Underwritten By: ACE American Insurance Company Philadelphia, PA 19106
|
|
|
- Nathan Horn
- 5 years ago
- Views:
Transcription


1 Up to $1,000,000 Student Accident Medical Insurance Protection Underwritten By: ACE American Insurance Company Philadelphia, PA (Form MA) Important Notice: The Plan does not provide benefits for sickness of any kind.
2
3
4 To File A Claim: 1. Use attached claim form 2. Fill out all necessary information 3. Be sure to sign and date the bottom 4. Enclose any itemized bills or receipts from services rendered. 5. Send claim forms, itemized bills and receipts to: Lefebvre Insurance, LLC 850 Franklin Street Wrentham, MA (800) All Claims must be filed within One (1)Year of the Date of Service or as soon as reasonably possible. ENROLLMENT FORM CHECKLIST Did You: Fill out all of the appropriate information on the enrollment form (MAKE SURE SCHOOL DISTRICT IS CLEARLY LISTED) Check the appropriate box(s) for the coverage you have selected. Enclose a CHECK or MONEY ORDER for the total Premium (your cancelled check or money order stub will serve as proof of payment) along with the completed enrollment form in an envelope. For questions, inquiries, and information contact: Lefebvre Insurance, LLC 850 Franklin Street Wrentham, MA (800)
5 Please Print DO NOT SEND CASH Enrollment Form MA STUDENT S LAST NAME STUDENT S FIRST NAME MIDDLE INITIAL BIRTH DATE (MM/DD/YYYY) GRADE PHONE HOME ADDRESS APT# CITY ST ZIP SCHOOL SYSTEM/DISTRICT SCHOOL NAME Any person who knowingly and with intent to defraud any insurance company or other person files an enrollment form for insurance or statement of claim containing any materially false information or conceals for the purpose of misleading, information concerning any fact material thereto commits a fraudulent act, which is a crime and subjects such person to criminal and civil penalties. SIGNATURE OF PARENT OR GUARDIAN DATE My signature above certifies that I have read and understand the Student Accident Insurance Protection brochure and agree to accept the terms and conditions stated herein. No obligation to purchase. School Year Rate CHECK YOUR SELECTION Coverage Plans Premiums 24-Hour Including Extended Dental 1$ Hour Only 1$50.00 School Time Only Including Extended Dental 1$16.00 School Time Only 1$18.00 Make checks payable to: Lefebvre Insurance, LLC. or ACE American Insurance Company How to Enroll 1. Decide whether you want the School Time, 24-Hour Accident Protection (with or without Dental). 2. Fill out the enrollment form and enclose the form along with a check or money order made payable to the Administrator shown for the correct amount. 3. Mail envelope to Lefebvre Insurance, LLC. 850 Franklin Street Wrentham, MA Your cancelled check or money order stub will be your receipt and confirmation of payment. (Please write the student s name and school name on your check.) (MA) Ver. 1

6 LEFEBVRE INSURANCE, LLC 850 FRANKLIN STREET WRENTHAM, MA CLAIM ASSISTANCE:
7 CLAIM PROCEDURES 1. Submit all itemized bills to both your family insurance carrier and the insurance carrier for your school/organization. These bills are generally a HICFA form (Physician) or a UB92 form (Hospital). The Physician or Hospital has an assignment of Benefits on file; which was completed on the initial treatment visit. This assignment of Benefits will be honored. If your Provider does not bill on a HICFA or UB92 Form, You will need to sign the authorization to pay Benefits to the Provider on the front of this form. 2. If your family insurance carrier is an HMO organization, CONTACT YOUR HMO PHYSICIAN AT ONCE. FAILURE TO DO SO MAY RESULT IN THE CLAIM BEING DENIED OR A SUBSTANTIALLY REDUCED BENEFIT. 3. Your family insurance carrier will send you an Explanation of Benefits (E.O.B.) listing the payments made by them. Upon receipt of the E.O.B., forward the E.O.B. along with any unpaid itemized bills and a completed claim form to the claim administrator: Lefebvre Insurance, LLC for processing: paid receipts and/or balance due statements are not accepted. 4. If you do not have other valid and collectible insurance (Auto, Employer Provided, Family Insurance or Self- Provided): complete the information on the claim form, sign where indicated, include all your itemized bills, etc., and forward to the claim administration for processing. FRAUD WARNING Any person who knowingly and with intent to defraud any insurance company or other person files a statement of claim containing any materially false information or conceals for the purpose of misleading information concerning any fact material thereto commits a fraudulent insurance act, which is a crime and subjects such person to criminal and civil penalties. THINGS TO REMEMBER 1. TO SUBMIT ADDITIONAL BILLS AFTER THE ORIGINAL FORM HAS BEEN SENT IN, BE SURE TO INCLUDE THE FOLLOWING: (A) NAME OF CLAIMANT; (B) DATE OF ACCIDENT; (C) NAME OF THE POLICYHOLDER (SCHOOL, COLLEGE OR ORGANIZATION). 2. IF YOUR FAMILY INSURANCE CARRIER IS AN HMO ORGANIZATION, CONTACT YOUR HMO PHYSICIAN AT ONCE. 3. NOTICE OF CLAIM MUST BE FILED WITHIN 90 DAYS. YOU HAVE 52 WEEKS (ONE YEAR) FROM THE DATE OF SERVICE TO PRESENT ALL BILLS FOR THE PAYMENT OF A CLAIM TO BE CONSIDERED. 4. AUTHORIZATION TO RELEASE MEDICAL INFORMATION (MUST BE SIGNED) 5. PAYMENT WILL BE MADE TO THE SOURCE OF SERVICE (HOSPITAL, PHYSICIAN, ETC.) UNLESS CLAIM FORM ACCOMPANYING THE BILL INDICATES OTHERWISE AT THE TIME THE CLAIM IS SUBMITTED. IF YOU PAID FOR THE SERVICES AND REIMBURSEMENT IS TO BE PAID TO YOU, PROOF OF PAYMENT WILL BE REQUIRED AT THE TIME THE CLAIM IS SUBMITTED.
STUDENT ACCIDENT INSURANCE SCHOOL YEAR
 STUDENT ACCIDENT INSURANCE 2012-2013 SCHOOL YEAR This is a reminder to parents with a child or children attending school in our School District that we do not carry medical insurance on students, but do
STUDENT ACCIDENT INSURANCE 2012-2013 SCHOOL YEAR This is a reminder to parents with a child or children attending school in our School District that we do not carry medical insurance on students, but do
Up to $1,000,000 Student Accident Medical Insurance Protection Underwritten By: AXIS Insurance Company AMA_MA_PD_ K-12_
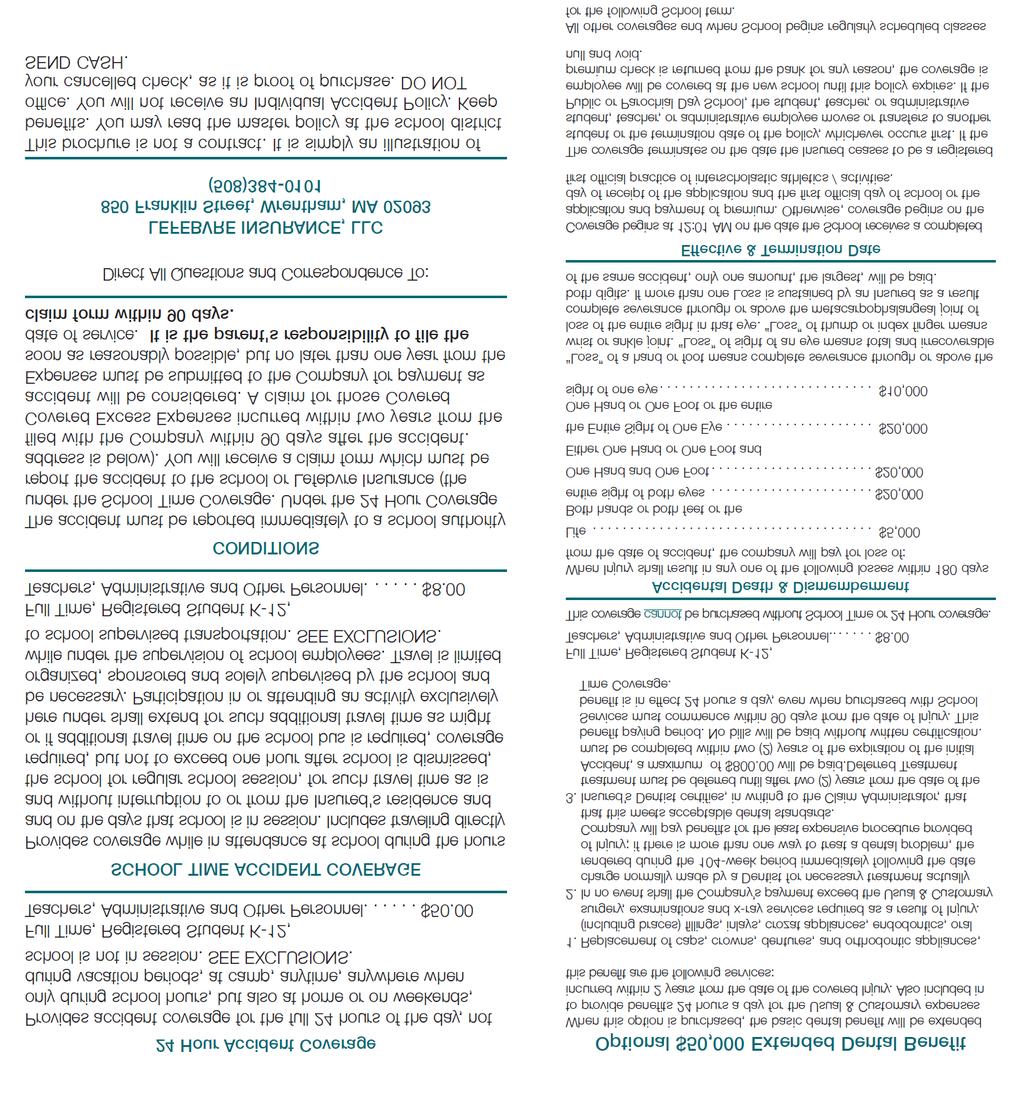
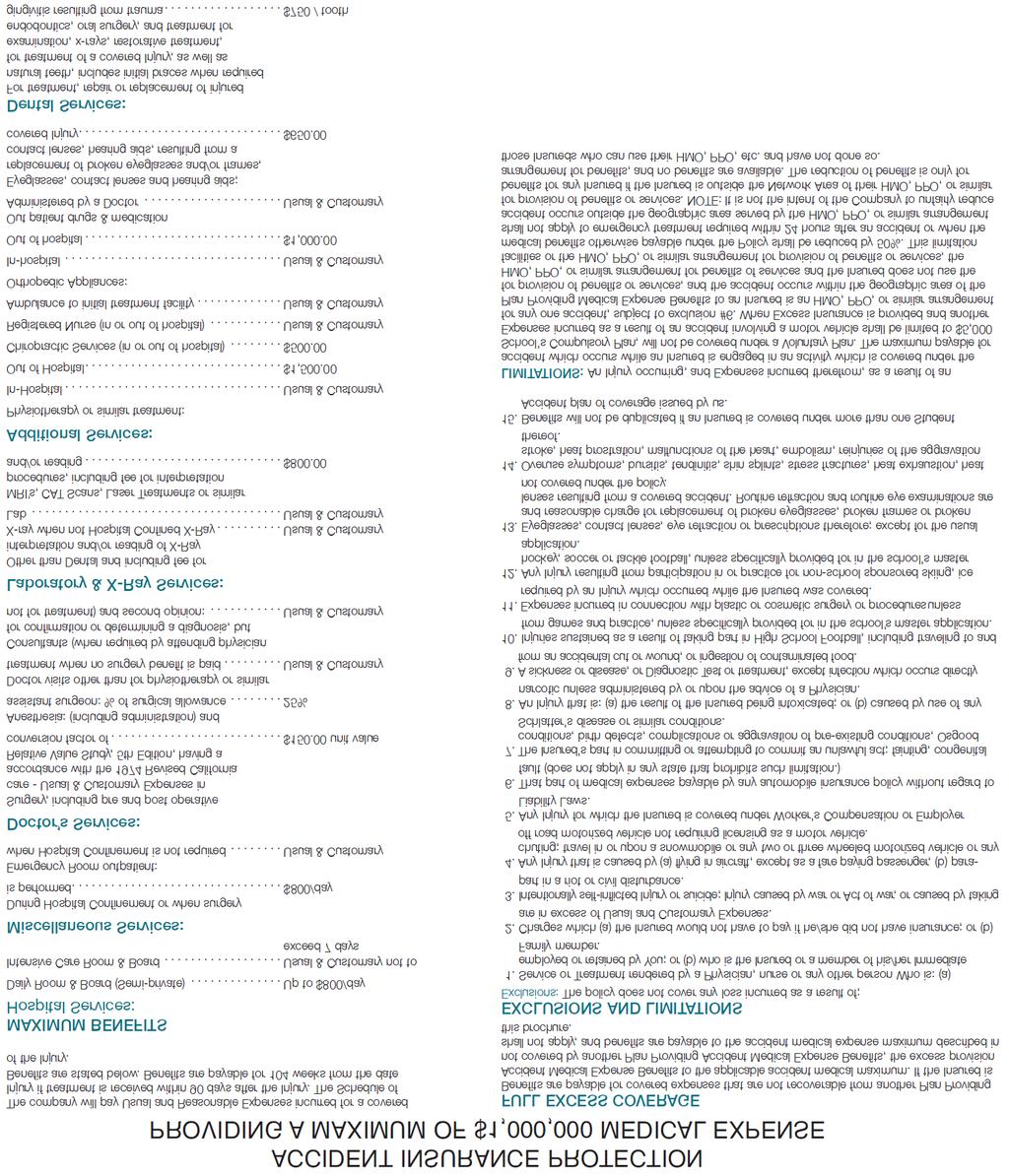
 Up to $1,000,000 Student Accident Medical Insurance Protection 2015-2016 Underwritten By: AXIS Insurance Company 24 Hour Accident Coverage Provides accident coverage for the full 24 hours of the day, not
Up to $1,000,000 Student Accident Medical Insurance Protection 2015-2016 Underwritten By: AXIS Insurance Company 24 Hour Accident Coverage Provides accident coverage for the full 24 hours of the day, not
STUDENT ACCIDENT INSURANCE SCHOOL YEAR
 STUDENT ACCIDENT INSURANCE 2017-2018 SCHOOL YEAR This is a reminder to parents with a child or children attending school in our School District that we do not carry medical insurance on students, but do
STUDENT ACCIDENT INSURANCE 2017-2018 SCHOOL YEAR This is a reminder to parents with a child or children attending school in our School District that we do not carry medical insurance on students, but do
INSTRUCTIONS FOR FILING A CLAIM LIMITED BENEFIT CANCER EXPENSE POLICY
 INSTRUCTIONS FOR FILING A CLAIM LIMITED BENEFIT CANCER EXPENSE POLICY The forms must be completed by the claimant. All questions on the forms must be answered in full. Incomplete or illegible answers may
INSTRUCTIONS FOR FILING A CLAIM LIMITED BENEFIT CANCER EXPENSE POLICY The forms must be completed by the claimant. All questions on the forms must be answered in full. Incomplete or illegible answers may
PART I POLICYHOLDER S REPORT
 1. PLEASE FULLY COMPLETE THIS FORM 2. ATTACH ITEMIZED BILLS 3. MAIL TO HSR E-mail : UBAclaims@hsri.com HSR Plaza II 4100 Medical Parkway Carrollton, Texas 75007 Phone: (972) 512-5600 Fax: (972) 512-5820
1. PLEASE FULLY COMPLETE THIS FORM 2. ATTACH ITEMIZED BILLS 3. MAIL TO HSR E-mail : UBAclaims@hsri.com HSR Plaza II 4100 Medical Parkway Carrollton, Texas 75007 Phone: (972) 512-5600 Fax: (972) 512-5820
Dear North Hills School District Families:
 Dear North Hills School District Families: The North Hills School District welcomes you to the 2018-2019 school year. With the start of a new school year, parents sometimes request information regarding
Dear North Hills School District Families: The North Hills School District welcomes you to the 2018-2019 school year. With the start of a new school year, parents sometimes request information regarding
For faster claim payment* please submit your claim online at
 Claims Made Easy For faster claim payment* please submit your claim online at www.combinedinsurance.com/claims FILING A CLAIM BY MAIL 1. Download the claim form 2. Print all six pages of the claim form
Claims Made Easy For faster claim payment* please submit your claim online at www.combinedinsurance.com/claims FILING A CLAIM BY MAIL 1. Download the claim form 2. Print all six pages of the claim form
STUDENT ACCIDENT REPORTING PROCEDURES INFORMATION SHEET
 Dear Parents, STUDENT ACCIDENT REPORTING PROCEDURES INFORMATION SHEET Your School Board continues to be vitally concerned about the health, safety, and welfare of all students. We encourage safety, but
Dear Parents, STUDENT ACCIDENT REPORTING PROCEDURES INFORMATION SHEET Your School Board continues to be vitally concerned about the health, safety, and welfare of all students. We encourage safety, but
ATHLETIC TRAINING ROOM POLICIES AND GUIDELINES NORTHWEST UNIVERSITY
 ATHLETIC TRAINING ROOM POLICIES AND GUIDELINES NORTHWEST UNIVERSITY Health care for intercollegiate athletes is unique to each sport and athlete. These policies and guidelines have been established to
ATHLETIC TRAINING ROOM POLICIES AND GUIDELINES NORTHWEST UNIVERSITY Health care for intercollegiate athletes is unique to each sport and athlete. These policies and guidelines have been established to
Underwritten by AXIS Insurance Company
 Up to $25,000 ($2,500 for Football) Student Accident Medical Insurance Protection 2017-2018 Underwritten by AXIS Insurance Company 24 Hour Accident Coverage Provides accident coverage for the full 24 hours
Up to $25,000 ($2,500 for Football) Student Accident Medical Insurance Protection 2017-2018 Underwritten by AXIS Insurance Company 24 Hour Accident Coverage Provides accident coverage for the full 24 hours
CLAIMS FILING INSTRUCTIONS
 ACCIDENT MEDICAL EXPENSE CLAIMS FILING INSTRUCTIONS In addition to the completed claim form, you must submit the following: For plans Underwritten by: National Health Insurance Company Integon National
ACCIDENT MEDICAL EXPENSE CLAIMS FILING INSTRUCTIONS In addition to the completed claim form, you must submit the following: For plans Underwritten by: National Health Insurance Company Integon National
Accident Medical Claim Form
 137 Main Street Dubuque, IA Accident Medical Claim Form Please read and follow these instructions should there be a need to file a claim for a covered accident. Your policy says you must notify us of your
137 Main Street Dubuque, IA Accident Medical Claim Form Please read and follow these instructions should there be a need to file a claim for a covered accident. Your policy says you must notify us of your
Individual Medicare Supplement Insurance
 Individual Medicare Supplement Insurance Application Form INSTRUCTIONS This is an application for Medicare Supplement Insurance underwritten by Group Health Incorporated ( GHI ), an EmblemHealth company.
Individual Medicare Supplement Insurance Application Form INSTRUCTIONS This is an application for Medicare Supplement Insurance underwritten by Group Health Incorporated ( GHI ), an EmblemHealth company.
PLEASE READ THIS INFORMATION CAREFULLY. It is important.
 PLEASE READ THIS INFORMATION CAREFULLY. It is important. PLEASE FOLLOW THESE INSTRUCTIONS TO FILE A CLAIM ALL INFORMATION MUST BE PROVIDED IN ORDER FOR CLAIM TO BE PROCESSED. PROCESSING OF YOUR CLAIM WILL
PLEASE READ THIS INFORMATION CAREFULLY. It is important. PLEASE FOLLOW THESE INSTRUCTIONS TO FILE A CLAIM ALL INFORMATION MUST BE PROVIDED IN ORDER FOR CLAIM TO BE PROCESSED. PROCESSING OF YOUR CLAIM WILL
Northwest University s Student Accident Excess Insurance Information
 Northwest University s Student Accident Excess Insurance Information Northwest University provides excess medical coverage for all students, and it is very important that Parents and Students understand
Northwest University s Student Accident Excess Insurance Information Northwest University provides excess medical coverage for all students, and it is very important that Parents and Students understand
Claim Form. What to Know About Filing Your Claim
 Corporate Office: Omaha, NE Administrative Services: PO Box 10464 Des Moines, IA 50306 137 Main Street Dubuque, IA 52001 Toll Free 855.637.6930 Claim Form What to Know About Filing Your Claim You can avoid
Corporate Office: Omaha, NE Administrative Services: PO Box 10464 Des Moines, IA 50306 137 Main Street Dubuque, IA 52001 Toll Free 855.637.6930 Claim Form What to Know About Filing Your Claim You can avoid
For faster claim payment* please submit your claim online at
 Claims Made Easy For faster claim payment* please submit your claim online at www.combinedinsurance.com/claims FILING A CLAIM BY MAIL 1. Download the claim form 2. Print all six pages of the claim form
Claims Made Easy For faster claim payment* please submit your claim online at www.combinedinsurance.com/claims FILING A CLAIM BY MAIL 1. Download the claim form 2. Print all six pages of the claim form
Hospital Indemnity Insurance
 Hospital Indemnity Insurance Instructions for filing a Claim Follow the instructions shown below in completing/providing documentation needed to file a claim for your hospital indemnity benefits. 1. Complete
Hospital Indemnity Insurance Instructions for filing a Claim Follow the instructions shown below in completing/providing documentation needed to file a claim for your hospital indemnity benefits. 1. Complete
Volunteer Accident Insurance Program
 Volunteer Accident Insurance Program Volunteer Information: As a registered OHSU volunteer you may be eligible for accident medical expense benefits if an injury or exposure occurs by accidental* means
Volunteer Accident Insurance Program Volunteer Information: As a registered OHSU volunteer you may be eligible for accident medical expense benefits if an injury or exposure occurs by accidental* means
GROUP LIFE CLAIM KIT FOR PROCESSING LIFE INSURANCE AND ACCIDENTAL DEATH BENEFITS INSTRUCTIONS FOR FILING A LIFE CLAIM
 GROUP LIFE CLAIM KIT FOR PROCESSING LIFE INSURANCE AND ACCIDENTAL DEATH BENEFITS INSTRUCTIONS FOR FILING A LIFE CLAIM PLEASE SUBMIT THE FOLLOWING: 1. THE CLAIM FORM (PAGE 2) FULLY COMPLETED BY THE EMPLOYER
GROUP LIFE CLAIM KIT FOR PROCESSING LIFE INSURANCE AND ACCIDENTAL DEATH BENEFITS INSTRUCTIONS FOR FILING A LIFE CLAIM PLEASE SUBMIT THE FOLLOWING: 1. THE CLAIM FORM (PAGE 2) FULLY COMPLETED BY THE EMPLOYER
Humana Insurance Company Cancer, Specified Disease and Intensive Care Coverage Claim Filing Instructions
 Humana Insurance Company Cancer, Specified Disease and Intensive Care Coverage Claim Filing Instructions How to file your first claim: 1. Complete each section of the first page of the claim form. 2. Attach
Humana Insurance Company Cancer, Specified Disease and Intensive Care Coverage Claim Filing Instructions How to file your first claim: 1. Complete each section of the first page of the claim form. 2. Attach
LOYAL AMERICAN LIFE INSURANCE COMPANY PO BOX 1604, DUNCAN, OKLAHOMA, Phone (800)
") INSTRUCTIONS FOR FILING A MEDICAL CLAIM CANCER TREATMENT The forms must be completed by the claimant. All questions on the forms must be answered in full. Incomplete or illegible answers may result in
INSTRUCTIONS FOR FILING A MEDICAL CLAIM CANCER TREATMENT The forms must be completed by the claimant. All questions on the forms must be answered in full. Incomplete or illegible answers may result in
Trip Cancellation/Interruption/Delay
 Trip Cancellation/Interruption/Delay HOW TO FILE A CLAIM 1. Complete all items on the attached claim form. 2. Attach the following documents: Copy of travel itinerary Verification of trip payment Original
Trip Cancellation/Interruption/Delay HOW TO FILE A CLAIM 1. Complete all items on the attached claim form. 2. Attach the following documents: Copy of travel itinerary Verification of trip payment Original
Life Insurance Benefits Application Instructions
 Application Instructions Please Read Carefully The application for life insurance benefits consists of the forms included in this packet, as well as the additional information noted under item 1 below.
