Provider Manual. Billing and Payment
|
|
|
- Raymond Gary McBride
- 5 years ago
- Views:
Transcription
1 Provider Manual Billing and Payment

2 Billing and Payment This section of the Manual was created to help guide you and your staff in working with Kaiser Permanente s billing and payment policies and procedures. It provides a quick and easy resource with contact phone numbers, detailed processes and site lists for services. If, at any time, you have a question or concern about the information in this Manual, you can reach our National Provider Contracting Department by calling (510)
3 Table of Contents INTRODUCTION... 6 SECTION 5: BILLING AND PAYMENT WHOM TO CONTACT WITH QUESTIONS METHODS OF CLAIMS FILING PAPER CLAIM FORMS RECORD AUTHORIZATION ONE MEMBER/ PROVIDER PER CLAIM FORM SUBMISSION OF MULTIPLE PAGE CLAIM ENTERING DATES MULTIPLE DATES OF SERVICES AND PLACE OF SERVICES BILLING INPATIENT CLAIMS THAT SPAN DIFFERENT YEARS SUPPORTING DOCUMENTATION FOR PAPER CLAIMS WHERE TO MAIL/FAX PAPER CLAIMS... ERROR! BOOKMARK NOT DEFINED ELECTRONIC DATA INTERCHANGE (EDI) ELECTRONIC CLAIMS FORMS SUPPORTING DOCUMENTATION FOR EDI CLAIMS TO INITIATE ELECTRONIC CLAIMS SUBMISSIONS ELECTRONIC SUBMISSION PROCESS HIPAA REQUIREMENTS CLEAN CLAIMS CLAIMS SUBMISSION TIMEFRAMES
4 5.21 PROOF OF TIMELY CLAIMS SUBMISSION FEDERAL TAX ID CHANGES IN FEDERAL TAX ID NATIONAL PROVIDER IDENTIFICATION (NPI) CODING FOR CLAIMS CODING STANDARDS MODIFIERS IN CPT AND HCPCS MODIFIER REVIEW CODING & BILLING VALIDATION CODING EDIT RULES MEDICAL CLAIMS REVIEW PROVIDER CLAIMS APPEALS CMS-1500 (12/90) FIELD DESCRIPTIONS CMS-1500 (12/90) Form CMS-1500 (08/05) FIELD DESCRIPTIONS CMS-1500 (08/05) Form CMS-1450 (UB-92) FIELD DESCRIPTIONS CMS-1450 (UB-92) Form CMS-1450 (UB-04) FIELD DESCRIPTIONS CMS-1450 (UB-04) Form BILLING REQUIREMENTS AND INSTRUCTION FOR SPECIFIC SERVICES Emergency Claims Member Cost Share Balance Billing Members COORDINATION OF BENEFITS (COB)
5 How to Determine the Primary Payor Description of COB Payment Methodologies COB Claims Submission Requirements and Procedures Members Enrolled in Two Kaiser Permanente Plans COB Claims Submission Timeframes COB FIELDS ON THE UB-92 and UB-04 CLAIM FORM COB FIELDS ON THE CMS-1500 (HCFA-1500) CLAIM FORM EXPLANATION OF PAYMENT (EOP)
6 Introduction At the heart of Kaiser Permanente s claim processing operation is the set of policies and procedures followed in determining the appropriate handling and reimbursement of claims received. It is the contracted Provider s responsibility to ensure prompt payment through proper and timely submission of itemized bills using a CMS-1500 claim form for all professional services and UB-04 (CMS-1450) for all facility services in accordance with the terms of the Agreement with Kaiser Permanente. Bills for authorized services must include the authorization number and should be submitted to the address listed on the Authorization Form. PLEASE DO NOT BILL OUR MEMBERS other than for copay and deductibles. Billed items that are incorrectly coded will be denied and the Provider will be required to re-bill with the correct codes. Incorrect coding is coding that does not comply with industry standard coding practices as adopted by Kaiser Permanente, or the use of codes which have been updated in the CPT Manual since the contract was signed. Final payment will be based on these reviews. Any bill submitted more than one hundred eighty (180) days after the date the Covered Services were provided, or the date of receipt of an EOB (from a payer other than Kaiser Permanente), shall not be paid, except as otherwise required by law, or stated in your Agreement. Provider shall submit claims and/or encounter data for services rendered. When submitting encounter data, the Provider certifies the information as complete and truthful to the best of its knowledge. A complete CMS-1500 for all professional services or CMS-1450 for all facility services is the best method for complying with the encounter data required. It is Kaiser Permanente s goal to assure that the Provider is compensated in a timely and accurate manner in accordance with the terms of the Agreement and applicable law. Kaiser Permanente will pay for authorized covered services rendered to Members within the time period identified in the Agreement with Kaiser Permanente Whom to Contact with Questions The following information is provided as a quick reference to the Kaiser Permanente system. Member Service Department To verify benefits or eligibility of a Kaiser Permanente Member, contact the Member Services department in the Member s health plan region. Providers can also find benefit information on the Members Kaiser Permanente ID card. 6
7 WHO TO CALL WITH QUESTIONS If you have questions relating to the submission of transplant claims to Kaiser Permanente for processing, please refer to the table below for the correct department/number to call: PLEASE CALL: IF YOU HAVE QUESTIONS ABOUT TELEPHONE (S): MEMBER SERVICES Benefits/Co-Pay Information Colorado Member Eligibility Denver: Claim Payment Inquiries or (303) Claim Status Colorado Springs: Claim Submission or (719) Explanation of Payment (EOP) Georgia Provider Appeals or (404) Hawaii or (808) Ohio or (216) Northwest or (503) Northern California Mid-Atlantic States or (301) Southern California
8 Topic 5.2 Methods of Claims Filing 5.3 Paper Claim Forms Instructions Kaiser Permanente accepts all transplant claims submitted by mail or electronically. CMS-1450 must be used by all facilities (e.g., hospitals). All applicable fields on the CMS-1450 must be completed by the hospitals billing office for services rendered. To avoid payment delays and for correct reporting of encounter data, the CMS-1450 fields listed on the following table must be completed. Additionally, standard codes must be used on bills: REVENUE CODE: Code used to identify specific accommodation, ancillary service or billing calculation CPT-4: Physicians Current Procedural Terminology HCPCS: Health Care Procedure Coding System ICD-9-CM: Index for diagnoses and procedure coding DSM-IV-R: Diagnostic coding for mental disorders If appropriate, attach surgical reports, consultation reports, or progress notes to the claim form. CMS-1500 must be used for all professional services and suppliers. Any professional services (for example, services rendered by radiologists, ER physicians, etc.) should be billed on CMS claim forms, unless you are contracted under a GLOBAL rate, in which case professional services should not be billed separately. Note: Effective October 2006, the center of Medicare & Medicaid Service (CMS) has revised the CMS form. The new CMS (08/05) version will accommodate the reporting of the National Provider Identifier (NPI). Kaiser Permanente began to accept the revised form on October 1, Kaiser Permanente will continue to accept CMS-1500 (12/90) based on CMS guidelines for accepting this form. The National Uniform Billing Committee (NUBC) has approved the new UB-04 (CMS-1450) as the replacement for UB-92. Kaiser began accepting the New UB-04 on October 1,
9 5.4 Record Authorization Number 5.5 One Member/ Provider per Claim Form 5.6 Submission of Multiple Page Claim 5.7 Entering Dates All services that require prior authorization must have an authorization number reflected on the claim form or a copy of the authorization form may be submitted with the claim. Authorized services must be rendered before the expiration date stated on the Transplant Authorization Form. Each authorization identifies a specific number of approved visits, as well as, specific services. Additional authorization must be obtained by contacting the Transplant Coordinator for care beyond the expiration date. Transplant authorizations are issued for three stages of a transplant case: 1. Pre-transplant Evaluation and Care: This stage usually begins when a patient is listed for transplantation. 2. Transplant Period: This stage begins the day of the transplant and concludes at the end of the follow up period as defined in the Agreement. This authorization will cover both inpatient and outpatient services. 3. Post Transplant: This stage covers outpatient follow-up services following the transplant period. One Member per Claim Form/One Provider per claim Do not bill for different Members on the same claim form Do not bill for different Providers on the same claim form. Separate claim forms must be completed for each Member and for each Provider If due to space constraints you must use a second claim form, please write continuation at the top of the second form, and attach the second claim form to the first claim with a paper clip. Enter the TOTAL CHARGE (Field 28) on the last page of your claim submission. An example of how to enter dates on the CMS-1500 (HCFA-1500) Claim Form is provided below. 9

10 5.8 Multiple Dates of Services and Place of Services 5.9 Billing Inpatient Claims That Span Different Years 5.10 Supporting Documentation for Paper Claims Multiple dates of services at the same location can be filed on the same claim form but must be entered on a separate line. Multiple dates of service at different locations must be filed on a separate claim form. Same date of the service at the same location can be filed on a separate claim form. Same date of service at different locations must be filed on a separate claim form. When an inpatient claim spans different years (for example, the patient was admitted in December and was discharged in January of the following year), it is NOT necessary to submit two claims for these services. Bill all services for this inpatient stay on one claim form (if possible), reflecting the correct date of admission and the correct date of discharge. Kaiser Permanente will apply the appropriate/applicable payment methodologies when processing these claims. Providers may be required to include supporting documentation with any invoice submitted to Kaiser Permanente for payment. If documentation is required, Providers will be notified in writing. When billing with an unlisted CPT code, to expedite claims processing and adjudication, Providers should submit supporting written documentation. 10
11 11
12 5.11 Where to Mail/Fax Paper Claims There are eight (8) Kaiser Permanente claims regions. Each region is responsible for processing their Members claims, regardless of where services have been rendered a denial or delay in processing a claim may occur, if a Provider bills to the wrong region. All claims should be mailed to the following addresses, as identified on the Transplant Authorization Form: Paper claims are not accepted via fax due to HIPAA regulations. No handwritten claims are accepted. Colorado Region Kaiser Foundation Health Plan Transplant Claims PO Box Denver, CO Georgia Region Kaiser Foundation Health Plan Transplant Claims PO Box Atlanta, GA Hawaii Region Kaiser Foundation Health Plan Claims and Referrals Dept. 80 Mahalani Street Wailuku, HI Mid-Atlantic States Kaiser Foundation Health Plan PO Box 6233A Rockville, MD A ATTN: Clinical Review Unit Northern California Kaiser Foundation Health Plan Transplant Medical Review Dept Franklin Street, 16 th Floor Oakland, CA Southern California Kaiser Foundation Health Plan California Claims Administration PO Box 7004 Downey, CA Ohio Region Kaiser Foundation Health Plan Claims and Referrals Dept. PO Box 5316 Cleveland, OH
13 5.12 Electronic Data Interchange (EDI) 5.13 Electronic Claims Forms 5.14 Supporting Documentation for EDI Claims 5.15 To Initiate Electronic Claims Submissions Electronic Claim Submissions: Kaiser Permanente encourages electronic submission of claims. EDI is an electronic exchange of information in a standardized format that adheres to all Health Insurance Portability and Accountability Act (HIPAA) requirements. EDI transactions replace the submission of paper claims. data elements (for example, claims data elements) are entered into the computer only ONCE - typically at the Provider s office, or at another location where services were rendered. Benefits of EDI Submission 1 Reduced Overhead Expenses: Administrative overhead expenses are reduced, because the need for handling paper claims is eliminated. 2 Improved Data Accuracy: Because the claims data submitted by the Provider is sent electronically to Kaiser Permanente via the Clearinghouse, data accuracy is improved, as there is no need for re-keying or re-entry of data. 3 Low Error Rate: Additionally, up-front edits applied to the claims data while information is being entered at the Provider s office, and additional payer-specific edits applied to the data by the Clearinghouse before the data is transmitted to the appropriate payer for processing, increase the percentage of clean claim submissions. 4 Bypass US Mail Delivery: The usage of envelopes and stamps is eliminated. Providers save time by bypassing the U.S. mail delivery system. 5 Standardized Transaction Formats: Industry-accepted standardized medical claim formats may reduce the number of exceptions currently required by multiple payers. Professional and facility claims can be submitted electronically via the current version of: 837P must be used for all professional services and suppliers. 837I must be used by all facilities (e.g., hospitals) Currently, not all Kaiser Permanente regions have the capability to accept claims with electronic attachments. These types of submissions will need to be submitted via the paper process. Providers interested in implementing EDI transactions with Kaiser Permanente should contact National EDI Business Operations for information via NEBO@kp.org. 13
14 5.16 Electronic Submission Process 1. Providers EDI Responsibilities: Once a Provider has entered all of the required data elements (e.g., all of the required data for a particular claim) into its claims processing system, the Provider then electronically sends all of this information to a Clearinghouse for further data sorting and distribution. 2. Clearinghouse s EDI Responsibilities: The Clearinghouse receives information electronically from a variety of Providers, which have chosen that particular Clearinghouse as their data sorter and distributor. The Clearinghouse batches all of the information it has received from the various Providers, sorts the information, and then electronically sends the information to the correct payer for processing. Data content required by HIPAA Transaction Implementation Guides is the responsibility of the Provider and the Clearinghouse. The Clearinghouse should ensure HIPAA Transaction Set Format compliance with HIPAA rules. In addition, Clearinghouses: Frequently supply the required PC software to enable direct data entry in the Provider s office. Edit the data which is electronically submitted to the Clearinghouse by the Provider s office, so that the data submission will be accepted by the appropriate payer for processing. Transmit the data to the correct payer in a format easily understood by the payer s computer system. Transmit electronic claim status reports from payers to Providers. 3. Kaiser Permanente s EDI Responsibilities: Kaiser Permanente receives EDI information after the Provider sends it to the Clearinghouse for distribution. The data is loaded into Kaiser Permanente s claims systems electronically and it is prepared for further processing. On the same day that Kaiser Permanente receives the EDI claims, Kaiser Permanente prepares an electronic acknowledgement which is transmitted back to the Clearinghouse. NOTE: If a Provider is not receiving Kaiser Permanente s electronic claim acknowledgement from the Clearinghouse, contact your billing service or the Clearinghouse and request that this be routinely forwarded to you. Additionally, Kaiser Permanente provides a KP EDITS Reject 14
15 Detail Report for those claims which were rejected by Kaiser Permanente because of fatal front-end errors. Any rejected claims may be re-submitted electronically once the claims have been corrected by the Provider. NOTE: See the Claims Status Category and Reason Codes at for a list of common Fatal Errors HIPAA Requirements 5.18 Clean Claims All electronic claim submissions must adhere to all HIPAA requirements. The following websites (listed in alphabetical order) include additional information on HIPAA and electronic loops and segments. If a Provider does not have internet access, HIPAA Implementation Guides can be ordered by calling Washington Publishing Company (WPC) at (301) Providers are responsible to submit clean claims as defined in the Agreement and further explained below. Kaiser Permanente considers a claim clean when the following requirements are met. Correct Form - Kaiser Permanente requires all professional claims to be submitted using the CMS Form 1500 and all facility claims (or appropriate ancillary services) to be submitted using the CMS Form CMS 1450 Standard Coding All fields should be completed using industry standard coding. Attachments Attachments should be included in your submission when circumstances require additional information. Completed Field Elements for CMS Form 1500 (08/05 or 12/90 based on CMS guidelines) or CMS 1450 (UB-04 or UB92 based on CMS guidelines) All applicable data elements of CMS forms should be completed. A claim is not considered to be Clean or payable if one or more of the following are missing or are in dispute: The standards or format used in the completion or submission of the claim The eligibility of a person for coverage The responsibility of another payor for all or part of the claim The amount of the claim or the amount currently due under the 15
16 claim The benefits covered The manner in which services were accessed or provided The claim was submitted fraudulently 5.19 Claims Submission Timeframes 5.20 Appeal of Timely Claims Submission Note: Failure to include all information will result in a delay in claim processing and payment and it will be returned for any missing information. A claim missing any of the required information will not be considered a clean claim. Timeframes for filing a claim: New Claims All invoices for services provided to Kaiser Permanente Members should be submitted within forty-five (45) days of the Member s date of discharge or as stated in the Agreement. Bills for all hospital and professional services that are included under the case rate should be batched and submitted with a summary sheet. Where there is a separate case rate for hospital and physician services, batch each service type together, with a separate summary sheet. COB Claims COB information must be received within 12 months of the request for commercial Members and 24 months for Medicare/Medicaid Members (If within the last three months of the year, Medicare/Medicaid Members have 27 months). Processing of your claim may be delayed for receipt of COB information. Claim corrections Must be received with 12 months of the original claim payment for commercial Members and 24 months for Medicare/Medicaid Members (If within the last three months of the year, Medicare/Medicaid Members have 27 months). Resubmitted claims along with proof of initial timely filing received within six (6) months of the original date of denial or explanation of payment will be allowed for reconsideration of claim processing and payment. Any claim resubmissions received for timely filing reconsideration beyond six (6) months of the original date of denial or explanation of payment will be denied as untimely filing. 16
