Important Questions Answers Why this Matters:
|
|
|
- Emerald Perkins
- 5 years ago
- Views:
Transcription
1 Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/ /31/2018 St. Francis Plan: SSM Health Coverage for: Individual, +1, Family Plan Type: PPO The Summary of Benefits and Coverage (SBC) document will help you choose a health plan. The SBC shows you how you and the plan would share the cost for covered health care services. NOTE: Information about the cost of this plan (called the premium) will be provided separately. This is only a summary. For more information about your coverage, or to get a copy of the complete terms of coverage, visit MyHR on the SSM Health intranet site or For general definitions of common terms, such as allowed amount, balance billing, coinsurance, copayment, deductible, provider, or other underlined terms see the Glossary. You can view the Glossary at or call (660) to request a copy. Important Questions Answers Why this Matters: What is the overall deductible? Are there services covered before you meet your deductible? Are there other deductibles for specific services? What is the out-of-pocket limit for this plan? 3 options available: $300/person or $600/family $500/person or $1,000/family $1,000/person or $2,000/family Does not apply to preventive services or services that require a co-payment. Yes. No. Limits vary for each of the 3 options For participating providers: $2,000/person or $4,000/family $3,500/person or $7,000/family $5,000/person or $10,000/family Non-participating providers: $3,000/person or $6,000/family $5,000/person or $10,000/family $7,500/person or $15,000/family Prescription drugs all plans: $1,600/person or $3,200/family Generally, you must pay all of the costs from providers up to the deductible amount before this plan begins to pay. If you have other family members on the plan, each family member must meet their own individual deductible until the total amount of deductible expenses paid by all family members meets the overall family deductible. Preventive care and services requiring a co-payment are covered before you meet your deductible. You do not have to meet deductibles for specific services. The out-of-pocket limit is the most you could pay in a year for covered services. If you have other family members in this plan, they have to meet their own out-of-pocket limits until the overall family out-of-pocket limit has been met. 1 of 8
2 What is not included in the out-of-pocket limit? Will you pay less if you use a network provider Do you need a referral to see a specialist Copayments for certain services, premiums, balance-billing charges, and health care this plan doesn t cover. Yes. For a list of preferred providers, visit MyHR on the SSM Health intranet site or medical-benefits-plans/st-francis. No. Even though you pay these expenses, they don t count toward the out of pocket limit This plan uses a provider network. You will pay less if you use a provider in the plan s network. You will pay the most if you use an out-of-network provider, and you might receive a bill from a provider for the difference between the provider s charge and what your plan pays (balance billing). Be aware, your network provider might use an out-of-network provider for some services (such as lab work). Check with your provider before you get services. You can see the specialist you choose without a referral. All coinsurance costs shown in this chart are after your deductible has been met, if a deductible applies. Common If you visit a health care provider s office or clinic Primary care visit to treat an injury or illness Specialist visit Preventive care/screening/ immunization $20 co-payment ($300 Plan) $25 co-payment ($500 & $1,000 Plans) $25 co-payment ($300 Plan) $30 co-payment ($500 & $1,000 Plans) No Charge No Charge Not covered Excludes any service that incurs a separate billing charge (i.e. billings from a lab, radiologist, etc.) Excludes any service that incurs a separate billing charge. Examples: billings from a lab, radiologist, etc. You may have to pay for services that are not preventive. Check what your plan will pay. One visit/screening per year. If you have a test Diagnostic test (xray, blood work) Imaging (CT/PET scans, MRIs) 2 of 8
3 Common If you need drugs to treat your illness or condition More information about prescription drug coverage is available at (Tier 1) Generic drugs and some low cost brands (Tier 2) Formulary and some high cost generics (Tier 3) Non formulary brands and high cost generics $12 co-payment/ $30 co-payment/ $35 co-payment/ $87.50 co-payment/ $70 co-payment/ $175 co-payment/ $12 co-payment/ $30 co-payment/ $35 co-payment/ $87.50 co-payment/ $70 co-payment/ $175 co-payment/ Not Covered Same as above Same as above All plans include an out-of-pocket maximum of $1,600/person or $3,200/family for prescription drugs. Covers up to a 30-day supply (retail prescription); day supply (mail order and retail prescription) Some drugs may require preauthorization. If the necessary preauthorization is not obtained, the drug may not be covered. You must use a participating Navitus pharmacy or the drug will not be covered. The prescription drug out-of-pocket maximum is separate from the medical plan out-of-pocket maximum. If you have outpatient surgery If you need immediate medical attention Facility fee (e.g., ambulatory surgery center) Physician/surgeon fees Emergency room care Physician/surgeon fees After deductible $200 co-payment, then 10% coinsurance 10% coinsurance $200 co-payment, Then 10% coinsurance 10% coinsurance $300 co-payment, then $200 co-payment, then 10% coinsurance 10% coinsurance Preauthorization required or a penalty will apply. Co-payment is waived if admitted. $200 co-payment, then 70% of charges if NOT a medical emergency. Emergency medical transportation 3 of 8
