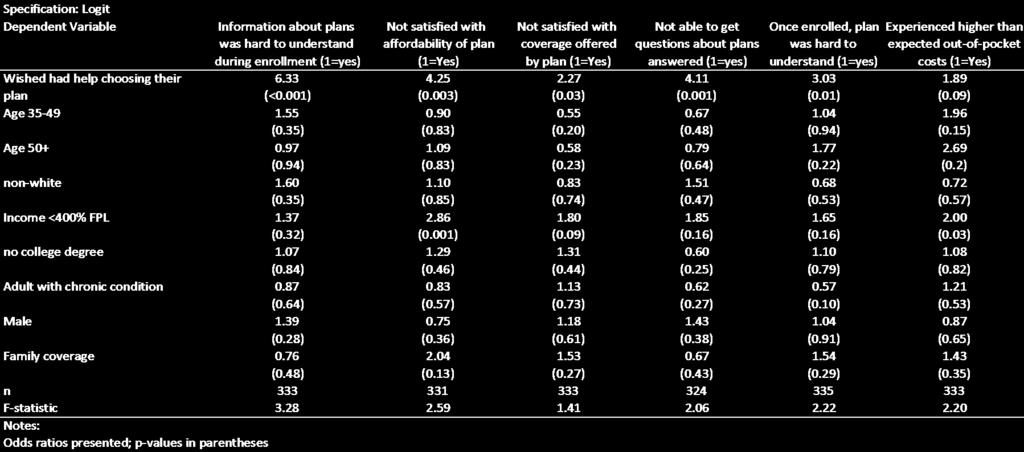
The following tables present the unadjusted results and. regression results that underlie the results reported in
|
|
|
- Kelley Allison
- 5 years ago
- Views:
Transcription
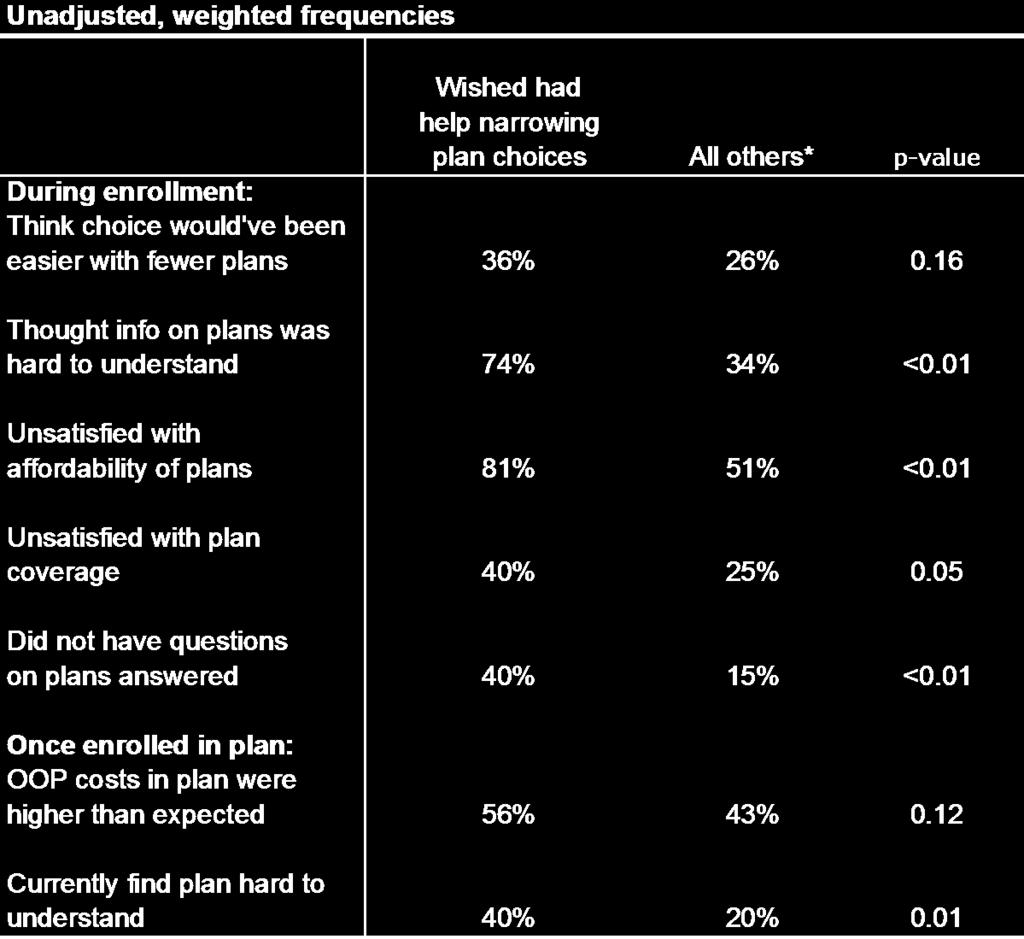
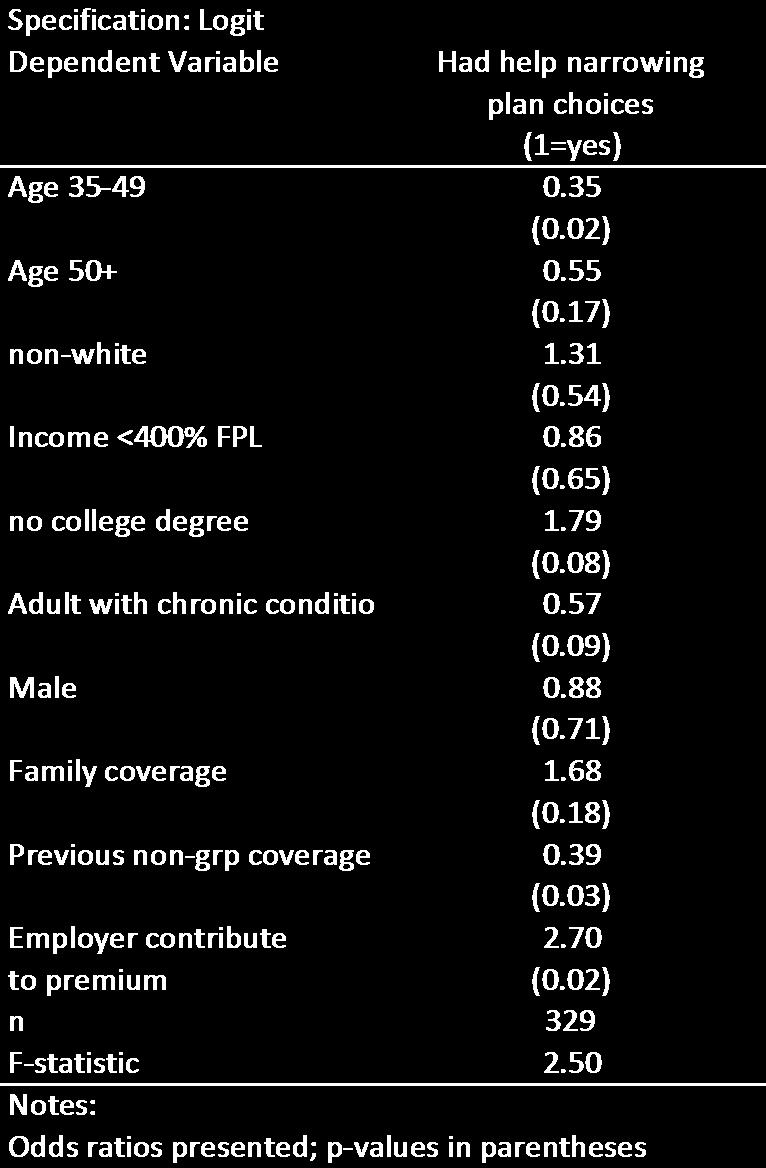
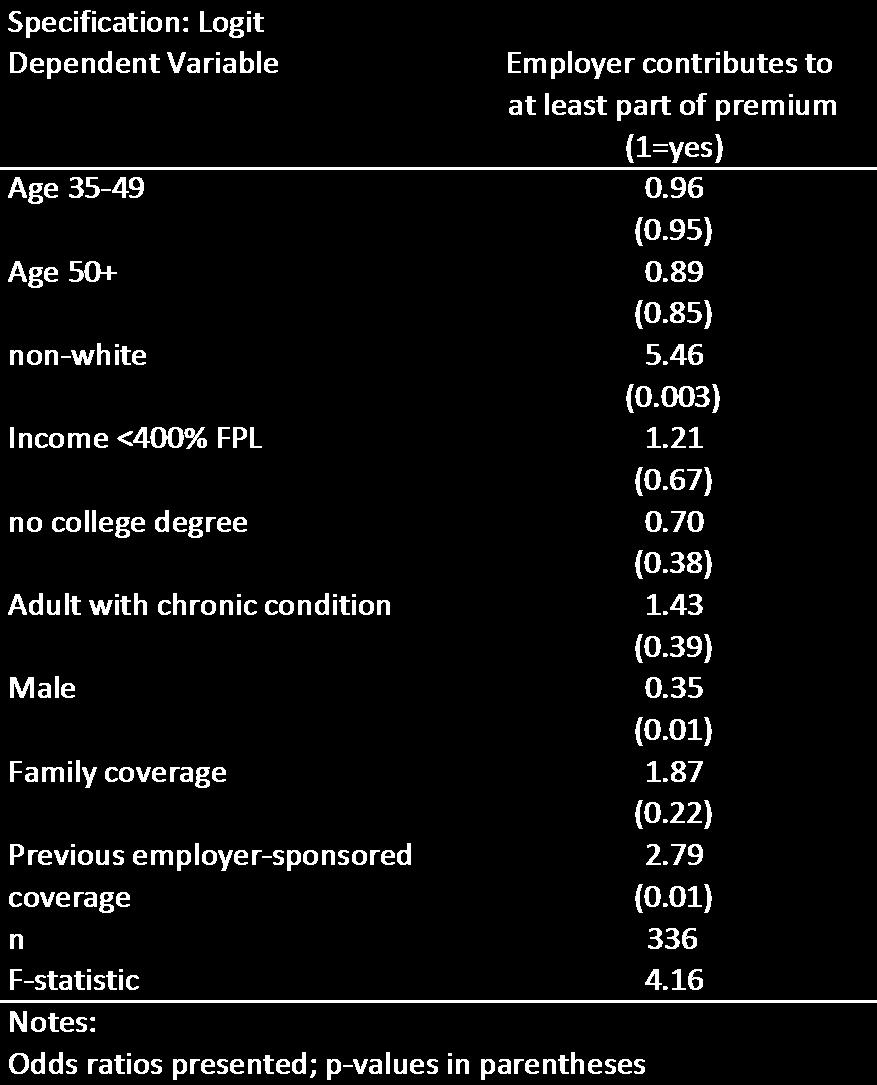
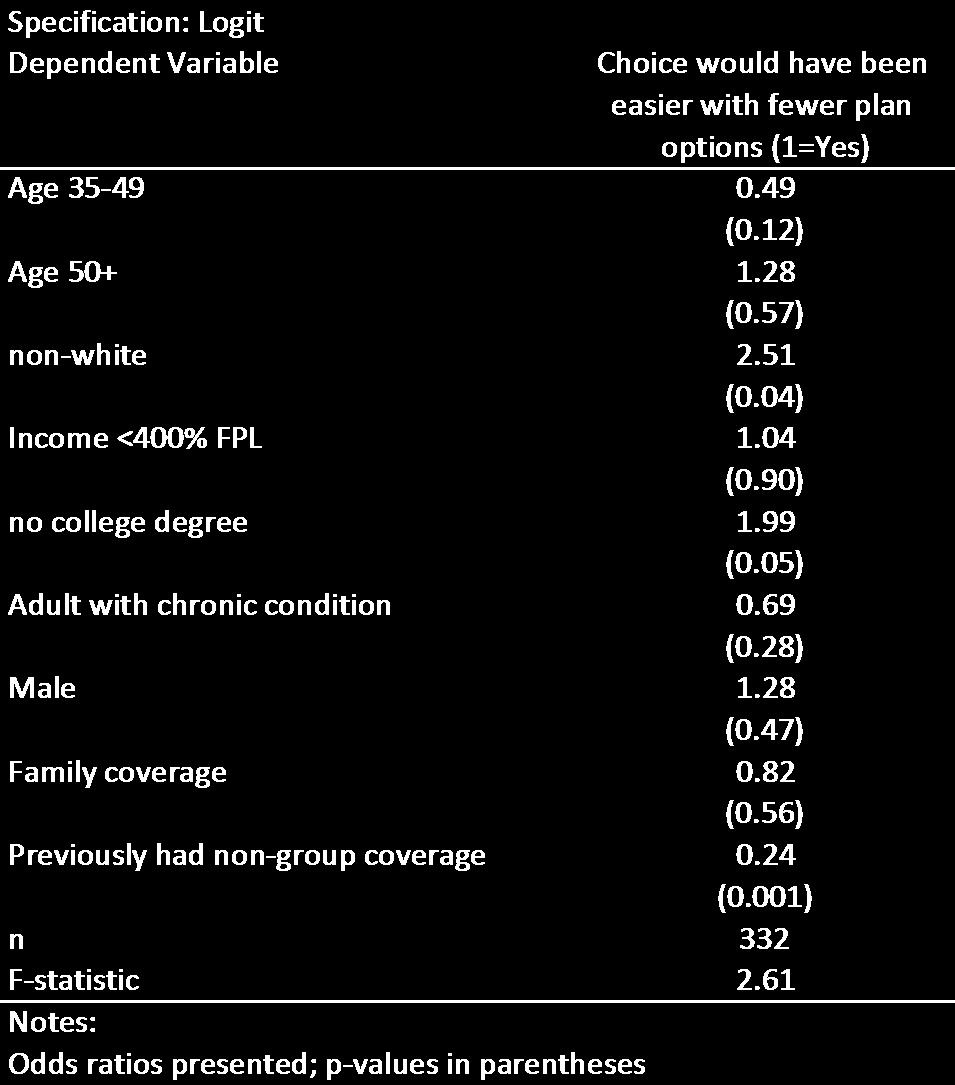
1 Sinaiko AD, Ross-Degnan D, Soumerai SB, Lieu T, Galbraith A. The experience of Massachusetts shows that consumers need help in navidgating insurance exchanges. Health Aff (Millwood). 2013;32(1). Technical Appendix The following tables present the unadjusted results and regression results that underlie the results reported in the paper Consumer Experience in a Health Insurance Exchange: Evidence from Massachusetts.
2 Unadjusted, weighted frequencies
3

4 Logit regression results
5
6
7
8


9 Commonwealth Connector Health Insurance Survey Sponsored by the National Institutes of Health This survey is about the experiences of people and their families in Harvard Pilgrim health insurance plans offered through the Commonwealth Connector. Your opinions are important. Your input will help us to make recommendations to improve health insurance and health care for people throughout the nation. Our records indicate that you have been enrolled in a Harvard Pilgrim health insurance plan from the Commonwealth Connector. We are interested in your experiences in the Harvard Pilgrim Connector plan, as well as the experiences of other family members who may be enrolled in this plan with you. 1. Are you currently enrolled in a Harvard Pilgrim health insurance plan from the Commonwealth Connector? Yes Continue with Question 2 on the next page No What was the main reason you disenrolled from this plan? (check one only) 1 The premium was too expensive 2 The deductibles and/or copays were too high 3 Wanted a better network of health care providers 4 Other insurance coverage became available 5 Employer changed plans or stopped offering coverage 6 Change in employment status 7 Moved out of state 8 Other (specify) Continue with Question 2 on the next page
10 PRIOR TO ENROLLING 2. Just before you enrolled in the Connector plan, what kind of insurance coverage did you have? (check all that apply) Uninsured Insurance from employer or union COBRA A different plan from the Commonwealth Connector Insurance purchased directly from a health plan or broker/agent MassHealth, Medicaid, Commonwealth Care Health Insurance Plan or some other public coverage Insurance through a business or professional association Other (specify) 3. Just before you enrolled in the Connector plan, what kind of insurance coverage did your spouse/partner have? (check all that apply) Not applicable (skip to Question 4) Uninsured Insurance from employer or union COBRA A different plan from the Commonwealth Connector Insurance purchased directly from a health plan or broker/agent MassHealth, Medicaid, Commonwealth Care Health Insurance Plan or some other public coverage Insurance through a business or professional association Other (specify) 4. Just before you enrolled in the Connector plan, what kind of insurance coverage did your children have? (check all that apply) Not applicable (skip to Question 5) Uninsured Insurance from employer or union COBRA A different plan from the Commonwealth Connector Insurance purchased directly from a health plan or broker/agent MassHealth, Medicaid, Commonwealth Care Health Insurance Plan or some other public coverage Insurance through a business or professional association Other (specify)
11 ENROLLING IN THE CONNECTOR PLAN When completing this section, please think about your experiences at the time you were deciding whether to enroll in the Harvard Pilgrim plan from the Commonwealth Connector (referred to below as the Connector plan or your plan ). 5. Were you considering other health plan options outside of the Connector? (check all that apply) Yes, a plan/plans from spouse/partner Yes, a plan/plans available directly from a health insurance plan Yes, a plan/plans available from a broker/agent Yes, COBRA Yes, a plan/plans from another source (specify) No 6. What sources did you use to get information about the Connector health plans? (check all that apply) Internet Print materials Broker/Agent Employer Friend/Family member Physician Social Worker Community service organization The Connector telephone line Other (specify) None
12 ENROLLING IN THE CONNECTOR PLAN 7. How strongly do you agree or disagree with the following statements about the time when you were deciding to enroll in the Connector plan? Strongly Agree Agree Disagree Strongly Disagree a. I would have had an easier time choosing a plan if there were fewer plans to choose from. b. It was hard to understand the information that was available about the different health plans. c. I was satisfied with the affordability of the plan. d. I was satisfied that I found a plan with the type of coverage I needed. e. I was able to get my questions about Connector plans answered. ENROLLIN G IN THE CONNECTOR PLAN 8. Did you have someone help you narrow down your choices to a few plans that were best for you? If yes: Who helped you narrow down your choices? (check all that apply) Broker/Agent Employer Friend/Family member Physician Social Worker Community service organization The Connector telephone line Other (specify) 2 No If no: Did you wish you had someone help you narrow down your choices? 2 No
13 ENROLLING IN THE CONNECTOR PLAN 9. When you were choosing your plan, did you estimate the amount you would have to pay out-of-pocket beyond the monthly premium under the different options available? 1 2 Yes No If yes: Did you compare the total costs among plans, including the estimated out-of-pocket cost and monthly premiums? 2 No 10. Which of the following were reasons you chose your plan? (Check all that apply) Good network of physicians and hospitals Network included a particular doctor Low out-of-pocket costs for services Lower cost of the premium Prior experience with this plan Specific benefits offered by the plan Plan s good reputation, recommended by others Other (specify) 11. Of these, which one was the most important reason you chose your plan? (check one only) 1 Good network of physicians and hospitals 2 Network included a particular doctor 3 Low out-of-pocket costs for services 4 Lower cost of the premium 5 Prior experience with this plan 6 Specific benefits offered by the plan 7 Plan s good reputation, recommended by others 8 Other (specify)
