PATIENT INFORMATION FORM
|
|
|
- Elisabeth Garrison
- 5 years ago
- Views:
Transcription
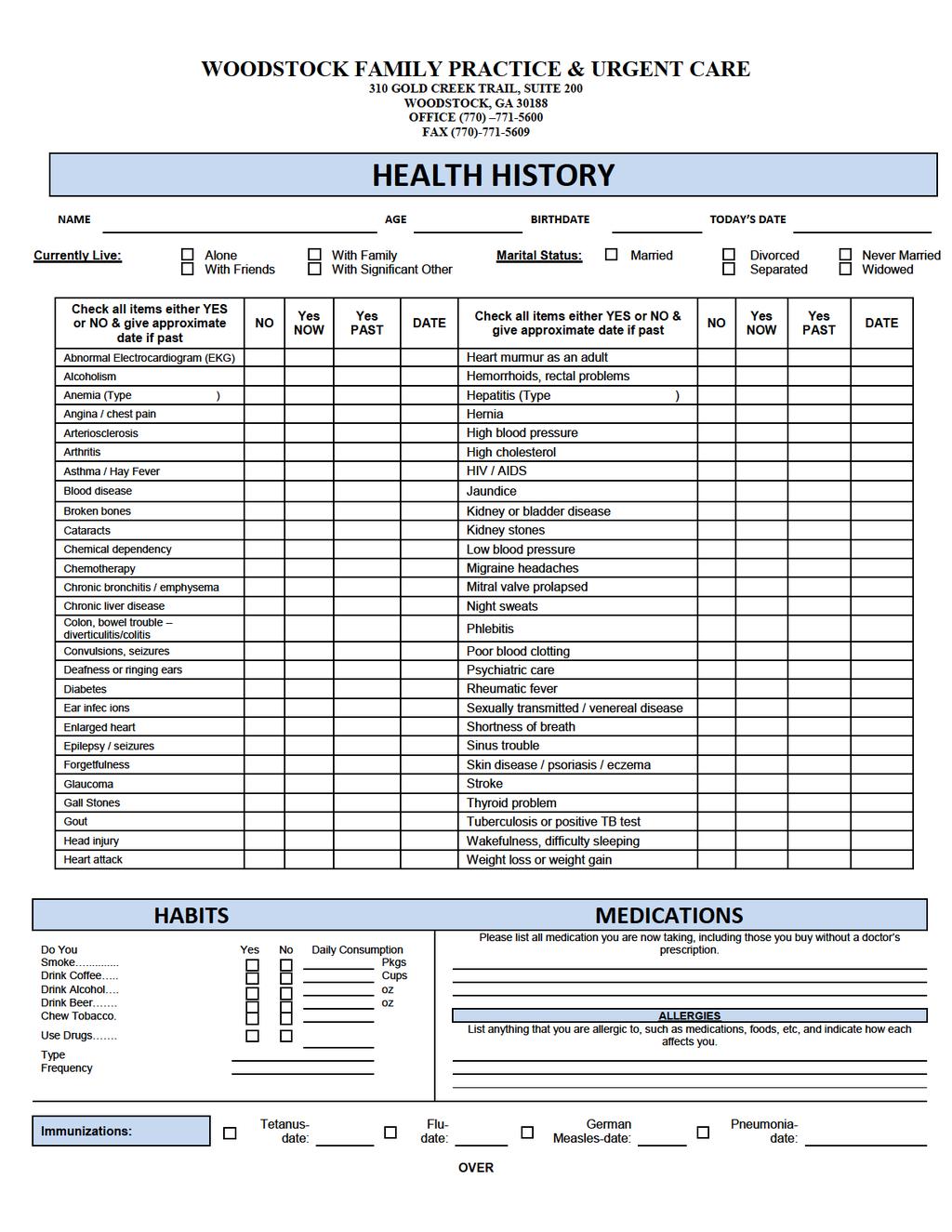
1 PATIENT INFORMATION FORM LAST NAME FIRST NAME M.I. ADDRESS: APT# CITY STATE ZIP (HOME) PHONE (WORK) Address (CELL) PHONE SSN BIRTHDATE SEX (M) (F) PATIENT S EMPLOYER OCCUPATION EMPLOYER S ADDRESS RACE (Please circle): Asian African Am. Hispanic White Refuse Other MARITAL STATUS: S M W D PREFERRED LANGUAGE ETHNICITY (Please Circle): Hispanic Not Hispanic Refuse Referral Source: EMERGENCY CONTACT NAME RELATIONSHIP EMERGENCY CONTACT PHONE NUMBER INSURANCE CARRIER INSURED S SSN INSURED S NAME INSURED S BIRTHDATE RELATIONSHIP TO PATIENT SECONDARY INSURANCE CARRIER INSURED S SSN INSURED S NAME INSURED S BIRTHDATE Pharmacy Information (telephone number/location): IF PATIENTS IS A MINOR, COMPLETE THE NEXT TWO LINES FATHER S NAME MOTHER S NAME PHONE PHONE INORDER TO MAINTAIN CONTINUITY OF CARE, I GIVE PERMISSION TO WOODSTOCK FAMILY PRACTICE & URGENT CARE TO RELEASE MY MEDICAL RECORDS TO ANY SPECIALISTS, HOSPITALS OR MEDICAL FACILITIES ASSOCIATED WITH MY CARE PLAN. I UNDERSTAND THAT WOODSTOCK FAMILY PRACTICE & URGENT CARE ABIDES BY HIPAA REGULATIONS AND THAT ONLY THE RECORDS PERTINENT TO THE VISIT WILL BE RELEASED. I AUTHORIZE THE RELEASE OF MEDICAL INFORMATION NECESSARY TO PROCESS INSURANCE CLAIMS. Patient Name: Responsible Party (If not the patient): Signature: Patient Birthdate: Contact Phone #: Date:
2 Patient Name: DOB: Date: HIPAA Privacy Policy It is the policy of our practice that all physicians and staff members preserve the integrity and the confidentiality of protected health information (PHI) pertaining to our patients. The purpose of this policy is to ensure that our entire practice have the necessary medical and PHI to provide our patients the highest quality medical care possible patients should not be afraid to provide information to our practice, physicians, staff members for purposes of treatment, payment, and healthcare procedures. Our HIPAA policy in its entirety can be obtained through our office at any time. Let us know if you would like to receive a copy prior to signing this consent. Authorization: Please initial Please initial I understand HIPAA and its policies. I authorize the release of medical information necessary to process insurance claims and to health care professionals for treatment of care. PRESCIPTION HISTORY AUTHORIZATION I,, authorize the review of my prescription history for reasons of evaluation and treatments. PATIENT CONFIDENTIALITY Patient confidentiality is a top priority at Woodstock Family Practice & Urgent Care. Therefore, it is important that you provide us with the following information to ensure there is not violation of your privacy. In the event that I,, am unable to be reached, Woodstock Family Practice & Urgent Care may leave my test results or lab results with the following: (please check all that apply) I may be reached at work. Telephone #: May leave normal results on answering machine/voice mail at work. May leave normal results on answering machine/voice mail at home. May leave normal results on answering machine/voice mail on cell phone. May leave all results on answering machine/voice mail at home/cell/work. Other; Describe: Release Authorization of Medical Information Also, it is our experience that some patients may or may not wish for our staff to discuss medical conditions/information with family members. Please specify any family members who may obtain or call and discuss your medical information. Signature: Date:
3 Insurance Information * YOU ARE RESPONSIBLE FOR SUPPLYING ALL CURRENT ACTIVE INSURANCE INFORMATION AND NOTIFYING OFFICE OF ANY CHANGES TO YOUR INSURANCE. YOUR ACCOUNT AT WOODSTOCK FAMILY PRACCTICE & URGENT CARE IS YOUR RESPONSIBILITY. INSURANCE YES NO (SELF PAY) RESPONSIBLE PARTY: SELF GUARANTOR RELATIONSHIP NAME ADDRESS CITY STATE ZIP DOB / / Advance Directive Information In the events that I m unable to make health care decision for myself, I designate the following individual as my agent to make health care decision for me: I do not have a designated surrogate decision Maker Surrogate Decision Maker NAME RELATIONSHIP ADDRESS CITY STATE ZIP PHONE Signature: Date:
4 FINANCIAL POLICY Patient Name: DOB: Date: Welcome to our office. We are pleased to have you as a patient. We are committed to meeting your health care needs. It is our goal to provide you with the best possible health care and to keep your insurance or other financial arrangements as simple as possible. In order to accomplish this in a cost-effective manner, we ask that you adhere to the following guidelines: 1. You are ultimately responsible for payment of services you rendered from our office. Please contact your insurance company to confirm coverage and benefits. We can never guarantee coverage for any service provided by our office. You are responsible for any services that the insurance does not cover, such as but not limited to well visits, procedures, injections and immunizations, balance left after all insurance payments and contracted adjustments. 2. It is your responsibility to provide us with your current address, telephone number, and insurance information at each visit. If you do not have proof of current insurance at your visit, you will be considered a self pay patient for that visit and payment in full will be due at the time of service. 3. It is your responsibility to contact your insurance carrier to confirm that our physicians participate in your plan and that we are your primary care provider. If your insurance is a managed care plan, our Doctor must be listed as the PCP. If our Doctor is not listed as the PCP, your visit will be considered a self pay patient for the visit and payment in full will be due at the time of service. 4. All co-payments and deductibles are collected at the time of service. 5. If you miss your appointment without notification, you will be charged a fee as below. APPLIED FEES: 1. Appointment cancelled less than 24 hours notice for appointments $ Appointment cancelled less than 48 hours notice for echocardiograms $ Patient NO SHOW for an appointment/physical/procedures $30.00/$50.00/$ Returned payment for Non-Sufficient Funds $ If patient account(s) is unpaid 90 days + interest charge will be applied $% applied 5. Collection Agency administrative charge $ To request medical records $ Completion of all forms (to include by not limited to) $ Adoption forms, Camp forms, FMLA, Disability, life insurance forms, school or camp physicals if not given at time of physical, other miscellaneous administrative forms required by third parties other than your insurance company. All of these activities add to our cost of caring for patients. Still, we are committed to providing you the best possible care. With you, our patient, we look forward to a lasting and healthy relationship and we thank you for your understanding and cooperation. PLEASE NOTE: You must be familiar with your insurance benefits. You are responsible for any balance on your account after 90 days of submission of claim to insurance company, whether your insurance has paid or not. PLEASE UNDERSTAND: We file insurance claim as a courtesy to our patients. You have a contract with your insurance company of choice. We are not responsible for how your insurance company handles its claims or for the benefits they pay. We do not guarantee what your insurance company will or will not do with each claim. This is performed as a courtesy to you. I have read and understand the financial policy stated above and agree to accept responsibility as described. Signature: Date:
5 ADMINISTRATIVE POLICY Patient Name: DOB: Date: REFERRAL/PRIOR AUTHORIZATION/PRIOR CERTIFICATION If your plan requires a referral, it is your responsibility to obtain this prior to being seen by a specialist. If we are required to obtain the referral or prior authorization/certification for you, please notify our office 5 days prior to the specialist s visit or procedure so that we have ample time to acquire this information from your insurance company. Per office policy, we do not back date referrals or prior authorization/certification. MEDICAL RECORD REQUEST All medical record requests must be on received in our office 7-10 business days prior to the date needed. Our fee for copies of medical records is based on the number of pages. Medical records requested by physicians treating the patient are free of charge. REFILL REQUEST and NURSE CALLS Please allow 3 business days for your refill request to be filled. Although we will try to return patient telephone request within 48 hrs, we ask that you kindly give our staff 72 hrs to return any requests. Please have the pharmacy fax the request to us at (770) Most medication refills may require a follow-up visit with the physician. Antibiotics and pain medication will not be called in after hours. An appointment with the physician will be required to replace lost or misplace prescriptions. COMPLETION OF ALL FORMS (to include by not limited to) Please notify our office 7-10 business days prior the forms needing to be completed. The forms may be completed earlier than that stated but please allow ample time for the completion of the forms. Our fee for completion of form is in our financial policy. 1. Adoption forms 2. Camp forms 3. FMLA, disability, life insurance forms 4. Travel letters 5. School forms 6. Sports Physical forms 7. Other miscellaneous administrative forms required by third parties other than your health insurance company OFFICE POLICY ON MANAGED CARE INSURERS We are pleased to meet the needs of our patients by enrolling with various managed care insurance programs. While we are able to provide you with this service, it is extremely difficult to keep track of all the individual insurance requirements of each plan. Even with the same insurance company, plans often may differ. Providing quality medical care for our patients is our primary concern, and we are more than willing to provide that care based on your insurance contract guidelines. We request at each visit that you advise us of your guidelines. Unfortunately, if you do not inform us of any special requirements in your contract and subsequently provide services, or order services such as label work or procedures that are not covered, the office will have no choice but to bill you directly for all said charges. All fees submitted and denied by your insurance carrier will become your responsibility. With your cooperation, you should be able to receive all benefits offered by your insurance plan, and we will be able to concentrate on caring for your medical needs. I have read and understand the administrative policy stated above and agree to accept responsibility as described. Signature: Date:
6 PATIENT CONSENT FORM During the course of my care and treatment, I understand that various types of tests, diagnostic or treatment procedures ( Procedures ) may be necessary. These Procedures may be performed by physicians, nurses, technicians, physician assistants or other healthcare professionals ( Healthcare Professionals ) at Woodstock Family Practice & Urgent Care. While routinely performed without incident, there may be material risks associated with each of these Procedures. I understand that it is not possible to list every risk for every Procedure and that this form only attempts to identify the most common material risks and the alternatives (if any) associated with the Procedures. I also understand that various Healthcare Professionals may have differing opinions as to what constitutes material risks and alternative Procedures. The Procedures may include, but are not limited to the following: (1) Needle Sticks, such as shots, injections, intravenous lines, or intravenous injections (IVs). The material risks associated with these types of Procedures include, but are not limited to, nerve damage, infection, infiltration (which is fluid leakage into surrounding tissue). (2) Physical tests, assessments and treatments such as vital signs, internal body examinations, wound cleansing, wound dressing, range of motion checks, and other similar procedures. The material risks associated with these types of Procedures include, but are not limited to allergic reactions, infection, severe loss of blood, muscular-skeletal or internal injuries, nerve damage, loss of limb function, paralysis or partial paralysis, disfiguring scar, worsening of the condition and death. Apart from using modified Procedure and/or refusal of treatment, no practical alternatives exists. (3) Administration of Medications whether orally, rectally, topically or through my eye, ear or nose. The material risks associated with these types of Procedures include, but are not limited to, perforation, puncture, infection, allergic reaction, brain damage or death. Apart from varying the method of administration and/or refusal of treatment, no practical alternative exists. (4) Drawing Blood, Bodily Fluids or Tissue Samples such as that done for laboratory testing and analysis. The material risks associated with this type of Procedure include but are not limited to, paralysis of partial paralysis, nerve damage, infection, bleeding and loss of limb function. Apart from long-term observation and/or refusal of treatment, no practical alternative exists. (5) Insertion of Internal Tubes such as bladder catheterizations, nasogastric tubes, rectal tubes, drainage tubes, enemas, etc. The material risks associated with these type of Procedure include, but are not limited to, internal injuries, bleeding, infection, allergic reaction, loss of bladder control and/or difficulty urinating after catheter removal. Apart from external collection devices or refusal of treatment, no practical alternatives exists. I understand that: The practice of medicine is not an exact science and that NO GUARANTEES OR ASSURANCES HAVE BEEN MADE TO ME concerning the outcome and/or result of any Procedures; The Healthcare Professional participating in my care will relay on my documented medical history, as well as other information obtained from me, family or others having knowledge about me, in determining whether to perform or recommend the Procedures therefore, I agree to provide accurate and complete information about my medical history and conditions; and By signing this form: I consent to healthcare Professionals performing Procedures as they may deem reasonably necessary or desirable in the exercise of their professional judgment, including those Procedures that may be unforeseen or not known to be needed at the time this consent is obtained; and I acknowledge that I have been informed in general terms of the nature and purpose of the Procedures; the material risks of the Procedures; and practical alternatives to the Procedures. If I have any questions or concerns regarding these Procedures, I will ask my physician to provide me with additional information. I also understand that my physician may ask me to sign additional informed Consent documents. Patient Name: Responsible Party (If not the patient): Signature: Patient Birthdate: Contact Phone # : Date:
7
8
Patient Registration Form
 Patient Registration Form PATIENT INFORMATION Full legal name (First, Middle, Last, suffix) Nickname Sex: Male Female Date of birth Social security number Race Preferred language Ethnicity: Hispanic n-hispanic
Patient Registration Form PATIENT INFORMATION Full legal name (First, Middle, Last, suffix) Nickname Sex: Male Female Date of birth Social security number Race Preferred language Ethnicity: Hispanic n-hispanic
PATIENT INFORMATION FORM
 PATIENT INFORMATION FORM Alpharetta Braselton Cumming East Cobb Johns Creek Marietta Sandy Springs Sugar Hill West Paces Woodstock www.napc.md ALL PATIENTS OR RESPONSIBLE PARTIES MUST COMPLETE THIS FORM
PATIENT INFORMATION FORM Alpharetta Braselton Cumming East Cobb Johns Creek Marietta Sandy Springs Sugar Hill West Paces Woodstock www.napc.md ALL PATIENTS OR RESPONSIBLE PARTIES MUST COMPLETE THIS FORM
PATIENT REGISTRATION FORM
 Today s Date / / PATIENT REGISTRATION FORM PATIENT INFORMATION Patient Name Last First Middle Is this your legal name? If not, what is your legal name? Birthdate Age Sex q YES q NO / / q M q F q T Street
Today s Date / / PATIENT REGISTRATION FORM PATIENT INFORMATION Patient Name Last First Middle Is this your legal name? If not, what is your legal name? Birthdate Age Sex q YES q NO / / q M q F q T Street
PATIENT INFORMATION. Name: Date of Birth: Age: Address: Social Security #: City: Sex: Marital Status: State: Zip: Language: GUARANTOR INFORMATION
 PATIENT INFORMATION Name: Date of Birth: Age: Address: Social Security #: City: Sex: Marital Status: State: Zip: Language: Home Phone#: Race: Work Phone#: Ethnicity/Nationality: Cell Phone#: Employer:
PATIENT INFORMATION Name: Date of Birth: Age: Address: Social Security #: City: Sex: Marital Status: State: Zip: Language: Home Phone#: Race: Work Phone#: Ethnicity/Nationality: Cell Phone#: Employer:
Accessible, Affordable, Quality Patient Centered Medical Home
 PATIENT REGISTRATION Child :Last Name: First Name: MI: D.O.B.: / / Sex: Primary Language: Ethnicity: Hispanic / Non-Hispanic / Unknown Race: Asian / Black / Hawaiian / White Primary Policy: Policy Holder
PATIENT REGISTRATION Child :Last Name: First Name: MI: D.O.B.: / / Sex: Primary Language: Ethnicity: Hispanic / Non-Hispanic / Unknown Race: Asian / Black / Hawaiian / White Primary Policy: Policy Holder
Welcome to Our Practice
 Welcome to Our Practice Greater Baltimore Medical Center (GBMC) welcomes you to our practice. We are dedicated to providing you with the kind of care that we would want for our own loved ones. This Information
Welcome to Our Practice Greater Baltimore Medical Center (GBMC) welcomes you to our practice. We are dedicated to providing you with the kind of care that we would want for our own loved ones. This Information
MacInnis Dermatology New Patient Registration Form
 MacInnis Dermatology New Patient Registration Form Please print and answer all questions in full Date Patient Information (please complete using your name as listed on your insurance card) Patient First
MacInnis Dermatology New Patient Registration Form Please print and answer all questions in full Date Patient Information (please complete using your name as listed on your insurance card) Patient First
Patient Registration Forms
 Patient Registration Forms PATIENT INFORMATION First Name: Middle: Last: DOB: / / Sex: M/F Primary Language: Address: City: ST ZIP Ethnicity: Hispanic / Non-Hispanic / Unknown Race: Asian / White / African
Patient Registration Forms PATIENT INFORMATION First Name: Middle: Last: DOB: / / Sex: M/F Primary Language: Address: City: ST ZIP Ethnicity: Hispanic / Non-Hispanic / Unknown Race: Asian / White / African
MEMORIAL AND KATY SURGICAL SPECIALISTS. Patient Information
 Patient Information Patient Name Last First Middle Address City State Zip Birthdate Age Sex M F Social Security# Race (Please circle) American Indian Asian Black Native Hawaiian Pacific Islander White
Patient Information Patient Name Last First Middle Address City State Zip Birthdate Age Sex M F Social Security# Race (Please circle) American Indian Asian Black Native Hawaiian Pacific Islander White
PATIENT MEDICAL RECORD # DATE OF BIRTH / / Male: Female: PATIENT NAME LAST FIRST MI FORMER LAST NAME MAILING ADDRESS CITY STATE ZIP
 PATIENT INFORMATION PATIENT MEDICAL RECORD # DATE OF BIRTH / / Male: Female: PATIENT NAME LAST FIRST MI FORMER LAST NAME MAILING ADDRESS CITY STATE ZIP HOME PHONE ( ) WORK PHONE ( ) CELL PHONE ( ) E-MAIL
PATIENT INFORMATION PATIENT MEDICAL RECORD # DATE OF BIRTH / / Male: Female: PATIENT NAME LAST FIRST MI FORMER LAST NAME MAILING ADDRESS CITY STATE ZIP HOME PHONE ( ) WORK PHONE ( ) CELL PHONE ( ) E-MAIL
PHARMACY INFORMATION
 NAAMAN CLINIC TODAY S DATE: Prefix Mr. Mrs. Miss Ms. Dr. Preferred Name: Patient s Name Address: First Middle Last Street & Apt # City State Zip SS# Birthdate Age: Sex: Female Male Marital Status: Single
NAAMAN CLINIC TODAY S DATE: Prefix Mr. Mrs. Miss Ms. Dr. Preferred Name: Patient s Name Address: First Middle Last Street & Apt # City State Zip SS# Birthdate Age: Sex: Female Male Marital Status: Single
Instructions: All sections must be completed. If not applicable, please indicate as N/A. PATIENT INFORMATION
 817 283 5252, Fax: 817 283 5283 Instructions: All sections must be completed. If not applicable, please indicate as N/A. PATIENT INFORMATION Last Name: First Name: M.I.: MALE FEMALE Home Address: City:
817 283 5252, Fax: 817 283 5283 Instructions: All sections must be completed. If not applicable, please indicate as N/A. PATIENT INFORMATION Last Name: First Name: M.I.: MALE FEMALE Home Address: City:
Patient Registration. All Inclusive Primary Care. PATIENT INFORMATION Name: (Last, First, MI) Address: City: State/Province: Zip: Country:
 Address: City: State/Province: Zip: Country:") Patient Registration PATIENT INFORMATION Name: (Last, First, MI) Address: City: State/Province: Zip: Country: Mailing Address (if different from above): Home Phone: Work: Mobile: Email: SSN: Birth Date:
Patient Registration PATIENT INFORMATION Name: (Last, First, MI) Address: City: State/Province: Zip: Country: Mailing Address (if different from above): Home Phone: Work: Mobile: Email: SSN: Birth Date:
Employer/Doctor Employer s Name Address: Referring Doctor Phone Number Primary Doctor Phone # Patient Information
 FINANCE INSURANCE ORTHOPEDIC SPINE AND SPORTS MEDICINE CENTER 2 FOREST AVEPARAMUS, NJ 07652 PATIENT QUESTIONAIRE Patient s Name: Last First (legal): Middle Initial: Address: City: State: Zip: Date of Birth:
FINANCE INSURANCE ORTHOPEDIC SPINE AND SPORTS MEDICINE CENTER 2 FOREST AVEPARAMUS, NJ 07652 PATIENT QUESTIONAIRE Patient s Name: Last First (legal): Middle Initial: Address: City: State: Zip: Date of Birth:
Please print and complete all the enclosed forms and bring them to your first appointment.
 Dear Valued Patient, Thank you for requesting an appointment in our office. Please print and complete all the enclosed forms and bring them to your first appointment. When you arrive at our office for
Dear Valued Patient, Thank you for requesting an appointment in our office. Please print and complete all the enclosed forms and bring them to your first appointment. When you arrive at our office for
It is very important to bring the following to your first visit:
 Dear New Patient: Welcome and thank you for choosing Capital Digestive Care! The enclosed packet contains important information for your upcoming appointment as well as our new patient registration forms.
Dear New Patient: Welcome and thank you for choosing Capital Digestive Care! The enclosed packet contains important information for your upcoming appointment as well as our new patient registration forms.
Today s Date (mm/dd/yyyy):
:") 115 Christopher Columbus Drive, Suite 301 Jersey City, New Jersey 07302 201-706-3808 http://www.drsmedicalassociates.com/ WELCOME TO DRS MEDICAL ASSOCIATES LLC. PLEASE COMPLETE THE FORM LEGIBLY AND ENTER
115 Christopher Columbus Drive, Suite 301 Jersey City, New Jersey 07302 201-706-3808 http://www.drsmedicalassociates.com/ WELCOME TO DRS MEDICAL ASSOCIATES LLC. PLEASE COMPLETE THE FORM LEGIBLY AND ENTER
Please print and complete all the enclosed forms and bring them to your first appointment.
 Dear Valued Patient, Thank you for requesting an appointment in our office. Please print and complete all the enclosed forms and bring them to your first appointment. When you arrive at our office for
Dear Valued Patient, Thank you for requesting an appointment in our office. Please print and complete all the enclosed forms and bring them to your first appointment. When you arrive at our office for
Patient Registration WELCOME TO OUR OFFICE
 Patient Registration WELCOME TO OUR OFFICE Date of Birth: Home Address: Apt / Unit: City: State: Zip: SSN: Telephone: Home: Cell: Work: Email: Marital Status: Name of Spouse / Partner: Preferred method
Patient Registration WELCOME TO OUR OFFICE Date of Birth: Home Address: Apt / Unit: City: State: Zip: SSN: Telephone: Home: Cell: Work: Email: Marital Status: Name of Spouse / Partner: Preferred method
WOMEN S PREMIER OBGYN REGISTRATION FORM
 WOMEN S PREMIER OBGYN REGISTRATION FORM Today s date: PCP: PATIENT INFORMATION Patient s last name: First: Middle: q Miss q Ms. Marital status (circle one) Single / Married / Divorced / Sep / Widow Is
WOMEN S PREMIER OBGYN REGISTRATION FORM Today s date: PCP: PATIENT INFORMATION Patient s last name: First: Middle: q Miss q Ms. Marital status (circle one) Single / Married / Divorced / Sep / Widow Is
PULMONARY AND CRITICAL CARE SPECIALISTS 160 Kingsley Lane, Suite 103 Norfolk, VA Phone: Fax:
 PATIENT INFORMATION Address: PULMONARY AND CRITICAL CARE SPECIALISTS 160 Kingsley Lane, Suite 103 Norfolk, VA 23505 Phone: 757-889-6677 Fax: 757-889-6652 PLEASE PRINT Today s Date: City: State: Zip: Age:
PATIENT INFORMATION Address: PULMONARY AND CRITICAL CARE SPECIALISTS 160 Kingsley Lane, Suite 103 Norfolk, VA 23505 Phone: 757-889-6677 Fax: 757-889-6652 PLEASE PRINT Today s Date: City: State: Zip: Age:
NOTICE TO OUR PATIENTS
 NOTICE TO OUR PATIENTS Although we participate with most insurance plans, you as the patient and/or insured party are responsible for co-pays, deductibles and any non-covered services, which are outlined,
NOTICE TO OUR PATIENTS Although we participate with most insurance plans, you as the patient and/or insured party are responsible for co-pays, deductibles and any non-covered services, which are outlined,
Patient Name: Last name First Name Middle Initial. Address: Street or Box City State Zip Phone: (Primary) (Cell) (Other) Date of Birth:
 (Cell) (Other) Date of Birth:") PATIENT REGISTRATION FORM Patient Name: Last name First Name Middle Initial Address: Street or Box City State Zip Phone: (Primary) (Cell) (Other) Date of Birth: Email: Gender: o Male o Female SSN# Marital
PATIENT REGISTRATION FORM Patient Name: Last name First Name Middle Initial Address: Street or Box City State Zip Phone: (Primary) (Cell) (Other) Date of Birth: Email: Gender: o Male o Female SSN# Marital
Please complete the first page, as well as read, sign, and date the following pages. Please do not hesitate to ask us any questions.
 Dear Patient, Please complete the first page, as well as read, sign, and date the following pages. Please do not hesitate to ask us any questions. Thank you, Arsenio Medical, P.C. Arsenio Medical, P.C.
Dear Patient, Please complete the first page, as well as read, sign, and date the following pages. Please do not hesitate to ask us any questions. Thank you, Arsenio Medical, P.C. Arsenio Medical, P.C.
Quick Patient Registration Form Patient Information:
 Quick Patient Registration Form Patient Information: Legal First Name: MI: Legal Last Name: Sex: M F Date of Birth: Primary Language: Marital Status: Married Single Partner Divorced Widowed Race: Ethnicity:
Quick Patient Registration Form Patient Information: Legal First Name: MI: Legal Last Name: Sex: M F Date of Birth: Primary Language: Marital Status: Married Single Partner Divorced Widowed Race: Ethnicity:
NEW PATIENT REGISTRATION PACKET
 NEW PATIENT REGISTRATION PACKET Today s Date DOB: Social Security # Last Name: First Name: Previous/Nickname: Sex: Male Female Marital Status: Married Single Divorced Widowed Other Patients Race: American
NEW PATIENT REGISTRATION PACKET Today s Date DOB: Social Security # Last Name: First Name: Previous/Nickname: Sex: Male Female Marital Status: Married Single Divorced Widowed Other Patients Race: American
PATIENT INFORMATION INSURANCE INFORMATION
 PATIENT INFORMATION RECORD (Please Print or Write Legibly) DATE ACCT # PATIENT INFORMATION NAME First Middle Init. Last MAILING ADDRESS CITY STATE ZIP SEX RACE Ethnicity: q hispanic/latino q Not Hispanic/Latino
PATIENT INFORMATION RECORD (Please Print or Write Legibly) DATE ACCT # PATIENT INFORMATION NAME First Middle Init. Last MAILING ADDRESS CITY STATE ZIP SEX RACE Ethnicity: q hispanic/latino q Not Hispanic/Latino
New Wave Internal Medicine Clinic
 Amber D. Colville, M.D. *Lydia Latour, M.D., * Ashleigh Teates NP-C Dear Patient, Thank you for your interest in becoming a new patient at New Wave Internal Medicine. Please fill out the enclosed paperwork
Amber D. Colville, M.D. *Lydia Latour, M.D., * Ashleigh Teates NP-C Dear Patient, Thank you for your interest in becoming a new patient at New Wave Internal Medicine. Please fill out the enclosed paperwork
Patient Registration Form
 Patient Registration Form Patient Information: Patient/Child First Name: MI: Last Name: Age: Date of Birth: Occupation: Ethnicity: Hispanic Not Hispanic Language: English Spanish Other Race: White Black
Patient Registration Form Patient Information: Patient/Child First Name: MI: Last Name: Age: Date of Birth: Occupation: Ethnicity: Hispanic Not Hispanic Language: English Spanish Other Race: White Black
BLAKE FRIEDEN MD, PA Registration Form
 BLAKE FRIEDEN MD, PA Registration Form Name: Today s Date: First Middle Last Home Address: City: State: Zip: Telephone: ( ) Birthdate: Age: Cell Phone: ( ) Social Security Number - - Race/Ethnicity: White
BLAKE FRIEDEN MD, PA Registration Form Name: Today s Date: First Middle Last Home Address: City: State: Zip: Telephone: ( ) Birthdate: Age: Cell Phone: ( ) Social Security Number - - Race/Ethnicity: White
Chief Complaint Form: Patient Name: Age: DOB: Occupation: Employer: Referring Physician: Town: Primary Care Physician: Town: Y N
 Chief Complaint Form: Patient Name: Date: First MI Last Preferred Name Age: DOB: Occupation: Employer: Send Note? Referring Physician: Town: Y N Primary Care Physician: Town: Y N Coach/ Trainer/ Team Doctor:
Chief Complaint Form: Patient Name: Date: First MI Last Preferred Name Age: DOB: Occupation: Employer: Send Note? Referring Physician: Town: Y N Primary Care Physician: Town: Y N Coach/ Trainer/ Team Doctor:
PATIENT REGISTARTION
 PATIENT REGISTARTION Patient Name: Last First MI Address: City: State: Zip Code: Tel # (h): Tel # (w): Cell #: S.S. #: DOB: Age: Email address: Male: Female: Marital Status Spouse or Parent Name Race Preferred
PATIENT REGISTARTION Patient Name: Last First MI Address: City: State: Zip Code: Tel # (h): Tel # (w): Cell #: S.S. #: DOB: Age: Email address: Male: Female: Marital Status Spouse or Parent Name Race Preferred
NAME (LAST, FIRST, MIDDLE) SSN# BIRTHDATE SEX NAME (LAST, FIRST, MIDDLE) SSN# BIRTHDATE SEX
 SSN# BIRTHDATE SEX NAME (LAST, FIRST, MIDDLE) SSN# BIRTHDATE SEX") PATIENT INFORMATION NAME (LAST, FIRST, MIDDLE) SSN# BIRTH SEX ADDRESS CITY, STATE & ZIP CODE EMAIL: MAILING ADDRESS (IF DIFFERENT FROM ADDRESS) CITY, STATE & ZIP CODE HOME PHONE CELL PHONE OTHER PHONE
PATIENT INFORMATION NAME (LAST, FIRST, MIDDLE) SSN# BIRTH SEX ADDRESS CITY, STATE & ZIP CODE EMAIL: MAILING ADDRESS (IF DIFFERENT FROM ADDRESS) CITY, STATE & ZIP CODE HOME PHONE CELL PHONE OTHER PHONE
Welcome to Sibley Primary Care
 Welcome to Sibley Primary Care We are pleased to have you join our practice. We understand that starting with a practice can be overwhelming and we ve provided this welcome packet to aid with your first
Welcome to Sibley Primary Care We are pleased to have you join our practice. We understand that starting with a practice can be overwhelming and we ve provided this welcome packet to aid with your first
WELCOME TO OUR OFFICE. Patient s Name: Today s Date: First Middle Last. Home Address: City: State: Zip: Telephone: Home ( ) Cellular: ( ) Work: ( )
 Cellular: ( ) Work: ( )") WELCOME TO OUR OFFICE Patient s Name: Today s Date: First Middle Last Home Address: City: State: Zip: Telephone: Home ( ) Cellular: ( ) Work: ( ) Email: Personal Work DOB: Age: SSN#: Ethnic Background:
WELCOME TO OUR OFFICE Patient s Name: Today s Date: First Middle Last Home Address: City: State: Zip: Telephone: Home ( ) Cellular: ( ) Work: ( ) Email: Personal Work DOB: Age: SSN#: Ethnic Background:
New Patient Intake and Medical History
 PATIENT INFORMATION New Patient Intake and Medical History Patient Name: Gender: Male Female DOB: Marital Status: Married Divorced Widowed Single Race: White American Indian Asian Black/African American
PATIENT INFORMATION New Patient Intake and Medical History Patient Name: Gender: Male Female DOB: Marital Status: Married Divorced Widowed Single Race: White American Indian Asian Black/African American
Address: City/State: Zip: Billing Address: City/State: Zip: Home Phone: Cell Phone: Appointment reminder: Voice Text - Which #:
 Office Use Only: Date of Intake: Appt date/time: Therapist: Insurance: Full Name: DOB: Sex: M F SSN: Page A-1 of 5 Billing Home Cell Work Email: Appointment reminder: Email Voice Text - Which #: Emergency
Office Use Only: Date of Intake: Appt date/time: Therapist: Insurance: Full Name: DOB: Sex: M F SSN: Page A-1 of 5 Billing Home Cell Work Email: Appointment reminder: Email Voice Text - Which #: Emergency
NORTH ATLANTA UROLOGY ASSOCIATES PC Howard C. Goldberg; M.D. Douglas A. Nyhoff; M.D. Paul L. Rubin; M.D. Jin S. Yeoh M.D.
 PATIENT INFORMATION SHEET First Name: Last Name: Date: Mailing Address: City: State: Zip: Home Number: Cell Number: Work Number: Fax Number: Sex: Male / Female (circle one) Age: Date of Birth: Marital
PATIENT INFORMATION SHEET First Name: Last Name: Date: Mailing Address: City: State: Zip: Home Number: Cell Number: Work Number: Fax Number: Sex: Male / Female (circle one) Age: Date of Birth: Marital
Trinity Family Physicians
 Trinity Family Physicians Consent and Authorization for Minors By law, a healthcare provider must attempt to contact a birth / custodial parent or legal guardian prior to rendering treatment to a minor
Trinity Family Physicians Consent and Authorization for Minors By law, a healthcare provider must attempt to contact a birth / custodial parent or legal guardian prior to rendering treatment to a minor
Patient's Name: Date of Birth:
 AUTHORIZATION TO USE AND/OR DISCLOSE HEALTH INFORMATION Magnolia Pediatrics 2497 Herndon Ave., suite #101, Clovis, CA 93611 Phone: (559) 538-3070 Fax: (559) 538-3071 Patient's Name: Date of Birth: Completion
AUTHORIZATION TO USE AND/OR DISCLOSE HEALTH INFORMATION Magnolia Pediatrics 2497 Herndon Ave., suite #101, Clovis, CA 93611 Phone: (559) 538-3070 Fax: (559) 538-3071 Patient's Name: Date of Birth: Completion
Family Foot and Ankle Centers Patient Registration Form (Please present your insurance cards to the receptionist upon arrival)
") Family Foot and Ankle Centers Patient Registration Form (Please present your insurance cards to the receptionist upon arrival) Patient s Name First Last M.I. Nickname Address # City State Zip code Phone:
Family Foot and Ankle Centers Patient Registration Form (Please present your insurance cards to the receptionist upon arrival) Patient s Name First Last M.I. Nickname Address # City State Zip code Phone:
Welcome to Compass Medical!
 ELECTRONIC FORM DISCLAIMER: Compass Medical is deeply committed to protecting our patient's rights to privacy and safeguarding patient information. Please know we are working hard to bring our patients
ELECTRONIC FORM DISCLAIMER: Compass Medical is deeply committed to protecting our patient's rights to privacy and safeguarding patient information. Please know we are working hard to bring our patients
COASTAL SKIN SURGERY & DERMATOLOGY
 DEMOGRAPHIC INFORMATION Last Name: First: Middle: Date of Birth: Age: Sex: M F Marital Status: SSN: Race: Ethnicity: Hispanic or Latino Not Hispanic or Latino Language: Mailing Address: Street apt/unit#
DEMOGRAPHIC INFORMATION Last Name: First: Middle: Date of Birth: Age: Sex: M F Marital Status: SSN: Race: Ethnicity: Hispanic or Latino Not Hispanic or Latino Language: Mailing Address: Street apt/unit#
New Patient Registration Form. New Patient Update Date: / /
 New Patient Registration Form New Patient Update Date: / / Children s Names Gender Birthdate Race* Ethnicity *Race = White American, Native American, Alaska Native, Asian American, Black or African American,
New Patient Registration Form New Patient Update Date: / / Children s Names Gender Birthdate Race* Ethnicity *Race = White American, Native American, Alaska Native, Asian American, Black or African American,
Minor Registration Forms Please Print Legibly. Demographics. *Patient Last Name: *First Name: Middle Initial:
 *Indicates Required Fields Minor Registration Forms Please Print Legibly Demographics *Patient Last Name: *First Name: Middle Initial: *Date of Birth: / / *Gender: Male Female *Prefix: Mr. Miss Ms. Mrs.
*Indicates Required Fields Minor Registration Forms Please Print Legibly Demographics *Patient Last Name: *First Name: Middle Initial: *Date of Birth: / / *Gender: Male Female *Prefix: Mr. Miss Ms. Mrs.
PATIENT INFORMATION. PRIMARY INSURANCE Ins Co. Name: PRIMARY POLICYHOLDER PARENT/GUARDIAN INFORMATION (REQUIRED IF PATIENT UNDER 18 YEARS OF AGE)
") PATIENT INFORMATION Name: Sex: of Birth: Social Security #: Address: Apt # City: State: Zip: Primary Phone: Primary Phone Type: Cell Home Work Secondary Phone: Secondary Phone Type: Cell Home Work Email:
PATIENT INFORMATION Name: Sex: of Birth: Social Security #: Address: Apt # City: State: Zip: Primary Phone: Primary Phone Type: Cell Home Work Secondary Phone: Secondary Phone Type: Cell Home Work Email:
We are limited, not by our abilities, but by our vision.
 We are limited, not by our abilities, but by our vision. WELCOME Thank you for choosing Advanced Eye Care Center as your eye healthcare provider! On behalf of Dr. Lawrence Shafron, Dr. Rodgers Eckhart,
We are limited, not by our abilities, but by our vision. WELCOME Thank you for choosing Advanced Eye Care Center as your eye healthcare provider! On behalf of Dr. Lawrence Shafron, Dr. Rodgers Eckhart,
Who to call for an emergency: Name: Address: Home Phone: ( ) - Work Phone: ( ) - Cell Phone: ( ) - Relationship:
 - Work Phone: ( ) - Cell Phone: ( ) - Relationship:") Patient Information: Patient Name: Social Security Number: / / Date of Birth: / / Sex: M / F (Circle one) Married/Single/Divorced/Widow Address: Zip Code: Home Phone: ( ) - E-mail Address: Cell Phone:
Patient Information: Patient Name: Social Security Number: / / Date of Birth: / / Sex: M / F (Circle one) Married/Single/Divorced/Widow Address: Zip Code: Home Phone: ( ) - E-mail Address: Cell Phone:
New Patient Registration Form
 New Patient Registration Form PATIENT INFORMATION Last Name (Legal): First Name (Legal): MI: Preferred Name: Date of Birth: Social Security #: Marital Status: Sex Assigned at Birth: Single Married Widowed
New Patient Registration Form PATIENT INFORMATION Last Name (Legal): First Name (Legal): MI: Preferred Name: Date of Birth: Social Security #: Marital Status: Sex Assigned at Birth: Single Married Widowed
PATIENT PROFILE. Marital Status: Please Check One [ ] Single [ ] Married [ ] Divorced [ ] Widowed. Address: City: Zip: Address: City: Zip:
![PATIENT PROFILE. Marital Status: Please Check One [ ] Single [ ] Married [ ] Divorced [ ] Widowed. Address: City: Zip: Address: City: Zip:](/thumbs/82/85694847.jpg "PATIENT PROFILE. Marital Status: Please Check One [ ] Single [ ] Married [ ] Divorced [ ] Widowed. Address: City: Zip: Address: City: Zip:") PATIENT PROFILE PATIENT INFORMATION: Name: Date of Birth: Marital Status: Please Check One [ ] Single [ ] Married [ ] Divorced [ ] Widowed Address: City: Zip: Home#: Message#: Name of Primary Physician,
PATIENT PROFILE PATIENT INFORMATION: Name: Date of Birth: Marital Status: Please Check One [ ] Single [ ] Married [ ] Divorced [ ] Widowed Address: City: Zip: Home#: Message#: Name of Primary Physician,
ADULT PATIENT REGISTRATION
 PATIENT NAME: (LAST) (FIRST) (M) CELL: ( ) HOME: ( ) PERSONAL E-MAIL: (FOR PATIENT PORTAL) DATE OF BIRTH: / / AGE: GENDER: MALE FEMALE SOCIAL SECURITY: - - MARITIAL STATUS: SINGLE MARRIED WIDOW(ER) OTHER
PATIENT NAME: (LAST) (FIRST) (M) CELL: ( ) HOME: ( ) PERSONAL E-MAIL: (FOR PATIENT PORTAL) DATE OF BIRTH: / / AGE: GENDER: MALE FEMALE SOCIAL SECURITY: - - MARITIAL STATUS: SINGLE MARRIED WIDOW(ER) OTHER
WELCOME TO OUR OFFICE PLEASE PRINT THE FOLLOWING INFORMATION THANK YOU
 DATE: / / WELCOME TO OUR OFFICE PLEASE PRINT THE FOLLOWING INFORMATION THANK YOU Richard L. Corbin, DPM, FACFAS PATIENT NAME: LAST FIRST MIDDLE SOCIAL SECURITY NUMBER: / / D.O.B: / / STREET ADDRESS: CITY:
DATE: / / WELCOME TO OUR OFFICE PLEASE PRINT THE FOLLOWING INFORMATION THANK YOU Richard L. Corbin, DPM, FACFAS PATIENT NAME: LAST FIRST MIDDLE SOCIAL SECURITY NUMBER: / / D.O.B: / / STREET ADDRESS: CITY:
Please bring the medications you are currently taking. If you had x- rays made, please bring the films with you when you come to the office.
 Dear Patient: We would like to take this opportunity to thank you for choosing our office for your urologic care and to welcome you to our office. We are pleased that you have chosen us to provide you
Dear Patient: We would like to take this opportunity to thank you for choosing our office for your urologic care and to welcome you to our office. We are pleased that you have chosen us to provide you
Sammy Lerma III, M.D. P.A. History and Physical Name: DOB: Age:
 History and Physical Name: DOB: Age: Reason for Visit : Current Medications: Previous Hospitalizations: Last Physician's Name: Previous Surgeries: Reason for Changing Physicians: Current Specialists: Medication
History and Physical Name: DOB: Age: Reason for Visit : Current Medications: Previous Hospitalizations: Last Physician's Name: Previous Surgeries: Reason for Changing Physicians: Current Specialists: Medication
PATIENT INFORMATION FORM RICHARD L. MALINICK, M.D. ORTHOPAEDIC SURGERY 1125 Via Verde, San Dimas, CA
 Email Address Last Name First Name Previous Name Address City State Zip Country Social Security - - Home Phone - - Cell Phone - - Work Phone - - Ext Drivers License State Responsible Party SELF (use info
Email Address Last Name First Name Previous Name Address City State Zip Country Social Security - - Home Phone - - Cell Phone - - Work Phone - - Ext Drivers License State Responsible Party SELF (use info
Please Present Insurance Card at Each Office Visit
 PATIENT REGISTRATION FORM RONALD J ESCUDERO, MD, FACS Please print clearly and fill out completely Patient Legal Name Birthdate Age Address Social Security # City ST ZIP Email Phone Numbers ( ) Home (
PATIENT REGISTRATION FORM RONALD J ESCUDERO, MD, FACS Please print clearly and fill out completely Patient Legal Name Birthdate Age Address Social Security # City ST ZIP Email Phone Numbers ( ) Home (
If it is not, call your insurance company and have them change the Children s Medical Center to one of Children s Medical Center physicians.
 **This form is for your personal use only and is a tool to help you understand your personal health benefits** Call your insurance company (phone number on the back of your insurance card) and ask them
**This form is for your personal use only and is a tool to help you understand your personal health benefits** Call your insurance company (phone number on the back of your insurance card) and ask them
Christina Agustin, MD Board Certified in Adult Psychiatry 1 Lake Bellevue Drive, Suite 101 Bellevue, WA Phone Fax:
 Christina Agustin, MD Board Certified in Adult Psychiatry 1 Lake Bellevue Drive, Suite 101 Bellevue, WA 98005 Phone 425-301-9869 Fax: 866-546-1618 Welcome to my practice. I look forward to meeting with
Christina Agustin, MD Board Certified in Adult Psychiatry 1 Lake Bellevue Drive, Suite 101 Bellevue, WA 98005 Phone 425-301-9869 Fax: 866-546-1618 Welcome to my practice. I look forward to meeting with
Patient Welcome Form!
 Arthritis and Rheumatology Clinical Center of Northern Virginia, PLLC 8130 Boone Blvd suite 340 Vienna VA 22182 Mahsa Tehrani MD 703-734-2222 Mahnaz Momeni MD Patient Welcome Form Dear new patient, Welcome
Arthritis and Rheumatology Clinical Center of Northern Virginia, PLLC 8130 Boone Blvd suite 340 Vienna VA 22182 Mahsa Tehrani MD 703-734-2222 Mahnaz Momeni MD Patient Welcome Form Dear new patient, Welcome
ADULT PATIENT INFORMATION SHEET ENT & Audiology Center of Southlake 660 W. Southlake Blvd. Suite 100, Southlake TX (817)
") ADULT PATIENT INFORMATION SHEET ENT & Audiology Center of Southlake 660 W. Southlake Blvd. Suite 100, Southlake TX 76092 (817) 416-9731 Date: Patient Name: (Last, First, Middle) DOB: SEX: PATIENT INFORMATION
ADULT PATIENT INFORMATION SHEET ENT & Audiology Center of Southlake 660 W. Southlake Blvd. Suite 100, Southlake TX 76092 (817) 416-9731 Date: Patient Name: (Last, First, Middle) DOB: SEX: PATIENT INFORMATION
West Cary Family Physicians 256 Towne Village Dr Cary, NC
 New Patient Registration Form - page 1 PATIENT INFORMATION Patient s first name: Patient s middle name: Patient s last name: Patient date of birth: Patient sex: Marital status: single married Patient s
New Patient Registration Form - page 1 PATIENT INFORMATION Patient s first name: Patient s middle name: Patient s last name: Patient date of birth: Patient sex: Marital status: single married Patient s
Stonebridge Adult Medicine, P.A. Registration Form (Please Print)
") Stonebridge Adult Medicine, P.A. Registration Form (Please Print) PATIENT INFORMATION Last Name: First Name: Is this your legal name? Yes No If not what is your legal name: Date of Birth: Sex: male female
Stonebridge Adult Medicine, P.A. Registration Form (Please Print) PATIENT INFORMATION Last Name: First Name: Is this your legal name? Yes No If not what is your legal name: Date of Birth: Sex: male female
Statement of Financial Responsibility
 : Patient Intake Form Patient Name: (Last) (First) (M): Cell Phone Home Phone Work Phone Mailing Address: City: State: Zip: Home Address: City: State: Zip: (If Different) Email How did you hear about us?
: Patient Intake Form Patient Name: (Last) (First) (M): Cell Phone Home Phone Work Phone Mailing Address: City: State: Zip: Home Address: City: State: Zip: (If Different) Email How did you hear about us?
Welcome to our Practice
 Welcome to our Practice First, let us thank you for putting your trust in Georgia Eye Partners and our team. Our goal in providing this packet of information is to make the process as easy as possible
Welcome to our Practice First, let us thank you for putting your trust in Georgia Eye Partners and our team. Our goal in providing this packet of information is to make the process as easy as possible
PATIENT DEMOGRAPHICS. Primary Insurance: Policy #: Group #: Secondary Insurance: Policy #: Group #:
 TEXAS DIABETES & ENDOCRINOLOGY, P.A. 6500 North Mopac*Bldg. 3, Ste. 200*Austin, TX 78731 5000 Davis Ln*Ste 200*Austin, TX 78749 170 Deep Wood Dr*Ste. 104*Round Rock, Tx 78681 Phone: (512) 458 8400*Fax:
TEXAS DIABETES & ENDOCRINOLOGY, P.A. 6500 North Mopac*Bldg. 3, Ste. 200*Austin, TX 78731 5000 Davis Ln*Ste 200*Austin, TX 78749 170 Deep Wood Dr*Ste. 104*Round Rock, Tx 78681 Phone: (512) 458 8400*Fax:
NEW PATIENT INFORMATION Salutation First Name MI Last Name Nickname
 NEW PATIENT INFORMATION Salutation First Name MI Last Name Nickname of Birth: Address: SSN: City: State: Zip: Home Phone: Daytime Phone: Mobile Phone: Which number do you prefer we use to contact you?
NEW PATIENT INFORMATION Salutation First Name MI Last Name Nickname of Birth: Address: SSN: City: State: Zip: Home Phone: Daytime Phone: Mobile Phone: Which number do you prefer we use to contact you?
PATIENT INFORMATION DEMOGRAPHICS. First Name Middle Initial Last Name Gender. Mailing address: Apt # City: State: ZIP Code: Home Phone Cell Phone
 PATIENT INFORMATION Gary S. Fields, DPM, FACFAS Kenneth M. Danis, DPM, FACFAS DEMOGRAPHICS First Name Middle Initial Last Name Gender SSN Birthdate Age Email M F Mailing address: Apt # City: State: ZIP
PATIENT INFORMATION Gary S. Fields, DPM, FACFAS Kenneth M. Danis, DPM, FACFAS DEMOGRAPHICS First Name Middle Initial Last Name Gender SSN Birthdate Age Email M F Mailing address: Apt # City: State: ZIP
PATIENT REGISTRATION FORM
 Today s PATIENT REGISTRATION FORM PATIENT INFORMATION Last Name: First: Mi. Init: DOB: Age: SSN: Gen: M F Marital Status: S M D W Race: African American American Indian Asian Caucasian Hispanic Pacific
Today s PATIENT REGISTRATION FORM PATIENT INFORMATION Last Name: First: Mi. Init: DOB: Age: SSN: Gen: M F Marital Status: S M D W Race: African American American Indian Asian Caucasian Hispanic Pacific
CENTRAL OHIO PLASTIC SURGERY, INC. (740)
") (740) 653-5064 Patient s Name Patient Information as of (enter today s date) (Please Print Legibly & Fill In or Correct All Fields) Last First Middle Nickname Address Street & Apt # City State Zip Home
(740) 653-5064 Patient s Name Patient Information as of (enter today s date) (Please Print Legibly & Fill In or Correct All Fields) Last First Middle Nickname Address Street & Apt # City State Zip Home
Billing Address for responsible party (if different from home): Subscriber: DOB: Employer:
: Subscriber: DOB: Employer:") Today s D Today s Date: Parent/Guardian Name: DOB: Cell: Home: Work: Email: Preferred Method of Contact: Parent/Guardian Name: DOB: Cell: Home: Work: Email: Preferred Method of Contact: Patients Home Address:
Today s D Today s Date: Parent/Guardian Name: DOB: Cell: Home: Work: Email: Preferred Method of Contact: Parent/Guardian Name: DOB: Cell: Home: Work: Email: Preferred Method of Contact: Patients Home Address:
Family Clinic 808 W.W. Ray Circle Bridgeport, TX / phone 940/ fax. Financial Policy
 Financial Policy Our staff would like to welcome you to our clinic and thank you for choosing us for your medical care. The following is an explanation of our financial policies. Our clinic is contracted
Financial Policy Our staff would like to welcome you to our clinic and thank you for choosing us for your medical care. The following is an explanation of our financial policies. Our clinic is contracted
PATIENT REGISTRATION FORM CAROLINA EAR, NOSE & THROAT
 PATIENT REGISTRATION FORM CAROLINA EAR, NOSE & THROAT Last Name: First: M.I.: Sex: Age: Date of Birth / / Social Security # - - Race: Ethnicity: Language Spoken: If patient is child / under 18: Parent
PATIENT REGISTRATION FORM CAROLINA EAR, NOSE & THROAT Last Name: First: M.I.: Sex: Age: Date of Birth / / Social Security # - - Race: Ethnicity: Language Spoken: If patient is child / under 18: Parent
Patient's Name: Date of Birth:
 AUTHORIZATION TO USE AND/OR DISCLOSE HEALTH INFORMATION Fresno Children s Pediatrics 7720 N Fresno Street, Ste #104, Fresno, CA 93720 Phone: (559) 438-2300 Fax: (559) 438-1531 Patient's Name: Date of Birth:
AUTHORIZATION TO USE AND/OR DISCLOSE HEALTH INFORMATION Fresno Children s Pediatrics 7720 N Fresno Street, Ste #104, Fresno, CA 93720 Phone: (559) 438-2300 Fax: (559) 438-1531 Patient's Name: Date of Birth:
New Patient Registration Form
 New Patient Registration Form PATIENT INFORMATION Last Name (Legal): First Name (Legal): MI: Preferred Name: Date of Birth: Social Security #: Marital Status: Sex Assigned at Birth: Single Married Widowed
New Patient Registration Form PATIENT INFORMATION Last Name (Legal): First Name (Legal): MI: Preferred Name: Date of Birth: Social Security #: Marital Status: Sex Assigned at Birth: Single Married Widowed
PATIENT APPLICATION FORM
 PATIENT APPLICATION FORM WELCOME TO OUR CLINIC! We specialize in assisting our patients to achieve their highest level of health through our spinal and postural corrective programs. Our approach is very
PATIENT APPLICATION FORM WELCOME TO OUR CLINIC! We specialize in assisting our patients to achieve their highest level of health through our spinal and postural corrective programs. Our approach is very
Our portals are encrypted and password-protected, too, so health data remains secure.
 Patient Portal Education Sheet We know you re busy. That s why Palmetto Health-USC Medical Group s physician practices are offering a way for you to manage your health care online. We offer convenient
Patient Portal Education Sheet We know you re busy. That s why Palmetto Health-USC Medical Group s physician practices are offering a way for you to manage your health care online. We offer convenient
Pediatric & Adolescent Center of NW Houston, PA & Northwest Houston Neurology, PA
 Pediatric & Adolescent Center of NW Houston, PA & Northwest Houston Neurology, PA Poonam Singh, M.D. * Elizabeth Sanchez Fowler, M.D. * Tonya Suffridge, M.D. * Anuradha Venkatachalam, M.D. Balbir Singh,
Pediatric & Adolescent Center of NW Houston, PA & Northwest Houston Neurology, PA Poonam Singh, M.D. * Elizabeth Sanchez Fowler, M.D. * Tonya Suffridge, M.D. * Anuradha Venkatachalam, M.D. Balbir Singh,
Tree House Pediatrics, PLLC
 Tree House Pediatrics, PLLC Office Policies Our goal is to provide and maintain a good physician-patient relationship. Letting you know in advance of our office policies allows for a good flow of communication
Tree House Pediatrics, PLLC Office Policies Our goal is to provide and maintain a good physician-patient relationship. Letting you know in advance of our office policies allows for a good flow of communication
Northtown Podiatry. You will be seeing the following physician. Your appointment is scheduled at the following Location WE DO NOT VALIDATE PARKING
 Northtown Podiatry You have an appointment on @ You will be seeing the following physician Dr. Joseph M. Anain, Jr. Dr. Michael Butler Dr. Daniel Keating Dr. Sean Keating Dr. Jules Bodo Your appointment
Northtown Podiatry You have an appointment on @ You will be seeing the following physician Dr. Joseph M. Anain, Jr. Dr. Michael Butler Dr. Daniel Keating Dr. Sean Keating Dr. Jules Bodo Your appointment
PEDIATRIC PATIENT REGISTRATION GALEN MEDICAL GROUP, PC
 PEDIATRIC PATIENT REGISTRATION GALEN MEDICAL GROUP, PC Your Child: Name Your Child s Full Name: Child Goes By: Gender: Male Female DOB: Age: SS#: Child s Home Address: City: State: Zip: Phone: Primary
PEDIATRIC PATIENT REGISTRATION GALEN MEDICAL GROUP, PC Your Child: Name Your Child s Full Name: Child Goes By: Gender: Male Female DOB: Age: SS#: Child s Home Address: City: State: Zip: Phone: Primary
PATIENT INFORMATION SHEET
 PATIENT INFORMATION SHEET Patient Name: DOB: Address: ADDRESS CITY, STATE, ZIP SSN: Mailing Address: ADDRESS CITY, STATE, ZIP Same as above Home phone: Cell phone: Work phone: Marital Status: Single /
PATIENT INFORMATION SHEET Patient Name: DOB: Address: ADDRESS CITY, STATE, ZIP SSN: Mailing Address: ADDRESS CITY, STATE, ZIP Same as above Home phone: Cell phone: Work phone: Marital Status: Single /
Premier Internal Medicine of Alpharetta, PC FINANCIAL POLICY
 Premier Internal Medicine of Alpharetta, PC FINANCIAL POLICY Thank you for choosing Premier Internal Medicine of Alpharetta, PC for your health care needs. We are committed to building a successful physician-patient
Premier Internal Medicine of Alpharetta, PC FINANCIAL POLICY Thank you for choosing Premier Internal Medicine of Alpharetta, PC for your health care needs. We are committed to building a successful physician-patient
Past Medical History
 Past Medical History Patient Name Age: Sex: M or F Allergies:_ of Birth Current Medicines: If Newborn: Was baby born in a Hospital: Y N If Yes what Hospital: Medical History BIRTH HISTORY (Please list
Past Medical History Patient Name Age: Sex: M or F Allergies:_ of Birth Current Medicines: If Newborn: Was baby born in a Hospital: Y N If Yes what Hospital: Medical History BIRTH HISTORY (Please list
NEW PATIENT INFORMATION
 NEW PATIENT INFORMATION GENERAL PATIENT INFORMATION (Please Print) Patient Name: of Birth: Sex: Male Female Marital Status: Single Married Divorced Other Street Address: Home Phone: City/State: Zip: Cell
NEW PATIENT INFORMATION GENERAL PATIENT INFORMATION (Please Print) Patient Name: of Birth: Sex: Male Female Marital Status: Single Married Divorced Other Street Address: Home Phone: City/State: Zip: Cell
PATIENT REGISTRATION FORM
 Today s Date: PATIENT REGISTRATION FORM PATIENT INFORMATION Last Name: First: Mi. Init: DOB: Age: SSN: Gen: M F Marital Status: S M D W Race: African American American Indian Asian Caucasian Hispanic Pacific
Today s Date: PATIENT REGISTRATION FORM PATIENT INFORMATION Last Name: First: Mi. Init: DOB: Age: SSN: Gen: M F Marital Status: S M D W Race: African American American Indian Asian Caucasian Hispanic Pacific
DILIP TAPADIYA, M.D. INC. Demographic Form
 Demographic Form 1. PATIENT Name Soc Sec No: City: State: Zip: Birthdate: Driver s License No: Sex: Home Phone: ( ) Cell Phone: ( ) Marital Status: Occupation: 2. RESPONSIBLE PARTY Name: Soc Sec No: City:
Demographic Form 1. PATIENT Name Soc Sec No: City: State: Zip: Birthdate: Driver s License No: Sex: Home Phone: ( ) Cell Phone: ( ) Marital Status: Occupation: 2. RESPONSIBLE PARTY Name: Soc Sec No: City:
ADDRESS: APT#: CITY: ZIP: IF ANOTHR PHYSICIAN, WHO?
 PEDIATRIC PATIENT INFORMATION SHEET ENT & AUDIOLOGY CENTER OF SOUTHLAKE PHONE: (817) 416-9731 FAX: (817) 416-9751 PATIENT NAME (LAST, FIRST, MIDDLE) AGE: SEX: ADDRESS: APT#: CITY: ZIP: PATIENT HOME PHONE:
PEDIATRIC PATIENT INFORMATION SHEET ENT & AUDIOLOGY CENTER OF SOUTHLAKE PHONE: (817) 416-9731 FAX: (817) 416-9751 PATIENT NAME (LAST, FIRST, MIDDLE) AGE: SEX: ADDRESS: APT#: CITY: ZIP: PATIENT HOME PHONE:
Local Address: City State Zip. Permanent Address: City State Zip. Secondary Insurance Co: Insurance Phone: Policy #:
 Patient Intake Form : Patient Name: (Last) (First) (M) Local Address: City State Zip Permanent Address: City State Zip Home Phone: Work Phone: Cell Phone: Birthdate: Age: Sex: M F Marital Status: Ethnicity:
Patient Intake Form : Patient Name: (Last) (First) (M) Local Address: City State Zip Permanent Address: City State Zip Home Phone: Work Phone: Cell Phone: Birthdate: Age: Sex: M F Marital Status: Ethnicity:
Glacier Ear, Nose & Throat, Head & Neck Surgery
 Patient Information Glacier Ear, Nose & Throat, Head & Neck Surgery Appt Date: Account #: Patient s SSN: First Name: MI: Last Name: Mailing Address: City: State: Zip: Date of Birth: Age: Sex: Marital Status:
Patient Information Glacier Ear, Nose & Throat, Head & Neck Surgery Appt Date: Account #: Patient s SSN: First Name: MI: Last Name: Mailing Address: City: State: Zip: Date of Birth: Age: Sex: Marital Status:
ADDRESS: APT#: CITY: ZIP: IF ANOTHR PHYSICIAN, WHO?
 ADULT DEPENDENT PATIENT INFORMATION SHEET ENT & AUDIOLOGY CENTER OF SOUTHLAKE PHONE: (817) 416-9731 FAX: (817) 416-9751 PATIENT NAME (LAST, FIRST, MIDDLE) AGE: SEX: ADDRESS: APT#: CITY: ZIP: PATIENT HOME
ADULT DEPENDENT PATIENT INFORMATION SHEET ENT & AUDIOLOGY CENTER OF SOUTHLAKE PHONE: (817) 416-9731 FAX: (817) 416-9751 PATIENT NAME (LAST, FIRST, MIDDLE) AGE: SEX: ADDRESS: APT#: CITY: ZIP: PATIENT HOME
PEDIATRIC REGISTRATION FORM
 PEDIATRIC REGISTRATION FORM **Today s Date: PATIENT INFORMATION: (Please use full legal name, no nicknames) *Last Name: *First Name: Middle Initial: *Address: City: State: Zip: *Sex: *Date of Birth: Age:
PEDIATRIC REGISTRATION FORM **Today s Date: PATIENT INFORMATION: (Please use full legal name, no nicknames) *Last Name: *First Name: Middle Initial: *Address: City: State: Zip: *Sex: *Date of Birth: Age:
Patient Registration. Patient Information. Guarantor Information (skip if same as patient) Emergency Contact Information. Insurance Information
 Emergency Contact Information. Insurance Information") Patient Registration Patient Information Patient name (Last, First) Patient date of birth Patient gender (M / F) Patient marital status Mailing address (address number & street) Patient Social Security
Patient Registration Patient Information Patient name (Last, First) Patient date of birth Patient gender (M / F) Patient marital status Mailing address (address number & street) Patient Social Security
Family address preferred for patient portal access:
 : Patient Relationship to Guarantor: of Birth: Sex: M F Social Security Number: Home Address: City: State: Zip Code: Pharmacy of Choice: Pharmacy Address: Pharmacy Phone Number: Siblings: Name Sex DOB
: Patient Relationship to Guarantor: of Birth: Sex: M F Social Security Number: Home Address: City: State: Zip Code: Pharmacy of Choice: Pharmacy Address: Pharmacy Phone Number: Siblings: Name Sex DOB
Advanced Podiatry. W E A R E V E R Y P L E A S E D T O H A V E Y O U W I T H U S! Please answer the following questions to help us become acquainted.
 W E A R E V E R Y P L E A S E D T O H A V E Y O U W I T H U S! Please answer the following questions to help us become acquainted. Date How did you hear about us? (Be Specific Please) First Name Last Name
W E A R E V E R Y P L E A S E D T O H A V E Y O U W I T H U S! Please answer the following questions to help us become acquainted. Date How did you hear about us? (Be Specific Please) First Name Last Name
PATIENT REGISTRATION (Please Print) Social Security # Address City State Zip. Address
 Social Security # Address City State Zip. Address") PATIENT REGISTRATION (Please Print) Date Name (Last) (First) (MI) Clinician Social Security # Address City State Zip Email Address Home Phone ( ) Mobile/Alt. Phone ( ) Work Phone ( ) PLEASE IDENTIFY WHICH
PATIENT REGISTRATION (Please Print) Date Name (Last) (First) (MI) Clinician Social Security # Address City State Zip Email Address Home Phone ( ) Mobile/Alt. Phone ( ) Work Phone ( ) PLEASE IDENTIFY WHICH
Welcome! Warren Parkway Suite 306 Frisco, TX PlastiksForKids.com. Please remember to bring: New Patient Paperwork
 Welcome! Thank you for choosing Dr. Christine Stiles to care for your child s plastic surgery needs. All appointments are on Monday afternoons. Dr. Stiles operates at the Pediatric Surgery Center. Plastiks
Welcome! Thank you for choosing Dr. Christine Stiles to care for your child s plastic surgery needs. All appointments are on Monday afternoons. Dr. Stiles operates at the Pediatric Surgery Center. Plastiks
FAMILY HISTORY CHILD/CHILDREN S NAME:
 FAMILY HISTORY CHILD/CHILDREN S NAME: FAMILY HISTORY (THINK IN TERMS OF THE CHILD S SIBLINGS, PARENTS, GRANDPARENTS, AUNTS, UNCLES AND FIRST COUSINS): ANY ALLERGIES, HAY FEVER, ASTHMA OR ECZEMA? WHO? ANY
FAMILY HISTORY CHILD/CHILDREN S NAME: FAMILY HISTORY (THINK IN TERMS OF THE CHILD S SIBLINGS, PARENTS, GRANDPARENTS, AUNTS, UNCLES AND FIRST COUSINS): ANY ALLERGIES, HAY FEVER, ASTHMA OR ECZEMA? WHO? ANY
Florida Orthopaedic Associates, P.A.
 Florida Orthopaedic Associates, P.A. PATIENT REGISTRATION Date Patient Name SSN Home Address City, St., Zip Date of Birth Age Male/Female Married/Single Phone Home/Work/Cell Phone Home/Work/Cell Employer
Florida Orthopaedic Associates, P.A. PATIENT REGISTRATION Date Patient Name SSN Home Address City, St., Zip Date of Birth Age Male/Female Married/Single Phone Home/Work/Cell Phone Home/Work/Cell Employer
Kipp M. Robins, MD * Aaron Paxman, PA * Family Audiology TODAY S DATE PATIENT S NAME: BIRTHDATE
 Kipp M. Robins, MD * Aaron Paxman, PA * Family Audiology PATIENT S NAME: TODAY S DATE BIRTHDATE WAS THERE A DOCTOR WHO REFERRED YOU? No Yes If yes, who Who is your Family or Primary care doctor? WHAT are
Kipp M. Robins, MD * Aaron Paxman, PA * Family Audiology PATIENT S NAME: TODAY S DATE BIRTHDATE WAS THERE A DOCTOR WHO REFERRED YOU? No Yes If yes, who Who is your Family or Primary care doctor? WHAT are
NARRA DERMATOLOGY AND AESTHETICS (425) Patient Information as of (enter today s date) (Please Print Legibly & Fill In or Correct All Fields)
 Patient Information as of (enter today s date) (Please Print Legibly & Fill In or Correct All Fields)") NARRA DERMATOLOGY AND AESTHETICS (425) 677-8867 Patient Information as of (enter today s date) (Please Print Legibly & Fill In or Correct All Fields) Patient s Name Address Last First Middle Street & Apt
NARRA DERMATOLOGY AND AESTHETICS (425) 677-8867 Patient Information as of (enter today s date) (Please Print Legibly & Fill In or Correct All Fields) Patient s Name Address Last First Middle Street & Apt