17 5.21 Proof of Timely Claims Submission 5.22 Claim Adjustments/ Corrections Claims submitted for consideration or reconsideration of timely filing must be reviewed with information that indicates the claim was initially submitted within the appropriate time frames outlined in Section Acceptable proof of timely filing may include the following documentation and/or situations: EDI Transmission reports (reports from a clearinghouse i.e., Emdeon) Remit notices Denial notices Hand-written or typed documentation is not acceptable proof of timely filing. Claim Adjustment Kaiser Permanente reserves the right to audit claims for adjustments and corrections to ensure services rendered are medically necessary, coding requirements are met as stated in this Manual, and payment is according to your Agreement. Necessary adjustments may be made by offsetting against future claims to any and all claims prior to or after payment. Periodically, Kaiser Permanente will perform audits on claims to determine if payments have been made appropriately. If our audit determines that an overpayment was made, you will be notified in writing of the amount of the overpayment and given instructions on the process and time frame for reimbursing Kaiser Permanente for the amount overpaid. If you do not send a check for the amount of the overpayment within the timeframe specified in your notice, future claims will be offset. Remit notices for claims that have been offset will reflect the amount deducted from the expected payment. Multiple claims may be affected until the entire balance of the overpayment is recovered. Correcting a previously submitted claim If your claim requires correction, you will receive a notice on the remit accompanying your rejected claim detailing the error. If corrections can be made, you should submit a corrected claim. The timeframe for submitting a corrected claim is either detailed in the notice you receive requesting corrections, or will default to the timely filing limit if not specified. Contracted Providers can submit a claim corrections if he/she has the following justifications: Original claim submitted with incorrect diagnosis 17
18 Original claim submitted with incorrect procedure(s) Original claim submitted with incorrect Member Original claim submitted with incorrect date of service Original claim submitted with incorrect contract rates applied Authorization has been obtained Any other information that has been added/corrected on the original claim. Procedures for submitting a paper claim correction to Kaiser Permanente for processing: Write CORRECTED CLAIM in the top (blank) portion of the standard claim form. Attach a copy of the corresponding page of Kaiser Permanente s Explanation of Payment (EOP) to each corrected claim, to prevent these claims from being rejected by Kaiser Permanente as duplicate claims. Attach with a paper clip. Mail the corrected claim(s) to Kaiser Permanente using the standard claims mailing address for the Member s health plan region. Kaiser Permanente prefers corrections to CMS-1500 (based on CMS guidelines) claims which were already accepted by Kaiser Permanente (regardless whether these claims were submitted on paper or electronically) to be submitted on paper claim forms. Corrections submitted electronically may inadvertently be denied as a duplicate claim. There are two ways to submit a CMS-1450 (UB-04 or UB92 based on CMS guidelines) claim correction to Kaiser Permanente for processing. Electronic: Please include the appropriate Type of Bill code when electronically submitting a corrected CMS-1450 (UB-04 or UB92 based on CMS guidelines) claim to Kaiser Permanente for processing. IMPORTANT: Claims submitted without the appropriate 3rd digit (xxx) in the Type of Bill code will be denied. Paper: Write CORRECTED CLAIM in the top (blank) portion of the standard claim form. Attach a copy of the corresponding page of Kaiser Permanente s Explanation of Benefit (EOB) to each corrected claim, to prevent these claims from being rejected by Kaiser Permanente as duplicate claims. Mail the corrected claim(s) to Kaiser Permanente using the standard claims mailing address for the Member s health plan region. 18
19 5.24 Rejected Claims Due to EDI Claims Error A detailed explanation of what should be adjusted and the reason(s) why it should be adjusted must be accompanied by supporting documentation to support the adjustment. Allow thirty (30) days from the receipt of your request to research and resolve your adjustment/correction request. 1. Electronic Claim Acknowledgement: Kaiser Permanente sends an electronic claim acknowledgement to the Clearinghouse. This claims acknowledgement will be forwarded to you as confirmation of all claims received by Kaiser Permanente. NOTE: If you are not receiving Kaiser Permanente s electronic claim receipt from the Clearinghouse the Clearinghouse and request that this be routinely forwarded to you. 2. Detailed Error Report: After receipt of your EDI claims from the Clearinghouse, Kaiser Permanente produces the EDI CLAIMS. KP EDIT Software then produces the Reject Report, which identifies specific Fatal Errors on non-accepted claims. Once the claims listed on the Reject Report are corrected, you may resubmit these claims electronically through the Clearinghouse. 19
20 5.25 Federal Tax ID Number The Federal Tax ID Number as reported on any and all claim form(s) must match the information filed with the Internal Revenue Service (IRS). 1 When completing IRS Form W-9, please note the following: Name: This should be the equivalent of your entity name, which you use to file your tax forms with the IRS. Sole Provider/Proprietor: List your name, as registered with the IRS. Group Practice/Facility: List your group or facility name, as registered with the IRS. 2. Business Name: Leave this field blank, unless you have registered with the IRS as a Doing Business As (DBA) entity. If you are doing business under a different name, enter that name on the IRS Form W Address/City, State, Zip Code: Enter the address where Kaiser Permanente should mail your IRS Form Taxpayer Identification Number (TIN): The number reported in this field (either the social security number or the employer identification number) MUST be used on all claims submitted to Kaiser Permanente. Sole Provider/Proprietor: Enter your taxpayer identification number, which will usually be your social security number (SSN), unless you have been assigned a unique employer identification number (because you are doing business as an entity under a different name). Group Practice/Facility: Enter your taxpayer identification number, which will usually be your unique employer identification number (EIN). If you have any questions regarding the proper completion of IRS Form W-9, or the correct reporting of your Federal Taxpayer ID Number on your claim forms, please contact the IRS help line in your area or refer to the following website: Completed IRS Form W-9 should be mailed to the following address: Kaiser Permanente Attn: National Provider Contracting and Network Management 300 Lakeside Drive, 13 th Floor Oakland, CA
21 IMPORTANT: If your Federal Tax ID Number should change, please notify us immediately, so that appropriate corrections can be made to Kaiser Permanente s files Changes in Federal Tax ID Number 5.27 National Provider Identification (NPI) 5.28 Coding for Claims 5.29 Coding Standards If your office/facility changes any pertinent information (i.e. tax identification number, phone or fax number, billing address, practice address, etc.) please mail or fax written notice, including the effective date of the change, as soon as possible, or if it at all possible, with 90 days advance notice. For changes in the Federal Tax-ID numbers, please include a W-9 form with the correct information. Kaiser Permanente Attn: National Provider Contracting and Network Management 300 Lakeside Drive, 13 th Floor Oakland, CA As of May 23, 2008, Kaiser Permanente will not be able to process electronic claims unless they contain NPI. If you have already obtained your NPI numbers (both Individual Type 1 and/or Organization/Group Type 2), please notify Kaiser Permanente Provider Contracting & Network Management department. Individual (Type 1) and Organization/Group (Type 2) NPI applications and instructions can be accessed at It is the Provider s responsibility to ensure that billing codes used on claims forms are current and accurate, that codes reflect the services provided and they are in compliant with Kaiser Permanente s coding standards. Incorrect and invalid coding may result in delays in payment or denial of payment. A full explanation of coding standards is provided in Section xxx of this manual. Incorrect and invalid coding may result in delays in payment or denial of payment. Coding All fields should be completed using industry standard coding as outlined below. ICD-9 To code diagnoses and hospital procedures on inpatient claims, use the International Classification of Diseases- 9th Revision-Clinical Modification (ICD-9-CM) developed by the Commission on Professional and Hospital Activities. ICD-9-CM Volumes 1 & 2 codes appear as three-, four- or fivedigit codes, depending on the specific disease or injury being described. Volume 3 hospital inpatient procedure codes appear as two-digit codes and require a third and/or fourth digit for coding specificity. 21
22 CPT-4 The Physicians' Current Procedural Terminology, Fourth Edition (CPT) code set is a systematic listing and coding of procedures and services performed by Participating Providers. CPT codes are developed by the American Medical Association (AMA). Each procedure code or service is identified with a five-digit code. If you would like to request a new code or suggest deleting or revising an existing code, obtain and complete a form from the AMA's Web site at or submit your request and supporting documentation to: CPT Editorial Research and Development American Medical Association 515 North State Street Chicago IL HCPCS The Healthcare Common Procedure Coding System (HCPCS) Level 2 identifies services and supplies. HCPCS Level 2 begin with letters A V and are used to bill services such as, home medical equipment, ambulance, orthotics and prosthetics, drug codes and injections. Revenue Code Approved by the Health Services Cost Review Commission for a hospital located in the State of Maryland, or of the national or state uniform billing data elements specifications for a hospital not located in that State. NDC (National Drug Codes) Prescribed drugs, maintained and distributed by the U.S. Department of Health and Human Services ASA (American Society of Anesthesiologists) Anesthesia services, the codes maintained and distributed by the American Society of Anesthesiologists 5.30 Modifiers in CPT and HCPCS DSM-IV (American Psychiatric Services) For psychiatric services, codes distributed by the American Psychiatric Association Modifiers submitted with an appropriate procedure code further define and/or explain a service provided. Valid modifiers and their descriptions can be found in the most current CPT or HCPCS coding book. Note CMS
23 Submitters: Kaiser Permanente processes up to (2) modifiers per claim line. When submitting claims, use modifiers to: Identify distinct or independent services performed on the same day Reflect services provided and documented in a patient's medical record Modifiers for Professional and Technical Services Modifier 26, Professional Component - Certain procedures consist of a physician component and a technical component. When the physician component is reported separately, adding the Modifier 26 to the CPT procedure code identifies the service. Modifier TC, Technical Component - The modifier TC is submitted with a CPT procedure code to bill for equipment and facility charges, to indicate the technical component. Use with diagnostic tests; e.g. radiation therapy, radiology, and pulmonary function tests. Indicates the Provider performed only the technical component portion of the service Modifier Review Modifiers Billed with Surgical Procedures Modifier 50 Bilateral Procedure Add Modifier 50 to the service line of a unilateral 5-digit CPT procedure code to indicate that a bilateral procedure was performed. Modifier 50 may be used to bill surgical procedures at the same operative session, or to bill diagnostic and therapeutic procedures that were performed bilaterally on the same day. Kaiser Permanente reserves the right to review use of modifiers to ensure accuracy and appropriateness. Improper use of modifiers may cause claims to pend and/or the return of claims for correction Coding & Billing Validation 5.33 Coding Edit Rules We perform code editing to enforce both Kaiser Permanente and nationally accepted coding and payment rules (see Section 5.34 of this Manual), and to verify the codes you submit are consistent based on the services rendered. Your claims will be subjected to McKesson code editing software ( CodeReview ). Kaiser Permanente applies coding edit rules to all claims submitted. The following examples outline some to the major categories of our coding edit rules, some of which CodeReview applies automatically as part of coding and billing validation. 23

24 These rules are subject to change and may be edited from time to time. Should you have any questions regarding code editing, please contact Claims Customer Service. Major Categories of Claim Coding Errors/Inconsistencies: AMA and CMS Guidelines CodeReview will correct input codes without valid modifiers to more closely correspond to accept coding practices by eliminating, replacing or flagging potential errors while accepting coding practices judged to be conventional by the American Medical Association (AMA) and the 24
25 Centers for Medicare & Medicaid Services (CMS). The CPT and HCPCS manuals explicitly detail and outline many of the rules included in the CodeReview. HCPCS codes related to CPT codes CodeReview also evaluates the combination of HCPCS codes and CPT codes. These codes are cross walked to identify where a HCPCS code is related to one or many CPT codes, and are evaluated based on the existing CPT rules. Unnecessary or disallowed codes are then rejected. HCPCS codes not related to CPT codes CodeReview also detects situations where HCPCS codes are not related to CPT codes. Rules developed as appropriate that are the result of the review of non-cpt related HCPCS codes are part of the knowledge base supporting CodeReview and do not conflict with the National Correct Coding Policy Initiative (NCCPI). Obsolete/Deleted Codes If obsolete or deleted codes cannot be cross walked to current or updated codes, claims submitted may be denied. Obsolete or deleted codes are updated each calendar year and are not accepted past the end date specified by CMS. Medicare claims with outdated codes will be subjected to denial as per CMS guidelines. Multiple/Duplicate Component Billing When procedures are billable for professional and technical components (i.e., with Modifiers 26 and TC), Kaiser Permanente monitors that the total amount paid for the service does not exceed what would have been paid if the procedure had been billed without the modifier(s). Kaiser Permanente reserves the right to adjust claims that are paid in excess of the total Medical Claims Review 5.35 Provider Claims Appeals Denied Codes Certain codes are always denied. To obtain a full list of these codes, please contact the Claims Customer Service Department in the Member s health plan region. Kaiser Permanente reserves the right to revise the list from time to time. In general, these codes relate to personal comfort items, non covered services, benefit exceptions and codes not reimbursable when billed in conjunction with Emergency services. Medical claims review is performed by comparing billing records with medical records to determine payment accuracy and to ensure claims are paid only for services delivered. If your office/facility has questions or concerns about the way a claim was processed by Kaiser Permanente, please contact the Member Services Department in the Member s health plan region. Many questions and 25
26 issues regarding claim payments, coding and submission policies can be resolved quickly over the phone. If your issue cannot be resolved through this initial contact, you have the right to appeal. See Section xxx of this Manual for a full explanation of this process CMS-1500 (12/90) Field Descriptions The fields identified in the table below as must be completed when submitting a CMS-1500 (12/90) claim form to Kaiser Permanente for processing: Note: The required fields for submission shown below are required by Kaiser Permanente but not necessarily required by CMS or other payers. For Medicare Members, please refer to Medicare Billing Requirements for appropriate field requirements and instructions/examples. FIELD FIELD NAME 1 MEDICARE/MEDICAID/ CHAMPUS/GROUP HEALTH PLAN/FECA BLK LUNG/OTHER REQUIRED FIELDS FOR CLAIM SUBMISSIONS Not INSTRUCTIONS/EXAMPLES Check the type of health insurance coverage applicable to this claim by checking the appropriate box. 1a INSURED S I.D. Enter the subscriber s plan identification number. 2 PATIENT S NAME Enter the patient s name. When submitting newborn claims, enter the newborn s first and last name. 3 PATIENT'S BIRTH DATE AND SEX Enter the patient s date of birth and gender. The date of birth must include the month, day and FOUR DIGITS for the year (MM/DD/YYYY). Example: 01/05/ INSURED'S NAME Enter the name of the insured (Last Name, First Name, Middle Initial), unless the insured and the patient are the same then the word SAME may be entered. 5 PATIENT'S ADDRESS Enter the patient s mailing address and telephone number. On the first line, enter the STREET ADDRESS; the second line is for the CITY and STATE; the third line is for the ZIP CODE and PHONE. 6 PATIENT'S RELATIONSHIP TO INSURED if 7 INSURED'S ADDRESS if Check the appropriate box for the patient s relationship to the insured. Enter the insured s address (STREET ADDRESS, CITY, STATE, ZIP CODE) and telephone number. When the address is the same as the patient s the word SAME may be entered. 26
