UnitedHealthcare Insurance Company Written Plan Description
|
|
|
- Laurence Shaw
- 6 years ago
- Views:
Transcription
1 UnitedHealthcare Insurance Company Written Plan Description [CHOICE][EXCLUSIVE PROVIDER PLAN] This coverage is provided by UnitedHealthcare Insurance Company (UnitedHealthcare). This coverage provides benefits only when a Preferred Provider (Network Provider) or a Non-Preferred Provider (Non-network Provider) is used, except as otherwise noted. If you have questions or need additional information, you may write to us at our Home Office at UnitedHealthcare Insurance Company 185 Asylum St. Hartford, CT or you may contact us, toll free, at A Network Provider is a hospital, physician or other health care provider who has contracted with us for the purpose of reducing health care costs by negotiating fees for services provided to Insured Persons. A non-network Provider is a hospital, physician or other health care provider who has not contracted with us. Please Note: this benefit plan includes limited Benefits for services provided by a Physician or health care provider that is not a Network provider. For a list of Network providers go to or call Customer Care at the telephone number on the back of your ID card. Benefits Annual Deductibles are calculated on a [calendar] [Policy] year basis. Out-of-Pocket Maximums are calculated on a [calendar] [Policy] year basis. [When Benefit limits apply, the limit stated includes Covered Health Services provided at a Designated Provider level of Benefits unless otherwise specifically stated.] Benefit limits are calculated on a [calendar] [Policy] year basis unless otherwise specifically stated. WPD.EPO.I.11.TX R1

2

3 WPD.EPO.I.11.TX R1

4

5
6

7
8

9

10

11

12

13
14 Benefits for Prescription Drug Products Benefits are available for Prescription Drug Products at a Network Pharmacy and are subject to Copayments and/or Coinsurance or other payments that vary depending on which of the tiers of the Prescription Drug List the Prescription Drug Product is listed. [Benefits are provided only when the Prescription Order or Refill has been issued by a Network Physician or other Network provider.] Benefits for Prescription Drug Products are available when the Prescription Drug Product meets the definition of a Covered Health Service or is prescribed to prevent conception. Supply Limits Benefits for Prescription Drug Products are subject to the supply limits that are stated in the Description and Supply Limits column of the Benefit Information table. For a single Copayment and/or Coinsurance, you may receive a Prescription Drug Product up to the stated supply limit. Note: Some products are subject to additional supply limits based on criteria that we have developed, subject to our periodic review and modification. The limit may restrict the amount dispensed per Prescription Order or Refill and/or the amount dispensed per month s supply, or may require that a minimum amount be dispensed. You may determine whether a Prescription Drug Product has been assigned a supply limit for dispensing through the Internet at [ or by calling Customer Care at the telephone number on your ID card. WPD.EPO.I.11.TX R1

15
16

17
18
19 Prior Authorization Requirements Before certain Prescription Drug Products are dispensed to you, either your Physician, your pharmacist or you are required to obtain prior authorization from us or our designee. The reason for obtaining prior authorization from us is to determine whether the Prescription Drug Product, in accordance with our approved guidelines, is each of the following: It meets the definition of a Covered Health Service. It is not an Experimental or Investigational or Unproven Service. We may also require you to obtain prior authorization from us or our designee so we can determine whether the Prescription Drug Product, in accordance with our approved guidelines, was prescribed by a Specialist Physician. Network Pharmacy Prior Authorization When Prescription Drug Products are dispensed at a Network Pharmacy, the prescribing provider, the pharmacist, or you are responsible for obtaining prior authorization from us. If you do not obtain prior authorization from us before the Prescription Drug Product is dispensed, you may pay more for that Prescription Order or Refill. The Prescription Drug Products requiring prior authorization are subject to our periodic review and modification. You may determine whether a particular Prescription Drug Product requires prior authorization through the Internet at [ or by calling Customer Care at the telephone number on your ID card. If you do not obtain prior authorization from us before the Prescription Drug Product is dispensed, you can ask us to consider reimbursement after you receive the Prescription Drug Product. You will be required to pay for the Prescription Drug Product at the pharmacy. You may seek reimbursement from us as described in the Certificate of Coverage (Certificate) in Section 5: How to File a Claim. [Therapeutic class charge and therapeutically equivalent charge (here and throughout) is variable by plan design.] When you submit a claim on this basis, you may pay more because you did not obtain prior authorization from us before the Prescription Drug Product was dispensed. The amount you are reimbursed will be based on the Prescription Drug Charge, less the required Copayment and/or Coinsurance [,Ancillary Charge] [,Therapeutic Class Charge] [,Therapeutically Equivalent Charge] and any deductible that applies. Benefits may not be available for the Prescription Drug Product after we review the documentation provided and we determine that the Prescription Drug Product is not a Covered Health Service or it is an Experimental or Investigational or Unproven Service. We may also require prior authorization for certain programs which may have specific requirements for participation and/ or activation of an enhanced level of Benefits associated with such programs. You may access information on available programs and any applicable prior authorization, participation or activation requirements associated with such programs through the Internet at [ or by calling Customer Care at the telephone number on your ID card. [Step Therapy] [Certain Prescription Drug Products for which Benefits are described under this Prescription Drug Rider or Pharmaceutical Products for which Benefits are described in your Certificate are subject to step therapy requirements. This means that in order to receive Benefits for such Prescription Drug Products and/or Pharmaceutical Products you are required to use a different Prescription Drug Product(s) or Pharmaceutical Product(s) first. You may determine whether a particular Prescription Drug Product or Pharmaceutical Product is subject to step therapy requirements through the Internet at [ or by calling Customer Care at the telephone number on your ID card.] What You Must Pay [The following bracketed provisions are variable based upon plan design.] [You are responsible for paying the [Annual Drug Deductible] [and] [Specialty Prescription Drug Product Annual Deductible].] [Benefits for Prescription Drug Products on the List of Preventive Medications are not subject to payment of the Annual Drug Deductible.] [Benefits for Preventive Care Medications are not subject to payment of the Annual Drug Deductible.] [Benefits for [insulin] [or] [diabetic supplies] are not subject to payment of the Annual Drug Deductible.] WPD.EPO.I.11.TX R1
