LIST OF DOCUMENTS REQUIRED FOR SETTLEMENT OF HOSPITALISATION CLAIMS
|
|
|
- Amberly Summers
- 6 years ago
- Views:
Transcription
1 LIST OF OCUENTS REQUIRE FOR SETTLEENT OF HOSPITALISATION CLAIS 1. FOR CLAIING HOSPITALISATION EXPENSES A CLAI FOR PART A: UL COPLETE B THE INSURE ON THE PRESCRIBE FORAT - ORIGINAL B CLAI FOR PART B: UL COPLETE AN SIGNE B THE HOSPITAL AUTHORITIES - ORIGINAL C AISSION NOTES CERTIFIE COP TPA I CAR XEROX COP E F G H I J K L N O P Q R S T U V W X AN OTHER I PROOF LIKE VOTER I/ L/ PASSPORT ETC - COP ARESS PROOF - COP REFERRAL LETTER, IF AN, TO HOSPITAL CERTIFIE COP ETAILE ISCHARGE SUAR - ORIGINAL EATH SUAR (INSTEA OF ischarge Summary) IF PATIENT HAS PASSE AWA URING HOSPITALISATION - ORIGINAL INVESTIGATION REPORTS - IN ORIGINAL FOR INVESTIGATIONS ONE URING HOSPITALISATION HISTOPATHOLOG REPORT, IF AN, IN ORIGINAL CERTIFIE COP OF OPERATION THEATRE (OT) NOTES WHERE SURGER IS PERFORE LC REPORT/ FIR FOR ACCIENT CASES CERTIFIE COP STICKER FOR THE IPLANTS USE - ORIGINAL SUPPPORTING INVOICE FOR THE IPLANTS USE CERTIFIE COP HOSPITAL AIN BILL - ORIGINAL BREAK-UP BILL FOR THE HOSPITAL AIN BILL - ORIGINAL ETAILE BILL FOR THE NON-AISSIBLE AOUNTS COLLECTE FRO THE PATIENT RECEIPT FOR THE AOUNT COLLECTE FRO THE PATIENT RECEIPT FOR THE CO-PA COLLECTE FRO THE PATIENT COP OF THE PRE-AUTH ENIE LETTER, IF AN, FOR CASHLESS ENIE CONFIRATION FRO THE HOSPITAL FOR NON-UTILISATION OF CASHLESS FACILIT, IF CASHLESS SANCTIONE PRESCRIPTIONS FOR EICINES PURCHASE URING HOSPITALISATION PHARAC BILLS IN ORIGINAL FOR EICINES PURCHASE URING HOSPITALISATION LIST OF BILLS SUBITTE WITH THE AOUNT UNER EACH BILL OCUENTS FOR NATIONAL ELECTRONIC FUN TRANSFER (NEFT) Z a. NEFT FORAT GIVING ETAILS OF BANK ACCOUNT CLAI AOUNT TO BE TRANSFERRE b. A COP OF THE PAGE OF BANK PASS BOOK CONTAINING A/C NUBER & NAE/ ARESS OF A/C HOLER. AA AB c. A CANCELLE CHEQUE FOR THE ABOVE ACCOUNT IN TO WHICH CLAI AOUNT HAS TO BE TRANSFERRE COVERING LETTER STATING OUR COPLETE CURRENT ARESS, CONTACT NUBER AN THE LIST OF OCUENTS ATTACHE AN OTHER OCUENT THAT THE CLAI PROCESSING TEA/ TPA REQUESTS 2. FOR CLAIING PRE-HOSPITALISATION EXPENSES a b c d e f g h CLAI FOR - PART A UL COPLETE AN SIGNE OP CONSULTATION PAPER, IF AN ORIGINAL CONSULTATION BILL/ CASH RECEIPT, IF AN PRESCRIPTION FOR EICINES PURCHASE PRIOR TO HOSPITALISATION PHARAC CASH BILLS FOR EICINES PURCHASE PRIOR TO HOSPITALISATION INVESTIGATION REPORTS - IN ORIGINAL FOR INVESTIGATIONS ONE PRIOR TO AISION, IF AN CASH BILLS FOR THE INVESTIGATIONS ONE PRIOR TO HOSPITALISATION REFERENCE LETTER FOR INVESTIGATION CONUCTE PRIOR TO HOSPITALISATION Page1
2 i j OCUENTS FOR NATIONAL ELECTRONIC FUN TRANSFER (NEFT) AS IN ITE 1 - Z ABOVE COVERING LETTER STATING OUR COPLETE CURRENT ARESS, CONTACT NUBER & LIST OF OCUENTS ATTACHE 3. FOR CLAIING POST-HOSPITALISATION EXPENSES a b c d e f g h i j CLAI FOR PART A UL COPLETE AN SIGNE OP CONSULTATION PAPER, IF AN ORIGINAL CONSULTATION BILL/ CASH RECEIPT, IF AN PRESCRIPTION FOR EICINES PURCHASE - POST-ISCHARGE PHARAC BILLS FOR EICINES PURCHASE - POST-ISCHARGE INVESTIGATION REPORTS - IN ORIGINAL FOR INVESTIGATIONS ONE - POST-ISCHARGE, IF AN CASH BILLS FOR THE INVESTIGATIONS ONE - POST-ISCHARGE REFERENCE LETTER FOR INVESTIGATION CONUCTE - POST-ISCHARGE OCUENTS FOR NATIONAL ELECTRONIC FUN TRANSFER (NEFT) AS IN ITE 1 - Z ABOVE COVERING LETTER STATING OUR COPLETE CURRENT ARESS, CONTACT NUBER AN THE LIST OF OCUENTS ATTACHE 4. FOR HOSPITALS CLAIING CASHLESS HOSPIALISATION EXPENSES APPROVE A B C E F G H I J K L N O P Q R S T U V W X Z CLAI FOR PART A: UL COPLETE B THE INSURE ON THE PRESCRIBE FORAT - ORIGINAL CLAI FOR PART B: UL COPLETE AN SIGNE B THE HOSPITAL AUTHORITIES - ORIGINAL AISSION NOTES CERTIFIE COP TPA I CAR XEROX COP AN OTHER I PROOF LIKE VOTER I/ L/ PASSPORT ETC - COP ARESS PROOF - COP PRE-AUTHORISATION REQUEST IN ORIGINAL UL SIGNE B THE INSURE AN THE HOSPITAL PRE-AUTHORISATION APPROVAL LETTER COP REFERRAL LETTER, IF AN, TO HOSPITAL CERTIFIE COP ETAILE ISCHARGE SUAR - ORIGINAL EATH SUAR (INSTEA OF ischarge Summary) IN CASE THE PATIENT HAS PASSE AWA URING HOSPITALISATION - ORIGINAL INVESTIGATION REPORTS - IN ORIGINAL FOR INVESTIGATIONS ONE URING HOSPITALISATION HISTOPATHOLOG REPORT, IF AN, IN ORIGINAL CERTIFIE COP OF OPERATION THEATRE (OT) NOTES WHERE SURGER IS PERFORE LC REPORT/ FIR FOR ACCIENT CASES CERTIFIE COP STICKER FOR THE IPLANTS USE - ORIGINAL SUPPPORTING INVOICE FOR THE IPLANTS USE CERTIFIE COP HOSPITAL AIN BILL - ORIGINAL BREAK-UP BILL FOR THE HOSPITAL AIN BILL - ORIGINAL ETAILE BILL FOR THE NON-AISSIBLE AOUNTS COLLECTE FRO THE PATIENT RECEIPT FOR THE AOUNT COLLECTE FRO THE PATIENT FOR THE NON-AISSIBLE AOUNTS RECEIPT FOR THE CO-PA COLLECTE FRO THE PATIENT PRESCRIPTIONS FOR EICINES PURCHASE URING HOSPITALISATION PHARAC BILLS IN ORIGINAL FOR EICINES PURCHASE URING HOSPITALISATION LIST OF BILLS SUBITTE WITH THE AOUNT UNER EACH BILL AN OTHER OCUENT THAT THE CLAI PROCESSING TEA/ TPA REQUESTS NOTE: (1) OU SHOUL SUBIT THE ABOVE OCUENTS ALONG WITH A COVERING LETTER (2) IF OU ARE SUBITTING PRE &/OR POST- HOSPITALISATION CLAIS SEPARATEL OU SHOUL SUBIT THE CLAI FOR UL COPLETE (3) ALSO SUBIT THIS CHECKLIST Page2
 Name of the Bank Policy No Name of the Insured Vidal I Card No Employee Id Cadre Name of the Claimant")

3 Annexure I Vidal Health TPA Pvt. Ltd IBA Hospitalisation Claim Reimbursement Statement (The Federal Bank Ltd.) Name of the Bank Policy No Name of the Insured Vidal I Card No Employee Id Cadre Name of the Claimant Relation to Claimant Nature of Illness ate of Submission Sl No Bill ate Bill No/escription Amount Claimed Remarks Signature of the Insured: Total Amount Claimed: Note: This form should be attached along with Signed Claim Format A.