Application Instructions Please Read Carefully The application for life insurance benefits consists of the forms included in this packet, as well as the additional information noted under item 1 below.
STUDENT ACCIDENT INSURANCE SCHOOL YEAR
 STUDENT ACCIDENT INSURANCE 2017-2018 SCHOOL YEAR This is a reminder to parents with a child or children attending school in our School District that we do not carry medical insurance on students, but do
STUDENT ACCIDENT INSURANCE 2017-2018 SCHOOL YEAR This is a reminder to parents with a child or children attending school in our School District that we do not carry medical insurance on students, but do
ADHD Physician Reporting Requirements for the Athletic Trainer
 ADHD Physician Reporting Requirements for the Athletic Trainer The following is the recommended minimum requirements for a letter from the prescribing physician to provide documentation to the Athletics
ADHD Physician Reporting Requirements for the Athletic Trainer The following is the recommended minimum requirements for a letter from the prescribing physician to provide documentation to the Athletics
Thank you. Should you have any questions, please call us at (800)
") Dear Policyholder: Please complete and sign the attached claim form. Additionally, the following items are needed in order to process your Medical/Dental claim in the most efficient and expedient way possible.
Dear Policyholder: Please complete and sign the attached claim form. Additionally, the following items are needed in order to process your Medical/Dental claim in the most efficient and expedient way possible.
North Carolina Application for Dental Insurance
 Section A. Dental Coverage Options: 1. Select who the coverage is for: Primary Applicant Only Primary Applicant and Dependent(s) Child(ren) Only 2. Select what coverage applicant(s) is/are applying for:
Section A. Dental Coverage Options: 1. Select who the coverage is for: Primary Applicant Only Primary Applicant and Dependent(s) Child(ren) Only 2. Select what coverage applicant(s) is/are applying for:
ZURICH AMERICAN INSURANCE COMPANY BLANKET ACCIDENT INSURANCE POLICY PROOF OF COVERED LOSS FORM Mail claims to: INSTRUCTIONS
 ZURICH AMERICAN INSURANCE COMPANY BLANKET ACCIDENT INSURANCE POLICY PROOF OF COVERED LOSS FORM Mail claims to: Administrative Concepts, Inc. 994 Old Eagle School Road Suite 1005 Wayne, PA 19087-1802 www.visit-aci.com
ZURICH AMERICAN INSURANCE COMPANY BLANKET ACCIDENT INSURANCE POLICY PROOF OF COVERED LOSS FORM Mail claims to: Administrative Concepts, Inc. 994 Old Eagle School Road Suite 1005 Wayne, PA 19087-1802 www.visit-aci.com
NATIONWIDE LIFE INSURANCE COMPANY NATIONAL CASUALTY COMPANY CLAIM FORM CLAIM FILING INSTRUCTIONS NOTE TO ORGANIZATIONS AND PATIENT
 NATIONWIDE LIFE INSURANCE COMPANY NATIONAL CASUALTY COMPANY CLAIM FORM THIS CLAIM CANNOT BE PROCESSED WITHOUT ALL OF THE BELOW INFORMATION AND STATEMENTS OF PAYMENTS FROM THE OTHER PLANS. CLAIM FILING
NATIONWIDE LIFE INSURANCE COMPANY NATIONAL CASUALTY COMPANY CLAIM FORM THIS CLAIM CANNOT BE PROCESSED WITHOUT ALL OF THE BELOW INFORMATION AND STATEMENTS OF PAYMENTS FROM THE OTHER PLANS. CLAIM FILING
Insurance Claim Filing Instructions
 Insurance Claim Filing Instructions PROOF OF LOSS CONSISTS OF THE FOLLOWING: 1. A completed and signed Claim form and Attending Physician s Statement. 2. For Hospital/Intensive Care/Hospital Services Coverage
Insurance Claim Filing Instructions PROOF OF LOSS CONSISTS OF THE FOLLOWING: 1. A completed and signed Claim form and Attending Physician s Statement. 2. For Hospital/Intensive Care/Hospital Services Coverage
Sun Life Assurance Company of Canada
 Long Term Disability Claim Packet - Claimant Instructions for the Claimant Please mail all documents 4-6 weeks before the end of your elimination period. Please make sure to initiate the Long Term Disability
Long Term Disability Claim Packet - Claimant Instructions for the Claimant Please mail all documents 4-6 weeks before the end of your elimination period. Please make sure to initiate the Long Term Disability
INTEGRATED DISABILITY CLAIM APPLICATION FOR FILING A SHORT TERM OR LONG TERM DISABILITY CLAIM
 BOSTON MUTUAL LIFE INSURANCE COMPANY 120 Royall Street Canton, Massachusetts 02021 INTEGRATED DISABILITY CLAIM APPLICATION FOR FILING A SHORT TERM OR LONG TERM DISABILITY CLAIM Where to send Claim forms:
BOSTON MUTUAL LIFE INSURANCE COMPANY 120 Royall Street Canton, Massachusetts 02021 INTEGRATED DISABILITY CLAIM APPLICATION FOR FILING A SHORT TERM OR LONG TERM DISABILITY CLAIM Where to send Claim forms:
Application for Group Coverage
 Application for Group Coverage Instructions: Thank you for applying for coverage from Independence Blue Cross (IBC). Follow the instructions below to complete your application. 1. Carefully review and
Application for Group Coverage Instructions: Thank you for applying for coverage from Independence Blue Cross (IBC). Follow the instructions below to complete your application. 1. Carefully review and
Insured Home Telephone Number Policy Number(s) ( ) Address Social Security Number Date of Birth
 ( ) Address Social Security Number Date of Birth") For use with policies issued by the following Unum Group ( Unum ) subsidiaries: Unum Life Insurance Company of America Provident Life and Accident Insurance Company The Paul Revere Life Insurance Company
For use with policies issued by the following Unum Group ( Unum ) subsidiaries: Unum Life Insurance Company of America Provident Life and Accident Insurance Company The Paul Revere Life Insurance Company
**MEDICAL PROVIDER** APPROVAL and BILL SUBMISSION PROCEDURE:
 Notice to USA Rugby: This form should be presented in conjunction with your primary insurance card to the medical provider prior to any medical treatment. **MEDICAL PROVIDER** APPROVAL and BILL SUBMISSION
Notice to USA Rugby: This form should be presented in conjunction with your primary insurance card to the medical provider prior to any medical treatment. **MEDICAL PROVIDER** APPROVAL and BILL SUBMISSION
VISION CLAIM FORM. Disease/Disorder of the Eye Impairment due to Accident Hospitalization Deceased -- Date Deceased: / /
 FILING CLAIM FOR (check all that apply): VISION CLAIM FORM Disease/Disorder of the Eye Impairment due to Accident Hospitalization Deceased -- Date Deceased: / / Vision Accident Short-Term Disability /
FILING CLAIM FOR (check all that apply): VISION CLAIM FORM Disease/Disorder of the Eye Impairment due to Accident Hospitalization Deceased -- Date Deceased: / / Vision Accident Short-Term Disability /
Claim Form and Instructions
 What can I do to avoid delays? Missing information will delay the processing of your claim. Please be sure you: Sign and return the attached Authorization and the Certification on page 3. Complete the
What can I do to avoid delays? Missing information will delay the processing of your claim. Please be sure you: Sign and return the attached Authorization and the Certification on page 3. Complete the
III. CLAIMS ADMINISTRATION
 III. CLAIMS ADMINISTRATION Insurance Providers: Sport Accident Insurance: National Union Fire Insurance Company of PA Liability Insurance: AXIS Insurance Company Claims Administration: Claims Representative
III. CLAIMS ADMINISTRATION Insurance Providers: Sport Accident Insurance: National Union Fire Insurance Company of PA Liability Insurance: AXIS Insurance Company Claims Administration: Claims Representative
SAMPLE. Mail all pages of your completed form to: TIAA-CREF, P.O. Box 1268, Charlotte, NC (Sorry, we can t accept faxed forms.