20 [You are responsible for paying the Annual Deductible stated in the Schedule of Benefits which is attached to your Certificate before Benefits for Prescription Drug Products under this Rider are available to you.] [Benefits for Prescription Drug Products on the List of Preventive Medications are not subject to payment of the Annual Deductible.] [Benefits for Preventive Care Medications are not subject to payment of the Annual Deductible.] [Benefits for [insulin] [or] [diabetic supplies] are not subject to payment of the Annual Deductible.] You are responsible for paying the applicable Copayment and/or Coinsurance described in the Benefit Information table [, in addition to any Ancillary Charge] [[, in addition to any] [or] Therapeutic Class Charge] [[, in addition to any] [or] Therapeutically Equivalent Charge]. [You are not responsible for paying a Copayment and/or Coinsurance for Preventive Care Medications.] [ 1 Applies when the plan design includes the mandatory generic program.] [An Ancillary Charge may apply when a covered Prescription Drug Product is dispensed at your [1or the provider s] request and there is another drug that is chemically the same available at a lower tier. When you choose the higher tiered drug of the two, you will pay the difference between the higher tiered drug and the lower tiered drug in addition to your Copayment and/or Coinsurance that applies to the [lower tiered drug] [higher tier drug]. [An Ancillary Charge does not apply to any [Annual Drug Deductible] [,] [Annual Deductible] [,] [Specialty Prescription Drug Product Annual Deductible] [,] [or] [Out-of-Pocket Drug Maximum] [,] [or] [Out-of-Pocket Maximum] [or] [Specialty Prescription Drug Product Out-of- Pocket Maximum].]] [A Therapeutic Class Charge may apply when the Prescription Drug Charge of the Prescription Drug Product exceeds the Maximum Allowable Amount. You are responsible for the Therapeutic Class Charge and any applicable Copayment and/ or Coinsurance.] [A Therapeutically Equivalent Charge may apply when the Prescription Drug Charge of the Prescription Drug Product exceeds the Maximum Allowable Amount. You are responsible for the Therapeutically Equivalent Charge and any applicable Copayment and/or Coinsurance.] The amount you pay for any of the following under this Rider will not be included in calculating any Out-of-Pocket Maximum stated in your Certificate: [Copayments for Prescription Drug Products [,including Specialty Prescription Drug Products].] [Coinsurance for Prescription Drug Products [,including Specialty Prescription Drug Products].] [Ancillary Charges.] [Therapeutic Class Charges.] [Therapeutically Equivalent Charges.] [The Annual Drug Deductible.] [The Specialty Prescription Drug Product Annual Deductible.] [Any amount you pay for Prescription Drug Products for Infertility that exceeds the Infertility Annual Maximum Benefit.] [Any amount you pay for Prescription Drug Products for Infertility that exceeds the Infertility Maximum Policy Benefit.] Any non-covered drug product. You are responsible for paying 100% of the cost (the amount the pharmacy charges you) for any non-covered drug product and our contracted rates (our Prescription Drug Charge) will not be available to you. Payment Information [The following provisions are plan design variable.] [The Annual Drug Deductibles are calculated on a [calendar] [Policy] year basis.] [The Specialty Prescription Drug Product Annual Deductibles are calculated on a [calendar] [Policy] year basis.] WPD.EPO.I.11.TX R1
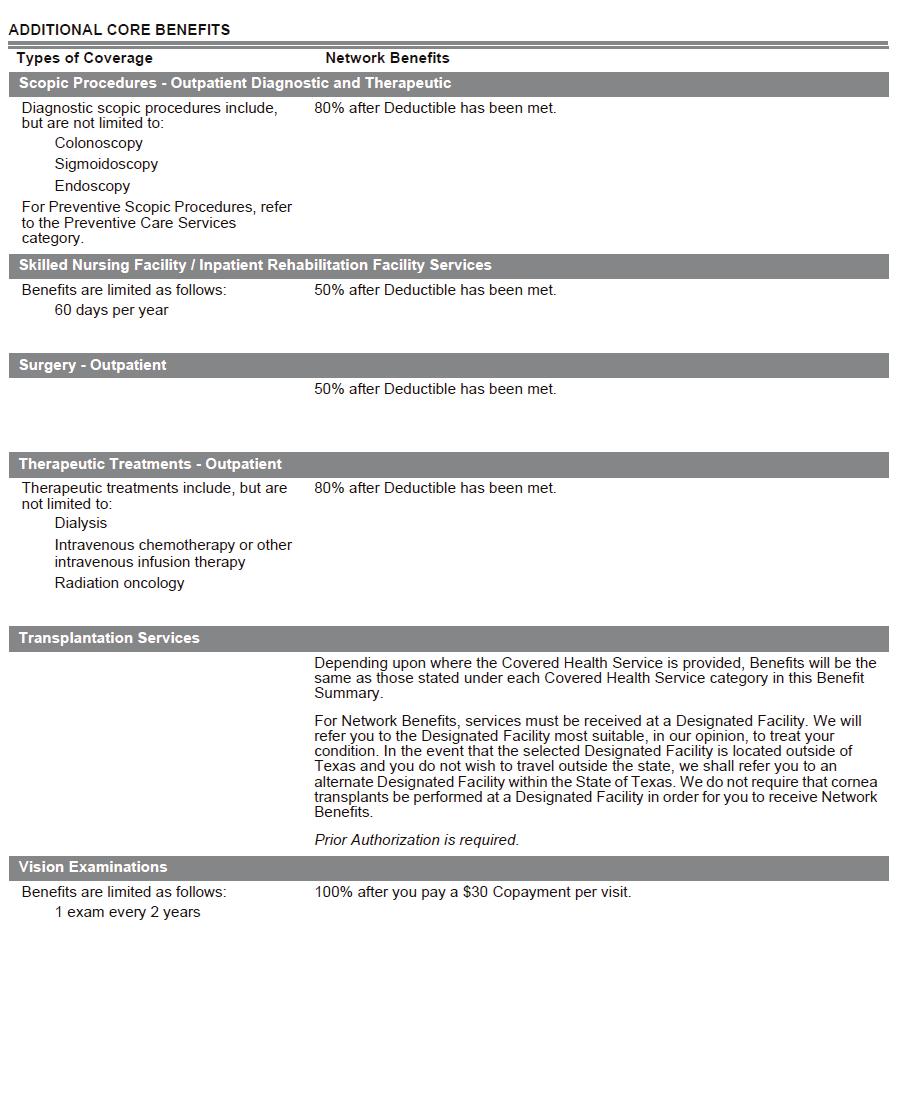
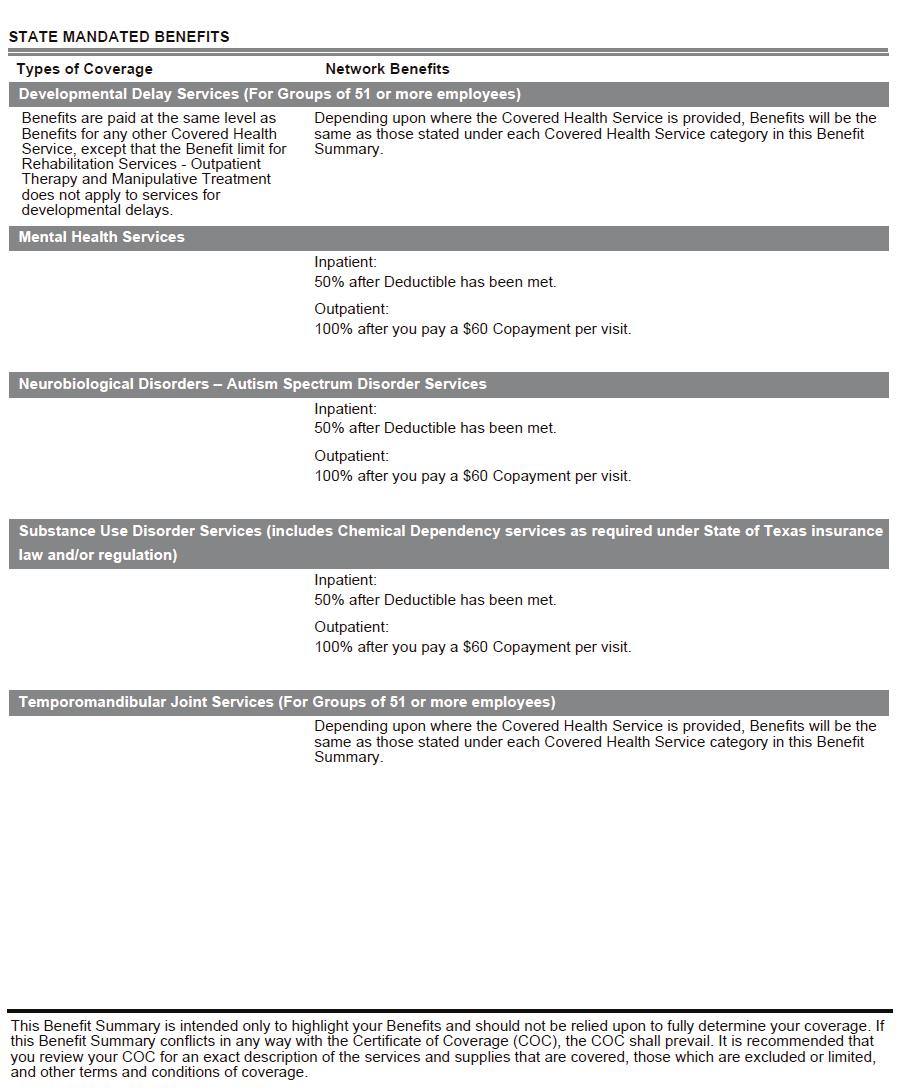
21 [The Out-of-Pocket Drug Maximums are calculated on a [calendar] [Policy] year basis.] [The Specialty Prescription Drug Product Out-of-Pocket Maximums are calculated on a [calendar] [Policy] year basis.] [The Infertility Annual Maximum Benefit is calculated on a [calendar] [Policy] year basis.] Emergency Care means health care services provided in a hospital emergency facility or other comparable facility to evaluate and stabilize medical conditions of a recent onset and severity, including but not limited to, severe pain, that would lead a prudent layperson, possessing an average knowledge of medicine and health, to believe that the person s condition, sickness or injury is of such a nature that failure to get immediate medical care could result in: placing the patient s health in serious jeopardy; serious impairment to bodily functions; serious dysfunction of any bodily organ or part; serious disfigurement; or in the case of a pregnant woman, serious jeopardy to the health of the fetus. Prior authorization is not required for emergency services. Benefits are provided for Emergency Health Services provided by a non-network physician or provider. Urgent care is health services that are required to prevent serious deterioration of your health and/or as a result of an unforeseen sickness, injury or the onset of acute or severe symptoms. Urgent care health services and after hours care must be provided by a Network physician or provider for the services to be covered. Out-of-area services received from a non-network physician or provider are not covered except in cases of an emergency. The Insured Person is responsible for payment of all noncovered services and/or services provided by a non-network provider (except in the case of emergency or if specific Covered Health Services are not available from a Network provider, upon request from your Network provider, you may be eligible for Benefits when Covered Health Services are received from non-network providers) including the deductible, coinsurance, copayment and out-of-pocket expense amounts shown in the Schedule of Benefits. Benefits apply to Covered Health Services that are provided by a Network Physician or other Network provider. Benefits for facility services apply when Covered Health Services are provided at a Network facility. Benefits include Physician services provided in a Network facility by a Network or a non-network radiologist, anesthesiologist, pathologist, Emergency room Physician and consulting Physician. Benefits also include Covered Health Services received at an Urgent Care Center outside your geographic area and Emergency Health Services. When Covered Health Services [1(other than Emergency Health Services)] are provided at a Network facility by a non-network [1Emergency care Physician] [,] [or] [radiologist] [,] [or] [anesthesiologist] [,] [or] [pathologist] [,] [or] [consulting Physician] [,] [or] [neonatologist] [,] [or] [intensivist] [,] [or] [assistant surgeon] [or] [surgical assistant], or at a Network clinic or Physician office by a non-network [Emergency care Physician] [,] [or] [radiologist] [,] [or] [anesthesiologist] [,] [or] [pathologist], Benefits will be reimbursed as set forth under Eligible Expenses as described at the end of the Schedule of Benefits. We do not Pay Benefits for Exclusions We will not pay Benefits for any of the services, treatments, items or supplies described in this section, even if either of the following is true: WPD.EPO.I.11.TX R1 It is recommended or prescribed by a Physician. It is the only available treatment for your condition. The services, treatments, items or supplies listed in this section are not Covered Health Services, except as may be specifically provided for in Section 1: Covered Health Services or through a Rider to the Policy. Benefit Limitations When Benefits are limited within any of the Covered Health Service categories described in Section 1: Covered Health Services, those limits are stated in the corresponding Covered Health Service category in the Schedule of Benefits. Limits may also apply to some Covered Health Services that fall under more than one Covered Health Service category. When this occurs, those limits are also stated in the Schedule of Benefits under the heading Benefit Limits. Please review all limits carefully, as we will not pay Benefits for any of the services, treatments, items or supplies that exceed these Benefit limits. Please note that in listing services or examples, when we say this includes, it is not our intent to limit the description to that specific list. When we do intend to limit a list of services or examples, we state specifically that the list is limited to.
22 Prior Authorization We require prior authorization for certain Covered Health Services. In general, Network providers are responsible for obtaining prior authorization before they provide these services to you. There are some Benefits, however, for which you are responsible for obtaining prior authorization. Services for which prior authorization is required are identified below and in the Schedule of Benefits table within each Covered Health Service category. We recommend that you confirm with us that all Covered Health Services listed below have been prior authorized as required. Before receiving these services from a Network provider, you may want to contact us to verify that the Hospital, Physician and other providers are Network providers and that they have obtained the required prior authorization. Network facilities and Network providers cannot bill you for services they fail to prior authorize as required. You can contact us by calling the telephone number for Customer Care on your ID card. To obtain prior authorization, call the telephone number for Customer Care on your ID card. This call starts the utilization review process. Once you have obtained the authorization, please review it carefully so that you understand what services have been authorized and what providers are authorized to deliver the services that are subject to the authorization. The utilization review process is a set of formal techniques designed to monitor the use of, or evaluate the clinical necessity, appropriateness, efficacy, or efficiency of, health care services, procedures or settings. Such techniques may include ambulatory review, prospective review, second opinion, certification, concurrent review, case management, discharge planning, retrospective review or similar programs. Covered Health Services which Require Prior Authorization Please note that prior authorization timelines apply. Refer to the applicable Benefit description in the Schedule of Benefits table to determine how far in advance you must obtain prior authorization. [Include bracketed variable benefit category listed below if: a) the benefit is included in the plan design and b) prior authorization is required. Include dollar amounts as applicable.] Ambulance - non-emergent air and ground. Clinical trials. [Congenital heart disease surgery.] [Dental services - accidental.] [Infertility services.] [In-vitro fertilization services.] [Obesity surgery.] [Speech and Hearing services.] Transplants. If you request a coverage determination at the time prior authorization is provided, the determination will be made based on the services you report you will be receiving. If the reported services differ from those actually received, our final coverage determination will be modified to account for those differences, and we will only pay Benefits based on the services actually delivered to you. If you choose to receive a service that has been determined not to be a Medically Necessary Covered Health Service, you will be responsible for paying all charges and no Benefits will be paid. Care Management When you seek prior authorization as required, we will work with you to implement the care management process and to provide you with information about additional services that are available to you, such as disease management programs, health education, and patient advocacy. If you are undergoing a course of treatment from a Network provider at the time that Network provider is no longer contracted with us, you may be entitled to continue that care covered at the Network benefit level. Continuity of care is available in special circumstances in which the treating Physician or health care provider reasonably believes discontinuing care by the treating Physician could cause harm to the Covered Person. Special circumstances include WPD.EPO.I.11.TX R1
23 Covered Persons with a disability acute condition, life-threatening illness or past the 24th week of Pregnancy. The continuity of care request must be submitted by the treating Physician or provider. If continuity of care is approved, it may not be continued beyond 90 days after the Physician or provider is no longer contracted with us, if the Covered Person has been diagnosed as having a terminal illness at the time of the termination, or the expiration of the nine month period after the effective date of the termination. If the Covered Person is past the 24th week of Pregnancy at the time of termination, coverage at the Network level will continue through the delivery of the child, immediate postpartum care and the follow-up checkup within the six week period after delivery. If you have questions regarding this transition of care reimbursement policy or would like help determining whether you are eligible for transition of care Benefits, please contact Customer Care at the telephone number on your ID card. To resolve a question, complaint, or appeal, contact Customer Care at the telephone number shown on your ID card. Customer Care representatives are available to take your call during regular business hours, Monday through Friday. If you would rather send your complaint to us in writing, the Customer Care representative can provide you with the appropriate address. We will promptly investigate each complaint. The total time for acknowledgement, investigation and resolution of the complaint shall not exceed 30 calendar days after we receive the written complaint. Complaints concerning presently occurring Emergencies or denials of continued stays for hospitalization shall be investigated and resolved in accordance with the medical immediacy, and will not exceed one business day from receipt of the complaint. We will not engage in any retaliatory action against any Covered Person, anyone who has filed a complaint on behalf of the Covered Person or against a physician or provider. For a list of Network providers go to [ or call Customer Care at the telephone number on your ID card. Network providers may be found throughout the entire state of Texas, through the UnitedHealthcare Choice network. A list of network providers can be obtained by contacting us at the address or telephone number at the beginning of this summary or you may visit the UnitedHealthcare provider lookup website at [ If you would like a printed copy of providers, we will send it free of charge upon request. The number of insureds in the service area or region, the number of preferred providers in the areas of practice, including internal medicine, family/general practice, pediatric practitioner practice, obstetrics and gynecology, anesthesiology, psychiatry, and general surgery, and the number of preferred provider hospitals in the service area may be found at [UHICEPO Access Plan and Waiver]. If you would like a printed copy of this information, we will send it free of charge upon request. Network adequacy including any waivers can also be obtained by contacting us at the telephone number listed above, or you may go to [UHICEPO Access Plan and Waiver]. A printed copy may be requested and provided free of charge. WPD.EPO.I.11.TX R1
24 The number of contracted providers by specialty and hospitals are listed below by region. Region 1 Panhandle including Amarillo and Lubbock Region 2 Northwest Texas including Wichita Falls and Abilene Region 3 Metroplex including Fort Worth and Dallas Region 4 Northeast Texas including Tyler Region 5 Southeast Texas including Beaumont Region 6 Gulf Coast including Houston and Huntsville Region 7 Central Texas including Austin and Waco Region 8 South Central Texas including San Antonio Region 9 West Texas, including Midland, Odessa and San Angelo Region 10 Far West Texas including El Paso Region 11 Rio Grande Valley including Brownsville, Corpus Christi, and Laredo REGION Allergy Anesthesia Cardiology , , Dermatology Endocrinology Gastroenterology Hematology / Oncology , Infectious Disease Medicine Neonatology Nephrology Neurology OB/GYN , , Ophthalmology Orthopedic Surgery Otorhino-laryngology Pathology PCPs - Adult ,993 1, ,428 2,946 1, ,125 PCPs - Pediatric , ,185 2,736 1, ,296 PCPs - Pediatrician , , Pediatric Specialists , , Podiatry Pulmonary Medicine Radiology Rheumatology Surgery Surgery Specialized , , Urology Ambulatory Surgery Dialysis Center Disability/ Medical Rehab Extended/ Skilled Care Facility General/Acute Care Hospitals Home Health Hospice Laboratory MRI Radiation Oncology Facilities XRay & Radiology WPD.EPO.I.11.TX R1
25 Region 1 Panhandle including Amarillo and Lubbock Region 2 Northwest Texas including Wichita Falls and Abilene Region 3 Metroplex including Fort Worth and Dallas Region 4 Northeast Texas including Tyler Region 5 Southeast Texas including Beaumont Region 6 Gulf Coast including Houston and Huntsville Active access plans are in the place in the following specialties/region: Region 7 Central Texas including Austin and Waco Region 8 South Central Texas including San Antonio Region 9 West Texas, including Midland, Odessa and San Angelo Region 10 Far West Texas including El Paso Region 11 Rio Grande Valley including Brownsville, Corpus Christi, and Laredo REGION Primary Care Physicians yes Pediatric Physicians yes yes yes yes yes Obstetrics and yes yes yes yes yes yes yes yes Gynecology Anesthesiology yes yes yes yes yes The plan s membership by region is below: ,646 2, ,914 5,192 8, ,552 Texas Department of Insurance Notice An exclusive provider benefit plan provides no benefits for services you receive from out-of-network providers, with specific exceptions as described in your policy and below. You have the right to an adequate network of preferred providers (known as network providers ). If you believe that the network is inadequate, you may file a complaint with the Texas Department of Insurance. If your insurer approves a referral for out-of-network services because no preferred provider is available, or if you have received out-of-network emergency care, your insurer must, in most cases, resolve the nonpreferred provider s bill so that you only have to pay any applicable coinsurance, copay, and deductible amounts. You may obtain a current directory of preferred providers at the following website: myuhc.com or by calling the telephone number on your ID card for assistance in finding available preferred providers. If you relied on materially inaccurate directory information, you may be entitled to have an out-of-network claim paid at the in-network level of benefits. Insurance coverage provided by or through UnitedHealthcare Insurance Company or its affiliates. Administrative services provided by United HealthCare Services, Inc. or their affiliates. Health Plan coverage provided by or through UnitedHealthcare of Texas, Inc. MT / United HealthCare Services, Inc A Texas EPO Plans COC Series WPD.EPO.I.11.TX R1
UnitedHealthcare Insurance Company Plan Summary
 UnitedHealthcare Insurance Company Plan Summary PROVIDER PLAN (TX PPO Plans) This coverage is provided by UnitedHealthcare Insurance Company (UnitedHealthcare). This coverage provides different benefits
UnitedHealthcare Insurance Company Plan Summary PROVIDER PLAN (TX PPO Plans) This coverage is provided by UnitedHealthcare Insurance Company (UnitedHealthcare). This coverage provides different benefits
Schedule of Benefits
 Schedule of Benefits NHP Prime HMO plan for GIC members Exclusively for members of the Group Insurance Commission health plan meets Minimum Creditable Coverage standards and will satisfy the individual
Schedule of Benefits NHP Prime HMO plan for GIC members Exclusively for members of the Group Insurance Commission health plan meets Minimum Creditable Coverage standards and will satisfy the individual
UnitedHealthcare Choice Plus. United HealthCare Insurance Company. Certificate of Coverage
 UnitedHealthcare Choice Plus United HealthCare Insurance Company Certificate of Coverage For the Definity Health Savings Account (HSA) Plan 7PC of East Central College Enrolling Group Number: 711369 Effective
UnitedHealthcare Choice Plus United HealthCare Insurance Company Certificate of Coverage For the Definity Health Savings Account (HSA) Plan 7PC of East Central College Enrolling Group Number: 711369 Effective
UnitedHealthcare Choice Plus. UnitedHealthcare Insurance Company. Certificate of Coverage
 UnitedHealthcare Choice Plus UnitedHealthcare Insurance Company Certificate of Coverage For the Health Savings Account (HSA) Plan 7PA of Educators Benefit Services, Inc. Enrolling Group Number: 717578
UnitedHealthcare Choice Plus UnitedHealthcare Insurance Company Certificate of Coverage For the Health Savings Account (HSA) Plan 7PA of Educators Benefit Services, Inc. Enrolling Group Number: 717578
Schedule of Benefits
 Schedule of Benefits NHP Prime HMO plan for GIC members Exclusively for members of the Group Insurance Commission health plan meets Minimum Creditable Coverage standards and will satisfy the individual
Schedule of Benefits NHP Prime HMO plan for GIC members Exclusively for members of the Group Insurance Commission health plan meets Minimum Creditable Coverage standards and will satisfy the individual
UnitedHealthcare Choice Plus. UnitedHealthcare Insurance Company. Certificate of Coverage
 UnitedHealthcare Choice Plus UnitedHealthcare Insurance Company Certificate of Coverage For the Plan 21D of Big Walnut Local School District Enrolling Group Number: 753271 Effective Date: January 1, 2016
UnitedHealthcare Choice Plus UnitedHealthcare Insurance Company Certificate of Coverage For the Plan 21D of Big Walnut Local School District Enrolling Group Number: 753271 Effective Date: January 1, 2016
UnitedHealthcare Navigate. UnitedHealthcare Insurance Company. Certificate of Coverage
 UnitedHealthcare Navigate UnitedHealthcare Insurance Company Certificate of Coverage For Aurora Public Schools Enrolling Group Number: 716622 Effective Date: July 1, 2012 Offered and Underwritten by UnitedHealthcare
UnitedHealthcare Navigate UnitedHealthcare Insurance Company Certificate of Coverage For Aurora Public Schools Enrolling Group Number: 716622 Effective Date: July 1, 2012 Offered and Underwritten by UnitedHealthcare
UnitedHealthcare Choice Plus. Certificate of Coverage
 UnitedHealthcare Choice Plus Certificate of Coverage For the Plan QZB of Engility Corporation Enrolling Group Number: 906094 Effective Date: January 1, 2017 Offered and Underwritten by UnitedHealthcare
UnitedHealthcare Choice Plus Certificate of Coverage For the Plan QZB of Engility Corporation Enrolling Group Number: 906094 Effective Date: January 1, 2017 Offered and Underwritten by UnitedHealthcare
UnitedHealthcare Choice Plus. UnitedHealthcare of North Carolina, Inc. and. UnitedHealthcare Insurance Company. Certificate of Coverage
 UnitedHealthcare Choice Plus UnitedHealthcare of North Carolina, Inc. and UnitedHealthcare Insurance Company Certificate of Coverage For the Health Reimbursement Account (HRA) Plan AFU5 of City of Dunn
UnitedHealthcare Choice Plus UnitedHealthcare of North Carolina, Inc. and UnitedHealthcare Insurance Company Certificate of Coverage For the Health Reimbursement Account (HRA) Plan AFU5 of City of Dunn
Optimum Choice, Inc. Optimum Choice. Certificate of Coverage
 Optimum Choice, Inc. Optimum Choice Certificate of Coverage For the Optimum Choice Health Savings Account (HSA) Plan of AIMS Health Plan Enrolling Group Number: 717578 Effective Date: January 1, 2017 Optimum
Optimum Choice, Inc. Optimum Choice Certificate of Coverage For the Optimum Choice Health Savings Account (HSA) Plan of AIMS Health Plan Enrolling Group Number: 717578 Effective Date: January 1, 2017 Optimum
UnitedHealthcare Choice Plus. UnitedHealthcare Insurance Company of Illinois. Certificate of Coverage
 UnitedHealthcare Choice Plus UnitedHealthcare Insurance Company of Illinois Certificate of Coverage For the Plan J4Z of YWCA of Metropolitan Chicago Enrolling Group Number: 742540 Effective Date: July
UnitedHealthcare Choice Plus UnitedHealthcare Insurance Company of Illinois Certificate of Coverage For the Plan J4Z of YWCA of Metropolitan Chicago Enrolling Group Number: 742540 Effective Date: July
Student Health Insurance Plan Insurance Company Coverage Period: 08/15/ /14/2015
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.studentplanscenter.com or by calling 1-800-756-3702.
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.studentplanscenter.com or by calling 1-800-756-3702.
Annual deductibles and maximums In-network Out-of-network Lifetime maximum
 SUMMARY OF BENEFITS City of Richmond & Richmond Public Schools (Plan B) Connecticut General Life Insurance Co. Annual deductibles and maximums Lifetime maximum Unlimited per individual Pre-Existing Condition
SUMMARY OF BENEFITS City of Richmond & Richmond Public Schools (Plan B) Connecticut General Life Insurance Co. Annual deductibles and maximums Lifetime maximum Unlimited per individual Pre-Existing Condition
CONNECTICUT GENERAL LIFE INSURANCE COMPANY a CIGNA company (called CG) CERTIFICATE RIDER
 CERTIFICATE RIDER") Home Office: Bloomfield, Connecticut Mailing Address: Hartford, Connecticut 06152 CONNECTICUT GENERAL LIFE INSURANCE COMPANY a CIGNA company (called CG) CERTIFICATE RIDER No. CR7BIASO5-3 Policyholder:
Home Office: Bloomfield, Connecticut Mailing Address: Hartford, Connecticut 06152 CONNECTICUT GENERAL LIFE INSURANCE COMPANY a CIGNA company (called CG) CERTIFICATE RIDER No. CR7BIASO5-3 Policyholder:
SUMMARY OF BENEFITS Connecticut General Life Insurance Co.
 SUMMARY OF BENEFITS General Life Insurance Co. Tolland and Tolland Public Schools (H.S.A) Health Savings Account Your coverage includes a health savings account that you can use to pay for eligible out-of-pocket
SUMMARY OF BENEFITS General Life Insurance Co. Tolland and Tolland Public Schools (H.S.A) Health Savings Account Your coverage includes a health savings account that you can use to pay for eligible out-of-pocket
SUMMARY OF BENEFITS. Cigna Health and Life Insurance Co. RADCO Open Access Plus - Plan 1
 SUMMARY OF BENEFITS Cigna Health and Life Insurance Co. RADCO Open Access Plus - Plan 1 General Services In-Network Out-of-Network Physician office visit Primary Care Physician (PCP) Physician Office Visit
SUMMARY OF BENEFITS Cigna Health and Life Insurance Co. RADCO Open Access Plus - Plan 1 General Services In-Network Out-of-Network Physician office visit Primary Care Physician (PCP) Physician Office Visit
DRAFT NCOIL OUT-OF-NETWORK BALANCE BILLING TRANSPARENCY MODEL ACT
 DRAFT NCOIL OUT-OF-NETWORK BALANCE BILLING TRANSPARENCY MODEL ACT Section 1. Title This Act shall be known as the Out-of-Network Balance Billing Transparency Act. Section 2. Purpose The purpose of this
DRAFT NCOIL OUT-OF-NETWORK BALANCE BILLING TRANSPARENCY MODEL ACT Section 1. Title This Act shall be known as the Out-of-Network Balance Billing Transparency Act. Section 2. Purpose The purpose of this
National Council of Insurance Legislators (NCOIL) OUT-OF-NETWORK BALANCE BILLING TRANSPARENCY MODEL ACT
 OUT-OF-NETWORK BALANCE BILLING TRANSPARENCY MODEL ACT") National Council of Insurance Legislators (NCOIL) OUT-OF-NETWORK BALANCE BILLING TRANSPARENCY MODEL ACT Adopted by the Health, Long Term Care, and Health Retirement Issues Committee on November 18, 2017
National Council of Insurance Legislators (NCOIL) OUT-OF-NETWORK BALANCE BILLING TRANSPARENCY MODEL ACT Adopted by the Health, Long Term Care, and Health Retirement Issues Committee on November 18, 2017
Description of Coverage for UnitedHealthcare of Illinois, Inc.
 UnitedHealthcare Choice UnitedHealthcare Core UnitedHealthcare Navigate Description of Coverage for UnitedHealthcare of Illinois, Inc. The Managed Care Reform and Patient Rights Act of 1999 established
UnitedHealthcare Choice UnitedHealthcare Core UnitedHealthcare Navigate Description of Coverage for UnitedHealthcare of Illinois, Inc. The Managed Care Reform and Patient Rights Act of 1999 established
PROVIDER MANUAL. In the Colorado Access Provider Manual, you will find information about:
 In the Colorado Access Provider Manual, you will find information about: Section 1. Colorado Access General Information Section 2. Colorado Access Policies Section 3. Quality Management Section 4. Provider
In the Colorado Access Provider Manual, you will find information about: Section 1. Colorado Access General Information Section 2. Colorado Access Policies Section 3. Quality Management Section 4. Provider
This is a summary of what the plan does and does not cover. This summary can also help you understand your share
 Benefit Summary Iowa - Heritage Select Plus HDHP - Plan IWAQ Modified What is a benefit summary? This is a summary of what the plan does and does not cover. This summary can also help you understand your
Benefit Summary Iowa - Heritage Select Plus HDHP - Plan IWAQ Modified What is a benefit summary? This is a summary of what the plan does and does not cover. This summary can also help you understand your
Important Questions Answers Why this Matters:
 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual Plan Type: Premium Plan This is only a summary. If you want more detail about your coverage and costs, you
Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual Plan Type: Premium Plan This is only a summary. If you want more detail about your coverage and costs, you
SUMMARY OF BENEFITS. Cigna Health and Life Insurance Co. RADCO Health Savings Account Open Access Plus
 SUMMARY OF BENEFITS Cigna Health and Life Insurance Co. RADCO Health Savings Account Open Access Plus General Services In-Network Out-of-Network Physician office visit Primary Care Physician (PCP) Physician
SUMMARY OF BENEFITS Cigna Health and Life Insurance Co. RADCO Health Savings Account Open Access Plus General Services In-Network Out-of-Network Physician office visit Primary Care Physician (PCP) Physician
SCHEDULE OF BENEFITS UNIVERSITY OF PITTSBURGH PPO PLAN - Applies to PA Child Welfare Resource Center
 SCHEDULE OF BENEFITS UNIVERSITY OF PITTSBURGH PPO PLAN - Applies to PA Child Welfare Resource Center The following Schedule of Benefits is part of your Certificate of Coverage. It sets forth benefit limits
SCHEDULE OF BENEFITS UNIVERSITY OF PITTSBURGH PPO PLAN - Applies to PA Child Welfare Resource Center The following Schedule of Benefits is part of your Certificate of Coverage. It sets forth benefit limits
Some of the services this plan doesn t cover are listed on page 5. See your policy Yes plan doesn t cover?
 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual Plan Type: Network This is only a summary. If you want more detail about your coverage and costs, you can
Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual Plan Type: Network This is only a summary. If you want more detail about your coverage and costs, you can
You can see the specialist you choose without permission from this plan.
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.crystalrunhealthinsurancecompany.com or by calling 1-844-638-6506.
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.crystalrunhealthinsurancecompany.com or by calling 1-844-638-6506.
SUMMARY OF BENEFITS. Montgomery College Open Access Plus Coinsurance Plan. Connecticut General Life Insurance Co. Notice of Grandfathered Plan Status
 SUMMARY OF BENEFITS Connecticut General Life Insurance Co. Notice of Grandfathered Plan Status This plan is being treated as a grandfathered health plan under the Patient Protection and Affordable Care
SUMMARY OF BENEFITS Connecticut General Life Insurance Co. Notice of Grandfathered Plan Status This plan is being treated as a grandfathered health plan under the Patient Protection and Affordable Care
HMO Louisiana, Inc.: Blue POS copay 80/60 $500 Summary of Benefits and Coverage: What this Plan Covers & What it Costs
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.bcbsla.com or by calling 1-800-495-2583. Important Questions
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.bcbsla.com or by calling 1-800-495-2583. Important Questions
HMO Beyond %_RX 10/30/50
 HMO Beyond 3030 100%_RX 10/30/50 Summary of Benefits and CoverageWhat this plan Covers & What it Costs: This is only a summary. If you want more detail about your coverage and costs, you can get the complete
HMO Beyond 3030 100%_RX 10/30/50 Summary of Benefits and CoverageWhat this plan Covers & What it Costs: This is only a summary. If you want more detail about your coverage and costs, you can get the complete
AvMed In-Network Tier A Providers: $1,500 individual / $3,000 family AvMed In-Network Tier B Providers: What is the overall deductible?
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.avmed.org or by calling 1-800-477-8768. Important Questions
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.avmed.org or by calling 1-800-477-8768. Important Questions
Schedule of Benefits. Plan Information Participating Provider Non-Participating Provider
 Schedule of Benefits Panther Basic HSA PPO - Premium Network Deductible: $1,500 / $3,000 Coinsurance: 30% Total Annual Out-of-Pocket: $5,000 / $10,000 Primary Care Provider: 30% after Deductible Specialist:
Schedule of Benefits Panther Basic HSA PPO - Premium Network Deductible: $1,500 / $3,000 Coinsurance: 30% Total Annual Out-of-Pocket: $5,000 / $10,000 Primary Care Provider: 30% after Deductible Specialist:
Important Questions Answers Why this Matters:
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the plan document at http://www.osc.ct.gov/benefits/docs/plandocumentfinal1012015.pdf. Important
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the plan document at http://www.osc.ct.gov/benefits/docs/plandocumentfinal1012015.pdf. Important
Important Questions Answers Why this Matters: In-network: $2,100 person /
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.mhc.coop or by calling (855) 488-0622. Important Questions
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.mhc.coop or by calling (855) 488-0622. Important Questions
Important Questions Answers Why this Matters:
 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual + Family Plan Type: PPO This is only a summary. If you want more detail about your coverage and costs, you
Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual + Family Plan Type: PPO This is only a summary. If you want more detail about your coverage and costs, you
Important Questions Answers Why this Matters:
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at https://eoc.anthem.com/eocdps/fi or by calling 1-800-542-9402.
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at https://eoc.anthem.com/eocdps/fi or by calling 1-800-542-9402.
Summary of Benefits Prominence HealthFirst Small Group Health Plan
 Prominence Nevada Gold A Plus In-Network Calendar Year Deductible (CYD) 2 $1,000 Single / $3,000 Family Summary of Benefits $2,000 Single / $6,000 Family Coinsurance - Member responsibility 20% coinsurance
Prominence Nevada Gold A Plus In-Network Calendar Year Deductible (CYD) 2 $1,000 Single / $3,000 Family Summary of Benefits $2,000 Single / $6,000 Family Coinsurance - Member responsibility 20% coinsurance
Important Questions Answers Why this Matters:
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.crystalrunhp.com or by calling 1-844-638-6506. Important
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.crystalrunhp.com or by calling 1-844-638-6506. Important
Tier 1: $0/$0 Tier 2: $500/$1,500 Tier 3:$1,000/$3,000 Does not apply to preventive care. What is the overall deductible?
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document by contacting benefits@northside.com or by calling 1-404-851-8393.
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document by contacting benefits@northside.com or by calling 1-404-851-8393.
Important Questions Answers Why this Matters: What is the overall deductible? Are there other deductibles for specific services?
 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual Plan Type: Prev. Plus Plan This is only a summary. If you want more detail about your coverage and costs,
Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual Plan Type: Prev. Plus Plan This is only a summary. If you want more detail about your coverage and costs,
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.networkhealth.com/benefits/sbc/individualpolicy.pdf or
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.networkhealth.com/benefits/sbc/individualpolicy.pdf or
Important Questions Answers Why this Matters:
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.askallegiance.com/mckinney or by calling 1-855-999-1054.
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.askallegiance.com/mckinney or by calling 1-855-999-1054.
California Natural Products: EPO Option Coverage Period: 01/01/ /31/2017
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.deltahealthsystems.com or by calling 1-209-858-2525 Ext
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.deltahealthsystems.com or by calling 1-209-858-2525 Ext
JHHSC/JHH EHP Medical Plan Coverage Period: 01/01/ /31/2014
 JHHSC/JHH EHP Medical Plan Coverage Period: 01/01/2014 12/31/2014 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual Plan Type: PPO This is only a summary.
JHHSC/JHH EHP Medical Plan Coverage Period: 01/01/2014 12/31/2014 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual Plan Type: PPO This is only a summary.
Employee Benefit Plan: Missoula County Public Schools Coverage Period: 01/01/ /31/2014 Summary of Benefits and Coverage:
 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual Plan Type: HDHP This is only a summary. If you want more detail about your coverage and costs, you can get
Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual Plan Type: HDHP This is only a summary. If you want more detail about your coverage and costs, you can get
Important Questions Answers Why this Matters: What is the overall deductible? Are there other deductibles for specific services?
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.empireblue.com or by calling 1-800-342-9816. Important
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.empireblue.com or by calling 1-800-342-9816. Important
Important Questions Answers Why this Matters:
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.anthem.com or by calling 1-855-333-5735. Important Questions
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.anthem.com or by calling 1-855-333-5735. Important Questions
HMO Louisiana, Inc.: Blue Connect POS Copay 70/50 $3000 Summary of Benefits and Coverage: What this Plan Covers & What it Costs
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.bcbsla.com or by calling 1-800-599-2583. Important Questions
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.bcbsla.com or by calling 1-800-599-2583. Important Questions
SUMMARY OF BENEFITS Fisk University Open Access Plus -BUY-UP PLAN Effective 10/1/2015 Customer Service:
 SUMMARY OF BENEFITS Fisk University Open Access Plus -BUY-UP PLAN Effective www.mycigna.com Customer Service: 866-494-2111 Cigna Health and Life Insurance Co. General Services In-Network Out-of-Network
SUMMARY OF BENEFITS Fisk University Open Access Plus -BUY-UP PLAN Effective www.mycigna.com Customer Service: 866-494-2111 Cigna Health and Life Insurance Co. General Services In-Network Out-of-Network
You don t have to meet deductibles for specific services, but see the chart starting on page 3 for other costs for services this plan covers.
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.nipponlifebenefits.com or by calling 1-800-374-1835.
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.nipponlifebenefits.com or by calling 1-800-374-1835.
Important Questions Answers Why this Matters:
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.anthem.com or by calling 1-800-843-6447. Important Questions
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.anthem.com or by calling 1-800-843-6447. Important Questions
Important Questions Answers Why this Matters:
 Important Questions Answers Why this Matters: What is the overall deductible? Are there other deductibles for specific services? Is there an out of pocket limit on my expenses? $1,500 single / $3,000 family
Important Questions Answers Why this Matters: What is the overall deductible? Are there other deductibles for specific services? Is there an out of pocket limit on my expenses? $1,500 single / $3,000 family
Schedule of Benefits Summary Group Name: Nebraska Bankers Association VEBA Effective Date: January 01, 2018
 Schedule of Benefits Summary Group Name: Nebraska Bankers Association VEBA Effective Date: January 01, 2018 Payment for Services Covered Services are reimbursed based on the Allowable Charge. Blue Cross
Schedule of Benefits Summary Group Name: Nebraska Bankers Association VEBA Effective Date: January 01, 2018 Payment for Services Covered Services are reimbursed based on the Allowable Charge. Blue Cross
SUMMARY OF BENEFITS. Alliance Behavioral Healthcare Open Access Plus Plan Effective 7/1/12. Cigna Health and Life Insurance Co.
 SUMMARY OF BENEFITS Cigna Health and Life Insurance Co. Alliance Behavioral Healthcare Effective 7/1/12 Network: GWH/CIGNA Open Access Plus CIGNA has multiple networks. Your plan is paired with the GWH-CIGNA
SUMMARY OF BENEFITS Cigna Health and Life Insurance Co. Alliance Behavioral Healthcare Effective 7/1/12 Network: GWH/CIGNA Open Access Plus CIGNA has multiple networks. Your plan is paired with the GWH-CIGNA
Anthem BlueCross BlueShield Christian Care Communities Blue Access PPO Coverage Period: 01/01/ /31/2015 Summary of Benefits and Coverage:
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.anthem.com or by calling 1-888-650-4047. Important Questions
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.anthem.com or by calling 1-888-650-4047. Important Questions
Benefits. Guide to. Small Business Health Plan Hawaii Choice - A
 Guide to Benefits Small Business Health Plan Hawaii Choice - A (Includes Drug and Children's Vision) Health Maintenance Organization (HMO) January 2016 An Independent Licensee of the Blue Cross and Blue
Guide to Benefits Small Business Health Plan Hawaii Choice - A (Includes Drug and Children's Vision) Health Maintenance Organization (HMO) January 2016 An Independent Licensee of the Blue Cross and Blue
Health Plan Benefits and Coverage Matrix
 Health Plan Benefits and Coverage Matrix THIS MATRI IS INTENDED TO BE USED TO HELP YOU COMPARE COVERAGE BENEFITS AND IS A SUMMARY ONLY. THE EVIDENCE OF COVERAGE AND PLAN CONTRACT SHOULD BE CONSULTED FOR
Health Plan Benefits and Coverage Matrix THIS MATRI IS INTENDED TO BE USED TO HELP YOU COMPARE COVERAGE BENEFITS AND IS A SUMMARY ONLY. THE EVIDENCE OF COVERAGE AND PLAN CONTRACT SHOULD BE CONSULTED FOR
Important Questions Answers Why this Matters:
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document by calling 1-585-343-0055 ext. 6415. Important Questions Answers
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document by calling 1-585-343-0055 ext. 6415. Important Questions Answers
Important Questions Answers Why this Matters:
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.summacare.com or by calling 1-800-996-8701. Important
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.summacare.com or by calling 1-800-996-8701. Important
Yes, written or oral approval is required, based upon medical policies.
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.uhc.com/calpers or by calling 1-877-359-3714. Important
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.uhc.com/calpers or by calling 1-877-359-3714. Important
You must pay all of the costs for these services up to the specific deductible amount before this plan begins to pay for these services.
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.avmed.org or by calling 1-800-477-8768. Important Questions
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.avmed.org or by calling 1-800-477-8768. Important Questions
Student Health Insurance Plan Insurance Company Coverage Period: 08/01/ /31/2016
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.studentplanscenter.com or by calling 1-800-756-3702.
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.studentplanscenter.com or by calling 1-800-756-3702.
Health Plan Benefits and Coverage Matrix
 Health Plan Benefits and Coverage Matrix THIS MATRI IS INTENDED TO BE USED TO HELP YOU COMPARE COVERAGE BENEFITS AND IS A SUMMARY ONLY. THE EVIDENCE OF COVERAGE AND PLAN CONTRACT SHOULD BE CONSULTED FOR
Health Plan Benefits and Coverage Matrix THIS MATRI IS INTENDED TO BE USED TO HELP YOU COMPARE COVERAGE BENEFITS AND IS A SUMMARY ONLY. THE EVIDENCE OF COVERAGE AND PLAN CONTRACT SHOULD BE CONSULTED FOR
Emergency Department: $175 Copayment per visit Coinsurance: 0%
 Schedule of Benefits UPMC Small Business Advantage Primary Care Provider: $25 Copayment per visit Gold PPO $1,000 $25/$50 - Premium Network Specialist: $50 Copayment per visit Deductible: $1,000 / $2,000
Schedule of Benefits UPMC Small Business Advantage Primary Care Provider: $25 Copayment per visit Gold PPO $1,000 $25/$50 - Premium Network Specialist: $50 Copayment per visit Deductible: $1,000 / $2,000
Bronze LINK Coverage Period: 01/01/ /31/2016
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.mhc.coop or by calling (855) 447-2900. Important Questions
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.mhc.coop or by calling (855) 447-2900. Important Questions
Important Questions Answers Why this Matters:
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at https://eoc.anthem.com/eocdps/aso or by calling (855) 333-5735.
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at https://eoc.anthem.com/eocdps/aso or by calling (855) 333-5735.
Important Questions Answers Why this Matters:
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.anthem.com or by calling 1-877-309-2955. Important Questions
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.anthem.com or by calling 1-877-309-2955. Important Questions
Important Questions Answers Why this Matters:
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.arcsvs.com or by calling 1-877-309-2955. Important Questions
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.arcsvs.com or by calling 1-877-309-2955. Important Questions
Scott & White Health Plan: ERS Coverage Period: 9/1/2015 8/31/2016 Summary of Benefits and Coverage:
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.ers.swhp.org or by calling (800) 321-7947, TTY (800)
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.ers.swhp.org or by calling (800) 321-7947, TTY (800)
UnitedHealthcare Life Ins Co: Silver Copay Select 2 Coverage Period: Beginning on or after 01/01/2015 Summary of Benefits and Coverage:
 UnitedHealthcare Life Ins Co: Silver Copay Select 2 Coverage Period: Beginning on or after 01/01/2015 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual/Family
UnitedHealthcare Life Ins Co: Silver Copay Select 2 Coverage Period: Beginning on or after 01/01/2015 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual/Family
New York Student Health Plan. This is Your INSURANCE CERTIFICATE OF COVERAGE. Issued by. Manhattan School of Music
 New York Student Health Plan This is Your INSURANCE CERTIFICATE OF COVERAGE Issued by Manhattan School of Music This Certificate of Coverage ( Certificate ) explains the benefits available to You under
New York Student Health Plan This is Your INSURANCE CERTIFICATE OF COVERAGE Issued by Manhattan School of Music This Certificate of Coverage ( Certificate ) explains the benefits available to You under
UnitedHealthcare Non-Differential PPO. UnitedHealthcare Insurance Company. Certificate of Coverage
 UnitedHealthcare Non-Differential PPO UnitedHealthcare Insurance Company Certificate of Coverage For the Plan 7IF of LADWP Enrolling Group Number: 742149 Effective Date: July 1, 2011 Offered and Underwritten
UnitedHealthcare Non-Differential PPO UnitedHealthcare Insurance Company Certificate of Coverage For the Plan 7IF of LADWP Enrolling Group Number: 742149 Effective Date: July 1, 2011 Offered and Underwritten
UnitedHealthcare: Choice Plus HRA Coverage Period: 01/01/ /31/2015 Summary of Benefits and Coverage
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.myuhc.com or by calling 1-866-314-0335. Important Questions
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.myuhc.com or by calling 1-866-314-0335. Important Questions
Other Participating UPMC Facilities Level 2 Benefit Period
 Schedule of Benefits Advantage Panther Gold Plan - Enhanced Access HMO Applies to Oakland and Titusville campuses HMO Deductible: $0 / $0 Coinsurance: 0% Total Annual Out-of-Pocket: $1,800 / $3,600 Primary
Schedule of Benefits Advantage Panther Gold Plan - Enhanced Access HMO Applies to Oakland and Titusville campuses HMO Deductible: $0 / $0 Coinsurance: 0% Total Annual Out-of-Pocket: $1,800 / $3,600 Primary
$0 See the chart starting on page 2 for your costs for services this plan covers.
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at https://www.chchealth.org/affordablehealth/planbrochure/silver.aspx
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at https://www.chchealth.org/affordablehealth/planbrochure/silver.aspx
Eastern Shore of Maryland Educational Consortium EPO (Non-Grandfathered) Coverage Period: 09/01/ /31/2017
 Coverage Period: 09/01/ /31/2017") Eastern Shore of Maryland Educational Consortium EPO (Non-Grandfathered) Coverage Period: 09/01/2016-08/31/2017 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual
Eastern Shore of Maryland Educational Consortium EPO (Non-Grandfathered) Coverage Period: 09/01/2016-08/31/2017 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual
SCHEDULE OF BENEFITS ADVANTAGE PANTHER GOLD PLAN Enhanced Access HMO Applies to Oakland, Johnstown, and Titusville campuses
 SCHEDULE OF BENEFITS ADVANTAGE PANTHER GOLD PLAN Enhanced Access HMO Applies to Oakland, Johnstown, and Titusville campuses This document is called a Schedule of Benefits. It is part of your Certificate
SCHEDULE OF BENEFITS ADVANTAGE PANTHER GOLD PLAN Enhanced Access HMO Applies to Oakland, Johnstown, and Titusville campuses This document is called a Schedule of Benefits. It is part of your Certificate
PROVIDER MANUAL. In the Colorado Access Provider Manual, you will find information about:
 In the Colorado Access Provider Manual, you will find information about: Section 1. Colorado Access General Information Section 2. Colorado Access Policies Section 3. Quality Management Section 4. Provider
In the Colorado Access Provider Manual, you will find information about: Section 1. Colorado Access General Information Section 2. Colorado Access Policies Section 3. Quality Management Section 4. Provider
Important Questions Answers Why this Matters:
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.etf.wi.gov or by calling 1-877-533-5020. Important Questions
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.etf.wi.gov or by calling 1-877-533-5020. Important Questions
Anthem Blue Cross CalPERS Exclusive Provider Organization EPO Monterey County Coverage Period: 01/01/ /31/2017
 CalPERS Exclusive Organization EPO Monterey County This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.anthem.com/ca/calpers
CalPERS Exclusive Organization EPO Monterey County This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.anthem.com/ca/calpers
Important Questions Answers Why this Matters:
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.etf.wi.gov or by calling 1-877-533-5020. Important Questions
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.etf.wi.gov or by calling 1-877-533-5020. Important Questions
1199SEIU National Benefit Fund Summary of Benefits and Coverage: What This Plan Covers and What It Costs
 1199SEIU National Benefit Fund Summary of Benefits and Coverage: What This Plan Covers and What It Costs Coverage Period: Beginning 04/01/2014 Coverage for: Wage Classes I & II and Early Retirees with
1199SEIU National Benefit Fund Summary of Benefits and Coverage: What This Plan Covers and What It Costs Coverage Period: Beginning 04/01/2014 Coverage for: Wage Classes I & II and Early Retirees with
An Overview of Your Health and Dental Benefits
 An Overview of Your Health and Dental Benefits Educators Health Alliance Direct Bill Plan 2 \ EDUCATORS HEALTH ALLIANCE HEALTH AND DENTAL PLAN OPTIONS Exclusively for Educators Health Alliance Direct Bill
An Overview of Your Health and Dental Benefits Educators Health Alliance Direct Bill Plan 2 \ EDUCATORS HEALTH ALLIANCE HEALTH AND DENTAL PLAN OPTIONS Exclusively for Educators Health Alliance Direct Bill
Important Questions Answers Why this Matters:
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.anthem.com or by calling 1-855-603-7982. Important Questions
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.anthem.com or by calling 1-855-603-7982. Important Questions
CalPERS: Sharp Performance Plus HMO Summary of Benefits and Coverage: What this Plan Covers & What it Costs
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.sharphealthplan.com/calpers or by calling 1-855-995-5004.
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.sharphealthplan.com/calpers or by calling 1-855-995-5004.
Total Health Care USA, Inc.: Total Saver Complete Summary of Benefits and Coverage: What this Plan Covers & What it Costs
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.thcmi.com or by calling 1-800-826-2862 Important Questions
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.thcmi.com or by calling 1-800-826-2862 Important Questions
Important Questions Answers Why this Matters:
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.healthplan.memorialhermann.org or by calling 1-888-594-0671.
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.healthplan.memorialhermann.org or by calling 1-888-594-0671.
NETWORK: $500 single / $1,000 family maximum for in-network providers and $750 single / $1,500 family maximum for out-ofnetwork
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.clftpaedi.com or by calling 888-244-5096. Important Questions
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.clftpaedi.com or by calling 888-244-5096. Important Questions
Important Questions Answers Why this Matters:
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.crystalrunhp.com or by calling 1-844-638-6506. Important
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.crystalrunhp.com or by calling 1-844-638-6506. Important
Important Questions Answers Why this Matters:
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.healthplan.memorialhermann.org or by calling 1-888-594-0671.
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.healthplan.memorialhermann.org or by calling 1-888-594-0671.
Benefits Summary Direct HMO / HMO For Groups with 2-50 Eligible Employees (Eff. 10/01/10, Pending NYS Dept. of Insurance Approval)
") Copayment Options 1 Inpatient Copayment Primary (PCP) Copayment Specialist Copayment ER Copayment Option 12 copayment* copayment 1 $50 copayment 1 $150 copayment *Per admission/maximum per calendar year
Copayment Options 1 Inpatient Copayment Primary (PCP) Copayment Specialist Copayment ER Copayment Option 12 copayment* copayment 1 $50 copayment 1 $150 copayment *Per admission/maximum per calendar year
Important Questions Answers Why this Matters:
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.capitalhealth.com or by calling 1-850-383-3311. Important
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.capitalhealth.com or by calling 1-850-383-3311. Important
Total Health Care USA, Inc.: Totally You Summary of Benefits and Coverage: What this Plan Covers & What it Costs
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.thcmi.com or by calling 1-800-826-2862 Important Questions
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.thcmi.com or by calling 1-800-826-2862 Important Questions
Important Questions Answers Why this Matters: For in-network providers Deductible is not applicable innetwork
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.anthem.com or by calling 1-800-922-6621. Important Questions
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.anthem.com or by calling 1-800-922-6621. Important Questions
Important Questions Answers Why this Matters: What is the overall deductible? Are there other deductibles for specific services?
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.avmed.org/go/state or by calling 1-888-762-8633 Important
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.avmed.org/go/state or by calling 1-888-762-8633 Important
BridgeSpan Health Company: BridgeSpan Oregon Standard Silver Plan Coverage Period: 01/01/2015
 BridgeSpan Health Company: BridgeSpan Oregon Standard Silver Plan Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage Period: 01/01/2015 01/01/2015 12/31/2015-12/31/2015 Coverage
BridgeSpan Health Company: BridgeSpan Oregon Standard Silver Plan Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage Period: 01/01/2015 01/01/2015 12/31/2015-12/31/2015 Coverage
Summary of Benefits Prominence HealthFirst Small Group Health Plan
 HealthFirst/ Calendar Year Deductible (CYD) 2 $1,000 Single / $3,000 Family Summary of Benefits $3,000 Single / $9,000 Family Coinsurance - Member responsibility 30% coinsurance 50% coinsurance Out-of-Pocket
HealthFirst/ Calendar Year Deductible (CYD) 2 $1,000 Single / $3,000 Family Summary of Benefits $3,000 Single / $9,000 Family Coinsurance - Member responsibility 30% coinsurance 50% coinsurance Out-of-Pocket
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan
 : Samford University Coverage Period: Beginning on or after 01/01/2015 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage For: Individual + Family Plan Type: PPO This is only
: Samford University Coverage Period: Beginning on or after 01/01/2015 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage For: Individual + Family Plan Type: PPO This is only
Important Questions Answers Why this Matters:
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at https://eoc.anthem.com/eocdps/fi or by calling (855) 333-5735.
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at https://eoc.anthem.com/eocdps/fi or by calling (855) 333-5735.
Anthem Blue Cross University of Southern California Modified Classic Choice HMO 30/40 Coverage Period: 01/01/ /31/2014
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.anthem.com/ca or by calling 1-800-888-8288. Important
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.anthem.com/ca or by calling 1-800-888-8288. Important
$0 family AvMed In-Network Tier B Providers: $0 individual / What is the overall deductible?
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.avmed.org or by calling 1-800-376-6651. Important Questions
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.avmed.org or by calling 1-800-376-6651. Important Questions