MMA Mandate: Medicare Contract Reform
|
|
|
- Dana Randall
- 5 years ago
- Views:
Transcription
1 MMA Mandate: Medicare Contract Reform Julie E. Chicoine, JD, RN, CPC The Ohio State University Medical Center
2 Medicare Program Created in 1965 Part A: Facilities, including hospitals and skilled nursing facilities Part B: Physician, laboratory and other services Part C: Medicare Advantage Part D: Prescription Drugs 2
3 Current Program Administration Part A Fiscal Intermediaries Part B Carriers Part C Medicare Advantage Part D Prescription Drug Plan 3
4 Program Scope Nearly 36 million or 86 percent of today s Medicare beneficiaries receive benefits through the fee-for for- service portion of the program Over 1 billion claims each year from over 1 million providers Report to Congress Medicare Contracting Reform: A Blueprint for a Better Medicare
5 Program Costs Consolidated Federal Funds Report released by the U.S. Census Bureau on December 27, 2005 ( More than $1 trillion of the $ 2.2 trillion in Federal spending during FY 2004 went to Medicare, Medicaid and Social Security 5
6 Medicare Prescription Drug Improvement and Modernization Act of 2003 Extensive overhaul of Medicare s administrative structure through: Elimination of all current contracts with Fiscal Intermediaries and Carriers Replacement with Medicare Administrative Contractors (MACs) 6
7 Current Contract Operations 51 Insurance Companies around the country 25 Fiscal Intermediaries 18 Carriers Multiple overlapping jurisdictions Uneven distribution of workload 7
8 Lack of Full and Open Competition Part A Competed to a limited number of contractors nominated by hospitals Part B Secretary of HHS is required by law to choose from a small pool of companies, specifically only health insurance companies 8
9 Separate Claims Process for Part A and B Claims Part A and B claims processed by separate contractors using separate operational mechanisms that do not communicate with one another Current systems have difficulty handling Medicare program changes and ensuring standardized application of program requirements No single Medicare point of contact for either beneficiaries or providers! 9
10 Specialization Restrictions CMS is limited in its ability to award separate contracts for individual claims administration activities in which certain companies may excel Operating data centers Educating providers 10
11 Absence of Performance- Based Incentives Current Contractors work under cost-based reimbursement contracts No financial incentive to improve their performance Example: July 2004 GAO report noted that only 4% of responses GAO received in 300 test calls posing four policy oriented questions to FIs and Carriers were correct and complete 11
12 Cumbersome Termination Procedures Contractors can terminate contract without cause and 180 days notice CMS may only terminate contracts after demonstrating poor performance or unresponsive contractor has failed substantially to carry out contract Contractor must be given opportunity for hearing before contract termination 12
13 Outdated Information Technology Existing claims processing system composed of three separate systems for processing claims Antiquated / outdated IT is inadequate for program s future needs Current system does not take full advantage of current technologies i.e., use of Internet to track/submit claims 13

14 Fiscal Intermediaries FY

15 Carriers FY
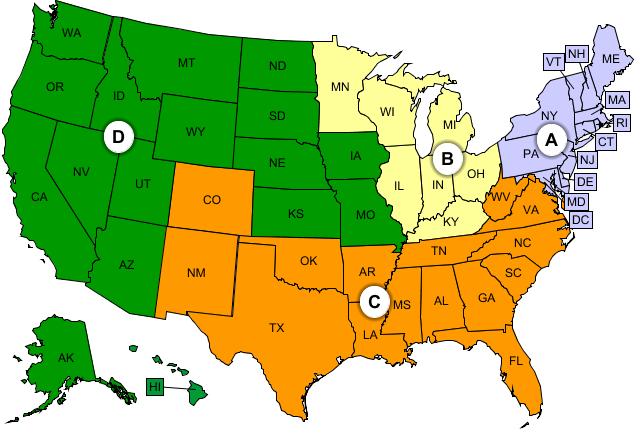
16 New Contract Model- Medicare Administrative Contractor 23 MAC contracts including: 15 Primary A/B MACs 4 Specialty MACs for home health and hospice 4 Specialty MACs for DME 16

17 Primary A/B Jurisdictions 17
18 DME MAC Contractors 18
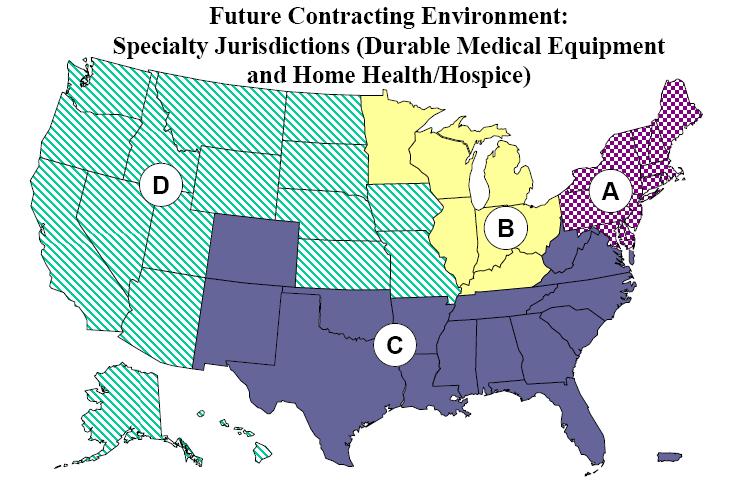
19 Home Health/Hospice 19
20 Jurisdiction Design CMS designed new MAC jurisdictions based on three criteria: Promoting competition Balanced allocation of work load Account for integration of claims processing activities 20
21 Improved Medicare Contracting New contacting organization responsible for: A/B Claims processing Beneficiary services Provider enrollment Appeals Provider education 21
22 Operational - Goals Deliver more efficient and effective services to both beneficiaries and providers, by Integrating claims processing for Parts A and B Creating modernized administrative IT platform that incorporates improved technology 22
23 Competition Full and open competition to any eligible entity Not exclusive to current Medicare contractors Non-insurance companies can compete Must comply with Federal Acquisition Regulations conflict of interest standards Must have sufficient financial assets to support contract performance functions No limit on number of contracts for which one entity can compete or be awarded 23
24 Customer-Centered Administration Contracting services for both Parts A and B consolidated to provide unified point of contact for Medicare Beneficiary and provider access through improved consolidated, standardized administrative services 24
25 Contract Performance Incentives Contracts will pay for performance incentives, allowing contractors to earn profits for efficient, innovative and cost- effective services Contracts will include specific performance requirements and standards for: Timely and accurate claims payment Education and outreach Customer satisfaction 25
26 Improved Contract Management CMS will compete contracts among a broader range of private sector organizations to allow for: Increased competition and cost efficiencies Strengthened CMS ability to managed contractors based on performance 26
27 Re-competition CMS will compete all MAC contracts within the initial cycle Re-complete all contracts at least once every five years CMS can terminate contracts for poor performance or for government s convenience No more automatic renewal 27
28 Unified Claims Management MACs will perform core claims processing for both A and B claims One Explanation of Benefits (EOB) for all health care services 28
29 Updated Information Technology Health Integrated General Ledger Accounting System Single, integrated financial accounting system to perform payment calculation, formatting and accounting of claims Web portal enables providers and beneficiaries to check claims status, beneficiary eligibility, and claims submission via secure Internet connection 29
30 Infrastructure for Comprehensive Care Current contract model with separate claims process make it difficult for Medicare to identify overall patterns of beneficiary care Under new model, Medicare data across all benefits will be collected and combined to provide comprehensive view of beneficiary s care Also enables data-mining for patterns of fraud and abuse 30
31 Data Centers Current 16 data centers play key role in Medicare FFS claims processing as part of program s IT platform CMS will consolidate number of data centers from 16 to 4, and contract directly with centers for claims processing support Distinct databases for beneficiaries, providers, claims data, and financial information 31
32 Contract Compliance Requirements Medicare Compliance Officer and committee committee Standards of conduct, policies and procedures Education and training Enforcing disciplinary policies and procedures Auditing and monitoring Responding to detected problems Developing corrective action plans Reporting to the Board 32
33 Liability Under False Claims Act MACs immune for payment errors unless they act with reckless disregard of contract obligations or with intent to defraud Liability includes Civil Monetary Penalties for conduct that constitutes violation of False Claims Act 33
34 Effect on Providers Single point of contact for all Part A and Part B claims related business MACs will assist providers with obtaining information on behalf of patients about items or services received from another provider or supplier that could affect claims payment Improved provider education and outreach Improved customer service - must answer written inquiries within 45 business days Role in contractor evaluation via surveys 34
35 Effect on Beneficiaries Single claim for Part A and Part B services Beneficiary Contact Centers - Single point of contact for program information needs, including availability of prescription drug coverage and other queries such as finding and comparing nursing homes MEDICARE for beneficiary questions 35
36 Effect on Current Program Contracts All existing FI and Carrier contractors must compete if they wish to remain a contractor CMS will not require A/B MACs to offer employment to staff of FIs and Carriers that do not successfully win a MAC contract ( outgoing contractor) 36
37 Effect on Local Coverage Decisions (LCDs) MACs will consolidate all LCDs for its jurisdiction with input from local provider communities CMS will continue to issue National Coverage Decisions from time to time 37
