MEMORANDUM. DATE: February 5, Participating Providers. FROM: Network Management Services
|
|
|
- Julianna Blake
- 6 years ago
- Views:
Transcription
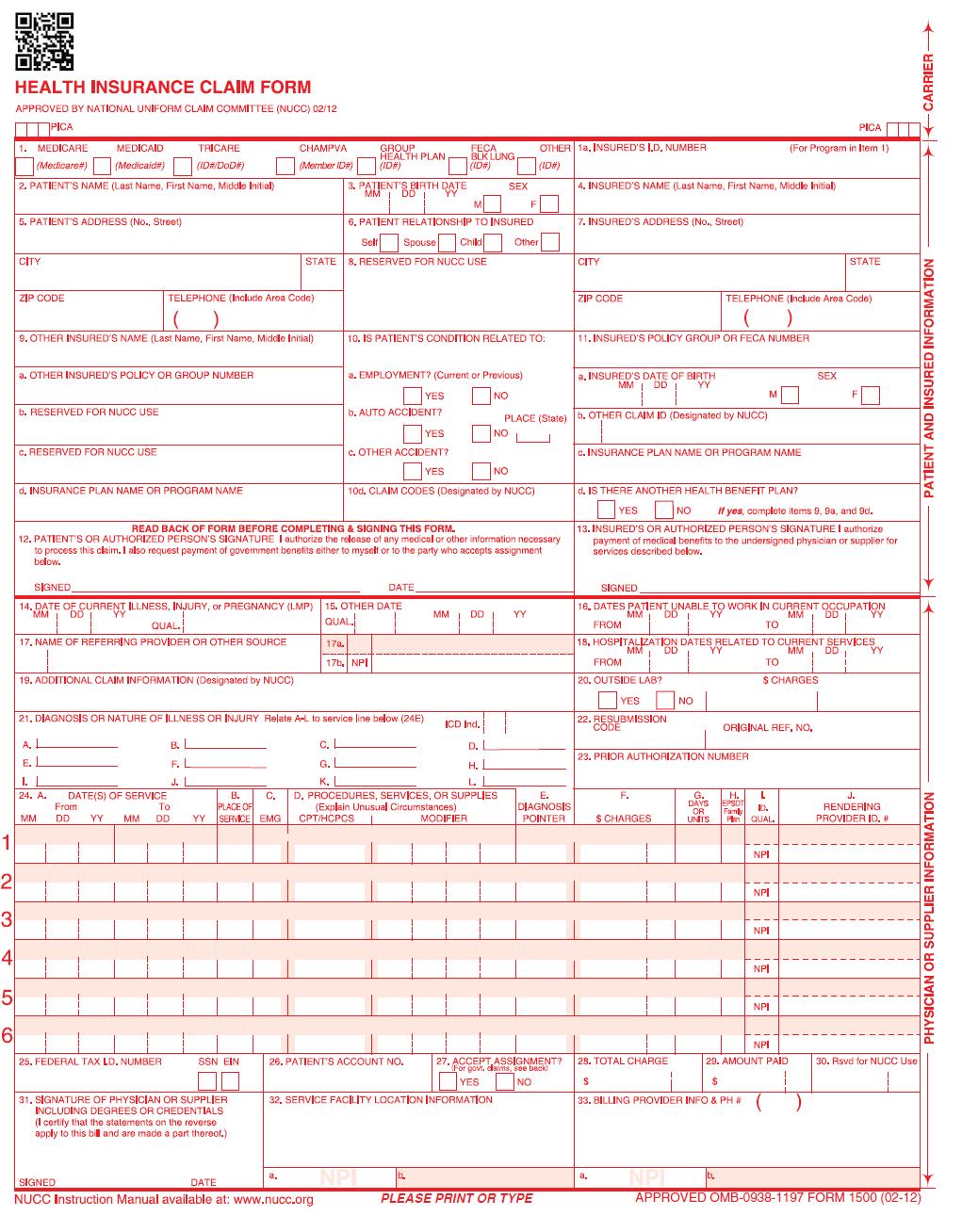
1 MEMORANDUM DATE: February 5, 2014 TO: Participating Providers FROM: Network Management Services RE: CMS 1500 Form Version 02/2012 Mandated as of April 1, 2014 Dear Participating Provider, We are pleased to announce that as of January, 6 th 2014, we may accept the new CMS 1500 Claim Form, Version 02/2012 in preparation for the upcoming transition to ICD-10. This form contains many exciting enhancements from previous versions, which include: Submission of up to 12 diagnosis codes on a single claim form, compared to only 4 on previous versions ICD-10 code friendly, in time for CMS October 1, 2014 deadline We have included to this memo a copy of the new form. For a full list of enhancements, a copy of this memo, and other useful aids, please visit our Provider Portal at and access the Quick Link listed below: New CMS 1500 Form Version 02/2012 Please note that starting April 1, 2014, this form will be a mandatory requirement set by CMS in order to submit paper claims. If you are currently submitting claims to Preferred Care Partners, electronically, please continue to do so. Preferred Care Partners continues to offer electronic claim submissions through Availity, at no additional cost to you. You may register directly at If you have any questions, please contact our Network Management Services Department at (877) You may also any questions to NMS@mypreferredcare.com. Sincerely, Network Management Services Department Doc#: PCP00003_
2 SAMPLE PLEASE PRINT OR TYPE APPROVED OMB FORM 1500 (02-12)
3
4 SAMPLE PLEASE PRINT OR TYPE APPROVED OMB FORM 1500 (02-12)
5 HEALTH INSURANCE CLAIM FORM APPROVED BY NATIONAL UNIFORM CLAIM COMMITTEE (NUCC) 02/12 PICA 1. MEDICARE MEDICAID TRICARE CHAMPVA GROUP FECA OTHER HEALTH PLAN BLK LUNG (Medicare#) (Medicaid#) (ID#/Do D# ) (Mem ber ID#) (ID#) (ID#) (ID#) 2. PATIENT S NAME (Last Name, First Name, Middle Initial) 3. PATIENT S BIRTH DATE SEX MM DD YY M 5. PATIENT S ADDRESS (No., Street) 6. PATIENT RELATIONSHIP TO INSURED CITY ZIP CODE TELEPHONE (Include Area Code) ( ) STATE Self Spouse Child Other 8. RESERVED FOR NUCC USE 9. OTHER INSURED S NAME (Last Name, First Name, Middle Initial) 10. IS PATIENT S CONDITION RELATED TO: a. OTHER INSURED S POLICY OR GROUP NUMBER a. EMPLOYMENT? (Current or Previous) b. RESERVED FOR NUCC USE b. AUTO ACCIDENT? c. RESERVED FOR NUCC USE c. OTHER ACCIDENT? YES NO YES NO YES NO d. INSURANCE PLAN NAME OR PROGRAM NAME 10d. CLAIM CODES (Designated by NUCC) F PLACE (State) READ BACK OF FORM BEFORE COMPLETING & SIGNING THIS FORM. 12. PATIENT S OR AUTHORIZED PERSON S SIGNATURE I authorize the release of any medical or other information necessary to process this claim. I also request payment of government benefits either to myself or to the party who accepts assignment below. PICA 1a. INSURED S I.D. NUMBER (For Program in Item 1) 4. INSURED S NAME (Last Name, First Name, Middle Initial) 7. INSURED S ADDRESS (No., Street) CITY STATE ZIP CODE TELEPHONE (Include Area Code) ( ) 11. INSURED S POLICY GROUP OR FECA NUMBER a. INSURED S DATE OF BIRTH SEX MM DD YY M F b. OTHER CLAIM ID (Designated by NUCC) c. INSURANCE PLAN NAME OR PROGRAM NAME d. IS THERE ANOTHER HEALTH BENEFIT PLAN? YES NO If yes, complete items 9, 9a and 9d. 13. INSURED S OR AUTHORIZED PERSON S SIGNATURE I authorize payment of medical benefits to the undersigned physician or supplier for services described below. PATIENT AND INSURED INFORMATION CARRIER SIGNED 14. DATE OF CURRENT ILLNESS, INJURY or PREGNANCY (LMP) MM DD YY QUAL. DATE 15. OTHER DATE QUAL. 17. NAME OF REFERRING PROVIDER OR OTHER SOURCE 17a. 19. ADDITIONAL CLAIM INFORMATION (Designated by NUCC) 17b. NPI MM DD YY SIGNED 16. DATES PATIENT UNABLE TO WORK IN CURRENT OCCUPATION MM DD YY MM DD YY FROM TO 18. HOSPITALIZATION DATES RELATED TO CURRENT SERVICES MM DD YY MM DD YY FROM TO 20. OUTSIDE LAB? $ CHARGES DIAGNOSIS OR NATURE OF ILLNESS OR INJURY Relate A-L to service line below (24E) ICD Ind. A. B. C. D. E. F. G. H. I. J. K. L. 24. A. DATE(S) OF SERVICE B. C. D. PROCEDURES, SERVICES, OR SUPPLIES E. From To PLACE OF (Explain Unusual Circumstances) DIAGNOSIS MM DD YY MM DD YY SERVICE EMG CPT/HCPCS MODIFIER POINTER 25. FEDERAL TAX I.D. NUMBER SSN EIN 26. PATIENT S ACCOUNT NO. 27. ACCEPT ASSIGNMENT? (For govt. claims, see back) YES NO 31. SIGNATURE OF PHYSICIAN OR SUPPLIER 32. SERVICE FACILITY LOCATION INFORMATION INCLUDING DEGREES OR CREDENTIALS (I certify that the statements on the reverse apply to this bill and are made a part thereof.) YES NO 22. RESUBMISSION CODE ORIGINAL REF. NO. 23. PRIOR AUTHORIZATION NUMBER F. G. H. I. J. DAYS EPSDT Family ID. RENDERING OR $ CHARGES UNITS Plan QUAL. PROVIDER ID. # 28. TOTAL CHARGE 29. AMOUNT PAID 30. Rsvd for NUCC Use $ $ NPI NPI NPI NPI NPI NPI 33. BILLING PROVIDER INFO & PH # ( ) PHYSICIAN OR SUPPLIER INFORMATION NPI a. b. SIGNED DATE NUCC Instruction Manual available at: PLEASE PRINT OR TYPE a. b. NPI APPROVED OMB FORM 1500 (02-12)
6 The 02/ Claim Form: Understanding the Changes to the Form
7 Common Myth The 1500 claim form (AKA HCFA 1500 or CMS 1500) is developed by the federal government. False. The 1500 claim form is developed and maintained by the NUCC. The form is in the public domain. The form is used by federal payer programs, e.g., Medicare, TRICARE, Black Lung, etc.
8 National Uniform Claim Committee The NUCC was formed in 1995 taking over for the Uniform Claim Form Task Force that initially developed the standard professional claim form NUCC assumed responsibility for the development and maintenance of the 1500 claim form Its members represent a broad base of payers, providers, standards developers, data content committees, public health organizations, and vendors The AMA is the Secretariat of the NUCC NUCC s Web site:
9 1500 Claim Form Revision Work Goal: Align the 1500 with changes in the P and accommodate ICD-10 reporting needs Work started in 2009 Reviewed existing data and needs for new Held a public comment period in October 2009 Defined the scope of the work to not change the existing look of the form or underlying layout Made changes and mock-up of the form Held a public comment period in June 2011 on proposed changes Completed final draft of form
10 1500 Claim Form Approval Updated form approved by NUCC in February 2012 (version 02/12) NUCC submitted updated form to CMS for approval CMS held a public comment period June 2012 OMB held a public comment period October 2012 NUCC received word of final approval in June 2013
11
12 Form Changes Header Replaced 1500 rectangular symbol with black and white two-dimensional QR Code (Quick Response Code) Changed symbol to give visual difference for 02/12 form Changed 08/05 to 02/12
13 Form Changes 1 Changed TRICARE CHAMPUS to TRICARE Replaced SSN with ID#
14 Form Changes 8 Deleted PATIENT STATUS and content of field PATIENT STATUS is not reported in 837P so not needed on the 1500 Changed title to RESERVED FOR NUCC USE
15 Form Changes 9b Deleted OTHER INSURED S DATE OF BIRTH, SEX OTHER INSURED S DATE OF BIRTH, SEX is not reported in 837P so not needed on the 1500 Changed title to RESERVED FOR NUCC USE
16 Form Changes 9c Deleted EMPLOYER S NAME OR SCHOOL EMPLOYER S NAME OR SCHOOL not reported in 837P so not needed on 1500 Changed title to RESERVED FOR NUCC USE
17 Form Changes 10d Changed title from RESERVED FOR LOCAL USE to CLAIM CODES (Designated by NUCC) Title changed to reflect usage of field
18 Form Changes 11b Deleted EMPLOYER S NAME OR SCHOOL EMPLOYER S NAME OR SCHOOL not reported in 837P so not needed on 1500 Changed title to OTHER CLAIM ID (Designated by NUCC) Added dotted line in the left-hand side of the field to accommodate a 2-byte qualifier Valid qualifiers are provided in the 02/12 Instruction Manual
19 Form Changes 14 Changed title to DATE OF CURRENT ILLNESS, INJURY, or PREGNANCY (LMP) Removed the arrow and text in the right-hand side of the field Added QUAL. with a dotted line to accommodate a 3 byte qualifier Valid qualifiers are provided in the 02/12 Instruction Manual
20 Form Changes 15 Changed title from IF PATIENT HAS HAD SAME OR SIMILAR ILLNESS. GIVE FIRST DATE to OTHER DATE Added QUAL. with two dotted lines to accommodate a 3-byte qualifier Valid qualifiers are provided in the 02/12 Instruction Manual
21 Form Changes 17 Added a dotted line in the left-hand side of the field to accommodate a 2-byte qualifier Valid qualifiers are provided in the 02/12 Instruction Manual
22 Form Changes 19 Changed title from RESERVED FOR LOCAL USE to ADDITIONAL CLAIM INFORMATION (Designated by NUCC) Title changed to reflect usage of field
23 Form Changes 21 Added ICD Ind. and two dotted lines to accommodate a 1-byte indicator Indicators provided in the 02/12 Instruction Manual Added 8 additional lines for diagnosis codes Changed labels of the diagnosis code lines to alpha characters (A L) Removed the period within the diagnosis code lines
24 Form Changes 22 Changed title from MEDICAID RESUBMISSION to RESUBMISSION. Title changed to reflect usage of field
25 Form Changes 30 Deleted BALANCE DUE. Changed title to Rsvd for NUCC Use. BALANCE DUE is not reported in 837P so not needed on 1500
26 Transitioning to the Updated Form The NUCC approved the following transition timeline: January 6, 2014: Payers begin receiving and processing paper claims submitted on the revised 1500 Claim Form (version 02/12). January 6 through March 31, 2014: Dual use period during which payers continue to receive and process paper claims submitted on the old 1500 Claim Form (version 08/05). April 1, 2014: Payers receive and process paper claims submitted only on the revised 1500 Claim Form (version 02/12). This timeline aligns with Medicare's transition timeline.
27 What Users of the 1500 Need to Do Talk to your practice management system vendor about upgrades to your system for the form Use up your stock of 08/05 forms Order 02/12 forms Talk to your current forms vendor Look at any payer-specific instructions you receive
28 NUCC Resources Materials located under the 1500 Claim Form tab: NUCC Website: Materials under the 1500 Claim Form tab on the 02/ Claim Form page The following resources are available: Sample 02/ Claim Form Change log of differences between the 08/05 and the 02/12 version NUCC instruction manual and change log 02/ Claim Form Map to the ASC X12 837P Frequently Asked Questions
You must write REHAB at the top center of the claim form!
 CMS 1500 (02/12 INSTRUCTIONS FOR REHABILITATION CENTER SERVICES You must write REHAB at the top center of the claim form! Locator # Description Instructions Alerts 1 Medicare / Medicaid / Tricare Champus
CMS 1500 (02/12 INSTRUCTIONS FOR REHABILITATION CENTER SERVICES You must write REHAB at the top center of the claim form! Locator # Description Instructions Alerts 1 Medicare / Medicaid / Tricare Champus
6.5.3 CMS-1500 Blank Paper Claim Form
 6.5.3 CMS-1500 Blank Paper Claim Form 1500 HEALTH INSURANCE CLAIM FORM APPROVED BY NATIONAL UNIFORM CLAIM COMMITTEE 08/05 PICA PICA CARRIER 1. MEDICARE MEDICAID TRICARE CHAMPVA GROUP FECA OTHER 1a. INSURED
6.5.3 CMS-1500 Blank Paper Claim Form 1500 HEALTH INSURANCE CLAIM FORM APPROVED BY NATIONAL UNIFORM CLAIM COMMITTEE 08/05 PICA PICA CARRIER 1. MEDICARE MEDICAID TRICARE CHAMPVA GROUP FECA OTHER 1a. INSURED
You must write DME at the top center of the claim form!
 CMS 1500 (02/12) INSTRUCTIONS FOR DME SERVICES You must write DME at the top center of the claim form! Field/Item # Description Instructions Alerts 1 Medicare / Medicaid / Tricare / ChampVA / Group Health
CMS 1500 (02/12) INSTRUCTIONS FOR DME SERVICES You must write DME at the top center of the claim form! Field/Item # Description Instructions Alerts 1 Medicare / Medicaid / Tricare / ChampVA / Group Health
CMS 1500 (02/12) INSTRUCTIONS FOR RHC/FQHC SERVICES
 INSTRUCTIONS FOR RHC/FQHC SERVICES") CMS 1500 (02/12) INSTRUCTIONS FOR RHC/FQHC SERVICES Locator # Description Instructions Alerts 1 Medicare / Medicaid / Tricare Champus / Champva / Group Health Plan / Feca Blk Lung Required -- Enter an
CMS 1500 (02/12) INSTRUCTIONS FOR RHC/FQHC SERVICES Locator # Description Instructions Alerts 1 Medicare / Medicaid / Tricare Champus / Champva / Group Health Plan / Feca Blk Lung Required -- Enter an
CMS-1500 (02/12) BILLING INSTRUCTIONS FOR APPLIED BEHAVIORAL ANALYSIS
 BILLING INSTRUCTIONS FOR APPLIED BEHAVIORAL ANALYSIS") CMS-1500 (02/12) BILLING INSTRUCTIONS FOR APPLIED BEHAVIORAL ANALYSIS Locator # Description Instructions Alerts 1 Medicare / Medicaid / Tricare Champus / Champva / Group Health Plan / Feca Blk Lung 1a
CMS-1500 (02/12) BILLING INSTRUCTIONS FOR APPLIED BEHAVIORAL ANALYSIS Locator # Description Instructions Alerts 1 Medicare / Medicaid / Tricare Champus / Champva / Group Health Plan / Feca Blk Lung 1a
DME Providers ACA Requirements for Ordering Providers
 DME Providers ACA Requirements for Ordering Providers On February 28, 2017 an RA message was published to address the ACA requirement that DME (Durable Medical Equipment) providers include the ordering
DME Providers ACA Requirements for Ordering Providers On February 28, 2017 an RA message was published to address the ACA requirement that DME (Durable Medical Equipment) providers include the ordering
Completing the CMS-1500 Claim Form
 Completing the CMS-1500 Claim Form Below are instructions for filling out a CMS-1500 Claim Form (version 08/05) when submitting a claim to CareFlorida. Each field on the form is described, and all required
Completing the CMS-1500 Claim Form Below are instructions for filling out a CMS-1500 Claim Form (version 08/05) when submitting a claim to CareFlorida. Each field on the form is described, and all required
Form DFS-F5-DWC-9 B. Completion Instructions
 Completion Instructions Submitted by Ambulatory Surgical Centers A. Header Information Health Care Providers shall enter Insurer/Carrier name, address and zip code in the blank area on top-right side of
Completion Instructions Submitted by Ambulatory Surgical Centers A. Header Information Health Care Providers shall enter Insurer/Carrier name, address and zip code in the blank area on top-right side of
LTSS BILLING GUIDELINES
 LTSS BILLING GUIDELINES 2016 Cigna-HealthSpring STAR+PLUS Provider Services Department: 1-877-653-0331 Website: StarPlus.CignaHealthSpring.com Provider portal: StarPlus.HsConnectOnline.com MCDTX_16_43293
LTSS BILLING GUIDELINES 2016 Cigna-HealthSpring STAR+PLUS Provider Services Department: 1-877-653-0331 Website: StarPlus.CignaHealthSpring.com Provider portal: StarPlus.HsConnectOnline.com MCDTX_16_43293
LOUISIANA MEDICAID PROGRAM ISSUED: 05/11/16 REPLACED: 09/28/15 CHAPTER 7: COMMUNITY CHOICES WAIVER APPENDIX D: CLAIMS FILING PAGE(S) 14 CLAIMS FILING
 14 CLAIMS FILING") CLAIMS FILING Hard copy billing of waiver services are billed on the paper CMS-1500 (02/12) claim form or electronically on the 837P Professional transaction. Effective for dates of service on or after
CLAIMS FILING Hard copy billing of waiver services are billed on the paper CMS-1500 (02/12) claim form or electronically on the 837P Professional transaction. Effective for dates of service on or after
LOUISIANA MEDICAID PROGRAM ISSUED: 02/04/15 REPLACED: 04/30/14 CHAPTER 18: DURABLE MEDICAL EQUIPMENT APPENDIX B CLAIMS FILING PAGE(S) 13 CLAIMS FILING
 13 CLAIMS FILING") CLAIMS FILING Hard copy billing of DME services are billed on the paper CMS-1500 (02/12) claim form or electronically on the 837P Professional transaction. Instructions in this appendix are for completing
CLAIMS FILING Hard copy billing of DME services are billed on the paper CMS-1500 (02/12) claim form or electronically on the 837P Professional transaction. Instructions in this appendix are for completing
CMS 1500 Claim Filing Instructions. 1 Not Required Type of health insurance coverage applicable to claim. Patient s type of coverage.
 Field Locator Requirements CMS 1500 Claim Filing Instructions Field Description 1 Not Required Type of health insurance coverage to claim Patient s type of coverage. 1a Required Insured s ID Number Identification
Field Locator Requirements CMS 1500 Claim Filing Instructions Field Description 1 Not Required Type of health insurance coverage to claim Patient s type of coverage. 1a Required Insured s ID Number Identification
Professional Providers ACA Requirements for Ordering Providers
 Professional Providers ACA Requirements for Ordering Providers On February 28, 2017 an RA message was published to address the ACA requirement that professional services providers include the ordering
Professional Providers ACA Requirements for Ordering Providers On February 28, 2017 an RA message was published to address the ACA requirement that professional services providers include the ordering
Crossover claims should be submitted to Molina Medicaid Solutions, P.O. Box 91020, Baton Rouge, LA
 Dear Provider, Thank you for your participation in the Louisiana Medicaid Program. Payment may be made to your provider type for recipients who also have Medicare coverage. For these recipients, Louisiana
Dear Provider, Thank you for your participation in the Louisiana Medicaid Program. Payment may be made to your provider type for recipients who also have Medicare coverage. For these recipients, Louisiana
National Uniform Claim Committee
 National Uniform Claim Committee 1500 Claim Form Map to the X12 837 Health Care Claim: Professional November 2008 The 1500 Claim Form Map to the X12 837 Health Care Claim: Professional includes data elements,
National Uniform Claim Committee 1500 Claim Form Map to the X12 837 Health Care Claim: Professional November 2008 The 1500 Claim Form Map to the X12 837 Health Care Claim: Professional includes data elements,
LTSS BILLING GUIDELINES
 LTSS BILLING GUIDELINES 2017 Cigna-HealthSpring Provider Services Department: 1-877-653-0331 STAR+PLUS Website: StarPlus.CignaHealthSpring.com TX MMP Website: Cigna.com/medicare/healthcare-professionals/tx-mmp
LTSS BILLING GUIDELINES 2017 Cigna-HealthSpring Provider Services Department: 1-877-653-0331 STAR+PLUS Website: StarPlus.CignaHealthSpring.com TX MMP Website: Cigna.com/medicare/healthcare-professionals/tx-mmp
Revised CMS-1500 Claim Form for Professional and General Services
 Revised CMS-1500 Claim Form for Professional and General Services The Form CMS-1500 (08-05) will be accepted by Louisiana Medicaid for all dates of submission beginning March 5, 2007, but will not be mandated
Revised CMS-1500 Claim Form for Professional and General Services The Form CMS-1500 (08-05) will be accepted by Louisiana Medicaid for all dates of submission beginning March 5, 2007, but will not be mandated
National Uniform Claim Committee
 National Uniform Claim Committee 02/12 1500 Claim Form Map to the X12 Health Care Claim: Professional (837) August 2018 The 1500 Claim Form Map to the X12 Health Care Claim: Professional (837) includes
National Uniform Claim Committee 02/12 1500 Claim Form Map to the X12 Health Care Claim: Professional (837) August 2018 The 1500 Claim Form Map to the X12 Health Care Claim: Professional (837) includes
LOUISIANA MEDICAID PROGRAM ISSUED: 04/01/16 REPLACED: 09/28/15 CHAPTER 9: ADULT DAY HEALTH CARE WAIVER APPENDIX E CLAIMS FILING PAGE(S) 12
 12") CLAIMS FILING Hard copy billing of waiver services are billed on the paper CMS-1500 (02/12) claim form or electronically on the 837P Professional transaction. Instructions in this appendix are for completing
CLAIMS FILING Hard copy billing of waiver services are billed on the paper CMS-1500 (02/12) claim form or electronically on the 837P Professional transaction. Instructions in this appendix are for completing
How to Bill for a School-Based Clinic
 How to Bill for a School-Based Clinic MDwise.org MDwise is a Hoosier Healthwise/HIP Plan Table of Contents Introduction... 3 The Importance of School-Based Clinics... 3 Covered Services... 4 Sick Visits...
How to Bill for a School-Based Clinic MDwise.org MDwise is a Hoosier Healthwise/HIP Plan Table of Contents Introduction... 3 The Importance of School-Based Clinics... 3 Covered Services... 4 Sick Visits...
National Uniform Claim Committee
 National Uniform Claim Committee 1500 Health Insurance Claim Form Reference Instruction Manual for 08/05 Version Disclaimer and Notices 2005 American Medical Association This document is published in cooperation
National Uniform Claim Committee 1500 Health Insurance Claim Form Reference Instruction Manual for 08/05 Version Disclaimer and Notices 2005 American Medical Association This document is published in cooperation
Blue Cross & Blue Shield of Rhode Island CMS-1500 (02/12) Form Completion Informational Guide
 Form Completion Informational Guide") Blue Cross & Blue Shield of Rhode Island CMS-1500 (02/12) Form Completion Informational Guide All professional provider services filed to Blue Cross & Blue Shield of Rhode Island (BCBSRI) must be filed
Blue Cross & Blue Shield of Rhode Island CMS-1500 (02/12) Form Completion Informational Guide All professional provider services filed to Blue Cross & Blue Shield of Rhode Island (BCBSRI) must be filed
Claim Form Billing Instructions CMS-1500 (08-05) Claim Form
 Claim Form") Claim Form Billing Instructions CMS-1500 (08-05) Claim Form Presbyterian Health Plan / Presbyterian Insurance Company, Inc Original: 06/24/07 Page 1 of 10 Presbyterian Health Plan / Presbyterian Insurance
Claim Form Billing Instructions CMS-1500 (08-05) Claim Form Presbyterian Health Plan / Presbyterian Insurance Company, Inc Original: 06/24/07 Page 1 of 10 Presbyterian Health Plan / Presbyterian Insurance
National Uniform Claim Committee
 National Uniform Claim Committee 1500 Health Insurance Claim Form Reference Instruction Manual for 08/05 Version Disclaimer and Notices 2005 American Medical Association This document is published in cooperation
National Uniform Claim Committee 1500 Health Insurance Claim Form Reference Instruction Manual for 08/05 Version Disclaimer and Notices 2005 American Medical Association This document is published in cooperation
Form DFS-F5-DWC-9 B. Completion Instructions. Submitted by Licensed Health Care Providers
 Form DFS-F5-DWC-9 B Completion Instructions Submitted by Licensed Health Care Providers A. Header Information Health Care Providers shall enter Insurer/Carrier name, address and zip code in the blank area
Form DFS-F5-DWC-9 B Completion Instructions Submitted by Licensed Health Care Providers A. Header Information Health Care Providers shall enter Insurer/Carrier name, address and zip code in the blank area
DEPARTMENT OF FINANCIAL SERVICES DIVISION OF WORKERS COMPENSATION
 DEPARTMENT OF FINANCIAL SERVICES DIVISION OF WORKERS COMPENSATION FORM DFS-F5-DWC-9-B. 1. TYPE OF CLAIM T 1a. INSURED S ID NUMBER Enter the Social Security Number or the Division-Assigned Number of the
DEPARTMENT OF FINANCIAL SERVICES DIVISION OF WORKERS COMPENSATION FORM DFS-F5-DWC-9-B. 1. TYPE OF CLAIM T 1a. INSURED S ID NUMBER Enter the Social Security Number or the Division-Assigned Number of the
INSTRUCTIONS FOR BILLING MEDICARE CROSSOVER SERVICES CMS-1500 (02/15) INSTRUCTIONS
 INSTRUCTIONS") INSTRUCTIONS FOR BILLING MEDICARE CROSSOVER SERVICES CMS-1500 (02/15) INSTRUCTIONS OVERVIEW OF MEDICARE CROSSOVER BILLING Professional services are billed on the CMS-1500 (02/12) claim form. A sample copy
INSTRUCTIONS FOR BILLING MEDICARE CROSSOVER SERVICES CMS-1500 (02/15) INSTRUCTIONS OVERVIEW OF MEDICARE CROSSOVER BILLING Professional services are billed on the CMS-1500 (02/12) claim form. A sample copy
C H A P T E R 8 : Billing on the CMS 1500 Claim Form
 C H A P T E R 8 : Billing on the CMS 1500 Claim Form Reviewed/Revised: 1/1/19, 10/1/2018 8.1 INTRODUCTION The CMS 1500 claim form is used to bill for non-facility services, including professional services,
C H A P T E R 8 : Billing on the CMS 1500 Claim Form Reviewed/Revised: 1/1/19, 10/1/2018 8.1 INTRODUCTION The CMS 1500 claim form is used to bill for non-facility services, including professional services,
LOUISIANA MEDICAID PROGRAM ISSUED: 07/01/13 REPLACED: CHAPTER 7: COMMUNITY CHOICES WAIVER APPENDIX D: CLAIMS FILING PAGE(S) 18 CLAIMS FILING
 18 CLAIMS FILING") CLAIMS FILING Community Choices Waiver services (except ADHC) must be filed by electronic claims submission 837P or on the CMS 1500 claim form. Claims for Adult Day Health Care Services must be filed by
CLAIMS FILING Community Choices Waiver services (except ADHC) must be filed by electronic claims submission 837P or on the CMS 1500 claim form. Claims for Adult Day Health Care Services must be filed by
DEPARTMENT OF FINANCIAL SERVICES DIVISION OF WORKERS COMPENSATION
 DEPARTMENT OF FINANCIAL SERVICES DIVISION OF WORKERS COMPENSATION FORM DFS-F5-DWC-9-A SHALL COMPLETE THE DWC-9 ACCORDING TO. 1. TYPE OF CLAIM T 1a. INSURED S I.D. NUMBER Enter the Social Security Number
DEPARTMENT OF FINANCIAL SERVICES DIVISION OF WORKERS COMPENSATION FORM DFS-F5-DWC-9-A SHALL COMPLETE THE DWC-9 ACCORDING TO. 1. TYPE OF CLAIM T 1a. INSURED S I.D. NUMBER Enter the Social Security Number
DEPARTMENT OF FINANCIAL SERVICES DIVISION OF WORKERS COMPENSATION
 DEPARTMENT OF FINANCIAL SERVICES DIVISION OF WORKERS COMPENSATION FORM DFS-F5-DWC-9-A SHALL COMPLETE THE DWC-9 ACCORDING TO. NAME STATUS COMMENTS SUBJECT TO 1. TYPE OF CLAIM T 1a. INSURED S I.D. NUMBER
DEPARTMENT OF FINANCIAL SERVICES DIVISION OF WORKERS COMPENSATION FORM DFS-F5-DWC-9-A SHALL COMPLETE THE DWC-9 ACCORDING TO. NAME STATUS COMMENTS SUBJECT TO 1. TYPE OF CLAIM T 1a. INSURED S I.D. NUMBER
Claim Form Billing Instructions: CMS-1500 Claim Form
 Claim Form Billing Instructions: CMS-1500 Claim Form Item Required Field? Description and Instructions number N/A Situational When submitting a Medicare Replacement Plan claim, write or stamp Medicare
Claim Form Billing Instructions: CMS-1500 Claim Form Item Required Field? Description and Instructions number N/A Situational When submitting a Medicare Replacement Plan claim, write or stamp Medicare
Chapter 5: Billing on the CMS 1500 Claim Form
 Chapter 5: Billing on the CMS 1500 Claim Form Introduction The CMS 1500 claim form is used to bill for non facility services, including professional services, freestanding surgery centers, transportation,
Chapter 5: Billing on the CMS 1500 Claim Form Introduction The CMS 1500 claim form is used to bill for non facility services, including professional services, freestanding surgery centers, transportation,
CMS-1500 Paper Claim Form Crosswalk to EMC Loops and Segments
 CMS-1500 Paper Claim Form Crosswalk to EMC Loops and Segments Claims submitted to NAS for payment are submitted in two different formats: paper (CMS-1500 Claim Form) and electronic: (ANSI 410A1) electronic
CMS-1500 Paper Claim Form Crosswalk to EMC Loops and Segments Claims submitted to NAS for payment are submitted in two different formats: paper (CMS-1500 Claim Form) and electronic: (ANSI 410A1) electronic
Claim Form Billing Instructions CMS 1500 Claim Form
 Claim Form Billing Instructions CMS 1500 Claim Form Item Required Field? Description and Instructions. 1 Optional Indicate the type of health insurance for which the claim is being submitted. 1a Required
Claim Form Billing Instructions CMS 1500 Claim Form Item Required Field? Description and Instructions. 1 Optional Indicate the type of health insurance for which the claim is being submitted. 1a Required
HCFA Mapping to BCBSNC Local Proprietary Format (LPF) and the HIPAA 837-Professional Implementation Guide
 and the HIPAA 837-Professional Implementation Guide") HCFA Mapping to BCBSNC Local Proprietary at (LPF) n/a Header and Trailer - Header & Footers information will be in the ISA/IEA, GS/GE & THE ST/SE HDR 1-3 TRL1-3 1 Leave blank n/a n/a 1a Insured s ID Enter
HCFA Mapping to BCBSNC Local Proprietary at (LPF) n/a Header and Trailer - Header & Footers information will be in the ISA/IEA, GS/GE & THE ST/SE HDR 1-3 TRL1-3 1 Leave blank n/a n/a 1a Insured s ID Enter
May National Uniform Claim Committee Health Insurance Claim Form Reference Instruction Manual for Form Version 08/05. Version 9.
 National Uniform Claim Committee 1500 Health Insurance Claim Form Reference Instruction Manual for Form Version 08/05 May 2014 5/14 5/14 Disclaimer and Notices 2014 American Medical Association This document
National Uniform Claim Committee 1500 Health Insurance Claim Form Reference Instruction Manual for Form Version 08/05 May 2014 5/14 5/14 Disclaimer and Notices 2014 American Medical Association This document
July National Uniform Claim Committee Health Insurance Claim Form Reference Instruction Manual for Form Version 02/12. Version 2.
 National Uniform Claim Committee 1500 Health Insurance Claim Form Reference Instruction Manual for Form Version 02/12 July 2014 7/14 7/14 Disclaimer and Notices 2014 American Medical Association This document
National Uniform Claim Committee 1500 Health Insurance Claim Form Reference Instruction Manual for Form Version 02/12 July 2014 7/14 7/14 Disclaimer and Notices 2014 American Medical Association This document
CMS-1500 Billing Guide for PROMISe Nurses
 CMS-1500 Billing Guide for PROMISe Nurses Purpose of the document Document format The purpose of this document is to provide a block-by-block reference guide to assist the following provider types in successfully
CMS-1500 Billing Guide for PROMISe Nurses Purpose of the document Document format The purpose of this document is to provide a block-by-block reference guide to assist the following provider types in successfully
Medical Paper Claims Submission Rejections and Resolutions
 NEWS & ANNOUNCEMENTS JUNE 29, 2018 UPDATE 18-446 12 PAGES Medical Paper Claims Submission Rejections and Resolutions The preferred and most efficient way for fast turnaround and claims accuracy is to submit
NEWS & ANNOUNCEMENTS JUNE 29, 2018 UPDATE 18-446 12 PAGES Medical Paper Claims Submission Rejections and Resolutions The preferred and most efficient way for fast turnaround and claims accuracy is to submit
HOW TO SUBMIT OWCP BILLS TO THE FEDERAL BLACK LUNG PROGRAM
 HOW TO SUBMIT OWCP - 1500 BILLS TO THE FEDERAL BLACK LUG PROGRAM OFFICE OF WORKERS COMPESATIO PROGRAMS DIVISIO OF COAL MIE WORKERS COMPESATIO The services performed by the following providers should be
HOW TO SUBMIT OWCP - 1500 BILLS TO THE FEDERAL BLACK LUG PROGRAM OFFICE OF WORKERS COMPESATIO PROGRAMS DIVISIO OF COAL MIE WORKERS COMPESATIO The services performed by the following providers should be
Completing a Paper CMS-1500 (02-12) Form
 Form") Completing a Paper CS-1500 (02-12) Information in this policy does not apply to members with the Choice or Choice Plus products offered through Passport Connect S. For UnitedHealthcare s related policies/procedures,
Completing a Paper CS-1500 (02-12) Information in this policy does not apply to members with the Choice or Choice Plus products offered through Passport Connect S. For UnitedHealthcare s related policies/procedures,
MICROMD PM SETUP SPECIFICATIONS FOR TN DOH PATIENT EXPORT
 MICROMD PM SETUP SPECIFICATIONS FOR TN DOH PATIENT EXPORT This document contains information regarding data format and setup specifics for the above interface. If you need any in-depth information about
MICROMD PM SETUP SPECIFICATIONS FOR TN DOH PATIENT EXPORT This document contains information regarding data format and setup specifics for the above interface. If you need any in-depth information about
Update NEWS & ANNOUNCEMENTS JUNE 29, 2018 UPDATE PAGES
 Update NEWS & ANNOUNCEMENTS JUNE 29, 2018 UPDATE 18-444 13 PAGES Medical Paper Claims Submission Rejections and Resolutions The preferred and most efficient way for fast turnaround and claims accuracy
Update NEWS & ANNOUNCEMENTS JUNE 29, 2018 UPDATE 18-444 13 PAGES Medical Paper Claims Submission Rejections and Resolutions The preferred and most efficient way for fast turnaround and claims accuracy
July National Uniform Claim Committee Health Insurance Claim Form Reference Instruction Manual for Form Version 02/12. Version 5.
 National Uniform Claim Committee 1500 Health Insurance Claim Form Reference Instruction Manual for Form Version 02/12 July 2017 7/17 7/17 ITEMS 1 13: PATIENT AND INSURED INFORMATION Note: If the patient
National Uniform Claim Committee 1500 Health Insurance Claim Form Reference Instruction Manual for Form Version 02/12 July 2017 7/17 7/17 ITEMS 1 13: PATIENT AND INSURED INFORMATION Note: If the patient
Understanding your ChiroTouch-Generated CMS 1500 Health Insurance Claim Form
 Understanding your ChiroTouch-Generated CMS 1500 Health Insurance Claim Form Click on any box on the claim form below for a guide to entering this information into ChiroTouch. ChiroTouch cannot advise
Understanding your ChiroTouch-Generated CMS 1500 Health Insurance Claim Form Click on any box on the claim form below for a guide to entering this information into ChiroTouch. ChiroTouch cannot advise
RULES OF DEPARTMENT OF COMMERCE AND INSURANCE DIVISION OF INSURANCE AND DIVISION OF TENNCARE
 RULES OF DEPARTMENT OF COMMERCE AND INSURANCE DIVISION OF INSURANCE AND DIVISION OF TENNCARE CHAPTER 0780-1-73 UNIFORM CLAIMS PROCESS FOR TENNCARE PARTICIPATING TABLE OF CONTENTS 0780-1-73-.01 Authority
RULES OF DEPARTMENT OF COMMERCE AND INSURANCE DIVISION OF INSURANCE AND DIVISION OF TENNCARE CHAPTER 0780-1-73 UNIFORM CLAIMS PROCESS FOR TENNCARE PARTICIPATING TABLE OF CONTENTS 0780-1-73-.01 Authority
Coding pathway: Pertussis see also Whooping cough Tabular List description: Whooping cough, unspecified organism
 Healthcare Document Specialist Lesson 24 Practice Exercise 24-1 1. 005.9 Coding pathway: Poisoning, food 005.9 Tabular List description: 005.9 Food poisoning, unspecified 2. 011.04 Coding pathway: Tuberculosis,
Healthcare Document Specialist Lesson 24 Practice Exercise 24-1 1. 005.9 Coding pathway: Poisoning, food 005.9 Tabular List description: 005.9 Food poisoning, unspecified 2. 011.04 Coding pathway: Tuberculosis,
Arkansas Department of Health and Human Services Division of Medical Services P.O. Box 1437, Slot S-295 Little Rock, AR
 Arkansas Department of Health and Human Services Division of Medical Services P.O. Box 1437, Slot S-295 Little Rock, AR 72203-1437 Fax: 501-682-2480 TDD: 501-682-6789 & 1-877-708-8191 Internet Website:
Arkansas Department of Health and Human Services Division of Medical Services P.O. Box 1437, Slot S-295 Little Rock, AR 72203-1437 Fax: 501-682-2480 TDD: 501-682-6789 & 1-877-708-8191 Internet Website:
NC Health Choice for Children How to Complete a HCFA 1500
 Please Note: 1) Your claims will process quicker if you TYPE the claim form instead of hand printing it 2) Do not use any colons, semi-colons, commas, etc when entering info in 24D 3) If you are providing
Please Note: 1) Your claims will process quicker if you TYPE the claim form instead of hand printing it 2) Do not use any colons, semi-colons, commas, etc when entering info in 24D 3) If you are providing
HYMOVIS Support Hotline HYMOVIS ( )
") Important Safety Information Indication HYMOVIS is indicated for the treatment of pain in osteoarthritis (OA) of the knee in patients who have failed to respond adequately to conservative non-pharmacologic
Important Safety Information Indication HYMOVIS is indicated for the treatment of pain in osteoarthritis (OA) of the knee in patients who have failed to respond adequately to conservative non-pharmacologic
1. CMS-1500 Billing Guide for PROMISe Early and Periodic Screening, Diagnosis, and Treatment (EPSDT) Services
 Services") Purpose of the document Document format The purpose of this document is to provide a block-by-block reference guide to assist the following provider types in successfully completing the CMS-1500 Claim
Purpose of the document Document format The purpose of this document is to provide a block-by-block reference guide to assist the following provider types in successfully completing the CMS-1500 Claim
Follow CMS-1500 Claim Form Guidelines (02/12 Version) to Avoid Claims Rejections
 to Avoid Claims Rejections") Follow CMS-1500 Claim Form Guidelines (02/12 Version) to Avoid Claims Rejections In January 2014, BlueCross implemented the CMS-1500 Claim Form (02/12 Version). Due to changes on this new version of the
Follow CMS-1500 Claim Form Guidelines (02/12 Version) to Avoid Claims Rejections In January 2014, BlueCross implemented the CMS-1500 Claim Form (02/12 Version). Due to changes on this new version of the
CHAPTER 6: BILLING AND PAYMENT
 CHAPTER 6: BILLING AND PAYMENT UNIT 5: 1500 CLAIM FORM GUIDELINES IN THIS UNIT TOPIC SEE PAGE The 1500 Health Insurance Claim Form 2 OCR Scanning of Paper Claims 4 Guidelines for Submitting Paper Claims
CHAPTER 6: BILLING AND PAYMENT UNIT 5: 1500 CLAIM FORM GUIDELINES IN THIS UNIT TOPIC SEE PAGE The 1500 Health Insurance Claim Form 2 OCR Scanning of Paper Claims 4 Guidelines for Submitting Paper Claims
Claims Claim Submission QUICK REFERENCE
 Claims Claim Submission QUICK REFERENCE This will review the process of how to submit a claim online and check the status of a previously submitted claim. Get Started 1. From, click Link and sign in NOTE:
Claims Claim Submission QUICK REFERENCE This will review the process of how to submit a claim online and check the status of a previously submitted claim. Get Started 1. From, click Link and sign in NOTE:
CMS-1500 (02-12) Health Insurance Claim Form
 Health Insurance Claim Form") (02-12) Health Insurance laim Physician and Non-Physician, Professional Services, Laboratory, Independent Diagnostic Testing Facilities (IDTF), Ambulance and other Transportation, EPSDT Service, Ambulatory
(02-12) Health Insurance laim Physician and Non-Physician, Professional Services, Laboratory, Independent Diagnostic Testing Facilities (IDTF), Ambulance and other Transportation, EPSDT Service, Ambulatory
Tips for Completing the CMS-1500 Version 02/12 Claim Form
 Tips for Completing the CMS-1500 Version 02/12 Claim Form As a provider partner, we value the services you provide and it is important to us that you are reimbursed for the work you do. To assure your
Tips for Completing the CMS-1500 Version 02/12 Claim Form As a provider partner, we value the services you provide and it is important to us that you are reimbursed for the work you do. To assure your
Mental Health/Substance Use Treatment Claim Form
 Mental Health/Substance Use Treatment Claim Form DIRECTIONS FOR COMPLETION If you are in treatment with a non-participating Beacon Health Options, Inc. (Beacon) provider and your provider has indicated
Mental Health/Substance Use Treatment Claim Form DIRECTIONS FOR COMPLETION If you are in treatment with a non-participating Beacon Health Options, Inc. (Beacon) provider and your provider has indicated
Claims Submission Process Overview. For Consumer-Directed Attendant Care and Waiver Care Providers
 Claims Submission Process Overview For Consumer-Directed Attendant Care and Waiver Care Providers Agenda Member Liability Claims Submission CMS-1500 Form Claims Reconsideration Member Liability for Payment
Claims Submission Process Overview For Consumer-Directed Attendant Care and Waiver Care Providers Agenda Member Liability Claims Submission CMS-1500 Form Claims Reconsideration Member Liability for Payment
WINASAP: A step-by-step walkthrough. Updated: 2/21/18
 WINASAP: A step-by-step walkthrough Updated: 2/21/18 Welcome to WINASAP! WINASAP allows a submitter the ability to submit claims to Wyoming Medicaid via an electronic method, either through direct connection
WINASAP: A step-by-step walkthrough Updated: 2/21/18 Welcome to WINASAP! WINASAP allows a submitter the ability to submit claims to Wyoming Medicaid via an electronic method, either through direct connection
Arkansas Medicaid Health Care Providers - Pharmacy. SUBJECT: PROPOSED - Provider Manual Update Transmittal #74
 Arkansas Department of Human Services Division of Medical Services Donaghey Plaza South P.O. Box 1437 Little Rock, Arkansas 72203-1437 Internet Website: www.medicaid.state.ar.us TO: Arkansas Medicaid Health
Arkansas Department of Human Services Division of Medical Services Donaghey Plaza South P.O. Box 1437 Little Rock, Arkansas 72203-1437 Internet Website: www.medicaid.state.ar.us TO: Arkansas Medicaid Health
Dental Network Office Manual
 July 2008 Provider Network News 3 Dental Network Office Manual /ilinkblue July 2008 Provider Network News 3 23XX4296 R08/10 Blue Cross and Blue Shield of Louisiana incorporated as Louisiana Health Services
July 2008 Provider Network News 3 Dental Network Office Manual /ilinkblue July 2008 Provider Network News 3 23XX4296 R08/10 Blue Cross and Blue Shield of Louisiana incorporated as Louisiana Health Services
web-denis resources Getting to web-denis resources Log in to web-denis. You ll need your password. Click BCN Provider Publications and Resources.
 web-denis resources Getting to web-denis resources Log in to web-denis. You ll need your password. Click BCN Provider Publications and Resources. 1 web-denis resources web-denis Behavioral Health page
web-denis resources Getting to web-denis resources Log in to web-denis. You ll need your password. Click BCN Provider Publications and Resources. 1 web-denis resources web-denis Behavioral Health page
UB-04 Completion Guide Hospital Services
 1 3a 2 3b 4 5 6 1 2 3a Provider Name, Address, and Telephone Number Pay-to Name, Address, and Secondary ID Fields Patient Control Number Enter the provider s name and mailing address and telephone number.
1 3a 2 3b 4 5 6 1 2 3a Provider Name, Address, and Telephone Number Pay-to Name, Address, and Secondary ID Fields Patient Control Number Enter the provider s name and mailing address and telephone number.
CMS-1500 Billing Guide for PROMISe MA Early Intervention (EI), EI Maintenance & Infants, Toddlers, & Families (ITF) Waiver Providers
, EI Maintenance & Infants, Toddlers, & Families (ITF) Waiver Providers") CS-1500 Billing Guide for PROISe A Early Intervention (EI), EI aintenance & Infants, Toddlers, & Families (ITF) Waiver Purpose of the document Document format The purpose of this document is to provide
CS-1500 Billing Guide for PROISe A Early Intervention (EI), EI aintenance & Infants, Toddlers, & Families (ITF) Waiver Purpose of the document Document format The purpose of this document is to provide
UB04 INSTRUCTIONS Home Health
 UB04 INSTRUCTIONS Home Health 1 Provider Name, Address, Telephone 2 Pay to Name/Address/ID Required. Enter the name and address of the facility Situational. Enter the name, address, and Louisiana Medicaid
UB04 INSTRUCTIONS Home Health 1 Provider Name, Address, Telephone 2 Pay to Name/Address/ID Required. Enter the name and address of the facility Situational. Enter the name, address, and Louisiana Medicaid
Archived SECTION 15-BILLING INSTRUCTIONS. Section 15 - Billing Instructions
 SECTION 15-BILLING INSTRUCTIONS 15.1 ELECTRONIC DATA INTERCHANGE... 2 15.2 INTERNET ELECTRONIC CLAIM SUBMISSION... 2 15.3 CMS-1500 CLAIM FORM... 3 15.4 PROVIDER COMMUNICATION UNIT... 3 15.5 RESUBMISSION
SECTION 15-BILLING INSTRUCTIONS 15.1 ELECTRONIC DATA INTERCHANGE... 2 15.2 INTERNET ELECTRONIC CLAIM SUBMISSION... 2 15.3 CMS-1500 CLAIM FORM... 3 15.4 PROVIDER COMMUNICATION UNIT... 3 15.5 RESUBMISSION
For faster claim payment* please submit your claim online at
 Claims Made Easy For faster claim payment* please submit your claim online at www.combinedinsurance.com/claims FILING A CLAIM BY MAIL 1. Download the claim form 2. Print all six pages of the claim form
Claims Made Easy For faster claim payment* please submit your claim online at www.combinedinsurance.com/claims FILING A CLAIM BY MAIL 1. Download the claim form 2. Print all six pages of the claim form
HNS CMS Claim Checklist
 HNS CMS 1500 - Claim Checklist Prior to submitting paper claims, please carefully check your completed claim form against this checklist. Please contact your HNS Service Representative if you have any
HNS CMS 1500 - Claim Checklist Prior to submitting paper claims, please carefully check your completed claim form against this checklist. Please contact your HNS Service Representative if you have any
Transplant Provider Manual Kaiser Permanente Self-Funded Program
 e Transplant Provider Manual Kaiser Permanente Self-Funded Program Billing and Payment Table of Contents 5 SECTION 5: BILLING AND PAYMENT...4 5.1 WHOM TO CONTACT WITH QUESTIONS...4 5.2 METHODS OF CLAIMS
e Transplant Provider Manual Kaiser Permanente Self-Funded Program Billing and Payment Table of Contents 5 SECTION 5: BILLING AND PAYMENT...4 5.1 WHOM TO CONTACT WITH QUESTIONS...4 5.2 METHODS OF CLAIMS
CMS-1500 (02-12) Health Insurance Claim Form
 Health Insurance Claim Form") (02-12) Health Insurance laim Physician and Non-Physician, Professional Services, Laboratory, Independent Diagnostic Testing Facilities (IDTF), Ambulance and other Transportation, EPSDT Service, Ambulatory
(02-12) Health Insurance laim Physician and Non-Physician, Professional Services, Laboratory, Independent Diagnostic Testing Facilities (IDTF), Ambulance and other Transportation, EPSDT Service, Ambulatory
Comparison Chart between different modifications CMS-1500 claims
 Fabiola Bounds Comparison Chart between different modifications CMS-1500 claims 1.- Modification to commercial primary CMS-1500 claim when the same commercial health insurance company provides a secondary
Fabiola Bounds Comparison Chart between different modifications CMS-1500 claims 1.- Modification to commercial primary CMS-1500 claim when the same commercial health insurance company provides a secondary
UB-04 Billing Instructions for Home Health Claims
 UB-04 Billing Instructions for Home Health Claims 1 Provider Name, Address, Telephone # 2 Pay to Name/Address/ID Required. Enter the name and address of the facility Situational. Enter the name, address,
UB-04 Billing Instructions for Home Health Claims 1 Provider Name, Address, Telephone # 2 Pay to Name/Address/ID Required. Enter the name and address of the facility Situational. Enter the name, address,
CMS-1500 (02-12) Miscellaneous Claim Form
 Miscellaneous Claim Form") (02-12) Miscellaneous laim Physician and Non-Physician, Professional Services, Laboratory, Independent Diagnostic Testing Facilities (IDTF), Ambulance and other Transportation, EPSDT Service, Ambulatory
(02-12) Miscellaneous laim Physician and Non-Physician, Professional Services, Laboratory, Independent Diagnostic Testing Facilities (IDTF), Ambulance and other Transportation, EPSDT Service, Ambulatory
Provider Manual. Billing and Payment
 Provider Manual Billing and Payment Billing and Payment This section of the Manual was created to help guide you and your staff in working with Kaiser Permanente s billing and payment policies and procedures.
Provider Manual Billing and Payment Billing and Payment This section of the Manual was created to help guide you and your staff in working with Kaiser Permanente s billing and payment policies and procedures.
VISION (EYEWEAR) PROVIDER MANUAL Chapter Forty-Six of the Medicaid Services Manual
 PROVIDER MANUAL Chapter Forty-Six of the Medicaid Services Manual") VISION (EYEWEAR) PROVIDER MANUAL Chapter Forty-Six of the Medicaid Services Manual Issued April 21, 2011 Claims/authorizations for dates of service on or after October 1, 2015 must use the applicable ICD-10
VISION (EYEWEAR) PROVIDER MANUAL Chapter Forty-Six of the Medicaid Services Manual Issued April 21, 2011 Claims/authorizations for dates of service on or after October 1, 2015 must use the applicable ICD-10
Network Health Claims Editing Portal
 Network Health Claims Editing Portal CPT codes, descriptions and other CPT material only are copyright 2010 American Medical Association (AMA). All Rights Reserved. No fee schedules, basic units, relative
Network Health Claims Editing Portal CPT codes, descriptions and other CPT material only are copyright 2010 American Medical Association (AMA). All Rights Reserved. No fee schedules, basic units, relative
CHAPTER 7: CLAIMS, BILLING, AND REIMBURSEMENT
 CHAPTER 7: CLAIMS, BILLING, AND REIMBURSEMENT UNIT 1: HEALTH OPTIONS CLAIMS SUBMISSION AND REIMBURSEMENT IN THIS UNIT TOPIC SEE PAGE General Information 2 Reporting Practitioner Identification Number 2
CHAPTER 7: CLAIMS, BILLING, AND REIMBURSEMENT UNIT 1: HEALTH OPTIONS CLAIMS SUBMISSION AND REIMBURSEMENT IN THIS UNIT TOPIC SEE PAGE General Information 2 Reporting Practitioner Identification Number 2
ANSI 837 v5010 to CMS-1500 Crosswalk
 to CMS- Crosswalk The implementation of ANSI ASC X12N electronic transactions to version 5010 presents substantial changes in the content of the data you will submit with your claims. In order to help
to CMS- Crosswalk The implementation of ANSI ASC X12N electronic transactions to version 5010 presents substantial changes in the content of the data you will submit with your claims. In order to help
TABLE OF CONTENTS CLAIMS
 TABLE OF CONTENTS CLAIMS CLAIMS OVERVIEW... 7-1 SUBMITTING A CLAIM... 7-1 PAPER CLAIMS SUBMISSION... 7-1 ELECTRONIC CLAIMS SUBMISSION... 7-2 TIMEFRAME FOR CLAIM SUBMISSION... 7-3 PROOF OF TIMELY FILING...
TABLE OF CONTENTS CLAIMS CLAIMS OVERVIEW... 7-1 SUBMITTING A CLAIM... 7-1 PAPER CLAIMS SUBMISSION... 7-1 ELECTRONIC CLAIMS SUBMISSION... 7-2 TIMEFRAME FOR CLAIM SUBMISSION... 7-3 PROOF OF TIMELY FILING...
UB04 INSTRUCTIONS Hospice Services
 UB04 INSTRUCTIONS Hospice Services 1 Provider Name, Address, Telephone 2 Pay to Name/Address/ID Required. Enter the name and address of the facility Situational. Enter the name, address, and Louisiana
UB04 INSTRUCTIONS Hospice Services 1 Provider Name, Address, Telephone 2 Pay to Name/Address/ID Required. Enter the name and address of the facility Situational. Enter the name, address, and Louisiana
CMS 1500 Paper Claim Billing Instructions Form number
 CMS 1500 Paper Claim Billing Instructions Form number 0938-1197 Please refer to the National Uniform Claim Committee official 1500 Health Insurance Claim Reference Instruction Manual for definition, field
CMS 1500 Paper Claim Billing Instructions Form number 0938-1197 Please refer to the National Uniform Claim Committee official 1500 Health Insurance Claim Reference Instruction Manual for definition, field
CHUBB WORKPLACE BENEFITS A BUSINESS UNIT OF COMBINED INSURANCE COMPANY OF AMERICA, A CHUBB COMPANY INSTRUCTIONS FOR FILING CLAIMS
 CHUBB WORKPLACE BENEFITS A BUSINESS UNIT OF COMBINED INSURANCE COMPANY OF AMERICA, A CHUBB COMPANY INSTRUCTIONS FOR FILING CLAIMS GETTING STARTED Follow the Claimant Instructions below to complete the
CHUBB WORKPLACE BENEFITS A BUSINESS UNIT OF COMBINED INSURANCE COMPANY OF AMERICA, A CHUBB COMPANY INSTRUCTIONS FOR FILING CLAIMS GETTING STARTED Follow the Claimant Instructions below to complete the
UB-04 Billing Instructions for Hemodialysis Claims
 UB-04 Billing Instructions for Hemodialysis Claims 1 Provider Name, Address, Telephone # 2 Pay to Name/Address/ID Required. Enter the name and address of the facility Situational. Enter the name, address,
UB-04 Billing Instructions for Hemodialysis Claims 1 Provider Name, Address, Telephone # 2 Pay to Name/Address/ID Required. Enter the name and address of the facility Situational. Enter the name, address,
Provider Claims and Billing Manual
 Provider Claims and Billing Manual Version Five Publication Date: October 2015 Claims and Billing Manual Claims and Billing Manual Table of Contents Claim Filing... 1 Procedures for Claim Submission...
