PLEASE READ THIS INFORMATION CAREFULLY. It is important.
|
|
|
- Frank Johns
- 5 years ago
- Views:
Transcription
1 PLEASE READ THIS INFORMATION CAREFULLY. It is important. PLEASE FOLLOW THESE INSTRUCTIONS TO FILE A CLAIM ALL INFORMATION MUST BE PROVIDED IN ORDER FOR CLAIM TO BE PROCESSED. PROCESSING OF YOUR CLAIM WILL BE DELAYED IF COMPLETE INFORMATION IS NOT RECEIVED NOTE: The accident policy benefits are limited and may not provide 100% coverage. Accident medical expense coverage under this policy is provided on an Excess Basis and benefits will only be paid under this plan after your own personal or group insurance has paid out its benefits. The maximum benefit for physician s outpatient treatment in connection with physical therapy and/or spinal manipulation is $1,000 per non-surgical injury for coverage purchased by the school. Completion of a claim form does not guarantee benefit payment. Each claim is reviewed according to the policy provisions. Claim Guidelines: The following claim guidelines must be followed. Answer all questions in detail (including all signatures on the front and back of the form). A claim form needs to be completed for each accident. If you have other insurance, submit your claim to your other insurer. When you receive the explanation of benefits (sample attached) notice from your primary carrier, send it to us along with the corresponding HCFA/UB04 medical bills and with the fully completed claim form. You must submit the provider s medical bills; balance due statements will not be processed. Medical bills must include the procedure & diagnosis code along with the Provider s federal identification number. These bills are: 1) HCFA-1500 (standard form used by Providers; sample attached) 2) UB-04 or UB-92 (standard form used by Hospitals sample attached) 3) ADA Dental Claim Form (All dental bills must be submitted through your primary insurance s medical and dental plans first before submitting the bills to WebTPA) It would be helpful if the following was given to all providers the injured person is seeking treatment from: 1. WebTPA contact information 2. Policy number found on the claim form This way the providers of service can work directly with the claim office and provide them with the correct billing forms (itemized bill to include procedure & diagnosis code and tax id number) needed to process a claim. If you already paid the medical bill, include a paid receipt or a copy of your cancelled check at the same time you submit the medical bill. Otherwise payment will be made to the providers of service (Hospital, Physician or Others). Send all correspondence to WebTPA, Inc., P.O. Box 2415 Grapevine, TX The claim form must be sent within 90 days of the date you first received medical care. Any bills not filed with the claim form should be sent, within 90 days of the date you received medical care, to the Company identified with claimant s name, Organization or School name and date of Accident. If you change your address, please notify WebTPA, Inc. by sending notification to WebTPA so that there is no delay in processing any claims. Please contact WebTPA, Inc. by calling if you would like to check the status of your claim or if you have any questions on how your claim was processed or the benefit paid. Common Causes For Delays In Processing Claims 1. Claim Forms Not Completed In Full or Not Submitted. 2. Balance Due, Balance Forward, or Past Due Statements Submitted for Bills. 3. Explanation of Benefits from Primary Carrier Not Provided with the Bills. KEEP COPIES OF ALL CLAIM FORMS, MEDICAL BILLS, AND CORRESPONDENCE FOR YOUR OWN RECORDS UNTIL YOUR CLAIM HAS BEEN PROCESSED.


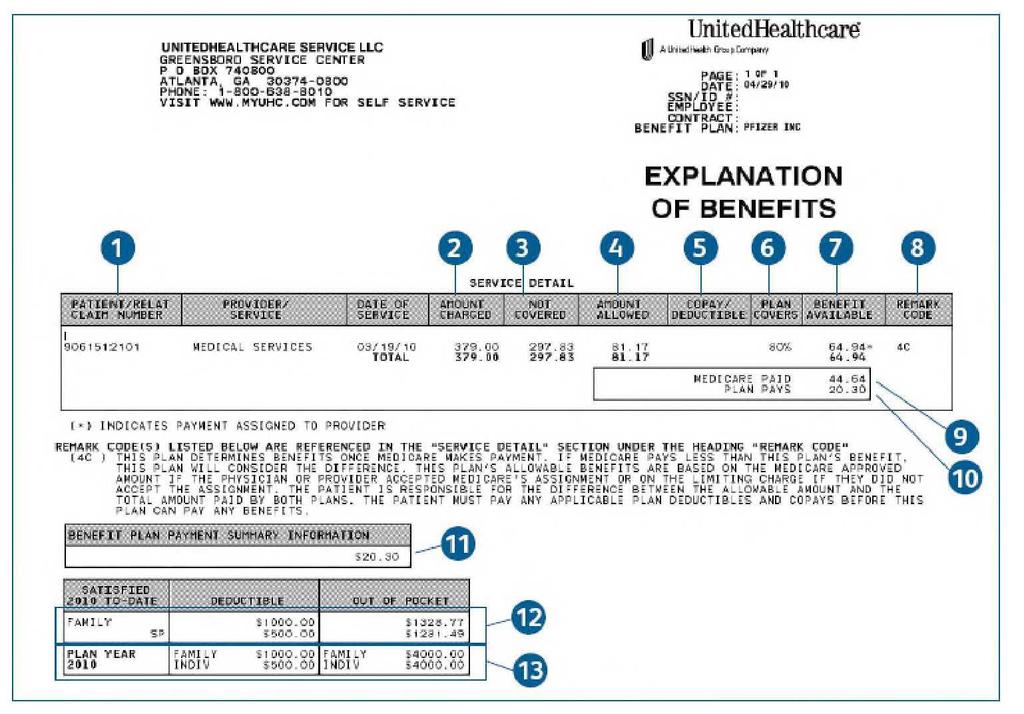
2 SAMPLE HCFA 1500 SAMPLE UB-04 SAMPLE EOB (EXPLANATION OF BENEFITS)

3 STUDENT ACCIDENT INSURANCE CLAIM FORM SIGNED CLAIM FORM IS REQUIRED 1. PLEASE FULLY COMPLETE THIS FORM PAGE 1 & PAGE 2 2. ATTACH HCFA/UB04-MEDICAL BILLS & EOBS FROM ANY OTHER INSURANCE YOU HAVE 3. SEND ALL CORRESPONDENCE TO: WEB-TPA P.O. Box 2415 Grapevine, TX Toll-Free: Fax: benefit.assist@webtpa.com IMPORTANT NOTICE: Your insurance plan is designed to provide maximum benefits for minimum premium. This plan of insurance is secondary to any health insurance you have. If you have other insurance, submit your claim (health and/or dental) to your other insurer. When you receive their Benefit Statement, send it to us along with your HCFA/UB04 (medical bills) and this completed form. Note: The accident policy benefits are limited and may not provide 100% coverage. IF PART 1-A & PART 1-B ARE NOT COMPLETED IN FULL THIS CLAIM CANNOT BE PROCESSED AND WILL BE RETURNED Organization/School District Name PART 1-A TO BE COMPLETED IN FULL BY THE ORGANIZATION/SCHOOL Policy Number District Name Phone No. ( ) Address Type of Activity/Sport If Athletics, designate P.E. Class Intramural Interscholastic Game Jr. Varsity Varsity Youth Adult Practice Other Name of injured person/student Date of Accident Accident Time Date of First Treatment Has treatment been completed? Yes No Where and how did accident occur? (Please be specific) Part of body Injured Right or Left At the time of the accident, was the claimant involved in a sponsored and supervised activity and were they a current student/member of the Organization/School District? Yes No Under whose supervision? Was he/she a witness? Yes No Authorized Signature Title Date (MUST BE SIGNED BY AN ORGANIZATION/SCHOOL OFFICIAL UNLESS INJURY DID NOT OCCUR DURING AN ORGANIZATION/SCHOOL ACTIVITY. SIGNATURE IS REQUIRED) PART 1-B TO BE COMPLETED IN FULL BY CLAIMANT OR BY PARENT/LEGAL GUARDIAN IF CLAIMANT IS A MINOR Injured Party/Student Legal Name Preferred/Nickname: Date of Birth Age Grade Level Male Female Address of Injured Person or Parents/Guardian Phone No. ( ) Address If Injured party is over age 18: Employer Name and Address Phone No. ( ) Self Employed Unemployed Father/Guardian Name Employer Name and Address Phone No. ( ) Self Employed Unemployed PLEASE CONTINUE TO THE NEXT PAGE OF THE FORM WHICH MUST BE COMPLETED IN FULL
