00 M F
 F: (512) Hours 8:30 to 5:00 M F") EMPLOYEE BENEFITS PLAN YEAR Prepared By: 600 West 5 th Street, Suite 200 Austin, TX 78701 Toll Free: 1.888.478.9595 O: (512) 478.9595 F: (512) 478.9494 Hours 8:30 to 5:00 M F Tom Ball Danny Peoples Account
EMPLOYEE BENEFITS PLAN YEAR Prepared By: 600 West 5 th Street, Suite 200 Austin, TX 78701 Toll Free: 1.888.478.9595 O: (512) 478.9595 F: (512) 478.9494 Hours 8:30 to 5:00 M F Tom Ball Danny Peoples Account
Best Buy HMO FLEX Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services
 Massachusetts Best Buy HMO 2000 - FLEX Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/2018 03/31/2018 Coverage for: Individual + Family
Massachusetts Best Buy HMO 2000 - FLEX Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/2018 03/31/2018 Coverage for: Individual + Family
We will begin our presentation in 5 minutes. As a friendly reminder, please remember to silence your phones. Thank you for your participation.
 Welcome! We will begin our presentation in 5 minutes. As a friendly reminder, please remember to silence your phones. Thank you for your participation. 1 Maternal Infant Health Program (MIHP) December
Welcome! We will begin our presentation in 5 minutes. As a friendly reminder, please remember to silence your phones. Thank you for your participation. 1 Maternal Infant Health Program (MIHP) December