4
5
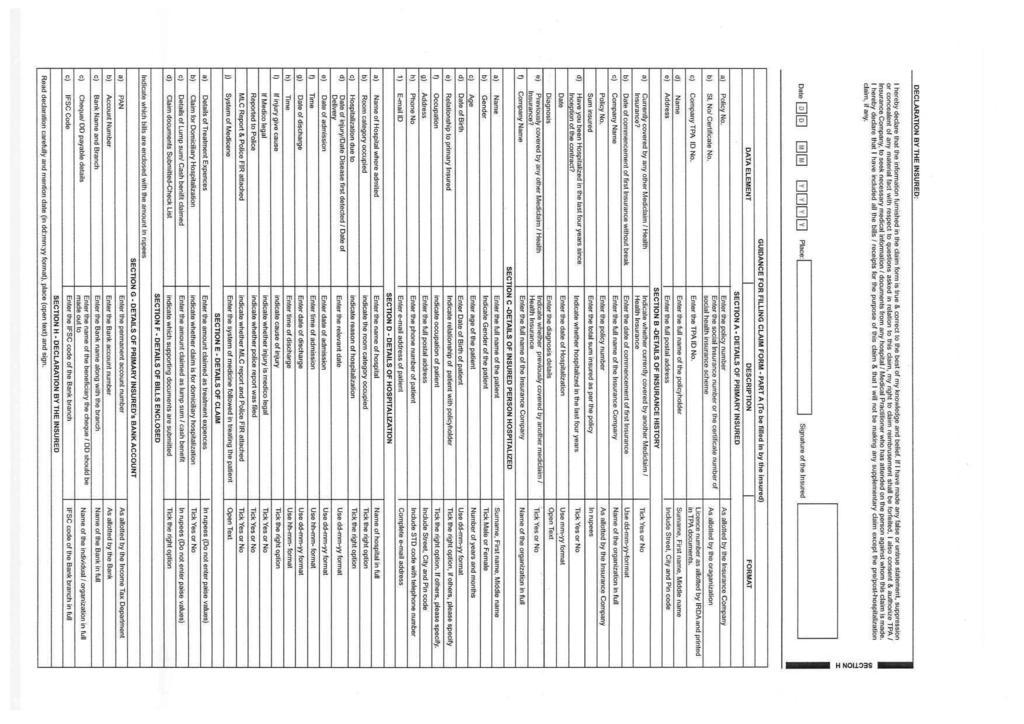
6 ETAILS OF HOSPITAL CLAI FOR - PART B TO BE FILLE IN B THE HOSPITAL The issue of this Form is not to be taken as an admission of liability Please include the original preauthorization request form in lieu of PART A (To be Filled in block letters) a) Name of the hospital: a) Hospital I: c) Name of the treating doctor: e) Qualification: ETAILS OF THE PATIENT AITTE a) Name of the Patient: f) ate of Admission: j) Type of Admission: Emergency Planned ay Care c) Type of Hospital: Network : Non Network : (if non network fill section E) f) Registration No. with State Code: g) Phone No. aternity k) If aternity I) Status at time of discharge: ischarge to home ischarge to another hospital eceased ETAILS OF AILENT IAGNOSE (PRIAR) a) IC 10 Codes I. Primary iagnosis ii. Additional iagnosis: iii. Co-morbidities: iv. Co-morbidities: c) Pre-authorization obtained: es e) If authorization by network hospital not obtained, give reason: escription b) No vi. If not reported to police give reason: d) Pre-authorization Number: h) ate of ischarge: i) ate of elivery: i. Procedure 1: ii. Procedure 2: iii. Procedure 3: iv. etails of Procedure: m) Total claimed amount IC 10 PCS f) Hospitalization due to injury: es No I. If es, give cause Self-inflicted Road Traffic Accident Substance abuse / alcohol consumption ii) If injury due to substance abuse / alcohol consumption, Test conducted to establish this: v. FIR No. CLAI OCUENTS SUBITTE - CHECK LIST Claim Form duly signed Original Pre-authorization request Copy of the Pre-authorization approval letter Copy of Photo I Card of patient Verified by hospital Hospital ischarge summary Operation Theatre Notes Hospital main bill Hospital break-up bill AITIONAL ETAILS IN CASE OF NON NETWORK HOSPITAL a) Address of the Hospital d) Hospital PAN: iii. Others: ECLARATION B THE HOSPITAL es No (If es, attach reports) Investigation reports iii. If edico legal: CT/R/USG/HPE investigation reports octor s reference slip for investigation ECG Pharmacy bills LC reports & Police FIR es No Original death summary from hospital where applicable Any other, please specify (ONL FILL IN CASE OF NON-NETWORK HOSPITAL) ii) Gravida Status: : escription iv. Reported to Police (PLEASE REA VER CAREFULL) We hereby declare that the information furnished in this Claim Form is true & correct to the best of our knowledge and belief. If we have made any false or untrue statement, suppression or concealment of any material fact, our right to claim under this claim shall be forfeited. ate: City: S U R N A E F I R S T N A E I L E N A E S U R N A E F I R S T N A E I L E N A E b) IP Registration Number: c) Gender: ale Female d) Age: ears onths e) ate of birth: g) Time: H H Pin Code: b) Phone No. c) Registration No. with State Code: State: e) Number of inpatient beds f) Facilities available in the hospital i. OT es No ii. ICU es No H H es No SECTION A SECTION B SECTION C SECTION SECTION E SECTION F Place: Signature and Seal of the Hospital Authority:
7 GUIANCE FOR FILLING CLAI FOR - PART B (To be filled in by the hospital) ATA ELEENT ESCRIPTION FORAT SECTION A - ETAILS OF HOSPITAL a) Name of the hospital: Enter the name of hospital Name of the hospital in full b) Hospital I c) Type of Hospital c) Name of treating doctor e) Qualification f) Registration No. with State Code g) Phone No. a) Name of Patient b) IP registration Number c) Gender d) Age e) ate of Birth f) ate of Admission g) Time h) ate of ischarge i) Time j) Type of Admission k) If aternity ate of elivery Gravida Status l) Status at time of discharge ) Total claimed amount a) IC 10 Code Primary iagnosis Additional iagnosis Co-morbidities b) IC 10 PCS Procedure 1 Procedure 2 Procedure 3 etails of Procedure c) Pre-authorization obtained d) Pre-authorization Number Enter I number of hospital Indicate whether in network or non network hospital Enter the name of the treating doctor Enter the qualification of the treating doctor Enter the registration number of the doctor along with the state code Enter the phone number of doctor SECTION B - ETAILS OF THE PATIENT AITTE Enter the name of patient Enter insurance provider registration number Indicate Gender of the patient Enter age of the patient Enter date of birth Enter date of admission Enter Time of admission Enter date of ischarge Enter time of ischarge Indicate type of admission of patient Enter ate of elivery if maternity Enter Gravida status if maternity Indicate status of patient at time of discharge Indicate the total claimed amount SECTION C - ETAILS OF AILENT IAGNOSE (PRIAR) Enter the IC 10 Code and description of the primary diagnosis Enter the IC 10 Code and description of the additional diagnosis Enter the IC 10 Code and description of the Co-morbidities Enter the IC 10 Code and description of the first procedure Enter the IC 10 Code and description of the second procedure Enter the IC 10 Code and description of the third procedure Enter the details of the procedure Indicate whether pre-authorization obtained Enter pre-authorization number As allocated by the TPA Tick the right option Name of doctor in full Abbreviations of educational qualifications As allocated by the edical Council of India Include ST code with telephone number Name of patient in full As allotted by the insurance provider Tick ale or Female Number of years and months Use dd-mm-yy format Use dd-mm-yy format Use hh:mm format Use dd-mm-yy format Use hh:mm format Tick the right option Use dd-mm-yy format Use standard format Tick the right option In rupees (o not enter paise values) Open text Tick es or No As allotted by TPA e) If authorization by network hospital not obtained, give reason Enter reason for not obtaining pre-authorization number Open text f) Hospitalization due to injury Cause If injury due to substance abuse/alcohol consumption test conducted to establish this edico Legal Reported to Police FIR No. If not reported to police, give reason Indicate which supporting documents are submitted a) Address b) Phone No. c) Registration No. with State Code d) Hospital PAN e) Number of Inpatient beds f) Facilities available in the hospital Indicate if hospitalization is due to injury Indicate cause of injury Indicate whether test conducted Indicate whether injury is medico legal Indicate whether police report was filed Enter first information report number Enter reason for not reporting to police SECTION - CLAI OCUENTS SUBITTE-CHECK LIST SECTION E - ETAILS IN CASE OF NON NETWORK HOSPITAL Enter the full postal address Enter the phone number of hospital Enter the registration number of the Hospital obtained from local body like City Corporation / unicipality Enter the permanent account number Enter the number of inpatient beds Indicate facilities available in the hospital SECTION F - ECLARATION B THE HOSPITAL Read declaration carefully and mention date (in dd:mm:yy format), place (open text) and sign. and stamp Tick es or No Tick the right option Tick es or No Tick es or No Tick es or No As issued by police authrities Open text Include Street, City and Pin Code Include ST code with telephone number As allocated by the City Corporation / unicipality As allocated by the Income Tax epartment igits Tick the right option. If others, please specify
8 ELECTRONIC CLEARING SERVICE (CREIT CLEARING) ANATE FOR For Claim under Policy No 1. A CARHOLER S NAE (B) ARESS (C) TELEPHONE / OBILE No: () E-AIL I: 2. TTK I No 3. PARTICULARS OF BANK ACCOUNT A. BANK NAE B. BRANCH NAE C. ARESS. 9 IGIT COE NUBER OF THE BANK & BRANCH APPEARING ON THE ICR CHEQUE ISSUE B THE BANK E. ACCOUNT TPE (SAVINGS ACCOUNT/ CURRENT ACCOUNT) F. ACCOUNT NUBER (AS APPEARING ON THE CHEQUE BOOK) G. BANK ACCOUNT HOLER NAE 4. ATE OF EFFECT: 5. IFSC COE (INIAN FINANCIAL SSTE COE) INFORATION FOR PAENT THROUGH RTGS OR NEFT 6. NEFT COE (NATIONAL ELECTRONIC FUNS TRANSFER COE) By submission of the above, I authorise /s Vidal Health TPA Private Ltd (formerly known as TTK Healthcare TPA Pvt Ltd) / the Insurance Company to settle the claim under reference through direct payment by ECS. I hereby declare & confirm that the particulars given above are correct and complete. I agree that I shall not hold the TPA/ Insurance Company responsible for delay or non-receipt of payment for any reason whatsoever after issue of instructions for transfer of payment by Insurer/ TPA based on the above. ate: Place: Signature of the Insured
ID: Yes. Yes. /No. months. b) Date of Birth: Spouse. Service Self Employed Homemaker Student Retired Other. ID:
 Date of Birth: Spouse. Service Self Employed Homemaker Student Retired Other. ID:") INSURANCE TPA SERVICES (I) PVT.LT. 6B, Paul ansions, Bishop Lefroy Road, Kolkata 700 020, West Bengal, India ETAILS OF PRIAR INSURE (To be filled in block letters) a) Policy b) Company/ TPA I CLAI FOR
INSURANCE TPA SERVICES (I) PVT.LT. 6B, Paul ansions, Bishop Lefroy Road, Kolkata 700 020, West Bengal, India ETAILS OF PRIAR INSURE (To be filled in block letters) a) Policy b) Company/ TPA I CLAI FOR
PARAMOUNT HEALTH SERVICES & INSURANCE TPA PRIVATE LIMITED (IRDA License No. 006) [formerly known as PARAMOUNT HEALTH SERVICES (TPA) PVT.
