A PRIMER FOR PRIMARY CARE
|
|
|
- Ernest Blankenship
- 5 years ago
- Views:
Transcription
1 MACRA / MIPS Transition to value-based payment in Medicare A PRIMER FOR PRIMARY CARE Robert Resnik MD MBA

2 Source: CMS
3 What does MACRA Accomplish? Repeals the Sustainable Growth Rate (SGR) Formula Changes the way that Medicare rewards clinicians for value over volume Streamlines multiple quality programs under the new Merit-Based Incentive Payments System (MIPS) Provides bonus payments for participation in eligible alternative payment models (APMs)

4 Source: CMS

5 Source: CMS
6 Composite Performance Score (CPS) MIPS defines four categories of eligible clinician performance These categories determine a MIPS composite performance score (CPS) of up to 100 points Relative weights CY2017 performance year and associated CY2019 payment year Quality (50%) Advancing Care Information (ACI, renamed from Meaningful Use) (25%) Clinical Practice Improvement Activities (CPIA) (15%) Resource Use (10%)
7 MIPS PERFORMANCE MEASURES Quality 50% 45% 30% Advancing Care 25% 25% 25% Resource Use 10% 15% 30% Clinical Practice Improvement 15% 15% 15% Quality PQRS Resource Use Value based payment modifier ADVANCING CARE EHR Incentive Clinical Practice Improvement Care Coordination, Population management, Expand Access, patient safety, beneficiary engagement

8 Source: CMS Billing up to $10,000 Treating up to 100 patients

9 Source: CMS

10 Source: CMS

11 Source: CMS

12 Source: CMS
13 Nominal Financial Risk A threshold to trigger losses no greater than 4% Shared losses become APM responsibility when exceeding expected expenditures from 0% to 4%. Example Expected spending threshold is $10,000,000 APM responsible for losses once spending exceeds $10,000,000 or responsibility for losses triggered once spending exceeds up to $400,000 APM responsible for all losses over $400,000 or 4% of threshold If APM does not start paying back losses say until 5% or after exceeding the target threshold by $500,000 then not considered nominal risk
14 Nominal Financial Loss Loss sharing of at least 30% APM must be responsible for losses of at least 30% or greater If total losses are $1 million the APM must be responsible for $300,000 or more It total losses are $ 1million and the APM is only responsible for $250,000 (25%) then APM does not qualify Maximum possible loss is at least 4% If total losses are $10,000,000 APM must be responsible for $400,000 or more in losses to be a qualified APM

15 Source: CMS
16 Comprehensive Primary Care Plus The Comprehensive Primary Care Plus (CPC+) program qualifies as an Advanced APM under the MACRA proposed rule. This program does not meet risk criteria but does meet the or standard to qualify as a Medical Home Model

17 Source: CMS

 First APM performance")
18 MACRA milestones 2016 Last performance year for PQRS, meaningful use, and VBPM Proposed rule outlining MIPS and APM criteria expected in the spring 2017 First performance measurement year for MIPS 2018 Separate PQRS, meaningful use, and VBPM programs / penalties sunset on Dec First MIPS payment adjustments applied, maximum +4% (phases up to + 9% in 2022) First APM performance assessed, 5% bonus payments made to qualifying participants
19 2019 (first year) penalty risks compared Prior Law 2019 adjustments PQRS -2% MU -5% VBPM Total penalty risk Bonus potential (VBPM only) -4% or more* -11% or more* Unknown (budget neutral)* *VBPM was in effect for 3 years before MACRA passed, and penalty risk was increased in each of these years; there were no ceilings or floors on penalties and bonuses, only a budget neutrality requirement. MIPS factors Quality measurement MU Resource use Clinical improvement activities 2019 scoring 50% of score 25% of score 10% of score 15% of score Total penalty risk Max of -4% Bonus potential Max of 4%, plus potential 10% for high performers
20 MIPS Financial Impacts MACRA defines two types of financial impacts for clinicians participating in MIPS: A small, annual inflationary adjustment to the Part B fee schedule The inflationary adjustment is an annual +0.5% increase for the payment years CY2016 to CY2019, which is the first payment year for MIPS under the QPP. The inflationary adjustment resumes in CY2026 and thereafter, where MIPS eligible clinicians will receive a +0.25% annual adjustment
21 MIPS Financial Impacts MIPS payment adjustments (incentives or penalties) based on the MIPS 100-point Composite Performance Score (CPS) The potential MIPS incentives and penalties via payment adjustments are much more substantial than the inflationary adjustments The calculated CPS could result in incentives reaching 37% of Medicare Part B payments by the fourth year of the program, while maximum penalties grow to 9%:
 2. Advancing Care Information (ACI, renamed from Meaningful Use) (25%) 3.")
22 COMPOSITE PERFORMANCE SCORE (CPS) Each performance category is scored separately Each as a percentage of maximum possible performance within that category Category-level scores are weighted by the appropriate category weight Weights are then summed to produce the CPS. 1. Quality (50%) 2. Advancing Care Information (ACI, renamed from Meaningful Use) (25%) 3. Clinical Practice Improvement Activities (CPIA) (15%) 4. Resource Use (10%)
23 Penalties and Incentives Program Performance Year Medicare Part B Payment Adjustment Year Maximum -% Medicare Part B Payment Adjustment Maximum +% Medicare Part B Payment Adjustment PQRS/VBM % penalty +4%*X incentive MIPS % penalty +4%*X incentive MIPS % penalty +5%*X incentive MIPS % penalty +7%*X incentive MIPS % penalty +9%*X incentive CMS budget-neutral program: Incentive offset by penalties For MIPS, x capped at 3.0 plus a 10% "exceptional performance bonus" For Performance Year 2020, up to 9% x % = 37% bonus
24 MIPS Adjustment Example for Year 2017 If a clinician has a CPS of zero, the penalty assessed is 4%, the maximum penalty. If a clinician earns a CPS of 100 points, then the incentive is 4%*X (adjustment multiplier) X is a budget-neutrality factor CMS calculates to set the total MIPS incentive pool in dollars equal to the total MIPS penalties Keeps the program budget neutral.

25 Source: CMS

26 Source: CMS
27 Performance Threshold Each performance year corresponds to a payment year For 2017 the performance year corresponds to a payment year of 2019 Each performance year CMS sets a performance threshold (PT) This is the number of points at which a provider earning PT points receives 0% adjustment to their Medicare Part B payments. Every incremental point above the PT results in progressively more incentives Each point the CPS is below the threshold, the clinician is assessed a proportional penalty until a floor (for %) is reached. Very few eligible clinicians will experience a zero payment adjustment Essentially, every CPS point translates directly into higher or lower reimbursement
28 The performance threshold is determined annually as the mean or median of the MIPS scores for all eligible providers in a prior period For the initial two payment years (2019 and 2020), the PT will be based on historical MIPS scores For payments in 2019 and 2020 the PT will be determined by a combination of historical performance on measures and activities related to PQRS, MU, VBM, and possibly other factors as determined by CMS.
29 MIPS TRACK EXTRA BONUS CMS has set aside about $500 million for the first six years of the program to reward exceptional performers in the MIPS track. CMS has defined these providers are in the 25 th percentile of possible composite performance scores (CPS)compared to the normal performance threshold.
30 Exceptional Performance Bonus - Example Normal performance threshold =64 Range above the performance threshold would be th percentile of those possible values would be (¼ * (100-64) Exceptional Performance Threshold = (.25*64) + 64 = 73. Providers with CPS 73 or > eligible for a bonus from the $500 million pool. Sliding scale is used based on score to determine percentage of bonus Providers at 73 = factor of 0.5 percent Providers at 100 = factor of 10 percent maximum additional adjustment factor. CMS will announce the exceptional performance threshold and normal performance threshold prior to the performance period.
31 Budget Neutrality X Factor Theoretically, the budget-neutrality X factor could reach a cappedvalued of 3.0 This will happen should there be many more clinicians penalized than receiving incentives in a given year For the CY2017 performance year, the base adjustment could reach as high as 4% x 3.0 = 12%, This will result in an even higher maximum incentive of 12% base + 10% exceptional performance bonus = 22%. Similarly, the maximum possible incentive for the CY2020 performance year could reach 9% x % = 37%.

32 MIPS Adjustment/Bonuses 32 Based on composite performance score EPs may receive an upward, downward or no payment adjustment Exceptional Performers see significant opportunities for additional bonuses/adjustments on top of traditional MIPS incentives Available in 2019 through 2024
33 CPS Scores in lowest ¼ or 0-25% percentile always receive the maximum negative adjustment for 2017 (-4%) CPS Scores in lowest percentile receive graduated reduction between maximum negative and zero for 2017 ( 0 to -4 %) CPS Scores between percentile >0% <=2% for each point above performance threshold CPS Scores at or above 75% or top 25% graded adjustment between approx. >2% to 4% plus bonus performance graded from 0.5(close to 75% to 10% at 100%. Can max out at 4%+10% or 14% for 2019 Remember budget neutrality factor can increase up to 3X or 3 x4% + 10% =22%
34 What is the MACRA impact on fees? RVU relative value unit Medicare physician fee schedule factor MIPS adjustment factor
35 Medicare physician fee schedule factor Each year this factor is updated 2015 it was it is Misvalued codes = -.77% RVU budget neutrality = -.02% Annual MACRA update =.50% none in Overall this resulted in -0.29% change Starting 2026 (.25%) for MIPS and.75% for APM

36 Source: CMS

37 Source: CMS

38 Source: CMS
39 COMPOSITE PERFORMANCE SCORE (CPS)
40 Individual vs. Group Rating MIPS clinicians can choose to be rated as an individual-clinician basis Or as a group of clinicians (defined by a tax ID) The choice applies across all performance categories. CPS could be significantly impacted depending upon whether that clinician is rated individually or inherits the CPS earned by an entire group. MIPS clinicians in Medicare ACOs must be rated as a group MIPS clinicians do not have the choice to be rated as individuals
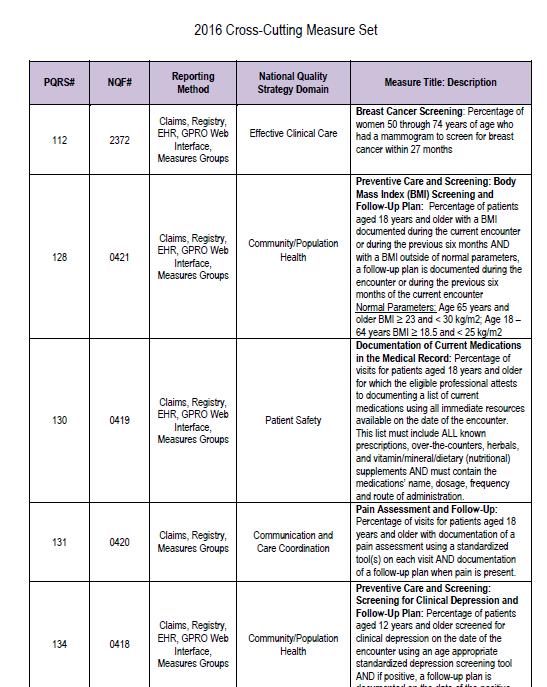
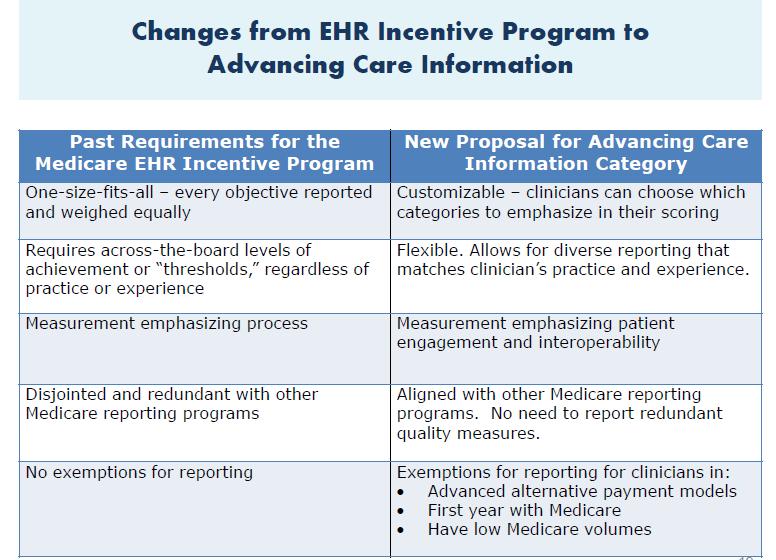
41 Quality Initial weight is 50% MIPS essentially adopts the quality measures and reporting methods from the PQRS and VBM programs. Although there are some changes to the PQRS reporting methods for the most part the quality reporting methods remain the same. For the registry, EHR, and qualified clinical data registry (QCDR) reporting methods, a clinician must typically select a minimum of six PQRS measures These can be across any combination of quality domains 1. one measure is a cross-domain-cutting measure 2. one measure is an outcome measure
42
43 Key Changes from Current Program (PQRS): Reduced from 9 measures to 6 measures No domain requirement Emphasis on outcome measurement
44 Clinician or group picks PQRS 6 measures CMS calculates Two additional measures for individual clinicians or groups <10 Three additional (for groups with 10+ clinicians) population These are (claims-based) quality measures Each PQRS and population quality measure is assigned a possible 10 quality points. Groups < 10 providers have maximum 80 quality points available Groups >= 10 providers have maximum 90 quality points available Each measure earns up to 10 points Points are calculated based upon the percentile-basis performance of that measure relative to national peer benchmarks
45 PQRS Examples #1. Diabetes: Hemoglobin A1c Poor Control #5. Heart Failure (HF): Angiotensin-Converting Enzyme (ACE) Inhibitor or Angiotensin Receptor Blocker (ARB) Therapy for Left Ventricular Systolic Dysfunction (LVSD) #6. Coronary Artery Disease (CAD): Antiplatelet Therapy #7. Coronary Artery Disease (CAD): Beta-Blocker Therapy Prior Myocardial Infarction (MI) or Left Ventricular Systolic Dysfunction (LVEF < 40%) #8. Heart Failure (HF): Beta-Blocker Therapy for Left Ventricular Systolic Dysfunction (LVSD) #39. Screening for Osteoporosis for Women Aged Years of Age #41. Osteoporosis: Pharmacologic Therapy for Men and Women Aged 50 Years and Older #48. Urinary Incontinence: Assessment of Presence or Absence of Urinary Incontinence in Women Aged 65 Years and Older #50. Urinary Incontinence: Plan of Care for Urinary Incontinence in Women Aged 65 Years and Older #52. Chronic Obstructive Pulmonary Disease (COPD): Inhaled Bronchodilator Therapy
46 If the Quality measure has a 69% measure rate then that measure would earn 8 out of 10 possible points. Decile Sample Quality Measure Benchmarks Possible Points Decile % Decile % Decile % Decile % Decile % Decile % Decile % Decile % Decile % Decile % 10
47 Example For an individual provider or group < 10 Add together the total points for each of the eight quality categories If each of the eight measures earned eight points each Total points = 8 x 8 = 64 out of possible 80 64/80 = 80% For 2017 Performance Year Quality has weight of 50% 50% x 80% x 100 = 40 points added to overall CPS
48 MIPS grants bonus points for certain quality reporting activities. 1. Two bonus points for reporting each extra outcome measure beyond the one required 2. Two bonus points for reporting the patient experience measure (CAHPS for MIPS survey counts as one patient experience measure) 3. One bonus point for reporting each extra high priority measure The total bonus points are capped at 5% (of the denominator of the quality score) Example 5% of 80 = 4 max bonus points in the previous example
49 Example Assume four bonus points were earned Quality score would increase to (64+4)/80 = 85% Quality weighted at 50% results in 42.5 CPS points (40 pt w/o bonus) Bonus points are not counted in the quality score denominator It is possible to get a quality score of greater than 100% If > 100% the quality score is truncated back down to 100%.
50 Advancing Care Information (ACI) Initial weight 25% MIPS has renamed MU to ACI No longer all-or-nothing compliance program Now a continuous scoring system MU measure rates are compared to benchmarks just like with quality MU program may have low compliance threshold Provider scoring 15% given same credit at another scoring 90% Under the ACI scoring system the provider scoring 15% will receive 2/10 points Provider scoring 90% will receive 10/10 So a historically high MU achiever may end up having a low ACI score if MU performance rates do not improve.
51 Source:CMS
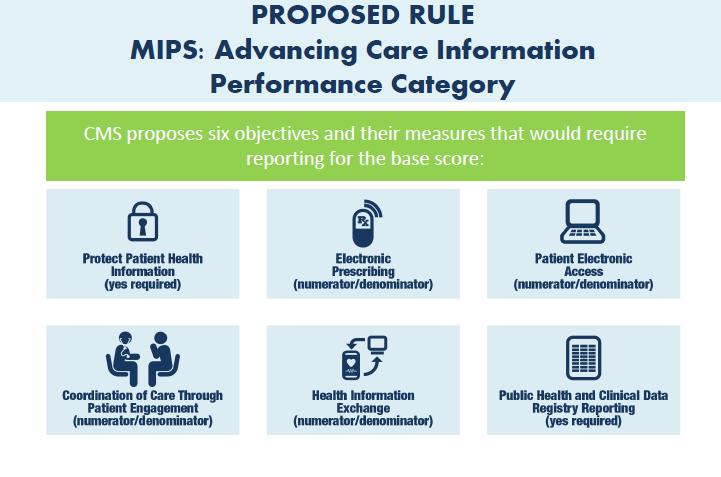
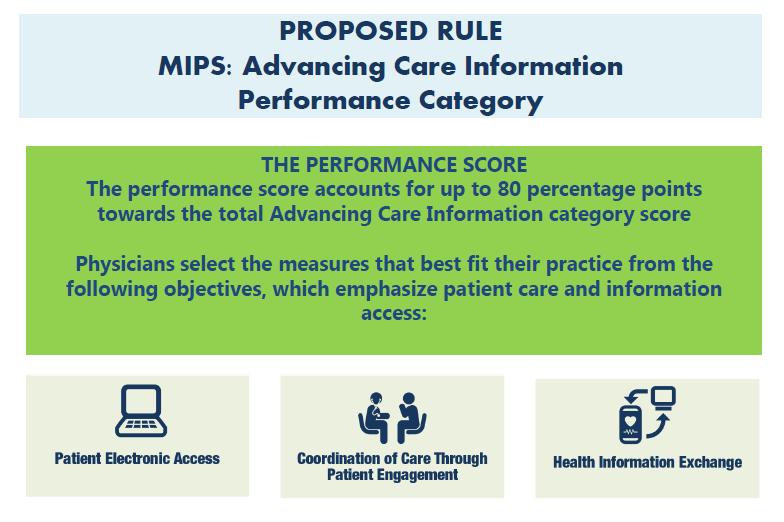
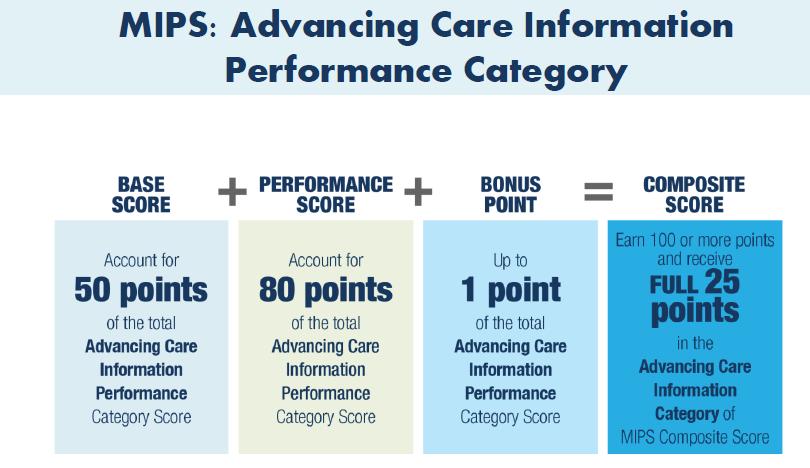
52 The ACI category defines 131 ACI performance points that can be earned: Base Score: 50 points for reporting either a non-zero numerator or a yes, as applies, for selected measures from the MU Modified Stage 2 or MU Stage 3 measure sets Performance Score: Up to 80 points for performance on eight measures per the decile scoring scale Bonus Point: Up to 1 bonus point for reporting to an additional public health registry The ACI percentage score is calculated by dividing the number of ACI points by 100 The percentage is capped at 100% if more than 100 ACI points be earned For example, 80 ACI points equates to 80% ACI performance score Weighted score for CPS = 80% (ACI performance) x 25% (ACI category weight) x 100 = 20 CPS points contributed by ACI.
53 Source:CMS
54 Source:CMS
55
56 Clinical Practice Improvement Activities (CPIA) Maximum points in CPIA category is 60 Report any combination of medium-weight activities (worth 10 points each) and/or high-weight activities (worth 20 points) each If a clinician is non-patient-facing, a small practice with 15 or fewer professionals, a practice in a rural area, or a practice in a geographic Health Professional Shortage Area (HPSA), then all activities are worth 30 points each - 2 Activities = 60 points If a clinician participates in an APM, the clinician earns 30 points and can earn additional points as described above If a clinician is in certain medical home models, the clinician automatically earns the full 60 points
57 Patient Centered Medical Home A patient-centered medical home will be recognized if it is: A nationally recognized accredited patient-centered medical home A Medicaid Medical Home Model Medical Home Model. The NCQA Patient-Centered Specialty Recognition will also be recognized, which qualifies as a comparable specialty practice. Nationally recognized accredited patient-centered medical homes are recognized if they are accredited by: (1) The Accreditation Association for Ambulatory Health Care (2) The National Committee for Quality Assurance (NCQA) PCMH recognition (3) The Joint Commission Designation (4) The Utilization Review Accreditation Commission (URAC)
58
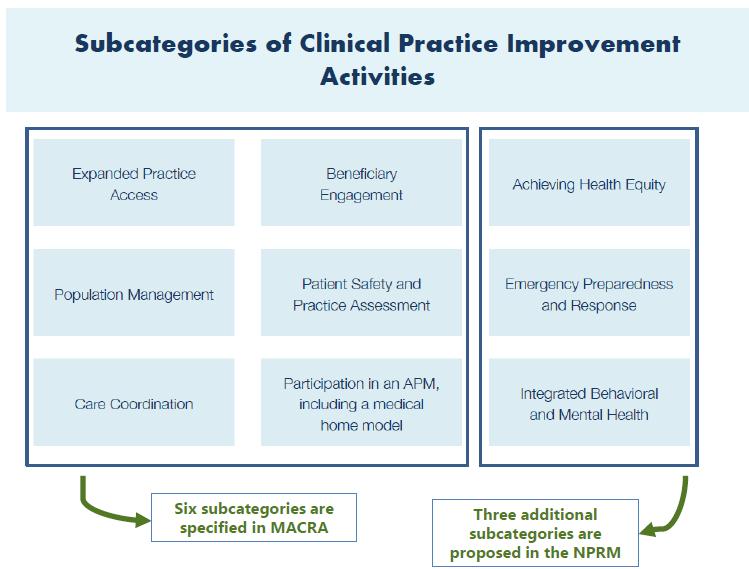
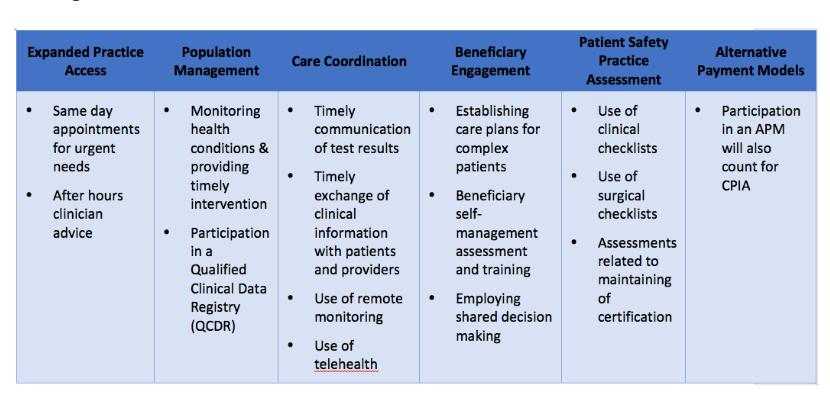
59 CPIA CATEGORIES Expanded Practice Access: expanded practice hours telehealth services participation in models designed to improve access to services Population Management: participation in chronic care management programs participation in rural and Indian Health Services programs participation in community programs with other stakeholders to address population health Use Qualified Clinical Data Registry (QCDR) to track population outcomes Care coordination: Use of a QCDR to share information timely communication and follow up participation in various CMS models designed to improve care coordination implementation of care coordination training implementation of plans to handle transitions of care active referral management
60 CPIA CATEGORIES Beneficiary Engagement: Use of EHR to document patient-reported outcomes Providing enhanced patient portals Participation in a QCDR that promotes the use of patient engagement tools Use of QCDR patient experience data to inform efforts to improve beneficiary engagement Patient Safety and Practice Assessment Use of QCDR data for ongoing practice assessments and patient safety improvements Use of tools such as the Surgical Risk Calculator Achieving Health Equity: Seeing new and follow-up Medicaid patients in a timely manner Use of QCDR for demonstrating performance of processes for screening for social determinants Emergency Response and Preparedness: Participation in disaster medical teams or participation in domestic International humanitarian volunteer work Integrated Behavioral and Mental Health: Tobacco intervention and smoking cessation efforts Integration with mental health services

