NEW PATIENT PACKET includes the following forms:
|
|
|
- Brian Alexander
- 6 years ago
- Views:
Transcription
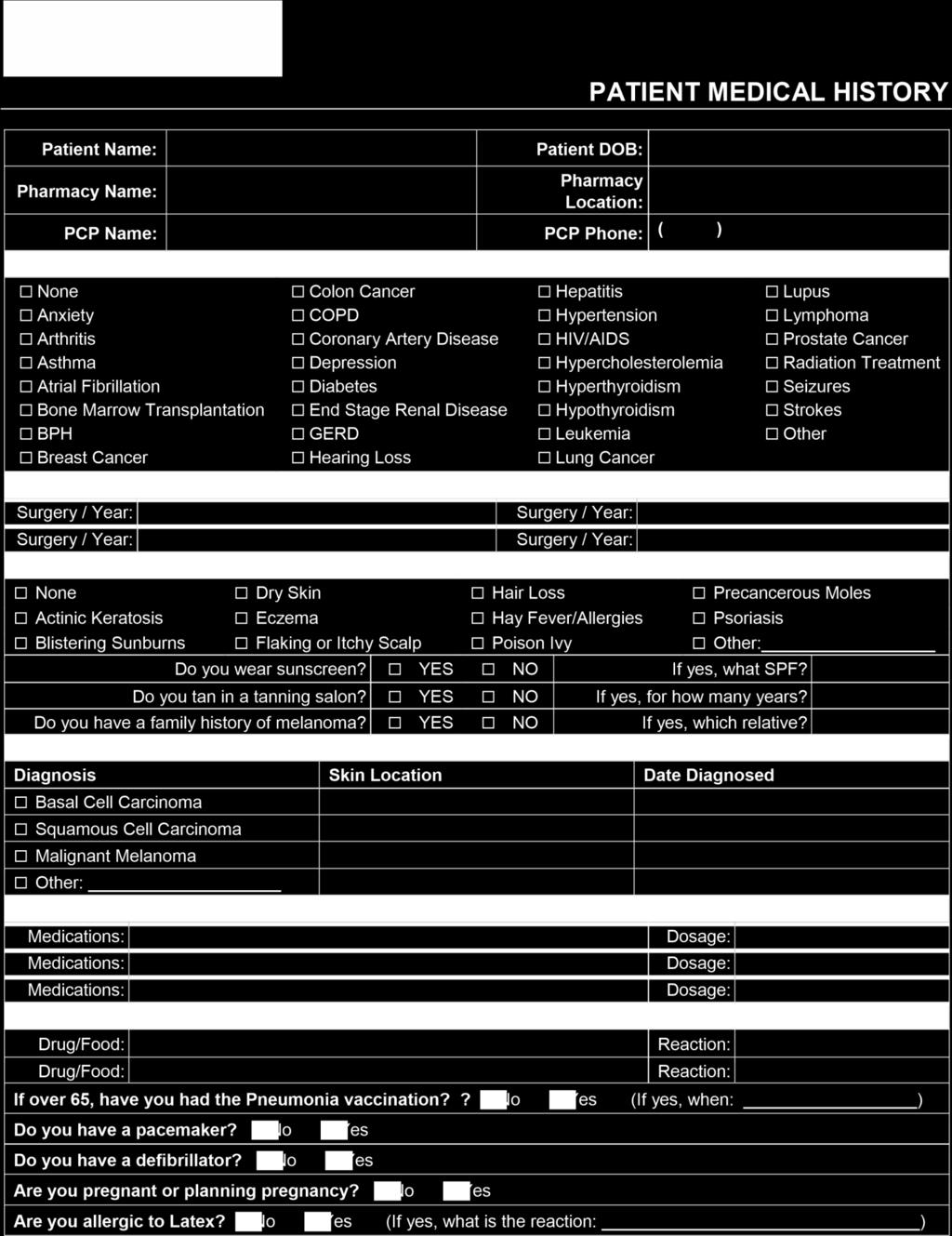
1 Thank you for choosing U.S. Dermatology Partners! We appreciate the opportunity to care for your health. REQUIRED ITEMS NEEDED FOR YOUR APPOINTMENT Completed New Patient Packet (see below) Valid Government Issued Photo ID Insurance Card(s) Form of Payment Written Insurance Referral provided by your PCP (if applicable) NEW PATIENT PACKET includes the following forms: New Patient Registration Form Acknowledgement of Office Policies Patient Consents Financial Policies PHI Communication Preferences Notice of Privacy Practices Medical History
2 NEW PATIENT REGISTRATION PATIENT INFORMATION Print Legal Name: DOB: Patient Nickname: Address: Home Phone: Cell Phone: PCP Name: How did you hear about our office? PCP Phone Number: COMMUNICATION PREFERENCES Preferred communication method for appointment reminders, patient surveys, office notifications, etc. Yes No Phone Call Yes No SMS (Text) Message Yes No Voice Reminders Yes No SPOUSE, PARENT, LEGAL GUARDIAN, EMERGENCY CONTACT INFORMATION Printed Name: Relationship: Address: Home Phone: Cell Phone: PRIMARY INSURANCE Insured s Full Name: Insurance Company: Insured s DOB: Sex: M / F Member No: Group No: Insured s Address: REV 08/2017
3 NEW PATIENT REGISTRATION SECONDARY INSURANCE Insured s Full Name: Insurance Company: Insured s DOB: Sex: M / F Member No: Group No: Insured s Address: RESPONSIBLE FINANCIAL PARTY (fill out if other than self) Printed Name: Relationship: Address: Home Phone: Cell Phone: By signing below, I certify that the information above is true and correct to the best of my knowledge. REV 08/2017
4 AC KNOWLEDGEMENT OF OFFICE P OLICIES Notice of Privacy Practices I have read a copy of the Notice of Privacy Practices which explains how my medical information will be used and disclosed. I authorize the release of any medical information necessary to evaluate and/or treat my condition. I further authorize the release of any medical information necessary to process insurance claims on my behalf. I understand that I am entitled to receive a copy of the Notice of Privacy Practices. Cancellation Policy for Medical Appointments It is my responsibility to call the office to cancel at least 24 hours prior to the scheduled appointment. U.S. Dermatology Partners reserves the right to charge a fee if the appointment is not cancelled at least 24 hours in advance. Additionally, the office reserves the right to reschedule appointments for which I am more than 15 minutes late. Cancellation Policy for Cosmetic Appointments Some types of cosmetic procedures or surgeries require a down payment to reserve the procedure date. U.S. Dermatology Partners reserves the right to charge a fee if the appointment is not cancelled at least 72 hours in advance. Cosmetic Retail Sales All retail sales are final. Due to the nature of the cosmetic products, no exchanges/refunds are allowed. Payment Policies Payment is due at the time of service. This amount includes any co-pay as well as the insurance deductible or co-insurance. I understand that I am financially responsible for all charges for services rendered on my behalf or on behalf of my dependent, whether or not they are covered by my insurance. Appointment Reminders I understand that I will receive appointment reminders and information on services via telephone, and/or text message based on the contact information I have provided. I further understand that I will have the option to opt out of future reminders. By signing below, I certify that I have read the above information and have had any questions answered. My signature also certifies my understanding and agreement with the above information. REV 02/2017
5 PATIENT CONSENTS Consent for Treatment I authorize U.S. Dermatology Partners to provide any healthcare services that my provider deems necessary for diagnosis and/or treatment. If a biopsy is performed, I authorize the dermatopathologist to send my specimen for a second opinion and/or obtain special tests, if medically necessary to ensure an accurate diagnosis. I understand that additional costs may result and that I will be responsible for any remaining balance that is not covered by my insurance company, Medicare and/or supplemental policy. Consent for Filing Insurance Claims I understand that in order to file claims and release medical information to any insurance companies I have listed in my financial record, U.S. Dermatology Partners is required to keep my signature on file. I hereby authorize U.S. Dermatology Partners to receive benefits directly from my insurance company when an assigned claim is filed. I also authorize U.S. Dermatology Partners to appeal any denials to my insurance companies on my behalf and authorize the release of any medical information to my insurance companies that is necessary for the processing of claims. Consent for Electronic Prescription History I understand that in order to offer the best patient care, U.S. Dermatology Partners will retrieve my prescription history that has been ordered and filled through Surescripts. I authorize U.S. Dermatology Partners to import the prescription history obtained through Surescripts into my electronic chart. Consent for Photos I understand that in the course of treatment photographs may be taken for clinical and educational purposes. No audio taping, videotaping, or photography is allowed by non-staff members. By signing below, I certify that I have read the above information and have had any questions answered. My signature also certifies my understanding and agreement with the above information. Rev 7/2017
6 FINANCIAL POLICIES Payment is required at the time services are rendered. We are allowed by contract with your insurance company to collect your co-payment(s) and/or co-insurance and any unmet deductible at the time of service. For patients with private insurance where we have no contract, you will be required to pay for your services in full at the time of service. I understand I will be responsible for any remaining balance not covered by my insurance company, Medicare and/or my supplemental policy. This also includes the full amount of any cosmetic services. Please contact your insurance company to verify benefits and coverage information. I understand that if I have a surgical procedure or biopsy performed, there are two charges: (1) a charge by the provider for collecting the Biopsy; and (2) a charge to examine the specimen by a Pathologist (who is chosen by my Rendering Provider). I understand that I will be billed separately by the Pathologist (also a medical doctor) who performs the reading. I understand that my insurance company may have a preferred laboratory for blood work. It is my responsibility to know which preferred laboratory I need to use. It is also my responsibility to inform my provider of this at the time services are rendered. I understand that a $25 returned check fee will be assessed to my account for any checks returned by my financial institution. By signing below, I certify that I have read the above information and have had any questions answered. My signature also certifies my understanding and agreement with the above information. REV 02/2017
7 PHI COMMUNICATION PREFERENCES I authorize U.S. Dermatology Partners to disclose any and all details of my medical diagnoses, treatment, and billing/claims information to the individuals listed below. This authorization is voluntary and I understand that I have the right to revoke this authorization by submitting a written request to the office. I understand that the information disclosed under this authorization may be disclosed again by the person or organization to which it is released. I understand that the below list may not be exhaustive and that my protected health information (PHI) may be disclosed to additional individuals based on my written authorization or as indicated in our Notice of Privacy Practices. This authorization shall remain in effect indefinitely unless revoked in writing by me. I elect not to authorize disclosure to any individuals at this time Check all that apply First and Last Name: Relationship: Telephone Number Medical Billing Communication for benign (non-cancerous) test results I hereby allow all benign (non-cancerous) test results to be put in a voice message on the phone number indicated in the box. Telephone Number By signing below, I certify that I have read the above information and have had any questions answered. My signature also certifies my understanding and agreement with the above information. REV 02/2017
8 As required by the Health Insurance Portability and Accountability Act of 1996 (HIPAA) A. OUR COMMITMENT TO YOUR PRIVACY Our practice is dedicated to maintaining the privacy of your individually identifiable health information. In conducting our business, we will create records regarding you and the treatment and services we provide to you. We are required by law to maintain the confidentiality of health information that identifies you. We also are required by law to provide you with this notice of our legal duties and the privacy practices that we maintain in our practice concerning your protected health information (PHI). By federal and state law, we must follow the terms of the notice of privacy practices that we have in effect at the time. We realize that these laws are complicated, but we must provide you with the following important information: How we may use and disclose your PHI Your privacy rights regarding your PHI Our obligations concerning the use and disclosure of your PHI The terms of this notice apply to all records containing your PHI that are created or retained by our practice. We reserve the right to revise or amend this Notice of Privacy Practices. Any revision or amendment to this notice will be effective for all of your records that our practice has created or maintained in the past, and for any of your records that we may create or maintain in the future. Our practice will post a copy of our current Notice in our offices in a visible location at all times, and you may request a copy of our most current Notice at any time. B. IF YOU HAVE QUESTIONS ABOUT THIS NOTICE, PLEASE CONTACT: U.S. Dermatology Partners Compliance/Privacy Officer or Surgery Center Administrator 5310 Harvest Hill Rd, Ste. 290, Dallas, TX compliance@usdermpartners.com C. WE MAY USE AND DISCLOSE YOUR PROTECTED HEALTH INFORMATION (PHI) IN THE FOLLOWING WAYS: 1. Treatment. Our practice may use your PHI to treat you. Many of the people who work for our practice including, but not limited to, our doctors and nurses may use or disclose your PHI in order to treat you or to assist others in your treatment. 2. Payment. Our practice may use and disclose your PHI in order to bill and collect payment for the services and items you may receive from us. 3. Health Care Operations. Our practice, and its affiliated entities and management company, may use and disclose your PHI to operate our business. As examples of the ways in which we may use and disclose your information for our operations, our practice may use your PHI to evaluate the quality of care you received from us, or to conduct costmanagement and business planning activities for our practice. 4. Appointment Reminders. Our practice may use and disclose your PHI to contact you and remind you of an appointment. We will notify you about your appointment utilizing an automated phone system, a personal call, text or by mail. This notification may involve leaving a message on an answering machine or other automated or electronic equipment for such purposes, which could (potentially) be received or intercepted by others. 5. Sign In Sheet. We may use and disclose medical information about you by having you sign in when you arrive at our office. We may also call out your name when we are ready to see you. 6. Treatment Options. Our practice may use and disclose your PHI to inform you of potential treatment options or alternatives. 7. Health-Related Benefits and Services. Our practice may use and disclose your PHI to inform you of health-related benefits or services that may be of interest to you. 8. Release of Information to Family/Friends. Our practice will routinely disclose to your responsible party(ies) the PHI directly relevant to his/her involvement with your health care, PHI related to payment of your health care, and PHI used for notification purposes. Our practice may release your PHI to another responsible party(ies) you identify, that is involved in your care. 9. Marketing. We may contact you to give you information about products or services related to your treatment, or care. We will not otherwise use or disclose your medical information for marketing purposes, without your prior written authorization. 10. Sale of Health Information. We will not sell your health information without your prior written authorization. REV 02/2017 NOTICE OF PRIVACY PRACTICES 11. Disclosures Required By Law. Our practice will use and disclose your PHI when we are required to do so by federal, state or local law. 12. Breach Notification. In the case of a breach of unsecured protected health information, we will notify you as required by law. D. USE AND DISCLOSURE OF PHI IN SPECIAL CIRCUMSTANCES The following categories describe unique scenarios in which we may use or disclose your protected health information: 1. Public Health Risk Reporting. Our practice may disclose your PHI to public health authorities that are authorized by law. For example, we are required to report certain communicable diseases to the state s public health department. 2. Law Enforcement. Your health information may be disclosed to law enforcement agencies, military, and national security without your permission, to support government audits and inspections, to facilitate law enforcement investigations, and to comply with government mandated reporting. 3. Workers Compensation. Our practice may release your PHI for workers compensation and similar programs that provide benefits for work-related injuries or illnesses. E. YOUR RIGHTS REGARDING YOUR PHI You have the following rights regarding the PHI that we maintain about you. These include: The right to request restrictions on the use and disclosure of your protected health information, including to request that a health plan not be informed of treatment for which patient paid entirely out of pocket. The right to prohibit the sale of your protected health information, its use for marketing purposes, or participation in research. The right to request to receive confidential communications concerning your medical condition and treatment in a specific manner. The right to inspect and obtain copies of your protected health information. The right to amend or submit corrections to your protected health information The right to receive an accounting of how and to whom your protected health information has been disclosed outside of our practice if not for treatment, payment, or health care operations. The right to file a complaint if you believe your privacy rights have been violated. Please file your complaint in writing. You will not be penalized for filing a complaint. The right to receive a printed copy of this notice. All requests must be in writing and directed to U.S. Dermatology Partners, Compliance/Privacy Officer at 5310 Harvest Hill Rd, Ste. 290, Dallas, TX Our practice may charge a fee for the costs associated with any request. F. RIGHT TO PROVIDE AN AUTHORIZATION FOR OTHER USES AND DISCLOSURES. Our practice will obtain your written authorization for uses and disclosures that are not identified by this notice or permitted by applicable law. Any authorization you provide to us regarding the use and disclosure of your PHI may be revoked at any time in writing. After you revoke your authorization, we will no longer use or disclose your PHI for the reasons described in the authorization. Please note, we are required to retain records of your care. If you believe your privacy rights have been violated, you may complain to the secretary of the U.S. Department of Health and Human Services or to the Compliance/Privacy Officer listed below. There will not be retaliation against you for filing a complaint. Again, if you have any questions regarding this notice or our health information privacy policies, please contact: U.S. Dermatology Partners Compliance/Privacy Officer 5310 Harvest Hill Rd, Suite 290, Dallas, TX compliance@usdermpartners.com

9 REV 07/2017
PATIENT INFORMATION PATIENT INFORMATION. Middle Initial: Nickname: Date of Birth: Marital Status: Address: City: State: Zip Code:
 PATIENT INFORMATION PATIENT INFORMATION First Name: Last Name: Middle Initial: Nickname: Date of Birth: Sex: Marital Status: Address: City: State: Zip Code: Home Phone: Cell Phone: Email: How did you hear
PATIENT INFORMATION PATIENT INFORMATION First Name: Last Name: Middle Initial: Nickname: Date of Birth: Sex: Marital Status: Address: City: State: Zip Code: Home Phone: Cell Phone: Email: How did you hear
It is very important to bring the following to your first visit:
 Dear New Patient: Welcome and thank you for choosing Capital Digestive Care! The enclosed packet contains important information for your upcoming appointment as well as our new patient registration forms.