4 Mother/Guardian Name Employer Name and Address Phone No. ( ) Self Employed Is claimant covered under any other medical and or dental insurance policy? Yes No Is claimant covered under a government sponsored insurance such as Medicare/Medicaid? Yes No Unemployed Name of all companies providing claimant insurance coverage or prepaid health plans Name of Company Address Policy # Are benefits due for this claim under these other insurance coverages? Yes No (See IMPORTANT NOTICE at top of form on page 1) Does your son or daughter have medical insurance coverage as an eligible dependent from a previous marriage as mandated in a divorce decree? Yes No If yes, please give name, address and phone number of responsible party AFFIDAVIT: I verify that the above statement on other insurance is accurate and complete. I understand that the intentional furnishing of incorrect information via the U.S. Mail may be fraudulent and violate federal laws as well as state laws. I agree that it is determined at a later date that there are other insurance benefits collectible on this claim I will reimburse Gerber Life Insurance Company to the extent for which Gerber Life Insurance Company would not have been liable. Signature: Injured Person, Parent or Guardian SIGNATURE IS REQUIRED AUTHORIZATION TO RELEASE INFORMATION: I hereby authorize any employer, health plan, insurance company, hospital, physician, health care profession, clinic, laboratory, pharmacy, medical facility or other person that has provided treatment, payment, or services in connection with this claim to disclose, when requested to do so, all information with respect to any injury, policy coverage, medical history, consultations, prescription or treatment, and copies of all hospital or medical records and itemized bills to WebTPA, Inc. and Gerber Life Insurance Company, it s agents, employees and representatives. I hereby authorize WebTPA, Inc. to discuss any information related to medical expenses incurred or treatments rendered in connection with this claim, with Special Markets Insurance Consultants, Inc. representatives and their assigned agents and to officials at the school or organization through which this policy is issued. A photo static copy of this authorization shall be considered as effective and valid as the original. Date: Signature: Injured Person, Parent or Guardian Date:
5 FRAUD NOTICE STATEMENTS NOTICE TO APPLICANTS: ANY PERSON WHO KNOWINGLY AND WITH INTENT TO DEFRAUD ANY INSURANCE COMPANY OR OTHER PERSON FILES AN APPLICATION FOR INSURANCE OR STATEMENT OF CLAIM CONTAINING ANY MATERIALLY FALSE INFORMATION, OR CONCEALS FOR THE PURPOSE OF MISLEADING, INFORMATION CONCERNING ANY FACT MATERIAL THERETO, COMMITS A FRAUDULENT INSURANCE ACT WHICH IS A CRIME AND SUBJECTS SUCH PERSON TO CRIMINAL AND CIVIL PENALTIES. RESIDENTS OF ALABAMA APPLICANTS: ANY PERSON WHO KNOWINGLY PRESENTS A FALSE OR FRAUDULENT CLAIM FOR PAYMENT OF A LOSS OR BENEFIT OR WHO KNOWINGLY PRESENTS FALSE INFORMATION IN AN APPLICATION FOR INSURANCE IS GUILTY OF A CRIME AND MAY BE SUBJECT TO RESTITUTION, FINES, OR CONFINEMENT IN PRISON, OR ANY COMBINATION THEREOF." RESIDENTS OF ALASKA APPLICANTS: A PERSON WHO KNOWINGLY AND WITH INTENT TO INJURE, DEFRAUD OR DECEIVE AN INSURANCE COMPANY FILES A CLAIM CONTAINING FALSE, INCOMPLETE OR MISLEADING INFORMATION MAY BE PROSECUTED UNDER STATE LAW. RESIDENTS OF ARKANSAS APPLICANTS: ANY PERSON WHO KNOWINGLY PRESENTS A FALSE OR FRAUDULENT CLAIM INSURANCE IS GUILTY OF A CRIME AND MAY BE SUBJECT TO FINES AND CONFINEMENT IN PRISON. RESIDENTS OF ARIZONA APPLICANTS: "FOR YOUR PROTECTION ARIZONA LAW REQUIRES THE FOLLOWING STATEMENT TO APPEAR ON THIS FORM. ANY PERSON WHO KNOWINGLY PRESENTS A FALSE OR FRAUDULENT CLAIM FOR PAYMENT OF A LOSS IS SUBJECT TO CRIMINAL AND CIVIL PENALTIES." RESIDENTS OF COLORADO APPLICANTS: IT IS UNLAWFUL TO KNOWINGLY PROVIDE FALSE, INCOMPLETE, OR MISLEADING FACTS OR INFORMATION TO AN INSURANCE COMPANY FOR THE PURPOSE OF DEFRAUDING OR ATTEMPTING TO DEFRAUD THE COMPANY. PENALTIES MAY INCLUDE IMPRISONMENT, FINES, DENIAL OF INSURANCE AND CIVIL DAMAGES. ANY INSURANCE COMPANY OR AGENT OF AN INSURANCE COMPANY WHO KNOWINGLY PROVIDES FALSE, INCOMPLETE, OR MISLEADING FACTS OR INFORMATION TO A POLICYHOLDER OR CLAIMANT FOR THE PURPOSE OF DEFRAUDING OR ATTEMPTING TO DEFRAUD THE POLICYHOLDER OR CLAIMANT WITH REGARD TO A SETTLEMENT OR AWARD PAYABLE FROM INSURANCE PROCEEDS SHALL BE REPORTED TO THE COLORADO DIVISION OF INSURANCE WITHIN THE DEPARTMENT OF REGULATORY AGENCIES. RESIDENTS OF CALIFORNIA APPLICANTS: "FOR YOUR PROTECTION CALIFORNIA LAW REQUIRES THE FOLLOWING TO APPEAR ON THIS FORM. ANY PERSON WHO KNOWINGLY PRESENTS FALSE OR FRAUDULENT CLAIM FOR THE PAYMENT OF A LOSS IS GUILTY OF A CRIME AND MAY BE SUBJECT TO FINES AND CONFINEMENT IN STATE PRISON." RESIDENTS OF DELAWARE APPLICANTS: "ANY PERSON WHO KNOWINGLY, AND WITH INTENT TO INJURE, DEFRAUD OR DECEIVE ANY INSURER, FILES A STATEMENT OF CLAIM CONTAINING ANY FALSE, INCOMPLETE OR MISLEADING INFORMATION IS GUILTY OF A FELONY." RESIDENTS OF DISTRICT OF COLUMBIA APPLICANTS: WARNING: IT IS A CRIME TO PROVIDE FALSE OR MISLEADING INFORMATION TO AN INSURER FOR THE PURPOSE OF DEFRAUDING THE INSURER OR ANY OTHER PERSON. PENALTIES INCLUDE IMPRISONMENT AND/OR FINES. IN ADDITION, AN INSURER MAY DENY INSURANCE BENEFITS IF FALSE INFORMATION MATERIALLY RELATED TO A CLAIM WAS PROVIDED BY THE APPLICANT. RESIDENTS OF FLORIDA APPLICANTS: ANY PERSON WHO, KNOWINGLY AND WITH INTENT TO INJURE, DEFRAUD, OR DECEIVE ANY INSURER FILES A STATEMENT OF CLAIM OR AN APPLICATION CONTAINING ANY FALSE, INCOMPLETE OR MISLEADING INFORMATION IS GUILTY OF A FELONY OF THE THIRD DEGREE. RESIDENTS OF IDAHO APPLICANTS: "ANY PERSON WHO KNOWINGLY, AND WITH INTENT TO DEFRAUD OR DECEIVE ANY INSURANCE COMPANY, FILES A STATEMENT OF CLAIM CONTAINING ANY FALSE, INCOMPLETE, OR MISLEADING INFORMATION IS GUILTY OF A FELONY." RESIDENTS OF INDIANA APPLICANTS: "A PERSON WHO KNOWINGLY AND WITH INTENT TO DEFRAUD AN INSURER FILES A STATEMENT OF CLAIM CONTAINING ANY FALSE, INCOMPLETE, OR MISLEADING INFORMATION COMMITS A FELONY." RESIDENTS OF KENTUCKY APPLICANTS: ANY PERSON WHO KNOWINGLY AND WITH INTENT TO DEFRAUD ANY INSURANCE COMPANY OR OTHER PERSON FILES A STATEMENT OF CLAIM CONTAINING ANY MATERIALLY FALSE INFORMATION, OR CONCEALS FOR THE PURPOSE OF MISLEADING, INFORMATION CONCERNING ANY FACT MATERIAL THERETO, COMMITS A FRAUDULENT INSURANCE ACT WHICH IS A CRIME. RESIDENTS OF LOUISIANA APPLICANTS: ANY PERSON WHO KNOWINGLY PRESENTS A FALSE OR FRAUDULENT CLAIM INSURANCE IS GUILTY OF A CRIME AND MAY BE SUBJECT TO FINES AND CONFINEMENT IN PRISON. RESIDENTS OF MAINE APPLICANTS: IT IS A CRIME TO KNOWINGLY PROVIDE FALSE, INCOMPLETE OR MISLEADING INFORMATION TO AN INSURANCE COMPANY FOR THE PURPOSE OF DEFRAUDING THE COMPANY. PENALTIES MAY INCLUDE IMPRISONMENT, FINES OR A DENIAL OF INSURANCE BENEFITS. RESIDENTS OF MARYLAND APPLICANTS: ANY PERSON WHO KNOWINGLY AND WILLFULLY PRESENTS A FALSE OR FRAUDULENT CLAIM FOR PAYMENT OF A LOSS OR BENEFIT OR WHO KNOWINGLY AND WILLFULLY PRESENTS FALSE INFORMATION IN AN APPLICATION FOR INSURANCE IS GUILTY OF A CRIME AND MAY BE SUBJECT TO FINES AND CONFINEMENT IN PRISON. RESIDENTS OF MINNESOTA APPLICANTS: A PERSON WHO FILES A CLAIM WITH INTENT TO DEFRAUD OR HELPS COMMIT A FRAUD AGAINST AN INSURER IS GUILTY OF A CRIME. RESIDENTS OF NEVADA APPLICANTS: ANY PERSON WHO KNOWINGLY FILES A STATEMENT OF CLAIM CONTAINING ANY MISREPRESENTATION OR ANY FALSE, INCOMPLETE OR MISLEADING INFORMATION MAY BE GUILTY OF A CRIMINAL ACT PUNISHABLE UNDER STATE OR FEDERAL LAW, OR BOTH, AND MAY BE SUBJECT TO CIVIL PENALTIES.
6 RESIDENTS OF NEW HAMPSHIRE APPLICANTS: "ANY PERSON WHO, WITH A PURPOSE TO INJURE, DEFRAUD, OR DECEIVE ANY INSURANCE COMPANY, FILES A STATEMENT OF CLAIM CONTAINING ANY FALSE, INCOMPLETE, OR MISLEADING INFORMATION IS SUBJECT TO PROSECUTION AND PUNISHMENT FOR INSURANCE FRAUD, AS PROVIDED IN RSA 638:20.'' RESIDENTS OF NEW JERSEY APPLICANTS: ANY PERSON WHO KNOWINGLY FILES A STATEMENT OF CLAIM CONTAINING ANY FALSE OR MISLEADING INFORMATION IS SUBJECT TO CRIMINAL AND CIVIL PENALTIES. RESIDENTS OF NEW MEXICO APPLICANTS: ANY PERSON WHO KNOWINGLY PRESENTS A FALSE OR FRAUDULENT CLAIM INSURANCE IS GUILTY OF A CRIME AND MAY BE SUBJECT TO CIVIL FINES AND CRIMINAL PENALTIES. RESIDENTS OF NEW YORK APPLICANTS: ANY PERSON WHO KNOWINGLY AND WITH INTENT TO DEFRAUD ANY INSURANCE COMPANY OR OTHER PERSON FILES AN APPLICATION FOR INSURANCE OR STATEMENT OF CLAIM CONTAINING ANY MATERIALLY FALSE INFORMATION, OR CONCEALS FOR THE PURPOSE OF MISLEADING, INFORMATION CONCERNING ANY FACT MATERIAL THERETO, COMMITS A FRAUDULENT INSURANCE ACT, WHICH IS A CRIME AND SHALL ALSO BE SUBJECT TO A CIVIL PENALTY NOT TO EXCEED FIVE THOUSAND DOLLARS AND THE STATED VALUE OF THE CLAIM FOR EACH SUCH VIOLATION. RESIDENTS OF OHIO APPLICANTS: ANY PERSON WHO, WITH INTENT TO DEFRAUD OR KNOWING THAT HE IS FACILITATING A FRAUD AGAINST ANY INSURER, SUBMITS AN APPLICATION OR FILES A CLAIM CONTAINING A FALSE OR DECEPTIVE STATEMENT IS GUILTY OF INSURANCE FRAUD. RESIDENTS OF OKLAHOMA APPLICANTS: WARNING. ANY PERSON WHO KNOWINGLY AND WITH INTENT TO INJURE, DEFRAUD OR DECEIVE ANY INSURER, MAKES ANY CLAIM FOR THE PROCEEDS OF AN INSURANCE POLICY CONTAINING ANY FALSE, INCOMPLETE OR MISLEADING INFORMATION IS GUILTY OF A FELONY. RESIDENTS OF OREGON APPLICANTS: ANY PERSON WHO KNOWINGLY AND WITH INTENT TO DEFRAUD ANY INSURANCE COMPANY OR OTHER PERSON FILES AN APPLICATION FOR INSURANCE OR STATEMENT OF CLAIM CONTAINING ANY MATERIALLY FALSE INFORMATION OR CONCEALS FOR THE PURPOSE OF MISLEADING, INFORMATION CONCERNING ANY FACT MATERIAL THERETO MAY BE SUBJECT TO PROSECUTION FOR INSURANCE FRAUD. RESIDENTS OF PENNSYLVANIA APPLICANTS: ANY PERSON WHO KNOWINGLY AND WITH INTENT TO DEFRAUD ANY INSURANCE COMPANY OR OTHER PERSON FILES AN APPLICATION FOR INSURANCE OR STATEMENT OF CLAIM CONTAINING ANY MATERIALLY FALSE INFORMATION OR CONCEALS FOR THE PURPOSE OF MISLEADING INFORMATION CONCERNING ANY FACT MATERIAL THERETO COMMITS A FRAUDULENT INSURANCE ACT WHICH IS A CRIME AND SUBJECTS SUCH PERSON TO CRIMINAL AND CIVIL PENALTIES. RESIDENTS OF RHODE ISLAND APPLICANTS: "ANY PERSON WHO KNOWINGLY PRESENTS A FALSE OR FRAUDULENT CLAIM INSURANCE IS GUILTY OF A CRIME AND MAY BE SUBJECT TO FINES AND CONFINEMENT IN PRISON." RESIDENTS OF TENNESSEE APPLICANTS: IT IS A CRIME TO KNOWINGLY PROVIDE FALSE, INCOMPLETE OR MISLEADING INFORMATION TO AN INSURANCE COMPANY FOR THE PURPOSE OF DEFRAUDING THE COMPANY. PENALTIES INCLUDE IMPRISONMENT, FINES AND DENIAL OF INSURANCE BENEFITS. RESIDENTS OF TEXAS APPLICANTS: "ANY PERSON WHO KNOWINGLY PRESENTS A FALSE OR FRAUDULENT CLAIM FOR THE PAYMENT OF A LOSS IS GUILTY OF A CRIME AND MAY BE SUBJECT TO FINES AND CONFINEMENT IN STATE PRISON." RESIDENTS OF VIRGINIA APPLICANTS: IT IS A CRIME TO KNOWINGLY PROVIDE FALSE, INCOMPLETE OR MISLEADING INFORMATION TO AN INSURANCE COMPANY FOR THE PURPOSE OF DEFRAUDING THE COMPANY. PENALTIES INCLUDE IMPRISONMENT, FINES AND DENIAL OF INSURANCE BENEFITS. RESIDENTS OF WASHINGTON APPLICANTS: IT IS A CRIME TO KNOWINGLY PROVIDE FALSE, INCOMPLETE, OR MISLEADING INFORMATION TO AN INSURANCE COMPANY FOR THE PURPOSES OF DEFRAUDING THE COMPANY. PENALTIES INCLUDE IMPRISONMENT, FINES, AND DENIAL OF INSURANCE BENEFITS. RESIDENTS OF WEST VIRGINIA APPLICANTS: "ANY PERSON WHO KNOWINGLY PRESENTS A FALSE OR FRAUDULENT CLAIM INSURANCE IS GUILTY OF A CRIME AND MAY BE SUBJECT TO FINES AND CONFINEMENT IN PRISON."
STUDENT ACCIDENT REPORTING PROCEDURES INFORMATION SHEET
 Dear Parents, STUDENT ACCIDENT REPORTING PROCEDURES INFORMATION SHEET Your School Board continues to be vitally concerned about the health, safety, and welfare of all students. We encourage safety, but
Dear Parents, STUDENT ACCIDENT REPORTING PROCEDURES INFORMATION SHEET Your School Board continues to be vitally concerned about the health, safety, and welfare of all students. We encourage safety, but
Section I Organization/School and Claimant Information (required)
") P.O. Box 25936 Overland Park, KS 66215 1-800-955-1991 or 913-327-0200 Section I Organization/School and Claimant Information (required) TO BE COMPLETED BY ORGANIZATION OR AUTHORIZED OFFICIAL Policy Effective
P.O. Box 25936 Overland Park, KS 66215 1-800-955-1991 or 913-327-0200 Section I Organization/School and Claimant Information (required) TO BE COMPLETED BY ORGANIZATION OR AUTHORIZED OFFICIAL Policy Effective
MEDICAL/SICKNESS CLAIM FORM
 1. PLEASE FULLY COMPLETE THIS FORM 2. ATTACH ITEMIZED BILLS 3. MAIL TO HSR E-mail: Berkley@HSRI.com HSR Plaza II 4100 Medical Parkway Carrollton, Texas 75007 Phone: (972) 512-5600 Fax: (972) 512-5820 Toll
1. PLEASE FULLY COMPLETE THIS FORM 2. ATTACH ITEMIZED BILLS 3. MAIL TO HSR E-mail: Berkley@HSRI.com HSR Plaza II 4100 Medical Parkway Carrollton, Texas 75007 Phone: (972) 512-5600 Fax: (972) 512-5820 Toll
Accidental Death HOW TO FILE A CLAIM
 Accidental Death HOW TO FILE A CLAIM 1. Complete all items on the attached claim form. 2. Attach the following documents (as applicable): Certified copy of death certificate (Required for all claims) Certified
Accidental Death HOW TO FILE A CLAIM 1. Complete all items on the attached claim form. 2. Attach the following documents (as applicable): Certified copy of death certificate (Required for all claims) Certified
Accidental Death Claim Instructions
 Phone : 1-877-722-1959 Fax: 443-279-2901 Accidental Death Claim Instructions The Claimant/ Insured should complete and sign the Accidental Death Insurance claim form in full and return it with the documentation
Phone : 1-877-722-1959 Fax: 443-279-2901 Accidental Death Claim Instructions The Claimant/ Insured should complete and sign the Accidental Death Insurance claim form in full and return it with the documentation
ZURICH AMERICAN INSURANCE COMPANY BLANKET ACCIDENT INSURANCE POLICY PROOF OF COVERED LOSS FORM Mail claims to: INSTRUCTIONS
 ZURICH AMERICAN INSURANCE COMPANY BLANKET ACCIDENT INSURANCE POLICY PROOF OF COVERED LOSS FORM Mail claims to: Administrative Concepts, Inc. 994 Old Eagle School Road Suite 1005 Wayne, PA 19087-1802 www.visit-aci.com
ZURICH AMERICAN INSURANCE COMPANY BLANKET ACCIDENT INSURANCE POLICY PROOF OF COVERED LOSS FORM Mail claims to: Administrative Concepts, Inc. 994 Old Eagle School Road Suite 1005 Wayne, PA 19087-1802 www.visit-aci.com
Critical Illness Insurance Insured s Statement (Please print Attach separate sheet if additional space required) Insured s Name Claim#:
 Insured s Name Claim#:") Critical Illness Insurance Insured s Statement (Please print Attach separate sheet if additional space required) INSURED INFORMATION Insured s Name Claim#: Soc. Sec. No. - - Date of Birth / / (MM/DD/YY)
Critical Illness Insurance Insured s Statement (Please print Attach separate sheet if additional space required) INSURED INFORMATION Insured s Name Claim#: Soc. Sec. No. - - Date of Birth / / (MM/DD/YY)
CLAIMS FILING INSTRUCTIONS
 ACCIDENT MEDICAL EXPENSE CLAIMS FILING INSTRUCTIONS In addition to the completed claim form, you must submit the following: For plans Underwritten by: National Health Insurance Company Integon National
ACCIDENT MEDICAL EXPENSE CLAIMS FILING INSTRUCTIONS In addition to the completed claim form, you must submit the following: For plans Underwritten by: National Health Insurance Company Integon National
**MEDICAL PROVIDER** APPROVAL and BILL SUBMISSION PROCEDURE:
 Notice to USA Rugby: This form should be presented in conjunction with your primary insurance card to the medical provider prior to any medical treatment. **MEDICAL PROVIDER** APPROVAL and BILL SUBMISSION
Notice to USA Rugby: This form should be presented in conjunction with your primary insurance card to the medical provider prior to any medical treatment. **MEDICAL PROVIDER** APPROVAL and BILL SUBMISSION
AAU Registered Member Sports Accident Claim Procedure
 AAU Registered Member Sports Accident Claim Procedure AAU members may be eligible for medical expense benefits for treatment of covered injuries sustained while participating in AAU Licensed activities.
