Health Care Plan Open Enrollment
|
|
|
- Jessie Cameron
- 6 years ago
- Views:
Transcription
1 Health Care Plan Open Enrollment


2 Agenda ACA Update Benefits update Health Care plan review Tips to save health care dollars FSA Open Enrollment Dental Open Enrollment Vision Open Enrollment
3 Employee Benefit Plan Updates OWU will be renewing with Anthem Deductibles, coinsurance, and out-ofpocket maximums will remain the same Medical and Rx co-pays remain the same New $0 copay for Anthem Live Health Online
4 Employee Benefit Plan Updates OWU will continue to offer The OWU Wellness Program to all employees. Opportunity to reduce your health care premiums or earn cash incentive for non-medical plan participants!
5 Individual Obligations If person chooses not to have insurance they will owe a tax: * Greater of 2.5% of income or $695, indexed and later * Per adult; children 50%; family max of 3x individual
6 User Inputs for Plan Parameters Use Integrated Medical and Drug Deductible? Apply Inpatient Copay per Day? HSA/HRA Options HSA/HRA Employer Contribution? Narrow Network Options Blended Network/POS Plan? Apply Skilled Nursing Facility Copay per Day? 1st Tier Utilization: Annual Contribution Amount: Use Separate OOP Maximum for Medical and Drug Spending? 2nd Tier Utilization: Indicate if Plan Meets CSR Standard? Desired Metal Tier Tier 1 Plan Benefit Design Tier 2 Plan Benefit Design Medical Drug Combined Medical Drug Combined Deductible ($) $1, $50.00 Coinsurance (%, Insurer's Cost Share) 90.00% % OOP Maximum ($) OOP Maximum if Separate ($) $3, Click Here for Important Instructions Tier 1 Tier 2 Tier 1 Tier 2 Type of Benefit Subject to Deductible? Subject to Coinsurance? Coinsurance, if different Copay, if separate Medical All All Emergency Room Services $ All Inpatient Hospital Services (inc. MHSA) Primary Care Visit to Treat an Injury or Illness (exc. Preventive, and X- rays) $30.00 Specialist Visit $60.00 Mental/Behavioral Health and Substance Abuse Disorder Outpatient Services Imaging (CT/PET Scans, MRIs) Rehabilitative Speech Therapy Subject to Deductible? Subject to Coinsurance? Coinsurance, if different Rehabilitative Occupational and Rehabilitative Physical Therapy Preventive Care/Screening/Immunization 100% $ % $0.00 Laboratory Outpatient and Professional Services X-rays and Diagnostic Imaging Skilled Nursing Facility Outpatient Facility Fee (e.g., Ambulatory Surgery Center) All All Copay, if separate Copay applies only after deductible? All All Outpatient Surgery Physician/Surgical Services Drugs All All Generics $10.00 Preferred Brand Drugs $35.00 Non-Preferred Brand Drugs $70.00 Specialty Drugs (i.e. high-cost) 25% Options for Additional Benefit Design Limits: Set a Maximum on Specialty Rx Coinsurance Payments? Specialty Rx Coinsurance Maximum: $250 Set a Maximum Number of Days for Charging an IP Copay? # Days (1-10): Begin Primary Care Cost-Sharing After a Set Number of Visits? # Visits (1-10): Begin Primary Care Deductible/Coinsurance After a Set Number of Copays? # Copays (1-10): Output Calculate Status/Error Messages: Calculation Successful. Actuarial Value: 80.40% Metal Tier: Gold All All All All
7 OWU Contribution Options < $35,999 EE/Count Current/ Month Renewal/ Month EE only 51 $42.00 $46.00 EE + SP 15 $ $ EE + Children 3 $ $ EE + Family 13 $ $ $36,000 - $59,999 $60,000 - $89,999 > $90,000 EE only 55 $71.00 $78.00 EE + SP 22 $ $ EE + Children 10 $ $ EE + Family 24 $ $ EE only 48 $99.00 $ EE + SP 8 $ $ EE + Children 9 $ $ EE + Family 48 $ $ EE only 20 $ $ EE + SP 15 $ $ EE + Children 3 $ $ EE + Family 5 $ $589.00
8 How Does OWU Compare? EMPLOYEE CONTRIBUTIONS < $35,999 Ohio Wesleyan University Industry EE Size Survey Benchmarks Client National Regional State Group Category Number of Health Plans Reported 4 7,993 2, Employee Share of Premiums Monthly Employee Premium Share ($) Single $46 $144 $139 $140 $115 $130 EE+1 EE+CH $177 $410 $370 $302 $364 $346 EE+SP $197 $513 $447 $369 $444 $410 Family $312 $761 $652 $533 $680 $589 Monthly Employee Premium Share (%) Single 7.1% 28.8% 27.4% 28.5% 20.8% 23.4% EE+1 EE+CH 14.4% 50.1% 58.2% 35.4% 37.1% 36.0% EE+SP 14.5% 47.4% 41.2% 36.0% 39.4% 37.3% Family 16.4% 51.6% 43.3% 36.9% 44.9% 39.0%
9 How Does OWU Compare? EMPLOYEE CONTRIBUTIONS $36,000 - $59,999 Ohio Wesleyan University Industry EE Size Survey Benchmarks Client National Regional State Group Category Number of Health Plans Reported 4 7,993 2, Employee Share of Premiums Monthly Employee Premium Share ($) Single $78 $144 $139 $140 $115 $130 EE+1 EE+CH $236 $410 $370 $302 $364 $346 EE+SP $262 $513 $447 $369 $444 $410 Family $405 $761 $652 $533 $680 $589 Monthly Employee Premium Share (%) Single 12.0% 28.8% 27.4% 28.5% 20.8% 23.4% EE+1 EE+CH 19.3% 50.1% 58.2% 35.4% 37.1% 36.0% EE+SP 19.3% 47.4% 41.2% 36.0% 39.4% 37.3% Family 21.2% 51.6% 43.3% 36.9% 44.9% 39.0%
10 How Does OWU Compare? EMPLOYEE CONTRIBUTIONS $60,000 - $89,9999 Ohio Wesleyan University Industry EE Size Survey Benchmarks Client National Regional State Group Category Number of Health Plans Reported 4 7,993 2, Employee Share of Premiums Monthly Employee Premium Share ($) Single $108 $144 $139 $140 $115 $130 EE+1 EE+CH $295 $410 $370 $302 $364 $346 EE+SP $327 $513 $447 $369 $444 $410 Family $497 $761 $652 $533 $680 $589 Monthly Employee Premium Share (%) Single 16.8% 28.8% 27.4% 28.5% 20.8% 23.4% EE+1 EE+CH 24.1% 50.1% 58.2% 35.4% 37.1% 36.0% EE+SP 24.1% 47.4% 41.2% 36.0% 39.4% 37.3% Family 26.1% 51.6% 43.3% 36.9% 44.9% 39.0%
11 How Does OWU Compare? EMPLOYEE CONTRIBUTIONS $90,000 + Ohio Wesleyan University Industry EE Size Survey Benchmarks Client National Regional State Group Category Number of Health Plans Reported 4 7,993 2, Employee Share of Premiums Monthly Employee Premium Share ($) Single $139 $144 $139 $140 $115 $130 EE+1 EE+CH $355 $410 $370 $302 $364 $346 EE+SP $392 $513 $447 $369 $444 $410 Family $589 $761 $652 $533 $680 $589 Monthly Employee Premium Share (%) Single 21.5% 28.8% 27.4% 28.5% 20.8% 23.4% EE+1 EE+CH 28.9% 50.1% 58.2% 35.4% 37.1% 36.0% EE+SP 28.9% 47.4% 41.2% 36.0% 39.4% 37.3% Family 30.1% 51.6% 43.3% 36.9% 44.9% 39.0%
12 How Does OWU Compare? PLAN DESIGN Ohio Wesleyan University Survey Benchmarks Client National Regional State Industry Group EE Size Category Number of Health Plans Reported 4 7,993 2, CoPays Primary Care Physician CoPay $30 $25 $25 $25 $25 $25 Specialty Care Physician CoPay $60 $40 $40 $50 $35 $30 Urgent Care CoPay $75 $50 $60 $75 $50 $40 Emergency Room CoPay $250 $150 $175 $250 $150 $150 Separate In-Hospital Admission CoPay $250 $250 $375 $250 $250 In-Network Benefits Deductible - Single $1,000 $1,000 $1,000 $1,000 $750 $1,000 Deductible - Family $2,000 $3,000 $3,000 $3,000 $1,500 $2,000 Plan Coinsurance 90% 80% 80% 80% 80% 80% Out-of-Pocket Maximum - Single $3,500 $4,000 $3,500 $3,200 $3,000 $3,000 Out-of-Pocket Maximum - Family $7,000 $8,700 $8,000 $7,000 $7,000 $7,000 Out-of-Network Benefits Deductible - Single $2,000 $2,000 $2,500 $2,000 $1,400 $1,500 Deductible - Family $4,000 $6,000 $6,000 $6,000 $3,000 $3,600 Plan Coinsurance 70% 60% 60% 60% 60% 60% Out-of-Pocket Maximum - Single $7,000 $8,000 $8,000 $8,000 $6,000 $5,500 Out-of-Pocket Maximum - Family $14,000 $16,500 $18,000 $16,000 $12,000 $12,000
13
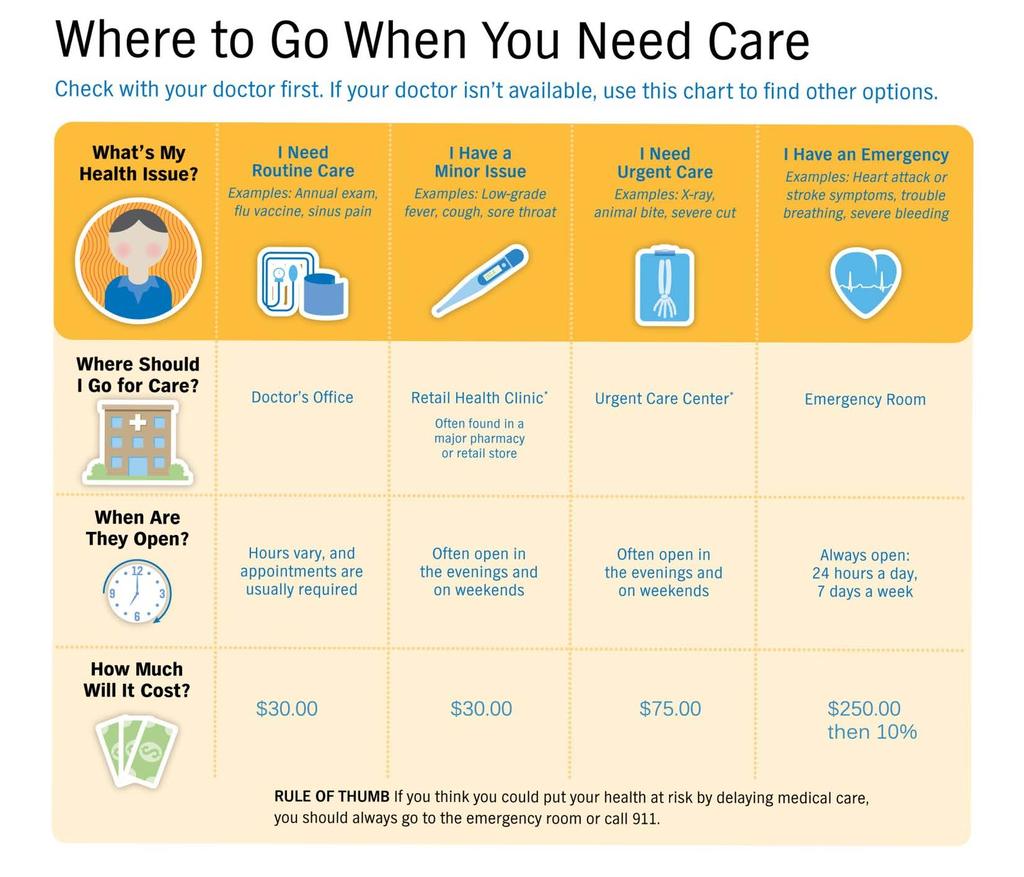
14 Anthem PPO Plan What are the amounts of the co-payments? Doctor Office Visits (In-Network) Primary Care Live Health Online Specialty Care $30 /visit $0 /Copay $60/visit Urgent Care Centers $75/visit (In/Out-of-Network) Emergency Room $250 Co-pay/visit; then you pay 10% (In/Out-of/Network) All deductibles, copayments and coinsurance apply toward the out-of-pocket maximum including prescription drugs.
15 Preventive Care Covered at 100% in-network

