Today s date: PATIENT INFORMATION. Address:
|
|
|
- Alberta Shields
- 6 years ago
- Views:
Transcription
1 Today s date: PATIENT INFORMATION Patient s last name: First: Middle: Please send appointment reminders to: Mobile phone #: Address: Mr. Mrs. Registration and Medical History Marital status Single / Married / Divorced / Separated / Widowed Birth date: M Yes No Yes No / / F Street address: Social Security no.: Home phone no.: P.O. box: City: State: ZIP Code: Sex: Occupation: Employer: Employer phone no.: I chose this office because (please check all Insurance that apply): Plan Radio Close to Friend Family home/work Billboard TV Other family members seen here: Subscriber s name: Patient s relationship to subscriber: INSURANCE INFORMATION Subscriber s S.S. Birth date: Group no.: Policy no.: no.: / / Self Other Spouse Child IN CASE OF EMERGENCY Name of local friend or relative (not living at Relationship to patient: same address): Home phone no.: The above information is true to the best of my knowledge. I authorize my insurance benefits be paid directly to the practice. I understand that I am financially responsible for any balance. I also authorize Smile Design Centre or insurance company to release any information required to process my claims. Patient/Guardian signature
2
3

4 Welcome to the Smile Design Centre! Thank you for choosing our practice for all of your dental needs and wants. Dental treatment is very important to your health and should not be postponed by financial concerns, so our collection policy is based on an open and honest discussion of our pricing and financial arrangements made in advance. Our philosophy is to make dentistry affordable to everyone, and we hope this helps you make us your dental home. For your convenience, we offer the following financial arrangements: 1. We accept Visa, MasterCard, Discover, American Express, and Care Credit. 2. An 8% discount will be given for check or cash payment 3 days prior to beginning any treatment that is over $ A 5% immediate payment courtesy will be given for treatment over $250 when paid in full by cash or check on the day of treatment. DENTAL INSURANCE: We are considered an in-network provider for most PPO networks. Please ask a business team member to confirm participation with your individual policy. FINANCIAL RESPONSIBILITY: I/We agree and personally guarantee, in consideration of services and materials provided by Smile Design Centre to be responsible for payment in full of the dental bill. Collection procedures began by statement sent in 20 day cycle, followed by telephone activity at 60 days delinquent, and if the account reaches 90 days past due Transworld Systems (third party collection agency) promptly seizes the account. In the event that this matter is turned over to Transworld Systems, I expect to pay a flat rate of $50 in addition to the original amount. ACKNOWLEDGEMENT SIGNATURE A PATIENT S APPOINTMENT RESPONSIBILITY: We make every effort to schedule your treatment at a convenient time. When your dental needs are diagnosed, if left alone over time, they only get worse. Therefore, it is very important that you keep your appointment as scheduled. Most of our patients are very understanding of how short notice appointment changes affect other patients of our practice, therefor we do request a 48-hour notice if you need to make appointment changes. Our policy concerning canceled or failed appointments is as follows: A patient with an appointment must call at least 48 BUSINESS hours in advance prior to canceling or rescheduling their appointment time. Short notice(less than 48 hours) cancellations and/or rescheduling can result in a charge of $50, which will be billed directly to you. With two short notice appointment changes within a 12-month period of time, we will require you to hold your next appointment on a credit card. After the THIRD cancellation or failed appointment within a 12-month period of time, we will provide treatment 30 days on an emergency basis only. At that time, we will give you the opportunity to find another dental office. Responsible Party s Signature Authorized Signature
5 AUTHORIZATION FOR INSURANCE SUBMISSION, HIPPA POLICY RECIEPT I hereby authorize the Smile Design Centre to affix my name to any and all claims or documents as related to any and all health benefits due me and my dependents. I hereby authorize payment of medical or dental benefits otherwise payable to me, directly to the Smile Design Centre.This Signature On File will be valid from this date. A photocopy of this document may act as an original. I understand by signing this form, I will consent to your use and disclosure of my protected health information to carry out treatment, payment activities, and healthcare operations. Your office will continue to use my health information in some of these ways: by calling me by my first and last name from your waiting room, by mailing me reminder appointment cards with reason for visit, and by calling to confirm appointments, as described in our Notice of Privacy Practices. OTHER ADULT(S) WHOM APPOINTMENT AND/OR PROTECTED HEALTH INFORMATION MAY BE RELEASED Name(s) for information to be released (if none, please specify) I have received a copy of this office s Notice of Privacy Practices on this date. Signature PARENT AND GUARDIANS OF MINOR CHILDREN ONLY I, being the parent or guardian, do hereby request and authorize the dental staff to perform necessary dental services for my child, but not limited to x-rays, and administration of anesthetics which are deemed advisable by the doctor, whether or not I am present at the actual appointment when the treatment is rendered. I also do hereby authorize the following named adults authority to make dental care decisions and receive information for the above-mentioned minor in my absence: Signed
WOMEN S PREMIER OBGYN REGISTRATION FORM
 WOMEN S PREMIER OBGYN REGISTRATION FORM Today s date: PCP: PATIENT INFORMATION Patient s last name: First: Middle: q Miss q Ms. Marital status (circle one) Single / Married / Divorced / Sep / Widow Is
WOMEN S PREMIER OBGYN REGISTRATION FORM Today s date: PCP: PATIENT INFORMATION Patient s last name: First: Middle: q Miss q Ms. Marital status (circle one) Single / Married / Divorced / Sep / Widow Is
Phoenix Orthopaedic Surgeons Joseph S. Gimbel, M. D. PATIENT REGISTRATION
 Phoenix Orthopaedic Surgeons Joseph S. Gimbel, M. D. PATIENT REGISTRATION DATE Chart # PATIENT NAME AGE DATE OF BIRTH MALE FEMALE PREFFERED LANGUAGE RACE/ETHNICITY SINGLE, MARRIED, DIVORCED, SEPARATED,WIDOWED
Phoenix Orthopaedic Surgeons Joseph S. Gimbel, M. D. PATIENT REGISTRATION DATE Chart # PATIENT NAME AGE DATE OF BIRTH MALE FEMALE PREFFERED LANGUAGE RACE/ETHNICITY SINGLE, MARRIED, DIVORCED, SEPARATED,WIDOWED
DeMercy Dental Crabapple Road, Ste. 140 Roswell, GA
 PATIENT REGISTRATION (Please print) Patient s Legal Name: Last First Middle Preferred Name: Street Address: City St Zip Phone Numbers: Home Cell Work Email address: Which method is best to confirm appointments
PATIENT REGISTRATION (Please print) Patient s Legal Name: Last First Middle Preferred Name: Street Address: City St Zip Phone Numbers: Home Cell Work Email address: Which method is best to confirm appointments
Morris Medical Center, P.A.
 Thank you for choosing our practice to assist in your healthcare needs. We appreciate the confidence you and your personal physician have placed in us. Please read the following instructions and information
Thank you for choosing our practice to assist in your healthcare needs. We appreciate the confidence you and your personal physician have placed in us. Please read the following instructions and information
Patient Welcome Form!
 Arthritis and Rheumatology Clinical Center of Northern Virginia, PLLC 8130 Boone Blvd suite 340 Vienna VA 22182 Mahsa Tehrani MD 703-734-2222 Mahnaz Momeni MD Patient Welcome Form Dear new patient, Welcome
Arthritis and Rheumatology Clinical Center of Northern Virginia, PLLC 8130 Boone Blvd suite 340 Vienna VA 22182 Mahsa Tehrani MD 703-734-2222 Mahnaz Momeni MD Patient Welcome Form Dear new patient, Welcome
What to bring to first appointment. You must have with you any related allergy testing, lab results, CT Scan or X-ray results, biopsy
 Jayanti J. Rao, M.D. Shaili N. Shah, M.D. What to bring to first appointment You must have with you any related allergy testing, lab results, CT Scan or X-ray results, biopsy results, list of current medications,
Jayanti J. Rao, M.D. Shaili N. Shah, M.D. What to bring to first appointment You must have with you any related allergy testing, lab results, CT Scan or X-ray results, biopsy results, list of current medications,
Ottesen Family Dentistry * Dr. Pamela Ottesen, DMD * *
 Ottesen Family Dentistry * Dr. Pamela Ottesen, DMD * 850-279-6657 * info@nicevilledental.com PATIENT REGISTRATION INFORMATION Today's Date: Patient Information First Name: Last Name: Middle Initial: Preferred
Ottesen Family Dentistry * Dr. Pamela Ottesen, DMD * 850-279-6657 * info@nicevilledental.com PATIENT REGISTRATION INFORMATION Today's Date: Patient Information First Name: Last Name: Middle Initial: Preferred
Trinity Family Physicians
 Trinity Family Physicians Consent and Authorization for Minors By law, a healthcare provider must attempt to contact a birth / custodial parent or legal guardian prior to rendering treatment to a minor
Trinity Family Physicians Consent and Authorization for Minors By law, a healthcare provider must attempt to contact a birth / custodial parent or legal guardian prior to rendering treatment to a minor
Secondary Insurance Information: Name of Insured: Relationship to Insured: Self Spouse Child Other
 PATIENT REGISTRATION First Name: Last Name: Middle: Preferred Name: Patient is: Responsible Party Policy Holder Responsible Party: ( if someone other than the patient ) First Name: Last Name: Middle Initial:
PATIENT REGISTRATION First Name: Last Name: Middle: Preferred Name: Patient is: Responsible Party Policy Holder Responsible Party: ( if someone other than the patient ) First Name: Last Name: Middle Initial:
PATIENT REGISTRATION
 TIME 10:15 AM PATIENT REGISTRATION DATE 6/15/2016 ID: Chart ID: First Name: Last Name: Middle Initial: Patient Is: Policy Holder Responsible Party Preferred Name: Responsible Party ( if someone other than
TIME 10:15 AM PATIENT REGISTRATION DATE 6/15/2016 ID: Chart ID: First Name: Last Name: Middle Initial: Patient Is: Policy Holder Responsible Party Preferred Name: Responsible Party ( if someone other than
Patient Dental History
 Justin M. Russo, DDS, PLLC What is the main reason for your visit today? Other/Comments: Patient Dental History Cleaning Tooth Pain Sensitivity Whitening Fresher Breath Implants Dentures When was your
Justin M. Russo, DDS, PLLC What is the main reason for your visit today? Other/Comments: Patient Dental History Cleaning Tooth Pain Sensitivity Whitening Fresher Breath Implants Dentures When was your
A SAMPLE FINANCIAL POLICY SHEET
 A SAMPLE FINANCIAL POLICY SHEET Our Practice Financial Policy In order to reduce confusion and misunderstanding between our patients and the practice we have adopted the following financial policy. If
A SAMPLE FINANCIAL POLICY SHEET Our Practice Financial Policy In order to reduce confusion and misunderstanding between our patients and the practice we have adopted the following financial policy. If
California Cardiovascular and Thoracic Surgeons
 California Cardiovascular and Thoracic Surgeons 168 North Brent Street, Suite 508 Ventura, CA 93003 Telephone (805) 643-2375 Fax (805) 643-3511 Your assistance in completing the following information thoroughly
California Cardiovascular and Thoracic Surgeons 168 North Brent Street, Suite 508 Ventura, CA 93003 Telephone (805) 643-2375 Fax (805) 643-3511 Your assistance in completing the following information thoroughly
PATIENT APPLICATION FORM
 PATIENT APPLICATION FORM WELCOME TO OUR CLINIC! We specialize in assisting our patients to achieve their highest level of health through our spinal and postural corrective programs. Our approach is very
PATIENT APPLICATION FORM WELCOME TO OUR CLINIC! We specialize in assisting our patients to achieve their highest level of health through our spinal and postural corrective programs. Our approach is very
STUDENT STATUS: FULL TIME PART TIME NOT A STUDENT RESPONSIBLE PARTY: SELF GUARANTOR RELATIONSHIP
 / / Date Wellspring LAST NAME FIRST NAME MIDDLE INITIAL ADDRESS CITY STATE ZIP HOME PHONE CELL PHONE WORK PHONE (EXT) PRIMARY CARE DOCTOR REFERRING PHYSICIAN / / SEX: F M OF BIRTH SOCIAL SECURITY # MARITAL
/ / Date Wellspring LAST NAME FIRST NAME MIDDLE INITIAL ADDRESS CITY STATE ZIP HOME PHONE CELL PHONE WORK PHONE (EXT) PRIMARY CARE DOCTOR REFERRING PHYSICIAN / / SEX: F M OF BIRTH SOCIAL SECURITY # MARITAL
DATE: PRIMARY LANGUAGE SPOKEN: PATIENT S LOCAL ADDRESS: (Street) (City) (Zip) PERMANENT ADDRESS (IF DIFFERENT):
 (City) (Zip) PERMANENT ADDRESS (IF DIFFERENT):") DATE: PRIMARY LANGUAGE SPOKEN: PATIENT NAME: _ Nick Name: (Last) (First) (Middle) CHECK ONE: SEX: M F CHECK ONE: MARRIED SINGLE WIDOWED DIVORCED RACE: _ DATE OF BIRTH: SOCIAL SECURITY: PATIENT S LOCAL
DATE: PRIMARY LANGUAGE SPOKEN: PATIENT NAME: _ Nick Name: (Last) (First) (Middle) CHECK ONE: SEX: M F CHECK ONE: MARRIED SINGLE WIDOWED DIVORCED RACE: _ DATE OF BIRTH: SOCIAL SECURITY: PATIENT S LOCAL
WELCOME Thank you for selecting our healthcare team! To help us meet your healthcare needs, please fill out this form completely.
 Page 1 of 4 WELCOME Thank you for selecting our healthcare team! To help us meet your healthcare needs, please fill out this form completely. Date: Dr: Chart #: Patient s Name: First MI Last Patient s
Page 1 of 4 WELCOME Thank you for selecting our healthcare team! To help us meet your healthcare needs, please fill out this form completely. Date: Dr: Chart #: Patient s Name: First MI Last Patient s
PATIENT DEMOGRAPHICS. Primary Insurance: Policy #: Group #: Secondary Insurance: Policy #: Group #:
 TEXAS DIABETES & ENDOCRINOLOGY, P.A. 6500 North Mopac*Bldg. 3, Ste. 200*Austin, TX 78731 5000 Davis Ln*Ste 200*Austin, TX 78749 170 Deep Wood Dr*Ste. 104*Round Rock, Tx 78681 Phone: (512) 458 8400*Fax:
TEXAS DIABETES & ENDOCRINOLOGY, P.A. 6500 North Mopac*Bldg. 3, Ste. 200*Austin, TX 78731 5000 Davis Ln*Ste 200*Austin, TX 78749 170 Deep Wood Dr*Ste. 104*Round Rock, Tx 78681 Phone: (512) 458 8400*Fax:
INSURANCE INFORMATION
 PATIENT INFORMATION Last Name First Name M.I. Marital Status: Married Single Divorced Widowed Social Security No.: - - Birth Date: / / Sex: M F Place of Birth: Driver s License Number: Preferred Language:
PATIENT INFORMATION Last Name First Name M.I. Marital Status: Married Single Divorced Widowed Social Security No.: - - Birth Date: / / Sex: M F Place of Birth: Driver s License Number: Preferred Language:
Welcome to a Brighter Morgantown!
 Welcome to a Brighter Morgantown! New Patient Information Payment Options E X C E L L E N C E I N D E N T I S T R Y S I N C E 1 9 2 7 Welcome to a Brighter Morgantown! Morgantown Dental Group would
Welcome to a Brighter Morgantown! New Patient Information Payment Options E X C E L L E N C E I N D E N T I S T R Y S I N C E 1 9 2 7 Welcome to a Brighter Morgantown! Morgantown Dental Group would
K A R A N J O HA R, M.D.
 P: : REGISTRATION FORM - MAJOR MEDICAL Last Name: First and Middle Name: Social Security #: Birthdate: Age: Sex: F M Marital Status: M S D W Home Address: City: State: Zip: *Does the above address, match
P: : REGISTRATION FORM - MAJOR MEDICAL Last Name: First and Middle Name: Social Security #: Birthdate: Age: Sex: F M Marital Status: M S D W Home Address: City: State: Zip: *Does the above address, match
Drs. Birdwell and Guffey. Comprehensive Family Dentistry. Dr. Vicki Davis Guffey, DDS 529 E Gov John Sevier Highway Phone (865)
") Drs. Birdwell and Guffey Comprehensive Family Dentistry Dr. Vicki Davis Guffey, DDS 529 E Gov John Sevier Highway Phone (865) 573-9629 Dr. Chris R. Birdwell, DDS Knoxville, TN 37920 Fax (865) 577-3966
Drs. Birdwell and Guffey Comprehensive Family Dentistry Dr. Vicki Davis Guffey, DDS 529 E Gov John Sevier Highway Phone (865) 573-9629 Dr. Chris R. Birdwell, DDS Knoxville, TN 37920 Fax (865) 577-3966
Permission to Discuss Medical Information HIPPA PATIENT ACKNOWLEDMENT. Patient Name:
 Patient Name: HIPPA PATIENT ACKNOWLEDMENT (Must be filled out by a parent/guardian if the patient is under the age of 18) We are required by law to maintain the privacy of protected health information
Patient Name: HIPPA PATIENT ACKNOWLEDMENT (Must be filled out by a parent/guardian if the patient is under the age of 18) We are required by law to maintain the privacy of protected health information
Is this your child s first visit to the dentist? Yes No If no, date of: last exam dental x-rays fluoride treatment
 PATIENT HEALTH INFORMATION The following information is requested to enable us to give the most consideration to your time and feelings. It is our sincere desire to give personal attention to each of our
PATIENT HEALTH INFORMATION The following information is requested to enable us to give the most consideration to your time and feelings. It is our sincere desire to give personal attention to each of our
PATIENT INFORMATION. Street address: Social Security no.: Home phone no.: ( ) City: State: ZIP Code:
 City: State: ZIP Code:") Today s date: PATIENT INFORMATION Patient s last name: First: Middle: Mr. Mrs. Miss Ms. Marital status (circle one) Single / Married / Divorced / Separated / Widow Is this your legal name? If not, what
Today s date: PATIENT INFORMATION Patient s last name: First: Middle: Mr. Mrs. Miss Ms. Marital status (circle one) Single / Married / Divorced / Separated / Widow Is this your legal name? If not, what
Allergies None Penicillin Sulfa Drugs Codeine Aspirin Tape Latex Iodine-Shellfish. Other allergies: Medications
 Today s Date: Height Weight Shoe size (CIRCLE) Allergies None Penicillin Sulfa Drugs Codeine Aspirin Tape Latex Iodine-Shellfish Other allergies: Medications SOCIAL HISTORY (CIRCLE) Do you smoke? No Yes
Today s Date: Height Weight Shoe size (CIRCLE) Allergies None Penicillin Sulfa Drugs Codeine Aspirin Tape Latex Iodine-Shellfish Other allergies: Medications SOCIAL HISTORY (CIRCLE) Do you smoke? No Yes
Carolina Dental Alliance
 Patient Registration First Name: Last Name: Date of Birth: SSN: Mailing Address: City State Zip Home Phone: Cell Phone: Responsible Party (ONLY COMPLETE IF SOMEONE OTHER THAN PATIENT) First Name: Last
Patient Registration First Name: Last Name: Date of Birth: SSN: Mailing Address: City State Zip Home Phone: Cell Phone: Responsible Party (ONLY COMPLETE IF SOMEONE OTHER THAN PATIENT) First Name: Last
425 North Wendover Road Charlotte, NC Birthdate: Social Security #: Male Female
 425 North Wendover Road Charlotte, NC 28211 PATIENT INFORMATION: Patient s Legal Name: Nickname: Birthdate: Social Security #: Male Female Status: Minor (under 18) Single Married Separated Divorced Widowed
425 North Wendover Road Charlotte, NC 28211 PATIENT INFORMATION: Patient s Legal Name: Nickname: Birthdate: Social Security #: Male Female Status: Minor (under 18) Single Married Separated Divorced Widowed
Lowrance Dental REGISTRATION FORM (Please Print)
") Today s Date: Patient s last name: First: Middle: Lowrance Dental REGISTRATION FORM (Please Print) PCP: PATIENT INFORMATION Mr. Mrs. Miss Ms. Marital status: Single Mar Div Sep Wid Is this your legal name?
Today s Date: Patient s last name: First: Middle: Lowrance Dental REGISTRATION FORM (Please Print) PCP: PATIENT INFORMATION Mr. Mrs. Miss Ms. Marital status: Single Mar Div Sep Wid Is this your legal name?
PATIENT INFORMATION Patient Name: Last First Middle Initial. Address. Street or P.O. Box City, State Zip
 PATIENT INFORMATION - 2018 Patient Name: Last First Middle Initial Address: Street or P.O. Box City, State Zip of Birth: / / Race: Gender: Male Female Social Security #: Marital Status: Single Married
PATIENT INFORMATION - 2018 Patient Name: Last First Middle Initial Address: Street or P.O. Box City, State Zip of Birth: / / Race: Gender: Male Female Social Security #: Marital Status: Single Married
WHITE ROCK DERMATOLOGY Garland Road, Suite 210; Dallas, TX Tel:
 10611 Garland Road, Suite 210; Dallas, TX 75218 Tel: 214-324-2881 Patient s Full Name: Gender: Age: Marital Status: Single Married Widowed Divorced DOB: Social Security Number: Occupation: Address: Apt
10611 Garland Road, Suite 210; Dallas, TX 75218 Tel: 214-324-2881 Patient s Full Name: Gender: Age: Marital Status: Single Married Widowed Divorced DOB: Social Security Number: Occupation: Address: Apt
Candace L. Peterson, DMD
 Candace L. Peterson, DMD PATIENT REGISTRATION Date A. Responsible Party SS # - - Last First Middle Home Address Birthdate E-mail City State Zip Code Home Phone ( ) - Cell Phone ( ) - Work Phone ( ) - Employer
Candace L. Peterson, DMD PATIENT REGISTRATION Date A. Responsible Party SS # - - Last First Middle Home Address Birthdate E-mail City State Zip Code Home Phone ( ) - Cell Phone ( ) - Work Phone ( ) - Employer
WELCOME! On behalf of our staff, we look forward to meeting you. Dr. Karen Anne Lunsford ENCLOSURE : 4 PAGES OF REGISTRATION
 32 Willimansett Street - Rte. 33 - Next to Big Y South Hadley, MA 01075 P 413.540.9500 / F 413.540.9505 www.bigwidesmiles.com WELCOME! Thank you for choosing our office for your dental services. We are
32 Willimansett Street - Rte. 33 - Next to Big Y South Hadley, MA 01075 P 413.540.9500 / F 413.540.9505 www.bigwidesmiles.com WELCOME! Thank you for choosing our office for your dental services. We are
First Middle Initial Last. SSN: Date of Birth . Address: City: State: Zip: Home Phone: Cell Phone: Sex: M F
 Patient Information First Middle Initial Last SSN: Date of Birth Email Address: City: State: Zip: Home Phone: Cell Phone: Sex: M F Do you prefer appointment confirmations via (check one or both): TEXT
Patient Information First Middle Initial Last SSN: Date of Birth Email Address: City: State: Zip: Home Phone: Cell Phone: Sex: M F Do you prefer appointment confirmations via (check one or both): TEXT
2460 India Hook Road, Suite 106 Rock Hill, SC Tel: (803) Fax: (803)
 Fax: (803)") 2460 India Hook Road, Suite 106 Rock Hill, SC 29732 E-mail: drj@rockhillkids.com Tel: (803) 327-3327 Fax: (803) 334-3474 Welcome to our practice! Please carefully complete this form so that we may better
2460 India Hook Road, Suite 106 Rock Hill, SC 29732 E-mail: drj@rockhillkids.com Tel: (803) 327-3327 Fax: (803) 334-3474 Welcome to our practice! Please carefully complete this form so that we may better
York Smile Care. First: Middle: Last: Jr/Sr: Street: City: State Zip: Home Phone: Work Phone: Cell Phone: Patient's Employer:
 Patient Information Circle One: Dr/Mr/Mrs/MS/Miss First: Middle: Last: Jr/Sr: Street: City: State Zip: Home Phone: Work Phone: Cell Phone: Patient's Employer: Email Address: May we contact you by Email(circle)
Patient Information Circle One: Dr/Mr/Mrs/MS/Miss First: Middle: Last: Jr/Sr: Street: City: State Zip: Home Phone: Work Phone: Cell Phone: Patient's Employer: Email Address: May we contact you by Email(circle)
NAME: LAST FIRST MI SEX: M F BIRTH DATE: / / AGE: SS# - - STATE ZIP HOME PHONE CELL. How did you hear about our office? STATE ZIP HOME PHONE WORK
 PATIENT INFORMATION NAME: LAST FIRST MI SEX: M F BIRTH DATE: / / AGE: SS# - - ADDRESS CITY STATE ZIP HOME PHONE CELL OTHER EMAIL How did you hear about our office? HEAD OF HOUSEHOLD NAME: LAST FIRST MI
PATIENT INFORMATION NAME: LAST FIRST MI SEX: M F BIRTH DATE: / / AGE: SS# - - ADDRESS CITY STATE ZIP HOME PHONE CELL OTHER EMAIL How did you hear about our office? HEAD OF HOUSEHOLD NAME: LAST FIRST MI
ADULT SELF ASSESSMENT
 ADULT SELF ASSESSMENT In filling out this form you are welcome to provide as much information as you would like. If you find a question that you desire to leave blank, you are welcome to do so for any
ADULT SELF ASSESSMENT In filling out this form you are welcome to provide as much information as you would like. If you find a question that you desire to leave blank, you are welcome to do so for any
New Patient Registration Form
 New Patient Registration Form Patient Information Name: (First) (Middle) (Last) SSN: of Birth / / Sex: Male Female Street Address (or PO Box): City: State: Zip: Marital Status: Single Married Divorced
New Patient Registration Form Patient Information Name: (First) (Middle) (Last) SSN: of Birth / / Sex: Male Female Street Address (or PO Box): City: State: Zip: Marital Status: Single Married Divorced
PATIENT REGISTRATION (Please Print) Social Security # Address City State Zip. Address
 Social Security # Address City State Zip. Address") PATIENT REGISTRATION (Please Print) Date Name (Last) (First) (MI) Clinician Social Security # Address City State Zip Email Address Home Phone ( ) Mobile/Alt. Phone ( ) Work Phone ( ) PLEASE IDENTIFY WHICH
PATIENT REGISTRATION (Please Print) Date Name (Last) (First) (MI) Clinician Social Security # Address City State Zip Email Address Home Phone ( ) Mobile/Alt. Phone ( ) Work Phone ( ) PLEASE IDENTIFY WHICH
PATIENT INFORMATION INSURANCE INFORMATION
 PATIENT INFORMATION RECORD (Please Print or Write Legibly) DATE ACCT # PATIENT INFORMATION NAME First Middle Init. Last MAILING ADDRESS CITY STATE ZIP SEX RACE Ethnicity: q hispanic/latino q Not Hispanic/Latino
PATIENT INFORMATION RECORD (Please Print or Write Legibly) DATE ACCT # PATIENT INFORMATION NAME First Middle Init. Last MAILING ADDRESS CITY STATE ZIP SEX RACE Ethnicity: q hispanic/latino q Not Hispanic/Latino
PLEASE PRINT CLEARLY
 PATIENT INFORMATION FORM Rev. 02/2018 PLEASE PRINT CLEARLY New Patient Name Change Address Change Insurance Policy/Holder Change PATIENT INFORMATION Last Name: _ First Name: Middle Initial: DOB: Sex: Male
PATIENT INFORMATION FORM Rev. 02/2018 PLEASE PRINT CLEARLY New Patient Name Change Address Change Insurance Policy/Holder Change PATIENT INFORMATION Last Name: _ First Name: Middle Initial: DOB: Sex: Male
Appointment Date: / / Appointment Time: Date: / / Account #:
 Appointment: / / AppointmentTime: : / / Account#: PATIENTINFORMATION Name:(Last) (First) (MI) Suffix/nickname: Birth: Sex: MaritalStatus: Address: City: State: Zip: HomePhone:_MobilePhone: WorkPhone: Employer:
Appointment: / / AppointmentTime: : / / Account#: PATIENTINFORMATION Name:(Last) (First) (MI) Suffix/nickname: Birth: Sex: MaritalStatus: Address: City: State: Zip: HomePhone:_MobilePhone: WorkPhone: Employer:
Connecticut Asthma & Allergy Center LLC Registration Form
 Name: Connecticut Asthma & Allergy Center LLC Registration Form Last First Middle Initial Date of Birth: / / Sex: Race: Ethnicity: Language: SS#: xxx-xx- Address: # Street Apt/PO Box Email: Town State
Name: Connecticut Asthma & Allergy Center LLC Registration Form Last First Middle Initial Date of Birth: / / Sex: Race: Ethnicity: Language: SS#: xxx-xx- Address: # Street Apt/PO Box Email: Town State
Policies and information:
 Policies and information: Basic Policies: Please be on time for your appointments. If you are late for your scheduled appointment, there is a chance that you will be rescheduled. We require at least 24
Policies and information: Basic Policies: Please be on time for your appointments. If you are late for your scheduled appointment, there is a chance that you will be rescheduled. We require at least 24
Dr. Jeff Eidsvig, D.C., TPI-CGFI 3060 Communications Parkway, Suite #104 Plano, Texas Patient Insurance Information
 Improving Lives & Performance Dr. Jeff Eidsvig, D.C., TPI-CGFI 3060 Communications Parkway, Suite #104 Plano, Texas 75093 972-312-9310 New Patient Information / Change of Information : New Patient Change
Improving Lives & Performance Dr. Jeff Eidsvig, D.C., TPI-CGFI 3060 Communications Parkway, Suite #104 Plano, Texas 75093 972-312-9310 New Patient Information / Change of Information : New Patient Change
Policy Change Request
 Individual and Family Plans Policy Change Request Thank you for continuing your individual health plan coverage with Providence Health Plan (PHP). Please visit www.providencehealthplan.com for additional
Individual and Family Plans Policy Change Request Thank you for continuing your individual health plan coverage with Providence Health Plan (PHP). Please visit www.providencehealthplan.com for additional
Welcome to our office!
 2007 Rainbow Drive Gadsden, AL 35901 Ph: 256-543-0009 Fax: 256-549-1221 Patient Information Page 1of 2 Welcome to our office! Dr. Shan Tian, D. C. Patient Information Please complete all questions. Today
2007 Rainbow Drive Gadsden, AL 35901 Ph: 256-543-0009 Fax: 256-549-1221 Patient Information Page 1of 2 Welcome to our office! Dr. Shan Tian, D. C. Patient Information Please complete all questions. Today
PATIENT MEDICAL RECORD # DATE OF BIRTH / / Male: Female: PATIENT NAME LAST FIRST MI FORMER LAST NAME MAILING ADDRESS CITY STATE ZIP
 PATIENT INFORMATION PATIENT MEDICAL RECORD # DATE OF BIRTH / / Male: Female: PATIENT NAME LAST FIRST MI FORMER LAST NAME MAILING ADDRESS CITY STATE ZIP HOME PHONE ( ) WORK PHONE ( ) CELL PHONE ( ) E-MAIL
PATIENT INFORMATION PATIENT MEDICAL RECORD # DATE OF BIRTH / / Male: Female: PATIENT NAME LAST FIRST MI FORMER LAST NAME MAILING ADDRESS CITY STATE ZIP HOME PHONE ( ) WORK PHONE ( ) CELL PHONE ( ) E-MAIL
Financial Policy and Agreement
 Financial Policy and Agreement Thank you for choosing us for your dental needs! We are committed to providing you with excellent care and convenient financial arrangements. Our financial arrangements are
Financial Policy and Agreement Thank you for choosing us for your dental needs! We are committed to providing you with excellent care and convenient financial arrangements. Our financial arrangements are
(Please Print using Black or Blue Ink) SEX: GENDER IDENTITY: MARITAL STATUS: SINGLE MARRIED OTHER
 SEX: GENDER IDENTITY: MARITAL STATUS: SINGLE MARRIED OTHER") PATIENT INFORMATION (Please Print using Black or Blue Ink) LAST NAME: FIRST NAME: MIDDLE INITIAL: ADDRESS: CITY: STATE: ZIP: SEX: GENDER IDENTITY: MARITAL STATUS: SINGLE MARRIED OTHER RACE (OPTIONAL):
PATIENT INFORMATION (Please Print using Black or Blue Ink) LAST NAME: FIRST NAME: MIDDLE INITIAL: ADDRESS: CITY: STATE: ZIP: SEX: GENDER IDENTITY: MARITAL STATUS: SINGLE MARRIED OTHER RACE (OPTIONAL):
Financial and Insurance Agreement
 Financial and Insurance Agreement I understand that payment for my dental treatment is due in full at the time services are rendered. The office accepts cash, check, Visa, Master Card, Discover. A service
Financial and Insurance Agreement I understand that payment for my dental treatment is due in full at the time services are rendered. The office accepts cash, check, Visa, Master Card, Discover. A service
Pediatric & Adolescent Center of NW Houston, PA & Northwest Houston Neurology, PA
 Pediatric & Adolescent Center of NW Houston, PA & Northwest Houston Neurology, PA Poonam Singh, M.D. * Elizabeth Sanchez Fowler, M.D. * Tonya Suffridge, M.D. * Anuradha Venkatachalam, M.D. Balbir Singh,
Pediatric & Adolescent Center of NW Houston, PA & Northwest Houston Neurology, PA Poonam Singh, M.D. * Elizabeth Sanchez Fowler, M.D. * Tonya Suffridge, M.D. * Anuradha Venkatachalam, M.D. Balbir Singh,
Date How did you hear about Shine? P A T I E NT I N F O R M A T I O N
 How did you hear about Shine? P A T I E NT I N F O R M A T I O N 1. Patient's Name of Birth / / Gender: Male Female 2. Patient's Name of Birth / / Gender: Male Female 3. Patient's Name of Birth / / Gender:
How did you hear about Shine? P A T I E NT I N F O R M A T I O N 1. Patient's Name of Birth / / Gender: Male Female 2. Patient's Name of Birth / / Gender: Male Female 3. Patient's Name of Birth / / Gender:
Allcare Rehabilitation
 Allcare Rehabilitation Welcome to Allcare Rehabilitation, Inc. Please complete the following information as accurately as possible as it is necessary we have this information to effectively file your insurance
Allcare Rehabilitation Welcome to Allcare Rehabilitation, Inc. Please complete the following information as accurately as possible as it is necessary we have this information to effectively file your insurance
Prince Family Dentistry
 Prince Family Dentistry 702-240-0202 830 S. Durango Dr., Ste. 104 Las Vegas, NV 89145 PATIENT INFORMATION Last Name First Name MI Preferred Name Birthdate {Male { Female SS# {Minor { Single { Married {
Prince Family Dentistry 702-240-0202 830 S. Durango Dr., Ste. 104 Las Vegas, NV 89145 PATIENT INFORMATION Last Name First Name MI Preferred Name Birthdate {Male { Female SS# {Minor { Single { Married {
CONSENT TO DENTAL TREATMENT
 DENTIST: Matthew Kelley DDS CONSENT TO DENTAL TREATMENT PATIENT: 1. I request and authorize the above listed provider of service, and/or such other persons as he may appoint to perform or assist in the
DENTIST: Matthew Kelley DDS CONSENT TO DENTAL TREATMENT PATIENT: 1. I request and authorize the above listed provider of service, and/or such other persons as he may appoint to perform or assist in the
PATIENT REGISTRATION
 First Name Middle Name Last Name Preferred Name PATIENT REGISTRATION Patient Information Byron C. Cotton, M.D., FAAP Gayla Woodson, MSN, CPNP First choice for infants thru young adult! First Patient Second
First Name Middle Name Last Name Preferred Name PATIENT REGISTRATION Patient Information Byron C. Cotton, M.D., FAAP Gayla Woodson, MSN, CPNP First choice for infants thru young adult! First Patient Second
Sinha Clinic Foxfield Road, Suite 240, St. Charles, IL Office: (630) Fax: (630)
 Fax: (630)") 2560 Foxfield Road, Suite 240, St. Charles, IL 60174 Office: (630) 762-9606 Fax: (630) 762-9605 www.sinhaclinic.com info@sinhaclinic.com Patient Name: Date: Home Phone: ( )- Cell Phone: ( )- Preferred
2560 Foxfield Road, Suite 240, St. Charles, IL 60174 Office: (630) 762-9606 Fax: (630) 762-9605 www.sinhaclinic.com info@sinhaclinic.com Patient Name: Date: Home Phone: ( )- Cell Phone: ( )- Preferred
PATIENT INFORMATION PERSONAL. Patient Name Last First MI (Preferred) Birthdate SS# DL# Gender M F Married Y N Work Phone Cell Phone
 Birthdate SS# DL# Gender M F Married Y N Work Phone Cell Phone") PATIENT INFORMATION We are pleased to welcome you to our office. For your convenience, our forms have ACTIVE FIELDS so you can fill them out on your computer and print them out. If you have any questions,
PATIENT INFORMATION We are pleased to welcome you to our office. For your convenience, our forms have ACTIVE FIELDS so you can fill them out on your computer and print them out. If you have any questions,
HARBORSIDE COUNSELING SERVICES CLIENT REGISTRATION
 HARBORSIDE COUNSELING SERVICES CLIENT REGISTRATION Thank you for choosing our office. In order to serve you properly, we will need the following information. PLEASE PRINT: Name: Date: (Parents/caregivers):
HARBORSIDE COUNSELING SERVICES CLIENT REGISTRATION Thank you for choosing our office. In order to serve you properly, we will need the following information. PLEASE PRINT: Name: Date: (Parents/caregivers):
Welcome to Our Practice
 Welcome to Our Practice Greater Baltimore Medical Center (GBMC) welcomes you to our practice. We are dedicated to providing you with the kind of care that we would want for our own loved ones. This Information
Welcome to Our Practice Greater Baltimore Medical Center (GBMC) welcomes you to our practice. We are dedicated to providing you with the kind of care that we would want for our own loved ones. This Information
PHARMACY INFORMATION
 NAAMAN CLINIC TODAY S DATE: Prefix Mr. Mrs. Miss Ms. Dr. Preferred Name: Patient s Name Address: First Middle Last Street & Apt # City State Zip SS# Birthdate Age: Sex: Female Male Marital Status: Single
NAAMAN CLINIC TODAY S DATE: Prefix Mr. Mrs. Miss Ms. Dr. Preferred Name: Patient s Name Address: First Middle Last Street & Apt # City State Zip SS# Birthdate Age: Sex: Female Male Marital Status: Single
ACKNOWLEDGEMENT OF RECEIPT OF NOTICE OF PRIVACY PRACTICES 2013 Murphy Dental 608 East Harmony Road, Suite 301 Fort Collins, CO 80525
 ACKNOWLEDGEMENT OF RECEIPT OF NOTICE OF PRIVACY PRACTICES 2013 Notice to Patient: We are required to provide you with a copy of our Notice of Privacy Practices, which states how we may use and/or disclose
ACKNOWLEDGEMENT OF RECEIPT OF NOTICE OF PRIVACY PRACTICES 2013 Notice to Patient: We are required to provide you with a copy of our Notice of Privacy Practices, which states how we may use and/or disclose
Fairview Dental. Patient Information: Patient First Name: MI: Last: Preferred Name: Date of birth: SS#: Address: City: Zip: Home Ph: Cell: :
 Patient Information: Fairview Dental Date: Patient First Name: MI: Last: Preferred Name: Date of birth: SS#: Address: City: Zip: Home Ph: Cell: : Email: Check one : Child Single Married Divorced Widowed
Patient Information: Fairview Dental Date: Patient First Name: MI: Last: Preferred Name: Date of birth: SS#: Address: City: Zip: Home Ph: Cell: : Email: Check one : Child Single Married Divorced Widowed
FINANCIAL RESPONSIBILITY Name: Relationship: Home Address: Home Phone #: Cell Phone #: Date of Birth: Social Security Number: Employer: Occupation:
 LITTLETON OB/GYN ASSOCIATES 7750 S Broadway, Suite 200 Littleton, CO 80122 303-730-6000 David J. Watson, MD Bruce R. Dorr, MD Jeannie Key, NP Jessica Anderson, NP WELCOME TO OUR OFFICE! DATE: PATIENT INFORMATION
LITTLETON OB/GYN ASSOCIATES 7750 S Broadway, Suite 200 Littleton, CO 80122 303-730-6000 David J. Watson, MD Bruce R. Dorr, MD Jeannie Key, NP Jessica Anderson, NP WELCOME TO OUR OFFICE! DATE: PATIENT INFORMATION
Name: last First middle Address: street city state zip code Mailing Address: ( if different) street city state zip code
 street city state zip code") 0 Mental Health Resources, PC (540) 899-9826 Fax (540) 373-3913 Date (or effective date of change) Patient Information DO NOT COMPLETE THIS FORM UNTIL YOU HAVE A CONFIRMED APPOINTMENT. Patient Information
0 Mental Health Resources, PC (540) 899-9826 Fax (540) 373-3913 Date (or effective date of change) Patient Information DO NOT COMPLETE THIS FORM UNTIL YOU HAVE A CONFIRMED APPOINTMENT. Patient Information
New Patient Information - Dr. Marc Edelstein
 Marc A. Edelstein M.D., FACP, FACG Internal Medicine and Gastroenterology Gastroenterology, Hepatology, and Nutrition Susan P. Edelstein M.D., FAAP Pediatrics and Pediatric Gastroenterology Pediatric Gastroenterology,
Marc A. Edelstein M.D., FACP, FACG Internal Medicine and Gastroenterology Gastroenterology, Hepatology, and Nutrition Susan P. Edelstein M.D., FAAP Pediatrics and Pediatric Gastroenterology Pediatric Gastroenterology,
IOANA A. BINA, M.D. Gastroenterology Tel: (707) Fax: (707)
 Fax: (707)") IOANA A. BINA, M.D. Gastroenterology Tel: (707) 963-3311 Fax: (707)963-3322 (circle) Today's Date: Best Contact Phone# Cell Home Work PATIENT INFORMATION Name: Soc Sec #: Last Name First Name Initial Address:
IOANA A. BINA, M.D. Gastroenterology Tel: (707) 963-3311 Fax: (707)963-3322 (circle) Today's Date: Best Contact Phone# Cell Home Work PATIENT INFORMATION Name: Soc Sec #: Last Name First Name Initial Address:
70 Hatfield Lane Goshen, New York SSN: First Name: MI: Last Name: Employment: Employed Unemployed Retired Employer: Employer Address:
 70 Hatfield Lane Goshen, New York 10924 SSN: First Name: MI: Last Name: Prefix (Ms., Mr.,) Sex: M F DOB: Marital Status: Single Married Divorced Widowed Spouse Name: Employment: Employed Unemployed Retired
70 Hatfield Lane Goshen, New York 10924 SSN: First Name: MI: Last Name: Prefix (Ms., Mr.,) Sex: M F DOB: Marital Status: Single Married Divorced Widowed Spouse Name: Employment: Employed Unemployed Retired
MasterCare Physical Therapy, Inc.
 Patient Financial Responsibility To all of our Patients: We will, as a courtesy, file your insurance claims for you. Please be advised that it is solely your responsibility to know and to understand your
Patient Financial Responsibility To all of our Patients: We will, as a courtesy, file your insurance claims for you. Please be advised that it is solely your responsibility to know and to understand your
LAS VEGAS ENDOCRINOLOGY
 Today s Date: Primary Care Provider: Patient Information Last Name: First Name: Date of Birth: Sex: M F Social Security #: Street Address: City: State: Zip: Occupation: Employer: Home Phone: Cell Phone:
Today s Date: Primary Care Provider: Patient Information Last Name: First Name: Date of Birth: Sex: M F Social Security #: Street Address: City: State: Zip: Occupation: Employer: Home Phone: Cell Phone:
PEDIATRIC PATIENT REGISTRATION GALEN MEDICAL GROUP, PC
 PEDIATRIC PATIENT REGISTRATION GALEN MEDICAL GROUP, PC Your Child: Name Your Child s Full Name: Child Goes By: Gender: Male Female DOB: Age: SS#: Child s Home Address: City: State: Zip: Phone: Primary
PEDIATRIC PATIENT REGISTRATION GALEN MEDICAL GROUP, PC Your Child: Name Your Child s Full Name: Child Goes By: Gender: Male Female DOB: Age: SS#: Child s Home Address: City: State: Zip: Phone: Primary
C.A.I. A Cardiovascular & Arrhythmia Institute
 Acknowledgement of Receipt of Notice of Privacy Practices By signing below I acknowledge that I have received the Notice of Privacy Practices of Cardiac Arrhythmia Institute, LLC, which explains its legal
Acknowledgement of Receipt of Notice of Privacy Practices By signing below I acknowledge that I have received the Notice of Privacy Practices of Cardiac Arrhythmia Institute, LLC, which explains its legal
Welcome,! Scheduled Appointment: at AM/PM Dr. Jamie C. Bales Dr. Brian H. Moore
 Welcome,! Thank you for choosing to continue your care at Neurology Specialists, PC! Enclosed is a packet of information that is needed for your upcoming appointment. We will need you to return this information
Welcome,! Thank you for choosing to continue your care at Neurology Specialists, PC! Enclosed is a packet of information that is needed for your upcoming appointment. We will need you to return this information
PATIENT INFORMATION. Caucasian or White Male Female. Unknown IN CASE OF EMERGENCY
 Name (Last, First, Middle Initial): PATIENT INFORMATION Salutation: Mr. Social Security # Preferred Language: Race: Ethnicity: American Indian or Alaska Native Hispanic or Latino Asian Not Hispanic or
Name (Last, First, Middle Initial): PATIENT INFORMATION Salutation: Mr. Social Security # Preferred Language: Race: Ethnicity: American Indian or Alaska Native Hispanic or Latino Asian Not Hispanic or
PATIENT INFORMATION PATIENT INFORMATION. Middle Initial: Nickname: Date of Birth: Marital Status: Address: City: State: Zip Code:
 PATIENT INFORMATION PATIENT INFORMATION First Name: Last Name: Middle Initial: Nickname: Date of Birth: Sex: Marital Status: Address: City: State: Zip Code: Home Phone: Cell Phone: Email: How did you hear
PATIENT INFORMATION PATIENT INFORMATION First Name: Last Name: Middle Initial: Nickname: Date of Birth: Sex: Marital Status: Address: City: State: Zip Code: Home Phone: Cell Phone: Email: How did you hear
If you are already an established patient of either Dr. Aroesty or Ms. Corrice, you do not have to reregister or fill out any additional paperwork.
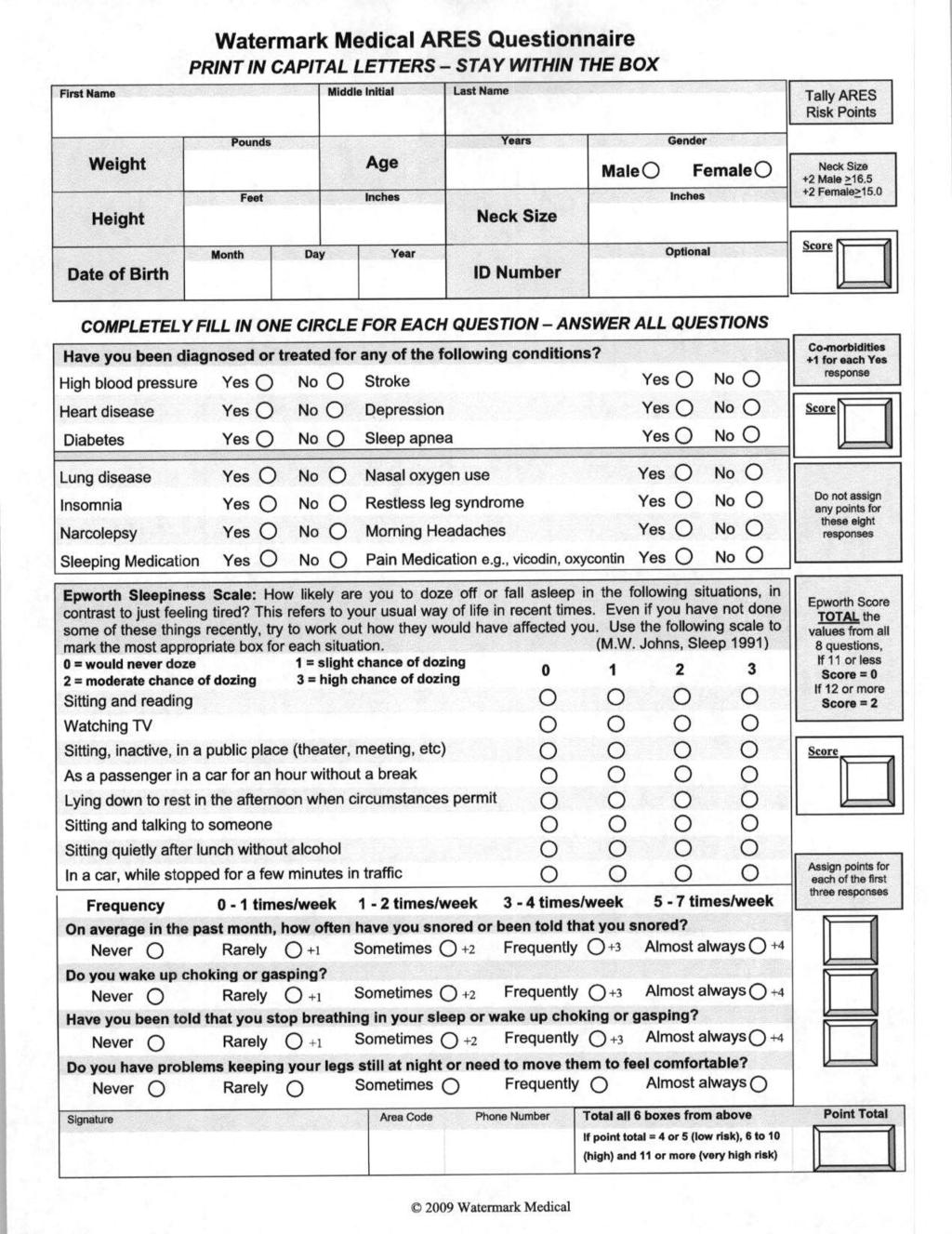
 To Our New Patient: Our staff would like to take this opportunity to welcome you to Garden State Snoring Solutions, LLC. It is our goal to make your visit with us as pleasant and comfortable as possible.
To Our New Patient: Our staff would like to take this opportunity to welcome you to Garden State Snoring Solutions, LLC. It is our goal to make your visit with us as pleasant and comfortable as possible.
Patient Registration Forms
 Patient Registration Forms PATIENT INFORMATION First Name: Middle: Last: DOB: / / Sex: M/F Primary Language: Address: City: ST ZIP Ethnicity: Hispanic / Non-Hispanic / Unknown Race: Asian / White / African
Patient Registration Forms PATIENT INFORMATION First Name: Middle: Last: DOB: / / Sex: M/F Primary Language: Address: City: ST ZIP Ethnicity: Hispanic / Non-Hispanic / Unknown Race: Asian / White / African
Patient Information. Responsible Party. Notify in case of emergency?
 We are pleased to welcome you and your child to our practice. Please take a few minutes to fill out this form as completely as you can. If you have questions, we'll be glad to help you. We look forward
We are pleased to welcome you and your child to our practice. Please take a few minutes to fill out this form as completely as you can. If you have questions, we'll be glad to help you. We look forward
Welcome! Warren Parkway Suite 306 Frisco, TX PlastiksForKids.com. Please remember to bring: New Patient Paperwork
 Welcome! Thank you for choosing Dr. Christine Stiles to care for your child s plastic surgery needs. All appointments are on Monday afternoons. Dr. Stiles operates at the Pediatric Surgery Center. Plastiks
Welcome! Thank you for choosing Dr. Christine Stiles to care for your child s plastic surgery needs. All appointments are on Monday afternoons. Dr. Stiles operates at the Pediatric Surgery Center. Plastiks
Patient Registration. All Inclusive Primary Care. PATIENT INFORMATION Name: (Last, First, MI) Address: City: State/Province: Zip: Country:
 Address: City: State/Province: Zip: Country:") Patient Registration PATIENT INFORMATION Name: (Last, First, MI) Address: City: State/Province: Zip: Country: Mailing Address (if different from above): Home Phone: Work: Mobile: Email: SSN: Birth Date:
Patient Registration PATIENT INFORMATION Name: (Last, First, MI) Address: City: State/Province: Zip: Country: Mailing Address (if different from above): Home Phone: Work: Mobile: Email: SSN: Birth Date:
Stonebridge Adult Medicine, P.A. Registration Form (Please Print)
") Stonebridge Adult Medicine, P.A. Registration Form (Please Print) PATIENT INFORMATION Last Name: First Name: Is this your legal name? Yes No If not what is your legal name: Date of Birth: Sex: male female
Stonebridge Adult Medicine, P.A. Registration Form (Please Print) PATIENT INFORMATION Last Name: First Name: Is this your legal name? Yes No If not what is your legal name: Date of Birth: Sex: male female
Greenberg Chiropractic LLC REGISTRATION FORM (Please Print)
") Today s Date: LLC REGISTRATION FORM (Please Print) PATIENT INFORMATION Patient s last name: First: Middle: Mr. Miss Marital status: Mrs. Ms. Single Mar Div Sep Wid Is this your legal name? If not, what
Today s Date: LLC REGISTRATION FORM (Please Print) PATIENT INFORMATION Patient s last name: First: Middle: Mr. Miss Marital status: Mrs. Ms. Single Mar Div Sep Wid Is this your legal name? If not, what
Family Physicians of Johnson City 303 Med Tech Parkway, Suite 100 Johnson City, TN 37604
 Family Physicians of Johnson City 303 Med Tech Parkway, Suite 100 Johnson City, TN 37604 Patient Registration Form Last Name First Name Middle Initial Sex: M F of Birth Address City State Zip Code Social
Family Physicians of Johnson City 303 Med Tech Parkway, Suite 100 Johnson City, TN 37604 Patient Registration Form Last Name First Name Middle Initial Sex: M F of Birth Address City State Zip Code Social
Welcome to our medical practice. We pride ourselves on providing you with the best medical care possible.