61 Source: CMS
62 There are currently 90 activities listed in the proposed ruling. Each activity is given a weight of either medium or high. CPIAs are weighted as high based on alignment with CMS national priorities Quality Innovation Network-Quality Improvement Organization (QIN/QIO) Comprehensive Primary Care Initiative An activity identified as a public health priority (such as emphasis on anticoagulation management or utilization of prescription drug monitoring programs).
63
64 Some examples of high-weighted activities (20 points) include: Beneficiary Engagement: Collection and follow-up on patient experience and satisfaction data on beneficiary engagement, including development of improvement plan. Access 24/7 practice access, with access to patient medical record; provision of same-day or next-day access to providers Patient Safety and Practice Assessment: Consultation of Prescription Drug Monitoring Program prior to the issuance of a Controlled Substance Schedule II (CSII) opioid prescription that lasts for longer than 3 days.
65 Examples of medium-weighted activities (10 points) include: Care Coordination: Ensure that there is bilateral exchange of necessary patient information to guide patient care that could include one or more of the following: Participate in a Health Information Exchange Use structured referral notes. Population Management: Participation in research that identifies interventions, tools, or processes that can improve a targeted patient population. Care plan : Engaging patients and family caregivers in developing a care plan and care priorities, documented in an EHR Initially, these activities must be conducted for a full 90 days during the performance year. A full list of proposed activities can be found on page 946 of the MACRA proposed rule.
66 Calculating the CPIA % score The CPIA percentage score is calculated by dividing the total CPIA points by 60. For example, 45 points would yield a 45/60 = 75% CPIA performance score CPIA is weighted at 15% 75% x 15% x 100 = points
67 Resource Use - Weight Year 1-10% MIPS rates clinicians for Resource Use (Medicare costs of attributed patients) will be based on 40+ cost measures to account for differences among specialties. No separate reporting requirements for clinicians Measures are calculated based on claims collected by CMS. Measures can earn up to 10 points each on a percentile benchmark scale The percentage score is then multiplied by the Resource Use category weight (10% for the CY2017 performance year) to deliver the CPS points contributed. If provider earns eight points on each of two included cost measures. Resource Use points = (8+8)/20 x 10% x 100 = 8 CPS points.
68
69

70 Source: CMS
71 Example of Calculating a CPS (COMPOSITE PERFORMANCE SCORE) Assuming that the numerical examples used for the four categories as described above all apply to the same clinician, we can calculate a total CPS from the components: Quality = (56 of 80 points) x 50% weight x 100 = 35 CPS points ACI = (50 of 100 points) x 25% weight x 100 = 12.5 CPS points CPIA = (40 of 60 points) x 15% weight x 100 = 10 CPS points Resource Use = (14 of 20 points) x 10% weight x 100 = 7 CPS points Total CPS points = = 64.5
72 MIPS will publish each eligible clinician s annual Composite Performance Score (CPS) and scores for each MIPS performance category within approximately 12 months after the end of the relevant performance year. Consumers will be able to see their providers rated on a scale of 0 to 100 and how their providers compare to peers nationally. This raises the level of transparency while releasing more specific data
73 MIPS APM Clinicians MIPS eligible clinician also participating in an APM and meeting certain additional requirements There are some special rules governing MIPS data submission for such a clinician. The MIPS Quality category may not require a separate data submission if the APM is already collecting quality data for CMS to analyze
74 MIPS APM clinician? Participation in an Alternative payment model (APM) APM includes only these payment models run by CMS (not by commercial payers): CMS Innovation Center Model (other than a Health Care Innovation Award) Medicare Shared Savings Program (MSSP ACOs) Demonstration under the Health Care Quality Demonstration Program Demonstration required by federal law The MIPS APM concept provides some relief to those APM clinicians who otherwise would be subject to the full range of MIPS requirements in addition to their APM obligations
75 Medicare Shared Savings Program MSSP Accountable care organization (ACOs) Track 1 (one-sided, incentive-only) Tracks 2 and 3 (two-sided) of MSSP All MSSP Tracks meet the criteria for MIPS APM entities. Track 1 is deemed non-advanced APM s Each provider MSSP Track 1 is subject to MIPS The ACO s MIP s eligible clinicians get some preferential treatment on scoring and data submission
76 What are the benefits of being a MIPS APM clinician? MIPS APM clinician benefits from special rules governing MIPS scoring and data submission These are designed to grant performance credit and reduce reporting burdens for APM MIPS eligible clinicians An APM provider who meets either the first-year-clinician or low-volume MIPS exemption is not subject to MIPS at all.
77 The rating of MIPS APM clinicians is based on the rating for their entire APM entity not the individual provider This is similar to how MIPS enables multiple clinicians billing through the same tax ID (TIN) to be rated for MIPS as a group There are some differences however: A MIPS APM entity may comprise of only a single MIPS eligible clinician (solo practice TIN in MSSP) MIPS normally requires at least two clinicians to be within a group of clinicians rated for MIPS as a group.
78 These providers do not inherit the MIPS performance of the entity as for MIPS normally, all clinicians billing through a TIN and choosing to be rated for MIPS as a group will inherit the MIPS composite performance score (CPS) earned by the group. A MIPS APM entity may be comprised of more than one unique participating TIN (ACO) MIPS normally has only one TIN is allowed per group of clinicians rated for MIPS as a group. A MIPS APM entity may include a participating TIN which contains clinicians billing through that TIN who do not participate in the MIPS APM entity
79 MIPS APM vs ADVANCED APM Different criteria to determine whether an APM is a MIPS APM vs an Advanced APM An Advanced APM may not include MIPS eligible clinicians on its participation list and, thereby, would not be deemed a MIPS APM
80 CMS requires reporting certain performance categories on an individual clinician basis For a MIPS APM CMS sums the associated measure values submitted for individual clinicians to derive the MIPS APM entity s group CPS. The entity s CPS becomes the MIPS eligible CPS as long as they are listed on the entity s list of participating clinicians as of December 31st of the performance year

81 Source: CMS
82 Medicare Shared Savings Program (MSSP) ACOs Quality: 50% weight - Requires group data submission via CMS Web Interface for the ACO s TIN (submitted on behalf of the entire ACO, not at the level of each TIN participating in the ACO) Resource Use: 0% weight (weight redistributed to CPIA and ACI categories as below) - Already evaluated by MSSP, so set to zero weight for MIPS. CPIA: 20% weight - Requires group data submission via allowed data submission methods for each TIN participating in the ACO. (15% weight for MIPS provider) The ACO s score is calculated as the average across TINs weighted by the number of MIPS eligible clinicians in each TIN. Any ACO participant TIN that is also deemed a patient-centered medical home or comparable specialty practice will receive the highest potential CPIA score. All other ACO participants TINs will receive a minimum of half the highest potential CPIA score. Advancing Care Information (ACI): 30% weight - Requires group data submission via allowed data submission methods for each TIN participating in the ACO, and the ACO s score is calculated as the average across TINs weighted by the number of MIPS eligible clinicians in each TIN. (25% MIPS)
83 It is important to understand ramifications of reduction of the MIPS Resource Use weight to 0% in all of the MIPS APM types Don t have to report in one category but now makes performance in each of other categories more important. Really consolidated to 3 categories
84 Next Generation ACOs Same as MSSP Quality (50% weight) Resource Use (0% weight) CPIA (20% weight) ACI (30% weight) Exception is that performance data for each MIPS eligible clinician, rather than for each ACO participant TIN, must be submitted to CMS. CMS averages all of the MIPS eligible clinician scores for each category to derive the category score for the ACO entity.
85 Clinicians that qualify currently to meet the requirements for the APM track cannot opt out of the APM track and into the MIPS track.
86 Notification of Track Officially providers may not know which track they fall into until 2018 when awaiting approval for the ADVANCED APM track So for performance year 2017 with payments in 2019 this could create some reporting issues. This could create some issues for Advanced APM s
87 Partial Qualifying APM Participants. APM organizations that participate in Advanced APM models, but have less than the required percentage of revenue at risk or patient counts APM must have at least 20% but less than 25% of their Medicare payments tied to APM APM must have at least 10% of their eligible Medicare patients tied to APM but not greater than 20% 2023 and beyond at least 50% but less than 75% of Medicare payments tied to APM 2023 and beyond must have at least 35% but less than 50% of Medicare patients tied to APM Partial APM do not qualify for APM Track Don t qualify for 5% bonus pay Can opt-in to MIPS and be judged just like other MIPS participants. If opt-out will not receive any payment adjustments for the year
88
89 Summary Previous year track does not dictate the next performance year track Each year providers will have a new opportunity to qualify for the APM track. By default any provider not on the APM track is assigned the MIPS track unless they are a first year Medicare provider or low volume Medicare provider. CMS has estimated that over 90%+ of providers will fall into MIPS track CMS has an estimate of 8-10% will be in the APM track
90 Quality - Summary Similar to PQRS Some measure will be claims based and calculated by CMS At present there will still be over 200 measures to choose from With over 80% of these being specific to specialists Providers only have to report on 6 measures vs current 9 measures under PQRS Bonus points for reporting on more than 6 measures Bonus points for using certified EMR technology
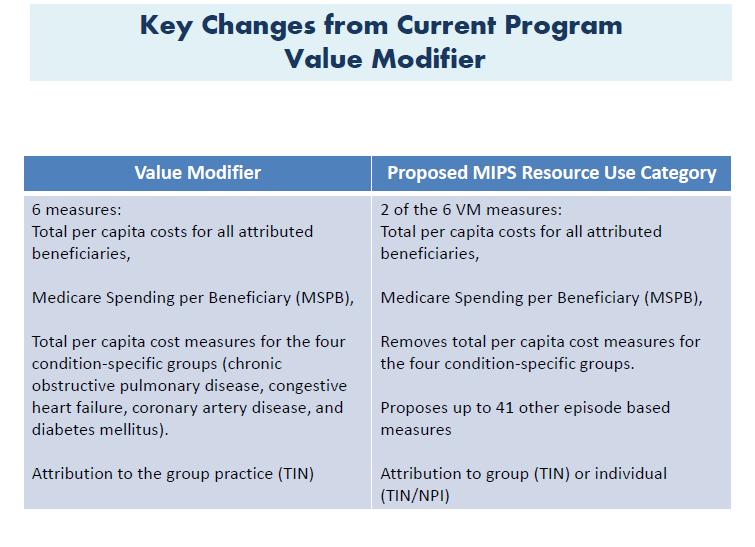
91 Cost /Resource Use- Summary Similar to Value Based Payment Modifier (VBPM) No changes to measures still on Part A and Part B with focus on per-capita cost for all beneficiaries and Medicare spending per beneficiary Expanded from 4 episode cost measures to over 40
92 Advanced Care Summary Builds on Meaningful Use Focus on expanding use of EMR Can report as group or individual NO longer all or nothing can get partial credit No longer requires reporting on clinical decision support and computerized clinical orders entry
93 Clinical Practice Improvement Activity- Summary New category that rewards physicians for practice improvement activities 90 activities in 9 categories Weighting Medium or High with associated point value difference Expanded Practice Access Beneficiary Engagement Achieving health equity Population Management Patient Safety
94 Reporting Requirements- Summary Providers can submit performance data as an individual, a group, or an APM entity. Must report same way across all four categories. If provider reports through an APM they must do so for all categories.
95 Part D Prescription Drugs MIPS only includes Part A and Part B (which includes some drug costs). There is a provision to include Part D in the future CMS is currently evaluating this option
96 Adding New Provider in Performance Year Payment adjustments are assigned at the level of the individual provider this is by TIN/NPI combination. New providers payments are based on prior-year performance at previous practice MIPS ties payment adjustments to the MIPS performance for the preceding 2 years. Providers practicing in multiple TIN s during performance year will receive a weighted score across all TIN s Provider joining in 2019 would be paid on their performance from Providers hired could bring in a positive or negative adjustment based on their previous performance
97 Medicare Advantage and MIPS For Performance years through 2019 there is no credit for MA patients Starting in 2021 (based on the 2019 performance year), CMS will allow providers to use other payer data to meet qualification for the Advanced APM model including Medicare Advantage Not all downside risk Medicare Advantage plans will qualify clinicians for the APM track in Consideration will also be given to the commercial alternative payment model must meet the same criteria that CMS uses to assess CMS-run APMs. CMS has also considered that full capitation risk arrangements would meet this Other Payer Advanced APM financial risk criterion.
98 APM MIPS ( MSSP Track 1) Get composite score of group Still have to do some TIN/Individual reporting No guaranteed bonus Get some preferential scoring but if PCMH get higher score Only rated on three categories rather than 4 in MIPS not Resource Use as this is evaluated by MSSP Dependent more on performance of group in fewer categories Have potential bonus if MSSP generates savings
99 Advanced APM No MIPS Get 5% bonus and elevated payments starting 2025 (0.75% increase over 0.25%) Have potential for savings and losses At some point improving cost becomes difficult and may lead to losses or dropping out of program Many ACO s have not generated savings.
100 MIPS SCORES and PATIENT RISK Risk adjustment included in both the quality and resource use categories. Quality category outcomes measures typically have risk adjustment embedded in their calculation. Resource use category will utilize risk adjustment standards from the VBPM. This will be adjusted for clinical factors and demographics. There was also be risk adjustment for Medicare spending per beneficiary (MSPB) measure. The possibility will exist that CMS may introduce risk adjustment for socioeconomic status on quality measured and resources use.
101 Initial Performance Threshold for 2019 There will be a proposed to pre-set the Performance Threshold (PT) using historical provider performance This will be derived from the current physician pay-forperformance programs. For 2019 CMS will use 2014 and 2015 PQRS, VBPM, and MU data to determine the PT CMS will make this performance threshold available prior to 2017 for 2019 payments
102 MIPS is a revenue neutral program Winners = Losers This is similar to the Value-Based Payment Modifier
103 Maximum Payments % (including bonus 4% max) % (including bonus 5% max) % (including bonus 7% max) % (including bonus 9% max) Budget neutrality adjustment 10% exceptional performance payout 3 X upward multiplier Ensure payout = penalties
104 MIPS Conversion Factor- Summary Each year provider gets MIPS payment adjustment factor + or - % Based on Composite Performance score from CMS will set a performance threshold (PT). Providers scoring above the PT will receive a bonus in the way of a positive MIPS adjustment factor Providers scoring below the PT will be subject to a penalty, or negative MIPS adjustment factor. MIPS payment adjustments will change every year. Not cumulative if -2% in 2019 and -4% in 2020 the overall factor in 2020 will still be -4% There will always be a two year lag in performance and payment
105 5 things to do now to prepare for the January 2017 start of MIPS Make sure all providers in your TIN understand MIPS and MACRA Estimate your MIPS score using your current MU, PQRS and VBM scores Optimize MU & PQRS/VBM Quality to maximize the MIPS score (comprise 75% of the CY2017 MIPS score) Evaluate staff, resources and organizational structure Identify CY2016 deadlines impacting CY2017 MIPS, e.g. Medicare Shared Savings Program Track 2/3 ACO or NCQA PCMH application deadlines to gain MIPS exemptions or points
106 APM entities anticipating having MIPS APM clinicians preparation 1. Determine whether your APM entity qualifies as a MIPS APM entity according to the eligibility rules. 2. Estimate the number of MIPS eligible clinicians in the MIPS APM entity 3. Estimate the MISP eligible clinicians Medicare Part B annual payments at risk under MIPS 4. This will help determine the amount of exposure your entity has to the MIPS APM scoring and data submission rules. 5. Estimate the MIPS composite performance score (CPS) for your MIPS APM entity 6. Begin to optimize the MIPS categories with performance gaps or high weightings
107 GOOD LUCK Questions
AAOS MACRA Proposed Rule Summary (Short)
") AAOS MACRA Proposed Rule Summary (Short) Merit-Based Incentive Payment System (MIPS), Advanced Alternative Payment Model (APM) Incentive, and Criteria for Physician-Focused Payment Models Ref: CMS-5517-P
AAOS MACRA Proposed Rule Summary (Short) Merit-Based Incentive Payment System (MIPS), Advanced Alternative Payment Model (APM) Incentive, and Criteria for Physician-Focused Payment Models Ref: CMS-5517-P
Medicare Quality Payment Program Overview (MACRA)
") Medicare Quality Payment Program Overview (MACRA) December 2016 Rev. 12/1/16 Some general observations MACRA is complex More than a replacement for the SGR Many of the new requirements are revisions to
Medicare Quality Payment Program Overview (MACRA) December 2016 Rev. 12/1/16 Some general observations MACRA is complex More than a replacement for the SGR Many of the new requirements are revisions to
MACRA: New Medicare Reimbursement Models Sharp HealthCare
 MACRA: New Medicare Reimbursement Models Sharp HealthCare August 15, 2016 Nathan M. Bays, Esq. General Counsel, The Health Management Academy Executive Director, Advisors Caitlin Greenbaum, MPH Director,
MACRA: New Medicare Reimbursement Models Sharp HealthCare August 15, 2016 Nathan M. Bays, Esq. General Counsel, The Health Management Academy Executive Director, Advisors Caitlin Greenbaum, MPH Director,
2018 Merit-Based Incentive Payment System (MIPS) Scoring Overview
 Scoring Overview") The Physicians Advocacy Institute s Medicare Quality Payment Program (QPP) Physician Education Initiative 2018 Merit-Based Incentive Payment System (MIPS) Scoring Overview 1 P a g e MEDICARE QPP PHYSICIAN
The Physicians Advocacy Institute s Medicare Quality Payment Program (QPP) Physician Education Initiative 2018 Merit-Based Incentive Payment System (MIPS) Scoring Overview 1 P a g e MEDICARE QPP PHYSICIAN