14 YOUR EXPERIENCE IN THE CONNECTOR PLAN When completing this section, please think about your experiences in the Connector plan during the past 12 months. If you are no longer enrolled in the Connector plan from Harvard Pilgrim, please think back to the last 12 months you were enrolled. 12. What is the amount that you pay out-of-pocket for the premium for this plan (not including any amount your employer contributes)? $ Is that payment 1 Weekly 2 Every two weeks 3 Twice a month 4 Monthly 5 Quarterly 6 Yearly 7 Other (specify) 13. Does your employer pay any part of the premium? 2 No 3 No, I am self-employed or the owner of a small business 4 No, I am not currently employed 14. How strongly do you agree or disagree with each of the following statements concerning the Connector plan? a. The plan is easy to understand 1 Strongly Agree 2 Agree 3 Disagree 4 Strongly Disagree b. The plan offers protection in the event of an expensive illness 1 Strongly Agree 2 Agree 3 Disagree 4 Strongly Disagree
15 YOUR EXPERIENCE IN THE CONNECTOR PLAN 15. Did your out-of-pocket costs in the Connector plan end up being as you expected? 2 No, actual costs were higher 3 No, actual costs were lower 16. During the last 12 months, were there times in the Connector plan when you had problems paying or were unable to pay any of your or your family s medical bills? 2 No 17. During the last 12 months in the Connector plan, did you: a. Have to set up a payment plan with a hospital or doctor's office? 2 No b. Have trouble paying for other basic bills like food, heat, or rent because of medical costs for you or a member of your family? 2 No c. Discuss the costs that you would have to pay for your care with your doctor? 2 No 3 Not applicable -- did not go to the doctor in the last 12 months d. Discuss the costs that you would have to pay for your child s health care with your child s doctor? 2 No 3 Not applicable -- no children in plan 4 Not applicable -- child did not go to the doctor in the last 12 months
16 ABOUT YOU AND YOUR FAMILY This next section asks about you and your family. 18. In general, how would you describe your health? 1 Excellent 2 Very good 3 Good 4 Fair 5 Poor 19. Do you or any of the adults in your plan have one of the conditions below, or another chronic condition? (Check all that apply) Abnormal uterine bleeding Arthritis Asthma Benign prostate enlargement Cancer Depression Diabetes Emphysema or lung disease Heart disease Hypertension or high blood pressure Other (write in): No chronic conditions 20. Do any of the children in your plan have one of the conditions below, or another chronic condition? (Check all that apply) No children in the plan (skip to question 22) Asthma Attention Deficit Hyperactivity Disorder/Attention Deficit Disorder (ADHD/ADD) Developmental Delay Diabetes Depression, anxiety, an eating disorder, or other emotional problems Epilepsy or other seizure disorder Other (write in): No chronic conditions 21. Please answer the following question for each child enrolled in the Connector plan with you: In general, how would you describe your child s health? a. Child #1 Excellent Very Good Good Fair Poor b. Child #2 c. Child #3 d. Child #4 e. Child #5
17 ABOUT YOU AND YOUR FAMILY 22. Are you Spanish/Hispanic/Latino? 2 No 23. What is your race? (Check one or more races to indicate what you consider yourself to be.) White Black or African American American Indian or Alaska Native Asian or Pacific Islander Other (specify): 24. What language do you usually speak at home? If you speak more than one, which do you speak most of the time? 1 English 2 Spanish 3 Other (specify): 25. Including you, how many family members live in your household? (write in) 26. In 2009, approximately what was your family s total income from all sources, before taxes? 1 Less than $20,000 6 $60,000 to under $75,000 2 $20,000 to under $30,000 7 $75,000 to under $100,000 3 $30,000 to under $40,000 8 $100,000 to under $125, $40,000 to under $50,000 $125,000 to under $150,000 5 $50,000 to under $60, $150,000 or more 27. What is the highest degree or level of school you completed? 1 8 th grade or less 2 Some high school 3 High school graduate -- high school diploma or equivalent 4 Some college or technical school 5 Bachelor's degree 6 Postgraduate training or degree
18
19 CLAIMS PERMISSION We would like to obtain information from your family s health plan medical claims data for those members in the Harvard Pilgrim Connector plan. These claims are computerized data from Harvard Pilgrim Health Care that show what services your family has used in the past 12 months. The different types of information we would like to collect are claims for hospitalizations, emergency department visits, and outpatient visits, including diagnoses, and prescription medications. The only people who will have access to claims will be the research team. All identifying information, including your name, address and telephone number, will be removed and your information will be used only to come up with averages. 28. Do we have your permission to obtain information from your family s claims? 1 2 Yes No To thank you for your time, we would like to send you a $30 gift card to your choice of Target or CVS. Please check which one you would like. 1 Target 2 CVS The following information is needed to send you the gift card: Name: Street Address: City: State: Zip Code: THANK YOU! Please return this survey by September 30, 2010 using the envelope provided: Commonwealth Connector Survey [Address]
20