Dear New Patient: Welcome and thank you for choosing Capital Digestive Care! The enclosed packet contains important information for your upcoming appointment as well as our new patient registration forms.
INSURANCE INFORMATION
 PATIENT INFORMATION Last Name First Name M.I. Marital Status: Married Single Divorced Widowed Social Security No.: - - Birth Date: / / Sex: M F Place of Birth: Driver s License Number: Preferred Language:
PATIENT INFORMATION Last Name First Name M.I. Marital Status: Married Single Divorced Widowed Social Security No.: - - Birth Date: / / Sex: M F Place of Birth: Driver s License Number: Preferred Language:
First Name: Middle Name: Last Name: Preferred Name: Address: City: State: Zip: Mother s First & Last Name: Mother s Home Phone: Mother s Work Phone:
 Patient Information First Name: Middle Name: Last Name: Date of Birth: Gender: M F Preferred Name: Address: City: State: Zip: Contact Information Mother s First & Last Name: Mother s Address (If different
Patient Information First Name: Middle Name: Last Name: Date of Birth: Gender: M F Preferred Name: Address: City: State: Zip: Contact Information Mother s First & Last Name: Mother s Address (If different
Trinity Family Physicians
 Trinity Family Physicians Consent and Authorization for Minors By law, a healthcare provider must attempt to contact a birth / custodial parent or legal guardian prior to rendering treatment to a minor
Trinity Family Physicians Consent and Authorization for Minors By law, a healthcare provider must attempt to contact a birth / custodial parent or legal guardian prior to rendering treatment to a minor
PHARMACY INFORMATION
 NAAMAN CLINIC TODAY S DATE: Prefix Mr. Mrs. Miss Ms. Dr. Preferred Name: Patient s Name Address: First Middle Last Street & Apt # City State Zip SS# Birthdate Age: Sex: Female Male Marital Status: Single
NAAMAN CLINIC TODAY S DATE: Prefix Mr. Mrs. Miss Ms. Dr. Preferred Name: Patient s Name Address: First Middle Last Street & Apt # City State Zip SS# Birthdate Age: Sex: Female Male Marital Status: Single
PLEASE PRINT CLEARLY
 PATIENT INFORMATION FORM Rev. 02/2018 PLEASE PRINT CLEARLY New Patient Name Change Address Change Insurance Policy/Holder Change PATIENT INFORMATION Last Name: _ First Name: Middle Initial: DOB: Sex: Male
PATIENT INFORMATION FORM Rev. 02/2018 PLEASE PRINT CLEARLY New Patient Name Change Address Change Insurance Policy/Holder Change PATIENT INFORMATION Last Name: _ First Name: Middle Initial: DOB: Sex: Male
Policies and information:
 Policies and information: Basic Policies: Please be on time for your appointments. If you are late for your scheduled appointment, there is a chance that you will be rescheduled. We require at least 24
Policies and information: Basic Policies: Please be on time for your appointments. If you are late for your scheduled appointment, there is a chance that you will be rescheduled. We require at least 24
MasterCare Physical Therapy, Inc.
 Patient Financial Responsibility To all of our Patients: We will, as a courtesy, file your insurance claims for you. Please be advised that it is solely your responsibility to know and to understand your
Patient Financial Responsibility To all of our Patients: We will, as a courtesy, file your insurance claims for you. Please be advised that it is solely your responsibility to know and to understand your
GREENWOOD DERMATOLOGY
 GREENWOOD DERMATOLOGY Larry J. Buckel, M.D. Thomas J. Eads, M.D. Laura T. Stitle, M.D. Thank you for choosing Greenwood Dermatology for your Dermatologic needs. Dermatologists are the experts in the diagnosis
GREENWOOD DERMATOLOGY Larry J. Buckel, M.D. Thomas J. Eads, M.D. Laura T. Stitle, M.D. Thank you for choosing Greenwood Dermatology for your Dermatologic needs. Dermatologists are the experts in the diagnosis
Please list any doctors you would like us to coordinate with for your medical care: Primary Care Doctor: Other Doctor:
 D E R M A T O L O G Y D E R M A T O P A T H O L O G Y M O H S M I C R O G R A P H I C S U R G E R Y P L A S T I C S U R G E R Y Patient Information: Patient Name: Date of Birth: Sex: Marital Status: Mailing
D E R M A T O L O G Y D E R M A T O P A T H O L O G Y M O H S M I C R O G R A P H I C S U R G E R Y P L A S T I C S U R G E R Y Patient Information: Patient Name: Date of Birth: Sex: Marital Status: Mailing
Important Facts Regarding Our Practice
 Important Facts Regarding Our Practice CANCELLATION or BROKEN APPOINTMENTS: Our time is as valuable as yours and the other patients scheduled to come in. We are able to extend a no charge fee to our patients
Important Facts Regarding Our Practice CANCELLATION or BROKEN APPOINTMENTS: Our time is as valuable as yours and the other patients scheduled to come in. We are able to extend a no charge fee to our patients
Long Pond Pediatrics & Osteopathy Dr. Sabine M. Schmitt, DO, FAAP, C.S.P.O.M.M. Dr. Shoshana Katz, MD, FAAP Dr. Kimberly Ingalls, MD, FAAP, M.P.
 Today s Date Long Pond Pediatrics & Osteopathy Dr. Sabine M. Schmitt, DO, FAAP, C.S.P.O.M.M. Dr. Shoshana Katz, MD, FAAP Dr. Kimberly Ingalls, MD, FAAP, M.P.H NAME OF PATIENT (CHILD) DOB SSN of child SEX
Today s Date Long Pond Pediatrics & Osteopathy Dr. Sabine M. Schmitt, DO, FAAP, C.S.P.O.M.M. Dr. Shoshana Katz, MD, FAAP Dr. Kimberly Ingalls, MD, FAAP, M.P.H NAME OF PATIENT (CHILD) DOB SSN of child SEX
Grayson and Associates, P. C.
 Grayson and Associates, P. C. PATIENT INFORMATION Patient Name Date of Birth Social Security Number - - Male Female Mailing Address City State Zip Email Is it ok for Grayson and Associates, P.C. to communicate
Grayson and Associates, P. C. PATIENT INFORMATION Patient Name Date of Birth Social Security Number - - Male Female Mailing Address City State Zip Email Is it ok for Grayson and Associates, P.C. to communicate
425 North Wendover Road Charlotte, NC Birthdate: Social Security #: Male Female
 425 North Wendover Road Charlotte, NC 28211 PATIENT INFORMATION: Patient s Legal Name: Nickname: Birthdate: Social Security #: Male Female Status: Minor (under 18) Single Married Separated Divorced Widowed
425 North Wendover Road Charlotte, NC 28211 PATIENT INFORMATION: Patient s Legal Name: Nickname: Birthdate: Social Security #: Male Female Status: Minor (under 18) Single Married Separated Divorced Widowed
Would you like to receive s with special offers from Carolina Vein Center? yes no
 Carolina Vein Center Patient Information Name: Date: Address: Home Phone: City: State: Zip: Work Phone: SS#: Marital Status: Occupation: Date of Birth: _ Cell Phone: Emergency Contact: E-Mail: Emergency
Carolina Vein Center Patient Information Name: Date: Address: Home Phone: City: State: Zip: Work Phone: SS#: Marital Status: Occupation: Date of Birth: _ Cell Phone: Emergency Contact: E-Mail: Emergency
MACRI DENTAL LLC 4380 S. Syracuse St. Suite 502 Denver, CO Patient Registration Form
 Personal Information Patient Registration Form Responsible Party First Name Initial Last Name Patient First Name Initial Last Name Address City State Zip Home Phone Work Cell Birthday Social Security Email
Personal Information Patient Registration Form Responsible Party First Name Initial Last Name Patient First Name Initial Last Name Address City State Zip Home Phone Work Cell Birthday Social Security Email
Doc Bresler s Cavity Busters - New Patient History Form