27 FIELD FIELD NAME REQUIRED FIELDS FOR CLAIM SUBMISSIONS INSTRUCTIONS/EXAMPLES 8 PATIENT STATUS if 9 OTHER INSURED'S NAME if Check the appropriate box for the patient s MARITAL STATUS, and check whether the patient is EMPLOYED or is a STUDENT. When additional insurance coverage exists, enter the last name, first name and middle initial of the insured. 9a OTHER INSURED S POLICY OR GROUP if Enter the policy and/or group number of the insured individual named in Field 9 (Other Insured s Name) above. NOTE: For each entry in Field 9A, there must be a corresponding entry in Field 9d. 9b OTHER INSURED S DATE OF BIRTH/SEX if Enter the other insured s date of birth and sex. The date of birth must include the month, day, and FOUR DIGITS for year (MM/DD/YYYY). Example: 01/05/2003 9c EMPLOYER S NAME OR SCHOOL NAME if Enter the name of the other insured s EMPLOYER or SCHOOL NAME (if a student). 9d 10a-c INSURANCE PLAN NAME OR PROGRAM NAME IS PATIENT CONDITION RELATED TO if Enter the name of the other insured s INSURANCE PLAN or program. Check Yes or No to indicate whether employment, auto liability, or other accident involvement applies to one or more of the services described in field 24. NOTE: If yes there must be a corresponding entry in Field 14 (Date of Current Illness/Injury). Place (State)- enter the State postal code. 10d RESERVED FOR LOCAL USE 11 INSURED S POLICY OR FECA 11a INSURED S DATE OF BIRTH Not Not Not Leave blank. If there is insurance primary to Medicare, enter the insured s policy or group number. Enter the insured s date of birth and sex, if different from Field 3. The date of birth must include the month, day, and FOUR digits for the year (MM/DD/YYYY). Example: 01/05/ b EMPLOYER S NAME OR SCHOOL NAME Not Enter the name of the employer or school (if a student), if applicable. 27
28 FIELD 11c 11d REQUIRED FIELDS FOR FIELD NAME CLAIM SUBMISSIONS INSURANCE PLAN OR Not PROGRAM NAME IS THERE ANOTHER HEALTH BENEFIT PLAN? INSTRUCTIONS/EXAMPLES Enter the insurance plan or program name. Check yes or no to indicate if there is another health benefit plan. For example, the patient may be covered under insurance held by a spouse, parent, or some other person. If yes then fields 9 and 9a-d must be completed. 12 PATIENT'S OR AUTHORIZED PERSON'S SIGNATURE 13 INSURED'S OR AUTHORIZED PERSON'S SIGNATURE 14 DATE OF CURRENT ILLNESS, INJURY, PREGNANCY 15 IF PATIENT HAS HAD SAME OR SIMILAR ILLNESS Not Not Not Not Have the patient or an authorized representative SIGN and DATE this block, unless the signature is on file. If the patient s representative signs, then the relationship to the patient must be indicated. Have the patient or an authorized representative SIGN this block, unless the signature is on file. Enter the date of the current illness or injury. If pregnancy, enter the date of the patient s last menstrual period. The date must include the month, day, and FOUR DIGITS for the year (MM/DD/YYYY). Example: 01/05/2006 Enter the previous date the patient had a similar illness, if applicable. The date must include the month, day, and FOUR DIGITS for the year (MM/DD/YYYY). Example: 01/05/ DATES PATIENT UNABLE Not TO WORK IN CURRENT OCCUPATION Enter the from and to dates that the patient is unable to work. The dates must include the month, day, and FOUR DIGITS for the year (MM/DD/YYYY). Example: 01/05/ NAME OF REFERRING PHYSICIAN OR OTHER SOURCE 17a ID OF REFERRING PHYSICIAN 18 HOSPITALIZATION DATES RELATED TO CURRENT SERVICES 19 RESERVED FOR LOCAL USE if Not Not if Enter the FIRST and LAST NAME of the referring or ordering physician. Enter the Identification Number of the physician whose name is listed in Field 17. Complete this block when a medical service is furnished as a result of, or subsequent to, a related hospitalization. If you are covering for another physician, enter the name of the physician (for whom you are covering) in this field. If a non-contracting Provider/Provider will be 28
29 FIELD FIELD NAME REQUIRED FIELDS FOR CLAIM SUBMISSIONS INSTRUCTIONS/EXAMPLES covering for you in your absence, please notify that individual of this requirement. 20 OUTSIDE LAB Not 21 DIAGNOSIS OR NATURE OF ILLNESS OR INJURY Enter the diagnosis/condition of the patient, indicated by an ICD-9-CM code number. Enter up to 4 diagnostic codes, in PRIORITY order (primary, secondary condition). 22 MEDICAID RESUBMISSION 23 PRIOR AUTHORIZATION Not if Enter the prior authorization number for those procedures requiring prior approval. 24a DATE(S) OF SERVICE Enter the month, day, and year (MM/DD/YY) for each procedure, service, or supply. Services must be entered chronologically (starting with the oldest date first). For each service date listed/billed, the following fields must also be entered: Units, Charges/Amount/Fee, Place of Service, Procedure Code, and corresponding Diagnosis Code. IMPORTANT: Do not submit a claim with a future date of service. Claims can only be submitted once the service has been rendered (for example: durable medical equipment). 24b PLACE OF SERVICE Enter the place of service code for each item used or service performed. 24c TYPE OF SERVICE Not Enter the type of service code, reflecting the type of service rendered. 24d PROCEDURES, SERVICES, OR SUPPLIES: CPT/HCPCS, MODIFIER Enter the CPT/HCPCS codes reflecting the procedures performed, services rendered, or supplies used. When applicable, enter also the appropriate CPT/HCPCS code modifier(s) in this field, next to the corresponding CPT/HCPCS procedure code(s). IMPORTANT: Enter the anesthesia time, reported as the beginning and end times of anesthesia in military time under the appropriate procedure code. 24e DIAGNOSIS CODE Enter EITHER the diagnosis reference number as shown in Field 21, OR the appropriate ICD-9-CM diagnosis code next to each procedure/service listed. 29
30 FIELD FIELD NAME REQUIRED FIELDS FOR CLAIM SUBMISSIONS INSTRUCTIONS/EXAMPLES 24f $ CHARGES Enter the FULL CHARGE for each listed service. Any necessary payment reductions will be made during claims adjudication (for example, multiple surgery reductions, maximum allowable limitations, co-pays etc). 24g DAYS OR UNITS Enter the number of days or units in this block. (For example: units of supplies, etc.) 24h EPSDT FAMILY PLAN Not 24i EMG Not 24j COB Not 24k RESERVED FOR LOCAL USE 25 FEDERAL TAX ID 26 PATIENT'S ACCOUNT NO. Not Enter the physician/supplier federal tax I.D. number. IMPORTANT: The Federal Tax ID Number in this field must match the information on file with the IRS. Enter the Member s account number assigned by the Provider s/provider s accounting system. IMPORTANT: This field aids in patient identification by the Provider/Provider. 27 ACCEPT ASSIGNMENT Not 28 TOTAL CHARGE Enter the total charges for the services rendered (total of all the charges listed in Field 24f). 29 AMOUNT PAID if Enter the amount paid (i.e., Member copayments or other insurance payments) to date in this field for the services billed. 30 BALANCE DUE Not Enter the balance due (total charges less amount paid). 31 SIGNATURE OF PHYSICIAN OR SUPPLIER Enter the signature of the physician/supplier or his/her representative, and the date the form was signed. For claims submitted electronically, include a computer printed name as the signature of the Provider or person entitled to reimbursement. 32 NAME/ADDRESS OF FACILITY WHERE if The name and address of the facility where services were rendered (if other than patient s 30
31 FIELD FIELD NAME SERVICES WERE RENDERED REQUIRED FIELDS FOR CLAIM SUBMISSIONS INSTRUCTIONS/EXAMPLES home or physician s office). 33 PHYSICIAN'S, SUPPLIER'S BILLING NAME, ADDRESS, ZIP CODE, AND PHONE If available, please enter your Provider or unique vendor number in the PIN # field. 31
32 CMS-1500 (12/90) Form 32
33 5.37 CMS-1500 (08/05) Field Descriptions The fields identified in the table below as must be completed when submitting a CMS-1500 (08/05) claim form to Kaiser Permanente for processing: Note: The required fields for submission shown below are required by Kaiser Permanente but not necessarily required by CMS or other payers. For Medicare Members, please refer to Medicare Billing Requirements for appropriate field requirements and instructions/examples. Note: The new CMS-1500 (08/05) form is revised to accommodate National Provider Identifiers (NPI). Kaiser currently accepts both forms. FIELD FIELD NAME 1 MEDICARE/ MEDICAID/ TRICARE CHAMPUS/ CHAMPVA/ GROUP HEALTH PLAN/FECA BLK LUNG/OTHER REQUIRED FIELDS FOR CLAIM SUBMISSIONS Not INSTRUCTIONS/EXAMPLES Check the type of health insurance coverage applicable to this claim by checking the appropriate box. 1a INSURED S I.D. Enter the subscriber s plan identification number. 2 PATIENT S NAME Enter the patient s name. When submitting newborn claims, enter the newborn s first and last name. 3 PATIENT'S BIRTH DATE AND SEX Enter the patient s date of birth and gender. The date of birth must include the month, day and FOUR DIGITS for the year (MM/DD/YYYY). Example: 01/05/ INSURED'S NAME Enter the name of the insured (Last Name, First Name, and Middle Initial), unless the insured and the patient are the same then the word SAME may be entered. 5 PATIENT'S ADDRESS Enter the patient s mailing address and telephone number. On the first line, enter the STREET ADDRESS; the second line is for the CITY and STATE; the third line is for the ZIP CODE and PHONE. 6 PATIENT'S RELATIONSHIP TO INSURED if 7 INSURED'S ADDRESS if 8 PATIENT STATUS if Check the appropriate box for the patient s relationship to the insured. Enter the insured s address (STREET ADDRESS, CITY, STATE, and ZIP CODE) and telephone number. When the address is the same as the patient s the word SAME may be entered. Check the appropriate box for the patient s MARITAL STATUS, and check whether the patient is EMPLOYED or is a STUDENT. 33
34 FIELD FIELD NAME REQUIRED FIELDS FOR CLAIM SUBMISSIONS 9 OTHER INSURED'S NAME if INSTRUCTIONS/EXAMPLES When additional insurance coverage exists, enter the last name, first name and middle initial of the insured. 9a 9b OTHER INSURED S POLICY OR GROUP if OTHER INSURED S DATE OF BIRTH/SEX if Enter the policy and/or group number of the insured individual named in Field 9 (Other Insured s Name) above. NOTE: For each entry in Field 9A, there must be a corresponding entry in Field 9d. Enter the other insured s date of birth and sex. The date of birth must include the month, day, and FOUR DIGITS for year (MM/DD/YYYY). Example: 01/05/2006 9c EMPLOYER S NAME OR SCHOOL NAME if Enter the name of the other insured s EMPLOYER or SCHOOL NAME (if a student). 9d 10a-c INSURANCE PLAN NAME OR PROGRAM NAME IS PATIENT CONDITION RELATED TO if Enter the name of the other insured s INSURANCE PLAN or program. Check Yes or No to indicate whether employment, auto liability, or other accident involvement applies to one or more of the services described in field 24. NOTE: If yes there must be a corresponding entry in Field 14 (Date of Current Illness/Injury). Place (State) - enter the State postal code. 10d RESERVED FOR LOCAL USE 11 INSURED S POLICY OR FECA Not Not If Leave blank. there is insurance primary to Medicare, enter the insured s policy or group number. 11a INSURED S DATE OF BIRTH Not Enter the insured s date of birth and sex, if different from Field 3. The date of birth must include the month, day, and FOUR digits for the year (MM/DD/YYYY). Example: 01/05/ b EMPLOYER S NAME OR SCHOOL NAME Not Enter the name of the employer or school (if a student), if applicable. 11c 11d INSURANCE PLAN OR PROGRAM NAME IS THERE ANOTHER HEALTH BENEFIT PLAN? Not Enter the insurance plan or program name. Check yes or no to indicate if there is another health benefit plan. For example, the patient may be covered under insurance held by a spouse, parent, or some other person. If yes then fields 9 and 9a-d must be completed. 12 PATIENT'S OR AUTHORIZED Not Have the patient or an authorized representative 34
35 FIELD FIELD NAME PERSON'S SIGNATURE REQUIRED FIELDS FOR CLAIM SUBMISSIONS INSTRUCTIONS/EXAMPLES SIGN and DATE this block, unless the signature is on file. If the patient s representative signs, then the relationship to the patient must be indicated. 13 INSURED'S OR AUTHORIZED PERSON'S SIGNATURE 14 DATE OF CURRENT ILLNESS, INJURY, PREGNANCY 15 IF PATIENT HAS HAD SAME OR SIMILAR ILLNESS 16 DATES PATIENT UNABLE TO WORK IN CURRENT OCCUPATION Not if Not Not Have the patient or an authorized representative SIGN this block, unless the signature is on file. Enter the date of the current illness or injury. If pregnancy, enter the date of the patient s last menstrual period. The date must include the month, day, and FOUR DIGITS for the year (MM/DD/YYYY). Example: 01/05/2006 Enter the previous date the patient had a similar illness, if applicable. The date must include the month, day, and FOUR DIGITS for the year (MM/DD/YYYY). Example: 01/05/2006 Enter the from and to dates that the patient is unable to work. The dates must include the month, day, and FOUR DIGITS for the year (MM/DD/YYYY). Example: 01/05/ NAME OF REFERRING PHYSICIAN OR OTHER SOURCE if Enter the FIRST and LAST NAME of the referring or ordering physician. 17a OTHER ID # Not In the shaded area, enter the non-npi ID number of the physician whose name is listed in Field 17. Enter the qualifier identifying the number in the field to the right of 17a. The NUCC defines the following qualifiers: 0B - State License Number 1B - Blue Shield Provider Number 1C - Medicare Provider Number 1D - Medicaid Provider Number 1G - Provider UPIN Number 1H - CHAMPUS Identification Number EI - Employer s Identification Number G2 - Provider Commercial Number LU - Location Number N5 - Provider Plan Network Identification Number SY - Social Security Number X5 - State Industrial Accident Provider Number ZZ - Provider Taxonomy 17b NPI In the non-shaded area enter the NPI number of the referring Provider 35
36 FIELD FIELD NAME 18 HOSPITALIZATION DATES RELATED TO CURRENT SERVICES REQUIRED FIELDS FOR CLAIM SUBMISSIONS Not INSTRUCTIONS/EXAMPLES Complete this block when a medical service is furnished as a result of, or subsequent to, a related hospitalization. 19 RESERVED FOR LOCAL USE if If you are covering for another physician, enter the name of the physician (for whom you are covering) in this field. If a non-contracting Provider/Provider will be covering for you in your absence, please notify that individual of this requirement. 20 OUTSIDE LAB CHARGES Not 21 DIAGNOSIS OR NATURE OF ILLNESS OR INJURY Enter the diagnosis/condition of the patient, indicated by an ICD-9-CM code number. Enter up to 4 diagnostic codes, in PRIORITY order (primary, secondary condition). 22 MEDICAID RESUBMISSION Not 23 PRIOR AUTHORIZATION 24a-g SUPPLEMENTAL INFORMATION if Enter the prior authorization number for those procedures requiring prior approval. Supplemental information can only be entered with a corresponding, completed service line. SUPPLEMENTAL INFORMATION, con t. The top area of the six service lines is shaded and is the location for reporting supplemental information. It is not intended to allow the billing of 12 lines of service. When reporting additional anesthesia services information (e.g., begin and end times), narrative description of an unspecified code, NDC, VP HIBCC codes, OZ GTIN codes or contract rate, enter the applicable qualifier and number/code/information starting with the first space in the shaded line of this field. Do not enter a space, hyphen, or other separator between the qualifier and the number/code/information. The following qualifiers are to be used when reporting these services. 7 - Anesthesia information ZZ - Narrative description of unspecified code N4 - National Drug Codes (NDC) VP - Vendor Product Number Health Industry Business Communications Council (HIBCC) Labeling Standard OZ - Product Number Health Care Uniform Code Council Global Trade Item Number (GTIN) CTR - Contract rate 36
37 FIELD FIELD NAME REQUIRED FIELDS FOR CLAIM SUBMISSIONS INSTRUCTIONS/EXAMPLES 24a DATE(S) OF SERVICE Enter the month, day, and year (MM/DD/YY) for each procedure, service, or supply. Services must be entered chronologically (starting with the oldest date first). For each service date listed/billed, the following fields must also be entered: Units, Charges/Amount/Fee, Place of Service, Procedure Code, and corresponding Diagnosis Code. IMPORTANT: Do not submit a claim with a future date of service. Claims can only be submitted once the service has been rendered (for example: durable medical equipment). 24b PLACE OF SERVICE Enter the place of service code for each item used or service performed. 24c EMG Not Enter Y for "YES" or leave blank if "NO" to indicate an EMERGENCY as defined in the electronic 837 Professional 4010A1 implementation guide. 24d PROCEDURES, SERVICES, OR SUPPLIES: CPT/HCPCS, MODIFIER Enter the CPT/HCPCS codes and MODIFIERS (if applicable) reflecting the procedures performed, services rendered, or supplies used. IMPORTANT: Enter the anesthesia time, reported as the beginning and end times of anesthesia in military time above the appropriate procedure code. 24e DIAGNOSIS POINTER Enter the diagnosis code reference number (pointer) as it relates the date of service and the procedures shown in Field 21, When multiple services are performed, the primary reference number for each service should be listed first, and other applicable services should follow. The reference number(s) should be a 1, or a 2, or a 3, or a 4; or multiple numbers as explained. IMPORTANT: (ICD-9-CM diagnosis codes must be entered in Item Number 21 only. Do not enter them in 24E.) 24f $ CHARGES Enter the FULL CHARGE for each listed service. Any necessary payment reductions will be made during claims adjudication (for example, multiple surgery reductions, maximum allowable limitations, co-pays etc). Do not use commas when reporting dollar 37
38 FIELD FIELD NAME REQUIRED FIELDS FOR CLAIM SUBMISSIONS INSTRUCTIONS/EXAMPLES amounts. Negative dollar amounts are not allowed. Dollar signs should not be entered. Enter 00 in the cents area if the amount is a whole number. 24g DAYS OR UNITS Enter the number of days or units in this block. (For example: units of supplies, etc.) 24h EPSDT FAMILY PLAN Not When entering the NDC units in addition to the HCPCS units, enter the applicable NDC units qualifier and related units in the shaded line. The following qualifiers are to be used: F2 - International Unit ML - Milliliter GR - Gram UN Unit 24i ID. QUAL Enter in the shaded area of 24I the qualifier identifying if the number is a non-npi. The Other ID# of the rendering Provider is reported in 24J in the shaded area. The NUCC defines the following qualifiers: 0B - State License Number 1B - Blue Shield Provider Number 1C - Medicare Provider Number 1D - Medicaid Provider Number 1G - Provider UPIN Number 1H - CHAMPUS Identification Number EI - Employer s Identification Number G2 - Provider Commercial Number LU - Location Number N5 - Provider Plan Network Identification Number SY - Social Security Number (The social security number may not be used for Medicare.) X5 - State Industrial Accident Provider Number ZZ - Provider Taxonomy 24j RENDERING PROVIDER ID # Enter the non-npi ID number in the shaded area of the field. Enter the NPI number in the non-shaded area of the field. Report the Identification Number in Items 24I and 24J only when different from data recorded in items 33a and 33b. 25 FEDERAL TAX ID Enter the physician/supplier federal tax I.D. number or Social Security number. Enter an X in the appropriate box to indicate which number is being reported. Only one box can be marked. 38
39 FIELD FIELD NAME REQUIRED FIELDS FOR CLAIM SUBMISSIONS INSTRUCTIONS/EXAMPLES IMPORTANT: The Federal Tax ID Number in this field must match the information on file with the IRS. 26 PATIENT'S ACCOUNT NO. Enter the Members account number assigned by the Provider s/provider s accounting system. 27 ACCEPT ASSIGNMENT Not IMPORTANT: This field aids in patient identification by the Provider/Provider. 28 TOTAL CHARGE Enter the total charges for the services rendered (total of all the charges listed in Field 24f). 29 AMOUNT PAID if 30 BALANCE DUE Not 31 SIGNATURE OF PHYSICIAN OR SUPPLIER INCLUDING DEGREES OR CREDENTIALS Enter the amount paid (i.e., Member copayments or other insurance payments) to date in this field for the services billed. Enter the balance due (total charges less amount paid). Enter the signature of the physician/supplier or his/her representative, and the date the form was signed. For claims submitted electronically, include a computer printed name as the signature of the health care Provider or person entitled to reimbursement. 32 SERVICE FACILITY LOCATION INFORMATION if The name and address of the facility where services were rendered (if other than patient s home or physician s office). Enter the name and address information in the following format: 1st Line Name 2nd Line Address 3rd Line City, State and Zip Code Do not use commas, periods, or other punctuation in the address (e.g., 123 N Main Street 101 instead of 123 N. Main Street, #101 ). Enter a space between town name and state code; do not include a comma. When entering a 9 digit zip code, include the hyphen. 32a NPI # Enter the NPI number of the service facility. 32b OTHER ID # Enter the two digit qualifier identifying the non-npi number followed by the ID number. Do not enter a space, hyphen, or other separator between the 39
40 FIELD FIELD NAME REQUIRED FIELDS FOR CLAIM SUBMISSIONS qualifier and number. INSTRUCTIONS/EXAMPLES 33 BILLING PROVIDER INFO & PH # 33a Enter the name, address and phone number of the billing entity. NPI # Enter the NPI number of the service facility location in 32a. 33b OTHER ID # Enter the two digit qualifier identifying the non-npi number followed by the ID number. Do not enter a space, hyphen, or other separator between the qualifier and number. If available, please enter your Provider or unique vendor number. 40
 Form 41")
41 CMS-1500 (08/05) Form 41
42 5.38 CMS-1450 (UB-92) Field Descriptions The fields identified in the table below as must be completed when submitting a CMS-1450 (UB-92) claim form to Kaiser Permanente for processing: Note: The required fields for submission shown below are required by Kaiser Permanente but not necessarily required by CMS or other payers. For Medicare Members, please refer to Medicare Billing Requirements for appropriate field requirements and instructions/examples. FIELD FIELD NAME 1 PROVIDER NAME and ADDRESS REQUIRED FIELDS FOR CLAIM SUBMISSIONS 2 BLANK Not Leave blank. INSTRUCTIONS/EXAMPLES The hospital/facility or person entitled to reimbursement s name and address and telephone number. 3 PATIENT CONTROL The Member s control number. IMPORTANT: This field aids in patient identification by the Provider/Provider. 4 TYPE OF BILL Enter the appropriate code to identify the specific type of bill being submitted. This code is required for the correct identification of inpatient vs. outpatient claims, interim, corrected, voids, etc. 5 FEDERAL TAX The hospital/facility or person entitled to 6 STATEMENT COVERS PERIOD reimbursement s federal tax ID number. The beginning and ending date of claim period. 7 COVERED DAYS Not The number of covered days for inpatient claims. 8 NON COVERED DAYS Not The number of non covered days for inpatient claims. 9 COINSURANCE DAYS Not The number of coinsurance days. 10 LIFETIME RESERVE DAYS Not The number of lifetime reserve days. 11 BLANK Not Leave blank. 12 PATIENT NAME The Member s name. 13 PATIENT ADDRESS The Member s address. 14 PATIENT BIRTH DATE The Member s birth date. 15 PATIENT SEX The Member s gender. 16 PATIENT MARITAL Not STATUS The Member s marital status. 42
43 FIELD FIELD NAME REQUIRED FIELDS FOR CLAIM SUBMISSIONS INSTRUCTIONS/EXAMPLES 17 ADMISSION DATE The date of admission. For inpatient claims only. 18 ADMISSION HOUR Enter the 2-digit code for the hour during 19 which the Member was admitted/seen for inpatient OR outpatient care. TYPE OF ADMISSION The type of admission (e.g. emergency, urgent, elective, newborn). 20 SOURCE OF ADMISSION The source of admission code. 21 DISCHARGE HOUR Not The discharge hour. 22 PATIENT STATUS Enter the correct Member discharge status code. 23 MEDICAL RECORD Not This is the number assigned to the patient s medical/health record by the Provider CONDITION CODES if 31 BLANK Not Leave blank. Enter any applicable codes which identify conditions relating to the claim that may affect claims processing a-b OCCURRENCE CODES AND DATES 36 a-b OCCURRENCE SPAN CODES AND DATES 37 INTERNAL CONTROL if if Not Enter the code and the associated date defining a significant event relating to this bill that may affect claims processing. Occurrence span codes and dates required if occurrence span from and thru dates are entered. Enter occurrence span codes. The internal control number. 38 RESPONSIBLE PARTY Not The responsible party name and address VALUE CODES and AMOUNT if Enter the code and related amount/value which is necessary to process the claim. 42 REVENUE CODE Identify the specific accommodation, ancillary service, or billing calculation, by assigning an appropriate revenue code. 43 REVENUE DESCRIPTION Not The revenue description. 44 PROCEDURE CODE AND MODIFIER 45 For ALL outpatient claims, enter BOTH a revenue code in Field 42 (Rev. CD.), and the corresponding CPT/HCPCS procedure code in this field. SERVICE DATE Not Outpatient Series Bills: A service date must be entered for all outpatient series bills whenever the from and through dates in Field 6 (Statement Covers Period: From/Through) are not the same. Submissions that are received without the required service date(s) will be 43
44 FIELD FIELD NAME REQUIRED FIELDS FOR CLAIM SUBMISSIONS INSTRUCTIONS/EXAMPLES rejected with a request for itemization. Multiple/Different Dates of Service: Multiple/different dates of service can be listed on ONE claim form. List each date on a separate line on the form, along with the corresponding revenue code (Field 42), procedure code (Field 44), and total charges (Field 47). 46 UNITS OF SERVICE The units of service. 47 TOTAL CHARGES Indicate the total charges pertaining to the related revenue code for the current billing period, as listed in Field NON COVERED POLICIES Not Non-covered charges. 49 BLANK Not Leave blank. 50 PAYER Be sure to enter (in appropriate ORDER on lines A, B, and C) the NAME and of each payer organization from whom you are expecting payment towards the claim. 51 PROVIDER The Provider number. 52 RELEASE OF Not INFORMATION CERTIFICATION The release of information. 53 ASSIGNMENT OF BENEFITS CERTIFICATION INDICATOR if Assignment of benefits. 54a-c PRIOR PAYMENTS if 55 ESTIMATED AMOUNT DUE Not If payment has already been received toward the claim by one of the payers listed in Field 50 (Payer) prior to the billing date, be sure to indicate this here. The estimated amount due. 56 BLANK Not Leave blank. 57 BLANK Not Leave blank. 58 INSURED S NAME The subscriber s name. 59 PATIENT S RELATION TO INSURED if The Member s relationship to the subscriber. 60 CERT-SSN-HIC-ID NO Enter the insured person s unique individual Member identification number (medical/health record number), as 44
45 FIELD FIELD NAME REQUIRED FIELDS FOR CLAIM SUBMISSIONS INSTRUCTIONS/EXAMPLES assigned by the payer organization. 61 INSURED S GROUP NAME 62 INSURED S GROUP Not Not The insured s group name. Enter the insured s group number as shown on the identification card. For Prepaid Services Claims enter "PPS". 63 TREATMENT AUTHORIZATION CODE if The authorization [?] number is entered in this field for ALL inpatient and outpatient claims, to ensure efficient claims processing. 64 EMPLOYMENT STATUS CODE Not The employment status code. 65 EMPLOYER NAME Not The employer s name. 66 EMPLOYER LOCATION Not The employer s location. 67 PRINCIPAL DIAGNOSIS CODE Enter the ICD-9-CM principal diagnosis code, on all inpatient and outpatient claims OTHER DIAGNOSES if CODES Enter other diagnoses codes corresponding to additional conditions. Must be a valid ICD-9 or DSM III diagnosis code. Diagnosis codes must be carried to their highest degree of detail. 76 ADMITTING DIAGNOSIS Enter the admitting ICD-9-CM diagnosis code on all inpatient claims. 77 EXTERNAL CAUSE OF INJURY CODE (E-CODE) Not Enter an ICD-9-CM E-code in this field (if applicable). 78 DRG ASSIGNMENT if 79 PROCEDURE CODING METHOD USE 80 PRINCIPAL PROCEDURE CODE AND DATE Not if Inpatient Claims DRG #: Enter the DRG which the Member groups to, even if you are being reimbursed under a different payment methodology. The procedure coding method used. Enter the ICD-9-CM procedure CODE and DATE on all inpatient AND outpatient claims for the principal surgical and/or obstetrical procedure which was performed (if applicable). 81 a c OTHER PROCEDURE CODES AND DATES if Enter other ICD-9-CM procedure CODE(S) and DATE(S) on all inpatient AND outpatient claims (in fields A through E ) for any additional surgical and/or obstetrical procedures which were performed (if 45
46 FIELD FIELD NAME 82 ATTENDING PHYSICIAN AND NAME REQUIRED FIELDS FOR CLAIM SUBMISSIONS INSTRUCTIONS/EXAMPLES applicable). Enter the unique physician identification number (UPIN) and the name of the attending physician for inpatient bills or the physician that requested the outpatient services. Inpatient Claims Attending Physician Enter the full name (first and last name) of the physician who is responsible for the care of the patient. 83 a-b OTHER PHYSICIAN ID AND NAME Not Outpatient Claims Referring Physician For ALL outpatient claims, enter the full name (first and last name) of the physician who referred the Member for the outpatient services billed on the claim. Enter the unique physician identification number and the name of any other physicians. 84 REMARKS Not Special annotations may be entered in this 85 PROVIDER REPRESENTATIVE Not field. The signature of the Provider representative or notation that the signature is on file with the third party payer. 86 DATE Not The date the claim was submitted. 46
 Form 47")
47 CMS-1450 (UB-92) Form 47
48 5.39 CMS-1450 (UB-04) Field Descriptions The fields identified in the table below as must be completed when submitting a CMS-1450 (UB-04) claim form to Kaiser Permanente for processing: Please Note: The fields required for submission below are required by Kaiser Permanente but not necessarily by CMS or other payers. For Medicare Members, please refer to Medicare s billing requirements for appropriate field requirements and instructions or examples. FIELD FIELD NAME 1 PROVIDER NAME and ADDRESS 2 3a 3b PAY-TO NAME, ADDRESS, CITY/STATE, ID # PATIENT CONTROL MEDICAL RECORD REQUIRED FIELDS FOR CLAIM SUBMISSIONS Not INSTRUCTIONS/EXAMPLES Enter the name and address of the hospital or person who rendered the services being billed. Enter the name and address of the hospital or person to receive the reimbursement. Enter the Member s control number. IMPORTANT: This field aids in patient identification by the Provider/Provider. Enter the number assigned to the patient s medical/health record by the Provider. 4 TYPE OF BILL Enter the appropriate code to identify the specific type of bill being submitted. This code is required for the correct identification of inpatient vs. outpatient claims, voids, etc. 5 FEDERAL TAX Enter the federal tax ID of the hospital or person entitled to reimbursement. 6 7 STATEMENT COVERS PERIOD BLANK Not Leave blank. Enter the beginning and ending date of service included in the claim. 8 PATIENT NAME Enter the Member s name. 9 PATIENT ADDRESS Enter the Member s address PATIENT BIRTH DATE PATIENT SEX Enter the Member s birth date. Enter the Member s gender. 12 ADMISSION DATE For inpatient claims only, enter the date of admission. 48
49 FIELD FIELD NAME REQUIRED FIELDS FOR CLAIM SUBMISSIONS INSTRUCTIONS/EXAMPLES 13 ADMISSION HOUR For either inpatient OR outpatient care, enter the 2- digit code for the hour during which the Member was admitted or seen ADMISSION TYPE ADMISSION SOURCE DISCHARGE HOUR (DHR) PATIENT STATUS if CONDITION CODES if 29 ACCIDENT (ACDT) STATE BLANK OCCURRENCE CODES AND DATES OCCURRENCE SPAN CODES AND DATES BLANK RESPONSIBLE PARTY VALUE CODES and AMOUNT Not Not if if Not Not if Indicate the type of admission (e.g. emergency, urgent, elective, and newborn). Enter the source of the admission type code. Enter the two-digit code for the hour during which the Member was discharged. Enter the discharge status code. Enter any applicable codes which identify conditions relating to the claim that may affect claims processing. Enter the two-character code indicating the state in which the accident occurred which necessitated medical treatment. Leave blank. Enter the code and the associated date defining a significant event relating to this bill that may affect claims processing. Enter the occurrence span code and associated dates defining a significant event relating to this bill that may affect claims processing. Leave blank. Enter the responsible party name and address. Enter the code and related amount/value which is necessary to process the claim. 42 REVENUE CODE Identify the specific accommodation, ancillary service, or billing calculation, by assigning an appropriate revenue code. 43 REVENUE DESCRIPTION Not Enter the revenue description. 44 PROCEDURE CODE AND MODIFIER For ALL outpatient claims, enter BOTH a revenue code in Field 42 (Rev. CD.), and the corresponding CPT/HCPCS procedure code in this field. 49
50 FIELD FIELD NAME REQUIRED FIELDS FOR CLAIM SUBMISSIONS INSTRUCTIONS/EXAMPLES 45 SERVICE DATE Outpatient Series Bills: A service date must be entered for all outpatient series bills whenever the from and through dates in Field 6 (Statement Covers Period: From/Through) are not the same. Submissions that are received without the required service date(s) will be rejected with a request for itemization. Multiple/Different Dates of Service: Multiple/different dates of service can be listed on ONE claim form. List each date on a separate line on the form, along with the corresponding revenue code (Field 42), procedure code (Field 44), and total charges (Field 47). 46 UNITS OF SERVICE 47 TOTAL CHARGES 49 BLANK Not NON COVERED CHARGES PAYER NAME Not 51 HEALTH PLAN ID The units of service. Indicate the total charges pertaining to the related revenue code for the current billing period, as listed in Field 6. Leave blank. Enter any non-covered charges. Enter (in appropriate ORDER on lines A, B, and C) the NAME and of each payer organization from whom you are expecting payment towards the claim. Enter the Provider number. 52 RELEASE OF INFORMATION (RLS INFO) Not Enter the release of information certification number 53 ASSIGNMENT OF BENEFITS (ASG BEN) if Enter the assignment of benefits certification number. 54a-c PRIOR PAYMENTS 55 ESTIMATED AMOUNT DUE 56 NATIONAL PROVIDER IDENTIFIER (NPI) if Not If payment has already been received toward the claim by one of the payers listed in Field 50 (Payer) prior to the billing date, enter the amounts here. Enter the estimated amount due. Enter the service Provider s National Provider Identifier (NPI). 50
51 FIELD FIELD NAME 57 OTHER PROVIDER ID 58 INSURED S NAME 59 PATIENT S RELATION TO INSURED 60 INSURED S UNIQUE ID 61 INSURED S GROUP NAME INSURED S GROUP TREATMENT AUTHORIZATION CODE 64 DOCUMENT CONTROL 65 EMPLOYER NAME 66 DX VERSION QUALIFIER 67 PRINCIPAL DIAGNOSIS CODE REQUIRED FIELDS FOR CLAIM SUBMISSIONS if if if if Not if Not INSTRUCTIONS/EXAMPLES Enter the service Provider s Kaiser-assigned Provider ID. Enter the subscriber s name. Enter the Member s relationship to the subscriber. Enter the insured person s unique individual Member identification number (medical/health record number), as assigned by Kaiser. Enter the insured s group name. Enter the insured s group number as shown on the identification card. For Prepaid Services claims enter "PPS". For ALL inpatient and outpatient claims, enter the referral number. Enter the document control number related to the Member or the claim. Enter the employer s name. Indicate the type of diagnosis codes being reported. Note: At the time of printing, Kaiser only accepts ICD- 9-CM diagnosis codes on the UB-04. Enter the principal diagnosis code, on all inpatient and outpatient claims. 67 A-Q OTHER DIAGNOSES CODES (a-c) BLANK ADMITTING DIAGNOSIS REASON FOR VISIT (PATIENT REASON DX) if Not Not Enter other diagnoses codes corresponding to additional conditions. Diagnosis codes must be carried to their highest degree of detail. Leave blank. Enter the admitting diagnosis code on all inpatient claims. Enter the diagnosis codes indicating the patient s reason for outpatient visit at the time of registration. 51