 Dear Patient: Welcome to our medical practice. We pride ourselves on providing you with the best medical care possible. Our relationship with you is important to us. Please complete all forms carefully
Dear Patient: Welcome to our medical practice. We pride ourselves on providing you with the best medical care possible. Our relationship with you is important to us. Please complete all forms carefully
FILING- THE PATIENT IS ULTIMATELY RESPONSIBLE FOR PAYMENT IN FULL OF THEIR ACCOUNT, NOT THE INSURANCE COMPANY.
 FINANCIAL AGREEMENT- PAYMENT IS REQUIRED FOR ALL DENTAL SERVICES AT THE TIME TREATMENT IS RENDERED. We accept Visa, MasterCard, Discover, American Express, Care Credit, Cash or Check. INSURANCE FILING-
FINANCIAL AGREEMENT- PAYMENT IS REQUIRED FOR ALL DENTAL SERVICES AT THE TIME TREATMENT IS RENDERED. We accept Visa, MasterCard, Discover, American Express, Care Credit, Cash or Check. INSURANCE FILING-
If you have questions about how much your fee will be, you may stop by or call with your income information before your appointment.
 238 Arsenal Street, Watertown, NY Family Practice Office: (315) 782-6400 Fax: (315) 782-1330 Adult Office: (315) 782-9903 Fax: (315) 788-0087 Dental Office: (315) 788-9834 Fax: (315) 788-5456 7785 N. State
238 Arsenal Street, Watertown, NY Family Practice Office: (315) 782-6400 Fax: (315) 782-1330 Adult Office: (315) 782-9903 Fax: (315) 788-0087 Dental Office: (315) 788-9834 Fax: (315) 788-5456 7785 N. State
Child s Name: Gender: M or F Last First MI. Date Of Birth: - - ADDRESS: CITY: STATE ZIP: REFERRING SOURCE. Physician Name Last First MI
 PATIENT INFORMATION PATIENT INTAKE FORM DATE: PT/OT/ST Child s Name: Gender: M or F Last First MI Date Of Birth: - - SS# - - ADDRESS: CITY: STATE ZIP: REFERRING SOURCE Physician Name Last First MI Phone:
PATIENT INFORMATION PATIENT INTAKE FORM DATE: PT/OT/ST Child s Name: Gender: M or F Last First MI Date Of Birth: - - SS# - - ADDRESS: CITY: STATE ZIP: REFERRING SOURCE Physician Name Last First MI Phone:
Welcome to Pediatric Dentistry of Greenville!
 Welcome to Pediatric Dentistry of Greenville! Child's Information Child's Name(Last, First, Middle Initial) Child's DOB: / / Child's Age Nickname: ( ) Male ( ) Female School : Grade: Child's Home Phone
Welcome to Pediatric Dentistry of Greenville! Child's Information Child's Name(Last, First, Middle Initial) Child's DOB: / / Child's Age Nickname: ( ) Male ( ) Female School : Grade: Child's Home Phone
 2014 Established Patient Registration Welcome to the New Year! We ask that all of our patients provide us with updated information, such as phone number, address, insurance, etc, as well as sign an updated
2014 Established Patient Registration Welcome to the New Year! We ask that all of our patients provide us with updated information, such as phone number, address, insurance, etc, as well as sign an updated
VEIN CENTER OF VENTURA
 168 N. Brent St., #508 Ventura, CA 93003 Tele: (805) 643-2855 Fax: (805) 643-3511 PATIENT INFORMATION Name of Birth SS # Marital Status: Sex: Home Address City State Zip Email Mailing Address (if different)
168 N. Brent St., #508 Ventura, CA 93003 Tele: (805) 643-2855 Fax: (805) 643-3511 PATIENT INFORMATION Name of Birth SS # Marital Status: Sex: Home Address City State Zip Email Mailing Address (if different)
Patient Registration PATIENTS WITH DENTAL INSURANCE ALL THIS INFORMATION IS NECESSARY TO VERIFY YOUR DENTAL COVERAGE!!
 Patient Registration Patient Name Date of Birth Age If child, Parent's name: Mr. Mrs. Ms. Dr. I prefer to be called Single Married Divorced Widowed M F Address City St Zip. Home Phone( ) Cell Phone( )
Patient Registration Patient Name Date of Birth Age If child, Parent's name: Mr. Mrs. Ms. Dr. I prefer to be called Single Married Divorced Widowed M F Address City St Zip. Home Phone( ) Cell Phone( )
Kalpana Thakur, M.D. PA Registration Form
 Registration Form (Please Print): : Patient Information Last Name: First: Middle: of Birth: Age: Sex: M F Marital Status: Single Married Other S.S. Number Home phone: Mobile: Street Address: City: State:
Registration Form (Please Print): : Patient Information Last Name: First: Middle: of Birth: Age: Sex: M F Marital Status: Single Married Other S.S. Number Home phone: Mobile: Street Address: City: State:
WELCOME- OUR PHILOSOPHY
 WELCOME- OUR PHILOSOPHY Dear Patient, Thank you for choosing me to provide your orthopedic care. My team and I will make every effort to treat you with courtesy, respect and kindness, while providing the
WELCOME- OUR PHILOSOPHY Dear Patient, Thank you for choosing me to provide your orthopedic care. My team and I will make every effort to treat you with courtesy, respect and kindness, while providing the
you like listed as your primary
 Patient Information Southlake Chiropractic welcomes you to our office. We strive to provide the best possible chiropractic care. Dr. Devos will conduct a thorough history and physical exam to decide how
Patient Information Southlake Chiropractic welcomes you to our office. We strive to provide the best possible chiropractic care. Dr. Devos will conduct a thorough history and physical exam to decide how
WELCOME TO OUR PRACTICE
 WELCOME TO OUR PRACTICE On behalf of the entire team at Pebblewood Dental, let us welcome you to our practice. We are grateful that you have chosen us to meet your dental needs, and trust that you will
WELCOME TO OUR PRACTICE On behalf of the entire team at Pebblewood Dental, let us welcome you to our practice. We are grateful that you have chosen us to meet your dental needs, and trust that you will
Name Preferred Name Sex. Home Address. Home Phone Age Date of Birth. School Grade. How did you hear about us?
 ID CHECKED (RESPONSIBLE PARTY) INFORMATION (CHILD UNDER 18) Name Preferred Name Sex Home Address Home Phone Age School Grade How did you hear about us? What is the name/phone number of the child s previous
ID CHECKED (RESPONSIBLE PARTY) INFORMATION (CHILD UNDER 18) Name Preferred Name Sex Home Address Home Phone Age School Grade How did you hear about us? What is the name/phone number of the child s previous
Permission Letter. Patient Name(s):
:") Permission Letter Patient Name(s): If someone other than the parent or legal guardian may bring your child (ren), please list their name(s) below. They must be 18 years of age and have a photo i.d. We
Permission Letter Patient Name(s): If someone other than the parent or legal guardian may bring your child (ren), please list their name(s) below. They must be 18 years of age and have a photo i.d. We
Patient Registration
 Patient Registration First Name: Middle Initial: Last Name: Address: City: State / Zip: Responsible Party (for patients under 18): Home Phone: Cell Phone: Work Phone: Date of Birth: Social Security Number:
Patient Registration First Name: Middle Initial: Last Name: Address: City: State / Zip: Responsible Party (for patients under 18): Home Phone: Cell Phone: Work Phone: Date of Birth: Social Security Number: