Provider Manual. Section 10: Pharmacy
|
|
|
- Diane Clark
- 6 years ago
- Views:
Transcription

1 Provider Manual Section 10: Pharmacy
2 Table of Contents SECTION 10: PHARMACY SERVICES PHARMACY FORMULARY FORMULARY ACCESS How to Use the Lexicomp Online Formulary SERVICES PROVIDED AND BENEFIT LIMITATIONS REQUESTING COVERAGE OF A NON-FORMULARY MEDICATION FOR AN INDIVIDUAL MEMBER Instructions for Completing Paper Request for Drug Coverage Forms: Request for Drug Coverage Form Request for Drug Coverage Form for COX-2 Inhibitor Use ADVERSE DRUG REACTION REPORTING Adverse Drug Reaction Report Form APPEAL PROCESS DISCOUNTS ON OVER-THE-COUNTER PRODUCTS SYNAGIS RSV Assessment Form MAIL ORDER PHARMACY GENERIC MEDICATION POLICY FIRST FILL PROCEDURE FOR KAISER PERMANENTE HEALTH MAINTENANCE ORGANIZATION (HMO) MEMBERS PLAN PHARMACIES Kaiser Permanente Medical Facility Pharmacy Directory
3 See Section 11 of this Manual for a description of Pharmacy Services for Self-Funded Plans Pharmacy Formulary Kaiser Permanente has two Formularies: Commercial and Medicare Part D. The medications included in the Kaiser Permanente Formularies are regulated by a group of Kaiser Permanente Practitioners, pharmacists and nurses known as the Pharmacy and Therapeutics Committee. This committee meets regularly to evaluate and choose medications that are most effective, safe and useful in caring for our Members. Using Formulary medications helps Kaiser Permanente maintain high quality of care for our Members, while helping to keep the cost of prescription medications affordable. Kaiser Permanente commercial plans use a closed Formulary, which means that only those medications included in the Kaiser Permanente Commercial Formulary are covered under the Member s prescription drug benefit. Members who choose to purchase a Non-formulary medication should expect to pay the full retail cost of the medication, unless issued a Formulary exception, also known as a prior authorization. Prescription drug coverage may vary, based upon the Member s health benefit plan. Not all Kaiser Permanente health plans include prescription drug coverage. Additionally, some prescription drug plans may exclude certain drugs, cover drugs at varying levels based upon drug cost or limit the amount of the drug the Member can receive with a prescription or Copayment. Members should consult their Evidence of Coverage (EOC) or call the Kaiser Permanente Customer Relations Department, Monday through Thursday, 8:15 a.m. to 5 p.m., and Friday, 9 a.m. to 5 p.m. at (toll free) for specific drug coverage information. The hearing/speech impaired may call (toll free TTY). The Kaiser Permanente Medicare Part D Formulary is a tiered, open Formulary. The Centers for Medicare & Medicaid Services (CMS) regulates this Formulary and requires Part D sponsors, like Kaiser Permanente, to include drug categories and classes that cover all disease states. The Kaiser Permanente Part D Formulary is developed nationally and approved by CMS. All Part D drugs qualified by Medicare are covered (except Medicare excluded drugs) and are on Kaiser Permanente s Medicare Part D Formulary. 3
4 2013 Kaiser Permanente Part D Design (CMS Approved) Tier Level Tier 1 Tier 2 Tier 3 Tier 4 Tier 5 Tier 6 Tier Name Value Generics (filed with CMS as preferred generics) Generics (filed with CMS as non-preferred generics) Brand Drugs (filed with CMS as preferred brand-name drugs) Non-Preferred Brand Drugs Specialty-Tier (no change) Injectable Part D Vaccines Kaiser Permanente Formularies are designed to meet the needs of the majority of our Members. The Pharmacy and Therapeutics Committee reviews and updates the Formularies throughout the year and notifies Plan Providers, pharmacists and other clinicians about any changes via Drug Therapy Advisories. Copies of Drug Therapy Advisories are available by calling your Network Associate, the Kaiser Permanente Customer Relations Department, Monday through Thursday, 8:15 a.m. to 5 p.m., and Friday, 9 a.m. to 5 p.m. at toll-free , option 1, or on the Kaiser Permanente Community Providers website at providers.kaiserpermanente.org/oh Formulary Access Contact your Network Associate or the Kaiser Permanente Customer Relations Department at toll-free , option 1, for a copy of current Kaiser Permanente Drug Formularies. Online access to the Kaiser Permanente Ohio Region Drug Formulary is also available through the Community Providers website at providers.kaiserpermanente.org/oh or Lexicomp Online. The Lexicomp Online Drug Formularies contains a search engine for easy information retrieval and convenient links to other Lexicomp Online references. Online Drug Formularies can be accessed through the internet at online.lexi.com/login (a login and password are required). Contact Regional Formulary Management Services at for information. Member drug Formularies are also available online at kp.org/formsandpubs. 4
5 How to Use the Lexicomp Online Formulary Login: Formulary Search: Formulary Information: Refined Search: Navigating Monograph Content: Access Mobile Device Software: Optional: Go to online.lexi.com/login Login: ohkprx Password: ohkprx From the opening screen, enter generic or brand drug name in the search box and click the Search button. To assist with searching, a possible keyword list will appear after you enter at least four characters. To select a suggested term, simply click on the desired search term and the system will automatically perform a search and display the results. To review the Ohio Formulary status of a drug, click on the hyperlink drug name listed under Kaiser Permanente Ohio Region database. Review the information in the respective Formulary Dosage Forms Covered fields within the drug monograph that opens in the right side frame. The formulary database monographs contain specific Kaiser Permanente Ohio information such as Formulary dosage forms, formulary restrictions, guidelines, and related information links. For many Non-formulary drugs, preferred Formulary alternatives may be listed in the Commercial Formulary field. Lexicomp Online allows users to perform a more refined search within a specific section of the monograph, by clicking the Limit search to drop-down arrow to view a list of possible sections that can be searched. To limit your search to a particular field, simply click on the desired listing from the drop-down list. Within a specific drug monograph window, Plan Providers can navigate the content quickly by using the Navigation Tree on the left side or the Jump To Section drop-down list on the top right. Click on the Mobile App Access link on the right of the Ohio Region Online Formulary home page for instructions to download the Lexicomp mobile device software. The Indexes button in the top left search frame may also be used to search the Kaiser Permanente Ohio Region database. This allows Plan Providers to view: A list of drugs starting with a selected letter by generic name or U.S. brand name. A list of available Charts/Special Topics or Freetext sections. All changes made in the past 7 to 30 days or new documents created in the last 90 days. A list of drugs in a specific pharmacology/therapeutic category. 5
6 10.3 Services Provided and Benefit Limitations Drugs are covered when prescriptions are required by Law and when they are listed in the Kaiser Permanente Formularies. This includes coverage for off-label Formulary drug usage in the treatment of a particular condition for a drug that is approved by the Food and Drug Administration and is recognized as safe and effective for that condition in published, authoritative medical, scientific, or pharmaceutical literature. The brand name form of a drug that appears on the Formulary will be provided only when the generic form is not available on the Formulary. Coverage of certain Formulary medications may be subject to restrictions established by the Pharmacy and Therapeutics Committee or by any federally mandated restrictions. If prescribed by a practitioner, a small number of non-prescription drugs (listed in the Kaiser Permanente Formularies) and accessories are also covered such as insulin and disposable insulin syringes/needles. Drugs and materials that must be administered by a practitioner, such as injections and tubing for administration of a drug, may be covered by the base medical benefit, not the Member s pharmacy benefit, and cannot be dispensed directly to the Member by an outpatient pharmacy. Drugs and accessories are covered only when Medically Necessary for treatment of a specific illness, injury or condition; prescribed by a practitioner or dentist; and obtained at pharmacies in Kaiser Permanente medical Facilities or at affiliated Plan pharmacies. Prescribed covered drugs and accessories are provided at a single Copayment for each prescription, not to exceed the amount prescribed, up to a 30-day supply except that, if the regular charge is less than the Copayment, Members pay the regular charge. Each prescription refill is provided on the same basis as the original prescription. If a prescription or refill is for a quantity greater than the limits described above, the charge is an additional Copayment for each multiple quantity or fraction of a 30-day supply. Kaiser Permanente reserves the right to dispense only a 30-day supply when the prescription or refill is of a quantity greater than a 30-day supply. Plan pharmacies provide up to a 30-day supply based upon the prescribed dosage, the standard manufacturer s package size, and specified dispensing limits. Some medications have other limitations on the amount or quantity of the drug that may be dispensed per prescription or Copayment. The following are not covered under the outpatient prescription drug benefit: Drugs when prescribed for cosmetic purposes. Drugs necessary for or related to an excluded service. Drugs used for the purpose of weight loss. Drugs and materials that require administration by medical personnel or observation by medical personnel during or after administration (these may be covered under the base medical benefit). Proton Pump Inhibitor drugs, unless Precertified for the treatment of Barretts Esophagitis and Zoellinger Syndrome. 6