52 FIELD FIELD NAME REQUIRED FIELDS FOR CLAIM SUBMISSIONS 71 PPS CODE if 72 EXTERNAL CAUSE OF INJURY CODE (ECI) (a e) BLANK PRINCIPAL PROCEDURE CODE AND DATE OTHER PROCEDURE CODES AND DATES if Not required if if 75 BLANK Not required INSTRUCTIONS/EXAMPLES Enter the DRG number which the procedures group, even if you are being reimbursed under a different payment methodology. Enter an ICD-9-CM E-code in this field (if applicable). Leave blank. Enter the ICD-9-CM procedure CODE and DATE on all inpatient AND outpatient claims for the principal surgical and/or obstetrical procedure which was performed (if applicable). Enter other ICD-9-CM procedure CODE(S) and DATE(S) on all inpatient AND outpatient claims (in fields A through E ) for any additional surgical and/or obstetrical procedures which were performed (if applicable). Leave blank. 76 ATTENDING PHYSICIAN / NPI / QUAL / ID Enter the National Provider Identifier (NPI) and the name of the attending physician for inpatient bills or the physician that requested the outpatient services. Inpatient Claims Attending Physician Enter the full name (first and last name) of the physician who is responsible for the care of the patient. Outpatient Claims Referring Physician For ALL outpatient claims, enter the full name (first and last name) of the physician who referred the Member for the outpatient services billed on the claim. 77 OPERATING PHYSICIAN / NPI/ QUAL/ ID OTHER PHYSICIAN/ NPI/ QUAL/ ID If if Enter the National Provider Identifier (NPI) and the name of the lead surgeon who performed the surgical procedure. Enter the National Provider Identifier (NPI) and name of any other physicians. REMARKS Not Special annotations may be entered in this field. 81 CODE-CODE Not required Enter the code qualifier and additional code, such as martial status, taxonomy, or ethnicity codes, as may be appropriate. 52
 Form 53")
53 CMS-1450 (UB-04) Form 53
54 5.40 Billing Requirements and Instruction for Specific Services Topic Emergency Claims Instructions An emergency claim is submitted when a center furnishes medically necessary emergency health services or supplies to a Kaiser Permanente Member without obtaining an authorization. The following circumstances must be present for Kaiser Permanente to consider payment of bills as part of an emergency claim: 1. The services and supplies would have been covered under the Members Health Plan, if they had been ordered, authorized, prescribed, or directed by a Plan Physician. 2. The services provided were immediately required because of an unforeseen illness or injury. Coverage depends on the advice of the treating physician, as well as the Kaiser Permanente determination of the situation in which care was provided and in consideration of the prudent layperson guidelines Member Cost Share Please Note: Kaiser Permanente makes a distinction between a Claim for Authorized Services or Referral and Emergency Claim, in terms of processing payment for contracted Providers. As a result, payment processing may be done by two different departments within Kaiser Permanente for referrals as opposed to claims. If a Member has received a transplant services referral, the Provider submits claims to the address listed on the authorization form. Depending on the benefit plan, Kaiser Permanente Members may be responsible to share some cost of the services provided. Copayment, coinsurance and deductible (collectively, Member Cost Share ) are the fees a Member is responsible to pay a Provider for certain covered services. This information varies by plan and all Providers are responsible for collecting Member Cost Share in accordance with Kaiser Permanente Member s benefits unless explicitly stated otherwise in your Agreement. Please verify applicable Member Cost Share at the time of service. Member Cost Share information can be obtained from: Kaiser Permanente Member Services Department in the Member s health plan region. Member ID Card. Copayments, co-insurance and deductible information are listed on the front of the Member ID card when applicable. 54
55 Balance Billing Members NOTICE TO ALL PROVIDERS: In no event including, but not limited to, nonpayment by or insolvency of a Payer or breach of this Agreement, shall Provider bill; charge; collect a deposit from; seek compensation, reimbursement, or remuneration from; impose surcharges; or have any recourse against any Member, person acting on the Member s behalf, state Medicaid plan, or any person other than the Payer for Covered Services provided under this Agreement. This Agreement does not prohibit Provider from collecting Member Cost Share amounts or fees for non-covered Services billed in accordance with the terms of the applicable Membership Agreement. The terms of this Section shall survive the termination or expiration of this Agreement regardless of the cause giving rise to termination, shall be construed to be for the benefit of Members, and shall supersede any oral or written agreement to the contrary now existing or hereafter entered into between Provider and the Member or persons acting on the Member's behalf. Without limiting the foregoing, Provider shall not seek payment from Members for: (1) amounts denied by Payer because billed charges were not customary or reasonable, (2) amounts denied because they were not medically necessary as determined under the Membership Agreement, or (3) Provider s failure to obtain Authorization for Services delivered; submit clinical data promptly; or submit a claim in accordance with the appropriate billing procedures, within the appropriate time frame, or in accordance with commonly accepted standard coding practices. 55
56 5.41 Coordination of Benefits (COB) Coordination of Benefits (COB) is a method for determining the order in which benefits are paid and the amounts which are payable when a Member is covered under more than one plan. It is intended to prevent duplication of benefits when an individual is covered by multiple plans providing benefits or services for medical or other care and treatment. Kaiser Permanente Providers are responsible for determining the primary payor and for billing the appropriate party. If Kaiser Permanente is not the primary carrier, an EOB is required with the claim CMS 1500 (HCFA 1500) submission. Topic How to Determine the Primary Payor Instructions The benefits of the plan that covers an individual as an employee, Member or subscriber other than as a dependent are determined before those of a plan that covers the individual as a dependent. When both parents cover a child, the birthday rule applies the payor for the parent whose birthday falls earlier in the calendar year (month and day) is the primary payor. When determining the primary payor for a child of separated or divorced parents, inquire about the court agreement or decree. In the absence of a divorce decree/court order stipulating parental healthcare responsibilities for a dependent child, insurance benefits for that child are applied according to the following order: Insurance carried by the: Natural parent with custody pays first Step-parent with custody pays next Natural parent without custody pays next Step-parent without custody pays last If the parents have joint custody of the dependent child, then benefits are applied according to the birthday rule referenced above. If this does not apply, call the Member Services Department in the Member s Health Plan Region. Kaiser Permanente is generally primary for working Medicareeligible Members when the CMS Working Aged regulation applies. 56
57 Topic Description of COB Payment Methodologies COB Claims Submission Requirements and Procedures Instructions Medicare is generally primary for retired Medicare Members over age 65, and for employee group health plan (EGHP) Members with End Stage Renal Disease (ESRD) for the first thirty (30) months of dialysis treatment. This does not apply to direct pay Members. Kaiser Permanente Coordination of Benefits allows benefits from multiple carriers to be added on top of each other so that the Member receives the full benefits from their primary carrier and the secondary carrier pays their entire benefit up to 100% of allowed charges. When Kaiser Permanente has been determined as the secondary payor, Kaiser Permanente pays the difference between the payment by the primary payor and the amount which would be have been paid if Kaiser Permanente was primary, less any amount for which the Member has financial responsibility. Benefit carve-out calculations are based on whether or not the Provider accepts Medicare assignment for the Provider contract corresponding to the claim. Medicare assignment means the Provider has agreed to accept the Medicare allowed amount as payment. Whenever Kaiser Permanente is the SECONDARY payer, claims can be submitted EITHER electronically or on one of the standard paper claim forms: Electronic Claims: If Kaiser Permanente is the secondary payer, send the completed electronic claim with the payment fields from the primary insurance carrier entered as follows: 837P claim transaction: Complete Field 29 (Amount Paid) 837I claim transaction: Complete Field 54 (Prior Payments) Paper Claims If Kaiser Permanente is the secondary payer, send the completed claim form with a copy of the corresponding Explanation of Benefit (EOB) or Explanation of Medicare Benefits (EOMB)/Medicare Summary Notice (MSN) from the primary insurance carrier attached to the paper claim to ensure efficient claims processing/adjudication. Kaiser Permanente cannot process a claim without an EOB or EOMB/MSN from the primary insurance carrier. 57
58 Topic Members Enrolled in Two Kaiser Permanente Plans COB Claims Submission Timeframes Instructions CMS-1500 claim form: Complete Field 29 (Amount Paid) CMS-1450 claim form: Complete Field 54 (Prior Payments) Some Members may be enrolled under two separate plans offered through Kaiser Permanente (dual coverage). In these situations, Providers need only submit ONE claim under the primary plan to Kaiser Permanente for processing. If Kaiser Permanente is the secondary payer, any Coordination of Benefits (COB) claims must be submitted for processing within 45 days of the date of the Explanation of Benefits (EOB) or EOMB/MSN COB FIELDS ON THE UB-92 and UB-04 CLAIM FORM The following fields should be completed on the CMS-1450 (UB-92 and UB-04) claim form to ensure timely and efficient claims processing. Incomplete, missing, or erroneous COB information in these fields may cause claims to be denied or pended and reimbursements delayed. For additional information, refer to the current UB-92/04 National Uniform Billing Data Element Specifications Manual. Claims submitted electronically must meet the same data requirements as paper claims. For electronic claim submissions, refer to a HIPAA website for additional information on electronic loops and segments. 58
59 837I LOOP # 2300 H1 FIELD (UB-92) FIELD NAME OCCURRENCE CODE/DATE INSTRUCTIONS/EXAMPLES Enter the appropriate occurrence code and date defining the specific event(s) relating to the claim billing period (UB-04) NOTE: If the injuries are a result of an accident, please complete Field 77 (E-Code) 2330B NM 2320 AMT 50 PAYER (Payer Identification) 54 PRIOR PAYMENTS (Payers and Patient) Enter the name and number (if known) for each payer organization from whom the Provider expects (or has received) payment towards the bill. List payers in the following order on the claim form: A = primary payer B = secondary payer C = tertiary payer Enter the amount(s), if any, that the Provider has received toward payment of the bill PRIOR to the billing date, by the indicated payer(s). List prior payments in the following order on the claim form: 2330A NM A = primary payer B = secondary payer C = tertiary payer 58 INSURED S NAME Enter the name (Last Name, First Name) of the individual in whose name insurance is being carried. List entries in the following order on the claim form: 2320 SBR 59 Patient s Relationship To Insured A = primary payer B = secondary payer C = tertiary payernote: For each entry in Field 58, there MUST be corresponding entries in Fields 59 through 62 (UB- 92 and UB-04) AND 64 through 65 (Field 65 only on the UB- 04). Enter the code indicating the relationship of the patient to the insured individual(s) listed in Field 58 (Insured s Name). List entries in the following order: A = primary payer B = secondary payer C = tertiary payer 2320 SBR 65 EMPLOYER NAME (Employer Name of the Insured) Enter the name of the employer who provides health care coverage for the insured individual (listed in Field 58). Record entries in the following order: A = primary payer B = secondary payer C = tertiary paper 2300 H1 2300H (UB-92) 67 A-Q (UB-04) 77(UB-92) 72 (UB- 04) DIAGNOSIS CODE The primary diagnosis code should be reported in Field 67. Additional diagnosis code can be entered in Field EXTERNAL CAUSE OF INJURY CODE (E- CODE) If applicable, enter an ICD-9-CM E-code in this field. 59
60 837I LOOP # 2330A NM 2320 SBR 2320 SBR FIELD FIELD NAME 60 CERT. SSN HIC ID NO. (Certificate/Social Security Number/Health Insurance Claim/Identification Number) 61 GROUP NAME (Insured Group Name) 62 INSURANCE GROUP NO. INSTRUCTIONS/EXAMPLES Enter the insured person s (listed in Field 58) unique individual Member identification number (medical/health record number), as assigned by the payer organization. List entries in the following order: A = primary payer B = secondary payer C = tertiary paper Enter the name of the group or plan through which the insurance is being provided to the insured individual (listed in Field 58). Record entries in the following order: A = primary payer B = secondary payer C = tertiary paper Enter the identification number, control number, or code assigned by the carrier or administrator to identify the GROUP under which the individual (listed in Field 58) is covered. List entries in the following order: A = primary payer B = secondary payer C = tertiary paper 2320 SBR 64 ESC (Employment Status Code of the Insured) Note: This field has been deleted from the UB-04. Enter the code used to define the employment status of the insured individual (listed in Field 58). Record entries in the following order: A = primary payer B = secondary payer C = tertiary paper COB FIELDS ON THE CMS-1500 (HCFA-1500) CLAIM FORM The following fields should be completed on the CMS-1500 (HCFA-1500) claim form, to ensure timely and efficient claims processing. Incomplete, missing, or erroneous COB information in these fields may cause claims to be denied or pended and reimbursements delayed. Claims submitted electronically must meet the same data requirements as paper claims. For electronic claim submissions, refer to a HIPAA website for additional information on electronic loops and segments. 60
61 837P LOOP # FIELD FIELD NAME INSTRUCTIONS/EXAMPLES 2330A NM 9 OTHER INSURED S NAME When additional insurance coverage exists (through a spouse, parent, etc.) enter the LAST NAME, FIRST NAME, and MIDDLE INITIAL of the insured. NOTE: This field must be completed when there is an entry in Field 11d (Is There Another Health Benefit Plan?). 2330A NM 9a OTHER INSURED S POLICY OR GROUP Enter the policy and/or group number of the insured individual named in Field 9. If you do not know the policy number, enter the Social Security number of the insured individual. NOTE: Field 9a must be completed when there is an entry in Field 11d (Is There Another Health Benefit Plan?). NOTE: For each entry in this field, there must be a corresponding Entry in 9d (Insurance Plan Name or Program Name) DMG 9b OTHER INSURED S DATE OF BIRTH/SEX Enter date of birth and sex, of the insured named in Field 9. The date of birth must include the month, day, and FOUR DIGITS for the year (MM/DD/YYYY). Example: 01/05/1971 NOTE: This field must be completed when there is an entry in Field 11d (Is There Another Health Benefit Plan?). N/A 9c EMPLOYER S NAME or SCHOOL NAME Enter the name of the employer or school name (if a student), of the insured named in Field 9. NOTE: This field must be completed when there is an entry in Field 11d (Is There Another Health Benefit Plan?). 2330B NM 9d INSURANCE PLAN NAME or PROGRAM NAME Enter the name of the insurance plan or program, of the insured individual named in Field 9. NOTE: This field must be completed when there is an entry in Field 11d (Is There Another Health Benefit Plan?) CLM 10 IS PATIENT S CONDITION RELATED TO: a. Employment? b. Auto Accident? c. Other Accident? Check yes or no to indicate whether employment, auto liability, or other accident involvement applies to one or more of the services described in Field 24. NOTE: If yes, there must be a corresponding entry in Field 14 (Date of Current Illness/ Injury) and in Field 21 (Diagnosis). PLACE (State) N/A 11d IS THERE ANOTHER HEALTH BENEFIT PLAN? PLACE (State) Enter the state the Auto Accident occurred in. Check yes or no to indicate if there is another health benefit plan. (For example, the patient may be covered 61
62 837P LOOP # FIELD FIELD NAME INSTRUCTIONS/EXAMPLES under insurance held by a spouse, parent, or some other person). NOTE: If yes, then Field Items 9 and 9a-d must be completed DTP 14 DATE OF CURRENT --Illness (First symptom) --Injury (Accident) --Pregnancy (LMP) 2300 H1 21 DIAGNOSIS OR NATURE OF ILLNESS OR INJURY Enter the date of the current illness or injury. The date must include the month, day, and FOUR DIGITS for the year (MM/DD/YYYY). Example: 01/05/2004 Enter the diagnosis and if applicable, enter the Supplementary Classification of External Cause of Injury and Poisoning Code. NOTE: This field must be completed when there is an entry in Field 10 (Is The Patient s Condition Related To) AMT 29 AMOUNT PAID Enter the amount paid by the primary insurance carrier in Field
63 5.42 Explanation of Payment (EOP) 63
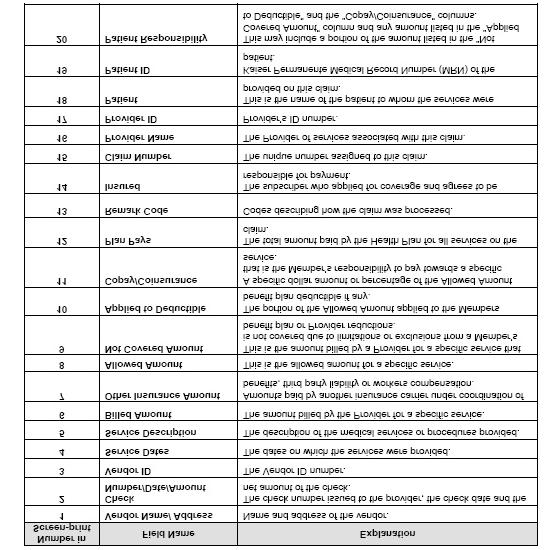
64 64
65 65
Provider Manual. Billing and Payment
 Provider Manual Billing and Payment 8/31/2011 Billing and Payment This section of the Manual was created to help guide you and your staff in working with Kaiser Permanente s billing and payment policies
Provider Manual Billing and Payment 8/31/2011 Billing and Payment This section of the Manual was created to help guide you and your staff in working with Kaiser Permanente s billing and payment policies
Transplant Provider Manual Kaiser Permanente Self-Funded Program
 e Transplant Provider Manual Kaiser Permanente Self-Funded Program Billing and Payment Table of Contents 5 SECTION 5: BILLING AND PAYMENT...4 5.1 WHOM TO CONTACT WITH QUESTIONS...4 5.2 METHODS OF CLAIMS
e Transplant Provider Manual Kaiser Permanente Self-Funded Program Billing and Payment Table of Contents 5 SECTION 5: BILLING AND PAYMENT...4 5.1 WHOM TO CONTACT WITH QUESTIONS...4 5.2 METHODS OF CLAIMS
Provider Manual. Section 5: Billing and Payment
 Provider Manual TABLE OF CONTENTS SECTION 5 SECTION 5: BILLING AND PAYMENT... 1 INTRODUCTION... 6 CLAIMS SUBMISSION GUIDE HIGHLIGHTS... 7 WHO TO CALL WITH QUESTIONS... 7 NATIONAL PROVIDER IDENTIFIER (NPI)...