PRIMER: MACRA and the Merit-based Incentive Payment System (MIPS) Tara O Neill Hayes January 31, 2016
 Tara O Neill Hayes January 31, 2016") PRIMER: MACRA and the Merit-based Incentive Payment System (MIPS) Tara O Neill Hayes January 31, 2016 Background On April 16, 2015, the Medicare Access and CHIP Reauthorization Act (MACRA) was signed into
PRIMER: MACRA and the Merit-based Incentive Payment System (MIPS) Tara O Neill Hayes January 31, 2016 Background On April 16, 2015, the Medicare Access and CHIP Reauthorization Act (MACRA) was signed into
Medicare Releases Final Rule for the Second Year of the Quality Payment Program
 Medicare Releases Final Rule for the Second Year of the Quality Payment Program On Nov. 2, 2017, CMS issued the Calendar Year 2018 Quality Payment Program (QPP) final rule for the second transition year
Medicare Releases Final Rule for the Second Year of the Quality Payment Program On Nov. 2, 2017, CMS issued the Calendar Year 2018 Quality Payment Program (QPP) final rule for the second transition year
CY 2018 Quality Payment Program Final Rule Summary
 CY 2018 Quality Payment Program Final Rule Summary On November 2, 2017, the Centers for Medicare and Medicaid Services (CMS) released its final rule outlining the requirements for year two of the Quality
CY 2018 Quality Payment Program Final Rule Summary On November 2, 2017, the Centers for Medicare and Medicaid Services (CMS) released its final rule outlining the requirements for year two of the Quality
Quality Payment Program Year 2
 Quality Payment Program Year 2 MIPS Highlights Raising the performance threshold to 15 points in Year 2 (from 3 points in the transition year). Allowing the use of 2014 Edition and/or 2015 Certified Electronic
Quality Payment Program Year 2 MIPS Highlights Raising the performance threshold to 15 points in Year 2 (from 3 points in the transition year). Allowing the use of 2014 Edition and/or 2015 Certified Electronic
4/8/17. The Changing Nature of Physician Payment and Health Care Reform in The AMA A Unifying Voice for Physicians
 The Changing Nature of Physician Payment and Health Care Reform in 2017 U of Mo Family Medicine Update April 7, 2017 David Barbe, MD MHA President-elect American Medical Association VP Regional Operations
The Changing Nature of Physician Payment and Health Care Reform in 2017 U of Mo Family Medicine Update April 7, 2017 David Barbe, MD MHA President-elect American Medical Association VP Regional Operations
2018 Quality Payment Program Final Rule. Summary
 Summary On Thursday, November 3, 2017, CMS issued the 2018 Quality Payment Program (QPP) final rule. Comments on the final rule are due January 1, 2018. The QPP encompasses the Merit-based Incentive Payment
Summary On Thursday, November 3, 2017, CMS issued the 2018 Quality Payment Program (QPP) final rule. Comments on the final rule are due January 1, 2018. The QPP encompasses the Merit-based Incentive Payment
Thank you, and enjoy the webinar.
 Disclaimer This webinar may be recorded. This webinar presents a sampling of best practices and overviews, generalities, and some laws. This should not be used as legal advice. Itentive recognizes that
Disclaimer This webinar may be recorded. This webinar presents a sampling of best practices and overviews, generalities, and some laws. This should not be used as legal advice. Itentive recognizes that
Key Financial and Operational Impacts from the Proposed Rule to Implement MACRA:
 Key Financial and Operational Impacts from the Proposed Rule to Implement MACRA: The proposed rule implementing Access and CHIP Reauthorization Act of 2015 (MACRA) was made available on May 9, 2016. A
Key Financial and Operational Impacts from the Proposed Rule to Implement MACRA: The proposed rule implementing Access and CHIP Reauthorization Act of 2015 (MACRA) was made available on May 9, 2016. A
MACRA Final Rule Summary
 MACRA Final Rule Summary On October 14, 2016, the Centers for Medicare and Medicaid Services (CMS) released its final rule implementing the Medicare Access and CHIP Reauthorization Act of 2015 (MACRA),
MACRA Final Rule Summary On October 14, 2016, the Centers for Medicare and Medicaid Services (CMS) released its final rule implementing the Medicare Access and CHIP Reauthorization Act of 2015 (MACRA),
AMGA MIPS Collaborative. June 21, 2017
 AMGA MIPS Collaborative June 21, 2017 Calculating the MIPS score The MIPS composite performance score will include four weighted categories: MIPS Composite Performance Score Quality Cost Improvement activities
AMGA MIPS Collaborative June 21, 2017 Calculating the MIPS score The MIPS composite performance score will include four weighted categories: MIPS Composite Performance Score Quality Cost Improvement activities
FACT SHEET. November 1, *See the HIMSS ACO Final Rule Executive Summary for more details on the One-Sided and Two-Sided Payment Models
 FACT SHEET Quality Reporting and Performance Improvement Requirements For Accountable Organizations Participating in the Medicare Shared Savings Program Background November 1, 2011 Section 3022 of the
FACT SHEET Quality Reporting and Performance Improvement Requirements For Accountable Organizations Participating in the Medicare Shared Savings Program Background November 1, 2011 Section 3022 of the
AMERICAN COLLEGE OF GASTROENTEROLOGY MAKING $ENSE OF MACRA
 AMERICAN COLLEGE OF GASTROENTEROLOGY 6400 Goldsboro Road, Suite 200, Bethesda, Maryland 20817-5842; P: 301-263-9000; F: 301-263-9025 MAKING $ENSE OF MACRA CMS.SGR MACRA MIPS APMs QCDRs ACOs Why does Washington
AMERICAN COLLEGE OF GASTROENTEROLOGY 6400 Goldsboro Road, Suite 200, Bethesda, Maryland 20817-5842; P: 301-263-9000; F: 301-263-9025 MAKING $ENSE OF MACRA CMS.SGR MACRA MIPS APMs QCDRs ACOs Why does Washington
2018 Quality Measure Benchmarks Overview
 2018 Quality Benchmarks Overview What Are Quality Benchmarks? When a clinician or group submits measures for the Merit-based Incentive Payment System (MIPS) quality performance category, each measure is
2018 Quality Benchmarks Overview What Are Quality Benchmarks? When a clinician or group submits measures for the Merit-based Incentive Payment System (MIPS) quality performance category, each measure is
Copyright Scottsdale Institute All Rights Reserved.
 Copyright Scottsdale Institute 2017. All Rights Reserved. No part of this document may be reproduced or shared with anyone outside of your organization without prior written consent from the author(s).
Copyright Scottsdale Institute 2017. All Rights Reserved. No part of this document may be reproduced or shared with anyone outside of your organization without prior written consent from the author(s).
MACRA: THE FINAL RULE. Last updated 12/13/16
 MACRA: THE FINAL RULE Last updated 12/13/16 1 Background April 2015 MACRA (Medicare Access & CHIP Reauthorization Act) is signed into law to repeal the sustainable growth rate (SGR) which drastically cut
MACRA: THE FINAL RULE Last updated 12/13/16 1 Background April 2015 MACRA (Medicare Access & CHIP Reauthorization Act) is signed into law to repeal the sustainable growth rate (SGR) which drastically cut
QUALITY PAYMENT PROGRAM YEAR 3 (2019) FINAL RULE OVERVIEW NOVEMBER 15, 2018
 FINAL RULE OVERVIEW NOVEMBER 15, 2018") QUALITY PAYMENT PROGRAM YEAR 3 (2019) FINAL RULE OVERVIEW NOVEMBER 15, 2018 Disclaimers This presentation was prepared as a tool to assist providers and is not intended to grant rights or impose obligations.
QUALITY PAYMENT PROGRAM YEAR 3 (2019) FINAL RULE OVERVIEW NOVEMBER 15, 2018 Disclaimers This presentation was prepared as a tool to assist providers and is not intended to grant rights or impose obligations.
CMS PROPOSES KEY PROVISIONS OF MACRA PHYSICIAN PAYMENT SYSTEM FOR 2019
 Thursday, April 28, 2016 CMS PROPOSES KEY PROVISIONS OF MACRA PHYSICIAN PAYMENT SYSTEM FOR 2019 The Centers for Medicare & Medicaid Services (CMS) late yesterday issued a proposed rule implementing key
Thursday, April 28, 2016 CMS PROPOSES KEY PROVISIONS OF MACRA PHYSICIAN PAYMENT SYSTEM FOR 2019 The Centers for Medicare & Medicaid Services (CMS) late yesterday issued a proposed rule implementing key
MACRA: APPLICATIONS & IMPLICATIONS September 13, /13/2016. Mark Blessing, CPA, FHFMA Partner
 MACRA: APPLICATIONS & IMPLICATIONS September 13, 2016 Mark Blessing, CPA, FHFMA Partner mblessing@bkd.com Zach Remmich Managing Consultant zremmich@bkd.com 1 TO RECEIVE CPE CREDIT Participate in entire
MACRA: APPLICATIONS & IMPLICATIONS September 13, 2016 Mark Blessing, CPA, FHFMA Partner mblessing@bkd.com Zach Remmich Managing Consultant zremmich@bkd.com 1 TO RECEIVE CPE CREDIT Participate in entire
A Practical Discussion of Value and Quality Based Payments What Do I Do Now?
 Emerging Challenges in Primary Care: 2016 A Practical Discussion of Value and Quality Based Payments What Do I Do Now? Modified from AHLA Physicians and Hospitals Law Institute 2016 Faculty Ellie Bane
Emerging Challenges in Primary Care: 2016 A Practical Discussion of Value and Quality Based Payments What Do I Do Now? Modified from AHLA Physicians and Hospitals Law Institute 2016 Faculty Ellie Bane
2018 Quality Payment Program (QPP) Measure Specification and Measure Flow Guide for Registry Submission of Individual Measures
 Measure Specification and Measure Flow Guide for Registry Submission of Individual Measures") 2018 Quality Payment Program (QPP) Measure Specification and Measure Flow Guide for Registry Submission of Individual Measures Utilized by Individual Eligible Clinicians for Registry Submissions or Clinical
2018 Quality Payment Program (QPP) Measure Specification and Measure Flow Guide for Registry Submission of Individual Measures Utilized by Individual Eligible Clinicians for Registry Submissions or Clinical
The MACRA Proposed Rule on MIPS and APMs: Summary and Key Takeaways
 The MACRA Proposed Rule on MIPS and APMs: Summary and Key Takeaways A White Paper May 2016 Impact Advisors LLC 400 E. Diehl Road Suite 190 Naperville IL 60563 1-800- 680-7570 Impact- Advisors.com Executive
The MACRA Proposed Rule on MIPS and APMs: Summary and Key Takeaways A White Paper May 2016 Impact Advisors LLC 400 E. Diehl Road Suite 190 Naperville IL 60563 1-800- 680-7570 Impact- Advisors.com Executive
AMERICAN COLLEGE OF GASTROENTEROLOGY MAKING $ENSE OF MACRA
 AMERICAN COLLEGE OF GASTROENTEROLOGY 6400 Goldsboro Road, Suite 200, Bethesda, Maryland 20817-5842; P: 301-263-9000; F: 301-263-9025 MAKING $ENSE OF MACRA CMS.SGR MACRA MIPS APMs QCDRs ACOs Why does Washington
AMERICAN COLLEGE OF GASTROENTEROLOGY 6400 Goldsboro Road, Suite 200, Bethesda, Maryland 20817-5842; P: 301-263-9000; F: 301-263-9025 MAKING $ENSE OF MACRA CMS.SGR MACRA MIPS APMs QCDRs ACOs Why does Washington
MACRA, MIPS, APMs & CPC+: What to Expect from All These Acronyms?! Monthly National Briefing April 26, 2016
 MACRA, MIPS, APMs & CPC+: What to Expect from All These Acronyms?! Monthly National Briefing April 26, 2016 1 Shari Erickson, MPH Vice President, Governmental Affairs & Medical Practice American College
MACRA, MIPS, APMs & CPC+: What to Expect from All These Acronyms?! Monthly National Briefing April 26, 2016 1 Shari Erickson, MPH Vice President, Governmental Affairs & Medical Practice American College
2015 ANNUAL QUALITY AND RESOURCE USE REPORT
 Download Your Report to: --> PDF 508 Compliance CSV 2015 ANNUAL QUALITY AND RESOURCE USE REPORT AND THE 2017 VALUE-BASED PAYMENT MODIFIER SOUTHEAST TEXAS MEDICAL ASSOCIATES LLP LAST FOUR DIGITS OF YOUR
Download Your Report to: --> PDF 508 Compliance CSV 2015 ANNUAL QUALITY AND RESOURCE USE REPORT AND THE 2017 VALUE-BASED PAYMENT MODIFIER SOUTHEAST TEXAS MEDICAL ASSOCIATES LLP LAST FOUR DIGITS OF YOUR
CY 2014 Physician Quality Reporting System (PQRS)
") CY 2014 Physician Quality Reporting System (PQRS) 101 Table of Contents Step 1: Understand PQRS and how it impacts you A. When was PQRS first established and implemented? B. What is PQRS? C. How does CMS
CY 2014 Physician Quality Reporting System (PQRS) 101 Table of Contents Step 1: Understand PQRS and how it impacts you A. When was PQRS first established and implemented? B. What is PQRS? C. How does CMS
MEDICARE ACCESS AND CHIP REAUTHORIZATION ACT (MACRA) MERIT-BASED INCENTIVE PAYMENT SYSTEM (MIPS) REVIEW
 MERIT-BASED INCENTIVE PAYMENT SYSTEM (MIPS) REVIEW") MEDICARE ACCESS AND CHIP REAUTHORIZATION ACT (MACRA) MERIT-BASED INCENTIVE PAYMENT SYSTEM (MIPS) REVIEW I. MIPS Overview 1) Medicare Access and CHIP Reauthorization Act of 2015 (MACRA) i) Signed into Law
MEDICARE ACCESS AND CHIP REAUTHORIZATION ACT (MACRA) MERIT-BASED INCENTIVE PAYMENT SYSTEM (MIPS) REVIEW I. MIPS Overview 1) Medicare Access and CHIP Reauthorization Act of 2015 (MACRA) i) Signed into Law
The Future Of Medicare Physician Reimbursement
 Portfolio Media. Inc. 111 West 19 th Street, 5th Floor New York, NY 10011 www.law360.com Phone: +1 646 783 7100 Fax: +1 646 783 7161 customerservice@law360.com The Future Of Medicare Physician Reimbursement
Portfolio Media. Inc. 111 West 19 th Street, 5th Floor New York, NY 10011 www.law360.com Phone: +1 646 783 7100 Fax: +1 646 783 7161 customerservice@law360.com The Future Of Medicare Physician Reimbursement
MACRA: Redefining How CMS Pays Doctors. White Paper ELLIS MAC KNIGHT, MD DAN KIEHL, JD CONTACT. Senior Vice President/CMO. Associate Consultant
 MACRA: Redefining How CMS Pays Doctors White Paper ELLIS MAC KNIGHT, MD Senior Vice President/CMO DAN KIEHL, JD Associate Consultant June 2016 CONTACT For further information about Coker Group and how
MACRA: Redefining How CMS Pays Doctors White Paper ELLIS MAC KNIGHT, MD Senior Vice President/CMO DAN KIEHL, JD Associate Consultant June 2016 CONTACT For further information about Coker Group and how
Get Straight on MACRA in 2018
 Quality Reporting Roundtable Get Straight on MACRA in 2018 FAQs, Advisory Board Guidance, and Resources Ye Hoffman, MS, CPHIMS Consultant March 27, 2018 research technology consulting 2 Manage Your Audio
Quality Reporting Roundtable Get Straight on MACRA in 2018 FAQs, Advisory Board Guidance, and Resources Ye Hoffman, MS, CPHIMS Consultant March 27, 2018 research technology consulting 2 Manage Your Audio
Scripps Health ACO Update
 June 2016 Scripps Health ACO Update Marc Reynolds Senior Vice President, Payer Relations Scripps Health Anil N. Keswani, MD Corporate Vice President, Population Health Management Scripps Health 10 Key
June 2016 Scripps Health ACO Update Marc Reynolds Senior Vice President, Payer Relations Scripps Health Anil N. Keswani, MD Corporate Vice President, Population Health Management Scripps Health 10 Key
2019 Quality Payment Program (QPP) Measure Specification and Measure Flow Guide for MIPS Clinical Quality Measures (CQMs)
 Measure Specification and Measure Flow Guide for MIPS Clinical Quality Measures (CQMs)") 2019 Quality Payment Program (QPP) Measure Specification and Measure Flow Guide for MIPS Clinical Quality Measures (CQMs) Utilized by Merit-based Incentive Payment System (MIPS) Eligible Clinicians, Groups,
2019 Quality Payment Program (QPP) Measure Specification and Measure Flow Guide for MIPS Clinical Quality Measures (CQMs) Utilized by Merit-based Incentive Payment System (MIPS) Eligible Clinicians, Groups,
What You Need to Know About CMS Quality and Resource Use Report
 What You Need to Know About CMS Quality and Resource Use Report Heidy Robertson-Cooper, MPA Maryland Family Medicine Summit June 24, 2016 Learning Objectives Describe the purpose of CMS Quality Resource
What You Need to Know About CMS Quality and Resource Use Report Heidy Robertson-Cooper, MPA Maryland Family Medicine Summit June 24, 2016 Learning Objectives Describe the purpose of CMS Quality Resource
Proposed 2018 Medicare Physician Payment and Quality Reporting Changes. Executive s Insights
 Proposed 2018 Medicare Physician Payment and Quality Reporting Changes MGMA MEMBER-EXCLUSIVE ANALYSIS The Centers for Medicare & Medicaid Services (CMS) recently proposed changes to both Medicare physician
Proposed 2018 Medicare Physician Payment and Quality Reporting Changes MGMA MEMBER-EXCLUSIVE ANALYSIS The Centers for Medicare & Medicaid Services (CMS) recently proposed changes to both Medicare physician
QUALITY PAYMENT PROGRAM YEAR 3 (2019) FINAL RULE OVERVIEW
 FINAL RULE OVERVIEW") QUALITY PAYMENT PROGRAM YEAR 3 (2019) FINAL RULE OVERVIEW NEAL LOGUE, HEALTH INSURANCE SPECIALIST, DIVISION OF FINANCIAL MANAGEMENT & FEE FOR SERVICE OPERATIONS DECEMBER 12, 2018 Disclaimers This presentation
QUALITY PAYMENT PROGRAM YEAR 3 (2019) FINAL RULE OVERVIEW NEAL LOGUE, HEALTH INSURANCE SPECIALIST, DIVISION OF FINANCIAL MANAGEMENT & FEE FOR SERVICE OPERATIONS DECEMBER 12, 2018 Disclaimers This presentation
September 6, Re: CMS-1600-P; CY 2014 Physician Fee Schedule Proposed rule comments
 September 6, 2013 Centers for Medicare & Medicaid Services Department of Health and Human Services Attention CMS-1600-P Mail Stop C4-26-05 7500 Security Boulevard Baltimore, MD 21244-1850 Re: CMS-1600-P;
September 6, 2013 Centers for Medicare & Medicaid Services Department of Health and Human Services Attention CMS-1600-P Mail Stop C4-26-05 7500 Security Boulevard Baltimore, MD 21244-1850 Re: CMS-1600-P;
You Down with QPP? Daniel Collins Director of Finance Orlando Health Physician Enterprise
 You Down with QPP? Daniel Collins Director of Finance Orlando Health Physician Enterprise Why Was the QPP created? Source: https://www.youtube.com/watch?v=7df7chghas4 What is QPP? Quality Payment Program
You Down with QPP? Daniel Collins Director of Finance Orlando Health Physician Enterprise Why Was the QPP created? Source: https://www.youtube.com/watch?v=7df7chghas4 What is QPP? Quality Payment Program
The Physician Value-Based Payment Modifier under the 2014 Medicare Physician Fee Schedule. December 3, 2013
 The Physician Value-Based Payment Modifier under the 2014 Medicare Physician Fee Schedule December 3, 2013 Medicare Learning Network This MLN Connects National Provider Call (MLN Connects Call) is part
The Physician Value-Based Payment Modifier under the 2014 Medicare Physician Fee Schedule December 3, 2013 Medicare Learning Network This MLN Connects National Provider Call (MLN Connects Call) is part
MACRA: Alternative Payment Models Proposed Rule CY 2016
 powered by Vizient & AAMC MACRA: Alternative Payment Models Proposed Rule CY 2016 June 2, 2016 Page 1 Housekeeping When you called in, did you enter your attendee ID number? Dial-in number: 1-866-469-3239
powered by Vizient & AAMC MACRA: Alternative Payment Models Proposed Rule CY 2016 June 2, 2016 Page 1 Housekeeping When you called in, did you enter your attendee ID number? Dial-in number: 1-866-469-3239
Topics to be covered. Do I have to participate in MACRA/MIPS/QPP? Choices for participation. Timelines. What is changing with QPP
 Topics to be covered Do I have to participate in MACRA/MIPS/QPP? Choices for participation Timelines What is changing with QPP I have no relevant financial relationships to disclose. Participant engagement
Topics to be covered Do I have to participate in MACRA/MIPS/QPP? Choices for participation Timelines What is changing with QPP I have no relevant financial relationships to disclose. Participant engagement
PQRS and erx Incentive Program Updates. Julie Orton Van, CPC, CPC-P, CEMC 2013 AAPC Regional Conference Orlando, FL
 PQRS and erx Incentive Program Updates Julie Orton Van, CPC, CPC-P, CEMC 2013 AAPC Regional Conference Orlando, FL The information in this presentation was current at the time it was created. Medicare
PQRS and erx Incentive Program Updates Julie Orton Van, CPC, CPC-P, CEMC 2013 AAPC Regional Conference Orlando, FL The information in this presentation was current at the time it was created. Medicare
MACRA Overview. April 2016
 MACRA Overview April 2016 CMS is Focused on Progression from Volume-Based to Value-Based Payments Hospitals have some value-based payment via Hospital VBP, readmissions, and HAC programs Other provider
MACRA Overview April 2016 CMS is Focused on Progression from Volume-Based to Value-Based Payments Hospitals have some value-based payment via Hospital VBP, readmissions, and HAC programs Other provider
On Track for MACRA The Provider s Guide to QPP
 On Track for MACRA The Provider s Guide to QPP Bizmatics, Inc. 4010 Moorpark Avenue, Suite 222 San Jose, CA 95117 www.prognocis.com training@bizmaticsinc.com Copyright 2017 Bizmatics, Inc. Overview CMS
On Track for MACRA The Provider s Guide to QPP Bizmatics, Inc. 4010 Moorpark Avenue, Suite 222 San Jose, CA 95117 www.prognocis.com training@bizmaticsinc.com Copyright 2017 Bizmatics, Inc. Overview CMS
Quality Payment Program Year 3
 Quality Payment Program Year 3 Final Rule Overview The Medicare Access and CHIP Reauthorization Act of 2015 (MACRA) ended the Sustainable Growth Rate (SGR) formula for clinician payment, and established
Quality Payment Program Year 3 Final Rule Overview The Medicare Access and CHIP Reauthorization Act of 2015 (MACRA) ended the Sustainable Growth Rate (SGR) formula for clinician payment, and established
Medicare Access and CHIP Reauthorization Act of 2015 (HR. 2; MACRA)
") Fact Sheet April 23, 2015 H.R.2 - Medicare Access and CHIP Reauthorization Act of 2015 (MACRA) Background. The Medicare Sustainable Growth Rate formula (SGR), passed by Congress in 1997, was intended to
Fact Sheet April 23, 2015 H.R.2 - Medicare Access and CHIP Reauthorization Act of 2015 (MACRA) Background. The Medicare Sustainable Growth Rate formula (SGR), passed by Congress in 1997, was intended to
MACRA Update: The Top 8 For Amy Mullins, MD, CPE, FAAFP Medical Director, Quality Improvement AAFP
 MACRA Update: The Top 8 For 2018 Amy Mullins, MD, CPE, FAAFP Medical Director, Quality Improvement AAFP Disclosure Statement It is the policy of the AAFP that all individuals in a position to control content
MACRA Update: The Top 8 For 2018 Amy Mullins, MD, CPE, FAAFP Medical Director, Quality Improvement AAFP Disclosure Statement It is the policy of the AAFP that all individuals in a position to control content
All About APMs: What Will It Take for Physicians to Earn the APM Bonus Under MACRA?
 All About APMs: What Will It Take for Physicians to Earn the APM Bonus Under MACRA? By Robert F. Atlas, David B. Tatge, and Lesley R. Yeung June 2016 On May 9, 2016, the Centers for Medicare & Medicaid
All About APMs: What Will It Take for Physicians to Earn the APM Bonus Under MACRA? By Robert F. Atlas, David B. Tatge, and Lesley R. Yeung June 2016 On May 9, 2016, the Centers for Medicare & Medicaid
HEALTH ECONOMICS AND REIMBURSEMENT
 HEALTH ECONOMICS AND REIMBURSEMENT VASCULAR CY 2016 MEDICARE PHYSICIAN FEE SCHEDULE (PFS) UPDATE Abbott Vascular is pleased to provide you with this summary of the Medicare Physician Fee Schedule (PFS)
HEALTH ECONOMICS AND REIMBURSEMENT VASCULAR CY 2016 MEDICARE PHYSICIAN FEE SCHEDULE (PFS) UPDATE Abbott Vascular is pleased to provide you with this summary of the Medicare Physician Fee Schedule (PFS)
Growth and Success of Accountable Care Organizations (ACOs) in the US from Dennis Horrigan June 2016
 in the US from Dennis Horrigan June 2016") Growth and Success of Accountable Care Organizations (ACOs) in the US from 2010-2016 Dennis Horrigan June 2016 Introducing Dennis Horrigan Dennis R. Horrigan President and Chief Executive Officer Catholic
Growth and Success of Accountable Care Organizations (ACOs) in the US from 2010-2016 Dennis Horrigan June 2016 Introducing Dennis Horrigan Dennis R. Horrigan President and Chief Executive Officer Catholic
CMS Proposals for Quality Reporting Programs Under the 2015 Medicare Physician Fee Schedule Proposed Rule
 CMS Proposals for Quality Reporting Programs Under the 2015 Medicare Physician Fee Schedule Proposed Rule PQRS, EHR Incentive Program, Physician Compare, and VBM Kate Goodrich, M.D., M.H.S. Director, Quality
CMS Proposals for Quality Reporting Programs Under the 2015 Medicare Physician Fee Schedule Proposed Rule PQRS, EHR Incentive Program, Physician Compare, and VBM Kate Goodrich, M.D., M.H.S. Director, Quality
ACOs/Shared Savings Demonstration Project: What Does It All Mean?
 ACOs/Shared Savings Demonstration Project: What Does It All Mean? None Conflicts of Interest Sean P. Roddy, MD Albany, NY Accountable Care Organizations Term introduced in 2006 by Fisher et al. the hospital
ACOs/Shared Savings Demonstration Project: What Does It All Mean? None Conflicts of Interest Sean P. Roddy, MD Albany, NY Accountable Care Organizations Term introduced in 2006 by Fisher et al. the hospital
MACRA Medicare Payment Reform and the Implications to Medicare Advantage Plans
 BEYOND THE NUMBERS MACRA Medicare Payment Reform and the Implications to Medicare Advantage Plans True BUSINESS PowerPoint Presentation Template November 2018 PRESENTED BY Bob Moné, FSA, MAAA Liz Myers,
BEYOND THE NUMBERS MACRA Medicare Payment Reform and the Implications to Medicare Advantage Plans True BUSINESS PowerPoint Presentation Template November 2018 PRESENTED BY Bob Moné, FSA, MAAA Liz Myers,
Health Care Policy Landscape: Market Trends & Frontline Perspectives
 Health Care Policy Landscape: Market Trends & Frontline Perspectives December 1, 2016 www.leavittpartners.com Post-Election, New Administration Insights Top 10 Health Policy Actions to Watch 1 2 3 4 Substantial
Health Care Policy Landscape: Market Trends & Frontline Perspectives December 1, 2016 www.leavittpartners.com Post-Election, New Administration Insights Top 10 Health Policy Actions to Watch 1 2 3 4 Substantial
Summary of the Quality Payment Program (QPP) Year 2 Final Rule
 Year 2 Final Rule") November 8, 2017 Summary of the Quality Payment Program (QPP) Year 2 Final Rule Medicare Program; CY 2018 Updates to the Quality Payment Program; and Quality Payment Program: Extreme and Uncontrollable
November 8, 2017 Summary of the Quality Payment Program (QPP) Year 2 Final Rule Medicare Program; CY 2018 Updates to the Quality Payment Program; and Quality Payment Program: Extreme and Uncontrollable
9/23/2016. Our Services. Transitioning from Fee-for-Service to Value-based Reimbursement. Key Trends and Strategies for Rural Health Providers
 Transitioning from Fee-for-Service to Value-based Reimbursement Key Trends and Strategies for Rural Health Providers Paul MacLellan, CEO >> Health care consulting company >> Wholly owned subsidiary of
Transitioning from Fee-for-Service to Value-based Reimbursement Key Trends and Strategies for Rural Health Providers Paul MacLellan, CEO >> Health care consulting company >> Wholly owned subsidiary of
Washington Update. Suzanne Falk, MPP Associate Director, Government Affairs
 Washington Update Suzanne Falk, MPP Associate Director, Government Affairs sfalk@mgma.org Agenda 2017 Medicare Physician Fee Schedule Highlights Miscellaneous Updates 2016 Quality Reporting Wrap-Up Quality
Washington Update Suzanne Falk, MPP Associate Director, Government Affairs sfalk@mgma.org Agenda 2017 Medicare Physician Fee Schedule Highlights Miscellaneous Updates 2016 Quality Reporting Wrap-Up Quality
MACRA: How the 2018 Quality Payment Program Final Rule Impacts Providers
 Medical Group Strategy Council MACRA: How the 2018 Quality Payment Program Final Rule Impacts Providers Rob Lazerow Managing Director Tony Panjamapirom Senior Consultant Hamza Hasan Practice Manager Julie
Medical Group Strategy Council MACRA: How the 2018 Quality Payment Program Final Rule Impacts Providers Rob Lazerow Managing Director Tony Panjamapirom Senior Consultant Hamza Hasan Practice Manager Julie
Final Policy, Payment, and Quality Provisions in the Medicare Physician Fee Schedule for Calendar Year 2018
 Final Policy, Payment, and Quality Provisions in the Medicare Physician Fee Schedule for Calendar Year 2018 Date 2017-11-02 Title Contact Final Policy, Payment, and Quality Provisions in the Medicare Physician
Final Policy, Payment, and Quality Provisions in the Medicare Physician Fee Schedule for Calendar Year 2018 Date 2017-11-02 Title Contact Final Policy, Payment, and Quality Provisions in the Medicare Physician
Aligning PQRS and Meaningful Use. Maximize your Medicare Reimbursement
 Aligning PQRS and Meaningful Use Maximize your Medicare Reimbursement INTRODUCTION Brux McClellan, MPH, MHA Project Coordinator, HealthInsight Payment Adjustments Incentive $$ & Payment Adjustments Value
Aligning PQRS and Meaningful Use Maximize your Medicare Reimbursement INTRODUCTION Brux McClellan, MPH, MHA Project Coordinator, HealthInsight Payment Adjustments Incentive $$ & Payment Adjustments Value
HOW TO UNDERSTAND YOUR QUALITY AND RESOURCE USE REPORT (QRUR)
") HOW TO UNDERSTAND YOUR QUALITY AND RESOURCE USE REPORT (QRUR) Kaitlin Nolte Kansas Foundation for Medical Care, Inc. QI Project Manager Kaitlin.nolte@area-A.hcqis.org greatplainsqin.org 785-273-2552 ext.
HOW TO UNDERSTAND YOUR QUALITY AND RESOURCE USE REPORT (QRUR) Kaitlin Nolte Kansas Foundation for Medical Care, Inc. QI Project Manager Kaitlin.nolte@area-A.hcqis.org greatplainsqin.org 785-273-2552 ext.
9/7/17. MACRA: The Knowns and the Unknowns. Disclosures. Goals and Objectives
 MACRA: The Knowns and the Unknowns Sharon K. Merrick, M.S., CCS-P Director of Payment and Practice Management American Society of Anesthesiologists Wisconsin Society of Anesthesiologists September 10,
MACRA: The Knowns and the Unknowns Sharon K. Merrick, M.S., CCS-P Director of Payment and Practice Management American Society of Anesthesiologists Wisconsin Society of Anesthesiologists September 10,
Federal Update Issues Impacting Rheumatologists and their Patients. Emily L. Graham, RHIA, CCS-P VP, Regulatory Affairs Hart Health Strategies, Inc.
 Federal Update Issues Impacting Rheumatologists and their Patients Emily L. Graham, RHIA, CCS-P VP, Regulatory Affairs Hart Health Strategies, Inc. Just a spoon full of DC? Agenda MACRA & Rheumatology
Federal Update Issues Impacting Rheumatologists and their Patients Emily L. Graham, RHIA, CCS-P VP, Regulatory Affairs Hart Health Strategies, Inc. Just a spoon full of DC? Agenda MACRA & Rheumatology
Volume to Value The Great Transformation of American Medicine
 Volume to Value The Great Transformation of American Medicine 2010-2020 Richard I. Fogel, MD FHRS Chief Clinical Officer St. Vincent Health October 2015 Fee for Service You get paid for what you do The
Volume to Value The Great Transformation of American Medicine 2010-2020 Richard I. Fogel, MD FHRS Chief Clinical Officer St. Vincent Health October 2015 Fee for Service You get paid for what you do The
2013 Medicare Physician Fee Schedule Proposed Rule Summary
 2013 Medicare Physician Fee Schedule Proposed Rule Summary On July 6, 2012, CMS issued the 2013 Medicare physician fee schedule (PFS) proposed rule, which was published in the Federal Register on July
2013 Medicare Physician Fee Schedule Proposed Rule Summary On July 6, 2012, CMS issued the 2013 Medicare physician fee schedule (PFS) proposed rule, which was published in the Federal Register on July
Health Industry Forum Key Policy Issues in the Evolution of Medicare ACO Programs
 Health Industry Forum Key Policy Issues in the Evolution of Medicare ACO Programs June 3, 2014 7 ACO Policy Issues 1. Assignment 2. Financial Benchmarks 3. Minimum Savings Rate 4. Pathway to Higher Risk
Health Industry Forum Key Policy Issues in the Evolution of Medicare ACO Programs June 3, 2014 7 ACO Policy Issues 1. Assignment 2. Financial Benchmarks 3. Minimum Savings Rate 4. Pathway to Higher Risk
Current Status Of Legislation on Quality Bench Marks
 Conflicts of Interest Current Status Of Legislation on Quality Bench Marks None Sean P. Roddy, MD Albany, NY Reason For Quality Measures Progressive increase in healthcare costs under the fee-for-service
Conflicts of Interest Current Status Of Legislation on Quality Bench Marks None Sean P. Roddy, MD Albany, NY Reason For Quality Measures Progressive increase in healthcare costs under the fee-for-service
DEPARTMENT OF HEALTH AND HUMAN SERVICES & 42 CFR 414 [CMS-5522-FC
 Executive Summary DEPARTMENT OF HEALTH AND HUMAN SERVICES Centers for Medicare & Medicaid Services 42 CFR Part 414 [CMS-5522-FC and IFC] RIN 0938-AT13 Medicare Program; CY 2018 Updates to the Quality Payment
Executive Summary DEPARTMENT OF HEALTH AND HUMAN SERVICES Centers for Medicare & Medicaid Services 42 CFR Part 414 [CMS-5522-FC and IFC] RIN 0938-AT13 Medicare Program; CY 2018 Updates to the Quality Payment
August 21, Ms. Seema Verma Administrator Centers for Medicare and Medicaid Services 7500 Security Boulevard Baltimore, Maryland
 August 21, 2016 Ms. Seema Verma Administrator Centers for Medicare and Medicaid Services 7500 Security Boulevard Baltimore, Maryland 21244-1850 Dear Ms. Verma: On behalf of AMGA, we appreciate the opportunity
August 21, 2016 Ms. Seema Verma Administrator Centers for Medicare and Medicaid Services 7500 Security Boulevard Baltimore, Maryland 21244-1850 Dear Ms. Verma: On behalf of AMGA, we appreciate the opportunity
NAACOS Analysis Shows ACOs In Top MIPS Performance Tier
 NAACOS Analysis Shows ACOs In Top MIPS Performance Tier The National Association of Accountable Care Organizations (NAACOS) is sharing results of its analysis of ACO performance in the Quality Payment
NAACOS Analysis Shows ACOs In Top MIPS Performance Tier The National Association of Accountable Care Organizations (NAACOS) is sharing results of its analysis of ACO performance in the Quality Payment
MACRA and the Evolving Health Care Landscape. Jarrod Fowler, M.H.A. FMA Director of Health Care Policy and Innovation
 MACRA and the Evolving Health Care Landscape Jarrod Fowler, M.H.A. FMA Director of Health Care Policy and Innovation MACRA The Medicare Access and CHIP Reauthorization Act of 2015 (MACRA) Passed Congress
MACRA and the Evolving Health Care Landscape Jarrod Fowler, M.H.A. FMA Director of Health Care Policy and Innovation MACRA The Medicare Access and CHIP Reauthorization Act of 2015 (MACRA) Passed Congress
New Medicare Merit-Based Incentive Payment System: Navigating Changes Under MACRA
 Presenting a live 90-minute webinar with interactive Q&A New Medicare Merit-Based Incentive Payment System: Navigating Changes Under MACRA Overcoming Challenges in Transforming Payment and Care Delivery
Presenting a live 90-minute webinar with interactive Q&A New Medicare Merit-Based Incentive Payment System: Navigating Changes Under MACRA Overcoming Challenges in Transforming Payment and Care Delivery
Health IT Public Policy Update
 Health IT Public Policy Update January 21, 2016 Tom Leary HIMSS Vice President Government Relations HHS Set Firm Goals for the Move to Value-Based Care Health Information Technology for Economic and Clinical
Health IT Public Policy Update January 21, 2016 Tom Leary HIMSS Vice President Government Relations HHS Set Firm Goals for the Move to Value-Based Care Health Information Technology for Economic and Clinical
Predictive Qualifying Alternative Payment Model (APM) Participants (QPs) Methodology Fact Sheet What is the Predictive QP Status Analysis?
 Participants (QPs) Methodology Fact Sheet What is the Predictive QP Status Analysis?") Predictive Qualifying Alternative Payment Model (APM) Participants (QPs) Methodology Fact Sheet What is the Predictive QP Status Analysis? One of the Quality Payment Program s goals is to be clear about
Predictive Qualifying Alternative Payment Model (APM) Participants (QPs) Methodology Fact Sheet What is the Predictive QP Status Analysis? One of the Quality Payment Program s goals is to be clear about
Update on Medicare s Physician Incentive Programs
 Physician Practice Roundtable Update on Medicare s Physician Incentive Programs An Overview of the Physician Quality Reporting System (PQRS), Value-Based Payment Modifier (VBPM), and Electronic Prescribing
Physician Practice Roundtable Update on Medicare s Physician Incentive Programs An Overview of the Physician Quality Reporting System (PQRS), Value-Based Payment Modifier (VBPM), and Electronic Prescribing
Washington Update. Suzanne Falk, MPP Associate Director, Government Affairs
 Washington Update Suzanne Falk, MPP Associate Director, Government Affairs sfalk@mgma.org Agenda 2017 Medicare Physician Fee Schedule Changes Miscellaneous Updates 2016 Quality Reporting Wrap-Up MACRA
Washington Update Suzanne Falk, MPP Associate Director, Government Affairs sfalk@mgma.org Agenda 2017 Medicare Physician Fee Schedule Changes Miscellaneous Updates 2016 Quality Reporting Wrap-Up MACRA
2018 Final Rule from CMS for the Quality Payment Program
 2018 Final Rule from CMS for the Quality Payment Program Starting at Noon EST Wed 12/6/2017 Dr. Dan Mingle Register for Webinars or Access Recordings http://mingleanalytics.com/webinars 2017 Mingle Analytics
2018 Final Rule from CMS for the Quality Payment Program Starting at Noon EST Wed 12/6/2017 Dr. Dan Mingle Register for Webinars or Access Recordings http://mingleanalytics.com/webinars 2017 Mingle Analytics
Current State of Medicare. Robert Roth & John Hellow Hooper, Lundy & Bookman, PC
 Current State of Medicare Robert Roth & John Hellow Hooper, Lundy & Bookman, PC Rule for FY 2016 A. FY 2017 Final Rule Released Aug. 2, 2016 (printed in Federal Register Aug. 22, 2016) B. FY 2018 Proposed
Current State of Medicare Robert Roth & John Hellow Hooper, Lundy & Bookman, PC Rule for FY 2016 A. FY 2017 Final Rule Released Aug. 2, 2016 (printed in Federal Register Aug. 22, 2016) B. FY 2018 Proposed
Current State of Medicare
 Current State of Medicare Robert Roth & John Hellow Hooper, Lundy & Bookman, PC Rule for FY 2016 A. FY 2017 Final Rule Released Aug. 2, 2016 (printed in Federal Register Aug. 22, 2016) B. FY 2018 Proposed
Current State of Medicare Robert Roth & John Hellow Hooper, Lundy & Bookman, PC Rule for FY 2016 A. FY 2017 Final Rule Released Aug. 2, 2016 (printed in Federal Register Aug. 22, 2016) B. FY 2018 Proposed
The Medicare Advantage program: Status report
 C H A P T E R12 The Medicare Advantage program: Status report C H A P T E R 12 The Medicare Advantage program: Status report Chapter summary In this chapter Each year the Commission provides a status
C H A P T E R12 The Medicare Advantage program: Status report C H A P T E R 12 The Medicare Advantage program: Status report Chapter summary In this chapter Each year the Commission provides a status
 SECTION II PATIENT CENTERED MEDICAL HOME (PCMH) CONTENTS 200.000 DEFINITIONS 210.000 ENROLLMENT AND CASELOAD MANAGEMENT 211.000 Enrollment Eligibility 212.000 Practice Enrollment 213.000 Enrollment Schedule
SECTION II PATIENT CENTERED MEDICAL HOME (PCMH) CONTENTS 200.000 DEFINITIONS 210.000 ENROLLMENT AND CASELOAD MANAGEMENT 211.000 Enrollment Eligibility 212.000 Practice Enrollment 213.000 Enrollment Schedule
2018 Merit-based Incentive Payment System (MIPS) Cost Performance Category Fact Sheet
 Cost Performance Category Fact Sheet") 2018 Merit-based Incentive Payment System (MIPS) Cost Performance Category Fact Sheet What is the Quality Payment Program? The Medicare Access and CHIP Reauthorization Act of 2015 (MACRA) ended the Sustainable
2018 Merit-based Incentive Payment System (MIPS) Cost Performance Category Fact Sheet What is the Quality Payment Program? The Medicare Access and CHIP Reauthorization Act of 2015 (MACRA) ended the Sustainable
2019 Quality Payment Program (QPP) Measure Specification and Measure Flow Guide for Medicare Part B Claims Measures
 Measure Specification and Measure Flow Guide for Medicare Part B Claims Measures") 2019 Quality Payment Program (QPP) Measure Specification and Measure Flow Guide for Medicare Part B Claims Measures Utilized by Merit-based Incentive Payment System (MIPS) Eligible Clinicians 11/20/2018
2019 Quality Payment Program (QPP) Measure Specification and Measure Flow Guide for Medicare Part B Claims Measures Utilized by Merit-based Incentive Payment System (MIPS) Eligible Clinicians 11/20/2018
Gulf Coast and LA HFMA Payer Summit Value-based contracts same healthcare business?
 Gulf Coast and LA HFMA Payer Summit Value-based contracts same healthcare business? Richard R. Vath, MD FMOLHS SVP/Chief Clinical Transformation Officer President Health Leaders Network and Medicare ACO
Gulf Coast and LA HFMA Payer Summit Value-based contracts same healthcare business? Richard R. Vath, MD FMOLHS SVP/Chief Clinical Transformation Officer President Health Leaders Network and Medicare ACO
Integrating Population Health Analytics and the EHR Environment Session 87, March 6, 2018
 Integrating Population Health Analytics and the EHR Environment Session 87, March 6, 2018 Nina M. Taggart, MD, Senior Medical Director, Population Health and Payer Relations, Lehigh Valley Health Network
Integrating Population Health Analytics and the EHR Environment Session 87, March 6, 2018 Nina M. Taggart, MD, Senior Medical Director, Population Health and Payer Relations, Lehigh Valley Health Network
2017 Proposed Rule MIPS Composite Performance Score Resource Use Performance Category
 Starting at Noon EDT 8/22/2016 2017 Proposed Rule MIPS Composite Performance Score Resource Use Performance Category Dr. Dan Mingle Register for Webinars or Access Recordings http://mingleanalytics.com/webinars
Starting at Noon EDT 8/22/2016 2017 Proposed Rule MIPS Composite Performance Score Resource Use Performance Category Dr. Dan Mingle Register for Webinars or Access Recordings http://mingleanalytics.com/webinars
Physician Compensation In Today s Changing Market
 Physician Compensation In Today s Changing Market PRESENTED BY: STEVE RICE, AREA PRESIDENT, INTEGRATED HEALTHCARE STRATEGIES STEVE MCCAMY, PRESIDENT AND CEO OF COVENANT MEDICAL GROUP NOVEMBER 9, 2016 Agenda
Physician Compensation In Today s Changing Market PRESENTED BY: STEVE RICE, AREA PRESIDENT, INTEGRATED HEALTHCARE STRATEGIES STEVE MCCAMY, PRESIDENT AND CEO OF COVENANT MEDICAL GROUP NOVEMBER 9, 2016 Agenda
Proposed ACO Rule: How Will It Affect Academic Medical Centers?
 Proposed ACO Rule: How Will It Affect Academic Medical Centers? This roundtable discussion is brought to you by the Teaching Hospitals and Academic Medical Centers Practice Group Wednesday, May 25, 2011
Proposed ACO Rule: How Will It Affect Academic Medical Centers? This roundtable discussion is brought to you by the Teaching Hospitals and Academic Medical Centers Practice Group Wednesday, May 25, 2011
RUPRI Center for Rural Health Policy Analysis. Rural Policy Brief. Brief No NOVEMBER
 RUPRI Center for www.banko Rural Health Policy Analysis Rural Policy Brief Brief No. 2018-6 NOVEMBER 2018 http://www.public-health.uiowa.edu/rupri/ Changes to the Merit-based Incentive Payment System Pertinent
RUPRI Center for www.banko Rural Health Policy Analysis Rural Policy Brief Brief No. 2018-6 NOVEMBER 2018 http://www.public-health.uiowa.edu/rupri/ Changes to the Merit-based Incentive Payment System Pertinent
2014 Physician Quality Reporting System: Group Reporting Requirements
 2014 Physician Quality Reporting System: Group Reporting Requirements Lisa Lentz, MPH, Health Insurance Specialist and LeTonya Smith, CRNP, Health Insurance Specialist Presentation to the American Medical
2014 Physician Quality Reporting System: Group Reporting Requirements Lisa Lentz, MPH, Health Insurance Specialist and LeTonya Smith, CRNP, Health Insurance Specialist Presentation to the American Medical
No change from proposed rule. healthcare providers and suppliers of services (e.g.,
 American College of Physicians Medicare Shared Savings/Accountable Care Organization (ACO) Final Rule Summary Analysis Category Final Rule Summary Change from Proposed Rule and Comments ACO refers to a
American College of Physicians Medicare Shared Savings/Accountable Care Organization (ACO) Final Rule Summary Analysis Category Final Rule Summary Change from Proposed Rule and Comments ACO refers to a
CY 2017 Proposed Physician Fee Schedule (CMS-1654-P) Summary of Key Provisions. July 15, 2016
 Summary of Key Provisions. July 15, 2016") CY 2017 Proposed Physician Fee Schedule (CMS-1654-P) Summary of Key Provisions July 15, 2016 The Centers for Medicare and Medicaid Services (CMS) on July 7 published a rule that updates the payment policies,
CY 2017 Proposed Physician Fee Schedule (CMS-1654-P) Summary of Key Provisions July 15, 2016 The Centers for Medicare and Medicaid Services (CMS) on July 7 published a rule that updates the payment policies,
Fact Sheet: 2019 Merit-based Incentive Payment System (MIPS) Payment Adjustments based on 2017 MIPS Final Scores
 Payment Adjustments based on 2017 MIPS Final Scores") Fact Sheet: 2019 Merit-based Incentive Payment System (MIPS) Payment Adjustments based on 2017 MIPS Final Scores The Medicare Access and CHIP Reauthorization Act of 2015 (MACRA) repealed the Medicare sustainable
Fact Sheet: 2019 Merit-based Incentive Payment System (MIPS) Payment Adjustments based on 2017 MIPS Final Scores The Medicare Access and CHIP Reauthorization Act of 2015 (MACRA) repealed the Medicare sustainable
2019 Merit-based Incentive Payment System (MIPS) Cost Performance Category Fact Sheet
 Cost Performance Category Fact Sheet") 2019 Merit-based Incentive Payment System (MIPS) Cost Performance Category Fact Sheet What is the Quality Payment Program? The Medicare Access and CHIP Reauthorization Act of 2015 (MACRA) ended the Sustainable
2019 Merit-based Incentive Payment System (MIPS) Cost Performance Category Fact Sheet What is the Quality Payment Program? The Medicare Access and CHIP Reauthorization Act of 2015 (MACRA) ended the Sustainable
WHERE THE FRONT LINE MEETS THE BOTTOM LINE: THE HEALTHCARE SYSTEM OF THE FUTURE
 WHERE THE FRONT LINE MEETS THE BOTTOM LINE: THE HEALTHCARE SYSTEM OF THE FUTURE AFT Nurses and Health Professionals Professional Issues Conference 2016 Fred Hyde, MD April 21, 2016 Trends for 2016-2022:
WHERE THE FRONT LINE MEETS THE BOTTOM LINE: THE HEALTHCARE SYSTEM OF THE FUTURE AFT Nurses and Health Professionals Professional Issues Conference 2016 Fred Hyde, MD April 21, 2016 Trends for 2016-2022:
CPC+ PAYMENT METHODOLOGIES: BENEFICIARY ATTRIBUTION, CARE MANAGEMENT FEE, PERFORMANCE-BASED INCENTIVE PAYMENT, AND PAYMENT UNDER THE MEDICARE
 CPC+ PAYMENT METHODOLOGIES: BENEFICIARY ATTRIBUTION, CARE MANAGEMENT FEE, PERFORMANCE-BASED INCENTIVE PAYMENT, AND PAYMENT UNDER THE MEDICARE PHYSICIAN FEE SCHEDULE Version 2 February 17, 2017 Table of
CPC+ PAYMENT METHODOLOGIES: BENEFICIARY ATTRIBUTION, CARE MANAGEMENT FEE, PERFORMANCE-BASED INCENTIVE PAYMENT, AND PAYMENT UNDER THE MEDICARE PHYSICIAN FEE SCHEDULE Version 2 February 17, 2017 Table of
CMS 1701 P UnityPoint Health. October 16, 2018
 CMS 1701 P UnityPoint Health 1776 West Lakes Parkway, Suite 400 West Des Moines, IA 50266 unitypoint.org October 16, 2018 Seema Verma, Administrator Centers for Medicare & Medicaid Services Department
CMS 1701 P UnityPoint Health 1776 West Lakes Parkway, Suite 400 West Des Moines, IA 50266 unitypoint.org October 16, 2018 Seema Verma, Administrator Centers for Medicare & Medicaid Services Department
Holy MACRA! Mark D. Kaufmann, M.D. Associate Clinical Professor Department of Dermatology Icahn School of Medicine at Mount Sinai October 27, 2017
 Holy MACRA! Mark D. Kaufmann, M.D. Associate Clinical Professor Department of Dermatology Icahn School of Medicine at Mount Sinai October 27, 2017 DISCLOSURE OF RELEVANT RELATIONSHIPS WITH INDUSTRY Mark
Holy MACRA! Mark D. Kaufmann, M.D. Associate Clinical Professor Department of Dermatology Icahn School of Medicine at Mount Sinai October 27, 2017 DISCLOSURE OF RELEVANT RELATIONSHIPS WITH INDUSTRY Mark