JOINT TASK FORCE ON HEALTH CARE COST REVIEW (Senate Bill 419)
|
|
|
- Hope Charles
- 5 years ago
- Views:
Transcription
1 May 11 th, 2018 JOINT TASK FORCE ON HEALTH CARE COST REVIEW (Senate Bill 419) 1
2 AGENDA 8:30-8:35 AM Welcome and Opening Remarks 8:35-9:30 AM Multi-stakeholder Approaches to Address Total Cost of Care 9:35-9:50 AM Summary of States Approaches to Cost Containment & Reform 9:50-10:00 AM BREAK 10:00-11:45 AM Task Force Discussion 11:50-11:55 AM Public Comment Opportunity 2
 3.")
3 Today s Objectives 1. Based on the information about Maryland, assess the potential impact and feasibility of a rate-setting model in Oregon (policy strategy #1 on matrix) 2. Based on cost containment and payment reform approaches in other states, evaluate alternative policy strategies that may help Oregon achieve similar policy goals (policy strategies #2-7 on matrix) 3. Discuss and confirm next steps for remaining meetings (3 in total) Develop and review policy proposals and recommendations (June 15 th ) Draft outline of report (July 13 th ) Finalize recommendations and report (August 17 th ) 3
4 ROADMAP Timeline November Draft Charter Background on SB 419 Solicit Input and Member Orientation December Historical overview of hospital rate setting Examine Maryland Model January Ongoing examination of Maryland model February No meeting (2018 session) March Oregon hospital financials Health care spending & pricing April Other states payment reform models (MA, PA, VT) May Total Cost of Care Task Force Discussion June-August Develop Policy Recs Draft & Finalize Report September 2018 Finalize and submit report to Oregon legislature Examine other states history with rate-setting Task Force Discussion 4
5 NOV RECAP Legislative history and intent of Senate Bill 419 (2017) Limit growth of health care expenditures in Oregon Address cost drivers in Oregon, with initial focus on hospital costs Assess potential impact and feasibility of the Maryland Model Consider and evaluate alternatives to accomplish goals in SB 419 Identified initial focus of the Task Force -- examine Maryland s hospital-rate setting model as well as investigate the state s more recent All-payer model Identified the types of data, information and reports task force members need 5
6 DEC RECAP Background and rationale for hospital rate setting in Maryland Impact of Maryland s Health Services Cost Review Commission on hospitals, health plans and providers Advantages and disadvantages of hospital rate-setting based on Maryland s more than four decades worth of experience Comparisons between Maryland and Oregon in terms of health care expenditures, types of hospitals, insurance market, demographics, and coverage 6
7 JAN RECAP Impact of Maryland s Health Services Cost Review Commission (HSCRC)- Commissioner and Research Perspectives Maryland s HSCRC - Medicaid Agency and Commission staff perspectives Description of development and operation of Maryland s all-payer rate setting it evolved from 1970s to present day, from rate-setting to all-payer global budget model Maryland has reduced per capita growth in hospital revenues for all payers, most recently under a global payment system Global budget transforms hospital payment, shifts volume-driven to value-driven Maryland has eliminated cost-shifting among private and public payers Key aspects of hospital global budget calculations, monitoring, and updates 7
8 MARCH 2018 RECAP Learned about Oregon s health care spending relative to other states: lower on utilization, higher on prices Key health care cost drivers including provider consolidation, new and costly treatments, consumers lack responsiveness to price (1) vertical integration: hospitals buying/partnering w/physician & ambulatory services, (2) horizontal integration - hospitals joining systems Competitive insurance market in Oregon Price variation among Oregon hospitals for services Federal and state hospital classifications: DRGs, Types A-C, Critical Access Hospitals Hospital financials in Oregon for DRG, Type A and B hospitals including recent trends around net revenue, operating expense & margin ( ) and payer mix 8
9 APRIL 2018 RECAP Massachusetts, Pennsylvania & Vermont Policies adopted and implemented by Vermont, Massachusetts, and Pennsylvania designed to reduce the growth of health care expenditures Opportunities and challenges with: Establishing models of accountable care organizations Creating multi-payer and all-payer approaches to transform health care payment Key factors to consider in establishing a statewide benchmark to cap the annual rate of growth. Brief exploration of how policies from the other states may help Oregon expand upon successful elements of its CCO model. 9
10 APRIL 2018 RECAP (cont.) Members observations at the end of the meeting: How best to build on the success of Oregon s CCOs with respect to what s complementary from the other states that may help Oregon extend successful elements of the CCO model. Establishing a statewide cap on the annual rate in health care costs in Oregon may allow the state to work towards an affordable system. Creating a statewide benchmark is an interesting approach in working towards a total cost of care model. A total cost of care model may collectively engage health systems, hospitals, and payers in Oregon and support efforts to transition away from FFS to a value-based payment system across both payers and provider types. Important to leverage existing infrastructure to works towards a more financially sustainable health care system. 10
11 MEDICARE 11

12 Source: Senior Health Insurance Benefits Assistance, DCBS. (2018) 12

13 Source: Senior Health Insurance Benefits Assistance, DCBS. (2018) 13
14 Medicare Advantage - Plan Types Health maintenance organizations (HMOs) and Local preferred provider organizations (PPOs) contract w/provider networks to deliver Medicare benefits. Nationally - HMOs account for the majority (63%) of total Medicare Advantage enrollment in 2017; local PPOs account for 26% of all Medicare Advantage enrollees Regional PPOs provide rural beneficiaries greater access to Medicare Advantage Plans Special Needs Plans (SNPs) are restricted to beneficiaries who are dually eligible for Medicaid or live in long-term care institutions Group Plans sponsored by unions and employers for retirees Medicare pays insurer a fixed amount per enrollee; employer/union pays for additional benefits Source: Medicare Payment Advisory Commission (MedPAC). Report to the Congress: Medicare Payment Policy, March
15 Original Medicare Fee for service model with bundled payments: Health services are bundled into groups known as Diagnostic Related Groups (DRGs) Reimbursement = (Base Rate) * (DRG multiplier) Reimbursement algorithm varies by setting (inpatient/outpatient) Certain hospital types are exempt from the DRG system and are paid on a cost basis (Type A & B hospitals) Multiple incentives, add-ons, performance and penalty mechanisms Sources: Source: Oregon Health Authority, Office of Health Analytics. Presentation March 9, 2018 to Joint Task Force. Senior Health Insurance Benefits Assistance, DCBS. (2018) 15
16 Payments to Medicare Advantage Plans Medicare pays Medicare Advantage plans a capitated (per enrollee) amount to provide all Part A and B benefits Medicare pays private plans a risk-adjusted per-person predetermined rate rather than a per-service rate Federal Medicare payments to MA plans are enrollee-specific, based on a plan s payment rate and an enrollee s risk score Risk scores account for differences in expected medical expenditures and are based in part on diagnoses that providers code. Medicare makes a separate payment to plans for providing prescription drug benefits under Medicare Part D Providers may charge different co-pay and deductible amounts, and can set rules about provider networks, referrals and out-of-network coverage Providers may contract with other providers on FFS or capitation basis Sources: Oregon Health Authority, Office of Health Analytics. Presentation March 9, 2018 to Joint Task Force. Kaiser Family Foundation. Medicare Advantage Fact Sheet (October 2017). Medicare Payment Advisory Commission (MedPAC). Report to the Congress: Medicare Payment Policy, March
17 Payments by Medicare (cont.) Nationally, MedPAC estimates 2018 payments to MA plans will average 101 percent of FFS spending; ranging 95% to 115% of traditional Medicare costs. Most claims in FFS Medicare are paid using procedure codes, which offer little incentive for providers to record more diagnosis codes than necessary to justify ordering a procedure. Goal for Medicare Advantage is to impose fiscal pressure on all providers of care to improve efficiency and reduce Medicare program costs and beneficiary premiums MA plans have a financial incentive to ensure that their providers record all possible diagnoses because higher enrollee risk scores result in higher payments to the plan (MedPAC 2018) Sources: Kaiser Family Foundation. Medicare Advantage Fact Sheet (October 2017). Medicare Payment Advisory Commission (MedPAC). Report to the Congress: Medicare Payment Policy, March
18 Medicare in Oregon 449,586 of the 816,139 Medicare covered lives in Oregon are Original Medicare (55% as of November 2017) compared to Medicare Advantage (44%) 22 stand-alone Medicare prescription drug plans 75 Medicare health-only or health & drug plans 38 companies offer Medicare Supplement policies (Medigap) Source: Senior Health Insurance Benefits Assistance, DCBS. (2018) 18
 Source: Centers for Medicare and Medicaid Services, Monthly Enrollment by State (April 2018).")
19 Medicare in Oregon 22 stand-alone Medicare prescription drug plans 75 Medicare health-only or health & drug plans 38 companies offer Medicare Supplement policies (Medigap) ~74,821 Dual Eligible Beneficiaries (*March 2018 OHP enrollment) Source: Centers for Medicare and Medicaid Services, Monthly Enrollment by State (April 2018). OHA Monthly Medicaid Population Report by Eligibility Group for Physical Health Plan, March
20 10 MA Carriers in Oregon cover >75% of All Medicare Beneficiaries Insurers (Organizations) Plan Types Enrollees Regence Blue Cross Blue Shield of Oregon Local PPO/HMO/HCPP 60,890 Moda Health Plan, Inc. Local PPO/HMO/HCPP 60,740 Altrio Health Plans PACE/Local PPO/HMO/HCPP 35,297 UnitedHealthcare Insurance Company Local PPO/HMO 28,527 Providence Health Local PPO/HMO/HCPP 22,534 PacificSource Community Health Plans Local PPO/HMO 22,279 Sierra Health and Life Insurance Company, Inc. Local PPO/HMO/HCPP 18,798 Kaiser Foundation Health Plan of the Northwest HMO 18,558 AETNA Life Insurance Company Local PPO/HMO 17,111 Total 284,734 Source: Centers for Medicare and Medicaid Services. Enrollment for April
21 Summary of States Approaches to Cost Containment & Reform 21
22 Payment Model and Scale Care Delivery Redesign Financial/Quality Targets Population Health Infrastructure Federal Feasibility Maryland: All-Payer Global Budgets for Hospitals ( ) State determines the total, all-payer revenue target (global budget) for each hospital to decouple revenue from volume and incentivize prevention Hospitals receive fixed global budgets (GBRs) to shift from volume to value-based payments All-payer model: Medicare, Medicaid managed care, and commercial payers (including Medicare Advantage) Hospitals transition from fee-for-service to fixed global budgets Funding for enhanced care management initiatives Funding for quality improvements Limit hospital per capita annual revenue growth to 3.58% Annual quality/value-based adjustments Generate $330 million in Medicare hospital savings over five-year period Reduce readmissions to Medicare national average Reduce hospital acquired conditions by 30% over five-year period (65 preventable complications) Other quality improvement targets (e.g. HCAHPS) Address population health: chronic conditions, deaths from opioid use, and senior health and quality of life (Total Cost of Care, ) Support physicians and other providers who work with high-need Medicare patients through Care Redesign program Health Services Cost Review Commission (40 FTE includes economists, statisticians, accountants, legal, staff, & other; $14.1 million annual budget, 100% from assessments) Robust data collection, reporting, and analytics Federal Medicare Waiver (1977) Participant in the CMS Innovation Center State determines federal Medicare payment amounts to hospitals Source: Maryland Health Services Cost Review Commission (HSCRC) presentation to SB 419 Task Force, January 19,
23 Payment Model and Scale Care Delivery Redesign Financial/Quality Targets Massachusetts: Health Care Cost Growth Benchmark ( ) Sets statewide target to control the growth of total health care expenditures across all payers (public and private); sets target to the state s long-term economic growth rate Health care cost growth benchmark for is 3.6% (actual is 3.55%) All-payer model includes Medicare, Medicaid and commercial payers Strengthens market functioning and system transparency Promotes efficient, high-quality delivery systems with aligned incentives Health Policy Commission promotes triple aim and innovative care delivery Certifies providers as patient-centered medical homes (PCMHs) and accountable care organizations in MA Fosters value-based payment Promotes collaboration and sustained community engagement around whole-person care Enhances transparency of system performance for providers, payers, patients, employers, and state agencies Reduce unnecessary hospital utilization, avoidable emergency department and readmission rates Increase use of APMs by commercial HMO and PPO provider types Total projected savings is $4.67 billion Reduce unnecessary hospital utilization, avoidable ED and readmission rates (per 1,000 individuals) Population Health Lower avoidable health care utilization At-risk adults without a doctor visit (see HPB performance Dashboard for list of metrics, pgs of 2017 Cost Trends Report) Health Policy Commission manages all-payer claims database (FTE ~60 staff, $8.5 million annual budget, fee-based) Infrastructure Collects additional provider and health plan data Robust data collection, reporting and analytics Federal Feasibility No federal participation Sources: Seltz, David (April 20, 2018). Introduction to the Health Policy Commission. Presentation to the Oregon Joint Task Force on Health Care Cost Review. Massachusetts Health Policy Commission (March 2018) Annual Health Care Cost Trends Report. 23
24 Payment Model and Scale Care Delivery Redesign Financial/Quality Targets Population Health Infrastructure Federal Feasibility Pennsylvania Rural Health Model ( ) Rural hospitals receive global budgets for all inpatient and outpatient services to provide for predictable and stable cash flows Global budgets to cover 90% of each hospital s revenue by year 2 30 hospitals will participate by year 3 (45% of all rural PA hospitals) Payers include Medicare FFS, Medicaid managed care, and commercial payers (including Medicare Advantage) Hospitals to redesign their delivery systems based on local health needs Hospitals are to build partnerships with other providers through care coordination and referral patterns to promote population health Hospitals may reduce excess beds, change service delivery lines, or transition operations to outpatient centers State to review hospital plans to ensure access and quality Estimated $35 million in Medicare savings Limit rural hospital cost per capita annualized growth rate to 3.38% across all participating payers Increase access to primary and specialty services Reduce deaths related to substance use disorder (SUD) and improve access to opioid treatment Improve chronic disease management and preventive screenings in target areas: cancer, cardiovascular disease, and obesity/diabetes Short-term: Department of Health to provide end-to-end assistance at no cost Long-term: Rural Health Redesign Center to provide technical assistance including data analytics, quality assurance, and other forms of technical assistance (requires enabling legislation) Participant in the CMS Innovation Center State determines federal Medicare payment amounts for participating rural hospitals Source: Hughes, L. (April 20, 2018). Pennsylvania s Rural Health Model Accelerating Health Care Innovation in Pennsylvania. April 2018 Presentation to the Oregon Joint Task Force on Health Care Cost Review. 24
25 Payment Model and Scale Care Delivery Redesign Financial/Quality Targets Population Health Infrastructure Federal Feasibility Vermont: All-Payer Accountable Care Organization (ACO) Model ( ) ACOs designed to incentivize value and quality using single-payment structure ACOs receive fixed prospective payments for hospitals; remaining providers on FFS or APMs Payers include Medicare FFS, Medicaid, and commercial payers By 2022, 70% of all all-payer beneficiaries and 90% of Medicare beneficiaries enrolled in ACO ACOs to provide a coordinated, system-wide, and integrated reform approach to address Triple Aim through 2022 Enhance care coordination Foster collaboration among community-based providers Transition from volume-driven fee-for-service payment to a value-based prospective model Limit cost growth target to no more than 3.5% in aggregate across all payers (excludes prescription drugs, dental, long-term care) Medicare growth target % below national average Statewide health outcomes and quality of care targets Improve access to primary care Reduce deaths due to suicide and drug overdose Reduce prevalence and morbidity of chronic disease Improve access to primary care Reduce deaths due to suicide and drug overdose Reduce prevalence and morbidity of chronic disease Independent Green Mountain Care Board has regulatory authority including payment and provider rate-setting Existing all-payer claims database, augmented with additional administrative and clinical data sources Participant in the CMS Innovation Center CMS investment of up to $17 million during first two performance years Complementary Medicaid 1115 Waiver (renewal) Sources: Backus, B., Costa, M. (April 20 th, 2018). The Vermont All-Payer Accountable Care Organization Model Agreement. Presentation to the 25 Joint Taskforce on Health Care Cost Review. Green Mountain Care Board,, All-payer Model One Page Summary
26 26
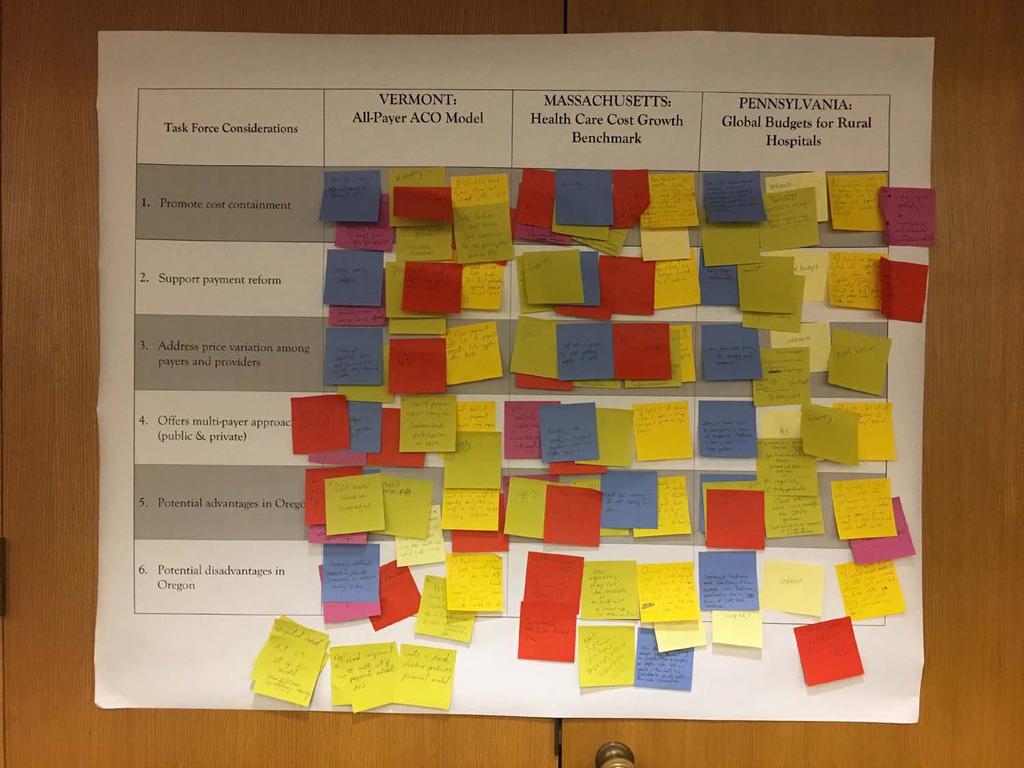
27 Promote cost containment Support payment reform Address price variation among payers and providers Offers multi-payer approach (public & private) Potential advantages in Oregon Potential disadvantages in Oregon VERMONT: All-Payer Accountable Care Organization (ACO) Model Gradual transition from fee-for-service to capitation/aco model Moderate cost containment and cost growth Use of specified goals, trend factors Inpatient and outpatient focus with hospitals and primary providers Early stages with gradual roll-out and adoption Aligns prospective payments across payers through ACOs Flexibility to use alternative payment models (APMs) and non-traditional health services Leverages the role of managed care in Vermont Limited to enrolled members/capitated lives Aligns payment models across several payers Limited, initially, to public payers (Medicare and Medicaid) Gradual participation of commercial payers to establish allpayer model Expansion of CCOs to Medicare and commercial members Expand ACO model like Vermont to reduce health care spending Transition from volume (FFS) to value-based payment Allow leverage of Oregon s existing CCO infrastructure Vermont is significantly different than Oregon (size, single dominant commercial payer) Vermont s experience of failed single-payer Potentially less Medicare funding Administration of policy oversight Limited ability to pay for services outside of ACO model MASSACHUSETTS: Health Care Cost Growth Benchmark Policy-driven; targets total cost of care Minimal through establishing growth target benchmark Benchmark applies to all types of expenditures and provider types Works towards establishing targets for APMs Health Policy Commission (HPC) promotes payment reform through research, public reporting, and promoting investments in new care models Establishes a uniform goal with a single target growth rate for everyone Benchmark may reduce price variation among providers and payers over time Comprehensive, all-payer Enhanced oversight Quicker movement to APMs Lacking strong enforcement to align payers Builds on Oregon s successful 3.4% rate of growth in Medicaid w/ccos Offers flexibility and a market-oriented solution Accountability by state through reporting, committees, and public hearings Mechanism to review and approve hospital budgets Promotes public accountability with minimal penalties Creates a fixed, stable, predictable rate of spending Administrative complexity of HPC; funding needs Feasibility of establishing a new agency Limited enforcement Incomplete measurement of results State as an outlier; questionable long-term ability to stay below annual growth target PENNSYLVANIA: Global Budgets for Rural Hospitals Focus is on rural hospital viability and use of incentives to promote cost containment Long-term strategy geared towards achieving all-payer approach to sustainable financing of rural hospitals Effective model for payment reform Promising model in its initial stages Innovation may drive payment reform through use of global budgets Payment reform offers stable funding and incentives Conceptually through use of global budgets Increases investments in population health; potential to lower utilization and decrease profits Multi-payer except for Medicare; incremental phase-in of commercial payers Voluntary model with use of global budgets among commercial and public payers (Medicaid) Moves away from fee-for-service reimbursement model; stable funding and rural health access Focus on rural hospitals may align with well w/oregon s A & B hospitals Offers unique rural health strategies Promotes rural health redesign with CCOs Potential support among payers and providers Incentivizes hospitals to invest in prevention & reduce volume Voluntary basis may be difficult for payment changes Limited usefulness without Medicare participation May not result in system-wide savings Unknown if rural hospitals in Oregon would embrace this payment model 27 Applicability of global budget to non-rural hospitals (e.g. DRGs)
28 Member Feedback Key Themes Promote Cost-containment Gradual transition from fee-for-service to capitation via accountable care organizations (ACO model) Reduce cost growth, address ability to contain costs, and establish targets for total cost of care Use of specified goals, spending targets, and trend factors Inpatient and outpatient focus among hospitals and primary care providers Use of benchmark applied to all types of health care expenditures and provider types Support Payment Reform Align prospective payments across payers through ACOs Flexibility to use alternative payment models (APMs) and targets including supporting non-traditional health services Address Price Variation Among Payers and Providers Align payment models across public and private payers to reduce price variations among provider types, services and locations 28
29 Member Feedback Key Themes Offers Multi-payer Approach (public and private) Comprehensive, all-payer is more effective Accelerate adoption and spread of APMs across payers Potential Advantages in Oregon Create a fixed, stable, predictable rate of spending/growth Build on Oregon s successful 3.4 percent rate of growth in Medicaid and the coordinated care model Flexible and market-oriented solution Mechanism(s) to review and approve hospital budgets Promote accountability through reporting, transparency, and public hearings Potential Disadvantages in Oregon Applicability to Oregon s unique health care environment Administration complexities Limited enforcement Limited data available to assess outcomes 29
30 Rate-Setting Design Considerations States that adopt rate-setting systems have to consider a number of design questions: 1. Scope: all-payer versus partial-payer whether rate-setting would be limited to private insurers or also include Medicare and Medicaid? 2. Services: whether to apply rate-setting to inpatient services, or also regulate outpatient and physician services? 3. Governance: who in the state would have the authority to oversee and manage the system, and how should it be funded? 4. Payment Structure: how to set payment methods per unit (paying for episodes vs. individual services) compared to payment rates (capping total annual revenue per hospital or revenue per admission) 5. Innovation: how to ensure the system supports payment innovations (e.g., use of incentives to pay higher rates in return for quality metrics/outcomes) 6. Transition Period: how to establish base rate(s), inflation factor, adjustments among hospital, annual updates Sommers, A., White, C., & Ginsburg, P. (2012). Addressing Hospital Pricing Leverage Through Regulation: State Rate Setting. National Institute for Health Care Reform Policy Review, 9 (May).
31 TASK FORCE DISCUSSION 31
32 Guidelines for Today s Discussion We will spend 10 minutes reviewing each policy strategy (7 strategies in total) Members will be asked to share their thoughts on each policy strategy (i.e., matrix homework assignment) Staff will capture the discussion using flip charts Chair Smith will invite members to elaborate on their responses for each policy strategy Dot Exercise (10-15 minutes) Staff will prepare written summary before the next meeting (June 15 th )
33 POLICY GOALS POLICY STRATEGIES Address Hospital Cost Drivers Promote Cost Containment Decrease Annual Expenditure Growth Reduce Price Variation Address Affordability Support Payment Reform Reduce Complexity Hospital Rate-Setting (MD) Establish and approve rates for costs of inpatient services Standardize basis of payment for services Global Budgets for Hospitals (MD and PA) Transition rural hospitals from costbased reimbursement to global budgets Incentivize prevention and population health Accountable Care Organizations (VT) Expand CCO model to Medicare enrollees (traditional/medicare Advantage) Align payment and incentives across payers 33
34 POLICY GOALS POLICY STRATEGIES Address Hospital Cost Drivers Promote Cost Containment Decrease Annual Expenditure Growth Reduce Price Variation Address Affordability Support Payment Reform Reduce Complexity Hospital Rate-Setting (MD) Establish and approve rates for costs of inpatient services Standardize basis of payment for services Global Budgets for Hospitals (MD and PA) Transition rural hospitals from costbased reimbursement to global budgets Incentivize prevention and population health Accountable Care Organizations (VT) Expand CCO model to Medicare enrollees (traditional/medicare Advantage) Align payment and incentives across payers 34
35 POLICY GOALS POLICY STRATEGIES Address Hospital Cost Drivers Promote Cost Containment Decrease Annual Expenditure Growth Reduce Price Variation Address Affordability Support Payment Reform Reduce Complexity Accountable Care Organizations (VT) Expand CCO model to Medicare enrollees (traditional/medicare Advantage) Align payment and incentives across payers Multi-payer/All-payer Participation (MD, PA & VT) Align and standardize payment models across Medicaid, Medicare, commercial (e.g., PEBB/OEBB), employersponsored plans 35
36 POLICY STRATEGIES Address Hospital Cost Drivers Promote Cost Containment Decrease Annual Expenditure Growth POLICY GOALS Reduce Price Variation Address Affordability Support Payment Reform Reduce Complexity Annual Growth Target & State Benchmark (MA & VT) Establish single target growth rate for all payers and providers Fixed, stable, and predictable rate of spending Allow market flexibility to meet benchmark(s) Create penalties and/or incentives for outliers Regulatory vs. Market-Based (MD, MA, PA, & VT) Public utility and ratesetting model with regulatory authority Independent authority to review rates; monitor and strengthen market functioning Public Reporting &Transparency (MD & MD) Create tools to increase visibility into cost and utilization data Statewide reporting and analysis of quality and cost across providers, health plans, and payers 36
37 POLICY STRATEGIES Address Hospital Cost Drivers Promote Cost Containment Decrease Annual Expenditure Growth POLICY GOALS Reduce Price Variation Address Affordability Support Payment Reform Reduce Complexity Annual Growth Target & State Benchmark (MA & VT) Establish single target growth rate for all payers and providers Fixed, stable, and predictable rate of spending Allow market flexibility to meet benchmark(s) Create penalties and/or incentives for outliers Regulatory vs. Market-Based (MD, MA, PA, & VT) Public utility and ratesetting model with regulatory authority Independent authority to review rates; monitor and strengthen market functioning Public Reporting &Transparency (MD & MD) Create tools to increase visibility into cost and utilization data Statewide reporting and analysis of quality and cost across providers, health plans, and payers 37
38 POLICY STRATEGIES Address Hospital Cost Drivers Promote Cost Containment Decrease Annual Expenditure Growth POLICY GOALS Reduce Price Variation Address Affordability Support Payment Reform Reduce Complexity Annual Growth Target & State Benchmark (MA & VT) Establish single target growth rate for all payers and providers Fixed, stable, and predictable rate of spending Allow market flexibility to meet benchmark(s) Create penalties and/or incentives for outliers Regulatory vs. Market-Based (MD, MA, PA, & VT) Public utility and ratesetting model with regulatory authority Independent authority to review rates; monitor and strengthen market functioning Public Reporting &Transparency (MD & MD) Create tools to increase visibility into cost and utilization data Statewide reporting and analysis of quality and cost across providers, health plans, and payers 38
39 Member Feedback Jesse O Brien, OSPIRG (OLIS) Establish a policy framework to enable Oregon to move in that direction incrementally instead of all at once, and that would allow the state to be flexible in implementing new payment and health care delivery models while holding the health care industry accountable for achieving a sustainable rate of health care cost growth. Formation of a Health Care Cost Commission similar to the one in Massachusetts. Empowering the Cost Commission to study and recommend a set of implementation and enforcement tools, subject to Legislative approval.
40 Guidelines for Dot Exercise 10 Minutes for Exercise Vote on all seven policy strategies Two dots per policy strategy (use no more 14 dots total) Vote with the dots that best communications your perspective and position on each policy strategy Green dot Yes, this concept supports Oregon s goals Red dot No, this concept does not support Oregon s goals Yellow Dot I am neutral on this concept Blue Dot I need more information before I can form an opinion
41 Next Steps LPRO staff to develop straw proposals based on feedback and guidance shared by members Remaining meetings June 15 th Develop recommendations July 13 th Create report outline and key content August 17 th Finalize recommendations and adopt report
42 PUBLIC COMMENT 42
43 Payment System Basics Bundling of services increases Capitation Cost-based payment Hospital not at-risk Services the hospital is at risk for across these different Bases of Payment 43
44 Payment System Basics (continued) Bundling of services increases Capitation Strength of cost containment incentives increases Provider more risk Payer less risk Services the hospital is at risk for across these different Bases of Payment 44
Maryland Health Services Cost Review Commission (HSCRC) Global Budget Revenue (GBR) under the Maryland All-Payer Model
 Global Budget Revenue (GBR) under the Maryland All-Payer Model") Maryland Health Services Cost Review Commission (HSCRC) Global Budget Revenue (GBR) under the Maryland All-Payer Model January 19, 2018 1 Goals of Today s Discussion Overview of Maryland s unique healthcare
Maryland Health Services Cost Review Commission (HSCRC) Global Budget Revenue (GBR) under the Maryland All-Payer Model January 19, 2018 1 Goals of Today s Discussion Overview of Maryland s unique healthcare
In accordance with Act 124 of 2018 (H.914)
") State of Vermont Green Mountain Care Board 144 State Street Montpelier VT 05620 Report to the Legislature REPORT ON THE GREEN MOUNTAIN CARE BOARD S PROGRESS IN MEETING ALL-PAYER ACO MODEL IMPLEMENTATION
State of Vermont Green Mountain Care Board 144 State Street Montpelier VT 05620 Report to the Legislature REPORT ON THE GREEN MOUNTAIN CARE BOARD S PROGRESS IN MEETING ALL-PAYER ACO MODEL IMPLEMENTATION
Adopting Multi-Payer and All- Payer Payment Models in States OCTOBER 25, 2016 WASHINGTON MARRIOTT WARDMAN PARK HOTEL WASHINGTON, DC
 Adopting Multi-Payer and All- Payer Payment Models in States OCTOBER 25, 2016 WASHINGTON MARRIOTT WARDMAN PARK HOTEL WASHINGTON, DC Medicaid and Private Payer Alignment for APMs Marni Bussell SIM Project
Adopting Multi-Payer and All- Payer Payment Models in States OCTOBER 25, 2016 WASHINGTON MARRIOTT WARDMAN PARK HOTEL WASHINGTON, DC Medicaid and Private Payer Alignment for APMs Marni Bussell SIM Project
Clinic Comparison Reporting. June 30, 2016
 Clinic Comparison Reporting June 30, 2016 Agenda Introduction and Background Meredith Roberts Tomasi, Q Corp Program Director Measures, Methodology and Reports Doug Rupp, Q Corp Senior Analyst Application
Clinic Comparison Reporting June 30, 2016 Agenda Introduction and Background Meredith Roberts Tomasi, Q Corp Program Director Measures, Methodology and Reports Doug Rupp, Q Corp Senior Analyst Application
Total Cost of Care in Oregon s Commercial Market. February 24, 2017
 Total Cost of Care in Oregon s Commercial Market February 24, 2017 Background: Q Corp About us Independent, nonprofit organization Neutral, multistakeholder collaboration Celebrated our 16 th anniversary
Total Cost of Care in Oregon s Commercial Market February 24, 2017 Background: Q Corp About us Independent, nonprofit organization Neutral, multistakeholder collaboration Celebrated our 16 th anniversary
Total Cost of Care in Oregon s Commercial Market. March 2, 2017
 Total Cost of Care in Oregon s Commercial Market March 2, 2017 Background: Q Corp About us Independent, nonprofit organization Neutral, multistakeholder collaboration Celebrated our 16 th anniversary Mission
Total Cost of Care in Oregon s Commercial Market March 2, 2017 Background: Q Corp About us Independent, nonprofit organization Neutral, multistakeholder collaboration Celebrated our 16 th anniversary Mission
All Payer Hospital System Modernization Payment Models Workgroup. Meeting Agenda
 All Payer Hospital System Modernization Payment Models Workgroup Meeting Agenda September 5, 2018 9:00 am to 11:00 am Health Services Cost Review Commission Conference Room 100 4160 Patterson Avenue Baltimore,
All Payer Hospital System Modernization Payment Models Workgroup Meeting Agenda September 5, 2018 9:00 am to 11:00 am Health Services Cost Review Commission Conference Room 100 4160 Patterson Avenue Baltimore,
San Francisco Health Service System Health Service Board
 San Francisco Health Service System Health Service Board Medicare Advantage Marketplace Overview December 13, 2018 Prepared by: Health & Benefits Medicare Advantage Marketplace Overview Agenda Medicare
San Francisco Health Service System Health Service Board Medicare Advantage Marketplace Overview December 13, 2018 Prepared by: Health & Benefits Medicare Advantage Marketplace Overview Agenda Medicare
RE: Additional Input regarding Accountable Care Organizations (ACOs) and the Medicare Shared Saving Program
 and the Medicare Shared Saving Program") 221 MAIN STREET, SUITE 1500 SAN FRANCISCO, CA 94105 PBGH.ORG OFFICE 415.281.8660 FACSIMILE 415.520.0927 February 14, 2011 Donald M. Berwick, M.D. Administrator Centers for Medicare and Medicaid Services
221 MAIN STREET, SUITE 1500 SAN FRANCISCO, CA 94105 PBGH.ORG OFFICE 415.281.8660 FACSIMILE 415.520.0927 February 14, 2011 Donald M. Berwick, M.D. Administrator Centers for Medicare and Medicaid Services
Total Cost of Care (TCOC) Workgroup. January 30, 2019
 Workgroup. January 30, 2019") Total Cost of Care (TCOC) Workgroup January 30, 2019 Agenda Introductions Updates on initiatives with CMS Y1 MPA (PY18) Implementation Timing Y2 MPA (PY19) MPA Operations Reporting and Attribution Stability
Total Cost of Care (TCOC) Workgroup January 30, 2019 Agenda Introductions Updates on initiatives with CMS Y1 MPA (PY18) Implementation Timing Y2 MPA (PY19) MPA Operations Reporting and Attribution Stability
Vermont Medicaid Next Generation Pilot Program 2017 Performance
 State of Vermont Department of Vermont Health Access NOB 1 South, 1 st Floor 280 State Drive Waterbury, Vermont 05671 REPORT TO THE GENERAL ASSEMBLY Vermont Medicaid Next Generation Pilot Program 2017
State of Vermont Department of Vermont Health Access NOB 1 South, 1 st Floor 280 State Drive Waterbury, Vermont 05671 REPORT TO THE GENERAL ASSEMBLY Vermont Medicaid Next Generation Pilot Program 2017
Medicare Advantage: Program Overview and Recent Experience. James Cosgrove, Ph.D. Director, Health Care U.S. Government Accountability Office
 Medicare Advantage: Program Overview and Recent Experience James Cosgrove, Ph.D. Director, Health Care U.S. Government Accountability Office January 15, 2009 01/15/2009 1 In 2008, About 22 Percent of Medicare
Medicare Advantage: Program Overview and Recent Experience James Cosgrove, Ph.D. Director, Health Care U.S. Government Accountability Office January 15, 2009 01/15/2009 1 In 2008, About 22 Percent of Medicare
Session 1: Mandated Report: Medicare Payment for Ambulance Services
 Medicare Payment Advisory Committee Meeting, Nov. 1 2 Session 1: Mandated Report: Medicare Payment for Ambulance Services Session 2: Reducing the Hospitalization Rate for Medicare Beneficiaries Receiving
Medicare Payment Advisory Committee Meeting, Nov. 1 2 Session 1: Mandated Report: Medicare Payment for Ambulance Services Session 2: Reducing the Hospitalization Rate for Medicare Beneficiaries Receiving
The Emergence of Value-Based Care: Present and Future Tense
 The Emergence of Value-Based Care: Present and Future Tense Erik Johnson, Vice President for Value-Based Care May 2016 What Is Value-Based Care? While the concept of value-based care has existed for years,
The Emergence of Value-Based Care: Present and Future Tense Erik Johnson, Vice President for Value-Based Care May 2016 What Is Value-Based Care? While the concept of value-based care has existed for years,
Vermont Legislative Joint Fiscal Office
 Vermont Legislative Joint Fiscal Office One Baldwin Street Montpelier, VT 05633-5701 (802) 828-2295 Fax: (802) 828-2483 ISSUE BRIEF Date: October 21, 2016 Prepared by: JFO Staff* DRAFT FOR DISCUSSION This
Vermont Legislative Joint Fiscal Office One Baldwin Street Montpelier, VT 05633-5701 (802) 828-2295 Fax: (802) 828-2483 ISSUE BRIEF Date: October 21, 2016 Prepared by: JFO Staff* DRAFT FOR DISCUSSION This
Medicare payment policy and its impact on program spending
 Medicare payment policy and its impact on program spending James E. Mathews, Ph.D. Deputy Director, Medicare Payment Advisory Commission February 8, 2013 Outline of today s presentation Brief background
Medicare payment policy and its impact on program spending James E. Mathews, Ph.D. Deputy Director, Medicare Payment Advisory Commission February 8, 2013 Outline of today s presentation Brief background
The Medicare Advantage program: Status report
 C H A P T E R12 The Medicare Advantage program: Status report C H A P T E R 12 The Medicare Advantage program: Status report Chapter summary In this chapter Each year the Commission provides a status
C H A P T E R12 The Medicare Advantage program: Status report C H A P T E R 12 The Medicare Advantage program: Status report Chapter summary In this chapter Each year the Commission provides a status
GMCB Update Health Reform Oversight Committee. Chair Kevin Mullin and Michael Barber October 25, 2018
 GMCB Update Health Reform Oversight Committee Chair Kevin Mullin and Michael Barber October 25, 2018 1 2 Hospital Budgets Hospitals initially requested a 2.9% increase in Net Patient Revenue (NPR) from
GMCB Update Health Reform Oversight Committee Chair Kevin Mullin and Michael Barber October 25, 2018 1 2 Hospital Budgets Hospitals initially requested a 2.9% increase in Net Patient Revenue (NPR) from
In This Issue (click to jump):
:") May 7, 2014 In This Issue (click to jump): Analysis of Trends in Health Spending 2013 2014 Spotlight on Medicare Advantage Enrollment Oncology Drug Trend Report S&P Predicts Shift from Job-Based Coverage
May 7, 2014 In This Issue (click to jump): Analysis of Trends in Health Spending 2013 2014 Spotlight on Medicare Advantage Enrollment Oncology Drug Trend Report S&P Predicts Shift from Job-Based Coverage
The 2018 Advance Notice and Draft Call Letter for Medicare Advantage
 The 2018 Advance Notice and Draft Call Letter for Medicare Advantage POLICY PRIMER FEBRUARY 2017 Summary Introduction On February 1, 2017, the Centers for Medicare & Medicaid Services (CMS) released the
The 2018 Advance Notice and Draft Call Letter for Medicare Advantage POLICY PRIMER FEBRUARY 2017 Summary Introduction On February 1, 2017, the Centers for Medicare & Medicaid Services (CMS) released the
Figure 1: Original APM Framework
 Contents Overview... 2 This Year s APM Measurement Effort... 3 Scope... 3 Data Source... 4 The LAN Survey... 4 The Blue Cross Blue Shield Association Survey... 8 The America s Health Insurance Plans Survey...
Contents Overview... 2 This Year s APM Measurement Effort... 3 Scope... 3 Data Source... 4 The LAN Survey... 4 The Blue Cross Blue Shield Association Survey... 8 The America s Health Insurance Plans Survey...
Medicare Advantage (Part C) Review
 Review") Medicare Advantage (Part C) Review 1 Medicare For people 65+ and under 65 with a disability 4 parts of Medicare Part A: Hospital Insurance Part B: Medical Insurance Part C: Medicare Advantage Plans Part
Medicare Advantage (Part C) Review 1 Medicare For people 65+ and under 65 with a disability 4 parts of Medicare Part A: Hospital Insurance Part B: Medical Insurance Part C: Medicare Advantage Plans Part
TRACKING MEDICARE HEALTH AND PRESCRIPTION DRUG PLANS Monthly Report for April 2007
 TRACKING MEDICARE HEALTH AND PRESCRIPTION DRUG PLANS Monthly Report for April 2007 Prepared by Stephanie Peterson and Marsha Gold, Mathematica Policy Research Inc. as part of work commissioned by the Kaiser
TRACKING MEDICARE HEALTH AND PRESCRIPTION DRUG PLANS Monthly Report for April 2007 Prepared by Stephanie Peterson and Marsha Gold, Mathematica Policy Research Inc. as part of work commissioned by the Kaiser
First a word about the rising cost of retiree healthcare
 Medicare Trends First a word about the rising cost of retiree healthcare The average 66-year-old couple is expected to spend nearly 60% of their Social Security income on medical bills, according to a
Medicare Trends First a word about the rising cost of retiree healthcare The average 66-year-old couple is expected to spend nearly 60% of their Social Security income on medical bills, according to a
Point of View: Medicare Profitability in a Reform Market
 Point of View: Profitability in a Reform Market Bill Eggbeer, Managing Director, & Krista Bowers, Director, BDC Advisors, LLC Introduction Overall, accounts for approximately 20% of the total domestic
Point of View: Profitability in a Reform Market Bill Eggbeer, Managing Director, & Krista Bowers, Director, BDC Advisors, LLC Introduction Overall, accounts for approximately 20% of the total domestic
Better Medicare Alliance Webinar: Medicare Advantage and Part D 2019 Advance Notice and Draft Call Letter. February 8, 2018
 Better Medicare Alliance Webinar: Medicare Advantage and Part D 2019 Advance Notice and Draft Call Letter February 8, 2018 RATE NOTICE CRASH Opening COURSE Remarks PAGE http://bettermedicarealliance.org/campaigns
Better Medicare Alliance Webinar: Medicare Advantage and Part D 2019 Advance Notice and Draft Call Letter February 8, 2018 RATE NOTICE CRASH Opening COURSE Remarks PAGE http://bettermedicarealliance.org/campaigns
Population-Based Healthcare: Structural Models and Options
 Population-Based Healthcare: Structural Models and Options George Choriatis, Esq. Rivkin Radler LLP Presented at: Annual Fall Meeting New York State Bar Association Health Law Section Albany, New York
Population-Based Healthcare: Structural Models and Options George Choriatis, Esq. Rivkin Radler LLP Presented at: Annual Fall Meeting New York State Bar Association Health Law Section Albany, New York
2018 Medicare Advantage and Part D Rate Announcement and Call Letter, and Request
 2018 Medicare Advantage and Part D Rate Announcement and Call Letter, and Request for Information Date 2017-04-03 Title 2018 Medicare Advantage and Part D Rate Announcement and Call Letter, and Request
2018 Medicare Advantage and Part D Rate Announcement and Call Letter, and Request for Information Date 2017-04-03 Title 2018 Medicare Advantage and Part D Rate Announcement and Call Letter, and Request
Medicare Health Plans
 Medicare Health Plans Part 2 Version 10.0 June 20, 2016 Terms and Conditions This training program is protected under United States Copyright laws, 17 U.S.C.A. 101, et seq. and international treaties.
Medicare Health Plans Part 2 Version 10.0 June 20, 2016 Terms and Conditions This training program is protected under United States Copyright laws, 17 U.S.C.A. 101, et seq. and international treaties.
Stuart H. Altman. The Changing Health Care System: Economic Forces Pushing States To Become More Involved
 The Changing Health Care System: Economic Forces Pushing States To Become More Involved Stuart H. Altman Sol Chaikin Professor of Health Policy The Heller School for Social Policy and Management Brandeis
The Changing Health Care System: Economic Forces Pushing States To Become More Involved Stuart H. Altman Sol Chaikin Professor of Health Policy The Heller School for Social Policy and Management Brandeis
Implementation of the Maryland All Payer Model Care Coordination, Integration, and Alignment. May 2015
 Implementation of the Maryland All Payer Model Care Coordination, Integration, and Alignment May 2015 1 HSCRC Strategic Roadmap State-Level Infrastructure (leverages many other large investments) Create
Implementation of the Maryland All Payer Model Care Coordination, Integration, and Alignment May 2015 1 HSCRC Strategic Roadmap State-Level Infrastructure (leverages many other large investments) Create
Healthcare Reform and Its Impact on the Care Delivery System
 Healthcare Reform and Its Impact on the Care Delivery System Agenda 1) The Era of Healthcare Reform 2) Healthcare Reform and Post-Acute Care 3) Succeeding in the Reform Era: Managing the Continuum of Health
Healthcare Reform and Its Impact on the Care Delivery System Agenda 1) The Era of Healthcare Reform 2) Healthcare Reform and Post-Acute Care 3) Succeeding in the Reform Era: Managing the Continuum of Health
Performance Measurement Work Group Meeting 01/17/2018
 Performance Measurement Work Group Meeting 01/17/2018 Agenda RY 2020 MHAC DRAFT FINAL Policy Modeling Additional Stakeholder feedback? RY 2020 RRIP Improvement Target National Forecasting (data delays);
Performance Measurement Work Group Meeting 01/17/2018 Agenda RY 2020 MHAC DRAFT FINAL Policy Modeling Additional Stakeholder feedback? RY 2020 RRIP Improvement Target National Forecasting (data delays);
January 16, Seema Verma Administrator Centers for Medicare & Medicaid Services 7500 Security Boulevard Baltimore, MD 21244
 Seema Verma Administrator Centers for Medicare & Medicaid Services 7500 Security Boulevard Baltimore, MD 21244 RE: CMS-4182-P: Medicare Program; Contract Year 2019 Policy and Technical Changes to the Medicare
Seema Verma Administrator Centers for Medicare & Medicaid Services 7500 Security Boulevard Baltimore, MD 21244 RE: CMS-4182-P: Medicare Program; Contract Year 2019 Policy and Technical Changes to the Medicare
The Health Insurance Market in Virginia. Maureen Dempsey, MD, MSc, ACC, FAAP Anthem Blue Cross and Blue Shield June 8, 2017
 The Health Insurance Market in Virginia Maureen Dempsey, MD, MSc, ACC, FAAP Anthem Blue Cross and Blue Shield June 8, 2017 Anthem Inc. at a Glance Broad geographic footprint and customer base ` BCBS plans
The Health Insurance Market in Virginia Maureen Dempsey, MD, MSc, ACC, FAAP Anthem Blue Cross and Blue Shield June 8, 2017 Anthem Inc. at a Glance Broad geographic footprint and customer base ` BCBS plans
TRACKING MEDICARE HEALTH AND PRESCRIPTION DRUG PLANS Monthly Report for February 2008
 TRACKING MEDICARE HEALTH AND PRESCRIPTION DRUG PLANS Monthly Report for February 2008 Prepared by Stephanie Peterson and Marsha Gold, Mathematica Policy Research Inc. as part of work commissioned by the
TRACKING MEDICARE HEALTH AND PRESCRIPTION DRUG PLANS Monthly Report for February 2008 Prepared by Stephanie Peterson and Marsha Gold, Mathematica Policy Research Inc. as part of work commissioned by the
Health Information Technology and Management
 Health Information Technology and Management CHAPTER 9 Healthcare Coding and Reimbursement Pretest (True/False) CPT-4 codes are used to bill for disease and illness. Medicare Part B provides medical insurance
Health Information Technology and Management CHAPTER 9 Healthcare Coding and Reimbursement Pretest (True/False) CPT-4 codes are used to bill for disease and illness. Medicare Part B provides medical insurance
Comprehensive Primary Care Payment Calculator User s Guide
 1 Comprehensive Primary Care Payment Calculator User s Guide Prepared by Health Data Decisions August 2017 Disclaimer: Information provided in connection with this calculator by FMAHealth and its contributors
1 Comprehensive Primary Care Payment Calculator User s Guide Prepared by Health Data Decisions August 2017 Disclaimer: Information provided in connection with this calculator by FMAHealth and its contributors
Deep Dive Medicare Advantage Advance Notices Part I and II
 Deep Dive Medicare Advantage Advance Notices Part I and II Noah Champagne, FSA, MAAA Noah Champagne is a consulting actuary in Milliman s New York office. Noah has a breadth of Medicare experience working
Deep Dive Medicare Advantage Advance Notices Part I and II Noah Champagne, FSA, MAAA Noah Champagne is a consulting actuary in Milliman s New York office. Noah has a breadth of Medicare experience working
Context: Innovation in Maryland
 May 15, 2014 Joshua M. Sharfstein, M.D. Maryland All-Payer Hospital Model Context: Innovation in Maryland 2 Josh Sharfstein, MD 1 BACKGROUND OF MARYLAND RATE REGULATION Health Services Cost Review Commission
May 15, 2014 Joshua M. Sharfstein, M.D. Maryland All-Payer Hospital Model Context: Innovation in Maryland 2 Josh Sharfstein, MD 1 BACKGROUND OF MARYLAND RATE REGULATION Health Services Cost Review Commission
No An act relating to health care financing and universal access to health care in Vermont. (S.88)
") No. 128. An act relating to health care financing and universal access to health care in Vermont. (S.88) It is hereby enacted by the General Assembly of the State of Vermont: Sec. 1. FINDINGS * * * HEALTH
No. 128. An act relating to health care financing and universal access to health care in Vermont. (S.88) It is hereby enacted by the General Assembly of the State of Vermont: Sec. 1. FINDINGS * * * HEALTH
10/17/2014 Risk-Based Payment Methodologies A National Perspective Art Jones, MD. AccountableCareInstitute.com
 10/17/2014 Risk-Based Payment Methodologies A National Perspective Art Jones, MD FQHCs Bridge the Gap in Care Bridge Built and Maintained by FFS Dollars 2 CMMI View of FFS Medicine 3 Accountability High
10/17/2014 Risk-Based Payment Methodologies A National Perspective Art Jones, MD FQHCs Bridge the Gap in Care Bridge Built and Maintained by FFS Dollars 2 CMMI View of FFS Medicine 3 Accountability High
Gulf Coast and LA HFMA Payer Summit Value-based contracts same healthcare business?
 Gulf Coast and LA HFMA Payer Summit Value-based contracts same healthcare business? Richard R. Vath, MD FMOLHS SVP/Chief Clinical Transformation Officer President Health Leaders Network and Medicare ACO
Gulf Coast and LA HFMA Payer Summit Value-based contracts same healthcare business? Richard R. Vath, MD FMOLHS SVP/Chief Clinical Transformation Officer President Health Leaders Network and Medicare ACO
Medicaid Payment and Delivery System Innovation: Minnesota s Experience
 Medicaid Payment and Delivery System Innovation: Minnesota s Experience MARIE ZIMMERMAN, MEDICAID DIRECTOR MINNESOTA DEPARTMENT OF HUMAN SERVICES MILBANK RSG 2015 Health Reforms in Minnesota MNSure (state
Medicaid Payment and Delivery System Innovation: Minnesota s Experience MARIE ZIMMERMAN, MEDICAID DIRECTOR MINNESOTA DEPARTMENT OF HUMAN SERVICES MILBANK RSG 2015 Health Reforms in Minnesota MNSure (state
Affordable Care Act Update: Implementing Medicare Costs Savings
 Affordable Care Act Update: Implementing Medicare Costs Savings This new law recognizes that Medicare isn t just something that you re entitled to when you reach 65; it s something that you ve earned.
Affordable Care Act Update: Implementing Medicare Costs Savings This new law recognizes that Medicare isn t just something that you re entitled to when you reach 65; it s something that you ve earned.
Part One: FEDERAL POLICY AND MEDICARE S IMPACT ON THE ECONOMY
 Introducing the first in a three-part series of white papers designed to explore 1) Why the nation s health system is facing a financial crisis, 2) How providers that accept Medicare Advantage plans and
Introducing the first in a three-part series of white papers designed to explore 1) Why the nation s health system is facing a financial crisis, 2) How providers that accept Medicare Advantage plans and
All Payer Hospital System Modernization Payment Models Workgroup. Meeting Agenda
 All Payer Hospital System Modernization Payment Models Workgroup Meeting Agenda January 16, 2018 1:00 pm to 3:00 pm Health Services Cost Review Commission Conference Room 100 4160 Patterson Avenue Baltimore,
All Payer Hospital System Modernization Payment Models Workgroup Meeting Agenda January 16, 2018 1:00 pm to 3:00 pm Health Services Cost Review Commission Conference Room 100 4160 Patterson Avenue Baltimore,
Medicare Overview. James Cosgrove, Director U.S. Government Accountability Office (GAO) February 8, 2013
 February 8, 2013") Medicare Overview James Cosgrove, Director U.S. Government Accountability Office (GAO) February 8, 2013 Presentation Outline General Structure, Eligibility, and Beneficiaries Medicare Providers Medicare
Medicare Overview James Cosgrove, Director U.S. Government Accountability Office (GAO) February 8, 2013 Presentation Outline General Structure, Eligibility, and Beneficiaries Medicare Providers Medicare
Estimated Federal Impact of a Proposal to Shift Hospice Spending to Medicare Advantage
 To: National Hospice and Palliative Care Organization From: Avalere Health Date: Re: Estimated Federal Impact of a Proposal to Shift Hospice Spending to Medicare Advantage Summary The National Hospice
To: National Hospice and Palliative Care Organization From: Avalere Health Date: Re: Estimated Federal Impact of a Proposal to Shift Hospice Spending to Medicare Advantage Summary The National Hospice
Catalyzing Payment Innovation. Suzanne Delbanco, Ph.D. Executive Director September 20, 2012
 Catalyzing Payment Innovation Suzanne Delbanco, Ph.D. Executive Director September 20, 2012 Payment Reform: Why Should We Care? The health care payment systems of the status quo continue to drain the value
Catalyzing Payment Innovation Suzanne Delbanco, Ph.D. Executive Director September 20, 2012 Payment Reform: Why Should We Care? The health care payment systems of the status quo continue to drain the value
March 28, Dear Administrator Slavitt:
 20555 Victor Parkway Livonia, MI 48152 tel 734-343-1000 trinity-health.org March 28, 2016 Andy Slavitt Administrator Center for Medicare and Medicaid Services U.S. Department of Health and Human Services
20555 Victor Parkway Livonia, MI 48152 tel 734-343-1000 trinity-health.org March 28, 2016 Andy Slavitt Administrator Center for Medicare and Medicaid Services U.S. Department of Health and Human Services
Medicare Advantage (MA) Proposed Benchmark Update and Other Adjustments for CY2020: In Brief
 Proposed Benchmark Update and Other Adjustments for CY2020: In Brief") Medicare Advantage (MA) Proposed Benchmark Update and Other Adjustments for CY2020: In Brief February 7, 2019 Congressional Research Service https://crsreports.congress.gov R45494 Contents Introduction...
Medicare Advantage (MA) Proposed Benchmark Update and Other Adjustments for CY2020: In Brief February 7, 2019 Congressional Research Service https://crsreports.congress.gov R45494 Contents Introduction...
Value of Medicare Advantage to Low-Income and Minority Medicare Beneficiaries. By: Adam Atherly, Ph.D. and Kenneth E. Thorpe, Ph.D.
 Value of Medicare Advantage to Low-Income and Minority Medicare Beneficiaries By: Adam Atherly, Ph.D. and Kenneth E. Thorpe, Ph.D. September 20, 2005 Value of Medicare Advantage to Low-Income and Minority
Value of Medicare Advantage to Low-Income and Minority Medicare Beneficiaries By: Adam Atherly, Ph.D. and Kenneth E. Thorpe, Ph.D. September 20, 2005 Value of Medicare Advantage to Low-Income and Minority
Health Service Board Rates and Benefits Committee Meeting
 Health Service Board Rates and Benefits Committee Meeting Blue Shield Medical Group ACO Review April 10, 2014 Prepared by Aon Hewitt Health and Benefits Contents History ACO Overview Evaluation Framework
Health Service Board Rates and Benefits Committee Meeting Blue Shield Medical Group ACO Review April 10, 2014 Prepared by Aon Hewitt Health and Benefits Contents History ACO Overview Evaluation Framework
March 1, Dear Mr. Kouzoukas:
 March 1, 2019 Mr. Demetrios L. Kouzoukas Principal Deputy Administrator and Director Center for Medicare Centers for Medicare & Medicaid Services 7500 Security Boulevard Baltimore, MD 21244 Re: Advance
March 1, 2019 Mr. Demetrios L. Kouzoukas Principal Deputy Administrator and Director Center for Medicare Centers for Medicare & Medicaid Services 7500 Security Boulevard Baltimore, MD 21244 Re: Advance
Medicare Payment Advisory Commission (MedPAC) January Meeting Summary
 January Meeting Summary") Medicare Payment Advisory Commission (MedPAC) January Meeting Summary The Medicare Payment Advisory Commission (MedPAC) is an independent Congressional agency established by the Balanced Budget Act of
Medicare Payment Advisory Commission (MedPAC) January Meeting Summary The Medicare Payment Advisory Commission (MedPAC) is an independent Congressional agency established by the Balanced Budget Act of
Healthcare Reform. North Carolina Dietetic Association September 12, Duke Medicine
 Healthcare Reform North Carolina Dietetic Association September 12, 2014 Take home messages Healthcare [and health insurance] is transforming at an accelerating pace Key metrics of concern relate to quality,
Healthcare Reform North Carolina Dietetic Association September 12, 2014 Take home messages Healthcare [and health insurance] is transforming at an accelerating pace Key metrics of concern relate to quality,
Developing Your Value Proposition. Timothy P. McNeill, RN, MPH
 Developing Your Value Proposition Timothy P. McNeill, RN, MPH What is a Value Proposition A value proposition is the service or feature that makes an organization attractive to potential customers The
Developing Your Value Proposition Timothy P. McNeill, RN, MPH What is a Value Proposition A value proposition is the service or feature that makes an organization attractive to potential customers The
Understanding the 2020 Medicare Advantage Advance Notice Part I
 Understanding the 2020 Medicare Advantage Advance Notice Part I Jennifer Carioto, FSA, MAAA Jennifer Carioto is a consulting actuary with the New York office of Milliman. She specializes in Medicare Advantage
Understanding the 2020 Medicare Advantage Advance Notice Part I Jennifer Carioto, FSA, MAAA Jennifer Carioto is a consulting actuary with the New York office of Milliman. She specializes in Medicare Advantage
9/23/2016. Our Services. Transitioning from Fee-for-Service to Value-based Reimbursement. Key Trends and Strategies for Rural Health Providers
 Transitioning from Fee-for-Service to Value-based Reimbursement Key Trends and Strategies for Rural Health Providers Paul MacLellan, CEO >> Health care consulting company >> Wholly owned subsidiary of
Transitioning from Fee-for-Service to Value-based Reimbursement Key Trends and Strategies for Rural Health Providers Paul MacLellan, CEO >> Health care consulting company >> Wholly owned subsidiary of
Draft Recommendations on the Update Factors for FY 2017
 Draft Recommendations on the Update Factors for FY 2017 May 2, 2016 Health Services Cost Review Commission 4160 Patterson Avenue Baltimore, Maryland 21215 (410) 764-2605 FAX: (410) 358-6217 This document
Draft Recommendations on the Update Factors for FY 2017 May 2, 2016 Health Services Cost Review Commission 4160 Patterson Avenue Baltimore, Maryland 21215 (410) 764-2605 FAX: (410) 358-6217 This document
Paying More for Less
 Paying More for Less Congress promises to help Medicare beneficiaries by covering prescription drugs BUT Medicare beneficiaries in New York will pay more under proposed reforms! The Impact of Medicare
Paying More for Less Congress promises to help Medicare beneficiaries by covering prescription drugs BUT Medicare beneficiaries in New York will pay more under proposed reforms! The Impact of Medicare
Medicare Advantage Value-Based Insurance Design Model Test. Responses to Stakeholder Inquiries. Last updated: November 10, 2015
 DEPARTMENT OF HEALTH & HUMAN SERVICES Centers for Medicare & Medicaid Services 7500 Security Boulevard Baltimore, Maryland 21244-1850 CENTER FOR MEDICARE AND MEDICAID INNOVATION Medicare Advantage Value-Based
DEPARTMENT OF HEALTH & HUMAN SERVICES Centers for Medicare & Medicaid Services 7500 Security Boulevard Baltimore, Maryland 21244-1850 CENTER FOR MEDICARE AND MEDICAID INNOVATION Medicare Advantage Value-Based
September 6, Re: CMS-1600-P; CY 2014 Physician Fee Schedule Proposed rule comments
 September 6, 2013 Centers for Medicare & Medicaid Services Department of Health and Human Services Attention CMS-1600-P Mail Stop C4-26-05 7500 Security Boulevard Baltimore, MD 21244-1850 Re: CMS-1600-P;
September 6, 2013 Centers for Medicare & Medicaid Services Department of Health and Human Services Attention CMS-1600-P Mail Stop C4-26-05 7500 Security Boulevard Baltimore, MD 21244-1850 Re: CMS-1600-P;
CURRENT DEVELOPMENTS IN VALUE BASED PAYMENT (VBP): Part 1 Recent Initiatives
: Part 1 Recent Initiatives") CURRENT DEVELOPMENTS IN VALUE BASED PAYMENT (VBP): Part 1 Recent Initiatives Presented by: Peter R. Epp, CPA S e p t e m b e r 2 9, 2 0 1 6 HMA I n t r o d u c t i o n One of the overarching objectives
CURRENT DEVELOPMENTS IN VALUE BASED PAYMENT (VBP): Part 1 Recent Initiatives Presented by: Peter R. Epp, CPA S e p t e m b e r 2 9, 2 0 1 6 HMA I n t r o d u c t i o n One of the overarching objectives
OPEN ENROLLMENT GUIDE
 OPEN ENROLLMENT CONTENTS UNDERSTANDING THE NEW MEDICARE CARD 3 UNDERSTANDING 4 UNDERSTANDING THE DIFFERENCE BETWEEN TRADITIONAL MEDICARE AND MEDICARE ADVANTAGE 9 UNDERSTANDING THE DIFFERENCE BETWEEN MEDICARE
OPEN ENROLLMENT CONTENTS UNDERSTANDING THE NEW MEDICARE CARD 3 UNDERSTANDING 4 UNDERSTANDING THE DIFFERENCE BETWEEN TRADITIONAL MEDICARE AND MEDICARE ADVANTAGE 9 UNDERSTANDING THE DIFFERENCE BETWEEN MEDICARE
2018 Merit-based Incentive Payment System (MIPS) Cost Performance Category Fact Sheet
 Cost Performance Category Fact Sheet") 2018 Merit-based Incentive Payment System (MIPS) Cost Performance Category Fact Sheet What is the Quality Payment Program? The Medicare Access and CHIP Reauthorization Act of 2015 (MACRA) ended the Sustainable
2018 Merit-based Incentive Payment System (MIPS) Cost Performance Category Fact Sheet What is the Quality Payment Program? The Medicare Access and CHIP Reauthorization Act of 2015 (MACRA) ended the Sustainable
Centers for Medicare & Medicaid Services: Innovation Center New Direction Request For Information: Medicare Advantage (MA) Innovation Models
 Innovation Models") Centers for Medicare & Medicaid Services: Innovation Center New Direction Request For Information: Medicare Advantage (MA) Innovation Models 1. Do you have any comments on the guiding principles or focus
Centers for Medicare & Medicaid Services: Innovation Center New Direction Request For Information: Medicare Advantage (MA) Innovation Models 1. Do you have any comments on the guiding principles or focus
Click this button to place your order.
 2018 Medicare 35th Edition What you need to know about Medicare in simple, practical terms. Click this button to place your order. 2018 MEDICARE CONTENTS 1 2 3 4 5 6 Published By PAGE INTRODUCTION Are
2018 Medicare 35th Edition What you need to know about Medicare in simple, practical terms. Click this button to place your order. 2018 MEDICARE CONTENTS 1 2 3 4 5 6 Published By PAGE INTRODUCTION Are
Public Employees Benefits Program Legislative Session Bill Tracking Updated: 3/27/2017
 Public Employees Benefits Program Legislative Session Bill Tracking Updated: 3/27/2017 Bill Number & Description Impact to PEBP & Bill Status AB249 (BDR 38-858) Requires the State Plan for Medicaid and
Public Employees Benefits Program Legislative Session Bill Tracking Updated: 3/27/2017 Bill Number & Description Impact to PEBP & Bill Status AB249 (BDR 38-858) Requires the State Plan for Medicaid and
Medicare: Changes, Challenges, and Opportunities for Grantmakers
 Medicare: Changes, Challenges, and Opportunities for Grantmakers November 6, 2013 Grantmakers in Health Tricia Neuman, Sc.D. Director, Program on Medicare Policy Kaiser Family Foundation Wednesday, November
Medicare: Changes, Challenges, and Opportunities for Grantmakers November 6, 2013 Grantmakers in Health Tricia Neuman, Sc.D. Director, Program on Medicare Policy Kaiser Family Foundation Wednesday, November
The Payment Reform GLOSSARY. Definitions and Explanations of the Terminology Used to Describe Methods of Paying for Healthcare Services.
 The Payment Reform GLOSSARY Definitions and Explanations of the Terminology Used to Describe Methods of Paying for Healthcare Services First Edition INTRODUCTION There is growing national recognition that
The Payment Reform GLOSSARY Definitions and Explanations of the Terminology Used to Describe Methods of Paying for Healthcare Services First Edition INTRODUCTION There is growing national recognition that
Provisions of the Medicare Modernization Act
 Provisions of the Medicare Modernization Act Medicare Prescription Drug Modernization and Improvement Act of 2003 (MMA) Todd Whitney, FSA, MAAA Wakely Consulting Group Highlights of New Act New Rx Benefit
Provisions of the Medicare Modernization Act Medicare Prescription Drug Modernization and Improvement Act of 2003 (MMA) Todd Whitney, FSA, MAAA Wakely Consulting Group Highlights of New Act New Rx Benefit
Evaluating the Fair Market Value of Pay for Performance
 April 2014 healthcare financial management FEATURE STORY Jen Johnson Alexandra Higgins Evaluating the Fair Market Value of Pay for Performance 1 AT A GLANCE When assessing a pay-for-performance arrangement,
April 2014 healthcare financial management FEATURE STORY Jen Johnson Alexandra Higgins Evaluating the Fair Market Value of Pay for Performance 1 AT A GLANCE When assessing a pay-for-performance arrangement,
DHCFP. Provider Payment: Trends and Methods in the Massachusetts Health Care System
 DHCFP Provider Payment: Trends and Methods in the Massachusetts Health Care System Prepared by Allison Barrett and Timothy Lake, Mathematica Policy Research, Inc. February 2010 Deval L. Patrick, Governor
DHCFP Provider Payment: Trends and Methods in the Massachusetts Health Care System Prepared by Allison Barrett and Timothy Lake, Mathematica Policy Research, Inc. February 2010 Deval L. Patrick, Governor
The Under Age 65 Project
 Medicare for Individuals Under Age 65 Webinar Series Choosing Traditional Medicare or Medicare Advantage: Pros and Cons for Individuals Under Age 65 October 20, 2016 Presented by Kathy Holt, M.B.A., J.D.,
Medicare for Individuals Under Age 65 Webinar Series Choosing Traditional Medicare or Medicare Advantage: Pros and Cons for Individuals Under Age 65 October 20, 2016 Presented by Kathy Holt, M.B.A., J.D.,
Presentation to the IOM Committee on Core Metrics Tom Williams, Dr PH, President & CEO, IHA January 7, 2014, Irvine, California
 Presentation to the IOM Committee on Core Metrics Tom Williams, Dr PH, President & CEO, IHA January 7, 2014, Irvine, California Organization: California multi-sector healthcare leadership group Mission:
Presentation to the IOM Committee on Core Metrics Tom Williams, Dr PH, President & CEO, IHA January 7, 2014, Irvine, California Organization: California multi-sector healthcare leadership group Mission:
Status: Time: 12:00 pm. Date: 3/19/10
 Federal Health System Reform 2010: An Update March 19, 2010 1 Status: Time: 12:00 pm. Date: 3/19/10 House votes: Saturday, Rules Committee 9:009 am Sunday, Floor consideration begins at 2:07 pm Process:
Federal Health System Reform 2010: An Update March 19, 2010 1 Status: Time: 12:00 pm. Date: 3/19/10 House votes: Saturday, Rules Committee 9:009 am Sunday, Floor consideration begins at 2:07 pm Process:
National APM Data Collection Frequently Asked Questions for 2018
 National APM Data Collection Frequently Asked Questions for 2018 Last updated on 1/25/18 Please note this document may be updated and improved periodically based on feedback from health plans and other
National APM Data Collection Frequently Asked Questions for 2018 Last updated on 1/25/18 Please note this document may be updated and improved periodically based on feedback from health plans and other
Presentation by Kevin Stone Senior Consultant and Principal Helms & Company Concord NH
 Presentation by Kevin Stone Senior Consultant and Principal Helms & Company Concord NH Medicaid is Largest Payer- covers 1/3 of entire population Vt. funded Medicaid Expansion program pre- ACA (VHAP; Catamount)
Presentation by Kevin Stone Senior Consultant and Principal Helms & Company Concord NH Medicaid is Largest Payer- covers 1/3 of entire population Vt. funded Medicaid Expansion program pre- ACA (VHAP; Catamount)
Medicare Accountable Care Organizations What & Why?
 Medicare Accountable Care Organizations What & Why? Third National Accountable Care Organization Congress David Saÿen, MBA Regional Administrator Centers for Medicare & Medicaid Services San Francisco
Medicare Accountable Care Organizations What & Why? Third National Accountable Care Organization Congress David Saÿen, MBA Regional Administrator Centers for Medicare & Medicaid Services San Francisco
Utah Partnership for Value: Update on Total Cost of Care Reports in Utah
 Utah Partnership for Value: Update on Total Cost of Care Reports in Utah 2014-2015 June 18 th, 2018 HealthInsight Utah and Utah Department of Health Office of Healthcare Statistics Zoom Instructions Audio/mute
Utah Partnership for Value: Update on Total Cost of Care Reports in Utah 2014-2015 June 18 th, 2018 HealthInsight Utah and Utah Department of Health Office of Healthcare Statistics Zoom Instructions Audio/mute
Medicare Program Structure
 Section 4 Medicare Program Structure Benefit Redesign 133 Premium Support 143 132 POLICy OPTIONS TO SUSTAIN MEDICARE FOR THE FUTURE Benefit Redesign OPTIonS reviewed This section discusses two policy options
Section 4 Medicare Program Structure Benefit Redesign 133 Premium Support 143 132 POLICy OPTIONS TO SUSTAIN MEDICARE FOR THE FUTURE Benefit Redesign OPTIonS reviewed This section discusses two policy options
Exhibit ES-1. Total National Health Expenditures (NHE), Current Projection and Alternative Scenarios
, Current Projection and Alternative Scenarios") Exhibit ES-1. Total National Health Expenditures (NHE), 2009 2020 Current Projection and Alternative Scenarios NHE in trillions $6 $5 Current projection (6.7% annual growth) Path proposals (5.5% annual
Exhibit ES-1. Total National Health Expenditures (NHE), 2009 2020 Current Projection and Alternative Scenarios NHE in trillions $6 $5 Current projection (6.7% annual growth) Path proposals (5.5% annual
A Practical Discussion of Value and Quality Based Payments What Do I Do Now?
 Emerging Challenges in Primary Care: 2016 A Practical Discussion of Value and Quality Based Payments What Do I Do Now? Modified from AHLA Physicians and Hospitals Law Institute 2016 Faculty Ellie Bane
Emerging Challenges in Primary Care: 2016 A Practical Discussion of Value and Quality Based Payments What Do I Do Now? Modified from AHLA Physicians and Hospitals Law Institute 2016 Faculty Ellie Bane
Following is a list of common health insurance terms and definitions*.
 Health Terms Glossary Following is a list of common health insurance terms and definitions*. Ambulatory Care Health services delivered on an outpatient basis. A patient's treatment at a doctor's office
Health Terms Glossary Following is a list of common health insurance terms and definitions*. Ambulatory Care Health services delivered on an outpatient basis. A patient's treatment at a doctor's office
TRACKING MEDICARE HEALTH AND PRESCRIPTION DRUG PLANS Monthly Report for January 2008
 TRACKING MEDICARE HEALTH AND PRESCRIPTION DRUG PLANS Monthly Report for January 2008 Prepared by Stephanie Peterson and Marsha Gold, Mathematica Policy Research Inc. as part of work commissioned by the
TRACKING MEDICARE HEALTH AND PRESCRIPTION DRUG PLANS Monthly Report for January 2008 Prepared by Stephanie Peterson and Marsha Gold, Mathematica Policy Research Inc. as part of work commissioned by the
The HPfHR 3-Tier System
 The HPfHR 3-Tier System The basic level (Tier 1) of the new healthcare system would cover the entire population- from cradle to grave and would include, based on evidenced based data, all medical, surgical
The HPfHR 3-Tier System The basic level (Tier 1) of the new healthcare system would cover the entire population- from cradle to grave and would include, based on evidenced based data, all medical, surgical
Risk adjustment is an important opportunity to ensure the sustainability of the exchanges and coverage for patients with chronic conditions.
 RISK ADJUSTMENT Risk adjustment is an important opportunity to ensure the sustainability of the exchanges and coverage for patients with chronic conditions. If risk adjustment is not implemented correctly,
RISK ADJUSTMENT Risk adjustment is an important opportunity to ensure the sustainability of the exchanges and coverage for patients with chronic conditions. If risk adjustment is not implemented correctly,
PREPARING FOR THE NEXT GENERATION OF MANAGED CARE CONTRACTING
 PREPARING FOR THE NEXT GENERATION OF MANAGED CARE CONTRACTING Nanci Robertson, RN BSN President - Robertson Consulting, Inc. Doral Jacobsen, MBA FACMPE CEO - Prosper Beyond, Inc. DORAL JACOBSEN AND NANCI
PREPARING FOR THE NEXT GENERATION OF MANAGED CARE CONTRACTING Nanci Robertson, RN BSN President - Robertson Consulting, Inc. Doral Jacobsen, MBA FACMPE CEO - Prosper Beyond, Inc. DORAL JACOBSEN AND NANCI
Medicaid Alternative Benefit Plans and Essential Health Benefits 9/10/13
 Medicaid Alternative Benefit Plans and Essential Health Benefits 9/10/13 Melissa Harris, Division Director Division of Benefits and Coverage Disabled and Elderly Health Programs Group Background Intended
Medicaid Alternative Benefit Plans and Essential Health Benefits 9/10/13 Melissa Harris, Division Director Division of Benefits and Coverage Disabled and Elderly Health Programs Group Background Intended
AFFORDABILITY REVIEW. Mysteries of the Medical Loss Ratio
 AFFORDABILITY REVIEW Mysteries of the Medical Loss Ratio NANCY DJORDJEVIC DIRECTOR, HEALTHCARE ANALYTICS APRIL 2016 WHO IS GORMAN HEALTH GROUP? Gorman Health Group is the leading solutions and consulting
AFFORDABILITY REVIEW Mysteries of the Medical Loss Ratio NANCY DJORDJEVIC DIRECTOR, HEALTHCARE ANALYTICS APRIL 2016 WHO IS GORMAN HEALTH GROUP? Gorman Health Group is the leading solutions and consulting
AAOS MACRA Proposed Rule Summary (Short)
") AAOS MACRA Proposed Rule Summary (Short) Merit-Based Incentive Payment System (MIPS), Advanced Alternative Payment Model (APM) Incentive, and Criteria for Physician-Focused Payment Models Ref: CMS-5517-P
AAOS MACRA Proposed Rule Summary (Short) Merit-Based Incentive Payment System (MIPS), Advanced Alternative Payment Model (APM) Incentive, and Criteria for Physician-Focused Payment Models Ref: CMS-5517-P
Session 75 OF, Advantages & Challenges for Provider Led Health Plans. Moderator: LuCretia Leola Hydell, ASA, MAAA
 Session 75 OF, Advantages & Challenges for Provider Led Health Plans Moderator: LuCretia Leola Hydell, ASA, MAAA Presenters: Jerry Clark, MD, FACP Josh Martin Mark Rishell SOA Antitrust Disclaimer SOA
Session 75 OF, Advantages & Challenges for Provider Led Health Plans Moderator: LuCretia Leola Hydell, ASA, MAAA Presenters: Jerry Clark, MD, FACP Josh Martin Mark Rishell SOA Antitrust Disclaimer SOA
Medicaid Benefits for Children and Adults: Issues Raised by the National Governors Association s Preliminary Recommendations
 Medicaid Benefits for Children and Adults: Issues Raised by the National Governors Association s Preliminary Recommendations July 12, 2005 Cindy Mann Overview The Medicaid benefit package determines which
Medicaid Benefits for Children and Adults: Issues Raised by the National Governors Association s Preliminary Recommendations July 12, 2005 Cindy Mann Overview The Medicaid benefit package determines which
The Case For Value ACA to MACRA to MIPS
 The Case For Value ACA to MACRA to MIPS 2016-2019 Robert E Nesse M.D. Professor of Family Medicine Mayo Medical School Senior Director of Health Care Policy and Payment Reform nesse.robert@mayo.edu What
The Case For Value ACA to MACRA to MIPS 2016-2019 Robert E Nesse M.D. Professor of Family Medicine Mayo Medical School Senior Director of Health Care Policy and Payment Reform nesse.robert@mayo.edu What
The high cost and uneven quality of healthcare have
 RESEARCH BRIEF NO. 20 NOVEMBER 2017 Health System Oversight by States: An Environmental Scan The high cost and uneven quality of healthcare have profound negative impacts on the health and financial security
RESEARCH BRIEF NO. 20 NOVEMBER 2017 Health System Oversight by States: An Environmental Scan The high cost and uneven quality of healthcare have profound negative impacts on the health and financial security
EXECUTIVE SUMMARY ENROLLMENT GROWS YET MARGINS DROP FOR OHIO S HEALTH INSURING CORPORATIONS. 970,000 Ohioans remained uninsured in 2014.
 OHA exists to collaborate with member hospitals and health systems to ensure a healthy Ohio. February 2016 EXECUTIVE SUMMARY ENROLLMENT GROWS YET MARGINS DROP FOR OHIO S HEALTH INSURING CORPORATIONS In
OHA exists to collaborate with member hospitals and health systems to ensure a healthy Ohio. February 2016 EXECUTIVE SUMMARY ENROLLMENT GROWS YET MARGINS DROP FOR OHIO S HEALTH INSURING CORPORATIONS In
The New York State Value-Based Payment (VBP) Roadmap. Behavioral Health Providers January 30, 2018
 Roadmap. Behavioral Health Providers January 30, 2018") The New York State Value-Based Payment (VBP) Roadmap Behavioral Health Providers January 30, 2018 1 Housekeeping All lines have been muted To ask a question at any time, use the Chat feature in WebEx We
The New York State Value-Based Payment (VBP) Roadmap Behavioral Health Providers January 30, 2018 1 Housekeeping All lines have been muted To ask a question at any time, use the Chat feature in WebEx We
Value Based Contracting
 Value Based Contracting CONCEPTS FOR THE MEDICAL PRACTICE dhgllp.com/healthcare 225 Peachtree Street NE, Suite 600 Atlanta, GA 30303 Bill Hannah PRINCIPAL Bill.Hannah@dhgllp.com 404.575.8921 Doral Davis-Jacobsen
Value Based Contracting CONCEPTS FOR THE MEDICAL PRACTICE dhgllp.com/healthcare 225 Peachtree Street NE, Suite 600 Atlanta, GA 30303 Bill Hannah PRINCIPAL Bill.Hannah@dhgllp.com 404.575.8921 Doral Davis-Jacobsen