Provider Manual TABLE OF CONTENTS SECTION 5 SECTION 5: BILLING AND PAYMENT... 1 INTRODUCTION... 6 CLAIMS SUBMISSION GUIDE HIGHLIGHTS... 7 WHO TO CALL WITH QUESTIONS... 7 NATIONAL PROVIDER IDENTIFIER (NPI)...
Provider Manual. Billing and Payment
 Provider Manual Billing and Payment Billing and Payment Kaiser Permanente s billing and payment policies and procedures aim to ensure that you receive timely payment for the care you provide. This section
Provider Manual Billing and Payment Billing and Payment Kaiser Permanente s billing and payment policies and procedures aim to ensure that you receive timely payment for the care you provide. This section
Provider Manual. Billing and Payment
 Provider Manual Billing and Payment Billing and Payment Kaiser Permanente s billing and payment policies and procedures aim to ensure that you receive timely payment for the care you provide. This section
Provider Manual Billing and Payment Billing and Payment Kaiser Permanente s billing and payment policies and procedures aim to ensure that you receive timely payment for the care you provide. This section
RULES OF DEPARTMENT OF COMMERCE AND INSURANCE DIVISION OF INSURANCE AND DIVISION OF TENNCARE
 RULES OF DEPARTMENT OF COMMERCE AND INSURANCE DIVISION OF INSURANCE AND DIVISION OF TENNCARE CHAPTER 0780-1-73 UNIFORM CLAIMS PROCESS FOR TENNCARE PARTICIPATING TABLE OF CONTENTS 0780-1-73-.01 Authority
RULES OF DEPARTMENT OF COMMERCE AND INSURANCE DIVISION OF INSURANCE AND DIVISION OF TENNCARE CHAPTER 0780-1-73 UNIFORM CLAIMS PROCESS FOR TENNCARE PARTICIPATING TABLE OF CONTENTS 0780-1-73-.01 Authority
1. All patient services must be billed on a fully completed CMS 1500 or UB04 form, unless otherwise indicated by contract.
 Claims 8.0 As a Participating Provider billing for services with a fee-for-service contract with MAPMG, please follow the procedures listed below. Participating Providers billing for services rendered
Claims 8.0 As a Participating Provider billing for services with a fee-for-service contract with MAPMG, please follow the procedures listed below. Participating Providers billing for services rendered
Kaiser Foundation Health Plan, Inc. CLAIMS SETTLEMENT PRACTICES PROVIDER DISPUTE RESOLUTION MECHANISMS Northern California Region
 Kaiser Foundation Health Plan, Inc. CLAIMS SETTLEMENT PRACTICES PROVIDER DISPUTE RESOLUTION MECHANISMS Northern California Region Kaiser Permanente ( KP ) values its relationship with the contracted community
Kaiser Foundation Health Plan, Inc. CLAIMS SETTLEMENT PRACTICES PROVIDER DISPUTE RESOLUTION MECHANISMS Northern California Region Kaiser Permanente ( KP ) values its relationship with the contracted community
Provider Manual. Billing and Payment
 Provider Manual Billing and Payment Billing and Payment Kaiser Permanente s billing and payment policies and procedures aim to ensure that you receive timely payment for the care you provide. This section
Provider Manual Billing and Payment Billing and Payment Kaiser Permanente s billing and payment policies and procedures aim to ensure that you receive timely payment for the care you provide. This section
Provider Manual. Billing and Payment
 Provider Manual Billing and Payment Billing and Payment Kaiser Permanente s billing and payment policies and procedures aim to ensure that you receive timely payment for the care you provide. This section
Provider Manual Billing and Payment Billing and Payment Kaiser Permanente s billing and payment policies and procedures aim to ensure that you receive timely payment for the care you provide. This section
CHAPTER 7: CLAIMS, BILLING, AND REIMBURSEMENT
 CHAPTER 7: CLAIMS, BILLING, AND REIMBURSEMENT UNIT 1: HEALTH OPTIONS CLAIMS SUBMISSION AND REIMBURSEMENT IN THIS UNIT TOPIC SEE PAGE General Information 2 Reporting Practitioner Identification Number 2
CHAPTER 7: CLAIMS, BILLING, AND REIMBURSEMENT UNIT 1: HEALTH OPTIONS CLAIMS SUBMISSION AND REIMBURSEMENT IN THIS UNIT TOPIC SEE PAGE General Information 2 Reporting Practitioner Identification Number 2
STRIDE sm (HMO) MEDICARE ADVANTAGE Claims
 MEDICARE ADVANTAGE Claims") 9 Claims Claims General Payment Guidelines An important element in claims filing is the submission of current and accurate codes to reflect the provider s services. HIPAA-AS mandates the following code
9 Claims Claims General Payment Guidelines An important element in claims filing is the submission of current and accurate codes to reflect the provider s services. HIPAA-AS mandates the following code
CMS 1500 Claim Filing Instructions. 1 Not Required Type of health insurance coverage applicable to claim. Patient s type of coverage.
 Field Locator Requirements CMS 1500 Claim Filing Instructions Field Description 1 Not Required Type of health insurance coverage to claim Patient s type of coverage. 1a Required Insured s ID Number Identification
Field Locator Requirements CMS 1500 Claim Filing Instructions Field Description 1 Not Required Type of health insurance coverage to claim Patient s type of coverage. 1a Required Insured s ID Number Identification
Chapter 5: Billing on the CMS 1500 Claim Form
 Chapter 5: Billing on the CMS 1500 Claim Form Introduction The CMS 1500 claim form is used to bill for non facility services, including professional services, freestanding surgery centers, transportation,
Chapter 5: Billing on the CMS 1500 Claim Form Introduction The CMS 1500 claim form is used to bill for non facility services, including professional services, freestanding surgery centers, transportation,
Billing Guidelines Manual for Contracted Professional HMO Claims Submission
 Billing Guidelines Manual for Contracted Professional HMO Claims Submission The Centers for Medicare and Medicaid Services (CMS) 1500 claim form is the acceptable standard for paper billing of professional
Billing Guidelines Manual for Contracted Professional HMO Claims Submission The Centers for Medicare and Medicaid Services (CMS) 1500 claim form is the acceptable standard for paper billing of professional
Fidelis Care uses TriZetto's Claims Editing Software to automatically review and edit health care claims submitted by physicians and facilities.
 BILLING AND CLAIMS Instructions for Submitting Claims The physician s office should prepare and electronically submit a CMS 1500 claim form. Hospitals should prepare and electronically submit a UB04 claim
BILLING AND CLAIMS Instructions for Submitting Claims The physician s office should prepare and electronically submit a CMS 1500 claim form. Hospitals should prepare and electronically submit a UB04 claim
Billing and Payment. To register, call UHC-FAST ( ) or your local Evercare provider representative.
 or your local Evercare provider representative.") Billing and Payment Billing and Claims On the Web www.unitedhealthcareonline.com Register for UnitedHealthcare Online SM, our free Web site for network physicians and health care professionals. At UnitedHealthcare
Billing and Payment Billing and Claims On the Web www.unitedhealthcareonline.com Register for UnitedHealthcare Online SM, our free Web site for network physicians and health care professionals. At UnitedHealthcare
6.5.3 CMS-1500 Blank Paper Claim Form
 6.5.3 CMS-1500 Blank Paper Claim Form 1500 HEALTH INSURANCE CLAIM FORM APPROVED BY NATIONAL UNIFORM CLAIM COMMITTEE 08/05 PICA PICA CARRIER 1. MEDICARE MEDICAID TRICARE CHAMPVA GROUP FECA OTHER 1a. INSURED
6.5.3 CMS-1500 Blank Paper Claim Form 1500 HEALTH INSURANCE CLAIM FORM APPROVED BY NATIONAL UNIFORM CLAIM COMMITTEE 08/05 PICA PICA CARRIER 1. MEDICARE MEDICAID TRICARE CHAMPVA GROUP FECA OTHER 1a. INSURED
The benefits of electronic claims submission improve practice efficiencies
 The benefits of electronic claims submission improve practice efficiencies Electronic claims submission vs. manual claims submission An electronic claim is a paperless patient claim form generated by computer
The benefits of electronic claims submission improve practice efficiencies Electronic claims submission vs. manual claims submission An electronic claim is a paperless patient claim form generated by computer
Chapter 7 General Billing Rules
 7 General Billing Rules Reviewed/Revised: 10/10/2017, 07/13/2017, 02/01/2017, 02/15/2016, 09/16/2015, 09/18/2014 General Information This chapter contains general information related to Health Choice Arizona
7 General Billing Rules Reviewed/Revised: 10/10/2017, 07/13/2017, 02/01/2017, 02/15/2016, 09/16/2015, 09/18/2014 General Information This chapter contains general information related to Health Choice Arizona
Completing the CMS-1500 Claim Form
 Completing the CMS-1500 Claim Form Below are instructions for filling out a CMS-1500 Claim Form (version 08/05) when submitting a claim to CareFlorida. Each field on the form is described, and all required
Completing the CMS-1500 Claim Form Below are instructions for filling out a CMS-1500 Claim Form (version 08/05) when submitting a claim to CareFlorida. Each field on the form is described, and all required
TABLE OF CONTENTS CLAIMS
 TABLE OF CONTENTS CLAIMS CLAIMS OVERVIEW... 7-1 SUBMITTING A CLAIM... 7-1 PAPER CLAIMS SUBMISSION... 7-1 ELECTRONIC CLAIMS SUBMISSION... 7-2 TIMEFRAME FOR CLAIM SUBMISSION... 7-3 PROOF OF TIMELY FILING...
TABLE OF CONTENTS CLAIMS CLAIMS OVERVIEW... 7-1 SUBMITTING A CLAIM... 7-1 PAPER CLAIMS SUBMISSION... 7-1 ELECTRONIC CLAIMS SUBMISSION... 7-2 TIMEFRAME FOR CLAIM SUBMISSION... 7-3 PROOF OF TIMELY FILING...
HUMBOLDT INDEPENDENT PRACTICE ASSOCIATION CLAIMS SETTLEMENT PRACTICES AND DISPUTE RESOLUTIONS MECHANISM
 HUMBOLDT INDEPENDENT PRACTICE ASSOCIATION CLAIMS SETTLEMENT PRACTICES AND DISPUTE RESOLUTIONS MECHANISM As required by Assembly Bill 1455, the California Department of Managed Health Care has set forth
HUMBOLDT INDEPENDENT PRACTICE ASSOCIATION CLAIMS SETTLEMENT PRACTICES AND DISPUTE RESOLUTIONS MECHANISM As required by Assembly Bill 1455, the California Department of Managed Health Care has set forth
INDIVIDUAL PRACTICE ASSOCIATION MEDICAL GROUP OF SANTA CLARA COUNTY (SCCIPA)
") INDIVIDUAL PRACTICE ASSOCIATION MEDICAL GROUP OF SANTA CLARA COUNTY (SCCIPA) AB 1455 Downstream Provider Notice CLAIMS SETTLEMENT PRACTICES & DISPUTE RESOLUTION MECHANISM As required by Assembly Bill 1455,
INDIVIDUAL PRACTICE ASSOCIATION MEDICAL GROUP OF SANTA CLARA COUNTY (SCCIPA) AB 1455 Downstream Provider Notice CLAIMS SETTLEMENT PRACTICES & DISPUTE RESOLUTION MECHANISM As required by Assembly Bill 1455,
Magellan Claims Settlement Practices and Dispute Resolution Notice to Providers Contracted with California Subsidiaries of Magellan Health, Inc.
 Magellan Claims Settlement Practices and Dispute Resolution Notice to Providers Contracted with California Subsidiaries of Magellan Health, Inc.* Revised effective Nov. 15, 2016 *Human Affairs International
Magellan Claims Settlement Practices and Dispute Resolution Notice to Providers Contracted with California Subsidiaries of Magellan Health, Inc.* Revised effective Nov. 15, 2016 *Human Affairs International
Please submit claims and encounters electronically via Office Ally at
 Claim Submission All claims must be submitted within 90 calendar days from the date of service for contracted providers unless otherwise stated in the provider service agreement. Please submit claims and
Claim Submission All claims must be submitted within 90 calendar days from the date of service for contracted providers unless otherwise stated in the provider service agreement. Please submit claims and
CLAIMS SETTLEMENT PRACTICES & DISPUTE RESOLUTION MECHANISM
 CLAIMS SETTLEMENT PRACTICES & DISPUTE RESOLUTION MECHANISM The California Department of Managed Health Care has set forth regulations establishing certain claim settlement practices and a process for resolving
CLAIMS SETTLEMENT PRACTICES & DISPUTE RESOLUTION MECHANISM The California Department of Managed Health Care has set forth regulations establishing certain claim settlement practices and a process for resolving
KPMAS also has the ability to receive your claims electronically through the Change Healthcare Clearinghouse.
 8.0 Claims As a Participating Provider billing for services with a fee-for-service contract with MAPMG, please follow the procedures listed below. Participating Providers billing for services rendered
8.0 Claims As a Participating Provider billing for services with a fee-for-service contract with MAPMG, please follow the procedures listed below. Participating Providers billing for services rendered
I. Claim submission instructions
 Humboldt Del Norte Independent Practice Association And Humboldt Del Norte Foundation for Medical Care Claims Settlement Practices and Dispute Resolutions Mechanism As required by Assembly Bill 1455, the
Humboldt Del Norte Independent Practice Association And Humboldt Del Norte Foundation for Medical Care Claims Settlement Practices and Dispute Resolutions Mechanism As required by Assembly Bill 1455, the
Claim Reconsideration Requests Reference Guide
 Claim Reconsideration Requests Reference Guide This reference tool provides instruction regarding the submission of a Claim Reconsideration Request form and details the supporting information required
Claim Reconsideration Requests Reference Guide This reference tool provides instruction regarding the submission of a Claim Reconsideration Request form and details the supporting information required
C H A P T E R 8 : Billing on the CMS 1500 Claim Form
 C H A P T E R 8 : Billing on the CMS 1500 Claim Form Reviewed/Revised: 1/1/19, 10/1/2018 8.1 INTRODUCTION The CMS 1500 claim form is used to bill for non-facility services, including professional services,
C H A P T E R 8 : Billing on the CMS 1500 Claim Form Reviewed/Revised: 1/1/19, 10/1/2018 8.1 INTRODUCTION The CMS 1500 claim form is used to bill for non-facility services, including professional services,
Preferred IPA of California Claims Settlement Practices Provider Notification
 Preferred IPA of California Claims Settlement Practices Provider Notification As required by Assembly Bill 1455, the California Department of Managed Health Care has set forth regulations establishing
Preferred IPA of California Claims Settlement Practices Provider Notification As required by Assembly Bill 1455, the California Department of Managed Health Care has set forth regulations establishing
Claim Submission. Molina Healthcare of Florida Inc. Marketplace Provider Manual
 Section 9. Claims As a contracted provider, it is important to understand how the claims process works to avoid delays in processing your claims. The following items are covered in this section for your
Section 9. Claims As a contracted provider, it is important to understand how the claims process works to avoid delays in processing your claims. The following items are covered in this section for your
2014 Provider Manual Kaiser Permanente Self-Funded Program Other Payors
 2014 Provider Manual Kaiser Permanente Self-Funded Program Other Payors Self-Funded Provider Manual Revised 12/2013 Page 1 Welcome to the Kaiser Permanente Self-Funded Program Self-Funded Provider Manual
2014 Provider Manual Kaiser Permanente Self-Funded Program Other Payors Self-Funded Provider Manual Revised 12/2013 Page 1 Welcome to the Kaiser Permanente Self-Funded Program Self-Funded Provider Manual
Arkansas Department of Health and Human Services Division of Medical Services P.O. Box 1437, Slot S-295 Little Rock, AR
 Arkansas Department of Health and Human Services Division of Medical Services P.O. Box 1437, Slot S-295 Little Rock, AR 72203-1437 Fax: 501-682-2480 TDD: 501-682-6789 & 1-877-708-8191 Internet Website:
Arkansas Department of Health and Human Services Division of Medical Services P.O. Box 1437, Slot S-295 Little Rock, AR 72203-1437 Fax: 501-682-2480 TDD: 501-682-6789 & 1-877-708-8191 Internet Website:
Claim Form Billing Instructions: CMS-1500 Claim Form
 Claim Form Billing Instructions: CMS-1500 Claim Form Item Required Field? Description and Instructions number N/A Situational When submitting a Medicare Replacement Plan claim, write or stamp Medicare
Claim Form Billing Instructions: CMS-1500 Claim Form Item Required Field? Description and Instructions number N/A Situational When submitting a Medicare Replacement Plan claim, write or stamp Medicare
Provider Training Tool & Quick Reference Guide
 Provider Training Tool & Quick Reference Guide Table of Contents I. Coastal Introduction II. Services III. Obtaining Authorization a. Coastal Intake Flow Chart b. Referral/Authorization Form (Sample) IV.
Provider Training Tool & Quick Reference Guide Table of Contents I. Coastal Introduction II. Services III. Obtaining Authorization a. Coastal Intake Flow Chart b. Referral/Authorization Form (Sample) IV.
Completing a Paper CMS-1500 (02-12) Form
 Form") Completing a Paper CS-1500 (02-12) Information in this policy does not apply to members with the Choice or Choice Plus products offered through Passport Connect S. For UnitedHealthcare s related policies/procedures,
Completing a Paper CS-1500 (02-12) Information in this policy does not apply to members with the Choice or Choice Plus products offered through Passport Connect S. For UnitedHealthcare s related policies/procedures,
Cenpatico South Carolina Frequently Asked Questions (FAQ)
") Cenpatico South Carolina Frequently Asked Questions (FAQ) GENERAL Who is Cenpatico? Cenpatico, a division of Centene Corporation, is one of the nation s most experienced behavioral health companies providing
Cenpatico South Carolina Frequently Asked Questions (FAQ) GENERAL Who is Cenpatico? Cenpatico, a division of Centene Corporation, is one of the nation s most experienced behavioral health companies providing
National Uniform Claim Committee
 National Uniform Claim Committee 1500 Health Insurance Claim Form Reference Instruction Manual for 08/05 Version Disclaimer and Notices 2005 American Medical Association This document is published in cooperation
National Uniform Claim Committee 1500 Health Insurance Claim Form Reference Instruction Manual for 08/05 Version Disclaimer and Notices 2005 American Medical Association This document is published in cooperation
5. Billing and Payment
 5. Billing and Payment It is your responsibility to submit itemized claims for Services provided to Members in a complete and timely manner in accordance with your Agreement, this Provider Manual and applicable
5. Billing and Payment It is your responsibility to submit itemized claims for Services provided to Members in a complete and timely manner in accordance with your Agreement, this Provider Manual and applicable
Glossary of Terms. Account Number/Client Code. Adjudication ANSI. Assignment of Benefits
 Account Number/Client Code Adjudication ANSI Assignment of Benefits This is the number you will see in the welcome letter you receive upon enrolling with Infinedi. You will also see this number on your
Account Number/Client Code Adjudication ANSI Assignment of Benefits This is the number you will see in the welcome letter you receive upon enrolling with Infinedi. You will also see this number on your
Complete Claims Processing
 Complete Claims Processing 1. All Complete Claims can be processed as soon as it is received. 2. Complete claims are identified properly by the claims processor when received from the mailroom, already
Complete Claims Processing 1. All Complete Claims can be processed as soon as it is received. 2. Complete claims are identified properly by the claims processor when received from the mailroom, already
Claims and Billing Manual
 2019 Claims and Billing Manual ProviDRs Care 1/2019 1 Contents Introduction... 3 How to Use This Manual... 3 About WPPA, Inc. dba ProviDRs Care... 3 How to Contact ProviDRs Care... 3 ProviDRs Care Network
2019 Claims and Billing Manual ProviDRs Care 1/2019 1 Contents Introduction... 3 How to Use This Manual... 3 About WPPA, Inc. dba ProviDRs Care... 3 How to Contact ProviDRs Care... 3 ProviDRs Care Network
Medical Paper Claims Submission Rejections and Resolutions
 NEWS & ANNOUNCEMENTS JUNE 29, 2018 UPDATE 18-446 12 PAGES Medical Paper Claims Submission Rejections and Resolutions The preferred and most efficient way for fast turnaround and claims accuracy is to submit
NEWS & ANNOUNCEMENTS JUNE 29, 2018 UPDATE 18-446 12 PAGES Medical Paper Claims Submission Rejections and Resolutions The preferred and most efficient way for fast turnaround and claims accuracy is to submit
National Uniform Claim Committee
 National Uniform Claim Committee 1500 Health Insurance Claim Form Reference Instruction Manual for 08/05 Version Disclaimer and Notices 2005 American Medical Association This document is published in cooperation
National Uniform Claim Committee 1500 Health Insurance Claim Form Reference Instruction Manual for 08/05 Version Disclaimer and Notices 2005 American Medical Association This document is published in cooperation
Passport Advantage Provider Manual Section 13.0 Provider Billing Manual Table of Contents
 Passport Advantage Provider Manual Section 13.0 Provider Billing Manual Table of Contents 13.1 Claim Submissions 13.2 Provider/Claims Specific Guidelines 13.3 Understanding the Remittance Advice 13.4 Denial
Passport Advantage Provider Manual Section 13.0 Provider Billing Manual Table of Contents 13.1 Claim Submissions 13.2 Provider/Claims Specific Guidelines 13.3 Understanding the Remittance Advice 13.4 Denial
CHOC Health Alliance Downstream Provider Notice CLAIMS SETTLEMENT PRACTICES & DISPUTE RESOLUTION MECHANISM
 CHOC Health Alliance Downstream Provider Notice CLAIMS SETTLEMENT PRACTICES & DISPUTE RESOLUTION MECHANISM As required by Assembly Bill 1455, the California Department of Managed Health Care has set forth
CHOC Health Alliance Downstream Provider Notice CLAIMS SETTLEMENT PRACTICES & DISPUTE RESOLUTION MECHANISM As required by Assembly Bill 1455, the California Department of Managed Health Care has set forth
Univera Community Health Participating Provider Manual
 Univera Community Health Participating Provider Manual 8.0 Billing and Remittance Table of Contents 8.1 Electronic Submission of Claims Required... 8 1 8.2 General Requirements for Claims Submission...
Univera Community Health Participating Provider Manual 8.0 Billing and Remittance Table of Contents 8.1 Electronic Submission of Claims Required... 8 1 8.2 General Requirements for Claims Submission...
Claim Form Billing Instructions UB-04 Claim Form
 Claim Form Billing Instructions UB-04 Claim Form Presbyterian Health Plan / Presbyterian Insurance Company, Inc 02/19/08 Page 1 of 5 Presbyterian Health Plan / Presbyterian Insurance Company, Inc 02/19/08
Claim Form Billing Instructions UB-04 Claim Form Presbyterian Health Plan / Presbyterian Insurance Company, Inc 02/19/08 Page 1 of 5 Presbyterian Health Plan / Presbyterian Insurance Company, Inc 02/19/08
Archived SECTION 15-BILLING INSTRUCTIONS. Section 15 - Billing Instructions
 SECTION 15-BILLING INSTRUCTIONS 15.1 ELECTRONIC DATA INTERCHANGE... 2 15.2 INTERNET ELECTRONIC CLAIM SUBMISSION... 2 15.3 CMS-1500 CLAIM FORM... 3 15.4 PROVIDER COMMUNICATION UNIT... 3 15.5 RESUBMISSION
SECTION 15-BILLING INSTRUCTIONS 15.1 ELECTRONIC DATA INTERCHANGE... 2 15.2 INTERNET ELECTRONIC CLAIM SUBMISSION... 2 15.3 CMS-1500 CLAIM FORM... 3 15.4 PROVIDER COMMUNICATION UNIT... 3 15.5 RESUBMISSION
Archived SECTION 15-BILLING INSTRUCTIONS. Section 15 - Billing Instructions
 SECTION 15-BILLING INSTRUCTIONS 15.1 ELECTRONIC DATA INTERCHANGE... 2 15.2 INTERNET ELECTRONIC CLAIM SUBMISSION... 2 15.3 CMS-1500 AND PHARMACY CLAIM FORMS... 3 15.4 PROVIDER COMMUNICATION UNIT... 3 15.5
SECTION 15-BILLING INSTRUCTIONS 15.1 ELECTRONIC DATA INTERCHANGE... 2 15.2 INTERNET ELECTRONIC CLAIM SUBMISSION... 2 15.3 CMS-1500 AND PHARMACY CLAIM FORMS... 3 15.4 PROVIDER COMMUNICATION UNIT... 3 15.5
Housekeeping. Link Participant ID with Audio. Mute your line UNMUTED. Raise your hand with questions
 Housekeeping Link Participant ID with Audio If your Participant ID has not been entered, dial #ParticipantID#. EXAMPLE: Participant ID is 16, then enter #16#. Mute your line UNMUTED MUTED OTHER MUTE OPTIONS
Housekeeping Link Participant ID with Audio If your Participant ID has not been entered, dial #ParticipantID#. EXAMPLE: Participant ID is 16, then enter #16#. Mute your line UNMUTED MUTED OTHER MUTE OPTIONS
Claim Form Billing Instructions CMS 1500 Claim Form
 Claim Form Billing Instructions CMS 1500 Claim Form Item Required Field? Description and Instructions. 1 Optional Indicate the type of health insurance for which the claim is being submitted. 1a Required
Claim Form Billing Instructions CMS 1500 Claim Form Item Required Field? Description and Instructions. 1 Optional Indicate the type of health insurance for which the claim is being submitted. 1a Required
Cedars-Sinai Medical Group Downstream Provider Notice CLAIMS SETTLEMENT PRACTICES & DISPUTE RESOLUTION MECHANISM
 Cedars-Sinai Medical Group Downstream Provider Notice CLAIMS SETTLEMENT PRACTICES & DISPUTE RESOLUTION MECHANISM As required by Assembly Bill 1455, the California Department of Managed Health Care has
Cedars-Sinai Medical Group Downstream Provider Notice CLAIMS SETTLEMENT PRACTICES & DISPUTE RESOLUTION MECHANISM As required by Assembly Bill 1455, the California Department of Managed Health Care has
LOUISIANA MEDICAID PROGRAM ISSUED: 07/01/13 REPLACED: CHAPTER 7: COMMUNITY CHOICES WAIVER APPENDIX D: CLAIMS FILING PAGE(S) 18 CLAIMS FILING
 18 CLAIMS FILING") CLAIMS FILING Community Choices Waiver services (except ADHC) must be filed by electronic claims submission 837P or on the CMS 1500 claim form. Claims for Adult Day Health Care Services must be filed by
CLAIMS FILING Community Choices Waiver services (except ADHC) must be filed by electronic claims submission 837P or on the CMS 1500 claim form. Claims for Adult Day Health Care Services must be filed by
Crossover claims should be submitted to Molina Medicaid Solutions, P.O. Box 91020, Baton Rouge, LA
 Dear Provider, Thank you for your participation in the Louisiana Medicaid Program. Payment may be made to your provider type for recipients who also have Medicare coverage. For these recipients, Louisiana
Dear Provider, Thank you for your participation in the Louisiana Medicaid Program. Payment may be made to your provider type for recipients who also have Medicare coverage. For these recipients, Louisiana
5. Billing and Payment
 5. Billing and Payment It is your responsibility to submit itemized claims for services provided to Members in a complete and timely manner in accordance with your Agreement, this Provider Manual and applicable
5. Billing and Payment It is your responsibility to submit itemized claims for services provided to Members in a complete and timely manner in accordance with your Agreement, this Provider Manual and applicable
Claim Form Billing Instructions CMS-1500 (08-05) Claim Form
 Claim Form") Claim Form Billing Instructions CMS-1500 (08-05) Claim Form Presbyterian Health Plan / Presbyterian Insurance Company, Inc Original: 06/24/07 Page 1 of 10 Presbyterian Health Plan / Presbyterian Insurance
Claim Form Billing Instructions CMS-1500 (08-05) Claim Form Presbyterian Health Plan / Presbyterian Insurance Company, Inc Original: 06/24/07 Page 1 of 10 Presbyterian Health Plan / Presbyterian Insurance
CLAIMS Section 6. Provider Service Center. Timely Claim Submission. Clean Claim. Prompt Payment
 Provider Service Center Harmony has a dedicated Provider Service Center (PSC) in place with established toll-free numbers. The PSC is composed of regionally aligned teams and dedicated staff designed to
Provider Service Center Harmony has a dedicated Provider Service Center (PSC) in place with established toll-free numbers. The PSC is composed of regionally aligned teams and dedicated staff designed to
Physicians Medical Group of San Jose, Inc.
 Physicians Medical Group of San Jose, Inc. AB 1455 REGULATIONS FOR CLAIMS SUBMISSIONS, CLAIMS SETTLEMENT, CLAIMS DISPUTES, AND FEE SCHEDULES As required by Assembly Bill 1455, the California Department
Physicians Medical Group of San Jose, Inc. AB 1455 REGULATIONS FOR CLAIMS SUBMISSIONS, CLAIMS SETTLEMENT, CLAIMS DISPUTES, AND FEE SCHEDULES As required by Assembly Bill 1455, the California Department
Section 7. Claims Procedures
 Section 7 Claims Procedures Timely Filing Guidelines 1 Claim Submissions 1 Claims for Referred Services 1 Claims for Authorized Services 2 Filing Electronic Claims 2 Filing Paper Claims 2 Claims Resubmission
Section 7 Claims Procedures Timely Filing Guidelines 1 Claim Submissions 1 Claims for Referred Services 1 Claims for Authorized Services 2 Filing Electronic Claims 2 Filing Paper Claims 2 Claims Resubmission
Mental Health/Substance Use Treatment Claim Form
 Mental Health/Substance Use Treatment Claim Form DIRECTIONS FOR COMPLETION If you are in treatment with a non-participating Beacon Health Options, Inc. (Beacon) provider and your provider has indicated
Mental Health/Substance Use Treatment Claim Form DIRECTIONS FOR COMPLETION If you are in treatment with a non-participating Beacon Health Options, Inc. (Beacon) provider and your provider has indicated
INSTRUCTIONS FOR BILLING MEDICARE CROSSOVER SERVICES CMS-1500 (02/15) INSTRUCTIONS
 INSTRUCTIONS") INSTRUCTIONS FOR BILLING MEDICARE CROSSOVER SERVICES CMS-1500 (02/15) INSTRUCTIONS OVERVIEW OF MEDICARE CROSSOVER BILLING Professional services are billed on the CMS-1500 (02/12) claim form. A sample copy
INSTRUCTIONS FOR BILLING MEDICARE CROSSOVER SERVICES CMS-1500 (02/15) INSTRUCTIONS OVERVIEW OF MEDICARE CROSSOVER BILLING Professional services are billed on the CMS-1500 (02/12) claim form. A sample copy
Section 7 Billing Guidelines
 Section 7 Billing Guidelines Billing, Reimbursement, and Claims Submission 7-1 Submitting a Claim 7-1 Corrected Claims 7-2 Claim Adjustments/Requests for Review 7-2 Behavioral Health Services Claims 7-3
Section 7 Billing Guidelines Billing, Reimbursement, and Claims Submission 7-1 Submitting a Claim 7-1 Corrected Claims 7-2 Claim Adjustments/Requests for Review 7-2 Behavioral Health Services Claims 7-3
Form DFS-F5-DWC-9 B. Completion Instructions. Submitted by Licensed Health Care Providers
 Form DFS-F5-DWC-9 B Completion Instructions Submitted by Licensed Health Care Providers A. Header Information Health Care Providers shall enter Insurer/Carrier name, address and zip code in the blank area
Form DFS-F5-DWC-9 B Completion Instructions Submitted by Licensed Health Care Providers A. Header Information Health Care Providers shall enter Insurer/Carrier name, address and zip code in the blank area
5. Billing and Payment
 5. Billing and Payment It is your responsibility to submit itemized claims for services provided to Members in a complete and timely manner in accordance with your Agreement, this Provider Manual and applicable
5. Billing and Payment It is your responsibility to submit itemized claims for services provided to Members in a complete and timely manner in accordance with your Agreement, this Provider Manual and applicable
3. The Health Plan accepts the standard current billing forms: the CMS 1500 (02/12) form and the UB- 04 hospital billing forms.