4 Common If you need immediate medical attention Urgent care $40 co-payment Not covered, unless medical emergency Not covered, unless medical emergency Physical exams for employment, school and recreation are not covered. If you have a hospital stay Facility fee (e.g., hospital room) Physician/surgeon fees $500 co-payment per day for 3 days, then Preauthorization required or a penalty will apply. Outpatient services $20 co-payment ($300 Plan Only) $25 co-payment ($500/$1000 Plans) $25 co-payment ($300 Plan Only) $30 co-payment ($500/$1000 Plans) Includes an individual session, a group or family therapy session or a brief office visit to adjust medication. If you need mental health, behavioral health, or substance abuse services Inpatient services Same as hospital stay facility and physician fees. Same as hospital stay facility and physician fees. Same as hospital stay facility and physician fees. Preauthorization required or a penalty will apply. Residential care services for mental health or substance abuse treatment are excluded. Partial Hospitalization Intensive Outpatient, or Partial Day program Preauthorization required or a penalty will apply. These services are typically provided in a hospital. 4 of 8
5 Common Office visits If you are pregnant Childbirth/delivery professional services Childbirth/delivery facility services 20% at coinsurance $500 co-payment per day for 3 days, then Maternity care may include tests and services described elsewhere in the SBC (i.e. ultrasound). Home health care Limited to 100 visits per year. Preauthorization is required or a penalty will apply. If you need help recovering or have other special health needs Rehabilitation services Habilitation services Chiropractic Services Same as above Same as above Same as above Assumes services are provided on an outpatient basis. Preauthorization is required or a penalty will apply. Same as above Same as above Same as above Assumes services are provided on an outpatient basis. Preauthorization is required or a penalty will apply. Same as above Same as above Same as above Skilled nursing care Same as above Same as above Same as above Limited to 20 visits per year. Limited to 70 visits per year. Preauthorization is required or a penalty will apply. Durable medical equipment Same as above Same as above Same as above Preauthorization required for rental or purchases over $500. Hospice services Preauthorization is required or a penalty will apply. 5 of 8
6 Common If your child needs dental or eye care Children s eye exam Not covered Not covered Not Covered None Children s glasses Not covered Not covered Not Covered None Children s dental check-up Not covered Not covered Not Covered None Excluded Services & Other Covered Services: Services Your Plan Generally Does NOT Cover (Check your policy or plan document for more information and a list of any other excluded services.) Artificial insemination or in vitro fertilization Cosmetic surgery Non-emergency care when travelling outside the U.S. Nutritional or Dietary Supplements Routine dental care Routine eye care Routine foot care Services, pharmaceuticals or supplies that are not medically necessary or meet plan provisions Other Covered Services (Limitations may apply to these services. This isn t a complete list. Please see your plan document.) Dietary counseling services Dental care as treatment for accidental injury to the jaw and/or natural teeth Hearing aids or cochlear implant when patient s condition meets specific criteria Weight Loss Programs when patients condition meets certain medical criteria Your Rights to Continue Coverage: There are agencies that can help if you want to continue your coverage after it ends. For more information on your rights to continue coverage, contact the COBRA Plan Administrator at You may also contact your state insurance department, the U.S. Department of Labor, Employee Benefits Security Administration at or or the U.S. Department of Health and Human Services at x61565 or Other coverage options may be available to you too, including buying individual insurance coverage through the Health Insurance Marketplace. For more information about the Marketplace, visit or call Your Grievance and Appeals Rights: There are agencies that can help if you have a complaint against your plan for a denial of a claim. This complaint is called a grievance or appeal. For more information about your rights, look at the explanation of benefits you will receive for that medical claim. Your plan documents also provide complete information to submit a claim, appeal, or a grievance for any reason to your plan. For more information about your rights, this notice, or assistance, contact SSM Health Medical Management at or the Department of Labor s Employee Benefit Security Administration at EBSA (3272) or Additionally, for Missouri and 6 of 8
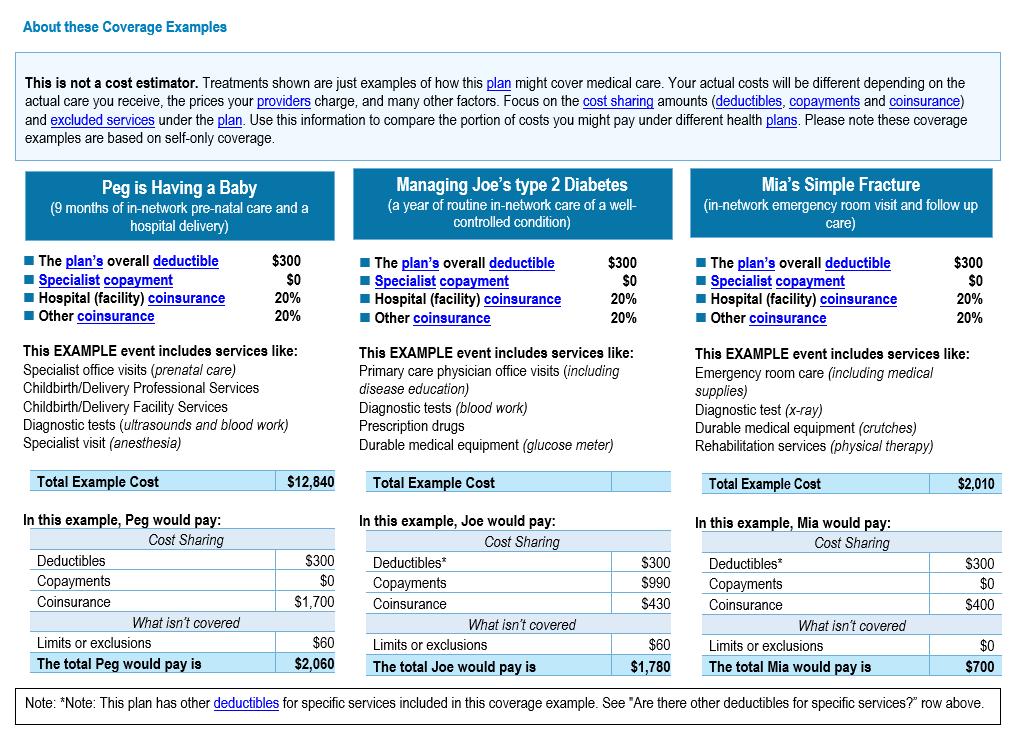
7 Illinois residents, a consumer assistance program can help you file your appeal details available at and Does this plan provide Minimum Essential Coverage? Yes. If you don t have Minimum Essential Coverage for a month, you ll have to make a payment when you file your tax return unless you qualify for an exemption from the requirement that you have health coverage for that month. Does this plan meet Minimum Value Standards? Yes. If your plan doesn t meet the Minimum Value Standards, you may be eligible for a premium tax credit to help you pay for a plan through the Marketplace. Language Access Services: CoreSource provides free language assistance services to help you communicate with us in your preferred language for health care. Ask your health care professional or call: ( ) Español CoreSource proporciona servicios de asistencia de idiomas para ayudarle a comunicarse con nosotros en su idioma preferido para obtener atención médica. Pregúntele a su profesional de atención médica o llame al: ( ) 简体中文 CoreSource 提供免费语言协助服务, 帮助您以母语与我们沟通健康护理 请咨询您的健康护理专员, 或拨打 :( ) To see examples of how this plan might cover costs for a sample medical situation, see the next section. 7 of 8
8 8 of 8
Important Questions Answers Why this Matters:
 Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/2018 12/31/2018 St.Mary sgood Plan: SSM Health Coverage for: Family Plan Type: PPO The
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/2018 12/31/2018 St.Mary sgood Plan: SSM Health Coverage for: Family Plan Type: PPO The
