PRODUCER APPOINTMENT INFORMATION FORM (PIF)
|
|
|
- Esther Dorsey
- 5 years ago
- Views:
Transcription
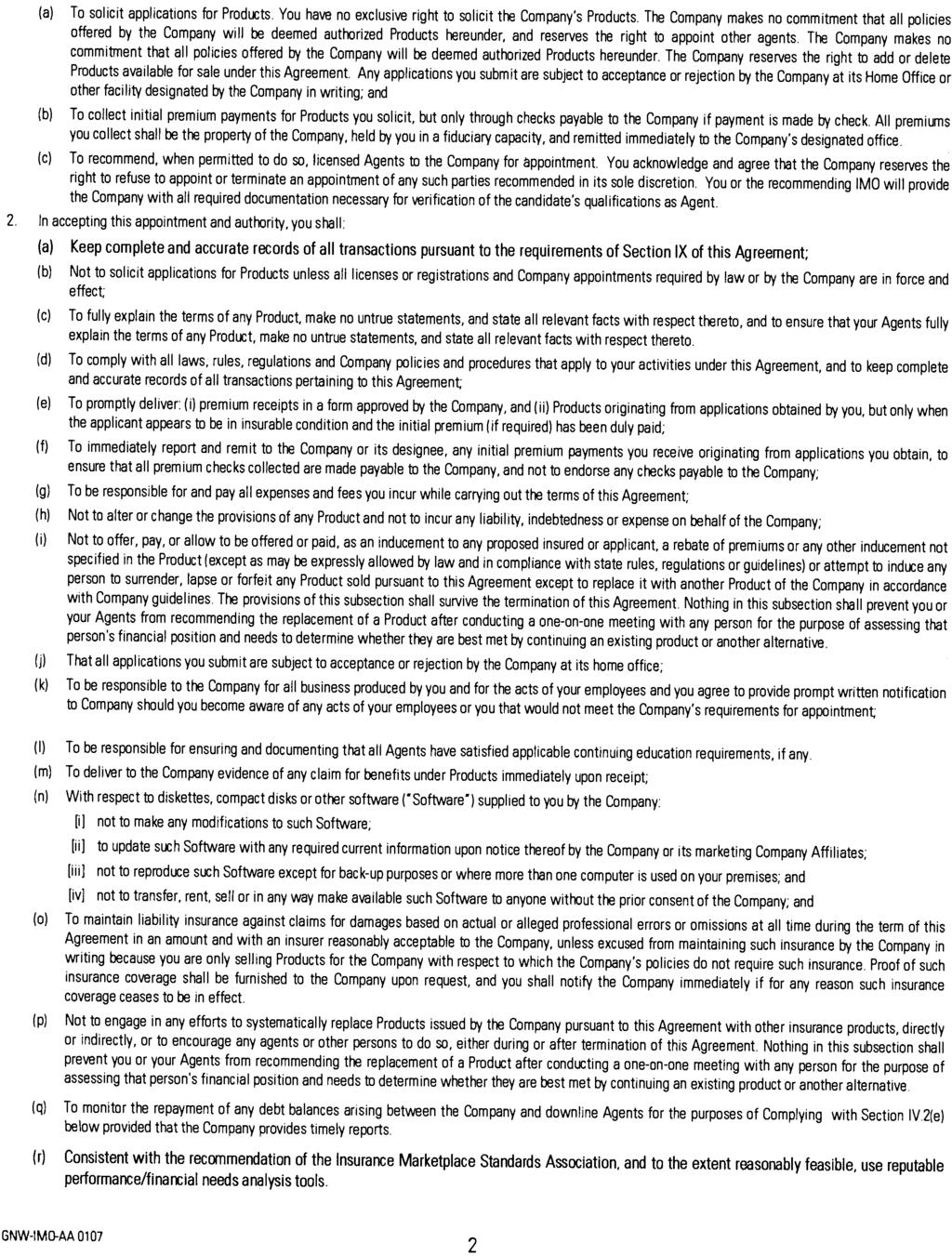
1 PRODUCER APPOINTMENT INFORMATION FORM (PIF) Please complete a separate PIF form for each party requesting an appointment. Do not combine business entity (firm/agency) appointment requests with individual information, or officer/principal information. 1. FORM PURPOSE Initial Appointment/Additional Additional State Appointment with current Change Hierarchy Company Appointment (Complete all sections.) companies (Complete sections 3, 5, 8) (Complete sections 3, 4, 8) 2. TYPE OF APPOINTMENT (Check ONLY one) Individual (complete 3a) Business Entity (Firm/Agency) (complete 3b) Officer/Principal (complete 3a) 3a. INDIVIDUAL INFORMATION First Name Middle Name Last Name Residence Address (No P.O. Box) City State Zip SSN #: NPN# (National Producer Number): Date of Birth:(mm/dd/ccyy) Gender F M Business Address City State Zip Business Phone ( ) Business Fax ( ) Preferred Mailing Address is Residence Business Address 3b. BUSINESS ENTITY (FIRM/AGENCY) APPOINTMENT (Must also complete a separate PIF Form for Officer) Business Name Tax ID # Business Address City State Zip Business Phone ( ) Business Fax ( ) Address Website Address Indicate type of taxable entity: Corporation Non-incorporated entity (e.g., Partnership, LLC) INFORMATION FOR SECTION BELOW TO BE PROVIDED BY TOP LEVEL AGENT/AGENCY 4. APPOINTING COMPANY AND COMMISSION HIERARCHY INFORMATION (use hierarchy transmittal if applicable) (Note: Provided you are properly licensed, you may be appointed to sell only those products for which your firm/agency is contracted.) List the General Agency or Sub Agent s name if the numbers are unknown. TOP LEVEL INTERMEDIATE LEVEL WRITING AGENT Submitting agent/agency agent/agency number commission New Business? Product Line/Company Name number (BGA/MGA) (sub GA, Member Firm) plan/schedule (select one) Fixed Life & Annuity: Genworth Life and Annuity Insurance Company* Genworth Life Insurance Company Genworth Life Insurance Company of NY Long Term Care: Genworth Life Insurance Company Genworth Life Insurance Company of NY Variable Life & Annuity: Genworth Life and Annuity Insurance Company Genworth Life Insurance Company of NY Medicare Supplement: Genworth Life Insurance Company Genworth Life and Annuity Insurance Company Linked Benefits (i.e. UL/LTC combo, SPDA/LTC combo): Genworth Life Insurance Company *Remember to attach Brokerage Authorization PIF-GNW Page 1 of 2 1/2007
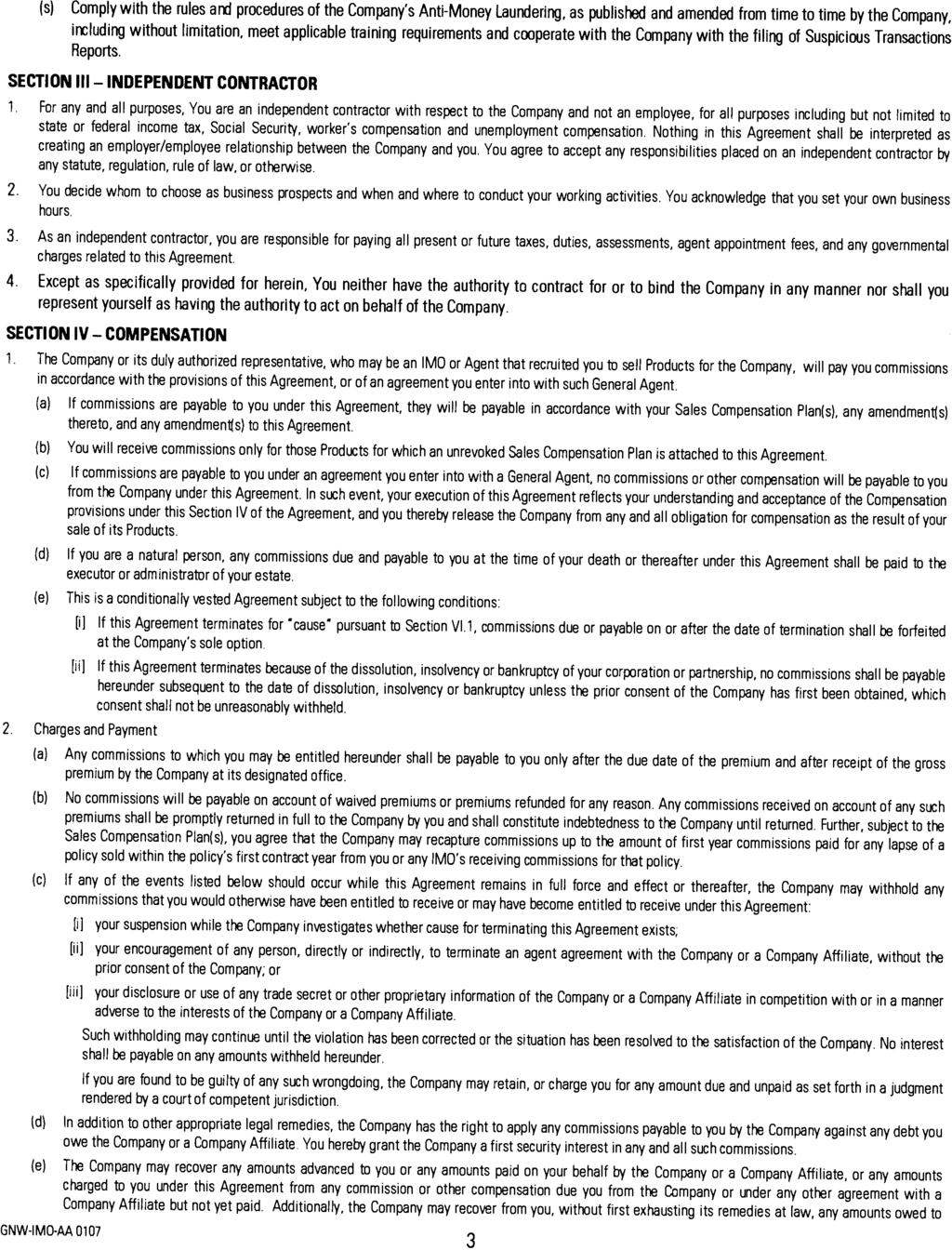
2 5. APPOINTMENT STATES REQUESTED Resident License State List Non-resident State(s) where appointment is requested. If FL, List Counties in which non-resident appointment is requested (required for in-person solicitation) If CA for fixed annuity, please provide proof you have completed the annuity training requirement. If MA or MD for Long Term Care, please submit the appropriate Acknowledgement Form (available at Genworth.com). For Long Term Care/LTC Partnership products, please provide certification or evidence of required training for states that require this. 6. PREVIOUS NAMES Please list all other names or aliases you have used in the last 7 years. For additional information, please use section 9 below. Previous First Name Previous Middle Name Previous Last Name 7. BUSINESS PRACTICES If you answer Yes to any questions below, please provide details by using Business Practices Details form. Yes No Yes No 1. Have you ever had an insurance or securities license denied, suspended, cancelled or revoked? 2. Has any regulatory body ever sanctioned, censured, penalized or otherwise disciplined you? 3. Has any state, federal or self-regulatory agency filed a complaint against you, fined, sanctioned, censured, penalized or otherwise disciplined you for a violation of their regulations or state or federal statutes? 4. Has a bonding or surety company ever denied, paid on, or revoked a bond for you? 5. Has any E&O carrier ever denied, paid claims on, or cancelled your coverage? 6. In the past ten years, have you personally filed a bankruptcy petition or declared bankruptcy? 7. In the past ten years, has any insurance or securities brokerage firm with whom you have been associated filed a bankruptcy petition or been declared bankrupt either during your association or within 5 years after termination of such association? 8. Are there any unsatisfied judgments, garnishments or liens against you? 9. Are you in debt to any insurance company? 10. Have you ever been convicted of, or pled guilty or nolo contendere to, any felony or misdemeanor other than a minor traffic offense? 11. Are you currently a party to any litigation or a subject of any investigation(s)? 12. Have you ever had an appointment with another insurance company denied or terminated for cause? 8. ACKNOWLEDGMENT I acknowledge and agree that this PIF is not a contract. I authorize and consent Genworth Financial, Inc. and its affiliates (collectively, the Company ) to obtain such additional background information about me as they deem necessary from time to time through independent investigation, NASD CRD reports and/or through a consumer reporting agency s consumer report (collectively, Background Reports ). I authorize the Company to share the information contained in this PIF or any other information that the Company may obtain, including Background Reports, with its affiliates for the purposes of establishing my eligibility and/or continuing eligibility for appointment with the Company and its affiliates as well as any other disclosure required by law. I hereby authorize my employers and other insurance companies I am or have been appointed with to release any and all information that they may have about me, personal or otherwise, to the Company, and I hereby release all such parties from all liability that may result from furnishing the same. I understand and agree that my appointment will, in part be based upon this PIF and the information in such Background Reports, and that any representation herein that is inaccurate or incomplete shall be grounds for termination of my appointment. I hereby certify under penalty of perjury that the information provided herein is accurate and complete. I have read, understood and agree to comply with the Guide to Ethical Market Conduct. Signature Date Title (if requesting a Business Entity (firm/agency) appointment or Officer/Principal appointment) 9. ADDITIONAL INFORMATION (use additional page if needed) PIF-GNW Page 2 of 2 1/2007
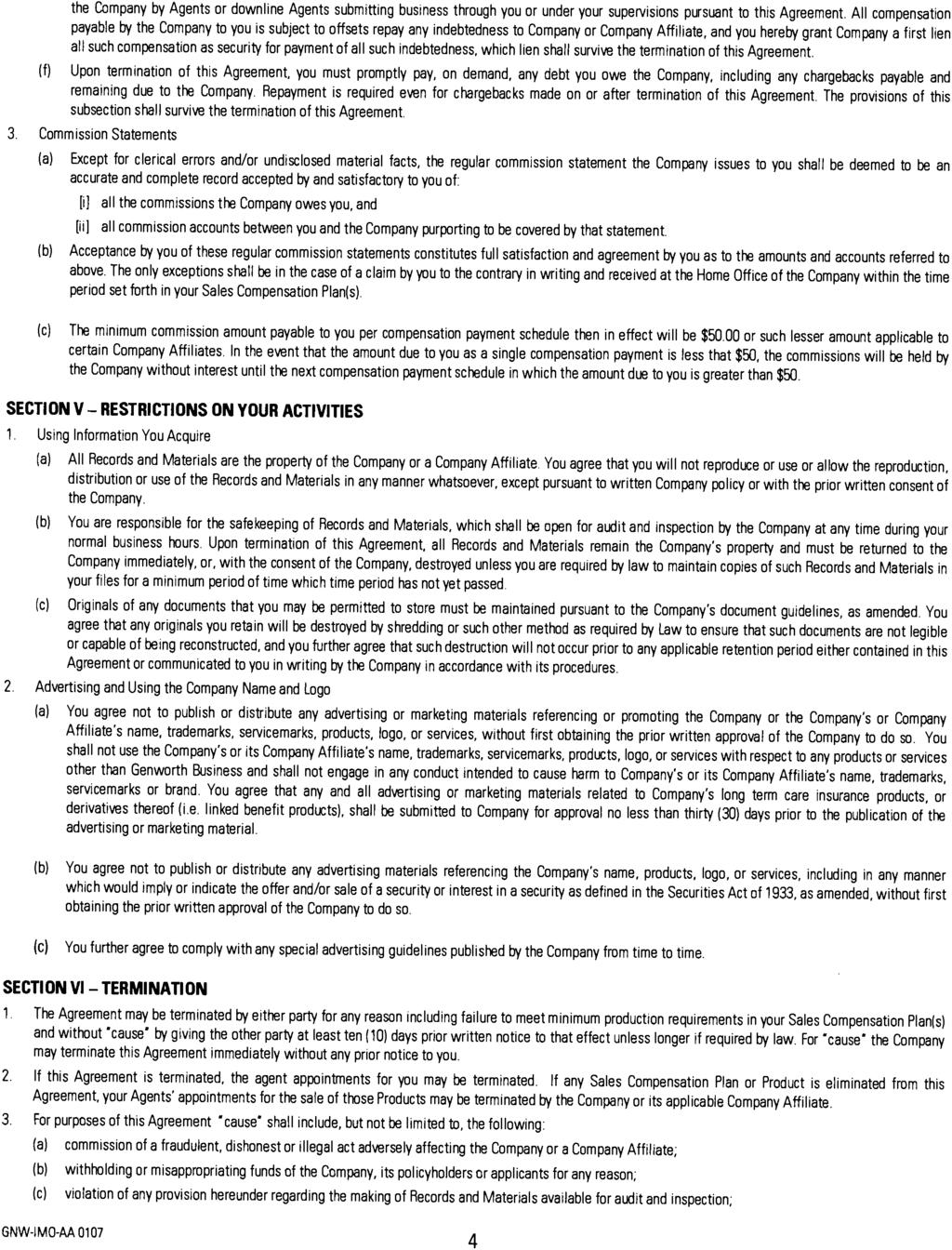
3 Disclosure of Intent to Obtain Consumer Reports This is to advise you that Genworth Financial, Inc. and its affiliates may obtain one or more consumer reports with respect to establishing your eligibility for employment, appointment, promotion, reassignment, and/or retention as an employee, agent and/or representative of Genworth Financial, Inc., or one or more of its affiliates. If requested, the report will be obtained from the investigative consumer-reporting agency named below: Business Information Group, Inc. P.O. Box 130 Southampton, PA (800) If a consumer report is obtained and you reside in a state with a legal requirement to provide a free copy of the consumer report upon request, we will automatically instruct the consumer reporting agency to send you a copy of the report at no charge. The report may contain information regarding your character, general reputation, personal characteristics and mode of living. The nature and scope of the report is: financial and credit history, criminal records search, licensing and disciplinary action history, and employment history verification. Authorization to Obtain Consumer Reports I hereby authorize Genworth Financial, Inc. and its affiliates to procure one or more consumer reports and to share the information obtained therefrom with each other with respect to establishing my eligibility for employment, appointment, promotion, reassignment, and/or retention as an employee, agent, and/or representative of Genworth Financial, Inc. or one or more of its affiliates. Date: Signature: Print Name: Title: (If requesting a firm/agency appointment or officer/principal appointment) 08/06
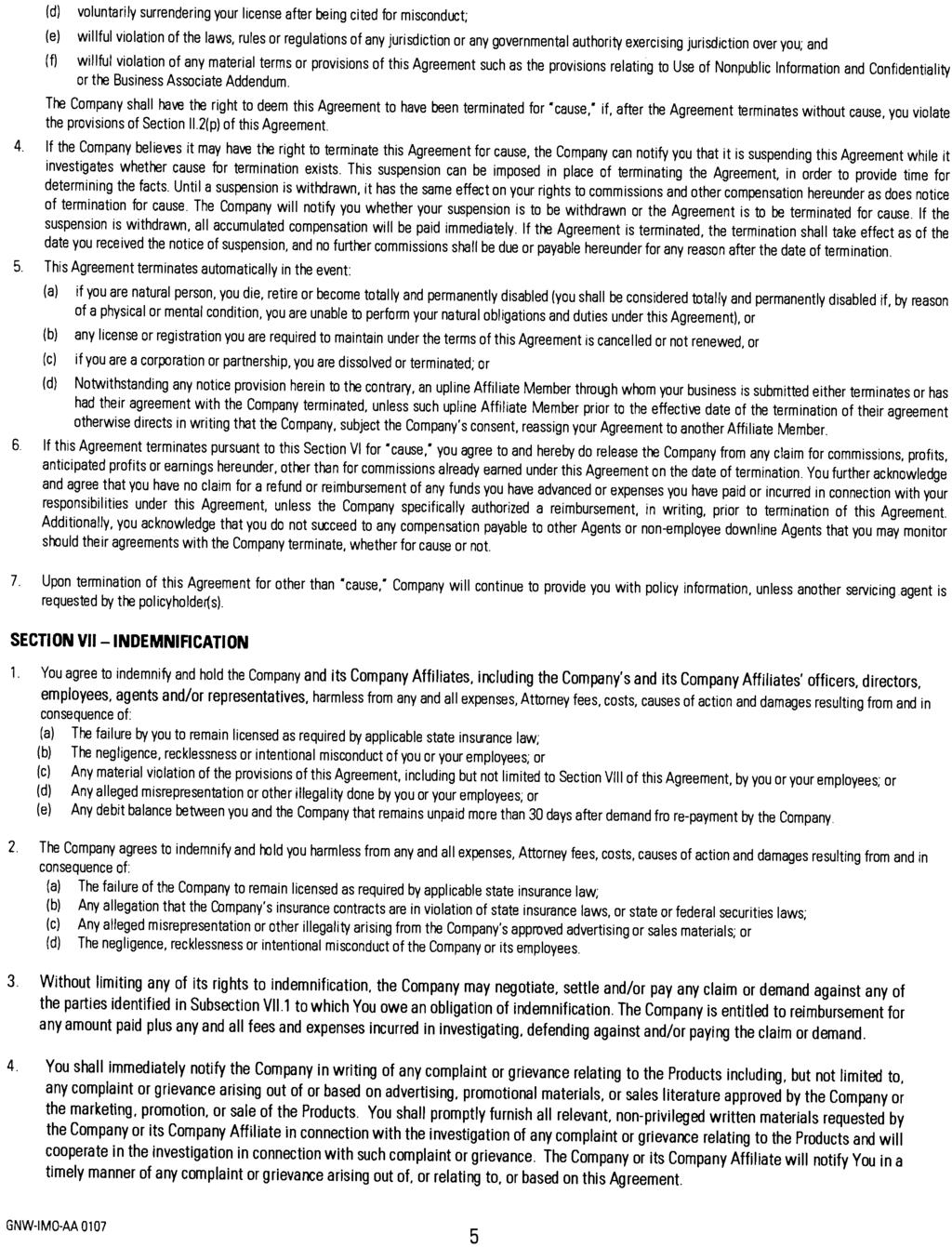