7 Nonprescription drugs and medications, except for nonprescription nicotine replacement products covered under the Kaiser Permanente drug Formulary. Non-formulary nicotine replacement products. Investigational or experimental drugs or drugs limited to investigational use. Replacement of lost or damaged prescriptions. Unless an exception is approved by Health Plan, drugs not approved by the FDA and in general use as of March 1 st, of the year immediately preceding the year in which the Member s agreement became effective or was last renewed. Non-formulary drugs at the request of the Member, when a Plan Practitioner believes that the Formulary alternative is effective. Drugs used to enhance athletic performance. Medical supplies such as dressings and antiseptics (these may be covered under a supplemental Durable Medical Equipment benefit). Vitamins and nutritional supplements that can be purchased without a prescription. Medical foods. Special medication packaging, other than Health Plan standard packaging, unless required by Law. Drugs used to shorten the duration of the common cold. Drugs prescribed for the treatment of involuntary infertility or sexual dysfunction may or may not be covered, depending on the Member s drug benefit. Not all Kaiser Permanente health benefit plans include coverage for prescription drugs. Some Members have limitations on the dollar amount of coverage. Members should consult their Evidence of Coverage (EOC) booklet or call the Kaiser Permanente Customer Relations Department, Monday through Thursday, 8:15 a.m. to 5 p.m., and Friday, 9 a.m. to 5 p.m. at (toll free) for more information. The hearing/speech impaired may call (toll free TTY). See Section 4 of this Manual for more information regarding coverage for infertility drugs and contraception Requesting Coverage of a Non-Formulary Medication for an Individual Member Kaiser Permanente Formularies are designed to meet the needs of the majority of our Members. However, there are times when use of a Non-formulary drug is Medically Necessary. Prescriptions for Non-formulary medications may be filled at Kaiser Permanente pharmacies. However, the Member should expect to pay the full retail cost unless the prescribing Practitioner has obtained approval for the Non-formulary medication or the Member has a benefit that provides coverage at a higher Nonformulary Copayment. There may be a delay in filling the prescription because the pharmacy may need to place a special order. Coverage of certain Formulary medications may also be subject to restrictions established by the Regional Pharmacy and Therapeutics Committee. Non-formulary medications may be covered under the Formulary Exception Policy in the 7
8 same manner as Formulary drugs for commercial Members if: Formulary medications have proven ineffective, or the Formulary medication causes or is reasonably expected by the Plan Practitioner to cause harmful or adverse reactions, and the use conforms to guidelines and criteria reviewed and approved by the Pharmacy and Therapeutics Committee. All Non-formulary medications for commercial Members require Authorization through Kaiser Permanente s Pharmacy Utilization Management Service prior to dispensing to assure coverage by the Member s drug benefit. To seek approval for coverage of a Non-formulary drug for a Member, prescribing Practitioners will need to complete the Request for Drug Coverage form (see Section of this Manual). When requesting coverage of a COX-2 inhibitor, use the specific form for these drugs (see Section of this Manual). Both forms are also available from Pharmacy Utilization Management Service by calling (toll free) or , any Kaiser Permanente medical Facility pharmacy, MedImpact at (toll free), or online in the Forms section of the Kaiser Permanente Community Provider s website at providers.kaiserpermanente.org/oh. Plan Providers may submit Request for Drug Coverage forms to Kaiser Permanente electronically via KP Online-Affiliate. See Section of this Manual for more information regarding electronic communication options for Plan Providers. The purpose of completing the form is to document the Medical Necessity for using Non-formulary medication. Practitioners should complete the form using specific laboratory data, physical exam findings, and other supporting documentation whenever possible Instructions for Completing Paper Request for Drug Coverage Forms: 1. Provide all information requested. 2. Submit a separate form for each patient and for each drug you wish to have reviewed. 3. Keep a copy for your records. 4. Fax the form(s) to the Kaiser Permanente Utilization Management Service at OR mail the form(s) to: Kaiser Permanente Pharmacy Utilization Management Service 5500 Lancaster Drive Brooklyn Heights, OH
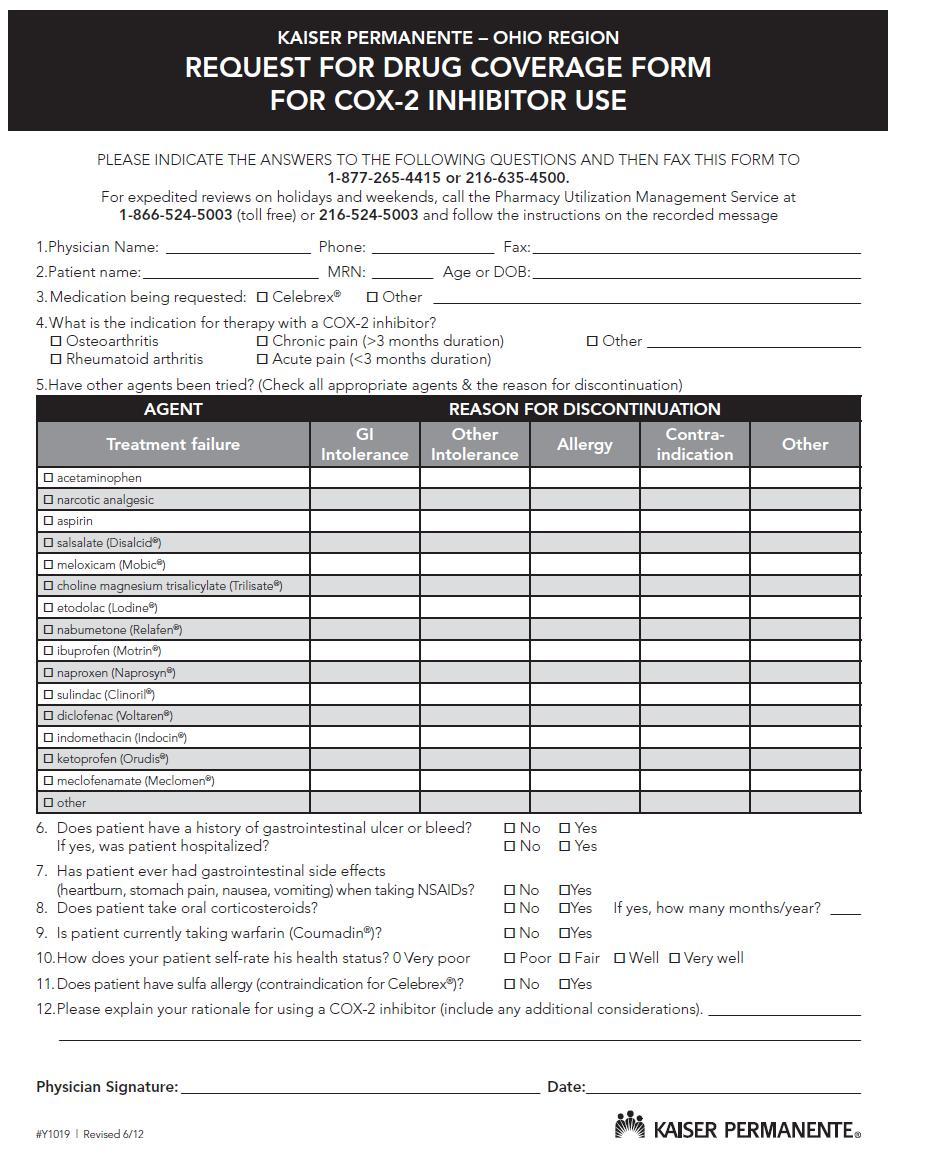
9 Requests will be processed within 15 calendar days from the time of receipt for Members with the Commercial Formulary drug benefit. Expedited requests may be made by calling the Pharmacy Utilization Management Service Center at (toll free) or The expedited process can take up to 24 hours for Members with the Commercial Formulary drug benefit. One of the following criteria must be met to make an expedited request: The drug is necessary to complete a specific course of therapy after discharge from an acute care facility. The time frame required for a standard review would compromise the Member s life, health or functional status. The drug requires administration in a time frame that will not be met using the standard process. Each request will be reviewed by the Pharmacy Utilization Management Service staff against criteria reviewed and approved by the Regional Pharmacy and Therapeutics Committee and the appropriate department Physician chiefs of the Ohio Permanente Medical Group (OPMG). Approvals will be granted only if the Practitioner can document the ineffectiveness of Formulary alternatives or the reasonable expectation of harm from the use of Formulary medications. In most cases, patients must have failed at least two Formulary alternatives or have experienced adverse effects from the use of the Formulary medications. If a request does not meet criteria, a pharmacist will recommend Formulary alternatives to the requesting Practitioner. However, if the requesting Practitioner disagrees with these recommendations, the request will be sent to a Pharmacy Utilization Management Service Center Practitioner for a decision. A response will be either faxed to the requesting Practitioner, if the form was submitted on paper, or via KP Online-Affiliate in response to electronic submissions. Members will be notified by mail. In most cases, approvals will be given an unlimited Authorization date, so that you will not be required to resubmit a request every year Request for Drug Coverage Form See the following page. 9
10 10
11 Request for Drug Coverage Form for COX-2 Inhibitor Use See the following page. 11
12 12
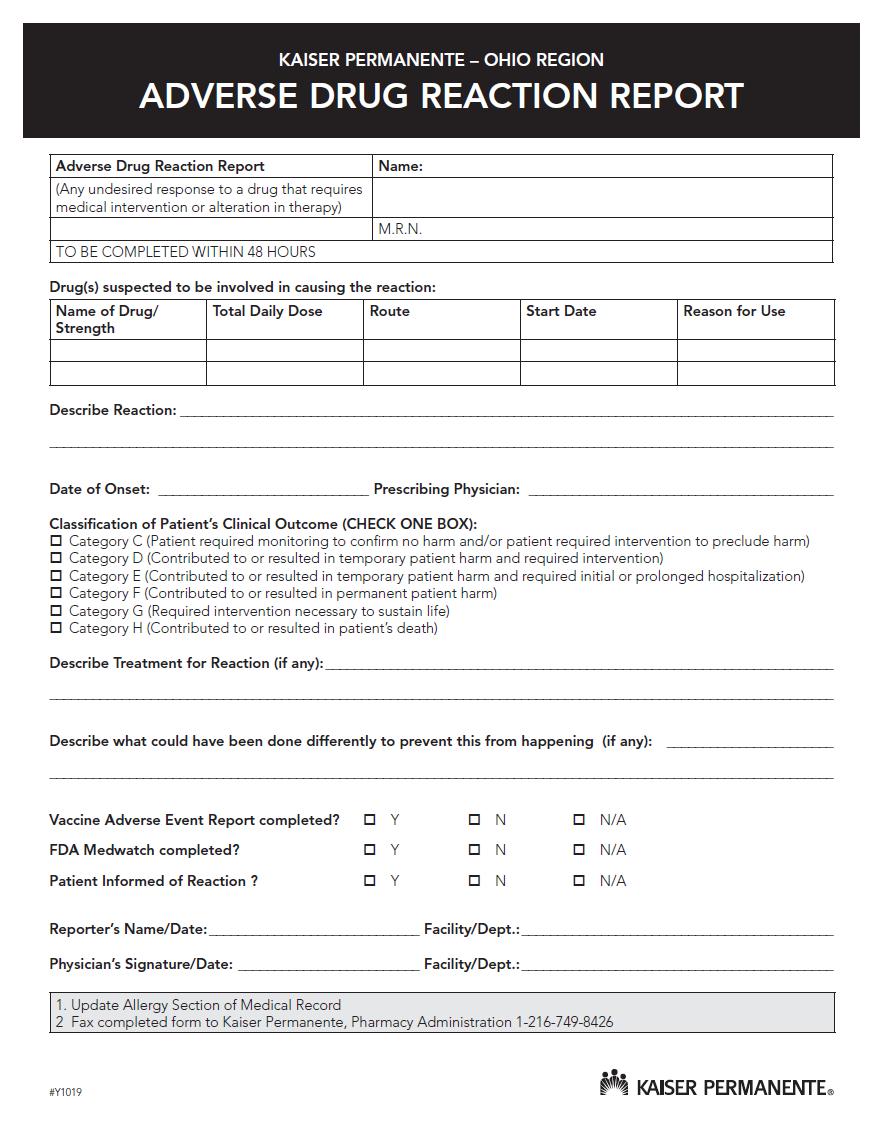