$300 person/$900 family
 Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/2019 12/31/2019 AeroVironment, Inc. Employee Benefit Plan: PPO Option Coverage for: Single
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/2019 12/31/2019 AeroVironment, Inc. Employee Benefit Plan: PPO Option Coverage for: Single
01/01/ /31/2019 UMR: PALO PINTO GENERAL HOSPITAL:
 Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/2019 12/31/2019 UMR: PALO PINTO GENERAL HOSPITAL: 7670-00-160036 001 Coverage for: Individual
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/2019 12/31/2019 UMR: PALO PINTO GENERAL HOSPITAL: 7670-00-160036 001 Coverage for: Individual
01/01/ /31/2018 FLORIDA SCHOOLS HEALTH INSURANCE PROG:
 Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/2018 12/31/2018 FLORIDA SCHOOLS HEALTH INSURANCE PROG: 7670-00-410536 010 020 Coverage
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/2018 12/31/2018 FLORIDA SCHOOLS HEALTH INSURANCE PROG: 7670-00-410536 010 020 Coverage
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/ /31/2019
 Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/2019-12/31/2019 Ensign: Copay 5000 (Collective Health) Coverage for: Individual or Family
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/2019-12/31/2019 Ensign: Copay 5000 (Collective Health) Coverage for: Individual or Family
Important Questions Answers Why This Matters: Network providers $500 Individual / $1,500 Family Non-Network providers $750 Individual / $2,250 Family
 Summary of Benefits and Coverage: What this Plan Covers & What You Pay for Covered Services Coverage Period: 07/01/2017-06/30/2018 GDS Associates Inc.: PPO Plan Coverage for: Individual/Family Plan Type:
Summary of Benefits and Coverage: What this Plan Covers & What You Pay for Covered Services Coverage Period: 07/01/2017-06/30/2018 GDS Associates Inc.: PPO Plan Coverage for: Individual/Family Plan Type:
Out-of-Network: Individual: $2,000 Family: $4,000. Yes. Preventive care services are covered before you meet your deductible.
 Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/2018 12/31/2018 Bartholomew Consolidated School Corp: Option 2 Coverage for: Individual
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/2018 12/31/2018 Bartholomew Consolidated School Corp: Option 2 Coverage for: Individual
Summary of Benefits and Coverage:
 Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 07/01/2017 06/30/2018 Johns Hopkins Student Health Program Coverage for: Individual and Family
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 07/01/2017 06/30/2018 Johns Hopkins Student Health Program Coverage for: Individual and Family
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/ /31/2019
 Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/2019-12/31/2019 The Home Depot Medical Plan: Kaiser Permanente California: Plus Plan Coverage
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/2019-12/31/2019 The Home Depot Medical Plan: Kaiser Permanente California: Plus Plan Coverage
Coverage for: Family/Individual Plan Type: PPO
 Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 03/01/2018 2/28/2019 Tri-Eagle Sales: Tri-Eagle Standard Option Coverage for: Family/Individual
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 03/01/2018 2/28/2019 Tri-Eagle Sales: Tri-Eagle Standard Option Coverage for: Family/Individual
Bronze 60 HMO. Individual & Family Plan Summary of Benefits and Coverage
 Bronze 60 HMO Individual & Family Plan Summary of Benefits and Coverage DMHC Approved Date 08/25/2017 Rev. 04/03/2018 Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered
Bronze 60 HMO Individual & Family Plan Summary of Benefits and Coverage DMHC Approved Date 08/25/2017 Rev. 04/03/2018 Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered
Coverage for: Individual / Family Plan Type: HDHP
 Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 1/1/2019 12/31/2019 : JLL All plans offered and underwritten by Kaiser Foundation Health Plan
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 1/1/2019 12/31/2019 : JLL All plans offered and underwritten by Kaiser Foundation Health Plan
Bronze 60 HMO. Employer Group Summary of Benefits and Coverage
 Bronze 60 HMO Employer Group Summary of Benefits and Coverage DMHC Approved Date 08/25/2017 Rev. 04/03/2018 Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage
Bronze 60 HMO Employer Group Summary of Benefits and Coverage DMHC Approved Date 08/25/2017 Rev. 04/03/2018 Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: Beginning on or after 1/1/2019
 Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: Beginning on or after 1/1/2019 Kalamazoo College, G-1013: Orange Plan Coverage for: Covered
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: Beginning on or after 1/1/2019 Kalamazoo College, G-1013: Orange Plan Coverage for: Covered
Silver 70 HMO. Individual & Family Plan Summary of Benefits and Coverage
 Silver 70 HMO Individual & Family Plan Summary of Benefits and Coverage DMHC Approved Date 08/25/2017 Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage
Silver 70 HMO Individual & Family Plan Summary of Benefits and Coverage DMHC Approved Date 08/25/2017 Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/ /31/2018
 The Summary of Benefits and Coverage (SBC) document will help you choose a health plan. The SBC shows you how you and the plan would share the cost for covered health care services. NOTE: Information about
The Summary of Benefits and Coverage (SBC) document will help you choose a health plan. The SBC shows you how you and the plan would share the cost for covered health care services. NOTE: Information about
Coverage for: Single, Family,& Other Plan Type: HMO
 Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 1/1/2018 12/31/2018 MercyCare Health Plans: MercyCare Gold Option A Coverage for: Single, Family,&
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 1/1/2018 12/31/2018 MercyCare Health Plans: MercyCare Gold Option A Coverage for: Single, Family,&
Deductible- Generally, you must pay all of the costs from providers up to the deductible amount before this plan begins to pay.
 Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 1/1/2019 12/31/2019 MercyCare Health Plans: MercyCare Bronze Option B Coverage for: Single,
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 1/1/2019 12/31/2019 MercyCare Health Plans: MercyCare Bronze Option B Coverage for: Single,
Coverage for: Family Plan Type: DHMO
 Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 10/01/2018-09/30/2019 Kaiser Permanente: DHMO 500 Coverage for: Family Plan Type: DHMO The Summary
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 10/01/2018-09/30/2019 Kaiser Permanente: DHMO 500 Coverage for: Family Plan Type: DHMO The Summary
Coverage Period: Beginning on or after 01/01/2018 Coverage for: Individual + Family Plan Type: PPO
 Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Thrifty White Stores, Inc.- HSA PLAN Coverage Period: Beginning on or after 01/01/2018 Coverage for: Individual
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Thrifty White Stores, Inc.- HSA PLAN Coverage Period: Beginning on or after 01/01/2018 Coverage for: Individual
Are there services covered before you meet your deductible? Yes, Preventive Care
 Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Univera Healthcare: Essential Plan 2 Plus Vision and Dental Coverage Period: 01/01/2019-12/31/2019 Coverage for:
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Univera Healthcare: Essential Plan 2 Plus Vision and Dental Coverage Period: 01/01/2019-12/31/2019 Coverage for:
Gold 80 HMO. Employer Group Summary of Benefits and Coverage
 Gold 80 HMO Employer Group Summary of Benefits and Coverage DMHC Approved Date 08/25/2017 Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: Beginning
Gold 80 HMO Employer Group Summary of Benefits and Coverage DMHC Approved Date 08/25/2017 Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: Beginning
Coverage for: Family Plan Type: HMO
 Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 10/01/2017-09/30/2018 Kaiser Permanente: Traditional Plan $30 OV, $10-30 Rx Coverage for: Family
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 10/01/2017-09/30/2018 Kaiser Permanente: Traditional Plan $30 OV, $10-30 Rx Coverage for: Family
Coverage Period: 01/01/ /31/2018 A nonprofit independent licensee of the BlueCross BlueShield Association
 Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Excellus BCBS: Essential Plan 2 Coverage Period: 01/01/2018-12/31/2018 A nonprofit independent licensee of the
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Excellus BCBS: Essential Plan 2 Coverage Period: 01/01/2018-12/31/2018 A nonprofit independent licensee of the
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 7/01/ /31/2018
 Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 7/01/2018-12/31/2018 The Home Depot Medical Plan: Cigna USVI OAP Coverage for: Associate + Family
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 7/01/2018-12/31/2018 The Home Depot Medical Plan: Cigna USVI OAP Coverage for: Associate + Family
Coverage for: Individual/Family Plan Type: PPO
 The Summary of Benefits and Coverage (SBC) document will help you choose a health plan. The SBC shows you how you and the plan would share the cost for covered health care services. NOTE: Information about
The Summary of Benefits and Coverage (SBC) document will help you choose a health plan. The SBC shows you how you and the plan would share the cost for covered health care services. NOTE: Information about
UMR: DIGNITY HEALTH: National PPO
 Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/2018-12/31/18 UMR: DIGNITY HEALTH: 7670-00-413007 001 National PPO Coverage for: Individual
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/2018-12/31/18 UMR: DIGNITY HEALTH: 7670-00-413007 001 National PPO Coverage for: Individual
Important Questions Answers Why This Matters: What is the overall deductible?
 Summary of Benefits and Coverage: What this Plan Covers & What You Pay for Covered Services Coverage Period: 09/01/2017-08/31/2018 Elim Christian Services: PPO Plan Coverage for: Individual/Family Plan
Summary of Benefits and Coverage: What this Plan Covers & What You Pay for Covered Services Coverage Period: 09/01/2017-08/31/2018 Elim Christian Services: PPO Plan Coverage for: Individual/Family Plan
Coverage for: Individual/Family Plan Type: PPO
 The Summary of Benefits and Coverage (SBC) document will help you choose a health plan. The SBC shows you how you and the plan would share the cost for covered health care services. NOTE: Information about
The Summary of Benefits and Coverage (SBC) document will help you choose a health plan. The SBC shows you how you and the plan would share the cost for covered health care services. NOTE: Information about
Coverage for: Individual/Family Plan Type: PPO
 The Summary of Benefits and Coverage (SBC) document will help you choose a health plan. The SBC shows you how you and the plan would share the cost for covered health care services. NOTE: Information about
The Summary of Benefits and Coverage (SBC) document will help you choose a health plan. The SBC shows you how you and the plan would share the cost for covered health care services. NOTE: Information about
Coverage for: Individual + Family Plan Type: PPO
 Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/2019 12/31/2019 UFCW & Participating Employers: Plan JSS2 Coverage for: Individual + Family
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/2019 12/31/2019 UFCW & Participating Employers: Plan JSS2 Coverage for: Individual + Family
Summary of Benefits and Coverage:
 Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 1/1/2018 1/1/2019 Kaiser Foundation Health Plan of Washington Options, Inc.: WCIF Access PPO
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 1/1/2018 1/1/2019 Kaiser Foundation Health Plan of Washington Options, Inc.: WCIF Access PPO
Coverage for: Individual/Family Plan Type: PPO
 The Summary of Benefits and Coverage (SBC) document will help you choose a health plan. The SBC shows you how you and the plan would share the cost for covered health care services. NOTE: Information about
The Summary of Benefits and Coverage (SBC) document will help you choose a health plan. The SBC shows you how you and the plan would share the cost for covered health care services. NOTE: Information about
Page 1 of 6. Important Questions Answers Why This Matters: What is the overall deductible?
 Summary of Bene ts and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/2019 to 12/31/2019 Staff Bene ts Management & Administrators: MEC Enhanced Coverage for:
Summary of Bene ts and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/2019 to 12/31/2019 Staff Bene ts Management & Administrators: MEC Enhanced Coverage for:
Coverage for: Individual/Family Plan Type: PPO
 The Summary of Benefits and Coverage (SBC) document will help you choose a health plan. The SBC shows you how you and the plan would share the cost for covered health care services. NOTE: Information about
The Summary of Benefits and Coverage (SBC) document will help you choose a health plan. The SBC shows you how you and the plan would share the cost for covered health care services. NOTE: Information about
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/ /31/2019
 Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/2019-12/31/2019 The Home Depot Medical Plan: Kaiser Permanente Hawaii: HMO Coverage for:
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/2019-12/31/2019 The Home Depot Medical Plan: Kaiser Permanente Hawaii: HMO Coverage for:
Summary of Benefits and Coverage:
 Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: Beginning on or After 01/01/2018 Aetna Plus Coverage for: Family Plan Type: PPO The Summary
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: Beginning on or After 01/01/2018 Aetna Plus Coverage for: Family Plan Type: PPO The Summary
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period:1/1/19 12/31/19
 Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period:1/1/19 12/31/19 The Health Plan: HMO Bronze Non-Group Coverage for: Individual/Family Plan Type:
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period:1/1/19 12/31/19 The Health Plan: HMO Bronze Non-Group Coverage for: Individual/Family Plan Type:
Coverage for: Individual/Family Plan Type: PPO
 The Summary of Benefits and Coverage (SBC) document will help you choose a health plan. The SBC shows you how you and the plan would share the cost for covered health care services. NOTE: Information about
The Summary of Benefits and Coverage (SBC) document will help you choose a health plan. The SBC shows you how you and the plan would share the cost for covered health care services. NOTE: Information about
What is the overall deductible?
 Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services 88/88/8888 88/88/8888 Robin with HealthPartners:NE WI EZ Empower HSA 3000-100 - Robin broad Coverage for: Single/Family
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services 88/88/8888 88/88/8888 Robin with HealthPartners:NE WI EZ Empower HSA 3000-100 - Robin broad Coverage for: Single/Family
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/ /31/2019
 Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/2019-12/31/2019 The Home Depot Medical Plan: Kaiser Permanente California: Gold HMO Coverage
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/2019-12/31/2019 The Home Depot Medical Plan: Kaiser Permanente California: Gold HMO Coverage
Coverage for: Group Plan Type: HMO
 Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 11/1/2017 11/1/2018 Kaiser Foundation Health Plan of Washington: Shoreline School District Coverage
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 11/1/2017 11/1/2018 Kaiser Foundation Health Plan of Washington: Shoreline School District Coverage
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/2019 to 12/31/2019
 Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/2019 to 12/31/2019 Metromont Corporation Employee Benefit Plan: RBP Plus Plan Coverage
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/2019 to 12/31/2019 Metromont Corporation Employee Benefit Plan: RBP Plus Plan Coverage
Coverage for: Individual/Family Plan Type: PPO
 The Summary of Benefits and Coverage (SBC) document will help you choose a health plan. The SBC shows you how you and the plan would share the cost for covered health care services. NOTE: Information about
The Summary of Benefits and Coverage (SBC) document will help you choose a health plan. The SBC shows you how you and the plan would share the cost for covered health care services. NOTE: Information about
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/ /31/2018
 Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/2018 12/31/2018 County of Butte Health Benefits Plan: PPO Medical Plan E Coverage for:
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/2018 12/31/2018 County of Butte Health Benefits Plan: PPO Medical Plan E Coverage for:
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/ /31/2020
 Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/2019-12/31/2020 HealthPartners:High Deductible Health Plan $4500 HSA Coverage for: All
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/2019-12/31/2020 HealthPartners:High Deductible Health Plan $4500 HSA Coverage for: All
What is the overall deductible? Are there services covered before you meet your deductible? Are there other deductibles for specific services?
 Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services 88/88/8888 88/88/8888 HealthPartners:EZ Empower HSA Embedded 6350-100 - Open Access Coverage for: Single/Family
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services 88/88/8888 88/88/8888 HealthPartners:EZ Empower HSA Embedded 6350-100 - Open Access Coverage for: Single/Family
Summary of Benefits and Coverage:
 Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 1/1/2018 1/1/2019 Kaiser Foundation Health Plan of Washington: Puget Sound Energy, Inc. Coverage
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 1/1/2018 1/1/2019 Kaiser Foundation Health Plan of Washington: Puget Sound Energy, Inc. Coverage
Goldcare ii AT A GLANCE
 2018-2019 Goldcare ii AT A GLANCE This is a summary of drug and health services covered by METROPLUS GOLDCARE II Health Plan October 1, 2018 - September 30, 2019 GOLDCARE II THE HEALTH PLAN FOR DAY CARE
2018-2019 Goldcare ii AT A GLANCE This is a summary of drug and health services covered by METROPLUS GOLDCARE II Health Plan October 1, 2018 - September 30, 2019 GOLDCARE II THE HEALTH PLAN FOR DAY CARE
Goldcare i AT A GLANCE
 2018-2019 Goldcare i AT A GLANCE This is a summary of drug and health services covered by METROPLUS GOLDCARE I Health Plan October 1, 2018 - September 30, 2019 GOLDCARE I THE HEALTH PLAN FOR DAY CARE WORKERS
2018-2019 Goldcare i AT A GLANCE This is a summary of drug and health services covered by METROPLUS GOLDCARE I Health Plan October 1, 2018 - September 30, 2019 GOLDCARE I THE HEALTH PLAN FOR DAY CARE WORKERS
What is the overall deductible? See the Common Medical Events chart below for your costs for services this plan covers.
 The Summary of Benefits and Coverage (SBC) document will help you choose a health plan. The SBC shows you how you and the plan would share the cost for covered health care services. NOTE: Information about
The Summary of Benefits and Coverage (SBC) document will help you choose a health plan. The SBC shows you how you and the plan would share the cost for covered health care services. NOTE: Information about
Coverage for: Individual/Family Plan Type: PPO
 The Summary of Benefits and Coverage (SBC) document will help you choose a health plan. The SBC shows you how you and the plan would share the cost for covered health care services. NOTE: Information about
The Summary of Benefits and Coverage (SBC) document will help you choose a health plan. The SBC shows you how you and the plan would share the cost for covered health care services. NOTE: Information about
You don't have to meet deductibles for specific services.
 Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Excellus BCBS: Excellus BluePPO A nonprofit independent licensee of the BlueCross BlueShield Association The
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Excellus BCBS: Excellus BluePPO A nonprofit independent licensee of the BlueCross BlueShield Association The
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/ /31/2018
 Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/2018 12/31/2018 Moda Health Plan, Inc.: Moda Health Oregon Standard Bronze HSA Plan (Beacon)
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/2018 12/31/2018 Moda Health Plan, Inc.: Moda Health Oregon Standard Bronze HSA Plan (Beacon)
The HPHC Insurance Company PPO
 Massachusetts The HPHC Insurance Company PPO Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/2018 12/31/2018 Coverage for: Individual
Massachusetts The HPHC Insurance Company PPO Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/2018 12/31/2018 Coverage for: Individual
Coverage for: Family Plan Type: HMO
 Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 10/01/2017-09/30/2018 Blue Shield: 30-20%; Rx 9-35 Coverage for: Family Plan Type: HMO The Summary
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 10/01/2017-09/30/2018 Blue Shield: 30-20%; Rx 9-35 Coverage for: Family Plan Type: HMO The Summary
MEBA Medical and Benefits Plan: Medicare Eligible Retiree (>20 + years of Pension Credit) Coverage Period: 01/1/ /31/2018
 Coverage Period: 01/1/ /31/2018") MEBA Medical and Benefits Plan: Medicare Eligible Retiree (>20 + years of Pension Credit) Coverage Period: 01/1/2018 12/31/2018 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage
MEBA Medical and Benefits Plan: Medicare Eligible Retiree (>20 + years of Pension Credit) Coverage Period: 01/1/2018 12/31/2018 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage
Summary of Benefits and Coverage:
 Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 1/1/2018 1/1/2019 Kaiser Foundation Health Plan of Washington: Kitsap County Classic Plan Coverage
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 1/1/2018 1/1/2019 Kaiser Foundation Health Plan of Washington: Kitsap County Classic Plan Coverage
What is the overall deductible? Are there services covered before you meet your deductible? Are there other deductibles for specific services?
 Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services 88/88/8888 88/88/8888 Robin with HealthPartners:NE WI EZ Empower HSA Rx Plus Embedded 2700-80 - Robin broad Coverage
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services 88/88/8888 88/88/8888 Robin with HealthPartners:NE WI EZ Empower HSA Rx Plus Embedded 2700-80 - Robin broad Coverage
Page 1 of 6. Important Questions Answers Why This Matters: What is the overall deductible?
 Summary of Bene ts and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/2019 to 12/31/2019 Staff Bene ts Management & Administrators: MEC Plus Coverage for: Eligible
Summary of Bene ts and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/2019 to 12/31/2019 Staff Bene ts Management & Administrators: MEC Plus Coverage for: Eligible
Trinity Health - Syracuse Essential Excellus BCBS: Signature Hybrid 5
 Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Trinity Health - Syracuse Essential Excellus BCBS: Signature Hybrid 5 Coverage Period: 01/01/2019-12/31/2019
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Trinity Health - Syracuse Essential Excellus BCBS: Signature Hybrid 5 Coverage Period: 01/01/2019-12/31/2019
See Medical SBC. See Medical SBC. See Medical SBC. For network pharmacy providers $2,100 individual / $4,200 family See Medical SBC.
 Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: [07/01/2017 06/30/2018] : Coverage for: _Single/Family Plan Type: _ASO Rx The Summary of Benefits
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: [07/01/2017 06/30/2018] : Coverage for: _Single/Family Plan Type: _ASO Rx The Summary of Benefits
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/ /31/2018
 Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/2018 12/31/2018 PG&E Anthem Health Account Plan (HAP) Coverage for: All Coverage Types
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/2018 12/31/2018 PG&E Anthem Health Account Plan (HAP) Coverage for: All Coverage Types
Trinity Health - Syracuse HSA - Ind Excellus BCBS: Excellus BluePPO Signature Deduct 3
 Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Trinity Health - Syracuse HSA - Ind Excellus BCBS: Excellus BluePPO Signature Deduct 3 Coverage Period: 01/01/2019-12/31/2019
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Trinity Health - Syracuse HSA - Ind Excellus BCBS: Excellus BluePPO Signature Deduct 3 Coverage Period: 01/01/2019-12/31/2019
Summary of Benefits and Coverage:
 Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 11/1/2017 11/1/2018 Kaiser Foundation Health Plan of Washington: Walla Walla School Dist. Plan
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 11/1/2017 11/1/2018 Kaiser Foundation Health Plan of Washington: Walla Walla School Dist. Plan
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 1/01/ /31/2019
 Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 1/01/2019-12/31/2019 PLUMBERS LOCAL 24 WELFARE FUND BUILDING TRADES DIVISION APPRENTICES Coverage
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 1/01/2019-12/31/2019 PLUMBERS LOCAL 24 WELFARE FUND BUILDING TRADES DIVISION APPRENTICES Coverage
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Service
 Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Service Custom Network Plan University of Missouri Coverage Period: 01/01/2019 12/31/2019 Coverage for: Employee & Family
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Service Custom Network Plan University of Missouri Coverage Period: 01/01/2019 12/31/2019 Coverage for: Employee & Family
The Harvard Pilgrim PPO Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services
 Massachusetts The Harvard Pilgrim PPO Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 12/01/2017 11/30/2018 Coverage for: Individual + Family
Massachusetts The Harvard Pilgrim PPO Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 12/01/2017 11/30/2018 Coverage for: Individual + Family
Coverage for: Family Plan Type: PPO
 Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 10/01/2018-09/30/2019 Blue Shield of California: 100-D $20; Rx 7-25 Coverage for: Family Plan
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 10/01/2018-09/30/2019 Blue Shield of California: 100-D $20; Rx 7-25 Coverage for: Family Plan
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 09/01/ /31/2018
 Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 09/01/2017-08/31/2018 HealthPartners:Graduate Assistants and Dependent Plan 1 Coverage for:
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 09/01/2017-08/31/2018 HealthPartners:Graduate Assistants and Dependent Plan 1 Coverage for:
Coverage for: Individual/Family Plan Type: PPO
 The Summary of Benefits and Coverage (SBC) document will help you choose a health plan. The SBC shows you how you and the plan would share the cost for covered health care services. NOTE: Information about
The Summary of Benefits and Coverage (SBC) document will help you choose a health plan. The SBC shows you how you and the plan would share the cost for covered health care services. NOTE: Information about
Summary of Benefits and Coverage:
 Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 1/1/2018 1/1/2019 Kaiser Foundation Health Plan of Washington: Pierce County Employees Coverage
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 1/1/2018 1/1/2019 Kaiser Foundation Health Plan of Washington: Pierce County Employees Coverage
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/ /31/2018
 Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/2018-12/31/2018 Whole Foods Market Premier Health Plan Coverage for: Team Members + Family
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/2018-12/31/2018 Whole Foods Market Premier Health Plan Coverage for: Team Members + Family
Coverage for: Individual/Family Plan Type: PPO
 The Summary of Benefits and Coverage (SBC) document will help you choose a health plan. The SBC shows you how you and the plan would share the cost for covered health care services. NOTE: Information about
The Summary of Benefits and Coverage (SBC) document will help you choose a health plan. The SBC shows you how you and the plan would share the cost for covered health care services. NOTE: Information about
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 09/01/ /31/2018
 \ Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 09/01/2017 08/31/2018 Texas A&M University System: A&M Care Plan Coverage for: Individual
\ Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 09/01/2017 08/31/2018 Texas A&M University System: A&M Care Plan Coverage for: Individual
$ 0. Not Applicable. Not Applicable. Yes. See rg or call (Press 2) for a list of participating providers.
 for a list of participating providers.") Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/18-12/31/18 Contra Costa Health Plan: Plan A COB Coverage for: Plan A COB Plan Type: HMO
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/18-12/31/18 Contra Costa Health Plan: Plan A COB Coverage for: Plan A COB Plan Type: HMO
01/01/ /31/2018 CCH
 Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/2018-12/31/2018 CCH Healthcare: American Plan Administrators/Cigna Coverage for: Individual,
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/2018-12/31/2018 CCH Healthcare: American Plan Administrators/Cigna Coverage for: Individual,
CROUSE HOSPITAL - Select Plan Excellus BCBS: Excellus BluePPO
 Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services CROUSE HOSPITAL - Select Plan Excellus BCBS: Excellus BluePPO Coverage Period: 01/01/2019-12/31/2019 A nonprofit
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services CROUSE HOSPITAL - Select Plan Excellus BCBS: Excellus BluePPO Coverage Period: 01/01/2019-12/31/2019 A nonprofit
Summary of Benefits and Coverage:
 Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/2018-12/31/2018 Premera BCBS of AK: Global 20 Plan Grandfathered $500 Deductible Coverage
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/2018-12/31/2018 Premera BCBS of AK: Global 20 Plan Grandfathered $500 Deductible Coverage
You don't have to meet deductibles for specific services.
 Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/2018-12/31/2018 Premera Blue Cross Blue Shield of Alaska: Plus Silver 2000 Coverage for:
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/2018-12/31/2018 Premera Blue Cross Blue Shield of Alaska: Plus Silver 2000 Coverage for:
Unlimited person/unlimited family
 Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/2019 12/31/2019 Cherokee County EPO Plan Employee Benefit Plan Coverage for: Single +
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/2019 12/31/2019 Cherokee County EPO Plan Employee Benefit Plan Coverage for: Single +
The HPHC Insurance Company PPO Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services
 Massachusetts The HPHC Insurance Company PPO Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/2018 12/31/2018 Coverage for: Individual
Massachusetts The HPHC Insurance Company PPO Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/2018 12/31/2018 Coverage for: Individual
You don t have to meet deductibles for specific services.
 Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/2019-12/31/2019 Highmark Blue Shield: PPO Blue Coverage for: Individual/Family Plan Type:
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/2019-12/31/2019 Highmark Blue Shield: PPO Blue Coverage for: Individual/Family Plan Type:
Independence Blue Cross: Health Savings PPO
 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage Period: 01/01/2018-12/31/2018 Independence Blue Cross: Health Savings PPO Coverage for: Individual + Family Plan Type: PPO
Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage Period: 01/01/2018-12/31/2018 Independence Blue Cross: Health Savings PPO Coverage for: Individual + Family Plan Type: PPO
Summary of Benefits and Coverage:
 Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: Beginning on or after 1/1/2018 Premera Blue Cross:Premera Blue Cross Balance HSA Qualilfied
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: Beginning on or after 1/1/2018 Premera Blue Cross:Premera Blue Cross Balance HSA Qualilfied
Coverage for: Individual + Family Plan Type: PPO
 Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/2019 12/31/2019 UFCW & Participating Employers: Plan JS Coverage for: Individual + Family
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/2019 12/31/2019 UFCW & Participating Employers: Plan JS Coverage for: Individual + Family
Calendar year aggregate deductible. Innetwork: $1,500 Individual / $3,000 Family. Out-of-network: $3,000 Individual / $6,000 Family.
 Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: Beginning on or after 1/1/2019 Premera Blue Cross:Premera Blue Cross Balance HSA Qualified 1500
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: Beginning on or after 1/1/2019 Premera Blue Cross:Premera Blue Cross Balance HSA Qualified 1500
Important Questions Answers Why this Matters:
 The Summary of Benefits and Coverage (SBC) document will help you choose a health plan. The SBC shows you how you and the plan would share the cost for covered health care services. NOTE: about the cost
The Summary of Benefits and Coverage (SBC) document will help you choose a health plan. The SBC shows you how you and the plan would share the cost for covered health care services. NOTE: about the cost
Important Questions Answers Why this Matters:
 The Summary of Benefits and Coverage (SBC) document will help you choose a health plan. The SBC shows you how you and the plan would share the cost for covered health care services. NOTE: Information about
The Summary of Benefits and Coverage (SBC) document will help you choose a health plan. The SBC shows you how you and the plan would share the cost for covered health care services. NOTE: Information about
The HPHC Insurance Company Best Buy HSA PPO Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services
 New Hampshire The HPHC Insurance Company Best Buy HSA PPO Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/2018 12/31/2018 Coverage for:
New Hampshire The HPHC Insurance Company Best Buy HSA PPO Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/2018 12/31/2018 Coverage for:
1/01/ /31/2019 IBEW LOCAL 351 WELFARE FUND
 Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 1/01/2019-12/31/2019 IBEW LOCAL 351 WELFARE FUND Coverage for: Family Plan Type: PPO The Summary
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 1/01/2019-12/31/2019 IBEW LOCAL 351 WELFARE FUND Coverage for: Family Plan Type: PPO The Summary
Coverage for: Individual + Family Plan Type: PPO
 Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/2018 12/31/2018 Moda Health Plan, Inc.: Moda Health Oregon Standard Silver (Affinity)
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/2018 12/31/2018 Moda Health Plan, Inc.: Moda Health Oregon Standard Silver (Affinity)
The HPHC Insurance Company PPO Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services
 Massachusetts The HPHC Insurance Company PPO Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 07/01/2018 06/30/2019 Coverage for: Individual
Massachusetts The HPHC Insurance Company PPO Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 07/01/2018 06/30/2019 Coverage for: Individual
Coverage for: Individual + Family Plan Type: PPO
 Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/2018 12/31/2018 Moda Health Plan, Inc.: Moda Health Oregon Standard Gold (Beacon) Coverage
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/2018 12/31/2018 Moda Health Plan, Inc.: Moda Health Oregon Standard Gold (Beacon) Coverage
The Harvard Pilgrim Best Buy ChoiceNet HMO Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services
 Massachusetts The Harvard Pilgrim Best Buy ChoiceNet HMO Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 07/01/2018 06/30/2019 Coverage for:
Massachusetts The Harvard Pilgrim Best Buy ChoiceNet HMO Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 07/01/2018 06/30/2019 Coverage for:
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/ /31/2018
 Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/2018 12/31/2018 Northwestern University: Select PPO Plan Coverage for: Individual + Family
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/2018 12/31/2018 Northwestern University: Select PPO Plan Coverage for: Individual + Family
Aetna: Health Savings PPO Plan (with HSA)
") Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage Period: 01/01/2018-12/31/2018 Aetna: Health Savings PPO Plan (with HSA) Coverage for: All Coverage Tiers Plan Type: PPO
Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage Period: 01/01/2018-12/31/2018 Aetna: Health Savings PPO Plan (with HSA) Coverage for: All Coverage Tiers Plan Type: PPO
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 10/01/ /31/2018
 Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 10/01/2017 09/31/2018 Moda Health Plan, Inc.: OEBB PPO (Connexus) Birch Coverage for: Family
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 10/01/2017 09/31/2018 Moda Health Plan, Inc.: OEBB PPO (Connexus) Birch Coverage for: Family
For in-network providers: $1,000 Per Person, $2,000 Family. What is the overall deductible?
 University of Utah Health Plans: Healthy Preferred EPO Coverage Period: 8/1/2018 7/31/2019 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Hughes Companies Plan Type:
University of Utah Health Plans: Healthy Preferred EPO Coverage Period: 8/1/2018 7/31/2019 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Hughes Companies Plan Type:
Standard Gold Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services
 Massachusetts Standard Gold Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/2018 12/31/2018 Coverage for: Individual + Family Plan Type:
Massachusetts Standard Gold Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/2018 12/31/2018 Coverage for: Individual + Family Plan Type: