Health Insurance 101 For 2015 Open Enrollment
|
|
|
- Edwin Fox
- 5 years ago
- Views:
Transcription

1 Health Insurance 101 For 2015 Open Enrollment

2 Objectives: Understand and Explain Basic Insurance Terms. How To Read An SBC Or Other SSP Tools To Answer Insurance Questions. Understand Your Part In The QHP Renewal Process. Know The Differences In Dental Policies For 2015.
3 Basic Insurance Terms
4 Premium vs. individual contribution Premium = The total amount that must be paid for an individual or family s health insurance plan. You and/or your employer usually pay it monthly, quarterly or yearly. Premium Individual or family contribution: The individual or family s portion of the premium that must be paid for an individual or family s health insurance plan. You usually pay it monthly, quarterly or yearly. Premium APTC or Employer Contribution = Individual/Family Contribution.

5 APTC Payment assistance: A tax credit that can help you afford coverage bought through the Marketplace. Unlike tax credits you can only claim when you file your taxes, these tax credits can be used right away to lower your monthly premium costs. Payment assistance is also called Advance Premium Tax Credits (APTC). Special Discounts lower the amount you have to pay for out-of-pocket costs like deductibles, coinsurance, and copayments. Special Discounts are also called Cost-Sharing Reductions (CSR). Payment Assistance and Special Discounts are only available on kynect!
6 Providers and Networks Provider: A health care professional or health care facility that is licensed, certified or accredited, as required by state law. Network: The facilities, providers and suppliers your health insurer or plan has contracted with to provide health care services. In-Network Provider : A provider who has a contract with your health insurer or plan to provide services to you at a discount. (Sometimes called participating or preferred provider). Out of Network Provider : A provider who doesn t have a contract with your health insurer or plan to provide services to you. You ll pay more to see an out of network provider. (Sometimes called a non-preferred or non-participating provider). Primary Care Provider (PCP): Medical Doctor or D.O. (Doctor of Osteopathic Medicine), advanced practice registered nurse or physician assistant who provides, coordinates or helps individuals access most healthcare services.
7 Type of Plans: Health Maintenance Organization (HMO) A type of health insurance plan that usually limits coverage to care from doctors who work for or contract with the HMO. It generally won't cover out-of-network care except in an emergency. An HMO may require you to live or work in its service area to be eligible for coverage. HMOs often provide integrated care and focus on prevention and wellness. Preferred Provider Organization (PPO) A type of health plan that contracts with medical providers, such as hospitals and doctors, to create a network of participating providers. You pay less if you use providers that belong to the plan s network. You can use doctors, hospitals, and providers outside of the network for an additional cost. Point of Service (POS) Plans A type of plan in which you pay less if you use doctors, hospitals, and other health care providers that belong to the plan s network. POS plans also require you to get a referral from your primary care doctor in order to see a specialist.
8 In-Network vs. Out-of-Network Deductible: The amount you owe for health care services your health insurance or plan covers before your health insurance or plan begins to pay. The deductible may not apply to all services. (Innetwork; Medical; Pharmacy; Integrated) Maximum Out-of-pocket (MOOP) Limit: The most you pay during a policy period (usually a year) before your health insurance or plan begins to pay 100% of the allowed amount. This amounts never include your premium, balancebilled charges or health care your health insurance or plan doesn t cover. Some health insurance or plans don t count all of your co-payments, deductibles, co-insurance payments, out-ofnetwork payments or other expenses toward the maximum out of pock limit.
9 In-Network vs. Out-of-Network COINSURANCE: An amount you may be required to pay as your share of the cost for services after* you pay any deductibles. Coinsurance is usually a percentage of the cost of the service (for example, 20%). COPAYMENT: An amount you may be required to pay as your share of the cost for a medical service or supply, like a doctor s visit, hospital outpatient visit or prescription drug. A co-payment is usually a set amount, rather than a percentage of the total cost.
10 Essential Health Benefits A set of health care service categories that must be covered by certain plans, starting in Health plans offered in the individual and small group markets offer a comprehensive package of items and services, known as essential health benefits. Essential health benefits must include items and services within at least the following 10 categories: ambulatory patient services; emergency services; hospitalization; maternity and newborn care; mental health and substance use disorder services, including behavioral health treatment; prescription drugs; rehabilitative and habilitative services and devices; laboratory services; preventive and wellness services and chronic disease management; and pediatric services, including oral and vision care.
11 Other Insurance Terms Appeal: A formal request to your health plan to reconsider a decision to deny coverage for healthcare. Excluded Services: Healthcare services that your health insurance plan doesn t pay for or cover(for example, cosmetic surgery) External Review: A formal independent review of a disagreement between you and your health plan about coverage for healthcare that was denied because your plan considered it to be either experimental or not medically necessary. Pre-Authorization: A decision by your health insurer or plan that the service requested for you is medically necessary. This is also called prior approval or precertification.
 may establish an HSA.")
12 HSA/HRA/FSA Health Savings Accounts (HSAs) An account established so that individuals covered by high-deductible health plans could receive taxpreferred treatment of money saved for medical expenses. Generally, an adult who is covered by a high-deductible health plan (and has no other first-dollar coverage) may establish an HSA. Health Reimbursement Arrangement (HRA) is an employerfunded, tax advantaged plan that reimburses employees for out of pocket medical expenses and individual health insurance premiums. Flexible Spending Account(FSA) (also known as a flexible spending arrangement) is a special account you put money into that you use to pay for certain out-of-pocket health care costs (Copayments and deductibles for certain medical and dental expenses.)
 but that don't cover any benefits other than 3 primary care visits per year before the plan's deductible is met.")

13 More Insurance Terms Catastrophic Health Plan Health plans that meet all of the requirements applicable to other Qualified Health Plans (QHPs) but that don't cover any benefits other than 3 primary care visits per year before the plan's deductible is met. To qualify for a catastrophic plan, you must be under 30 years old OR get a "hardship exemption. Formulary A list of prescription drugs covered by a prescription drug plan or another insurance plan offering prescription drug benefits. Also called a Prescription Drug List.

14 How to kynect Brochure
15 Other Resources (uniform glossary) (Coverage to care)
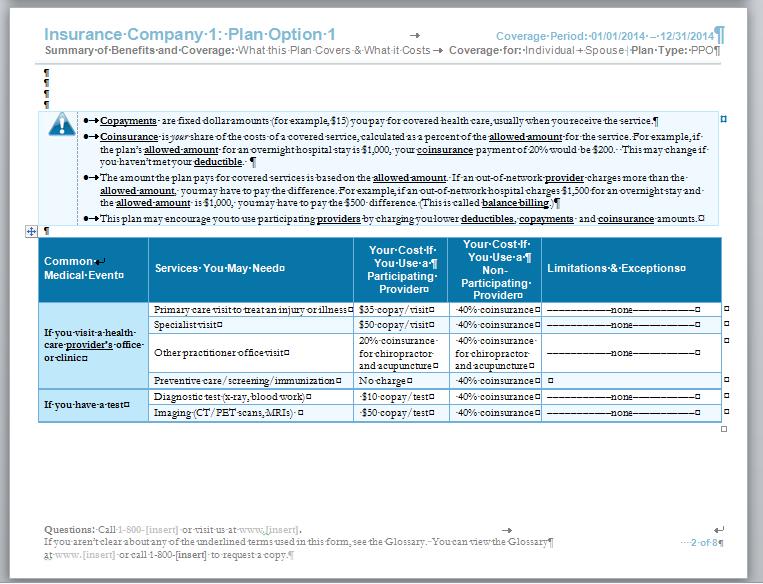
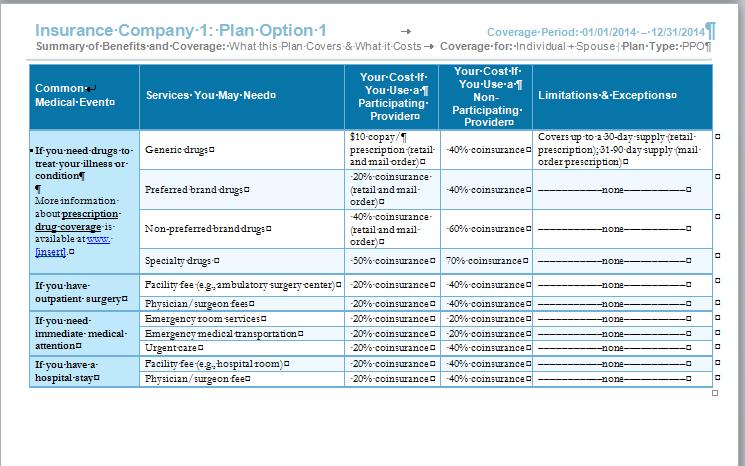
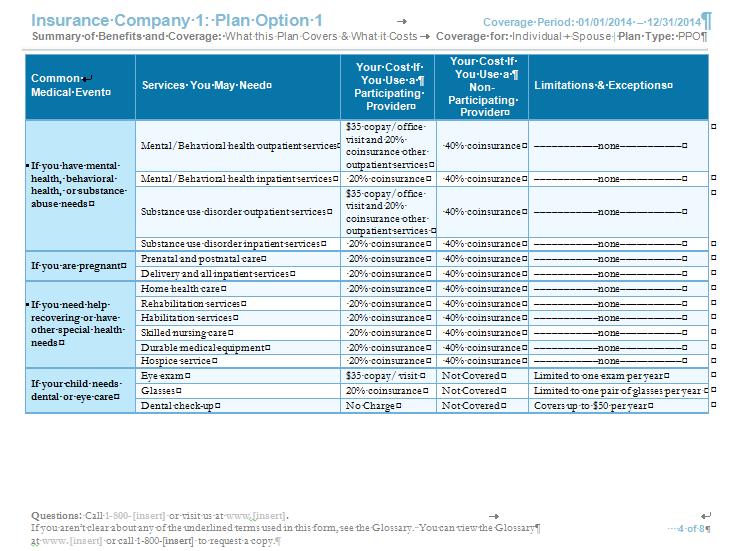
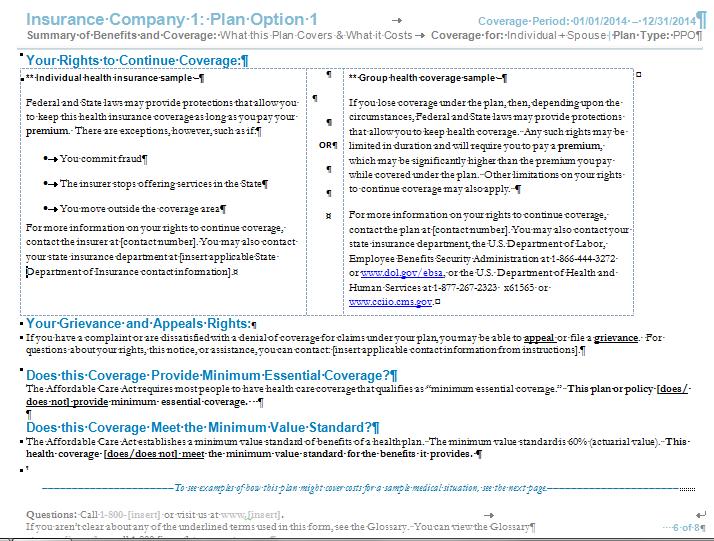
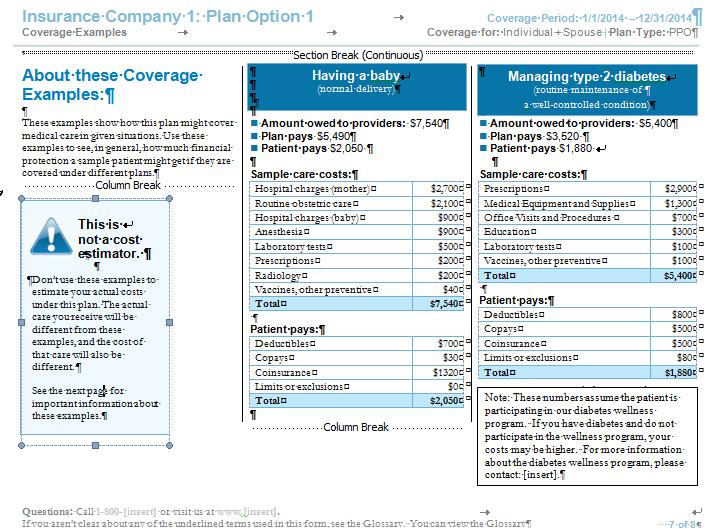
16 How To Read An SBC Or Other SSP Tools To Answer Insurance Questions.
17 SBC means: Statement of Benefits and Cost- Sharing? Summary of Benefit and Coverage? San Bernardino County? Somebody Better Call the Contact Center?
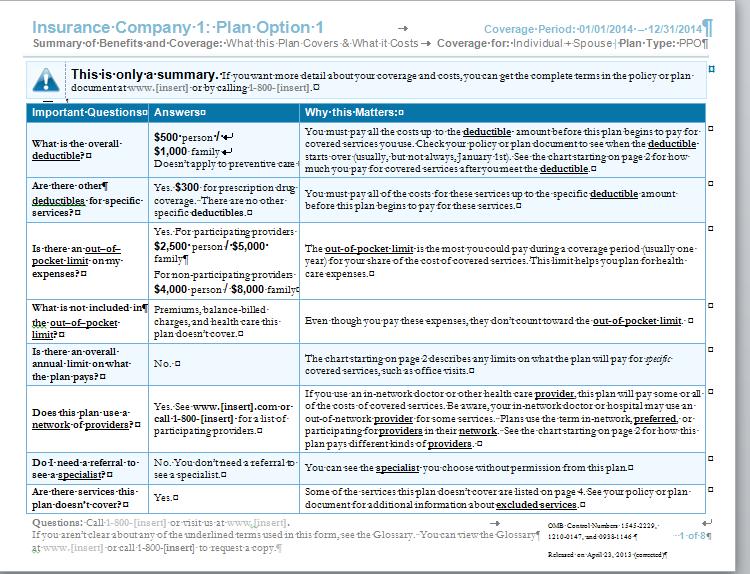
18 SBC
19 10/22/
20 10/22/
21 10/22/
22 10/22/
23 10/22/
24 10/22/
25 10/22/

26 An example how to use the SBC How does her plan work: Meg had a horrible pain in her stomach and it did not go away. She finally went to ER at 3 am. They ordered bloodwork and an x-ray. It turned out to be appendicitis so she was admitted to the hospital and had her surgery the following morning. She was released from the hospital the following day. Thankfully, the hospital and all the providers who saw Meg were innetwork participating providers and prior to this episode, she had $450 applied to her deductible. Before Meg s insurance information was added her bill would look like this: Service Billed Charge After Insurance Discount Co-pay or co-insurance ER 2500 ER physician 1200 Blood work 300 X-Ray 550 Hospital charges 4500 Anesthesia 800 Surgery 1000 TOTALS $10,850
27 An example how to use the SBC Now Let s look at Meg s Bill After insurance Discount: Service Billed Charge After Insurance Discount Co-pay or coinsurance ER ER physician Blood work X-Ray Hospital charges Anesthesia Surgery TOTALS $10,850 $5,650

28 10.0 Privacy & Security What does Meg Actually Pay? Service Billed Charge After Insurance Discount Co-pay or co-insurance ER ER physician Blood work $10 X-Ray $50 Hospital charges Anesthesia Surgery TOTALS $10,850 $5,650 $1,170 10/22/

29 Plan Comparison Tools

30 Plan Comparison Tools

31 Plan Comparison Tools

32 Plan Comparison Tools
33 Plan Comparison Tools

34 Plan Comparison Tools

35 Plan Comparison Tools


36 10/22/
37 Open Enrollment Timeline 11/01/14* Open Enrollment Notices sent 11/15/14 Open Enrollment begins 12/15/14 Last day to enroll with an effective date of 1/1/15 01/01/15 Effective Date of Coverage if enrolled by 12/15/14 02/01/15 Effective Date of Coverage if enrolled by 1/15/15 02/15/15 Open Enrollment ends 03/01/15 Effective Date of Coverage if enrolled by 02/15/15

38 Open Enrollment Notices 1. Notice of Open Enrollment for those who will be automatically (passively) reenrolled in their current plan for the 2015 Plan Year. This notice will provide general information about open enrollment such as dates and allowed changes. 2. Notice of Open Enrollment for those who cannot be automatically (passively) reenrolled due various reasons. 3. Notice of Open Enrollment for those who have not authorized data checks with the federal hub for the upcoming year
 The QHP is no longer available in 2015.")
39 Renewal Process A qualified individual enrolled in a QHP that remains eligible for coverage will remain in the QHP selected in the previous year unless: The individual terminates coverage from QHP The individual enrolls in another QHP (if available) The QHP is no longer available in 2015.
40 Know The Differences In Dental Policies For 2015.


41 What s new for 2015

42 Dental insurance Includes 2015 Open Enrollment

43 Dental Shopping
44 Dental shopping

45 Dental plan comparison

46 Dental Plan Comparison
47 Dental Plan
48 Other Brief reminders

49 Enrollment Periods Open Enrollment 2015 November 15 to February 15 Continuous Open Enrollment For Medicaid or SHOP Special Enrollment For Qualifying Life Events
50 6.3 SHOP Enhancements SHOP Amnesty Period kynect will produce a report on the number of Employers who utilize the Amnesty Period in order to participate in SHOP. Employer creates enrollment (Contribution is turned back on 11/15) (Open Enrollment closes 12/15) (Contribution/Participation is turned off) Employees are notified and may enroll Coverage is effective 1/1/15 10/15 11/14 11/15 12/15 10/15/14 11/15/14 12/15/14 01/01/15

51
MCHO Informational Series
 MCHO Informational Series Glossary of Health Insurance & Medical Terminology How to use this glossary This glossary has many commonly used terms, but isn t a full list. These glossary terms and definitions
MCHO Informational Series Glossary of Health Insurance & Medical Terminology How to use this glossary This glossary has many commonly used terms, but isn t a full list. These glossary terms and definitions
Total Health Care USA, Inc.: Total Saver Complete Summary of Benefits and Coverage: What this Plan Covers & What it Costs
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.thcmi.com or by calling 1-800-826-2862 Important Questions
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.thcmi.com or by calling 1-800-826-2862 Important Questions
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.networkhealth.com/benefits/sbc/individualpolicy.pdf or
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.networkhealth.com/benefits/sbc/individualpolicy.pdf or
Some of the services this plan doesn t cover are listed on page 5. See your policy Yes plan doesn t cover?
 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual Plan Type: Network This is only a summary. If you want more detail about your coverage and costs, you can
Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual Plan Type: Network This is only a summary. If you want more detail about your coverage and costs, you can
Total Health Care USA, Inc.: Total Gold Premier Summary of Benefits and Coverage: What this Plan Covers & What it Costs
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.thcmi.com or by calling 1-800-826-2862 Important Questions
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.thcmi.com or by calling 1-800-826-2862 Important Questions
Important Questions Answers Why this Matters: What is the overall deductible? Are there other deductibles for specific services?
 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual Plan Type: Prev. Plus Plan This is only a summary. If you want more detail about your coverage and costs,
Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual Plan Type: Prev. Plus Plan This is only a summary. If you want more detail about your coverage and costs,
Enhanced. Oakland University. Important Questions Answers Why this Matters:
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.hap.org or by calling 1-800-422-4641. Important Questions
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.hap.org or by calling 1-800-422-4641. Important Questions
University of Virginia Physicians Group: Anthem HealthKeepers- $750/$1,500 Deductible Coverage Period: 07/01/ /30/2017
 University of Virginia Physicians Group: Anthem HealthKeepers- $750/$1,500 Deductible Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage Period: 07/01/2016-06/30/2017 Coverage
University of Virginia Physicians Group: Anthem HealthKeepers- $750/$1,500 Deductible Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage Period: 07/01/2016-06/30/2017 Coverage
Important Questions Answers Why this Matters:
 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual Plan Type: Premium Plan This is only a summary. If you want more detail about your coverage and costs, you
Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual Plan Type: Premium Plan This is only a summary. If you want more detail about your coverage and costs, you
Important Questions Answers Why this Matters: In-Network- $1,150
 BB&T: Select PPO Coverage Period: 01/01/2017-12/31/2017 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual/Family Plan Type: PPO Important Questions Answers
BB&T: Select PPO Coverage Period: 01/01/2017-12/31/2017 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual/Family Plan Type: PPO Important Questions Answers
Anthem Blue Cross University of the Pacific Student Health Plan PPO with Student Health Center (100/80/60) Coverage Period: 08/01/ /31/2016
 Coverage Period: 08/01/ /31/2016") Anthem Blue Cross University of the Pacific Student Health Plan PPO with Student Health Center (100/80/60) Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage Period: 08/01/2015-07/31/2016
Anthem Blue Cross University of the Pacific Student Health Plan PPO with Student Health Center (100/80/60) Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage Period: 08/01/2015-07/31/2016
You don t have to meet deductibles for specific services, but see the chart starting on page 3 for other costs for services this plan covers.
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.nipponlifebenefits.com or by calling 1-800-374-1835.
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.nipponlifebenefits.com or by calling 1-800-374-1835.
CalPERS: Sharp Performance Plus HMO Summary of Benefits and Coverage: What this Plan Covers & What it Costs
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.sharphealthplan.com/calpers or by calling 1-855-995-5004.
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.sharphealthplan.com/calpers or by calling 1-855-995-5004.
You can see the specialist you choose without permission from this plan.
 IU Health Plans: IU Health Plans Bronze Simple HSA Coverage Period: 1/1/2016-12/31/2016 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual/Family Plan Type:
IU Health Plans: IU Health Plans Bronze Simple HSA Coverage Period: 1/1/2016-12/31/2016 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual/Family Plan Type:
Montgomery County Public Schools- PPO Coverage Period: 10/01/ /30/2017
 Montgomery County Public Schools- PPO Coverage Period: 10/01/2016 09/30/2017 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual/Family Plan Type: PPO This
Montgomery County Public Schools- PPO Coverage Period: 10/01/2016 09/30/2017 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual/Family Plan Type: PPO This
$200 individual/$400 family combined network and out-of-network.
 Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/2019-12/31/2019 New Castle County Government : Blue Choice PPO Coverage for: Individual/Family
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/2019-12/31/2019 New Castle County Government : Blue Choice PPO Coverage for: Individual/Family
Employee Benefit Plan: Missoula County Public Schools Coverage Period: 01/01/ /31/2014 Summary of Benefits and Coverage:
 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual Plan Type: HDHP This is only a summary. If you want more detail about your coverage and costs, you can get
Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual Plan Type: HDHP This is only a summary. If you want more detail about your coverage and costs, you can get
Highmark Blue Cross Blue Shield: PPO Coverage Period: 01/01/ /31/2017
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.highmarkbcbs.com or by calling 1-800-241-5704. Important
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.highmarkbcbs.com or by calling 1-800-241-5704. Important
Important Questions Answers Why this Matters:
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.anthem.com or by calling 1-800-421-1880. Important Questions
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.anthem.com or by calling 1-800-421-1880. Important Questions
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/ /31/2019
 Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/2019 12/31/2019 Highmark West Virginia: my Blue Access WV EPO Silver 3500-2 Free PCP Visits
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/2019 12/31/2019 Highmark West Virginia: my Blue Access WV EPO Silver 3500-2 Free PCP Visits
Important Questions Answers Why this Matters: In-network: $0/Individual; $0/Family Out-of-network: $750/Individual; $1,500/Family
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.anthem.com or by calling 1-800-421-1880. Important Questions
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.anthem.com or by calling 1-800-421-1880. Important Questions
Important Questions Answers Why this Matters:
 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual + Family Plan Type: PPO This is only a summary. If you want more detail about your coverage and costs, you
Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual + Family Plan Type: PPO This is only a summary. If you want more detail about your coverage and costs, you
covered services you use. Check your policy plan or plan document to see when the deductible $6,000 individual / $12,000 deductible?
 Ambetter of Arkansas: Ambetter Balanced Care 7 (2016) Coverage Period: 01/01/2016-12/31/2016 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual/Family Plan
Ambetter of Arkansas: Ambetter Balanced Care 7 (2016) Coverage Period: 01/01/2016-12/31/2016 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual/Family Plan
$0 See the chart starting on page 2 for your costs for services this plan covers.
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.hap.org or by calling 1-800-422-4641. Important Questions
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.hap.org or by calling 1-800-422-4641. Important Questions
Preferred Blue PPO $500 Deductible Coverage Period: on or after 01/01/2016 Summary of Benefits and Coverage: What this Plan Covers & What it Costs
 Preferred Blue PPO $500 Deductible Coverage Period: on or after 01/01/2016 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual and Family Plan Type: PPO This
Preferred Blue PPO $500 Deductible Coverage Period: on or after 01/01/2016 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual and Family Plan Type: PPO This
Important Questions Answers Why this Matters: What is the overall deductible? $0 Are there other deductibles for specific services?
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.bcbsga.com/usg or by calling 1-800-424-8950. Important
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.bcbsga.com/usg or by calling 1-800-424-8950. Important
Companion Life Insurance Company: New England Culinary Institute Coverage Period: 7/1/14-7/1/15
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.chpstudent.com or by calling 1-800-633-7867. Important
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.chpstudent.com or by calling 1-800-633-7867. Important
TAKECARE STANDARD OPTION: $5/100%/$0 $150 HCP
 TAKECARE STANDARD OPTION: $5/100%/$0 $150 HCP Coverage Period: 1/1/17-12/31/17 Summary of Benefits and Coverage Coverage for: Self Only, Self Plus One or Self and Family Plan Type: POS This is only a summary.
TAKECARE STANDARD OPTION: $5/100%/$0 $150 HCP Coverage Period: 1/1/17-12/31/17 Summary of Benefits and Coverage Coverage for: Self Only, Self Plus One or Self and Family Plan Type: POS This is only a summary.
Coverage Period: 1/1/ /31/2016. Western Health Advantage: WHA Silver 70 HSA HMO 2000/20% w/child Dental. Coverage For: Self Only Plan Type: HMO
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.westernhealth.com or by calling 1-888-563-2250. Important
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.westernhealth.com or by calling 1-888-563-2250. Important
You can see the specialist you choose without permission from this plan.
 Prominence HealthFirst of Texas: Silver 10 Coverage Period: 1/1/2016-12/31/2016 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual/Family Plan Type: HMO This
Prominence HealthFirst of Texas: Silver 10 Coverage Period: 1/1/2016-12/31/2016 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual/Family Plan Type: HMO This
You don t have to meet deductibles for specific services.
 Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/2019-12/31/2019 Highmark Blue Cross Blue Shield: BlueCare Custom PPO Coverage for: Individual/Family
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/2019-12/31/2019 Highmark Blue Cross Blue Shield: BlueCare Custom PPO Coverage for: Individual/Family
You don t have to meet deductibles for specific services.
 Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/2019-12/31/2019 Highmark Blue Shield: PPO Blue Coverage for: Individual/Family Plan Type:
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/2019-12/31/2019 Highmark Blue Shield: PPO Blue Coverage for: Individual/Family Plan Type:
BridgeSpan Health Company: BridgeSpan Silver HDHP 2000 MyChoice Northwest
 BridgeSpan Health Company: BridgeSpan Silver HDHP 2000 MyChoice Northwest Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage Period: 01/01/2016 12/31/2016 Coverage for: Individual
BridgeSpan Health Company: BridgeSpan Silver HDHP 2000 MyChoice Northwest Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage Period: 01/01/2016 12/31/2016 Coverage for: Individual
: Federal Employees Standard Option Coverage Period: 01/01/ /31/2017 Summary of Benefits and Coverage
 This is only a summary. Please read the FEHB Plan brochure (RI 73-815) that contains the complete terms of this plan. All benefits are subject to the definitions, limitations, and exclusions set forth
This is only a summary. Please read the FEHB Plan brochure (RI 73-815) that contains the complete terms of this plan. All benefits are subject to the definitions, limitations, and exclusions set forth
Western Health Advantage: WHA Platinum 90 HMO 0/20 w/child Dental. Coverage Period: 1/1/ /31/2016
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.westernhealth.com or by calling 1-888-563-2250. Important
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.westernhealth.com or by calling 1-888-563-2250. Important
$ 400 person/ $1,200 family; Waived for inpatient and outpatient hospital charges at Centers of Excellence and Hospitals of Distinction.
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.mbpet.net or by calling 1-888-742-3380. Important Questions
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.mbpet.net or by calling 1-888-742-3380. Important Questions
You must pay all of the costs for these services up to the specific deductible amount before the plan begins to pay for these services.
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.anthem.com or by calling 1-800-552-9159. Important Questions
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.anthem.com or by calling 1-800-552-9159. Important Questions
$1,500 individual/$3,000 family network. $3,000 individual/$6,000 family out-ofnetwork.
 Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/2018-12/31/2018 Journey Health Systems: PPO Coverage for: Individual/Family Plan Type:
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/2018-12/31/2018 Journey Health Systems: PPO Coverage for: Individual/Family Plan Type:
Anthem Blue Cross Life and Health Insurance Company San Bernardino Community College District Premier PPO 250/15/10
 Anthem Blue Cross Life and Health Insurance Company San Bernardino Community College District Premier PPO 250/15/10 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage Period:
Anthem Blue Cross Life and Health Insurance Company San Bernardino Community College District Premier PPO 250/15/10 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage Period:
Important Questions Answers Why this Matters:
 This is only a summary. Medical benefits are covered through Anthem Blue Cross and Blue Shield. If you want more detail about your coverage and costs for health benefits, you can get the complete terms
This is only a summary. Medical benefits are covered through Anthem Blue Cross and Blue Shield. If you want more detail about your coverage and costs for health benefits, you can get the complete terms
Western Health Advantage: WHA Bronze 60 HMO 6000/70 w/child Dental. Coverage Period: 1/1/ /31/2016
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.westernhealth.com or by calling 1-888-563-2250. Important
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.westernhealth.com or by calling 1-888-563-2250. Important
You don t have to meet deductibles for specific services.
 Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/2019-12/31/2019 Highmark Blue Cross Blue Shield: BlueCare HMO Coverage for: Individual/Family
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/2019-12/31/2019 Highmark Blue Cross Blue Shield: BlueCare HMO Coverage for: Individual/Family
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/ /31/2019
 Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/2019 12/31/2019 Highmark West Virginia: my Blue Access WV EPO Silver 4450 HSA Coverage
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/2019 12/31/2019 Highmark West Virginia: my Blue Access WV EPO Silver 4450 HSA Coverage
BridgeSpan Health Company: BridgeSpan Oregon Standard Silver Plan Value PPO
 BridgeSpan Health Company: BridgeSpan Oregon Standard Silver Plan Value PPO Summary of Benefits and Coverage: What this Plan Covers & What it Costs Questions: Call 1 (855) 857-9943 or visit us at www.bridgespanhealth.com.
BridgeSpan Health Company: BridgeSpan Oregon Standard Silver Plan Value PPO Summary of Benefits and Coverage: What this Plan Covers & What it Costs Questions: Call 1 (855) 857-9943 or visit us at www.bridgespanhealth.com.
National Elevator Industry: Health Benefit Plan Summary of Benefits and Coverage: What this Plan Covers & What it Costs
 National Elevator Industry: Health Benefit Plan Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage Period: 01/01/2016-12/31/2016 Coverage for: Individual + Family Plan Type:
National Elevator Industry: Health Benefit Plan Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage Period: 01/01/2016-12/31/2016 Coverage for: Individual + Family Plan Type:
Important Questions Answers Why this Matters:
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.crystalrunhp.com or by calling 1-844-638-6506. Important
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.crystalrunhp.com or by calling 1-844-638-6506. Important
$300 Individual; $ 800 Family. Applies to out-of-network services only. What is the overall deductible?
 What is the overall deductible? This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.indecscorp.com or by
What is the overall deductible? This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.indecscorp.com or by
GLOSSARY OF KEY AFFORDABLE CARE ACT AND COMMON HEALTH PLAN TERMS
 GLOSSARY OF KEY AFFORDABLE CARE ACT AND COMMON HEALTH PLAN TERMS Note: in the event of any conflict between this glossary and your plan document/summary plan description (SPD) or policy/certificate, the
GLOSSARY OF KEY AFFORDABLE CARE ACT AND COMMON HEALTH PLAN TERMS Note: in the event of any conflict between this glossary and your plan document/summary plan description (SPD) or policy/certificate, the
What is the overall deductible? Are there other deductibles for specific services? Is there an out-ofpocket
 Regence BlueShield: Regence Direct Silver with Dental, Vision, Individual Assistance Program Coverage Period: Beginning on or after 01/01/2014 Summary of Benefits and Coverage: What this Plan Covers &
Regence BlueShield: Regence Direct Silver with Dental, Vision, Individual Assistance Program Coverage Period: Beginning on or after 01/01/2014 Summary of Benefits and Coverage: What this Plan Covers &
$0 individual/$0 family network. $250 individual/$500 family out-ofnetwork.
 Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/2018-12/31/2018 Highmark Blue Shield: PPO Coverage for: Individual/Family Plan Type: PPO
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/2018-12/31/2018 Highmark Blue Shield: PPO Coverage for: Individual/Family Plan Type: PPO
$350 individual/$700 family network. $700 individual/$1,400 family out-ofnetwork.
 Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 04/01/2018-03/31/2019 Gannon University: PPO Coverage for: Individual/Family Plan Type: PPO
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 04/01/2018-03/31/2019 Gannon University: PPO Coverage for: Individual/Family Plan Type: PPO
LVAIC-Muhlenberg College: Lehigh Valley Flex Blue PPO Coverage Period: 01/01/ /31/2017
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.highmarkblueshield.com or by calling 1-800-345-3806.
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.highmarkblueshield.com or by calling 1-800-345-3806.
Important Questions Answers Why this Matters:
 Anthem BlueCross Classic PPO 250/20/20 / $10/$30/$50/30% Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage Period: 01/01/2015-12/31/2015 Coverage For: Individual/Family Plan
Anthem BlueCross Classic PPO 250/20/20 / $10/$30/$50/30% Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage Period: 01/01/2015-12/31/2015 Coverage For: Individual/Family Plan
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/ /31/2018
 Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/2018-12/31/2018 Pennsylvania Turnpike Commission: Highmark PPO Blue Coverage for: Individual/Family
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/2018-12/31/2018 Pennsylvania Turnpike Commission: Highmark PPO Blue Coverage for: Individual/Family
Important Questions Answers Why this Matters:
 Anthem BlueCross Solution PPO 1500/15/20 / $15/$30/$50/30% Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage Period: 11/01/2014-10/31/2015 Coverage For: Individual/Family
Anthem BlueCross Solution PPO 1500/15/20 / $15/$30/$50/30% Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage Period: 11/01/2014-10/31/2015 Coverage For: Individual/Family
Important Questions Answers Why this Matters: What is the overall deductible? $0 Are there other deductibles for specific services?
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.bcbsga.com/bor or by calling 1-800-424-8950. Important
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.bcbsga.com/bor or by calling 1-800-424-8950. Important
Even though you pay these expenses, they don t count toward the out-ofpocket limit.
 Anthem Blue Cross CSEBA Classic HMO-6-C Coverage Period: 07/01/2016-06/30/2017 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual/Family Plan Type: HMO This
Anthem Blue Cross CSEBA Classic HMO-6-C Coverage Period: 07/01/2016-06/30/2017 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual/Family Plan Type: HMO This
Vista360health: Traditional HMO Silver Coverage Period: 01/01/ /31/2016 Summary of Benefits and Coverage:
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document by emailing info@vista360health.com or by calling 1-866-607-0117.
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document by emailing info@vista360health.com or by calling 1-866-607-0117.
Total Health Care USA, Inc.: Totally You Summary of Benefits and Coverage: What this Plan Covers & What it Costs
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.thcmi.com or by calling 1-800-826-2862 Important Questions
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.thcmi.com or by calling 1-800-826-2862 Important Questions
Important Questions Answers Why this Matters:
 Anthem BlueCross Value HMO 20/30/20% Select Plus HMO / $10/$30/$45/20% Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage Period: 01/01/2014-12/31/2014 Coverage For: Individual/Family
Anthem BlueCross Value HMO 20/30/20% Select Plus HMO / $10/$30/$45/20% Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage Period: 01/01/2014-12/31/2014 Coverage For: Individual/Family
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan
 : Samford University Coverage Period: Beginning on or after 01/01/2015 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage For: Individual + Family Plan Type: PPO This is only
: Samford University Coverage Period: Beginning on or after 01/01/2015 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage For: Individual + Family Plan Type: PPO This is only
You can see the specialist you choose without permission from this plan.
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.crystalrunhealthinsurancecompany.com or by calling 1-844-638-6506.
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.crystalrunhealthinsurancecompany.com or by calling 1-844-638-6506.
What is the overall deductible? Are there other deductibles for specific services? Is there an out-ofpocket-limit
 Ambetter Balanced Care 10 (2016) + Vision Coverage Period: 01/01/2016-12/31/2016 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual/Family Plan Type: EPO This
Ambetter Balanced Care 10 (2016) + Vision Coverage Period: 01/01/2016-12/31/2016 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual/Family Plan Type: EPO This
Important Questions Answers Why this Matters: What is the overall deductible?
 Molina Healthcare of Texas, Inc.: Molina Silver 250 Plan Coverage Period: 01/01/2014-12/31/2014 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual + Family
Molina Healthcare of Texas, Inc.: Molina Silver 250 Plan Coverage Period: 01/01/2014-12/31/2014 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual + Family
Anthem Blue Cross: Anthem Silver DirectAccess, a Multi-State Plan Coverage Period: 01/01/ /31/2014
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.anthem.com/ca or by calling 1-855-333-5730. Important
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.anthem.com/ca or by calling 1-855-333-5730. Important
Important Questions Answers Why this Matters: For PPO Providers: $1,500 Member/$3,000 Family For Non-PPO Providers:
 Anthem Blue Cross Life and Health Insurance Company ACWA / JPIA: Account Based Health Plan (EV85) Coverage Period: 01/01/2015-12/31/2015 Summary of Benefits and Coverage: What this Plan Covers & What it
Anthem Blue Cross Life and Health Insurance Company ACWA / JPIA: Account Based Health Plan (EV85) Coverage Period: 01/01/2015-12/31/2015 Summary of Benefits and Coverage: What this Plan Covers & What it
$0 See the chart starting on page 2 for your costs for services this plan covers. Yes. For brand name drugs. Individual $150 / Family $300.
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.sharphealthplan.com or by calling 1-800-359-2002. Important
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.sharphealthplan.com or by calling 1-800-359-2002. Important
FEEL BETTER ABOUT YOUR CHOICES
 2015 FEEL BETTER ABOUT YOUR CHOICES CHOOSE WELLCARE. CHOOSE A PLAN TO FIT YOUR NEEDS. Information on individual and family plans inside. Kentucky Boone, Bullitt, Campbell, Clay, Harlan, Jefferson, Jessamine,
2015 FEEL BETTER ABOUT YOUR CHOICES CHOOSE WELLCARE. CHOOSE A PLAN TO FIT YOUR NEEDS. Information on individual and family plans inside. Kentucky Boone, Bullitt, Campbell, Clay, Harlan, Jefferson, Jessamine,
Anthem BlueCross BlueShield Blue Access PPO Option 10 / Rx Option 7 Summary of Benefits and Coverage: What this Plan Covers & What it Costs
 Anthem BlueCross BlueShield Blue Access PPO Option 10 / Rx Option 7 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage Period: 07/01/2015-0 /30/2016 Coverage For: Individual/Family
Anthem BlueCross BlueShield Blue Access PPO Option 10 / Rx Option 7 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage Period: 07/01/2015-0 /30/2016 Coverage For: Individual/Family
Important Questions Answers Why this Matters:
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.crystalrunhp.com or by calling 1-844-638-6506. Important
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.crystalrunhp.com or by calling 1-844-638-6506. Important
Coverage Period: Western Health Advantage: Plan A - Sierra 50 Silver. Summary of Benefits and Coverage: What this Plan Covers & What it Costs
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.westernhealth.com or by calling 1-888-563-2250. Important
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.westernhealth.com or by calling 1-888-563-2250. Important
HealthKeepers, Inc. Anthem HealthKeepers University of Virginia Physicians Group Anthem HealthKeepers- $750/$1,500 deductible
 HealthKeepers, Inc. Anthem HealthKeepers University of Virginia Physicians Group Anthem HealthKeepers- $750/$1,500 deductible Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage
HealthKeepers, Inc. Anthem HealthKeepers University of Virginia Physicians Group Anthem HealthKeepers- $750/$1,500 deductible Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage
Tri-County Schools Insurance Group: Basic Plan Coverage Period: 01/01/ /31/2014
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.tcsig.com or by calling Delta Health Systems at 1-800-464-7627.
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.tcsig.com or by calling Delta Health Systems at 1-800-464-7627.
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan
 Anthem BlueCross BlueShield Premier Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage Period: 01/01/2013-01/01/2014 Coverage For: Individual/Family Plan Type: PPO This is
Anthem BlueCross BlueShield Premier Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage Period: 01/01/2013-01/01/2014 Coverage For: Individual/Family Plan Type: PPO This is
Wellesley College Health Insurance Program Information
 Wellesley College Health Insurance Program Information Beginning August 15, 2014 Health Services All Wellesley College students, including Davis Scholars and Exchange students are encouraged to seek services
Wellesley College Health Insurance Program Information Beginning August 15, 2014 Health Services All Wellesley College students, including Davis Scholars and Exchange students are encouraged to seek services
Blue Care Elect Preferred Northeastern University
 Blue Care Elect Preferred Northeastern University Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage Period: on or after 01/01/2014 Coverage for: Individual and Family Plan
Blue Care Elect Preferred Northeastern University Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage Period: on or after 01/01/2014 Coverage for: Individual and Family Plan
Regence BlueCross BlueShield of Oregon: Preferred Plan A $500 Coverage Period: 01/01/ /31/2017
 Regence BlueCross BlueShield of Oregon: Preferred Plan A $500 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage Period: 01/01/2017 12/31/2017 Coverage for: Individual & Eligible
Regence BlueCross BlueShield of Oregon: Preferred Plan A $500 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage Period: 01/01/2017 12/31/2017 Coverage for: Individual & Eligible
Important Questions Answers Why this Matters:
 Anthem BlueCross BlueShield Blue Access PPO Option 20 / Rx Option 7 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage Period: 01/01/2015-12/31/2015 Coverage For: Individual/Family
Anthem BlueCross BlueShield Blue Access PPO Option 20 / Rx Option 7 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage Period: 01/01/2015-12/31/2015 Coverage For: Individual/Family
Important Questions Answers Why this Matters:
 Anthem BlueCross Value HMO 25/40/20% Select Plus HMO / $10/$30/$45/20% Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage Period: 01/01/2015-12/31/2015 Coverage For: Individual/Family
Anthem BlueCross Value HMO 25/40/20% Select Plus HMO / $10/$30/$45/20% Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage Period: 01/01/2015-12/31/2015 Coverage For: Individual/Family
Important Questions Answers Why this Matters:
 Anthem BlueCross BlueShield Blue Access PPO Option D54 / Rx Option 7 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage Period: 04/01/2013-03/31/2014 Coverage For: Individual/Family
Anthem BlueCross BlueShield Blue Access PPO Option D54 / Rx Option 7 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage Period: 04/01/2013-03/31/2014 Coverage For: Individual/Family
Anthem Blue Cross Placentia-Yorba Linda USD Custom Premier PPO 500/30/10 (500/30/90/60) High Option Coverage Period: 07/01/ /30/2017
 High Option Coverage Period: 07/01/ /30/2017") Anthem Blue Cross Placentia-Yorba Linda USD Custom Premier PPO 500/30/10 (500/30/90/60) High Option Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage Period: 07/01/2016-06/30/2017
Anthem Blue Cross Placentia-Yorba Linda USD Custom Premier PPO 500/30/10 (500/30/90/60) High Option Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage Period: 07/01/2016-06/30/2017
Does not apply to Network Preventive deductible?
 Wittenberg University: Blue Access (PPO) Option 2 Coverage Period: 01/01/2016-12/31/2016 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual/Family Plan Type:
Wittenberg University: Blue Access (PPO) Option 2 Coverage Period: 01/01/2016-12/31/2016 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual/Family Plan Type:
, TTY/TDD
 Ambetter from MHS: Ambetter Balanced Care 1 (2016) Coverage Period: 01/01/2016-12/31/2016 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual/Family Plan Type:
Ambetter from MHS: Ambetter Balanced Care 1 (2016) Coverage Period: 01/01/2016-12/31/2016 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual/Family Plan Type:
Glossary of Health Coverage and Medical Terms x
 Glossary of Health Coverage and Medical Terms x x x This glossary defines many commonly used terms, but isn t a full list. These glossary terms and definitions are intended to be educational and may be
Glossary of Health Coverage and Medical Terms x x x This glossary defines many commonly used terms, but isn t a full list. These glossary terms and definitions are intended to be educational and may be
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan
 BlueCross BlueShield Healthcare Plan of Georgia Premier Plus POS Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage Period: 01/01/2013-01/01/2014 Coverage For: Individual/Family
BlueCross BlueShield Healthcare Plan of Georgia Premier Plus POS Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage Period: 01/01/2013-01/01/2014 Coverage For: Individual/Family
Yes, written or oral approval is required, based upon medical policies.
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.uhc.com/calpers or by calling 1-877-359-3714. Important
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.uhc.com/calpers or by calling 1-877-359-3714. Important
Important Questions Answers Why this Matters:
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.anthem.com/ca or by calling 1-855-333-5730. Important
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.anthem.com/ca or by calling 1-855-333-5730. Important
Important Questions Answers Why this Matters:
 Molina Healthcare of Texas, Inc.: Molina Choice Bronze Plan Coverage Period: 01/01/2015-12/31/2015 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual + Family
Molina Healthcare of Texas, Inc.: Molina Choice Bronze Plan Coverage Period: 01/01/2015-12/31/2015 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual + Family
Custom Extrusion, Inc.: Non-Grandfathered Coverage Period: 7/1/15 6/30/16
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.chpbenefits.com or by calling 1-800-633-7867. Important
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.chpbenefits.com or by calling 1-800-633-7867. Important
Important Questions Answers Why this Matters:
 Anthem BlueCross BlueShield Blue Access PPO Option 14 / Rx Option AE Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage Period: 01/01/2015-12/31/2015 Coverage For: Individual/Family
Anthem BlueCross BlueShield Blue Access PPO Option 14 / Rx Option AE Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage Period: 01/01/2015-12/31/2015 Coverage For: Individual/Family
$3,500 individual / $7,000 family. Does not apply to office visits, generic drugs and preventative services.
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.mdwise.org/marketplace or by calling 1-855-417-5615 Important
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.mdwise.org/marketplace or by calling 1-855-417-5615 Important
What is the overall deductible?
 Molina Healthcare of California: Molina Silver 70 HMO Coverage Period: 01/01/2014 12/31/2014 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual + Family Plan
Molina Healthcare of California: Molina Silver 70 HMO Coverage Period: 01/01/2014 12/31/2014 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual + Family Plan
Coverage for: Individual and Family Plan Type: POS. Important Questions Answers Why this Matters: $250 member / $500 two-person /
 Blue Choice New England Plan 2 Berkshire Health Group Coverage Period: on or after 07/01/2016 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual and Family
Blue Choice New England Plan 2 Berkshire Health Group Coverage Period: on or after 07/01/2016 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual and Family
Important Questions Answers Why this Matters:
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.myiuhealthplans.com or by calling 1.866.895.5975. Important
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.myiuhealthplans.com or by calling 1.866.895.5975. Important
Important Questions Answers Why this Matters:
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.myiuhealthplans.com or by calling 1.866.895.5975 Important
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.myiuhealthplans.com or by calling 1.866.895.5975 Important
Important Questions Answers Why this Matters:
 Anthem BlueCross Anthem Elements Choice PPO 6000 / Generic Premium $15/$35/30% 500 Deductible Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage Period: 01/01/2015-12/31/2015
Anthem BlueCross Anthem Elements Choice PPO 6000 / Generic Premium $15/$35/30% 500 Deductible Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage Period: 01/01/2015-12/31/2015
You can see the specialist you choose without permission from this plan.
 Northwest Laborers-Employers Health & Security Trust: Coverage Period: 04/01/2013 03/31/2014 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual/Family Plan
Northwest Laborers-Employers Health & Security Trust: Coverage Period: 04/01/2013 03/31/2014 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual/Family Plan
Important Questions Answers Why this Matters:
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.anthem.com or by calling 1-877-309-2955. Important Questions
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.anthem.com or by calling 1-877-309-2955. Important Questions
Important Questions Answers Why this Matters:
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.capitalhealth.com or by calling 1-850-383-3311. Important
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.capitalhealth.com or by calling 1-850-383-3311. Important
No You don t have to meet deductibles for specified services, but see the chart starting on page 2 for other costs for services this plan covers.
 Molina Healthcare of Utah, Inc.: Molina Silver 150 Plan Coverage Period: 01/01/2016-12/31/2016 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual + Family
Molina Healthcare of Utah, Inc.: Molina Silver 150 Plan Coverage Period: 01/01/2016-12/31/2016 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual + Family