AAU Registered Member Sports Accident Claim Procedure AAU members may be eligible for medical expense benefits for treatment of covered injuries sustained while participating in AAU Licensed activities.
HOSPITAL INDEMNITY CLAIM FORM
 HOSPITAL INDEMNITY CLAIM FORM Please read the important information below: r Please be sure your policy number(s) is/are written on the claim form. r The claim form must be completed and signed by the
HOSPITAL INDEMNITY CLAIM FORM Please read the important information below: r Please be sure your policy number(s) is/are written on the claim form. r The claim form must be completed and signed by the
OUTPATIENT PHYSICIAN S TREATMENT CLAIM FORM
 OUTPATIENT PHYSICIAN S TREATMENT CLAIM FORM If you have any questions regarding benefits available, or how to file your claim, or if you would like to appeal any determination, please contact our Customer
OUTPATIENT PHYSICIAN S TREATMENT CLAIM FORM If you have any questions regarding benefits available, or how to file your claim, or if you would like to appeal any determination, please contact our Customer
Transamerica Premier Life Insurance Company
 Insurance Claim Filing Instructions PROOF OF LOSS CONSISTS OF THE FOLLOWING: 1. A completed and signed Claim form and Attending Physician s Statement. 2. For Hospital/Intensive Care/Hospital Services Coverage
Insurance Claim Filing Instructions PROOF OF LOSS CONSISTS OF THE FOLLOWING: 1. A completed and signed Claim form and Attending Physician s Statement. 2. For Hospital/Intensive Care/Hospital Services Coverage
EMPLOYER PLAN - CLAIM FOR BENEFITS EMPLOYEE STATEMENT
 ! "! # $ % & ' ( ) * * +, - -. % / 0 ' ( 1 2 3!. % 1 1 / % 0 ' ( ' 2 4 4 4 5 6 7 8 9 * 8 3 7 8! 8 9 7! * 5 9 EMPLOYER PLAN - CLAIM FOR BENEFITS EMPLOYEE STATEMENT (BENEFITS MAY BE DELAYED IF CLAIM FORM
! "! # $ % & ' ( ) * * +, - -. % / 0 ' ( 1 2 3!. % 1 1 / % 0 ' ( ' 2 4 4 4 5 6 7 8 9 * 8 3 7 8! 8 9 7! * 5 9 EMPLOYER PLAN - CLAIM FOR BENEFITS EMPLOYEE STATEMENT (BENEFITS MAY BE DELAYED IF CLAIM FORM
GROUP SHORT-TERM DISABILITY STATEMENT OF EMPLOYEE
 Lincoln Life & Annuity Company of New York GROUP SHORT-TERM DISABILITY STATEMENT OF EMPLOYEE 1. Full Name (last, first, middle initial) 2. Social Security Number 3. Phone Number (include area code) 4.
Lincoln Life & Annuity Company of New York GROUP SHORT-TERM DISABILITY STATEMENT OF EMPLOYEE 1. Full Name (last, first, middle initial) 2. Social Security Number 3. Phone Number (include area code) 4.
Trip Delay. 3. Please upload the completed and signed claim form and all required documents to myclaimsagent.com or mail to:
 Trip Delay HOW TO FILE A CLAIM 1. Complete all items on the attached claim form. 2. Attach the following documents (as applicable): Confirmation of the non-refundable amounts for the unused Common Carrier
Trip Delay HOW TO FILE A CLAIM 1. Complete all items on the attached claim form. 2. Attach the following documents (as applicable): Confirmation of the non-refundable amounts for the unused Common Carrier
ULI205 Page 1 of 6. Date: Signature: Print Name:
 Administrator s Office PO BOX 25326 Overland Park, Kansas 66225-5326 1-800-237-4463 Unified Life Insurance Company ACCIDENT/SICKNESS DISABILITY CLAIM FORM INSURED S PORTION Insured Name: Address: Date
Administrator s Office PO BOX 25326 Overland Park, Kansas 66225-5326 1-800-237-4463 Unified Life Insurance Company ACCIDENT/SICKNESS DISABILITY CLAIM FORM INSURED S PORTION Insured Name: Address: Date
POLICYHOLDER / CERTIFICATEHOLDER
 CLAIM FORM AND INSTRUCTIONS If you have any questions regarding benefits available, or how to file your claim, or if you would like to appeal any determination, please contact our Customer Care Center
CLAIM FORM AND INSTRUCTIONS If you have any questions regarding benefits available, or how to file your claim, or if you would like to appeal any determination, please contact our Customer Care Center
ID Theft Insurance HOW TO FILE A CLAIM
 ID Theft Insurance HOW TO FILE A CLAIM 1. Complete all items on the attached claim form. 2. Attach the following documents (as applicable): The completed claim form Copy of all correspondence, police reports,
ID Theft Insurance HOW TO FILE A CLAIM 1. Complete all items on the attached claim form. 2. Attach the following documents (as applicable): The completed claim form Copy of all correspondence, police reports,
INDIVIDUAL DISABILITY NOTICE OF CLAIM
 INDIVIDUAL DISABILITY NOTICE OF CLAIM Please check the box next to your insurance company s name. Central United Life Investors Consolidated Sun America Loyal Gold Cross UniLife Unum American States Page
INDIVIDUAL DISABILITY NOTICE OF CLAIM Please check the box next to your insurance company s name. Central United Life Investors Consolidated Sun America Loyal Gold Cross UniLife Unum American States Page
Insurance Claim Filing Instructions
 Insurance Claim Filing Instructions PROOF OF LOSS CONSISTS OF THE FOLLOWING: 1. A completed and signed Claim form and Attending Physician s Statement. 2. For Hospital/Intensive Care/Hospital Services Coverage
Insurance Claim Filing Instructions PROOF OF LOSS CONSISTS OF THE FOLLOWING: 1. A completed and signed Claim form and Attending Physician s Statement. 2. For Hospital/Intensive Care/Hospital Services Coverage
Employee Leasing/Temporary Employment Agency Application
 Employee Leasing/Temporary Employment Agency Application All questions must be answered in full. Application must be signed and dated by the applicant. Applicant s Name Agent Applicant Mailing Address
Employee Leasing/Temporary Employment Agency Application All questions must be answered in full. Application must be signed and dated by the applicant. Applicant s Name Agent Applicant Mailing Address
Loss/Collision Damage Waiver HOW TO FILE A CLAIM
 Loss/Collision Damage Waiver HOW TO FILE A CLAIM 1. Complete all items on the attached claim form. 2. Attach the following documents (as applicable): Copy of rental car agreement Copy of police report
Loss/Collision Damage Waiver HOW TO FILE A CLAIM 1. Complete all items on the attached claim form. 2. Attach the following documents (as applicable): Copy of rental car agreement Copy of police report
Trip Cancellation/Interruption/Delay
 Trip Cancellation/Interruption/Delay HOW TO FILE A CLAIM 1. Complete all items on the attached claim form. 2. Attach the following documents: Copy of travel itinerary Verification of trip payment Original
Trip Cancellation/Interruption/Delay HOW TO FILE A CLAIM 1. Complete all items on the attached claim form. 2. Attach the following documents: Copy of travel itinerary Verification of trip payment Original
INSTRUCTIONS FOR FILING A CRITICAL ILLNESS CLAIM
 CLAIM FORM AND INSTRUCTIONS If you have any questions while completing your claim or need assistance, please call Keeler & Associates (GoToSMBO.com) at 877-282-0808. 7:00 A.M. to 4:00 P.M. Central Standard
CLAIM FORM AND INSTRUCTIONS If you have any questions while completing your claim or need assistance, please call Keeler & Associates (GoToSMBO.com) at 877-282-0808. 7:00 A.M. to 4:00 P.M. Central Standard
NATIONWIDE LIFE INSURANCE COMPANY NATIONAL CASUALTY COMPANY CLAIM FORM INSTRUCTIONS
 NATIONWIDE LIFE INSURANCE COMPANY NATIONAL CASUALTY COMPANY CLAIM FORM INSTRUCTIONS THIS CLAIM CANNOT BE PROCESSED WITHOUT ALL OF THE BELOW INFORMATION AND STATEMENTS OF PAYMENTS FROM THE OTHER PLANS.
NATIONWIDE LIFE INSURANCE COMPANY NATIONAL CASUALTY COMPANY CLAIM FORM INSTRUCTIONS THIS CLAIM CANNOT BE PROCESSED WITHOUT ALL OF THE BELOW INFORMATION AND STATEMENTS OF PAYMENTS FROM THE OTHER PLANS.
INSTRUCTIONS FOR FILING A CLAIM LIMITED BENEFIT CANCER EXPENSE POLICY
 INSTRUCTIONS FOR FILING A CLAIM LIMITED BENEFIT CANCER EXPENSE POLICY The forms must be completed by the claimant. All questions on the forms must be answered in full. Incomplete or illegible answers may
INSTRUCTIONS FOR FILING A CLAIM LIMITED BENEFIT CANCER EXPENSE POLICY The forms must be completed by the claimant. All questions on the forms must be answered in full. Incomplete or illegible answers may
NATIONWIDE LIFE INSURANCE COMPANY NATIONAL CASUALTY COMPANY CLAIM FORM CLAIM FILING INSTRUCTIONS NOTE TO ORGANIZATIONS AND PATIENT
 NATIONWIDE LIFE INSURANCE COMPANY NATIONAL CASUALTY COMPANY CLAIM FORM THIS CLAIM CANNOT BE PROCESSED WITHOUT ALL OF THE BELOW INFORMATION AND STATEMENTS OF PAYMENTS FROM THE OTHER PLANS. CLAIM FILING
NATIONWIDE LIFE INSURANCE COMPANY NATIONAL CASUALTY COMPANY CLAIM FORM THIS CLAIM CANNOT BE PROCESSED WITHOUT ALL OF THE BELOW INFORMATION AND STATEMENTS OF PAYMENTS FROM THE OTHER PLANS. CLAIM FILING
NON-PROFIT ORGANIZATION MANAGEMENT LIABILITY RENEWAL APPLICATION
 NON-PROFIT ORGANIZATION MANAGEMENT LIABILITY RENEWAL APPLICATION NOTICE: THIS IS A CLAIMS MADE AND REPORTED POLICY THAT APPLIES ONLY TO THOSE CLAIMS FIRST MADE AGAINST THE INSURED DURING THE POLICY PERIOD
NON-PROFIT ORGANIZATION MANAGEMENT LIABILITY RENEWAL APPLICATION NOTICE: THIS IS A CLAIMS MADE AND REPORTED POLICY THAT APPLIES ONLY TO THOSE CLAIMS FIRST MADE AGAINST THE INSURED DURING THE POLICY PERIOD
Supplemental Insurance Claim Form Packet
 Supplemental Insurance Claim Form Packet The Chesapeake Life Insurance Company strives to provide easy and accurate claim filing information to our Insured. This packet contains all the required forms
Supplemental Insurance Claim Form Packet The Chesapeake Life Insurance Company strives to provide easy and accurate claim filing information to our Insured. This packet contains all the required forms
Excess Baggage Protection Baggage Delay
 CHUBB Excess Baggage Protection Baggage Delay HOW TO FILE A CLAIM 1. Complete all items on the attached claim form. 2. Attach the following documents: Copy of payment or denial from common carrier (e.g.,
CHUBB Excess Baggage Protection Baggage Delay HOW TO FILE A CLAIM 1. Complete all items on the attached claim form. 2. Attach the following documents: Copy of payment or denial from common carrier (e.g.,
Application/Change Form For Individual Dental Insurance
 U?Te Empl And its Affiliates and Subsidiaries P.O. Box 659020, Sacramento, CA 95865 Application/Change Form For Individual Dental Insurance AGENT/AGENCY INFORMATION Please print clearly and mark carefully.
U?Te Empl And its Affiliates and Subsidiaries P.O. Box 659020, Sacramento, CA 95865 Application/Change Form For Individual Dental Insurance AGENT/AGENCY INFORMATION Please print clearly and mark carefully.
GROUP CATASTROPHE MAJOR MEDICAL PLAN
 GROUP CATASTROPHE MAJOR MEDICAL PLAN Sponsored by NYSUT Member Benefits Catastrophe Major Medical (CMM) Insurance Trust PLEASE NOTE USE THIS CLAIM FORM FOR BENEFIT PERIOD START DATES PRIOR TO JANUARY 1,
GROUP CATASTROPHE MAJOR MEDICAL PLAN Sponsored by NYSUT Member Benefits Catastrophe Major Medical (CMM) Insurance Trust PLEASE NOTE USE THIS CLAIM FORM FOR BENEFIT PERIOD START DATES PRIOR TO JANUARY 1,
CHUBB WORKPLACE BENEFITS A BUSINESS UNIT OF COMBINED INSURANCE COMPANY OF AMERICA, A CHUBB COMPANY INSTRUCTIONS FOR FILING CLAIMS
 CHUBB WORKPLACE BENEFITS A BUSINESS UNIT OF COMBINED INSURANCE COMPANY OF AMERICA, A CHUBB COMPANY INSTRUCTIONS FOR FILING CLAIMS GETTING STARTED Follow the Claimant Instructions below to complete the
CHUBB WORKPLACE BENEFITS A BUSINESS UNIT OF COMBINED INSURANCE COMPANY OF AMERICA, A CHUBB COMPANY INSTRUCTIONS FOR FILING CLAIMS GETTING STARTED Follow the Claimant Instructions below to complete the
Hired and Non-Owned Liability Supplemental Application All questions must be answered in full. Application must be signed and dated by the applicant.
 Agency Name: Address: Contact Name: Phone: Fax: Email: Applicant s Name Hired and Non-Owned Liability Supplemental Application All questions must be answered in full. Application must be signed and dated
Agency Name: Address: Contact Name: Phone: Fax: Email: Applicant s Name Hired and Non-Owned Liability Supplemental Application All questions must be answered in full. Application must be signed and dated
EMPLOYER PLAN - CLAIM FOR BENEFITS EMPLOYEE STATEMENT
 EMPLOYER PLAN - CLAIM FOR BENEFITS EMPLOYEE STATEMENT (BENEFITS MAY BE DELAYED IF CLAIM FORM IS NOT FULLY COMPLETED) Please sign this page and the authorization on page two of this form to avoid delays
EMPLOYER PLAN - CLAIM FOR BENEFITS EMPLOYEE STATEMENT (BENEFITS MAY BE DELAYED IF CLAIM FORM IS NOT FULLY COMPLETED) Please sign this page and the authorization on page two of this form to avoid delays
MAPFRE INSURANCE Claim Form c/o InsureandGo USA 7300 Corporate Center Drive Suite 601 Miami, FL 33126
 MAPFRE INSURANCE Claim Form c/o InsureandGo USA 7300 Corporate Center Drive Suite 601 Miami, FL 33126 Claim No.: Emergency Medical / Dental Expense Name of Insured Home Address State City Zip Home Telephone
MAPFRE INSURANCE Claim Form c/o InsureandGo USA 7300 Corporate Center Drive Suite 601 Miami, FL 33126 Claim No.: Emergency Medical / Dental Expense Name of Insured Home Address State City Zip Home Telephone
accident plan claim form
 The Lincoln National Life Insurance Company, PO Box 2609, Omaha, NE 68103-2609 toll free (877) 815-9256 Fax (877) 668-5331 www.lincoln4benefits.com accident plan claim form How To Use this Form to File
The Lincoln National Life Insurance Company, PO Box 2609, Omaha, NE 68103-2609 toll free (877) 815-9256 Fax (877) 668-5331 www.lincoln4benefits.com accident plan claim form How To Use this Form to File
American Heritage Life Insurance Company 1776 American Heritage Life Drive Jacksonville, Florida
 CLAIM FORM If you have any questions regarding benefits available, or how to file your claim, or if you would like to appeal any determination, please contact our customer service department at 1-800-348-4489
CLAIM FORM If you have any questions regarding benefits available, or how to file your claim, or if you would like to appeal any determination, please contact our customer service department at 1-800-348-4489
MISCELLANEOUS PROFESSIONAL LIABILITY APPLICATION
 MISCELLANEOUS PROFESSIONAL LIABILITY APPLICATION CLAIMS MADE AND REPORTED FORM ALL QUESTIONS MUST BE ANSWERED IN FULL. APPLICATION MUST BE SIGNED AND DATED BY THE PRINCIPAL, OFFICER OR PARTNER Applicant
MISCELLANEOUS PROFESSIONAL LIABILITY APPLICATION CLAIMS MADE AND REPORTED FORM ALL QUESTIONS MUST BE ANSWERED IN FULL. APPLICATION MUST BE SIGNED AND DATED BY THE PRINCIPAL, OFFICER OR PARTNER Applicant
Cancer Claim Filing Instructions
 Cancer Claim Filing Instructions Page one Insured s Statement of Claim Complete policy and insured information and answer all questions. Page two Authorization Claimant or Authorized Representative must
Cancer Claim Filing Instructions Page one Insured s Statement of Claim Complete policy and insured information and answer all questions. Page two Authorization Claimant or Authorized Representative must
Accident Claim Package
 Accident Claim Package By furnishing this form, the Company does not confirm there is insurance in force and does not waive any of its rights or defenses. CLAIMANT S STATEMENT 1. Insured s Full Name 2.
Accident Claim Package By furnishing this form, the Company does not confirm there is insurance in force and does not waive any of its rights or defenses. CLAIMANT S STATEMENT 1. Insured s Full Name 2.
ACE Privacy Protection Privacy & Network Liability Insurance Program Renewal Application
 ACE Privacy Protection Privacy & Network Liability Insurance Program Renewal Application NOTICE The Policy for which you are applying is written on a claims made and reported basis. Only claims first made
ACE Privacy Protection Privacy & Network Liability Insurance Program Renewal Application NOTICE The Policy for which you are applying is written on a claims made and reported basis. Only claims first made
FAQ'S REGARDING WAIVER OF GROUP LIFE INSURANCE PREMIUM SUBMITTING AN APPLICATION FOR WAIVER OF GROUP LIFE INSURANCE PREMIUM
 Guardian Life Insurance Company P.O. Box 14334 Lexington, KY 40512 Phone: 1-800-525-4542 Fax: 610-807-8266 FAQ'S REGARDING WAIVER OF GROUP LIFE INSURANCE PREMIUM What is Waiver of Premium? Waiver of premium
Guardian Life Insurance Company P.O. Box 14334 Lexington, KY 40512 Phone: 1-800-525-4542 Fax: 610-807-8266 FAQ'S REGARDING WAIVER OF GROUP LIFE INSURANCE PREMIUM What is Waiver of Premium? Waiver of premium
To avoid delays in processing of your claim form, complete each section attaching documentation below when it applies.
 CONTINENTAL AMERICAN INSURANCE COMPANY Post Office Box 84075 * Columbus, GA. 31993 Phone (800) 433-3036 * Fax (866) 849-2970 HOSPITAL INDEMNITY CLAIM FORM INSTRUCTIONS To avoid delays in processing of
CONTINENTAL AMERICAN INSURANCE COMPANY Post Office Box 84075 * Columbus, GA. 31993 Phone (800) 433-3036 * Fax (866) 849-2970 HOSPITAL INDEMNITY CLAIM FORM INSTRUCTIONS To avoid delays in processing of
REQUEST FOR GROUP LIFE INSURANCE BENEFITS
 REQUEST FOR GROUP LIFE INSURANCE BENEFITS (PROOF OF DEATH FOR GROUP INSURANCE) INSTRUCTIONS: 1. Claimant, please fill in and sign SECTION 1 below. 2. Please include a finalized Certified Death Certificate.
REQUEST FOR GROUP LIFE INSURANCE BENEFITS (PROOF OF DEATH FOR GROUP INSURANCE) INSTRUCTIONS: 1. Claimant, please fill in and sign SECTION 1 below. 2. Please include a finalized Certified Death Certificate.
PRIVATE COMPANY SUPPLEMENTAL CLAIM FORM
 PRIVATE COMPANY SUPPLEMENTAL CLAIM FORM Name of Insurance Company to which application is made INSTRUCTIONS: This form is to be completed by an Applicant who has been involved in any claim or suit during
PRIVATE COMPANY SUPPLEMENTAL CLAIM FORM Name of Insurance Company to which application is made INSTRUCTIONS: This form is to be completed by an Applicant who has been involved in any claim or suit during
For faster claim payment* please submit your claim online at
 Claims Made Easy For faster claim payment* please submit your claim online at www.combinedinsurance.com/claims FILING A CLAIM BY MAIL 1. Download the claim form 2. Print all six pages of the claim form
Claims Made Easy For faster claim payment* please submit your claim online at www.combinedinsurance.com/claims FILING A CLAIM BY MAIL 1. Download the claim form 2. Print all six pages of the claim form
LIFE INSURANCE DEATH CLAIM
 LIFE INSURANCE DEATH CLAIM We want to ensure you receive your benefit payment promptly, so please complete the applicable sections and be sure to enclose the documentation requested. Each named beneficiary
LIFE INSURANCE DEATH CLAIM We want to ensure you receive your benefit payment promptly, so please complete the applicable sections and be sure to enclose the documentation requested. Each named beneficiary
LIFE CLAIM KIT FOR PROCESSING LIFE INSURANCE AND ACCIDENTAL DEATH BENEFITS
 LIFE CLAIM KIT FOR PROCESSING LIFE INSURANCE AND ACCIDENTAL DEATH BENEFITS INSTRUCTIONS FOR FILING A LIFE CLAIM On behalf of Boston Mutual Life Insurance Company, please accept our sincere condolences
LIFE CLAIM KIT FOR PROCESSING LIFE INSURANCE AND ACCIDENTAL DEATH BENEFITS INSTRUCTIONS FOR FILING A LIFE CLAIM On behalf of Boston Mutual Life Insurance Company, please accept our sincere condolences
Send this signed form and any accompanying documents to Seven Corners within 180 days from the date of service using any of the following methods:
 Claim Form Please submit this completed Claim form with the itemized bills and receipts. A separate Claim Form is needed for each member. Please tape small receipts on a full size sheet of paper. Failure
Claim Form Please submit this completed Claim form with the itemized bills and receipts. A separate Claim Form is needed for each member. Please tape small receipts on a full size sheet of paper. Failure
Claim Filing Instructions
 Claim Filing Instructions Trip Cancellation Claim You were unable to depart on your covered trip 2. If cancellation was the result of an illness/injury, please have the patient s physician complete the
Claim Filing Instructions Trip Cancellation Claim You were unable to depart on your covered trip 2. If cancellation was the result of an illness/injury, please have the patient s physician complete the
Claim Form and Instructions
 What can I do to avoid delays? Missing information will delay the processing of your claim. Please be sure you: Sign and return the attached Authorization and the Certification on page 3. Complete the
What can I do to avoid delays? Missing information will delay the processing of your claim. Please be sure you: Sign and return the attached Authorization and the Certification on page 3. Complete the
All proofs of loss must be received in our office within 15 months from date incurred.
 Cancer, Specified Disease and Intensive Care Coverage Underwritten by: MetLife Insurance Company Administered by: Bay Bridge Administrators LLC Claim Filing Instructions How to file your first claim: 1.
Cancer, Specified Disease and Intensive Care Coverage Underwritten by: MetLife Insurance Company Administered by: Bay Bridge Administrators LLC Claim Filing Instructions How to file your first claim: 1.
EMPLOYEE STOCK OWNERSHIP PLAN RENEWAL QUESTIONNAIRE
 EMPLOYEE STOCK OWNERSHIP PLAN RENEWAL QUESTIONNAIRE Name of Insurance Company to which application is made COMPLETION OF THIS QUESTIONNAIRE IS REQUIRED WHEN SEEKING COVERAGE FOR A STANDALONE EMPLOYEE STOCK
EMPLOYEE STOCK OWNERSHIP PLAN RENEWAL QUESTIONNAIRE Name of Insurance Company to which application is made COMPLETION OF THIS QUESTIONNAIRE IS REQUIRED WHEN SEEKING COVERAGE FOR A STANDALONE EMPLOYEE STOCK
Dismemberment Claim Form
 Dismemberment Claim Form The Lincoln National Life Insurance Company PO Box 2649, Omaha, NE 68103-2649 Toll Free (800) 423-2765 Fax (800) 462-4660 www.lincolnfinancial.com To avoid a delay or denial of
Dismemberment Claim Form The Lincoln National Life Insurance Company PO Box 2649, Omaha, NE 68103-2649 Toll Free (800) 423-2765 Fax (800) 462-4660 www.lincolnfinancial.com To avoid a delay or denial of
INSTRUCTIONS FOR FILING GROUP VOLUNTARY STD / LTD / WAIVER OF PREMIUM CLAIMS
 CLAIM FORM AND INSTRUCTIONS If you have any questions regarding our determination of your claim, or if you would like to appeal any determination, please contact our Customer Care Center at 1-800-348-4489
CLAIM FORM AND INSTRUCTIONS If you have any questions regarding our determination of your claim, or if you would like to appeal any determination, please contact our Customer Care Center at 1-800-348-4489
SENIOR SAFEGUARD DEATH CLAIM
 SENIOR SAFEGUARD DEATH CLAIM We want to ensure you receive your benefit payment promptly, so please complete the applicable sections and be sure to enclose the documentation requested. Each named beneficiary
SENIOR SAFEGUARD DEATH CLAIM We want to ensure you receive your benefit payment promptly, so please complete the applicable sections and be sure to enclose the documentation requested. Each named beneficiary
DISABILITY CLAIM FORM
 DISABILITY CLAIM FORM If you have any questions regarding benefits available, or how to file your claim, or if you would like to appeal any determination, please contact our Customer Care Center at 1-800-348-4489,
DISABILITY CLAIM FORM If you have any questions regarding benefits available, or how to file your claim, or if you would like to appeal any determination, please contact our Customer Care Center at 1-800-348-4489,
Rental Car Collision Claim Form
 Call for help: 800-461-6920 (toll free) or 317-582-2629 (worldwide) or 317-818-2809 (collect) Rental Car Collision Claim Form Helpful Tips º º If you have no other insurance, submit copies of bills that
Call for help: 800-461-6920 (toll free) or 317-582-2629 (worldwide) or 317-818-2809 (collect) Rental Car Collision Claim Form Helpful Tips º º If you have no other insurance, submit copies of bills that
Accident Claim. File Your Claim Online. Optional Service Release Agreement
 Accident Claim Colonial Life ACCIDENT FAX: 1-800-880-9325 Telephone: 1-800-325-4368 FAX this direction FAX this form: 1-800-880-9325 Or mail: P.O. Box 100195, Columbia, SC 29202 From: Number of pages:
Accident Claim Colonial Life ACCIDENT FAX: 1-800-880-9325 Telephone: 1-800-325-4368 FAX this direction FAX this form: 1-800-880-9325 Or mail: P.O. Box 100195, Columbia, SC 29202 From: Number of pages:
Thank you. Should you have any questions, please call us at (800)
") Dear Policyholder: Please complete and sign the attached claim form. Additionally, the following items are needed in order to process your Medical/Dental claim in the most efficient and expedient way possible.
Dear Policyholder: Please complete and sign the attached claim form. Additionally, the following items are needed in order to process your Medical/Dental claim in the most efficient and expedient way possible.
Reimburse the Church through Missionary Medical. Claims submission made easy
 Reimburse the Church through Missionary Medical Claims submission made easy This form can be used to submit a claim for medical or pharmaceutical services.* (* if Mission funds were used). If you're filing
Reimburse the Church through Missionary Medical Claims submission made easy This form can be used to submit a claim for medical or pharmaceutical services.* (* if Mission funds were used). If you're filing
Security Guard / Patrol Application
 Applicant s Name Security Guard / Patrol Application All questions must be answered in full. Application must be signed and dated by the applicant. Agent Applicant Mailing Address Applicant s Phone Number
Applicant s Name Security Guard / Patrol Application All questions must be answered in full. Application must be signed and dated by the applicant. Agent Applicant Mailing Address Applicant s Phone Number
Humana Insurance Company Cancer, Specified Disease and Intensive Care Coverage Claim Filing Instructions
 Humana Insurance Company Cancer, Specified Disease and Intensive Care Coverage Claim Filing Instructions How to file your first claim: 1. Complete each section of the first page of the claim form. 2. Attach
Humana Insurance Company Cancer, Specified Disease and Intensive Care Coverage Claim Filing Instructions How to file your first claim: 1. Complete each section of the first page of the claim form. 2. Attach
Group Cancer Claim Form
 Group Cancer Claim Form Send to Guardian Life Insurance, Cancer Claims, PO Box 14317, Lexington, KY 40512 Customer Service: 1-800-541-7846 Fax: (920) 749-6275 Documents can be returned electronically at
Group Cancer Claim Form Send to Guardian Life Insurance, Cancer Claims, PO Box 14317, Lexington, KY 40512 Customer Service: 1-800-541-7846 Fax: (920) 749-6275 Documents can be returned electronically at
How to Apply for Long Term Disability Conversion Insurance
 How to Apply for Long Term Disability Conversion Insurance Please follow these steps to apply for Conversion: 1. Complete the LTD Conversion Application provided in this package. Please answer each question
How to Apply for Long Term Disability Conversion Insurance Please follow these steps to apply for Conversion: 1. Complete the LTD Conversion Application provided in this package. Please answer each question
Claimant s Statement for Life Insurance Benefits
 Headquarters: 6200 S. Gilmore Road, Fairfield, OH 45014-5141 Mailing address: P.O. Box 145496, Cincinnati, OH 45250-5496 cinfin.com 513-870-2000 Claimant s Statement for Life Insurance Benefits If you
Headquarters: 6200 S. Gilmore Road, Fairfield, OH 45014-5141 Mailing address: P.O. Box 145496, Cincinnati, OH 45250-5496 cinfin.com 513-870-2000 Claimant s Statement for Life Insurance Benefits If you
Insured s Name: Policy Number: Claim Number: Caregiver s Name: (PLEASE PRINT) Tasks Performed. Location In2. Location Out2. Shift Charge.
 Tasks Performed. Location In2. Location Out2. Shift Charge.") BST Invoice for Independent Health Care Providers Mail Address: Fax Number: Phone Number: Visit Us Online: Genworth Life & Annuity Insurance Company, Genworth Life Insurance Company, Genworth Life Insurance
BST Invoice for Independent Health Care Providers Mail Address: Fax Number: Phone Number: Visit Us Online: Genworth Life & Annuity Insurance Company, Genworth Life Insurance Company, Genworth Life Insurance
GROUP SHORT-TERM DISABILITY STATEMENT OF EMPLOYEE
 GROUP SHORT-TERM DISABILITY STATEMENT OF EMPLOYEE 1. Full Name (last, first, middle initial) 2. Social Security Number 3. Phone Number (include area code) 4. Street Address & Mailing Address 5. City 6.
GROUP SHORT-TERM DISABILITY STATEMENT OF EMPLOYEE 1. Full Name (last, first, middle initial) 2. Social Security Number 3. Phone Number (include area code) 4. Street Address & Mailing Address 5. City 6.
Toll-free: Fax: Call toll-free Monday through Friday, 8 a.m. to 8 p.m. Eastern Time.
 For use with policies issued by the following Unum Group [ Unum ] subsidiaries: Unum Life Insurance Company of America Provident Life and Accident Insurance Company OUR COMMITMENT TO YOU You have our commitment
For use with policies issued by the following Unum Group [ Unum ] subsidiaries: Unum Life Insurance Company of America Provident Life and Accident Insurance Company OUR COMMITMENT TO YOU You have our commitment
IF YES TO THE ABOVE, PLEASE RESPOND TO THE FOLLOWING QUESTIONS. IF NO, PLEASE SIGN, DATE AND RETURN TO THE UNDERWRITER.
 Hartford Fire Insurance Company UNDERWRITING QUESTIONNAIRE SERVICING CONTRACTORS NAME OF INSURED: 1. Do you currently use independent contractors for servicing loans? IF YES TO THE ABOVE, PLEASE RESPOND
Hartford Fire Insurance Company UNDERWRITING QUESTIONNAIRE SERVICING CONTRACTORS NAME OF INSURED: 1. Do you currently use independent contractors for servicing loans? IF YES TO THE ABOVE, PLEASE RESPOND
ATTENTION! READ THIS FIRST!!
 ATTENTION! READ THIS FIRST!! How to File an Allstate Cancer Claim: Please call our office with any questions 877-282-0808 1. Please follow the instruction on the first page of the claim form. To continue
ATTENTION! READ THIS FIRST!! How to File an Allstate Cancer Claim: Please call our office with any questions 877-282-0808 1. Please follow the instruction on the first page of the claim form. To continue
Property/Casualty Insurance Renewal Survey
 P.O. Box 5670 Cortland, NY 13045 Phone (800) 822-3747 Fax: (607) 756-5051 Email: applications@ mcneilandcompany.com GENERAL INFORMATION Date of survey: Renewal Date: Date proposal needed: Legal Name of
P.O. Box 5670 Cortland, NY 13045 Phone (800) 822-3747 Fax: (607) 756-5051 Email: applications@ mcneilandcompany.com GENERAL INFORMATION Date of survey: Renewal Date: Date proposal needed: Legal Name of
Insured Home Telephone Number Policy Number(s) ( ) Address Social Security Number Date of Birth
 ( ) Address Social Security Number Date of Birth") For use with policies issued by the following Unum Group ( Unum ) subsidiaries: Unum Life Insurance Company of America Provident Life and Accident Insurance Company The Paul Revere Life Insurance Company
For use with policies issued by the following Unum Group ( Unum ) subsidiaries: Unum Life Insurance Company of America Provident Life and Accident Insurance Company The Paul Revere Life Insurance Company
DISABILITY CLAIM FORM
 DISABILITY CLAIM FORM If you have any questions regarding benefits available, or how to file your claim, or if you would like to appeal any determination, please contact our Customer Care Center at 1-800-348-4489,
DISABILITY CLAIM FORM If you have any questions regarding benefits available, or how to file your claim, or if you would like to appeal any determination, please contact our Customer Care Center at 1-800-348-4489,
Accident Medical Claim Form
 137 Main Street Dubuque, IA Accident Medical Claim Form Please read and follow these instructions should there be a need to file a claim for a covered accident. Your policy says you must notify us of your
137 Main Street Dubuque, IA Accident Medical Claim Form Please read and follow these instructions should there be a need to file a claim for a covered accident. Your policy says you must notify us of your
EVENT PARTY OR WEDDING PLANNER SUPPLEMENTAL APPLICATION
 EVENT PARTY OR WEDDING PLANNER SUPPLEMENTAL APPLICATION Applicant s Name TO BE USED WITH COMMERCIAL GENERAL LIABILITY APPLICATION (ACORD 125) All questions must be answered in full. Application must be
EVENT PARTY OR WEDDING PLANNER SUPPLEMENTAL APPLICATION Applicant s Name TO BE USED WITH COMMERCIAL GENERAL LIABILITY APPLICATION (ACORD 125) All questions must be answered in full. Application must be
CANCER CLAIM FORM INSTRUCTIONS. To avoid delays in processing of your claim form, complete each section attaching documentation below when it applies.
 Post Office Box 84075 * Columbus, GA. 31993 Phone (800) 433-3036 * Fax (866) 849-2970 groupclaimfiling@aflac.com CANCER CLAIM FORM INSTRUCTIONS To avoid delays in processing of your claim form, complete
Post Office Box 84075 * Columbus, GA. 31993 Phone (800) 433-3036 * Fax (866) 849-2970 groupclaimfiling@aflac.com CANCER CLAIM FORM INSTRUCTIONS To avoid delays in processing of your claim form, complete
Present Crime Insurance Program: (Include primary AND excess, if applicable) If not applicable, please check here:
 If not applicable, please check here:") , a stock insurance company, herein called the Insurer The Hartford CrimeSHIELD Advanced Policy EMPLOYEE THEFT CLIENT PREMISES (THEFT OF CLIENT S PROPERTY APPLICATION) Agency Name: Billing Method: Agency/Broker
, a stock insurance company, herein called the Insurer The Hartford CrimeSHIELD Advanced Policy EMPLOYEE THEFT CLIENT PREMISES (THEFT OF CLIENT S PROPERTY APPLICATION) Agency Name: Billing Method: Agency/Broker
Machinery, Equipment And Rigging Supplemental Application
 Machinery, Equipment And Rigging Supplemental Application TO BE USED WITH COMMERCIAL GENERAL LIABILITY APPLICATION (ACORD 125) All questions must be answered in full. Application must be signed and dated
Machinery, Equipment And Rigging Supplemental Application TO BE USED WITH COMMERCIAL GENERAL LIABILITY APPLICATION (ACORD 125) All questions must be answered in full. Application must be signed and dated
Hunting Club/Hunting Preserve Application
 > Hunting Club/Hunting Preserve Application All questions must be answered in full. Application must be signed and dated
> Hunting Club/Hunting Preserve Application All questions must be answered in full. Application must be signed and dated
Hospital Confinement/Outpatient Surgery Claim
 FAX this direction Hospital Confinement/Outpatient Surgery Claim FAX this form: 1-800-880-9325 From: Or mail: P.O. Box 100195, Columbia, SC 29202 File Your Claim Online Number of pages: u Simply log into
FAX this direction Hospital Confinement/Outpatient Surgery Claim FAX this form: 1-800-880-9325 From: Or mail: P.O. Box 100195, Columbia, SC 29202 File Your Claim Online Number of pages: u Simply log into
Legalis Consilium EMPLOYMENT DATES
 Legalis Consilium NEW LAWYER SUPPLEMENT FOR LAWYERS PROFESSIONAL LIABILITY INSURANCE THIS APPLICATION IS FOR A CLAIMS MADE AND REPORTED INSURANCE POLICY 1. Firm: Policy Number: 2. Complete the following
Legalis Consilium NEW LAWYER SUPPLEMENT FOR LAWYERS PROFESSIONAL LIABILITY INSURANCE THIS APPLICATION IS FOR A CLAIMS MADE AND REPORTED INSURANCE POLICY 1. Firm: Policy Number: 2. Complete the following
The Accelerated Benefits Option ( ABO )
") The Accelerated Benefits Option ( ABO ) Metropolitan Life Insurance Company Group Life Claims Telephone Number: 1-800-638-6420 Please read the following important information before completing the attached
The Accelerated Benefits Option ( ABO ) Metropolitan Life Insurance Company Group Life Claims Telephone Number: 1-800-638-6420 Please read the following important information before completing the attached
LIFE CLAIM KIT FOR PROCESSING LIFE INSURANCE AND ACCIDENTAL DEATH BENEFITS
 LIFE CLAIM KIT FOR PROCESSING LIFE INSURANCE AND ACCIDENTAL DEATH BENEFITS INSTRUCTIONS FOR FILING A LIFE CLAIM On behalf of Boston Mutual Life Insurance Company, please accept our sincere condolences
LIFE CLAIM KIT FOR PROCESSING LIFE INSURANCE AND ACCIDENTAL DEATH BENEFITS INSTRUCTIONS FOR FILING A LIFE CLAIM On behalf of Boston Mutual Life Insurance Company, please accept our sincere condolences
Policy #(s) Relationship to Deceased Social Security Number/EIN
 Relationship to Deceased Social Security Number/EIN") Member Life Insurance and Annuities Companies: Annuity Investors Life Insurance Company Great American Life Insurance Company Manhattan National Life Insurance Company Administration for Life Insurance
Member Life Insurance and Annuities Companies: Annuity Investors Life Insurance Company Great American Life Insurance Company Manhattan National Life Insurance Company Administration for Life Insurance
Thank you. Should you have any questions, please call us at (800)
") Dear Policyholder: Please complete and sign the attached claim form. Additionally, the following items are needed in order to process your Trip Cancellation claim in the most efficient and expedient way
Dear Policyholder: Please complete and sign the attached claim form. Additionally, the following items are needed in order to process your Trip Cancellation claim in the most efficient and expedient way
Faster, Easier Online Claim Filing Instructions
 Extension of Disability Claim Filing Instructions To be used to extend an ongoing disability previously filed Faster, Easier Online Claim Filing Instructions Account Number: Reduce your claim processing
Extension of Disability Claim Filing Instructions To be used to extend an ongoing disability previously filed Faster, Easier Online Claim Filing Instructions Account Number: Reduce your claim processing
Cancer Lump-Sum Benefit Claim Form
 Cancer Lump-Sum Benefit Claim Form Please check your policy for the benefit eligibility or call Sterling Customer Service at 1-866-459-1755 for help. Please use blue or black ink only and print legibly
Cancer Lump-Sum Benefit Claim Form Please check your policy for the benefit eligibility or call Sterling Customer Service at 1-866-459-1755 for help. Please use blue or black ink only and print legibly
RELATIONSHIP TO THE POLICYHOLDER: HEALTH SCREENING INFORMATION
 ACCIDENT WELLNESS BENEFIT CLAIM FORM INSTRUCTIONS Please use black or blue ink only and print legibly when completing this form in its entirety. Keep a copy of the supporting documentation and this completed
ACCIDENT WELLNESS BENEFIT CLAIM FORM INSTRUCTIONS Please use black or blue ink only and print legibly when completing this form in its entirety. Keep a copy of the supporting documentation and this completed
Abuse And Molestation Liability Application
 Abuse And Molestation Liability Application THIS APPLICATION IS ON AN OCCURRENCE COVERAGE BASIS THIS APPLICATION IS ON A CLAIMS-MADE COVERAGE BASIS NOTICE: THIS APPLICATION IS FOR A COVERAGE PART WRITTEN
Abuse And Molestation Liability Application THIS APPLICATION IS ON AN OCCURRENCE COVERAGE BASIS THIS APPLICATION IS ON A CLAIMS-MADE COVERAGE BASIS NOTICE: THIS APPLICATION IS FOR A COVERAGE PART WRITTEN
THE HARTFORD CRIMESHIELD SM ADVANCED POLICY BOND SMALL BUSINESS APPLICATION FOR EMPLOYEE THEFT CLIENT PREMISES ONLY
 < >, a stock insurance company, herein called the Insurer THE HARTFORD CRIMESHIELD SM ADVANCED POLICY BOND SMALL BUSINESS APPLICATION FOR EMPLOYEE THEFT CLIENT PREMISES ONLY AGENCY NAME: HARTFORD AGENCY
< >, a stock insurance company, herein called the Insurer THE HARTFORD CRIMESHIELD SM ADVANCED POLICY BOND SMALL BUSINESS APPLICATION FOR EMPLOYEE THEFT CLIENT PREMISES ONLY AGENCY NAME: HARTFORD AGENCY
SPECIAL EVENT SUPPLEMENTAL APPLICATION
 SPECIAL EVENT SUPPLEMENTAL APPLICATION SUBMISSION REQUIREMENTS Currently valued insurance company loss runs for the current policy period plus three (3) prior years (for accounts where premium exceeds
SPECIAL EVENT SUPPLEMENTAL APPLICATION SUBMISSION REQUIREMENTS Currently valued insurance company loss runs for the current policy period plus three (3) prior years (for accounts where premium exceeds
GROUP LIFE AND/OR ACCIDENTAL DEATH CLAIM FORM
 OUR COMMITMENT For use with policies issued by the following Unum Group [ Unum ] subsidiaries: Unum Life Insurance Company of America Provident Life and Accident Insurance Company The Paul Revere Life
OUR COMMITMENT For use with policies issued by the following Unum Group [ Unum ] subsidiaries: Unum Life Insurance Company of America Provident Life and Accident Insurance Company The Paul Revere Life
Baggage Delay. Helpful Tips. Call for help: (toll free) or (worldwide) or (collect)
 or (worldwide) or (collect)") Call for help: 800-461-6920 (toll free) or 317-582-2629 (worldwide) or 317-818-2809 (collect) Baggage Delay Claim Helpful Tips º º Include documentation from your common carrier (airline, cruise line,
Call for help: 800-461-6920 (toll free) or 317-582-2629 (worldwide) or 317-818-2809 (collect) Baggage Delay Claim Helpful Tips º º Include documentation from your common carrier (airline, cruise line,
Solar or Wind Energy Facilities Application
 Solar or Wind Energy Facilities Application All questions must be answered in full. Application must be signed and dated by the applicant. APPLICANT S NAME AND MAILING ADDRESS AGENT / PRODUCER INFORMATION
Solar or Wind Energy Facilities Application All questions must be answered in full. Application must be signed and dated by the applicant. APPLICANT S NAME AND MAILING ADDRESS AGENT / PRODUCER INFORMATION
Short Term Disability Claim Form Statement Of Employee
 Short Term Disability Claim Form Statement Of Employee 1. Your Information Full Name (First) (M.I.) (Last Name) Social Security Number Date of Birth Street Address Phone Number h Male h Female City State
Short Term Disability Claim Form Statement Of Employee 1. Your Information Full Name (First) (M.I.) (Last Name) Social Security Number Date of Birth Street Address Phone Number h Male h Female City State
Life Insurance Claimant s Statement
 Life Insurance Claimant s Statement Policy Policy number(s) Information Name of Deceased Other names by which the deceased may have been known 55 No. 300 West, Suite 375 Salt Lake City, Utah 84101 (801)
Life Insurance Claimant s Statement Policy Policy number(s) Information Name of Deceased Other names by which the deceased may have been known 55 No. 300 West, Suite 375 Salt Lake City, Utah 84101 (801)
POLICY INFORMATION PATIENT INFORMATION CLAIM INFORMATION
 PO Box 83043 Lincoln, NE 68501-3043 866-863-9753 Fax: 402-479-0146 If filing a claim for Wellness Screening Benefit or RX Benefit* no form is needed, please call 866-863-9753. * When you call, it is helpful
PO Box 83043 Lincoln, NE 68501-3043 866-863-9753 Fax: 402-479-0146 If filing a claim for Wellness Screening Benefit or RX Benefit* no form is needed, please call 866-863-9753. * When you call, it is helpful