 [formerly known as PARAMOUNT HEALTH SERVICES (TPA) PVT.") PARAOUNT HEALTH SERVICES & INSURANCE TPA PRIVATE LIITE (IRA License. 006) [formerly known as PARAOUNT HEALTH SERVICES (TPA) PVT.LT] Plot no.a-442, Road -28,.I..C Industrial Area, Wagale Estate, Ram Nagar,
PARAOUNT HEALTH SERVICES & INSURANCE TPA PRIVATE LIITE (IRA License. 006) [formerly known as PARAOUNT HEALTH SERVICES (TPA) PVT.LT] Plot no.a-442, Road -28,.I..C Industrial Area, Wagale Estate, Ram Nagar,
SECTION A SECTION 8 SECTION C SECTION D SECTION E SECTION F SECTION G
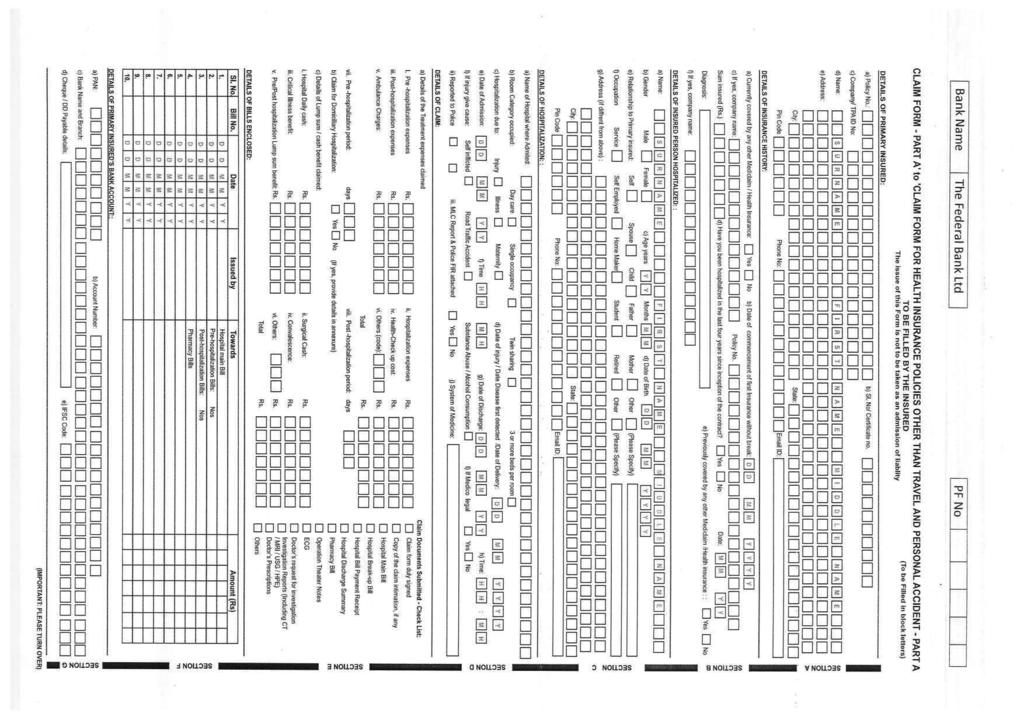
 CLAIM FORM - PART A TO 8E FILLED IN 8Y THE INSURED The issue of this Form is not to be taken as an admission of liability (To be filled in block letters) DETAILS OF PRIMARY INSURED: a) Policy No: b) Sl.
CLAIM FORM - PART A TO 8E FILLED IN 8Y THE INSURED The issue of this Form is not to be taken as an admission of liability (To be filled in block letters) DETAILS OF PRIMARY INSURED: a) Policy No: b) Sl.
5 easy ways to speed up the claims process
 Please return your completed claim form to: CignaTTK Health Insurance Company Limited OR Nearest Cigna TTK Branch. Corporate Office: 10th Floor, Commerz, International Business Park, Oberoi Garden City,
Please return your completed claim form to: CignaTTK Health Insurance Company Limited OR Nearest Cigna TTK Branch. Corporate Office: 10th Floor, Commerz, International Business Park, Oberoi Garden City,
5 easy ways to speed up the claims process
 Please return your completed claim form to: CignaTTK Health Insurance Company Limited OR Nearest Cigna TTK Branch. Corporate Office: 401/402, Raheja Titanium, Western Express Highway, Goregaon (East),
Please return your completed claim form to: CignaTTK Health Insurance Company Limited OR Nearest Cigna TTK Branch. Corporate Office: 401/402, Raheja Titanium, Western Express Highway, Goregaon (East),
HDFC ERGO General Insurance Company Limited
 HFC ERGO General Insurance Company Limited CLAI FOR FOR HEALTH INSURANCE POLICIES OTHER THAN TRAVEL AN PERSONAL ACCIENT CLAI FOR PART A To be filled in by e Insured The issue of is form is not to be taken
HFC ERGO General Insurance Company Limited CLAI FOR FOR HEALTH INSURANCE POLICIES OTHER THAN TRAVEL AN PERSONAL ACCIENT CLAI FOR PART A To be filled in by e Insured The issue of is form is not to be taken
CLAIM FORM FOR HEALTH INSURANCE POLICIES OTHER THAN TRAVEL AND PERSONAL ACCIDENT PART A
 SBI General Insurance Company Limited CLAIM FORM FOR HEALTH INSURANCE POLICIES OTHER THAN TRAVEL AND PERSONAL ACCIDENT PART A TO BE FILLED IN BY THE INSURED The issue of this Form is not to be taken as
SBI General Insurance Company Limited CLAIM FORM FOR HEALTH INSURANCE POLICIES OTHER THAN TRAVEL AND PERSONAL ACCIDENT PART A TO BE FILLED IN BY THE INSURED The issue of this Form is not to be taken as
HDFC ERGO General Insurance Company Limited
 HFC ERGO General Insurance Company Limited CLAI FOR FOR HEALTH INSURANCE POLICIES OTHER THAN TRAVEL AN PERSONAL ACCIENT CLAI FOR PART A To be filled in by the Insured The issue of this form is not to be
HFC ERGO General Insurance Company Limited CLAI FOR FOR HEALTH INSURANCE POLICIES OTHER THAN TRAVEL AN PERSONAL ACCIENT CLAI FOR PART A To be filled in by the Insured The issue of this form is not to be
Claim form for health insurance policies other than travel and personal accident - PART A
 M M Claim form for health insurance policies other than travel and personal accident - PART A TO BE FILLED IN BY THE INSURED (TO BE FILLED IN BLOCK LETTERS) The issue of this Form is not to be taken as
M M Claim form for health insurance policies other than travel and personal accident - PART A TO BE FILLED IN BY THE INSURED (TO BE FILLED IN BLOCK LETTERS) The issue of this Form is not to be taken as
HDFC ERGO General Insurance Company Limited
 HFC ERGO General Insurance Company Limited CLAI FOR FOR HEALTH INSURANCE POLICIES OTHER THAN TRAVEL AN PERSONAL ACCIENT CLAI FOR PART A To be filled in by e Insured The issue of is form is not to be taken
HFC ERGO General Insurance Company Limited CLAI FOR FOR HEALTH INSURANCE POLICIES OTHER THAN TRAVEL AN PERSONAL ACCIENT CLAI FOR PART A To be filled in by e Insured The issue of is form is not to be taken
CLAIM FORM. CLAIM FORM PART A TO BE FILLED IN BY THE INSURED The issue of this Form is not to be taken as an admission of liability
 CLAIM FORM CLAIM FORM PART A TO BE FILLED IN BY THE INSURED The issue of this Form is not to be taken as an admission of liability SECTION A DETAILS OF PRIMARY INSURED a) Policy No b) Sl. No/ Certificate
CLAIM FORM CLAIM FORM PART A TO BE FILLED IN BY THE INSURED The issue of this Form is not to be taken as an admission of liability SECTION A DETAILS OF PRIMARY INSURED a) Policy No b) Sl. No/ Certificate
MediRaksha. Claim Form. Part A (To be filled in by the Insured)
") MediRaksha Claim Form Tata AIG General Insurance Company Limited: A-501, 5th Floor, Building.4, Infinity Park, Gen. A.K. Vaidya Marg, Dindoshi, Malad (East), Mumbai 400 097 IMPORTANT: The Issue of this
MediRaksha Claim Form Tata AIG General Insurance Company Limited: A-501, 5th Floor, Building.4, Infinity Park, Gen. A.K. Vaidya Marg, Dindoshi, Malad (East), Mumbai 400 097 IMPORTANT: The Issue of this
Claim form for health insurance policies other than travel and personal accident - PART A
 M M Claim form for health insurance policies other than travel and personal accident - PART A TO BE FILLED IN BY THE INSURED (TO BE FILLED IN BLOCK LETTERS) The issue of this Form is not to be taken as
M M Claim form for health insurance policies other than travel and personal accident - PART A TO BE FILLED IN BY THE INSURED (TO BE FILLED IN BLOCK LETTERS) The issue of this Form is not to be taken as
In addition to above, if the claim amount is more than Rs 1 Lakh then following additional documents are required:
 Health Insurance Ab Health Hamesha Broad Guidelines for Claim Process 1. Please ensure Claim form is completely filled, signed and submitted in original. 2. Please provide at least two contactable mobile
Health Insurance Ab Health Hamesha Broad Guidelines for Claim Process 1. Please ensure Claim form is completely filled, signed and submitted in original. 2. Please provide at least two contactable mobile
PARAMOUNT HEALTH SERVICES & INSURANCE TPA PRIVATE LIMITED (IRDA License No. 006) [formerly known as PARAMOUNT HEALTH SERVICES (TPA) PVT.
 [formerly known as PARAMOUNT HEALTH SERVICES (TPA) PVT.") PARAMOUNT HEALTH SERVICES & INSURANCE TPA PRIVATE LIMITED (IRDA License No. 006) [formerly known as PARAMOUNT HEALTH SERVICES (TPA) PVT.LTD] Plot no.a-442, Road No-28,M.I.D.C Industrial Area, Wagale Estate,
PARAMOUNT HEALTH SERVICES & INSURANCE TPA PRIVATE LIMITED (IRDA License No. 006) [formerly known as PARAMOUNT HEALTH SERVICES (TPA) PVT.LTD] Plot no.a-442, Road No-28,M.I.D.C Industrial Area, Wagale Estate,
State: b) Date of commencement of first Insurance without break: State: d) Date of Injury / Date Disease first detected /Date of Delivery:
 Date of commencement of first Insurance without break: State: d) Date of Injury / Date Disease first detected /Date of Delivery:") DETAILS OF PRIMARY INSURED a) PolicyNo Vipul Medcorp lnsurance TPA Pvt Ltd. Redefining Healthcare Services... CLAIM FORM FOR HEALTH INSURANCE POLICIES OTHER THAN TRAVEL AND PERSONAL ACCIDENT - PART A TO
DETAILS OF PRIMARY INSURED a) PolicyNo Vipul Medcorp lnsurance TPA Pvt Ltd. Redefining Healthcare Services... CLAIM FORM FOR HEALTH INSURANCE POLICIES OTHER THAN TRAVEL AND PERSONAL ACCIDENT - PART A TO
MEDSAVE HEALTHCARE (TPA) LIMITED F- 701, Lado Sarai, Mehrauli New Delhi Web: CHECKLIST OF ENCLOSURES FOR SUBMISSION OF CLAIM
 LIMITED F- 701, Lado Sarai, Mehrauli New Delhi Web: CHECKLIST OF ENCLOSURES FOR SUBMISSION OF CLAIM") Toll Free No: 180011142 callcenter@medsave.in ESAVE HEALTHCARE (TPA) LIITE F- 701, Lado Sarai, ehrauli New elhi 110030 Web: www.medsave.in CHECKLIST OF ENCLOSURES FOR SUBISSION OF CLAI [Please tick the
Toll Free No: 180011142 callcenter@medsave.in ESAVE HEALTHCARE (TPA) LIITE F- 701, Lado Sarai, ehrauli New elhi 110030 Web: www.medsave.in CHECKLIST OF ENCLOSURES FOR SUBISSION OF CLAI [Please tick the
National Insurance Company Limited
 DETAILS OF THE THIRD PARTY ADMINISTRATOR a) Name of TPA / Insurance Company: b) Toll free phone number: c) Toll free Fax: CIN No. - U10200WB1906GOI001713 IRDA Regn. No. - 58 PLEASE FAX / SCAN PAGE 1 ONLY
DETAILS OF THE THIRD PARTY ADMINISTRATOR a) Name of TPA / Insurance Company: b) Toll free phone number: c) Toll free Fax: CIN No. - U10200WB1906GOI001713 IRDA Regn. No. - 58 PLEASE FAX / SCAN PAGE 1 ONLY
Claim Form
 SECTION A - DETAILS OF PRIMARY INSURED (The issue of this Form is not to be taken as an admission of liability) PART A TO BE FILLED IN BY THE INSURED a) Policy No. : b) Sl. No/ Certificate No. : c) Company/
SECTION A - DETAILS OF PRIMARY INSURED (The issue of this Form is not to be taken as an admission of liability) PART A TO BE FILLED IN BY THE INSURED a) Policy No. : b) Sl. No/ Certificate No. : c) Company/
(Surname) (First Name) (Middle Name) (DD/MM/YYYY) (Surname) (First Name) (Middle Name)
 (First Name) (Middle Name) (DD/MM/YYYY) (Surname) (First Name) (Middle Name)") Health Insurance Ab Health Hamesha Claim Form - ASSURE Part A 1. To be filled in by the Insured. 2. The issue of this Form is not to be taken as an admission of liability. 3. To be filled in block letters.
Health Insurance Ab Health Hamesha Claim Form - ASSURE Part A 1. To be filled in by the Insured. 2. The issue of this Form is not to be taken as an admission of liability. 3. To be filled in block letters.
To: All Affiliates/Office Bearers/Central Committee Members Dear Sir/Madam,
 ALL INIA CANARA BANK RETIREES FEERATION (Regd.) (Affiliated to All India Bank Retirees Federation) A.K.Nayak Bhavan, 2 nd Floor, 14, Second Line Beach, Chennai 600001. Ref No:97:2015 November 11, 2015
ALL INIA CANARA BANK RETIREES FEERATION (Regd.) (Affiliated to All India Bank Retirees Federation) A.K.Nayak Bhavan, 2 nd Floor, 14, Second Line Beach, Chennai 600001. Ref No:97:2015 November 11, 2015
Ab Health Hamesha. Health Insurance. Broad Guidelines for Claim Process. Brief description of the key documents required along with the claim form
 Health Insurance Ab Health Hamesha Broad Guidelines for Claim Process 1. Please ensure Claim form is completely filled, signed and submitted in original. 2. Please provide at least two contactable mobile
Health Insurance Ab Health Hamesha Broad Guidelines for Claim Process 1. Please ensure Claim form is completely filled, signed and submitted in original. 2. Please provide at least two contactable mobile
Claim Form. Do You Know
 Claim Form Do You Know SECTIONA - DETAILS OF PRIMARY INSURED CLAIM FORM (The issue of this Form is not to be taken as an admission of liability) PART A TO BE FILLED IN BY THE INSURED a) Policy No. : b)
Claim Form Do You Know SECTIONA - DETAILS OF PRIMARY INSURED CLAIM FORM (The issue of this Form is not to be taken as an admission of liability) PART A TO BE FILLED IN BY THE INSURED a) Policy No. : b)
Membership Number: Suite. Deluxe Room. k) Type of hospitalization: Emergency / Planned. Rs. vi. External aids: viii.opd: ix.
 Type of hospitalization: Emergency / Planned. Rs. vi. External aids: viii.opd: ix.") CHOLAMANDALAM MS GENERAL INSURANCE COMPANY LIMITED Claims Processing Centre: Shaw Wallace Building, New No. 319, Old No.154, 2nd Floor, Thambu Chetty Street, Parrys, Chennai- 600001 Toll Free Ph No.: 1800
CHOLAMANDALAM MS GENERAL INSURANCE COMPANY LIMITED Claims Processing Centre: Shaw Wallace Building, New No. 319, Old No.154, 2nd Floor, Thambu Chetty Street, Parrys, Chennai- 600001 Toll Free Ph No.: 1800
CLAIM FORM (The issue of this Form is not to be taken as an admission of liability) PART A. Pin Code : Phone No. : d) Age (YY/MM) : Y Y M M
 PART A. Pin Code : Phone No. : d) Age (YY/MM) : Y Y M M") Claim Form Do You Know SECTIONA - DETAILS OF PRIMARY INSURED CLAIM FORM (The issue of this Form is not to be taken as an admission of liability) PART A TO BE FILLED IN BY THE INSURED a) Policy No. : b)
Claim Form Do You Know SECTIONA - DETAILS OF PRIMARY INSURED CLAIM FORM (The issue of this Form is not to be taken as an admission of liability) PART A TO BE FILLED IN BY THE INSURED a) Policy No. : b)
 CLAIM FORM FOR HEALTH INSURANCE POLICIES FOR INJURY/ILLNESS- (PART-A) TO BE FILLED IN BYTHE INSURED- STUDENT SAFETY ILLNESS & EMPLOYEE MEDICLAIM POLICY The issue of this Form is not to be taken as an admission
CLAIM FORM FOR HEALTH INSURANCE POLICIES FOR INJURY/ILLNESS- (PART-A) TO BE FILLED IN BYTHE INSURED- STUDENT SAFETY ILLNESS & EMPLOYEE MEDICLAIM POLICY The issue of this Form is not to be taken as an admission
M/S.NATCO PHARMA LTD.