4 FOR CALIFORNIA RESIDENT AGENTS ONLY Pursuant to the California Investigative Consumer Reporting Agencies Act, Genworth Financial, Inc. is required to provide you with the summary of provisions listed below. California Investigative Consumer Reporting Agencies Act Summary of the Provisions of Section (a) An investigative consumer reporting agency shall supply files and information required under Section during normal business hours and on reasonable notice. (b) Files maintained on a consumer shall be made available for the consumer s visual inspection, as follows: (1) In person, if he appears in person and furnishes proper identification. A copy of his file shall also be available to the consumer for a fee not to exceed the actual costs of duplication services provided. (2) By certified mail, if he makes a written request, with proper identification, for copies to be sent to a specified addressee. Investigative consumer reporting agencies complying with requests for certified mailings under this section shall not be liable for disclosures to third parties caused by mishandling of mail after such mailings leave the investigative consumer reporting agencies. (3) A summary of all information contained in files on a consumer and required to be provided by Section shall be provided by telephone, if the consumer has made a written request, with proper identification for telephone disclosure, and the toll charge, if any, for the telephone call is prepaid by or charged directly to the consumer. (c) The term proper identification as used in subdivision (b) shall mean that information generally deemed sufficient to identify a person. Such information includes documents such as a valid driver s license, social security account number, military identification card, and credit cards. Only if the consumer is unable to reasonably identify himself with the information described above, may an investigative consumer-reporting agency require additional information concerning the consumer s employment and personal or family history in order to verify his identity. (d) The investigative consumer reporting agency shall provide trained personnel to explain to the consumer any information furnished him pursuant to Section (e) The investigative consumer reporting agency shall provide a written explanation of any coded information contained in files maintained on a consumer. This written explanation shall be distributed whenever a file is provided to a consumer for visual inspection as required under Section (f) The consumer shall be permitted to be accompanied by one other person of his choosing, who shall furnish reasonable identification. An investigative consumer reporting agency may require the consumer to furnish a written statement granting permission to the consumer reporting agency to discuss the consumer s file in such person s presence. 08/06
5
6
7
8
9
10
11
12
13
14
15
Genworth Life Contract
 Genworth Life Contract Please complete all pages of the contract and send it back to Stephens- Matthews with a copy of each state license you choose to appoint in Send to: Fax - 888-984-2614, E-mail -
Genworth Life Contract Please complete all pages of the contract and send it back to Stephens- Matthews with a copy of each state license you choose to appoint in Send to: Fax - 888-984-2614, E-mail -
Producer Information And Appointment Form (PIF)
") Aetna Health Insurance Company Aetna Health and Life Insurance Company Aetna Life Insurance Company American Continental Insurance Company Continental Life Insurance Company of Brentwood, Tennessee Aetna
Aetna Health Insurance Company Aetna Health and Life Insurance Company Aetna Life Insurance Company American Continental Insurance Company Continental Life Insurance Company of Brentwood, Tennessee Aetna
SUMMARY OF PRODUCER APPOINTMENT REQUIREMENTS FOR CURRENTLY LICENSED PRODUCERS
 Exhibit 2 SUMMARY OF PRODUCER APPOINTMENT REQUIREMENTS FOR CURRENTLY LICENSED PRODUCERS Refer to the "Appointment Requirements for Currently Licensed Producers" chart (the "Chart") for complete details.
Exhibit 2 SUMMARY OF PRODUCER APPOINTMENT REQUIREMENTS FOR CURRENTLY LICENSED PRODUCERS Refer to the "Appointment Requirements for Currently Licensed Producers" chart (the "Chart") for complete details.
ANNUITY AGENT CONTRACT TRANSMITTAL FORM
 ANNUITY AGENT CONTRACT TRANSMITTAL FORM This form should be completed for: Any new agents being contracted by you, or Any changes you are requesting to an existing agent s commission level. Agents requesting
ANNUITY AGENT CONTRACT TRANSMITTAL FORM This form should be completed for: Any new agents being contracted by you, or Any changes you are requesting to an existing agent s commission level. Agents requesting
GENWORTH Contracting Checklist
 GENWORTH Contracting Checklist Agent/Agency: Direct Upline: Agent #: Documents To Be Completed & Returned: Training Requirements Acknowledgement Producer Information and Appointment Form and Executive
GENWORTH Contracting Checklist Agent/Agency: Direct Upline: Agent #: Documents To Be Completed & Returned: Training Requirements Acknowledgement Producer Information and Appointment Form and Executive
Anthem Contract. Medicare Health Benefits 2716 S. 6 th Avenue Tucson, Arizona (520) or (844) Fax (520)
 or (844) Fax (520)") Anthem Contract Medicare Health Benefits 2716 S. 6 th Avenue Tucson, Arizona 85713 (520)760-6223 or (844) 245-4152 Fax (520) 760-6224 Please COMPLETE the following: 1. PDS 2. Signature pages Please SEND
Anthem Contract Medicare Health Benefits 2716 S. 6 th Avenue Tucson, Arizona 85713 (520)760-6223 or (844) 245-4152 Fax (520) 760-6224 Please COMPLETE the following: 1. PDS 2. Signature pages Please SEND
Social Security #: Gender: Resident State Insurance License #: Resident Insurance State: Last Name: First Name: Middle: Title:
 Social Security #: Gender: Email: Resident State Insurance License #: Resident Insurance State: Last Name: First Name: Middle: Title: Phone: Fax: Cell: Marital Status: Driver's Lic. #: DL State: Spouse
Social Security #: Gender: Email: Resident State Insurance License #: Resident Insurance State: Last Name: First Name: Middle: Title: Phone: Fax: Cell: Marital Status: Driver's Lic. #: DL State: Spouse
Appointment Application Applicant Page
 Appointment Application Applicant Page American General Life Insurance Company The United States Life Insurance Company in the City of New York P.O. Box 9978, Amarillo, TX 79105-5978 Fax 1-877-484-3142
Appointment Application Applicant Page American General Life Insurance Company The United States Life Insurance Company in the City of New York P.O. Box 9978, Amarillo, TX 79105-5978 Fax 1-877-484-3142
NORTH AMERICAN Contracting Checklist
 NORTH AMERICAN Contracting Checklist Agent/Agency: Direct Upline: Agent #: Documents To Be Completed & Returned: Contract Application [6798Z] Commission Direct Deposit Authorization Form [6772Z] w/ Voided
NORTH AMERICAN Contracting Checklist Agent/Agency: Direct Upline: Agent #: Documents To Be Completed & Returned: Contract Application [6798Z] Commission Direct Deposit Authorization Form [6772Z] w/ Voided
Contract Information and Signature Form
 Contract Information and Signature Form If contracting as a: Producer only - complete sections 1, 3 & Individual FCRA Authorization Form Business Entity only - complete sections 2 & 3 Business Entity &
Contract Information and Signature Form If contracting as a: Producer only - complete sections 1, 3 & Individual FCRA Authorization Form Business Entity only - complete sections 2 & 3 Business Entity &
Background Information And Authorization
 Background information Please respond to all questions for you personally and any organization over which you have exercised control. If you answer yes to any questions, you must attach a signed and dated
Background information Please respond to all questions for you personally and any organization over which you have exercised control. If you answer yes to any questions, you must attach a signed and dated
Sign and date the Application For Appointment: Recruiter s signature is required. Read, sign and date the Authorization for Release of Information.
 225 South East Street P.O. Box 7192 Indianapolis, IN 46207-7192 Sub-Agent Contracting Kit Instructions: Complete the Application For Appointment: Include Social Security number. Complete Anti-Money Laundering
225 South East Street P.O. Box 7192 Indianapolis, IN 46207-7192 Sub-Agent Contracting Kit Instructions: Complete the Application For Appointment: Include Social Security number. Complete Anti-Money Laundering
CONTRACTING DATA FORMS
 CONTRACTING DATA FORMS AGENT SERVICES OF AMERICA Please fill out the attached packet in its entirety and return to us; pcosta@agentsvs.com Or by fax to 866-462-002 or mail 400 komis Ave So., Venice, FL
CONTRACTING DATA FORMS AGENT SERVICES OF AMERICA Please fill out the attached packet in its entirety and return to us; pcosta@agentsvs.com Or by fax to 866-462-002 or mail 400 komis Ave So., Venice, FL
Capital Marketing Group, Inc Agent Contracting Kit
 Please complete the forms in this document to request appointment to the companies of your choice. Enclose a copy of your CURRENT E & O Insurance Certificate when you return. If this coverage is for your
Please complete the forms in this document to request appointment to the companies of your choice. Enclose a copy of your CURRENT E & O Insurance Certificate when you return. If this coverage is for your
Contracting & Appointment Instructions
 Contracting & Appointment Instructions In order to complete your contracting request, please complete the following contracting questionnaire. We will then input this information into our contracting system,
Contracting & Appointment Instructions In order to complete your contracting request, please complete the following contracting questionnaire. We will then input this information into our contracting system,
LIFE IMC CONTRACT TRANSMITTAL. If Business is submitted with or prior to a contracting application or contract change please indicate below:
 LIFE IMC CONTRACT TRANSMITTAL *O2681IMCC* *O2681IMCC* Agent : Agent Code (if known): If Business is submitted with or prior to a contracting application or contract change please indicate below: c Pending
LIFE IMC CONTRACT TRANSMITTAL *O2681IMCC* *O2681IMCC* Agent : Agent Code (if known): If Business is submitted with or prior to a contracting application or contract change please indicate below: c Pending
Contract Information and Signature Form
 Contract Information and Signature Form If contracting as a: Producer only - complete sections 1, 3 & Individual FCRA Authorization Form Business Entity only - complete sections 2 & 3 Business Entity &
Contract Information and Signature Form If contracting as a: Producer only - complete sections 1, 3 & Individual FCRA Authorization Form Business Entity only - complete sections 2 & 3 Business Entity &
Contract Information and Signature Form
 Contract Information and Signature Form If contracting as a: Producer only - complete sections 1, 3 & Individual FCRA Authorization Form Business Entity only - complete sections 2 & 3 Business Entity &
Contract Information and Signature Form If contracting as a: Producer only - complete sections 1, 3 & Individual FCRA Authorization Form Business Entity only - complete sections 2 & 3 Business Entity &
Contract Information and Signature Form
 If contracting as a: Section 1 Contract Information and Signature Form Producer only - complete sections 1, 3 & Individual FCRA Authorization Form Business Entity only - complete sections 2 & 3 Business
If contracting as a: Section 1 Contract Information and Signature Form Producer only - complete sections 1, 3 & Individual FCRA Authorization Form Business Entity only - complete sections 2 & 3 Business
Producer Set-Up Packet
 Producer Set-Up Packet USE HIGH RESOLUTION SCANNER OR HIGH QUALITY FAX Social Security #: Gender: Date of Birth: / / Email: Resident Insurance: Lic. # & State Last Name: First Name: MI: Phone: Fax: Cell:
Producer Set-Up Packet USE HIGH RESOLUTION SCANNER OR HIGH QUALITY FAX Social Security #: Gender: Date of Birth: / / Email: Resident Insurance: Lic. # & State Last Name: First Name: MI: Phone: Fax: Cell:
AUTOMATED APPOINTMENT SYSTEM
 Westland Financial Services, Inc. 1717 Kettner Blvd. Suite 200 San Diego, CA 92101 Office (800)238-8144 Fax (888)238-8154 www.westlandinc.com AUTOMATED APPOINTMENT SYSTEM Quick one time set up Westland
Westland Financial Services, Inc. 1717 Kettner Blvd. Suite 200 San Diego, CA 92101 Office (800)238-8144 Fax (888)238-8154 www.westlandinc.com AUTOMATED APPOINTMENT SYSTEM Quick one time set up Westland
Contracting & Appointment Instructions
 Contracting & Appointment Instructions In order to complete your contracting request, please complete the following contracting questionnaire. This information will be entered into our online contracting
Contracting & Appointment Instructions In order to complete your contracting request, please complete the following contracting questionnaire. This information will be entered into our online contracting
 Appointment Application AIG Life Brokerage A division of the American International Companies. Part 1 Individual and Principal of Corporation. This is Required Information. Please Print Clearly Social
Appointment Application AIG Life Brokerage A division of the American International Companies. Part 1 Individual and Principal of Corporation. This is Required Information. Please Print Clearly Social
Contract Information and Signature Form
 Contract Information and Signature Form If contracting as a: Producer only - complete sections 1, 3 & Individual FCRA Authorization Form Business Entity only - complete sections 2 & 3 Business Entity &
Contract Information and Signature Form If contracting as a: Producer only - complete sections 1, 3 & Individual FCRA Authorization Form Business Entity only - complete sections 2 & 3 Business Entity &
Licensing/Contracting Requirements
 Licensing/Contracting Requirements Licensing/Contracting Requirements Once you ve completed the forms and signed where needed, you can fax (856-983-5063) or email (john@safemoney.com) these pages to John
Licensing/Contracting Requirements Licensing/Contracting Requirements Once you ve completed the forms and signed where needed, you can fax (856-983-5063) or email (john@safemoney.com) these pages to John
Agent!Contracting!&!Appointment!
 AgentContracting&Appointment WeappreciateyourconsiderationinallowingMCDBenefitsLLCtoaddressyour Life,Annuity&Disabilityneeds.Weareexcitedtohaveyouonboardandlook forwardtoservicingyou.inordertoprocessyourlicensingrequest,please
AgentContracting&Appointment WeappreciateyourconsiderationinallowingMCDBenefitsLLCtoaddressyour Life,Annuity&Disabilityneeds.Weareexcitedtohaveyouonboardandlook forwardtoservicingyou.inordertoprocessyourlicensingrequest,please
Gerber Life Insurance Company
 Gerber Life Insurance Company 445 State Street, Fremont MI 49412 www.gerberlife.com Gerber Life Insurance Company (Please print clearly and complete all questions, where applicable. This form is good for
Gerber Life Insurance Company 445 State Street, Fremont MI 49412 www.gerberlife.com Gerber Life Insurance Company (Please print clearly and complete all questions, where applicable. This form is good for
You can submit your paperwork one of the following ways:
 Tired of filling out contracting paperwork? Simply fill out this document and send it back to us. This will provide us with the necessary information to fill out your contracts FOR YOU. By signing this
Tired of filling out contracting paperwork? Simply fill out this document and send it back to us. This will provide us with the necessary information to fill out your contracts FOR YOU. By signing this
We appreciate the opportunity to work with you on your insurance business! We want the setup process to be as easy for you as possible!
 Dear Valued Agent Partner, We appreciate the opportunity to work with you on your insurance business! We want the setup process to be as easy for you as possible! In order to set you up to write business
Dear Valued Agent Partner, We appreciate the opportunity to work with you on your insurance business! We want the setup process to be as easy for you as possible! In order to set you up to write business
Contracting Instructions
 Contracting Instructions Mark Wall & Company utilizes a contracting vendor, SureLC, for contracting and appointments with the insurance carriers we work with. For you, the advantage to this system, is
Contracting Instructions Mark Wall & Company utilizes a contracting vendor, SureLC, for contracting and appointments with the insurance carriers we work with. For you, the advantage to this system, is
PRODUCER SET UP PACKET CHECKLIST
 PRODUCER SET UP PACKET CHECKLIST Provide a copy of any LTC CE or Annuity CE certificates Provide a copy of your E&O Insurance Provide a copy of your Insurance License(s) If selecting "Agency" on page 2,
PRODUCER SET UP PACKET CHECKLIST Provide a copy of any LTC CE or Annuity CE certificates Provide a copy of your E&O Insurance Provide a copy of your Insurance License(s) If selecting "Agency" on page 2,
American General Life Companies Member companies of American International Group, Inc.
 Hierarchy Structure American General Life Companies Member companies of American International Group, Inc. 1. If requesting appointment, please provide MGA s name and Agent No. (if applicable): PGP-N9594
Hierarchy Structure American General Life Companies Member companies of American International Group, Inc. 1. If requesting appointment, please provide MGA s name and Agent No. (if applicable): PGP-N9594
Contracting & Appointment Instructions
 Contracting & Appointment Instructions In order to complete your contracting request, please complete the following contracting questionnaire. We will then input this information into our contracting system,
Contracting & Appointment Instructions In order to complete your contracting request, please complete the following contracting questionnaire. We will then input this information into our contracting system,
Please note No appointments will be processed until new business is submitted, unless you reside in a pre-appointment state.
 To Our Valued Select Brokers Advisors, We appreciate your consideration in allowing Pinnacle Insurance & Financial Services, LLC, to address your insurance appointment needs. We are excited to have the
To Our Valued Select Brokers Advisors, We appreciate your consideration in allowing Pinnacle Insurance & Financial Services, LLC, to address your insurance appointment needs. We are excited to have the
Contract Checklist for General Agent (Corporation w/special Agent)
") Contract Checklist for General Agent (Corporation w/special Agent) Name: REQUIRED DOCUMENTS FOR CONTRACTING General Agent Agreement o Signature Page Signed & d o Full Name Printed or Typed o Tax Identification
Contract Checklist for General Agent (Corporation w/special Agent) Name: REQUIRED DOCUMENTS FOR CONTRACTING General Agent Agreement o Signature Page Signed & d o Full Name Printed or Typed o Tax Identification
Appointment Instructions
 Appointment Instructions In order to complete your appointment request, please complete the following personal information packet (PIP). Upon receipt of your PIP, your information will be input into our
Appointment Instructions In order to complete your appointment request, please complete the following personal information packet (PIP). Upon receipt of your PIP, your information will be input into our
Contracting & Appointment Instructions
 Contracting & Appointment Instructions In order to complete your contracting request, please complete the following contracting questionnaire. The information in this questionnaire will be input into our
Contracting & Appointment Instructions In order to complete your contracting request, please complete the following contracting questionnaire. The information in this questionnaire will be input into our
Midland National Life Insurance Company Contracting Checklist
 Midland National Life Insurance Company Contracting Checklist This checklist is intended to provide you with a list of steps to help have a successful appointment with Midland National. Follow these easy
Midland National Life Insurance Company Contracting Checklist This checklist is intended to provide you with a list of steps to help have a successful appointment with Midland National. Follow these easy
Here is a complete list of the forms and paperwork included, which we need for you to return.
 Dear Valued Agent, Thank you for your interest in doing business with The Tavenner Agency! In order to get you setup with our agency with the least amount of effort required of you, we have incorporated
Dear Valued Agent, Thank you for your interest in doing business with The Tavenner Agency! In order to get you setup with our agency with the least amount of effort required of you, we have incorporated
527 Plymouth Road, Suite 403 Plymouth Meeting, PA Phone: Fax: Fast Start Packet
 527 Plymouth Road, Suite 403 Plymouth Meeting, PA 19462 Phone: 866-496-5330 Fax: 610-729-7699 Fast Start Packet Complete all personal information on the following 2 pages. Answer all background questions.
527 Plymouth Road, Suite 403 Plymouth Meeting, PA 19462 Phone: 866-496-5330 Fax: 610-729-7699 Fast Start Packet Complete all personal information on the following 2 pages. Answer all background questions.
GLOBAL CONTRACT INSTRUCTIONS: REQUIRED DOCUMENTS:
 GLOBAL CONTRACT INSTRUCTIONS: 1. 2. Complete all items found below. Your Choice: Either fax completed Global Contract along with the required documents to: (623) 463-2336 or Scan and e-mail to your Agency
GLOBAL CONTRACT INSTRUCTIONS: 1. 2. Complete all items found below. Your Choice: Either fax completed Global Contract along with the required documents to: (623) 463-2336 or Scan and e-mail to your Agency
SOLICITOR CONTRACTING SET-UP PACKET. Who are you soliciting for: Please list which carriers are needed immediately due to upcoming business:
 O N E S O U R C E. E N D L E S S P O S S I B I L I T I E S. SOLICITOR CONTRACTING SET-UP PACKET Who are you soliciting for: Items of Importance: E&O Insurance Please provide a current certificate Anti-Money
O N E S O U R C E. E N D L E S S P O S S I B I L I T I E S. SOLICITOR CONTRACTING SET-UP PACKET Who are you soliciting for: Items of Importance: E&O Insurance Please provide a current certificate Anti-Money
1. Tennessee Brokerage Agency Licensing Questionnaire 2. Signed Signature Page 3. Signed Disclosure Release Page
 Dear Valued Agent, We appreciate your consideration in allowing Tennessee Brokerage Agency (TBA) to address your life insurance appointment needs and we are excited to have the privilege of offering you
Dear Valued Agent, We appreciate your consideration in allowing Tennessee Brokerage Agency (TBA) to address your life insurance appointment needs and we are excited to have the privilege of offering you
If this is your FIRST licensing request through our office since 12/15/11 you MUST complete the following pages:
 1502 West Highway 54, Suite 401 Durham, NC 27707 919.489.3600 (T) 919.419.0401 (F) 800.928.4998 (T) www.tbrins.com Agent Name: CARRIER(s) Requesting Contract with: If this is your FIRST licensing request
1502 West Highway 54, Suite 401 Durham, NC 27707 919.489.3600 (T) 919.419.0401 (F) 800.928.4998 (T) www.tbrins.com Agent Name: CARRIER(s) Requesting Contract with: If this is your FIRST licensing request
Demographic Information. 17 Business Web Site Address 18 Business Address ( ) -
 -") (Please Print or Type) Check appropriate boxes for license requested. Resident License Non-Resident License o Identify Home State: o Identify Home State License #: New Application Additional Line(s) of
(Please Print or Type) Check appropriate boxes for license requested. Resident License Non-Resident License o Identify Home State: o Identify Home State License #: New Application Additional Line(s) of
Global Contract Instructions
 Global Contract Instructions 1. 2. Complete all items found below. Scan and e-mail the completed contract to: sherman@unkefermail.com Required Documents: Completed Producer Set-Up Packet (Global Contract)
Global Contract Instructions 1. 2. Complete all items found below. Scan and e-mail the completed contract to: sherman@unkefermail.com Required Documents: Completed Producer Set-Up Packet (Global Contract)
Certificate of Fraternal Society
 COMMONWEALTH OF MASSACHUSETTS Office of Consumer Affairs and Business Regulation DIVISION OF INSURANCE Certificate of Fraternal Society (Please Print or Type) Name of the Society Address of the Fraternal
COMMONWEALTH OF MASSACHUSETTS Office of Consumer Affairs and Business Regulation DIVISION OF INSURANCE Certificate of Fraternal Society (Please Print or Type) Name of the Society Address of the Fraternal
We appreciate your consideration in allowing The Palmer Agency to address your life insurance appointment needs.
 Dear Valued Agent: We appreciate your consideration in allowing The Palmer Agency to address your life insurance appointment needs. In order to complete your licensing request, please complete the following
Dear Valued Agent: We appreciate your consideration in allowing The Palmer Agency to address your life insurance appointment needs. In order to complete your licensing request, please complete the following
S. DAKOTA License Fee $ The Representative must complete and mail the resident South Dakota license application to NMC.
 S. DAKOTA License Fee $25 Total Licensing Fees: $25 Resident License 1. The Representative must complete and mail the resident South Dakota license application to NMC. 2. The Licensing Department processes
S. DAKOTA License Fee $25 Total Licensing Fees: $25 Resident License 1. The Representative must complete and mail the resident South Dakota license application to NMC. 2. The Licensing Department processes
Hello and welcome to HBW Partners Tax Services (HBWPTS)!
!") 7152 Knapp St NE Ada, MI 49301 www.hbwtaxservices.com p) 616.682.4604 f) 616.682.5367 pathway@hbwsecurities.com Hello and welcome to HBW Partners Tax Services (HBWPTS)! A little about us: HBWPTS is one
7152 Knapp St NE Ada, MI 49301 www.hbwtaxservices.com p) 616.682.4604 f) 616.682.5367 pathway@hbwsecurities.com Hello and welcome to HBW Partners Tax Services (HBWPTS)! A little about us: HBWPTS is one
AGENT/AGENCY APPLICATION FOR APPOINTMENT
 AGENT/AGENCY APPLICATION FOR APPOINTMENT Page 1 of 23 1605 LBJ Freeway, Suite 710, Dallas, TX 75234 Toll Free 844-770-2400 Rev. 4/8/16 PDF processed with CutePDF evaluation edition www.cutepdf.com INDIVIDUAL
AGENT/AGENCY APPLICATION FOR APPOINTMENT Page 1 of 23 1605 LBJ Freeway, Suite 710, Dallas, TX 75234 Toll Free 844-770-2400 Rev. 4/8/16 PDF processed with CutePDF evaluation edition www.cutepdf.com INDIVIDUAL
DISCLOSURE REGARDING BACKGROUND INVESTIGATION
 DISCLOSURE REGARDING BACKGROUND INVESTIGATION Employer: Southern Connecticut State University Department: Position: [IMPORTANT -- PLEASE READ CAREFULLY BEFORE SIGNING] Employer ( the Company ) may obtain
DISCLOSURE REGARDING BACKGROUND INVESTIGATION Employer: Southern Connecticut State University Department: Position: [IMPORTANT -- PLEASE READ CAREFULLY BEFORE SIGNING] Employer ( the Company ) may obtain
4135 NW Urbandale Drive Urbandale, IA
 4135 NW Urbandale Drive Urbandale, IA 50322 www.biltd.com 800.362.1097 Thank you for requesting a carrier appointment through Brokers International. If this is your first time contracting with us, please
4135 NW Urbandale Drive Urbandale, IA 50322 www.biltd.com 800.362.1097 Thank you for requesting a carrier appointment through Brokers International. If this is your first time contracting with us, please
CONTRACTING SET-UP PACKET
 O N E S O U R C E. E N D L E S S P O S S I B I L I T I E S. Who referred you to First Protective: Items of Importance: CONTRACTING SET-UP PACKET E&O Insurance Please provide a current certificate Anti-Money
O N E S O U R C E. E N D L E S S P O S S I B I L I T I E S. Who referred you to First Protective: Items of Importance: CONTRACTING SET-UP PACKET E&O Insurance Please provide a current certificate Anti-Money
These documents can be ed to Attn: C&L Dept.
 Philip C.K. Hu, CFP President Dear Valued Agent, We appreciate your consideration in allowing Transpacific Financial Inc to address your contracting needs and we are excited to have the privilege of offering
Philip C.K. Hu, CFP President Dear Valued Agent, We appreciate your consideration in allowing Transpacific Financial Inc to address your contracting needs and we are excited to have the privilege of offering
Agent/Agency Licensing
 1502 West Highway 54, Suite 401 Durham, NC 27707 919.489.3600 (T) 919.419.0401 (F) 800.928.4998 (T) www.tbrins.com Agent/Agency Licensing Agent Name: CARRIER(s) Requesting Contract with: If this is your
1502 West Highway 54, Suite 401 Durham, NC 27707 919.489.3600 (T) 919.419.0401 (F) 800.928.4998 (T) www.tbrins.com Agent/Agency Licensing Agent Name: CARRIER(s) Requesting Contract with: If this is your
UNIVERSAL CONTRACTING INSTRUCTIONS:
 UNIVERSAL CONTRACTING INSTRUCTIONS: 1. Please complete all requested items. If Universal Contracting is returned incomplete, it will increase processing time. Please scrub the documents prior to submission.
UNIVERSAL CONTRACTING INSTRUCTIONS: 1. Please complete all requested items. If Universal Contracting is returned incomplete, it will increase processing time. Please scrub the documents prior to submission.
Sun Life Insurance (PIC) Licensing Checklist
 Licensing Checklist") Sun Life Insurance (PIC) Licensing Checklist Please complete the following contracting papers. Remember to sign in the required areas. The more complete the application, the sooner it will be approved.
Sun Life Insurance (PIC) Licensing Checklist Please complete the following contracting papers. Remember to sign in the required areas. The more complete the application, the sooner it will be approved.
1. General information. 2. Level Selection All health products are subject to transfer rules. 3. Requested Appointment States (optional)
") 1. General information 2. Level Selection All health products are subject to transfer rules 0 3. Requested Appointment States (optional) INTERNAL USE ONLY Add RL4 If contracting as a: Contract Information
1. General information 2. Level Selection All health products are subject to transfer rules 0 3. Requested Appointment States (optional) INTERNAL USE ONLY Add RL4 If contracting as a: Contract Information
Contracting Information and Signature Form
 Contracting Information and Signature Form If contracting as a: Producer only - complete sections 1, 3 & Individual FCRA Authorization Form Business Entity only - complete sections 2 & 3 Section 1 Business
Contracting Information and Signature Form If contracting as a: Producer only - complete sections 1, 3 & Individual FCRA Authorization Form Business Entity only - complete sections 2 & 3 Section 1 Business
CONTRACT REQUEST FORM
 CONTRACT REQUEST FORM PLEASE COMPLETELY FILL OUT ALL FIELDS AND INCLUDE A COPY OF YOUR INSURANCE LICENSE, DRIVERS LICENSE, E&O INSURANCE AND A VOIDED CHECK. Once you have completed the contract please
CONTRACT REQUEST FORM PLEASE COMPLETELY FILL OUT ALL FIELDS AND INCLUDE A COPY OF YOUR INSURANCE LICENSE, DRIVERS LICENSE, E&O INSURANCE AND A VOIDED CHECK. Once you have completed the contract please
Agent/Agency Licensing
 1502 West Highway 54, Suite 401 Durham, NC 27707 919.489.3600 (T) 919.419.0401 (F) 800.928.4998 (T) Agent/Agency Licensing Agent Name: CARRIER(s) Requesting Contract with: STATE(s) Requesting Appointment
1502 West Highway 54, Suite 401 Durham, NC 27707 919.489.3600 (T) 919.419.0401 (F) 800.928.4998 (T) Agent/Agency Licensing Agent Name: CARRIER(s) Requesting Contract with: STATE(s) Requesting Appointment
Contracting & Appointment Instructions
 Contracting & Appointment Instructions In order to complete your contracting request, please complete the following contracting questionnaire. The information in this questionnaire will be input in to
Contracting & Appointment Instructions In order to complete your contracting request, please complete the following contracting questionnaire. The information in this questionnaire will be input in to
MUTUAL OF OMAHA INSURANCE COMPANY AND ITS AFFILIATES BACKGROUND AND INFORMATION SHEET. Name: Home Address (must be a physical street address):
:") MUTUAL OF OMAHA INSURANCE COMPANY AND ITS AFFILIATES BACKGROUND AND INFORMATION SHEET Name: Social Security Number: Date of Birth: Home Address (must be a physical street address): Home Phone: Cell Phone:
MUTUAL OF OMAHA INSURANCE COMPANY AND ITS AFFILIATES BACKGROUND AND INFORMATION SHEET Name: Social Security Number: Date of Birth: Home Address (must be a physical street address): Home Phone: Cell Phone:
Additionally, we ll also need you to fax, image or mail to us the following:
 Dear Advisor, The most meaningful commitment we have made to you is to do all we can to make life insurance easier for you to include in your practice. A significant component of that is to reduce your
Dear Advisor, The most meaningful commitment we have made to you is to do all we can to make life insurance easier for you to include in your practice. A significant component of that is to reduce your
BROKER/DEALER DATA Broker/Dealer I am an NASD registered representative with Tax ID. # located at:
 *APP* American National Insurance Company License/Appointment Data Sheet Please attach a copy of your NASD CRD status report and a copy of your state variable license(s). To sell American National variable
*APP* American National Insurance Company License/Appointment Data Sheet Please attach a copy of your NASD CRD status report and a copy of your state variable license(s). To sell American National variable
DISCLOSURE AND AUTHORIZATION FOR CONSUMER AND/OR INVESTIGATIVE CONSUMER REPORT. Company Name:
 DISCLOSURE AND AUTHORIZATION FOR CONSUMER AND/OR INVESTIGATIVE CONSUMER REPORT Company Name: In connection with your application and/or employment with above listed Company (hereinafter the Company ) this
DISCLOSURE AND AUTHORIZATION FOR CONSUMER AND/OR INVESTIGATIVE CONSUMER REPORT Company Name: In connection with your application and/or employment with above listed Company (hereinafter the Company ) this
Contracting and Appointment Instructions
 Contracting and Appointment Instructions In order to complete your contracting request, please complete the following contracting questionnaire. We will then input this information into our contracting
Contracting and Appointment Instructions In order to complete your contracting request, please complete the following contracting questionnaire. We will then input this information into our contracting
Independent Agent Appointment Agreement (Registered Representative)
") Independent Agent Appointment Agreement (Registered Representative) Independent Agent Appointment Agreement (Registered Representative) This Agreement is made as of the date signed below by ( Agent ) and
Independent Agent Appointment Agreement (Registered Representative) Independent Agent Appointment Agreement (Registered Representative) This Agreement is made as of the date signed below by ( Agent ) and
PLEASE SUBMIT CHECKLIST AND ALL OTHER PAPERWORK VIA FAX: OR
 Producer Appointment Checklist Individual Producers For completion: Important Information Complete if submitting new business Producer Appointment Application Producer Agreement (Fixed Products) Complete
Producer Appointment Checklist Individual Producers For completion: Important Information Complete if submitting new business Producer Appointment Application Producer Agreement (Fixed Products) Complete
ACT is designed to speed you through the Contracting process at
 ACT is designed to speed you through the Contracting process at ACA. 1. Fill in the ACT Appointment Data Sheet 2. Sign the Authorization To Execute 3. Sign the Efficient Forms Signature Authorization We
ACT is designed to speed you through the Contracting process at ACA. 1. Fill in the ACT Appointment Data Sheet 2. Sign the Authorization To Execute 3. Sign the Efficient Forms Signature Authorization We
Thank You. Merci. Gracias. Danka Schein. Mahalo. Domo Arigato. Dziekuje. Spacibo. Thanks
 Thank You Merci Gracias Danka Schein Mahalo Domo Arigato Dziekuje Spacibo Thanks Thank you for your interest in contracting with The Life Insurance Brokerage Pro, Inc. (The Life Pro). Please fill out the
Thank You Merci Gracias Danka Schein Mahalo Domo Arigato Dziekuje Spacibo Thanks Thank you for your interest in contracting with The Life Insurance Brokerage Pro, Inc. (The Life Pro). Please fill out the
For questions regarding the completion of this packet, please contact Amanda Barnes ext. 7018
 Dear Valued Agent, We appreciate your consideration in allowing Designs in Life to address your contracting needs and we are excited to have the privilege of offering you our services. In order to complete
Dear Valued Agent, We appreciate your consideration in allowing Designs in Life to address your contracting needs and we are excited to have the privilege of offering you our services. In order to complete
Thanks for Contracting Through Davis Life & Annuity!
 Thanks for Contracting Through Davis Life & Annuity! To ensure a timely and smooth process, please include the following: Completed and signed contract / SureLC packet Copy of all resident and non-resident
Thanks for Contracting Through Davis Life & Annuity! To ensure a timely and smooth process, please include the following: Completed and signed contract / SureLC packet Copy of all resident and non-resident
(c) "Subject" means the commercial enterprise about which a commercial credit report has been compiled.
 Subject means the commercial enterprise about which a commercial credit report has been compiled.") CALIFORNIA CIVIL CODE SECTION 1785.41 1785.44 1785.41. Consumer credit reporting is subject to the regulations of the Consumer Credit Reporting Agencies Act. Commercial credit reports, which differ significantly,
CALIFORNIA CIVIL CODE SECTION 1785.41 1785.44 1785.41. Consumer credit reporting is subject to the regulations of the Consumer Credit Reporting Agencies Act. Commercial credit reports, which differ significantly,
Appointment Instructions
 Appointment Instructions In order to complete your appointment request, please complete the following contracting packet. Upon receipt, your information will be entered into our online system, which allows
Appointment Instructions In order to complete your appointment request, please complete the following contracting packet. Upon receipt, your information will be entered into our online system, which allows
L I C E N S I N G P A C K E T
 L I C E N S I N G P A C K E T Please complete all fields on the following pages. Completion of this packet satisfies your appointment with any of the carriers we represent. E&O Coverage will need to be
L I C E N S I N G P A C K E T Please complete all fields on the following pages. Completion of this packet satisfies your appointment with any of the carriers we represent. E&O Coverage will need to be
Sunlife Financial Contracting Instructions
 Sunlife Financial Contracting Instructions Some of these forms will be used for some situations and not for others. Please follow the instructions below that pertain to your situation, and remember, required
Sunlife Financial Contracting Instructions Some of these forms will be used for some situations and not for others. Please follow the instructions below that pertain to your situation, and remember, required
OneAmerica Producer Contracting
 OneAmerica Producer Contracting Use the checklist on the next page as a reference. Proper completion and submission of the necessary forms will help expedite the processing of your appointment. After completing
OneAmerica Producer Contracting Use the checklist on the next page as a reference. Proper completion and submission of the necessary forms will help expedite the processing of your appointment. After completing
Gerber Life Insurance Company
 Gerber Life Insurance Company Please print clearly and complete all questions. Agents Legal Name: Alias/Other Name(s): Citizen of the U.S.: q Yes q No (If no, please provide proof of eligibility to work
Gerber Life Insurance Company Please print clearly and complete all questions. Agents Legal Name: Alias/Other Name(s): Citizen of the U.S.: q Yes q No (If no, please provide proof of eligibility to work
Your Producer Set-up Packet
 Your Producer Set-up Packet Dear Agent, This is your Producer Set-up Packet. This completed document allows us to complete most of your carrier contracting without the need to have you fill out endless
Your Producer Set-up Packet Dear Agent, This is your Producer Set-up Packet. This completed document allows us to complete most of your carrier contracting without the need to have you fill out endless
Demographic Information. Is the business entity affiliated with a financial institution/bank? Yes No
 (Please Print or Type) Check appropriate box for license requested. Resident License Non-Resident License o Identify Home State: o Identify Home State License #: Demographic Information 1 Business Entity
(Please Print or Type) Check appropriate box for license requested. Resident License Non-Resident License o Identify Home State: o Identify Home State License #: Demographic Information 1 Business Entity
PFG Marketing Group, Inc. Is Now Offering SureLC Contracting
 CONTRACTING INSTRUCTIONS: 1. Print this entire document 2. Choose the insurance carriers below you wish to be contracted with 3. Choose the states below you wish to be appointed in 4. Complete all areas
CONTRACTING INSTRUCTIONS: 1. Print this entire document 2. Choose the insurance carriers below you wish to be contracted with 3. Choose the states below you wish to be appointed in 4. Complete all areas
Yes No. To: (Mo./Yr.) (Mo./Yr.) Other Education Training (including business, trade, or military service schools, etc.)
 (Mo./Yr.) Other Education Training (including business, trade, or military service schools, etc.)") APPLICATION FOR EMPLOYMENT/INDEPENDENT CONTRACTOR 7761 Garden Grove Blvd. Garden Grove, CA 92841 Phone: (714) 898-8888 Fax: (714) 908-8097 Nhan Hoa Comprehensive Health Care Clinic ( Nhan Hoa ) provides
APPLICATION FOR EMPLOYMENT/INDEPENDENT CONTRACTOR 7761 Garden Grove Blvd. Garden Grove, CA 92841 Phone: (714) 898-8888 Fax: (714) 908-8097 Nhan Hoa Comprehensive Health Care Clinic ( Nhan Hoa ) provides
Return completed packet to Mercury Brokerage Group Licensing Dept. to or fax to
 Contracting Packet Return completed packet to Mercury Brokerage Group Licensing Dept. Email to tspencer@emercury.com, or fax to 214.210.5998 Thank you for choosing Mercury Brokerage Group as your general
Contracting Packet Return completed packet to Mercury Brokerage Group Licensing Dept. Email to tspencer@emercury.com, or fax to 214.210.5998 Thank you for choosing Mercury Brokerage Group as your general
Uniform Application for Business Entity Adjuster License/Registration (Please Print or Type)
") Business Entity License/Registration (Please Print or Type) Check appropriate box for license requested. Resident License Resident Designated Home State: License #: Non-Resident Designated Home State:
Business Entity License/Registration (Please Print or Type) Check appropriate box for license requested. Resident License Resident Designated Home State: License #: Non-Resident Designated Home State:
DISCLOSURE AND AUTHORIZATION FOR CONSUMER AND/OR INVESTIGATIVE CONSUMER REPORT. Company Name:
 DISCLOSURE AND AUTHORIZATION FOR CONSUMER AND/OR INVESTIGATIVE CONSUMER REPORT Company Name: In connection with your application and/or employment with above listed Company (hereinafter the Company ) this
DISCLOSURE AND AUTHORIZATION FOR CONSUMER AND/OR INVESTIGATIVE CONSUMER REPORT Company Name: In connection with your application and/or employment with above listed Company (hereinafter the Company ) this
Disclosure of Intent to Obtain Consumer Report and/or Investigative Consumer Report for Employment Purposes
 Disclosure of Intent to Obtain Consumer Report and/or Investigative Consumer Report for Employment Purposes By this document and pursuant to the Fair Credit Reporting Act (FCRA), 4-County Electric Power
Disclosure of Intent to Obtain Consumer Report and/or Investigative Consumer Report for Employment Purposes By this document and pursuant to the Fair Credit Reporting Act (FCRA), 4-County Electric Power
Please be advised that a wet signature is required on the signature page.
 17110 Marcy Street, Suite 100 Omaha, NE 68118 (800) 397-9999 fax: (402) 334-6300 Please complete the attached forms along with the documents noted below and return via secure email to licensing@fb-inc.com
17110 Marcy Street, Suite 100 Omaha, NE 68118 (800) 397-9999 fax: (402) 334-6300 Please complete the attached forms along with the documents noted below and return via secure email to licensing@fb-inc.com
CRIMINAL BACKGROUND CHECK CONSENT AND AUTHORIZATION TO OBTAIN CONSUMER REPORT FAIR CREDIT REPORTING ACT CONSUMER DISCLOSURE AND GENERAL AUTHORIZATION
 CRIMINAL BACKGROUND CHECK CONSENT AND AUTHORIZATION TO OBTAIN CONSUMER REPORT FAIR CREDIT REPORTING ACT CONSUMER DISCLOSURE AND GENERAL AUTHORIZATION I understand that National Audubon Society, Inc. (
CRIMINAL BACKGROUND CHECK CONSENT AND AUTHORIZATION TO OBTAIN CONSUMER REPORT FAIR CREDIT REPORTING ACT CONSUMER DISCLOSURE AND GENERAL AUTHORIZATION I understand that National Audubon Society, Inc. (
APPLICATION CHECKLIST IMPORTANT Submit all items on the checklist below with your application to ensure faster processing.
 State of Florida Department of Business and Professional Regulation Board of Employee Leasing Companies Application for Licensure as an Employee Leasing Company Controlling Person Form # DBPR ELC 1 1 of
State of Florida Department of Business and Professional Regulation Board of Employee Leasing Companies Application for Licensure as an Employee Leasing Company Controlling Person Form # DBPR ELC 1 1 of
Producer Background Questionnaire and Data Sheet
 Producer Background Questionnaire and Data Sheet Home Office: Purchase, NY 10577 www.jackson.com Business Through Broker/Dealer, Broker/Dealer Affiliated Agency, or Bank Agency For Insurance License Appointment
Producer Background Questionnaire and Data Sheet Home Office: Purchase, NY 10577 www.jackson.com Business Through Broker/Dealer, Broker/Dealer Affiliated Agency, or Bank Agency For Insurance License Appointment
EAST GEORGIA REGIONAL MEDICAL CENTER STATESBORO, GEORGIA APPLICATION FOR VOLUNTEER SERVICES
 EAST GEORGIA REGIONAL MEDICAL CENTER STATESBORO, GEORGIA 30458 APPLICATION FOR VOLUNTEER SERVICES DATE Names: Last First Middle Initial Address: P.O. Box or Route Street City State Zip Code Telephone Number:
EAST GEORGIA REGIONAL MEDICAL CENTER STATESBORO, GEORGIA 30458 APPLICATION FOR VOLUNTEER SERVICES DATE Names: Last First Middle Initial Address: P.O. Box or Route Street City State Zip Code Telephone Number:
Final Expense Approval Instructions Checklist from American Continental Insurance Company
 Final Expense Approval Instructions Checklist from American Continental Insurance Company Page 1 of 1 American Continental Insurance Company A Genworth Financial Company 101 Continental Place Brentwood,
Final Expense Approval Instructions Checklist from American Continental Insurance Company Page 1 of 1 American Continental Insurance Company A Genworth Financial Company 101 Continental Place Brentwood,
Manager Contracting Coversheet
 Manager Contracting Coversheet Direct Upline Name: Direct Upline Email Address: Agent Name: Resident State: Agent Email: Agent Phone: Agent City and State of birth: MANAGERS ONLY PLEASE SELECT CARRIER
Manager Contracting Coversheet Direct Upline Name: Direct Upline Email Address: Agent Name: Resident State: Agent Email: Agent Phone: Agent City and State of birth: MANAGERS ONLY PLEASE SELECT CARRIER
Gerber Life Insurance Company
 Gerber Life Insurance Company Please print clearly and complete all questions. Agents Legal Name: Alias/Other Name(s): Citizen of the U.S.: q Yes q No (If no, please provide proof of eligibility to work
Gerber Life Insurance Company Please print clearly and complete all questions. Agents Legal Name: Alias/Other Name(s): Citizen of the U.S.: q Yes q No (If no, please provide proof of eligibility to work
Insurance Designers of Dallas makes contracting. Fast & Easy
 Insurance Designers of Dallas makes contracting Fast & Easy 1. Fill out the entire packet & sign 2. Return the completed packet to Chelsie Parker E Mail: cparker@insdesign.com Fax: 214 368 0308 (no cover
Insurance Designers of Dallas makes contracting Fast & Easy 1. Fill out the entire packet & sign 2. Return the completed packet to Chelsie Parker E Mail: cparker@insdesign.com Fax: 214 368 0308 (no cover
SPECIMEN. Sign and date the Application For Appointment: Recruiter s signature is required.
 General Agent Contracting Kit Instructions: 225 South East Street P.O. Box 7192 Indianapolis, IN 46207-7192 Complete the Application For Appointment: Include Social Security number. Submit a copy of a
General Agent Contracting Kit Instructions: 225 South East Street P.O. Box 7192 Indianapolis, IN 46207-7192 Complete the Application For Appointment: Include Social Security number. Submit a copy of a
Gerber Life Contracting Package
 Gerber Life Contracting Package Return the completed contracting package to Lovett Financial, Inc. You may mail, fax to us at 813-935-2605 or email it to newbusiness@lovettfinancial.net. Once you write
Gerber Life Contracting Package Return the completed contracting package to Lovett Financial, Inc. You may mail, fax to us at 813-935-2605 or email it to newbusiness@lovettfinancial.net. Once you write
Gerber Life Insurance Company ( Gerber Life ) Producer Information Questionnaire
 Producer Information Questionnaire") Gerber Life Insurance Company 1311 Mamaroneck Avenue, Suite 350, White Plains, NY 10605 www.gerberlife.com Business Address: (Must be a street address) Business Phone: Business Fax: Indicate with an x,
Gerber Life Insurance Company 1311 Mamaroneck Avenue, Suite 350, White Plains, NY 10605 www.gerberlife.com Business Address: (Must be a street address) Business Phone: Business Fax: Indicate with an x,