 For account information, or to check the status of your request or any questions: Call 800 842-2252 Monday Friday 8 a.m. 10 p.m. (ET) Saturday 9 a.m. 6 p.m. (ET) Or visit us online at tiaa-cref.org 24
For account information, or to check the status of your request or any questions: Call 800 842-2252 Monday Friday 8 a.m. 10 p.m. (ET) Saturday 9 a.m. 6 p.m. (ET) Or visit us online at tiaa-cref.org 24
Trip Delay. 3. Please upload the completed and signed claim form and all required documents to myclaimsagent.com or mail to:
 Trip Delay HOW TO FILE A CLAIM 1. Complete all items on the attached claim form. 2. Attach the following documents (as applicable): Confirmation of the non-refundable amounts for the unused Common Carrier
Trip Delay HOW TO FILE A CLAIM 1. Complete all items on the attached claim form. 2. Attach the following documents (as applicable): Confirmation of the non-refundable amounts for the unused Common Carrier
CHUBB WORKPLACE BENEFITS A BUSINESS UNIT OF COMBINED INSURANCE COMPANY OF AMERICA, A CHUBB COMPANY INSTRUCTIONS FOR FILING CLAIMS
 CHUBB WORKPLACE BENEFITS A BUSINESS UNIT OF COMBINED INSURANCE COMPANY OF AMERICA, A CHUBB COMPANY INSTRUCTIONS FOR FILING CLAIMS GETTING STARTED Follow the Claimant Instructions below to complete the
CHUBB WORKPLACE BENEFITS A BUSINESS UNIT OF COMBINED INSURANCE COMPANY OF AMERICA, A CHUBB COMPANY INSTRUCTIONS FOR FILING CLAIMS GETTING STARTED Follow the Claimant Instructions below to complete the
Legal Name of Employer (include d/b/a) Business Address: (Street) (City) (State) (Zip Code)
 Business Address: (Street) (City) (State) (Zip Code)") COMPANION LIFE INSURANCE COMPANY P.O. BOX 100102 COLUMBIA, SC 29202-3102 Group Supplemental Medical Expense Insurance Employer Application EMPLOYER INFORMATION (Please type/print in ink) Legal Name of
COMPANION LIFE INSURANCE COMPANY P.O. BOX 100102 COLUMBIA, SC 29202-3102 Group Supplemental Medical Expense Insurance Employer Application EMPLOYER INFORMATION (Please type/print in ink) Legal Name of
All proofs of loss must be received in our office within 15 months from date incurred.
 Cancer, Specified Disease and Intensive Care Coverage Underwritten by: MetLife Insurance Company Administered by: Bay Bridge Administrators LLC Claim Filing Instructions How to file your first claim: 1.
Cancer, Specified Disease and Intensive Care Coverage Underwritten by: MetLife Insurance Company Administered by: Bay Bridge Administrators LLC Claim Filing Instructions How to file your first claim: 1.
SICKNESS CLAIM FORM. Failure to complete this form in its entirety may result in a delay in processing this claim. Hospital Indemnity Policy Number
 SICKNESS CLAIM FORM FILING CLAIM FOR (check all that apply): Sickness Pregnancy Hospitalization Deceased - Date Deceased: / / Cancer Failure to complete this form in its entirety may result in a delay
SICKNESS CLAIM FORM FILING CLAIM FOR (check all that apply): Sickness Pregnancy Hospitalization Deceased - Date Deceased: / / Cancer Failure to complete this form in its entirety may result in a delay
What to Expect Whe n Yo u Ha v e A Cl a i m
 10. Can I fax my claim form? Yes, we can accept faxes at 508-853-2867; we also ask that the original be sent via mail. Our fax number appears in the upper left-hand corner of our Claim Forms for your convenience.
10. Can I fax my claim form? Yes, we can accept faxes at 508-853-2867; we also ask that the original be sent via mail. Our fax number appears in the upper left-hand corner of our Claim Forms for your convenience.
Continue your Aetna life insurance coverage with these options.
 Aetna Life Insurance Company PO Box 14418 Des Moines, IA 50306-3418 Phone: 1-800-882-8395 Fax: 1-515-330-3296 Continue your Aetna life insurance coverage with these options. Thank you for your interest
Aetna Life Insurance Company PO Box 14418 Des Moines, IA 50306-3418 Phone: 1-800-882-8395 Fax: 1-515-330-3296 Continue your Aetna life insurance coverage with these options. Thank you for your interest
GROUP CATASTROPHE MAJOR MEDICAL PLAN
 GROUP CATASTROPHE MAJOR MEDICAL PLAN Sponsored by NYSUT Member Benefits Catastrophe Major Medical (CMM) Insurance Trust PLEASE NOTE USE THIS CLAIM FORM FOR BENEFIT PERIOD START DATES PRIOR TO JANUARY 1,
GROUP CATASTROPHE MAJOR MEDICAL PLAN Sponsored by NYSUT Member Benefits Catastrophe Major Medical (CMM) Insurance Trust PLEASE NOTE USE THIS CLAIM FORM FOR BENEFIT PERIOD START DATES PRIOR TO JANUARY 1,
ULI205 Page 1 of 6. Date: Signature: Print Name:
 Administrator s Office PO BOX 25326 Overland Park, Kansas 66225-5326 1-800-237-4463 Unified Life Insurance Company ACCIDENT/SICKNESS DISABILITY CLAIM FORM INSURED S PORTION Insured Name: Address: Date
Administrator s Office PO BOX 25326 Overland Park, Kansas 66225-5326 1-800-237-4463 Unified Life Insurance Company ACCIDENT/SICKNESS DISABILITY CLAIM FORM INSURED S PORTION Insured Name: Address: Date
Supplemental Insurance Claim Form Packet
 Supplemental Insurance Claim Form Packet The Chesapeake Life Insurance Company strives to provide easy and accurate claim filing information to our Insured. This packet contains all the required forms
Supplemental Insurance Claim Form Packet The Chesapeake Life Insurance Company strives to provide easy and accurate claim filing information to our Insured. This packet contains all the required forms
Y O U R E N R O L L M E N T K I T GROUP INSURANCE. Optional Term Life Optional Dependent Term Life
 Y O U R E N R O L L M E N T K I T GROUP INSURANCE Optional Term Life Optional Dependent Term Life Issued by The Prudential Insurance Company of America Diocese of Palm Beach Help Protect the Most Important
Y O U R E N R O L L M E N T K I T GROUP INSURANCE Optional Term Life Optional Dependent Term Life Issued by The Prudential Insurance Company of America Diocese of Palm Beach Help Protect the Most Important
INDIVIDUAL DISABILITY NOTICE OF CLAIM
 INDIVIDUAL DISABILITY NOTICE OF CLAIM Please check the box next to your insurance company s name. Central United Life Investors Consolidated Sun America Loyal Gold Cross UniLife Unum American States Page
INDIVIDUAL DISABILITY NOTICE OF CLAIM Please check the box next to your insurance company s name. Central United Life Investors Consolidated Sun America Loyal Gold Cross UniLife Unum American States Page
BUSINESS AUTO APPLICATION
 DIRECTIONS: 1. Fill in the application by filling in the blue fields on all pages. 1. 2. Please Complete fill in the all application enrollment the fields with form (all the pages) (all correct pages)
DIRECTIONS: 1. Fill in the application by filling in the blue fields on all pages. 1. 2. Please Complete fill in the all application enrollment the fields with form (all the pages) (all correct pages)
OUTPATIENT PHYSICIAN S TREATMENT CLAIM FORM
 OUTPATIENT PHYSICIAN S TREATMENT CLAIM FORM If you have any questions regarding benefits available, or how to file your claim, or if you would like to appeal any determination, please contact our Customer
OUTPATIENT PHYSICIAN S TREATMENT CLAIM FORM If you have any questions regarding benefits available, or how to file your claim, or if you would like to appeal any determination, please contact our Customer
Group life portability Employee kit. Life insurance. options. Solutions for employees making a career transition
 Group life portability Employee kit Life insurance options Solutions for employees making a career transition How to take your life insurance benefits with you Did you know that you may be eligible to
Group life portability Employee kit Life insurance options Solutions for employees making a career transition How to take your life insurance benefits with you Did you know that you may be eligible to
Application for Individual Coverage
 Application for Individual Coverage Instructions: 1. This Application should be used if you wish to enroll in an Individual plan purchased directly from Independence Blue Cross. The health plans available
Application for Individual Coverage Instructions: 1. This Application should be used if you wish to enroll in an Individual plan purchased directly from Independence Blue Cross. The health plans available
New York Life Insurance Company
 The Company You Keep New York Life Insurance Company Group Membership Association Claims PO Box 30782 Tampa FL 33630-3782 (800) 792-9686 Dear Beneficiary: Please accept our condolences on your recent loss.
The Company You Keep New York Life Insurance Company Group Membership Association Claims PO Box 30782 Tampa FL 33630-3782 (800) 792-9686 Dear Beneficiary: Please accept our condolences on your recent loss.
CLAIM FORM FOR LIFE INSURANCE PROCEEDS
 Lunar Financial Group Support@LunarFinancialGroupCom Dear Beneficiary: Please accept our condolences on your recent loss. We understand this is a difficult time, and we hope that we can alleviate any concerns
Lunar Financial Group Support@LunarFinancialGroupCom Dear Beneficiary: Please accept our condolences on your recent loss. We understand this is a difficult time, and we hope that we can alleviate any concerns
2016 Application for Small Employer Coverage
 2016 Application for Small Employer Coverage Instructions: Thank you for applying for coverage from Independence Blue Cross. Follow the instructions below to complete your application. 1. Carefully review
2016 Application for Small Employer Coverage Instructions: Thank you for applying for coverage from Independence Blue Cross. Follow the instructions below to complete your application. 1. Carefully review
RETURN THIS COPY TO JOHN HANCOCK. City/Town: State: Zip:
 HIPAA Authorization ATTN: R-02-B Long-Term Care PO Box 852 Boston, MA 02117-0852 Insured Name : Phone: 800-233-1449 Fax: 617-572-7979 Claim Number: Insured Street Address: RETURN THIS COPY TO JOHN HANCOCK
HIPAA Authorization ATTN: R-02-B Long-Term Care PO Box 852 Boston, MA 02117-0852 Insured Name : Phone: 800-233-1449 Fax: 617-572-7979 Claim Number: Insured Street Address: RETURN THIS COPY TO JOHN HANCOCK
Group Long Term Disability
 Group Long Term Disability Life Insurance Company of rth America Connecticut General Life Insurance Company Cigna Life Insurance Company of New York Great-West Healthcare Administered by Cigna Group Long
Group Long Term Disability Life Insurance Company of rth America Connecticut General Life Insurance Company Cigna Life Insurance Company of New York Great-West Healthcare Administered by Cigna Group Long
ALLSTATE LIFE INSURANCE COMPANY OF NEW YORK AP4 INDIVIDUAL ACCIDENT POLICY WITH OPTIONAL RIDER CLAIM FORM
 ALLSTATE LIFE INSURANCE COMPANY OF NEW YORK AP4 INDIVIDUAL ACCIDENT POLICY WITH OPTIONAL RIDER CLAIM FORM If you have any questions regarding benefits available, or how to file your claim, or if you would
ALLSTATE LIFE INSURANCE COMPANY OF NEW YORK AP4 INDIVIDUAL ACCIDENT POLICY WITH OPTIONAL RIDER CLAIM FORM If you have any questions regarding benefits available, or how to file your claim, or if you would
THIS SPACE INTENTIONALLY LEFT BLANK
 INSTRUCTIONS: 1. Please make certain that all pertinent questions are answered and the proper supporting documents are included before forwarding claim to avoid unnecessary delay in processing the claim.
INSTRUCTIONS: 1. Please make certain that all pertinent questions are answered and the proper supporting documents are included before forwarding claim to avoid unnecessary delay in processing the claim.
NATIONWIDE LIFE INSURANCE COMPANY NATIONAL CASUALTY COMPANY CLAIM FORM INSTRUCTIONS
 NATIONWIDE LIFE INSURANCE COMPANY NATIONAL CASUALTY COMPANY CLAIM FORM INSTRUCTIONS THIS CLAIM CANNOT BE PROCESSED WITHOUT ALL OF THE BELOW INFORMATION AND STATEMENTS OF PAYMENTS FROM THE OTHER PLANS.
NATIONWIDE LIFE INSURANCE COMPANY NATIONAL CASUALTY COMPANY CLAIM FORM INSTRUCTIONS THIS CLAIM CANNOT BE PROCESSED WITHOUT ALL OF THE BELOW INFORMATION AND STATEMENTS OF PAYMENTS FROM THE OTHER PLANS.
Dental Select Enrollment Kit
 Dental Select Enrollment Kit General Info Producer: Phone: Group Name: Email: Fax: Effective: Submission Checklist document/item doc # revised Group Application APP.01.9000286 2017-06 Original proposal
Dental Select Enrollment Kit General Info Producer: Phone: Group Name: Email: Fax: Effective: Submission Checklist document/item doc # revised Group Application APP.01.9000286 2017-06 Original proposal
Cancer Lump-Sum Benefit Claim Form
 Cancer Lump-Sum Benefit Claim Form Please check your policy for the benefit eligibility or call Sterling Customer Service at 1-866-459-1755 for help. Please use blue or black ink only and print legibly
Cancer Lump-Sum Benefit Claim Form Please check your policy for the benefit eligibility or call Sterling Customer Service at 1-866-459-1755 for help. Please use blue or black ink only and print legibly
CLAIM FORM FOR LIFE INSURANCE PROCEEDS
 New York Life Insurance Company Group Membership Association Claims 1200 E. Glen Ave. Peoria Heights, IL 61616 Dear Beneficiary: Please accept our condolences on your recent loss. We understand this is
New York Life Insurance Company Group Membership Association Claims 1200 E. Glen Ave. Peoria Heights, IL 61616 Dear Beneficiary: Please accept our condolences on your recent loss. We understand this is
Sun Life Assurance Company of Canada
 Long Term Disability Claim Packet - Claimant Instructions for the Claimant Please mail all documents 4-6 weeks before the end of your elimination period. Please make sure to initiate the Long Term Disability
Long Term Disability Claim Packet - Claimant Instructions for the Claimant Please mail all documents 4-6 weeks before the end of your elimination period. Please make sure to initiate the Long Term Disability
2018 Application for Small Employer Coverage
 2018 Application for Small Employer Coverage Instructions: Thank you for applying for coverage from Independence Blue Cross. Follow the instructions below to complete your application. 1. Carefully review
2018 Application for Small Employer Coverage Instructions: Thank you for applying for coverage from Independence Blue Cross. Follow the instructions below to complete your application. 1. Carefully review
POLICYHOLDER / CERTIFICATEHOLDER
 CLAIM FORM AND INSTRUCTIONS If you have any questions regarding benefits available, or how to file your claim, or if you would like to appeal any determination, please contact our Customer Care Center
CLAIM FORM AND INSTRUCTIONS If you have any questions regarding benefits available, or how to file your claim, or if you would like to appeal any determination, please contact our Customer Care Center
Chubb Travel Protection
 Chubb Travel Protection Claim Forms Table of Contents Claim Form Page Main 1 Attending Physician Statement 9 Car Rental Collision Damage 12 Accidental Death & Dismemberment 17 Chubb Travel Protection Claim
Chubb Travel Protection Claim Forms Table of Contents Claim Form Page Main 1 Attending Physician Statement 9 Car Rental Collision Damage 12 Accidental Death & Dismemberment 17 Chubb Travel Protection Claim
Sun Life Assurance Company of Canada Group Enrollment form
 Sun Life Assurance Company of Canada Group Enrollment form Complete all sections of the Group Enrollment Form. Make sure you complete and sign the form during the enrollment period or within 31 days of
Sun Life Assurance Company of Canada Group Enrollment form Complete all sections of the Group Enrollment Form. Make sure you complete and sign the form during the enrollment period or within 31 days of
Reimburse the Church through Missionary Medical. Claims submission made easy
 Reimburse the Church through Missionary Medical Claims submission made easy This form can be used to submit a claim for medical or pharmaceutical services.* (* if Mission funds were used). If you're filing
Reimburse the Church through Missionary Medical Claims submission made easy This form can be used to submit a claim for medical or pharmaceutical services.* (* if Mission funds were used). If you're filing
Medico Dental Insurance Portfolio
 INSURANCE COMPANY Medico Dental Insurance Portfolio n Dental n D.V.H. $1,000 n D.V.H. $1,500 APPLICATION BOOKLET PRODUCER INSTRUCTIONS Please complete the following: Application for Dental or Dental, Vision
INSURANCE COMPANY Medico Dental Insurance Portfolio n Dental n D.V.H. $1,000 n D.V.H. $1,500 APPLICATION BOOKLET PRODUCER INSTRUCTIONS Please complete the following: Application for Dental or Dental, Vision
2019 Application for Small Employer Coverage
 2019 Application for Small Employer Coverage Instructions: Thank you for applying for coverage from Independence Blue Cross. Follow the instructions below to complete your application. 1. Carefully review
2019 Application for Small Employer Coverage Instructions: Thank you for applying for coverage from Independence Blue Cross. Follow the instructions below to complete your application. 1. Carefully review
GROUP SHORT-TERM DISABILITY STATEMENT OF EMPLOYEE
 GROUP SHORT-TERM DISABILITY STATEMENT OF EMPLOYEE 1. Full Name (last, first, middle initial) 2. Social Security Number 3. Phone Number (include area code) 4. Street Address & Mailing Address 5. City 6.
GROUP SHORT-TERM DISABILITY STATEMENT OF EMPLOYEE 1. Full Name (last, first, middle initial) 2. Social Security Number 3. Phone Number (include area code) 4. Street Address & Mailing Address 5. City 6.
AAU Registered Member Sports Accident Claim Procedure
 AAU Registered Member Sports Accident Claim Procedure AAU members may be eligible for medical expense benefits for treatment of covered injuries sustained while participating in AAU Licensed activities.
AAU Registered Member Sports Accident Claim Procedure AAU members may be eligible for medical expense benefits for treatment of covered injuries sustained while participating in AAU Licensed activities.
Rental Car Collision Claim Form
 Call for help: 800-461-6920 (toll free) or 317-582-2629 (worldwide) or 317-818-2809 (collect) Rental Car Collision Claim Form Helpful Tips º º If you have no other insurance, submit copies of bills that
Call for help: 800-461-6920 (toll free) or 317-582-2629 (worldwide) or 317-818-2809 (collect) Rental Car Collision Claim Form Helpful Tips º º If you have no other insurance, submit copies of bills that
Liberty Mutual Insurance Group Benefits
 Liberty Mutual Insurance Group Benefits DirectPath All Full-Time, Eligible Employees This kit contains everything you need to enroll in your group benefits from Liberty Mutual Insurance*. This kit contains
Liberty Mutual Insurance Group Benefits DirectPath All Full-Time, Eligible Employees This kit contains everything you need to enroll in your group benefits from Liberty Mutual Insurance*. This kit contains
Medico Dental Insurance Portfolio
 INSURANCE COMPANY Medico Dental Insurance Portfolio n Dental n D.V.H. $1,000 n Dental Plus n D.V.H. $1,500 APPLICATION BOOKLET PRODUCER INSTRUCTIONS Please complete the following: Application for Dental
INSURANCE COMPANY Medico Dental Insurance Portfolio n Dental n D.V.H. $1,000 n Dental Plus n D.V.H. $1,500 APPLICATION BOOKLET PRODUCER INSTRUCTIONS Please complete the following: Application for Dental
Short Term Disability Claim Application
 Claim Application To file an application for Short Term Disability benefits, please follow the instructions below to avoid unnecessary delays. Any cost for completion of this form will be at the insured
Claim Application To file an application for Short Term Disability benefits, please follow the instructions below to avoid unnecessary delays. Any cost for completion of this form will be at the insured
EDUCATORS PROFESSIONAL LIABILITY INSURANCE PLAN APPLICATION CLAIMS-MADE PROFESSIONAL LIABILITY Underwritten By: Liberty Insurance Underwriters Inc.
 EDUCATORS PROFESSIONAL LIABILITY INSURANCE PLAN APPLICATION CLAIMS-MADE PROFESSIONAL LIABILITY Underwritten By: Liberty Insurance Underwriters Inc. HOW TO APPLY: 1. Complete application below. 2. Note
EDUCATORS PROFESSIONAL LIABILITY INSURANCE PLAN APPLICATION CLAIMS-MADE PROFESSIONAL LIABILITY Underwritten By: Liberty Insurance Underwriters Inc. HOW TO APPLY: 1. Complete application below. 2. Note
Optional Life Insurance Benefits
 Optional Life Insurance Benefits for Employees of Franklin Pierce University A Worldwide Presence Our parent company s operations currently service millions of people in the United States, Canada, the
Optional Life Insurance Benefits for Employees of Franklin Pierce University A Worldwide Presence Our parent company s operations currently service millions of people in the United States, Canada, the
MEDICAL/SICKNESS CLAIM FORM
 1. PLEASE FULLY COMPLETE THIS FORM 2. ATTACH ITEMIZED BILLS 3. MAIL TO HSR E-mail: Berkley@HSRI.com HSR Plaza II 4100 Medical Parkway Carrollton, Texas 75007 Phone: (972) 512-5600 Fax: (972) 512-5820 Toll
1. PLEASE FULLY COMPLETE THIS FORM 2. ATTACH ITEMIZED BILLS 3. MAIL TO HSR E-mail: Berkley@HSRI.com HSR Plaza II 4100 Medical Parkway Carrollton, Texas 75007 Phone: (972) 512-5600 Fax: (972) 512-5820 Toll
Group Short-Term Disability Claim Form and Instructions
 Fax to: Claims 1.800.880.9325 From: Fax Number: Date: Number of pages:_ Group Short-Term Disability Claim Form and Instructions What can I do to avoid delays? Missing information is one of the major causes
Fax to: Claims 1.800.880.9325 From: Fax Number: Date: Number of pages:_ Group Short-Term Disability Claim Form and Instructions What can I do to avoid delays? Missing information is one of the major causes
Enrollment Application
 Enrollment Application Follow these easy steps to apply for a Humana Medicare Supplement insurance policy. 1 Have Your Medicare Card Ready Please print legibly and complete the entire form. You will need
Enrollment Application Follow these easy steps to apply for a Humana Medicare Supplement insurance policy. 1 Have Your Medicare Card Ready Please print legibly and complete the entire form. You will need
Transamerica Premier Life Insurance Company
 Insurance Claim Filing Instructions PROOF OF LOSS CONSISTS OF THE FOLLOWING: 1. A completed and signed Claim form and Attending Physician s Statement. 2. For Hospital/Intensive Care/Hospital Services Coverage
Insurance Claim Filing Instructions PROOF OF LOSS CONSISTS OF THE FOLLOWING: 1. A completed and signed Claim form and Attending Physician s Statement. 2. For Hospital/Intensive Care/Hospital Services Coverage
State of Florida Accelerated Benefits Claim Form
 State of Florida Account Participating Agencies and Departments Payroll Deduction Code 262 MAIL COMPLETED FORM TO: Cigna PO Box 22328 Pittsburgh, PA 15222-0328 Toll Free #: 18002382125 Fax #: 4124023506
State of Florida Account Participating Agencies and Departments Payroll Deduction Code 262 MAIL COMPLETED FORM TO: Cigna PO Box 22328 Pittsburgh, PA 15222-0328 Toll Free #: 18002382125 Fax #: 4124023506
Application for Conversion of Group Term Life & Accidental Death Insurance Aetna Life Insurance Company
 Application for Conversion of Group Term Life & Accidental Death Insurance Aetna Life Insurance Company Application and payment of the first premium must be made within the time limit shown in your certificate
Application for Conversion of Group Term Life & Accidental Death Insurance Aetna Life Insurance Company Application and payment of the first premium must be made within the time limit shown in your certificate
GROUP SHORT-TERM DISABILITY STATEMENT OF EMPLOYEE
 Lincoln Life & Annuity Company of New York GROUP SHORT-TERM DISABILITY STATEMENT OF EMPLOYEE 1. Full Name (last, first, middle initial) 2. Social Security Number 3. Phone Number (include area code) 4.
Lincoln Life & Annuity Company of New York GROUP SHORT-TERM DISABILITY STATEMENT OF EMPLOYEE 1. Full Name (last, first, middle initial) 2. Social Security Number 3. Phone Number (include area code) 4.
PROTECT YOUR LOVED ONES AND YOUR INCOME
 X HELP PROTECT YOUR LOVED ONES AND YOUR INCOME Management Consulting & Research, LLC All Full Time Employees Optional Term Life Insurance with Matching OAD&D Optional Dependent Life Insurance with Matching
X HELP PROTECT YOUR LOVED ONES AND YOUR INCOME Management Consulting & Research, LLC All Full Time Employees Optional Term Life Insurance with Matching OAD&D Optional Dependent Life Insurance with Matching
Salary Reduction Contributions Enrollment Form
 Salary Reduction Contributions Enrollment Form Employee Information Employer Name Employee Name (Last, First, Middle) Employee Street Address Department - - Social Security Number / to / (mm/dd) Plan Year
Salary Reduction Contributions Enrollment Form Employee Information Employer Name Employee Name (Last, First, Middle) Employee Street Address Department - - Social Security Number / to / (mm/dd) Plan Year
INSTRUCTIONS FOR FILING A CRITICAL ILLNESS CLAIM
 CLAIM FORM AND INSTRUCTIONS If you have any questions while completing your claim or need assistance, please call Keeler & Associates (GoToSMBO.com) at 877-282-0808. 7:00 A.M. to 4:00 P.M. Central Standard
CLAIM FORM AND INSTRUCTIONS If you have any questions while completing your claim or need assistance, please call Keeler & Associates (GoToSMBO.com) at 877-282-0808. 7:00 A.M. to 4:00 P.M. Central Standard
Accidental Death HOW TO FILE A CLAIM
 Accidental Death HOW TO FILE A CLAIM 1. Complete all items on the attached claim form. 2. Attach the following documents (as applicable): Certified copy of death certificate (Required for all claims) Certified
Accidental Death HOW TO FILE A CLAIM 1. Complete all items on the attached claim form. 2. Attach the following documents (as applicable): Certified copy of death certificate (Required for all claims) Certified
ENROLLMENT FORM - STUDENT ACCIDENT INSURANCE School Year
 ENROLLMENT FORM - STUDENT ACCIDENT INSURANCE 2018-2019 School Year ENROLLMENT INSTRUCTIONS Fill out this enrollment form completely. Make your check or money order payable to Cabot Risk Strategies LLC.
ENROLLMENT FORM - STUDENT ACCIDENT INSURANCE 2018-2019 School Year ENROLLMENT INSTRUCTIONS Fill out this enrollment form completely. Make your check or money order payable to Cabot Risk Strategies LLC.
LIFE INSURANCE DEATH CLAIM
 LIFE INSURANCE DEATH CLAIM We want to ensure you receive your benefit payment promptly, so please complete the applicable sections and be sure to enclose the documentation requested. Each named beneficiary
LIFE INSURANCE DEATH CLAIM We want to ensure you receive your benefit payment promptly, so please complete the applicable sections and be sure to enclose the documentation requested. Each named beneficiary
CLAIM FORM. DATE OF BIRTH: 3. PATIENT'S NAME & ADDRESS- IF ADDRESS IS NEW, PLEASE CHECK BOX r PHONE: ( )
") PRIMERICA LIFE INSURANCE COMPANY as Administered by Senior Health Ins. Co. of Pennsylvania Home Office: Boston, MA P.O. Box 64913 St. Paul, MN 55164 Telephone: 1-877-451-5824 CLAIM FORM The patient or
PRIMERICA LIFE INSURANCE COMPANY as Administered by Senior Health Ins. Co. of Pennsylvania Home Office: Boston, MA P.O. Box 64913 St. Paul, MN 55164 Telephone: 1-877-451-5824 CLAIM FORM The patient or
IRONSHORE INSURANCE INC. One State Street Plaza, 8 th Floor New York, NY Tel: Toll Free: (877) IRON-411
 IRON-411") IRONSHORE INSURANCE INC. One State Street Plaza, 8 th Floor New York, NY 10004 Tel: 646-826-6600 Toll Free: (877) IRON-411 CONSULTANTS PROFESSIONAL LIABILITY INSURANCE APPLICATION THE APPLICANT IS APPLYING
IRONSHORE INSURANCE INC. One State Street Plaza, 8 th Floor New York, NY 10004 Tel: 646-826-6600 Toll Free: (877) IRON-411 CONSULTANTS PROFESSIONAL LIABILITY INSURANCE APPLICATION THE APPLICANT IS APPLYING
AIG Benefit Solutions
 PLEASE ANSWER ALL QUESTIONS FULLY AS THIS WILL HELP EXPEDITE THE EVALUATION OF THIS CLAIM. POLICYHOLDER S STATEMENT Policy Number: 3803Z1 Name of Insured (Policyholder) Address (Street, City, State, Zip
PLEASE ANSWER ALL QUESTIONS FULLY AS THIS WILL HELP EXPEDITE THE EVALUATION OF THIS CLAIM. POLICYHOLDER S STATEMENT Policy Number: 3803Z1 Name of Insured (Policyholder) Address (Street, City, State, Zip
State of New Jersey Department of the Treasury DIVISION OF PENSIONS & BENEFITS P.O. Box 295, Trenton, NJ
 RD-0988-0418 State of New Jersey Department of the Treasury DIVISION OF PENSIONS & BENEFITS PO Box 295, Trenton, NJ 08625-0295 Defined Contribution Retirement Program (DCRP) PUBLIC EMPLOYEES RETIREMENT
RD-0988-0418 State of New Jersey Department of the Treasury DIVISION OF PENSIONS & BENEFITS PO Box 295, Trenton, NJ 08625-0295 Defined Contribution Retirement Program (DCRP) PUBLIC EMPLOYEES RETIREMENT