 /S.NATCO PHARA LT. UNITE INIA INSURANCE COPAN LIITE Policy No : 052100/28/15/P112796862 Policy Start ate-21/01/2016 Policy End ate 20/01/2017 2/18/2016 1 India Health Care Services ( TPA ) Pvt Ltd Contents
/S.NATCO PHARA LT. UNITE INIA INSURANCE COPAN LIITE Policy No : 052100/28/15/P112796862 Policy Start ate-21/01/2016 Policy End ate 20/01/2017 2/18/2016 1 India Health Care Services ( TPA ) Pvt Ltd Contents
1S CLAIMANT STATEMENT FORM (HEALTH CLAIMS)
") 24x7 CustomerHelpline No: 1860 266 7766 CLAIM FORM - PART A TO BE FILLE IN BY THE INSURE The issue of this Form is not to be taken as an admission of liability 1S CLAIMANT STATEMENT FORM (HEALTH CLAIMS)
24x7 CustomerHelpline No: 1860 266 7766 CLAIM FORM - PART A TO BE FILLE IN BY THE INSURE The issue of this Form is not to be taken as an admission of liability 1S CLAIMANT STATEMENT FORM (HEALTH CLAIMS)
CLAIM FORM (The issue of this Form is not to be taken as an admission of liability) PART A. Pin Code : Phone No. :
 PART A. Pin Code : Phone No. :") Claim Form Do You Know SECTIONA - DETAILS OF PRIMARY INSURED CLAIM FORM (The issue of this Form is not to be taken as an admission of liability) PART A TO BE FILLED IN BY THE INSURED a) Policy No. : b)
Claim Form Do You Know SECTIONA - DETAILS OF PRIMARY INSURED CLAIM FORM (The issue of this Form is not to be taken as an admission of liability) PART A TO BE FILLED IN BY THE INSURED a) Policy No. : b)
PARAMOUNT HEALTH SERVICES & INSURANCE TPA PRIVATE LIMITED (IRDA License No. 006) [formerly known as PARAMOUNT HEALTH SERVICES (TPA) PVT.
 [formerly known as PARAMOUNT HEALTH SERVICES (TPA) PVT.") PARAMOUNT HEALTH SERVICES & INSURANCE TPA PRIVATE LIMITED (IRDA License No. 006) [formerly known as PARAMOUNT HEALTH SERVICES (TPA) PVT.LTD] Plot no.a-442, Road No-28,M.I.D.C Industrial Area, Wagale Estate,
PARAMOUNT HEALTH SERVICES & INSURANCE TPA PRIVATE LIMITED (IRDA License No. 006) [formerly known as PARAMOUNT HEALTH SERVICES (TPA) PVT.LTD] Plot no.a-442, Road No-28,M.I.D.C Industrial Area, Wagale Estate,
Claim Form - my:health Medisure Prime Insurance
 Claim Form - my:health Medisure Prime Insurance GUIDELINES TO FILL THE FORM 1. Please fill the form in BLOCK LETTERS. Please answer all questions fully and correctly. All details with * are mandatory.
Claim Form - my:health Medisure Prime Insurance GUIDELINES TO FILL THE FORM 1. Please fill the form in BLOCK LETTERS. Please answer all questions fully and correctly. All details with * are mandatory.
C I R C U L A R. For Reimbursement claims of Hospitalization / Domiciliary Hospitalization/ Domiciliary treatment expenses:
 ALLAHABA BANK PERSONNEL AMINISTRATION EPARTMENT (HUMAN RELATIONS SECTION) Head Office : 2, Netaji Subhas Road, Kolkata 700 001 Instruction Circular. 13993/AMN(HR)/2015-2016/20 ate : 06-11-2015 To ALL OFFICES
ALLAHABA BANK PERSONNEL AMINISTRATION EPARTMENT (HUMAN RELATIONS SECTION) Head Office : 2, Netaji Subhas Road, Kolkata 700 001 Instruction Circular. 13993/AMN(HR)/2015-2016/20 ate : 06-11-2015 To ALL OFFICES
a) Currently covered by any other Mediclaim / Health Insurance: Yes No b) If yes, Policy Type: Individual Group
 Currently covered by any other Mediclaim / Health Insurance: Yes No b) If yes, Policy Type: Individual Group") CLAIM FORM FOR HEALTH INSURANCE POLICIES OTHER THAN TRAVEL AND PERSONAL ACCIDENT - PART A TO BE FILLED IN BY THE INSURED SECTION A - DETAILS OF PRIMARY INSURED: (To be filled in block letters) a) Policy
CLAIM FORM FOR HEALTH INSURANCE POLICIES OTHER THAN TRAVEL AND PERSONAL ACCIDENT - PART A TO BE FILLED IN BY THE INSURED SECTION A - DETAILS OF PRIMARY INSURED: (To be filled in block letters) a) Policy
ICICI Lombard Health Care Claim Form - Hospitalisation (Issuance of this form is not to be taken as an admission of liability)
") ICICI Lombard Health Care Claim Form - Hospitalisation (Issuance of this form is not to be taken as an admission of liability) ICICI Lombard Health Care Do You Know «Non-submission of original bills and
ICICI Lombard Health Care Claim Form - Hospitalisation (Issuance of this form is not to be taken as an admission of liability) ICICI Lombard Health Care Do You Know «Non-submission of original bills and
ICICI Lombard Health Care Claim Form - Hospitalisation (Issuance of this form is not to be taken as an admission of liability)
") ICICI Lombard Health Care Claim Form - Hospitalisation (Issuance of this form is not to be taken as an admission of liability) Overview Health Claim Form - Hospitalization ICICI Lombard Health Care Part
ICICI Lombard Health Care Claim Form - Hospitalisation (Issuance of this form is not to be taken as an admission of liability) Overview Health Claim Form - Hospitalization ICICI Lombard Health Care Part
ICICI Lombard Health Care Claim Form - Hospitalisation (Issuance of this form is not to be taken as an admission of liability)
") ICICI Lombard Health Care Claim Form - Hospitalisation (Issuance of this form is not to be taken as an admission of liability) Overview Health Claim Form - Hospitalization Documents Submitted ICICI Lombard
ICICI Lombard Health Care Claim Form - Hospitalisation (Issuance of this form is not to be taken as an admission of liability) Overview Health Claim Form - Hospitalization Documents Submitted ICICI Lombard
HRMD CIRCULAR NO Medical Insurance Scheme for Retired Officers/Retired employees Operational Guidelines
 Human Resources anagement ivision (Hospitalisation Cell), Head Office: New elhi Phone No. 011 26174730 Email hrdhospitalisation@pnb.co.in FAX 011 26196491 arch 11, 2016 TO ALL OFFICES HR CIRCULAR NO. 300
Human Resources anagement ivision (Hospitalisation Cell), Head Office: New elhi Phone No. 011 26174730 Email hrdhospitalisation@pnb.co.in FAX 011 26196491 arch 11, 2016 TO ALL OFFICES HR CIRCULAR NO. 300
Student Retired Student Others. Mobile Home Work. Student Retired Student Others. Self-inflicted road traffic accident substance abuse alcohol abuse
 HEALTH INSURANCE Aditya Birla Health Insurance Co. Limited Claim Form Part A - Personal Accident SECTION A 1. Details of the Proposer: a) Policy No.: b) Name of the Insured: c) Date of Birth: d) Marital
HEALTH INSURANCE Aditya Birla Health Insurance Co. Limited Claim Form Part A - Personal Accident SECTION A 1. Details of the Proposer: a) Policy No.: b) Name of the Insured: c) Date of Birth: d) Marital
HEALTH INSURANCE GUIDE BOOK FOR SERVICING LIC S EMPLOYEES POLICY
 Page1 HEALTH INSURANCE GUIDE BOOK FOR SERVICING LIC S EMPLOYEES POLICY Vidal Health TPA Pvt. Ltd., Tower No. 2, First Floor, SJR I Park, EPIP Area, Whitefield, Bangalore-560 066 Toll free number - Kerala:1800
Page1 HEALTH INSURANCE GUIDE BOOK FOR SERVICING LIC S EMPLOYEES POLICY Vidal Health TPA Pvt. Ltd., Tower No. 2, First Floor, SJR I Park, EPIP Area, Whitefield, Bangalore-560 066 Toll free number - Kerala:1800
FAQ (FREQUENTLY ASKED QUESTIONS) ON MEDICAL INSURANCE SCHEME FOR RETIRED EMPLOYEES OF PUNJAB & SIND BANK
 ON MEDICAL INSURANCE SCHEME FOR RETIRED EMPLOYEES OF PUNJAB & SIND BANK") FAQ (FREQUENTLY ASKED QUESTIONS) ON MEDICAL INSURANCE SCHEME FOR RETIRED EMPLOYEES OF PUNJAB & SIND BANK 1. What is the definition of family under the scheme? The family of a retired employee includes
FAQ (FREQUENTLY ASKED QUESTIONS) ON MEDICAL INSURANCE SCHEME FOR RETIRED EMPLOYEES OF PUNJAB & SIND BANK 1. What is the definition of family under the scheme? The family of a retired employee includes
Preauthorization Form Request For Cashless Hospitalisation For Medical Insurance Policy
 Aditya Birla Health Insurance Co. Limited Preauthorization Form Request For Cashless Hospitalisation For Medical Insurance Policy DETAILS OF THE THIRD PARTY ADMINISTRATOR (To be filled in block letters)
Aditya Birla Health Insurance Co. Limited Preauthorization Form Request For Cashless Hospitalisation For Medical Insurance Policy DETAILS OF THE THIRD PARTY ADMINISTRATOR (To be filled in block letters)
PARAMOUNT HEALTH SERVICES & INSURANCE TPA PRIVATE LIMITED (IRDA License No. 006) [formerly known as PARAMOUNT HEALTH SERVICES (TPA) PVT.
 [formerly known as PARAMOUNT HEALTH SERVICES (TPA) PVT.") PARAMOUNT HEALTH SERVICES & INSURANCE TPA PRIVATE LIMITE (IRA License No. 006) [formerly known as PARAMOUNT HEALTH SERVICES (TPA) PVT.LT] Plot no.a-442, Road No-28,M.I..C Indurial Area, Wagale Eate, Ram
PARAMOUNT HEALTH SERVICES & INSURANCE TPA PRIVATE LIMITE (IRA License No. 006) [formerly known as PARAMOUNT HEALTH SERVICES (TPA) PVT.LT] Plot no.a-442, Road No-28,M.I..C Indurial Area, Wagale Eate, Ram
HDFC LIFE - CANCER CARE CLAIM FORM
 PSNF542702031602 Comp/feb/Int/4632 Page 1/7 HDFC LIFE - CANCER CARE CLAIM FORM PART A This form is to be filled by the claimant in block letters. The issue of this form is not to be taken as an admission
PSNF542702031602 Comp/feb/Int/4632 Page 1/7 HDFC LIFE - CANCER CARE CLAIM FORM PART A This form is to be filled by the claimant in block letters. The issue of this form is not to be taken as an admission
Personal Accident. Claim Form. Important Notes
 Personal Accident Claim Form Important Notes This claim form is to facilitate your claim in the event of you or a member of your family is confined to hospital while being Insured under a Personal Accident
Personal Accident Claim Form Important Notes This claim form is to facilitate your claim in the event of you or a member of your family is confined to hospital while being Insured under a Personal Accident
CLAIM FORM. Particulars Claim 1 Claim 2 Claim 3 Claim 4
 MDINDIA HEALTHCARE SERVICES (TPA) PVT. LTD. 302, Lalita Towers, Behind Railway Station, Near Hotel Rajpath Dinesh Mills Road, Vadodara- 390 005 (Gujarat). UAN Voice No. 1860-233-4446. UAN Fax No. 1860-233-4447
MDINDIA HEALTHCARE SERVICES (TPA) PVT. LTD. 302, Lalita Towers, Behind Railway Station, Near Hotel Rajpath Dinesh Mills Road, Vadodara- 390 005 (Gujarat). UAN Voice No. 1860-233-4446. UAN Fax No. 1860-233-4447
Grab. Prolonged Medical Leave Insurance Claim Form. Important Notes
 Grab Prolonged Medical Leave Insurance Claim Form Important Notes This claim form is to facilitate your claim in the event of you or a member of your family is Insured under a Personal Accident policy.
Grab Prolonged Medical Leave Insurance Claim Form Important Notes This claim form is to facilitate your claim in the event of you or a member of your family is Insured under a Personal Accident policy.
CLAIM FORM. Particulars Claim 1 Claim 2 Claim 3 Claim 4
 MDINDIA HEALTHCARE SERVICES (TPA) PVT. LTD. 18/13, WEA, Ground Floor, Ganga Plaza, Pusa Lane, Karol bagh, New Delhi - 110 005 UAN Voice No. 1860-233-4446. UAN Fax No. 1860-233-4447 E-mail ID: delhi@mdindia.com.
MDINDIA HEALTHCARE SERVICES (TPA) PVT. LTD. 18/13, WEA, Ground Floor, Ganga Plaza, Pusa Lane, Karol bagh, New Delhi - 110 005 UAN Voice No. 1860-233-4446. UAN Fax No. 1860-233-4447 E-mail ID: delhi@mdindia.com.
Issuance of this form does not amount to admission of any liability of under the policy on the part of the insurers
 The Oriental Insurance Company Limited HOSPITALISATION AND DOMICILIARY HOSPITALISATION BENEFIT POLICY CLAIM FORM Claim Number Issuance of this form does not amount to admission of any liability of under
The Oriental Insurance Company Limited HOSPITALISATION AND DOMICILIARY HOSPITALISATION BENEFIT POLICY CLAIM FORM Claim Number Issuance of this form does not amount to admission of any liability of under
Frequently Asked Questions (FAQs)
") Mediclaim Policy for Ex Employees of RITES Frequently Asked Questions (FAQs) 1. What is Mediclaim policy? A mediclaim insurance policy ensures that your and your family s medical expenses are borne, or
Mediclaim Policy for Ex Employees of RITES Frequently Asked Questions (FAQs) 1. What is Mediclaim policy? A mediclaim insurance policy ensures that your and your family s medical expenses are borne, or
Health Insurance Benefit plan Monster.com India Pvt Ltd. Family Health Plan (TPA) Limited. Hyderabad
 Limited. Hyderabad") Health Insurance Benefit plan 2016 2017 Monster.com India Pvt Ltd. Family Health Plan (TPA) Limited Hyderabad Medical Benefit Coverage Details Enrolment in the program Cashless Process Non-Cashless Claims
Health Insurance Benefit plan 2016 2017 Monster.com India Pvt Ltd. Family Health Plan (TPA) Limited Hyderabad Medical Benefit Coverage Details Enrolment in the program Cashless Process Non-Cashless Claims
Health Benefit plan EXCERS TECHNOLOGIES PVT LTD Family Health Plan (TPA) Limited. Hyderabad
 Limited. Hyderabad") Health Benefit plan 2017 2018 EXCERS TECHNOLOGIES PVT LTD Family Health Plan (TPA) Limited Hyderabad Hospitalization Insurance Cover Insurer: The Bharti Axa General Ins. Co. Ltd Coverage: 27 January 2017
Health Benefit plan 2017 2018 EXCERS TECHNOLOGIES PVT LTD Family Health Plan (TPA) Limited Hyderabad Hospitalization Insurance Cover Insurer: The Bharti Axa General Ins. Co. Ltd Coverage: 27 January 2017
HRDD CIRCULAR NO. 723
 Human Resources Development Division (Hospitalisation Cell), Head Office: New Delhi Phone No. 011-26174730 Email hrdhospitalisation@pnb.co.in FAX 011-26196491 November 19, 2015 TO ALL OFFICES HRDD CIRCULAR
Human Resources Development Division (Hospitalisation Cell), Head Office: New Delhi Phone No. 011-26174730 Email hrdhospitalisation@pnb.co.in FAX 011-26196491 November 19, 2015 TO ALL OFFICES HRDD CIRCULAR
Easy Travel Insurance CLAIM FORM
 Easy Travel Insurance Apollo Munich Health Insurance Co. Ltd. 10th Floor, Tower-B, Building No. 10, CLAIM FORM Issuance of this form does not amount to admission of any liability or a waiver of any of
Easy Travel Insurance Apollo Munich Health Insurance Co. Ltd. 10th Floor, Tower-B, Building No. 10, CLAIM FORM Issuance of this form does not amount to admission of any liability or a waiver of any of
MEDICLAIM CARD DOWNLOAD & IMPORTANT INFORMATION ABOUT MEDICLAIM POLICY
 MEDICLAIM CARD DOWNLOAD & IMPORTANT INFORMATION ABOUT MEDICLAIM POLICY Our Group Mediclaim Policy has been renewed through The Oriental Insurance Company Limited and TPA is Paramount Health Services (PHS).
MEDICLAIM CARD DOWNLOAD & IMPORTANT INFORMATION ABOUT MEDICLAIM POLICY Our Group Mediclaim Policy has been renewed through The Oriental Insurance Company Limited and TPA is Paramount Health Services (PHS).
Tata AIA Life Insurance Company Limited (hereinafter called the Company ) DEATH CLAIM INTIMATION - CUM - CLAIMANT S STATEMENT
 DEATH CLAIM INTIMATION - CUM - CLAIMANT S STATEMENT") Tata AIA Life Insurance Company Limited (hereinafter called the Company ) DEATH CLAIM INTIMATION - CUM - CLAIMANT S STATEMENT Guidelines / Notes: 1. Death benefit is payable subject to policy being inforce
Tata AIA Life Insurance Company Limited (hereinafter called the Company ) DEATH CLAIM INTIMATION - CUM - CLAIMANT S STATEMENT Guidelines / Notes: 1. Death benefit is payable subject to policy being inforce
FAQs Health Claims. Page 1 of 7
 FAQs Health Claims Index FAQs Related To Questions Page Number (From & To) General Claim Intimation Q 1 2 Cashless Claims Q2 To Q4 2 3 Reimbursement Claim Q5 To Q7 3 Claim Settlement Turnaround Time Q8
FAQs Health Claims Index FAQs Related To Questions Page Number (From & To) General Claim Intimation Q 1 2 Cashless Claims Q2 To Q4 2 3 Reimbursement Claim Q5 To Q7 3 Claim Settlement Turnaround Time Q8
Please tick to select status Singapore Citizen/PR International (non STP) International (STP)
 International (STP)") AXA INSURANCE PTE LTD 8 Shenton Way #24-01 AXA Tower Singapore 068811 Tel: (65) 6338 7288 Fax: (65) 6338 2552 www.axa.com.sg Please complete this claim from fully. Incomplete forms may delay claim settlement
AXA INSURANCE PTE LTD 8 Shenton Way #24-01 AXA Tower Singapore 068811 Tel: (65) 6338 7288 Fax: (65) 6338 2552 www.axa.com.sg Please complete this claim from fully. Incomplete forms may delay claim settlement
Overseas Secondment. Claim Form. Important Notes
 Overseas Secondment Claim Form Important Notes To facilitate the processing of your claim, you are required to complete Sections A, B and C for all claim submissions. The issue and acceptance of this form
Overseas Secondment Claim Form Important Notes To facilitate the processing of your claim, you are required to complete Sections A, B and C for all claim submissions. The issue and acceptance of this form
HDFC ERGO General Insurance Company Limited
 GROUP PERSONAL ACCIENT CLAIM FORM Claimant s Statement Form A ate of Birth: Name and address of employer: M M Marital Status: Married Unmarried Insured s Occupation: oes the insured have any other insurance?
GROUP PERSONAL ACCIENT CLAIM FORM Claimant s Statement Form A ate of Birth: Name and address of employer: M M Marital Status: Married Unmarried Insured s Occupation: oes the insured have any other insurance?
American Express Cardmember / Business Travel
 American Express Cardmember / Business Travel Claim Form The information requested and supporting documents required for your claim are detailed below each section. Further documents or information may
American Express Cardmember / Business Travel Claim Form The information requested and supporting documents required for your claim are detailed below each section. Further documents or information may
CyberSmart. Claim Form. Important Notes
 CyberSmart Claim Form Important Notes This claim form is to facilitate your claim in the event of you, a spouse or a dependent who is a named insured, has incurred expenses which falls within the definition
CyberSmart Claim Form Important Notes This claim form is to facilitate your claim in the event of you, a spouse or a dependent who is a named insured, has incurred expenses which falls within the definition
HDFC ERGO General Insurance Company Limited
 HFC ERGO General Insurance Company Limited INIVIUAL PERSONAL ACCIENT - CLAIM FORM Claimant s Statement INSURE INFORMATION Form A ate of Bir: Phone. (Off): Name and address of employer: M M Marital Status:
HFC ERGO General Insurance Company Limited INIVIUAL PERSONAL ACCIENT - CLAIM FORM Claimant s Statement INSURE INFORMATION Form A ate of Bir: Phone. (Off): Name and address of employer: M M Marital Status:
Easy Travel. Claim Form.