More Than One-Quarter of Insured Adults Were Underinsured in 2016
 Exhibit 1 More Than One-Quarter of Insured Adults Were Underinsured in 216 Percent adults ages 19 64 insured all year who were underinsured* 28 22 23 23 2 12 13 1 23 25 21 212 214 216 * Underinsured defined
Exhibit 1 More Than One-Quarter of Insured Adults Were Underinsured in 216 Percent adults ages 19 64 insured all year who were underinsured* 28 22 23 23 2 12 13 1 23 25 21 212 214 216 * Underinsured defined
Table 1. Underinsured Indicators Among Adults Ages Insured All Year, 2003, 2005, 2010, 2012, 2014, 2016
 How Well Does Insurance Coverage Protect Consumers from Health Care Costs? Tables 1 The following tables are supplemental to a Commonwealth Fund issue brief, S. R. Collins, M. Z. Gunja, and M. M. Doty,
How Well Does Insurance Coverage Protect Consumers from Health Care Costs? Tables 1 The following tables are supplemental to a Commonwealth Fund issue brief, S. R. Collins, M. Z. Gunja, and M. M. Doty,
Exhibit ES-1. Nearly Three of Five Adults Who Lost a Job with Health Benefits in Past Two Years Became Uninsured
 Exhibit ES-1. Nearly Three of Five Adults Who Lost a Job with Health Benefits in Past Two Years Became Uninsured Percent of adults ages 19 64 Total
Exhibit ES-1. Nearly Three of Five Adults Who Lost a Job with Health Benefits in Past Two Years Became Uninsured Percent of adults ages 19 64 Total
Alaska Member Opinion Survey Annotated Questionnaire
 Alaska 2012 Member Opinion Survey Annotated Questionnaire 2012 Weighted n= 599; Response Rate=24.0%; Sampling Error= ±3.9% NATIONAL 2012 Weighted n= 36,947; Response Rate=27%; Sampling Error= ±.051% Not
Alaska 2012 Member Opinion Survey Annotated Questionnaire 2012 Weighted n= 599; Response Rate=24.0%; Sampling Error= ±3.9% NATIONAL 2012 Weighted n= 36,947; Response Rate=27%; Sampling Error= ±.051% Not
Rhode Island Member Opinion Survey Annotated Questionnaire
 Rhode Island 2012 Member Opinion Survey Annotated Questionnaire 2012 Weighted n= 683; Response Rate=27.3%; Sampling Error= ±3.7% NATIONAL 2012 Weighted n= 36,947; Response Rate=27%; Sampling Error= ±.051%
Rhode Island 2012 Member Opinion Survey Annotated Questionnaire 2012 Weighted n= 683; Response Rate=27.3%; Sampling Error= ±3.7% NATIONAL 2012 Weighted n= 36,947; Response Rate=27%; Sampling Error= ±.051%
Arizona Member Opinion Survey Annotated Questionnaire
 Arizona 2012 Member Opinion Survey Annotated Questionnaire 2012 Weighted n= 744; Response Rate=29.7%; Sampling Error= ±3.5% NATIONAL 2012 Weighted n= 36,947; Response Rate=27%; Sampling Error= ±.051% Not
Arizona 2012 Member Opinion Survey Annotated Questionnaire 2012 Weighted n= 744; Response Rate=29.7%; Sampling Error= ±3.5% NATIONAL 2012 Weighted n= 36,947; Response Rate=27%; Sampling Error= ±.051% Not
New Hampshire Member Opinion Survey Annotated Questionnaire
 New Hampshire 2012 Member Opinion Survey Annotated Questionnaire 2012 Weighted n= 685; Response Rate=27.4%; Sampling Error= ±3.7% NATIONAL 2012 Weighted n= 36,947; Response Rate=27%; Sampling Error= ±.051%
New Hampshire 2012 Member Opinion Survey Annotated Questionnaire 2012 Weighted n= 685; Response Rate=27.4%; Sampling Error= ±3.7% NATIONAL 2012 Weighted n= 36,947; Response Rate=27%; Sampling Error= ±.051%
Idaho Member Opinion Survey Annotated Questionnaire
 Idaho 2012 Member Opinion Survey Annotated Questionnaire 2012 Weighted n= 767; Response Rate=30.9%; Sampling Error= ±3.5% NATIONAL 2012 Weighted n= 36,947; Response Rate=27%; Sampling Error= ±.051% Not
Idaho 2012 Member Opinion Survey Annotated Questionnaire 2012 Weighted n= 767; Response Rate=30.9%; Sampling Error= ±3.5% NATIONAL 2012 Weighted n= 36,947; Response Rate=27%; Sampling Error= ±.051% Not
Indiana Member Opinion Survey Annotated Questionnaire
 Indiana 2012 Member Opinion Survey Annotated Questionnaire 2012 Weighted n= 723; Response Rate=28.9%; Sampling Error= ±3.6% NATIONAL 2012 Weighted n= 36,947; Response Rate=27%; Sampling Error= ±.051% Not
Indiana 2012 Member Opinion Survey Annotated Questionnaire 2012 Weighted n= 723; Response Rate=28.9%; Sampling Error= ±3.6% NATIONAL 2012 Weighted n= 36,947; Response Rate=27%; Sampling Error= ±.051% Not
Puerto Rico Member Opinion Survey Annotated Questionnaire
 Puerto Rico 2012 Member Opinion Survey Annotated Questionnaire 2012 Weighted n= 680; Response Rate=28.4%; Sampling Error= ±3.7% NATIONAL 2012 Weighted n= 36,947; Response Rate=27%; Sampling Error= ±.051%
Puerto Rico 2012 Member Opinion Survey Annotated Questionnaire 2012 Weighted n= 680; Response Rate=28.4%; Sampling Error= ±3.7% NATIONAL 2012 Weighted n= 36,947; Response Rate=27%; Sampling Error= ±.051%
HealthyCare Card Application
 HealthyCare Card Application This is an application for the HealthyCare Card, a program of Healthy Community Network. The HealthyCare Card (HCC) is a community program which provides discounts to care
HealthyCare Card Application This is an application for the HealthyCare Card, a program of Healthy Community Network. The HealthyCare Card (HCC) is a community program which provides discounts to care
Long-Term Carein Connecticut:ASurvey
 Long-Term Carein Connecticut:ASurvey ofaarpmembers April2008 Long-Term Care in Connecticut: A Survey of AARP Members Report Prepared by Katherine Bridges Copyright 2008 AARP Knowledge Management 601 E
Long-Term Carein Connecticut:ASurvey ofaarpmembers April2008 Long-Term Care in Connecticut: A Survey of AARP Members Report Prepared by Katherine Bridges Copyright 2008 AARP Knowledge Management 601 E
Patient Identification Form
 Identification Information Weill Cornell Community Clinic Patient Identification Form Today s Date: / / Name: (last) (first) (middle) DOB (mm/dd/yyyy): / / Current Address: (street) (city) (state) (zip)
Identification Information Weill Cornell Community Clinic Patient Identification Form Today s Date: / / Name: (last) (first) (middle) DOB (mm/dd/yyyy): / / Current Address: (street) (city) (state) (zip)
Issue Brief. Findings From the 2007 EBRI/Commonwealth Fund Consumerism in Health Survey. No March 2008
 Issue Brief No. 315 March 2008 Findings From the 2007 EBRI/Commonwealth Fund Consumerism in Health Survey By Paul Fronstin, EBRI, and Sara R. Collins, The Commonwealth Fund Third annual survey This Issue
Issue Brief No. 315 March 2008 Findings From the 2007 EBRI/Commonwealth Fund Consumerism in Health Survey By Paul Fronstin, EBRI, and Sara R. Collins, The Commonwealth Fund Third annual survey This Issue
CENTRAL OHIO PLASTIC SURGERY, INC. (740)
") (740) 653-5064 Patient s Name Patient Information as of (enter today s date) (Please Print Legibly & Fill In or Correct All Fields) Last First Middle Nickname Address Street & Apt # City State Zip Home
(740) 653-5064 Patient s Name Patient Information as of (enter today s date) (Please Print Legibly & Fill In or Correct All Fields) Last First Middle Nickname Address Street & Apt # City State Zip Home
A Medicare Information
 Alaska Medicare Supplement Enrollment Application for Plans A, F, High Deductible F, G and N P.O. Box 327, MS 295 Seattle, WA 98111-9220 1-888-669-2583 Fax: 425-918-5278 You are eligible to apply for a
Alaska Medicare Supplement Enrollment Application for Plans A, F, High Deductible F, G and N P.O. Box 327, MS 295 Seattle, WA 98111-9220 1-888-669-2583 Fax: 425-918-5278 You are eligible to apply for a
How Well Does Insurance Coverage Protect Consumers from Health Care Costs?
 How Well Does Insurance Coverage Protect Consumers from Health Care Costs? Findings from the Commonwealth Fund Biennial Health Insurance Survey, 216 Sara R. Collins, Ph.D. Vice President, Health Care Coverage
How Well Does Insurance Coverage Protect Consumers from Health Care Costs? Findings from the Commonwealth Fund Biennial Health Insurance Survey, 216 Sara R. Collins, Ph.D. Vice President, Health Care Coverage
Figure ES-1. Difficulty Getting Care on Nights, Weekends, Holidays Without Going to ER
 Figure ES-1. Difficulty Getting Care on Nights, Weekends, Holidays Without Going to ER Percent saying very or somewhat difficult 1 53 56 6 59 32 32 42 44 7 * 6 * Significant difference between below and
Figure ES-1. Difficulty Getting Care on Nights, Weekends, Holidays Without Going to ER Percent saying very or somewhat difficult 1 53 56 6 59 32 32 42 44 7 * 6 * Significant difference between below and
Health Care in California: The Chronically Ill
 Health Care in California: The Chronically Ill A report for the California HealthCare Foundation prepared by Prepared for the California HealthCare Foundation by Harris Interactive Contents About this
Health Care in California: The Chronically Ill A report for the California HealthCare Foundation prepared by Prepared for the California HealthCare Foundation by Harris Interactive Contents About this
Early Experience With High-Deductible and Consumer-Driven Health Plans: Findings From the EBRI/ Commonwealth Fund Consumerism in Health Care Survey
 Issue Brief No. 288 December 2005 Early Experience With High-Deductible and Consumer-Driven Health Plans: Findings From the EBRI/ Commonwealth Fund Consumerism in Health Care Survey by Paul Fronstin, EBRI,
Issue Brief No. 288 December 2005 Early Experience With High-Deductible and Consumer-Driven Health Plans: Findings From the EBRI/ Commonwealth Fund Consumerism in Health Care Survey by Paul Fronstin, EBRI,
Continued on Reverse Side
 PATIENT REGISTRATION FORM Date Male Female First Middle Last Email Address Mailing Address City State Zip Code Home Phone Work Phone Cell Phone Social Security Date of Birth Ethnicity: Hispanic or Latino
PATIENT REGISTRATION FORM Date Male Female First Middle Last Email Address Mailing Address City State Zip Code Home Phone Work Phone Cell Phone Social Security Date of Birth Ethnicity: Hispanic or Latino
VASCULAR HEART & LUNG ASSOCIATES
 PATIENT INFORMATION Last Name: First Name: M.I: Address: City: State: ZIP: Telephone (Cell): (Home): (Circle preferred contact method). Email: Date of Birth (MM/DD/YEAR): / / Age: Sex: SS# Ethnicity [circle]:
PATIENT INFORMATION Last Name: First Name: M.I: Address: City: State: ZIP: Telephone (Cell): (Home): (Circle preferred contact method). Email: Date of Birth (MM/DD/YEAR): / / Age: Sex: SS# Ethnicity [circle]:
Massachusetts Application for Health and Dental Coverage and Help Paying Costs
 Massachusetts Application for Health and Dental Coverage and Help Paying Costs HOW TO APPLY USE THIS APPLICATION TO SEE WHAT COVERAGE CHOICES YOU MAY QUALIFY FOR. WHO CAN USE THIS APPLICATION? You can
Massachusetts Application for Health and Dental Coverage and Help Paying Costs HOW TO APPLY USE THIS APPLICATION TO SEE WHAT COVERAGE CHOICES YOU MAY QUALIFY FOR. WHO CAN USE THIS APPLICATION? You can
Citizens Health Care Working Group Wesson, Mississippi Listening Session March 29, 2006 Data Sheet
 Wesson, Mississippi Data Sheet Percent Total A Are you male or female? 42.9% 3 1 Male 57.1% 4 2 Female Percent Total B How old are you? 0.0% 1 Under 25 14.3% 1 2 25 to 44 85.7% 6 3 45 to 64 0.0% 4 Over
Wesson, Mississippi Data Sheet Percent Total A Are you male or female? 42.9% 3 1 Male 57.1% 4 2 Female Percent Total B How old are you? 0.0% 1 Under 25 14.3% 1 2 25 to 44 85.7% 6 3 45 to 64 0.0% 4 Over
AFFORDABLE CARE ACT FAQ
 AFFORDABLE CARE ACT FAQ What is the Healthcare Insurance Marketplace? The Marketplace is a new way to find quality health coverage. It can help if you don t have coverage now or if you have it but want
AFFORDABLE CARE ACT FAQ What is the Healthcare Insurance Marketplace? The Marketplace is a new way to find quality health coverage. It can help if you don t have coverage now or if you have it but want
Application for Health Coverage and Help Paying Costs Instructions
 Application for Health Coverage and Help Paying Costs Instructions Commonwealth of Massachusetts EOHHS Please read these instructions before you fill out the application. Apply faster online! Go to: MAhealthconnector.org.
Application for Health Coverage and Help Paying Costs Instructions Commonwealth of Massachusetts EOHHS Please read these instructions before you fill out the application. Apply faster online! Go to: MAhealthconnector.org.
Chart Book: The Far-Reaching Benefits of the Affordable Care Act s Medicaid Expansion
 820 First Street NE, Suite 510 Washington, DC 20002 Tel: 202-408-1080 Fax: 202-408-1056 center@cbpp.org www.cbpp.org October 2, 2018 Chart Book: The Far-Reaching Benefits of the Affordable Care Act s Medicaid
820 First Street NE, Suite 510 Washington, DC 20002 Tel: 202-408-1080 Fax: 202-408-1056 center@cbpp.org www.cbpp.org October 2, 2018 Chart Book: The Far-Reaching Benefits of the Affordable Care Act s Medicaid
2005 Health Confidence Survey Wave VIII
 2005 Health Confidence Survey Wave VIII June 30 August 6, 2005 Hello, my name is [FIRST AND LAST NAME]. I am calling from National Research, a research firm in Washington, D.C. May I speak to the youngest
2005 Health Confidence Survey Wave VIII June 30 August 6, 2005 Hello, my name is [FIRST AND LAST NAME]. I am calling from National Research, a research firm in Washington, D.C. May I speak to the youngest
National Survey of Enrollees in Consumer Directed Health Plans
 Chartpack Kaiser Family Foundation National Survey of Enrollees in Consumer Directed Health Plans November 2006 Methodology The National Survey of Enrollees in Consumer Directed Health Plans was designed,
Chartpack Kaiser Family Foundation National Survey of Enrollees in Consumer Directed Health Plans November 2006 Methodology The National Survey of Enrollees in Consumer Directed Health Plans was designed,
The Impact of Program Changes on Health Care for the OHP Standard Population: Early Results from a Prospective Cohort Study
 Portland State University PDXScholar Sociology Faculty Publications and Presentations Sociology 2004 The Impact of Program Changes on Health Care for the OHP Standard Population: Early Results from a Prospective
Portland State University PDXScholar Sociology Faculty Publications and Presentations Sociology 2004 The Impact of Program Changes on Health Care for the OHP Standard Population: Early Results from a Prospective
PATIENT REGISTRATION / INFORMATION SHEET
 PATIENT REGISTRATION / INFORMATION SHEET Name: LAST FIRST MIDDLE Date of Birth: Gender: M F Marital Status: Social Security Number: Email Address*: Street Address: City: State: Zip: Home Phone: Cell Phone:
PATIENT REGISTRATION / INFORMATION SHEET Name: LAST FIRST MIDDLE Date of Birth: Gender: M F Marital Status: Social Security Number: Email Address*: Street Address: City: State: Zip: Home Phone: Cell Phone:
Mark A. Gapinski, MD, SC 25 N. Winfield Road, Suite 511 Winfield, IL
 Mark A. Gapinski, MD, SC 25 N. Winfield Road, Suite 511 Winfield, IL 60190 630-462-4963 Dear Patient, Thank you for choosing Dr. Mark Gapinski s office for your gynecological care! Please fill out the
Mark A. Gapinski, MD, SC 25 N. Winfield Road, Suite 511 Winfield, IL 60190 630-462-4963 Dear Patient, Thank you for choosing Dr. Mark Gapinski s office for your gynecological care! Please fill out the
Issue Brief. Does Medicaid Make a Difference? The COMMONWEALTH FUND. Findings from the Commonwealth Fund Biennial Health Insurance Survey, 2014
 Issue Brief JUNE 2015 The COMMONWEALTH FUND Does Medicaid Make a Difference? Findings from the Commonwealth Fund Biennial Health Insurance Survey, 2014 The mission of The Commonwealth Fund is to promote
Issue Brief JUNE 2015 The COMMONWEALTH FUND Does Medicaid Make a Difference? Findings from the Commonwealth Fund Biennial Health Insurance Survey, 2014 The mission of The Commonwealth Fund is to promote
ALPINE SCHOOL DISTRICT
 ALPINE SCHOOL DISTRICT LUNCH AND BREAKFAST PAYMENT OPTIONS Payments for meals can be made to your school lunch manager, or at the Food Service Office, 490 North State, Lindon, Utah 84042 Payments may also
ALPINE SCHOOL DISTRICT LUNCH AND BREAKFAST PAYMENT OPTIONS Payments for meals can be made to your school lunch manager, or at the Food Service Office, 490 North State, Lindon, Utah 84042 Payments may also
Andrea Simons, DPM Davina Cross, DPM Schavey Road, Suite 2, DeWitt, MI (517) Patient History. Name: (First) (MI) (Last)
 Patient History. Name: (First) (MI) (Last)") Today s : Andrea Simons, DPM Davina Cross, DPM 13105 Schavey Road, Suite 2, DeWitt, MI 48820 (517) 668-6166 Patient History of Birth: Social Security #: Name: (First) (MI) (Last) Prefers to be called Address:
Today s : Andrea Simons, DPM Davina Cross, DPM 13105 Schavey Road, Suite 2, DeWitt, MI 48820 (517) 668-6166 Patient History of Birth: Social Security #: Name: (First) (MI) (Last) Prefers to be called Address:
New Patient Information
 New Patient Information LAST FIRST NAME NAME M.I. DATE OF SOC. MARITAL BIRTH SEC. SEX STATUS PRIMARY ADDRESS PHONE CELL CITY STATE ZIP PHONE WORK EMPLOYER PHONE REFERRING/ LAST YOUR PRIMARY PHYSICIAN SEEN
New Patient Information LAST FIRST NAME NAME M.I. DATE OF SOC. MARITAL BIRTH SEC. SEX STATUS PRIMARY ADDRESS PHONE CELL CITY STATE ZIP PHONE WORK EMPLOYER PHONE REFERRING/ LAST YOUR PRIMARY PHYSICIAN SEEN
Sara R. Collins, Ph.D. Vice President, Health Care Coverage and Access The Commonwealth Fund. Alliance for Health Reform Briefing July 11, 2014
 Health Insurance Coverage and Access to Care After the Affordable Care Act s First Open Enrollment Period: Findings from The Commonwealth Fund Affordable Care Act Tracking Survey, April-June 2014 Sara
Health Insurance Coverage and Access to Care After the Affordable Care Act s First Open Enrollment Period: Findings from The Commonwealth Fund Affordable Care Act Tracking Survey, April-June 2014 Sara
Referring Physician: Primary Care Physician: Other Physician(s)/Specialty: EMERGENCY CONTACT INFORMATION INSURANCE INFORMATION
/Specialty: EMERGENCY CONTACT INFORMATION INSURANCE INFORMATION") PATIENT INFORMATION Name: Date of Birth: Sex: Male Status: Single Married Divorced Widowed Other 502 Elm Street NE Language: Female Race: American Indian or Alaska Native Native Hawaiian or Or Pacific
PATIENT INFORMATION Name: Date of Birth: Sex: Male Status: Single Married Divorced Widowed Other 502 Elm Street NE Language: Female Race: American Indian or Alaska Native Native Hawaiian or Or Pacific
HAMILTON FOOT AND ANKLE CARE, LLC 9865 E. 116 th St. #300 Fishers, IN (317)
") HAMILTON FOOT AND ANKLE CARE, LLC 9865 E. 116 th St. #300 Fishers, IN 46037 (317)-284-8888 Patient Name: Date of Birth: / / First MI Last SS#: Address: City: State: Zip Code: Cell Phone: ( ) - Home Phone:
HAMILTON FOOT AND ANKLE CARE, LLC 9865 E. 116 th St. #300 Fishers, IN 46037 (317)-284-8888 Patient Name: Date of Birth: / / First MI Last SS#: Address: City: State: Zip Code: Cell Phone: ( ) - Home Phone:
EMPLOYEE S GROUP ENROLLMENT APPLICATION
 EMPLOYEE S GROUP ENROLLMENT APPLICATION Wisconsin Physicians Services Insurance Corporation ( WPS )( Insurer ) or Third Party Administrator ( TPA ) does NOT guarantee approval of this application for any
EMPLOYEE S GROUP ENROLLMENT APPLICATION Wisconsin Physicians Services Insurance Corporation ( WPS )( Insurer ) or Third Party Administrator ( TPA ) does NOT guarantee approval of this application for any
Health Insurance and Health Care Affordability Perceptions Among Individual Insurance Market Enrollees in California in 2017
 Insurance and Care Affordability Perceptions Among Individual Insurance Market Enrollees in California in 27 Authors: Vicki Fung, PhD, Catherine Liang, John Hsu, MD, MPH Affiliations: The Mongan Institute
Insurance and Care Affordability Perceptions Among Individual Insurance Market Enrollees in California in 27 Authors: Vicki Fung, PhD, Catherine Liang, John Hsu, MD, MPH Affiliations: The Mongan Institute
PATIENT INFORMATION DATE: / / SS # - - DOB: / / NAME: (last) (first) (middle) ADDRESS: CITY: STATE: ZIP: PHONE (HOME): (CELL):
 (first) (middle) ADDRESS: CITY: STATE: ZIP: PHONE (HOME): (CELL):") ADULT NEW PATIENT PACKET PATIENT INFORMATION DOCTOR: DATE: / / SS # - - DOB: / / NAME: (last) (first) (middle) ADDRESS: CITY: STATE: ZIP: PHONE (HOME): (CELL): EMAIL: GENDER: M F Marital Status APPOINTMENT
ADULT NEW PATIENT PACKET PATIENT INFORMATION DOCTOR: DATE: / / SS # - - DOB: / / NAME: (last) (first) (middle) ADDRESS: CITY: STATE: ZIP: PHONE (HOME): (CELL): EMAIL: GENDER: M F Marital Status APPOINTMENT
New York City Has a Higher Percentage of Uninsured than Does New York State or the Nation
 New York City Has a Higher Percentage of Uninsured than Does New York State or the Nation Percent uninsured 3 28% 19% 19% 1 National* New York State* New York City* *Source: March 1996 Current Population
New York City Has a Higher Percentage of Uninsured than Does New York State or the Nation Percent uninsured 3 28% 19% 19% 1 National* New York State* New York City* *Source: March 1996 Current Population
Insurance, Access, and Quality of Care Among Hispanic Populations Chartpack
 Insurance, Access, and Quality of Care Among Hispanic Populations 23 Chartpack Prepared by Michelle M. Doty The Commonwealth Fund For the National Alliance for Hispanic Health Meeting October 15 17, 23
Insurance, Access, and Quality of Care Among Hispanic Populations 23 Chartpack Prepared by Michelle M. Doty The Commonwealth Fund For the National Alliance for Hispanic Health Meeting October 15 17, 23
EMI HEALTH MEDIGAP APPLICATION - WEBSITE
 EMI Health 5101 S. Commerce Dr. Murray, Ut ah 84107 801-262-7475 EMI HEALTH MEDIGAP APPLICATION - WEBSITE Please select one - this application request is for: Open Enrollment If you are applying for coverage
EMI Health 5101 S. Commerce Dr. Murray, Ut ah 84107 801-262-7475 EMI HEALTH MEDIGAP APPLICATION - WEBSITE Please select one - this application request is for: Open Enrollment If you are applying for coverage
The Importance of Health Coverage
 The Importance of Health Coverage Today, approximately 90 percent of U.S. residents have health insurance with significant gains in health coverage occuring over the past five years. Health insurance facilitates
The Importance of Health Coverage Today, approximately 90 percent of U.S. residents have health insurance with significant gains in health coverage occuring over the past five years. Health insurance facilitates
Exhibit 1. Nearly Three of Five Adults Who Lost a Job with Health Benefits in the Past Two Years Became Uninsured
 Exhibit 1. Nearly Three of Five Adults Who Lost a Job with Health Benefits in the Past Two Years Became Uninsured Percent of adults ages 19 64 Total^
Exhibit 1. Nearly Three of Five Adults Who Lost a Job with Health Benefits in the Past Two Years Became Uninsured Percent of adults ages 19 64 Total^
PATIENT REGISTRATION FORM
 Patient Information PATIENT REGISTRATION FORM (Name) First: M.I. Last: Address: City: State: Zip: D.O.B. Email: (Phones) Home: Cell: Work: Fill out both above and below section with patient information,
Patient Information PATIENT REGISTRATION FORM (Name) First: M.I. Last: Address: City: State: Zip: D.O.B. Email: (Phones) Home: Cell: Work: Fill out both above and below section with patient information,
PATIENT INTAKE AND MEDICAL INFORMATION
 PATIENT INTAKE AND MEDICAL INFORMATION PATIENT INFORMATION: Todays Date: DOB: GENDER: M F SSN (required): Marital Status: Divorced Married Separated Single Widowed Address: City: State: Zip: Phone (H):
PATIENT INTAKE AND MEDICAL INFORMATION PATIENT INFORMATION: Todays Date: DOB: GENDER: M F SSN (required): Marital Status: Divorced Married Separated Single Widowed Address: City: State: Zip: Phone (H):
SOUTH SHORE NEPHROLOGY, P.C.
 SOUTH SHORE NEPHROLOGY, P.C. Please fill out this form along with all the documents included in the patient packet and bring it with you for your upcoming appointment. Be sure to bring your insurance card(s)
SOUTH SHORE NEPHROLOGY, P.C. Please fill out this form along with all the documents included in the patient packet and bring it with you for your upcoming appointment. Be sure to bring your insurance card(s)
ASSESSING THE RESULTS
 HEALTH REFORM IN MASSACHUSETTS EXPANDING TO HEALTH INSURANCE ASSESSING THE RESULTS May 2012 Health Reform in Massachusetts, Expanding Access to Health Insurance Coverage: Assessing the Results pulls together
HEALTH REFORM IN MASSACHUSETTS EXPANDING TO HEALTH INSURANCE ASSESSING THE RESULTS May 2012 Health Reform in Massachusetts, Expanding Access to Health Insurance Coverage: Assessing the Results pulls together
CareFirst Applicants
 CareFirst Applicants Application Instructions for Care First 1.Print all pages of the application including instructions 2.Complete all questions and sections of the application. 3.Select your preferred
CareFirst Applicants Application Instructions for Care First 1.Print all pages of the application including instructions 2.Complete all questions and sections of the application. 3.Select your preferred
Mailing Address: Name: FIRST MIDDLE LAST. Mailing address: If different from patient. Telephone Numbers: Home Day Number
 Dermatology Center South PC 2800 Ross Clark Circle, Suite 2 DOTHAN, ALABAMA 36301 REGISTRATION FORM FOR DEPENDENTS] Patietnt Name: First Middle Initial Last of Birth: / / Sex: Male Female Month Day Year
Dermatology Center South PC 2800 Ross Clark Circle, Suite 2 DOTHAN, ALABAMA 36301 REGISTRATION FORM FOR DEPENDENTS] Patietnt Name: First Middle Initial Last of Birth: / / Sex: Male Female Month Day Year
kaiser medicaid commission on and the uninsured How Will Health Reform Impact Young Adults? By Karyn Schwartz and Tanya Schwartz Executive Summary
 I S S U E P A P E R kaiser commission on medicaid and the uninsured How Will Health Reform Impact Young Adults? By Karyn Schwartz and Tanya Schwartz Executive Summary May 2010 The health reform law that
I S S U E P A P E R kaiser commission on medicaid and the uninsured How Will Health Reform Impact Young Adults? By Karyn Schwartz and Tanya Schwartz Executive Summary May 2010 The health reform law that
DRS. NUSSBAUM, LUNDBERG, ALTMAN & PICKETT David N. Nussbaum, DPM, Lori A. Lundberg, DPM Scott Altman, DPM & Scott Pickett, DPM WELCOME TO OUR OFFICE
 DRS. NUSSBAUM, LUNDBERG, ALTMAN & PICKETT David N. Nussbaum, DPM, Lori A. Lundberg, DPM Scott Altman, DPM & Scott Pickett, DPM 35 Five Mile Woods Road 67 Prospect Avenue, Suite 140 Catskill, New York 12414
DRS. NUSSBAUM, LUNDBERG, ALTMAN & PICKETT David N. Nussbaum, DPM, Lori A. Lundberg, DPM Scott Altman, DPM & Scott Pickett, DPM 35 Five Mile Woods Road 67 Prospect Avenue, Suite 140 Catskill, New York 12414
Minnesota State Survey Annotated Questionnaire Weighted n=402; Sampling Error= ±5.0%
 S1. Are you over or under age 50? 50 and over 100% 49 or younger 0% S2. May I speak to someone in your household who is age 50 or older? Yes 100% No 0% S3. Are you a resident of... Minnesota 2011 53 State
S1. Are you over or under age 50? 50 and over 100% 49 or younger 0% S2. May I speak to someone in your household who is age 50 or older? Yes 100% No 0% S3. Are you a resident of... Minnesota 2011 53 State
2010 HEALTH INSURANCE SURVEY
 2010 HEALTH INSURANCE SURVEY PRINCETON SURVEY RESEARCH ASSOCIATES FOR THE COMMONWEALTH FUND FINAL QUESTIONNAIRE LANDLINE INTRODUCTION: Hello, I am calling for Princeton Survey Research. We are conducting
2010 HEALTH INSURANCE SURVEY PRINCETON SURVEY RESEARCH ASSOCIATES FOR THE COMMONWEALTH FUND FINAL QUESTIONNAIRE LANDLINE INTRODUCTION: Hello, I am calling for Princeton Survey Research. We are conducting
Employee Enrollment Form
 Employee Enrollment Form (DO NOT STAPLE) To speed the enrollment process, please be thorough and fill out all sections that apply. Group To Be Name Completed by Employer Requested Effective Date of Coverage/Date
Employee Enrollment Form (DO NOT STAPLE) To speed the enrollment process, please be thorough and fill out all sections that apply. Group To Be Name Completed by Employer Requested Effective Date of Coverage/Date
Massachusetts Health Reform Tracking Survey
 Toplines Kaiser Family Foundation/Harvard School of Public Health/Blue Cross Blue Shield of Massachusetts Foundation Massachusetts Health Reform Tracking Survey June 2007 Methodology The Kaiser Family
Toplines Kaiser Family Foundation/Harvard School of Public Health/Blue Cross Blue Shield of Massachusetts Foundation Massachusetts Health Reform Tracking Survey June 2007 Methodology The Kaiser Family
PATIENT INFORMATION FORM RICHARD L. MALINICK, M.D. ORTHOPAEDIC SURGERY 1125 Via Verde, San Dimas, CA
 Email Address Last Name First Name Previous Name Address City State Zip Country Social Security - - Home Phone - - Cell Phone - - Work Phone - - Ext Drivers License State Responsible Party SELF (use info
Email Address Last Name First Name Previous Name Address City State Zip Country Social Security - - Home Phone - - Cell Phone - - Work Phone - - Ext Drivers License State Responsible Party SELF (use info
QUESTIONS? AGE 65 AND OLDER? NEED PRESCRIPTION HELP? APPLY ANYTIME * APPLICATION ENCLOSED * PACE AND PACENET CALL CARDHOLDER SERVICES
 QUESTIONS? CALL CARDHOLDER SERVICES 1-800-225-7223 Hearing Impaired Callers Using TTY/TDD should call: 1-800-222-9004 24 HOUR FAX NUMBER 1-888-656-0372 EMAIL ADDRESS papace@magellanhealth.com Teresa Tom
QUESTIONS? CALL CARDHOLDER SERVICES 1-800-225-7223 Hearing Impaired Callers Using TTY/TDD should call: 1-800-222-9004 24 HOUR FAX NUMBER 1-888-656-0372 EMAIL ADDRESS papace@magellanhealth.com Teresa Tom
Massachusetts Application for Free and Reduced Price School Meals
 Grade STEP 1 2016-2017 Massachusetts Application for Free and Reduced Price School Meals If you have received a Notice of Direct Certification from the school district for free meals, do not complete this
Grade STEP 1 2016-2017 Massachusetts Application for Free and Reduced Price School Meals If you have received a Notice of Direct Certification from the school district for free meals, do not complete this
Uninsured Americans with Chronic Health Conditions:
 Uninsured Americans with Chronic Health Conditions: Key Findings from the National Health Interview Survey Prepared for the Robert Wood Johnson Foundation by The Urban Institute and the University of Maryland,
Uninsured Americans with Chronic Health Conditions: Key Findings from the National Health Interview Survey Prepared for the Robert Wood Johnson Foundation by The Urban Institute and the University of Maryland,
OFFICE VISIT CHECKLIST
 Eau Claire Location: 3802 W Oakwood Mall Drive * Telephone 715.839.9280 * Fax 715.839.9348 Chippewa Falls Location: 2829 County Highway I, Suite 2A * Telephone 715.839.9280 * Fax 715.726.2087 OFFICE VISIT
Eau Claire Location: 3802 W Oakwood Mall Drive * Telephone 715.839.9280 * Fax 715.839.9348 Chippewa Falls Location: 2829 County Highway I, Suite 2A * Telephone 715.839.9280 * Fax 715.726.2087 OFFICE VISIT
Nebraska Ryan White Program
 For office use only: Date Received: MR#: Nebraska Ryan White Program Application Information Date: Check all the programs applying for: Part B Part C Part D ADAP ADAP co-payment assistance Wait list If
For office use only: Date Received: MR#: Nebraska Ryan White Program Application Information Date: Check all the programs applying for: Part B Part C Part D ADAP ADAP co-payment assistance Wait list If