13 10.5 Adverse Drug Reaction Reporting An adverse drug reaction (ADR) is any non-preventable, unexpected, unintended, undesired, or excessive response to a medication (including allergic and idiosyncratic reactions) that: Requires discontinuing the medication (therapeutic or diagnostic). Requires changing the medication therapy. Requires modifying the dose (except for minor adjustments or dosage titration within normal limits). Necessitates admission to a hospital or clinical decision unit. Prolongs stay in a health care facility. Necessitates supportive treatment. Significantly complicates diagnosis. Negatively affects prognosis. Results in temporary or permanent patient harm, disability, or death. Example: a severe adverse reaction to penicillin in a patient with no prior allergic history or other contraindications. All new ADRs should be reported by the Plan Physician, nurse, or other health care provider by completely filling in the requested/applicable information concerning the reaction on the Adverse Drug Reaction Report form (see the following section of this manual). Plan Providers can download an Adverse Drug Reaction Report form in the Forms section of the Kaiser Permanente Community Provider s website at providers.kaiserpermanente.org/oh. Once the form is completed, signed, and dated, it should be faxed to Kaiser Permanente Pharmacy Administration at the number on the form. Pharmacy Administration staff will add noted allergies in the Kaiser Permanente electronic medical record system, HealthConnect, in an effort to prevent further prescribing of the drug. All information received on ADR forms is entered into an annual, cumulative spreadsheet for tracking and trending. In addition, the Kaiser Permanente Pharmacy Department computer system is updated. The Regional Pharmacy & Therapeutics Committee is responsible for reviewing quarterly summary reports and distributing recommendations and/or results as to Plan physicians and other professional staff Adverse Drug Reaction Report Form See the following page. 13
14 14
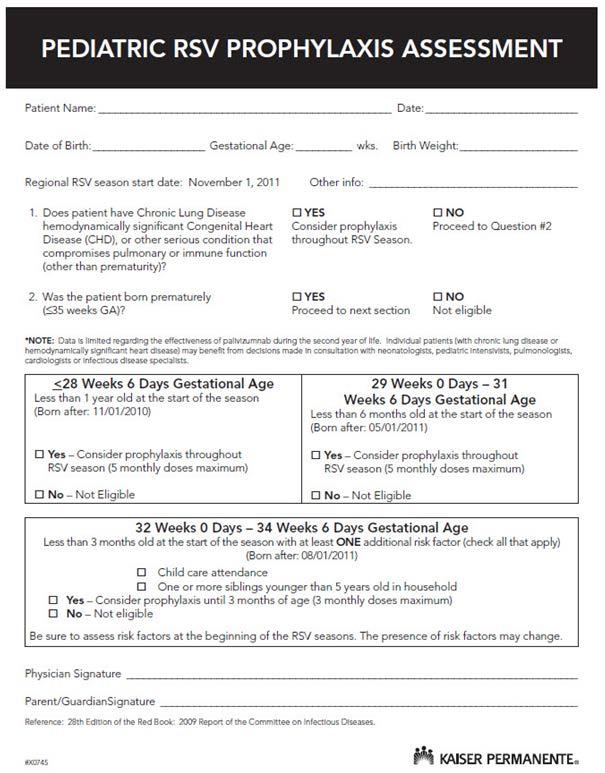
15 10.6 Appeal Process If coverage is denied, the prescribing Practitioner can appeal the decision by submitting written comments, documents, records and other information needed in the reconsideration process to: OR Kaiser Permanente Appeals Unit P.O. Box Cleveland, OH by contacting the Kaiser Permanente Appeals Unit at (toll free) or The prescribing Practitioner will be notified in writing as to the outcome of his/her Appeal. Additionally, a Member may file an appeal by contacting the Customer Relations Department, Monday through Thursday, 8:15 a.m. to 5 p.m., and Friday, 9 a.m. to 5 p.m. at (toll free). The hearing/speech impaired may call (toll free TTY) or See Section 4.12 of this Manual for more information regarding Member and Provider Appeal policies and Procedures Discounts on Over-the-Counter Products Pharmacies at Kaiser Permanente Medical Facilities offer a large selection of over-thecounter (OTC) products exclusively to our Members at very competitive prices. Some of the key OTC product categories include: Cough, cold and allergy. Gastrointestinal and digestive aids. Oral analgesics and pain relievers. Skin care items such as sunscreen, hydrocortisone, antibacterials, and antifungals. Vitamins including multiple and prenatal. Feminine products such as clotrimazole vaginal cream. A Kaiser Permanente pharmacist is available to answer Members questions and assist them in the selection of products to meet their health care needs Synagis Synagis injections are covered for Kaiser Permanente Members who meet American Academy of Pediatrics medical criteria. All Synagis injections must be Precertified. To Precertify a Synagis injection, complete a Kaiser Permanente Referrals Management and Clinical Review Referral form (see Section of this Manual) and attach a completed RSV Assessment form (see the following section of this Manual). Plan 15
16 Providers can download Referral and RSV Assessment forms in the Forms section of the Kaiser Permanente Community Provider s website at providers.kaiserpermanente.org/oh. Specify on the Referral form if you will: Administer the Synagis from your own supply, or order the Synagis from Kaiser Permanente s Advance Care Pharmacy for administration in your office, or direct the Member to a Synagis Clinic at a Kaiser Permanente medical Facility. Synagis Clinics are available at the Kaiser Permanente medical Facilities in Bedford, Chapel Hill, Cleveland Heights and Parma. Note: If you do not administer Synagis in your office, and the Member resides more than 30 miles from a Kaiser Permanente Synagis Clinic, Kaiser Permanente will consider authorizing injections from a Plan Home Health Care Provider. Fax the completed forms for review to the Referrals Management and Clinical Review Department at To order Synagis from Kaiser Permanente's Advanced Care Pharmacy (ACP) following receipt of your Authorization number, call , option 2, Monday through Friday, 8:30 a.m. to 5 p.m. and arrange for delivery to your office. After hours, call the pager at RSV Assessment Form See the following page. 16
17 17
18 10.9 Mail Order Pharmacy Members may be able to order larger quantities of maintenance medications through the Direct Mail Pharmacy for their mail order benefit Copayment. Not all prescriptions are available for mail order Service Generic Medication Policy Kaiser Permanente s Direct Mail Pharmacy 5500 Lancaster Drive Brooklyn Heights, OH Phone: (toll free) Kaiser Permanente has over 30 years experience in the successful use of generic drugs. Our comprehensive quality assurance program for the selection of drugs is managed by a group of experts with many years of experience in evaluating generic drugs. Kaiser Permanente pharmacies stock only generic products that have met the high standards of both the Food and Drug Administration and of Kaiser Permanente. Generic drugs offer Kaiser Permanente a means of providing quality care with a significant reduction in cost. These savings are directly passed on to our Members in the form of lower prescription prices and indirectly in lower membership rates. Medications selected for Formulary inclusion are in accordance with the principles of high quality pharmaceutical care and the standards set forth by the Kaiser Permanente National Drug Purchasing Department. Medications that are designated as Nonformulary are not covered under the drug benefit. Members pay the full Member cash price for the Non-formulary product unless a medical exception is approved. Prescribing Practitioners may prohibit generic substitution under Ohio s generic substitution Law. In this case, the pharmacist may not select and dispense a generic equivalent without Authorization from the prescriber. However, the corresponding Nonformulary brand will not be covered unless a medical exception has been approved. Members may request the Non-formulary brand name equivalent of a Formulary generic product. However, the Non-formulary brand will not be covered unless a medical exception has been approved or the Member has a tiered Copayment benefit under which it is covered at a higher Copayment First Fill Procedure for Kaiser Permanente Health Maintenance Organization (HMO) Members Effective January 1, 2012, in the event of an urgent/emergent situation or when a Kaiser Permanente Pharmacy is unavailable, Kaiser Permanente HMO Members can have prescription(s) filled one time each 365 days, per medication, per strength, at any Rite Aid or Walgreens Pharmacy within the Ohio Service Area. Members pay their standard 18
19 prescription Copayments for first fill medications. Formulary rules apply. Any subsequent prescriptions or refills required for the same strength medication during the next 365 days must be obtained through a Kaiser Permanente Plan or Mail Order Pharmacy. Members can easily order refills online at kp.org. See Section of this Manual for a list of Kaiser Permanente Plan Pharmacies Plan Pharmacies An ancillary directory with a listing of participating and Plan operated pharmacies is posted on the Kaiser Permanente s Community Provider s website at providers.kaiserpermanente.org/oh. If you prefer a paper directory, contact your Network Associate or the Kaiser Permanente Customer Relations Department, Monday through Thursday, 8:15 a.m. to 5 p.m., and Friday, 9 a.m. to 5 p.m. at toll-free , option Kaiser Permanente Medical Facility Pharmacy Directory See the following page. 19
20 KAISER PERMANENTE PHARMACY LOCATION Kaiser Permanente Avon Medical Offices American Way Avon, OH Kaiser Permanente Bedford Medical Offices Rockside Road Bedford, Ohio Kaiser Permanente Concord Medical Offices 7536 Fredle Drive Concord, Ohio Kaiser Permanente Fairlawn Medical Offices 4055 Embassy Parkway, Suite 110 Fairlawn, Ohio Kaiser Permanente Kent Medical Offices 2500 State Road 59, Suite 28 Kent, Ohio Kaiser Permanente Mentor Medical Offices 7695 Mentor Avenue Mentor, Ohio Kaiser Permanente Parma Medical Center Snow Road Parma, Ohio Kaiser Permanente Strongsville Medical Offices Royalton Road Strongsville, Ohio Kaiser Permanente Willoughby Medical Offices 5105 SOM Center Road Willoughby, Ohio PHONE NUMBER KAISER PERMANENTE PHARMACY LOCATION (toll free) Kaiser Permanente Chapel Hill Medical Offices 1260 Independence Avenue Akron, Ohio (toll free) Kaiser Permanente Cleveland Heights Medical Center 10 Severance Circle Cleveland, Ohio (toll free) Kaiser Permanente Direct Mail Pharmacy 5500 Lancaster Driver Brooklyn Heights, Ohio (toll free) Kaiser Permanente Home Infusion Pharmacy Snow Road Parma, Ohio (toll free) Kaiser Permanente Medina Medical Offices 3443 Medina Road, Suite 108 Medina, Ohio (toll free) Kaiser Permanente North Canton Medical Offices 4914 Portage St. NW North Canton, Ohio (toll free) Kaiser Permanente Rocky River Medical Offices Center Ridge Road, Suite 500 Rocky River, Ohio (toll free) Kaiser Permanente Twinsburg Medical Offices 8920 Canyon Falls Blvd., Suite 100 Twinsburg, Ohio (toll free) PHONE NUMBER (toll free) (toll free) (toll free) (toll free) (toll free) (toll free) (toll free) (toll free) 20
Provider Manual. Section 10: Pharmacy
 Provider Manual Section 10: Pharmacy Table of Contents SECTION 10: PHARMACY SERVICES... 3 10.1 PHARMACY FORMULARY... 3 10.2 FORMULARY ACCESS... 4 10.2.1 How to Use the Lexicomp Online Formulary... 5 10.3
Provider Manual Section 10: Pharmacy Table of Contents SECTION 10: PHARMACY SERVICES... 3 10.1 PHARMACY FORMULARY... 3 10.2 FORMULARY ACCESS... 4 10.2.1 How to Use the Lexicomp Online Formulary... 5 10.3
PHARMACY BENEFIT MEMBER BOOKLET
 PHARMACY BENEFIT MEMBER BOOKLET Printed on: VALUE, QUALITY AND CONFIDENCE Costco Health Solutions Customer Care HOURS: 24 Hours a Day 7 Days a Week (877) 908-6024 (toll-free) TTY 711 MAILING ADDRESS: Costco
PHARMACY BENEFIT MEMBER BOOKLET Printed on: VALUE, QUALITY AND CONFIDENCE Costco Health Solutions Customer Care HOURS: 24 Hours a Day 7 Days a Week (877) 908-6024 (toll-free) TTY 711 MAILING ADDRESS: Costco
Outpatient Prescription Drug Benefits
 Outpatient Prescription Drug Benefits Supplement to Your HMO/POS Evidence of Coverage Summary of Benefits Member Calendar Year Brand Drug Deductible Per Member Applicable to all covered Brand Drugs, including
Outpatient Prescription Drug Benefits Supplement to Your HMO/POS Evidence of Coverage Summary of Benefits Member Calendar Year Brand Drug Deductible Per Member Applicable to all covered Brand Drugs, including
See Medical Benefit Summary See Medical Benefit Summary
 Benefit Summary Outpatient Prescription Drug Products Oregon Plan I1 Standard Drugs: 15/30/50 Your Co-payment and/or Co-insurance is determined by the tier to which the Prescription Drug List (PDL) Management
Benefit Summary Outpatient Prescription Drug Products Oregon Plan I1 Standard Drugs: 15/30/50 Your Co-payment and/or Co-insurance is determined by the tier to which the Prescription Drug List (PDL) Management
See Medical Benefit Summary See Medical Benefit Summary
 Benefit Summary Outpatient Prescription Drug Products Illinois Plan MM Standard Drugs: 0/0/0 Your Co-payment and/or Co-insurance is determined by the tier to which the Prescription Drug List (PDL) Management
Benefit Summary Outpatient Prescription Drug Products Illinois Plan MM Standard Drugs: 0/0/0 Your Co-payment and/or Co-insurance is determined by the tier to which the Prescription Drug List (PDL) Management
See Medical Benefit Summary. See Medical Benefit Summary
 YOUR BENEFITS Benefit Summary Outpatient Prescription Drug Copper PPO Pharmacy Plan Standard Retail Network With CVS This document is provided as a sample and does not reflect actual benefits. A customized
YOUR BENEFITS Benefit Summary Outpatient Prescription Drug Copper PPO Pharmacy Plan Standard Retail Network With CVS This document is provided as a sample and does not reflect actual benefits. A customized
Value Three-Tier EFFECTIVE DATE: 01/01/2016 FORM #1779_03
 Value Three-Tier This brochure is a legal document that explains the prescription drug benefits provided by Harvard Pilgrim Health Care, Inc. (HPHC) to Members with plans that include outpatient pharmacy
Value Three-Tier This brochure is a legal document that explains the prescription drug benefits provided by Harvard Pilgrim Health Care, Inc. (HPHC) to Members with plans that include outpatient pharmacy
Blue Shield of California Life & Health Insurance Company
 Blue Shield of California Life & Health Insurance Company Outpatient Prescription Drug Benefit Rider Insurance Certificate Outpatient Prescription Drug Benefit Summary of Benefits Insured Calendar Year
Blue Shield of California Life & Health Insurance Company Outpatient Prescription Drug Benefit Rider Insurance Certificate Outpatient Prescription Drug Benefit Summary of Benefits Insured Calendar Year
The Health Plan has processes in place that explain how members, pharmacists, and physicians:
 Introduction Overview The Health Plan shall promote optimal therapeutic use of pharmaceuticals by encouraging the use of cost effective generic and/or brand drugs in certain therapeutic classes. The Health
Introduction Overview The Health Plan shall promote optimal therapeutic use of pharmaceuticals by encouraging the use of cost effective generic and/or brand drugs in certain therapeutic classes. The Health
See Medical Benefit Summary See Medical Benefit Summary. See Medical Benefit Summary See Medical Benefit Summary. Up to 31-day supply
 YOUR BENEFITS Benefit Summary Outpatient Prescription Drug Keller ISD High Deductible 2019 Pharmacy Plan This document is provided as a sample and does not reflect actual benefits. A customized Benefit
YOUR BENEFITS Benefit Summary Outpatient Prescription Drug Keller ISD High Deductible 2019 Pharmacy Plan This document is provided as a sample and does not reflect actual benefits. A customized Benefit
Primary Choice Plan Premium Three-Tier
 Primary Choice Plan Premium Three-Tier This brochure is a legal document that explains the prescription drug benefits provided by the Group Insurance Commission (GIC) to their Members on a self-insured
Primary Choice Plan Premium Three-Tier This brochure is a legal document that explains the prescription drug benefits provided by the Group Insurance Commission (GIC) to their Members on a self-insured
Provider Manual Section 12.0 Outpatient Pharmacy Services
 Provider Manual Section 12.0 Outpatient Pharmacy Services Table of Contents 12.1 Prescribing Outpatient Medications for Enrollees 12.2 Prescription Medications & Prior Authorization 12.3 Pharmacy Lock-In
Provider Manual Section 12.0 Outpatient Pharmacy Services Table of Contents 12.1 Prescribing Outpatient Medications for Enrollees 12.2 Prescription Medications & Prior Authorization 12.3 Pharmacy Lock-In
Overview of the BCBSRI Prescription Management Program
 Overview of the BCBSRI Prescription Management Program A. Prescription Drugs Dispensed at a Pharmacy This plan covers prescription drugs listed on the Blue Cross & Blue Shield RI (BCBSRI) formulary and
Overview of the BCBSRI Prescription Management Program A. Prescription Drugs Dispensed at a Pharmacy This plan covers prescription drugs listed on the Blue Cross & Blue Shield RI (BCBSRI) formulary and
See Medical Benefit Summary See Medical Benefit Summary. See Medical Benefit Summary See Medical Benefit Summary
 Benefit Summary Outpatient Prescription Drug Missouri 10/35/60 Plan 2V Your Co-payment and/or Co-insurance is determined by the tier to which the Prescription Drug List (PDL) Management Committee has assigned
Benefit Summary Outpatient Prescription Drug Missouri 10/35/60 Plan 2V Your Co-payment and/or Co-insurance is determined by the tier to which the Prescription Drug List (PDL) Management Committee has assigned
Sharp Health Plan Outpatient Prescription Drug Benefit
 Sharp Health Plan Outpatient Prescription Drug Benefit GENERAL INFORMATION This supplemental Evidence of Coverage and Disclosure Form is provided in addition to your Member Handbook and Health Plan Benefits
Sharp Health Plan Outpatient Prescription Drug Benefit GENERAL INFORMATION This supplemental Evidence of Coverage and Disclosure Form is provided in addition to your Member Handbook and Health Plan Benefits
Prescription Drug Brochure
 Value Five-Tier Prescription Drug Brochure This brochure is a legal document that explains the prescription drug benefits provided by Harvard Pilgrim Health Care, Inc. (HPHC) to Members with plans that
Value Five-Tier Prescription Drug Brochure This brochure is a legal document that explains the prescription drug benefits provided by Harvard Pilgrim Health Care, Inc. (HPHC) to Members with plans that
Benefit Summary. Outpatient Prescription Drug Products Virginia Plan 2V Standard Drugs: 10/35/60. Annual Drug Deductible - Network and Out-of-Network
 Benefit Summary Outpatient Prescription Drug Products Virginia Plan 2V Standard Drugs: 10/35/60 Your Co-payment and/or Co-insurance is determined by the tier to which the Prescription Drug List (PDL) Management
Benefit Summary Outpatient Prescription Drug Products Virginia Plan 2V Standard Drugs: 10/35/60 Your Co-payment and/or Co-insurance is determined by the tier to which the Prescription Drug List (PDL) Management
Prominence Health Plan. Pharmacy Benefits Guide Program Overview
 Prominence Health Plan Pharmacy Benefits Guide Program Overview January 2016 PROMINENCE HEALTH PLAN PHARMACY BENEFITS GUIDE Contents FORWARD 2 REFERENCE DOCUMENTS 2 FORMULARY 2 GENERIC DRUGS FREQUENTLY
Prominence Health Plan Pharmacy Benefits Guide Program Overview January 2016 PROMINENCE HEALTH PLAN PHARMACY BENEFITS GUIDE Contents FORWARD 2 REFERENCE DOCUMENTS 2 FORMULARY 2 GENERIC DRUGS FREQUENTLY
Prescription Drug Coverage
 The Company s medical plans automatically include coverage for prescription drugs which is administered by Envision Pharmaceutical Services, Inc. (Envision Rx) for prescriptions filled at retail pharmacies
The Company s medical plans automatically include coverage for prescription drugs which is administered by Envision Pharmaceutical Services, Inc. (Envision Rx) for prescriptions filled at retail pharmacies
10.1 Summary Prescription drug coverage for you and your eligible Dependents Three-tier Copayment plan Retail and maintenance programs
 10.1 Summary Prescription drug coverage for you and your eligible Dependents Three-tier Copayment plan Retail and maintenance programs Through the Prescription Drug Plan, you and your eligible Dependents
10.1 Summary Prescription drug coverage for you and your eligible Dependents Three-tier Copayment plan Retail and maintenance programs Through the Prescription Drug Plan, you and your eligible Dependents
Blue Essentials, Blue Advantage HMO SM and Blue Premier SM Provider Manual - Pharmacy
 Blue Essentials, Blue Advantage HMO SM and Blue Premier SM Provider Manual - In this Section there are references unique to Blue Essentials, Blue Advantage HMO and Blue Premier. These network specific
Blue Essentials, Blue Advantage HMO SM and Blue Premier SM Provider Manual - In this Section there are references unique to Blue Essentials, Blue Advantage HMO and Blue Premier. These network specific
Chapter 10 Prescriptions Benefits and Drug Formulary
 10 Prescription Benefits and Drug Formulary Health Choice Generations is a Medicare Advantage Special Needs Plan (SNP) with Medicare Part D Prescription Drug Coverage. Medicare Part D drugs covered by
10 Prescription Benefits and Drug Formulary Health Choice Generations is a Medicare Advantage Special Needs Plan (SNP) with Medicare Part D Prescription Drug Coverage. Medicare Part D drugs covered by
PLAN DESIGN AND BENEFITS PROVIDED BY AETNA LIFE INSURANCE COMPANY
 Benefits and Premiums are effective January 01, 2018 through December 31, 2018 PHARMACY - PRESCRIPTION DRUG BENEFITS PLAN DESIGN AND BENEFITS PROVIDED BY AETNA LIFE INSURANCE COMPANY Prescription drug
Benefits and Premiums are effective January 01, 2018 through December 31, 2018 PHARMACY - PRESCRIPTION DRUG BENEFITS PLAN DESIGN AND BENEFITS PROVIDED BY AETNA LIFE INSURANCE COMPANY Prescription drug
Provider Manual Amendments
 Amendments L.A. Care Health Plan Revised 11/2015 lacare.org LA1478 11/15 16.0 Pharmacy Overview L.A. Care s prescription drug formulary is designed to support the achievement of positive member health
Amendments L.A. Care Health Plan Revised 11/2015 lacare.org LA1478 11/15 16.0 Pharmacy Overview L.A. Care s prescription drug formulary is designed to support the achievement of positive member health
Get the most from your
 Get the most from your FOREIGN SERVICE BENEFIT PLAN (FSBP) Welcome to Express Scripts What s Inside Your benefit at a glance...2 FSBP s preferred medicines...2 Coverage limits...3 Home delivery overseas...5
Get the most from your FOREIGN SERVICE BENEFIT PLAN (FSBP) Welcome to Express Scripts What s Inside Your benefit at a glance...2 FSBP s preferred medicines...2 Coverage limits...3 Home delivery overseas...5
SHARP HEALTH PLAN MEDICARE ADVANTAGE POLICY AND PROCEDURE Product Line (check all that apply):
:") SHARP HEALTH PLAN MEDICARE ADVANTAGE POLICY AND PROCEDURE Product Line (check all that apply): Title: SHP Pharmacy Management Policy and Procedure for Part D Coverage Determination All Group HMO Individual
SHARP HEALTH PLAN MEDICARE ADVANTAGE POLICY AND PROCEDURE Product Line (check all that apply): Title: SHP Pharmacy Management Policy and Procedure for Part D Coverage Determination All Group HMO Individual
SecurityBlue HMO. Link to Specific Guidance Regarding Exceptions and Appeals
 SecurityBlue HMO Conditions and Limitations Potential for Contract Termination Disenrollment Rights and Instructions Exceptions, Prior Authorization, Appeals and Grievances Out-of-Network Coverage Quality
SecurityBlue HMO Conditions and Limitations Potential for Contract Termination Disenrollment Rights and Instructions Exceptions, Prior Authorization, Appeals and Grievances Out-of-Network Coverage Quality
Kroll Ontrack, LLC Prescription Drug Plan. Plan Document and Summary Plan Description
 Kroll Ontrack, LLC Prescription Drug Plan Plan Document and Summary Plan Description Effective December 9, 2016 Kroll Ontrack, LLC reserves the right to amend the Kroll Ontrack, LLC Health & Welfare Plan
Kroll Ontrack, LLC Prescription Drug Plan Plan Document and Summary Plan Description Effective December 9, 2016 Kroll Ontrack, LLC reserves the right to amend the Kroll Ontrack, LLC Health & Welfare Plan
UnitedHealthcare SignatureValue TM Offered by UnitedHealthcare of California Pharmacy Schedule of Benefits
 CALIFORNIA UnitedHealthcare SignatureValue TM Offered by UnitedHealthcare of California Pharmacy Schedule of Benefits (FOR HSA-QUALIFIED DEDUCTIBLE PLANS) Summary of Benefits Retail Pharmacy Copayment
CALIFORNIA UnitedHealthcare SignatureValue TM Offered by UnitedHealthcare of California Pharmacy Schedule of Benefits (FOR HSA-QUALIFIED DEDUCTIBLE PLANS) Summary of Benefits Retail Pharmacy Copayment
APPENDIX B: VENDOR DRUG PROGRAM TEXAS MEDICAID PROVIDER PROCEDURES MANUAL: VOL. 1
 APPENDIX B: VENDOR DRUG PROGRAM TEXAS MEDICAID PROVIDER PROCEDURES MANUAL: VOL. 1 APRIL 2018 TEXAS MEDICAID PROVIDER PROCEDURES MANUAL: VOL. 1 APRIL 2018 APPENDIX B: VENDOR DRUG PROGRAM Table of Contents
APPENDIX B: VENDOR DRUG PROGRAM TEXAS MEDICAID PROVIDER PROCEDURES MANUAL: VOL. 1 APRIL 2018 TEXAS MEDICAID PROVIDER PROCEDURES MANUAL: VOL. 1 APRIL 2018 APPENDIX B: VENDOR DRUG PROGRAM Table of Contents
Annual Notice of Changes for 2018
 Kaiser Permanente Senior Advantage Hawaii Island (HMO) offered by Kaiser Foundation Health Plan, Inc., Hawaii Region Annual Notice of Changes for 2018 You are currently enrolled as a member of Kaiser Permanente
Kaiser Permanente Senior Advantage Hawaii Island (HMO) offered by Kaiser Foundation Health Plan, Inc., Hawaii Region Annual Notice of Changes for 2018 You are currently enrolled as a member of Kaiser Permanente
Prescription Benefits State of Maryland. CVS Caremark manages your prescription drug benefit under a contract with the State of Maryland.
 Prescription Benefits State of Maryland CVS Caremark manages your prescription drug benefit under a contract with the State of Maryland. Introduction This Prescription Benefit document describes how to
Prescription Benefits State of Maryland CVS Caremark manages your prescription drug benefit under a contract with the State of Maryland. Introduction This Prescription Benefit document describes how to
21 - Pharmacy Services
 21 - Pharmacy Services The role of Health Plan of Nevada s (HPN) Pharmacy Services is to evaluate and determine the appropriateness of quality drug therapy while maintaining and improving therapeutic outcomes.
21 - Pharmacy Services The role of Health Plan of Nevada s (HPN) Pharmacy Services is to evaluate and determine the appropriateness of quality drug therapy while maintaining and improving therapeutic outcomes.
Your Prescription Drug
 Your Prescription Drug BENEFIT PROGRAM This prescription drug benefit program provides pharmacy coverage for you and your family. P r e s c ription Dru g Covered benefits Coverage* includes self-administered
Your Prescription Drug BENEFIT PROGRAM This prescription drug benefit program provides pharmacy coverage for you and your family. P r e s c ription Dru g Covered benefits Coverage* includes self-administered
SBCFF Modified Rx 10/30/45 Prescription Drug Benefits
 Rx Benefits SBCFF Modified Rx 10/30/45 Prescription Drug Benefits This summary of benefits has been updated to comply with federal and state requirements, including applicable provisions of the recently
Rx Benefits SBCFF Modified Rx 10/30/45 Prescription Drug Benefits This summary of benefits has been updated to comply with federal and state requirements, including applicable provisions of the recently
Princeton University Prescription Drug Plan Summary Plan Description
 Princeton University Prescription Drug Plan Summary Plan Description Princeton University Prescription Drug Plan Summary Plan Description January 2018 Introduction... 1 How the Plan Works... 2 Formulary...
Princeton University Prescription Drug Plan Summary Plan Description Princeton University Prescription Drug Plan Summary Plan Description January 2018 Introduction... 1 How the Plan Works... 2 Formulary...
POLICY STATEMENT: PROCEDURE:
 PAGE 1 OF 12 POLICY STATEMENT: NPS shall provide an automated process to assist beneficiaries who are transitioning from drug regimens or therapies that are not covered on the Part D Plan S are on the
PAGE 1 OF 12 POLICY STATEMENT: NPS shall provide an automated process to assist beneficiaries who are transitioning from drug regimens or therapies that are not covered on the Part D Plan S are on the
HOW TO MAKE A COMPLAINT, REQUEST A COVERAGE DECISION,
 OPTIMA MEDICARE HMO HOW TO MAKE A COMPLAINT, REQUEST A COVERAGE DECISION, OR FILE AN APPEAL ABOUT COVERED MEDICARE PART C MEDICAL CARE AND SERVICES OR COVERED PART D PRESCRIPTION DRUGS Optima Medicare
OPTIMA MEDICARE HMO HOW TO MAKE A COMPLAINT, REQUEST A COVERAGE DECISION, OR FILE AN APPEAL ABOUT COVERED MEDICARE PART C MEDICAL CARE AND SERVICES OR COVERED PART D PRESCRIPTION DRUGS Optima Medicare
Keystone 65 Part D Rider An Addendum to Your Evidence of Coverage
 Keystone 65 Part D Rider An Addendum to Your Evidence of Coverage Effective January 1, 2008 through December 31, 2008 1-800-645-3965 TTY/TDD: 1-888-857-4816 Seven days a week 8 a.m. 8 p.m. Benefits underwritten
Keystone 65 Part D Rider An Addendum to Your Evidence of Coverage Effective January 1, 2008 through December 31, 2008 1-800-645-3965 TTY/TDD: 1-888-857-4816 Seven days a week 8 a.m. 8 p.m. Benefits underwritten
Prescription Medication Schedule of Benefits
 Prescription Medication Schedule of Benefits Rx Member Cost-Sharing: $15/$35/$70/$70 When you go to a pharmacy that participates in the UPMC Health Plan pharmacy network, you will be able to receive coverage
Prescription Medication Schedule of Benefits Rx Member Cost-Sharing: $15/$35/$70/$70 When you go to a pharmacy that participates in the UPMC Health Plan pharmacy network, you will be able to receive coverage
PRESCRIPTION DRUG EXPENSE BENEFIT 2019
 PRESCRIPTION DRUG EXPENSE BENEFIT 2019 Welcome to the Prescription Drug benefit, administered by Express Scripts, Inc. (ESI). To receive the highest level of benefits, prescription drugs must be obtained
PRESCRIPTION DRUG EXPENSE BENEFIT 2019 Welcome to the Prescription Drug benefit, administered by Express Scripts, Inc. (ESI). To receive the highest level of benefits, prescription drugs must be obtained
Summary of Benefit Plan Changes and Clarifications
 July 2006 Summary of Benefit Plan Changes and Clarifications Retired Employees Formerly Represented by IAM 725, SPFPA 159 and 160, IUOE 501 (Weldors) and 501 (Engineers), AFSO 1/SPFPA, DASO, and IBT 848
July 2006 Summary of Benefit Plan Changes and Clarifications Retired Employees Formerly Represented by IAM 725, SPFPA 159 and 160, IUOE 501 (Weldors) and 501 (Engineers), AFSO 1/SPFPA, DASO, and IBT 848
Prescription Drug Rider
 Prescription Drug Rider Rx Member Cost-Sharing: $10/$25/$40/$40 According to this prescription drug program, you may receive coverage for prescription drugs in the amounts specified in your rider when
Prescription Drug Rider Rx Member Cost-Sharing: $10/$25/$40/$40 According to this prescription drug program, you may receive coverage for prescription drugs in the amounts specified in your rider when
Prescription Drug Schedule of Benefits
 Prescription Drug Schedule of Benefits Rx Member Cost-Sharing: $5/$15/$35/$35 When you go to a pharmacy that participates in the UPMC Health Plan pharmacy network, you will be able to receive coverage
Prescription Drug Schedule of Benefits Rx Member Cost-Sharing: $5/$15/$35/$35 When you go to a pharmacy that participates in the UPMC Health Plan pharmacy network, you will be able to receive coverage
We re happy you ve chosen a BlueMedicare Preferred HMO plan for your health care needs.
 Dear Valued Member, We re happy you ve chosen a BlueMedicare Preferred HMO plan for your health care needs. We ve enclosed your BlueMedicare Preferred HMO Owner s Manual. This helpful guide explains how
Dear Valued Member, We re happy you ve chosen a BlueMedicare Preferred HMO plan for your health care needs. We ve enclosed your BlueMedicare Preferred HMO Owner s Manual. This helpful guide explains how
BlueRx PDP. Link to Specific Guidance Regarding Exceptions and Appeals
 BlueRx PDP Conditions and Limitations Potential for Contract Termination Disenrollment Rights and Instructions Exceptions, Prior Authorization, Appeals and Grievances Out-of-Network Coverage Quality Assurance
BlueRx PDP Conditions and Limitations Potential for Contract Termination Disenrollment Rights and Instructions Exceptions, Prior Authorization, Appeals and Grievances Out-of-Network Coverage Quality Assurance
Prescription Medication Rider
 Prescription Medication Rider Rx Member Cost-Sharing: $16/$40/$80/$90 According to this prescription medication program, you may receive coverage for prescription medications in the amounts specified in
Prescription Medication Rider Rx Member Cost-Sharing: $16/$40/$80/$90 According to this prescription medication program, you may receive coverage for prescription medications in the amounts specified in
APPENDIX B: VENDOR DRUG PROGRAM TEXAS MEDICAID PROVIDER PROCEDURES MANUAL: VOL. 1
 APPENDIX B: VENDOR DRUG PROGRAM TEXAS MEDICAID PROVIDER PROCEDURES MANUAL: VOL. 1 DECEMBER 2016 TEXAS MEDICAID PROVIDER PROCEDURES MANUAL: VOL. 1 DECEMBER 2016 APPENDIX B: VENDOR DRUG PROGRAM Table of
APPENDIX B: VENDOR DRUG PROGRAM TEXAS MEDICAID PROVIDER PROCEDURES MANUAL: VOL. 1 DECEMBER 2016 TEXAS MEDICAID PROVIDER PROCEDURES MANUAL: VOL. 1 DECEMBER 2016 APPENDIX B: VENDOR DRUG PROGRAM Table of
Classification: Clinical Department Policy Number: Subject: Medicare Part D General Transition
 Classification: Clinical Department Policy Number: 3404.00 Subject: Medicare Part D General Transition Effective Date: 01/01/2019 Process Date Revised: 07/20/2018 Date Reviewed: 05/29/2018 POLICY STATEMENT:
Classification: Clinical Department Policy Number: 3404.00 Subject: Medicare Part D General Transition Effective Date: 01/01/2019 Process Date Revised: 07/20/2018 Date Reviewed: 05/29/2018 POLICY STATEMENT:
Your Pharmacy Benefits Handbook
 Your Pharmacy Benefits Handbook Summary of FCPS Prescription Benefits Available Through CVS Caremark Pharmacy Benefit Manager for Aetna/Innovation Health and CareFirst BlueChoice Advantage Plans Plan Year
Your Pharmacy Benefits Handbook Summary of FCPS Prescription Benefits Available Through CVS Caremark Pharmacy Benefit Manager for Aetna/Innovation Health and CareFirst BlueChoice Advantage Plans Plan Year
PHARMACY GENERAL INFORMATION
 Pharmacy Program Cenpatico Integrated Care (Cenpatico IC) is committed to providing appropriate high quality and cost-effective medication therapy to all Cenpatico IC members. Cenpatico IC works with providers
Pharmacy Program Cenpatico Integrated Care (Cenpatico IC) is committed to providing appropriate high quality and cost-effective medication therapy to all Cenpatico IC members. Cenpatico IC works with providers
Health Plan of Marathon Oil Company Prescription Drug Program Choice Plus Traditional Option
 Health Plan of Marathon Oil Company Prescription Drug Program Choice Plus Traditional Option This summary plan description constitutes part of the Health Plan of Marathon Oil Company plan document along
Health Plan of Marathon Oil Company Prescription Drug Program Choice Plus Traditional Option This summary plan description constitutes part of the Health Plan of Marathon Oil Company plan document along
TRANSITION POLICY. Members Health Insurance Company
 Members Health Insurance Company TRANSITION POLICY POLICY The Company will maintain an appropriate transition process, consistent with 42 CFR 423.120(b)(3), Chapter 6 of the Medicare Prescription Drug
Members Health Insurance Company TRANSITION POLICY POLICY The Company will maintain an appropriate transition process, consistent with 42 CFR 423.120(b)(3), Chapter 6 of the Medicare Prescription Drug
Medicare Transition POLICY AND PROCEDURES
 Medicare Transition POLICY AND PROCEDURES POLICY The Plan will maintain an appropriate transition process, consistent with 42 CFR 423.120(b)(3), Chapter 6 of the Medicare Prescription Drug Benefit Manual
Medicare Transition POLICY AND PROCEDURES POLICY The Plan will maintain an appropriate transition process, consistent with 42 CFR 423.120(b)(3), Chapter 6 of the Medicare Prescription Drug Benefit Manual
Summary Plan Description Accenture Prescription Drug Plan
 Summary Plan Description Accenture Prescription Drug Plan Effective January 1, 2018 Group Number: ACCRXS1 TABLE OF CONTENTS SECTION 1 - WELCOME... 1 SECTION 2 PLAN HIGHLIGHTS... 3 SECTION 3 - ADDITIONAL
Summary Plan Description Accenture Prescription Drug Plan Effective January 1, 2018 Group Number: ACCRXS1 TABLE OF CONTENTS SECTION 1 - WELCOME... 1 SECTION 2 PLAN HIGHLIGHTS... 3 SECTION 3 - ADDITIONAL
For: Choice POS II - Clerical & Technical and Service & Maintenance Employees Choice POS II (Base Rx) Plan
 Plan") Schedule of Benefits Employer: Yale University ASA: 877076 Issue Date: June 23, 2016 Effective Date: January 1, 2016 Schedule: 2A Booklet Base: 2 For: Choice POS II - Clerical & Technical and Service &
Schedule of Benefits Employer: Yale University ASA: 877076 Issue Date: June 23, 2016 Effective Date: January 1, 2016 Schedule: 2A Booklet Base: 2 For: Choice POS II - Clerical & Technical and Service &
About Kaiser Permanente Medicare Advantage Standard DC
 Kaiser Permanente Medicare Advantage Standard DC (HMO) offered by Kaiser Foundation Health Plan of the Mid-Atlantic States, Inc. Annual Notice of Changes for 2019 You are currently enrolled as a member
Kaiser Permanente Medicare Advantage Standard DC (HMO) offered by Kaiser Foundation Health Plan of the Mid-Atlantic States, Inc. Annual Notice of Changes for 2019 You are currently enrolled as a member
Chapter 8 Section 9.1
 Other Services Chapter 8 Section 9.1 Issue Date: August 2002 Authority: 32 CFR 199.2(b), 32 CFR 199.4(b)(2)(vi), (b)(3)(iii), (b)(5)(v), (d)(3)(vi), (e)(11)(i), 32 CFR 199.5(d)(12); 32 CFR 199.17, and
Other Services Chapter 8 Section 9.1 Issue Date: August 2002 Authority: 32 CFR 199.2(b), 32 CFR 199.4(b)(2)(vi), (b)(3)(iii), (b)(5)(v), (d)(3)(vi), (e)(11)(i), 32 CFR 199.5(d)(12); 32 CFR 199.17, and
CHAPTER 8 Section 9.1, pages 1 through 7 Section 9.1, pages 1 through 7. CHAPTER 10 Section 7.1, pages 1 and 2 Section 7.
 CHANGE 20 6010.60-M MAY 3, 2018 REMOVE PAGE(S) INSERT PAGE(S) CHAPTER 8 Section 9.1, pages 1 through 7 Section 9.1, pages 1 through 7 CHAPTER 10 Section 7.1, pages 1 and 2 Section 7.1, pages 1 and 2 2
CHANGE 20 6010.60-M MAY 3, 2018 REMOVE PAGE(S) INSERT PAGE(S) CHAPTER 8 Section 9.1, pages 1 through 7 Section 9.1, pages 1 through 7 CHAPTER 10 Section 7.1, pages 1 and 2 Section 7.1, pages 1 and 2 2
Benefits and Premiums are effective January 01, 2018 through December 31, 2018 PLAN DESIGN AND BENEFITS PROVIDED BY AETNA LIFE INSURANCE COMPANY
 PHARMACY - PRESCRIPTION DRUG BENEFITS Prescription drug calendar year deductible $0 Prescription drug calendar year deductible must be satisfied before any Medicare Prescription Drug benefits are paid.
PHARMACY - PRESCRIPTION DRUG BENEFITS Prescription drug calendar year deductible $0 Prescription drug calendar year deductible must be satisfied before any Medicare Prescription Drug benefits are paid.
Prescription Medication Rider
 Prescription Medication Rider Rx Member Cost-Sharing: $16/$40/$80/$90 HealthyU HIA/HRA According to this prescription medication program, you may receive coverage for prescription medications in the amounts
Prescription Medication Rider Rx Member Cost-Sharing: $16/$40/$80/$90 HealthyU HIA/HRA According to this prescription medication program, you may receive coverage for prescription medications in the amounts
EVIDENCE OF COVERAGE:
 EVIDENCE OF COVERAGE: Your Medicare Prescription Drug Coverage as a Member of Medi-Pak Rx Premier January 1 December 31, 2008. This booklet gives the details about your Medicare prescription drug coverage
EVIDENCE OF COVERAGE: Your Medicare Prescription Drug Coverage as a Member of Medi-Pak Rx Premier January 1 December 31, 2008. This booklet gives the details about your Medicare prescription drug coverage
Benefits and Premiums are effective January 01, 2017 through December 31, This is what you pay for Network & Out-of-Network Providers $0
 Benefits and Premiums are effective January 01, 2017 through December 31, 2017 PLAN DESIGN AND BENEFITS PROVIDED BY AETNA LIFE INSURANCE COMPANY PLAN FEATURES Network & Out-of-Network Annual Deductible
Benefits and Premiums are effective January 01, 2017 through December 31, 2017 PLAN DESIGN AND BENEFITS PROVIDED BY AETNA LIFE INSURANCE COMPANY PLAN FEATURES Network & Out-of-Network Annual Deductible
Rx Benefits. Generic $10.00 Brand name formulary drug $30.00
 Rx Benefits VCCCD - Faculty Custom Prescription Drug Benefits Mandatory Generic Substitution This summary of benefits has been updated to comply with federal and state requirements, including applicable
Rx Benefits VCCCD - Faculty Custom Prescription Drug Benefits Mandatory Generic Substitution This summary of benefits has been updated to comply with federal and state requirements, including applicable
PURPOSE OF THE POLICY STATEMENT OF THE POLICY PROCEDURES
 PURPOSE OF THE POLICY The purpose of this policy is to describe Health Alliance s process for transitions and ensure that continued drug coverage is provided to new and current Part D members. The transition
PURPOSE OF THE POLICY The purpose of this policy is to describe Health Alliance s process for transitions and ensure that continued drug coverage is provided to new and current Part D members. The transition
Florida Medicaid. Prescribed Drugs Services Coverage Policy. Agency for Health Care Administration. Draft Rule
 Florida Medicaid Prescribed Drugs Services Coverage Policy Agency for Health Care Administration Draft Rule Table of Contents Introduction... 1 1.1 Description... 1 1.2 Legal Authority... 1 1.3 Definitions...
Florida Medicaid Prescribed Drugs Services Coverage Policy Agency for Health Care Administration Draft Rule Table of Contents Introduction... 1 1.1 Description... 1 1.2 Legal Authority... 1 1.3 Definitions...
Prescription Drug Rider
 Prescription Drug Rider P L A N C E R T I F I C A T E Drug 516 Jan 2014 01:14 HMSA s Prescription Drug Rider This summary is intended to provide a condensed explanation of plan benefits. Certain limitations,
Prescription Drug Rider P L A N C E R T I F I C A T E Drug 516 Jan 2014 01:14 HMSA s Prescription Drug Rider This summary is intended to provide a condensed explanation of plan benefits. Certain limitations,
Excellus BlueCross BlueShield Participating Provider Manual. 5.0 Pharmacy Management
 Excellus BlueCross BlueShield Participating Provider Manual 5.0 Pharmacy Management 5.1 Pharmacy Benefits The Health Plan is committed to effectively managing prescription drug benefit costs and providing
Excellus BlueCross BlueShield Participating Provider Manual 5.0 Pharmacy Management 5.1 Pharmacy Benefits The Health Plan is committed to effectively managing prescription drug benefit costs and providing
$0 $0 N/A. Pneumococcal, Flu, Hepatitis B Not Not Covered Routine GYN Care (Cervical and Vaginal Cancer Screenings)
") PLAN FEATURES Network Providers Out-of-Network Providers Combined In and Out of Network Deductible (Plan Level/includes Network Deductible) $0 $0 Member Coinsurance Applies to all expenses unless otherwise
PLAN FEATURES Network Providers Out-of-Network Providers Combined In and Out of Network Deductible (Plan Level/includes Network Deductible) $0 $0 Member Coinsurance Applies to all expenses unless otherwise
Get the most from your prescription benefit
 Get the most from your prescription benefit TE Connectivity HealthFund HRA Plan Welcome to Express Scripts What s Inside Your benefit at a glance...2 Your plan s preferred medicines...2 Prior authorization...2
Get the most from your prescription benefit TE Connectivity HealthFund HRA Plan Welcome to Express Scripts What s Inside Your benefit at a glance...2 Your plan s preferred medicines...2 Prior authorization...2
2019 Transition Policy and Procedure
 2019 Transition Policy and Procedure POLICY Steward Health Choice Generations (SHCG) provides a Part D drug transition process in order to prevent enrollee medication coverage gaps. SHCG s transition process
2019 Transition Policy and Procedure POLICY Steward Health Choice Generations (SHCG) provides a Part D drug transition process in order to prevent enrollee medication coverage gaps. SHCG s transition process
Chapter 8 Section 9.1
 Other Services Chapter 8 Section 9.1 Issue Date: August 2002 Authority: 32 CFR 199.2(b), 32 CFR 199.4(b)(2)(vi), (b)(3)(iii), (b)(5)(v), (d)(3)(vi), (e)(11)(i), 32 CFR 199.5(d)(12); 32 CFR 199.17, and
Other Services Chapter 8 Section 9.1 Issue Date: August 2002 Authority: 32 CFR 199.2(b), 32 CFR 199.4(b)(2)(vi), (b)(3)(iii), (b)(5)(v), (d)(3)(vi), (e)(11)(i), 32 CFR 199.5(d)(12); 32 CFR 199.17, and
I. PURPOSE. A. The primary objectives of Molina Healthcare s Transition Policy and Procedure are:
 I. PURPOSE The purpose of the Policy and Procedure is to ensure necessary continuity of treatment and to provide adequate time and transition process to introduce the enrollee and their prescribing physician
I. PURPOSE The purpose of the Policy and Procedure is to ensure necessary continuity of treatment and to provide adequate time and transition process to introduce the enrollee and their prescribing physician
Benefits and Premiums are effective January 01, 2017 through December 31, 2017 PLAN DESIGN AND BENEFITS PROVIDED BY AETNA LIFE INSURANCE COMPANY
 Benefits and Premiums are effective January 01, 2017 through December 31, 2017 PLAN FEATURES Network & Out-of- Annual Deductible $300 This is the amount you have to pay out of pocket before the plan will
Benefits and Premiums are effective January 01, 2017 through December 31, 2017 PLAN FEATURES Network & Out-of- Annual Deductible $300 This is the amount you have to pay out of pocket before the plan will
Benefits and Premiums are effective January 01, 2019 through December 31, 2019 PLAN DESIGN AND BENEFITS PROVIDED BY AETNA LIFE INSURANCE COMPANY
 The maximum out-of-pocket limit applies to all covered Medicare Part A and B benefits including deductible. Combined Annual Maximum Out-of-Pocket Amount (Plan Level / includes deductible) Annual Maximum
The maximum out-of-pocket limit applies to all covered Medicare Part A and B benefits including deductible. Combined Annual Maximum Out-of-Pocket Amount (Plan Level / includes deductible) Annual Maximum
HSA Prescription Benefit Plan Summary
 Getting Started Access your pharmacy benefits with your Premier Health Employee Plan member ID card. Your card will allow you to fill a prescription at a Premier pharmacy, participating retail pharmacy,
Getting Started Access your pharmacy benefits with your Premier Health Employee Plan member ID card. Your card will allow you to fill a prescription at a Premier pharmacy, participating retail pharmacy,
Plan highlights and rates. Effective January to June 2011
 Plan highlights and rates Effective January to June 2011 2011 Small Business RATE AREA 4 Contents 2 3 4 5 6 7 8 9 10 11 12 13 14 15 17 Copayment plans Predictable out-of-pocket costs and no annual deductible
Plan highlights and rates Effective January to June 2011 2011 Small Business RATE AREA 4 Contents 2 3 4 5 6 7 8 9 10 11 12 13 14 15 17 Copayment plans Predictable out-of-pocket costs and no annual deductible
Paramount Care, Inc.: LUCAS COUNTY EMPLOYEES Summary of Benefits and Coverage: What this Plan Covers & What it Costs
 This is only a summary*: A quick reference guide to coverage and costs under the Plan. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document
This is only a summary*: A quick reference guide to coverage and costs under the Plan. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document
SPD Prescription Drugs Plan
 Prescription Drugs Plan 08/01/2017 3-1 Your Prescription Drug Benefits The prescription drug benefit available to you is based on the medical plan in which you are enrolled. Regardless of the benefit design
Prescription Drugs Plan 08/01/2017 3-1 Your Prescription Drug Benefits The prescription drug benefit available to you is based on the medical plan in which you are enrolled. Regardless of the benefit design
2018 Summary of Benefits
 2018 Summary of Benefits Barry, Christian, Greene, Jasper, Lawrence, and Newton Counties, MO H1664--001 Benefits effective January 1, 2018 H1664_18_2916SB Accepted 09302017 This booklet provides you with
2018 Summary of Benefits Barry, Christian, Greene, Jasper, Lawrence, and Newton Counties, MO H1664--001 Benefits effective January 1, 2018 H1664_18_2916SB Accepted 09302017 This booklet provides you with
Prescription Drug Benefits
 Stryker s healthcare plan provides benefits for covered prescription drugs, including contraceptives, insulin and diabetic supplies. Benefits are paid for covered drugs that are medically necessary for
Stryker s healthcare plan provides benefits for covered prescription drugs, including contraceptives, insulin and diabetic supplies. Benefits are paid for covered drugs that are medically necessary for
Western Health Advantage: City of Sacramento $40 copay plan Rx N Coverage Period: 1/1/ /31/2016
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.westernhealth.com or by calling 1-888-563-2250. Important
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.westernhealth.com or by calling 1-888-563-2250. Important
Aetna Select Medical Plan PLAN FEATURES NETWORK OUT-OF-NETWORK. Plan Maximum Out of Pocket Limit excludes precertification penalties.
 Schedule of Benefits Employer: Yale University ASA: 877076 Issue Date: July 25, 2016 Effective Date: January 1, 2016 Schedule: 12D Booklet Base: 12 For: Aetna Select - Security Staff (Outside CT) Electing
Schedule of Benefits Employer: Yale University ASA: 877076 Issue Date: July 25, 2016 Effective Date: January 1, 2016 Schedule: 12D Booklet Base: 12 For: Aetna Select - Security Staff (Outside CT) Electing
Your Medicare Prescription Drug Coverage as a Member of UA Medicare Group Part D EVIDENCE OF COVERAGE (EOC)
") January 1 December 31 2010 Your Medicare Prescription Drug Coverage as a Member of UA Medicare Group Part D EVIDENCE OF COVERAGE (EOC) This booklet gives you the details about your Medicare prescription
January 1 December 31 2010 Your Medicare Prescription Drug Coverage as a Member of UA Medicare Group Part D EVIDENCE OF COVERAGE (EOC) This booklet gives you the details about your Medicare prescription
Health Savings Plan (HSP)
") Health Savings Plan (HSP) Combined Evidence of Coverage and Disclosure Form University of California Carrier ID: UCOP Effective Date: January 1, 2017 1 This booklet constitutes a summary of the Prescription
Health Savings Plan (HSP) Combined Evidence of Coverage and Disclosure Form University of California Carrier ID: UCOP Effective Date: January 1, 2017 1 This booklet constitutes a summary of the Prescription
2015 PacificSource Medicare Part D Transition Process for contracts H3864 & H4754:
 2015 PacificSource Medicare Part D Transition Process for contracts H3864 & H4754: Essentials Rx 6 (HMO), Essentials Rx 14 (HMO), Essentials Rx 15 (HMO), Essentials Rx 16 (HMO), Essentials Rx 19 (HMO),
2015 PacificSource Medicare Part D Transition Process for contracts H3864 & H4754: Essentials Rx 6 (HMO), Essentials Rx 14 (HMO), Essentials Rx 15 (HMO), Essentials Rx 16 (HMO), Essentials Rx 19 (HMO),
This is an ERISA plan, and you have certain rights under this plan. Please contact your Employer for additional information.
 Schedule of Benefits Employer: Adobe Systems Incorporated MSA: 660819 Issue Date: January 1, 2018 Effective Date: January 1, 2018 Schedule: 1A Booklet Base: 1 For: Aetna Choice POS II with Health Fund
Schedule of Benefits Employer: Adobe Systems Incorporated MSA: 660819 Issue Date: January 1, 2018 Effective Date: January 1, 2018 Schedule: 1A Booklet Base: 1 For: Aetna Choice POS II with Health Fund
Prescription Drug Benefits
 Stryker s healthcare plan provides benefits for covered prescription drugs, including contraceptives, insulin and diabetic supplies. Benefits are paid for covered drugs that are medically necessary for
Stryker s healthcare plan provides benefits for covered prescription drugs, including contraceptives, insulin and diabetic supplies. Benefits are paid for covered drugs that are medically necessary for
MESSA Saver Rx PRESCRIPTION DRUG RIDER BOOKLET
 MESSA Saver Rx PRESCRIPTION DRUG RIDER BOOKLET MESSA Saver Rx Prescription Drug Program The MESSA Saver Rx Prescription Drug Program is made available by a Group Operating Agreement between MESSA and Blue
MESSA Saver Rx PRESCRIPTION DRUG RIDER BOOKLET MESSA Saver Rx Prescription Drug Program The MESSA Saver Rx Prescription Drug Program is made available by a Group Operating Agreement between MESSA and Blue
Benefits and Premiums are effective January 01, 2019 through December 31, 2019 PLAN DESIGN AND BENEFITS PROVIDED BY AETNA HEALTH PLANS INC.
 Benefits and Premiums are effective January 01, 2019 through December 31, 2019 PLAN FEATURES Network Providers Annual Maximum Out-of-Pocket Amount $3,400 The maximum out-of-pocket limit applies to all
Benefits and Premiums are effective January 01, 2019 through December 31, 2019 PLAN FEATURES Network Providers Annual Maximum Out-of-Pocket Amount $3,400 The maximum out-of-pocket limit applies to all
Share a Clear View. El Paso Children's Hospital. Printed on:
 Share a Clear View El Paso Children's Hospital Printed on: Share a Clear View NAVITUS CUSTOMER CARE HOURS: 24 Hours a Day 7 Days a Week 855-673-6504 (toll-free) TTY (toll-free) 711 MAILING ADDRESS: Navitus
Share a Clear View El Paso Children's Hospital Printed on: Share a Clear View NAVITUS CUSTOMER CARE HOURS: 24 Hours a Day 7 Days a Week 855-673-6504 (toll-free) TTY (toll-free) 711 MAILING ADDRESS: Navitus
$300 $300. Unless otherwise indicated, the Deductible must be met prior to benefits being payable.
 PLAN FEATURES Network Providers Out-of-Network Providers Combined In and Out of Network Deductible (Plan Level/includes Network Deductible) $300 $300 Unless otherwise indicated, the Deductible must be
PLAN FEATURES Network Providers Out-of-Network Providers Combined In and Out of Network Deductible (Plan Level/includes Network Deductible) $300 $300 Unless otherwise indicated, the Deductible must be
Arkansas State University System Prescription Drug Program
 Arkansas State University System Prescription Drug Program The Arkansas State University (ASU) prescription drug program involves a partnership with the University of Arkansas for Medical Sciences (UAMS)
Arkansas State University System Prescription Drug Program The Arkansas State University (ASU) prescription drug program involves a partnership with the University of Arkansas for Medical Sciences (UAMS)
For: Choice POS II High Deductible Health Plan - Faculty, Managerial & Professional Employees
 Schedule of Benefits Employer: Yale University ASA: 877076 Issue Date: July 28, 2017 Effective Date: January 1, 2017 Schedule: 6A Booklet Base: 6 For: Choice POS II High Deductible Health Plan - Faculty,
Schedule of Benefits Employer: Yale University ASA: 877076 Issue Date: July 28, 2017 Effective Date: January 1, 2017 Schedule: 6A Booklet Base: 6 For: Choice POS II High Deductible Health Plan - Faculty,
This is an ERISA plan, and you have certain rights under this plan. Please contact your Employer for additional information.
 Schedule of Benefits Employer: Adobe Systems Incorporated MSA: 660819 Issue Date: January 1, 2018 Effective Date: January 1, 2018 Schedule: 2B Booklet Base: 2 For: Aetna Choice POS II HDHP - HealthSave
Schedule of Benefits Employer: Adobe Systems Incorporated MSA: 660819 Issue Date: January 1, 2018 Effective Date: January 1, 2018 Schedule: 2B Booklet Base: 2 For: Aetna Choice POS II HDHP - HealthSave
Annual Notice of Changes for 2015
 Kaiser Permanente Medicare Plus High w/part D (AB) plan (Cost) offered by Kaiser Foundation Health Plan of the Mid-Atlantic States, Inc. Annual Notice of Changes for 2015 You are currently enrolled as
Kaiser Permanente Medicare Plus High w/part D (AB) plan (Cost) offered by Kaiser Foundation Health Plan of the Mid-Atlantic States, Inc. Annual Notice of Changes for 2015 You are currently enrolled as
Provider Manual. Section 3: Fully-Insured Member Eligibility and Benefits Verification
 Provider Manual Section 3: Fully-Insured Member Eligibility Table of Contents SECTION 3: FULLY-INSURED MEMBER ELIGIBILITY AND BENEFITS VERIFICATION... 4 3.1 MEMBER ELIGIBILITY VERIFICATION... 4 3.1.1 Newborn
Provider Manual Section 3: Fully-Insured Member Eligibility Table of Contents SECTION 3: FULLY-INSURED MEMBER ELIGIBILITY AND BENEFITS VERIFICATION... 4 3.1 MEMBER ELIGIBILITY VERIFICATION... 4 3.1.1 Newborn
Martin s Point Generations Advantage Policy and Procedure Form
 Martin s Point Generations Advantage Policy and Procedure Form Policy #: PartD.923 Effective Date: 4/16/10 Policy Title: Part D Transition Policy Section of Manual: Medicare Prescription Drug Benefit Manual
Martin s Point Generations Advantage Policy and Procedure Form Policy #: PartD.923 Effective Date: 4/16/10 Policy Title: Part D Transition Policy Section of Manual: Medicare Prescription Drug Benefit Manual
Annual Notice of Changes for 2015
 Kaiser Permanente Medicare Plus Standard w/part D (B Only) plan (Cost) offered by Kaiser Foundation Health Plan of the Mid-Atlantic States, Inc. Annual Notice of Changes for 2015 You are currently enrolled
Kaiser Permanente Medicare Plus Standard w/part D (B Only) plan (Cost) offered by Kaiser Foundation Health Plan of the Mid-Atlantic States, Inc. Annual Notice of Changes for 2015 You are currently enrolled
Version: 15/02/2017 [ TPID: ] Page 1
![Version: 15/02/2017 [ TPID: ] Page 1](/thumbs/88/117441870.jpg "Version: 15/02/2017 [ TPID: ] Page 1") PLAN FEATURES NETWORK CARE OUT-OF-NETWORK CARE Primary Care Physician Selection Not required Not required Deductible (per calendar year) $1,500 Individual $3,000 Family $3,000 Individual $9,000 Family
PLAN FEATURES NETWORK CARE OUT-OF-NETWORK CARE Primary Care Physician Selection Not required Not required Deductible (per calendar year) $1,500 Individual $3,000 Family $3,000 Individual $9,000 Family