 Issuance of this form does not amount to admission of any liability or a waiver of any of the terms and conditions of the insurance contract. If any claim is in any manner dishonest or fraudulent, or is
Issuance of this form does not amount to admission of any liability or a waiver of any of the terms and conditions of the insurance contract. If any claim is in any manner dishonest or fraudulent, or is
SCBGH/PAOF/V1.2. Personal Account Opening Form
 SCBGH/PAOF/V1.2 Personal Account Opening Form NB: Before you sign this application form, please read our Client Terms, Current and Savings Account Terms and Personal Loan Terms, and other terms indicated
SCBGH/PAOF/V1.2 Personal Account Opening Form NB: Before you sign this application form, please read our Client Terms, Current and Savings Account Terms and Personal Loan Terms, and other terms indicated
TRAVEL INSURANCE (BUSINESS AND HOLIDAY) Claim Form
 Claim Form") SBI General Insurance Company Limited IRDA Reg. No. 144 dated 15/12/2009 CIN: U66000MH2009PLC190546 TRAVEL INSURANCE (BUSINESS AND HOLIDAY) Claim Form Call (Toll Free) 1800 22 1111 1800 102 1111 www.sbigeneral.in
SBI General Insurance Company Limited IRDA Reg. No. 144 dated 15/12/2009 CIN: U66000MH2009PLC190546 TRAVEL INSURANCE (BUSINESS AND HOLIDAY) Claim Form Call (Toll Free) 1800 22 1111 1800 102 1111 www.sbigeneral.in
Customer Guide Book. EasyHealth
 Customer Guide Book EasyHealth Apollo Munich Health Insurance Company Limited (AMHI) congratulates you on your health insurance choice and welcomes you into the select group of Easy Health policyholders.
Customer Guide Book EasyHealth Apollo Munich Health Insurance Company Limited (AMHI) congratulates you on your health insurance choice and welcomes you into the select group of Easy Health policyholders.
Disability/Sickness Claim
 AXA Builing 6 Chiswick Park 566 Chiswick High Roa Lonon W4 5HR 0370 900 0161 Step 1: Check Your Policy Documents Disability/Sickness Claim Important tes You must be 100% unable to work an be in active
AXA Builing 6 Chiswick Park 566 Chiswick High Roa Lonon W4 5HR 0370 900 0161 Step 1: Check Your Policy Documents Disability/Sickness Claim Important tes You must be 100% unable to work an be in active
SECTION 1 (To be completed by the Life Assured who is at least 18 years old or the Policyowner if the Life Assured is below 18 years old)
") C041017 PruCustomer Line: 1800-333 0 3333 CRISIS COVER CLAIM FORM Kidney Failure / Surgical Removal of One Kidney / Chronic Kidney Disease Major Organ (Kidney)Transplantation Important tes 1. Please note
C041017 PruCustomer Line: 1800-333 0 3333 CRISIS COVER CLAIM FORM Kidney Failure / Surgical Removal of One Kidney / Chronic Kidney Disease Major Organ (Kidney)Transplantation Important tes 1. Please note
( UNDER SECTION RULES 31(3) ) FORM OF APPLICATION FOR FINAL PAYMENT OF ZILLA PARISHAD PROVIDENT FUND BALANCE
 ) FORM OF APPLICATION FOR FINAL PAYMENT OF ZILLA PARISHAD PROVIDENT FUND BALANCE") A P P E N D I X ( H ) ( UNDER SECTION RULES 31(3) ) FORM OF APPLICATION FOR FINAL PAYMENT OF ZILLA PARISHAD PROVIDENT FUND BALANCE ( Retirement / Resignation / Removal / Transfer Of Balance / Death Case
A P P E N D I X ( H ) ( UNDER SECTION RULES 31(3) ) FORM OF APPLICATION FOR FINAL PAYMENT OF ZILLA PARISHAD PROVIDENT FUND BALANCE ( Retirement / Resignation / Removal / Transfer Of Balance / Death Case
SECTION 1 (To be completed by the Life Assured who is at least 18 years old or the Policyowner if the Life Assured is below 18 years old)
") C041017 TERMINAL ILLNESS CLAIM FORM PruCustomer Line: 1800-333 0 3333 Important tes 1. Please note that, under the policy terms and conditions, the policy may be void if any information provided in this
C041017 TERMINAL ILLNESS CLAIM FORM PruCustomer Line: 1800-333 0 3333 Important tes 1. Please note that, under the policy terms and conditions, the policy may be void if any information provided in this
Personal accident claim form
 The issue of this claim form does not imply an admission of liability by us. Only a fully completed and signed claim form can receive our further assessment and consideration. Index Sections 1, 2, 9 and
The issue of this claim form does not imply an admission of liability by us. Only a fully completed and signed claim form can receive our further assessment and consideration. Index Sections 1, 2, 9 and
CLAIMS FORM FOR GROUP TRAVEL INSURANCE. Claimant s Name : Claimant s Address: Phone No.(Mobile): Phone No.(Res) : ID:
: Phone No.(Res) : ID:") CLAIMS FORM FOR GROUP TRAVEL INSURANCE Claimant s Name : Claimant s Address: Phone No.(Mobile): Phone No.(Res) : E-mail ID: Policy Start Date : dd/mm/yyyy Policy End Date : dd/mm/yyyy In what capacity
CLAIMS FORM FOR GROUP TRAVEL INSURANCE Claimant s Name : Claimant s Address: Phone No.(Mobile): Phone No.(Res) : E-mail ID: Policy Start Date : dd/mm/yyyy Policy End Date : dd/mm/yyyy In what capacity
PERSONAL ACCIDENT OR SICKNESS CLAIM FORM
 PERSONAL ACCIDENT OR SICKNESS CLAIM FORM This form must be completed truthfully and accurately. The list of documents required is not exhaustive and we reserve our right to request from you any additional
PERSONAL ACCIDENT OR SICKNESS CLAIM FORM This form must be completed truthfully and accurately. The list of documents required is not exhaustive and we reserve our right to request from you any additional
FAQ S on Medical Insurance Scheme. 1) Who is a United India TPA? And How will I know my United India TPA?
 Who is a United India TPA? And How will I know my United India TPA?") FAQ S on Medical Insurance Scheme 1) Who is a United India TPA? And How will I know my United India TPA? Third Party Administrator is An IRDA licensed TPA who is engaged by the Insurance Company in Servicing
FAQ S on Medical Insurance Scheme 1) Who is a United India TPA? And How will I know my United India TPA? Third Party Administrator is An IRDA licensed TPA who is engaged by the Insurance Company in Servicing
HDFC ERGO General Insurance Company Limited
 HFC ERGO General Insurance Company Limited GROUP PERSONAL ACCIENT CLAIM FORM Claimant s Statement INSURE INFORMATION Form A ate of Bir: Phone. (Off): Name and address of employer: M M Marital Status: Married
HFC ERGO General Insurance Company Limited GROUP PERSONAL ACCIENT CLAIM FORM Claimant s Statement INSURE INFORMATION Form A ate of Bir: Phone. (Off): Name and address of employer: M M Marital Status: Married
SWAVALAMBAN National Pension System (NPS)
") Form 503 Page 1 SWAVALAMBAN National Pension System (NPS) Withdrawal of Accumulated Pension Wealth by Claimant due to the death of the subscriber (Please fill all the details in CAPITAL LETTERS & in BLACK
Form 503 Page 1 SWAVALAMBAN National Pension System (NPS) Withdrawal of Accumulated Pension Wealth by Claimant due to the death of the subscriber (Please fill all the details in CAPITAL LETTERS & in BLACK
CRISIS COVER CLAIM FORM Benign Brain Tumour / Surgical Removal of Pituitary Tumor / Surgery for Subdural Hematoma
 C041017 PruCustomer Line: 1800-333 0 3333 CRISIS COVER CLAIM FORM Benign Brain Tumour / Surgical Removal of Pituitary Tumor / Surgery for Subdural Hematoma Important tes 1. Please note that, under the
C041017 PruCustomer Line: 1800-333 0 3333 CRISIS COVER CLAIM FORM Benign Brain Tumour / Surgical Removal of Pituitary Tumor / Surgery for Subdural Hematoma Important tes 1. Please note that, under the
RAFFLES SHIELD CLAIM FORM
 RAFFLES SHIELD CLAIM FORM IMPORTANT NOTES: It is important to read the notes below before you complete the claim form. PREPARING REQUIRED DOCUMENTS Please complete this form in FULL and submit the following
RAFFLES SHIELD CLAIM FORM IMPORTANT NOTES: It is important to read the notes below before you complete the claim form. PREPARING REQUIRED DOCUMENTS Please complete this form in FULL and submit the following
CASHLESS PROCESS (How to avail cashless)
") FIS CLAIM PROCESS CASHLESS PROCESS (How to avail cashless) Employee need to contact the hospital prior to His/ Her Admission and provides Pre-authorization request form to VIPUL MED COPR through Hospital
FIS CLAIM PROCESS CASHLESS PROCESS (How to avail cashless) Employee need to contact the hospital prior to His/ Her Admission and provides Pre-authorization request form to VIPUL MED COPR through Hospital
SHRAVAK AROGYAM PHASE-II
 FREQUENTLY ASKED QUESTIONS 1. About JIO? JIO is a vibrant organization for total unity of Jains, to serve all living beings & bring all round progress. JIO intends to be the global organization of visionaries
FREQUENTLY ASKED QUESTIONS 1. About JIO? JIO is a vibrant organization for total unity of Jains, to serve all living beings & bring all round progress. JIO intends to be the global organization of visionaries
Reliance Wealth + Health Plan
 Reliance Wealth + Health Plan CLAIM FORM HOSPITAL CASH BENEFIT (To be filled in block letters by the Claimant/Principal Insured) Please answer all questions carefully. Also attach the copy of the health
Reliance Wealth + Health Plan CLAIM FORM HOSPITAL CASH BENEFIT (To be filled in block letters by the Claimant/Principal Insured) Please answer all questions carefully. Also attach the copy of the health
Claim form. Hospitalisation & Medical Expense
 Contact us for more information: T 0860 223 252 F 011 783 0812 myclaim@chubb.com Claim form Hospitalisation & Medical Expense Please write in black ink and use block capital letters. Please return the
Contact us for more information: T 0860 223 252 F 011 783 0812 myclaim@chubb.com Claim form Hospitalisation & Medical Expense Please write in black ink and use block capital letters. Please return the
Form 103-GD Page 1 National Pension System (NPS)
") Form 103-GD Page 1 National Pension System (NPS) Withdrawal of Accumulated Pension Wealth by Claimant due to the death of the subscriber (Please fill all the details in CAPITAL LETTERS & in BLACK INK only.)
Form 103-GD Page 1 National Pension System (NPS) Withdrawal of Accumulated Pension Wealth by Claimant due to the death of the subscriber (Please fill all the details in CAPITAL LETTERS & in BLACK INK only.)
Tiger Airways Pte Ltd Claim Form
 Tiger Airways Pte Ltd Claim Form IMPORTANT NOTE: Please answer all questions contained in this claim form as leaving items blank, using ticks, dashes and N/A may make it necessary for us to return your
Tiger Airways Pte Ltd Claim Form IMPORTANT NOTE: Please answer all questions contained in this claim form as leaving items blank, using ticks, dashes and N/A may make it necessary for us to return your
NATIONAL INSURANCE COMPANY LTD. (Subsidiary of General Insurance Corporation of India) Regd. Office: 3, MIDDLETON STREET.
 Regd. Office: 3, MIDDLETON STREET.") NATIONAL INSURANCE COMPANY LTD. (Subsidiary of General Insurance Corporation of India) Regd. Office: 3, MIDDLETON STREET. CALCUTTA 7000 071 ISSUING OFFICE HOSPITALISATION AND DOMICILIARY HOSPITALISATION
NATIONAL INSURANCE COMPANY LTD. (Subsidiary of General Insurance Corporation of India) Regd. Office: 3, MIDDLETON STREET. CALCUTTA 7000 071 ISSUING OFFICE HOSPITALISATION AND DOMICILIARY HOSPITALISATION
 This is to certify that following are the family members under (HUF) S. No. Name Gender (Male/Female) Relationship with Karta PAN No./ Birth Certificate No.* Date of Birth 1. D D M M Y Y Y Y 2. D D M M
This is to certify that following are the family members under (HUF) S. No. Name Gender (Male/Female) Relationship with Karta PAN No./ Birth Certificate No.* Date of Birth 1. D D M M Y Y Y Y 2. D D M M
maxima APPLICATION FORM
 axia APPLICATION OR SECTION 1 CHOICE O OPTION Choose ONE prouct option b placing x in the appropriate box Coprehensive Options Saver Options Hospital Plans AXIA PLUS AXIA ADVANCED AXIA CORE AXIA EXEC AXIA
axia APPLICATION OR SECTION 1 CHOICE O OPTION Choose ONE prouct option b placing x in the appropriate box Coprehensive Options Saver Options Hospital Plans AXIA PLUS AXIA ADVANCED AXIA CORE AXIA EXEC AXIA
AIA SINGAPORE ACCIDENT & HOSPITALISATION CLAIM FORM
 AIA SINGAPORE ACCIDENT & HOSPITALISATION CLAIM FORM Important Notes: 1) AIA HealthShield Gold claims for Singaporeans and Permanent Residents must be submitted electronically via the medical institutions
AIA SINGAPORE ACCIDENT & HOSPITALISATION CLAIM FORM Important Notes: 1) AIA HealthShield Gold claims for Singaporeans and Permanent Residents must be submitted electronically via the medical institutions
Claim Form - Travel Insurance
 Claim Form - Travel Insurance Important tice: To enable us to process your claim, please submit the duly completed claim form with supporting documents in original as listed in the subsequent section.
Claim Form - Travel Insurance Important tice: To enable us to process your claim, please submit the duly completed claim form with supporting documents in original as listed in the subsequent section.
MEDICAL LIFESTYLE CLAIM FORM IN RESPECT OF:
 Liberty Group Limited an Authorised Financial Services Provider Liberty Centre, 1 Ameshoff Street, Braamfontein, Johannesburg, 2001 Private Bag X78, Braamfontein, 2017 Contact Centre number: 0860 102 219
Liberty Group Limited an Authorised Financial Services Provider Liberty Centre, 1 Ameshoff Street, Braamfontein, Johannesburg, 2001 Private Bag X78, Braamfontein, 2017 Contact Centre number: 0860 102 219
HDFC ERGO General Insurance Company Limited
 HDFC ERGO General Insurance Company Limited Overseas Travel Insurance Claim Form (To be filled in by the Insured Policyholder or Insured s Representative duly authorised by Power of Attorney. Issuance
HDFC ERGO General Insurance Company Limited Overseas Travel Insurance Claim Form (To be filled in by the Insured Policyholder or Insured s Representative duly authorised by Power of Attorney. Issuance
FAQ ON MEDICAL INSURANCE SCHEME FOR RETIREES
 FAQ ON MEDICAL INSURANCE SCHEME FOR RETIREES What is the policy number? Policy No. 500100/48/15/14/00000522 What is the Policy Period? 06/11/2015 to 31/10/2016 Who are covered under this policy? Employee
FAQ ON MEDICAL INSURANCE SCHEME FOR RETIREES What is the policy number? Policy No. 500100/48/15/14/00000522 What is the Policy Period? 06/11/2015 to 31/10/2016 Who are covered under this policy? Employee
THE ORIENTAL INSURANCE COMPANY LIMITED Regd. Office: Oriental House, A-25/27, Asaf Ali Road, New Delhi
 THE ORIENTAL INSURANCE COMPANY LIMITED Regd. Office: Oriental House, A-25/27, Asaf Ali Road, New Delhi 110 002. Issuing Office HOSPITALISATION AND DOMICILIARY HOSPITALISATION BENEFIT POLICY CLAIM FORM
THE ORIENTAL INSURANCE COMPANY LIMITED Regd. Office: Oriental House, A-25/27, Asaf Ali Road, New Delhi 110 002. Issuing Office HOSPITALISATION AND DOMICILIARY HOSPITALISATION BENEFIT POLICY CLAIM FORM
Personal Account Application Form Joint Personal Current Account PLEASE COMPLETE IN BLOCK CAPITALS
 Personal Account Application Form Joint Personal Current Account PLEASE COPLETE IN BLOCK CAPITALS IPORTANT NOTE: This Authorisation and Application Form is only appropriate for requests to open a joint
Personal Account Application Form Joint Personal Current Account PLEASE COPLETE IN BLOCK CAPITALS IPORTANT NOTE: This Authorisation and Application Form is only appropriate for requests to open a joint
PARTICULARS OF POLICYHOLDER / INSURED PERSON / CLAIMANT (to be completed for all claims) NRIC/Passport No.
 NRIC/Passport No.") Travel Claim Form The acceptance of this Form is NOT an admission of liability on the part of HL Assurance Pte. Ltd.. Any documentary proof or report required by HL Assurance Pte. Ltd. shall be furnished
Travel Claim Form The acceptance of this Form is NOT an admission of liability on the part of HL Assurance Pte. Ltd.. Any documentary proof or report required by HL Assurance Pte. Ltd. shall be furnished
GROUP DISABILITY CLAIM FORM
 GROUP DISABILITY CLAIM FORM Dear insured employee, We are sorry to learn about your illness/accident. In order for us to process your claim, we require the following: (1) Group Disability Claim Form (2)
GROUP DISABILITY CLAIM FORM Dear insured employee, We are sorry to learn about your illness/accident. In order for us to process your claim, we require the following: (1) Group Disability Claim Form (2)
EDUCATION MAINTENANCE ALLOWANCE (EMA) SESSION 2010/11 COMPLETE FORM IN BLACK OR BLUE INK
 SESSION 2010/11 COMPLETE FORM IN BLACK OR BLUE INK") B62449 EA Glasgow 14/7/10 14:52 Page 1 Glasgow City Council Customer and Business Services Grant Section PO Box 26816 GLASGOW G2 9AF Tel: 0141 276 1177 Email: frances.ross@education.glasgow.gov.uk EUCATION
B62449 EA Glasgow 14/7/10 14:52 Page 1 Glasgow City Council Customer and Business Services Grant Section PO Box 26816 GLASGOW G2 9AF Tel: 0141 276 1177 Email: frances.ross@education.glasgow.gov.uk EUCATION
What to do on the death of an investor The next steps. Please note this booklet contains important client information and closure forms.
 What to o on the eath of an investor The next steps Please note this booklet contains iportant client inforation an closure fors. Contents 02 The Probate proceure 03 What ocuents are neee? 04 Ke points
What to o on the eath of an investor The next steps Please note this booklet contains iportant client inforation an closure fors. Contents 02 The Probate proceure 03 What ocuents are neee? 04 Ke points
Blue Care Income Protection Claim Form
 Blue Care Income Protection Claim Form INCOME PROTECTION CLAIMS In order to alleviate any delay in the processing time of your claim, please ensure the following: The claim form is returned with all fields
Blue Care Income Protection Claim Form INCOME PROTECTION CLAIMS In order to alleviate any delay in the processing time of your claim, please ensure the following: The claim form is returned with all fields