Health Care Costs Survey
 Summary and Chartpack The USA Today/Kaiser Family Foundation/Harvard School of Public Health Health Care Costs Survey August 2005 Methodology The USA Today/Kaiser Family Foundation/Harvard University Survey
Summary and Chartpack The USA Today/Kaiser Family Foundation/Harvard School of Public Health Health Care Costs Survey August 2005 Methodology The USA Today/Kaiser Family Foundation/Harvard University Survey
Application for Health Coverage & Help Paying Costs
 Application for Health Coverage & Help Paying Costs Use this application to see what coverage choices you qualify for Affordable private health insurance plans that offer comprehensive coverage to help
Application for Health Coverage & Help Paying Costs Use this application to see what coverage choices you qualify for Affordable private health insurance plans that offer comprehensive coverage to help
Eye Associates of Georgetown, LLPC
 Eye Associates of Georgetown, LLPC Paige Quinlivan, O.D. & David Quinlivan, O.D. Mr. Mrs. Ms. Miss. Rev. Dr. Name : (Last) (First) (Mid. Intl.) Nickname: (if any) Address: City: State: Zip Code Cell Phone:
Eye Associates of Georgetown, LLPC Paige Quinlivan, O.D. & David Quinlivan, O.D. Mr. Mrs. Ms. Miss. Rev. Dr. Name : (Last) (First) (Mid. Intl.) Nickname: (if any) Address: City: State: Zip Code Cell Phone:
Chiropractic Case History / Patient Information
 Chiropractic Case History / Patient Information Date: Name: Social Security #: Home Phone:( ) Address: City: State: Zip: E mail address: Cell Phone:( ) Age: Birth Date: / / Marital Status: M S W D Occupation:
Chiropractic Case History / Patient Information Date: Name: Social Security #: Home Phone:( ) Address: City: State: Zip: E mail address: Cell Phone:( ) Age: Birth Date: / / Marital Status: M S W D Occupation:
Welcome to Compass Medical!
 ELECTRONIC FORM DISCLAIMER: Compass Medical is deeply committed to protecting our patient's rights to privacy and safeguarding patient information. Please know we are working hard to bring our patients
ELECTRONIC FORM DISCLAIMER: Compass Medical is deeply committed to protecting our patient's rights to privacy and safeguarding patient information. Please know we are working hard to bring our patients
Understanding Obamacare
 Understanding Obamacare What is The Affordable Care Act? The stated purpose of The Patient Protection and Affordable Care Act or Affordable Care Act, or ACA, or Obamacare is to "increase the number of
Understanding Obamacare What is The Affordable Care Act? The stated purpose of The Patient Protection and Affordable Care Act or Affordable Care Act, or ACA, or Obamacare is to "increase the number of
NEW PATIENT INFORMATION
 NEW PATIENT INFORMATION PATIENT Last Name First Name Email Address FIT Box Address City INSURED PARTY Company Policy No. Group No. Policy Holder Policy Holder DOB Phone State ZIP Cell or Home Phone Student
NEW PATIENT INFORMATION PATIENT Last Name First Name Email Address FIT Box Address City INSURED PARTY Company Policy No. Group No. Policy Holder Policy Holder DOB Phone State ZIP Cell or Home Phone Student
Illinois Standard Health Employee Application for Small Employers
 Illinois Standard Health Employee Application for Small Employers INSURER USE ONLY Policy/Group No. Section No. Effective Date New Hire Waiting Period For assistance in completing this application, please
Illinois Standard Health Employee Application for Small Employers INSURER USE ONLY Policy/Group No. Section No. Effective Date New Hire Waiting Period For assistance in completing this application, please
Policy Brief. protection?} Do the insured have adequate. The Impact of Health Reform on Underinsurance in Massachusetts:
 protection?} The Impact of Health Reform on Underinsurance in Massachusetts: Do the insured have adequate Reform Policy Brief Massachusetts Health Reform Survey Policy Brief {PREPARED BY} Sharon K. Long
protection?} The Impact of Health Reform on Underinsurance in Massachusetts: Do the insured have adequate Reform Policy Brief Massachusetts Health Reform Survey Policy Brief {PREPARED BY} Sharon K. Long
Family Foot and Ankle Centers Patient Registration Form (Please present your insurance cards to the receptionist upon arrival)
") Family Foot and Ankle Centers Patient Registration Form (Please present your insurance cards to the receptionist upon arrival) Patient s Name First Last M.I. Nickname Address # City State Zip code Phone:
Family Foot and Ankle Centers Patient Registration Form (Please present your insurance cards to the receptionist upon arrival) Patient s Name First Last M.I. Nickname Address # City State Zip code Phone:
Saline Heart Group, PA
 www.salineheartgroup.com Patient Account # Date: Patient Information In order for us to provide you with the best possible care, please fill out these forms as completely and accurately as possible. Last
www.salineheartgroup.com Patient Account # Date: Patient Information In order for us to provide you with the best possible care, please fill out these forms as completely and accurately as possible. Last
FINANCIAL POLICY AND AGREEMENT
 FINANCIAL POLICY AND AGREEMENT Our office is committed to providing excellent, affordable medical care. You have the right and responsibility of knowing the cost of your medical treatment. Should you be
FINANCIAL POLICY AND AGREEMENT Our office is committed to providing excellent, affordable medical care. You have the right and responsibility of knowing the cost of your medical treatment. Should you be
Exhibit 1. One-Quarter of All U.S. Working-Age Adults Have Visited the Health Insurance Marketplaces
 Exhibit 1. One-Quarter of All U.S. Working-Age Adults Have Visited the Health Insurance Marketplaces Have you gone to this new marketplace to shop for health insurance? This could be by mail, in person,
Exhibit 1. One-Quarter of All U.S. Working-Age Adults Have Visited the Health Insurance Marketplaces Have you gone to this new marketplace to shop for health insurance? This could be by mail, in person,
Burnet Eye Care & Llano Eye Care P.O. Box 426 Burnet, TX phone 102 E Young St Llano, TX phone
 Burnet Eye Care & Llano Eye Care P.O. Box 426 Burnet, TX 78611 512-756-2131 phone 102 E Young St Llano, TX 78643 325-247-2020 phone PATIENT REGISTRATION Patient s Name Today's Date Mailing Address City
Burnet Eye Care & Llano Eye Care P.O. Box 426 Burnet, TX 78611 512-756-2131 phone 102 E Young St Llano, TX 78643 325-247-2020 phone PATIENT REGISTRATION Patient s Name Today's Date Mailing Address City
First Middle Last Nickname (if any) Present Age Date of Birth
 Present Age Date of Birth") EMERGENCY CONTACTS SIBLINGS INSURANCE PARENT/GUARDIAN PATIENT Gerald A. Stagg, MD, FAAP Joel D. Chapman, MD, FAAP J. Colton Bradshaw, MD, FAAP Marc E. Kimball, MD, FAAP Michael D. Henry, MD, FAAP Christopher
EMERGENCY CONTACTS SIBLINGS INSURANCE PARENT/GUARDIAN PATIENT Gerald A. Stagg, MD, FAAP Joel D. Chapman, MD, FAAP J. Colton Bradshaw, MD, FAAP Marc E. Kimball, MD, FAAP Michael D. Henry, MD, FAAP Christopher
WELCOME TO FETZER FAMILY CHIROPRACTIC
 WELCOME TO FETZER FAMILY CHIROPRACTIC Patient Information Thank you for choosing Fetzer Family Chiropractic for your health care needs. Please complete this form in ink. If you have any questions or concerns,
WELCOME TO FETZER FAMILY CHIROPRACTIC Patient Information Thank you for choosing Fetzer Family Chiropractic for your health care needs. Please complete this form in ink. If you have any questions or concerns,
2800 Ross Clark Circle, Suite 2 Dothan, AL
 2800 Ross Clark Circle, Suite 2 Dothan, AL 36301 334-677-1690 Minor Patient Registration Form First Name M.I. Last Name Preferred Name: Street Address: Apt, Lot, Suite # City: State: Zip: DOB: Age: Sex:
2800 Ross Clark Circle, Suite 2 Dothan, AL 36301 334-677-1690 Minor Patient Registration Form First Name M.I. Last Name Preferred Name: Street Address: Apt, Lot, Suite # City: State: Zip: DOB: Age: Sex:
To Enroll in CareOregon Advantage, Please Provide the Following Information: ( ) Please Provide Your Medicare Insurance Information
 Please Provide Your Medicare Insurance Information") PLAN USE ONLY: Received Date Time Enter Date ES Submit Date ES To Enroll in CareOregon Advantage, Please Provide the Following Information: Please check which plan you want to enroll in: CareOregon Advantage
PLAN USE ONLY: Received Date Time Enter Date ES Submit Date ES To Enroll in CareOregon Advantage, Please Provide the Following Information: Please check which plan you want to enroll in: CareOregon Advantage
 California Department of Education, May 2016 School Year 2016-2017 Sunrise Middle School Application for Free and Reduced-Price Meals: State Meal Program Complete one application per household. Read the
California Department of Education, May 2016 School Year 2016-2017 Sunrise Middle School Application for Free and Reduced-Price Meals: State Meal Program Complete one application per household. Read the
Eye Associates of Georgetown, LLPC
 Eye Associates of Georgetown, LLPC Paige Quinlivan, O.D. & David Quinlivan, O.D. Mr. Mrs. Ms. Miss. Rev. Dr. Name : (Last) (First) (Mid. Intl.) Nickname: (if any) Address: City: State: Zip Code Cell Phone:
Eye Associates of Georgetown, LLPC Paige Quinlivan, O.D. & David Quinlivan, O.D. Mr. Mrs. Ms. Miss. Rev. Dr. Name : (Last) (First) (Mid. Intl.) Nickname: (if any) Address: City: State: Zip Code Cell Phone:
Medford Foot & Ankle Clinic, P.C.
 MICHAEL A. DEKORTE, DPM, FACFAS* RICK E. MCCLURE, DPM, FACFAS* JEFFERY D. ZIMMER, DPM Dear Patient, Thank you for choosing Medford Foot and Ankle Clinic for your podiatric care. Enclosed are the registration
MICHAEL A. DEKORTE, DPM, FACFAS* RICK E. MCCLURE, DPM, FACFAS* JEFFERY D. ZIMMER, DPM Dear Patient, Thank you for choosing Medford Foot and Ankle Clinic for your podiatric care. Enclosed are the registration
Social Security No: Home Phone: _. Employer: Work Phone: _. Employer Address: Occupation: _. Spouse/Parent Name: Phone No: _
 THE NATIONAL RETINA INSTITUTE LEADERS IN THE TREATMENT OF RETINAL DISEASES Patient Information Form Patient Name: Date of Birth: -,--I _----'--/ Age: Social Security No: Home Phone: _ Street Address: --------------------------------------
THE NATIONAL RETINA INSTITUTE LEADERS IN THE TREATMENT OF RETINAL DISEASES Patient Information Form Patient Name: Date of Birth: -,--I _----'--/ Age: Social Security No: Home Phone: _ Street Address: --------------------------------------
National Civic Engagement Survey Spring 2015 Descriptive Statistics
 National Civic Engagement Survey Spring 2015 Descriptive Statistics In spring 2015, nine community colleges from across the state were provided a small stipend to participate in the Civic Engagement Survey
National Civic Engagement Survey Spring 2015 Descriptive Statistics In spring 2015, nine community colleges from across the state were provided a small stipend to participate in the Civic Engagement Survey
Patient Demographic Information
 Patient Demographic Information Write your name as it appears on your insurance card. Please complete this form in its entirety Name: Male Female Date of Birth: Primary Insurance: Secondary Insurance:
Patient Demographic Information Write your name as it appears on your insurance card. Please complete this form in its entirety Name: Male Female Date of Birth: Primary Insurance: Secondary Insurance:
Research Brief. Who Are the Uninsured Eligible for Premium Subsidies in the Health Insurance Exchanges?
 Research Brief Findings From HSC NO. 18, DECEMBER 2010 Who Are the Eligible for Premium Subsidies in the Health Insurance Exchanges? BY PETER J. CUNNINGHAM A key provision of the national health reform
Research Brief Findings From HSC NO. 18, DECEMBER 2010 Who Are the Eligible for Premium Subsidies in the Health Insurance Exchanges? BY PETER J. CUNNINGHAM A key provision of the national health reform
Endocrinology of the Rockies, PC. PATIENT REGISTRATION FORM E. 9th Ave. Ste. 245, Denver, CO 80220
 1 PATIENT REGISTRATION FORM 2018 4545 E. 9th Ave. Ste. 245, Denver, CO 80220 Patient Name (Last, First, M.I.): Prefer to be called: Address: City: State: Zip: Home phone: ( ) Work phone: ( ) Day phone:
1 PATIENT REGISTRATION FORM 2018 4545 E. 9th Ave. Ste. 245, Denver, CO 80220 Patient Name (Last, First, M.I.): Prefer to be called: Address: City: State: Zip: Home phone: ( ) Work phone: ( ) Day phone:
THE COMMONWEALTH FUND SURVEY OF HEALTH CARE IN NEW YORK CITY
 THE COMMONWEALTH FUND SURVEY OF HEALTH CARE IN NEW YORK CITY David Sandman, Cathy Schoen, Catherine Des Roches, and Meron Makonnen MARCH 1998 THE COMMONWEALTH FUND The Commonwealth Fund is a philanthropic
THE COMMONWEALTH FUND SURVEY OF HEALTH CARE IN NEW YORK CITY David Sandman, Cathy Schoen, Catherine Des Roches, and Meron Makonnen MARCH 1998 THE COMMONWEALTH FUND The Commonwealth Fund is a philanthropic
FREE/REDUCED LUNCH PACKET
 FREE/REDUCED LUNCH PACKET CHILD S NAME ( PLEASE PRINT ) PLEASE FILL OUT ONE APPLICATION PER FAMILY. You DO NOT have to fill out more than one application. If you have already completed an application,
FREE/REDUCED LUNCH PACKET CHILD S NAME ( PLEASE PRINT ) PLEASE FILL OUT ONE APPLICATION PER FAMILY. You DO NOT have to fill out more than one application. If you have already completed an application,
Introduction. My name is. I am calling from the University of Montana in Missoula on behalf of the State of Montana.
 Introduction My name is. I am calling from the University of Montana in Missoula on behalf of the State of Montana. We're calling households across the state to see how well people are accessing health
Introduction My name is. I am calling from the University of Montana in Missoula on behalf of the State of Montana. We're calling households across the state to see how well people are accessing health
Application for Health Coverage & Help Paying Costs
 04.24.13 Application for Health Coverage & Help Paying Costs Use this application to see what coverage choices you qualify for Affordable private health insurance plans that offer comprehensive coverage
04.24.13 Application for Health Coverage & Help Paying Costs Use this application to see what coverage choices you qualify for Affordable private health insurance plans that offer comprehensive coverage
Massachusetts Application for Health and Dental Coverage and Help Paying Costs
 Massachusetts Application for Health and Dental Coverage and Help Paying Costs Commonwealth of Massachusetts EOHHS THINGS TO KNOW HOW TO APPLY Use this application to see what coverage choices you may
Massachusetts Application for Health and Dental Coverage and Help Paying Costs Commonwealth of Massachusetts EOHHS THINGS TO KNOW HOW TO APPLY Use this application to see what coverage choices you may
EMPLOYEE S GROUP ENROLLMENT APPLICATION
 EMPLOYEE S GROUP ENROLLMENT APPLICATION Instructions: Please complete all applicable areas of this application. Please print using black ink. Wisconsin Physicians Service Insurance Corporation ( WPS )/Delta
EMPLOYEE S GROUP ENROLLMENT APPLICATION Instructions: Please complete all applicable areas of this application. Please print using black ink. Wisconsin Physicians Service Insurance Corporation ( WPS )/Delta
Mantonya Chiropractic Center LLC. New Patient Information Form (Please Print and complete all areas)
") DR NP X-ray # Mantonya Chiropractic Center LLC New Patient Information Form (Please Print and complete all areas) Name Today'sDate Legal First Middle Last Mailing Address City State Zip Birth Date Age
DR NP X-ray # Mantonya Chiropractic Center LLC New Patient Information Form (Please Print and complete all areas) Name Today'sDate Legal First Middle Last Mailing Address City State Zip Birth Date Age
Hamilton Local School District. Parent/Guardian:
 Hamilton Local School District J. Michael Meade, Director of Operations Hamilton Local School District Columbus, OH 43207 Phone: 614.491.8044 x 1236 Fax: 614.491.8323 Parent/Guardian: www.hamiltonrangers.org
Hamilton Local School District J. Michael Meade, Director of Operations Hamilton Local School District Columbus, OH 43207 Phone: 614.491.8044 x 1236 Fax: 614.491.8323 Parent/Guardian: www.hamiltonrangers.org
3. Should you be unable to keep your appointment, please call us at (209) to cancel or reschedule, as soon as possible.
 to cancel or reschedule, as soon as possible.") To Our Patients, Welcome to the family practice office which has served Ripon and surrounding communities since the early 1970 s. We look forward to providing you with quality medical care. The following
To Our Patients, Welcome to the family practice office which has served Ripon and surrounding communities since the early 1970 s. We look forward to providing you with quality medical care. The following