Provider Claims and Billing Manual Version Five Publication Date: October 2015 Claims and Billing Manual Claims and Billing Manual Table of Contents Claim Filing... 1 Procedures for Claim Submission...
UB 04 BILLING INSTRUCTIONS Nursing Facility & ICF/DD
 UB 04 BILLING INSTRUCTIONS Nursing Facility & ICF/DD Locator # Description Instructions Alerts 1 Provider Name, Address, Telephone # 2 Pay to Name/Address/ID Required. Enter the name and address of the
UB 04 BILLING INSTRUCTIONS Nursing Facility & ICF/DD Locator # Description Instructions Alerts 1 Provider Name, Address, Telephone # 2 Pay to Name/Address/ID Required. Enter the name and address of the
UB04 INSTRUCTIONS END STAGE RENAL DISEASE
 UB04 INSTRUCTIONS END STAGE RENAL DISEASE 1 Provider Name, Address, Telephone 2 Pay to Name/Address/ID 3a Patient Control Number Required. Enter the name and address of the facility Situational. Enter
UB04 INSTRUCTIONS END STAGE RENAL DISEASE 1 Provider Name, Address, Telephone 2 Pay to Name/Address/ID 3a Patient Control Number Required. Enter the name and address of the facility Situational. Enter
Interim 837 Changes Issue Brief
 WEDI Strategic National Implementation Process (SNIP) s and Code Sets Workgroup 837 Subworkgroup Interim 837 s Issue Brief s for ASC X12 837 s: Version 005010 to 006020 TM 4/9/2015 Disclaimer This document
WEDI Strategic National Implementation Process (SNIP) s and Code Sets Workgroup 837 Subworkgroup Interim 837 s Issue Brief s for ASC X12 837 s: Version 005010 to 006020 TM 4/9/2015 Disclaimer This document
HMSA Basic Claims Filing: CMS March 21, 2017
 HMSA Basic Claims Filing: CMS 1500 March 21, 2017 Agenda Plan Types Checking Eligibility CMS 1500-Interactive Tool CMS 1500 Manual Step-by-step Instructions Other Party Liability Tips to prevent common
HMSA Basic Claims Filing: CMS 1500 March 21, 2017 Agenda Plan Types Checking Eligibility CMS 1500-Interactive Tool CMS 1500 Manual Step-by-step Instructions Other Party Liability Tips to prevent common
TRANSPORTATION. [Type text] [Type text] [Type text] Version
![TRANSPORTATION. [Type text] [Type text] [Type text] Version](/thumbs/89/101159249.jpg "TRANSPORTATION. [Type text] [Type text] [Type text] Version") New York State Billing Guidelines [Type text] [Type text] [Type text] Version 2016-01 5/26/2016 EMEDNY INFORMATION emedny is the name of the New York State Medicaid system. The emedny system allows New
New York State Billing Guidelines [Type text] [Type text] [Type text] Version 2016-01 5/26/2016 EMEDNY INFORMATION emedny is the name of the New York State Medicaid system. The emedny system allows New
Provider Training Tool & Quick Reference Guide
 Provider Training Tool & Quick Reference Guide Table of Contents I. Coastal Introduction II. Services III. Obtaining Authorization a. Coastal Intake Flow Chart b. Referral/Authorization Form (Sample) IV.
Provider Training Tool & Quick Reference Guide Table of Contents I. Coastal Introduction II. Services III. Obtaining Authorization a. Coastal Intake Flow Chart b. Referral/Authorization Form (Sample) IV.
UB04 BILLING INSTRUCTIONS Nursing Facility & ICF/IID
 UB04 BILLING INSTRUCTIONS Nursing Facility & ICF/IID 1 Provider Name, Address, Telephone 2 Pay to Name/Address/ID Required. Enter the name and address of the facility Situational. Enter the name, address,
UB04 BILLING INSTRUCTIONS Nursing Facility & ICF/IID 1 Provider Name, Address, Telephone 2 Pay to Name/Address/ID Required. Enter the name and address of the facility Situational. Enter the name, address,
Claim Form Billing Instructions UB-04 Claim Form
 Claim Form Billing Instructions UB-04 Claim Form Presbyterian Health Plan / Presbyterian Insurance Company, Inc 02/19/08 Page 1 of 5 Presbyterian Health Plan / Presbyterian Insurance Company, Inc 02/19/08
Claim Form Billing Instructions UB-04 Claim Form Presbyterian Health Plan / Presbyterian Insurance Company, Inc 02/19/08 Page 1 of 5 Presbyterian Health Plan / Presbyterian Insurance Company, Inc 02/19/08
Quick Guide to Secondary Claims
 Quick Guide to Secondary Claims Would you like to: Please click below what you would like help with to be directed to that specific section in this guide. Convert your primary claim to a secondary claims
Quick Guide to Secondary Claims Would you like to: Please click below what you would like help with to be directed to that specific section in this guide. Convert your primary claim to a secondary claims
DEPARTMENT OF FINANCIAL SERVICES DIVISION OF WORKERS COMPENSATION
 DEPARTMENT OF FINANCIAL SERVICES DIVISION OF WORKERS COMPENSATION FORM (UB-04). 1 PROVIDER NAME, ADDRESS AND TELEPHONE NUMBER Enter the provider's name and a valid telephone number and the physical address
DEPARTMENT OF FINANCIAL SERVICES DIVISION OF WORKERS COMPENSATION FORM (UB-04). 1 PROVIDER NAME, ADDRESS AND TELEPHONE NUMBER Enter the provider's name and a valid telephone number and the physical address
DEPARTMENT OF FINANCIAL SERVICES DIVISION OF WORKERS COMPENSATION
 DEPARTMENT OF FINANCIAL SERVICES DIVISION OF WORKERS COMPENSATION FORM (UB-04). 1 PROVIDER NAME, ADDRESS AND TELEPHONE NUMBER Enter the provider's name and a valid telephone number and the physical address
DEPARTMENT OF FINANCIAL SERVICES DIVISION OF WORKERS COMPENSATION FORM (UB-04). 1 PROVIDER NAME, ADDRESS AND TELEPHONE NUMBER Enter the provider's name and a valid telephone number and the physical address
New MN ITS Direct Data Entry (DDE) Screens Professional (837P)
 Screens Professional (837P)") New MN ITS Direct Data Entry (DDE) Screens Professional (837P) This handout is intended to accompany the MN ITS DDE Professional 837P Training Webinar session. It is not intended to replace the MN-ITS
New MN ITS Direct Data Entry (DDE) Screens Professional (837P) This handout is intended to accompany the MN ITS DDE Professional 837P Training Webinar session. It is not intended to replace the MN-ITS
HIPAA 5010 Frequently Asked Questions
 HIPAA 5010 Frequently Asked Questions Table of Contents 1. Navicure s Online Claim Form........5 Q: Will the format change on Navicure s online HCFA 1500 claim form?... 5 2. General 5010 Questions.............5
HIPAA 5010 Frequently Asked Questions Table of Contents 1. Navicure s Online Claim Form........5 Q: Will the format change on Navicure s online HCFA 1500 claim form?... 5 2. General 5010 Questions.............5
Archived SECTION 15 - BILLING INSTRUCTIONS. Section 15 - Billing Instructions
 SECTION 15 - BILLING INSTRUCTIONS 15.1 ELECTRONIC DATA INTERCHANGE...2 15.2 INTERNET ELECTRONIC CLAIM SUBMISSION...2 15.3 UB-04 CLAIM FORM...3 15.4 PROVIDER RELATIONS COMMUNICATION UNIT...3 15.5 RESUBMISSION
SECTION 15 - BILLING INSTRUCTIONS 15.1 ELECTRONIC DATA INTERCHANGE...2 15.2 INTERNET ELECTRONIC CLAIM SUBMISSION...2 15.3 UB-04 CLAIM FORM...3 15.4 PROVIDER RELATIONS COMMUNICATION UNIT...3 15.5 RESUBMISSION
Did you know that there is a new version of the CMS 1500 form? You need to be prepared to switch.
 Introduction Did you know that there is a new version of the CMS 1500 form? You need to be prepared to switch. We are now in the dual use time frame. Payers are accepting the new form (CMS 1500 02/12)
Introduction Did you know that there is a new version of the CMS 1500 form? You need to be prepared to switch. We are now in the dual use time frame. Payers are accepting the new form (CMS 1500 02/12)