Term Life, Disability & Beneficiary Enrollment Form
|
|
|
- Jessie Goodman
- 6 years ago
- Views:
Transcription
1 Term Life, Disability & Beneficiary Enrollment Form Important notice: This form replaces all other enrollment forms on file, and must be signed and dated for enrollment or beneficiary to be valid. Section 1 Member Information This enrollment is for: mnew Member mopen Enrollment mbeneficiary Designation Only mchange Reason for change: Name Date of Birth Gender mm mf Social Security Number Agency Employed Home Phone Mailing Address City/State Zip Work Phone Date of change: Marital Status msingle mmarried mdomestic Partnership (per Certificate of Registered Domestic Partnership) mwidowed mdivorced mdomestic Partner (per Affidavit of Domestic Partnership)* *If enrolling a domestic partner attach a completed SEIU Local 503 Affidavit of Domestic Partnership form. am Free $2,500 Member Term Life How many hours per month do you work in your SEIU Local 503 represented position? Section 2 Voluntary Term Life Insurance (you must work at least 40 hours per month to enroll in life insurance) You must be enrolled in member term life to apply for spouse/partner or child term life. Spouse/partner term life amount cannot exceed member term life amount. Member Term Life (Member term life benefit levels are $10,000, $20,000, $30,000 $40,000, $50,000, $60,000, $70,000, $80,000, $90,000, $100,000, $110,000, $120,000, $130,000, $140,000 or $150,000) m$10,000 m$20,000 m$30,000 m$40,000 mincrease Member Life to $ Spouse/Partner Term Life (Spouse term life benefit levels are $10,000, $20,000, $30,000 $40,000, $50,000, $60,000, $70,000, $80,000, $90,000, $100,000, $110,000, $120,000, $130,000, $140,000 or $150,000) m$10,000 or m$20,000 mincrease Spouse Life to $ Spouse/Partner Name Date of Birth Relationship Child Term Life m$5,000 or m$10,000 Child Name Date of Birth Relationship Section 3 Voluntary Short Term Disability Insurance (you must work at least 80 hours per month to enroll in short term disability insurance) Short Term Disability Insurance: $ mclass 1 mclass 2 mclass 3 mclass 4 (current monthly salary) Monthly Salary: up to $999 $1,000-$2,999 $3,000-$3,999 $4,000 and up Section 4 Beneficiary Designation (attach an additional sheet if more space is required. Additional sheet must be signed and dated to be valid) You may choose a beneficiary(s) to receive life benefits. If no beneficiary survives, payment will be made in accordance with the terms of the policy. Unless designated otherwise, beneficiary designations for all life coverage will be the same. For Spouse/Partner and Child Term Life, you are the beneficiary. Name of Beneficiary Social Security # Date of Birth Address Relationship Primary Contingent Section 5 Signature for Enrollment, Beneficiary Designation and Authorization for Payroll Deduction I hereby apply for benefits under SEIU Local 503 group insurance plan issued by LifeMap Assurance Company. I authorize my employer to deduct from my salary the amount necessary to cover my premium for the group coverage (if payroll deduction is available).* The amount of such insurance and the premium thereon is subject to change as determined by the salary and age schedule as outlined in the benefit booklet and master policy issued by LifeMap Assurance Company. Signature Date * Please read the information on the back of this form. FOR SEIU USE ONLY MEMBER DATE CODE DEDUCTION AMOUNT AGENCY EFFECTIVE DATE A M S C D Please keep a photocopy for your records and mail this original to: SEIU Local 503 at P.O. Box 12159, Salem, Oregon 97309, to memberbenefits@seiu503.org or fax to (503) Revised 9/2017 GWNN
2 Insurance will become effective the 1st of the month for which payroll deduction is taken. If the deduction is taken on the last day of the month, the insurance will become effective the 1st of the following month. Payroll deduction may not be available through all employers. Contact your payroll department or the SEIU Local 503 benefits department if you have any questions. If payroll deduction is not available you will be required to self pay your premium. Benefit Eligibility To be eligible for coverage under this plan you must maintain your membership with SEIU Local 503. You must work at least 40 hours per month in your SEIU Local 503 represented position to purchase life insurance. You must work at least 80 hours per month in your SEIU Local 503 represented position to purchase short term disability insurance. You must be scheduled for the minimum required hours and actively working for your insurance to take effect. Dependents eligible for coverage include spouse/partner and all unmarried dependent children under age 26. If enrolling a domestic partner attach a completed Affidavit of Domestic Partnership form or indicate on the front of this form that you have obtained a Certificate of Registered Domestic Partnership. If a dependent cannot perform the normal activities of a person of his or her age and sex on the date of his or her coverage would begin his or her coverage will not begin until he or she is so able. Enrollment Change Elections can only be changed or canceled during an Open Enrollment period or with a qualified status event. You must notify SEIU Local 503 Member Benefits within 31 days of the qualified event to be eligible for the enrollment change. Termination of Coverage Coverage under the term life plan ends when the participant fails to make the required monthly premium payment, or fails to meet the eligibility requirements and/or is no longer a member of SEIU Local 503. If a plan participant retires or terminates employment, life insurance will be continued without cost for 31 days. Within that period, you may convert your Voluntary Term Life Insurance to an individual guaranteed permanent policy. Application for conversion must be made within 31 days of retirement or employment termination. It is your responsibility to contact the SEIU Local 503 Benefits Department to request an application for conversion. If a plan participant terminates employment prior to age 65 Voluntary Term Life Insurance benefits can be ported. You must apply within 31 days from the date your employment terminated. It is your responsibility to contact the SEIU Local 503 Benefits Department to request an application for portability. Benefit eligibility and termination provisions are detailed in the LifeMap Assurance Company Benefit Booklet. The booklet is located on the SEIU Local 503 website member benefits page at seiu503.org. You can obtain a printed copy of the booklet by contacting the SEIU Local 503 Member Benefits Department at the number below. The plan may be amended from time to time or terminated in its entirety at any time by SEIU Local 503. SEIU Local 503 PO Box Salem, Oregon SEIU (7348)
 $ Child(ren) $ Verified Applying for: Total Amount of Insurance requested (Show existing PLUS any increase) Supplemental Life STD Class Member $ Spouse/DP $")
 Social Security Number Birthdate Gender Place of Birth Mo Day Yr M")
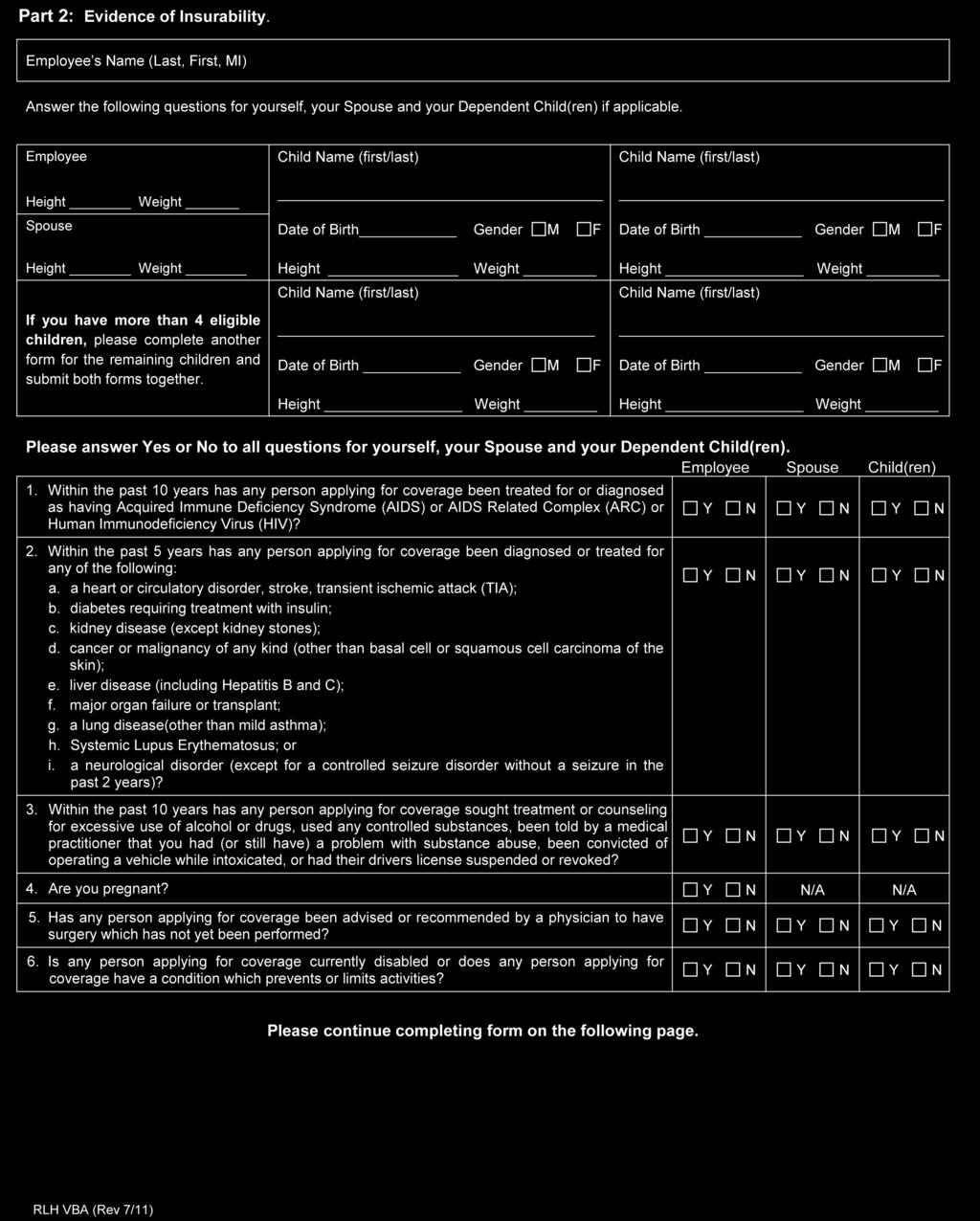
3 P.O. Box 1271 MS E8L Portland, OR Mail to: SEIU Local 503 P.O. Box Salem, OR Evidence of Insurability Form Part I This box for SEIU use only: Existing Voluntary Coverage: Member $ Spouse/Domestic Partner (DP) $ Child(ren) $ Verified Applying for: Total Amount of Insurance requested (Show existing PLUS any increase) Supplemental Life STD Class Member $ Spouse/DP $ Child(ren) $ Member Name Phone Number Residence Address Street City State Zip Code Social Security Number Birthdate Gender Place of Birth Annual Salary Mo Day Yr M F $ / / Name of organization providing insurance Policy Number Occupation Date of Employment SEIU Local 503 OR Spouse / DP Name (if applying for coverage) Social Security Number Birthdate Gender Place of Birth Mo Day Yr M F / / Agreements I request to be insured and authorize payroll deductions to cover the cost of coverage. Information in this application is given to obtain insurance, and the statements and answers are represented, to the best of my (our) knowledge and belief, to be true and complete. I (we) understand that (a) the insurance applied for shall not take effect until the application is approved and I will be notified of the insurance Effective Date; and (b) all insurance is subject to the eligibility provisions of the Policy; and (c) I must be Actively at Work (as defined in the Group Policy) to be insured. If I am not Actively at Work on the date my (our) coverage would become effective, my (our) coverage will not begin until the day I return to work. Authorization to Release Information: I authorize any licensed physician, medical practitioner, hospital, clinic, or other medical or medically related facility, insurance company or other organization, institution or person that has any records or knowledge of me or my health to give the LifeMap Assurance Company or its reinsurers any such information (including information about drug or alcohol use or abuse, mental illness, HIV (AIDS virus) or other sexually transmitted diseases). This authorization is valid for 24 months from the date it is signed. I agree that a photocopy of this authorization shall be as valid as the original. I acknowledge that I have received a copy of the Privacy Notice. Insurance Fraud Warning: Unless specific state language is provided below, the following general fraud notice applies: Any person who knowingly provides false, incomplete, or misleading information to an insurance company for the purpose of defrauding the company may be guilty of a crime. Penalties may include imprisonment, fines, and denial of insurance benefits. For residents of Washington: It is a crime to knowingly provide false, incomplete, or misleading information to an insurance company for the purpose of defrauding the company. Penalties include imprisonment, fines, and denial of insurance benefits. If your answers on this application are incorrect or untrue, LifeMap Assurance Company has the right to deny benefits or rescind your coverage for up to two years from the date coverage becomes effective. X Member Signature Date Signed Spouse / DP (if applying for coverage) Date Signed X FORM RLH161 Front (7/99) SEIU OR (Please complete all three pages of this form.)
4

5 Employee s Name (Last, First, MI)
6 AUTHORIZATION TO DISCLOSE PROTECTED HEALTH INFORMATION I authorize any physician, pharmacy benefit manager, retail pharmacy, clearing house, health plan or insurance company to disclose prescription drug information about me within their possession to Milliman IntelliScript on behalf of LifeMap Assurance Company ( LifeMap ). The purpose of this disclosure is for Milliman to provide the information to LifeMap to evaluate my application for Life, Disability, and/or Critical Illness insurance products. I understand that this prescription drug information may contain sensitive data, including data related to the treatment of sexually transmitted diseases, HIV/AIDS, mental health and reproduction or contraception (including prenatal care and abortion). I specifically authorize the disclosure of prescription drug information that is related to alcohol or substance abuse and I understand that my alcohol and substance abuse records are protected under Federal law (42 CFR Part 2) and cannot be disclosed without my written consent unless otherwise provided for in 42 CFR Part 2. I also understand that I may cancel this approval at any time, as described below. I understand and acknowledge the following: Once any person(s) or entity(ies) discloses my information to an authorized recipient the privacy protections provided by law may no longer apply. I may cancel this authorization at any time by sending written notice to LifeMap Assurance Company, Attn: Individual Underwriting, PO Box 1271 M/S E8L, Portland, OR Cancellation of this authorization will not affect any actions taken by any entity disclosing information before receiving the cancellation notice. Completing this authorization is a condition to be eligible for and enrolled in LifeMap Life, Disability and/or Critical Illness insurance products. None of the authorized person(s) and entity(ies) above nor Milliman are responsible for any action taken by an authorized recipient of my protected health information. This authorization will expire two years from the data signed unless a shorter time frame is requested here (mm/dd/yyyy):. Applicant Full Name (please print clearly) SEIU LOCAL 503 Group Name Date of Birth (MM/DD/YYYY) OR Group Number Applicant Signature Date If you are signing this authorization on behalf of another individual, please complete the following and attach documentation demonstrating your authority to act on behalf of the individuals (e.g., Power of Attorney, Guardianship, Conservatorship, etc.) Name of Personal Representative Relationship Phone Signature of Personal Representative Date LifeMap EOI AuthRx v (8/17)
7 SEIU LOCAL 503 AFFIDAVIT OF DOMESTIC PARTNERSHIP information practices notice SECTION ONE AFFIRMATION OF DOMESTIC PARTNERSHIP (1) Are each eighteen (18) years of age or older. (2) Share a close personal relationship and are responsible for each other s common welfare. (3) Are each other s sole domestic partner. (4) Are not married to anyone nor have had another domestic partner within the prior six months. (5) Are not related by blood closer than would bar marriage in the State of Oregon. (6) Have jointly shared the same regular and permanent residence for at least six (6) months immediately preceding the date of this affidavit with the intent to continue doing so indefinitely. (7) Have signed a domestic partner declaration (applicable in jurisdictions, which provides for domestic partner declarations). (8) Are jointly financially responsible for basic living expenses defined as the cost of food, shelter, and any other expenses of maintaining a household. Domestic partners need not contribute equally or jointly to the cost of these expenses as long as they agree that both are responsible for the cost. If requested I would be able to provide at least three of the following as verification of our joint responsibility. (a) Joint mortgage or lease. (b) Designation of the domestic partner as primary beneficiary for a life insurance or a retirement contract. (c) Designation of the domestic partner as primary beneficiary in the employee s will. (d) Durable power of attorney for health care or financial management. (e) Joint ownership of a motor vehicle, a joint checking account, or a joint credit account. (f) A relationship or cohabitation contract which obligates each of the parties to provide support for the other party. SECTION TWO DECLARATION OF MEMBER (1) I understand that my domestic partner is eligible for enrollment: (a) Within 90 days of my becoming a new member of SEIU Local 503. (b) During an open enrollment period. (c) Within 31 days of meeting the criteria listed in Section One. (2) I understand that children of my domestic partner are eligible if they meet the requirement for an eligible dependent as defined by LifeMap Assurance Company, and/or ARAG Group. (3) I understand that this affidavit shall be terminated upon the death of my domestic partner or by a change in circumstance attested to in this Affidavit. (4) I agree to file a Statement of Termination of Domestic Partnership with the SEIU Local 503 Benefits Department within 30 days of any change to circumstances attested to in this Affidavit. (5) After such termination, I understand that another Affidavit of Domestic Partnership cannot be filed with the SEIU Local 503 Benefits Department until such time as the conditions of Section One above have been met.
8 SECTION THREE DECLARATION OF PARTNERS (1) We understand that the information contained in the Affidavit relates to eligibility for benefits under the SEIU Local 503 life and/or legal insurance program. Any other use of this information will be subject to disclosure only upon either of our written authorization or as required by law. (2) We understand that a civil action may be brought against us for any losses, including reasonable attorney fees and court costs, because of willful falsification of information contained in this Affidavit of Domestic Partnership. (3) We understand that in addition to the eligibility requirements of SEIU Local 503 member benefit program for domestic partner coverage, there are terms and conditions of coverage set forth in the Service Agreement of each insurance plan offered through SEIU Local 503, plans which we agree to be bound. (4) We understand willful falsification of information contained in this Affidavit will result in termination of enrollment pursuant to this agreement by the SEIU Local 503 member benefit program. We certify under penalty of perjury under the laws or the State of Oregon, that the foregoing is true and accurate to the best of our knowledge Signature of Member Print Name Signature of Domestic Partner Print Name Member SSN Date *This affidavit of domestic partnership is for SEIU Local 503 life and/or legal insurance enrollment only and must be received by the SEIU Local 503 Benefits Department to be valid.* Fax completed enrollment forms and domestic partner affidavit to (503) , mail to SEIU Local 503, PO Box 12159, Salem, OR or to memberbenefits@seiu503.org.
 721-7161 * (800)")
9 LifeMap Assurance Company 200 SW Market St P.O. Box 1271, M/S E8L Portland, OR (503) * (800) PRIVACY NOTICE 18
Assurance Company. Term Life Eligibility. Child Term Life Insurance. Member Term Life Insurance LIFE INSURANCE
 Assurance Company Voluntary Term Life and Short Term Disability Insurance Term Life Eligibility If you are a member and work at least 40 hours per month, you are eligible to apply for member Voluntary
Assurance Company Voluntary Term Life and Short Term Disability Insurance Term Life Eligibility If you are a member and work at least 40 hours per month, you are eligible to apply for member Voluntary
Legal Insurance from ARAG
 Legal Insurance from ARAG Designed for SEIU Local 503 Members LEGAL INSURANCE Save Time and Money with Legal Insurance Legal insurance helps you address everyday situations like dealing with traffic tickets,
Legal Insurance from ARAG Designed for SEIU Local 503 Members LEGAL INSURANCE Save Time and Money with Legal Insurance Legal insurance helps you address everyday situations like dealing with traffic tickets,
Legal Insurance from ARAG
 Legal Insurance from ARAG Designed for SEIU Local 503 Members LEGAL INSURANCE Legal is everywhere. Protect yourself and your family with legal insurance. Have you ever stopped to think about how many events
Legal Insurance from ARAG Designed for SEIU Local 503 Members LEGAL INSURANCE Legal is everywhere. Protect yourself and your family with legal insurance. Have you ever stopped to think about how many events
Application Enrollment Form for AVMA LIFE Trust Group Insurance Program
 Application Enrollment Form for AVMA LIFE Trust Group Insurance Program Complete this form and return to: AVMA LIFE Trust Program Administrator 1200 E. Glen Ave. Peoria Heights, IL 61616-5384 Please print
Application Enrollment Form for AVMA LIFE Trust Group Insurance Program Complete this form and return to: AVMA LIFE Trust Program Administrator 1200 E. Glen Ave. Peoria Heights, IL 61616-5384 Please print
Group Policy G SOCIAL SECURITY NO. WEIGHT LBS. BILLING ADDRESS / / CITY STATE ZIP CODE HOME PHONE
 Group Term Life Insurance Application Please complete and return this form to: Worldwide Assurance for Employees of Public Agencies (WAEPA) 433 Park Ave., Falls Church, VA 22046 (800)368-3484 www.waepa.org
Group Term Life Insurance Application Please complete and return this form to: Worldwide Assurance for Employees of Public Agencies (WAEPA) 433 Park Ave., Falls Church, VA 22046 (800)368-3484 www.waepa.org
RETURN THIS COPY TO JOHN HANCOCK. City/Town: State: Zip:
 HIPAA Authorization ATTN: R-02-B Long-Term Care PO Box 852 Boston, MA 02117-0852 Insured Name : Phone: 800-233-1449 Fax: 617-572-7979 Claim Number: Insured Street Address: RETURN THIS COPY TO JOHN HANCOCK
HIPAA Authorization ATTN: R-02-B Long-Term Care PO Box 852 Boston, MA 02117-0852 Insured Name : Phone: 800-233-1449 Fax: 617-572-7979 Claim Number: Insured Street Address: RETURN THIS COPY TO JOHN HANCOCK
SMALL GROUP ENROLLMENT/CHANGE FORM COMPLETE THIS APPLICATION IN ITS ENTIRETY IN BLUE OR BLACK INK. DO NOT USE PENCIL OR HIGHLIGHTER.
 22259 SMALL GROUP ENROLLMENT/CHANGE FORM COMPLETE THIS APPLICATION IN ITS ENTIRETY IN BLUE OR BLACK INK. DO NOT USE PENCIL OR HIGHLIGHTER. q ENROLLING (Complete sections I, II, IV, and V) q WAIVING (Complete
22259 SMALL GROUP ENROLLMENT/CHANGE FORM COMPLETE THIS APPLICATION IN ITS ENTIRETY IN BLUE OR BLACK INK. DO NOT USE PENCIL OR HIGHLIGHTER. q ENROLLING (Complete sections I, II, IV, and V) q WAIVING (Complete
MOSERS Continued Dependent Life Insurance for a Disabled Child Instructions
 Continued Dependent Life Insurance Instructions Your application for consists of four forms. Every space should be filled in to avoid delay in processing your application. If a section does not apply,
Continued Dependent Life Insurance Instructions Your application for consists of four forms. Every space should be filled in to avoid delay in processing your application. If a section does not apply,
State of Florida Accelerated Benefits Claim Form
 State of Florida Account Participating Agencies and Departments Payroll Deduction Code 262 MAIL COMPLETED FORM TO: Cigna PO Box 22328 Pittsburgh, PA 15222-0328 Toll Free #: 18002382125 Fax #: 4124023506
State of Florida Account Participating Agencies and Departments Payroll Deduction Code 262 MAIL COMPLETED FORM TO: Cigna PO Box 22328 Pittsburgh, PA 15222-0328 Toll Free #: 18002382125 Fax #: 4124023506
Group Customer #
 ENROLLMENT CHANGE FORM ENROLLMENT PERIOD FROM OCTOBER 29, 2018 NOVEMBER 16, 2018 GROUP CUSTOMER INFORMATION (To be Completed by the Recordkeeper) Name of Group Customer/Employer Group Customer # 113484
ENROLLMENT CHANGE FORM ENROLLMENT PERIOD FROM OCTOBER 29, 2018 NOVEMBER 16, 2018 GROUP CUSTOMER INFORMATION (To be Completed by the Recordkeeper) Name of Group Customer/Employer Group Customer # 113484
If you do not submit the Evidence of Insurability form within the 31-day period, your request for coverage will be withdrawn.
 For the Employees, the Evidence of Insurability form must be completed if: You are requesting optional life insurance after your first 31 days of eligibility; or The requested amount causes your coverage
For the Employees, the Evidence of Insurability form must be completed if: You are requesting optional life insurance after your first 31 days of eligibility; or The requested amount causes your coverage
Employee last name Employee first name M.I. Employee Social Security no.* (required)
") Employee Form For 1 100 Employee Small Groups California Instructions: If you are cancelling coverage for a dependent or changing a name, please provide a reason in the designated sections. Complete electronically,
Employee Form For 1 100 Employee Small Groups California Instructions: If you are cancelling coverage for a dependent or changing a name, please provide a reason in the designated sections. Complete electronically,
POLICY INFORMATION PATIENT INFORMATION CLAIM INFORMATION
 PO Box 83043 Lincoln, NE 68501-3043 866-863-9753 Fax: 402-479-0146 If filing a claim for Wellness Screening Benefit or RX Benefit* no form is needed, please call 866-863-9753. * When you call, it is helpful
PO Box 83043 Lincoln, NE 68501-3043 866-863-9753 Fax: 402-479-0146 If filing a claim for Wellness Screening Benefit or RX Benefit* no form is needed, please call 866-863-9753. * When you call, it is helpful
or my newly adopted/placed for adoption child(ren): placement date)
: placement date)") Washington Individual Enrollment Application Effective January 1, 2016 This application is for health care coverage purchased directly from Premera Blue Cross (Premera). For timely and proper processing,
Washington Individual Enrollment Application Effective January 1, 2016 This application is for health care coverage purchased directly from Premera Blue Cross (Premera). For timely and proper processing,
Hospital Indemnity Insurance Claim Form
 Hospital Indemnity Insurance Claim Form Things to know before you begin If you are submitting a claim for a Hospitalization which you have not yet reported to us, please complete this claim form. Once
Hospital Indemnity Insurance Claim Form Things to know before you begin If you are submitting a claim for a Hospitalization which you have not yet reported to us, please complete this claim form. Once
PPO Enrollment Application
 PPO Enrollment Application Welcome to Anthem Blue Cross and Blue Shield (Anthem). This is your Enrollment Application and Form. Because we are dedicated to making the enrollment process easy for you, this
PPO Enrollment Application Welcome to Anthem Blue Cross and Blue Shield (Anthem). This is your Enrollment Application and Form. Because we are dedicated to making the enrollment process easy for you, this
ACCIDENT WELLNESS BENEFIT CLAIM FORM
 ACCIDENT WELLNESS BENEFIT CLAIM FORM Failure to complete all sections may result in a delay in processing this claim. Please review your policy for specific benefits covered under your plan Benefits are
ACCIDENT WELLNESS BENEFIT CLAIM FORM Failure to complete all sections may result in a delay in processing this claim. Please review your policy for specific benefits covered under your plan Benefits are
Health Screening Benefit Claim Form
 Part 1 Health Screening Benefit Claim Form Things to know before you begin Complete Part 1 of the claim form (pages 1-5). In addition to Part 1, you will also need to submit Proof Requirements. There are
Part 1 Health Screening Benefit Claim Form Things to know before you begin Complete Part 1 of the claim form (pages 1-5). In addition to Part 1, you will also need to submit Proof Requirements. There are
GROUP LIFE AND/OR ACCIDENTAL DEATH CLAIM FORM
 OUR COMMITMENT For use with policies issued by the following Unum Group [ Unum ] subsidiaries: Unum Life Insurance Company of America Provident Life and Accident Insurance Company The Paul Revere Life
OUR COMMITMENT For use with policies issued by the following Unum Group [ Unum ] subsidiaries: Unum Life Insurance Company of America Provident Life and Accident Insurance Company The Paul Revere Life
LTD EMPLOYER'S STATEMENT
 LTD EMPLOYER'S STATEMENT INSTRUCTIONS TO EMPLOYER: Complete the Employer's Statement & attach job description. Instruct employee to complete Employee's Statement and have Physician's Statement completed.
LTD EMPLOYER'S STATEMENT INSTRUCTIONS TO EMPLOYER: Complete the Employer's Statement & attach job description. Instruct employee to complete Employee's Statement and have Physician's Statement completed.
ACCIDENT WELLNESS BENEFIT CLAIM FORM
 CONTINENTAL AMERICAN INSURANCE COMPANY Post Office Box 84075 * Columbus, GA. 31993 Phone (800) 433-3036 * Fax (866) 849-2970 ACCIDENT WELLNESS BENEFIT CLAIM FORM Failure to complete all sections may result
CONTINENTAL AMERICAN INSURANCE COMPANY Post Office Box 84075 * Columbus, GA. 31993 Phone (800) 433-3036 * Fax (866) 849-2970 ACCIDENT WELLNESS BENEFIT CLAIM FORM Failure to complete all sections may result
Washington State Enrollment Form for Medical and/or Prescription Insurance for Individuals and Families
 Washington State Enrollment Form for Medical and/or Prescription Insurance for Individuals and Families PLEASE PRINT IN BLACK INK AGENT/AGENCY INFORMATION Agent Name: Agent Number: Key Agency Contact:
Washington State Enrollment Form for Medical and/or Prescription Insurance for Individuals and Families PLEASE PRINT IN BLACK INK AGENT/AGENCY INFORMATION Agent Name: Agent Number: Key Agency Contact:
RELATIONSHIP TO THE POLICYHOLDER: HEALTH SCREENING INFORMATION
 ACCIDENT WELLNESS BENEFIT CLAIM FORM INSTRUCTIONS Please use black or blue ink only and print legibly when completing this form in its entirety. Keep a copy of the supporting documentation and this completed
ACCIDENT WELLNESS BENEFIT CLAIM FORM INSTRUCTIONS Please use black or blue ink only and print legibly when completing this form in its entirety. Keep a copy of the supporting documentation and this completed
*ABONY1201* Group Insurance. Accelerated Benefit Option Claim Form New York (Use for employee/member and dependent claims.)
") Accelerated Benefit Option Claim Form New York (Use for employee/member and dependent claims) How to present a claim Beneficiary s Signature (Required only if irrevocable) GL2002202 (12) Ed 4/2017 *ABONY1201*
Accelerated Benefit Option Claim Form New York (Use for employee/member and dependent claims) How to present a claim Beneficiary s Signature (Required only if irrevocable) GL2002202 (12) Ed 4/2017 *ABONY1201*
Please Print in Black Ink To Be Completed by Proposed Insured. Last First MI DOB Sex SSN - - Address Street or Post Office Box
 Application for Accident Insurance (A35000 Series) Application to American Family Life Assurance Company of Columbus (Aflac) Worldwide Headquarters Columbus, Georgia 31999 New Conversion Policy Number
Application for Accident Insurance (A35000 Series) Application to American Family Life Assurance Company of Columbus (Aflac) Worldwide Headquarters Columbus, Georgia 31999 New Conversion Policy Number
New York Life Insurance Company
 The Company You Keep New York Life Insurance Company Group Membership Association Claims PO Box 30782 Tampa FL 33630-3782 (800) 792-9686 Dear Beneficiary: Please accept our condolences on your recent loss.
The Company You Keep New York Life Insurance Company Group Membership Association Claims PO Box 30782 Tampa FL 33630-3782 (800) 792-9686 Dear Beneficiary: Please accept our condolences on your recent loss.
Please complete in blue or black ink only. Section A: Employee Information Last name First name M.I. Social Security no.
 Employee Enrollment Application For 2 50 Employee Small s Georgia You, the employee, must complete this application. You are solely responsible for its accuracy and completeness. To avoid the possibility
Employee Enrollment Application For 2 50 Employee Small s Georgia You, the employee, must complete this application. You are solely responsible for its accuracy and completeness. To avoid the possibility
Group Term Life Insurance for The Missouri Bar 10-year level premium
 Group Term Life Insurance for The Missouri Bar 10-year level premium For Missouri Bar members, their families and their employees About life insurance Life insurance provides basic protection for your
Group Term Life Insurance for The Missouri Bar 10-year level premium For Missouri Bar members, their families and their employees About life insurance Life insurance provides basic protection for your
Toll-free: Fax: Call toll-free Monday through Friday, 8 a.m. to 8 p.m. Eastern Time.
 For use with policies issued by the following Unum Group [ Unum ] subsidiaries: Unum Life Insurance Company of America Provident Life and Accident Insurance Company OUR COMMITMENT TO YOU You have our commitment
For use with policies issued by the following Unum Group [ Unum ] subsidiaries: Unum Life Insurance Company of America Provident Life and Accident Insurance Company OUR COMMITMENT TO YOU You have our commitment
CLAIM FORM. DATE OF BIRTH: 3. PATIENT'S NAME & ADDRESS- IF ADDRESS IS NEW, PLEASE CHECK BOX r PHONE: ( )
") PRIMERICA LIFE INSURANCE COMPANY as Administered by Senior Health Ins. Co. of Pennsylvania Home Office: Boston, MA P.O. Box 64913 St. Paul, MN 55164 Telephone: 1-877-451-5824 CLAIM FORM The patient or
PRIMERICA LIFE INSURANCE COMPANY as Administered by Senior Health Ins. Co. of Pennsylvania Home Office: Boston, MA P.O. Box 64913 St. Paul, MN 55164 Telephone: 1-877-451-5824 CLAIM FORM The patient or
The Prudential Insurance Company of America 751 Broad Street, Newark NJ 07102
 The Prudential Insurance Company of America 751 Broad Street, Newark NJ 0710 Control # 51540 Please print all answers using black ink. 1 Member Information Request for Term Life Coverage Form Return this
The Prudential Insurance Company of America 751 Broad Street, Newark NJ 0710 Control # 51540 Please print all answers using black ink. 1 Member Information Request for Term Life Coverage Form Return this
BENEFICIARY S STATEMENT Failure to complete all sections may result in a delay in processing of the claim.
 Post Office Box 84075 * Columbus, GA. 31993 Phone (800) 433-3036 * Fax (866) 849-2970 groupclaimfiling@aflac.com BENEFICIARY S STATEMENT Failure to complete all sections may result in a delay in processing
Post Office Box 84075 * Columbus, GA. 31993 Phone (800) 433-3036 * Fax (866) 849-2970 groupclaimfiling@aflac.com BENEFICIARY S STATEMENT Failure to complete all sections may result in a delay in processing
Last name First name MI. Apt / Suite / PO box number Gender m Female m Male Language of choice m English m Spanish City State Zip code County / Parish
 Large group employee enrollment form The offering company(ies) listed on the signature page, severally or collectively, as the content may require, are referred to in this application as Humana. Print
Large group employee enrollment form The offering company(ies) listed on the signature page, severally or collectively, as the content may require, are referred to in this application as Humana. Print
Voluntary Life Insurance
 Voluntary Life Insurance Benefit Highlights for CAJON VALLEY UNION SD What is voluntary life insurance? Voluntary life insurance is coverage that you pay for. Voluntary life insurance pays your beneficiary
Voluntary Life Insurance Benefit Highlights for CAJON VALLEY UNION SD What is voluntary life insurance? Voluntary life insurance is coverage that you pay for. Voluntary life insurance pays your beneficiary
SPECIAL INSTRUCTIONS
 GUL Proof of Death Send to: Guardian Group Universal Life Service Center Customer Service: 888-482-7302 Fax: 888-232-1683 P.O. Box 19005 Greenville, SC 29602-9005 SPECIAL INSTRUCTIONS Generally, the proofs
GUL Proof of Death Send to: Guardian Group Universal Life Service Center Customer Service: 888-482-7302 Fax: 888-232-1683 P.O. Box 19005 Greenville, SC 29602-9005 SPECIAL INSTRUCTIONS Generally, the proofs
Short Term Disability Claim Form
 Short Term Disability Claim Form Important notice to employee Please read carefully: You or someone acting on your behalf should complete Section 1 and then have your employer complete Section 2. Have
Short Term Disability Claim Form Important notice to employee Please read carefully: You or someone acting on your behalf should complete Section 1 and then have your employer complete Section 2. Have
Accident Benefits Claim Instructions
 Claim Instructions Your Accident Benefit Claim This packet contains the forms necessary to apply for. Every space on these forms should be filled in to avoid delay in processing your application. If a
Claim Instructions Your Accident Benefit Claim This packet contains the forms necessary to apply for. Every space on these forms should be filled in to avoid delay in processing your application. If a
Life Insurance/Disability Income EnroIIment Application
 Life Insurance/Disability Income EnroIIment Application Social Security Number: PERSONAL INFORMATION Name of employee (last, first, middle initial) Address (number and street) Telephone number (with area
Life Insurance/Disability Income EnroIIment Application Social Security Number: PERSONAL INFORMATION Name of employee (last, first, middle initial) Address (number and street) Telephone number (with area
Request for Group Insurance From: New York Life Insurance Company 51 Madison Avenue New York, NY 10010
 1200 E. Glen Ave., Peoria Heights, IL 61616-5348 Request for Group Insurance From: New York Life Insurance Company 51 Madison Avenue New York, NY 10010 Plan Administrator: 1200 E. Glen Ave., Peoria Heights,
1200 E. Glen Ave., Peoria Heights, IL 61616-5348 Request for Group Insurance From: New York Life Insurance Company 51 Madison Avenue New York, NY 10010 Plan Administrator: 1200 E. Glen Ave., Peoria Heights,
CITY OF SANTA MONICA AFFIDAVIT OF DOMESTIC PARTNERSHIP
 CITY OF SANTA MONICA AFFIDAVIT OF DOMESTIC PARTNERSHIP I, (herein referred to as the Employee), and (herein referred to as the Partner) hereby declare under penalty of perjury that we are domestic partners
CITY OF SANTA MONICA AFFIDAVIT OF DOMESTIC PARTNERSHIP I, (herein referred to as the Employee), and (herein referred to as the Partner) hereby declare under penalty of perjury that we are domestic partners
key* E V11.0
 key* 00434441 0004 E V11.0 The Guardian Life Insurance Company of America The Guardian Life Insurance company of America underwrites group term life, accidental death and dismemberment, Short term disability,
key* 00434441 0004 E V11.0 The Guardian Life Insurance Company of America The Guardian Life Insurance company of America underwrites group term life, accidental death and dismemberment, Short term disability,
Medical Mutual of Ohio Employee Application/Change Form For Individuals in Groups with 20+ Eligible Employees
 INSURANCE WAIVER Medical Mutual of Ohio Employee Application/Change Form For Individuals in Groups with 20+ Eligible Employees COMPLETE THE WAIVER SECTION BELOW ONLY if you do not want any coverage or
INSURANCE WAIVER Medical Mutual of Ohio Employee Application/Change Form For Individuals in Groups with 20+ Eligible Employees COMPLETE THE WAIVER SECTION BELOW ONLY if you do not want any coverage or
Group Long Term Disability Claim Filing Instructions
 Group Long Term Disability Claim Filing Instructions Have you 1. Completed the Employee s Statement in full? 2. Had the physician treating you complete the Attending Physician s Statement, and had it returned
Group Long Term Disability Claim Filing Instructions Have you 1. Completed the Employee s Statement in full? 2. Had the physician treating you complete the Attending Physician s Statement, and had it returned
Life Claim Statement Employee/Claimant
 Life Claim Statement Employee/Claimant If you live in the state of Arizona, the following statement applies to you: For your protection Arizona Law requires the following statement to appear on this form.
Life Claim Statement Employee/Claimant If you live in the state of Arizona, the following statement applies to you: For your protection Arizona Law requires the following statement to appear on this form.
Step by Step Guide to Anthem Blue Cross Enrollment Application. FOR Adding/Dropping Dependents for Anthem Medical
 Step by Step Guide to Anthem Blue Cross Enrollment Application FOR ing/dropping Dependents for Anthem Medical For members of the California Association of REALTORS Use this form to: or drop dependents
Step by Step Guide to Anthem Blue Cross Enrollment Application FOR ing/dropping Dependents for Anthem Medical For members of the California Association of REALTORS Use this form to: or drop dependents
Hospital Indemnity Insurance
 Hospital Indemnity Insurance Instructions for filing a Claim Follow the instructions shown below in completing/providing documentation needed to file a claim for your hospital indemnity benefits. 1. Complete
Hospital Indemnity Insurance Instructions for filing a Claim Follow the instructions shown below in completing/providing documentation needed to file a claim for your hospital indemnity benefits. 1. Complete
New York Life Insurance Company
 New York Life Insurance Company PO Box 30713 Tampa FL 33630-3713 Dear Beneficiary: Please accept our condolences on your recent loss. We understand this is a difficult time, and we hope that we can alleviate
New York Life Insurance Company PO Box 30713 Tampa FL 33630-3713 Dear Beneficiary: Please accept our condolences on your recent loss. We understand this is a difficult time, and we hope that we can alleviate
Group Long Term Disability
 Group Long Term Disability Life Insurance Company of rth America Connecticut General Life Insurance Company Cigna Life Insurance Company of New York Great-West Healthcare Administered by Cigna Group Long
Group Long Term Disability Life Insurance Company of rth America Connecticut General Life Insurance Company Cigna Life Insurance Company of New York Great-West Healthcare Administered by Cigna Group Long
INSURED STATEMENT OF CLAIM
 INSURED STATEMENT OF CLAIM Last Name First MI Policy Number Address Apt No. City State Zip Telephone No. - - Home Cell Work E-Mail Address: Birth Date / / Soc. Sec. No. Gender: M F Height Weight Spouse
INSURED STATEMENT OF CLAIM Last Name First MI Policy Number Address Apt No. City State Zip Telephone No. - - Home Cell Work E-Mail Address: Birth Date / / Soc. Sec. No. Gender: M F Height Weight Spouse
*87101* Group Insurance. Group Life Insurance Claim Form (Use for employee/member and dependent death claims)
") Group Life Insurance Claim Form (Use for employee/member and dependent death claims) How to complete and submit a Group Life Insurance Claim Form Group Insurance Please send the completed form and all
Group Life Insurance Claim Form (Use for employee/member and dependent death claims) How to complete and submit a Group Life Insurance Claim Form Group Insurance Please send the completed form and all
Proof of Loss of Limb(s) or Sight Statements
 or Sight Statements") P.O. Box 7948 Lake Forest, IL 60045-7948 Phone 1-800-307-3929 Fax (847)615-3866 Proof of Loss of Limb(s) or Sight Statements TICE OF CLAIM Instructions A. Employer 1. Complete Part III Statement of Employer.
P.O. Box 7948 Lake Forest, IL 60045-7948 Phone 1-800-307-3929 Fax (847)615-3866 Proof of Loss of Limb(s) or Sight Statements TICE OF CLAIM Instructions A. Employer 1. Complete Part III Statement of Employer.
Disability Benefits Claim
 This form must be completed by the Attending Physician & the Policyholder and be returned promptly for consideration of benefits. All questions and sections on this form must be answered in full. Incomplete
This form must be completed by the Attending Physician & the Policyholder and be returned promptly for consideration of benefits. All questions and sections on this form must be answered in full. Incomplete
NATIONAL SLOVAK SOCIETY OF THE UNITED STATES OF AMERICA
 NATIONAL SLOVAK SOCIETY OF THE UNITED STATES OF AMERICA A Fraternal Benefit Society Application for Life Insurance Assembly/Circle #: Certificate #: 1. Proposed Insured: Male Female Height Weight Phone
NATIONAL SLOVAK SOCIETY OF THE UNITED STATES OF AMERICA A Fraternal Benefit Society Application for Life Insurance Assembly/Circle #: Certificate #: 1. Proposed Insured: Male Female Height Weight Phone
Standard Insurance Company. Individual Client Services PO Box 711 Portland OR Policy Change Form and Application Supplement A
 Individual Client Services PO Box 711 Portland OR 97207 Policy Change Form and Application Supplement A Disclosure Notice - Information Practices Standard Insurance Company (Standard) is committed to
Individual Client Services PO Box 711 Portland OR 97207 Policy Change Form and Application Supplement A Disclosure Notice - Information Practices Standard Insurance Company (Standard) is committed to
CLAIM FORM FOR LIFE INSURANCE PROCEEDS
 Lunar Financial Group Support@LunarFinancialGroupCom Dear Beneficiary: Please accept our condolences on your recent loss. We understand this is a difficult time, and we hope that we can alleviate any concerns
Lunar Financial Group Support@LunarFinancialGroupCom Dear Beneficiary: Please accept our condolences on your recent loss. We understand this is a difficult time, and we hope that we can alleviate any concerns
Voluntary Benefits Disability Income Claim Form Claimant Initial Statement of Disability
 Amalgamated Life Insurance Company Disability Benefits Claim Department P.O. Box 5453, White Plains, NY 10602-5453 Toll-Free: 1-866-975-4089 / Fax: 1-914-367-4114 Voluntary Benefits Disability Income Claim
Amalgamated Life Insurance Company Disability Benefits Claim Department P.O. Box 5453, White Plains, NY 10602-5453 Toll-Free: 1-866-975-4089 / Fax: 1-914-367-4114 Voluntary Benefits Disability Income Claim
3. Remarks. 4. Remarks. GL Ed. 07/2016 Page 1 of 5
 PART 1 TO BE COMPLETED BY THE EMPLOYEE OR PARTICIPANT Please complete Section I and then complete Section II, III, or IV, whichever is applicable to the dependent named in Section 1. The Physician s Statement
PART 1 TO BE COMPLETED BY THE EMPLOYEE OR PARTICIPANT Please complete Section I and then complete Section II, III, or IV, whichever is applicable to the dependent named in Section 1. The Physician s Statement
Short Term Disability Claim Form
 Life and Disability products underwritten by. ANTHEM is a registered trademark of Anthem Insurance Companies, Inc. 63823MUMENLIC Rev. 3/17 1 of 6 1928530 63823MUMENLIC Short Term Disability Claim Packet
Life and Disability products underwritten by. ANTHEM is a registered trademark of Anthem Insurance Companies, Inc. 63823MUMENLIC Rev. 3/17 1 of 6 1928530 63823MUMENLIC Short Term Disability Claim Packet
Thank you. Should you have any questions, please call us at (800)
") Dear Policyholder: Please complete and sign the attached claim form. Additionally, the following items are needed in order to process your Medical/Dental claim in the most efficient and expedient way possible.
Dear Policyholder: Please complete and sign the attached claim form. Additionally, the following items are needed in order to process your Medical/Dental claim in the most efficient and expedient way possible.
Instructions for Completing this Long Term Care Claim Form
 A Brief Overview of a Long Term Care Policy Claim eligibility under a Long Term Care insurance policy is based on a loss of Activities of Daily Living (ADLs) or the presence of a Cognitive Impairment which
A Brief Overview of a Long Term Care Policy Claim eligibility under a Long Term Care insurance policy is based on a loss of Activities of Daily Living (ADLs) or the presence of a Cognitive Impairment which
AIG Benefit Solutions
 PLEASE ANSWER ALL QUESTIONS FULLY AS THIS WILL HELP EXPEDITE THE EVALUATION OF THIS CLAIM. POLICYHOLDER S STATEMENT Policy Number: 3803Z1 Name of Insured (Policyholder) Address (Street, City, State, Zip
PLEASE ANSWER ALL QUESTIONS FULLY AS THIS WILL HELP EXPEDITE THE EVALUATION OF THIS CLAIM. POLICYHOLDER S STATEMENT Policy Number: 3803Z1 Name of Insured (Policyholder) Address (Street, City, State, Zip
American Heritage Life Insurance Company 1776 American Heritage Life Drive Jacksonville, Florida
 CLAIM FORM If you have any questions regarding benefits available, or how to file your claim, or if you would like to appeal any determination, please contact our customer service department at 1-800-348-4489
CLAIM FORM If you have any questions regarding benefits available, or how to file your claim, or if you would like to appeal any determination, please contact our customer service department at 1-800-348-4489
Please answer these brief questions. Member Spouse 1. Has the applicant/member or spouse, if applying, ever had, been diagnosed with, or been treated
 To Apply: Send this completed form with your premium check payable to: ADMINISTRATOR NCRA GROUP INSURANCE PROGRAM P.O. Box 10374 Des Moines, IA 50306-8812 QUESTIONS? 1-800-503-9230 customerservice.service@mercer.com
To Apply: Send this completed form with your premium check payable to: ADMINISTRATOR NCRA GROUP INSURANCE PROGRAM P.O. Box 10374 Des Moines, IA 50306-8812 QUESTIONS? 1-800-503-9230 customerservice.service@mercer.com
DAYTIME PHONE: EMPLOYEE I.D.: HIRE DATE:
 Mercer Voluntary Benefits Duke University and Health System Ref #58215 Metropolitan Life Insurance Company, New York, NY SUPPLEMENTAL LIFE INSURANCE ENROLLMENT FORM 078428010103 EMPLOYEE NAME: Last First
Mercer Voluntary Benefits Duke University and Health System Ref #58215 Metropolitan Life Insurance Company, New York, NY SUPPLEMENTAL LIFE INSURANCE ENROLLMENT FORM 078428010103 EMPLOYEE NAME: Last First
ACCIDENTAL DEATH WHOLE LIFE PROTECTOR
 ACCIDENTAL DEATH WHOLE LIFE PROTECTOR Regular Mail: United Home Life Insurance Company P.O. Box 7192 Indianapolis, IN 46207-7192 FAX Number: 317-692-7711 Telephone: 800-428-3001 # pages including cover
ACCIDENTAL DEATH WHOLE LIFE PROTECTOR Regular Mail: United Home Life Insurance Company P.O. Box 7192 Indianapolis, IN 46207-7192 FAX Number: 317-692-7711 Telephone: 800-428-3001 # pages including cover
Disability Insurance Claim Packet Instructions
 Claim Packet Instructions Your Disability Benefit Claim This packet contains the forms necessary to apply for disability benefits. It also addresses common questions about Disability claims. Please save
Claim Packet Instructions Your Disability Benefit Claim This packet contains the forms necessary to apply for disability benefits. It also addresses common questions about Disability claims. Please save
Please answer these brief questions. Member Spouse 1. Has the applicant/member or spouse, if applying, ever had, been diagnosed with, or been treated
 To Apply: Send this completed form with your premium check payable to: ADMINISTRATOR SPJ GROUP INSURANCE PROGRAM P.O. Box 10374 Des Moines, IA 50306-8812 QUESTIONS? 1-800-503-9230 customerservice.service@mercer.com
To Apply: Send this completed form with your premium check payable to: ADMINISTRATOR SPJ GROUP INSURANCE PROGRAM P.O. Box 10374 Des Moines, IA 50306-8812 QUESTIONS? 1-800-503-9230 customerservice.service@mercer.com
Section VII is answered Number of 2. Complete all appropriate items, sign and date.
 Group Hospitalization and Medical Services, Inc. 840 First Street, NE Washington, DC 20065 Enrollment Form (Maryland Small Groups) THIS IS NOT AN APPLICATION FOR INSURANCE HOW TO COMPLETE THIS FORM: 1.
Group Hospitalization and Medical Services, Inc. 840 First Street, NE Washington, DC 20065 Enrollment Form (Maryland Small Groups) THIS IS NOT AN APPLICATION FOR INSURANCE HOW TO COMPLETE THIS FORM: 1.
LOYAL AMERICAN LIFE INSURANCE COMPANY PO BOX 1604, DUNCAN, OKLAHOMA, Phone (800)
") INSTRUCTIONS FOR FILING A MEDICAL CLAIM CANCER TREATMENT The forms must be completed by the claimant. All questions on the forms must be answered in full. Incomplete or illegible answers may result in
INSTRUCTIONS FOR FILING A MEDICAL CLAIM CANCER TREATMENT The forms must be completed by the claimant. All questions on the forms must be answered in full. Incomplete or illegible answers may result in
Sun Life Assurance Company of Canada Group Enrollment form
 Sun Life Assurance Company of Canada Group Enrollment form Complete all sections of the Group Enrollment Form. Make sure you complete and sign the form during the enrollment period or within 31 days of
Sun Life Assurance Company of Canada Group Enrollment form Complete all sections of the Group Enrollment Form. Make sure you complete and sign the form during the enrollment period or within 31 days of
Short Term Disability Claim Form
 Short Term Disability Claim Form Important notice to employee Please read carefully: You or someone acting on your behalf should complete Section 1 and then have your employer complete Section 2. Have
Short Term Disability Claim Form Important notice to employee Please read carefully: You or someone acting on your behalf should complete Section 1 and then have your employer complete Section 2. Have
INSURED STATEMENT OF CLAIM
 INSURED STATEMENT OF CLAIM Last Name First MI Address Apt No. City State Zip Telephone No. - - Home Cell Work E-Mail Address: Birth Date / / Soc. Sec. No. Policy Number Gender: M F Height Weight Spouse
INSURED STATEMENT OF CLAIM Last Name First MI Address Apt No. City State Zip Telephone No. - - Home Cell Work E-Mail Address: Birth Date / / Soc. Sec. No. Policy Number Gender: M F Height Weight Spouse
Dental / Vision / Chiropractic / Life Enrollment Form
 721 South Parker, Suite 200, Orange, CA 92868 Phone: (866) 412-9279 Fax (866) 412-9280 www.choicebuilder.com Dental / / Chiropractic / Life Enrollment Form Form must be Completed in Full, Signed and Dated
721 South Parker, Suite 200, Orange, CA 92868 Phone: (866) 412-9279 Fax (866) 412-9280 www.choicebuilder.com Dental / / Chiropractic / Life Enrollment Form Form must be Completed in Full, Signed and Dated
Short Term Disability Claim Form
 Short Term Disability Claim Form Important notice to employee Please read carefully: You or someone acting on your behalf should complete Section 1 and then have your employer complete Section 2. Have
Short Term Disability Claim Form Important notice to employee Please read carefully: You or someone acting on your behalf should complete Section 1 and then have your employer complete Section 2. Have
Please send your completed form to: Claims Department P.O. Box Atlanta, Georgia 30342
 ** THE ATTACHED FORM IS TO BE USED IN FILING FOR DISABILITY BENEFITS ** PLEASE FOLLOW THESE INSTRUCTIONS CAREFULLY 1) The Loan Information Statement at the top of the claim form should be completed by
** THE ATTACHED FORM IS TO BE USED IN FILING FOR DISABILITY BENEFITS ** PLEASE FOLLOW THESE INSTRUCTIONS CAREFULLY 1) The Loan Information Statement at the top of the claim form should be completed by
Toll-free: Fax: Call toll-free Monday through Friday, 8 a.m. to 8 p.m. Eastern Time.
 For use with policies issued by the following Unum Group [ Unum ] subsidiaries: Unum Life Insurance Company of America Provident Life and Accident Insurance Company OUR COMMITMENT TO YOU We understand
For use with policies issued by the following Unum Group [ Unum ] subsidiaries: Unum Life Insurance Company of America Provident Life and Accident Insurance Company OUR COMMITMENT TO YOU We understand
Salary Reduction Contributions Enrollment Form
 Salary Reduction Contributions Enrollment Form Employee Information Employer Name Employee Name (Last, First, Middle) Employee Street Address Department - - Social Security Number / to / (mm/dd) Plan Year
Salary Reduction Contributions Enrollment Form Employee Information Employer Name Employee Name (Last, First, Middle) Employee Street Address Department - - Social Security Number / to / (mm/dd) Plan Year
GROUP CATASTROPHE MAJOR MEDICAL PLAN
 GROUP CATASTROPHE MAJOR MEDICAL PLAN Sponsored by NYSUT Member Benefits Catastrophe Major Medical (CMM) Insurance Trust PLEASE NOTE USE THIS CLAIM FORM FOR BENEFIT PERIOD START DATES PRIOR TO JANUARY 1,
GROUP CATASTROPHE MAJOR MEDICAL PLAN Sponsored by NYSUT Member Benefits Catastrophe Major Medical (CMM) Insurance Trust PLEASE NOTE USE THIS CLAIM FORM FOR BENEFIT PERIOD START DATES PRIOR TO JANUARY 1,
The Prudential Insurance Company of America
 The Prudential Insurance Company of America 751 Broad Street, Newark NJ 0710 State Bar of Texas 47080 Please print all answers using black ink. Request for LTD Coverage Form Return this completed form
The Prudential Insurance Company of America 751 Broad Street, Newark NJ 0710 State Bar of Texas 47080 Please print all answers using black ink. Request for LTD Coverage Form Return this completed form
MARITAL STATUS Single Married Divorced Widowed COVERAGE LEVEL MEDICAL POS PLAN HDHP PLAN SINGLE EMPLOYEE + SPOUSE EMPLOYEE + CHILD FAMILY DECLINE
 COMPANY NAME: Braun Northwest, Inc. GROUP #: 15972 THIS FORM IS TO BE COMPLETED FOR NEW ENROLLMENTS AND CHANGES PLEASE PRINT CLEARLY AND COMPLETE THE ENTIRE FORM (ALL INFORMATION MUST BE COMPLETED OR ENROLLMENT
COMPANY NAME: Braun Northwest, Inc. GROUP #: 15972 THIS FORM IS TO BE COMPLETED FOR NEW ENROLLMENTS AND CHANGES PLEASE PRINT CLEARLY AND COMPLETE THE ENTIRE FORM (ALL INFORMATION MUST BE COMPLETED OR ENROLLMENT
Date employed (mo/day/yr)
") Minnesota Life Insurance Company - A Securian Company 600 Congress Avenue Suite 2160 Austin, T 78701 For claim information: FC 22 abc Please return this completed form to Minnesota Life at the above address.
Minnesota Life Insurance Company - A Securian Company 600 Congress Avenue Suite 2160 Austin, T 78701 For claim information: FC 22 abc Please return this completed form to Minnesota Life at the above address.
PUYALLUP SCHOOL DISTRICT. Domestic Partner Health Coverage
 PUYALLUP SCHOOL DISTRICT Domestic Partner Health Coverage Instructions: To cover your domestic partner and/or your partner s children under your District dental, vision or health plan please review this
PUYALLUP SCHOOL DISTRICT Domestic Partner Health Coverage Instructions: To cover your domestic partner and/or your partner s children under your District dental, vision or health plan please review this
INSTRUCTIONS FOR FILING A CLAIM LIMITED BENEFIT CANCER EXPENSE POLICY
 INSTRUCTIONS FOR FILING A CLAIM LIMITED BENEFIT CANCER EXPENSE POLICY The forms must be completed by the claimant. All questions on the forms must be answered in full. Incomplete or illegible answers may
INSTRUCTIONS FOR FILING A CLAIM LIMITED BENEFIT CANCER EXPENSE POLICY The forms must be completed by the claimant. All questions on the forms must be answered in full. Incomplete or illegible answers may
Statement of Long Term Disability
 Claim Filing Instructions This Statement of Long Term Disability (LTD) includes the forms required to apply for LTD benefits. If a form is received incomplete, unsigned or undated, it will be returned
Claim Filing Instructions This Statement of Long Term Disability (LTD) includes the forms required to apply for LTD benefits. If a form is received incomplete, unsigned or undated, it will be returned
Guide to Making your Claim
 U.S. Long-Term Care Claims Operations Guide to Making your Claim What you ll find in this packet Initial Claim Form: Use this form to begin your claim. Medical Authorization: This form allows us to get
U.S. Long-Term Care Claims Operations Guide to Making your Claim What you ll find in this packet Initial Claim Form: Use this form to begin your claim. Medical Authorization: This form allows us to get
*10001* Group Disability Insurance. Disability Claim Instructions. Instructions to File a Claim for Disability Benefits
 Disability Claim Instructions Instructions to File a Claim for Disability Benefits 1. Notify your employer of your absence, that you will be filing a claim and request they provide Prudential with their
Disability Claim Instructions Instructions to File a Claim for Disability Benefits 1. Notify your employer of your absence, that you will be filing a claim and request they provide Prudential with their
For faster claim payment* please submit your claim online at
 Claims Made Easy For faster claim payment* please submit your claim online at www.combinedinsurance.com/claims FILING A CLAIM BY MAIL 1. Download the claim form 2. Print all six pages of the claim form
Claims Made Easy For faster claim payment* please submit your claim online at www.combinedinsurance.com/claims FILING A CLAIM BY MAIL 1. Download the claim form 2. Print all six pages of the claim form
New Business New Hire New Renewal New COBRA Qualifying/Triggering Event. Address. Spouse/Domestic Partner Child 1 Child 2 Child 3
 721 South Parker, Suite 200, Orange, CA 92868 (800) 558-8003 www.calchoice.com / / Life / Enrollment Application Select one A Personal Information Company Name COMPLETE WAIVER SECTION ON PAGE 4 IF YOU
721 South Parker, Suite 200, Orange, CA 92868 (800) 558-8003 www.calchoice.com / / Life / Enrollment Application Select one A Personal Information Company Name COMPLETE WAIVER SECTION ON PAGE 4 IF YOU
CHUBB WORKPLACE BENEFITS A BUSINESS UNIT OF COMBINED INSURANCE COMPANY OF AMERICA, A CHUBB COMPANY INSTRUCTIONS FOR FILING CLAIMS
 CHUBB WORKPLACE BENEFITS A BUSINESS UNIT OF COMBINED INSURANCE COMPANY OF AMERICA, A CHUBB COMPANY INSTRUCTIONS FOR FILING CLAIMS GETTING STARTED Follow the Claimant Instructions below to complete the
CHUBB WORKPLACE BENEFITS A BUSINESS UNIT OF COMBINED INSURANCE COMPANY OF AMERICA, A CHUBB COMPANY INSTRUCTIONS FOR FILING CLAIMS GETTING STARTED Follow the Claimant Instructions below to complete the
Employee Enrollment Application
 Employee Enrollment Application Group Size 51+ Eligible Employees - Medically Underwritten Your Anthem enrollment application is inside. It is essential that you read it carefully and complete all the
Employee Enrollment Application Group Size 51+ Eligible Employees - Medically Underwritten Your Anthem enrollment application is inside. It is essential that you read it carefully and complete all the
ELA Settlement Services, LLC Data Collection Form
 ELA Settlement Services, LLC Data Collection Form Complete the following forms, and mail, fax or email with any relevant documents to: ELA Settlement Services 1435 Morris Ave. P.O. Box 3137 Union, NJ 07083
ELA Settlement Services, LLC Data Collection Form Complete the following forms, and mail, fax or email with any relevant documents to: ELA Settlement Services 1435 Morris Ave. P.O. Box 3137 Union, NJ 07083
Thank you. Should you have any questions, please call us at (800)
") Dear Policyholder: Please complete and sign the attached claim form. Additionally, the following items are needed in order to process your Trip Cancellation claim in the most efficient and expedient way
Dear Policyholder: Please complete and sign the attached claim form. Additionally, the following items are needed in order to process your Trip Cancellation claim in the most efficient and expedient way
The Long Term Disability Benefits application includes claim forms and an Authorization.
 Long Term Disability Benefits Claim Packet Instructions Your Disability Benefit Claim This packet contains the forms necessary to apply for Long Term Disability benefits. Every space on these forms should
Long Term Disability Benefits Claim Packet Instructions Your Disability Benefit Claim This packet contains the forms necessary to apply for Long Term Disability benefits. Every space on these forms should
Disability Insurance Claim Packet Instructions. Your Disability Benefit Claim. The Standard Benefit Administrators. How To Apply For Benefits
 Claim Packet Instructions Your Disability Benefit Claim This packet contains the forms necessary to apply for disability benefits. It also addresses common questions about Disability claims. Please save
Claim Packet Instructions Your Disability Benefit Claim This packet contains the forms necessary to apply for disability benefits. It also addresses common questions about Disability claims. Please save
Name (First, Middle, Last) Social Security #
 Social Security #") ENROLLMENT CHANGE FORM Metropolitan Life Insurance Company, New York, NY GROUP CUSTOMER INFORMATION (To be Completed by the Recordkeeper) Name of Group Customer/Employer Group Customer # 143103 Report
ENROLLMENT CHANGE FORM Metropolitan Life Insurance Company, New York, NY GROUP CUSTOMER INFORMATION (To be Completed by the Recordkeeper) Name of Group Customer/Employer Group Customer # 143103 Report
GROUP DISABILITY CLAIM APPLICATION
 GROUP DISABILITY CLAIM APPLICATION SM Short Term Disability (STD) SEND TO: P.O. BOX 9461 PORTLAND, ME 04104-5056 TEL: (888) 234-2641 FAX: (800) 293-4781 Long Term Disability (LTD) SEND TO: P.O. BOX 9461
GROUP DISABILITY CLAIM APPLICATION SM Short Term Disability (STD) SEND TO: P.O. BOX 9461 PORTLAND, ME 04104-5056 TEL: (888) 234-2641 FAX: (800) 293-4781 Long Term Disability (LTD) SEND TO: P.O. BOX 9461
Insurance Claim Filing Instructions
 Insurance Claim Filing Instructions PROOF OF LOSS CONSISTS OF THE FOLLOWING: 1. A completed and signed Claim form and Attending Physician s Statement. 2. For Hospital/Intensive Care/Hospital Services Coverage
Insurance Claim Filing Instructions PROOF OF LOSS CONSISTS OF THE FOLLOWING: 1. A completed and signed Claim form and Attending Physician s Statement. 2. For Hospital/Intensive Care/Hospital Services Coverage
TRUSTMARK INSURANCE COMPANY
 TRUSTMARK INSURANCE COMPANY CRITICAL ILLNESS/CANCER CLAIM FORM Attn: Dept. P383 PO BOX 7937 LAKE FOREST IL 60045-7937 1-800-918-8877 FAX 1-847-615-3128 www.trustmarkins.com/customersolutions This form
TRUSTMARK INSURANCE COMPANY CRITICAL ILLNESS/CANCER CLAIM FORM Attn: Dept. P383 PO BOX 7937 LAKE FOREST IL 60045-7937 1-800-918-8877 FAX 1-847-615-3128 www.trustmarkins.com/customersolutions This form
Cancer Lump-Sum Benefit Claim Form
 Cancer Lump-Sum Benefit Claim Form Please check your policy for the benefit eligibility or call Sterling Customer Service at 1-866-459-1755 for help. Please use blue or black ink only and print legibly
Cancer Lump-Sum Benefit Claim Form Please check your policy for the benefit eligibility or call Sterling Customer Service at 1-866-459-1755 for help. Please use blue or black ink only and print legibly
Medico Dental Insurance Portfolio
 INSURANCE COMPANY Medico Dental Insurance Portfolio n Dental n D.V.H. $1,000 n Dental Plus n D.V.H. $1,500 APPLICATION BOOKLET PRODUCER INSTRUCTIONS Please complete the following: Application for Dental
INSURANCE COMPANY Medico Dental Insurance Portfolio n Dental n D.V.H. $1,000 n Dental Plus n D.V.H. $1,500 APPLICATION BOOKLET PRODUCER INSTRUCTIONS Please complete the following: Application for Dental