Vendor Application Wholesaler / Distributor Checklist
|
|
|
- Mariah Casey
- 6 years ago
- Views:
Transcription
1 Vendor Application Wholesaler / Distributor Checklist Thank you for choosing to do business with HyGen Pharmaceuticals, Inc. Please take a few minutes to fill out and fax or scan and over the following items. Description Completed & Signed New Vendor Application Form Required Completely filled out. Completed & Signed Guaranty & Indemnification Form Required Completed & Signed Pharmaceutical Pedigree Agreement Required Copy of Resident State Wholesale License Required Copy of Washington State Wholesale License Required Copy of Federal DEA registration (if applicable) Copy of Resident State Controlled Substance License (if applicable) Copy of Most Recent Facility Inspection Reports (if applicable) Copy of VAWD Certificate (if applicable) List of Other State(s) of Licensure including Registration/Permit Numbers
2 New Vendor Application Form Company Information Legal Company Name: DBA: Year established: Ownership Type (Check One): Corporation Partnership Sole Proprietorship LLC Other: State of incorporation (if LLC or Corporation): Shipping Address: Billing Address: Office Toll Free: Remittance Address: Accounting Contact: Name: Sales Contact: Name: Company Contact & Title: Warehouse Contact: State Wholesale License #: Exp. Date: Federal DEA Lic#: Exp. Date: WA Out of State Wholesale License #: Exp. Date: Federal Tax ID #: Dunn & Bradstreet# Please list all owners with 10% or more ownership Terms: Credit Limit: HyGen Cust #:
3 Licensing When was the last inspection by the State Board of Pharmacy? Were any deficiencies noted? If so, have they been corrected? When was the last inspection by the DEA (if applicable)? Were any deficiencies noted? If so, have they been corrected? Has the company ever had any disciplinary actions by a local, state, or federal authority with regards to pharmaceutical storage, handling, and distribution? YES NO If yes, please explain: Facility What is the size of the facility (in sq. feet): Is the facility VAWD Certified? YES NO APPLIED If yes, please include a copy of VAWD License. Does the company have temperature and humidity monitoring equipment? YES Does the company record temperature and humidity readings? YES NO Does the company have adequate refrigeration equipment with temperature humidity monitoring in place for refrigerated pharmaceuticals? YES NO Does the company have a list of excluded vendors? YES NO Does the company have an Authorized Distributor list (AD list)? YES The undersigned certifies that all the information provided herein is true and correct. Further the company agrees to promptly notify HyGen Pharmaceuticals, Inc. if any of the information provided should change. The undersigned must be an officer/owner of the company. Date: Name: Title: Signature: NO NO
4 Guaranty & Indemnification Agreement It is both the desire and goal of HyGen Pharmaceuticals, Inc. (hereinafter "HyGen") to comply with all Federal State and local laws and to comply with applicable provisions of the Prescription Drug Marketing (hereinafter "PDMA") Act of 1987 including amendments of 1992 and all subsequent revisions, amendments, regulations and guidelines which have been promulgated by the Food and Drug Administration. Accordingly, HyGen requires that all vendors represent and warrant that the following statements are true and correct. 1. All products offered for sale to HyGen are owned free and clear of any encumbrances or restrictions on title at the time of said sale. In addition, all products offered for sale are not adulterated or misbranded within the meaning of the Food, Drug and Cosmetic Act and are not articles which may not be introduced into interstate commerce under the Act. 2. Any products offered for sale to HyGen have not been obtained through fraud, misrepresentation or concealment of any material facts. 3. That Vendor shall comply fully with all Federal, State and local laws applicable to the purchase, handling, sale or distribution of the products sold to HyGen. 4. That Vendor shall provide prompt notice to HyGen of any civil, criminal or administrative action by Federal, State or local authorities regarding the Vendor, its employees, or its officers with respect to alleged violations of Federal, State or local ordinances or regulations and to provide HyGen with full and complete information regarding the disposition of any such action. 5. That Vendor shall provide to HyGen a copy of the Vendor's Sales Tax Exemption Certificate, whether it be a resale certificate, blanket exemption or direct payment exemption, and to notify HyGen promptly of any changes which affects the Vendor s exemption status. 6. Vendor represents and warrants that it has authorized distribution status for product sold to HyGen or, for those products as to which it does not have authorized status shall establish such internal controls and maintain such records as will assure compliance with its obligations under this Agreement and permit it to maintain the appropriate paper trails and pedigrees which must be provided to HyGen with every sale of RX product to HyGen. 7. Any products offered for sale to HyGen have no restrictions on their sale to HyGen or their resale by HyGen. 8. Any products offered for sale to HyGen are not in violation of the PDMA of 1987, the PDMA Amendments of 1992, or any other Federal, State or local ordinance or regulation. 9. The Vendor, to the extent that the Vendor may lawfully do so, hereby consents to the exclusive jurisdiction of the Courts of the State of Washington and the United States District Court for the District of Washington, as well as to the jurisdiction of all Courts to which an appeal may be taken from such courts, for the purpose of any suit, action or other proceeding arising out of any of the creditor's obligations arising hereunder or with respect to the transactions contemplated hereby, and expressly waives any and an objections it or he may have as to venue, including, without limitation, the inconvenience of such forum, in any of such Courts. 10. Vendor shall provide to HyGen a list of all manufacturers with which Vendor has a direct status, as defined by PDMA. 11. Any products that are damaged in the course of shipment from Vendor to HyGen shall be the sole responsibility of Vendor. THE UNDERSIGNED VENDOR HEREBY CERTIFIES THAT THEY HAVE READ, UNDERSTAND AND AGREE TO THE ABOVE AND THAT THE STATEMENTS CONTAINED HEREIN ARE TRUE AND CORRECT AND THAT THEY ARE AUTHORIZED TO EXECUTE THIS AGREEMENT. BY: Signature: Print Name: Title: Company Name: Vendor s Federal Tax ID#: Date:
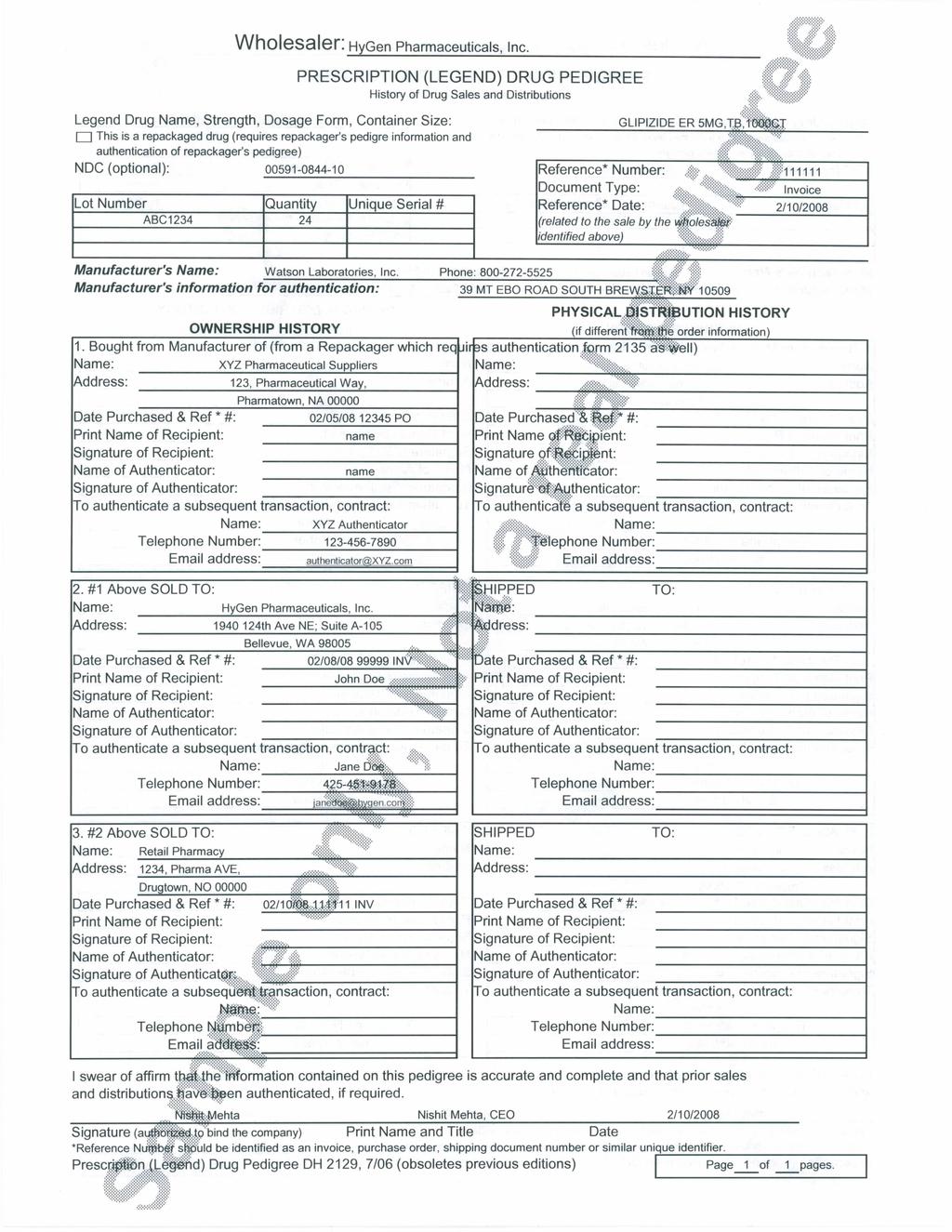
5 Pharmaceutical Pedigree Agreement Due to the recent discoveries of counterfeit product, HyGen Pharmaceuticals, Inc. is committed to insuring that the products that we represent were obtained with the highest integrity. Pursuant to section 503 (e) (1) of the Federal Food, Drug, and Cosmetic Act ( The Act ) as amended, 21 U.S.C. & 353 (e) (1) (vendor) hereby guarantees to HyGen Pharmaceuticals Inc. (1) That no article sold to HyGen Pharmaceuticals, Inc. (a) is adulterated or misbranded within the meaning of Act, 21 U.S.C. & 310 et seq., as amended; (b) is an article which may not, under the provisions of section 404, 505, or 512 of the Act be introduced in interstate commerce; (c) is an article which was re-imported in violation of section 801 (d) is a drug sample; or (e) is a drug that was previously sold to a hospital, health care entity or charitable organization, which may not, under the provision of section 503 (c) of the Act be sold, traded, purchased or otherwise exchanged; and (2) That it is an "Authorized Distributor of Record (ADR) for the following manufacturers (attach if necessary) subject to section 503 (b) of the Act: Manufacturer: Acct # Manufacturer: Acct# In the event the Vendor ceases to be an ADR for the above referenced manufacturers, OR if Vendor becomes an ADR for additional manufacturers Vendor agrees to provide prompt notice to HyGen Pharmaceuticals, Inc. of such change. Statement Identifying Pharmaceutical Sales (Pedigree/Paper Trail) (sample form included) must accompany all products sold to HyGen Pharmaceuticals, Inc. It may be shipped with product or faxed to us at. This listing MUST trace the product back to a verified distributor with dates of purchase for each transaction and completed physical addresses for all suppliers listed. The pedigrees that HyGen Pharmaceuticals, Inc. receives from it's non manufacturing vendors will be randomly verified/validated to ensure the integrity of the product it receives. If the pedigree is unable to be verified, HyGen Pharmaceuticals, Inc. reserves the right to send product back to vendor. Any product shipped to HyGen Pharmaceuticals, Inc. that does not include proper paperwork will be quarantined for 5 business days. Our receiving department will notify the vendor and request paperwork. If the proper invoice and pedigree are not received in by the 5th business day, the product will be sent back to vendor. If any of the vendors continually fail to provide the complete and acceptable paper work for any product shipped to them, their status with will be put on hold until that vendors complies with all paperwork requirements. Signature: Date: Company Name: Name of company Owner/Officer: Title:
6
FAIRFAX PHARMACEUTICAL WHOLESALER INC NEW CUSTOMER APPLICATION
 FAIRFAX PHARMACEUTICAL WHOLESALER INC NEW CUSTOMER APPLICATION PLEASE PRINT OR TYPE SECTION A- GENERAL INFORMATION Business/trade name: Business/trade address: SECTION B- FINANCIAL INFORMATION -Type of
FAIRFAX PHARMACEUTICAL WHOLESALER INC NEW CUSTOMER APPLICATION PLEASE PRINT OR TYPE SECTION A- GENERAL INFORMATION Business/trade name: Business/trade address: SECTION B- FINANCIAL INFORMATION -Type of
THANK YOU FOR YOUR INTEREST IN BILL HICKS & CO., LTD
 BILL HICKS & CO., LTD. Office: (763) 476-6200 15155 23 RD Avenue North Fax: (763) 476-8963 Minneapolis, Minnesota 55447-4740 Toll Free: (800) 223-0702 THANK YOU FOR YOUR INTEREST IN BILL HICKS & CO., LTD
BILL HICKS & CO., LTD. Office: (763) 476-6200 15155 23 RD Avenue North Fax: (763) 476-8963 Minneapolis, Minnesota 55447-4740 Toll Free: (800) 223-0702 THANK YOU FOR YOUR INTEREST IN BILL HICKS & CO., LTD
commercial credit application
 commercial credit application IRBY ELECTRICAL DISTRIBUTOR Please complete the following application in its entirety to ensure prompt processing of the account setup. You are welcome to email the final
commercial credit application IRBY ELECTRICAL DISTRIBUTOR Please complete the following application in its entirety to ensure prompt processing of the account setup. You are welcome to email the final
Account Manager: Legal Name of Firm. DBA Name of Parent Company (If subsidiary) Street: Business Mailing Address. Street: Business Shipping Address
 Street: Business Mailing Address. Street: Business Shipping Address") This agreement is made between CCM Inc Corporation, also referred to as CCM Inc, and the Customer completing this form. The Customer certifies that all information provided is true and correct. Customer
This agreement is made between CCM Inc Corporation, also referred to as CCM Inc, and the Customer completing this form. The Customer certifies that all information provided is true and correct. Customer
*SLA LICENSE SERIAL #: *NY STATE TAX ID #:
 SOUTHERN GLAZER S WINE & SPIRITS OF UPSTATE NEW YORK, LLC P.O. BOX 4705 SYRACUSE, NEW YORK 13221-4705 PHONE: (315) 428-2100 FAX: (315) 410-5463 ACCOUNT # For office use only APPLICATION AND CREDIT AGREEMENT
SOUTHERN GLAZER S WINE & SPIRITS OF UPSTATE NEW YORK, LLC P.O. BOX 4705 SYRACUSE, NEW YORK 13221-4705 PHONE: (315) 428-2100 FAX: (315) 410-5463 ACCOUNT # For office use only APPLICATION AND CREDIT AGREEMENT
Alabama State Board of Pharmacy New Wholesale Distribution Application
 Alabama State Board of Pharmacy New Wholesale Distribution Application Date Received Wholesale Distributor: A person other than a manufacturer, the co-licensed partner of a manufacturer, a third-party
Alabama State Board of Pharmacy New Wholesale Distribution Application Date Received Wholesale Distributor: A person other than a manufacturer, the co-licensed partner of a manufacturer, a third-party
AUTHORIZED DEALER REQUIREMENTS
 AUTHORIZED DEALER REQUIREMENTS Thank you for your interest in becoming a BOTE Board Dealer. We are pleased to extend the opportunity for you business to establish a dealer account with BOTE, LLC, DBA BOTE
AUTHORIZED DEALER REQUIREMENTS Thank you for your interest in becoming a BOTE Board Dealer. We are pleased to extend the opportunity for you business to establish a dealer account with BOTE, LLC, DBA BOTE
Alabama State Board of Pharmacy New Third-Party Logistics Application
 Alabama State Board of Pharmacy New Third-Party Logistics Application Date Received Third-Party Logistics Provider: An entity that provides or coordinates warehousing or other logistics services of a product
Alabama State Board of Pharmacy New Third-Party Logistics Application Date Received Third-Party Logistics Provider: An entity that provides or coordinates warehousing or other logistics services of a product
Name of Individual or Legal Entity Responsible for Payment. City State Zip City State Zip. Phone Number Fax Number Phone Number Fax Number
 2801 Horace Shepard Drive Dothan, AL 36303 1. Account Information APPLICATION FOR NEW ACCOUNT The following is an application for credit with ONCOLOGY SUPPLY, also known as creditor within the general
2801 Horace Shepard Drive Dothan, AL 36303 1. Account Information APPLICATION FOR NEW ACCOUNT The following is an application for credit with ONCOLOGY SUPPLY, also known as creditor within the general
INFUSED ONCOLOGY PRODUCT RETURNS POLICY EARLY RETURNS PROGRAM
 INFUSED ONCOLOGY PRODUCT RETURNS POLICY EARLY RETURNS PROGRAM Effective Date: January 2, 2017 The purpose of the Infused Oncology Product Returns Policy Early Returns Program ( Policy ) is to allow Health
INFUSED ONCOLOGY PRODUCT RETURNS POLICY EARLY RETURNS PROGRAM Effective Date: January 2, 2017 The purpose of the Infused Oncology Product Returns Policy Early Returns Program ( Policy ) is to allow Health
FRESENIUS KABI USA, LLC GENERAL TERMS AND CONDITIONS FOR THE SUPPLY OF GOODS AND SERVICES
 FRESENIUS KABI USA, LLC GENERAL TERMS AND CONDITIONS FOR THE SUPPLY OF GOODS AND SERVICES 1. General Terms: These General Terms and Conditions shall apply to and be incorporated by this reference in all
FRESENIUS KABI USA, LLC GENERAL TERMS AND CONDITIONS FOR THE SUPPLY OF GOODS AND SERVICES 1. General Terms: These General Terms and Conditions shall apply to and be incorporated by this reference in all
Welcome to Monoprice, Inc.
 Welcome to Monoprice, Inc. Enclosed is Monoprice, Inc. Account Application Form. Please complete the application form and send it back to our sales department. Once you have become our customer, you can
Welcome to Monoprice, Inc. Enclosed is Monoprice, Inc. Account Application Form. Please complete the application form and send it back to our sales department. Once you have become our customer, you can
RULES OF THE TENNESSEE BOARD OF PHARMACY CHAPTER MANUFACTURERS, OUTSOURCING FACILITIES, OXYGEN SUPPLIERS AND WHOLESALERS/DISTRIBUTORS
 RULES OF THE TENNESSEE BOARD OF PHARMACY CHAPTER 1140-09 MANUFACTURERS, OUTSOURCING FACILITIES, OXYGEN SUPPLIERS AND TABLE OF CONTENTS 1140-09-.01 Manufacturer, Outsourcing Facility, Oxygen 1140-09-.04
RULES OF THE TENNESSEE BOARD OF PHARMACY CHAPTER 1140-09 MANUFACTURERS, OUTSOURCING FACILITIES, OXYGEN SUPPLIERS AND TABLE OF CONTENTS 1140-09-.01 Manufacturer, Outsourcing Facility, Oxygen 1140-09-.04
Alaska Ship Supply Dutch Harbor / Captains Bay A division of Western Pioneer, Inc.
 Alaska Ship Supply Dutch Harbor / Captains Bay A division of Western Pioneer, Inc. Corporate Office PO Box 70438 Seattle, WA 98127-0438 (206) 789-1930 (800) 426-6783 Fax (206) 784-8348 COMMERCIAL BUSINESS
Alaska Ship Supply Dutch Harbor / Captains Bay A division of Western Pioneer, Inc. Corporate Office PO Box 70438 Seattle, WA 98127-0438 (206) 789-1930 (800) 426-6783 Fax (206) 784-8348 COMMERCIAL BUSINESS
APPLICATION FOR BUSINESS CREDIT
 _. Return Completed Application to: Pike Industries, Inc. 3 Eastgate Park Road Belmont, NH 03220 Phone: 603.527.5100 Fax: 603.527.5101 Email: r1arremit@pikeindustries.com APPLICATION FOR BUSINESS CREDIT
_. Return Completed Application to: Pike Industries, Inc. 3 Eastgate Park Road Belmont, NH 03220 Phone: 603.527.5100 Fax: 603.527.5101 Email: r1arremit@pikeindustries.com APPLICATION FOR BUSINESS CREDIT
FleetPride, Inc. Standard Terms and Conditions of Purchase
 FleetPride, Inc. 1. Terms of Agreement: The following terms and conditions of sale (these Standard Terms and Conditions ) contain general provisions applicable to all FleetPride, Inc. ( FleetPride ) supply
FleetPride, Inc. 1. Terms of Agreement: The following terms and conditions of sale (these Standard Terms and Conditions ) contain general provisions applicable to all FleetPride, Inc. ( FleetPride ) supply
Avella Wholesale, Inc.
 Credit Application Form Applicant Information Applicant Name: Address: Company Information Company Name: DBA Name (If Applicable): Company Address: Tax ID (FEINISSN): Billing Contact: Banking Information
Credit Application Form Applicant Information Applicant Name: Address: Company Information Company Name: DBA Name (If Applicable): Company Address: Tax ID (FEINISSN): Billing Contact: Banking Information
Institutional Investor Waiver Application Form
 MARYLAND STATE LOTTERY COMMISSION 1800 Washington Blvd., Suite 330, Baltimore, Maryland 21230 Institutional Investor Waiver Application Form Institutional Investor: Applicant: VLT Form 1009 (Rev June 2011)
MARYLAND STATE LOTTERY COMMISSION 1800 Washington Blvd., Suite 330, Baltimore, Maryland 21230 Institutional Investor Waiver Application Form Institutional Investor: Applicant: VLT Form 1009 (Rev June 2011)
State of Florida Department of Business and Professional Regulation Division of Drugs, Devices, and Cosmetics
 State of Florida Department of Business and Professional Regulation Division of Drugs, Devices, and Cosmetics Application for a Restricted Prescription Drug Distributor Health Care Entity Form.: DBPR-DDC-207
State of Florida Department of Business and Professional Regulation Division of Drugs, Devices, and Cosmetics Application for a Restricted Prescription Drug Distributor Health Care Entity Form.: DBPR-DDC-207
Welcome to Ariola Imports Miami!
 Welcome to Ariola Imports Miami! Please find the attached forms in order to enter your business in our system, and in order to establish a line of credit with our company. We ask you to please complete
Welcome to Ariola Imports Miami! Please find the attached forms in order to enter your business in our system, and in order to establish a line of credit with our company. We ask you to please complete
7/14/16. Hendry County Purchase Order Terms and Conditions
 Hendry County Purchase Order Terms and Conditions 1. Offer The order set forth in the Purchase Order is subject to cancellation by HENDRY COUNTY without notice if not accepted by VENDOR within fourteen
Hendry County Purchase Order Terms and Conditions 1. Offer The order set forth in the Purchase Order is subject to cancellation by HENDRY COUNTY without notice if not accepted by VENDOR within fourteen
FAR EAST BROKERS, INC. PURCHASE ORDER TERMS AND CONDITIONS
 1. ACCEPTANCE a. By accepting this order for products, Supplier accepts all terms and conditions set forth by FAR EAST BROKERS, INC. ( Buyer ) on this Purchase Order ( Order or Agreement ), whether printed
1. ACCEPTANCE a. By accepting this order for products, Supplier accepts all terms and conditions set forth by FAR EAST BROKERS, INC. ( Buyer ) on this Purchase Order ( Order or Agreement ), whether printed
SERVICES USA. Contents: Requirements Checklist: Application Shipping Schedule Disclosure Page Credit Card Authorization Terms & Conditions
 SERVICES USA CUSTOMER APPLICATION Contents: Application Shipping Schedule Disclosure Page Credit Card Authorization Terms & Conditions Requirements Checklist: Complete pages 2 5 and return Return copy
SERVICES USA CUSTOMER APPLICATION Contents: Application Shipping Schedule Disclosure Page Credit Card Authorization Terms & Conditions Requirements Checklist: Complete pages 2 5 and return Return copy
Co-Applicant. Phone. Fax. Business Information
 Applicant Legal Business List all trade names and D.B.A. if applicable Parent if applicant is a subsidiary Amount of Credit Requested: Will you furnish a financial statement upon request? Purchase Order
Applicant Legal Business List all trade names and D.B.A. if applicable Parent if applicant is a subsidiary Amount of Credit Requested: Will you furnish a financial statement upon request? Purchase Order
THE STANDARD VENDOR APPOINTMENT AGREEMENT FOR PRODUCTS TO BE SOLD THROUGH [WEBSITE]
![THE STANDARD VENDOR APPOINTMENT AGREEMENT FOR PRODUCTS TO BE SOLD THROUGH [WEBSITE]](/thumbs/85/92088699.jpg "THE STANDARD VENDOR APPOINTMENT AGREEMENT FOR PRODUCTS TO BE SOLD THROUGH [WEBSITE]") THE STANDARD VENDOR APPOINTMENT AGREEMENT FOR PRODUCTS TO BE SOLD THROUGH [WEBSITE] This Standard Vendor Appointment Agreement (the Agreement ) is by and between [NAME OF COMPANY] (that owns and controls
THE STANDARD VENDOR APPOINTMENT AGREEMENT FOR PRODUCTS TO BE SOLD THROUGH [WEBSITE] This Standard Vendor Appointment Agreement (the Agreement ) is by and between [NAME OF COMPANY] (that owns and controls
CORRESPONDENT LENDING APPLICATION PACKET CHECKLIST. Required CMG Forms: *Note: Signature stamps, digital signatures and typed initials not accepted
 Minimum Requirements: CORRESPONDENT LENDING APPLICATION PACKET CHECKLIST Length of time the company has been in business - 2 years Length of time with banking experience 1 year Minimum net worth - $2 Million
Minimum Requirements: CORRESPONDENT LENDING APPLICATION PACKET CHECKLIST Length of time the company has been in business - 2 years Length of time with banking experience 1 year Minimum net worth - $2 Million
State of Florida Department of Business and Professional Regulation Division of Drugs, Devices and Cosmetics
 State of Florida Department of Business and Professional Regulation Division of Drugs, Devices and Cosmetics Application for Veterinary Prescription Drug Wholesale Distributor Permit Form.: DBPR-DDC-216
State of Florida Department of Business and Professional Regulation Division of Drugs, Devices and Cosmetics Application for Veterinary Prescription Drug Wholesale Distributor Permit Form.: DBPR-DDC-216
State of Florida Department of Business and Professional Regulation Division of Drugs, Devices, and Cosmetics
 State of Florida Department of Business and Professional Regulation Division of Drugs, Devices, and Cosmetics Application for a Restricted Prescription Drug Distributor Government Programs Form.: DBPR-DDC-211
State of Florida Department of Business and Professional Regulation Division of Drugs, Devices, and Cosmetics Application for a Restricted Prescription Drug Distributor Government Programs Form.: DBPR-DDC-211
PRACTITIONER COMPLAINT FORM
 PRACTITIONER COMPLAINT FORM You may use this form to file a complaint against a dentist or dental hygienist. Your complaint may be disclosed to members, employees and consultants of the Board of Dental
PRACTITIONER COMPLAINT FORM You may use this form to file a complaint against a dentist or dental hygienist. Your complaint may be disclosed to members, employees and consultants of the Board of Dental
CUSTOMER CREDIT APPLICATION
 CREDIT LIMIT REQUEST: $ CUSTOMER CREDIT APPLICATION Date: Customer warrants that the following information is accurate and complete: (Attach additional sheets as needed) Name of Customer (Legal Name) Trade
CREDIT LIMIT REQUEST: $ CUSTOMER CREDIT APPLICATION Date: Customer warrants that the following information is accurate and complete: (Attach additional sheets as needed) Name of Customer (Legal Name) Trade
ATTACHMENT B PHARMACY CREDENTIALING FORM
 ATTACHMENT B PHARMACY CREDENTIALING FORM Thank you for your continued interest in the WellDyneRx Pharmacy Network. Please complete this form in its entirety to ensure continued network participation. If
ATTACHMENT B PHARMACY CREDENTIALING FORM Thank you for your continued interest in the WellDyneRx Pharmacy Network. Please complete this form in its entirety to ensure continued network participation. If
DISCOUNT LINE APPLICATION
 12130 Hempstead Road, Houston, Texas 77092 Telephone: (713) 235-8800 Fax: (713) 232-2542 DISCOUNT LINE APPLICATION COMPANY INFORMATION Exact legal name of business Trade Names (Assumed Names) within last
12130 Hempstead Road, Houston, Texas 77092 Telephone: (713) 235-8800 Fax: (713) 232-2542 DISCOUNT LINE APPLICATION COMPANY INFORMATION Exact legal name of business Trade Names (Assumed Names) within last
PHARMACEUTICAL PRODUCT PURCHASE ORDER TERMS AND CONDITIONS (Rev. 2/26/16) **READ CAREFULLY**
 **READ CAREFULLY**") 1. Definitions. PHARMACEUTICAL PRODUCT PURCHASE ORDER TERMS AND CONDITIONS (Rev. 2/26/16) **READ CAREFULLY** As used in these Terms and Conditions, Vendor means the seller specified in the Master Pharmaceutical
1. Definitions. PHARMACEUTICAL PRODUCT PURCHASE ORDER TERMS AND CONDITIONS (Rev. 2/26/16) **READ CAREFULLY** As used in these Terms and Conditions, Vendor means the seller specified in the Master Pharmaceutical
Purchase Order Financing Application
 Purchase Order Financing Application Requested Facility Size $ Referred by: Projected Annual Sales: $ Current Amount of Open A/R: $ GENERAL BUSINESS INFORMATION Legal Name(s) of Business: Trade Name(s)
Purchase Order Financing Application Requested Facility Size $ Referred by: Projected Annual Sales: $ Current Amount of Open A/R: $ GENERAL BUSINESS INFORMATION Legal Name(s) of Business: Trade Name(s)
IMS Company Terms and Conditions of Sale
 IMS Company Terms and Conditions of Sale Seller s Terms and Conditions of Sale apply to all purchases made by Buyer from Seller and all Invoices, emails, packing lists, or any other method of confirming
IMS Company Terms and Conditions of Sale Seller s Terms and Conditions of Sale apply to all purchases made by Buyer from Seller and all Invoices, emails, packing lists, or any other method of confirming
CORROSEAL DEALER PROGRAM. Policies & Procedures
 CORROSEAL DEALER PROGRAM Policies & Procedures CREDIT TERMS FOR NEW DEALER OPENING ORDERS All credit and credit limits must be pre-approved by the Rodda Paint Credit Manager prior to negotiating a buying
CORROSEAL DEALER PROGRAM Policies & Procedures CREDIT TERMS FOR NEW DEALER OPENING ORDERS All credit and credit limits must be pre-approved by the Rodda Paint Credit Manager prior to negotiating a buying
*NOTIFY THE DEPARTMENT IN WRITING OF ANY UPDATES
 APPLICATION FOR A PERMIT UNDER CHAPTER 499, FLORIDA STATUTES Florida Department of Business and Professional Regulation Drugs, Devices, and Cosmetics Program 1940 North Monroe Street, Tallahassee FL 323990783
APPLICATION FOR A PERMIT UNDER CHAPTER 499, FLORIDA STATUTES Florida Department of Business and Professional Regulation Drugs, Devices, and Cosmetics Program 1940 North Monroe Street, Tallahassee FL 323990783
New Customer Package. Credit Application Contact Sheet Insurance Requirements (with example)
") New Customer Package Credit Application Contact Sheet Insurance Requirements (with example) Please fill out the downloaded forms and provide a certificate of insurance complying with all of the requirements
New Customer Package Credit Application Contact Sheet Insurance Requirements (with example) Please fill out the downloaded forms and provide a certificate of insurance complying with all of the requirements
ATLANTIC CONCRETE PRODUCTS, INC.
 P.O. Box 129 Tullytown, PA 19007-0098 Tel.(215) 945-5600 Fax (215) 945-5016 CREDIT APPLICATION DATE: TOTAL PAGES: 1 of 5 TO: FROM: Steve Schlussel Accts Receivable Mgr COMPANY: COMPANY: Atlantic Concrete
P.O. Box 129 Tullytown, PA 19007-0098 Tel.(215) 945-5600 Fax (215) 945-5016 CREDIT APPLICATION DATE: TOTAL PAGES: 1 of 5 TO: FROM: Steve Schlussel Accts Receivable Mgr COMPANY: COMPANY: Atlantic Concrete
Thank you for your interest in becoming a customer of Cheney Brothers, Inc.
 Delivering Southern Hospitality Since 1925 www.cheneybrothers.com Thank you for your interest in becoming a customer of Cheney Brothers, Inc. The following pages are for opening an account, information
Delivering Southern Hospitality Since 1925 www.cheneybrothers.com Thank you for your interest in becoming a customer of Cheney Brothers, Inc. The following pages are for opening an account, information
Alabama State Board of Pharmacy New Manufacturer Application
 Alabama State Board of Pharmacy New Manufacturer Application Date Received Manufacturer: A person or entity, except a pharmacy, who prepares, derives, produces, researches, test, labels, or packages any
Alabama State Board of Pharmacy New Manufacturer Application Date Received Manufacturer: A person or entity, except a pharmacy, who prepares, derives, produces, researches, test, labels, or packages any
ASHI DIAMONDS, LLC. 18 EAST 48TH STREET, 14TH FLOOR NEW YORK, N.Y ((212) ~ FAX (212) ~ ((800) 622-ASHI
 ~ FAX (212) ~ ((800) 622-ASHI") ASHI DIAMONDS, LLC. 18 EAST 48TH STREET, 14TH FLOOR NEW YORK, N.Y. 10017 ((212) 319-8291 ~ FAX (212) 319-4341 ~ ((800) 622-ASHI S E C U R I T Y A G R E E M E N T This Purchase Money Security Interest Agreement
ASHI DIAMONDS, LLC. 18 EAST 48TH STREET, 14TH FLOOR NEW YORK, N.Y. 10017 ((212) 319-8291 ~ FAX (212) 319-4341 ~ ((800) 622-ASHI S E C U R I T Y A G R E E M E N T This Purchase Money Security Interest Agreement
PATIENT COMPLAINT FORM
 PATIENT COMPLAINT FORM You may use this form to file a complaint against a dentist or dental hygienist. Your complaint may be disclosed to members, employees and consultants of the Board of Dental Examiners
PATIENT COMPLAINT FORM You may use this form to file a complaint against a dentist or dental hygienist. Your complaint may be disclosed to members, employees and consultants of the Board of Dental Examiners
State of Florida Department of Business and Professional Regulation Division of Drugs, Devices, and Cosmetics
 State of Florida Division of Drugs, Devices, and Cosmetics Application for Compressed Medical Gas Wholesale Distributor Form.: DBPR-DDC-217 APPLICATION CHECKLIST IMPORTANT Submit all items on the checklist
State of Florida Division of Drugs, Devices, and Cosmetics Application for Compressed Medical Gas Wholesale Distributor Form.: DBPR-DDC-217 APPLICATION CHECKLIST IMPORTANT Submit all items on the checklist
State of Florida Department of Business and Professional Regulation Division of Drugs, Devices, and Cosmetics. Form No.
 State of Florida Department of Business and Professional Regulation Division of Drugs, Devices, and Cosmetics Application for Permit as a Medical Gas Wholesale Distributor Form.: DBPR-DDC-217 APPLICATION
State of Florida Department of Business and Professional Regulation Division of Drugs, Devices, and Cosmetics Application for Permit as a Medical Gas Wholesale Distributor Form.: DBPR-DDC-217 APPLICATION
NOVARTIS VACCINES AND DIAGNOSTICS, INC. TERMS AND CONDITIONS FOR PURCHASES OF FLUVIRIN (Influenza Virus Vaccine)
") NOVARTIS VACCINES AND DIAGNOSTICS, INC. TERMS AND CONDITIONS FOR PURCHASES OF FLUVIRIN (Influenza Virus Vaccine) Effective January 1, 2015 1. Purchase, Sale and Use of Product. These terms and conditions
NOVARTIS VACCINES AND DIAGNOSTICS, INC. TERMS AND CONDITIONS FOR PURCHASES OF FLUVIRIN (Influenza Virus Vaccine) Effective January 1, 2015 1. Purchase, Sale and Use of Product. These terms and conditions
Property Information:
 For Office Use Only CUST ID: SALES ID: TM NAME: MG Code: 6186 INTERNAL ID: Guest Supply, LLC Guest Packaging Date of Application Name of Person Completing Application Title Property Information: Name of
For Office Use Only CUST ID: SALES ID: TM NAME: MG Code: 6186 INTERNAL ID: Guest Supply, LLC Guest Packaging Date of Application Name of Person Completing Application Title Property Information: Name of
GRAND RAPIDS CRANE CO LLC.
 GRAND RAPIDS CRANE CO LLC. New Customer Application Contents: 1. Index 2. Application of Credit 3. Application of Credit 4. Application of Credit Please Email or Fax completed form to justin@grandrapidscrane.com
GRAND RAPIDS CRANE CO LLC. New Customer Application Contents: 1. Index 2. Application of Credit 3. Application of Credit 4. Application of Credit Please Email or Fax completed form to justin@grandrapidscrane.com
Royal Group, Inc. or Royal Plastics Group USA Group Company name CREDIT APPLICATION
 Royal Group, Inc. or Royal Plastics Group USA Group Company name CREDIT APPLICATION Tel:( 905) 652 2780 Fax:( 905) 652 8003 New Application For which Royal Group Company Credit Update Please select the
Royal Group, Inc. or Royal Plastics Group USA Group Company name CREDIT APPLICATION Tel:( 905) 652 2780 Fax:( 905) 652 8003 New Application For which Royal Group Company Credit Update Please select the
balances before being applied to current balances, unless elected otherwise by the Company. 5. The Company reserves the right to grant, at its sole di
 THIS ONLINE CUSTOMER AGREEMENT ( Agreement ) is made by and between Ziemek Laboratories, Inc., a Washington corporation ( Company ) and the customer who has agreed to and accepted this Agreement by separate
THIS ONLINE CUSTOMER AGREEMENT ( Agreement ) is made by and between Ziemek Laboratories, Inc., a Washington corporation ( Company ) and the customer who has agreed to and accepted this Agreement by separate
CARRIER ENTERPRISE NORTHEAST, LLC ( CE ) (PLEASE PRINT CLEARLY) Credit Agreement
 (PLEASE PRINT CLEARLY) Credit Agreement") CARRIER ENTERPRISE NORTHEAST, LLC ( CE ) Date Credit Agreement (PLEASE PRINT CLEARLY) Company Name of Applicant (If applicant is a corporation or LLC, give name as it appears in the ARTICLES OF INCORPORATION)
CARRIER ENTERPRISE NORTHEAST, LLC ( CE ) Date Credit Agreement (PLEASE PRINT CLEARLY) Company Name of Applicant (If applicant is a corporation or LLC, give name as it appears in the ARTICLES OF INCORPORATION)
COEN CARD APPLICATION AND ACKNOWLEDGEMENT OF TERMS NEW CUSTOMER
 COEN CARD APPLICATION AND ACKNOWLEDGEMENT OF TERMS NEW CUSTOMER COMPANY INFORMATION AND CONTACT DETAILS Legal Name of Company ( Applicant ): Telephone: Fax: Credit Limit Desired: DBA, if applicable: Accounts
COEN CARD APPLICATION AND ACKNOWLEDGEMENT OF TERMS NEW CUSTOMER COMPANY INFORMATION AND CONTACT DETAILS Legal Name of Company ( Applicant ): Telephone: Fax: Credit Limit Desired: DBA, if applicable: Accounts
INSTRUCTION SHEET FOR NON-RESIDENT (OUT-OF-STATE) DRUG OUTLET (PHARMACY)
 DRUG OUTLET (PHARMACY)") Vermont Secretary of State Office of Professional Regulation VERMONT BOARD OF PHARMACY 89 Main Street, 3 rd Floor Montpelier, VT 05620-3402 Ph: (802) 828-2373 Fax: (802) 828-2465 Web Site: www.vtprofessionals.org
Vermont Secretary of State Office of Professional Regulation VERMONT BOARD OF PHARMACY 89 Main Street, 3 rd Floor Montpelier, VT 05620-3402 Ph: (802) 828-2373 Fax: (802) 828-2465 Web Site: www.vtprofessionals.org
C O M M E R C I A L C R E D I T A P P L I C A T I O N
 PLEASE CHECK SITE LOCATIONS BELOW C O M M E R C I A L C R E D I T A P P L I C A T I O N Office: 907-276-2688 Toll Free: 800-478-2688 Fax: 907-276-374 l Anchorage Bethel Dillingham Dutch Harbor Fairbanks
PLEASE CHECK SITE LOCATIONS BELOW C O M M E R C I A L C R E D I T A P P L I C A T I O N Office: 907-276-2688 Toll Free: 800-478-2688 Fax: 907-276-374 l Anchorage Bethel Dillingham Dutch Harbor Fairbanks
Indiana Health Coverage Programs IHCP PROVIDER AGREEMENT
 IHCP PROVIDER AGREEMENT By execution of this Agreement, the undersigned entity ( Provider ) requests enrollment as a provider in the Indiana Health Coverage Programs. As an enrolled provider in the Indiana
IHCP PROVIDER AGREEMENT By execution of this Agreement, the undersigned entity ( Provider ) requests enrollment as a provider in the Indiana Health Coverage Programs. As an enrolled provider in the Indiana
FAR EAST BROKERS AND CONSULTANTS, INC. PURCHASE ORDER TERMS AND CONDITIONS
 FAR EAST BROKERS AND CONSULTANTS, INC. PURCHASE ORDER TERMS AND CONDITIONS 1. ACCEPTANCE a. By accepting this order for products, Supplier accepts all terms and conditions set forth by FAR EAST BROKERS
FAR EAST BROKERS AND CONSULTANTS, INC. PURCHASE ORDER TERMS AND CONDITIONS 1. ACCEPTANCE a. By accepting this order for products, Supplier accepts all terms and conditions set forth by FAR EAST BROKERS
Fax: (905) Phone:
 Phone:") Please fax or email your completed account application to: DRIVE MEDICAL CANADA Fax: (905) 787-8550 Phone: 866-752-1363 Email: canadacustomerservice@drivemedical.com * Be Sure to Include Your Sales Representatives
Please fax or email your completed account application to: DRIVE MEDICAL CANADA Fax: (905) 787-8550 Phone: 866-752-1363 Email: canadacustomerservice@drivemedical.com * Be Sure to Include Your Sales Representatives
BECK EQUIPMENT, INC Preble Rd, Preble, NY Toll Free: (866) / Fax: (607)
 / Fax: (607)") Legal Company Name BECK EQUIPMENT, INC. RENTAL APPLICATION To apply for rentals from Beck Equipment, Inc., please provide the following information. Fill out completely and return by fax to (607) 749-5640.