38 Effect on Functional Contractors CMS will maintain its relationships with functional contractors that have increased the efficiency of Medicare services including: Coordination of benefits contractor Program safeguard contractors Qualified independent contractors for Medicare appeals 38
39 Coordination of Benefits Contractor CMS established one COB contractor to consolidate pre-pay pay Medicare secondary payer activities among all FFS contractors COB responsible for identifying health benefits available to Medicare beneficiary and coordinating payment process Under reform, current COB will operate in conjunction with MACs 39
40 Program Safeguard Contractors MMA allows MACs to be awarded contracts that include some safeguard functions CMS expects PSCs to continue to perform these activities in close coordination with MACs 40
41 Qualified Independent Contractors QICs provide a second level of appeal, reviewing redeterminations of FIs and carriers CMS expects to have QICs conducting all second-level appeals, through a more independent process, with greater reliance on physician reviews, standard protocols and an improved data system 41
42 Quality Improvement Organizations QIOs make initial determinations and reconsiderations regarding certain hospital discharges and review complaints about quality of care CMS expects QIOs to continue to perform these services in close coordination with MACs 42
43 Unique Provider Identification Number Registry UPIN is a central registry, used by all contractors, that assigns numbers to all types of providers MACs will send requests to UPIN registry during enrollment process and receive number in return 43
44 National Provider Identifier CMS is currently replacing UPINs and Provider Identification Numbers with the National Provider Identifier (NPI) NPI implementation process as mandated by HIPAA will be used by MACs 44
45 Impact on Part C and Part D Programs MMA - New regional areas for Medicare Advantage preferred provider organization plans and for Prescription Drug Plans No impact on Part C or Part D MMA did not require that the MAC areas match up with Part C or Part D regions 45
46 MAC Transition Goals Minimize disruption to beneficiaries and providers Prevent disruption of claims processing Complete transition activities within the required period Ensure that costs represent effective and efficient use of resources Ensure that all relevant parties are informed of progress and status 46
47 Timeline Start up Cycle September 2005 RFP released for Jurisdiction 3 (Arizona, Montana, North Dakota, Utah and Wyoming) June 2006 CMS will award RFP for Jurisdiction 3 MAC and begin operational transition 47
48 Reform Timeline Cycle 1 September 2006 RFPs for A/B Jurisdictions 1, 2, 4, 5, 7, 12, and 13 September 2007 Award date and operational transition 48
49 Reform Timeline Cycle 2 September 2007 RFP A/B Jurisdictions 6, 8, 9, 10, 11, 14 and 15 and Home Health/Hospice MACs Award date for Jurisdictions 1, 2, 4, 5, 7, 12 and 13 September 2008 Award date for Jurisdictions 6, 8, 9, 10, 11, and 15 and Home Health/Hospice MACs 49
50 DME MAC Awarded January 2006 DME MAC Contractors NHIC AdminaStar Palmetto GBA, LLC Noridian Administrative Services 50
51 Projected Savings $900 million by Fiscal Year 2010 Beyond 2011, CMS estimates annual savings of $100 million, through administrative reductions alone 51
52 Trend Emerging Focus on Federal Health Care Program Compliance Corporate Responsibility and Corporate Compliance for Healthcare Boards of Directors. Resource Paper, OIG, (April 2, 2003) Proposed Amendments to the U.S. Sentencing Guidelines for Organizations. U.S. Sentencing Commission, (December 30, 2003) OIG Roundtable discussions with Heath Care Industry. (OIG/HCCA, July 30, 2004) Supplemental Compliance Guidance for Hospitals OIG (January 27, 2005) Draft OIG Compliance Program Guidance for Recipients of PHS Research Awards (November 28, 2005) 52
53 Civil False Claims Act 31 U.S.C This act applies to any person who knowingly presents, or causes to be presented, a false or fraudulent claim to the United States government for payment. Knowingly means, actual knowledge, reckless disregard or deliberate ignorance of the falsity of the claim. Majority of providers are prosecuted under reckless disregard standard in that they knew or should have known that their conduct departed from generally accepted billing practices. 53
54 Civil Monetary Penalties 42 U.S.C. 1320a-7a The Secretary, DHHS has authority to impose civil monetary penalties $5,000 to $10,000 fine for each health care claim submitted for payment Treble damages - three times the amount unlawfully collected from the United States government Federal Healthcare Program exclusion, Mandatory exclusion for no less than five years, or Permissive exclusion for no less then three years Civil monetary penalties will be imposed against those who contract with excluded parties 54
55 Corporate Transparency The organization must have dedicated and knowledgeable compliance professionals at the helm The organization must monitor and audit itself to prevent and detect violations of law The organization must implement ongoing risk assessment as an essential component of its compliance program Enhanced evaluation of program s auditing and monitoring systems Core principle is that health care providers must identify and address risk areas. 55
56 Enhance Compliance By: Prevention and detection - Gathering, evaluating and channeling compliance information Enhancing communications and developing strategies for MAC interactions Enhancing cooperation and communication among Part A and Part B providers and suppliers Setting priorities and focusing on Material Risk Areas 56
57 Additional Information on Medicare Contracting Reform CMS website: eform/ Continually updated with new information Open Door Forums 57
Medicare Program Integrity: Overview and Issues
 Medicare Program Integrity: Overview and Issues Marjorie Kanof, M.D. Managing Director, Health Care U.S. Government Accountability Office February 22, 2007 1 Overview Introduction to Medicare What is Program
Medicare Program Integrity: Overview and Issues Marjorie Kanof, M.D. Managing Director, Health Care U.S. Government Accountability Office February 22, 2007 1 Overview Introduction to Medicare What is Program
Medicare Program Integrity: Activities to Protect Medicare from Payment Errors, Fraud, and Abuse
 Order Code RL34217 Medicare Program Integrity: Activities to Protect Medicare from Payment Errors, Fraud, and Abuse October 24, 2007 Holly Stockdale Analyst in Medicare Domestic Social Policy Division
Order Code RL34217 Medicare Program Integrity: Activities to Protect Medicare from Payment Errors, Fraud, and Abuse October 24, 2007 Holly Stockdale Analyst in Medicare Domestic Social Policy Division
RAC Preparation Checklist
 RAC Preparation Checklist A. Select an internal RAC Team using individuals from key departments and identify individual roles (if any) in the RAC process. Communicate each individual s roles to others
RAC Preparation Checklist A. Select an internal RAC Team using individuals from key departments and identify individual roles (if any) in the RAC process. Communicate each individual s roles to others
Recovery Audit Contractors The Beginning to Now and Overview RACs Challenged by Providers? A Recent OIG Report May Be Indicating Just That 1 CEU
 Recovery Audit Contractors The Beginning to Now and Overview RACs Challenged by Providers? A Recent OIG Report May Be Indicating Just That 1 CEU Article submitted by Carl James Byron, III ATC-L, CHA CPC,
Recovery Audit Contractors The Beginning to Now and Overview RACs Challenged by Providers? A Recent OIG Report May Be Indicating Just That 1 CEU Article submitted by Carl James Byron, III ATC-L, CHA CPC,
Medicare Audit and Appeals: Practical Advice on Preparing for and Responding to RAC, ZPIC, and MAC Audits. February Overview
 Medicare Audit and Appeals: Practical Advice on Preparing for and Responding to RAC, ZPIC, and MAC Audits February 2012 B. Scott McBride Baker & Hostetler LLP smcbride@bakerlaw.com Anna M. Grizzle Bass,
Medicare Audit and Appeals: Practical Advice on Preparing for and Responding to RAC, ZPIC, and MAC Audits February 2012 B. Scott McBride Baker & Hostetler LLP smcbride@bakerlaw.com Anna M. Grizzle Bass,
How to Prepare for and Respond to RAC Audits. Kathleen H. Drummy, Esq.
 How to Prepare for and Respond to RAC Audits by Kathleen H. Drummy, Esq. What is a RAC? 2 IMPROPER PAYMENT INFORMATION ACT Requires federal agencies to measure improper payment rates Focus is on where
How to Prepare for and Respond to RAC Audits by Kathleen H. Drummy, Esq. What is a RAC? 2 IMPROPER PAYMENT INFORMATION ACT Requires federal agencies to measure improper payment rates Focus is on where
Fraud and Abuse in the Medicare Program
 Fraud and Abuse in the Medicare Program 1 / March 2009 Learning Objectives Define what fraud is and identify examples of fraud. Identify proactive measures to mitigate risk to your business or organization.
Fraud and Abuse in the Medicare Program 1 / March 2009 Learning Objectives Define what fraud is and identify examples of fraud. Identify proactive measures to mitigate risk to your business or organization.
FALSE CLAIMS ACT ENFORCEMENT: RECENT TRENDS AND STEPS TO ENSURE COMPLIANCE AND AVOID FRAUD ALLEGATIONS
 FALSE CLAIMS ACT ENFORCEMENT: RECENT TRENDS AND STEPS TO ENSURE COMPLIANCE AND AVOID FRAUD ALLEGATIONS The Carolinas Center s 39 th Annual Hospice & Palliative Care Conference Columbia, SC Presenters:
FALSE CLAIMS ACT ENFORCEMENT: RECENT TRENDS AND STEPS TO ENSURE COMPLIANCE AND AVOID FRAUD ALLEGATIONS The Carolinas Center s 39 th Annual Hospice & Palliative Care Conference Columbia, SC Presenters:
Special Advisory Bulletin
 Special Advisory Bulletin The Effect of Exclusion From Participation in Federal Health Care Programs September 1999 A. Introduction The Office of Inspector General (OIG) was established in the U.S. Department
Special Advisory Bulletin The Effect of Exclusion From Participation in Federal Health Care Programs September 1999 A. Introduction The Office of Inspector General (OIG) was established in the U.S. Department
Medical Monitoring Program: PPACA and CMS Final Recommended Guidelines vs. Rules: New License Monthly Screening Requirements
 PPACA and CMS Final Recommended Guidelines vs. Rules: New License Monthly Screening Requirements The Patient Protection and Affordable Care Act of 2010, as amended by the Health Care and Education Reconciliation
PPACA and CMS Final Recommended Guidelines vs. Rules: New License Monthly Screening Requirements The Patient Protection and Affordable Care Act of 2010, as amended by the Health Care and Education Reconciliation
Federal and State False Claims Act Education Policy
 *TEAMHealth Policies and Procedures Policy Name: Federal and State False Claims Act Education Policy Effective Date: January 1, 2017 Approved By: Executive Compliance Committee Replaces Policy Dated: January
*TEAMHealth Policies and Procedures Policy Name: Federal and State False Claims Act Education Policy Effective Date: January 1, 2017 Approved By: Executive Compliance Committee Replaces Policy Dated: January
Current Payor Audit Mechanics and How to Defend Against Them. Role of Office of Inspector General in Federal Audits
 Current Payor Audit Mechanics and How to Defend Against Them Stephen Bittinger Healthcare Reimbursement Attorney NEXSEN PRUET, LLC Role of Office of Inspector General in Federal Audits Most Recent OIG
Current Payor Audit Mechanics and How to Defend Against Them Stephen Bittinger Healthcare Reimbursement Attorney NEXSEN PRUET, LLC Role of Office of Inspector General in Federal Audits Most Recent OIG
THE MEDICARE RECOVERY AUDIT CONTRACTOR (RAC) PROGRAM: An Evaluation of the 3-Year Demonstration
 PROGRAM: An Evaluation of the 3-Year Demonstration") THE MEDICARE RECOVERY AUDIT CONTRACTOR (RAC) PROGRAM: An Evaluation of the 3-Year Demonstration June 2008 THE MEDICARE RECOVERY AUDIT CONTRACTOR (RAC) PROGRAM: An Evaluation of the 3-Year Demonstration
THE MEDICARE RECOVERY AUDIT CONTRACTOR (RAC) PROGRAM: An Evaluation of the 3-Year Demonstration June 2008 THE MEDICARE RECOVERY AUDIT CONTRACTOR (RAC) PROGRAM: An Evaluation of the 3-Year Demonstration
DEFICIT REDUCTION ACT AND FALSE CLAIMS POLICY INFORMATION FOR All MASSACHUSETTS WORKFORCE MEMBERS
 DEFICIT REDUCTION ACT AND FALSE CLAIMS POLICY INFORMATION FOR All MASSACHUSETTS WORKFORCE MEMBERS The Company is committed to preventing health care fraud, waste and abuse and complying with applicable
DEFICIT REDUCTION ACT AND FALSE CLAIMS POLICY INFORMATION FOR All MASSACHUSETTS WORKFORCE MEMBERS The Company is committed to preventing health care fraud, waste and abuse and complying with applicable
Medicare Program Integrity: Activities to Protect Medicare from Payment Errors, Fraud, and Abuse
 : Activities to Protect Medicare from Payment Errors, Fraud, and Abuse Holly Stockdale Analyst in Health Care Financing March 15, 2010 Congressional Research Service CRS Report for Congress Prepared for
: Activities to Protect Medicare from Payment Errors, Fraud, and Abuse Holly Stockdale Analyst in Health Care Financing March 15, 2010 Congressional Research Service CRS Report for Congress Prepared for
Self-Disclosure: Why, When, Where and How
 American Bar Association Washington Health Law Summit Self-Disclosure: Why, When, Where and How December 8, 2015 Margaret Hutchinson U.S. Attorney s Office for the Eastern District of Pennsylvania Kaitlyn
American Bar Association Washington Health Law Summit Self-Disclosure: Why, When, Where and How December 8, 2015 Margaret Hutchinson U.S. Attorney s Office for the Eastern District of Pennsylvania Kaitlyn
This course is designed to provide Part B providers with an overview of the Medicare Fraud and Abuse program including:
 This course is designed to provide Part B providers with an overview of the Medicare Fraud and Abuse program including: Medicare Trust Fund Defining Fraud & Abuse Examples of Fraud & Abuse Fraud & Abuse
This course is designed to provide Part B providers with an overview of the Medicare Fraud and Abuse program including: Medicare Trust Fund Defining Fraud & Abuse Examples of Fraud & Abuse Fraud & Abuse
COMPLIANCE; It s Not an Option
 COMPLIANCE; It s Not an Option AAPC April 17, 2013 Rose B. Moore, CPC, CPC-I, CPC-H, CPMA, CEMC, CMCO, CCP, CEC, PCS, CMC, CMOM, CMIS, CERT, CMA-ophth President/CEO Medical Consultant Concepts, LLC Copyright
COMPLIANCE; It s Not an Option AAPC April 17, 2013 Rose B. Moore, CPC, CPC-I, CPC-H, CPMA, CEMC, CMCO, CCP, CEC, PCS, CMC, CMOM, CMIS, CERT, CMA-ophth President/CEO Medical Consultant Concepts, LLC Copyright
Third National Medicare RAC Summit
 Third National Medicare RAC Summit Zone Program Integrity Contractors (ZPICs) Cristine M. Miller, CMPE, CCP, CHC Thursday, March 4, 2010 RAC Audit Preparation Cristine Miller Certified Medical Practice
Third National Medicare RAC Summit Zone Program Integrity Contractors (ZPICs) Cristine M. Miller, CMPE, CCP, CHC Thursday, March 4, 2010 RAC Audit Preparation Cristine Miller Certified Medical Practice
Medicare Overpayment 60 Day Rule
 Medicare Overpayment 60 Day Rule What Your Compliance and Auditing Departments Need to Know Objectives Review the key legal, operational and technical takeaways from the ACA 60 Day Report and Repay Statute.
Medicare Overpayment 60 Day Rule What Your Compliance and Auditing Departments Need to Know Objectives Review the key legal, operational and technical takeaways from the ACA 60 Day Report and Repay Statute.
There is nothing wrong with change, if it is in the right direction Winston Churchil
 Changes Changes 2012 2012 There is nothing wrong with change, if it is in the right direction Winston Churchill New tools provided by the Affordable Care Act are strengthening the Obama administration
Changes Changes 2012 2012 There is nothing wrong with change, if it is in the right direction Winston Churchill New tools provided by the Affordable Care Act are strengthening the Obama administration
Charging, Coding and Billing Compliance
 GWINNETT HEALTH SYSTEM CORPORATE COMPLIANCE Charging, Coding and Billing Compliance 9510-04-10 Original Date Review Dates Revision Dates 01/2007 05/2009, 09/2012 POLICY Gwinnett Health System, Inc. (GHS),
GWINNETT HEALTH SYSTEM CORPORATE COMPLIANCE Charging, Coding and Billing Compliance 9510-04-10 Original Date Review Dates Revision Dates 01/2007 05/2009, 09/2012 POLICY Gwinnett Health System, Inc. (GHS),
C. Enrollees: A Medicaid beneficiary who is currently enrolled in the MCCMH PIHP.
 professionally recognized standards for health care. It also includes beneficiary practices that result in unnecessary cost to the Medicaid program. 42 CFR 455.2 B. CMS: Centers for Medicare & Medicaid
professionally recognized standards for health care. It also includes beneficiary practices that result in unnecessary cost to the Medicaid program. 42 CFR 455.2 B. CMS: Centers for Medicare & Medicaid
3/17/2015. HCCA Compliance Institute April 19, Legal Obligations to Disclose and Refund. Background on Government Approach to Overpayments
 HCCA Compliance Institute April 19, 2015 Exploring CMS s Proposed Rule on Reporting and Refunding Overpayments Gary W. Eiland, Partner King & Spalding LLP Houston, Texas Background on Government Approach
HCCA Compliance Institute April 19, 2015 Exploring CMS s Proposed Rule on Reporting and Refunding Overpayments Gary W. Eiland, Partner King & Spalding LLP Houston, Texas Background on Government Approach
Compliance. What Every Coder Needs to Know
 Compliance What Every Coder Needs to Know Presented to: AAPC Springfield Regional Conference Cynthia Trapp, CHFP, CMPE, CPC, CPC I, CCS P, CHC, PCA October 8, 2010 1 Objectives History and Consumer Demand
Compliance What Every Coder Needs to Know Presented to: AAPC Springfield Regional Conference Cynthia Trapp, CHFP, CMPE, CPC, CPC I, CCS P, CHC, PCA October 8, 2010 1 Objectives History and Consumer Demand
Policy to Provide Information for Combating Fraud, Waste and Abuse and the Ability of Employees to Report Wrongdoing
 1 of 8 and Abuse and the Ability of Employees to Report Wrongdoing 1. Purpose The purpose of this policy is to provide information for combating fraud, waste and abuse and the ability of employees to report
1 of 8 and Abuse and the Ability of Employees to Report Wrongdoing 1. Purpose The purpose of this policy is to provide information for combating fraud, waste and abuse and the ability of employees to report
Navigating ZPIC Audits: Challenges and Solutions for Health Care Providers
 Navigating ZPIC Audits: Challenges and Solutions for Health Care Providers American Health Care Association (AHCA) Scot T. Hasselman and Rahul Narula April 24, 2012 Navigating ZPIC Audits Today s Topics
Navigating ZPIC Audits: Challenges and Solutions for Health Care Providers American Health Care Association (AHCA) Scot T. Hasselman and Rahul Narula April 24, 2012 Navigating ZPIC Audits Today s Topics
AMENDED ANTI-FRAUD PLAN FOR AVMED, INC. Amended November 2014
 AMENDED ANTI-FRAUD PLAN FOR AVMED, INC. Amended November 2014 AvMed, Inc. hereby amends the Anti-Fraud Plan of its Special Investigations Unit ("SIU") which was created to identify, investigate, and rectify
AMENDED ANTI-FRAUD PLAN FOR AVMED, INC. Amended November 2014 AvMed, Inc. hereby amends the Anti-Fraud Plan of its Special Investigations Unit ("SIU") which was created to identify, investigate, and rectify
SUNY DOWNSTATE MEDICAL CENTER POLICY AND PROCEDURE. No:
 SUNY DOWNSTATE MEDICAL CENTER POLICY AND PROCEDURE Subject: Complying with the Deficit Reduction Act of 2005: Detection & Prevention of Fraud, Waste & Abuse Page 1 of 4 Prepared by: Shoshana Milstein Original
SUNY DOWNSTATE MEDICAL CENTER POLICY AND PROCEDURE Subject: Complying with the Deficit Reduction Act of 2005: Detection & Prevention of Fraud, Waste & Abuse Page 1 of 4 Prepared by: Shoshana Milstein Original
Federal Fraud and Abuse Enforcement in the ASC Space
 Federal Fraud and Abuse Enforcement in the ASC Space SCOTT R. GRUBMAN, ESQ. PARTNER CHILIVIS COCHRAN LARKINS & BEVER, LLP (ATLANTA GA) Fraud & Abuse Enforcement Landscape FBI CMS OCR MFCU DCIS DOJ HHS-OIG
Federal Fraud and Abuse Enforcement in the ASC Space SCOTT R. GRUBMAN, ESQ. PARTNER CHILIVIS COCHRAN LARKINS & BEVER, LLP (ATLANTA GA) Fraud & Abuse Enforcement Landscape FBI CMS OCR MFCU DCIS DOJ HHS-OIG
CAHABA GOVERNMENT BENEFITS ADMINISTRATORS, LLC, UNDERSTATED MEDICARE ADMINISTRATIVE CONTRACT ALLOWABLE PENSION COSTS
 Department of Health and Human Services OFFICE OF INSPECTOR GENERAL CAHABA GOVERNMENT BENEFITS ADMINISTRATORS, LLC, UNDERSTATED MEDICARE ADMINISTRATIVE CONTRACT ALLOWABLE PENSION COSTS Inquiries about
Department of Health and Human Services OFFICE OF INSPECTOR GENERAL CAHABA GOVERNMENT BENEFITS ADMINISTRATORS, LLC, UNDERSTATED MEDICARE ADMINISTRATIVE CONTRACT ALLOWABLE PENSION COSTS Inquiries about
2012 Checklist for Community Pharmacy. Medicare Part D-Related Information
 NATIONAL COMMUNITY PHARMACISTS ASSOCIATION 2012 Checklist for Community Pharmacy Medicare Part D-Related Information Medicare Part D Valid Prescriber Identifiers For 2012, CMS will continue to permit the
NATIONAL COMMUNITY PHARMACISTS ASSOCIATION 2012 Checklist for Community Pharmacy Medicare Part D-Related Information Medicare Part D Valid Prescriber Identifiers For 2012, CMS will continue to permit the
CMS Part D UPDATES. Kim Brandt Director, Program Integrity Centers for Medicare & Medicaid Services
 CMS Part D UPDATES Kim Brandt Director, Program Integrity Centers for Medicare & Medicaid Services Regulatory Changes - 42 CFR Parts 422 and 423 Outline of the presentation: I. Regulatory changes that
CMS Part D UPDATES Kim Brandt Director, Program Integrity Centers for Medicare & Medicaid Services Regulatory Changes - 42 CFR Parts 422 and 423 Outline of the presentation: I. Regulatory changes that
American Bar Association. Technical Session Between the Department of Health and Human Services and the Joint Committee on Employee Benefits
 American Bar Association Technical Session Between the Department of Health and Human Services and the Joint Committee on Employee Benefits May 2, 2006 The following notes are based upon the personal comments
American Bar Association Technical Session Between the Department of Health and Human Services and the Joint Committee on Employee Benefits May 2, 2006 The following notes are based upon the personal comments
False Claims Liability, Anti-Retaliation Protections, and Detecting and Responding to Fraud, Waste, and Abuse
 False Claims Liability, Anti-Retaliation Protections, and Detecting and Responding to Fraud, Waste, and 1. SCOPE 1.1 System-wide, including Marshfield Clinic Health System (MCHS), Inc. and its affiliated
False Claims Liability, Anti-Retaliation Protections, and Detecting and Responding to Fraud, Waste, and 1. SCOPE 1.1 System-wide, including Marshfield Clinic Health System (MCHS), Inc. and its affiliated
Managing Financial Interests: The Anti Kickback Statute (AKS)
") Managing Financial Interests: The Anti Kickback Statute (AKS) Board of Commissioners Meeting February 15, 2012 Presented by: Mic Sager, Compliance Officer Context: Business Transactions o Health Care is
Managing Financial Interests: The Anti Kickback Statute (AKS) Board of Commissioners Meeting February 15, 2012 Presented by: Mic Sager, Compliance Officer Context: Business Transactions o Health Care is
Improving Integrity in Nursing Centers
 Improving Integrity in Nursing Centers Susan Edwards Reed Smith LLP AHCA/NCAL s General Counsel Goals of this webinar Introduce you to AHCA/NCAL s Fraud and Abuse Toolkit Provide you with a basic understanding
Improving Integrity in Nursing Centers Susan Edwards Reed Smith LLP AHCA/NCAL s General Counsel Goals of this webinar Introduce you to AHCA/NCAL s Fraud and Abuse Toolkit Provide you with a basic understanding
DEFICIT REDUCTION ACT AND FALSE CLAIMS POLICY INFORMATION FOR All NEW YORK WORKFORCE MEMBERS
 DEFICIT REDUCTION ACT AND FALSE CLAIMS POLICY INFORMATION FOR All NEW YORK WORKFORCE MEMBERS The Company is committed to preventing health care fraud, waste and abuse and complying with applicable state
DEFICIT REDUCTION ACT AND FALSE CLAIMS POLICY INFORMATION FOR All NEW YORK WORKFORCE MEMBERS The Company is committed to preventing health care fraud, waste and abuse and complying with applicable state
Zone Program Integrity Contractors (ZPICs), 2013 TEXAS HEALTH CARE ASSOCIATION SUMMER MEETING
, 2013 TEXAS HEALTH CARE ASSOCIATION SUMMER MEETING") Zone Program Integrity Contractors (ZPICs), 2013 TEXAS HEALTH CARE ASSOCIATION SUMMER MEETING Carla J. Cox Jackson Walker L.L.P. cjcox@jw.com 512-236-2040 1 Zone Program Integrity Contractors (ZPICs) ZPICs
Zone Program Integrity Contractors (ZPICs), 2013 TEXAS HEALTH CARE ASSOCIATION SUMMER MEETING Carla J. Cox Jackson Walker L.L.P. cjcox@jw.com 512-236-2040 1 Zone Program Integrity Contractors (ZPICs) ZPICs
GOALS OF THIS PRESENTATION HOW WE GOT HERE WHERE WE ARE MANDATORY COMPLIANCE REQUIREMENTS LESSONS FROM MANDATORY COMPLIANCE IN NEW YORK MY PREDICTIONS
 MANDATORY COMPLIANCE: WHAT THE FUTURE LOOKS LIKE HCCA SOUTH ATLANTIC REGIONAL MEETING 1/28/11 JAMES G. SHEEHAN NEW YORK MEDICAID INSPECTOR GENERAL James.Sheehan@Omig.NY.gov GOALS OF THIS PRESENTATION HOW
MANDATORY COMPLIANCE: WHAT THE FUTURE LOOKS LIKE HCCA SOUTH ATLANTIC REGIONAL MEETING 1/28/11 JAMES G. SHEEHAN NEW YORK MEDICAID INSPECTOR GENERAL James.Sheehan@Omig.NY.gov GOALS OF THIS PRESENTATION HOW
Medicare Audit and Appeals: Practical Advice on Preparing for and Responding to RAC, ZPIC, and MAC Audits. February 2012
 Medicare Audit and Appeals: Practical Advice on Preparing for and Responding to RAC, ZPIC, and MAC Audits February 2012 Presented by: B. Scott McBride, Esq. Baker & Hostetler LLP smcbride@bakerlaw.com
Medicare Audit and Appeals: Practical Advice on Preparing for and Responding to RAC, ZPIC, and MAC Audits February 2012 Presented by: B. Scott McBride, Esq. Baker & Hostetler LLP smcbride@bakerlaw.com
Beware Excluded Individuals and Entities
 Beware Excluded Individuals and Entities Publication 7/30/2014 Kim Stanger Partner 208.383.3913 Boise kcstanger@hollandhart.com Federal laws generally prohibit providers from billing for services ordered
Beware Excluded Individuals and Entities Publication 7/30/2014 Kim Stanger Partner 208.383.3913 Boise kcstanger@hollandhart.com Federal laws generally prohibit providers from billing for services ordered
CLAIMS Section 6. Provider Service Center. Timely Claim Submission. Clean Claim. Prompt Payment
 Provider Service Center Harmony has a dedicated Provider Service Center (PSC) in place with established toll-free numbers. The PSC is composed of regionally aligned teams and dedicated staff designed to
Provider Service Center Harmony has a dedicated Provider Service Center (PSC) in place with established toll-free numbers. The PSC is composed of regionally aligned teams and dedicated staff designed to
Cardinal McCloskey Community Services. Corporate Compliance. False Claims Act and Whistleblower Provisions
 Cardinal McCloskey Community Services Corporate Compliance False Claims Act and Whistleblower Provisions Purpose: Cardinal McCloskey Community Services is committed to prompt, complete and accurate billing
Cardinal McCloskey Community Services Corporate Compliance False Claims Act and Whistleblower Provisions Purpose: Cardinal McCloskey Community Services is committed to prompt, complete and accurate billing
ADVANCE BENEFICIARY NOTICE OF NONCOVERAGE
 ADVANCE BENEFICIARY NOTICE OF NONCOVERAGE Administrative Consultant Service, LLC CMS Guidelines for Advance Beneficiary Notice (ABN) June 1, 2012 Inside this issue: Revisions to ABN Guidelines Medical
ADVANCE BENEFICIARY NOTICE OF NONCOVERAGE Administrative Consultant Service, LLC CMS Guidelines for Advance Beneficiary Notice (ABN) June 1, 2012 Inside this issue: Revisions to ABN Guidelines Medical
Fraud, Waste and Abuse: Compliance Program. Section 4: National Provider Network Handbook
 Fraud, Waste and Abuse: Compliance Program Section 4: National Provider Network Handbook December 2015 2 Our Philosophy Magellan takes provider fraud, waste and abuse We engage in considerable efforts
Fraud, Waste and Abuse: Compliance Program Section 4: National Provider Network Handbook December 2015 2 Our Philosophy Magellan takes provider fraud, waste and abuse We engage in considerable efforts
Transparency, Reporting & Data Mining
 Transparency, Reporting & Data Mining Kimberly Brandt, CHC, JD Alston & Bird, LLP Shawn DeGroot, CHC-F, CCEP, CHRC Vice President of Corporate Responsibility Regional Health Size and Scope of Data 2 1
Transparency, Reporting & Data Mining Kimberly Brandt, CHC, JD Alston & Bird, LLP Shawn DeGroot, CHC-F, CCEP, CHRC Vice President of Corporate Responsibility Regional Health Size and Scope of Data 2 1
IHCP Rendering Provider Agreement and Attestation Form
 Version 6.4E, July 2017 Page 1 of 5 This agreement must be completed, signed, and returned to the IHCP for processing. By execution of this Agreement, the undersigned entity ( Provider ) requests enrollment
Version 6.4E, July 2017 Page 1 of 5 This agreement must be completed, signed, and returned to the IHCP for processing. By execution of this Agreement, the undersigned entity ( Provider ) requests enrollment
Rendering Provider Agreement
 Rendering Provider Agreement IHCP Rendering Provider Enrollment and Profile Maintenance Packet indianamedicaid.com To enroll multiple rendering providers, complete a separate IHCP Rendering Provider Enrollment
Rendering Provider Agreement IHCP Rendering Provider Enrollment and Profile Maintenance Packet indianamedicaid.com To enroll multiple rendering providers, complete a separate IHCP Rendering Provider Enrollment
FAQ: Federal Regulations and Coding Compliance
 Question 1: Why is coding compliance important? Answer 1: Coding compliance is part of the overall effort of medical practices to comply with regulations in the coding area. Compliant claims are an indication
Question 1: Why is coding compliance important? Answer 1: Coding compliance is part of the overall effort of medical practices to comply with regulations in the coding area. Compliant claims are an indication
Corporate Compliance Topic: False Claims Act and Whistleblower Provisions
 Purpose: INDEPENDENT LIVING, Inc. (also referred to as ILI, ) is committed to prompt, complete and accurate billing of all services provided to individuals. ILI and its employees, contractors and agents
Purpose: INDEPENDENT LIVING, Inc. (also referred to as ILI, ) is committed to prompt, complete and accurate billing of all services provided to individuals. ILI and its employees, contractors and agents
The False Claims Act and Off-Label Promotion: Understanding and Minimizing the Risks for Pharmaceutical Manufacturers
 4th Annual Pharmaceutical Regulatory Congress November 12, 2003 The False Claims Act and Off-Label Promotion: Understanding and Minimizing the Risks for Pharmaceutical Manufacturers John T. Bentivoglio
4th Annual Pharmaceutical Regulatory Congress November 12, 2003 The False Claims Act and Off-Label Promotion: Understanding and Minimizing the Risks for Pharmaceutical Manufacturers John T. Bentivoglio
HOSPITAL COMPLIANCE POTENTIAL IMPLICATION OF FRAUD AND ABUSE LAWS AND REGULATIONS FOR HOSPITALS
 HOSPITAL COMPLIANCE H C C A R E G I O N A L C O N F E R E N C E A P R I L 2 8, 2 0 1 6 S A N J U A N, P U E R T O R I C O S A N C H E Z B E T A N C E S, S I F R E & M U Ñ O Z N O Y A, C S P J A I M E S
HOSPITAL COMPLIANCE H C C A R E G I O N A L C O N F E R E N C E A P R I L 2 8, 2 0 1 6 S A N J U A N, P U E R T O R I C O S A N C H E Z B E T A N C E S, S I F R E & M U Ñ O Z N O Y A, C S P J A I M E S
SANCTION SCREENING: OIG HIGH RISK PRIORITY
 SANCTION SCREENING: OIG HIGH RISK PRIORITY Overview Healthcare organizations and entities have as a Condition of Participation the affirmative duty to screen all those with whom they have a business relationship
SANCTION SCREENING: OIG HIGH RISK PRIORITY Overview Healthcare organizations and entities have as a Condition of Participation the affirmative duty to screen all those with whom they have a business relationship
4 years after services are furnished.
 RECORD TYPE RETENTION PERIOD AUTHORITY MEDICARE 1 42 U.S.C. 1395x (v)(1)(i) Contracts with Subcontractors Any contract between a provider and a subcontractor and between an organization related to the
RECORD TYPE RETENTION PERIOD AUTHORITY MEDICARE 1 42 U.S.C. 1395x (v)(1)(i) Contracts with Subcontractors Any contract between a provider and a subcontractor and between an organization related to the
False Claims Act Enforcement in the Managed Care Space: Recent Trends and Proactive Compliance Tips
 False Claims Act Enforcement in the Managed Care Space: Recent Trends and Proactive Compliance Tips Thomas Clarkson* U.S. Attorney s Office Southern District of Georgia Scott R. Grubman Chilivis Cochran
False Claims Act Enforcement in the Managed Care Space: Recent Trends and Proactive Compliance Tips Thomas Clarkson* U.S. Attorney s Office Southern District of Georgia Scott R. Grubman Chilivis Cochran
Telemedicine Fraud and Abuse Under the Microscope
 Telemedicine Fraud and Abuse Under the Microscope Session 232, February 14, 2019 Douglas Grimm, Esq., Arent Fox LLP Hillary Stemple, Esq., Arent Fox LLP 1 Conflicts of Interest Douglas Grimm, Esq. Has
Telemedicine Fraud and Abuse Under the Microscope Session 232, February 14, 2019 Douglas Grimm, Esq., Arent Fox LLP Hillary Stemple, Esq., Arent Fox LLP 1 Conflicts of Interest Douglas Grimm, Esq. Has
Anti-Kickback Statute and False Claims Act Enforcement
 Anti-Kickback Statute and False Claims Act Enforcement Nicholas Gachassin, III, Esq. Gachassin Law Firm, LLC Nick3@gachassin.com Press Conference on Health Care Fraud and the Affordable Care Act May 13,
Anti-Kickback Statute and False Claims Act Enforcement Nicholas Gachassin, III, Esq. Gachassin Law Firm, LLC Nick3@gachassin.com Press Conference on Health Care Fraud and the Affordable Care Act May 13,
AND THE NEED TO UNDERTAKE
 COMPLIANCE CHALLENGE: UNDERSTANDING FEDERAL AND STATE EXCLUSION/DEBARMENT ACTIONS, THEIR IMPLICATIONS, AND THE NEED TO UNDERTAKE REGULAR SANCTION SCREENING Overview Risks associated with exclusions Federal
COMPLIANCE CHALLENGE: UNDERSTANDING FEDERAL AND STATE EXCLUSION/DEBARMENT ACTIONS, THEIR IMPLICATIONS, AND THE NEED TO UNDERTAKE REGULAR SANCTION SCREENING Overview Risks associated with exclusions Federal
DEPARTMENT OF HEALTH AND HUMAN SERVICES. Medicare Program; Reporting and Returning of Overpayments
 This document is scheduled to be published in the Federal Register on 02/16/2012 and available online at http://federalregister.gov/a/2012-03642, and on FDsys.gov CMS-6037-P DEPARTMENT OF HEALTH AND HUMAN
This document is scheduled to be published in the Federal Register on 02/16/2012 and available online at http://federalregister.gov/a/2012-03642, and on FDsys.gov CMS-6037-P DEPARTMENT OF HEALTH AND HUMAN
GETTING SERIOUS ABOUT MEDICAID COMPLIANCE:SECTION 6402 OF PPACA AND THE DUTY OF DISCLOSURE OF IDENTIFIED OVERPAYMENTS 7/14/10
 GETTING SERIOUS ABOUT MEDICAID COMPLIANCE:SECTION 6402 OF PPACA AND THE DUTY OF DISCLOSURE OF IDENTIFIED OVERPAYMENTS 7/14/10 JAMES G. SHEEHAN NEW YORK MEDICAID INSPECTOR GENERAL James.Sheehan@OMIG.NY.GOV
GETTING SERIOUS ABOUT MEDICAID COMPLIANCE:SECTION 6402 OF PPACA AND THE DUTY OF DISCLOSURE OF IDENTIFIED OVERPAYMENTS 7/14/10 JAMES G. SHEEHAN NEW YORK MEDICAID INSPECTOR GENERAL James.Sheehan@OMIG.NY.GOV
MENTAL HEALTH MENTAL RETARDATION OF TARRANT COUNTY. Board Policy. Number A.3 July 31, 2001 COMPLIANCE PLAN
 MENTAL HEALTH MENTAL RETARDATION OF TARRANT COUNTY Board Policy Board Policy Adopted: Number A.3 July 31, 2001 OVERVIEW COMPLIANCE PLAN As adopted by the Board of Trustees on July 31, 2001 The Board of
MENTAL HEALTH MENTAL RETARDATION OF TARRANT COUNTY Board Policy Board Policy Adopted: Number A.3 July 31, 2001 OVERVIEW COMPLIANCE PLAN As adopted by the Board of Trustees on July 31, 2001 The Board of
Health Care Reform Update: Impact on Providers, Payors and Compliance
 Health Care Reform Update: Impact on Providers, Payors and Compliance Kenneth Zeko (KPMG LLP) Daniel E. Gospin (EpsteinBeckerGreen) February 18, 2011 HCCA Southwest Regional Conference Dallas, TX 1 Overview
Health Care Reform Update: Impact on Providers, Payors and Compliance Kenneth Zeko (KPMG LLP) Daniel E. Gospin (EpsteinBeckerGreen) February 18, 2011 HCCA Southwest Regional Conference Dallas, TX 1 Overview
LITIGATING AWP. Mitch Lazris/Lyndon Tretter Hogan & Hartson L.L.P. November 15, 2002
 LITIGATING AWP Mitch Lazris/Lyndon Tretter Hogan & Hartson L.L.P. November 15, 2002 Litigation Landscape Federal Gov t/states/private Class Actions Payment Systems Medicare (based on 95% of AWP) Medicare
LITIGATING AWP Mitch Lazris/Lyndon Tretter Hogan & Hartson L.L.P. November 15, 2002 Litigation Landscape Federal Gov t/states/private Class Actions Payment Systems Medicare (based on 95% of AWP) Medicare
FUNDAMENTALS OF MEDICARE INTRO
 FUNDAMENTALS OF MEDICARE INTRO Barry D. Alexander, Esq.* Nelson Mullins Riley & Scarborough, LLP 4140 ParkLake Ave., GlenLake One, 2 nd Floor Raleigh, NC 27612 919.877.3802 barry.alexander@nelsonmullins.com
FUNDAMENTALS OF MEDICARE INTRO Barry D. Alexander, Esq.* Nelson Mullins Riley & Scarborough, LLP 4140 ParkLake Ave., GlenLake One, 2 nd Floor Raleigh, NC 27612 919.877.3802 barry.alexander@nelsonmullins.com
American Bar Association. Technical Session Between the Centers for Medicare and Medicaid Services and the Joint Committee on Employee Benefits
 American Bar Association Technical Session Between the Centers for Medicare and Medicaid Services and the Joint Committee on Employee Benefits May 5, 2008 The following notes are based upon the personal
American Bar Association Technical Session Between the Centers for Medicare and Medicaid Services and the Joint Committee on Employee Benefits May 5, 2008 The following notes are based upon the personal
This policy applies to all employees, including management, contractors, and agents. For purpose of this policy, a contractor or agent is defined as:
 Policy and Procedure: Corporate Compliance Topic: Purpose: Choice of NY is committed to prompt, complete, and accurate billing of all services provided to individuals. Choice of NY and its employees, contractors,
Policy and Procedure: Corporate Compliance Topic: Purpose: Choice of NY is committed to prompt, complete, and accurate billing of all services provided to individuals. Choice of NY and its employees, contractors,
RACs and Beyond. Kristen Smith, MHA, PT. Peter Thomas, JD Ron Connelly, JD Christina Hughes, JD, MPH. Senior Consultant, Fleming-AOD.
 RACs and Beyond Kristen Smith, MHA, PT Senior Consultant, Fleming-AOD Peter Thomas, JD Ron Connelly, JD Christina Hughes, JD, MPH The Powers Firm RACs and Beyond Objectives Describe the various types of
RACs and Beyond Kristen Smith, MHA, PT Senior Consultant, Fleming-AOD Peter Thomas, JD Ron Connelly, JD Christina Hughes, JD, MPH The Powers Firm RACs and Beyond Objectives Describe the various types of
7/25/2018. Government Enforcement in the Clinical Laboratory Space. The Statutes & Regulations. The Stark Law. The Stark Law.
 Government Enforcement in the Clinical Laboratory Space 2 SCOTT R. GRUBMAN, ESQ. The Statutes & Regulations 3 4 AKA the physician self-referral law The Rule: If physician (or immediate family member) has
Government Enforcement in the Clinical Laboratory Space 2 SCOTT R. GRUBMAN, ESQ. The Statutes & Regulations 3 4 AKA the physician self-referral law The Rule: If physician (or immediate family member) has
Version 7.5, August 2017 Page 1 of 11
 Version 7.5, August 2017 Page 1 of 11 Overview IHCP Waiver Rendering Provider Enrollment and Profile Maintenance Packet indianamedicaid.com Before You Begin! You are encouraged to use the Provider Healthcare
Version 7.5, August 2017 Page 1 of 11 Overview IHCP Waiver Rendering Provider Enrollment and Profile Maintenance Packet indianamedicaid.com Before You Begin! You are encouraged to use the Provider Healthcare
Auditing RACphobia. Lamon Willis, CPCO, CPC-I, CPC-H, CPC AHIMA-Approved ICD-10-CM/PCS Trainer Xerox Healthcare Consultant
 Auditing RACphobia Lamon Willis, CPCO, CPC-I, CPC-H, CPC AHIMA-Approved ICD-10-CM/PCS Trainer Xerox Healthcare Consultant 1 Agenda Overview of present industry landscape in relation to auditing Audit Entities
Auditing RACphobia Lamon Willis, CPCO, CPC-I, CPC-H, CPC AHIMA-Approved ICD-10-CM/PCS Trainer Xerox Healthcare Consultant 1 Agenda Overview of present industry landscape in relation to auditing Audit Entities
Agenda. Strategic Considerations in Resolving Voluntary Government Disclosures
 Strategic Considerations in Resolving Voluntary Government Disclosures Health Care Compliance Association Annual Compliance Institute Patrick Garcia Hall, Render, Killian, Heath, & Lyman, P.C. Kenneth
Strategic Considerations in Resolving Voluntary Government Disclosures Health Care Compliance Association Annual Compliance Institute Patrick Garcia Hall, Render, Killian, Heath, & Lyman, P.C. Kenneth
2/24/2017. Agenda. Determine Potential Liability. Strategic Considerations in Resolving Voluntary Government Disclosures. Relevant legal authorities:
 Strategic Considerations in Resolving Voluntary Government Disclosures Health Care Compliance Association Annual Compliance Institute Patrick Garcia Hall, Render, Killian, Heath, & Lyman, P.C. Kenneth
Strategic Considerations in Resolving Voluntary Government Disclosures Health Care Compliance Association Annual Compliance Institute Patrick Garcia Hall, Render, Killian, Heath, & Lyman, P.C. Kenneth
Medicare. Claim Review Programs: MR, NCCI Edits, MUEs, CERT, and RAC. Official CMS Information for Medicare Fee-For-Service Providers
 Medicare Claim Review Programs: MR, NCCI Edits, MUEs, CERT, and RAC R Official CMS Information for Medicare Fee-For-Service Providers Background Since 1996, the Centers for Medicare & Medicaid Services
Medicare Claim Review Programs: MR, NCCI Edits, MUEs, CERT, and RAC R Official CMS Information for Medicare Fee-For-Service Providers Background Since 1996, the Centers for Medicare & Medicaid Services
Claim Rejections and Appeals Process Practical Tools for Seminar Learning
 Claim Rejections and Appeals Process Practical Tools for Seminar Learning Copyright 2007 American Health Information Management Association. All rights reserved. Disclaimer The American Health Information
Claim Rejections and Appeals Process Practical Tools for Seminar Learning Copyright 2007 American Health Information Management Association. All rights reserved. Disclaimer The American Health Information
Challenges in Maintaining a Laboratory Compliance Program
 Challenges in Maintaining a Laboratory Compliance Program Christopher P. Young, CHC Writer, G2 Compliance Advisor cpyoung@labcomply.com - 602-277-5365 Objectives Learn the latest developments in clinical
Challenges in Maintaining a Laboratory Compliance Program Christopher P. Young, CHC Writer, G2 Compliance Advisor cpyoung@labcomply.com - 602-277-5365 Objectives Learn the latest developments in clinical
The Indiana Family and Social Services Administration Office of Medicaid Policy & Planning. Indiana Health Coverage Programs Program Integrity (PI)
") The Indiana Family and Social Services Administration Office of Medicaid Policy & Planning Indiana Health Coverage Programs Program Integrity (PI) 2018 IHCP Provider Workshops Agenda Program Integrity
The Indiana Family and Social Services Administration Office of Medicaid Policy & Planning Indiana Health Coverage Programs Program Integrity (PI) 2018 IHCP Provider Workshops Agenda Program Integrity
Table of Contents. DME MAC Jurisdiction C Supplier Manual. Table of Contents. 1. Introduction
 DME MAC Jurisdiction C Supplier Manual Table of Contents 1. Welcome CGS s Role as a DME MAC What is Medicare? What is DME? Deductible and Coinsurance Eligibility Medicare ID Health Insurance Claim Number
DME MAC Jurisdiction C Supplier Manual Table of Contents 1. Welcome CGS s Role as a DME MAC What is Medicare? What is DME? Deductible and Coinsurance Eligibility Medicare ID Health Insurance Claim Number
Medicare Part D: Retiree Drug Subsidy
 A D V I S O R Y S E R V I C E S Medicare Part D: Retiree Drug Subsidy Programs to Control Fraud, Waste, and Abuse September, 2006 K P M G L L P Overview Summary Medicare Part D Prescription Drug Program
A D V I S O R Y S E R V I C E S Medicare Part D: Retiree Drug Subsidy Programs to Control Fraud, Waste, and Abuse September, 2006 K P M G L L P Overview Summary Medicare Part D Prescription Drug Program
Medicare Contractor Provider Satisfaction Survey Administration
 Medicare Contractor Provider Satisfaction Survey- 2009 Administration Public Report September 11, 2009 Prepared for: Centers for Medicare & Medicaid Services 7500 Security Boulevard Baltimore, MD 21244
Medicare Contractor Provider Satisfaction Survey- 2009 Administration Public Report September 11, 2009 Prepared for: Centers for Medicare & Medicaid Services 7500 Security Boulevard Baltimore, MD 21244
Medical Ethics. Paul W. Kim, JD, MPH O B E R K A L E R
 Medical Ethics Paul W. Kim, JD, MPH O B E R K A L E R 410-347-7344 pwkim@ober.com 1 Agenda Federal Fraud & Abuse Laws Federal Privacy Laws Enrollment Audits Post-Payment Audits Pre-Payment Reviews 2 False
Medical Ethics Paul W. Kim, JD, MPH O B E R K A L E R 410-347-7344 pwkim@ober.com 1 Agenda Federal Fraud & Abuse Laws Federal Privacy Laws Enrollment Audits Post-Payment Audits Pre-Payment Reviews 2 False
Fact Sheet. AARP Public Policy Institute. Improving the Medicare Appeals Process
 Fact Sheet Improving the Medicare Appeals Process AARP Public Policy Institute The Medicare appeals process designed to protect beneficiaries access to treatment and quality of care can be streamlined
Fact Sheet Improving the Medicare Appeals Process AARP Public Policy Institute The Medicare appeals process designed to protect beneficiaries access to treatment and quality of care can be streamlined
Medicare Parts C & D Fraud, Waste, and Abuse Training
 Medicare Parts C & D Fraud, Waste, and Abuse Training IMPORTANT NOTE All persons who provide health or administrative services to Medicare enrollees must satisfy FWA training requirements. This module
Medicare Parts C & D Fraud, Waste, and Abuse Training IMPORTANT NOTE All persons who provide health or administrative services to Medicare enrollees must satisfy FWA training requirements. This module
Medicare Parts C & D Fraud, Waste, and Abuse Training and General Compliance Training. Developed by the Centers for Medicare & Medicaid Services
 Medicare Parts C & D Fraud, Waste, and Abuse Training and General Compliance Training Developed by the Centers for Medicare & Medicaid Services Important Notice This training module consists of two parts:
Medicare Parts C & D Fraud, Waste, and Abuse Training and General Compliance Training Developed by the Centers for Medicare & Medicaid Services Important Notice This training module consists of two parts:
Can Negligence Really Trigger False Claims Act Exposure?
 What s the Future of the CMS 60-Day Overpayment Rule? Can Negligence Really Trigger False Claims Act Exposure? Barbara Rowland Washington, D.C. Office Chair Internal Investigations & White Collar Defense
What s the Future of the CMS 60-Day Overpayment Rule? Can Negligence Really Trigger False Claims Act Exposure? Barbara Rowland Washington, D.C. Office Chair Internal Investigations & White Collar Defense
A DISCUSSION WITH THE OIG
 1 A DISCUSSION WITH THE OIG MICHAEL J ARMSTRONG REGIONAL INSPECTOR GENERAL FOR AUDIT SERVICES STEPHEN J CONWAY DIRECTOR, ADVANCED AUDIT TECHNIQUES ROBERT K DECONTI CHIEF, ADMINISTRATIVE & CIVIL REMEDIES
1 A DISCUSSION WITH THE OIG MICHAEL J ARMSTRONG REGIONAL INSPECTOR GENERAL FOR AUDIT SERVICES STEPHEN J CONWAY DIRECTOR, ADVANCED AUDIT TECHNIQUES ROBERT K DECONTI CHIEF, ADMINISTRATIVE & CIVIL REMEDIES
SOUTH NASSAU COMMUNITIES HOSPITAL One Healthy Way, Oceanside, NY 11572
 SOUTH NASSAU COMMUNITIES HOSPITAL One Healthy Way, Oceanside, NY 11572 POLICY TITLE: Compliance with Applicable Federal and State False Claims Acts POLICY NUMBER: OF-ADM-232 DEPARTMENT: Hospital-wide BACKGROUND/PURPOSE
SOUTH NASSAU COMMUNITIES HOSPITAL One Healthy Way, Oceanside, NY 11572 POLICY TITLE: Compliance with Applicable Federal and State False Claims Acts POLICY NUMBER: OF-ADM-232 DEPARTMENT: Hospital-wide BACKGROUND/PURPOSE
GAINSHARING & PAY FOR PERFORMANCE -- P4P UPDATE ON RECENT DEVELOPMENTS AND INITIATIVES
 GAINSHARING & PAY FOR PERFORMANCE -- P4P UPDATE ON RECENT DEVELOPMENTS AND INITIATIVES presented by Robert D. Girard, Esq. Davis Wright Tremaine LLP A. Gain-Sharing B. Provider P4P programs C. Government
GAINSHARING & PAY FOR PERFORMANCE -- P4P UPDATE ON RECENT DEVELOPMENTS AND INITIATIVES presented by Robert D. Girard, Esq. Davis Wright Tremaine LLP A. Gain-Sharing B. Provider P4P programs C. Government
AGENCY POLICY. IDENTIFICATION NUMBER: CCD001 DATE APPROVED: Nov 1, 2017 POLICY NAME: False Claims & Whistleblower SUPERSEDES: May 18, 2009
 IDENTIFICATION NUMBER: CCD001 DATE APPROVED: Nov 1, 2017 POLICY NAME: False Claims & Whistleblower SUPERSEDES: May 18, 2009 Provisions OWNER S DEPARTMENT: Compliance APPLICABILITY: All Agency Programs
IDENTIFICATION NUMBER: CCD001 DATE APPROVED: Nov 1, 2017 POLICY NAME: False Claims & Whistleblower SUPERSEDES: May 18, 2009 Provisions OWNER S DEPARTMENT: Compliance APPLICABILITY: All Agency Programs
CORPORATE COMPLIANCE POLICY AND PROCEDURE
 Title: Fraud Waste and Abuse Laws in Health Care Policy # 1011 Sponsor: Corporate Compliance Approved by: Russell J. Matuszak, Interim Director, Corporate Compliance and Chief Privacy Officer Issued: Page:
Title: Fraud Waste and Abuse Laws in Health Care Policy # 1011 Sponsor: Corporate Compliance Approved by: Russell J. Matuszak, Interim Director, Corporate Compliance and Chief Privacy Officer Issued: Page:
Amy Bingham, Compliance Director Reviewed Only Date: 6/05,1/31/2011, 1/24/2012 Supersedes and replaces: "CC-02 - Anti-
 MOLINA HEALTHCARE Polic:y and Procedure No. C 08 of Utah Effective Date: November 2003 Reviewed and Revised Ollie: 2/6/08; 2/25/0S; 11 /5/0S; II/ IS/OS, 3/4/09, 6/9/09, S/31 / 1O Amy Bingham, Compliance
MOLINA HEALTHCARE Polic:y and Procedure No. C 08 of Utah Effective Date: November 2003 Reviewed and Revised Ollie: 2/6/08; 2/25/0S; 11 /5/0S; II/ IS/OS, 3/4/09, 6/9/09, S/31 / 1O Amy Bingham, Compliance
The Indiana Family and Social Services Administration Office of Medicaid Policy & Planning
 The Indiana Family and Social Services Administration Office of Medicaid Policy & Planning Indiana Health Coverage Programs Program Integrity (PI) 2017 Annual IHCP Provider Workshops James Waddick, Jr.,
The Indiana Family and Social Services Administration Office of Medicaid Policy & Planning Indiana Health Coverage Programs Program Integrity (PI) 2017 Annual IHCP Provider Workshops James Waddick, Jr.,
Sharmin Rahman, BS Consultant, Compliance. Senior Manager, Compliance. Objectives. We the People - Government Authority
 Exclusion Checks: Who? What? When? Where? How? Sharmin Rahman, BS Consultant, Compliance Karen Voiles,MBA,CHC, CHPC, CHRC Senior Manager, Compliance Objectives We the People - Government Authority Legislative
Exclusion Checks: Who? What? When? Where? How? Sharmin Rahman, BS Consultant, Compliance Karen Voiles,MBA,CHC, CHPC, CHRC Senior Manager, Compliance Objectives We the People - Government Authority Legislative
Stark Self-Disclosure. Thomas S. Crane 1/ Mintz Levin Cohn Ferris Glovsky and Popeo, PC
 Stark Self-Disclosure Thomas S. Crane 1/ Mintz Levin Cohn Ferris Glovsky and Popeo, PC A. Background 1. Stark Law The Physician Self-Referral Statute (or the Stark Law ) prohibits a physician from referring
Stark Self-Disclosure Thomas S. Crane 1/ Mintz Levin Cohn Ferris Glovsky and Popeo, PC A. Background 1. Stark Law The Physician Self-Referral Statute (or the Stark Law ) prohibits a physician from referring
Approval Signatures: *This policy is based on VO legacy policy LC310 issued 12/4/06 and last approved 3/14/14
 Category: A Page 1 of 5 Beacon Health Options Policies and Procedure cover the operations of all entities within the BVO Holdings, LLC corporate structure, including but not limited to Beacon Health Strategies
Category: A Page 1 of 5 Beacon Health Options Policies and Procedure cover the operations of all entities within the BVO Holdings, LLC corporate structure, including but not limited to Beacon Health Strategies
Certifying Employee Training Navicent Health s Corporate Integrity Agreement Year Two
 Certifying Employee Training Navicent Health s Corporate Integrity Agreement Year Two Corporate Integrity Agreement Effective 4/23/2015 Term of five years Basic Requirement: Maintain a Compliance Program
Certifying Employee Training Navicent Health s Corporate Integrity Agreement Year Two Corporate Integrity Agreement Effective 4/23/2015 Term of five years Basic Requirement: Maintain a Compliance Program
COMPLIANCE DEPARTMENT. LSUHSC-S Louisiana State University Health Sciences Center Shreveport ACKNOWLEDGEMENT RECEIPT
 COMPLIANCE DEPARTMENT LSUHSC-S Louisiana State University Health Sciences Center Shreveport ACKNOWLEDGEMENT RECEIPT for COMPLIANCE, HIPAA PRIVACY, AND INFORMATION SECURITY SELF-STUDY GUIDE I hereby certify
COMPLIANCE DEPARTMENT LSUHSC-S Louisiana State University Health Sciences Center Shreveport ACKNOWLEDGEMENT RECEIPT for COMPLIANCE, HIPAA PRIVACY, AND INFORMATION SECURITY SELF-STUDY GUIDE I hereby certify
Required CMS Contract Clauses Revised 8/28/14 CMS MCM Guidance Chapter 21
 Required CMS Contract Clauses Revised 8/28/14 CMS MCM Guidance Chapter 21 The following provisions are required to be incorporated into all contracts with first tier, downstream, or related entities as
Required CMS Contract Clauses Revised 8/28/14 CMS MCM Guidance Chapter 21 The following provisions are required to be incorporated into all contracts with first tier, downstream, or related entities as
Health Law 101: Issue-Spotting In Dealing With Health-Care Providers. by William H. Hall Jr.
 Health Law 101: Issue-Spotting In Dealing With Health-Care Providers by William H. Hall Jr. The anti-kickback statute prohibits arrangements that might be common in other industries. Health care is among
Health Law 101: Issue-Spotting In Dealing With Health-Care Providers by William H. Hall Jr. The anti-kickback statute prohibits arrangements that might be common in other industries. Health care is among
Coverage of IDE Clinical Trial Costs: Navigating the Medicare Maze
 Coverage of IDE Clinical Trial Costs: Navigating the Medicare Maze by Jeffrey D. Zigler, JD 12 November 2011 Regulatory professionals recognize the value of clinical research in the medical device development
Coverage of IDE Clinical Trial Costs: Navigating the Medicare Maze by Jeffrey D. Zigler, JD 12 November 2011 Regulatory professionals recognize the value of clinical research in the medical device development