16 Preventive Care Covered at 100% in-network
17 Preventive Care Covered at 100% in-network
18

19 co-branding logo here LiveHealth Online. See a doctor 24/7 with LiveHealth Online Meet with a doctor via video, chat or phone Choice of credentialed providers Accessibility anytime, anywhere No appointments or waiting rooms


20 Immediate, Live Consultations An Online Visit thru LiveHealth Online is a covered benefit $0 Co-Pay for Health eprescribing to your local pharmacy A choice of physicians that meets the consumer s needs


21 Anthem Plan Benefits Prescription Drug Benefit Retail $10 Co-Pay for Tier 1 Drugs $35 Co-Pay for Tier 2 Drugs $70 Co-Pay for Tier 3 Drugs 25% to a Max of $250 for Tier 4 Drugs $50 deductible applies then copays Maximum 30 day supply per prescription *Anthem formulary list of all 4 copay tiers is available on the OWU HR web page.


22 Anthem Plan Benefits Prescription Drug Benefit Mail Order* $10.00 Co-Pay for Tier 1 Drugs $70.00 Co-Pay for Tier 2 Drugs $ Co-Pay for Tier 3 Drugs 25% to a Max of $250 for Tier 4 Drugs Maximum 90 day supply per prescription; Tier 4 30 day supply, includes diabetic test strips *Anthem formulary list of all 4 copay tiers is available on the OWU HR web page.

23
24

25



26
27 OWU PPO Plan Calendar Year Deductible $1,000 Per Person $2,000 Family Maximum Your Individual Out-of-Pocket Expenses $1,000 Co-Insurance after the Deductible (Per Calendar Year) 90% of next $25,000 10% of next $25,000 + $2,500 $3,500 Insurance Company Pays (Per Calendar Year) 100% Total Out-of-Pocket Expense Per Person ($7,000 Family Maximum) All deductibles, copayments and coinsurance apply toward the out-of-pocket maximum including prescription copayments.
28 Anthem PPO Plan Diagnostic Testing Services In-Network MRI s 100% CT Scans 100% PET Scans 100% Nuclear Medicine 100% X-Ray s/radiology 100%
29 ANTHEM PPO PLAN In-Network Deductible $1,000 Per Person $2,000 Family maximum Out of Pocket* $3,500 Per Person (including deductible) $7,000 Family maximum (including deductible) Out-of-Network Deductible $2,000 Per Person $4,000 Family maximum Out of Pocket* $7,000 Per Person (including deductible) $14,000 Family maximum (including deductible) *Out-of-Pocket maximums include co-payments in-network
30 Tips To Save $$$ Verify your doctor and the provider is in Anthem s network Remind the receptionist that your co-pay for a preventive care visit is $0 Confirm preventive care procedures are eligible prior to the appointment & that it will be billed as a preventive when leaving the provider s office Verify physician referrals to labs/facilities are in the network Utilize Anthem s transparency tools to save money Request in-office tests such as lab/x-ray be sent to an in-network lab or physician for evaluation Always reference Anthem s Explanation of Benefits (EOB) prior to paying the provider Use the OneRx app to help find the lowest price for prescriptions Take the Preferred Drug List with you to the doctor visit Request generic drug when available

31

32
33
34
35

36 ConditionCare Receive guidance on following your care plan Consult with nurse coaches Better manage your health

")
37 HEALTH MANAGEMENT TOOLS ConditionCare helps participants manage the following conditions: Asthma (Pediatric & Adult) Chronic Obstructive Pulmonary Disease Coronary Artery Disease Diabetes (Pediatric & Adult; Types 1 & 2) Heart Failure

38 24/7 NurseLine Receive instant health care information Consult with registered nurses Available by phone 24 hours a day, toll-free 38


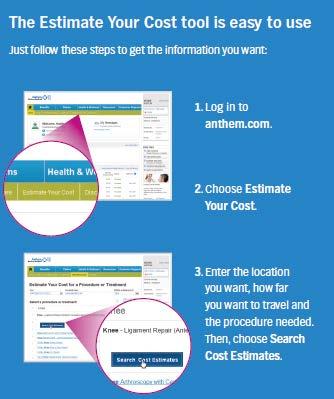
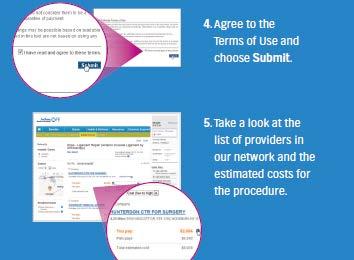
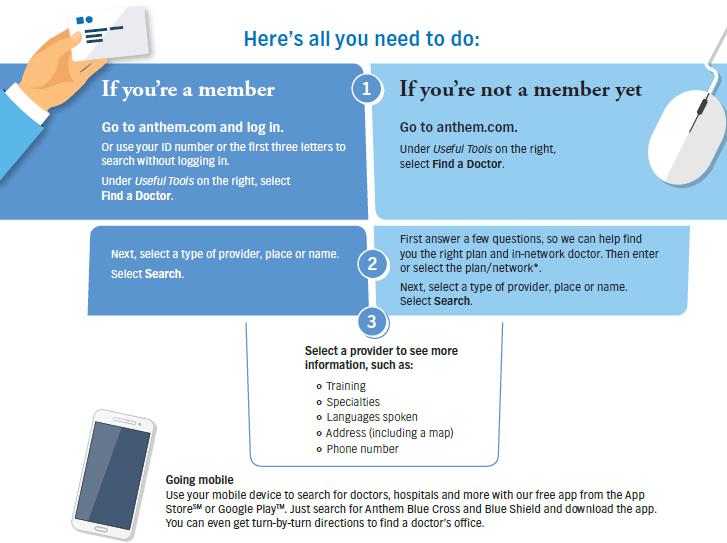
39 Tools to help you choose Open Enrollment book Read this guide to help compare your plan options Find a Doctor Search for information about doctors in your area Interactive Videos Learn more about your health plan and how to effectively use it Estimate Your Cost Find cost estimates for common inpatient, outpatient and diagnostic services 39
40 ANTHEM Dependent Age Status End of the month in which the dependent turns 26 unless the dependent is eligible for another employer-sponsored health plan other than that of a parent
41 WHO TO CALL WITH QUESTIONS Anthem Member Services: Benefit Information Claim Inquiries Provider Searches Changes to member data ID Cards, Provider Directories
42 FLEXIBLE SPENDING ACCOUNT
43 PLAN DETAILS Ohio Wesleyan University Sponsored Plan Allowing Faculty and Staff to Make Pre-Tax Contributions for: Health Care Account Dependent Care Account Eligibility Requirements $2,600 Annual Election Maximum $5,000 Annual Election Maximum All full time Faculty and Staff Do not need to participate in the Medical; Dental or Vision Plan Annual Voluntary Election May not have a HSA and a Health Care FSA (IRS Rule) Plan year will begin July 1, 2017 June 30, 2018
 to pay for eligible expenses at point of service - No more paying cash, and waiting for reimbursement The FSA")
44 FSA BENEFITS CARD Your employer offers a limited use FSA Benefits Card for you to use to pay for your FSA eligible expenses. The FSA Benefits Card allows employees participating in a FSA (medical or dependent care) to pay for eligible expenses at point of service - No more paying cash, and waiting for reimbursement The FSA Benefits Card can be used at eligible merchant locations such as: Doctor and Dentist offices Pharmacies Vision service locations Dependent care facilities (available funds are limited to actual account balance)

45 HOW TO FILE A CLAIM File claims online at hrpro.biz and click on the Login button in the top right corner Complete paper claim form and fax, mail or with itemized receipts or provider Explanation of Benefits (EOBs) to HRPro: Fax: (248) accounts@hrpro.biz Mail: 1423 East 11 Mile Road Royal Oak, MI 48067
 For savings accounts, attach a deposit slip Once complete, fax all information to HRPro at")
46 HOW TO SET UP DIRECT DEPOSIT Complete the Direct Deposit Authorization Form For checking accounts, attach a voided check (or photocopy of a check) For savings accounts, attach a deposit slip Once complete, fax all information to HRPro at

47 SMARTPHONE MOBILE APP There is a mobile app available to view your account balance from your smartphone. You are able to upload your itemized receipts and attach them to claims on the Employee Portal or from your smartphone. This works for claims you submit for reimbursement and debit card transactions requiring documentation for substantiation.
48 ELIGIBLE EXPENSES Health Care Account Medical, Dental and Vision expenses Deductible Coinsurance Co-payments for office visits, prescription drugs, etc. Some Expenses not covered by insurance Dependent Care Account Daycare expenses during work hours Daycare/babysitting for children under 13 Preschool programs After-school care Home care for disabled dependent age 13 and over
49 ELIGIBLE EXPENSES Day Care expense must be to provide gainful employment If married, spouse must also be employed Dependent must reside with employee Payment for providing care may not be made to another dependent Care provider must disclose TAX ID #
50 DENTAL PLANS
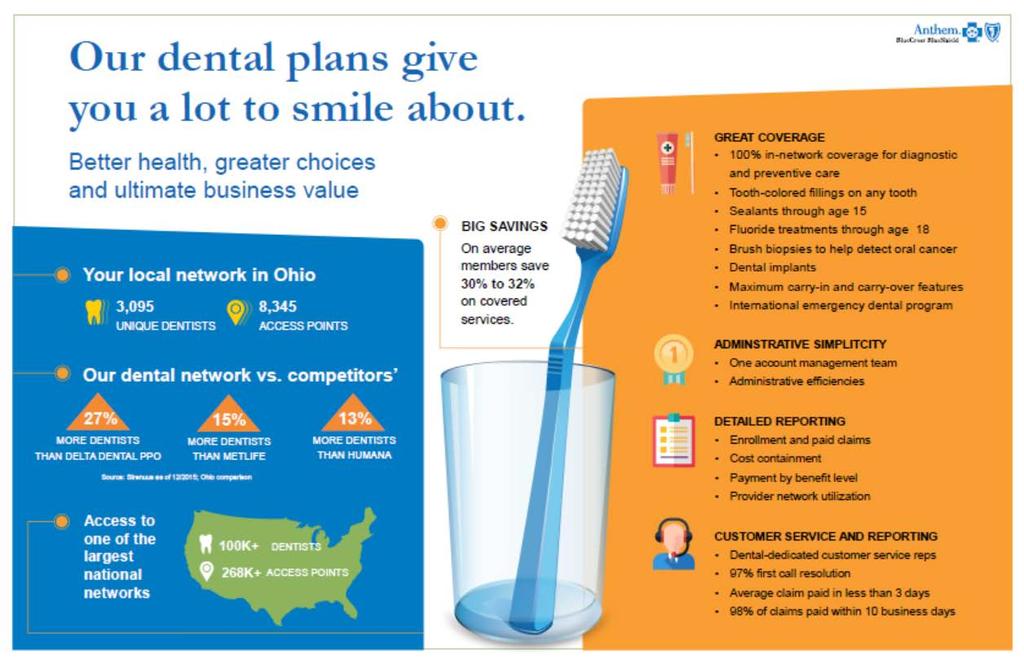
51 KEY FEATURES OF THE DENTAL PLANS Your choice of a Low and High Plan 100% for Routine Preventive services (1) Administrated by the Anthem Benefits are subject to Anthem Contract Limitations
52
53 KEY FEATURES OF THE DENTAL PLANS Receive your care from the Dentist of your choice No Network Requirement Optional network of dentists to receive a discount for services Benefits are subject to Anthem Contract Limitations
54 LOW DENTAL PLAN Deductible Amount = $50.00/Person/year; Family Max (3) Preventive Plan Pays 100% In-Network 90% Out-of-Network (No Deductible) Oral Exams Teeth Cleanings X-Rays Basic Plan Pays 80% In-Network 60% Out-of-Network Amalgam fillings Front composite fillings Simple Extractions Calendar Year Maximum Amount $1,000 per person Major Plan Pays 50% in-network 25% out-of-network Periodontics Endodontics Oral Surgery Crowns Dentures Bridges Dental implants Those who are actively managed in the Anthem Diabetic or Maternal Health Care Management programs will be eligible for an additional dental cleaning or periodontal maintenance procedure per benefit period.
55 HIGH DENTAL PLAN Deductible Amount = $50.00/Person/year; Family Max (3) Preventive Plan Pays 100% In-Network 100% Out-of-Network (No Deductible) Oral exams Teeth cleaning X-Rays Basic Plan Pays 90% In-Network 80% Out-of-Network Sealants Amalgam Filling From Composite Filling Back Composite Filling Simple Extractions Major Plan Pays 60% In-Network 50% Out-of-Network Periodontics Endodontics Oral Surgery Crowns Dentures Bridges Dental Implants Calendar year max amount $1,000 Calendar year max amount $1,500 (Anthem Dental Providers) Orthodontics 50% $1,000 Child only Lifetime max Those who are actively managed in the Anthem Diabetic or Maternal Health Care Management programs will be eligible for an additional dental cleaning or periodontal maintenance procedure per benefit period.
56
57
58 OTHER KEY PIECES OF THE PREFERRED DENTAL PLAN In most cases, the dentist will directly bill Anthem for services Annual Maximum Benefit is $1,000 per person Optional Network of Dentists available to receive discounts Annual Maximum Benefit increases to $1,500 per person when services are provided in Anthem s Network of Dentists
59 HOW THE OPTIONAL NETWORK SAVES YOU MONEY Go to (click find a doctor) Select the Dental Complete network View network of Dentists in your area Visit participating Dentists and receive treatment Dentist will directly bill Anthem at a lower prenegotiated rate and receive their payment directly from Anthem The Dentist can not charge the difference between the negotiated rate and their normal fee (the plan s benefits will apply toward the negotiated rate)
60 ANTHEM DENTAL PLANS Monthly Payroll Deductions (1) Effective July 1, 2017 Employee Employee + One Dependent Family Basic Plan $23.26 $45.60 $74.49 Preferred Plan $32.50 $64.39 $ (1) Pre-tax deductions. Actual net cost will be reduced based upon IRS Section 125 election and personal income tax bracket.
61 VISION PLANS
62 BASIC VISION PLAN Exam every 12 months, $20 co-pay Prescription glasses every 24 months, $20 co-pay Contacts, no co-pay applies ( 24 months) Coverage from a VSP Doctor
63 PREFERRED VISION PLAN Exam every 12 months, $10 co-pay Prescription lenses every 12 months, covered in full Contacts, no co-pay applies ( 12 months) Frames every 24 months, $25.00 $ Allowance Coverage from a VSP Doctor
64 FIND A VSP PROVIDER Go to View Network of Doctors in your area Visit participating Doctors and receive treatment Call
65 VSP PLANS Payroll Deductions (1) Effective July 1, 2017 Employee Basic Plan $8.09 Preferred Plan $9.49 Family $22.87 $26.82 (1) Pre-tax deductions. Actual net cost will be reduced based upon IRS Section 125 election and personal income tax bracket.
66 OPEN ENROLLMENT You may add or remove dependents Enroll or terminate from plan Election is effective 7/1/17 Election is in effect until 6/30/18; unless a qualified change in your status occurs Open Enrollment will be April 24 th through May 19 th 2017
67 QUALIFIED CHANGE IN YOUR STATUS? Change in marital status Change of dependents Involuntary loss of coverage through spouse s employer Change of spouse s employment resulting in loss of coverage Must notify Human Resources within 30 days of change!

68 Who to call with questions? For Claim or Benefit Assistance Stephanie Boehm Employee Benefits Account Manager ClearPath Benefit Advisors x 1866 Fax: sboehm@clearpathbenefits.com



69
70 OWU WELLNESS PROGRAM OVERVIEW Where s the gain? OWU benefits when its employees are healthy, and able to carry-out their work responsibilities efficiently and effectively Employees benefit by leading healthy lifestyles, and are therefore happier, more stable, more dependable, more satisfied Everyone benefits when human resource costs are under control (both insurance premiums and productivity)

71 OWU WELLNESS PROGRAM OVERVIEW Incentives: $25 one time premium credit for the year; or $25 through payroll for completing the wellness assessment One time $75 premium credit for the year or $75 through payroll for achieving 40 credits
72 HOW DO I SIGN-UP? OWU Wellness P/W = OWU
73 BASIC PROGRAM TRACKING (APRIL-MARCH TRACKING CYCLE) Earn 40 Credits in 12- month period to earn incentive
74
75
76
77

78
79 QUESTIONS?
Health Care Plan Open Enrollment
 Health Care Plan Open Enrollment 2016-17 Agenda ACA Update Benefits update Health Care plan review Tips to save health care dollars FSA Open Enrollment Dental Open Enrollment Vision Open Enrollment Employee
Health Care Plan Open Enrollment 2016-17 Agenda ACA Update Benefits update Health Care plan review Tips to save health care dollars FSA Open Enrollment Dental Open Enrollment Vision Open Enrollment Employee
Chapter 11: Actuarial Value Calculator
 Chapter 11: Actuarial Value Calculator Overview To satisfy actuarial value (AV) requirements (45 CFR 156.140 and 156.420), QHP issuers are required to use the Actuarial Value Calculator (AVC) developed
Chapter 11: Actuarial Value Calculator Overview To satisfy actuarial value (AV) requirements (45 CFR 156.140 and 156.420), QHP issuers are required to use the Actuarial Value Calculator (AVC) developed
Minimum Value and Actuarial Value Determinations Under the Affordable Care Act
 Minimum Value and Actuarial Value Determinations Under the Affordable Care Act Catherine Jo Erwin, MAAA, FSA Member, MV/AV Practice Note Work Group John Stenson, MAAA, FSA Chairperson, MV/AV Practice Note
Minimum Value and Actuarial Value Determinations Under the Affordable Care Act Catherine Jo Erwin, MAAA, FSA Member, MV/AV Practice Note Work Group John Stenson, MAAA, FSA Chairperson, MV/AV Practice Note
HealthTrust: Access Blue 20-RX10/20/45 Coverage Period: 07/01/ /30/2017
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.anthem.com or by calling 1-800-870-3122. Important Questions
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.anthem.com or by calling 1-800-870-3122. Important Questions
Important Questions Answers Why this Matters:
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.anthem.com or by calling 1-888-650-4047. Important Questions
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.anthem.com or by calling 1-888-650-4047. Important Questions
Important Questions Answers Why this Matters:
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.crystalrunhp.com or by calling 1-844-638-6506. Important
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.crystalrunhp.com or by calling 1-844-638-6506. Important
OEBB Summary of Vision Benefits Plan Year
 OEBB Summary of Vision Benefits 2017 18 Plan Year You will not receive an ID card from VSP. No ID card needed at your appointment, simply tell them you have VSP. To find out more, go to vsp.com or call
OEBB Summary of Vision Benefits 2017 18 Plan Year You will not receive an ID card from VSP. No ID card needed at your appointment, simply tell them you have VSP. To find out more, go to vsp.com or call
Anthem BlueCross BlueShield Blue Access PPO Option 10 / Rx Option 7 Summary of Benefits and Coverage: What this Plan Covers & What it Costs
 Anthem BlueCross BlueShield Blue Access PPO Option 10 / Rx Option 7 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage Period: 07/01/2015-0 /30/2016 Coverage For: Individual/Family
Anthem BlueCross BlueShield Blue Access PPO Option 10 / Rx Option 7 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage Period: 07/01/2015-0 /30/2016 Coverage For: Individual/Family
You must pay all of the costs for these services up to the specific deductible amount before the plan begins to pay for these services.
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.anthem.com or by calling 1-800-552-9159. Important Questions
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.anthem.com or by calling 1-800-552-9159. Important Questions
Important Questions Answers Why this Matters:
 Anthem BlueCross BlueShield Blue Access PPO Option 20 / Rx Option 7 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage Period: 01/01/2015-12/31/2015 Coverage For: Individual/Family
Anthem BlueCross BlueShield Blue Access PPO Option 20 / Rx Option 7 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage Period: 01/01/2015-12/31/2015 Coverage For: Individual/Family
[Ambetter Secure Care 1 (2018) with 3 Free PCP Visits-Standard Gold On Exchange Plan]
![[Ambetter Secure Care 1 (2018) with 3 Free PCP Visits-Standard Gold On Exchange Plan]](/thumbs/72/67333205.jpg "[Ambetter Secure Care 1 (2018) with 3 Free PCP Visits-Standard Gold On Exchange Plan]") [Plan Information] [Health Plan:] [Primary Member:] [Ambetter Secure Care 1 (2018) with 3 Free PCP Visits-Standard Gold On Exchange Plan] [John Doe] [Member ID:] [01213456] [Date of Birth:] [08/12/62]
[Plan Information] [Health Plan:] [Primary Member:] [Ambetter Secure Care 1 (2018) with 3 Free PCP Visits-Standard Gold On Exchange Plan] [John Doe] [Member ID:] [01213456] [Date of Birth:] [08/12/62]
HealthTrust: LUMENOS $2500 Coverage Period: 07/01/ /30/2017
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.anthem.com or by calling 1-888-224-4896. Important Questions
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.anthem.com or by calling 1-888-224-4896. Important Questions
Clergy Benefit Comparison Effective January 1, 2018
 Clergy Benefit Comparison Effective January 1, 2018 HMO-POS Plan Personal Care Account (Provided by VUMPI) There is no Personal Care Account There is no Personal Care Account $750 Individual, $2,250 Family
Clergy Benefit Comparison Effective January 1, 2018 HMO-POS Plan Personal Care Account (Provided by VUMPI) There is no Personal Care Account There is no Personal Care Account $750 Individual, $2,250 Family
Important Questions Answers Why this Matters:
 Anthem BlueCross BlueShield Blue Access PPO Option D54 / Rx Option 7 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage Period: 04/01/2013-03/31/2014 Coverage For: Individual/Family
Anthem BlueCross BlueShield Blue Access PPO Option D54 / Rx Option 7 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage Period: 04/01/2013-03/31/2014 Coverage For: Individual/Family
$1,500 Individual/$3,000 Family for participating providers. $3,000 Individual/$6,000. Important Questions Answers Why this Matters:
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.calcpahealth.com or by calling 1-877-480-7923. Important
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.calcpahealth.com or by calling 1-877-480-7923. Important
Medical Plan 2019 Coverage Options
 Medical Plan 2019 Coverage Options These documents provide a convenient overview of your health care insurance rates and coverage (medical, including pharmacy; dental; vision) and your contribution limits
Medical Plan 2019 Coverage Options These documents provide a convenient overview of your health care insurance rates and coverage (medical, including pharmacy; dental; vision) and your contribution limits
Important Questions Answers Why this Matters:
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.summacare.com or by calling 1-800-996-8701. Important
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.summacare.com or by calling 1-800-996-8701. Important
Important Questions Answers Why this Matters:
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document by calling 1-585-343-0055 ext. 6415. Important Questions Answers
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document by calling 1-585-343-0055 ext. 6415. Important Questions Answers
Washington Counties Insurance Fund 2017 Benefit Plan Comparison for Retirees
 Washington Counties Insurance Fund 2017 Benefit Plan Comparison for Retirees Retiree Medical Plans for Under Age 65 (former WCIF medical enrollees only) Retiree Medical Plans for Over Age 65 (all eligible
Washington Counties Insurance Fund 2017 Benefit Plan Comparison for Retirees Retiree Medical Plans for Under Age 65 (former WCIF medical enrollees only) Retiree Medical Plans for Over Age 65 (all eligible
Important Questions Answers Why this Matters:
 Anthem BlueCross BlueShield Blue Access PPO Option 14 / Rx Option AE Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage Period: 01/01/2015-12/31/2015 Coverage For: Individual/Family
Anthem BlueCross BlueShield Blue Access PPO Option 14 / Rx Option AE Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage Period: 01/01/2015-12/31/2015 Coverage For: Individual/Family
Important Questions Answers Why this Matters: Network: $3,500 Individual $7,000 Family Non-Network: $10,000 Individual $20,000 Family
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.inhealthohio.org or by calling 1-800-580-8502. Important
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.inhealthohio.org or by calling 1-800-580-8502. Important
Important Questions Answers Why this Matters:
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at https://eoc.anthem.com/eocdps/fi or by calling (855) 333-5735.
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at https://eoc.anthem.com/eocdps/fi or by calling (855) 333-5735.
Important Questions Answers Why this Matters:
 Anthem BlueCross BlueShield Lumenos Health Savings Account (with copays) Option 1 Rx 9 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage Period: 10/01/2014-09/30/2015 Coverage
Anthem BlueCross BlueShield Lumenos Health Savings Account (with copays) Option 1 Rx 9 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage Period: 10/01/2014-09/30/2015 Coverage
University of Cincinnati Medical Plan Summary and Comparison Non AAUP - Effective January 1- December 31, 2018
 Annual Deductible Annual Health Savings Account Funding (UC) $1500 individual $3,000 family Varies by Annual Base Pay as of 1/1/18 $3,000 per person $6,000 family Varies by Annual Base Pay as of 1/1/18
Annual Deductible Annual Health Savings Account Funding (UC) $1500 individual $3,000 family Varies by Annual Base Pay as of 1/1/18 $3,000 per person $6,000 family Varies by Annual Base Pay as of 1/1/18
Important Questions Answers Why this Matters:
 Anthem BlueCross BlueShield Lumenos Health Savings Account Option 56 Rx9 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage Period: 12/01/2013-11/30/2014 Coverage For: Individual/Family
Anthem BlueCross BlueShield Lumenos Health Savings Account Option 56 Rx9 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage Period: 12/01/2013-11/30/2014 Coverage For: Individual/Family
Important Questions Answers Why this Matters:
 This is only a summary. Medical benefits are covered through Anthem Blue Cross and Blue Shield. If you want more detail about your coverage and costs for health benefits, you can get the complete terms
This is only a summary. Medical benefits are covered through Anthem Blue Cross and Blue Shield. If you want more detail about your coverage and costs for health benefits, you can get the complete terms
Anthem BlueCross BlueShield Christian Care Communities Blue Access PPO Coverage Period: 01/01/ /31/2015 Summary of Benefits and Coverage:
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.anthem.com or by calling 1-888-650-4047. Important Questions
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.anthem.com or by calling 1-888-650-4047. Important Questions
Important Questions Answers Why this Matters:
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.anthem.com or by calling 1-800-843-6447. Important Questions
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.anthem.com or by calling 1-800-843-6447. Important Questions
Important Questions Answers Why this Matters:
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.anthem.com or by calling 1-855-333-5735. Important Questions
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.anthem.com or by calling 1-855-333-5735. Important Questions
Important Questions Answers Why this Matters:
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.anthem.com or by calling 1-877-309-2955. Important Questions
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.anthem.com or by calling 1-877-309-2955. Important Questions
Senior Care Network: Blue Access PPO and Blue Access Choice PPO Coverage Period: 01/01/ /31/2016
 Senior Care Network: Blue Access PPO and Blue Access Choice PPO Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage Period: 01/01/2016-12/31/2016 Coverage for: Individual/Family
Senior Care Network: Blue Access PPO and Blue Access Choice PPO Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage Period: 01/01/2016-12/31/2016 Coverage for: Individual/Family
HEALTH PLAN BENEFITS AND COVERAGE MATRIX
 HEALTH PLAN BENEFITS AND COVERAGE MATRIX THIS MATRIX IS INTENDED TO BE USED TO HELP YOU COMPARE COVERAGE BENEFITS AND IS A SUMMARY ONLY. THE EVIDENCE OF COVERAGE AND PLAN CONTRACT SHOULD BE CONSULTED FOR
HEALTH PLAN BENEFITS AND COVERAGE MATRIX THIS MATRIX IS INTENDED TO BE USED TO HELP YOU COMPARE COVERAGE BENEFITS AND IS A SUMMARY ONLY. THE EVIDENCE OF COVERAGE AND PLAN CONTRACT SHOULD BE CONSULTED FOR
Important Questions Answers Why this Matters:
 Important Questions Answers Why this Matters: What is the overall deductible? Are there other deductibles for specific services? Is there an out of pocket limit on my expenses? $1,500 single / $3,000 family
Important Questions Answers Why this Matters: What is the overall deductible? Are there other deductibles for specific services? Is there an out of pocket limit on my expenses? $1,500 single / $3,000 family
Important Questions Answers Why this Matters:
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at https://eoc.anthem.com/eocdps/aso or by calling (855) 333-5735.
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at https://eoc.anthem.com/eocdps/aso or by calling (855) 333-5735.
Does not apply to Network Preventive deductible?
 Wittenberg University: Blue Access (PPO) Option 2 Coverage Period: 01/01/2016-12/31/2016 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual/Family Plan Type:
Wittenberg University: Blue Access (PPO) Option 2 Coverage Period: 01/01/2016-12/31/2016 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual/Family Plan Type:
Important Questions Answers Why this Matters:
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at https://eoc.empireblue.com/eocdps/fi or by calling 1-855-220-3341.
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at https://eoc.empireblue.com/eocdps/fi or by calling 1-855-220-3341.
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan
 Anthem BlueCross BlueShield Premier Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage Period: 01/01/2013-01/01/2014 Coverage For: Individual/Family Plan Type: PPO This is
Anthem BlueCross BlueShield Premier Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage Period: 01/01/2013-01/01/2014 Coverage For: Individual/Family Plan Type: PPO This is
Employee. Package. Benefits N O V E M B E R 1, O C T O B E R 3 1,
 2017-2018 Employee Benefits Package ENROLLMENT ELECTIONS EFFECTIVE: N O V E M B E R 1, 2 0 1 7 - O C T O B E R 3 1, 2 0 1 8 TBC- FISHERBROYLES OE 2017-2018 Medical Plan- W2 In-Network In-Network In-Network
2017-2018 Employee Benefits Package ENROLLMENT ELECTIONS EFFECTIVE: N O V E M B E R 1, 2 0 1 7 - O C T O B E R 3 1, 2 0 1 8 TBC- FISHERBROYLES OE 2017-2018 Medical Plan- W2 In-Network In-Network In-Network
2018 EMPLOYEE BENEFITS PRESENTATION
 2018 EMPLOYEE BENEFITS PRESENTATION 2018 BENEFITS MEETING Agenda 1 Overview 2 3 4 5 6 7 Touchpoints & Pocketpal Medical BCBS MA HRA Benefit Strategies Alex FSA Benefit Strategies Dental Delta Dental 8
2018 EMPLOYEE BENEFITS PRESENTATION 2018 BENEFITS MEETING Agenda 1 Overview 2 3 4 5 6 7 Touchpoints & Pocketpal Medical BCBS MA HRA Benefit Strategies Alex FSA Benefit Strategies Dental Delta Dental 8
Your Plan: Anthem Bronze PPO 6000/0%/6000 w/hsa Your Network: Prudent Buyer PPO
 Your Plan: Anthem Bronze PPO 6000/0%/6000 w/hsa Your Network: Prudent Buyer PPO This summary of benefits is a brief outline of coverage, designed to help you with the selection process. This summary does
Your Plan: Anthem Bronze PPO 6000/0%/6000 w/hsa Your Network: Prudent Buyer PPO This summary of benefits is a brief outline of coverage, designed to help you with the selection process. This summary does
Anthem BlueCross BlueShield Eastern Kentucky University Economy Coverage Period: {01/01/ /31/2013} Summary of Benefits and Coverage:
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.anthem.com or by calling 1-888-650-4047. For prescription
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.anthem.com or by calling 1-888-650-4047. For prescription
Important Questions Answers Why this Matters:
 Southeastern Indiana School Insurance Consortium: Plan F Blue Access for Health Savings Accounts Coverage Period: 01/01/2015-12/31/2015 Summary of Benefits and Coverage: What this Plan Covers & What it
Southeastern Indiana School Insurance Consortium: Plan F Blue Access for Health Savings Accounts Coverage Period: 01/01/2015-12/31/2015 Summary of Benefits and Coverage: What this Plan Covers & What it
Marsh and McLennan: Anthem Blue Cross and Blue Shield $2,850 Deductible Plan Coverage Period: 01/01/ /31/2017
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at https://eoc.anthem.com/eocdps/aso or by calling (855) 570-1150.
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at https://eoc.anthem.com/eocdps/aso or by calling (855) 570-1150.
Important Questions Answers Why this Matters:
 Anthem BlueCross BlueShield MMEBG Blue Access PPO Coverage Period: 07/01/2015-06/30/2016 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual/Family Plan Type:
Anthem BlueCross BlueShield MMEBG Blue Access PPO Coverage Period: 07/01/2015-06/30/2016 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual/Family Plan Type:
Important Questions Answers Why this Matters:
 Amtrust Financial Services: Blue Access (PPO) Coverage Period: 03/01/2016-12/31/2016 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual/Family Plan Type: PPO
Amtrust Financial Services: Blue Access (PPO) Coverage Period: 03/01/2016-12/31/2016 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual/Family Plan Type: PPO
You can see the specialist you choose without permission from this plan.
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.pibf.org or by calling 1-918-280-4800. Important Questions
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.pibf.org or by calling 1-918-280-4800. Important Questions
Prepared By: 600 West 5 th Street, Suite 200 Austin, TX Toll Free: O: (512) F: (512) Hours 8:30 to 5:00 M F
 F: (512) Hours 8:30 to 5:00 M F") EMPLOYEE BENEFITS PLAN YEAR Prepared By: 600 West 5 th Street, Suite 200 Austin, TX 78701 Toll Free: 1.888.478.9595 O: (512) 478.9595 F: (512) 478.9494 Hours 8:30 to 5:00 M F Tom Ball Danny Peoples Account
EMPLOYEE BENEFITS PLAN YEAR Prepared By: 600 West 5 th Street, Suite 200 Austin, TX 78701 Toll Free: 1.888.478.9595 O: (512) 478.9595 F: (512) 478.9494 Hours 8:30 to 5:00 M F Tom Ball Danny Peoples Account
Important Questions Answers Why this Matters: $300 Single/$600 Family for Network Providers. $500 Single/$1,000 Family for Non- What is the overall
 Bellefontaine City Schools: Blue Access (PPO) Coverage Period: 04/01/2015-03/31/2016 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual/Family Plan Type: PPO
Bellefontaine City Schools: Blue Access (PPO) Coverage Period: 04/01/2015-03/31/2016 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual/Family Plan Type: PPO
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.networkhealth.com/benefits/sbc/individualpolicy.pdf or
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.networkhealth.com/benefits/sbc/individualpolicy.pdf or
Regence BlueShield: Regence Gold 1000 Preferred
 Regence BlueShield: Regence Gold 1000 Preferred Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage Period: 01/01/2016 12/31/2016 Coverage for: Individual & Eligible Family
Regence BlueShield: Regence Gold 1000 Preferred Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage Period: 01/01/2016 12/31/2016 Coverage for: Individual & Eligible Family
Important Questions Answers Why this Matters: What is the overall deductible? Are there other deductibles for specific services?
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.avmed.org/go/state or by calling 1-888-762-8633 Important
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.avmed.org/go/state or by calling 1-888-762-8633 Important
Western Kentucky University Anthem BlueCross BlueShield Basic PPO Plan Coverage Period: 01/01/ /31/2018 Summary of Benefits and Coverage:
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at https://eoc.anthem.com/eocdps/aso or by calling 1-888-650-4047.
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at https://eoc.anthem.com/eocdps/aso or by calling 1-888-650-4047.
Important Questions Answers Why this Matters:
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.arcsvs.com or by calling 1-877-309-2955. Important Questions
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.arcsvs.com or by calling 1-877-309-2955. Important Questions
Important Questions Answers Why this Matters: For in-network providers Deductible is not applicable innetwork
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.anthem.com or by calling 1-800-922-6621. Important Questions
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.anthem.com or by calling 1-800-922-6621. Important Questions
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.summacare.com or by calling 1-800-996-8701. Important
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.summacare.com or by calling 1-800-996-8701. Important
Important Questions Answers Why this Matters:
 Anthem BlueCross BlueShield Anthem KeyCare 25 / $10/$30/$50/20% Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage Period: 11/01/2015-10/31/2016 Coverage For: Individual/Family
Anthem BlueCross BlueShield Anthem KeyCare 25 / $10/$30/$50/20% Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage Period: 11/01/2015-10/31/2016 Coverage For: Individual/Family
Important Questions Answers Why this Matters:
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.soundhealthwellness.com or by calling 1-800-225-7620.
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.soundhealthwellness.com or by calling 1-800-225-7620.
GUIDE TO MEDICAL AND DENTAL PLANS
 GUIDE TO MEDICAL AND DENTAL PLANS B e n e f i t s e f f e c t i v e J u l y 1, 2 0 1 4 t h r o u g h J u n e 3 0, 2 0 1 5 Choosing your benefits is an important decision. This guide provides you with the
GUIDE TO MEDICAL AND DENTAL PLANS B e n e f i t s e f f e c t i v e J u l y 1, 2 0 1 4 t h r o u g h J u n e 3 0, 2 0 1 5 Choosing your benefits is an important decision. This guide provides you with the
Anthem BlueCross BlueShield St. Charles Community College Blue Access & Blue Access Choice PPO Coverage Period: 01/01/ /31/2016
 Anthem BlueCross BlueShield St. Charles Community College Blue Access & Blue Access Choice PPO Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage Period: 01/01/2016-12/31/2016
Anthem BlueCross BlueShield St. Charles Community College Blue Access & Blue Access Choice PPO Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage Period: 01/01/2016-12/31/2016
Anthem BlueCross BlueShield MMEBG HSA 2 Lumenos Health Savings Accounts (Blue Preferred Select) Coverage Period: 07/01/ /30/2017
 Coverage Period: 07/01/ /30/2017") Anthem BlueCross BlueShield MMEBG HSA 2 Lumenos Health Savings Accounts (Blue Preferred Select) Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage Period: 07/01/2016-06/30/2017
Anthem BlueCross BlueShield MMEBG HSA 2 Lumenos Health Savings Accounts (Blue Preferred Select) Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage Period: 07/01/2016-06/30/2017
BENEFITS ENROLLMENT. Take Action
 2017 BENEFITS ENROLLMENT Take Action You must take action and select benefits or waive coverage; you only have 31 days from your date of hire to make elections What s inside Welcome... Error! Bookmark
2017 BENEFITS ENROLLMENT Take Action You must take action and select benefits or waive coverage; you only have 31 days from your date of hire to make elections What s inside Welcome... Error! Bookmark
Upper Arlington City School District: Lumenos Health Savings Accounts Coverage Period: 01/01/ /31/2016
 Upper Arlington City School District: Lumenos Health Savings Accounts Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage Period: 01/01/2016-12/31/2016 Coverage for: Individual/Family
Upper Arlington City School District: Lumenos Health Savings Accounts Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage Period: 01/01/2016-12/31/2016 Coverage for: Individual/Family
County of Cuyahoga: MMO SuperMed EPO
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.medmutual.com/sbc or by calling 1-800-540-2583. Important
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.medmutual.com/sbc or by calling 1-800-540-2583. Important
Anthem BlueCross BlueShield MMEBG HSA 2 Lumenos Health Savings Accounts (Blue Preferred Select) Coverage Period: 07/01/ /30/2016
 Coverage Period: 07/01/ /30/2016") Anthem BlueCross BlueShield MMEBG HSA 2 Lumenos Health Savings Accounts (Blue Preferred Select) Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage Period: 07/01/2015-06/30/2016
Anthem BlueCross BlueShield MMEBG HSA 2 Lumenos Health Savings Accounts (Blue Preferred Select) Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage Period: 07/01/2015-06/30/2016
Small Group Plans Plan Information
 Small Group Plans 2018 Plan Information Good health begins with good choices. We want coverage to be as clear and understandable as possible. Whatever your budget, we can help find the right health plan
Small Group Plans 2018 Plan Information Good health begins with good choices. We want coverage to be as clear and understandable as possible. Whatever your budget, we can help find the right health plan
What is the overall deductible? are separate and do not. towards each other. Are there other deductibles for specific services?
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at https://eoc.anthem.com/eocdps/fi or by calling (855) 333-5735.
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at https://eoc.anthem.com/eocdps/fi or by calling (855) 333-5735.
Important Questions Answers Why this Matters:
 Anthem BlueCross BlueShield Lumenos Health Savings Account Option 51 Rx 9 What this Plan Covers & What it Costs Coverage Period: 01/01/2013-12/31/2013 Individual/Family CDHP This is only a summary. If
Anthem BlueCross BlueShield Lumenos Health Savings Account Option 51 Rx 9 What this Plan Covers & What it Costs Coverage Period: 01/01/2013-12/31/2013 Individual/Family CDHP This is only a summary. If
Important Questions Answers Why this Matters: Network: $500 Individual / $1,000 Family Non-Network: $1,000 Individual / $2,000 Family
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.healthscopebenefits.com or by calling 1-800-262-4772.
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.healthscopebenefits.com or by calling 1-800-262-4772.
You must pay all the costs up to the deductible amount before this plan. covered services after you meet the deductible.
 Secure Choice Health Savings Account Partner Coverage Period: Beginning on or after 01-01-2016 Summary of Benefits and Coverage: What this Plan covers & What it Costs Coverage for: S, S+1, and Family coverage
Secure Choice Health Savings Account Partner Coverage Period: Beginning on or after 01-01-2016 Summary of Benefits and Coverage: What this Plan covers & What it Costs Coverage for: S, S+1, and Family coverage
Annual Enrollment Meetings
 Non-Union Annual Enrollment Meetings Hussmann Corporation Non-Union Benefit Overview Effective January 1, 2014 Optional Benefits Medical/Pharmacy (PPO & CHP) Health Savings Account (HSA) Flexible Spending
Non-Union Annual Enrollment Meetings Hussmann Corporation Non-Union Benefit Overview Effective January 1, 2014 Optional Benefits Medical/Pharmacy (PPO & CHP) Health Savings Account (HSA) Flexible Spending
Network Providers. deductible?
 Hoosier Heartland School Trust: Plan 1 Blue Access (PPO) Coverage Period: 1/01/2017-08/31/2017 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual/Family Plan
Hoosier Heartland School Trust: Plan 1 Blue Access (PPO) Coverage Period: 1/01/2017-08/31/2017 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual/Family Plan
Important Questions Answers Why this Matters:
 Amtrust Financial Services: Lumenos Health Savings Accounts Enhanced Plan - Non- Embedded Coverage Period: 03/01/2016-12/31/2016 Summary of Benefits and Coverage: What this Plan Covers & What it Costs
Amtrust Financial Services: Lumenos Health Savings Accounts Enhanced Plan - Non- Embedded Coverage Period: 03/01/2016-12/31/2016 Summary of Benefits and Coverage: What this Plan Covers & What it Costs
Important Questions Answers Why this Matters:
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.anthem.com/ca or by calling 1-855-333-5730. Important
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.anthem.com/ca or by calling 1-855-333-5730. Important
BridgeSpan Health Company: BridgeSpan Silver HDHP 2000 MyChoice Northwest
 BridgeSpan Health Company: BridgeSpan Silver HDHP 2000 MyChoice Northwest Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage Period: 01/01/2016 12/31/2016 Coverage for: Individual
BridgeSpan Health Company: BridgeSpan Silver HDHP 2000 MyChoice Northwest Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage Period: 01/01/2016 12/31/2016 Coverage for: Individual
Marsh and McLennan: Anthem Blue Cross and Blue Shield $400 Deductible Plan Coverage Period: 01/01/ /31/2017
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at https://eoc.anthem.com/eocdps/aso or by calling (855) 570-1150.
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at https://eoc.anthem.com/eocdps/aso or by calling (855) 570-1150.
Anthem Blue Cross Blue Shield: Anthem Silver DirectAccess - cbka Coverage Period: 01/01/ /31/2014
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.anthem.com or by calling 1-888-231-5046. Important Questions
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.anthem.com or by calling 1-888-231-5046. Important Questions
Your Plan: Anthem Silver PPO 2000/35%/6850 Your Network: Prudent Buyer PPO
 Your Plan: Anthem Silver PPO 2000/35%/6850 Your Network: Prudent Buyer PPO This summary of benefits is a brief outline of coverage, designed to help you with the selection process. This summary does not
Your Plan: Anthem Silver PPO 2000/35%/6850 Your Network: Prudent Buyer PPO This summary of benefits is a brief outline of coverage, designed to help you with the selection process. This summary does not
BENEFITS ENROLLMENT. Take Action
 2018-19 BENEFITS ENROLLMENT Take Action You must take action and select benefits or waive coverage; you only have 31 days from your start date to make elections for the 2018-19 plan year. What s inside
2018-19 BENEFITS ENROLLMENT Take Action You must take action and select benefits or waive coverage; you only have 31 days from your start date to make elections for the 2018-19 plan year. What s inside
Medical and Dental Benefits Guide. Oregon Groups with 1 50 employees
 Medical and Dental Benefits Guide Oregon Groups with 1 50 employees For plans effective on or after January 1, 2016 Provider network 4 Wellness rewards 5 Health support programs 6 Tools to manage care
Medical and Dental Benefits Guide Oregon Groups with 1 50 employees For plans effective on or after January 1, 2016 Provider network 4 Wellness rewards 5 Health support programs 6 Tools to manage care
What is the overall deductible? Are there other deductibles for specific services?
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.anthem.com/cuhealthplan or by calling 1-800-735-6072.
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.anthem.com/cuhealthplan or by calling 1-800-735-6072.
Important Questions Answers Why this Matters: In-network: $0/Individual; $0/Family Out-of-network: $500/Individual; $1,000/Family
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at https://eoc.anthem.com/eocdps/aso or by calling 1-800-445-7490.
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at https://eoc.anthem.com/eocdps/aso or by calling 1-800-445-7490.
Blue Care Elect $250 Deductible MIIA Coverage Period: on or after 07/01/2015
 Blue Care Elect $250 Deductible MIIA Coverage Period: on or after 07/01/2015 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual and Family Plan Type: PPO This
Blue Care Elect $250 Deductible MIIA Coverage Period: on or after 07/01/2015 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual and Family Plan Type: PPO This
Important Questions Answers Why this Matters:
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.pibf.org or by calling 1-918-280-4800. Important Questions
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.pibf.org or by calling 1-918-280-4800. Important Questions
University of Cincinnati Medical Plan Summary and Comparison Effective January 1- December 31, 2018-AAUP only
 Annual Deductible Annual Health Savings Account Funding (UC) $1500 individual $3,000 family Varies by Annual Base Pay as of 1/1/2018 $3,000 per person $6,000 family Varies by Annual Base Pay as of 1/1/2018
Annual Deductible Annual Health Savings Account Funding (UC) $1500 individual $3,000 family Varies by Annual Base Pay as of 1/1/2018 $3,000 per person $6,000 family Varies by Annual Base Pay as of 1/1/2018
AvMed In-Network Tier A Providers: $1,500 individual / $3,000 family AvMed In-Network Tier B Providers: What is the overall deductible?
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.avmed.org or by calling 1-800-477-8768. Important Questions
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.avmed.org or by calling 1-800-477-8768. Important Questions
You can see the specialist you choose without permission from this plan.
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.crystalrunhealthinsurancecompany.com or by calling 1-844-638-6506.
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.crystalrunhealthinsurancecompany.com or by calling 1-844-638-6506.
New England Carpenters Health Benefits Fund: Plan 1 Summary of Benefits and Coverage: What this Plan Covers & What it Costs
 New England Carpenters Health Benefits Fund: Plan 1 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage Period: 01/01/2016-12/31/2016 Coverage for: Individual + Family Plan
New England Carpenters Health Benefits Fund: Plan 1 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage Period: 01/01/2016-12/31/2016 Coverage for: Individual + Family Plan
Important Questions Answers Why this Matters:
 Anthem BlueCross Solution PPO 1500/15/20 / $15/$30/$50/30% Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage Period: 11/01/2014-10/31/2015 Coverage For: Individual/Family
Anthem BlueCross Solution PPO 1500/15/20 / $15/$30/$50/30% Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage Period: 11/01/2014-10/31/2015 Coverage For: Individual/Family
2018 Medical Plan Comparison Chart
 2018 Medical Plan Comparison Chart USC TROJAN CARE EPO USC Custom TIER 1: Keck Medicine TIER 2: Anthem TIER 3: Out-of-network TIER 1: USC Custom TIER 2: Anthem Is a referral required to see a specialist?
2018 Medical Plan Comparison Chart USC TROJAN CARE EPO USC Custom TIER 1: Keck Medicine TIER 2: Anthem TIER 3: Out-of-network TIER 1: USC Custom TIER 2: Anthem Is a referral required to see a specialist?
Important Questions Answers Why this Matters: In-network: $0/Individual; $0/Family Out-of-network: $750/Individual; $1,500/Family
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.anthem.com or by calling 1-800-421-1880. Important Questions
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.anthem.com or by calling 1-800-421-1880. Important Questions
Important Questions Answers Why this Matters:
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.empireblue.com or by calling 1-855-333-5734. Important
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.empireblue.com or by calling 1-855-333-5734. Important
$500 Individual/$1,000 Family See the chart starting on page 2 for your costs for services this plan covers.
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.cvtrust.org or by calling 1-800-288-9870. Important Questions
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.cvtrust.org or by calling 1-800-288-9870. Important Questions
Important Questions Answers Why this Matters:
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.anthem.com or by calling 1-800-421-1880. Important Questions
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.anthem.com or by calling 1-800-421-1880. Important Questions
You don t have to meet deductibles for specific services, but see the chart starting on page 2 for other costs for services this plan covers.
 Massachusetts The Harvard Pilgrim HMO Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage Period: 01/01/2017 12/31/2017 Coverage for: Individual + Family Plan Type: HMO This
Massachusetts The Harvard Pilgrim HMO Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage Period: 01/01/2017 12/31/2017 Coverage for: Individual + Family Plan Type: HMO This
University of New Mexico
 University of New Mexico FY17 Open Enrollment Guide for Pre-65 Medical and Dental Plans Dates: May 4 May 20, 2016 Coverage Effective: July 1, 2016 June 30, 2017 Division of Human Resources Overview and
University of New Mexico FY17 Open Enrollment Guide for Pre-65 Medical and Dental Plans Dates: May 4 May 20, 2016 Coverage Effective: July 1, 2016 June 30, 2017 Division of Human Resources Overview and
Important Questions Answers Why this Matters:
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.anthem.com or by calling 1-855-603-7982. Important Questions
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.anthem.com or by calling 1-855-603-7982. Important Questions
Benefit Summary
 2018-2019 Benefit Summary Your Health Your Decision Welcome to your 2018-2019 Benefits Enrollment What s in the Guide? Enrollment Process....3 Medical........ 4 gap Plan.....5 Dental.....6 Vision... 7
2018-2019 Benefit Summary Your Health Your Decision Welcome to your 2018-2019 Benefits Enrollment What s in the Guide? Enrollment Process....3 Medical........ 4 gap Plan.....5 Dental.....6 Vision... 7
$0 See the chart starting on page 2 for your costs for services this plan covers.
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.paramount insurancecompany.com or by calling 1-800-462-3589
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.paramount insurancecompany.com or by calling 1-800-462-3589
What is the overall deductible? Are there other deductibles for specific services?
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.anthem.com or by calling 1-888-224-4902. Important Questions
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.anthem.com or by calling 1-888-224-4902. Important Questions
Anthem BlueCross BlueShield Anthem Lumenos HSA Plan /0 Summary of Benefits and Coverage:
 Anthem BlueCross BlueShield Anthem Lumenos HSA Plan 449 5000/0 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage Period: 11/01/2015-10/31/2016 Coverage For: Individual/Family
Anthem BlueCross BlueShield Anthem Lumenos HSA Plan 449 5000/0 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage Period: 11/01/2015-10/31/2016 Coverage For: Individual/Family