Maine Department of Health and Human Services Authorization for Release of Information
|
|
|
- Annice Sullivan
- 6 years ago
- Views:
Transcription
1 Maine Department of Health and Human Services Authorization for Release of Information We are committed to the privacy of your health information. Please read this form carefully. Office of Maine Care Services Office for Family Independence Maine Centers for Disease Control and Prevention Dorothea Dix Psychiatric Center Riverview Psychiatric Center Individual s Name: Substance Abuse and Mental Health Services Office of Child and Family Services Office of Aging and Disability Services Other: Individual s Date of Birth: Individual s Social Security Number: Individual s Address: Street Town/City State Zip Code Records to be released, including written, electronic and verbal communication: All Healthcare, including treatment, services, supplies and medicines Billing, payment, income, banking, tax, asset, and/or other information regarding financial eligibility for DHHS program benefits such as MaineCare Limit to the following date(s) or type(s) of information: (e.g. lab test dated June 2, 2013 or hospital records from 1/1/12-1/15/12 ) I authorize the DHHS office(s) checked above to: Release my information to: Obtain my information from: Name: Address: Street Town/City State Zip Code Fax No., where applicable: Phone No. to verify Receipt of Fax If requesting that electronic information be transmitted by , please clearly print the address below: I understand that DHHS systems may not be able to send my information securely through . I understand that and the internet have risks that DHHS cannot control and that the information potentially could be read by a third party. I accept those risks and still request that DHHS send my information by . Initials Please allow the office(s) named above to disclose my information for the following purpose(s): Legal Insurance Coordination of Care Personal Request Other: DHHS Authorization Form 11/13 Page 1 of 2
2 By initialing below, I wish for my release to include the following types of records: Mental health treatment provider or program Substance/Alcohol/drug abuse treatment provider or program HIV infection status or test results: Maine law requires us to tell you that releasing this information may have implications. Positive implications may include giving you more complete care, and negative implications may include discrimination if the data is misused. DHHS will protect your HIV data, and all your records, as the law requires. I (individual/personal representative of individual named above,) give permission to the DHHS office(s) listed above to release and/or share my records as written on this form. This form will remain in effect for one year from the date below. Other releases of my information are permitted during that time unless I revoke this form. I further understand and agree that: DHHS will not condition my treatment, payment for services, or benefits on whether I sign this form, unless I need to sign this form so that the right offices of DHHS can decide if I qualify for benefits. I have the right to make a written request to access and copy my healthcare or billing information, and a copy fee will be charged as permitted by law. If I want a review of my mental health program or provider records before they are released, I can check here. I understand that the review will be supervised. I may take back my permission to share the records listed on this form at any time by contacting the Privacy Officer of the specific DHHS office at: I understand that taking back my permission does not apply to the information that was already shared with my signature on this form. If I revoke my permission, it may be the basis for denial of health benefits or other insurance coverage. I may refuse to disclose all or some health care information, but that refusal may result in improper diagnosis or treatment, denial of coverage or a claim for health benefits or other insurance, or other adverse consequences. DHHS offices will keep my information confidential as required by law. If I give my permission to share my records with people who are not required by law to keep them private, they may no longer be protected by confidentiality laws. If alcohol or drug provider or program records are included in this release, DHHS will tell the person receiving the records that they may not be shared with others who are not on this form without my written permission, unless required or permitted by law. I am signing this form voluntarily and I have a right to a signed copy of this form if I request one. Date: Signature Personal Representative s authority to sign: DHHS Authorization Form 11/13 Page 2 of 2
3
4
5
6
7

8
9
10

11
12
13 Letter to Client Enclosing Copies of Pleadings and Notices JES 18 [Date] [Client Name] [Client Address] [Client Address Re: Special Needs Trust Dear Mr./Mrs./Ms. : The petition to the Probate Court to establish the Special Needs Trust has been filed with and accepted by the County Probate Court. Enclosed are copies of the complete Petition to Establish a Special Needs Trust with schedules A and B, as well as a copy of the draft Order to Establish the Special Needs Trust that we expect Judge to sign. Before Judge will sign the Order, we must provide notice of this proceeding to the Department of Health and Human Services and to the Social Security Administration. Those notices have been mailed and both have 21 days to respond to the notice of proceeding. Therefore, Judge will likely not review the petition until sometime after. I will be in touch with you as soon as we hear anything from the Court. Once Judge signs the Order, we will meet to sign the trust agreement. We will also review the draft Letter to Trustee and Letter to Trust Professional together to discuss your questions before final versions of these Letters are prepared. I welcome your questions and comments. Sincerely, Legal Assistant Enclosures 77
14
15 Letter to Forward Joinder/Sponsor Agreement to Pooled Trust JES 19 [DATE] Mail correspondence regarding Maine Pooled Disability Trust to: Ms. Joan C. Cook Maine Pooled Disability Trust P.O. Box 495 Kennebunkport, Maine Mail correspondence regarding Maine Trust for People with Disabilities to: James Houle, Esq. The Maine Trust for People with Disabilities P.O. Box 9729 Portland, ME Re: [CLIENT] Dear [Joan/Jim]: Enclosed is a completed Sponsor Agreement for the consideration of the Board of the Maine Pooled Disability Trust (MPDT). This firm represents [through in his/her capacity as.] OR Enclosed is a completed Joinder Agreement for the consideration of the Board of the Maine Trust for People with Disabilities (MTPD). This firm represents [through in his/her capacity as.] Please let me know when the Board has had an opportunity to consider and act on the enclosed Sponsor Agreement. If the Sponsor Agreement is accepted and a sub-account is established at the MPDT/MTPD, please confirm that you will communicate with all the agencies currently providing benefits to to advise that a sub-account at the MPDT/MTPD has been established. Thank you for your consideration. Very truly yours, Jane Skelton jskelton@maineelderlaw.com JES/ Enclosure cc: [CLIENT] 79
16 80
17 45-Day Letter JES 20 [Date] [Client Name] [Client Address] [Client Address Re: Special Needs Trust Dear Mr./Mrs./Ms. : On, 20, we mailed you draft documents for your review. These draft documents have no legal effect. Please let us know how we can help you get these in final form to be signed by you. As a reminder, I am being assisted by in this matter, and the direct phone number to s desk is If it would be helpful, will schedule a follow-up conference with me to take place by phone or in person. If we have not heard from you within the next six weeks, we shall assume that you do not want to proceed at this time, and I will arrange to close this firm s file. We can re-open the file in the future, but I would then need to charge for my time in reviewing the file again at my then-current hourly rate. I hope we hear from you soon. Best regards/very truly yours, Attorney Attorney/Assistant Enclosure 81
18 82
19 90-Day Letter JES 21 [Date] [Client Name] [Client Address] [Client Address Re: Special Needs Trust Dear Mr./Mrs./Ms. : On, 20, we mailed you draft documents for your review. As we have not heard from you since then, we assume you need further assistance at this time. I will arrange to close our firm s file. If you decide you would like our advice and assistance in the future, do not hesitate to contact us. [IF THERE IS AN OUTSTANDING INVOICE, MENTION HERE. You have our invoice for legal services provided to date. Although we are closing our file, fees and expenses are payable. If you have questions or want to set up a payment plan, please contact in our Accounting Department. Her number is.] This confirms that we have returned all original documents and papers you gave us in connection with this matter. Consistent with our firm s standard practice, we will maintain a digital file in this matter for eight years. Best wishes to you,. Best regards/very truly yours, Attorney Attorney/Assistant Enclosure 83
20 84
21 Document Execution Checklist JES - 22 ESTATE PLANNING DOCUMENT EXECUTION CHECKLIST Client Name(s) Client/Matter # Location of signing: Date: Responsible Attorney: 1. Order prebill for review by responsible attorney before meeting. Is there an unpaid balance?. Does responsible attorney want to deliver final invoice at the signing meeting? Other billing comments: 2. Review and assemble documents to be signed: Revocable Living Trust Agreement Certification of Trust Will Financial Power of Attorney Advance Health Care Directive Beneficiary Designation Forms Personal Property Memorandum Directive for remains/funeral instructions Other: 3. List everyone present in the room Testator(s) Lawyer: Also serving as a witness Notary: Two Disinterested Witnesses Anyone else: Name: Relationship to Testator: Name: Relationship to Testator: Comments: 85
