Name Date of Birth / / First M.I. Last. Address City State Zip. Home Phone Cell Phone Work Phone. Address
|
|
|
- Derek Cox
- 5 years ago
- Views:
Transcription
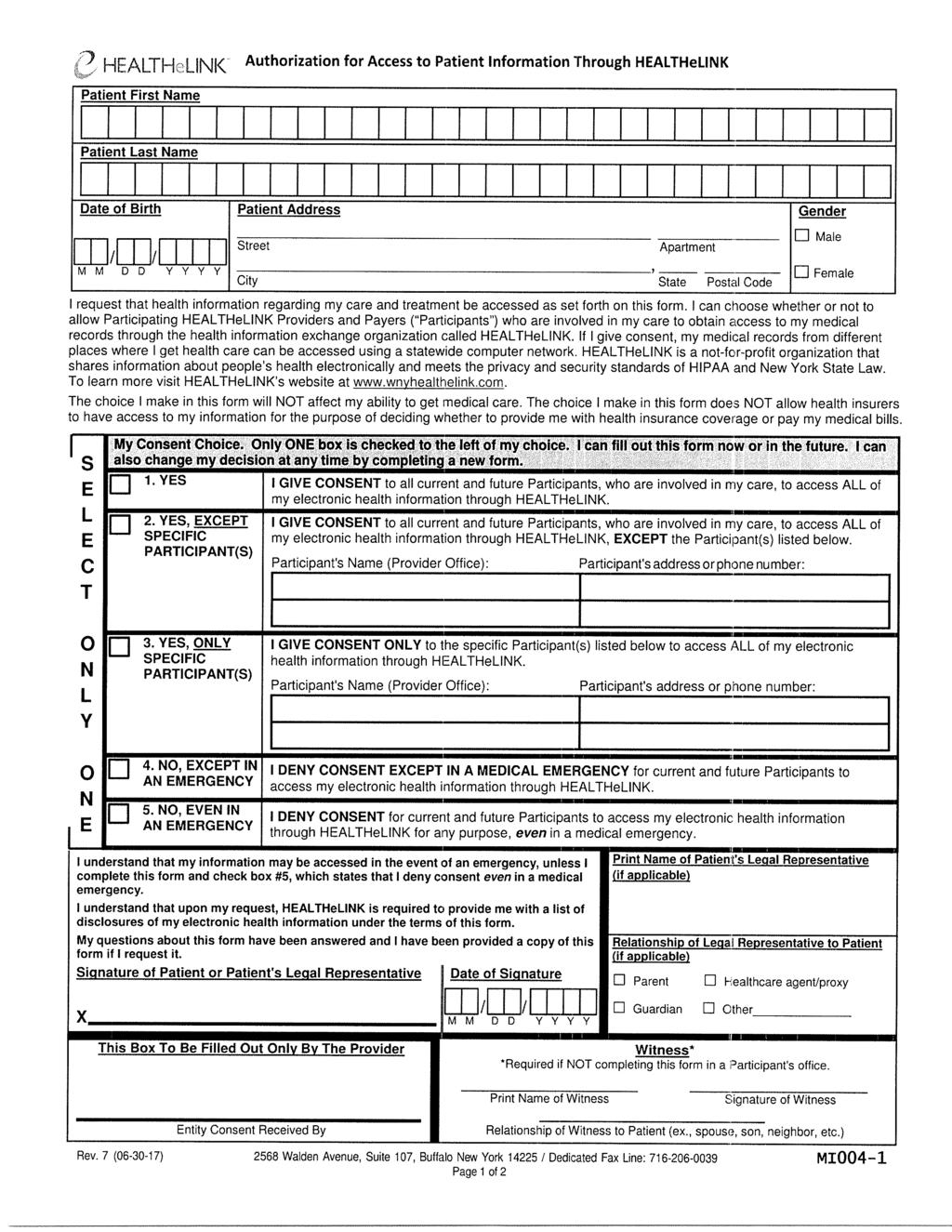
 675 2500 (716) 204 4263 PATIE")
1 3055 SOUTHWESTERN BLVD SHERIDAN DR. ORCHARD PARK, NY AMHERST, NY (716) (716) PATIENT INFORMATION (Please Print) Today s Date: / / Name Date of Birth / / First M.I. Last Address _ City State Zip Home Phone Cell Phone Work Phone Address Social Security # Marital Status Sex M F Race Language of Choice Ethnicity Primary Care Physician Name Address INSURANCE INFORMATION (Please present insurance card at time of check in) Primary Insurance ID Number Name of Primary Insured Date of Birth Social Security # Relationship to Patient Secondary Insurance ID Number Name of Secondary Insured Date of Birth Social Security # Relationship to Patient Pharmacy Address I authorize release of any medical information to my primary care and/or referring physician and those necessary to process insurance claims, insurance applications, and/or prescriptions. I also request payment of government benefits either to myself or to the party who accepts assignment below. I also authorize payment of medical benefits be made to the above- named physician for all services rendered to me. I understand that even though I have insurance coverage, I am responsible for payment of services, deductibles and/or co-payments. PATIENT OR RESPONSIBLE PARTY SIGNATURE *Please be advised we do not accept workers compensation or no fault claims.*
2 3055 SOUTHWESTERN BLVD SHERIDAN DR. ORCHARD PARK, NY AMHERST, NY (716) (716) PATIENT INFORMATION (Please Print) Today s Date: / / Name Date of Birth / / First M.I. Last Primary Care Physician Referring Physician if other than above DO YOU HAVE A HISTORY OF OR ARE YOU CURRENTLY EXPERIENCING ANY OF THE FOLLOWING? Please circle all that apply. General: weakness frequent infections Head: headache sinus pain and congestion Eyes: cataracts contacts or glasses blurred vision double vision glaucoma Ears: hearing loss ringing infections earache Mouth: bleeding gums sore tongue Neck: swollen glands tender glands enlarged thyroid Respiratory: wheezing cough pneumonia Cardiac: chest pain palpitations ankle swelling murmur rheumatic fever GI: nausea vomiting diarrhea constipation heartburn stomach ulcer blood in your stool loss of appetite abdominal pain gallbladder disease Urinary: pain frequency blood in your urine nightly urination kidney stones Genital: sexually transmitted disease vaginal/penile discharge prostatitis sexual dysfunction Endo: diabetes thyroid disease temperature intolerance excessive thirst Heme: anemia bleeding disorder transfusions blood clots Skin: hives itching leg ulcers acne psoriasis Neuro: fainting numbness tingling seizures tremors stroke Psych: depression anxiety panic attacks Other
3 PLEASE NOTE DATE IF YOU HAVE HAD ANY OF THE FOLLOWING: Flu vaccine Pneumonia shot Tetanus shot Hepatitis shots Shingles shot Skin test for TB Mammogram Pap smear Last menstrual period Age at Menopause PSA level PLEASE LIST YOUR MEDICATIONS AND HOW OFTEN YOU TAKE THEM: (or attach an additional sheet listing all your medications) PLEASE LIST ANY ALLEGERIES YOU HAVE: PLEASE LIST YOUR MEDICAL PROBLEMS:
4 PLEASE LIST SURGICAL HISTORY: SOCIAL HISTORY: Occupation Currently you are: working / retired / disabled / sick leave Who lives in your household? List your Pets Do you smoke? How much? How long? Recreational drugs? Alcohol? How often? Do you exercise? How often?
5 Dr. Joseph M. Grisanti Dr. Michael W. Grisanti Dr. Linda M. Burns Dr. Harbrinder Sandhu ACKNOWLEDGEMENT OF RECEIPT OF PRIVACE NOTICE I,, understand that Buffalo Rheumatology may share my health information for treatment, billing, and healthcare operations. I have been offered a copy of the Notice of Privacy Practices that describes how my health information may be used and shared. My signature below constitutes my acknowledgement that I have reviewed the copy of the Notice of Privacy Practices. PATIENT PRIVACY INFORMATION Please list ANY family members or other persons, if any, whom we may inform about your general medical condition and/or your diagnosis. Name Name Phone Number Phone Number Can confidential messages be left on your home answering machine, your cell phone or with another person? Yes No Can we call you at work? Yes No Can we send via mail? Yes No Signature of Patient Signature of Legal Representative Date Relationship to Patient Patient's Date of Birth 3055 SOUTHWESTERN BLVD SHERIDAN DR. ORCHARD PARK, NY AMHERST, NY (716) (716)
6
7
8 3055 SOUTHWESTERN BLVD SHERIDAN DR. ORCHARD PARK, NY AMHERST, NY (716) (716) Buffalo Rheumatology and Medicine PLLC Financial Policy Thank you for choosing Buffalo Rheumatology and Medicine PLLC as your healthcare provider. The billing department will work with you to fulfill your payment responsibility. Buffalo Rheumatology and Medicine PPLC requires payment at the time of service. All applicable co-pays will be collected at the time of check-in for your appointment. You are responsible for any deductibles or co-insurances in accordance with your health insurance policy as well. Our office will collect a portion of this amount at the time of appointment check-in. Self-Pay patients who require treatment without insurance will be required to pay $50 $200 depending upon services rendered. This payment is to be made promptly after the patient has seen the provider before future appointments are made to ensure continuation of care by Buffalo Rheumatology and Medicine PLLC. Deductibles and Co-insurances Patients with deductible or co-insurance plans will be required to pre-pay a portion out of pocket before services are rendered. Procedures and drug administration quotes will be given prior to the patient s appointment. Pre-collection amounts are estimates only, as we are unable to determine services reimbursement due to the amount of different insurance plans. You will be billed for any remaining amount due after payment is received from insurance and prepayment is applied, or refunded should you overpay. Non-participating/Non-contractual Insurance Plans Should Buffalo Rheumatology and Medicine PLLC not participate with your healthcare plan, you will be required to pay out of pocket for services rendered ranging from $50 $200. This amount will be collected promptly after services are rendered, before scheduling future appointments to ensure continuation of care by Buffalo Rheumatology and Medicine PLLC. Any questions or concerns regarding any of this policy please feel free to contact our billing department at Payment plans are available for those who qualify. Signature Date
PATIENT INFORMATION. Last Name: First Name: Middle Initial: Address:
 PATIENT INFORMATION Today s Date: Last Name: First Name: Middle Initial: Address: STREET CITY STATE ZIP CODE Gender: Male Female Social Security #: Date of Birth: Home Phone: Cell Phone Work Phone: E-mail:
PATIENT INFORMATION Today s Date: Last Name: First Name: Middle Initial: Address: STREET CITY STATE ZIP CODE Gender: Male Female Social Security #: Date of Birth: Home Phone: Cell Phone Work Phone: E-mail:
Bellingham Arthritis & Rheumatology Center. 470 Birchwood Avenue, Suite C, Bellingham, WA (P) (F)
 (F)") Bellingham Arthritis & Rheumatology Center 470 Birchwood Avenue, Suite C, Bellingham, WA 98225 (P) 360-734-5754 (F) 360-734-0586 Patient Name SSN Last First M.I. Date of Birth Age Sex: Male Female Address
Bellingham Arthritis & Rheumatology Center 470 Birchwood Avenue, Suite C, Bellingham, WA 98225 (P) 360-734-5754 (F) 360-734-0586 Patient Name SSN Last First M.I. Date of Birth Age Sex: Male Female Address
Patient Information Form
 ALASKA DIGESTIVE AND LIVER DISEASE, LLC Ronald J Boisen, M.D. Daryl M. McClendon, M.D. Jeffrey W. Molloy, M.D. Patient Information Form Patient s Name: Age: DOB: Sex: Male Female Marital Status: S M W
ALASKA DIGESTIVE AND LIVER DISEASE, LLC Ronald J Boisen, M.D. Daryl M. McClendon, M.D. Jeffrey W. Molloy, M.D. Patient Information Form Patient s Name: Age: DOB: Sex: Male Female Marital Status: S M W
Haroon Rehman, MD 3200 Talon Drive. Suite 300 Richardson, TX Phone: Fax: Address: City: ST: ZIP:
 Haroon Rehman, MD 3200 Talon Drive. Suite 300 Richardson, TX 75082 972-649-5937 Fax: 972-807-0385 Patients General Information Last Name: First Name: Patient s SSN: of Birth MM/DD/YYYY: / / Age: Sex: M/F
Haroon Rehman, MD 3200 Talon Drive. Suite 300 Richardson, TX 75082 972-649-5937 Fax: 972-807-0385 Patients General Information Last Name: First Name: Patient s SSN: of Birth MM/DD/YYYY: / / Age: Sex: M/F
HIPAA PATIENT CONSENT FORM
 HIPAA PATIENT CONSENT FORM Our Notice of Privacy Practices provides information about how we may use and disclose protected health information about you. The Notice contains a Patient Rights section describing
HIPAA PATIENT CONSENT FORM Our Notice of Privacy Practices provides information about how we may use and disclose protected health information about you. The Notice contains a Patient Rights section describing
Last Name: First Name: MI: Address: Apt #: City: State: Zip: Home #: Work #: Emergency #: Birthdate: SSN: Sex: Marital Status: Employer: Occupation:
 Patient Registration How did you hear about us? Newspaper Friend/Family Website Other: Patient Information Last Name: First Name: MI: Address: Apt #: City: _ State: Zip: Home #: Work #: Emergency #: Birthdate:
Patient Registration How did you hear about us? Newspaper Friend/Family Website Other: Patient Information Last Name: First Name: MI: Address: Apt #: City: _ State: Zip: Home #: Work #: Emergency #: Birthdate:
1421 S. Potomac Street, Suite 120 Aurora, CO Please print and complete all parts.
 Thomas J. Savage, DPM Jay H. Dworkin, DPM PC 1421 S. Potomac Street, Suite 120 Aurora, CO 80012 303.923.3369 www.metrofoot.org 303.923.3882(fax) Please print and complete all parts. Date PATIENT INFORMATION
Thomas J. Savage, DPM Jay H. Dworkin, DPM PC 1421 S. Potomac Street, Suite 120 Aurora, CO 80012 303.923.3369 www.metrofoot.org 303.923.3882(fax) Please print and complete all parts. Date PATIENT INFORMATION
Chong S Kim, MD ENT and Facial Plastic Surgeon
 Chong S Kim, MD ENT and Facial Plastic Surgeon 100 Commons Way, Suite 701 300 Perrine Rd., Suite 301 Holmdel, NJ 07733 Old Bridge, N.J 08857 Phone: 732-796-0182 Phone: 732-727-1355 Fax: 732-796-0186 Fax:
Chong S Kim, MD ENT and Facial Plastic Surgeon 100 Commons Way, Suite 701 300 Perrine Rd., Suite 301 Holmdel, NJ 07733 Old Bridge, N.J 08857 Phone: 732-796-0182 Phone: 732-727-1355 Fax: 732-796-0186 Fax:
Address. City/State/Zip. Marital Status: S M D W Sex: M F Date of Birth / / Age. Primary Phone Secondary Phone. Employer PARENT/GUARDIAN
 PATIENT INFORMATION First Name M.I Last Name Address City/State/Zip SSN.#_ Marital Status: S M D W Sex: M F of Birth / / Age Primary Phone Secondary Phone Employer Email PARENT/GUARDIAN Name of Birth /
PATIENT INFORMATION First Name M.I Last Name Address City/State/Zip SSN.#_ Marital Status: S M D W Sex: M F of Birth / / Age Primary Phone Secondary Phone Employer Email PARENT/GUARDIAN Name of Birth /
ROBERT H. OLIVER, M.D., PLLC Otolaryngology Head And Neck Surgery Otolaryngic Allergy Chart #
 Chart # PATIENT INFORMATION Please Print, Complete Fully, And Return To The Front Desk Circle One: Mr. Mrs. Ms. Miss. Dr. Child Please Circle: Sex: Male Female Marital Status: S M Other Widowed Patient
Chart # PATIENT INFORMATION Please Print, Complete Fully, And Return To The Front Desk Circle One: Mr. Mrs. Ms. Miss. Dr. Child Please Circle: Sex: Male Female Marital Status: S M Other Widowed Patient
PATIENT INFORMATION SHEET
 PATIENT INFORMATION SHEET Patient Name: DOB: Address: ADDRESS CITY, STATE, ZIP SSN: Mailing Address: ADDRESS CITY, STATE, ZIP Same as above Home phone: Cell phone: Work phone: Marital Status: Single /
PATIENT INFORMATION SHEET Patient Name: DOB: Address: ADDRESS CITY, STATE, ZIP SSN: Mailing Address: ADDRESS CITY, STATE, ZIP Same as above Home phone: Cell phone: Work phone: Marital Status: Single /
Gentle Family & Cosmetic Care. Raj Zanzi, DMD WELCOME. Insiya Zanzi, DDS
 WELCOME We are pleased to welcome you to our practice. Please take a few minutes to fill out this form as completely as you can. If you have any questions we ll be glad to help you. We look forward to
WELCOME We are pleased to welcome you to our practice. Please take a few minutes to fill out this form as completely as you can. If you have any questions we ll be glad to help you. We look forward to
PATIENT REGISTRATION FORM Account #:
 PATIENT REGISTRATION FORM Account #: All forms must be completed and signed prior to treatment. GENERAL INFORMATION Patient Name: First Middle Last Address: Home Phone No: Work Phone No: Cell Phone No:
PATIENT REGISTRATION FORM Account #: All forms must be completed and signed prior to treatment. GENERAL INFORMATION Patient Name: First Middle Last Address: Home Phone No: Work Phone No: Cell Phone No:
PATIENT REGISTRATION FORM CAROLINA EAR, NOSE & THROAT
 PATIENT REGISTRATION FORM CAROLINA EAR, NOSE & THROAT Last Name: First: M.I.: Sex: Age: Date of Birth / / Social Security # - - Race: Ethnicity: Language Spoken: If patient is child / under 18: Parent
PATIENT REGISTRATION FORM CAROLINA EAR, NOSE & THROAT Last Name: First: M.I.: Sex: Age: Date of Birth / / Social Security # - - Race: Ethnicity: Language Spoken: If patient is child / under 18: Parent
ROCKWALL SURGICAL SPECIALISTS
 PATIENT REGISTRATION FORM Patient s name (Last, First, Middle Initial) Sex (M or F) Date of Birth Address City State Zip Home Phone Cell Phone Email Marital Status Social Security Number Driver s License
PATIENT REGISTRATION FORM Patient s name (Last, First, Middle Initial) Sex (M or F) Date of Birth Address City State Zip Home Phone Cell Phone Email Marital Status Social Security Number Driver s License
ROCKWALL SURGICAL SPECIALISTS
 ROCKWALL SURGICAL SPECIALISTS Dr. David Ritter Dr. Ashley Egan Dr. Jon Harris Phone (972) 412-7700 Fax (972) 412-7710 PATIENT REGISTRATION FORM Patient s name (Last, First, Middle Initial) Sex (M or F)
ROCKWALL SURGICAL SPECIALISTS Dr. David Ritter Dr. Ashley Egan Dr. Jon Harris Phone (972) 412-7700 Fax (972) 412-7710 PATIENT REGISTRATION FORM Patient s name (Last, First, Middle Initial) Sex (M or F)
PAYMENT POLICY: Payment or partial payment is required on the day of visit.
 Patient Information Date Patient Name (First) (M.I.) (Last) Date of Birth SSN Gender Male Female Transgender-Male Transgender-Female Marital Status Race Ethnicity Preferred Language Patient Address City
Patient Information Date Patient Name (First) (M.I.) (Last) Date of Birth SSN Gender Male Female Transgender-Male Transgender-Female Marital Status Race Ethnicity Preferred Language Patient Address City
Patient Information Last Name First Name Middle Initial
 Patient Information Last Name First Name Middle Initial Street Address Apt# City State Zip Code Social Security # Home Phone Cell Phone Email D.O.B Sex(M/F) Occupation Relation to Insured Self Spouse Child
Patient Information Last Name First Name Middle Initial Street Address Apt# City State Zip Code Social Security # Home Phone Cell Phone Email D.O.B Sex(M/F) Occupation Relation to Insured Self Spouse Child
West Houston Infectious Disease Associates. Address: Number Street Apt. No. City State Zip. Home Phone: Cell: Work:
 Carson T. Lo M.D. West Houston Infectious Disease Associates Linda S. Yancey, M.D. NEW PATIENT INFORMATION Thank you for choosing West Houston Infectious Disease Associates. Please completely fill out
Carson T. Lo M.D. West Houston Infectious Disease Associates Linda S. Yancey, M.D. NEW PATIENT INFORMATION Thank you for choosing West Houston Infectious Disease Associates. Please completely fill out
PATIENT INFORMATION FORM RICHARD L. MALINICK, M.D. ORTHOPAEDIC SURGERY 1125 Via Verde, San Dimas, CA
 Email Address Last Name First Name Previous Name Address City State Zip Country Social Security - - Home Phone - - Cell Phone - - Work Phone - - Ext Drivers License State Responsible Party SELF (use info
Email Address Last Name First Name Previous Name Address City State Zip Country Social Security - - Home Phone - - Cell Phone - - Work Phone - - Ext Drivers License State Responsible Party SELF (use info
Villa Medical Arts New Patient Forms
 Villa Medical Arts New Patient Forms New Patients, To expedite your check- in process, please print and complete the following pages. If you have access to a fax machine, please fax them along with a copy
Villa Medical Arts New Patient Forms New Patients, To expedite your check- in process, please print and complete the following pages. If you have access to a fax machine, please fax them along with a copy
Birth Date: Age: Sex: Ethnicity: Carrier: Cardholder's Name: Carrier: Cardholder's Name:
 Patient Information Patient's Last Name: First: MI: Social Security Number: Birth Date: Age: Sex: Ethnicity: Street Address: City: State: ZIP Code: Home Phone: Cell Phone: Work Phone: E-Mail Address: Referring
Patient Information Patient's Last Name: First: MI: Social Security Number: Birth Date: Age: Sex: Ethnicity: Street Address: City: State: ZIP Code: Home Phone: Cell Phone: Work Phone: E-Mail Address: Referring
PATIENT REGISTRATION
 PATIENT REGISTRATION Patient s Name Date Street Address City State & Zip Home Phone ( ) Sex Age Date of Birth Cell Phone ( ) Email Address Race Primary Language Employer Occupation Work Phone ( ) May we
PATIENT REGISTRATION Patient s Name Date Street Address City State & Zip Home Phone ( ) Sex Age Date of Birth Cell Phone ( ) Email Address Race Primary Language Employer Occupation Work Phone ( ) May we
Gary W. White, M.D. Dean A. Cione, M.D. Jeremy S. Carrasco, M.D. Ramsey A. Stone, M.D
 PATIENT REGISTRATION FORM First Name: MI: Last Name: Date of Birth: Address: Apt#: City: State: Zip: Home Phone: ( ) Cell Phone: ( ) Work Phone ( ) SS#: - - SEX: Female Male E-mail Address: Ethnicity:
PATIENT REGISTRATION FORM First Name: MI: Last Name: Date of Birth: Address: Apt#: City: State: Zip: Home Phone: ( ) Cell Phone: ( ) Work Phone ( ) SS#: - - SEX: Female Male E-mail Address: Ethnicity:
Patient Registration Form
 Patient Registration Form Date: Name: Maiden Name: (First) (MI) (Last) SSN: Birth Date: Age: Marital Status: Sex: M or F Race: Ethnicity: Language: Mailing Address: City: State: Zip: Physical Address:
Patient Registration Form Date: Name: Maiden Name: (First) (MI) (Last) SSN: Birth Date: Age: Marital Status: Sex: M or F Race: Ethnicity: Language: Mailing Address: City: State: Zip: Physical Address:
Name (Last, First, MI): Date of Birth: / /
: Date of Birth: / /") Name (Last, First, MI): Address: Age: City: State: Zip: Sex: Male / Female Phone #: (Home): (Cell): (Work): Personal Email: Social Security #: Race: Ethnicity: Hispanic/Latino Non-Hispanic/Latino Other
Name (Last, First, MI): Address: Age: City: State: Zip: Sex: Male / Female Phone #: (Home): (Cell): (Work): Personal Email: Social Security #: Race: Ethnicity: Hispanic/Latino Non-Hispanic/Latino Other
Arizona Retina Associates
 PATIENT INFORMATION PLEASE PRINT CLEARLY AND COMPLETE ENTIRE FORM Name FIRST MIDDLE INITIAL LAST SUFFIX (Jr., etc.) Address STREET CITY STATE ZIP Age Birthdate SS# Marital Status S M D W Sex M F Occupation
PATIENT INFORMATION PLEASE PRINT CLEARLY AND COMPLETE ENTIRE FORM Name FIRST MIDDLE INITIAL LAST SUFFIX (Jr., etc.) Address STREET CITY STATE ZIP Age Birthdate SS# Marital Status S M D W Sex M F Occupation
HIPAA Authorization Release Form
 HIPAA Authorization Release Form I,, give permission to all my health care and medical services providers and payers to disclose and release my protected health information described below to: Name(s):
HIPAA Authorization Release Form I,, give permission to all my health care and medical services providers and payers to disclose and release my protected health information described below to: Name(s):
New Patient Medical Information Survey Revised 3/2013
 New Patient Medical Information Survey Revised 3/2013 We are glad you chose the Augusta Surgical Group to meet your surgical needs. Please take a few minutes to fill out this form, as it will help us provide
New Patient Medical Information Survey Revised 3/2013 We are glad you chose the Augusta Surgical Group to meet your surgical needs. Please take a few minutes to fill out this form, as it will help us provide
Today s Date: Street Address: City: State: Zip: Mailing Address (only if different): Circle: MALE or FEMALE Married Status: Social Security: - -
: Circle: MALE or FEMALE Married Status: Social Security: - -") New Patient Forms Today s Date: Name (Last, First, MI): Date of Birth: Today s Date: Street Address: City: State: Zip: Mailing Address (only if different): _ Home Phone: _ ( ) Cell Phone: _ ( ) Work Phone:
New Patient Forms Today s Date: Name (Last, First, MI): Date of Birth: Today s Date: Street Address: City: State: Zip: Mailing Address (only if different): _ Home Phone: _ ( ) Cell Phone: _ ( ) Work Phone:
Southern Oregon Wellness Clinic 2921 Doctors Park Drive Phone (541) Fax (541)
 Fax (541)") CONDITIONS OF SERVICES RENDERED FINANCIAL AGREEMENT: I agree, whether I sign as agent or as patient, that in consideration of the services to be rendered to the patient, I hereby individually obligate
CONDITIONS OF SERVICES RENDERED FINANCIAL AGREEMENT: I agree, whether I sign as agent or as patient, that in consideration of the services to be rendered to the patient, I hereby individually obligate
If you are employed, please provide the follow information regarding your employer; Employer Name: Work Address:
 Personal Information Patient Registration Form Today s Date: Patients First Name: Date of Birth: / / Social Security #: - - Patients Last Name: Sex: Male / Female Marital Status: Married Single Divorced
Personal Information Patient Registration Form Today s Date: Patients First Name: Date of Birth: / / Social Security #: - - Patients Last Name: Sex: Male / Female Marital Status: Married Single Divorced
Welcome To Our Office Please Print
 1 PATIENT INFORMATION Date Home Phone ( ) E-mail Street City State Zip Marital Status Children? Ages Occupation May we call you at work? Y N Work Hours SPOUSE/DOMESTIC PARTNER INFORMATION (If appropriate)
1 PATIENT INFORMATION Date Home Phone ( ) E-mail Street City State Zip Marital Status Children? Ages Occupation May we call you at work? Y N Work Hours SPOUSE/DOMESTIC PARTNER INFORMATION (If appropriate)
Other Scan(s): List All Your Medical Diagnosis: Chemotherapy? YES NO If yes, please list treatment regimen:
: List All Your Medical Diagnosis: Chemotherapy? YES NO If yes, please list treatment regimen:") Patient Name: Today s Date: Preferred Language: Date of Birth: Age: SSN: Race: Ethnicity: Home Phone: Cell Phone: Work Phone: Best contact phone number should we need to reach you about your treatment:
Patient Name: Today s Date: Preferred Language: Date of Birth: Age: SSN: Race: Ethnicity: Home Phone: Cell Phone: Work Phone: Best contact phone number should we need to reach you about your treatment:
CENTRAL FLORIDA ORAL & MAXILLOFACIAL SURGERY, PA PATIENT REGISTRATION Date: PATIENT INFORMATION
 CENTRAL FLORIDA ORAL & MAXILLOFACIAL SURGERY, PA PATIENT REGISTRATION Date: Pre-fix: Patient s Legal First Name: PATIENT INFORMATION Legal Last Name: Nickname: Mr Mrs Ms Dr Street Address: Home Phone #:
CENTRAL FLORIDA ORAL & MAXILLOFACIAL SURGERY, PA PATIENT REGISTRATION Date: Pre-fix: Patient s Legal First Name: PATIENT INFORMATION Legal Last Name: Nickname: Mr Mrs Ms Dr Street Address: Home Phone #:
Caritas Medical Center, LLC
 Caritas Medical Center, LLC KIDNEY DISEASE AND HYPERTENSION SPECIALIST 105 NORTH PARK TRAIL SUITE 300 STOCKBRIDGE, GA 30281 OFFICE: 678 284 0800 FAX: 678 284 9299 WWW.CARITASMED.COM DR. LEO OVADJE DR.
Caritas Medical Center, LLC KIDNEY DISEASE AND HYPERTENSION SPECIALIST 105 NORTH PARK TRAIL SUITE 300 STOCKBRIDGE, GA 30281 OFFICE: 678 284 0800 FAX: 678 284 9299 WWW.CARITASMED.COM DR. LEO OVADJE DR.
Chief Complaint Form: Patient Name: Age: DOB: Occupation: Employer: Referring Physician: Town: Primary Care Physician: Town: Y N
 Chief Complaint Form: Patient Name: Date: First MI Last Preferred Name Age: DOB: Occupation: Employer: Send Note? Referring Physician: Town: Y N Primary Care Physician: Town: Y N Coach/ Trainer/ Team Doctor:
Chief Complaint Form: Patient Name: Date: First MI Last Preferred Name Age: DOB: Occupation: Employer: Send Note? Referring Physician: Town: Y N Primary Care Physician: Town: Y N Coach/ Trainer/ Team Doctor:
Tracy Blum Physical Therapy, Inc NEW PATIENT REGISTRATION FORM PATIENT INFORMATION. Last Name: First Name: Middle Initial: Social Security no.
 Tracy Blum Physical Therapy, Inc NEW PATIENT REGISTRATION FORM PATIENT INFORMATION Last Name: First Name: Middle Initial: Date of Birth: / / Age: Sex: M F Social Security #: / / Marital Status (circle
Tracy Blum Physical Therapy, Inc NEW PATIENT REGISTRATION FORM PATIENT INFORMATION Last Name: First Name: Middle Initial: Date of Birth: / / Age: Sex: M F Social Security #: / / Marital Status (circle
PLEASE MARK (X) NEXT TO DOCUMENTS YOU HAVE: LIVING WILL POWER OF ATTORNEY DO NOT RESUSCITATE ORDER
 NEXT TO DOCUMENTS YOU HAVE: LIVING WILL POWER OF ATTORNEY DO NOT RESUSCITATE ORDER") CAREFIRST FAMILY PRACTICE 3631 W BURLEIGH BLVD TAVARES FL 32778 P.(352)742-0025 F.(352)742-8167 PATIENT NAME ALLERGIES TO MEDICATIONS TODAY'S DATE: DOB Hospital Admissions-Indicate the year you were admitted
CAREFIRST FAMILY PRACTICE 3631 W BURLEIGH BLVD TAVARES FL 32778 P.(352)742-0025 F.(352)742-8167 PATIENT NAME ALLERGIES TO MEDICATIONS TODAY'S DATE: DOB Hospital Admissions-Indicate the year you were admitted
PATIENT REGISTRATION
 PATIENT REGISTRATION Patient Acct#: Doctor: Referring Phy.: PATIENT INFORMATION Name: Address: Email: Date of Birth: Social Security #: City, State: Home Phone: Marital Status: married single divorced
PATIENT REGISTRATION Patient Acct#: Doctor: Referring Phy.: PATIENT INFORMATION Name: Address: Email: Date of Birth: Social Security #: City, State: Home Phone: Marital Status: married single divorced
EAR, NOSE, AND THROAT ASSOCIATES, PC Financial Policy Effective September 1, 2014
 EAR, NOSE, AND THROAT ASSOCIATES, PC Financial Policy Effective September 1, 2014 Patient name: Account# Ear, Nose and Throat Associates, PC, believes that in the interest of good health care practices,
EAR, NOSE, AND THROAT ASSOCIATES, PC Financial Policy Effective September 1, 2014 Patient name: Account# Ear, Nose and Throat Associates, PC, believes that in the interest of good health care practices,
PATIENT QUESTIONNAIRE DATE OF VISIT: Pg. 1
 PATIENT QUESTIONNAIRE DATE OF VISIT: Pg. 1 PATIENT NAME DATE OF BIRTH AGE PLEASE PROVIDE THE FOLLOWING MEDICAL INFORMATION TO THE BEST OF YOUR ABILITY: What problems are you here for today? List any allergies
PATIENT QUESTIONNAIRE DATE OF VISIT: Pg. 1 PATIENT NAME DATE OF BIRTH AGE PLEASE PROVIDE THE FOLLOWING MEDICAL INFORMATION TO THE BEST OF YOUR ABILITY: What problems are you here for today? List any allergies
Cardholder Name: Patient Name: Relation to Patient: Sex: Cardholder s DOB: Co-pay: Member ID#: Group #:
 2121 Whitesburg Drive, Suite C Huntsville, AL 35801 Name: DOB: Sex: Age: Address: City: State: Zip Code: Primary Phone: Secondary Phone: SSN: Preferred Language: Race: Employer: Occupation: Work Phone:
2121 Whitesburg Drive, Suite C Huntsville, AL 35801 Name: DOB: Sex: Age: Address: City: State: Zip Code: Primary Phone: Secondary Phone: SSN: Preferred Language: Race: Employer: Occupation: Work Phone:
Jandali Plastic Surgery
 Jandali Plastic Surgery PATIENT INFORMATION FORM : FirstMiddle Last Address: City State Zip Code Home Phone #( ) - Work #( ) - Cell #( ) - Emergency # ( ) - Emergency Contact Social Security Number - -
Jandali Plastic Surgery PATIENT INFORMATION FORM : FirstMiddle Last Address: City State Zip Code Home Phone #( ) - Work #( ) - Cell #( ) - Emergency # ( ) - Emergency Contact Social Security Number - -
Patient Registration Form
 Patient Registration Form Name: Last Name First Name MI (Previous Last name) SSN #: Address: Date of Birth: Sex: o M o F Home phone: Work phone: Cell phone: Email: Race: o Caucasian o Hispanic o Bi-racial
Patient Registration Form Name: Last Name First Name MI (Previous Last name) SSN #: Address: Date of Birth: Sex: o M o F Home phone: Work phone: Cell phone: Email: Race: o Caucasian o Hispanic o Bi-racial
Date: Patient Health Information. Patient Name: First Middle Last Nickname. Date of Birth: Age: Sex: Male Female. Referring Physician:
 Date: Patient Health Information Patient Name: First Middle Last Nickname Date of Birth: Age: Sex: Male Female Referring Physician: Family Physician: City: City: What is the main reason for your visit?
Date: Patient Health Information Patient Name: First Middle Last Nickname Date of Birth: Age: Sex: Male Female Referring Physician: Family Physician: City: City: What is the main reason for your visit?
PATIENT REGISTRATION
 PATIENT REGISTRATION Please print clearly so that we can process your information quickly and efficiently. Thank you! Name (First, M.I., Last) of Birth Age Male / Female Marital Status: S M W D Address
PATIENT REGISTRATION Please print clearly so that we can process your information quickly and efficiently. Thank you! Name (First, M.I., Last) of Birth Age Male / Female Marital Status: S M W D Address
Capstone Family Practice- Patient Registration
 Capstone Family Practice- Patient Registration Patient Information: Last name: First Name: Middle name: Date of birth: / / Gender: Social security number: - - Marital status: Home phone number: ( ) - Work
Capstone Family Practice- Patient Registration Patient Information: Last name: First Name: Middle name: Date of birth: / / Gender: Social security number: - - Marital status: Home phone number: ( ) - Work
PATIENT HISTORY FORM. DOB: Age: Male Female Marital Status. Address: Preferred Method of Contact: Home Cell Work Text
 PATIENT HISTORY FORM Name: SSN: (Last) (First) (MI) DOB: Age: Male Female Marital Status Address: (Street) (City) (State) (Zip) Home Phone: Cell: Work: Email Address: Preferred Method of Contact: Home
PATIENT HISTORY FORM Name: SSN: (Last) (First) (MI) DOB: Age: Male Female Marital Status Address: (Street) (City) (State) (Zip) Home Phone: Cell: Work: Email Address: Preferred Method of Contact: Home
Greater Austin Allergy, Asthma & Immunology
 Greater Austin Allergy, Asthma & Immunology phone: (512) 732-2774 fax: (512) 329-6871 PATIENT INFORMATION Patient Name DOB Age SSN Today s Date Sex Single Married Widowed Divorced Present Address City,
Greater Austin Allergy, Asthma & Immunology phone: (512) 732-2774 fax: (512) 329-6871 PATIENT INFORMATION Patient Name DOB Age SSN Today s Date Sex Single Married Widowed Divorced Present Address City,
Tri-Valley Internal Medicine Group New Patient Registration Form
 Tri-Valley Internal Medicine Group New Patient Registration Form Patient Information Patient s Last Name First Name MI Sex M F Patient s of Birth Age Social Security # (Billing/Identification Purpose)
Tri-Valley Internal Medicine Group New Patient Registration Form Patient Information Patient s Last Name First Name MI Sex M F Patient s of Birth Age Social Security # (Billing/Identification Purpose)
Tri-Valley Internal Medicine Group Registration Form
 Registration Form Patient Information Patient's Name: Last Name First Name DOB Age Sex: M F Patient Address: City: State: Zip Code: Home Number: Cell Number: Must have patient SSN# for Billing Purpose
Registration Form Patient Information Patient's Name: Last Name First Name DOB Age Sex: M F Patient Address: City: State: Zip Code: Home Number: Cell Number: Must have patient SSN# for Billing Purpose
If you are prescribed any medications, where would you like the script sent? Pharmacy Name: Pharmacy Phone:
 AMELIA A. PARÉ, M.D. PATIENT REGISTRATION Date of visit: PATIENT INFORMATION (PLEASE PRINT) Name: Date of Birth: Age: Male Female Race Social Security #: Marital Status: Single Married Divorced Widowed
AMELIA A. PARÉ, M.D. PATIENT REGISTRATION Date of visit: PATIENT INFORMATION (PLEASE PRINT) Name: Date of Birth: Age: Male Female Race Social Security #: Marital Status: Single Married Divorced Widowed
New Patient Packet. Thank you for choosing Shasta Regional Medical Group. Our office looks forward to serving you.
 New Patient Packet Thank you for choosing Shasta Regional Medical Group. Our office looks forward to serving you. Prior to your appointment: Please complete the attached New Patient Paperwork. Be sure
New Patient Packet Thank you for choosing Shasta Regional Medical Group. Our office looks forward to serving you. Prior to your appointment: Please complete the attached New Patient Paperwork. Be sure
CROSSROADS HEALTH CLINIC Thank you for choosing us as your Health Care Provider.
 PATIENT INFORMATION First Name: Middle Initial: Last Name: Mailing Address: Street Address: City: County: State: Zip: Phone #: Work: Ext: Would you like us to text you? Yes No Cell #: Driver s License
PATIENT INFORMATION First Name: Middle Initial: Last Name: Mailing Address: Street Address: City: County: State: Zip: Phone #: Work: Ext: Would you like us to text you? Yes No Cell #: Driver s License
ADVANCED GASTROENTEROLOGY RESEARCH & ENDOSCOPY CENTERS
 NEW PATIENT QUESTIONNAIRE Family Physician: Patient s Social Security #: (Social security number mandatory) Address: e-mail address: I understand that my e-mail will only be used for educational information.
NEW PATIENT QUESTIONNAIRE Family Physician: Patient s Social Security #: (Social security number mandatory) Address: e-mail address: I understand that my e-mail will only be used for educational information.
Patient Information. Emergency Contact Name: Pharmacy Information. Medical Release
 Patient Information Patient's Last Name: First: Birth MI: Age: Social Security Number: Sex: Ethnicity: Street Address: City: State: ZIP Code: Home Phone: Cell Phone: Work Phone: E-Mail Address: Employer
Patient Information Patient's Last Name: First: Birth MI: Age: Social Security Number: Sex: Ethnicity: Street Address: City: State: ZIP Code: Home Phone: Cell Phone: Work Phone: E-Mail Address: Employer
Any pertinent medical records
 Hello, and welcome to Arizona Pulmonary Specialists, Ltd. You are scheduled to see on at. Please plan to arrive 20 minutes prior to this time. If you are unable to keep this appointment for any reason,
Hello, and welcome to Arizona Pulmonary Specialists, Ltd. You are scheduled to see on at. Please plan to arrive 20 minutes prior to this time. If you are unable to keep this appointment for any reason,
Patient Registration Form
 Patient Registration Form PATIENT INFORMATION Please Print Last Name: First: M.I. Mailing Address: City: State: Zip Code: Date of Birth: Gender: M F Married Single Widowed Divorced Separated Partnered
Patient Registration Form PATIENT INFORMATION Please Print Last Name: First: M.I. Mailing Address: City: State: Zip Code: Date of Birth: Gender: M F Married Single Widowed Divorced Separated Partnered
GREENLAKE PRIMARY CARE PATIENT INFORMATION
 GREENLAKE PRIMARY CARE PATIENT INFORMATION Patient s Name First Initial Last Name you like to be called Referred by Gender: M F Social Security # - - Birth Date (Mo/Day/Yr) Address Street/ P.O. Box (Apt
GREENLAKE PRIMARY CARE PATIENT INFORMATION Patient s Name First Initial Last Name you like to be called Referred by Gender: M F Social Security # - - Birth Date (Mo/Day/Yr) Address Street/ P.O. Box (Apt
Surgical Group of Gainesville, PA
 Surgical Group of Gainesville, PA REGISTRATION FORM Peter Sarantos, MD* FACS Bruce W. Brient, MD* FACS Stanley V. DeTurris, MD* FACS Brian E. Pickens, MD* FACS Timothy A. Hipp, MD* FACS Jeffery Jeffrey
Surgical Group of Gainesville, PA REGISTRATION FORM Peter Sarantos, MD* FACS Bruce W. Brient, MD* FACS Stanley V. DeTurris, MD* FACS Brian E. Pickens, MD* FACS Timothy A. Hipp, MD* FACS Jeffery Jeffrey
Acknowledgment of Receipt of Notice
 Acknowledgment of Receipt of Notice patient acknowledgment I acknowledge receipt of a copy of Maximum Mobility s Notice of Privacy Practices with an effective of January 1, 2012. printed name of patient
Acknowledgment of Receipt of Notice patient acknowledgment I acknowledge receipt of a copy of Maximum Mobility s Notice of Privacy Practices with an effective of January 1, 2012. printed name of patient
Patient Information. Name Date. Address City Zip. Age Date of Birth / / Marital Status M S D W. Social Security # Driver s License #
 Patient Information Name Date Address City Zip Age Date of Birth / / Marital Status M S D W # of Children Social Security # Driver s License # May Ashby Chiropractic Clinic communicate with you by: Telephone
Patient Information Name Date Address City Zip Age Date of Birth / / Marital Status M S D W # of Children Social Security # Driver s License # May Ashby Chiropractic Clinic communicate with you by: Telephone
NEW PATIENT INFORMATION
 1240 EAGLES LANDING PARKWAY SUITE 100 STOCKBRIDGE GA 30281 PHONE 770) 506-0100 FAX 770) 507-2597 NEW PATIENT INFORMATION Print Name: DOB: / / SSN: - - Gender: Age: Race: Marital Status: Employment Status:
1240 EAGLES LANDING PARKWAY SUITE 100 STOCKBRIDGE GA 30281 PHONE 770) 506-0100 FAX 770) 507-2597 NEW PATIENT INFORMATION Print Name: DOB: / / SSN: - - Gender: Age: Race: Marital Status: Employment Status:
CASCADE SURGEONS 875 Wesley St. Ste 230 Arlington WA (360)
") CASCADE SURGEONS 875 Wesley St. Ste 230 Arlington WA 98223-1668 (360) 435-6097 M.C. WHITMAN III, M.D., FACS PETER WOLFF, M.D., FACS DEAR You have been referred to Cascade Surgeons, the office of Dr. Whitman
CASCADE SURGEONS 875 Wesley St. Ste 230 Arlington WA 98223-1668 (360) 435-6097 M.C. WHITMAN III, M.D., FACS PETER WOLFF, M.D., FACS DEAR You have been referred to Cascade Surgeons, the office of Dr. Whitman
Christine LaComb, RN, FNP-C th Street Suite B Groves, TX (409) Phone (409) Fax
 Phone (409) Fax") Christine LaComb, RN, FNP-C 6000 39 th Street Suite B Groves, TX. 77619 (409) 962-8509 Phone (409) 962-0763 Fax Welcome To Our Practice! In Order To Properly Serve You, Please Complete The Following Forms
Christine LaComb, RN, FNP-C 6000 39 th Street Suite B Groves, TX. 77619 (409) 962-8509 Phone (409) 962-0763 Fax Welcome To Our Practice! In Order To Properly Serve You, Please Complete The Following Forms
PATIENT INFORMATION PRIMARY INSURANCE INFORMATION
 1001 Medical Plaza Dr. The Woodlands, TX 77380 www.woodlandsretina.com Tel: 281-367-9700 Fax: 281-367-9701 PATIENT INFORMATION Patient s Legal Name: Date of Today s Visit: Social Security # Date of Birth:
1001 Medical Plaza Dr. The Woodlands, TX 77380 www.woodlandsretina.com Tel: 281-367-9700 Fax: 281-367-9701 PATIENT INFORMATION Patient s Legal Name: Date of Today s Visit: Social Security # Date of Birth:
Phone: (512) Fax: (512)
 Fax: (512)") Phone: (512) 732 2774 Fax: (512) 329 6871 NEW PATIENT INFORMATION Patient Name DOB Age SSN Today s Date Gender Single Married Widowed Divorced Address/City/State/Zip Email: Cell phone Occupation (if minor,
Phone: (512) 732 2774 Fax: (512) 329 6871 NEW PATIENT INFORMATION Patient Name DOB Age SSN Today s Date Gender Single Married Widowed Divorced Address/City/State/Zip Email: Cell phone Occupation (if minor,
PATIENT INFORMATION FORM - DIABETES
 PATIENT INFORMATION FORM - DIABETES PATIENT NAME: DATE OF BIRTH / / (mm/dd/yr) SOCIAL SECURITY NO - - ADDRESS HOME PHONE: ( ) CELL PHONE: ( ) WORK PHONE: ( ) EMPLOYER EMAIL: MARITAL STATUS S M W D SEP
PATIENT INFORMATION FORM - DIABETES PATIENT NAME: DATE OF BIRTH / / (mm/dd/yr) SOCIAL SECURITY NO - - ADDRESS HOME PHONE: ( ) CELL PHONE: ( ) WORK PHONE: ( ) EMPLOYER EMAIL: MARITAL STATUS S M W D SEP
TEXT YES VOICE YES PHONE NUMBER PHONE NUMBER
 Dr. Gann's Diet of Hope Name: D.O.B To allow patients to easily access their statements and communicate with Providers we are glad to provide you access to our Patient Portal. Please provide your email
Dr. Gann's Diet of Hope Name: D.O.B To allow patients to easily access their statements and communicate with Providers we are glad to provide you access to our Patient Portal. Please provide your email
2014 Patient Information
 2014 Patient Information Last Name: First Name: Date of Birth: Telephone #: Address: City, State, Zip: Employed Retired Disabled Employer: Telephone #: Primary Care Physician Name: Primary Care Physician
2014 Patient Information Last Name: First Name: Date of Birth: Telephone #: Address: City, State, Zip: Employed Retired Disabled Employer: Telephone #: Primary Care Physician Name: Primary Care Physician
Please bring the medications you are currently taking. If you had x- rays made, please bring the films with you when you come to the office.
 Dear Patient: We would like to take this opportunity to thank you for choosing our office for your urologic care and to welcome you to our office. We are pleased that you have chosen us to provide you
Dear Patient: We would like to take this opportunity to thank you for choosing our office for your urologic care and to welcome you to our office. We are pleased that you have chosen us to provide you
Patient Registration Form
 Arizona Retina Institute Patient Registration Form Patientʼs Name:" " " " " " " Todayʼs Date:" /" / Patientʼs Social Security#" " " " " Date of Birth:" /" / Gender: Male " Female Marital Status: Single
Arizona Retina Institute Patient Registration Form Patientʼs Name:" " " " " " " Todayʼs Date:" /" / Patientʼs Social Security#" " " " " Date of Birth:" /" / Gender: Male " Female Marital Status: Single
INFECTIOUS DISEASE SERVICES OF GEORGIA, P.C. ROSWELL CUMMING JOHNS CREEK REGISTRATION FORM
 INFECTIOUS DISEASE SERVICES OF GEORGIA, P.C. REGISTRATION FORM Information provided on this form is considered protected health information and is protected by Federal and State Privacy Regulations. PLEASE
INFECTIOUS DISEASE SERVICES OF GEORGIA, P.C. REGISTRATION FORM Information provided on this form is considered protected health information and is protected by Federal and State Privacy Regulations. PLEASE
Social Security No: Home Phone: _. Employer: Work Phone: _. Employer Address: Occupation: _. Spouse/Parent Name: Phone No: _
 THE NATIONAL RETINA INSTITUTE LEADERS IN THE TREATMENT OF RETINAL DISEASES Patient Information Form Patient Name: Date of Birth: -,--I _----'--/ Age: Social Security No: Home Phone: _ Street Address: --------------------------------------
THE NATIONAL RETINA INSTITUTE LEADERS IN THE TREATMENT OF RETINAL DISEASES Patient Information Form Patient Name: Date of Birth: -,--I _----'--/ Age: Social Security No: Home Phone: _ Street Address: --------------------------------------
PATIENT REGISTRATION INFORMATION
 COLUMBIADOCTORS OPHTHALMOLOGY Edward S. Harkness Eye Institute - 635 W. 165 th Street, New York, NY 10032 880 3 rd Avenue 2 nd Floor, New York, NY 10022 Morgan Stanley Children s Hospital of New York 3959
COLUMBIADOCTORS OPHTHALMOLOGY Edward S. Harkness Eye Institute - 635 W. 165 th Street, New York, NY 10032 880 3 rd Avenue 2 nd Floor, New York, NY 10022 Morgan Stanley Children s Hospital of New York 3959
Secondary Insurance Co. Name & Address: Subscriber s Name: Subscriber Soc. Sec. No. Group number:
 M a u r i c i o R o n d e r o s, D D S, M S, M P H I. PATIENT INFORMATION: Last Name: First Name: MI: Mr. Mrs. Ms. Male Female Birth date (M/D/Y): Marital status: Dr. Other: Address: City, State: Zip:
M a u r i c i o R o n d e r o s, D D S, M S, M P H I. PATIENT INFORMATION: Last Name: First Name: MI: Mr. Mrs. Ms. Male Female Birth date (M/D/Y): Marital status: Dr. Other: Address: City, State: Zip:
**The Dermatology Clinic sends all appointment reminders via text**
 PATIENT INITIAL EVALUATION INFORMATION (Adult) DATE Patient Name Date of Birth / / First Middle Last Month Day Year Mailing Address Street City State Zip Home Phone Work Phone Cell Phone **The Dermatology
PATIENT INITIAL EVALUATION INFORMATION (Adult) DATE Patient Name Date of Birth / / First Middle Last Month Day Year Mailing Address Street City State Zip Home Phone Work Phone Cell Phone **The Dermatology
INSTRUCTIONS. Once you complete the forms, save the file to your desktop for your records, then attach in an to:
 INSTRUCTIONS For your convenience you can fill out the following forms on your computer if you have Adobe Acrobat Reader installed. Fields are highlighted in blue. Use the tab key to move from field to
INSTRUCTIONS For your convenience you can fill out the following forms on your computer if you have Adobe Acrobat Reader installed. Fields are highlighted in blue. Use the tab key to move from field to
RESPONSIBLE PARTY DEMOGRAPHIC INFORMATION
 BRYAN LEATHERMAN, M.D. PATIENT DEMOGRAP H I C INFORMATION Last Name First Name Middle Preferred Name Maiden Prefix Suffix DOB Sex SSN Ethnicity Marital Status Driver s License # Primary Language English
BRYAN LEATHERMAN, M.D. PATIENT DEMOGRAP H I C INFORMATION Last Name First Name Middle Preferred Name Maiden Prefix Suffix DOB Sex SSN Ethnicity Marital Status Driver s License # Primary Language English
Marietta Podiatry Group Patient Registration Form
 Marietta Podiatry Group Patient Registration Form CHART # 1. Patient Information (Please include all information as shown on insurance card.) Patient s Last Name Patient s First Name Date of Birth 2 Gender:
Marietta Podiatry Group Patient Registration Form CHART # 1. Patient Information (Please include all information as shown on insurance card.) Patient s Last Name Patient s First Name Date of Birth 2 Gender:
Borland-Groover Clinic PATIENT GENERATED MEDICAL HISTORY Name: DOB: Primary Care Physician: Pharmacy: Pharmacy Phone #:
 PATIENT GENERATED MEDICAL HISTORY Name: DOB: Email: Primary Care Physician: Referring: Pharmacy: Pharmacy Phone #: Place Sticker Here Directions: Please circle any of the following you have personally
PATIENT GENERATED MEDICAL HISTORY Name: DOB: Email: Primary Care Physician: Referring: Pharmacy: Pharmacy Phone #: Place Sticker Here Directions: Please circle any of the following you have personally
EMERGENCY CONTACT INFORMATION PATIENT EMPLOYER INFORMATION GUARANTOR / POLICY HOLDER INFORMATION INSURANCE INFORMATION
 Physician Name: Kyle F. Dickson, M.D. PATIENT DEMOGRAPHIC INFORMATION SHEET Last Name First Name Middle Social Security No. of Birth Age Male or Female (Please circle one) Marital Status: M S W D (Please
Physician Name: Kyle F. Dickson, M.D. PATIENT DEMOGRAPHIC INFORMATION SHEET Last Name First Name Middle Social Security No. of Birth Age Male or Female (Please circle one) Marital Status: M S W D (Please
PATIENT REGISTRATION FORM
 PATIENT REGISTRATION FORM PATIENT INFORMATION Name: Date of Birth: Age: Address : Social Security #: City: Sex: Marital Status: State: Zip: Language: Pt Declines Home Phone#: Race: Pt Declines Work Phone#:
PATIENT REGISTRATION FORM PATIENT INFORMATION Name: Date of Birth: Age: Address : Social Security #: City: Sex: Marital Status: State: Zip: Language: Pt Declines Home Phone#: Race: Pt Declines Work Phone#:
Birmingham Internal Medicine Associates, PC
 Birmingham Internal Medicine Associates, PC Medical History Form Date: Who referred you? Name: Date of Birth: Race (circle one) : *American Indian/Alaskan Native * Asian * Black/African American * Hawaiian/Pacific
Birmingham Internal Medicine Associates, PC Medical History Form Date: Who referred you? Name: Date of Birth: Race (circle one) : *American Indian/Alaskan Native * Asian * Black/African American * Hawaiian/Pacific
Welcome to Family Tree Dental Care Midway Rd., Ste 106A Farmers Branch, TX 75244
 Patient Information: Patient s Name: Address: City, Zip Code: Email address: Sex: M/F SSN: Date of Birth: Age: Marital Status: Home Phone: Cell Phone: Work Phone: Responsible for Account/Subscriber/Guardian
Patient Information: Patient s Name: Address: City, Zip Code: Email address: Sex: M/F SSN: Date of Birth: Age: Marital Status: Home Phone: Cell Phone: Work Phone: Responsible for Account/Subscriber/Guardian
KNIGHTSBRIDGE INTERNAL MEDICINE & CARDIOLOGY, INC. New and Current Patient Information Sheet
 KNIGHTSBRIDGE INTERNAL MEDICINE & CARDIOLOGY, INC. New and Current Patient Information Sheet PATIENT INFORMATION Name: (First)(MI) (Last)_Date: _ Date of Birth Age Sex: M F Marital Status: S M W D Race:
KNIGHTSBRIDGE INTERNAL MEDICINE & CARDIOLOGY, INC. New and Current Patient Information Sheet PATIENT INFORMATION Name: (First)(MI) (Last)_Date: _ Date of Birth Age Sex: M F Marital Status: S M W D Race:
12319 N Mopac Expy, Bldg C, Suite #300, Austin, Tx (512) NEW PATIENT INFORMATION P L E A S E P R I N T
 NEW PATIENT INFORMATION P L E A S E P R I N T") NEW PATIENT INFORMATION P L E A S E P R I N T Name: First Middle Last Date: Address: Street City State Zip ( ) ( ) ( ) / / - - Home Telephone Cell# Work Telephone: Patient Date of Birth AGE Patient SSN
NEW PATIENT INFORMATION P L E A S E P R I N T Name: First Middle Last Date: Address: Street City State Zip ( ) ( ) ( ) / / - - Home Telephone Cell# Work Telephone: Patient Date of Birth AGE Patient SSN
Thank You, Colorado Kidney Care Team. Review of systems
 1 Welcome to Colorado Kidney Care! This packet contains important information to ensure a productive and thorough visit. Please take the time to complete these forms in as much detail as possible. Please
1 Welcome to Colorado Kidney Care! This packet contains important information to ensure a productive and thorough visit. Please take the time to complete these forms in as much detail as possible. Please
Obstetrics and Gynecology 50 Medical Drive Suite 100 (806) Borger, TX
 Borger, TX") PATIENT INFORMATION First Name MI Last Name Date of Birth Age: Social Security # Race Ethnicity: Sex: Female / Male Marital Status: S M W D Email Address: Mailing Address City State Zip Physical Address
PATIENT INFORMATION First Name MI Last Name Date of Birth Age: Social Security # Race Ethnicity: Sex: Female / Male Marital Status: S M W D Email Address: Mailing Address City State Zip Physical Address
2790 SW Wilshire Blvd., Burleson, TX Phone: Fax: Dr. Nathan Berry Dr. Adam Stewart Dr.
 2790 SW Wilshire Blvd., Burleson, TX 76028 Phone: 817-484- 2020 Fax: 817-484- 2015 Dear: Thank you for choosing Berry Stewart Eye Center for your eye care. To prepare for your upcoming appointment, please
2790 SW Wilshire Blvd., Burleson, TX 76028 Phone: 817-484- 2020 Fax: 817-484- 2015 Dear: Thank you for choosing Berry Stewart Eye Center for your eye care. To prepare for your upcoming appointment, please
PATIENT INFORMATION. Patient s Last Name First M.I. Home Phone Work Phone Cell Phone Home Address City State Zip Address
 PATIENT INFORMATION Patient s Last Name First M.I. Home Phone Work Phone Cell Phone Home Address City State Zip E-Mail Address Social Security # Sex Marital Status Patient s Date of Birth Age Spouse s
PATIENT INFORMATION Patient s Last Name First M.I. Home Phone Work Phone Cell Phone Home Address City State Zip E-Mail Address Social Security # Sex Marital Status Patient s Date of Birth Age Spouse s
Patient Registration Form
 Patient Registration Form Appointment Date/Time Appointment Reason First Name & MI Date of Birth Patient Information Last Name Address Social Security # City State Zip Home Phone Work Phone Cell Phone
Patient Registration Form Appointment Date/Time Appointment Reason First Name & MI Date of Birth Patient Information Last Name Address Social Security # City State Zip Home Phone Work Phone Cell Phone
Georgia Foot & Ankle
 Georgia Foot & Ankle PLEASE PRINT CLEARLY Today s Date / / Name Date of birth / / First MI Last SSN Marital Status M S D W Age Weight Height Male Female Address City State Zip Phone (Home) (Work) (Cell)
Georgia Foot & Ankle PLEASE PRINT CLEARLY Today s Date / / Name Date of birth / / First MI Last SSN Marital Status M S D W Age Weight Height Male Female Address City State Zip Phone (Home) (Work) (Cell)
PATIENT INFORMATION. Home Address: Phone Numbers: Primary Work . Whom may we thank for referring you? EMPLOYMENT INFORMATION. Employer: Position:
 Patient Registration Form Rev. 2017 PATIENT INFORMATION Patient Name: Today s Social Security Number: (Last 4 Digits) Birth Gender: Male Female Marital Status: Married Single Widowed Divorced Home Address:
Patient Registration Form Rev. 2017 PATIENT INFORMATION Patient Name: Today s Social Security Number: (Last 4 Digits) Birth Gender: Male Female Marital Status: Married Single Widowed Divorced Home Address:
Secondary Insurance Carrier Name of Insured Member ID# Group # Birthdate of Insured / / Employer SS # of Insured / / Relation to Insured
 PATIENT MEDICAL & PAYMENT INFORMATION SHEET TODAY S DATE Patient Name Date of Birth: / / Age Local Address Social Security # / / City State Zip Code Home Phone # ( ) - Permanent Address Cell Phone # (
PATIENT MEDICAL & PAYMENT INFORMATION SHEET TODAY S DATE Patient Name Date of Birth: / / Age Local Address Social Security # / / City State Zip Code Home Phone # ( ) - Permanent Address Cell Phone # (
Patient Information Please print legibly and complete all information. If a prompt does not apply, please draw a line through the space provided.
 Patient Information Please print legibly and complete all information. If a prompt does not apply, please draw a line through the space provided. Last Name: First Name: Primary Care Physician: Referring
Patient Information Please print legibly and complete all information. If a prompt does not apply, please draw a line through the space provided. Last Name: First Name: Primary Care Physician: Referring
MICHAEL K. BLOCK, DPM, LLC PATIENT FINANCIAL POLICY
 MICHAEL K. BLOCK, DPM, LLC PATIENT FINANCIAL POLICY Dear Patient, Thank you for choosing Michael K. Block, DPM, LLC for your podiatric needs. We value our relationship with you and would like to tell you
MICHAEL K. BLOCK, DPM, LLC PATIENT FINANCIAL POLICY Dear Patient, Thank you for choosing Michael K. Block, DPM, LLC for your podiatric needs. We value our relationship with you and would like to tell you
Patient Information. Patient Name (First, Middle Initial, Last): Mailing Address (include City, State, and zip):
: Mailing Address (include City, State, and zip):") Patient Information Patient Name (First, Middle Initial, Last): Mailing Address (include City, State, and zip): Street Address (if different than mailing): Home Phone: Work Phone: OK to Leave Message at
Patient Information Patient Name (First, Middle Initial, Last): Mailing Address (include City, State, and zip): Street Address (if different than mailing): Home Phone: Work Phone: OK to Leave Message at
New Patient Packet Please print and complete the following 6 pages. Bring the completed forms to your scheduled appointment. Thank you!
 New Patient Packet Please print and complete the following 6 pages. Bring the completed forms to your scheduled appointment. Thank you! Washington Ear, Nose and Throat 80 Landings Drive, Suite 207 Washington,
New Patient Packet Please print and complete the following 6 pages. Bring the completed forms to your scheduled appointment. Thank you! Washington Ear, Nose and Throat 80 Landings Drive, Suite 207 Washington,