 Doc Bresler s Cavity Busters - New Patient History Form Patient s Name Nickname Date of Birth Age Female Male Address City,State,Zip Code Home Phone Mother s Name Occupation Email Address Cell Phone Father
Doc Bresler s Cavity Busters - New Patient History Form Patient s Name Nickname Date of Birth Age Female Male Address City,State,Zip Code Home Phone Mother s Name Occupation Email Address Cell Phone Father
PATIENT INFORMATION. PARENT OR RESPONSIBLE PARTY (if different from patient)
") PATIENT INFORMATION Last Name DOB Home Address Home Phone Driver s License # Employer Name Work Address First Name Age Sex Marital Status Cell Phone SSN Email Work Phone Person to contact in case of an
PATIENT INFORMATION Last Name DOB Home Address Home Phone Driver s License # Employer Name Work Address First Name Age Sex Marital Status Cell Phone SSN Email Work Phone Person to contact in case of an
Notice of Privacy Practices
 Notice of Privacy Practices (HIPAA Form) Allergy, Asthma, and Immunology of North Texas, PA THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND HOW YOU CAN GET ACCESS
Notice of Privacy Practices (HIPAA Form) Allergy, Asthma, and Immunology of North Texas, PA THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND HOW YOU CAN GET ACCESS
DIABETES & ENDOCRINE CENTER OF ORLANDO, P.A. WELCOME LETTER 3113 LAWTON ROAD, SUITE 100 ORLANDO, FL
 DIABETES & ENDOCRINE CENTER OF ORLANDO, P.A. 3113 LAWTON ROAD, SUITE 100 ORLANDO, FL 32803 407-894-3241 WELCOME LETTER We would like to take this opportunity to welcome you to our practice. Our records
DIABETES & ENDOCRINE CENTER OF ORLANDO, P.A. 3113 LAWTON ROAD, SUITE 100 ORLANDO, FL 32803 407-894-3241 WELCOME LETTER We would like to take this opportunity to welcome you to our practice. Our records
Quick Patient Registration Form Patient Information:
 Quick Patient Registration Form Patient Information: Legal First Name: MI: Legal Last Name: Sex: M F Date of Birth: Primary Language: Marital Status: Married Single Partner Divorced Widowed Race: Ethnicity:
Quick Patient Registration Form Patient Information: Legal First Name: MI: Legal Last Name: Sex: M F Date of Birth: Primary Language: Marital Status: Married Single Partner Divorced Widowed Race: Ethnicity:
Allergies None Penicillin Sulfa Drugs Codeine Aspirin Tape Latex Iodine-Shellfish. Other allergies: Medications
 Today s Date: Height Weight Shoe size (CIRCLE) Allergies None Penicillin Sulfa Drugs Codeine Aspirin Tape Latex Iodine-Shellfish Other allergies: Medications SOCIAL HISTORY (CIRCLE) Do you smoke? No Yes
Today s Date: Height Weight Shoe size (CIRCLE) Allergies None Penicillin Sulfa Drugs Codeine Aspirin Tape Latex Iodine-Shellfish Other allergies: Medications SOCIAL HISTORY (CIRCLE) Do you smoke? No Yes
Insurance Information My Plan is a: PPO HMO POS (Point of Service) Other. Patient Name Address City State Zip
 Other. Patient Name Address City State Zip") Patient Information Form Patient Name Address City State Zip Phone#: Home Cell Work Ext Date of Birth Gender Employer Primary Care/Referring Physician Physician s Name Phone # How did you hear about our
Patient Information Form Patient Name Address City State Zip Phone#: Home Cell Work Ext Date of Birth Gender Employer Primary Care/Referring Physician Physician s Name Phone # How did you hear about our
6677 W. Thunderbird F N. Hayden Rd. H-100 Glendale, Az Scottsdale, Az
 Eye Physicians & Surgeons of Arizona 6677 W. Thunderbird F-101 10603 N. Hayden Rd. H-100 Glendale, Az. 85306 Scottsdale, Az. 85260 George R. Reiss, MD Shamil S. Patel, MD Vinay M. Dewan, MD Christina M.
Eye Physicians & Surgeons of Arizona 6677 W. Thunderbird F-101 10603 N. Hayden Rd. H-100 Glendale, Az. 85306 Scottsdale, Az. 85260 George R. Reiss, MD Shamil S. Patel, MD Vinay M. Dewan, MD Christina M.
HARBORSIDE COUNSELING SERVICES CLIENT REGISTRATION
 HARBORSIDE COUNSELING SERVICES CLIENT REGISTRATION Thank you for choosing our office. In order to serve you properly, we will need the following information. PLEASE PRINT: Name: Date: (Parents/caregivers):
HARBORSIDE COUNSELING SERVICES CLIENT REGISTRATION Thank you for choosing our office. In order to serve you properly, we will need the following information. PLEASE PRINT: Name: Date: (Parents/caregivers):
Cardiology Consultants of Atlanta, P.C N. Decatur Rd. Suite 395, Decatur GA, (404) phone (678) fax
 phone (678) fax") OFFICE POLICIES AND PROCEDURES Thank you for choosing Cardiology Consultants of Atlanta for your cardiovascular care. We realize that you have a choice in medical providers and are pleased that you have
OFFICE POLICIES AND PROCEDURES Thank you for choosing Cardiology Consultants of Atlanta for your cardiovascular care. We realize that you have a choice in medical providers and are pleased that you have
MacInnis Dermatology New Patient Registration Form
 MacInnis Dermatology New Patient Registration Form Please print and answer all questions in full Date Patient Information (please complete using your name as listed on your insurance card) Patient First
MacInnis Dermatology New Patient Registration Form Please print and answer all questions in full Date Patient Information (please complete using your name as listed on your insurance card) Patient First
Franklin Medical Center 514 route 33 west, suite 6 Millstone, n.j Office: fax:
 Franklin Medical Center 514 route 33 west, suite 6 Millstone, n.j. 08535 Office: 732-851-7007 fax: 732-786-0012 Today s date: Patient name: Last name first name middle initial Date of birth Age Male/Female
Franklin Medical Center 514 route 33 west, suite 6 Millstone, n.j. 08535 Office: 732-851-7007 fax: 732-786-0012 Today s date: Patient name: Last name first name middle initial Date of birth Age Male/Female
PATIENT REGISTRATION FORM
 Today s Date / / PATIENT REGISTRATION FORM PATIENT INFORMATION Patient Name Last First Middle Is this your legal name? If not, what is your legal name? Birthdate Age Sex q YES q NO / / q M q F q T Street
Today s Date / / PATIENT REGISTRATION FORM PATIENT INFORMATION Patient Name Last First Middle Is this your legal name? If not, what is your legal name? Birthdate Age Sex q YES q NO / / q M q F q T Street
Address: City/State: Zip: Billing Address: City/State: Zip: Home Phone: Cell Phone: Appointment reminder: Voice Text - Which #:
 Office Use Only: Date of Intake: Appt date/time: Therapist: Insurance: Full Name: DOB: Sex: M F SSN: Page A-1 of 5 Billing Home Cell Work Email: Appointment reminder: Email Voice Text - Which #: Emergency
Office Use Only: Date of Intake: Appt date/time: Therapist: Insurance: Full Name: DOB: Sex: M F SSN: Page A-1 of 5 Billing Home Cell Work Email: Appointment reminder: Email Voice Text - Which #: Emergency
Employer/Doctor Employer s Name Address: Referring Doctor Phone Number Primary Doctor Phone # Patient Information
 FINANCE INSURANCE ORTHOPEDIC SPINE AND SPORTS MEDICINE CENTER 2 FOREST AVEPARAMUS, NJ 07652 PATIENT QUESTIONAIRE Patient s Name: Last First (legal): Middle Initial: Address: City: State: Zip: Date of Birth:
FINANCE INSURANCE ORTHOPEDIC SPINE AND SPORTS MEDICINE CENTER 2 FOREST AVEPARAMUS, NJ 07652 PATIENT QUESTIONAIRE Patient s Name: Last First (legal): Middle Initial: Address: City: State: Zip: Date of Birth:
Our portals are encrypted and password-protected, too, so health data remains secure.
 Patient Portal Education Sheet We know you re busy. That s why Palmetto Health-USC Medical Group s physician practices are offering a way for you to manage your health care online. We offer convenient
Patient Portal Education Sheet We know you re busy. That s why Palmetto Health-USC Medical Group s physician practices are offering a way for you to manage your health care online. We offer convenient
PEDIATRIC PATIENT REGISTRATION GALEN MEDICAL GROUP, PC
 PEDIATRIC PATIENT REGISTRATION GALEN MEDICAL GROUP, PC Your Child: Name Your Child s Full Name: Child Goes By: Gender: Male Female DOB: Age: SS#: Child s Home Address: City: State: Zip: Phone: Primary
PEDIATRIC PATIENT REGISTRATION GALEN MEDICAL GROUP, PC Your Child: Name Your Child s Full Name: Child Goes By: Gender: Male Female DOB: Age: SS#: Child s Home Address: City: State: Zip: Phone: Primary
CREEKSIDE DENTAL REGISTRATION FORM. Please Print PATIENT INFORMATION. Patient s Last Name: First: Middle:
 Today s date CREEKSIDE DENTAL REGISTRATION FORM Please Print PATIENT INFORMATION Patient s Last Name: First: Middle: Home Phone #: Work #: Cell #: Email Address: Street Address: City: State: Zip Code:
Today s date CREEKSIDE DENTAL REGISTRATION FORM Please Print PATIENT INFORMATION Patient s Last Name: First: Middle: Home Phone #: Work #: Cell #: Email Address: Street Address: City: State: Zip Code:
WOMEN S PREMIER OBGYN REGISTRATION FORM
 WOMEN S PREMIER OBGYN REGISTRATION FORM Today s date: PCP: PATIENT INFORMATION Patient s last name: First: Middle: q Miss q Ms. Marital status (circle one) Single / Married / Divorced / Sep / Widow Is
WOMEN S PREMIER OBGYN REGISTRATION FORM Today s date: PCP: PATIENT INFORMATION Patient s last name: First: Middle: q Miss q Ms. Marital status (circle one) Single / Married / Divorced / Sep / Widow Is
WELCOME TO SPORTS CONDITIONING AND REHABILITATION
 WELCOME TO We are pleased you have chosen, (SCAR) for your physical therapy needs. We know there are many choices and we appreciate your confidence in us. You will find we provide unsurpassed individualized
WELCOME TO We are pleased you have chosen, (SCAR) for your physical therapy needs. We know there are many choices and we appreciate your confidence in us. You will find we provide unsurpassed individualized
PATIENT INFORMATION FORM
 PATIENT INFORMATION FORM NAME: Age: DATE OF BIRTH: SSN: Sex: MARITAL STATUS: PRIMARY CARE PHYS: DRIVER S LICENSE # STATE IF CHILD, GUARDIAN S NAME: ADDRESS: City State Zip Code PHONE: Home Phone Cell Phone
PATIENT INFORMATION FORM NAME: Age: DATE OF BIRTH: SSN: Sex: MARITAL STATUS: PRIMARY CARE PHYS: DRIVER S LICENSE # STATE IF CHILD, GUARDIAN S NAME: ADDRESS: City State Zip Code PHONE: Home Phone Cell Phone
Alaska Center for Dermatology, P. C Piper Street Suite T4-020 Anchorage, AK telephone fax
 3841 Piper Street Suite T4-020 Anchorage, AK 99508 telephone 907.646.8500 fax 907.646.9760 Please print all information clearly. Patient Patient Registration Form Name of Birth / / first middle initial
3841 Piper Street Suite T4-020 Anchorage, AK 99508 telephone 907.646.8500 fax 907.646.9760 Please print all information clearly. Patient Patient Registration Form Name of Birth / / first middle initial
Need help with frequent crisis, housing, transportation?
 Need help with frequent crisis, housing, transportation? Kentucky Counseling Center will provide help FREE of charge to qualifying Medicaid recipients. Our Case Management program may assist in the following
Need help with frequent crisis, housing, transportation? Kentucky Counseling Center will provide help FREE of charge to qualifying Medicaid recipients. Our Case Management program may assist in the following
Employer/Occupation Employer Phone Emergency Contact Relation Phone Referring/Family Physician Phone
 PATIENT DATA Please fill out this form so that we will have enough information to effectively bill your insurance. (Only1 form is needed for each patient) Name Date of Birth Sex: F / M Address Phone #1
PATIENT DATA Please fill out this form so that we will have enough information to effectively bill your insurance. (Only1 form is needed for each patient) Name Date of Birth Sex: F / M Address Phone #1
COASTAL SKIN SURGERY & DERMATOLOGY
 DEMOGRAPHIC INFORMATION Last Name: First: Middle: Date of Birth: Age: Sex: M F Marital Status: SSN: Race: Ethnicity: Hispanic or Latino Not Hispanic or Latino Language: Mailing Address: Street apt/unit#
DEMOGRAPHIC INFORMATION Last Name: First: Middle: Date of Birth: Age: Sex: M F Marital Status: SSN: Race: Ethnicity: Hispanic or Latino Not Hispanic or Latino Language: Mailing Address: Street apt/unit#
M F Last Name First Name Middle Initial Gender. Home Phone: Work Phone: Cell Phone: Physical Address: Mailing Address (if different):
:") Welcome to Patient Information: Date of Birth: M F Last Name First Name Middle Initial Gender Home Phone: Work Phone: Cell Phone: Physical Address: Mailing Address (if different): Employer: Occupation:
Welcome to Patient Information: Date of Birth: M F Last Name First Name Middle Initial Gender Home Phone: Work Phone: Cell Phone: Physical Address: Mailing Address (if different): Employer: Occupation:
HIPAA Notice of Privacy Practices
 HIPAA Notice of Privacy Practices THIS NOTICE DESCRIBES HOW YOUR MEDICAL INFORMATION MAY BE USED AND DISCLOSED AND HOW YOU CAN GET ACCESS TO THIS INFORMATION. PLEASE REVIEW IT CAREFULLY. This HIPAA Notice
HIPAA Notice of Privacy Practices THIS NOTICE DESCRIBES HOW YOUR MEDICAL INFORMATION MAY BE USED AND DISCLOSED AND HOW YOU CAN GET ACCESS TO THIS INFORMATION. PLEASE REVIEW IT CAREFULLY. This HIPAA Notice
1641 Tamiami Trail Port Charlotte, Fl Phone: Fax: Health Insurance Portability and Accountability Act of 1996
 1641 Tamiami Trail Port Charlotte, Fl. 33948 Phone: 941-629-6262 Fax: 941-629-1782 Health Insurance Portability and Accountability Act of 1996 HIPAA OMNIBUS NOTICE OF PRIVACY PRACTICES Effective April
1641 Tamiami Trail Port Charlotte, Fl. 33948 Phone: 941-629-6262 Fax: 941-629-1782 Health Insurance Portability and Accountability Act of 1996 HIPAA OMNIBUS NOTICE OF PRIVACY PRACTICES Effective April
Advanced Hearing & Balance Center 3025 Shrine Road, Suite 490 Brunswick, GA PATIENT INFORMATION
 Advanced Hearing & Balance Center 3025 Shrine Road, Suite 490 Brunswick, GA 31520 912-267-1569 PATIENT INFORMATION NAME DATE OF BIRTH FIRST MIDDLE LAST GOES BY SS# EMAIL MARITAL STATUS HOME PHONE# CELL
Advanced Hearing & Balance Center 3025 Shrine Road, Suite 490 Brunswick, GA 31520 912-267-1569 PATIENT INFORMATION NAME DATE OF BIRTH FIRST MIDDLE LAST GOES BY SS# EMAIL MARITAL STATUS HOME PHONE# CELL
Clinic Hours Monday Friday 7:00 AM 4:00 PM (end times may vary); Select Saturdays (by appointment)
; Select Saturdays (by appointment)") Thank you for scheduling an appointment with Clinical Neurology Specialists West. Following is some information that will help familiarize you with our practice. Patient Education / Physician and Provider
Thank you for scheduling an appointment with Clinical Neurology Specialists West. Following is some information that will help familiarize you with our practice. Patient Education / Physician and Provider
North Atlanta Urology Associates
 Patient Information Sheet Account No. Co-Pay $ Referral: Yes No Verbal Patient Name: Date: Mailing Address: Home Phone: Cell Phone/Work: Sex: Male Female Age: Birth Date: Marital Status: Social Security#
Patient Information Sheet Account No. Co-Pay $ Referral: Yes No Verbal Patient Name: Date: Mailing Address: Home Phone: Cell Phone/Work: Sex: Male Female Age: Birth Date: Marital Status: Social Security#
ADVANCED DERMATOLOGY & SKIN SURGERY, P.A.
 ADVANCED DERMATOLOGY & SKIN SURGERY, P.A. Thank you for scheduling an appointment with Advanced Dermatology. We are committed to your treatment and well being and will work hard to serve your needs. In
ADVANCED DERMATOLOGY & SKIN SURGERY, P.A. Thank you for scheduling an appointment with Advanced Dermatology. We are committed to your treatment and well being and will work hard to serve your needs. In
Joseph A. Khawly, MD FACS Eric R. Holz, MD FACS Arthur W. Willis, MD FACS Hassan T. Rahman, MD FACS Emmanuel Y. Chang, MD PhD FACS Jonathan H.
 Joseph A. Khawly, MD FACS PATIENT INFORMATION Patient s name (first and last): Marital Status: Is this your legal name? If not, what is your legal name? Former name: Birth Date: Age: Gender: YES NO M F
Joseph A. Khawly, MD FACS PATIENT INFORMATION Patient s name (first and last): Marital Status: Is this your legal name? If not, what is your legal name? Former name: Birth Date: Age: Gender: YES NO M F
KILGORE EYE CARE CENTER
 KILGORE EYE CARE CENTER Dr. J.T. Roberts O.D. Dr. Jadie Roberts O.D. Dr. Shiloh Roberts O.D. 1100 Stone Rd Suite 2020 Kilgore, Texas 75662 (903) 983-2020 work (903) 983-4000 fax Dear Patient: Welcome to
KILGORE EYE CARE CENTER Dr. J.T. Roberts O.D. Dr. Jadie Roberts O.D. Dr. Shiloh Roberts O.D. 1100 Stone Rd Suite 2020 Kilgore, Texas 75662 (903) 983-2020 work (903) 983-4000 fax Dear Patient: Welcome to
PEDRO J. MORALES, M.D. & TIM P. CARLSON, M.D., P.A. NOTICE OF PRIVACY PRACTICES UPDATED 01/01/2014
 PEDRO J. MORALES, M.D. & TIM P. CARLSON, M.D., P.A. NOTICE OF PRIVACY PRACTICES UPDATED 01/01/2014 PLEASE REVIEW, SIGN AND RETURN TO THE FRONT DESK OR MAIL TO: 2191 9 TH Avenue North, Suite 220 St. Petersburg,
PEDRO J. MORALES, M.D. & TIM P. CARLSON, M.D., P.A. NOTICE OF PRIVACY PRACTICES UPDATED 01/01/2014 PLEASE REVIEW, SIGN AND RETURN TO THE FRONT DESK OR MAIL TO: 2191 9 TH Avenue North, Suite 220 St. Petersburg,
Phoenix Orthopaedic Surgeons Joseph S. Gimbel, M. D. PATIENT REGISTRATION
 Phoenix Orthopaedic Surgeons Joseph S. Gimbel, M. D. PATIENT REGISTRATION DATE Chart # PATIENT NAME AGE DATE OF BIRTH MALE FEMALE PREFFERED LANGUAGE RACE/ETHNICITY SINGLE, MARRIED, DIVORCED, SEPARATED,WIDOWED
Phoenix Orthopaedic Surgeons Joseph S. Gimbel, M. D. PATIENT REGISTRATION DATE Chart # PATIENT NAME AGE DATE OF BIRTH MALE FEMALE PREFFERED LANGUAGE RACE/ETHNICITY SINGLE, MARRIED, DIVORCED, SEPARATED,WIDOWED
Patient Information Form
 Patient Information Form Patient Name: Today s : Address: City: State: Zip: Home Phone: Cell Phone: Carrier: DOB: Age: Gender: Social Security Number: Employer Name: Occupation : Address: Email Address:
Patient Information Form Patient Name: Today s : Address: City: State: Zip: Home Phone: Cell Phone: Carrier: DOB: Age: Gender: Social Security Number: Employer Name: Occupation : Address: Email Address:
Please bring your insurance card, photo identification, and corresponding copayment with you when you check in for your appointment for all visits.
 DIVISION 22 Silver Spring Office 10313 Georgia Avenue, Suite 202 Silver Spring, MD 20902 Rockville Office 15225 Shady Grove Road, Suite 306 Rockville, MD 20850 Phone:301-681-9101 Fax: 301-681-3525 Dear
DIVISION 22 Silver Spring Office 10313 Georgia Avenue, Suite 202 Silver Spring, MD 20902 Rockville Office 15225 Shady Grove Road, Suite 306 Rockville, MD 20850 Phone:301-681-9101 Fax: 301-681-3525 Dear
Pediatric & Adolescent Center of NW Houston, PA & Northwest Houston Neurology, PA
 Pediatric & Adolescent Center of NW Houston, PA & Northwest Houston Neurology, PA Poonam Singh, M.D. * Elizabeth Sanchez Fowler, M.D. * Tonya Suffridge, M.D. * Anuradha Venkatachalam, M.D. Balbir Singh,
Pediatric & Adolescent Center of NW Houston, PA & Northwest Houston Neurology, PA Poonam Singh, M.D. * Elizabeth Sanchez Fowler, M.D. * Tonya Suffridge, M.D. * Anuradha Venkatachalam, M.D. Balbir Singh,
Connecticut Asthma & Allergy Center LLC Registration Form
 Name: Connecticut Asthma & Allergy Center LLC Registration Form Last First Middle Initial Date of Birth: / / Sex: Race: Ethnicity: Language: SS#: xxx-xx- Address: # Street Apt/PO Box Email: Town State
Name: Connecticut Asthma & Allergy Center LLC Registration Form Last First Middle Initial Date of Birth: / / Sex: Race: Ethnicity: Language: SS#: xxx-xx- Address: # Street Apt/PO Box Email: Town State
NORTH ATLANTA UROLOGY ASSOCIATES PC Howard C. Goldberg; M.D. Douglas A. Nyhoff; M.D. Paul L. Rubin; M.D. Jin S. Yeoh M.D.
 PATIENT INFORMATION SHEET First Name: Last Name: Date: Mailing Address: City: State: Zip: Home Number: Cell Number: Work Number: Fax Number: Sex: Male / Female (circle one) Age: Date of Birth: Marital
PATIENT INFORMATION SHEET First Name: Last Name: Date: Mailing Address: City: State: Zip: Home Number: Cell Number: Work Number: Fax Number: Sex: Male / Female (circle one) Age: Date of Birth: Marital
Center for Emotional Wellness & Healing, LLC 100 Heritage Valley Rd, Ste. 1, Sewell, NJ 08080
 100 Heritage Valley Rd, Ste. 1, Sewell, NJ 08080 INTAKE FORM Name: DOB: Age: Street: City/Town: Zip Code: Home Phone: May We Leave a Message? Yes No Cell Phone: May We Leave a Voice Message? Yes No May
100 Heritage Valley Rd, Ste. 1, Sewell, NJ 08080 INTAKE FORM Name: DOB: Age: Street: City/Town: Zip Code: Home Phone: May We Leave a Message? Yes No Cell Phone: May We Leave a Voice Message? Yes No May
Welcome to Our Practice
 Welcome to Our Practice Greater Baltimore Medical Center (GBMC) welcomes you to our practice. We are dedicated to providing you with the kind of care that we would want for our own loved ones. This Information
Welcome to Our Practice Greater Baltimore Medical Center (GBMC) welcomes you to our practice. We are dedicated to providing you with the kind of care that we would want for our own loved ones. This Information
I do / do not (circle one) authorize Vitalogy Skincare and its designated representatives to release medical information to (print name) Relationship
 authorize Vitalogy Skincare and its designated representatives to release medical information to (print name) Relationship") RECEIPT OF NOTICE OF PRIVACY PRACTICES I, (print patient name), have read a copy of Vitalogy Skincare s Notice of Privacy Practices. (This document is available at the front desk or at Vitalogyskincare.com.)
RECEIPT OF NOTICE OF PRIVACY PRACTICES I, (print patient name), have read a copy of Vitalogy Skincare s Notice of Privacy Practices. (This document is available at the front desk or at Vitalogyskincare.com.)
Patient Registration Form Please complete all the information below in print, please do not leave any questions blank. Thank You!
 Patient Registration Form Please complete all the information below in print, please do not leave any questions blank. Thank You! PATIENT INFORMATION: Last Name: First Name: Middle: Date of Birth: Home
Patient Registration Form Please complete all the information below in print, please do not leave any questions blank. Thank You! PATIENT INFORMATION: Last Name: First Name: Middle: Date of Birth: Home
PATIENT INFORMATION. Child s Name: DOB: Address: Phone: Zip: School: Emergency Contact: Phone: Relationship to Patient:
 PATIENT INFORMATION Child s Name: DOB: Address: Phone: Zip: School: Father s Name: Occupation: Phone: (work) Email Address: Mother s Name: Occupation: Phone: (work) Email Address: DOB: Social Security
PATIENT INFORMATION Child s Name: DOB: Address: Phone: Zip: School: Father s Name: Occupation: Phone: (work) Email Address: Mother s Name: Occupation: Phone: (work) Email Address: DOB: Social Security
Financial Responsibility and Communication Authorization Form
 Financial Responsibility and Communication Authorization Form Patient Name: Patient DOB: Impact Concussion Testing and Biosway Concussion Testing ImPACT: We will file the charges for ImPACT testing to
Financial Responsibility and Communication Authorization Form Patient Name: Patient DOB: Impact Concussion Testing and Biosway Concussion Testing ImPACT: We will file the charges for ImPACT testing to
Patient Information Form ~.
 4201 S. Minnesota Ave, Suite 112 Sioux Falls, SD 57105 612 Sioux Point Road, Suite 600 Dakota Dunes, SD 57049 Patient Information Form ~. Patient Name: First MI Last Address: City: State: Zip: Home Phone:
4201 S. Minnesota Ave, Suite 112 Sioux Falls, SD 57105 612 Sioux Point Road, Suite 600 Dakota Dunes, SD 57049 Patient Information Form ~. Patient Name: First MI Last Address: City: State: Zip: Home Phone:
PATIENT DATA SHEET PLEASE COMPLETE IN FULL AND SIGN
 Patient ID Updated: 11/28/2017 PATIENT DATA SHEET PLEASE COMPLETE IN FULL AND SIGN Last Name: First Name: MI: Address: City: State: Zip: Home Phone: Cell Phone: Email: Second Address: From: To: City: State:
Patient ID Updated: 11/28/2017 PATIENT DATA SHEET PLEASE COMPLETE IN FULL AND SIGN Last Name: First Name: MI: Address: City: State: Zip: Home Phone: Cell Phone: Email: Second Address: From: To: City: State:
Barrett Spinal Care, PC 441 S Muskogee Ave. Tahlequah, OK Notice of Patient Privacy Policy
 Barrett Spinal Care, PC 441 S Muskogee Ave. Tahlequah, OK 74464 918-453-0112 Notice of Patient Privacy Policy This notice describes how medical information about you may be used and disclosed, and how
Barrett Spinal Care, PC 441 S Muskogee Ave. Tahlequah, OK 74464 918-453-0112 Notice of Patient Privacy Policy This notice describes how medical information about you may be used and disclosed, and how
Patient or Parent/Guardian Signature:
 Tri State Foot and Ankle Center, LLC Dr. Harold Gruber, DPM Dr. Sandra Hudak, DPM 2018 Naamans Rd. Wilmington, DE 19810 Phone: 302-475-1299 Fax: 302-475-0579 722 Yorklyn Rd. Hockessin, DE 19707 Phone:
Tri State Foot and Ankle Center, LLC Dr. Harold Gruber, DPM Dr. Sandra Hudak, DPM 2018 Naamans Rd. Wilmington, DE 19810 Phone: 302-475-1299 Fax: 302-475-0579 722 Yorklyn Rd. Hockessin, DE 19707 Phone:
NEW PATIENT FORMS OUR LOCATIONS
 NEW PATIENT FORMS Welcome to Evans Dermatology Partners. These New Patient Forms will help us get to know you a bit better. You may complete them by hand, or fill them in electronically, and bring them
NEW PATIENT FORMS Welcome to Evans Dermatology Partners. These New Patient Forms will help us get to know you a bit better. You may complete them by hand, or fill them in electronically, and bring them
Notice of Privacy Practices
 Notice of Privacy Practices THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED, AND HOW YOU CAN GET ACCESS TO THIS INFORMATION. PLEASE REVIEW IT CAREFULLY. PURPOSE STATEMENT
Notice of Privacy Practices THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED, AND HOW YOU CAN GET ACCESS TO THIS INFORMATION. PLEASE REVIEW IT CAREFULLY. PURPOSE STATEMENT
New Patient Name Change Address Change General Update Today s Date / / Name: Date of Birth: / / SS# Gender: Male Female.
 Please fill out with Blue or Black Ink PATIENT INFORMATION: Name: New Patient Name Change Address Change General Update Today s Date / / Last First M.I. Nickname Previous Name Date of Birth: / / SS# Gender:
Please fill out with Blue or Black Ink PATIENT INFORMATION: Name: New Patient Name Change Address Change General Update Today s Date / / Last First M.I. Nickname Previous Name Date of Birth: / / SS# Gender:
WELCOME TO RED BANK SMILES! PLEASE, TAKE A MOMENT TO PROVIDE US WITH THE FOLLOWING INFORMATION
 ! WELCOME TO RED BANK SMILES! PLEASE, TAKE A MOMENT TO PROVIDE US WITH THE FOLLOWING INFORMATION I. PATIENT INFORMATION NAME: Name you prefer to be called by, or pronunciation: BIRTHDATE: / / SEX: M /
! WELCOME TO RED BANK SMILES! PLEASE, TAKE A MOMENT TO PROVIDE US WITH THE FOLLOWING INFORMATION I. PATIENT INFORMATION NAME: Name you prefer to be called by, or pronunciation: BIRTHDATE: / / SEX: M /
PRO SPORTS THERAPY, INC. (P.S.T.)
") PRO SPORTS THERAPY, INC. (P.S.T.) Dear Patient, Thank you for choosing Pro Sports Therapy. Enclosed is the paperwork we need you to complete and bring to your upcoming physical therapy evaluation appointment.
PRO SPORTS THERAPY, INC. (P.S.T.) Dear Patient, Thank you for choosing Pro Sports Therapy. Enclosed is the paperwork we need you to complete and bring to your upcoming physical therapy evaluation appointment.
Family address preferred for patient portal access:
 : Patient Relationship to Guarantor: of Birth: Sex: M F Social Security Number: Home Address: City: State: Zip Code: Pharmacy of Choice: Pharmacy Address: Pharmacy Phone Number: Siblings: Name Sex DOB
: Patient Relationship to Guarantor: of Birth: Sex: M F Social Security Number: Home Address: City: State: Zip Code: Pharmacy of Choice: Pharmacy Address: Pharmacy Phone Number: Siblings: Name Sex DOB
Medical Information Sheet
 Medical Information Sheet Name: Date: Age: Sex: M F Height: Weight: Dominant hand: R L Occupation: Presently working: Y N Reason for being seen today: Date of Onset: Involved side: R L Both Describe any
Medical Information Sheet Name: Date: Age: Sex: M F Height: Weight: Dominant hand: R L Occupation: Presently working: Y N Reason for being seen today: Date of Onset: Involved side: R L Both Describe any
COREY M. NOTIS, M.D., P.A.
 COREY M. NOTIS, M.D., P.A. Registration Form Last Name: First Name Address: City: State: Zip Code: Home Phone: Work Phone Cell Phone: Date of Birth: Social Security # Emergency Contact Name: Phone #: Occupation:
COREY M. NOTIS, M.D., P.A. Registration Form Last Name: First Name Address: City: State: Zip Code: Home Phone: Work Phone Cell Phone: Date of Birth: Social Security # Emergency Contact Name: Phone #: Occupation:
GETTING TO KNOW YOU. 1. How important is it for you to keep your teeth healthy for a lifetime?
 Robert W. Renger, D.D.S., L.L.C. 510 W. 32 nd St. Joplin, MO 64804 417-781-6700 GETTING TO KNOW YOU 1. How important is it for you to keep your teeth healthy for a lifetime? 2. If you could change one
Robert W. Renger, D.D.S., L.L.C. 510 W. 32 nd St. Joplin, MO 64804 417-781-6700 GETTING TO KNOW YOU 1. How important is it for you to keep your teeth healthy for a lifetime? 2. If you could change one
New Patient Referral and Insurance Verification Form
 New Patient Referral and Insurance Verification Form Today s Date: Prior Patient: Y N How did you hear about our practice? Physician: Dr., Internet:, Family/Friend:, Advertising:, Insurance:, Other:. Patient
New Patient Referral and Insurance Verification Form Today s Date: Prior Patient: Y N How did you hear about our practice? Physician: Dr., Internet:, Family/Friend:, Advertising:, Insurance:, Other:. Patient
Patient Health Questionnaire
 Patient Health Questionnaire Patient s Name: Date of Birth: Drug / Food Allergies: Please list any and all allergies you have pertaining to medications and food, along with the reaction. Current Medical
Patient Health Questionnaire Patient s Name: Date of Birth: Drug / Food Allergies: Please list any and all allergies you have pertaining to medications and food, along with the reaction. Current Medical
Is this your child s first visit to the dentist? Yes No If no, date of: last exam dental x-rays fluoride treatment
 PATIENT HEALTH INFORMATION The following information is requested to enable us to give the most consideration to your time and feelings. It is our sincere desire to give personal attention to each of our
PATIENT HEALTH INFORMATION The following information is requested to enable us to give the most consideration to your time and feelings. It is our sincere desire to give personal attention to each of our
ADKINS CHIROPRACTIC LIFE CENTER 157 KEVELING DRIVE SALINE, MICHIGAN Notice of Patient Privacy Policy
 ADKINS CHIROPRACTIC LIFE CENTER 157 KEVELING DRIVE SALINE, MICHIGAN 48176 734 429 2410 Notice of Patient Privacy Policy This notice describes how medical information about you may be used and disclosed,
ADKINS CHIROPRACTIC LIFE CENTER 157 KEVELING DRIVE SALINE, MICHIGAN 48176 734 429 2410 Notice of Patient Privacy Policy This notice describes how medical information about you may be used and disclosed,
TEXAS EAR, NOSE AND THROAT SPECIALISTS, L.L.P. NOTICE OF PRIVACY PRACTICES
 TEXAS EAR, NOSE AND THROAT SPECIALISTS, L.L.P. NOTICE OF PRIVACY PRACTICES THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND HOW YOU CAN GET ACCESS TO THIS INFORMATION.
TEXAS EAR, NOSE AND THROAT SPECIALISTS, L.L.P. NOTICE OF PRIVACY PRACTICES THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND HOW YOU CAN GET ACCESS TO THIS INFORMATION.
Saint Louis University Notice of Privacy Practices Effective Date: April 14, 2003 Amended: September 22, 2013
 Saint Louis University Notice of Privacy Practices Effective Date: April 14, 2003 Amended: September 22, 2013 This notice describes how medical information about you may be used and disclosed and how you
Saint Louis University Notice of Privacy Practices Effective Date: April 14, 2003 Amended: September 22, 2013 This notice describes how medical information about you may be used and disclosed and how you
New Beginning Pediatric Rehab ~ Maryland s Trusted Rehabilitation Practice ~ (410) Office (877) Fax
 Office (877) Fax") PATIENT/PARENT INFORMATION Patient Full Name: Patient s Date of Birth: Parent(s) Name: Cell Number: Address: Home Number: Email: How did you hear of us? (Physician,Google,Friend,Yellow Pages,Other) Authorized
PATIENT/PARENT INFORMATION Patient Full Name: Patient s Date of Birth: Parent(s) Name: Cell Number: Address: Home Number: Email: How did you hear of us? (Physician,Google,Friend,Yellow Pages,Other) Authorized
PHYSICAL THERAPY & CHIROPRACTIC CARE
 PHYSICAL THERAPY & CHIROPRACTIC CARE Patient Information Name: Social Security #: Date of Birth: Telephone: Home: _ Cell: Email: (Communications are for appointments, office information & newsletters)
PHYSICAL THERAPY & CHIROPRACTIC CARE Patient Information Name: Social Security #: Date of Birth: Telephone: Home: _ Cell: Email: (Communications are for appointments, office information & newsletters)
Sammy Lerma III, M.D. P.A. History and Physical Name: DOB: Age:
 History and Physical Name: DOB: Age: Reason for Visit : Current Medications: Previous Hospitalizations: Last Physician's Name: Previous Surgeries: Reason for Changing Physicians: Current Specialists: Medication
History and Physical Name: DOB: Age: Reason for Visit : Current Medications: Previous Hospitalizations: Last Physician's Name: Previous Surgeries: Reason for Changing Physicians: Current Specialists: Medication
New Client Information Sheet
 New Client Information Sheet PSY Family Services Please complete ALL questions 301 W. Rosedale, Fort Worth, TX 76104 1. Client Demographics Patient Name: Last: First: Middle: Sex: ( )M ( )F DOB: Age: School
New Client Information Sheet PSY Family Services Please complete ALL questions 301 W. Rosedale, Fort Worth, TX 76104 1. Client Demographics Patient Name: Last: First: Middle: Sex: ( )M ( )F DOB: Age: School
Patient Information DOB. Female Male Single Married Divorced Widowed. Address City State Zip Code. SSN Home Phone Cell Address
 Patient Information Patient Name Date First Middle Last DOB Nick Name Female Male Single Married Divorced Widowed SSN Home Phone Cell Email Primary Insurance Carrier Policy Holder Name Relationship to
Patient Information Patient Name Date First Middle Last DOB Nick Name Female Male Single Married Divorced Widowed SSN Home Phone Cell Email Primary Insurance Carrier Policy Holder Name Relationship to
Welcome to Rosenman & Leventhal, P.C.
 Welcome to Rosenman & Leventhal, P.C. Thank you for choosing our practice for all of your dermatological needs. Please have ALL of the attached paperwork filled out completely before arriving to our office.
Welcome to Rosenman & Leventhal, P.C. Thank you for choosing our practice for all of your dermatological needs. Please have ALL of the attached paperwork filled out completely before arriving to our office.
Child s Name: Gender: M or F Last First MI. Date Of Birth: - - ADDRESS: CITY: STATE ZIP: REFERRING SOURCE. Physician Name Last First MI
 PATIENT INFORMATION PATIENT INTAKE FORM DATE: PT/OT/ST Child s Name: Gender: M or F Last First MI Date Of Birth: - - SS# - - ADDRESS: CITY: STATE ZIP: REFERRING SOURCE Physician Name Last First MI Phone:
PATIENT INFORMATION PATIENT INTAKE FORM DATE: PT/OT/ST Child s Name: Gender: M or F Last First MI Date Of Birth: - - SS# - - ADDRESS: CITY: STATE ZIP: REFERRING SOURCE Physician Name Last First MI Phone:
Christina Agustin, MD Board Certified in Adult Psychiatry 1 Lake Bellevue Drive, Suite 101 Bellevue, WA Phone Fax:
 Christina Agustin, MD Board Certified in Adult Psychiatry 1 Lake Bellevue Drive, Suite 101 Bellevue, WA 98005 Phone 425-301-9869 Fax: 866-546-1618 Welcome to my practice. I look forward to meeting with
Christina Agustin, MD Board Certified in Adult Psychiatry 1 Lake Bellevue Drive, Suite 101 Bellevue, WA 98005 Phone 425-301-9869 Fax: 866-546-1618 Welcome to my practice. I look forward to meeting with
Patient Registration
 Patient Registration Date: / / Patient s First Name: Last Name: MI: Street Address: City,State,Zip: Primary Phone #: Home / Work / Mobile (circle one) Secondary Phone #: Home / Work / Mobile (circle one)
Patient Registration Date: / / Patient s First Name: Last Name: MI: Street Address: City,State,Zip: Primary Phone #: Home / Work / Mobile (circle one) Secondary Phone #: Home / Work / Mobile (circle one)
Patient Registration. All Inclusive Primary Care. PATIENT INFORMATION Name: (Last, First, MI) Address: City: State/Province: Zip: Country:
 Address: City: State/Province: Zip: Country:") Patient Registration PATIENT INFORMATION Name: (Last, First, MI) Address: City: State/Province: Zip: Country: Mailing Address (if different from above): Home Phone: Work: Mobile: Email: SSN: Birth Date:
Patient Registration PATIENT INFORMATION Name: (Last, First, MI) Address: City: State/Province: Zip: Country: Mailing Address (if different from above): Home Phone: Work: Mobile: Email: SSN: Birth Date:
Client Information Juneau Physical Therapy
 Client Information Patient Name Date of Birth Social Security # Sex F M Mailing Address City State Zip Home Phone Cell Phone Work Phone Email Address (optional) Patient Employed by Emergency Contact Relationship
Client Information Patient Name Date of Birth Social Security # Sex F M Mailing Address City State Zip Home Phone Cell Phone Work Phone Email Address (optional) Patient Employed by Emergency Contact Relationship
MICHIGAN HEALTHCARE PROFESSIONALS, P.C.
 MICHIGAN HEALTHCARE PROFESSIONALS, P.C. PATIENT NOTICE OF PRIVACY PRACTICES As Required by the Privacy Regulations Created as a Result of the Health Insurance Portability and Accountability Act of 1996-(HIPAA),
MICHIGAN HEALTHCARE PROFESSIONALS, P.C. PATIENT NOTICE OF PRIVACY PRACTICES As Required by the Privacy Regulations Created as a Result of the Health Insurance Portability and Accountability Act of 1996-(HIPAA),
GENTLE DENTAL CARE OF ROCHESTER PC
 Patient Rules GENTLE DENTAL CARE OF ROCHESTER PC 1. All Forms and letters require 1 week to complete. This includes school forms, dental records, copy of x-rays, prior authorization request, referrals,
Patient Rules GENTLE DENTAL CARE OF ROCHESTER PC 1. All Forms and letters require 1 week to complete. This includes school forms, dental records, copy of x-rays, prior authorization request, referrals,
WELCOME TO OUR OFFICE. Patient s Name: Today s Date: First Middle Last. Home Address: City: State: Zip: Telephone: Home ( ) Cellular: ( ) Work: ( )
 Cellular: ( ) Work: ( )") WELCOME TO OUR OFFICE Patient s Name: Today s Date: First Middle Last Home Address: City: State: Zip: Telephone: Home ( ) Cellular: ( ) Work: ( ) Email: Personal Work DOB: Age: SSN#: Ethnic Background:
WELCOME TO OUR OFFICE Patient s Name: Today s Date: First Middle Last Home Address: City: State: Zip: Telephone: Home ( ) Cellular: ( ) Work: ( ) Email: Personal Work DOB: Age: SSN#: Ethnic Background:
Welcome! Warren Parkway Suite 306 Frisco, TX PlastiksForKids.com. Please remember to bring: New Patient Paperwork
 Welcome! Thank you for choosing Dr. Christine Stiles to care for your child s plastic surgery needs. All appointments are on Monday afternoons. Dr. Stiles operates at the Pediatric Surgery Center. Plastiks
Welcome! Thank you for choosing Dr. Christine Stiles to care for your child s plastic surgery needs. All appointments are on Monday afternoons. Dr. Stiles operates at the Pediatric Surgery Center. Plastiks
Acknowledgement That You Have Received Our HIPAA Privacy Notice
 Acknowledgement That You Have Received Our HIPAA Privacy Notice Simply Spoken Therapy is required by law to keep your health information and records safe. This information may include: Notes from your
Acknowledgement That You Have Received Our HIPAA Privacy Notice Simply Spoken Therapy is required by law to keep your health information and records safe. This information may include: Notes from your
BILL L. JOU, M.D., INC.
 BILL L. JOU, M.D., INC. AUTHORIZATION TO TREAT I (and/or the undersigned on behalf of the patient) voluntarily consent to allow Dr. Bill L. Jou and staff to provide such evaluation and/or care and treatments
BILL L. JOU, M.D., INC. AUTHORIZATION TO TREAT I (and/or the undersigned on behalf of the patient) voluntarily consent to allow Dr. Bill L. Jou and staff to provide such evaluation and/or care and treatments