22 Notary and witnesses must be continuously present in the room during the entire execution ceremony and be able to see the testator signing the documents. Other family members should usually not be present. Lawyer should usually not serve as the notary. 4. Before Signing Will 86 Introduce all participants. Evaluate capacity of testator and determine whether: 1. Intact No or very minimal evidence of diminished capacity; 2. Mild problems Some evidence of diminished capacity; 3. More than mild problems Substantial evidence of diminished capacity; or 4. Severe problems Client lacks capacity to proceed with representation and transaction. If more than mild problems, complete four page Capacity Worksheet for Lawyers from ABA s Assessment of Older Adults with Diminished Capacity: A Handbook for Lawyer. R Review all documents with client Testator and witnesses sign revocable trust, if applicable 5. Procedure for signing Will: Ask the Testator to confirm: You are [testator name], you intend this document to be your Last Will and Testament, you want to sign it, you want the two of us (identify the witnesses) to witness your signature to your Will, and you are signing willingly. Testator responds in the affirmative. Ask the Testator to initial at the bottom of each page (including the final page if it follows the signature page) and sign above the typed name at the end. Testator initials and signs. Check to be sure all pages are initialed. The lawyer or notary asks the testator: Do you declare [to the notary] that you have signed this as your Last Will and Testament, willingly, as your free and voluntary act, that you are 18 years of age or older, of sound mind and under no constraint or undue influence? Testator responds in the affirmative. The lawyer or notary asks the witnesses: Do you each declare that you have witnessed [the testator] signing this instrument as his/her Last Will, that he/she signed it willingly, and that to the best of your knowledge [the testator] is 18 years of age or older, of sound mind, and under no constraint or undue influence? Witnesses respond in the affirmative. Witnesses sign. Notary signs and affixes seal. 6. Client and witnesses sign other documents: General Durable Financial Power of Attorney Advance Health Care Directive Beneficiary Designation Forms Personal Property Memorandum Other:
23 7. Determine clients wishes regarding storage of the original documents and delivery of copies (and confirm in closing letter). Ask client if they would like us to store the original will. (We prefer to deliver other original documents to the client for safe keeping, but will store powers of attorney and trust documents if requested). Ask clients if they would like to receive electronic (.PDF) copies of documents instead of or in addition to paper copies. Original documents to be retained by RW: None Will Financial Power of Attorney Advance Health Care Directive Other: Original documents delivered to clients at signing: None Financial Power of Attorney Advance Health Care Directive Specify: Original documents to be mailed to client with closing letter: None Specify: Copies to be mailed to clients with closing letter: None Specify (how many copies of each).pdf copies to be ed to clients: None All: ( address): Copies or.pdfs to be sent to others (family members, physicians, financial advisors, etc.) None Specify which documents and address: 87
24 8. Determine disposition of prior original documents. N/A no prior documents Client physically destroyed prior will in my presence. RW is retaining prior original will (e.g., capacity is in doubt and testator prefers prior will to intestacy) Comments: Advised clients to destroy prior original wills (confirm in closing letter) Comments: Client destroyed other original documents (specify): 9. Additional Comments/Issues for Follow Up /Matters to confirm in closing letter: 10. Following the signing meeting: o o o Responsible assistant saves this completed checklist as the memorandum of the signing meeting. Responsible assistant drafts closing letter for review by responsible attorney Responsible attorney reviews and signs closing letter. Send letter to trustee/tax professional, if applicable. Send final bill if applicable. Inventory and Storage of Documents: Document information is entered in data base spread sheet maintained in Worldox (Forms/Estate Planning/Estate Planning Aids) R XLS Any original documents are stored in RW vault PDFs of documents are saved to client file on Worldox 88
25 Letter to Maine DHHS for Approval of d4a Trust JES-23 Date Mr. Reinhold Bansmer Senior MaineCare Program Manager 19 Union Street State House Station #11 Augusta, ME Re: Special Needs Trust Dear Ron: Enclosed is a copy of the executed Special Needs Trust which meets the requirements of 42 U.S.C. 1396p(d)(4)(A) and Part 16, Section 4.53(A)(6)(a), of the MaineCare Eligibility Manual. Also enclosed is a DHHS Authorization and Release signed by which authorizes you to communicate with this firm. Please confirm that when s assets are transferred to the Trustee of this trust, the transfer will not result in a transfer penalty. Please also confirm that assets held in the trust will not be countable to for the purpose of his continued eligibility for MaineCare nursing home benefits. The necessary provisions for a trust pursuant to 42 U.S.C. 1396p(d)(4)(A) and Part 16, Section 4.53(A)(6)(a), of the MaineCare Eligibility Manual are outlined below: a. Will the trust be established for a disabled individual under age 65? Yes, is an individual with disabilities. He receives MaineCare benefits. He also receives Social Security Disability Income and Medicare benefits. was born on, and he is years old. He resides at Rehab and Living Center. b. Will the trust be established with the assets of a disabled individual? The trust will be funded with assets to which is entitled. Those assets were held in a trust following the death of his father and for the benefit of his mother,. Mrs. has now died. Those trust assets are being distributed to and his siblings. c. Is the disabled individual the beneficiary of the trust? During his lifetime, is the sole beneficiary of the trust. See Section 1.04 of the trust agreement. d. Did the individual with disabilities who has capacity establish the trust, or was the trust established by a parent, grandparent, legal guardian or court? 89
26 The individual with disabilities has capacity and established the trust. e. Does the trust provide that any state will be reimbursed for medical assistance paid on his or her behalf upon the termination of the trust or the death of the beneficiary? See Articles Three and Four of the enclosed trust agreement. Any assets remaining in the Trust upon termination of the trust, whether at the time of s death or otherwise, after payment of any and all legal obligations of the Trust, shall be reported to and available for reimbursement to the State of Maine and any other states that have provided with medical assistance prior to distributions to friends and family. f. Does the trust meet the special needs trust exception to the extent that assets of the beneficiary were put in the trust prior to the beneficiary attaining age 65? Yes. See the previous answers. g. Is the trust irrevocable? The trust agreement states that the trust is irrevocable. See Section In addition, there are named residual beneficiaries who are specifically identifiable in Section Thank you for your kind attention to the enclosed documents and your consideration of the request for approval of the form of the Special Needs Trust. Very truly yours, Attorney Attorney/Assistant Enclosure cc: 90
27 Summary Index Sheet JES 24 LAST FIRST INITIAL (Name of Testator) Testator s Address: DATE EXECUTED: LOCATION OF ORIGINAL WILL: FILE # PERSONAL REPRESENTATIVE(s) AND ADDRESS(es): RESPONSIBLE ATTY: WILL dated: Original located at: Simple Complex Disclaimer Marital Family/Credit Shelter SNT Pourover POA dated: Original located at: AGENTS: AHCD dated: Original located at: AGENTS: TRUST dated: Original located at: Type: Revocable Irrevocable Insurance Real Estate MAPT VAPT 1 st Party SNT 3 rd Party SNT Conduit/Stand Alone Retirement Charitable Other OTHER: 91
28 92
DRAFTING INSTRUCTIONS: [DRAFTING INSTRUCTIONS APPEAR IN GREEN. DELETE THESE INSTRUCTIONS WHEN YOU HAVE COMPLETED DRAFTING YOUR WILL]
![DRAFTING INSTRUCTIONS: [DRAFTING INSTRUCTIONS APPEAR IN GREEN. DELETE THESE INSTRUCTIONS WHEN YOU HAVE COMPLETED DRAFTING YOUR WILL]](/thumbs/95/125056444.jpg "DRAFTING INSTRUCTIONS: [DRAFTING INSTRUCTIONS APPEAR IN GREEN. DELETE THESE INSTRUCTIONS WHEN YOU HAVE COMPLETED DRAFTING YOUR WILL]") Will Single Person DRAFTING INSTRUCTIONS: [DRAFTING INSTRUCTIONS APPEAR IN GREEN. DELETE THESE INSTRUCTIONS WHEN YOU HAVE COMPLETED DRAFTING YOUR WILL] Insert the names of relevant people at the parts
Will Single Person DRAFTING INSTRUCTIONS: [DRAFTING INSTRUCTIONS APPEAR IN GREEN. DELETE THESE INSTRUCTIONS WHEN YOU HAVE COMPLETED DRAFTING YOUR WILL] Insert the names of relevant people at the parts
Powers of Attorney. Public Legal Education and Information Service of New Brunswick
 Powers of Attorney Public Legal Education and Information Service of New Brunswick Powers of Attorney Public Legal Education and Information Service of New Brunswick (PLEIS-NB) is a non-profit, charitable
Powers of Attorney Public Legal Education and Information Service of New Brunswick Powers of Attorney Public Legal Education and Information Service of New Brunswick (PLEIS-NB) is a non-profit, charitable
Representative Payee Application
 Representative Payee Application I hereby authorize Greater Triangle Representative Payee Services, Inc. to manage by benefits and to serve as my organizational representative payee. I understand that
Representative Payee Application I hereby authorize Greater Triangle Representative Payee Services, Inc. to manage by benefits and to serve as my organizational representative payee. I understand that
This is a legal document. You are strongly encouraged to seek independent, professional advice before signing.
 Jewish Los Angeles Special Needs Financial Services Inc. JOINDER AGREEMENT for Jewish Los Angeles Special Needs Master Trust II 3 rd Person Special Needs Trusts This is a legal document. You are strongly
Jewish Los Angeles Special Needs Financial Services Inc. JOINDER AGREEMENT for Jewish Los Angeles Special Needs Master Trust II 3 rd Person Special Needs Trusts This is a legal document. You are strongly
USING A POOLED INCOME TRUST TO ELIMINATE A MEDICAID SPEND DOWN MARIE T. VAZ, STAFF ATTORNEY
 USING A POOLED INCOME TRUST TO ELIMINATE A MEDICAID SPEND DOWN by MARIE T. VAZ, STAFF ATTORNEY Evelyn Frank Legal Resources Program New York Legal Assistance Group New York City 197 198 Using a Pooled
USING A POOLED INCOME TRUST TO ELIMINATE A MEDICAID SPEND DOWN by MARIE T. VAZ, STAFF ATTORNEY Evelyn Frank Legal Resources Program New York Legal Assistance Group New York City 197 198 Using a Pooled
General Instructions For Completing This Joinder Agreement
 General Instructions For Completing This Joinder Agreement An Important Note to Grantors: Please read the entire Joinder Agreement carefully, including all of the exhibits. Some of the exhibits require
General Instructions For Completing This Joinder Agreement An Important Note to Grantors: Please read the entire Joinder Agreement carefully, including all of the exhibits. Some of the exhibits require
Trinity Family Physicians
 Trinity Family Physicians Consent and Authorization for Minors By law, a healthcare provider must attempt to contact a birth / custodial parent or legal guardian prior to rendering treatment to a minor
Trinity Family Physicians Consent and Authorization for Minors By law, a healthcare provider must attempt to contact a birth / custodial parent or legal guardian prior to rendering treatment to a minor
Peace of Mind. Give Yourself. Essential Forms for Future Planning: Living Will Power of Attorney Health Care Proxy. ...and much more.
 Give Yourself Peace of Mind Essential Forms for Future Planning: Living Will Power of Attorney Health Care Proxy...and much more. Onondaga County Department of Adult & Long Term Care Services Office for
Give Yourself Peace of Mind Essential Forms for Future Planning: Living Will Power of Attorney Health Care Proxy...and much more. Onondaga County Department of Adult & Long Term Care Services Office for
PATIENT REGISTRATION FORM
 Today s Date / / PATIENT REGISTRATION FORM PATIENT INFORMATION Patient Name Last First Middle Is this your legal name? If not, what is your legal name? Birthdate Age Sex q YES q NO / / q M q F q T Street
Today s Date / / PATIENT REGISTRATION FORM PATIENT INFORMATION Patient Name Last First Middle Is this your legal name? If not, what is your legal name? Birthdate Age Sex q YES q NO / / q M q F q T Street
THE STATE BAR OF CALIFORNIA DO I NEED A WILL? GET THE LEGAL FACTS OF LIFE
 THE STATE BAR OF CALIFORNIA DO I NEED A WILL? GET THE LEGAL FACTS OF LIFE Do I need a will? 1 What is a will? 2 Does a will cover everything I own? 3 What happens if I don t have a will? 4 Are there various
THE STATE BAR OF CALIFORNIA DO I NEED A WILL? GET THE LEGAL FACTS OF LIFE Do I need a will? 1 What is a will? 2 Does a will cover everything I own? 3 What happens if I don t have a will? 4 Are there various
Name: DOB: SS: Mailing Address: City: State: Zip: Home #: Cell phone #: Martital Status: Address:
 Patient Information: Name: DOB: SS: Mailing Address: City: State: Zip: Home #: Cell phone #: Martital Status: Email Address: Race: Ethnicity: Gender: Primary Language: Preferred Spoken Language: Would
Patient Information: Name: DOB: SS: Mailing Address: City: State: Zip: Home #: Cell phone #: Martital Status: Email Address: Race: Ethnicity: Gender: Primary Language: Preferred Spoken Language: Would
HARBORSIDE COUNSELING SERVICES CLIENT REGISTRATION
 HARBORSIDE COUNSELING SERVICES CLIENT REGISTRATION Thank you for choosing our office. In order to serve you properly, we will need the following information. PLEASE PRINT: Name: Date: (Parents/caregivers):
HARBORSIDE COUNSELING SERVICES CLIENT REGISTRATION Thank you for choosing our office. In order to serve you properly, we will need the following information. PLEASE PRINT: Name: Date: (Parents/caregivers):
Client Contract. Client Full Name: Social Security Number: POA/Guardian Name: Phone: Address:
 Client Contract Client Full DOB: Social Security Number: POA/Guardian Phone: _ I, or my advocate, have discussed my needs with my POA/Guardian. I agree to have Thrive serve has my representative payee
Client Contract Client Full DOB: Social Security Number: POA/Guardian Phone: _ I, or my advocate, have discussed my needs with my POA/Guardian. I agree to have Thrive serve has my representative payee
KEEP THEM SAFE POOLED TRUST I. (A Trust for Persons with Disabilities) BENEFICIARY PROFILE SHEET AND JOINDER AGREEMENT
 BENEFICIARY PROFILE SHEET AND JOINDER AGREEMENT") KEEP THEM SAFE POOLED TRUST I (A Trust for Persons with Disabilities) BENEFICIARY PROFILE SHEET AND JOINDER AGREEMENT WELCOME TO KEEP THEM SAFE POOLED TRUST I As part of your application process, please
KEEP THEM SAFE POOLED TRUST I (A Trust for Persons with Disabilities) BENEFICIARY PROFILE SHEET AND JOINDER AGREEMENT WELCOME TO KEEP THEM SAFE POOLED TRUST I As part of your application process, please
FUTURE PLANNING, GUARDIANSHIP AND TRUSTS
 KEEP IN MIND: AGE 18 FUTURE PLANNING, GUARDIANSHIP AND TRUSTS Darcy J. Chamberlin Chamberlin Law Group 1200 Harger Road, Suite 209 Oak Brook, IL 60523-1816 630-571-0222 www.clgattorney.com Legal Decision-Making
KEEP IN MIND: AGE 18 FUTURE PLANNING, GUARDIANSHIP AND TRUSTS Darcy J. Chamberlin Chamberlin Law Group 1200 Harger Road, Suite 209 Oak Brook, IL 60523-1816 630-571-0222 www.clgattorney.com Legal Decision-Making
In addition there are several aspects of your disability claim that you should be aware of:
 Dear Colleague: American Airlines has partnered with Harvey Watt and Company as the Claim Administrator for the Pilot Long Term Disability Plan (the Plan). We have enclosed the Claim Application along
Dear Colleague: American Airlines has partnered with Harvey Watt and Company as the Claim Administrator for the Pilot Long Term Disability Plan (the Plan). We have enclosed the Claim Application along
RIGHTS OF MASSACHUSETTS INDIVIDUALS WITH A REPRESENTATIVE PAYEE. Prepared by the Mental Health Legal Advisors Committee August 2017
 RIGHTS OF MASSACHUSETTS INDIVIDUALS WITH A REPRESENTATIVE PAYEE Prepared by the Mental Health Legal Advisors Committee August 2017 What is a representative payee? 2 When does the Social Security Administration
RIGHTS OF MASSACHUSETTS INDIVIDUALS WITH A REPRESENTATIVE PAYEE Prepared by the Mental Health Legal Advisors Committee August 2017 What is a representative payee? 2 When does the Social Security Administration
New York Public Employee Retirement System Special Durable Power of Attorney (Rev. 6/18)
") Office of the New York State Comptroller 110 State Street, Albany, New York 12244-0001 Received New York Public Employee Retirement System Special Durable Power of Attorney (Rev. 6/18) This is a Public
Office of the New York State Comptroller 110 State Street, Albany, New York 12244-0001 Received New York Public Employee Retirement System Special Durable Power of Attorney (Rev. 6/18) This is a Public
INFORMATION FORM. Page 1 of 17
 INFORMATION FORM Page 1 of 17 Client Information and Acknowledgment of Informed Consent to Treatment Therapist: Neila Senter, LPCC, is a licensed independent counselor engaged in the private practice of
INFORMATION FORM Page 1 of 17 Client Information and Acknowledgment of Informed Consent to Treatment Therapist: Neila Senter, LPCC, is a licensed independent counselor engaged in the private practice of
If you wish to apply for a distribution at this time, please follow the instructions below:
 Dear DC 401(a) Retirement Plan Participant: You recently contacted ING and requested a Distribution Package for the DC 401(a) Retirement Plan. Before completing the necessary forms, we recommend that you
Dear DC 401(a) Retirement Plan Participant: You recently contacted ING and requested a Distribution Package for the DC 401(a) Retirement Plan. Before completing the necessary forms, we recommend that you
ALABAMA STATE BAR WILLS FOR HEROES PROGRAM
 ALABAMA STATE BAR WILLS FOR HEROES PROGRAM In order to make the Wills for Heroes project as convenient as possible we will be holding the program on site. For the process to run smoothly and take as little
ALABAMA STATE BAR WILLS FOR HEROES PROGRAM In order to make the Wills for Heroes project as convenient as possible we will be holding the program on site. For the process to run smoothly and take as little
2017 National Conference on Special Needs Planning and Special Needs Trusts
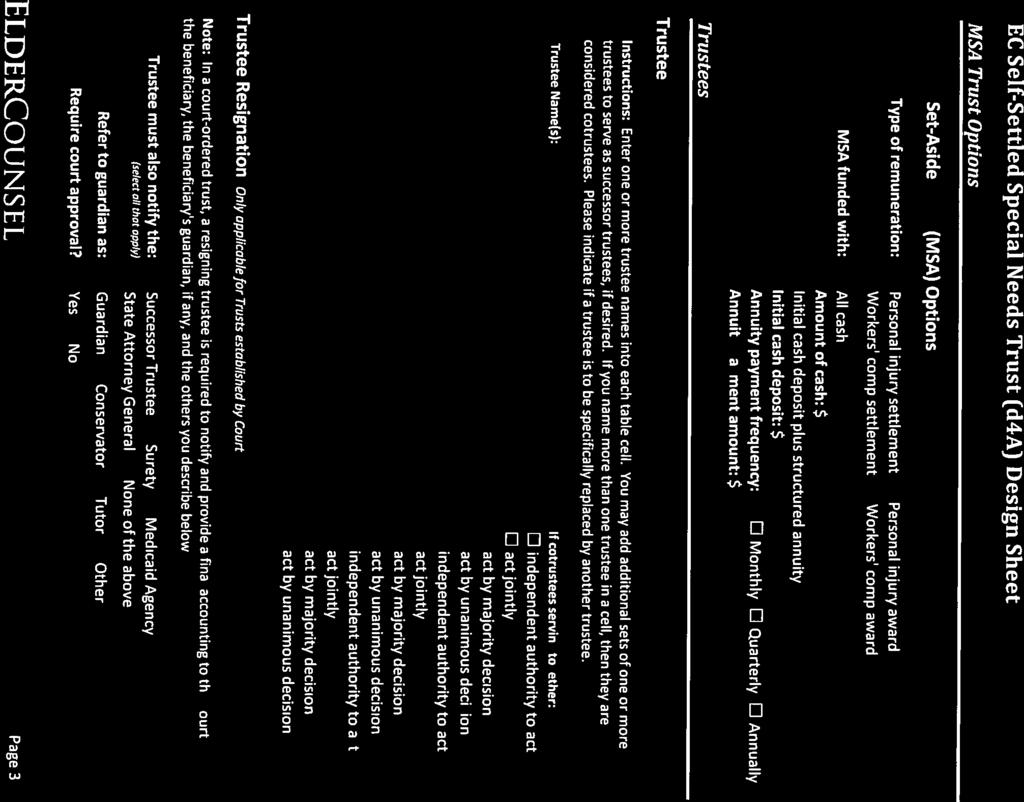
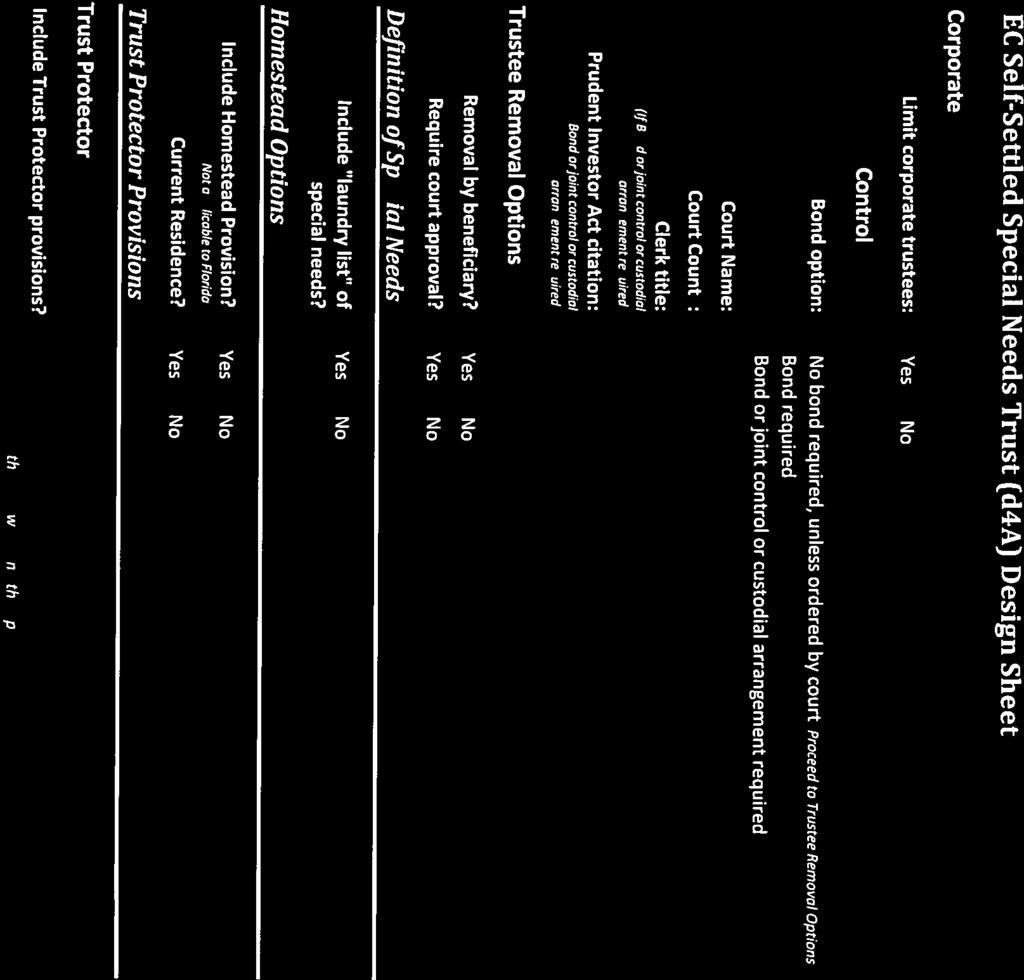
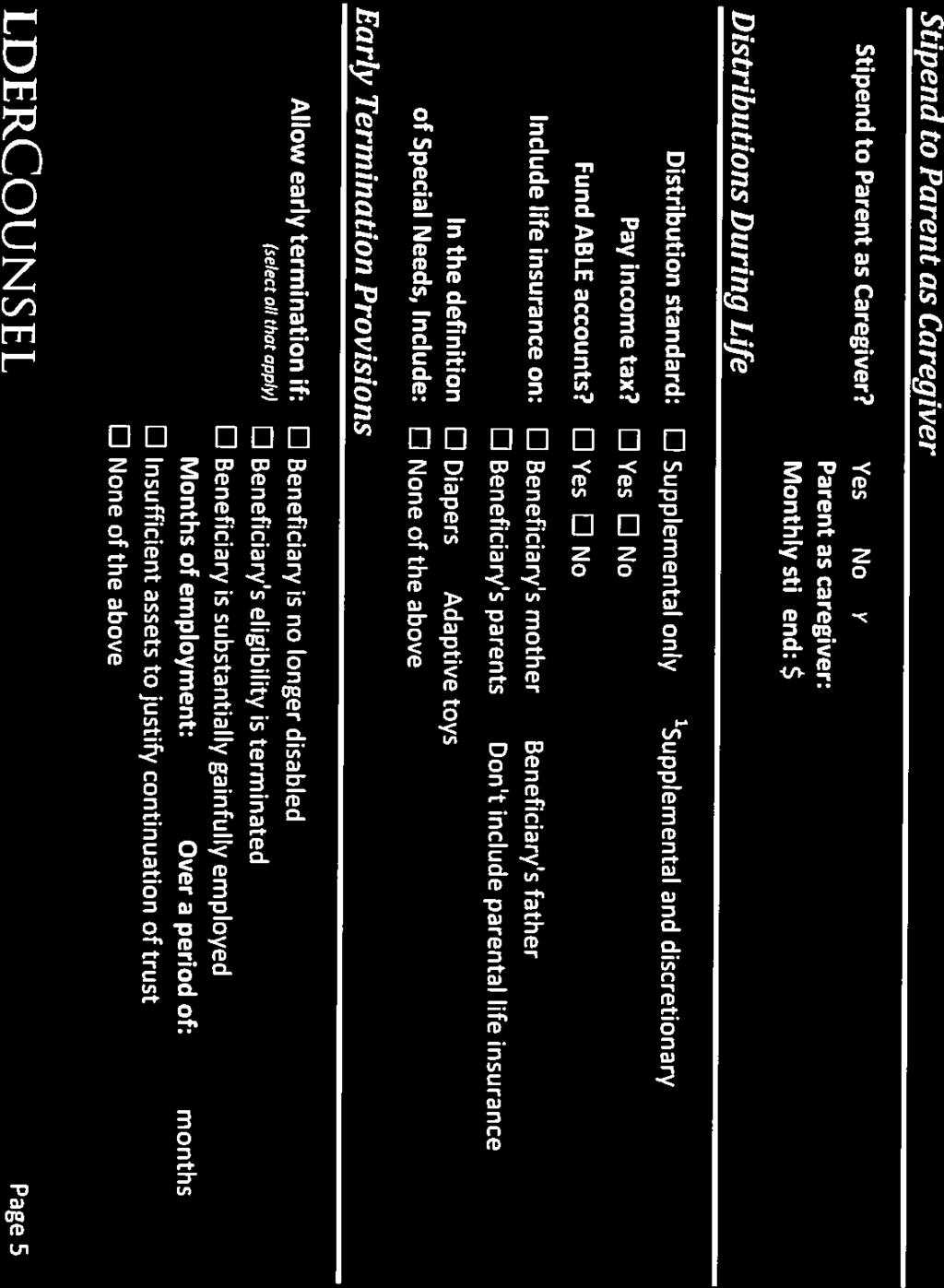
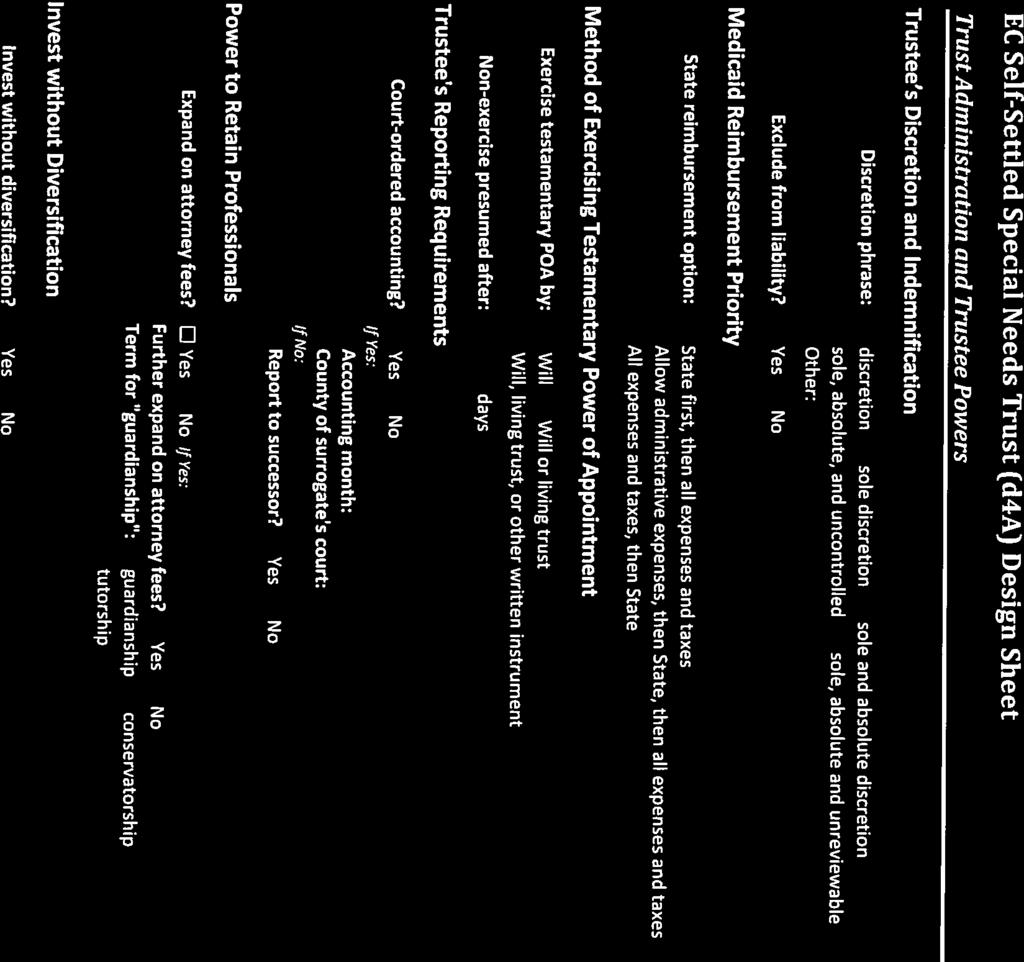
 2017 National Conference on Special Needs Planning and Special Needs Trusts FIRST PARTY SPECIAL NEEDS TRUST SYSTEMS By: Jane Skelton, Esq. and Crystal West Edwards, Esq. Jane Skelton, Esq. is a past Chair
2017 National Conference on Special Needs Planning and Special Needs Trusts FIRST PARTY SPECIAL NEEDS TRUST SYSTEMS By: Jane Skelton, Esq. and Crystal West Edwards, Esq. Jane Skelton, Esq. is a past Chair
Personal Representatives
 Personal Representatives DISCLAIMER: THE PURPOSE OF THIS CLASS IS TO PROVIDE YOU WITH INFORMATION TO ASSIST YOU IN COMPLETING YOUR DUTIES AS PERSONAL REPRESENTATIVE. IT IS NOT MEANT AS A SUBSTITUTE FOR
Personal Representatives DISCLAIMER: THE PURPOSE OF THIS CLASS IS TO PROVIDE YOU WITH INFORMATION TO ASSIST YOU IN COMPLETING YOUR DUTIES AS PERSONAL REPRESENTATIVE. IT IS NOT MEANT AS A SUBSTITUTE FOR
Requirements vary from state to state. Generally, for your will to be valid, the following requirements must be satisfied.
 1 Wills What is a will? A will may be the most vital piece of your estate plan, even if your estate is a modest one. It is a legal document that lets you direct how your property will be dispersed (among
1 Wills What is a will? A will may be the most vital piece of your estate plan, even if your estate is a modest one. It is a legal document that lets you direct how your property will be dispersed (among
COMMUNITY FUND MANAGEMENT FOUNDATION POOLED MEDICAID PAYBACK TRUST POOLED MEDICAID PAYBACK SUB-ACCOUNT
 COMMUNITY FUND MANAGEMENT FOUNDATION POOLED MEDICAID PAYBACK TRUST POOLED MEDICAID PAYBACK SUB-ACCOUNT JOINDER AGREEMENT AND APPLICATION FOR ADMISSION TO ESTABLISH POOLED MEDICAID PAYBACK TRUST SUB-ACCOUNT
COMMUNITY FUND MANAGEMENT FOUNDATION POOLED MEDICAID PAYBACK TRUST POOLED MEDICAID PAYBACK SUB-ACCOUNT JOINDER AGREEMENT AND APPLICATION FOR ADMISSION TO ESTABLISH POOLED MEDICAID PAYBACK TRUST SUB-ACCOUNT
Bastrop County Court Guardian of the Person and Estate: Court-Ordered Instructions. Cause No. G - Guardianship of:
 Cause No. G - Guardianship of: Thank you for considering appointment as the Guardian of the Person and Estate of a minor or incapacitated individual (the Ward). As such a Guardian, the State of Texas,
Cause No. G - Guardianship of: Thank you for considering appointment as the Guardian of the Person and Estate of a minor or incapacitated individual (the Ward). As such a Guardian, the State of Texas,
For purposes of this article only, annuity is defined as a policy or. contract that is a private agreement or an investment contract or an insurance
 (1) Repeal Section 50960. 50960. Definitions. (a) For purposes of this article only, annuity is defined as a policy or contract that is a private agreement or an investment contract or an insurance policy
(1) Repeal Section 50960. 50960. Definitions. (a) For purposes of this article only, annuity is defined as a policy or contract that is a private agreement or an investment contract or an insurance policy
AGREEMENT AND INFORMED CONSENT FOR TREATMENT
 Joseph M. Cereghino, Psy.D. Licensed Psychologist Family Institute, P.C. 4110 Pacific Ave., Suite 102, Forest Grove, OR 97116 Tigard Office: 9600 SW Oak St., Suite 280, Tigard, OR 97223 (503) 601-5400
Joseph M. Cereghino, Psy.D. Licensed Psychologist Family Institute, P.C. 4110 Pacific Ave., Suite 102, Forest Grove, OR 97116 Tigard Office: 9600 SW Oak St., Suite 280, Tigard, OR 97223 (503) 601-5400
Contact CANHR s Lawyer Referral Service (LRS) by visiting or calling (800)
 by visiting or calling (800)") Updated 4/25/2016 Incapacity: Plan for it now FACT SHEET CANHR is a private, nonprofit 501(c)(3) organization dedicated to improving the quality of care and the quality of life for long term care consumers
Updated 4/25/2016 Incapacity: Plan for it now FACT SHEET CANHR is a private, nonprofit 501(c)(3) organization dedicated to improving the quality of care and the quality of life for long term care consumers
STATUTORY DURABLE POWER OF ATTORNEY
 STATUTORY DURABLE POWER OF ATTORNEY Author s Comments: This Durable Power of Attorney is based on the Connecticut Statutory Short Form Power of Attorney Act, CGS 1-42 to 1-56. You will notice this form
STATUTORY DURABLE POWER OF ATTORNEY Author s Comments: This Durable Power of Attorney is based on the Connecticut Statutory Short Form Power of Attorney Act, CGS 1-42 to 1-56. You will notice this form
INSTRUCTIONS FOR COMPLETING THE JOINDER AGREEMENT
 INSTRUCTIONS FOR COMPLETING THE JOINDER AGREEMENT To enroll in the Pooled Trust, a Joinder Agreement must be completed. By signing the Joinder, the Settlor agrees to the terms of The Family Trust Master
INSTRUCTIONS FOR COMPLETING THE JOINDER AGREEMENT To enroll in the Pooled Trust, a Joinder Agreement must be completed. By signing the Joinder, the Settlor agrees to the terms of The Family Trust Master
GENERAL ESTATE PLANNING QUESTIONS
 What is estate planning? GENERAL ESTATE PLANNING QUESTIONS Estate planning is a process to consider alternatives for, to think through, and to set up legally effective arrangements that would meet your
What is estate planning? GENERAL ESTATE PLANNING QUESTIONS Estate planning is a process to consider alternatives for, to think through, and to set up legally effective arrangements that would meet your
Get Started Will Planning
 Get Started Will Planning Revised February 2014 How to use this booklet The purpose of this booklet is to allow you to summarize key information about your Will plans to assist you in working with a lawyer
Get Started Will Planning Revised February 2014 How to use this booklet The purpose of this booklet is to allow you to summarize key information about your Will plans to assist you in working with a lawyer
National Electrical Annuity Plan Disability Benefit Application
 National Electrical Annuity Plan Disability Benefit Application To avoid delays in the processing and payment of your benefit, please follow these instructions carefully and completely. 1. Print all information
National Electrical Annuity Plan Disability Benefit Application To avoid delays in the processing and payment of your benefit, please follow these instructions carefully and completely. 1. Print all information
or my newly adopted/placed for adoption child(ren): placement date)
: placement date)") Washington Individual Enrollment Application Effective January 1, 2016 This application is for health care coverage purchased directly from Premera Blue Cross (Premera). For timely and proper processing,
Washington Individual Enrollment Application Effective January 1, 2016 This application is for health care coverage purchased directly from Premera Blue Cross (Premera). For timely and proper processing,
THE ARC OF OHIO INC. ACCOUNT OF THE COMMUNITY FUND MANAGEMENT FOUNDATION POOLED MEDICAID PAYBACK TRUST POOLED MEDICAID PAYBACK SUB-ACCOUNT
 THE ARC OF OHIO INC. ACCOUNT OF THE COMMUNITY FUND MANAGEMENT FOUNDATION POOLED MEDICAID PAYBACK TRUST POOLED MEDICAID PAYBACK SUB-ACCOUNT JOINDER AGREEMENT AND APPLICATION FOR ADMISSION TO ESTABLISH POOLED
THE ARC OF OHIO INC. ACCOUNT OF THE COMMUNITY FUND MANAGEMENT FOUNDATION POOLED MEDICAID PAYBACK TRUST POOLED MEDICAID PAYBACK SUB-ACCOUNT JOINDER AGREEMENT AND APPLICATION FOR ADMISSION TO ESTABLISH POOLED
BILL L. JOU, M.D., INC.
 BILL L. JOU, M.D., INC. AUTHORIZATION TO TREAT I (and/or the undersigned on behalf of the patient) voluntarily consent to allow Dr. Bill L. Jou and staff to provide such evaluation and/or care and treatments
BILL L. JOU, M.D., INC. AUTHORIZATION TO TREAT I (and/or the undersigned on behalf of the patient) voluntarily consent to allow Dr. Bill L. Jou and staff to provide such evaluation and/or care and treatments
Presented By: Michael J. Wittick Attorney & Counselor at Law Member, WealthCounsel LLC
 Issues in Special Needs Trust Planning Presented By: Michael J. Wittick Attorney & Counselor at Law Member, WealthCounsel LLC Facts of Life Persons with disabilities are living longer and public benefits
Issues in Special Needs Trust Planning Presented By: Michael J. Wittick Attorney & Counselor at Law Member, WealthCounsel LLC Facts of Life Persons with disabilities are living longer and public benefits
AUTHORIZATION TO USE, DISCLOSE, & RELEASE PROTECTED HEALTH INFORMATION
 AUTHORIZATION TO USE, DISCLOSE, & RELEASE PROTECTED HEALTH INFORMATION I understand the following: I have the right to refuse to sign this form for authorization to disclose or release my protected health
AUTHORIZATION TO USE, DISCLOSE, & RELEASE PROTECTED HEALTH INFORMATION I understand the following: I have the right to refuse to sign this form for authorization to disclose or release my protected health
Welcome to Rx Help Centers!
 Welcome to Rx Help Centers! Congratulations! We are thrilled that you have chosen Rx Help Centers as your personal prescription advocate! Rx Help Centers is proud to work on your behalf to save you money
Welcome to Rx Help Centers! Congratulations! We are thrilled that you have chosen Rx Help Centers as your personal prescription advocate! Rx Help Centers is proud to work on your behalf to save you money
Legal first and last name of person being assessed today: Marital Status: Social Security #: State: Zip: Employer:
 Admissions Staff Place Patient ID Sticker Here Patient Registration Please read and complete both sides of this form Date: Time: Legal first and last name of person being assessed today: Date of Birth:
Admissions Staff Place Patient ID Sticker Here Patient Registration Please read and complete both sides of this form Date: Time: Legal first and last name of person being assessed today: Date of Birth:
Transamerica Financial Life Insurance Company Home Office: Purchase, NY Administrative Office: 100-G Executive Drive Edgewood, NY
 Transamerica Financial Life Insurance Company Home Office: Purchase, NY Administrative Office: 100-G Executive Drive Edgewood, NY 11717-8331 Hardship Withdrawal Form READ THE ATTACHED IRS SPECIAL TAX NOTICE
Transamerica Financial Life Insurance Company Home Office: Purchase, NY Administrative Office: 100-G Executive Drive Edgewood, NY 11717-8331 Hardship Withdrawal Form READ THE ATTACHED IRS SPECIAL TAX NOTICE
Patient Information PATIENT NAME: DOB: AGE: ADDRESS: ZIP CODE: EMPLOYER NAME: WORK PHONE: RACE: SEX: Male Female PRIMARY DOCTOR: NAME: TELEPHONE#
 Patient Information Welcome to our office. We appreciate the confidence that you have placed with us regarding your healthcare needs. To assist us in serving you, please complete the following forms as
Patient Information Welcome to our office. We appreciate the confidence that you have placed with us regarding your healthcare needs. To assist us in serving you, please complete the following forms as
Planning for a Family Member s Future: the Special Needs Trust
 SPEAKER NOTES Planning for a Family Member s Future: the Special Needs Trust Summarized by Thomas T. Thomas How can we plan for our mentally disabled son or daughter s future after we have gone? One answer
SPEAKER NOTES Planning for a Family Member s Future: the Special Needs Trust Summarized by Thomas T. Thomas How can we plan for our mentally disabled son or daughter s future after we have gone? One answer
Powers of Attorney. This booklet contains forms for Continuing Power of Attorney for Property and Power of Attorney for Personal Care
 Powers of Attorney This booklet contains forms for Continuing Power of Attorney for Property and Power of Attorney for Personal Care Ministry of the Attorney General Ce document, intitulé Les procurations,
Powers of Attorney This booklet contains forms for Continuing Power of Attorney for Property and Power of Attorney for Personal Care Ministry of the Attorney General Ce document, intitulé Les procurations,
If you have questions about how much your fee will be, you may stop by or call with your income information before your appointment.
 238 Arsenal Street, Watertown, NY Family Practice Office: (315) 782-6400 Fax: (315) 782-1330 Adult Office: (315) 782-9903 Fax: (315) 788-0087 Dental Office: (315) 788-9834 Fax: (315) 788-5456 7785 N. State
238 Arsenal Street, Watertown, NY Family Practice Office: (315) 782-6400 Fax: (315) 782-1330 Adult Office: (315) 782-9903 Fax: (315) 788-0087 Dental Office: (315) 788-9834 Fax: (315) 788-5456 7785 N. State
FAMILY ESTATE PLAN QUESTIONNAIRE
 FAMILY ESTATE PLAN QUESTIONNAIRE This information will assist us in counseling you regarding your estate plan. Please complete this questionnaire and return it to us. If more space is needed, attach additional
FAMILY ESTATE PLAN QUESTIONNAIRE This information will assist us in counseling you regarding your estate plan. Please complete this questionnaire and return it to us. If more space is needed, attach additional
HFM/CASCADE DENTAL PLAN APPLICATION ADULT APPLICANT (age 18 and over)
") HFM/CASCADE DENTAL PLAN APPLICATION ADULT APPLICANT (age 18 and over) SECTION 1: INSTRUCTIONS 1. This form is for use by adults wishing to apply for Delta Dental benefits through the HFM/Cascade Dental
HFM/CASCADE DENTAL PLAN APPLICATION ADULT APPLICANT (age 18 and over) SECTION 1: INSTRUCTIONS 1. This form is for use by adults wishing to apply for Delta Dental benefits through the HFM/Cascade Dental
Linda Smoling Moore, Ph.D. Licensed Psychologist
 Linda Smoling Moore, Ph.D. Licensed Psychologist 5601 River Road, Suite C-19 301-654-4320 Bethesda, Maryland 20816 Fax: 301-598-3947 PSYCHOTHERAPIST-PATIENT SERVICES AGREEMENT Welcome to my practice. This
Linda Smoling Moore, Ph.D. Licensed Psychologist 5601 River Road, Suite C-19 301-654-4320 Bethesda, Maryland 20816 Fax: 301-598-3947 PSYCHOTHERAPIST-PATIENT SERVICES AGREEMENT Welcome to my practice. This
(Furtherance of Autism with Intervention, Treatment, and Health services) F.A.I.T.H. is all you need!!! ASSIGNMENT OF BENEFITS AND FINANCIAL AGREEMENT
 F.A.I.T.H. is all you need!!! ASSIGNMENT OF BENEFITS AND FINANCIAL AGREEMENT") F.A.I.T.H. is all you need Client name : Insurance Company: Eligibility Dates/Number of sessions: Co-pay per visit: Deductible: ASSIGNMENT OF BENEFITS AND FINANCIAL AGREEMENT Cost-share per visit: Other:
F.A.I.T.H. is all you need Client name : Insurance Company: Eligibility Dates/Number of sessions: Co-pay per visit: Deductible: ASSIGNMENT OF BENEFITS AND FINANCIAL AGREEMENT Cost-share per visit: Other:
WELCOME TO KAYAL ORTHOPAEDIC CENTER, P.C.
 WELCOME TO KAYAL ORTHOPAEDIC CENTER, P.C. PATIENT S NAME: TODAY S DATE: E-MAIL ADDRESS: PATIENT S DATE OF BIRTH: BRIEFLY DESCRIBE THE REASON FOR TODAY S VISIT DATE OF ONSET OR INJURY: IS TODAY S VISIT
WELCOME TO KAYAL ORTHOPAEDIC CENTER, P.C. PATIENT S NAME: TODAY S DATE: E-MAIL ADDRESS: PATIENT S DATE OF BIRTH: BRIEFLY DESCRIBE THE REASON FOR TODAY S VISIT DATE OF ONSET OR INJURY: IS TODAY S VISIT
Special Needs Planning Information Guide
 Special Needs Planning Information Guide We are a full service special needs planning firm focusing on families who have a loved one with special needs prepare for their care, supervision, and quality
Special Needs Planning Information Guide We are a full service special needs planning firm focusing on families who have a loved one with special needs prepare for their care, supervision, and quality
Would you like to receive s with special offers from Carolina Vein Center? yes no
 Carolina Vein Center Patient Information Name: Date: Address: Home Phone: City: State: Zip: Work Phone: SS#: Marital Status: Occupation: Date of Birth: _ Cell Phone: Emergency Contact: E-Mail: Emergency
Carolina Vein Center Patient Information Name: Date: Address: Home Phone: City: State: Zip: Work Phone: SS#: Marital Status: Occupation: Date of Birth: _ Cell Phone: Emergency Contact: E-Mail: Emergency
for Medicaid trusts. Medicaid qualifying trusts (MQTs). Other trusts.
. Other trusts.") BEM 401 1 of 18 TRUSTS - MA DEPARTMENT POLICY MA Only This item contains Medicaid policy for trusts. The item is divided into three parts: Medicaid trusts. Medicaid qualifying trusts (MQTs). Other trusts.
BEM 401 1 of 18 TRUSTS - MA DEPARTMENT POLICY MA Only This item contains Medicaid policy for trusts. The item is divided into three parts: Medicaid trusts. Medicaid qualifying trusts (MQTs). Other trusts.
WELCOME TO OUR OFFICE. Patient s Name: Today s Date: First Middle Last. Home Address: City: State: Zip: Telephone: Home ( ) Cellular: ( ) Work: ( )
 Cellular: ( ) Work: ( )") WELCOME TO OUR OFFICE Patient s Name: Today s Date: First Middle Last Home Address: City: State: Zip: Telephone: Home ( ) Cellular: ( ) Work: ( ) Email: Personal Work DOB: Age: SSN#: Ethnic Background:
WELCOME TO OUR OFFICE Patient s Name: Today s Date: First Middle Last Home Address: City: State: Zip: Telephone: Home ( ) Cellular: ( ) Work: ( ) Email: Personal Work DOB: Age: SSN#: Ethnic Background:
The Arc of New Mexico POOLED MASTER TRUST I JOINDER AGREEMENT
 The Arc of New Mexico POOLED MASTER TRUST I JOINDER AGREEMENT This is a legal document. You are encouraged to seek independent, professional advice before signing. The undersigned hereby enrolls in, adopts
The Arc of New Mexico POOLED MASTER TRUST I JOINDER AGREEMENT This is a legal document. You are encouraged to seek independent, professional advice before signing. The undersigned hereby enrolls in, adopts
Accident Benefits Claim Instructions
 Claim Instructions Your Accident Benefit Claim This packet contains the forms necessary to apply for. Every space on these forms should be filled in to avoid delay in processing your application. If a
Claim Instructions Your Accident Benefit Claim This packet contains the forms necessary to apply for. Every space on these forms should be filled in to avoid delay in processing your application. If a
Successor Trustee Handbook
 TO: The Successor Trustees You are probably now taking over as the Successor Trustee for the Trustmaker. We have prepared this handbook to give you some general instructions and ideas of the job you are
TO: The Successor Trustees You are probably now taking over as the Successor Trustee for the Trustmaker. We have prepared this handbook to give you some general instructions and ideas of the job you are
PLEASE READ BEFORE COMPLETING THE JOINDER AGREEMENT
 PLEASE READ BEFORE COMPLETING THE JOINDER AGREEMENT The following is information to consider when completing a Trust IV Joinder Agreement for trust subaccounts funded with the Beneficiary's own money such
PLEASE READ BEFORE COMPLETING THE JOINDER AGREEMENT The following is information to consider when completing a Trust IV Joinder Agreement for trust subaccounts funded with the Beneficiary's own money such
REQUEST FOR DISTRIBUTION OF BENEFITS
 The Liberty National Life Insurance Company Defined Contribution Plan REQUEST FOR DISTRIBUTION OF BENEFITS INSTRUCTlONS: 1. Read the Retirement Annuity Explanation. 2. Read the Special Tax Notice Regarding
The Liberty National Life Insurance Company Defined Contribution Plan REQUEST FOR DISTRIBUTION OF BENEFITS INSTRUCTlONS: 1. Read the Retirement Annuity Explanation. 2. Read the Special Tax Notice Regarding
LOCAL UNION 903 I.B.E.W. PENSION PLAN {the Plan}
 LOCAL UNION 903 I.B.E.W. PENSION PLAN {the Plan} 414(K) ACCOUNT WITHDRAWAL PROCEDURE WITHDRAWAL BEFORE RETIREMENT Fund Office Alabama Administrators 1717 Old Shell Road Mobile, AL 36604 (251) 478-5412
LOCAL UNION 903 I.B.E.W. PENSION PLAN {the Plan} 414(K) ACCOUNT WITHDRAWAL PROCEDURE WITHDRAWAL BEFORE RETIREMENT Fund Office Alabama Administrators 1717 Old Shell Road Mobile, AL 36604 (251) 478-5412
PLEASE READ BEFORE COMPLETING THE JOINDER AGREEMENT
 JOINDER PLEASE READ BEFORE COMPLETING THE JOINDER AGREEMENT The following is information to consider when completing a Trust Joinder Agreement for Trust Sub- Accounts funded with the Beneficiary s own
JOINDER PLEASE READ BEFORE COMPLETING THE JOINDER AGREEMENT The following is information to consider when completing a Trust Joinder Agreement for Trust Sub- Accounts funded with the Beneficiary s own
New York Life Insurance Company
 New York Life Insurance Company PO Box 30713 Tampa FL 33630-3713 Dear Beneficiary: Please accept our condolences on your recent loss. We understand this is a difficult time, and we hope that we can alleviate
New York Life Insurance Company PO Box 30713 Tampa FL 33630-3713 Dear Beneficiary: Please accept our condolences on your recent loss. We understand this is a difficult time, and we hope that we can alleviate
ESTATE PLANNING AND WILL INFORMATION FORM
 ESTATE PLANNING AND WILL INFORMATION FORM ROLSCH LAW OFFICES 423-3RD AVENUE SE P.O. BOX 189 ROCHESTER, MN 55903 PHONE: (507) 280-1943 FAX: (507) 280-4283 WHEN YOU HAVE COMPLETED THIS FORM, please return
ESTATE PLANNING AND WILL INFORMATION FORM ROLSCH LAW OFFICES 423-3RD AVENUE SE P.O. BOX 189 ROCHESTER, MN 55903 PHONE: (507) 280-1943 FAX: (507) 280-4283 WHEN YOU HAVE COMPLETED THIS FORM, please return
Christina Agustin, MD Board Certified in Adult Psychiatry 1 Lake Bellevue Drive, Suite 101 Bellevue, WA Phone Fax:
 Christina Agustin, MD Board Certified in Adult Psychiatry 1 Lake Bellevue Drive, Suite 101 Bellevue, WA 98005 Phone 425-301-9869 Fax: 866-546-1618 Welcome to my practice. I look forward to meeting with
Christina Agustin, MD Board Certified in Adult Psychiatry 1 Lake Bellevue Drive, Suite 101 Bellevue, WA 98005 Phone 425-301-9869 Fax: 866-546-1618 Welcome to my practice. I look forward to meeting with
Planning for Special Needs and Ohio s STABLE Account. Presented by Logan Philipps, Esq.
 Planning for Special Needs and Ohio s STABLE Account Presented by Logan Philipps, Esq. Concerns for Families Everything will be fine as long as my child dies before I do. Will my typical child have to
Planning for Special Needs and Ohio s STABLE Account Presented by Logan Philipps, Esq. Concerns for Families Everything will be fine as long as my child dies before I do. Will my typical child have to
COMMUNITY FUND MANAGEMENT FOUNDATION MASTER TRUST MASTER TRUST SUB-ACCOUNT JOINDER AGREEMENT AND APPLICATION FOR ADMISSION AS GRANTOR
 COMMUNITY FUND MANAGEMENT FOUNDATION MASTER TRUST MASTER TRUST SUB-ACCOUNT JOINDER AGREEMENT AND APPLICATION FOR ADMISSION AS GRANTOR TO BE ADMINISTERED IN ACCORDANCE WITH THE TERMS AND CONDITIONS OF THE
COMMUNITY FUND MANAGEMENT FOUNDATION MASTER TRUST MASTER TRUST SUB-ACCOUNT JOINDER AGREEMENT AND APPLICATION FOR ADMISSION AS GRANTOR TO BE ADMINISTERED IN ACCORDANCE WITH THE TERMS AND CONDITIONS OF THE
A brief guide to our Flexible Trust
 A brief guide to our Flexible Trust A Trust is a legal document and Trust Laws are complex, often with a lot of confusing legal jargon. At British Seniors we pride ourselves on doing the right thing by
A brief guide to our Flexible Trust A Trust is a legal document and Trust Laws are complex, often with a lot of confusing legal jargon. At British Seniors we pride ourselves on doing the right thing by
New Patient Information Form
 PATIENT INFORMATION New Patient Information Form Patient s Patient s Preferred Name Middle Initial Date of Birth SSN# Primary Language YES NO Email Address Race/Ethnicity Is patient of Hispanic Origin?
PATIENT INFORMATION New Patient Information Form Patient s Patient s Preferred Name Middle Initial Date of Birth SSN# Primary Language YES NO Email Address Race/Ethnicity Is patient of Hispanic Origin?
2) An estate represents a deceased person's assets after all debts are paid. Answer: TRUE Diff: 1 Question Status: Previous edition
 An estate represents a deceased person's assets after all debts are paid. Answer: TRUE Diff: 1 Question Status: Previous edition") Personal Finance, 6e (Madura) Chapter 20 Estate Planning 20.1 Purpose of a Will 1) Two key goals of estate planning are to ensure that your estate passes to the proper beneficiaries and to ensure that
Personal Finance, 6e (Madura) Chapter 20 Estate Planning 20.1 Purpose of a Will 1) Two key goals of estate planning are to ensure that your estate passes to the proper beneficiaries and to ensure that
How to Prepare a Last Will and Testament
 How to Prepare a Last Will and Testament The Simplest Way The simplest way to ensure that your funds, property and personal effects will be distributed after your death according to your wishes is to prepare
How to Prepare a Last Will and Testament The Simplest Way The simplest way to ensure that your funds, property and personal effects will be distributed after your death according to your wishes is to prepare
PSYCHOLOGICAL HEALTH ASSOCIATES, PA PSYCHOLOGIST-PATIENT SERVICES.
 PSYCHOLOGICAL HEALTH ASSOCIATES, PA PSYCHOLOGIST-PATIENT SERVICES. Welcome to my practice. I am happy to have you as a client. This document (the Agreement) contains important information about my professional
PSYCHOLOGICAL HEALTH ASSOCIATES, PA PSYCHOLOGIST-PATIENT SERVICES. Welcome to my practice. I am happy to have you as a client. This document (the Agreement) contains important information about my professional
GOALS OF ESTATE PLANNING 12/12/2011 SUCCESSION PLANNING SUCCESSION PLANNING IMPEDIMENTS TO ACHIEVING ESTATE PLANNING GOALS
 SUCCESSION PLANNING Why is succession planning so important Avoid sacrificing land for liquidity http://bit.ly/vwx5jn SUCCESSION PLANNING 1. Discuss your vision and goals for the land with your spouse
SUCCESSION PLANNING Why is succession planning so important Avoid sacrificing land for liquidity http://bit.ly/vwx5jn SUCCESSION PLANNING 1. Discuss your vision and goals for the land with your spouse
FLORIDA MEDICAL CLINIC, P.A. Your Life, Our Specialty
 FLORIDA MEDICAL CLINIC, P.A. Your Life, Our Specialty Consent for Purposes of Treatment, Payment and Health Care Operations I consent to the use or disclosure of my protected health information by Florida
FLORIDA MEDICAL CLINIC, P.A. Your Life, Our Specialty Consent for Purposes of Treatment, Payment and Health Care Operations I consent to the use or disclosure of my protected health information by Florida
2337 TRUST PROPERTY OBRA 93
 2337 TRUST PROPERTY OBRA 93 POLICY STATEMENT Effective with all trusts created on or after 8-11-93 by the A/R or someone acting on behalf of the A/R, the corpus of a trust is either (1) a resource available
2337 TRUST PROPERTY OBRA 93 POLICY STATEMENT Effective with all trusts created on or after 8-11-93 by the A/R or someone acting on behalf of the A/R, the corpus of a trust is either (1) a resource available
ACCIDENTAL DEATH WHOLE LIFE PROTECTOR
 ACCIDENTAL DEATH WHOLE LIFE PROTECTOR Regular Mail: United Home Life Insurance Company P.O. Box 7192 Indianapolis, IN 46207-7192 FAX Number: 317-692-7711 Telephone: 800-428-3001 # pages including cover
ACCIDENTAL DEATH WHOLE LIFE PROTECTOR Regular Mail: United Home Life Insurance Company P.O. Box 7192 Indianapolis, IN 46207-7192 FAX Number: 317-692-7711 Telephone: 800-428-3001 # pages including cover
MILLE LACS BAND OF OJIBWE
 Name: Suffix: SS#: - - Last Name First Name Middle Initial DOB: Sex: M F Marital Status: Address: Single Married Divorced Never Married Separated Unknown Widow/Widower Street City State Zip County Home
Name: Suffix: SS#: - - Last Name First Name Middle Initial DOB: Sex: M F Marital Status: Address: Single Married Divorced Never Married Separated Unknown Widow/Widower Street City State Zip County Home
ESTATE PLANNING DICTIONARY
 ESTATE PLANNING DICTIONARY Administrator For estates administered prior to April 1, 2012, the fiduciary appointed by the Probate Court to settle your estate if you die without a Will (intestate). Attorney-in-fact
ESTATE PLANNING DICTIONARY Administrator For estates administered prior to April 1, 2012, the fiduciary appointed by the Probate Court to settle your estate if you die without a Will (intestate). Attorney-in-fact
Estate Planning Basics
 Your Retirement Advisor 508-798-5115 lynnt@yourretirementadvisor.com www.yourretirementadvisor.com Estate Planning Basics Page 1 of 12, see disclaimer on final page What Is Estate Planning? Estate planning
Your Retirement Advisor 508-798-5115 lynnt@yourretirementadvisor.com www.yourretirementadvisor.com Estate Planning Basics Page 1 of 12, see disclaimer on final page What Is Estate Planning? Estate planning
WILLS. a. If you die without a will you forfeit your right to determine the distribution of your probate estate.
 WILLS 1. Do you need a will? a. If you die without a will you forfeit your right to determine the distribution of your probate estate. b. The State of Arkansas decides by statute how your estate is distributed.
WILLS 1. Do you need a will? a. If you die without a will you forfeit your right to determine the distribution of your probate estate. b. The State of Arkansas decides by statute how your estate is distributed.
Loan Distribution Form
 Loan Distribution Form READ THE ATTACHED IRS SPECIAL TAX NOTICE AND WRITTEN EXPLANATION OF QUALIFIED JOINT AND 50% CONTINGENT SUVIVIOR ANNUITY FORM OF BENEFIT BEFORE COMPLETING THIS FORM Please Note: Do
Loan Distribution Form READ THE ATTACHED IRS SPECIAL TAX NOTICE AND WRITTEN EXPLANATION OF QUALIFIED JOINT AND 50% CONTINGENT SUVIVIOR ANNUITY FORM OF BENEFIT BEFORE COMPLETING THIS FORM Please Note: Do
The Consumer s Guide to Special Needs Planning
 The Consumer s Guide to Special Needs Planning INCLUDING: How to provide for the present and future needs of a person with disabilities First-Party and Third-Party Special Needs Trusts The Role of the
The Consumer s Guide to Special Needs Planning INCLUDING: How to provide for the present and future needs of a person with disabilities First-Party and Third-Party Special Needs Trusts The Role of the
Full Representative Payee (Enrollment & 4 forms)
") P:(508) 794-9909 F:(888) 877-4420 689 Main Street Walpole, MA 02081 HelpMeBudget.org HelpMeBudgetStaff@Gmail.com Full Representative Payee (Enrollment & 4 forms) Checklist Complete our online enrollment
P:(508) 794-9909 F:(888) 877-4420 689 Main Street Walpole, MA 02081 HelpMeBudget.org HelpMeBudgetStaff@Gmail.com Full Representative Payee (Enrollment & 4 forms) Checklist Complete our online enrollment
Give the Gift That Truly Matters A Gift Towards a Child s Retirement
 Give the Gift That Truly Matters A Gift Towards a Child s Retirement When you create a RIC-E Trust, you contribute as little as $5,000, and you designate a child or grandchild to receive the money when
Give the Gift That Truly Matters A Gift Towards a Child s Retirement When you create a RIC-E Trust, you contribute as little as $5,000, and you designate a child or grandchild to receive the money when
I/We enclose a fully executed copy of the Trustee Amendment for your records. I/We would also like to provide you with the information listed below.
 Dear Fiduciary Support: I/We enclose a fully executed copy of the Trustee Amendment for your records. I/We would also like to provide you with the information listed below. 1. Choose one: I/We have already
Dear Fiduciary Support: I/We enclose a fully executed copy of the Trustee Amendment for your records. I/We would also like to provide you with the information listed below. 1. Choose one: I/We have already
JOINDER AGREEMENT FOR ARC-MN POOLED TRUST FOR A BENEFICIARY S ASSETS
 JOINDER AGREEMENT FOR ARC-MN POOLED TRUST FOR A BENEFICIARY S ASSETS This Joinder Agreement ( Agreement ) is by and between The Arc Minnesota ( Trustee ) and ( Grantor ) for the benefit of ( Beneficiary
JOINDER AGREEMENT FOR ARC-MN POOLED TRUST FOR A BENEFICIARY S ASSETS This Joinder Agreement ( Agreement ) is by and between The Arc Minnesota ( Trustee ) and ( Grantor ) for the benefit of ( Beneficiary
RE: Pension Application Member ID #: XXX-XX. Dear Participant,
 2357 59 th Street St. Louis, MO 63110 (314) 644-2777 ext. 3 1-800-489-0228 Fax: (314) 645-6226 RE: Pension Application Member ID #: XXX-XX Dear Participant, Congratulations! Our office was recently notified
2357 59 th Street St. Louis, MO 63110 (314) 644-2777 ext. 3 1-800-489-0228 Fax: (314) 645-6226 RE: Pension Application Member ID #: XXX-XX Dear Participant, Congratulations! Our office was recently notified
Welcome To Our Office
 Welcome To Our Office Since 1977 The Miami Counseling & Resource Center ( MCRC ) is a large, private Center that has been helping individuals, couples, and families in Miami for over 30 years, and we are
Welcome To Our Office Since 1977 The Miami Counseling & Resource Center ( MCRC ) is a large, private Center that has been helping individuals, couples, and families in Miami for over 30 years, and we are
BENEFICIARY STATEMENT INSTRUCTIONS
 Farm Bureau Life Insurance Company 5400 University Avenue West Des Moines, Iowa 50266-5997 800-247-4170 / FAX: 1-800-814-5561 BENEFICIARY STATEMENT INSTRUCTIONS INSTRUCTIONS FOR COMPLETION OF BENEFICIARY
Farm Bureau Life Insurance Company 5400 University Avenue West Des Moines, Iowa 50266-5997 800-247-4170 / FAX: 1-800-814-5561 BENEFICIARY STATEMENT INSTRUCTIONS INSTRUCTIONS FOR COMPLETION OF BENEFICIARY
JOINDER AGREEMENT FOR ARC-MN POOLED TRUST FOR A THIRD PARTY S ASSETS FOR THE BENEFIT OF A BENEFICIARY
 JOINDER AGREEMENT FOR ARC-MN POOLED TRUST FOR A THIRD PARTY S ASSETS FOR THE BENEFIT OF A BENEFICIARY This Joinder Agreement ( Agreement ) is by and between The Arc Minnesota ( Trustee ) and ( Grantor(s)
JOINDER AGREEMENT FOR ARC-MN POOLED TRUST FOR A THIRD PARTY S ASSETS FOR THE BENEFIT OF A BENEFICIARY This Joinder Agreement ( Agreement ) is by and between The Arc Minnesota ( Trustee ) and ( Grantor(s)
GENERAL INFORMATION. Our office is located on the southwest corner of Shaw Ave. and Teilman between Fruit and West.
 I would like to welcome you to my practice and am pleased to have you as a patient. I am providing you with this informational letter to help you understand how this office operates. Every effort will
I would like to welcome you to my practice and am pleased to have you as a patient. I am providing you with this informational letter to help you understand how this office operates. Every effort will
BENEFIT APPLICATION FORM
 BENEFIT APPLICATION FORM NAME OF APPLICANT PHONE NO. ( ) ADDRESS SOC. SEC. NO. NAME OF PARTICIPANT (If different from applicant) DATE OF BIRTH SOC. SEC. NO. Under and subject to the provisions of the HAWAII
BENEFIT APPLICATION FORM NAME OF APPLICANT PHONE NO. ( ) ADDRESS SOC. SEC. NO. NAME OF PARTICIPANT (If different from applicant) DATE OF BIRTH SOC. SEC. NO. Under and subject to the provisions of the HAWAII
MOSERS Continued Dependent Life Insurance for a Disabled Child Instructions
 Continued Dependent Life Insurance Instructions Your application for consists of four forms. Every space should be filled in to avoid delay in processing your application. If a section does not apply,
Continued Dependent Life Insurance Instructions Your application for consists of four forms. Every space should be filled in to avoid delay in processing your application. If a section does not apply,
Estate Planning, Medi-Cal, Advance Directives & Special Needs Trusts
 Estate Planning, Medi-Cal, Advance Directives & Special Needs Trusts B R U C E A. F E D E R, E S Q. K A T O, F E D E R & S U Z U K I, L L P 6 8 5 M A R K E T S T R E E T, S U I T E 5 4 0 S A N F R A N
Estate Planning, Medi-Cal, Advance Directives & Special Needs Trusts B R U C E A. F E D E R, E S Q. K A T O, F E D E R & S U Z U K I, L L P 6 8 5 M A R K E T S T R E E T, S U I T E 5 4 0 S A N F R A N
MEDICAID SPEND DOWN AND MEDICAID ELIGIBLE TRUSTS
 MEDICAID SPEND DOWN AND MEDICAID ELIGIBLE TRUSTS Medicare v. Medicaid Medicare is a single payer (government) medical system for those over 65, those who have been on Social Security Disability Insurance
MEDICAID SPEND DOWN AND MEDICAID ELIGIBLE TRUSTS Medicare v. Medicaid Medicare is a single payer (government) medical system for those over 65, those who have been on Social Security Disability Insurance
Statutory Scheme of Final Disposition Authority; 2011 Amendments
 INDIANA FUNERAL DIRECTORS ASSOCIATION 2011 District Meetings Disclaimer: It is always recommended that counsel be consulted regarding any individual or business planning decision. The information and/or
INDIANA FUNERAL DIRECTORS ASSOCIATION 2011 District Meetings Disclaimer: It is always recommended that counsel be consulted regarding any individual or business planning decision. The information and/or
Sheet Metal Workers Local Union No. 292 Annuity Fund Benefit Distribution Application. Application Checklist
 Sheet Metal Workers Local Union No. 292 Annuity Fund Benefit Distribution Application Application Checklist Please submit copies of the following documents with your application for benefits: Birth Certificate
Sheet Metal Workers Local Union No. 292 Annuity Fund Benefit Distribution Application Application Checklist Please submit copies of the following documents with your application for benefits: Birth Certificate
Cause No. Guardianship of: Guardian of the Person and Estate: Court-Ordered Instructions
 Cause No. Guardianship of: Guardian of the Person and Estate: Court-Ordered Instructions Thank you for accepting appointment as the Guardian of the Person and Estate of a minor or incapacitated individual
Cause No. Guardianship of: Guardian of the Person and Estate: Court-Ordered Instructions Thank you for accepting appointment as the Guardian of the Person and Estate of a minor or incapacitated individual
REAL ESTATE INFORMATION NEEDED BY McCORMICK COUNTY PROBATE COURT. Deed Book: Page: TMS#: Value: Deed Book: Page: TMS#: Value:
 REAL ESTATE INFORMATION NEEDED BY McCORMICK COUNTY PROBATE COURT List below property of: Decedent Deed Book: Page: TMS#: Value: Deed Book: Page: TMS#: Value: Deed Book: Page: TMS#: Value: Completed by:
REAL ESTATE INFORMATION NEEDED BY McCORMICK COUNTY PROBATE COURT List below property of: Decedent Deed Book: Page: TMS#: Value: Deed Book: Page: TMS#: Value: Deed Book: Page: TMS#: Value: Completed by:
Asset Protection. A planning, conversation, and resource guide
 Asset Protection A planning, conversation, and resource guide LOREM IPSUM A PLANNING, CONVERSATION, AND RESOURCE GUIDE Use this guide to help create a plan for protecting those you love and what you have.
Asset Protection A planning, conversation, and resource guide LOREM IPSUM A PLANNING, CONVERSATION, AND RESOURCE GUIDE Use this guide to help create a plan for protecting those you love and what you have.