Legal Company Name BECK EQUIPMENT, INC. RENTAL APPLICATION To apply for rentals from Beck Equipment, Inc., please provide the following information. Fill out completely and return by fax to (607) 749-5640.
THIS MATTER came on to be considered at a prehearing conference (hereinafter,
 BEFORE THE NORTH CAROLNA BOARD OF PHARMACY n the Matter of: MEDSAVE NC. d/b/a KNG'S PHARMACY AND COMPOUNDNG LAB (Permit No. 5304 CONSENT ORDER THS MATTER came on to be considered at a prehearing conference
BEFORE THE NORTH CAROLNA BOARD OF PHARMACY n the Matter of: MEDSAVE NC. d/b/a KNG'S PHARMACY AND COMPOUNDNG LAB (Permit No. 5304 CONSENT ORDER THS MATTER came on to be considered at a prehearing conference
FATIGUE TECHNOLOGY INC. PURCHASE ORDER TERMS AND CONDITIONS DATED JANUARY 4, 2006
 FATIGUE TECHNOLOGY INC. PURCHASE ORDER TERMS AND CONDITIONS DATED JANUARY 4, 2006 1. CONTRACT. Fatigue Technology Inc. s, hereinafter called FTI, purchase order, or change order to a purchase order, collectively
FATIGUE TECHNOLOGY INC. PURCHASE ORDER TERMS AND CONDITIONS DATED JANUARY 4, 2006 1. CONTRACT. Fatigue Technology Inc. s, hereinafter called FTI, purchase order, or change order to a purchase order, collectively
COEN CARD APPLICATION AND ACKNOWLEDGEMENT OF TERMS
 Coen Oil Company, Inc. (including Coen Zappi Oil Company) 1045 West Chestnut Street Washington, PA 15301 724-223-5500 Fax: 724-223-5501 www.coenoil.com COEN CARD APPLICATION AND ACKNOWLEDGEMENT OF TERMS
Coen Oil Company, Inc. (including Coen Zappi Oil Company) 1045 West Chestnut Street Washington, PA 15301 724-223-5500 Fax: 724-223-5501 www.coenoil.com COEN CARD APPLICATION AND ACKNOWLEDGEMENT OF TERMS
Kansas Credit Services Organization Instructions for Application of Registration
 STATE OF KANSAS OFFICE OF THE STATE BANK COMMISSIONER CONSUMER AND MORTGAGE LENDING DIVISION 700 SW Jackson St., Suite 300 Topeka, Kansas 66603-3796 785-296-2266 Fax: 785-296-6037 Kansas Credit Services
STATE OF KANSAS OFFICE OF THE STATE BANK COMMISSIONER CONSUMER AND MORTGAGE LENDING DIVISION 700 SW Jackson St., Suite 300 Topeka, Kansas 66603-3796 785-296-2266 Fax: 785-296-6037 Kansas Credit Services
WHY SPIRITUS? Some of our Vendors
 Spiritus Distribution is the Catholic division of New Day Christian, an independently owned distribution company that has served the evangelical Christian market for over 30 years. Spiritus provides the
Spiritus Distribution is the Catholic division of New Day Christian, an independently owned distribution company that has served the evangelical Christian market for over 30 years. Spiritus provides the
Effective February 17, 2017
 Seqirus Terms and Conditions for Purchases of Seasonal Influenza Vaccine Products: FLUVIRIN (Influenza Virus Vaccine); FLUAD (Influenza Vaccine); AFLURIA (Influenza Vaccine) and FLUCELVAX QUADRIVALENT
Seqirus Terms and Conditions for Purchases of Seasonal Influenza Vaccine Products: FLUVIRIN (Influenza Virus Vaccine); FLUAD (Influenza Vaccine); AFLURIA (Influenza Vaccine) and FLUCELVAX QUADRIVALENT
IHCP Rendering Provider Agreement and Attestation Form
 Version 6.4E, July 2017 Page 1 of 5 This agreement must be completed, signed, and returned to the IHCP for processing. By execution of this Agreement, the undersigned entity ( Provider ) requests enrollment
Version 6.4E, July 2017 Page 1 of 5 This agreement must be completed, signed, and returned to the IHCP for processing. By execution of this Agreement, the undersigned entity ( Provider ) requests enrollment
CREDIT APPLICATION. On behalf of Lodge Lumber Company, Inc., I would like to thank you for your interest in doing business with our company.
 Page 1 CREDIT APPLICATION On behalf of Lodge Lumber Company, Inc., I would like to thank you for your interest in doing business with our company. Along with this letter is a copy of our Credit Application.
Page 1 CREDIT APPLICATION On behalf of Lodge Lumber Company, Inc., I would like to thank you for your interest in doing business with our company. Along with this letter is a copy of our Credit Application.
3776 S.R. 93 N.E., Crooksville, OH Toll Free (866) * Phone (740) * Fax (740)
 * Phone (740) * Fax (740)") 3776 S.R. 93 N.E., Crooksville, OH 43731 Toll Free (866) 818-4435 * Phone (740) 982-3030 * Fax (740) 982-3055 www.valueautoauction.com Name of Dealer: Telephone ( ) (Legal Name if Different) Fax# ( ) (Hereinafter
3776 S.R. 93 N.E., Crooksville, OH 43731 Toll Free (866) 818-4435 * Phone (740) 982-3030 * Fax (740) 982-3055 www.valueautoauction.com Name of Dealer: Telephone ( ) (Legal Name if Different) Fax# ( ) (Hereinafter
Rendering Provider Agreement
 Rendering Provider Agreement IHCP Rendering Provider Enrollment and Profile Maintenance Packet indianamedicaid.com To enroll multiple rendering providers, complete a separate IHCP Rendering Provider Enrollment
Rendering Provider Agreement IHCP Rendering Provider Enrollment and Profile Maintenance Packet indianamedicaid.com To enroll multiple rendering providers, complete a separate IHCP Rendering Provider Enrollment
State of Florida Department of Business and Professional Regulation Division of Drugs, Devices, and Cosmetics
 State of Florida Division of Drugs, Devices, and Cosmetics Application for Change of Physical Location Form.: DBPR-DDC-109 APPLICATION CHECKLIST IMPORTANT Submit all items on the checklist below with your
State of Florida Division of Drugs, Devices, and Cosmetics Application for Change of Physical Location Form.: DBPR-DDC-109 APPLICATION CHECKLIST IMPORTANT Submit all items on the checklist below with your
Fax the documents listed below to to start today!
 CASHWAY FUNDING STARTUP KIT FREE ACCOUNT IN 5 MINUTES Welcome to Cashway Funding! Now you can join other successful trucking companies and enjoy the benefits of a profitable and growing trucking business.
CASHWAY FUNDING STARTUP KIT FREE ACCOUNT IN 5 MINUTES Welcome to Cashway Funding! Now you can join other successful trucking companies and enjoy the benefits of a profitable and growing trucking business.
GILEAD SCIENCES, INC. PURCHASE ORDER TERMS AND CONDITIONS
 GILEAD SCIENCES, INC. PURCHASE ORDER TERMS AND CONDITIONS 1. ACCEPTANCE: Supplier has read and understands this purchase order (this order ) and agrees that Supplier s written acceptance, delivery of any
GILEAD SCIENCES, INC. PURCHASE ORDER TERMS AND CONDITIONS 1. ACCEPTANCE: Supplier has read and understands this purchase order (this order ) and agrees that Supplier s written acceptance, delivery of any
FINANCIAL CASUALTY & SURETY, INC
 FINANCIAL CASUALTY & SURETY, INC The Bail Insurance Company 3131 Eastside St. Suite 600 Houston, Texas 77098 P.O. Box 4479 Houston, Texas 77210-4479 Toll Free: 877.737.2245 Fax: 713. 580.6401 fcs APPLICATION
FINANCIAL CASUALTY & SURETY, INC The Bail Insurance Company 3131 Eastside St. Suite 600 Houston, Texas 77098 P.O. Box 4479 Houston, Texas 77210-4479 Toll Free: 877.737.2245 Fax: 713. 580.6401 fcs APPLICATION
WHOLESALER DANGEROUS DRUGS & DANGEROUS DEVICES SELF- ASSESSMENT
 California State Board of Pharmacy 1625 N. Market Blvd., Suite N219 Sacramento, California 95834 (916) 574-7900 FAX (916) 574-8618 STATE AND CONSUMER SERVICES AGENCY DEPARTMENT OF CONSUMER AFFAIRS ARNOLD
California State Board of Pharmacy 1625 N. Market Blvd., Suite N219 Sacramento, California 95834 (916) 574-7900 FAX (916) 574-8618 STATE AND CONSUMER SERVICES AGENCY DEPARTMENT OF CONSUMER AFFAIRS ARNOLD
State of Florida Department of Business and Professional Regulation Division of Drugs, Devices, and Cosmetics
 State of Florida Department of Business and Professional Regulation Division of Drugs, Devices, and Cosmetics Application for a Compressed Medical Gas Manufacturer Form.: DBPR-DDC-204 APPLICATION CHECKLIST
State of Florida Department of Business and Professional Regulation Division of Drugs, Devices, and Cosmetics Application for a Compressed Medical Gas Manufacturer Form.: DBPR-DDC-204 APPLICATION CHECKLIST
State of Florida Department of Business and Professional Regulation Division of Drugs, Devices and Cosmetics
 State of Florida Department of Business and Professional Regulation Division of Drugs, Devices and Cosmetics Application for Retail Pharmacy Drug Wholesale Distributor Permit Form.: DBPR-DDC-218 APPLICATION
State of Florida Department of Business and Professional Regulation Division of Drugs, Devices and Cosmetics Application for Retail Pharmacy Drug Wholesale Distributor Permit Form.: DBPR-DDC-218 APPLICATION
PAUL DANIEL BOTTOMLEY, ATTORNEY FOR PLAINTIFF UNITED STATES OF AMERICA FOR THE DISTRICT OF 0F MONTANA BUTTE DIVISION UNITED STATES OF 0F AMERICA,
 Case 2:13-cr-00004-DLC 2:13-cr-OOOO4-DLC Document 7 Filed 04/19/13 Page 1 of 14 JESSICA T. FEHR JESSICA T. FEHR Assistant U.S. Attorney U.S. Attorney s Office nd 26012 2 Avenue North, Ste. 3200 Billings,
Case 2:13-cr-00004-DLC 2:13-cr-OOOO4-DLC Document 7 Filed 04/19/13 Page 1 of 14 JESSICA T. FEHR JESSICA T. FEHR Assistant U.S. Attorney U.S. Attorney s Office nd 26012 2 Avenue North, Ste. 3200 Billings,
BOARD OF PHARMACY. REQUIREMENTS AND INSTRUCTIONS FOR FILING - MISCELLANEOUS PERMIT Access this form via website at:
 BOARD OF PHARMACY REQUIREMENTS AND INSTRUCTIONS FOR FILING - MISCELLANEOUS PERMIT Access this form via website at: www.hawaii.gov/dcca/areas/pvl Miscellaneous Permits - Check Business Intended on Application:
BOARD OF PHARMACY REQUIREMENTS AND INSTRUCTIONS FOR FILING - MISCELLANEOUS PERMIT Access this form via website at: www.hawaii.gov/dcca/areas/pvl Miscellaneous Permits - Check Business Intended on Application:
AGREEMENT REGARDING SALES TERMS, CONDITIONS AND PROCEDURES
 AGREEMENT REGARDING SALES TERMS, CONDITIONS AND PROCEDURES THIS AGREEMENT, entered into as of, 2014, by and between Crown Building Products, LLC, 2155 FM 1187, Mansfield, TX 76063 ( Crown or Manufacturer
AGREEMENT REGARDING SALES TERMS, CONDITIONS AND PROCEDURES THIS AGREEMENT, entered into as of, 2014, by and between Crown Building Products, LLC, 2155 FM 1187, Mansfield, TX 76063 ( Crown or Manufacturer
Local Rebate Yes No Paid Local Growth Yes No Paid Annually Semi-Annually Quarterly Monthly Annually Semi-Annually Quarterly Monthly
 NEW VENDOR PROFILE VENDOR INFORMATION Vendor Name: Address: City, State, Zip: Phone #: Fax #: Regional Sales Rep: Phone #: Ext: Cell # Fax # Email Address: CUSTOMER SERVICE INFORMATION CSR: Phone #: Ext.#
NEW VENDOR PROFILE VENDOR INFORMATION Vendor Name: Address: City, State, Zip: Phone #: Fax #: Regional Sales Rep: Phone #: Ext: Cell # Fax # Email Address: CUSTOMER SERVICE INFORMATION CSR: Phone #: Ext.#
GLOBAL PC DIRECT, INC Fremont Blvd, Fremont, CA Tel: (510) Fax: (510)
 Fax: (510)") RESELLER CREDIT APPLICATION COMPANY INFORMATION: Legal Business Name: Business Trade Name-DBA: Billing Address: City: State: Zip: Shipping Address: City: State: Zip: Business Phone: Business is: Public
RESELLER CREDIT APPLICATION COMPANY INFORMATION: Legal Business Name: Business Trade Name-DBA: Billing Address: City: State: Zip: Shipping Address: City: State: Zip: Business Phone: Business is: Public
CIRCOM DEVELOPMENT CORPORATION CONVERTIBLE PROMISSORY NOTE SUBSCRIPTION AGREEMENT
 CIRCOM DEVELOPMENT CORPORATION CONVERTIBLE PROMISSORY NOTE SUBSCRIPTION AGREEMENT Circom Development Corporation 6511 119 th Avenue East Puyallup, Washington 98372 Gentlemen: The undersigned ( Investor
CIRCOM DEVELOPMENT CORPORATION CONVERTIBLE PROMISSORY NOTE SUBSCRIPTION AGREEMENT Circom Development Corporation 6511 119 th Avenue East Puyallup, Washington 98372 Gentlemen: The undersigned ( Investor
PLEASE. To Process your Application we must have the following:
 PLEASE To Process your Application we must have the following: Complete and return the entire application. An Owner/Principle/Officer must sign. Please include a copy of Photo ID for the parties signing
PLEASE To Process your Application we must have the following: Complete and return the entire application. An Owner/Principle/Officer must sign. Please include a copy of Photo ID for the parties signing
CREDIT APPLICATION / APPLICANT AGREEMENT
 CREDIT APPLICATION / APPLICANT AGREEMENT This Credit Application / Applicant Agreement (the Application ) is between Lubbock Rent All & Supply, LLC ( LRA ), and the applicant named on page one below (
CREDIT APPLICATION / APPLICANT AGREEMENT This Credit Application / Applicant Agreement (the Application ) is between Lubbock Rent All & Supply, LLC ( LRA ), and the applicant named on page one below (
Lift Works, Inc. Credit Application
 Credit Application 600 Industrial Dr ~ St. Charles, IL 60174 AR PH: (630) 957-4317 AR FX: (630) 957-4193 Main PH: (630) 833-4626 Main FX: (630) 833-4628 Complete Credit Application Form and fax to (630)
Credit Application 600 Industrial Dr ~ St. Charles, IL 60174 AR PH: (630) 957-4317 AR FX: (630) 957-4193 Main PH: (630) 833-4626 Main FX: (630) 833-4628 Complete Credit Application Form and fax to (630)
HULL & COMPANY, INC. DBA: Hull & Company MacDuff E&S Insurance Brokers PRODUCER AGREEMENT
 HULL & COMPANY, INC. DBA: Hull & Company MacDuff E&S Insurance Brokers PRODUCER AGREEMENT THIS PRODUCER AGREEMENT (this Agreement ), dated as of, 20, is made and entered into by and between Hull & Company,
HULL & COMPANY, INC. DBA: Hull & Company MacDuff E&S Insurance Brokers PRODUCER AGREEMENT THIS PRODUCER AGREEMENT (this Agreement ), dated as of, 20, is made and entered into by and between Hull & Company,
COMMERCIAL CREDIT APPLICATION
 COMMERCIAL CREDIT APPLICATION DATE COMPLETE LEGAL NAME OF BUSINESS DBA NAME OF PARENT COMPANY (if applicable) BILLING ADDRESS STREET ADDRESS PHONE NUMBER CELL E-MAIL ADDRESS FAX NUMBER CONTRACTORS LICENSE
COMMERCIAL CREDIT APPLICATION DATE COMPLETE LEGAL NAME OF BUSINESS DBA NAME OF PARENT COMPANY (if applicable) BILLING ADDRESS STREET ADDRESS PHONE NUMBER CELL E-MAIL ADDRESS FAX NUMBER CONTRACTORS LICENSE
AGENT AGREEMENT. WHEREAS, Eoil has granted Agent the right to solicit automobile dealers for use of the Coupons offered by Eoil; and
 AGENT AGREEMENT This Agreement is entered into on (date), by and between OIL4Charity, LLC dba Eoilchange.com hereinafter referred to as Eoil, and (Agent Name) located at (Agent Address), hereinafter referred
AGENT AGREEMENT This Agreement is entered into on (date), by and between OIL4Charity, LLC dba Eoilchange.com hereinafter referred to as Eoil, and (Agent Name) located at (Agent Address), hereinafter referred
State of Florida Department of Business and Professional Regulation Division of Drugs, Devices, and Cosmetics
 State of Florida Department of Business and Professional Regulation Division of Drugs, Devices, and Cosmetics Application for Permit as a Medical Oxygen Retail Establishment Form.: DBPR-DDC-223 APPLICATION
State of Florida Department of Business and Professional Regulation Division of Drugs, Devices, and Cosmetics Application for Permit as a Medical Oxygen Retail Establishment Form.: DBPR-DDC-223 APPLICATION
Please submit the attached Credit Application if you are interested in obtaining credit terms with us.
 Credit Application! Please submit the attached Credit Application if you are interested in obtaining credit terms with us. Credit Terms If you have not purchased from us before, we request that your first
Credit Application! Please submit the attached Credit Application if you are interested in obtaining credit terms with us. Credit Terms If you have not purchased from us before, we request that your first
FedNat Underwriters PO Box Ft. Lauderdale, FL Phone: (800) (option 3) Fax: (954)
 (option 3) Fax: (954)") AGENCY QUESTIONNAIRE Thank you for your interest in representing FedNat Insurance Company / Monarch National Insurance Company and other nationally recognized insurance companies. Please complete the questionnaire
AGENCY QUESTIONNAIRE Thank you for your interest in representing FedNat Insurance Company / Monarch National Insurance Company and other nationally recognized insurance companies. Please complete the questionnaire
Thank you for your interest in becoming a broker for the Counter Products offered through Sonoran National!
 BROKER PACKET Thank you for your interest in becoming a broker for the Counter Products offered through Sonoran National! Once we receive the completed Broker Questionnaire, along with a copy of your current
BROKER PACKET Thank you for your interest in becoming a broker for the Counter Products offered through Sonoran National! Once we receive the completed Broker Questionnaire, along with a copy of your current
RETAILER PURCHASE AGREEMENT. Nederland
 RETAILER PURCHASE AGREEMENT Nederland RETAILER PURCHASE AGREEMENT \ NEDERLAND SilcSkin Nederland 2e Schansstraat 65- A Rotterdam 3025 XL Nederland Phone: {31} 6.2471.1699 Email: verkoop@silcskinnederland.nl
RETAILER PURCHASE AGREEMENT Nederland RETAILER PURCHASE AGREEMENT \ NEDERLAND SilcSkin Nederland 2e Schansstraat 65- A Rotterdam 3025 XL Nederland Phone: {31} 6.2471.1699 Email: verkoop@silcskinnederland.nl
Compliance and Fraud, Waste, and Abuse Awareness Training. First Tier, Downstream, and Related Entities
 Compliance and Fraud, Waste, and Abuse Awareness Training First Tier, Downstream, and Related Entities 1 Course Outline Overview Purpose of training Effective Compliance program Definition of Fraud, Waste,
Compliance and Fraud, Waste, and Abuse Awareness Training First Tier, Downstream, and Related Entities 1 Course Outline Overview Purpose of training Effective Compliance program Definition of Fraud, Waste,
ADAM H. PUTNAM COMMISSIONER
 FLORIDA DEPARTMENT OF AGRICULTURE AND CONSUMER SERVICES ADAM H. PUTNAM COMMISSIONER PAWNBROKING REGISTRATION APPLICATION Chapter 539.001, Florida Statutes Rule 5J13.002, Florida Administrative Code Florida
FLORIDA DEPARTMENT OF AGRICULTURE AND CONSUMER SERVICES ADAM H. PUTNAM COMMISSIONER PAWNBROKING REGISTRATION APPLICATION Chapter 539.001, Florida Statutes Rule 5J13.002, Florida Administrative Code Florida
Deising s Bakery and Restaurant North Front Street Kingston, New York Tel: Fax:
 Deising s Bakery and Restaurant 109-121 North Front Street Kingston, New York 12401 Tel: 845-338-7757 Fax: 845-338-1327 PLEASE FOLLOW THESE SIMPLE GUIDELINES FOR PLACING YOUR WHOLESALE ORDER: 1. ALL orders
Deising s Bakery and Restaurant 109-121 North Front Street Kingston, New York 12401 Tel: 845-338-7757 Fax: 845-338-1327 PLEASE FOLLOW THESE SIMPLE GUIDELINES FOR PLACING YOUR WHOLESALE ORDER: 1. ALL orders
SELECT SOURCE TERMS AND CONDITIONS
 SELECT SOURCE TERMS AND CONDITIONS In the course of its business, Reseller will purchase Ingram Micro Products and will sell Ingram Micro Products to customers located in the United States ( End Users
SELECT SOURCE TERMS AND CONDITIONS In the course of its business, Reseller will purchase Ingram Micro Products and will sell Ingram Micro Products to customers located in the United States ( End Users
State of New Mexico Medicaid Program Electronic Data Interchange (EDI) Provider Enrollment Application
 Provider Enrollment Application") State of New Mexico Medicaid Program Electronic Data Interchange (EDI) Provider Enrollment Application New Mexico EDI Provider Enroll App 7-27-17 1 Name and Business Organization Information Direct EDI
State of New Mexico Medicaid Program Electronic Data Interchange (EDI) Provider Enrollment Application New Mexico EDI Provider Enroll App 7-27-17 1 Name and Business Organization Information Direct EDI
TIMKEN EUROPE GENERAL TERMS & CONDITIONS OF SALE 1. TERMS AND CONDITIONS OF SALE
 TIMKEN EUROPE GENERAL TERMS & CONDITIONS OF SALE 1. TERMS AND CONDITIONS OF SALE All sales of Timken products (the "Product(s)") by Timken Europe shall be governed by the terms and conditions set forth
TIMKEN EUROPE GENERAL TERMS & CONDITIONS OF SALE 1. TERMS AND CONDITIONS OF SALE All sales of Timken products (the "Product(s)") by Timken Europe shall be governed by the terms and conditions set forth
Consumer Credit Division
 Consumer Credit Division Loan Broker Registration Kit fcaa.gov.sk.ca fid@gov.sk.ca Saskatchewan Loan Broker Registration Kit Consumer Credit Division Suite 601, 1919 Saskatchewan Drive Regina, Canada S4P
Consumer Credit Division Loan Broker Registration Kit fcaa.gov.sk.ca fid@gov.sk.ca Saskatchewan Loan Broker Registration Kit Consumer Credit Division Suite 601, 1919 Saskatchewan Drive Regina, Canada S4P
Your interest in material and service is appreciated and we thank you for your cooperation in the above matter.
 Desert Electric Supply MAIN OFFICE, 74-875 VELIE WAY 83311 AVE 45; STE 102 4605 E. SUNNY DUNES ROAD PALM DESERT, CA 92260 INDIO, CA 92201 PALM SPRINGS, CA 92264 (760) 568-5991 (760) 404-0010 (760) 327-1146
Desert Electric Supply MAIN OFFICE, 74-875 VELIE WAY 83311 AVE 45; STE 102 4605 E. SUNNY DUNES ROAD PALM DESERT, CA 92260 INDIO, CA 92201 PALM SPRINGS, CA 92264 (760) 568-5991 (760) 404-0010 (760) 327-1146