 form and the UB- 04 hospital billing forms.") BILLING PROCEDURES SECTION 11 Billing Procedures 1. All claims should be submitted to: The Health Plan 1110 Main St Wheeling WV 26003 Claim forms must be completed in their entirety. The efficiency with
BILLING PROCEDURES SECTION 11 Billing Procedures 1. All claims should be submitted to: The Health Plan 1110 Main St Wheeling WV 26003 Claim forms must be completed in their entirety. The efficiency with
LOUISIANA MEDICAID PROGRAM ISSUED: 05/11/16 REPLACED: 09/28/15 CHAPTER 7: COMMUNITY CHOICES WAIVER APPENDIX D: CLAIMS FILING PAGE(S) 14 CLAIMS FILING
 14 CLAIMS FILING") CLAIMS FILING Hard copy billing of waiver services are billed on the paper CMS-1500 (02/12) claim form or electronically on the 837P Professional transaction. Effective for dates of service on or after
CLAIMS FILING Hard copy billing of waiver services are billed on the paper CMS-1500 (02/12) claim form or electronically on the 837P Professional transaction. Effective for dates of service on or after
HOW TO SUBMIT OWCP BILLS TO THE FEDERAL BLACK LUNG PROGRAM
 HOW TO SUBMIT OWCP - 1500 BILLS TO THE FEDERAL BLACK LUG PROGRAM OFFICE OF WORKERS COMPESATIO PROGRAMS DIVISIO OF COAL MIE WORKERS COMPESATIO The services performed by the following providers should be
HOW TO SUBMIT OWCP - 1500 BILLS TO THE FEDERAL BLACK LUG PROGRAM OFFICE OF WORKERS COMPESATIO PROGRAMS DIVISIO OF COAL MIE WORKERS COMPESATIO The services performed by the following providers should be
Form DFS-F5-DWC-9 B. Completion Instructions
 Completion Instructions Submitted by Ambulatory Surgical Centers A. Header Information Health Care Providers shall enter Insurer/Carrier name, address and zip code in the blank area on top-right side of
Completion Instructions Submitted by Ambulatory Surgical Centers A. Header Information Health Care Providers shall enter Insurer/Carrier name, address and zip code in the blank area on top-right side of
Blue Cross & Blue Shield of Rhode Island CMS-1500 (02/12) Form Completion Informational Guide
 Form Completion Informational Guide") Blue Cross & Blue Shield of Rhode Island CMS-1500 (02/12) Form Completion Informational Guide All professional provider services filed to Blue Cross & Blue Shield of Rhode Island (BCBSRI) must be filed
Blue Cross & Blue Shield of Rhode Island CMS-1500 (02/12) Form Completion Informational Guide All professional provider services filed to Blue Cross & Blue Shield of Rhode Island (BCBSRI) must be filed
LOUISIANA MEDICAID PROGRAM ISSUED: 02/04/15 REPLACED: 04/30/14 CHAPTER 18: DURABLE MEDICAL EQUIPMENT APPENDIX B CLAIMS FILING PAGE(S) 13 CLAIMS FILING
 13 CLAIMS FILING") CLAIMS FILING Hard copy billing of DME services are billed on the paper CMS-1500 (02/12) claim form or electronically on the 837P Professional transaction. Instructions in this appendix are for completing
CLAIMS FILING Hard copy billing of DME services are billed on the paper CMS-1500 (02/12) claim form or electronically on the 837P Professional transaction. Instructions in this appendix are for completing
CLAIMS SETTLEMENT PRACTICES, DISPUTE RESOLUTION MECHANISM, AND FEE SCHEDULE NOTICE
 CLAIMS SETTLEMENT PRACTICES, DISPUTE RESOLUTION MECHANISM, AND FEE SCHEDULE NOTICE As required by Assembly Bill 1455, the California Department of Managed Health Care has set forth regulations establishing
CLAIMS SETTLEMENT PRACTICES, DISPUTE RESOLUTION MECHANISM, AND FEE SCHEDULE NOTICE As required by Assembly Bill 1455, the California Department of Managed Health Care has set forth regulations establishing
20. CLAIMS PROCESSING. A. Claims Processing APPLIES TO: A. This policy applies to all IEHP Medi-Cal Providers. POLICY:
 A. Claims Processing APPLIES TO: A. This policy applies to all IEHP Medi-Cal Providers. POLICY: A. All Capitated Providers are delegated the responsibility of claims processing for noncapitated services
A. Claims Processing APPLIES TO: A. This policy applies to all IEHP Medi-Cal Providers. POLICY: A. All Capitated Providers are delegated the responsibility of claims processing for noncapitated services
Chapter 9 Billing on the UB Claim Form
 9 Billing on the UB Claim Form Reviewed/Revised: 10/10/2017, 02/01/2017, 02/15/2016, 09/16/2015, 09/18/2014 Introduction The UB claim form is used to bill for all hospital inpatient, outpatient, emergency
9 Billing on the UB Claim Form Reviewed/Revised: 10/10/2017, 02/01/2017, 02/15/2016, 09/16/2015, 09/18/2014 Introduction The UB claim form is used to bill for all hospital inpatient, outpatient, emergency
Administrative Guide
 Physician, Health Care Professional, Facility and Ancillary Provider Administrative Guide 2012 KanCare Program DRAFT PENDING ADDITIONAL UPDATES AND STATE OF KANSAS APPROVAL DRAFT PENDING ADDITIONAL UPDATES
Physician, Health Care Professional, Facility and Ancillary Provider Administrative Guide 2012 KanCare Program DRAFT PENDING ADDITIONAL UPDATES AND STATE OF KANSAS APPROVAL DRAFT PENDING ADDITIONAL UPDATES
Revised CMS-1500 Claim Form for Professional and General Services
 Revised CMS-1500 Claim Form for Professional and General Services The Form CMS-1500 (08-05) will be accepted by Louisiana Medicaid for all dates of submission beginning March 5, 2007, but will not be mandated
Revised CMS-1500 Claim Form for Professional and General Services The Form CMS-1500 (08-05) will be accepted by Louisiana Medicaid for all dates of submission beginning March 5, 2007, but will not be mandated
C H A P T E R 9 : Billing on the UB Claim Form
 C H A P T E R 9 : Billing on the UB Claim Form Reviewed/Revised: 10/1/2018 9.0 INTRODUCTION The UB claim form is used to bill for all hospital inpatient, outpatient, emergency room services, dialysis clinic,
C H A P T E R 9 : Billing on the UB Claim Form Reviewed/Revised: 10/1/2018 9.0 INTRODUCTION The UB claim form is used to bill for all hospital inpatient, outpatient, emergency room services, dialysis clinic,
MEMORANDUM. DATE: February 5, Participating Providers. FROM: Network Management Services
 MEMORANDUM DATE: February 5, 2014 TO: Participating Providers FROM: Network Management Services RE: CMS 1500 Form Version 02/2012 Mandated as of April 1, 2014 Dear Participating Provider, We are pleased
MEMORANDUM DATE: February 5, 2014 TO: Participating Providers FROM: Network Management Services RE: CMS 1500 Form Version 02/2012 Mandated as of April 1, 2014 Dear Participating Provider, We are pleased
Chapter 7. Billing and Claims Processing
 Chapter 7. Billing and Claims Processing 7.1 Electronic Claims Submission 3 7.1.1 How it Works... 3 7.1.2 Advantages... 3 7.1.3 How to Initiate... 4 7.1.4 Transactions Available... 5 7.1.5 NAIC Codes...
Chapter 7. Billing and Claims Processing 7.1 Electronic Claims Submission 3 7.1.1 How it Works... 3 7.1.2 Advantages... 3 7.1.3 How to Initiate... 4 7.1.4 Transactions Available... 5 7.1.5 NAIC Codes...
XPressClaim Help. Diagnosis 1,2,3,etc. Enter the number(s) of the corresponding diagnosis code(s) that applies to this service.
 of the corresponding diagnosis code(s) that applies to this service.") Keying Information Professional Claims CMS 1500 Claim type Please select the type of claim: 1- Original claim 7- Replacement of prior claim Please note: 7- Replacement of prior claim should only be selected
Keying Information Professional Claims CMS 1500 Claim type Please select the type of claim: 1- Original claim 7- Replacement of prior claim Please note: 7- Replacement of prior claim should only be selected
National Uniform Claim Committee
 National Uniform Claim Committee 1500 Claim Form Map to the X12 837 Health Care Claim: Professional November 2008 The 1500 Claim Form Map to the X12 837 Health Care Claim: Professional includes data elements,
National Uniform Claim Committee 1500 Claim Form Map to the X12 837 Health Care Claim: Professional November 2008 The 1500 Claim Form Map to the X12 837 Health Care Claim: Professional includes data elements,
Tips for Completing the CMS-1500 Version 02/12 Claim Form
 Tips for Completing the CMS-1500 Version 02/12 Claim Form As a provider partner, we value the services you provide and it is important to us that you are reimbursed for the work you do. To assure your
Tips for Completing the CMS-1500 Version 02/12 Claim Form As a provider partner, we value the services you provide and it is important to us that you are reimbursed for the work you do. To assure your
20. CLAIMS PROCESSING. A. Claims Processing APPLIES TO:
 20. CLAIMS PROCESSING A. Claims Processing APPLIES TO: A. This policy applies to all Capitated Providers (Payers) delegated for claims payment for IEHP DualChoice Cal MediConnect Plan (Medicare Medicaid
20. CLAIMS PROCESSING A. Claims Processing APPLIES TO: A. This policy applies to all Capitated Providers (Payers) delegated for claims payment for IEHP DualChoice Cal MediConnect Plan (Medicare Medicaid
Archived SECTION 15 - BILLING INSTRUCTIONS. Section 15 - Billing Instructions
 SECTION 15 - BILLING INSTRUCTIONS 15.1 ELECTRONIC DATA INTERCHANGE...2 15.2 INTERNET ELECTRONIC CLAIM SUBMISSION...2 15.3 UB-04 CLAIM FORM...3 15.4 PROVIDER RELATIONS COMMUNICATION UNIT...3 15.5 RESUBMISSION
SECTION 15 - BILLING INSTRUCTIONS 15.1 ELECTRONIC DATA INTERCHANGE...2 15.2 INTERNET ELECTRONIC CLAIM SUBMISSION...2 15.3 UB-04 CLAIM FORM...3 15.4 PROVIDER RELATIONS COMMUNICATION UNIT...3 15.5 RESUBMISSION
CMS Provider Payment Dispute Resolution Mechanism
 CMS Provider Payment Dispute Resolution Mechanism The Centers for Medicare and Medicaid Services (CMS) established an independent provider payment dispute resolution process for disputes between non-contracted
CMS Provider Payment Dispute Resolution Mechanism The Centers for Medicare and Medicaid Services (CMS) established an independent provider payment dispute resolution process for disputes between non-contracted
Section 6 - Claims Procedures
 Section 6 - Claims Procedures Claim Submission Procedures 1 Filing Electronic Claims 1 Filing Paper Claims 1 Claims for Referred Services 3 Claims for Authorized Services 3 Claims Resubmission Policy 3
Section 6 - Claims Procedures Claim Submission Procedures 1 Filing Electronic Claims 1 Filing Paper Claims 1 Claims for Referred Services 3 Claims for Authorized Services 3 Claims Resubmission Policy 3
Provider Claims and Billing Manual
 Provider Claims and Billing Manual Version Five Publication Date: October 2015 Claims and Billing Manual Claims and Billing Manual Table of Contents Claim Filing... 1 Procedures for Claim Submission...
Provider Claims and Billing Manual Version Five Publication Date: October 2015 Claims and Billing Manual Claims and Billing Manual Table of Contents Claim Filing... 1 Procedures for Claim Submission...
HCFA Mapping to BCBSNC Local Proprietary Format (LPF) and the HIPAA 837-Professional Implementation Guide
 and the HIPAA 837-Professional Implementation Guide") HCFA Mapping to BCBSNC Local Proprietary at (LPF) n/a Header and Trailer - Header & Footers information will be in the ISA/IEA, GS/GE & THE ST/SE HDR 1-3 TRL1-3 1 Leave blank n/a n/a 1a Insured s ID Enter
HCFA Mapping to BCBSNC Local Proprietary at (LPF) n/a Header and Trailer - Header & Footers information will be in the ISA/IEA, GS/GE & THE ST/SE HDR 1-3 TRL1-3 1 Leave blank n/a n/a 1a Insured s ID Enter
HOW TO SUBMIT OWCP-04 BILLS TO ACS
 HOW TO SUBMIT OWCP-04 BILLS TO ACS OFFICE OF WORKERS COMPENSATION PROGRAMS DIVISION OF ENERGY EMPLOYEES OCCUPATIONAL ILLNESS COMPENSATION The following services should be billed on the OWCP-04 Form: General
HOW TO SUBMIT OWCP-04 BILLS TO ACS OFFICE OF WORKERS COMPENSATION PROGRAMS DIVISION OF ENERGY EMPLOYEES OCCUPATIONAL ILLNESS COMPENSATION The following services should be billed on the OWCP-04 Form: General
Sunflower Health Plan. Regional Provider Workshop
 Sunflower Health Plan Regional Provider Workshop Agenda & Objectives e Third Party Liability (TPL) & Coordination of Benefits (COB) Claims Submission Requirements Overview Sunflower TPL & COB Claims Processing
Sunflower Health Plan Regional Provider Workshop Agenda & Objectives e Third Party Liability (TPL) & Coordination of Benefits (COB) Claims Submission Requirements Overview Sunflower TPL & COB Claims Processing
20. CLAIMS PROCESSING. A. Claims Processing APPLIES TO: A. This policy applies to all IEHP Medi-Cal Providers. POLICY:
 A. Claims Processing APPLIES TO: A. This policy applies to all IEHP Providers. POLICY: A. All Capitated Providers are delegated the responsibility of claims processing for non- Capitated services and are
A. Claims Processing APPLIES TO: A. This policy applies to all IEHP Providers. POLICY: A. All Capitated Providers are delegated the responsibility of claims processing for non- Capitated services and are
* PREPARING FOR THE TRANSITION TO HIPAA VERSION 5010: MISCELLANEOUS CHANGES IN FACILITY BILLING AS A RESULT THE TRANSITION TO VERSION 5010 *
 * PREPARING FOR THE TRANSITION TO HIPAA VERSION 5010: MISCELLANEOUS CHANGES IN FACILITY BILLING AS A RESULT OF THE TRANSITION TO VERSION 5010 * Read this bulletin on-line via NaviNet NOVEMBER 3, 2010 MS-PROV-2010-001
* PREPARING FOR THE TRANSITION TO HIPAA VERSION 5010: MISCELLANEOUS CHANGES IN FACILITY BILLING AS A RESULT OF THE TRANSITION TO VERSION 5010 * Read this bulletin on-line via NaviNet NOVEMBER 3, 2010 MS-PROV-2010-001
C H A P T E R 7 : General Billing Rules
 C H A P T E R 7 : General Billing Rules Reviewed/Revised: 10/1/18 7.0 GENERAL INFORMATION This chapter contains general information related to Steward Health Choice Arizona s billing rules and requirements.
C H A P T E R 7 : General Billing Rules Reviewed/Revised: 10/1/18 7.0 GENERAL INFORMATION This chapter contains general information related to Steward Health Choice Arizona s billing rules and requirements.
HIPAA 5010 Frequently Asked Questions
 HIPAA 5010 Frequently Asked Questions Table of Contents 1. Navicure s Online Claim Form........5 Q: Will the format change on Navicure s online HCFA 1500 claim form?... 5 2. General 5010 Questions.............5
HIPAA 5010 Frequently Asked Questions Table of Contents 1. Navicure s Online Claim Form........5 Q: Will the format change on Navicure s online HCFA 1500 claim form?... 5 2. General 5010 Questions.............5
CPT ONLY COPYRIGHT 2012 AMERICAN MEDICAL ASSOCIATION. ALL RIGHTS RESERVED CLEAN CLAIM EXAMPLE AND INSTRUCTIONS
 CPT ONLY COPYRIGHT 2012 AMERICAN MEDICAL ASSOCIATION. ALL RIGHTS RESERVED CLEAN CLAIM EXAMPLE AND INSTRUCTIONS CLEAN CLAIM EXAMPLE AND INSTRUCTIONS CMS- 1500 Provider Definitions The following definitions
CPT ONLY COPYRIGHT 2012 AMERICAN MEDICAL ASSOCIATION. ALL RIGHTS RESERVED CLEAN CLAIM EXAMPLE AND INSTRUCTIONS CLEAN CLAIM EXAMPLE AND INSTRUCTIONS CMS- 1500 Provider Definitions The following definitions
SECTION G BILLING AND CLAIMS
 CLAIMS PAYMENT METHODS SECTION G Abrazo Advantage Health Plan (AAHP) offers 2 forms of payment for services provided; paper check and electronic funds transfer (direct deposit). Electronic Funds Transfer
CLAIMS PAYMENT METHODS SECTION G Abrazo Advantage Health Plan (AAHP) offers 2 forms of payment for services provided; paper check and electronic funds transfer (direct deposit). Electronic Funds Transfer
Provider Orientation. style. Click to edit Master subtitle style. December, 2017
 Click EMHS to Employee edit Master Health title Plan Provider Orientation Click to edit Master subtitle December, 2017 Pam Hageny Director of Health Plan Operations & Provider Network Beacon Health EMHS
Click EMHS to Employee edit Master Health title Plan Provider Orientation Click to edit Master subtitle December, 2017 Pam Hageny Director of Health Plan Operations & Provider Network Beacon Health EMHS
LOUISIANA MEDICAID PROGRAM ISSUED: 04/01/16 REPLACED: 09/28/15 CHAPTER 9: ADULT DAY HEALTH CARE WAIVER APPENDIX E CLAIMS FILING PAGE(S) 12
 12") CLAIMS FILING Hard copy billing of waiver services are billed on the paper CMS-1500 (02/12) claim form or electronically on the 837P Professional transaction. Instructions in this appendix are for completing
CLAIMS FILING Hard copy billing of waiver services are billed on the paper CMS-1500 (02/12) claim form or electronically on the 837P Professional transaction. Instructions in this appendix are for completing