Emerging Cost Report Issues. Julie Quinn CPA, MBA VP of Cost Reporting & Provider Education Health Services Associates
|
|
|
- Clara Benson
- 5 years ago
- Views:
Transcription



1 Emerging Cost Report Issues Julie Quinn CPA, MBA VP of Cost Reporting & Provider Education Health Services Associates
2 Due FIVE months after your year end Currently still requiring hard copy of signature pages Electronic files submitted on disk or through Medicare contractor s portal
3 Reconciles interim payments to actual cost per visit Sets future interim reimbursement rates Influenza and Pneumococcal vaccines Medicare bad debt
4 COST / VISTS = RHC RATE
5 Independent RHCs: Subject to a ceiling/cap Cap = $83.45 Provider based >50 bed hospital: Capped same as independent Provider based <50 bed hospital: Actual cost per visit
6 Cost: Worksheet A/M-1 A-1, Ind., A-6 PB is where we reclassfiy cost A-2, Ind, A-8 PB is where we take things off and put things on Visits: Worksheet B/M-2 Rate/Settlement: Worksheet C/M-3 Vaccines: Worksheet B-1/M-4
7 Put all costs on this worksheet Must match your financials Use supplemental worksheets (A-1/A-2) to reclassify and exclude
8 Healthcare Costs Overhead Non- RHC
9 Compensation for healthcare staff Compensation for physician supervision Medical Supplies Malpractice/License fees/cme
10 TWO TYPES FACILITY ADMINISTRATIVE
11 Rent Insurance Interest on Mortgage Utilities Other building expenses
12 Office salaries Office supplies Legal/Accounting Telephone/IT costs Other administrative costs
13 Overhead Healthcare Non-RHC
14 Only include items that use overhead! Most common Non-RHC Technical component of Lab, X-Ray, EKG Other items not covered under the RHC program or paid outside of the RHC rate ONLY LEAVE AMOUNTS IN THE NON-RHC SECTION IF THEY NEED TO CAPTURE OVERHEAD
15 Does it use overhead at the clinic? (space, staff, etc.) RECLASSIFY! If it is a non-allowable expense that does not use overhead: EXCLUDE!
16 Method A: Staff performing lab, X-ray, EKG duties Allocate % of time for non-rhc carve out for staff performing non-rhc lab/x-ray/ekg duties vs. RHC duties Time studies of staff to support the allocated carve out Method B Time studies for each specific test Calculate time per test Multiply by number of tests performed Multiply by average hourly wage Reclassify resulting non-rhc wages into nonreimbursable cost center
17 Is CCM done in the clinic, by clinic staff? Reclassify direct healthcare staff costs into Non-RHC cost center New line on independent reports Is CCM handled by an outside company? Exclude direct CCM costs Exclude associated billing costs/incremental overhead costs
18 RHCs may serve as an originating site for telehealth services Originating site is the location of the patient at the time of service Cost of providing telehealth services must be classified in the Non-RHC section
19 If staff performing CCM and/or Telemedicine wear multiple hats in your clinic, use same calculations/methods as Lab/X-Ray/EKG Reclassify staff cost Report direct costs directly into the Non- RHC cost center New line on independent cost report, Line 55.60
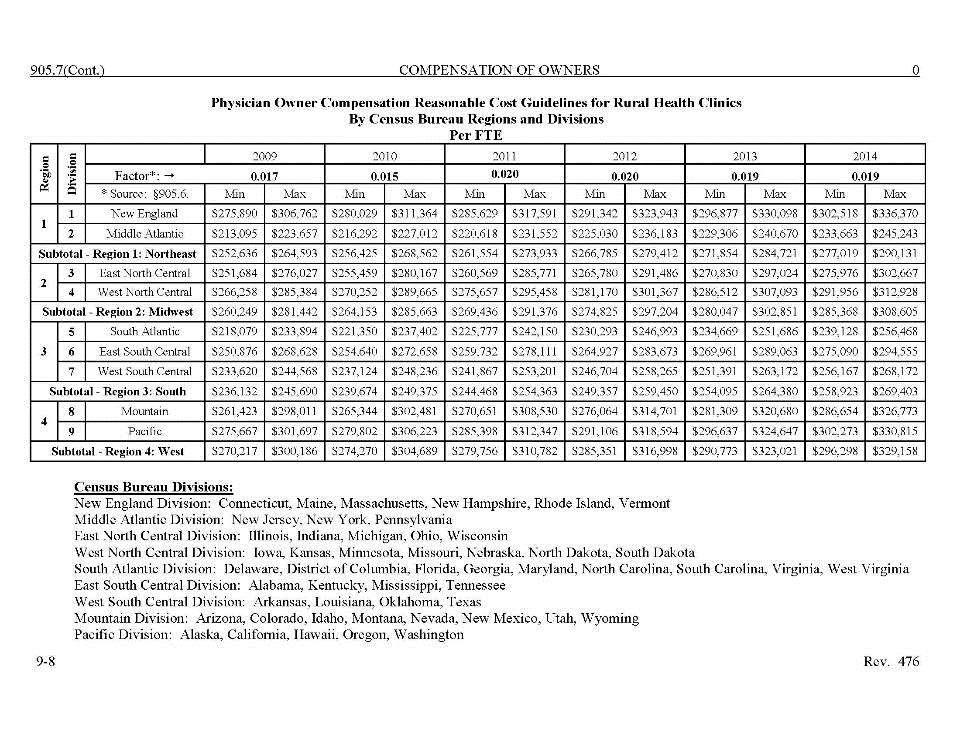
20 Depreciation should be adjusted from tax basis to Medicare basis (straight line) Owner s compensation for sole proprietors and partnerships
21 Provider Reimbursement Manual, Chapter 9 was updated in 2018 Section issued specific guidelines for Rural Health Clinics. Owner s compensation for sole proprietors and partnerships can be added to cost report, whether paid or not
22
23 Entertainment Gifts Charitable Contributions Automobile Expense where not related to patient care
24 Interest income up to interest expense Medical Records income Income from space rented to others (unless you can identify costs) Other miscellaneous income
25 Medicare allows actual cost (only) for items and services purchased from a related party
26 Example: Clinic owner also owns the building clinic pays building rent to clinic owner Medicare cost report will zero out the rent and add back what it costs the building owner: Property Taxes Mortgage Interest Building depreciation and maintenance
27 Definition: Face-to-face encounter with qualified provider during which covered services are performed. Broken down by provider type (MD, PA, NP) Count only face-to-face encounters Do not include visits for hospital, non covered services, non qualified providers or injections
28 Visits are reported by type of clinician Physician Physician Assistant Nurse Practitioner All clinician s working on a regular basis should be included in visits subject to the productivity standard Physician Services Under Agreement for the occasional fill in (locum tenens)
29 Medicare will charge the clinic with a minimum number of visits per FTE, whether performed or not 4,200 visits per employed or independent contractor physician FTE 2,100 visits per midlevel FTE Physician Services under agreement not subject to productivity standards limited application (cannot work on a regular basis)
30 Productivity Standard applied in aggregate Total visits (all providers subject to the FTE calculation) is compared to total minimum productivity standard A productive midlevel with visits in excess of their productivity standard can be used to offset a physician shortfall
31 FTE is based upon how many hours the practitioner is available to provide patient care FTE is calculated by practitioner type (Physician, PA, NP)
32 Seasonal Influenza and Pneumovax reporting has four data elements: Vaccine Staff Time Ratio Total vaccines given of each to ALL insurance types Total Medicare vaccines given of each (Medicare log must accompany cost report) Cost of vaccines (include invoices if possible)
33 Clinic must maintain logs of Influenza and Pneumococcal vaccines administered Invoices for the cost of Influenza and Pneumococcal vaccine should be submitted with the cost report Submit vaccine logs electronically if possible
34 Data is pulled from the clinic s PS&R Medicare visits include preventive visits Deductibles Total Medicare charges Medicare preventive charges
35 Data is pulled from the clinic s PS&R Coinsurance info only Medicare payments be sure to include MSP payments and lump sum settlements, if any. Bad Debts Total Bad Debt Dual Eligible
36 A copy of your PS&R (Provider Statistical and Reimbursement System report) will need to be obtained by the clinic electronically through CMS s Enterprise Portal at Go to the following link to access the PS&R: NOTE: If you need access or are having difficulty changing your password, please call their help desk at
37 Login using your user ID and password (you may have a two step authentication) Enter your user ID and Password Request Report (at the top under blue CMS banner) Select Request Summary It should be defaulted to the By Report Type button select Report Type 710 and hit the >> button to move it into the selected report types field Do the same for report type 71S Hit Continue Leave interval as year and input 01/01/207 in the start date field Hit Apply Hit Continue Select PDF, and hit Continue Hit Submit The next hour or two, check back to the report inbox for your report.
38 Compare PSR total to your Medicare visit count. Is this accurate? If not, determine why: Were incidental services included in the visit count Were dual-eligible counted twice Did more than one visit get counted on one day (surgical procedure/office visit)
39 Medicare bad debt form must accompany cost report of total bad debt being claimed. Medicare bad debt is claimed on the cost report based on the fiscal year in which the bad debt was written off, not date of service.
40 Medicare Bad Debt IS: Deductibles and Coinsurance amounts uncollectible from Medicare beneficiaries after reasonable collection efforts
41 Medicare Bad Debt IS NOT: Uncollected deductibles and coinsurance from: private pay patients, or any other non- Medicare beneficiary Medicare Advantage or Medicare Part B Charity, Courtesy, and Third-Party Payer Allowances Uncollected amounts due from other payers Disputed Medicare claims
42 Debt must be related to covered services and derived from deductible and coinsurance amounts. Provider must establish that reasonable collection efforts were made. Debt was actually uncollectible when claimed as worthless. Sound business judgment established that there was no likelihood of recovery at any time in the future.
43 The CFR at 42 CFR (f) requires that the uncollectible Medicare deductible and coinsurance be charged off as bad debts in the accounting period when the bad debt is determined to be worthless.
44 Bad debt log is for Medicare deductibles and coinsurance deemed uncollectible and written off clinic s books during the cost reporting period. It can, and most often does, contain dates of service prior to the current cost reporting period. Based on write off date, not date of service!
45 Two types of Medicare bad debts: Indigent or Medically Indigent Patients No collection efforts required for Medicaid beneficiaries. Must bill Medicaid and retain remittance advice as documentation Patients not deemed to be indigent: Collection efforts required
46 Automatic indigence determination for Medicare/Medicaid dual-eligible beneficiaries Must bill Medicaid for proof of eligibility and apply any Medicaid payments, if applicable. Must have a processed State Medicaid remittance advice before allowing dual eligible bad debts
47 Indigent patients not eligible for Medicaid: Indigence must be determined by the provider, not by the patient (i.e., a patient's signed declaration of his inability to pay his medical bills cannot be considered proof of indigence Take into account a patient's total resources which would include, but are not limited to, an analysis of assets (only those convertible to cash, and unnecessary for the patient's daily living), liabilities, and income and expenses
48 Indigent patients not eligible for Medicaid: Determine that no source other than the patient would be legally responsible for the patient's medical bill; e.g., title XIX, local welfare agency, or guardian and Patient's file should contain documentation of the method by which indigence was determined in addition to all backup information to substantiate the determination.
49 First bill must be sent within reasonable timeframe 90 days for most MACs SAME EFFORT applied to any bill: Collection letters Phone calls Collection agency (if used for non- Medicare patients)
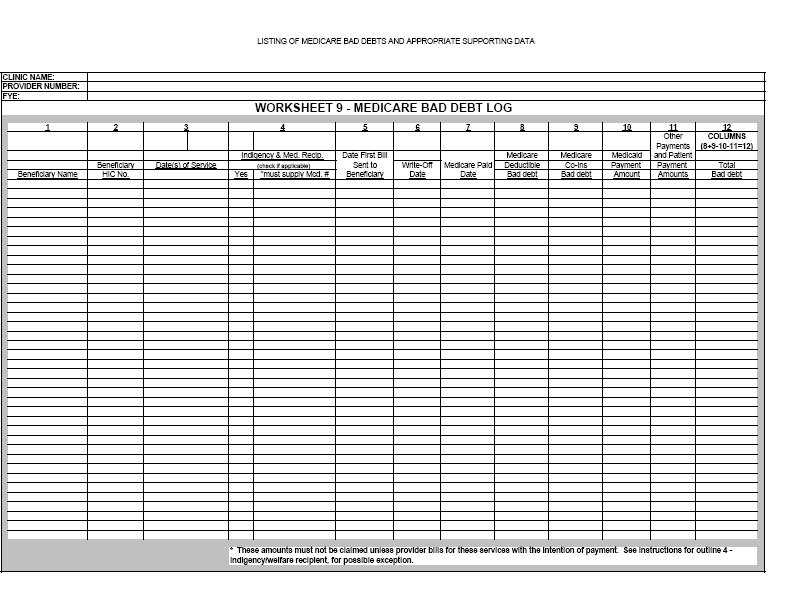
50 If after reasonable and customary attempts to collect a bill, the debt remains unpaid more than 120 days from the date the first bill is mailed to the beneficiary, the debt may be deemed uncollectible. Any payments received from the beneficiary re-starts the 120 uncollectability timeframe
51 Must be consistent among all payer types Must involve the issuance of a bill on or shortly after the date of service Should include other actions such as: Subsequent billings Collection Letters Telephone Calls or personal contacts with this party Must constitute a GENUINE, rather than a token, collection effort.
52 May involve the use of a Collection Agency in addition to or in lieu of subsequent billing by the clinic. If used: Refer all uncollected patient charges of like amount regardless of class of patient If the collection agency collects from the beneficiary, the FULL AMOUNT collected must be applied to the Medicare bad debt Collection agency fees applicable to the collection of the debt can be recorded as an administrative expense on the clinic s financial statements
53 Do NOT include a MEDICARE COLLECTION POLICY section within your collection policy. (This will indicate different treatment/procedures for the collection of Medicare bad debts and cause your bad debts to be disallowed at audit)
54 Within the section of the collection policy that outlines the procedure for bad debt write off (consistent among all patient classes), include a section that explains how to complete the Medicare bad debt log: How to fill out the log Documentation maintenance Referral to the cost report
55 Indigent Patients Medicaid dual-eligible beneficiary: Medicaid remittance advice indicating payment or denial of payment. Indigent, not Medicaid eligible: Documentation of the method by which indigence was determined in addition to all backup information to substantiate the determination
56 Non-Indigent Patients Collection efforts must be documented in the patient s file Copies of bills Documentation of phone calls/personal contact Follow up letters
57 Patient Name HIC number Date of service Whether the patient has been deemed indigent and their Medicaid number if this was the method utilized to determine indigence Date the first bill was sent to the beneficiary Date the bad debt was written off Remittance advice date Deductible and coinsurance amount Total Medicare bad debt (reduced by recoveries)
58
59
Cost Reports 101: Just the Important Pages. Julie Quinn. CPA, VP of Cost Reporting & Provider Education Health Services Associates
 Cost Reports 101: Just the Important Pages Julie Quinn CPA, VP of Cost Reporting & Provider Education Health Services Associates Julie Quinn, CPA VP, Cost Reporting & Provider Education Health Services
Cost Reports 101: Just the Important Pages Julie Quinn CPA, VP of Cost Reporting & Provider Education Health Services Associates Julie Quinn, CPA VP, Cost Reporting & Provider Education Health Services
David S. James, CPA. Advanced RHC Cost Reporting
 North American Healthcare Management Services David S. James, CPA Advanced Rural Health Clinic Cost Reporting Advanced RHC Cost Reporting Advanced RHC Cost Reporting 1. RHC General Information 2. Related
North American Healthcare Management Services David S. James, CPA Advanced Rural Health Clinic Cost Reporting Advanced RHC Cost Reporting Advanced RHC Cost Reporting 1. RHC General Information 2. Related
RHC Medicare Cost Reporting 101 Katie Jo Raebel, CPA, Partner March 20, 2019
 RHC Medicare Cost Reporting 101 Katie Jo Raebel, CPA, Partner March 20, 2019 Wipfli LLP Critical Access Hospital and Rural Health Clinic Conference 0 Today s Agenda Rural Health Clinic Medicare Cost Report
RHC Medicare Cost Reporting 101 Katie Jo Raebel, CPA, Partner March 20, 2019 Wipfli LLP Critical Access Hospital and Rural Health Clinic Conference 0 Today s Agenda Rural Health Clinic Medicare Cost Report
Focusing on the Quadruple Aim
 Focusing on the Quadruple Aim Cost Reporting Pitfalls and Big Rocks May 2, 2017 Wipfli LLP 1 Rural Health Clinic Medicare Cost Report Overview Allowable Costs Non-RHC Costs Provider Staffing RHC Visits/Productivity
Focusing on the Quadruple Aim Cost Reporting Pitfalls and Big Rocks May 2, 2017 Wipfli LLP 1 Rural Health Clinic Medicare Cost Report Overview Allowable Costs Non-RHC Costs Provider Staffing RHC Visits/Productivity
North American Healthcare Management Services David S. James, CPA Cost Report Basics
 North American Healthcare Management Services David S. James, CPA Cost Report Basics RHC Cost Reporting Basics 1. RHC General Information 2. Cost Report Worksheets 3. Reclassifications Examples 4. Adjustments
North American Healthcare Management Services David S. James, CPA Cost Report Basics RHC Cost Reporting Basics 1. RHC General Information 2. Cost Report Worksheets 3. Reclassifications Examples 4. Adjustments
RHC Cost Reporting RHC Update Seminar Fall, 2017
 RHC Cost Reporting RHC Update Seminar Fall, 2017 Contact Information Mark Lynn, CPA (Inactive) RHC Consultant Healthcare Business Specialists Suite 214, 502 Shadow Parkway Chattanooga, Tennessee 37421
RHC Cost Reporting RHC Update Seminar Fall, 2017 Contact Information Mark Lynn, CPA (Inactive) RHC Consultant Healthcare Business Specialists Suite 214, 502 Shadow Parkway Chattanooga, Tennessee 37421
Rural Health Clinic: Topics in Billing, Cost Reporting & Reimbursement
 Rural Health Clinic: Topics in Billing, Cost Reporting & Reimbursement Date or subtitle November 1, 2010 www.wipfli.com 1 Discussion Overview RHC Billing Resources CMS Charts; CMS Manuals Billing for Pneumococcal,
Rural Health Clinic: Topics in Billing, Cost Reporting & Reimbursement Date or subtitle November 1, 2010 www.wipfli.com 1 Discussion Overview RHC Billing Resources CMS Charts; CMS Manuals Billing for Pneumococcal,
Rural Health Clinic: Topics in Billing, Cost Reporting & Reimbursement
 Rural Health Clinic: Topics in Billing, Cost Reporting & Reimbursement Discussion Overview RHC Billing Resources CMS Charts; CMS Manuals 2012 RHC Maximum Rates; Fee Schedule Payment Changes RHC Billing/Reimbursement;
Rural Health Clinic: Topics in Billing, Cost Reporting & Reimbursement Discussion Overview RHC Billing Resources CMS Charts; CMS Manuals 2012 RHC Maximum Rates; Fee Schedule Payment Changes RHC Billing/Reimbursement;
Helpful Tips on Preparing Your Next Cost Report June 19, 2018
 Helpful Tips on Preparing Your Next Cost Report June 19, 2018 Contact Information Mark Lynn, CPA (Inactive) RHC Consultant Healthcare Business Specialists Suite 214, 502 Shadow Parkway Chattanooga, Tennessee
Helpful Tips on Preparing Your Next Cost Report June 19, 2018 Contact Information Mark Lynn, CPA (Inactive) RHC Consultant Healthcare Business Specialists Suite 214, 502 Shadow Parkway Chattanooga, Tennessee
REGION IV MEDICARE WORKSHOP NAVIGATING MEDICARE PPS INCLUDING THE NEW FQHC COST REPORT FORM CMS
 REGION IV MEDICARE WORKSHOP NAVIGATING MEDICARE PPS INCLUDING THE NEW FQHC COST REPORT FORM CMS-224-14 Presented by: Jeffrey Allen, CPA, Partner June 15 th and 16 th - 2017 TODAY S AGENDA Introduction
REGION IV MEDICARE WORKSHOP NAVIGATING MEDICARE PPS INCLUDING THE NEW FQHC COST REPORT FORM CMS-224-14 Presented by: Jeffrey Allen, CPA, Partner June 15 th and 16 th - 2017 TODAY S AGENDA Introduction
MEDICARE COST REPORT 101 OCTOBER
 MEDICARE COST REPORT 101 OCTOBER 24, 2018 1 PRESENTERS JULIANNE KIPPLE HEALTHCARE DIRECTOR 402.827.2075 JKIPPLE@LUTZ.US KIRK DELPERDANG HEALTHCARE MANAGER 402.827.2361 KDELPERDANG@LUTZ.US AGENDA CMS REIMBURSEMENT
MEDICARE COST REPORT 101 OCTOBER 24, 2018 1 PRESENTERS JULIANNE KIPPLE HEALTHCARE DIRECTOR 402.827.2075 JKIPPLE@LUTZ.US KIRK DELPERDANG HEALTHCARE MANAGER 402.827.2361 KDELPERDANG@LUTZ.US AGENDA CMS REIMBURSEMENT
5-13 Form CMS
 5-13 Form CMS-222-92 2990 (Cont.) This report is required by law (42 USC. 1395g: CFR 413.20(b)). Failure to report can result FORM APPROVED in all payments made during the reporting period being deemed
5-13 Form CMS-222-92 2990 (Cont.) This report is required by law (42 USC. 1395g: CFR 413.20(b)). Failure to report can result FORM APPROVED in all payments made during the reporting period being deemed
Northern California HFMA - Spring Conference. Identification, Documentation, Claiming Medicare Allowable Bad Debts on Your Medicare Cost Report
 Northern California HFMA - Spring Conference MEDICARE BAD DEBTS Identification, Documentation, Claiming Medicare Allowable Bad Debts on Your Medicare Cost Report Presented by : Rodney A. Phillips CPA CGMA
Northern California HFMA - Spring Conference MEDICARE BAD DEBTS Identification, Documentation, Claiming Medicare Allowable Bad Debts on Your Medicare Cost Report Presented by : Rodney A. Phillips CPA CGMA
Reimbursement and Funding Methodology. Florida Medicaid Reform Section 1115 Waiver. Low Income Pool
 Reimbursement and Funding Methodology Florida Medicaid Reform Section 1115 Waiver Low Income Pool Submitted June 26, 2009 1 Table of Contents I. OVERVIEW... 3 II. REIMBURSEMENT METHODOLOGY... 5 III. DEFINITIONS...
Reimbursement and Funding Methodology Florida Medicaid Reform Section 1115 Waiver Low Income Pool Submitted June 26, 2009 1 Table of Contents I. OVERVIEW... 3 II. REIMBURSEMENT METHODOLOGY... 5 III. DEFINITIONS...
HERE WE GO AGAIN: THE LATEST ON ICD-10 AND MEDICARE AUDITS
 HERE WE GO AGAIN: THE LATEST ON ICD-10 AND MEDICARE AUDITS TODAY S OBJECTIVES International Classification of Diseases (ICD )-10: Delay to 2015? Medicare Cost Report : Desk Review and Audit Findings 2
HERE WE GO AGAIN: THE LATEST ON ICD-10 AND MEDICARE AUDITS TODAY S OBJECTIVES International Classification of Diseases (ICD )-10: Delay to 2015? Medicare Cost Report : Desk Review and Audit Findings 2
CT Nursing Facilities 2017 Legislation: Reimbursement Presentation to the Membership of CAHCF. December 7, 2017
 CT Nursing Facilities 2017 Legislation: Reimbursement Presentation to the Membership of CAHCF Vincent Ruocco, CPA Partner vruocco@odpkf.com December 7, 2017 Discussion CT Medicaid rates effective July
CT Nursing Facilities 2017 Legislation: Reimbursement Presentation to the Membership of CAHCF Vincent Ruocco, CPA Partner vruocco@odpkf.com December 7, 2017 Discussion CT Medicaid rates effective July
MEDICARE BAD DEBTS. Northwest Ohio HFMA February 14, 2018
 MEDICARE BAD DEBTS Northwest Ohio HFMA February 14, 2018 AGENDA Understanding Medicare Bad Debts (MBD) Medicare Bad Debt Categories Medicare Administrative Contractor (MAC) Audit 2 UNDERSTANDING MBD 3
MEDICARE BAD DEBTS Northwest Ohio HFMA February 14, 2018 AGENDA Understanding Medicare Bad Debts (MBD) Medicare Bad Debt Categories Medicare Administrative Contractor (MAC) Audit 2 UNDERSTANDING MBD 3
Health Financial Systems MCRS/PC-WIN FOR SAMPLE HEALTH CENTER IN LIEU OF FORM CMS (03/2010) PREPARED 8/20/2012( 9:28)
 PREPARED 8/20/2012( 9:28)") Health Financial Systems MCRS/PC-WIN FOR SAMPLE HEALTH CENTER IN LIEU OF FORM CMS-222-92(03/2010) PREPARED 8/20/2012( 9:28) THIS REPORT IS REQUIRED BY LAW (42 USC 1395g: CFR413.20(b)). FAILURE TO REPORT
Health Financial Systems MCRS/PC-WIN FOR SAMPLE HEALTH CENTER IN LIEU OF FORM CMS-222-92(03/2010) PREPARED 8/20/2012( 9:28) THIS REPORT IS REQUIRED BY LAW (42 USC 1395g: CFR413.20(b)). FAILURE TO REPORT
TRANSMITTAL 16 CHANGES PAGE 1 (SIGNIFICANT CMS FORM AND PROGRAM CHANGES CONTAINED IN COMPU-MAX VERSION 2013.
 1728-94 TRANSMITTAL 16 CHANGES PAGE 1 Compu-Max 1728-94 Version 2013.08 contains changes required by Transmittal 16 to Form CMS-1728-94. This transmittal updates Chapter 32, Home Health Agency Cost Report,
1728-94 TRANSMITTAL 16 CHANGES PAGE 1 Compu-Max 1728-94 Version 2013.08 contains changes required by Transmittal 16 to Form CMS-1728-94. This transmittal updates Chapter 32, Home Health Agency Cost Report,
Using Analytics to Maximize Revenue and Minimize Out-of-pocket Burden on Patients The underinsured and how hospitals can meet the challenges
 Using Analytics to Maximize Revenue and Minimize Out-of-pocket Burden on Patients The underinsured and how hospitals can meet the challenges HFMA Lone Star Waco Road Show September 21, 2018 Todd Doze CEO,
Using Analytics to Maximize Revenue and Minimize Out-of-pocket Burden on Patients The underinsured and how hospitals can meet the challenges HFMA Lone Star Waco Road Show September 21, 2018 Todd Doze CEO,
4012 FORM CMS
 4012 FORM CMS-2552-10 09-17 4012. Worksheet S-10 - Hospital Uncompensated and Indigent Care Data--Section 112(b) of the Balanced Budget Refinement Act (BBRA) requires that short-term acute care hospitals
4012 FORM CMS-2552-10 09-17 4012. Worksheet S-10 - Hospital Uncompensated and Indigent Care Data--Section 112(b) of the Balanced Budget Refinement Act (BBRA) requires that short-term acute care hospitals
Guide to Completing Worksheet S-10 September 23, 2015
 Guide to Completing Worksheet S-10 September 23, 2015 The information presented is intended to provide guidance on completing Worksheet S-10 in accordance with Form CMS-2552-10 (Hospital Cost Report) instructions
Guide to Completing Worksheet S-10 September 23, 2015 The information presented is intended to provide guidance on completing Worksheet S-10 in accordance with Form CMS-2552-10 (Hospital Cost Report) instructions
MEDICARE BAD DEBT A REVENUE OPPORTUNITY. Call
 MEDICARE BAD DEBT A REVENUE OPPORTUNITY Who Me? Shawn K. Gretz VP of Sales for Americollect *People seeking legal advice should always consult with an attorney. Call 1-920-645-6017 Email sales@americollect.com
MEDICARE BAD DEBT A REVENUE OPPORTUNITY Who Me? Shawn K. Gretz VP of Sales for Americollect *People seeking legal advice should always consult with an attorney. Call 1-920-645-6017 Email sales@americollect.com
Reimbursement and Funding Methodology. Florida Medicaid Reform Section 1115 Waiver. Low Income Pool
 Reimbursement and Funding Methodology Florida Medicaid Reform Section 1115 Waiver Low Income Pool February 1, 2013 Table of Contents I. OVERVIEW 3 II. REIMBURSEMENT METHODOLOGY 6 III. DEFINITIONS 6 IV.
Reimbursement and Funding Methodology Florida Medicaid Reform Section 1115 Waiver Low Income Pool February 1, 2013 Table of Contents I. OVERVIEW 3 II. REIMBURSEMENT METHODOLOGY 6 III. DEFINITIONS 6 IV.
Hospital Cost Report Training Level II Critical Reimbursement Strategies // General Session Dallas - Hilton Dallas/Southlake Town Square
 Hospital Cost Report Training Level II Critical Reimbursement Strategies // General Session Dallas - Hilton Dallas/Southlake Town Square JULY 27-28, 2016 All information provided is of a general nature
Hospital Cost Report Training Level II Critical Reimbursement Strategies // General Session Dallas - Hilton Dallas/Southlake Town Square JULY 27-28, 2016 All information provided is of a general nature
Cost Reporting 101: Your Medicare Cost Report from A - M
 Cost Reporting 101: Your Medicare Cost Report from A - M Paul Traczek, CPA, Partner Holly Pokrandt, CPA, Partner September 27, 2018 Cost Reporting 101: A Crash Course in the Basics What will be covered
Cost Reporting 101: Your Medicare Cost Report from A - M Paul Traczek, CPA, Partner Holly Pokrandt, CPA, Partner September 27, 2018 Cost Reporting 101: A Crash Course in the Basics What will be covered
What Hospitals Need to Know About Cost Report Changes
 What Hospitals Need to Know About Cost Report Changes Sue Brammer Partner, Kansas City Kevin Wellen Senior Managing Consultant, St. Louis To receive CPE credit: Participate in the entire webinar Answer
What Hospitals Need to Know About Cost Report Changes Sue Brammer Partner, Kansas City Kevin Wellen Senior Managing Consultant, St. Louis To receive CPE credit: Participate in the entire webinar Answer
J11 Part A Provider Audit and Reimbursement Update. February 5, 2014
 J11 Part A Provider Audit and Reimbursement Update February 5, 2014 Agenda A & R Operational Update SSI/DSH Update PSR Update Wage Index 2015 Bad Debt Update EHR Audits Contacts 2 Audit and Reimbursement
J11 Part A Provider Audit and Reimbursement Update February 5, 2014 Agenda A & R Operational Update SSI/DSH Update PSR Update Wage Index 2015 Bad Debt Update EHR Audits Contacts 2 Audit and Reimbursement
CMS Reasonable Collection Requirement Probate and Bankruptcy
 CMS Reasonable Collection Requirement Probate and Bankruptcy Introduction Angela Horn Contributor to national publications Longterm Living, Healthcare Finance News, HFM Magazine, Credit and Collections
CMS Reasonable Collection Requirement Probate and Bankruptcy Introduction Angela Horn Contributor to national publications Longterm Living, Healthcare Finance News, HFM Magazine, Credit and Collections
Medicare Accounts Receivable Management Strategies. Your Speakers
 Medicare Accounts Receivable Management Strategies Leading Age Michigan 2014 Annual Leadership Institute Friday, August 15, 2014 8:30 am 9:30 am 1 Your Speakers Janet Potter, CPA, MAS Manager, Healthcare
Medicare Accounts Receivable Management Strategies Leading Age Michigan 2014 Annual Leadership Institute Friday, August 15, 2014 8:30 am 9:30 am 1 Your Speakers Janet Potter, CPA, MAS Manager, Healthcare
Reimbursement and Funding Methodology For Demonstration Year 11. Florida s 1115 Managed Medical Assistance Waiver. Low Income Pool
 Reimbursement and Funding Methodology For Demonstration Year 11 Florida s 1115 Managed Medical Assistance Waiver Low Income Pool November 30, 2015 1 Table of Contents I. OVERVIEW... 3 II. REIMBURSEMENT
Reimbursement and Funding Methodology For Demonstration Year 11 Florida s 1115 Managed Medical Assistance Waiver Low Income Pool November 30, 2015 1 Table of Contents I. OVERVIEW... 3 II. REIMBURSEMENT
Wise Health System and Wise Health Clinics, Revenue Cycle
 Title: Department/Service Line: Location: Document Location ID: Financial Assistance Wise Health System and Wise Health Clinics, Revenue Cycle WHS.SYS.PCP Origination Date: 5/2017 Last Review Date: 6/2017
Title: Department/Service Line: Location: Document Location ID: Financial Assistance Wise Health System and Wise Health Clinics, Revenue Cycle WHS.SYS.PCP Origination Date: 5/2017 Last Review Date: 6/2017
NOTE: cost reporting period filed on or before November 15, 2004
 11-17 FORM CMS-2552-10 4033.2 Line 17.50--Enter the Pioneer ACO demonstration payment adjustment amount. Obtain this amount from the PS&R. Do not use this line for services rendered on or after January
11-17 FORM CMS-2552-10 4033.2 Line 17.50--Enter the Pioneer ACO demonstration payment adjustment amount. Obtain this amount from the PS&R. Do not use this line for services rendered on or after January
(Cont.) FORM CMS Line 4--Enter the amount of outlier payments made for OPPS services rendered during the cost reporting period. C
 FORM CMS Line 4--Enter the amount of outlier payments made for OPPS services rendered during the cost reporting period. C") 03-18 FORM CMS-2552-10 4030.2 4030.2 Part B - Medical and Other Health Services--Use Worksheet E, Part B, to calculate reimbursement settlement for hospitals, subproviders, and SNFs. Use a separate copy
03-18 FORM CMS-2552-10 4030.2 4030.2 Part B - Medical and Other Health Services--Use Worksheet E, Part B, to calculate reimbursement settlement for hospitals, subproviders, and SNFs. Use a separate copy
PERSPECTIVE HEALTHCARE WIPFLI. Critical Access Hospital Medicare Cost Report - Annual Checkup. December 2007
 WIPFLI HEALTHCARE December 2007 expert advice innovative solutions performance improvement PERSPECTIVE Critical Access Hospital Medicare Cost Report - Annual Checkup While filing a Medicare cost report
WIPFLI HEALTHCARE December 2007 expert advice innovative solutions performance improvement PERSPECTIVE Critical Access Hospital Medicare Cost Report - Annual Checkup While filing a Medicare cost report
Allowability of Costs for an FQHC Initial Rate Setting or Change in Scope of Services September 27, 2017 Version 1
 Allowability of Costs for an FQHC Initial Rate Setting or Change in Scope of Services September 27, 2017 Version 1 Purpose: To ensure as efficient and clear a process for health center rate setting and
Allowability of Costs for an FQHC Initial Rate Setting or Change in Scope of Services September 27, 2017 Version 1 Purpose: To ensure as efficient and clear a process for health center rate setting and
Uncompensated Care Payments and Worksheet S-10. HFMA Maine Chapter
 Uncompensated Care Payments and Worksheet S-10 HFMA Maine Chapter January 11, 2018 Disproportionate Share & Uncompensated Care Payments 2 Medicare DSH Payments Total payment is the sum of the following:
Uncompensated Care Payments and Worksheet S-10 HFMA Maine Chapter January 11, 2018 Disproportionate Share & Uncompensated Care Payments 2 Medicare DSH Payments Total payment is the sum of the following:
02-03 FORM CMS
 3527 FORM HCFA 2540-96 01-01 3527. WORKSHEET C - RATIO OF COST TO CHARGES FOR ANCILLARY OUTPATIENT COST CENTERS This worksheet computes the ratio of cost to charges for ancillary services and, for costs
3527 FORM HCFA 2540-96 01-01 3527. WORKSHEET C - RATIO OF COST TO CHARGES FOR ANCILLARY OUTPATIENT COST CENTERS This worksheet computes the ratio of cost to charges for ancillary services and, for costs
Prior Authorization All non-emergent services rendered by non-contracted providers require prior authorization, unless specified otherwise.
 Prior Authorization All non-emergent services rendered by non-contracted providers require prior authorization, unless specified otherwise. Abortions, Hysterectomies and Sterilizations Ambulance Emergency
Prior Authorization All non-emergent services rendered by non-contracted providers require prior authorization, unless specified otherwise. Abortions, Hysterectomies and Sterilizations Ambulance Emergency
2018 Provider Manual
 2018 Provider Manual Table of Contents Client Conditions of Participation... 3 Provider Conditions of Participation... 4 Provider and Participant Services... 6 Timely Filing... 8 Prior Authorization...
2018 Provider Manual Table of Contents Client Conditions of Participation... 3 Provider Conditions of Participation... 4 Provider and Participant Services... 6 Timely Filing... 8 Prior Authorization...
I. Determine practitioner(s) or groups eligible to participate in the Physician UPL Supplemental Payment program.
 or groups eligible to participate in the Physician UPL Supplemental Payment program.") Physician UPL Supplemental Payment Program Instructions and Frequently Asked Questions Revised 01/16/2018 Latest Approved State Plan Amendment - #17-0011 The Louisiana Department of Health (LDH) has been
Physician UPL Supplemental Payment Program Instructions and Frequently Asked Questions Revised 01/16/2018 Latest Approved State Plan Amendment - #17-0011 The Louisiana Department of Health (LDH) has been
Cost Analysis Data Entry Workbook Guide
 Cost Analysis Data Entry Workbook Guide January 2016 Table of Contents I. Introduction to Cost Analysis... 1 II. Overview of Workbook... 2 III. Worksheet Guidance... 3 Overview of the Cost Analysis Workbook...
Cost Analysis Data Entry Workbook Guide January 2016 Table of Contents I. Introduction to Cost Analysis... 1 II. Overview of Workbook... 2 III. Worksheet Guidance... 3 Overview of the Cost Analysis Workbook...
February 19, Dear Ms. Verma,
 Seema Verma Administrator Centers for Medicare & Medicaid Services Hubert H. Humphrey Building 200 Independence Avenue, S.W., Room 445-G Washington, DC 20201 Dear Ms. Verma, On behalf of our nearly 5,000
Seema Verma Administrator Centers for Medicare & Medicaid Services Hubert H. Humphrey Building 200 Independence Avenue, S.W., Room 445-G Washington, DC 20201 Dear Ms. Verma, On behalf of our nearly 5,000
National Association of Rural Health Clinics. Billing Overview. Shannon Chambers Janet Lytton. CRHCP Code:
 National Association of Rural Health Clinics Billing Overview Shannon Chambers Janet Lytton CRHCP Code: 998-40 RHC Services An RHC Encounter is defined as a medically-necessary, face-to face (one-on-one)
National Association of Rural Health Clinics Billing Overview Shannon Chambers Janet Lytton CRHCP Code: 998-40 RHC Services An RHC Encounter is defined as a medically-necessary, face-to face (one-on-one)
Critical Access Hospital Billing and Reimbursement Strategies
 Critical Access Hospital Billing and Reimbursement Strategies Minnesota Rural Health Conference July 19, 2005 Ralph J. Llewellyn, CPA, CHFP rllewellyn@eidebailly.com (701) 239-8594 Objectives Provide basic
Critical Access Hospital Billing and Reimbursement Strategies Minnesota Rural Health Conference July 19, 2005 Ralph J. Llewellyn, CPA, CHFP rllewellyn@eidebailly.com (701) 239-8594 Objectives Provide basic
I. Cost Finding and Cost Reporting
 FLORIDA TITLE XIX COUNTY HEALTH DEPARTMENT REIMBURSEMENT PLAN VERSION XV EFFECTIVE DATE: July 1, 2017 I. Cost Finding and Cost Reporting A. Each county health department (CHD) participating in the Florida
FLORIDA TITLE XIX COUNTY HEALTH DEPARTMENT REIMBURSEMENT PLAN VERSION XV EFFECTIVE DATE: July 1, 2017 I. Cost Finding and Cost Reporting A. Each county health department (CHD) participating in the Florida
Cost Report Compliance Issues for Critical Access Hospitals
 Cost Report Compliance Issues for Critical Access Hospitals OIG s Compliance Guidance Model Compliance Plan Published February 23, 1998 Supplemental Guidance: January 31, 2005 False or Fraudulent Cost
Cost Report Compliance Issues for Critical Access Hospitals OIG s Compliance Guidance Model Compliance Plan Published February 23, 1998 Supplemental Guidance: January 31, 2005 False or Fraudulent Cost
Creation Date: 12/17/15 Title: Financial Assistance Program Revision History: Revenue Cycle
 Renown Health Policies & Procedures Current Version Effective Date: Page 1 of 9 6/18/18 Creation Date: 12/17/15 Title: Financial Assistance Program Revision History: Type: Number: Revenue Cycle Renown.SPC.6
Renown Health Policies & Procedures Current Version Effective Date: Page 1 of 9 6/18/18 Creation Date: 12/17/15 Title: Financial Assistance Program Revision History: Type: Number: Revenue Cycle Renown.SPC.6
CRITICAL ACCESS HOSPITAL Reimbursement Strategies and Opportunities
 CRITICAL ACCESS HOSPITAL Reimbursement Strategies and Opportunities MICHAEL R. BELL & COMPANY, PLLC 12 EAST ROWAN, SUITE 2 SPOKANE, WASHINGTON 99207 (509) 489-4524 Quick Fix Does Medicare Owe You Money
CRITICAL ACCESS HOSPITAL Reimbursement Strategies and Opportunities MICHAEL R. BELL & COMPANY, PLLC 12 EAST ROWAN, SUITE 2 SPOKANE, WASHINGTON 99207 (509) 489-4524 Quick Fix Does Medicare Owe You Money
Medicare Update Rural Hospi Rural Hospi al Fi al nance
 Medicare Update Rural Hospital Finance Workshop- August 24, 2012 PS&R Redesign Update PS&R Redesign Issue-Negative Charges A problem has occurred in the claims processing system where non covered charges
Medicare Update Rural Hospital Finance Workshop- August 24, 2012 PS&R Redesign Update PS&R Redesign Issue-Negative Charges A problem has occurred in the claims processing system where non covered charges
Medicare Claims Processing Manual Chapter 9 - Rural Health Clinics/ Federally Qualified Health Centers
 Medicare Claims Processing Manual Chapter 9 - Rural Health Clinics/ Federally Qualified Health Centers Transmittals for Chapter 9 Table of Contents (Rev. 3434, 12-31-15) 10 - Rural Health Clinic (RHC)
Medicare Claims Processing Manual Chapter 9 - Rural Health Clinics/ Federally Qualified Health Centers Transmittals for Chapter 9 Table of Contents (Rev. 3434, 12-31-15) 10 - Rural Health Clinic (RHC)
RULES OF TENNESSEE DEPARTMENT OF HEALTH DIVISION OF MEDICAID CHAPTER PSYCHIATRIC HOSPITAL REIMBURSEMENT PROGRAM TABLE OF CONTENTS
 RULES OF TENNESSEE DEPARTMENT OF HEALTH DIVISION OF MEDICAID CHAPTER 1200-13-9 PSYCHIATRIC HOSPITAL REIMBURSEMENT PROGRAM TABLE OF CONTENTS 1200-13-9-.01 Definitions 1200-13-9-09 Minimum Occupancy Adjustment
RULES OF TENNESSEE DEPARTMENT OF HEALTH DIVISION OF MEDICAID CHAPTER 1200-13-9 PSYCHIATRIC HOSPITAL REIMBURSEMENT PROGRAM TABLE OF CONTENTS 1200-13-9-.01 Definitions 1200-13-9-09 Minimum Occupancy Adjustment
I. Determine practitioner(s) or groups eligible to participate in the Physician UPL Supplemental Payment program.
 or groups eligible to participate in the Physician UPL Supplemental Payment program.") Physician UPL Supplemental Payment Program Instructions and Frequently Asked Questions Revised 07/19/2018 Latest Approved State Plan Amendment - #17-0011 The Louisiana Department of Health (LDH) has been
Physician UPL Supplemental Payment Program Instructions and Frequently Asked Questions Revised 07/19/2018 Latest Approved State Plan Amendment - #17-0011 The Louisiana Department of Health (LDH) has been
Reimbursement & Cost Report Strategies. Reducing cost is NOT always the solution.
 Reimbursement & Cost Report Strategies Reducing cost is NOT always the solution. 1 Summary Reimbursement cuts = organizations reduce costs Some fixed cost cuts help bottom line, others harm Other reimbursement
Reimbursement & Cost Report Strategies Reducing cost is NOT always the solution. 1 Summary Reimbursement cuts = organizations reduce costs Some fixed cost cuts help bottom line, others harm Other reimbursement
Medicare DSH Dissecting Uncompensated Care Cost
 Medicare DSH Dissecting Uncompensated Care Cost September 17, 2018 Northern California HFMA HEALTHCARE: A Brave New World Annual Fall Conference Uncompensated Care Recognition Services 1 Uncompensated
Medicare DSH Dissecting Uncompensated Care Cost September 17, 2018 Northern California HFMA HEALTHCARE: A Brave New World Annual Fall Conference Uncompensated Care Recognition Services 1 Uncompensated
Healthcare Financial Management Association Certification Program. Module I: The Business of Health Care Learner s Guide
 Healthcare Financial Management Association Certification Program Module I: The Business of Health Care Learner s Guide For examination period beginning June 2015 1 Course 1 - The Big Picture Learning
Healthcare Financial Management Association Certification Program Module I: The Business of Health Care Learner s Guide For examination period beginning June 2015 1 Course 1 - The Big Picture Learning
The Impact of ACA on Dialysis Reimbursement
 The Impact of ACA on Dialysis Reimbursement Bruce J. Thompson, CPA CMA www.gaiasoftware.com 43 rd Annual FRAA Conference July 23, 2016 Yes -Potbelly Pigs are Smart Meet Milo Medicare Cost Report General
The Impact of ACA on Dialysis Reimbursement Bruce J. Thompson, CPA CMA www.gaiasoftware.com 43 rd Annual FRAA Conference July 23, 2016 Yes -Potbelly Pigs are Smart Meet Milo Medicare Cost Report General
PROVIDER REIMBURSEMENT REVIEW BOARD DECISION ON THE RECORD 20ll-D31
 PROVIDER REIMBURSEMENT REVIEW BOARD DECISION ON THE RECORD 20ll-D31 PROVIDER- George Washington University Hospital Washington, D.C. DATE OF HEARING - May 25, 2010 Provider No.: 09-0001 Cost Reporting
PROVIDER REIMBURSEMENT REVIEW BOARD DECISION ON THE RECORD 20ll-D31 PROVIDER- George Washington University Hospital Washington, D.C. DATE OF HEARING - May 25, 2010 Provider No.: 09-0001 Cost Reporting
Form CMS Update Transmittals 20 and 21
 Form CMS-2552 2552-96 Update Transmittals 20 and 21 Don Fry, Director, KPMG LLP, Los Angeles, CA Joe Sellars, Director, KPMG LLP, Jacksonville, FL New York ICR Road Shows April 12-16, 2010 Summary of effective
Form CMS-2552 2552-96 Update Transmittals 20 and 21 Don Fry, Director, KPMG LLP, Los Angeles, CA Joe Sellars, Director, KPMG LLP, Jacksonville, FL New York ICR Road Shows April 12-16, 2010 Summary of effective
Cost Survey 2016 Instructions Alaska Medicaid Personal Care and Home & Community Based Waiver Services
 Cost Survey 2016 Instructions Alaska Medicaid Personal Care and Home & Community Based Waiver Services General Information This cost survey must be used to report costs in accordance with 7 AAC 145.531-537.
Cost Survey 2016 Instructions Alaska Medicaid Personal Care and Home & Community Based Waiver Services General Information This cost survey must be used to report costs in accordance with 7 AAC 145.531-537.
Federally Qualified Health Center (FQHC) / Rural Health Clinic (RHC) Prospective Payment System (PPS) Frequently Asked Questions.
 / Rural Health Clinic (RHC) Prospective Payment System (PPS) Frequently Asked Questions.") Federally Qualified Health Center (FQHC) / Rural Health Clinic (RHC) Prospective Payment System (PPS) Frequently Asked Questions General 1. Is there language in our agreement around updated contracts with
Federally Qualified Health Center (FQHC) / Rural Health Clinic (RHC) Prospective Payment System (PPS) Frequently Asked Questions General 1. Is there language in our agreement around updated contracts with
SDMGMA Third Party Payer Day. Anja Aplan, Payment Control Officer
 SDMGMA Third Party Payer Day Anja Aplan, Payment Control Officer Agenda Medicaid Overview Third Party Liability Common TPL Errors NPI and Taxonomy Billing Transportation Billing Diagnosis codes Aid Category
SDMGMA Third Party Payer Day Anja Aplan, Payment Control Officer Agenda Medicaid Overview Third Party Liability Common TPL Errors NPI and Taxonomy Billing Transportation Billing Diagnosis codes Aid Category
New IPPS Regulations & Cost Report Forms ( ) Hospital Finance & Reimbursement Workshop Columbia, SC November 15, 2011
 Hospital Finance & Reimbursement Workshop Columbia, SC November 15, 2011") New IPPS Regulations & Cost Report Forms (2552-10) Hospital Finance & Reimbursement Workshop Columbia, SC November 15, 2011 Disclaimer All information provided is of a general nature and is not intended
New IPPS Regulations & Cost Report Forms (2552-10) Hospital Finance & Reimbursement Workshop Columbia, SC November 15, 2011 Disclaimer All information provided is of a general nature and is not intended
Small Rural Hospital Transition (SRHT) Project Guide
 Project Guide") Small Rural Hospital Transition (SRHT) Project Guide Understanding the Hospital Medicare Cost Report Uncompensated and Indigent Care Data Form CMS-2552-10 (Worksheet S-10) September 22, 2015 525 S. Lake
Small Rural Hospital Transition (SRHT) Project Guide Understanding the Hospital Medicare Cost Report Uncompensated and Indigent Care Data Form CMS-2552-10 (Worksheet S-10) September 22, 2015 525 S. Lake
Cracking the Code on Managing Costs and Forecasting Revenue in a PPS Environment
 Cracking the Code on Managing Costs and Forecasting Revenue in a PPS Environment January 18, 2018 Peter R. Epp, CPA CohnReznick LLP Todays Moderator Nicole Cadovius, MBA, CAPS, FAAIDD Director, Practice
Cracking the Code on Managing Costs and Forecasting Revenue in a PPS Environment January 18, 2018 Peter R. Epp, CPA CohnReznick LLP Todays Moderator Nicole Cadovius, MBA, CAPS, FAAIDD Director, Practice
MANUAL/DEPARTMENT ORIGINATION DATE DECEMBER 2015 LAST DATE OF REVIEW OR REVISION APPROVED BY
 MANUAL/DEPARTMENT ADMINISTRATIVE POLICY AND PROCEDURE MANUAL ORIGINATION DATE DECEMBER 2015 LAST DATE OF REVIEW OR REVISION REVIEW: MARCH 2016 REVISION: JULY 2017, DECEMBER 2017 APPROVED BY TITLE: FINANCIAL
MANUAL/DEPARTMENT ADMINISTRATIVE POLICY AND PROCEDURE MANUAL ORIGINATION DATE DECEMBER 2015 LAST DATE OF REVIEW OR REVISION REVIEW: MARCH 2016 REVISION: JULY 2017, DECEMBER 2017 APPROVED BY TITLE: FINANCIAL
JUPITER MEDICAL CENTER, INC. AND AFFILIATED COMPANIES. Jupiter, Florida. CONSOLIDATED FINANCIAL STATEMENTS September 30, 2014 and 2013
 JUPITER MEDICAL CENTER, INC. AND AFFILIATED COMPANIES Jupiter, Florida CONSOLIDATED FINANCIAL STATEMENTS Jupiter, Florida CONSOLIDATED FINANCIAL STATEMENTS CONTENTS INDEPENDENT AUDITOR S REPORT... 1 FINANCIAL
JUPITER MEDICAL CENTER, INC. AND AFFILIATED COMPANIES Jupiter, Florida CONSOLIDATED FINANCIAL STATEMENTS Jupiter, Florida CONSOLIDATED FINANCIAL STATEMENTS CONTENTS INDEPENDENT AUDITOR S REPORT... 1 FINANCIAL
Health Care Pricing: Establishing Fees, Discounts, Charging Interest, Out-of- Network Arrangements and Other Issues
 Health Care Pricing: Establishing Fees, Discounts, Charging Interest, Out-of- Network Arrangements and Other Issues By: David M. Glaser 612.492.7143 dglaser@fredlaw.com February 2016 Pricing There are
Health Care Pricing: Establishing Fees, Discounts, Charging Interest, Out-of- Network Arrangements and Other Issues By: David M. Glaser 612.492.7143 dglaser@fredlaw.com February 2016 Pricing There are
Prior Authorization All non-emergent services rendered by non-contracted providers require prior authorization, unless specified otherwise.
 Prior Authorization All non-emergent services rendered by non-contracted providers require prior authorization, unless specified otherwise. Abortions, Hysterectomies and Sterilizations Ambulance Emergency
Prior Authorization All non-emergent services rendered by non-contracted providers require prior authorization, unless specified otherwise. Abortions, Hysterectomies and Sterilizations Ambulance Emergency
CUSTOMER WAIVER OF CO-PAYS AND DEDUCTIBLES
 CUSTOMER WAIVER OF CO-PAYS AND DEDUCTIBLES SCOPE: All Envision Physician Services colleagues associated with the billing and coding process in any way, including all internal and external billing companies
CUSTOMER WAIVER OF CO-PAYS AND DEDUCTIBLES SCOPE: All Envision Physician Services colleagues associated with the billing and coding process in any way, including all internal and external billing companies
Direct patient care services
 01-10 FORM CMS-2552-96 3605.2 LDP room during a typical month, and apply that percentage through the rest of the year to determine the number of labor and delivery days to report on line 29. Maternity
01-10 FORM CMS-2552-96 3605.2 LDP room during a typical month, and apply that percentage through the rest of the year to determine the number of labor and delivery days to report on line 29. Maternity
IN THE MATTER OF: Docket No MSB, Case No. DECISION AND ORDER
 STATE OF MICHIGAN MICHIGAN ADMINISTRATIVE HEARING SYSTEM FOR THE DEPARTMENT OF COMMUNITY HEALTH P.O. Box 30763, Lansing, MI 48909 (877) 833-0870; Fax: (517) 334-9505 IN THE MATTER OF: Docket No. 2011-52196
STATE OF MICHIGAN MICHIGAN ADMINISTRATIVE HEARING SYSTEM FOR THE DEPARTMENT OF COMMUNITY HEALTH P.O. Box 30763, Lansing, MI 48909 (877) 833-0870; Fax: (517) 334-9505 IN THE MATTER OF: Docket No. 2011-52196
Comprehensive Revenue Cycle Management:
 Comprehensive Revenue Cycle Management: An Introduction to Our Processes and Protocols 200 Old Country Road, Suite 470 Mineola, NY 11501 Phone: 516-294-4118 Fax: 516-294-9268 www.businessdynamicslimited.com
Comprehensive Revenue Cycle Management: An Introduction to Our Processes and Protocols 200 Old Country Road, Suite 470 Mineola, NY 11501 Phone: 516-294-4118 Fax: 516-294-9268 www.businessdynamicslimited.com
Archived 12.1 THE BASIS FOR ESTABLISHING A RATE OF PAYMENT DETERMINING A FEE... 2
 SECTION 12 - REIMBURSEMENT METHODOLOGY 12.1 THE BASIS FOR ESTABLISHING A RATE OF PAYMENT... 2 12.2 DETERMINING A FEE... 2 12.2.A LONG-TERM CARE DISPENSING FEE REQUIREMENTS... 3 12.2.B CREDITS ON MEDICATIONS
SECTION 12 - REIMBURSEMENT METHODOLOGY 12.1 THE BASIS FOR ESTABLISHING A RATE OF PAYMENT... 2 12.2 DETERMINING A FEE... 2 12.2.A LONG-TERM CARE DISPENSING FEE REQUIREMENTS... 3 12.2.B CREDITS ON MEDICATIONS
Passport Advantage Provider Manual Section 13.0 Provider Billing Manual Table of Contents
 Passport Advantage Provider Manual Section 13.0 Provider Billing Manual Table of Contents 13.1 Claim Submissions 13.2 Provider/Claims Specific Guidelines 13.3 Understanding the Remittance Advice 13.4 Denial
Passport Advantage Provider Manual Section 13.0 Provider Billing Manual Table of Contents 13.1 Claim Submissions 13.2 Provider/Claims Specific Guidelines 13.3 Understanding the Remittance Advice 13.4 Denial
VACCINES FOR CHILDREN PROGRAM PROVIDER AGREEMENT
 VACCINES FOR CHILDREN PROGRAM PROVIDER AGREEMENT FACILITY INFORMATION Facility Name: Facility Address: VFC Pin: City: County: State: Zip: Telephone: Fax: Shipping Address (if different than facility address):
VACCINES FOR CHILDREN PROGRAM PROVIDER AGREEMENT FACILITY INFORMATION Facility Name: Facility Address: VFC Pin: City: County: State: Zip: Telephone: Fax: Shipping Address (if different than facility address):
A Guide to Submitting Medicaid Requests for Other Payer Advanced APM Determinations (Payer Initiated Submission Form)
") A Guide to Submitting Medicaid Requests for Other Payer Advanced APM Determinations (Payer Initiated Submission Form) Purpose Through the Payer Initiated Submission Form (the Form ), the Centers for Medicare
A Guide to Submitting Medicaid Requests for Other Payer Advanced APM Determinations (Payer Initiated Submission Form) Purpose Through the Payer Initiated Submission Form (the Form ), the Centers for Medicare
Scope: All services billed for by Renown Regional, Renown South Meadows, Renown Skilled Nursing, and Renown Rehabilitation Hospital
 Page 1 of 9 Scope: All services billed for by Renown Regional, Renown South Meadows, Renown Skilled Nursing, and Renown Rehabilitation Hospital Purpose: To provide financial assistance to those without
Page 1 of 9 Scope: All services billed for by Renown Regional, Renown South Meadows, Renown Skilled Nursing, and Renown Rehabilitation Hospital Purpose: To provide financial assistance to those without
Billing and Collection Standard Operating Guidelines
 Tuscarawas County Health Department Billing and Collection Standard Operating Guidelines Medical Clinic and Alcohol and Addiction Program Version 1.0 Effective May 11, 2018 Revision Table Date Revision
Tuscarawas County Health Department Billing and Collection Standard Operating Guidelines Medical Clinic and Alcohol and Addiction Program Version 1.0 Effective May 11, 2018 Revision Table Date Revision
Scope: All services billed for by Renown Regional, Renown South Meadows, Renown Skilled Nursing, and Renown Rehabilitation Hospital
 Page 1 of 9 Scope: All services billed for by Renown Regional, Renown South Meadows, Renown Skilled Nursing, and Renown Rehabilitation Hospital Purpose: To provide financial assistance to those without
Page 1 of 9 Scope: All services billed for by Renown Regional, Renown South Meadows, Renown Skilled Nursing, and Renown Rehabilitation Hospital Purpose: To provide financial assistance to those without
Scope: All services billed for by Renown Regional, Renown South Meadows, Renown Skilled Nursing, and Renown Rehabilitation Hospital
 Page 1 of 9 Scope: All services billed for by Renown Regional, Renown South Meadows, Renown Skilled Nursing, and Renown Rehabilitation Hospital Purpose: To provide financial assistance to those without
Page 1 of 9 Scope: All services billed for by Renown Regional, Renown South Meadows, Renown Skilled Nursing, and Renown Rehabilitation Hospital Purpose: To provide financial assistance to those without
Rev. 12 FORM CMS ( ) (INSTRUCTIONS FOR THIS WORKSHEET ARE PUBLISHED IN CMS PUB. 15-2, SECTION )
 (INSTRUCTIONS FOR THIS WORKSHEET ARE PUBLISHED IN CMS PUB. 15-2, SECTION )") COMPLEX IDENTIFICATION DATA FROM PART I Hospital and Hospital Health Care Complex Address: 1 Street: P.O. Box: 1 2 City: State: ZIP Code: County: 2 Hospital and Hospital-Based Component Identification:
COMPLEX IDENTIFICATION DATA FROM PART I Hospital and Hospital Health Care Complex Address: 1 Street: P.O. Box: 1 2 City: State: ZIP Code: County: 2 Hospital and Hospital-Based Component Identification:
Gonzales Healthcare Systems Policy
 Gonzales Healthcare Systems Policy Subject: Financial Policy and Healthcare Transparency Purpose: To provide affordable and quality healthcare to our community. Therefore, it is essential that we establish
Gonzales Healthcare Systems Policy Subject: Financial Policy and Healthcare Transparency Purpose: To provide affordable and quality healthcare to our community. Therefore, it is essential that we establish
Instructions - financial assistance application
 Instructions - financial assistance application Encompass Health Rehabilitation Hospital of Altoona 2005 Valley View Boulevard Altoona, PA 16602 814.944.3535 encompasshealth.com/altoonarehab Section A
Instructions - financial assistance application Encompass Health Rehabilitation Hospital of Altoona 2005 Valley View Boulevard Altoona, PA 16602 814.944.3535 encompasshealth.com/altoonarehab Section A
JUPITER MEDICAL CENTER, INC. AND AFFILIATED COMPANIES. Jupiter, Florida. CONSOLIDATED FINANCIAL STATEMENTS September 30, 2015 and 2014
 JUPITER MEDICAL CENTER, INC. AND AFFILIATED COMPANIES Jupiter, Florida CONSOLIDATED FINANCIAL STATEMENTS Jupiter, Florida CONSOLIDATED FINANCIAL STATEMENTS CONTENTS INDEPENDENT AUDITOR S REPORT... 1 FINANCIAL
JUPITER MEDICAL CENTER, INC. AND AFFILIATED COMPANIES Jupiter, Florida CONSOLIDATED FINANCIAL STATEMENTS Jupiter, Florida CONSOLIDATED FINANCIAL STATEMENTS CONTENTS INDEPENDENT AUDITOR S REPORT... 1 FINANCIAL
Medicaid Program; Disproportionate Share Hospital Payments Uninsured Definition
 CMS-2315-F This document is scheduled to be published in the Federal Register on 12/03/2014 and available online at http://federalregister.gov/a/2014-28424, and on FDsys.gov DEPARTMENT OF HEALTH AND HUMAN
CMS-2315-F This document is scheduled to be published in the Federal Register on 12/03/2014 and available online at http://federalregister.gov/a/2014-28424, and on FDsys.gov DEPARTMENT OF HEALTH AND HUMAN
THIS MEMBERSHIP AND THE PREPAID SERVICES PROVIDED UNDER THIS CONTRACT ARE NOT INSURANCE
 THIS MEMBERSHIP AND THE PREPAID SERVICES PROVIDED UNDER THIS CONTRACT ARE NOT INSURANCE CAGE FREE CARE PREPAID PRIMARY CARE MEMBERSHIP CONTRACT 1. NOTICE. The Cage Free Care Membership Program is not health
THIS MEMBERSHIP AND THE PREPAID SERVICES PROVIDED UNDER THIS CONTRACT ARE NOT INSURANCE CAGE FREE CARE PREPAID PRIMARY CARE MEMBERSHIP CONTRACT 1. NOTICE. The Cage Free Care Membership Program is not health
U.S. PHYSICAL THERAPY, INC. (EXACT NAME OF REGISTRANT AS SPECIFIED IN ITS CHARTER)
") UNITED STATES SECURITIES AND EXCHANGE COMMISSION WASHINGTON, D.C. 20549 FORM 10-Q (MARK ONE) QUARTERLY REPORT PURSUANT TO SECTION 13 OR 15(d) OF THE SECURITIES EXCHANGE ACT OF 1934 FOR THE QUARTERLY PERIOD
UNITED STATES SECURITIES AND EXCHANGE COMMISSION WASHINGTON, D.C. 20549 FORM 10-Q (MARK ONE) QUARTERLY REPORT PURSUANT TO SECTION 13 OR 15(d) OF THE SECURITIES EXCHANGE ACT OF 1934 FOR THE QUARTERLY PERIOD
UNITED WAY OF MERCED COUNTY FINANCIAL STATEMENTS YEAR ENDED JUNE 30, 2015, WITH COMPARATIVE TOTALS FOR 2014
 FINANCIAL STATEMENTS YEAR ENDED JUNE 30, 2015, WITH COMPARATIVE TOTALS FOR 2014 FINANCIAL STATEMENTS YEAR ENDED JUNE 30, 2015, WITH COMPARATIVE TOTALS FOR 2014 TABLE OF CONTENTS PAGE INDEPENDENT AUDITORS
FINANCIAL STATEMENTS YEAR ENDED JUNE 30, 2015, WITH COMPARATIVE TOTALS FOR 2014 FINANCIAL STATEMENTS YEAR ENDED JUNE 30, 2015, WITH COMPARATIVE TOTALS FOR 2014 TABLE OF CONTENTS PAGE INDEPENDENT AUDITORS
CHAPTER ALLOWABLE COST REIMBURSEMENT FOR NON-STATE OPERATED INTERMEDIATE CARE FACILITIES FOR INDIVIDUALS WITH AN INTELLECTUAL DISABILITY
 Ch. 6211 COST REIMBURSEMENT 55 CHAPTER 6211. ALLOWABLE COST REIMBURSEMENT FOR NON-STATE OPERATED INTERMEDIATE CARE FACILITIES FOR INDIVIDUALS WITH AN INTELLECTUAL DISABILITY Sec. 6211.1. Purpose. 6211.2.
Ch. 6211 COST REIMBURSEMENT 55 CHAPTER 6211. ALLOWABLE COST REIMBURSEMENT FOR NON-STATE OPERATED INTERMEDIATE CARE FACILITIES FOR INDIVIDUALS WITH AN INTELLECTUAL DISABILITY Sec. 6211.1. Purpose. 6211.2.
Chapter 1 Section 38. Reimbursement of State Vaccine Programs (SVPs)
") General Chapter 1 Section 38 Issue Date: November 29, 2017 Authority: 32 CFR 199.6(d)(5); 32 CFR 199.14(j)(4); National Defense Authorization Act for Fiscal Year 2017 (NDAA FY 2017, Public Law (PL) 114-328
General Chapter 1 Section 38 Issue Date: November 29, 2017 Authority: 32 CFR 199.6(d)(5); 32 CFR 199.14(j)(4); National Defense Authorization Act for Fiscal Year 2017 (NDAA FY 2017, Public Law (PL) 114-328
Original Date. Policy & Procedure Manual Written/Reviewed By: VP, Chief Financial Officer. Date: Date:
 Policy: Charity Care-Financial Assistance Policy Policy & Procedure Manual Written/Reviewed By: VP, Chief Financial Officer Approved By: Norman Regional Hospital Authority Date: 5/8/2017 Date: 5/8/2017
Policy: Charity Care-Financial Assistance Policy Policy & Procedure Manual Written/Reviewed By: VP, Chief Financial Officer Approved By: Norman Regional Hospital Authority Date: 5/8/2017 Date: 5/8/2017
Medicare Reimbursement Update and Financial Improvement Tools for Rural Hospitals
 acumen Medicare Reimbursement Update and Financial Improvement Tools for Rural Hospitals Presented by Ann King White, CPA BKD, LLP June 15, 2017 insight ideas attention reach expertise depth agility talent
acumen Medicare Reimbursement Update and Financial Improvement Tools for Rural Hospitals Presented by Ann King White, CPA BKD, LLP June 15, 2017 insight ideas attention reach expertise depth agility talent
CMS Quality Payment Program
 CMS Quality Payment Program Guide for Managed Care Organizations Providing State Medicaid Agencies with Information and Documentation for Submitting Medicaid Requests for Other Payer Advanced APM Determinations
CMS Quality Payment Program Guide for Managed Care Organizations Providing State Medicaid Agencies with Information and Documentation for Submitting Medicaid Requests for Other Payer Advanced APM Determinations
Atchison Hospital Association, Inc. and Riverbend Regional Healthcare Foundation. Consolidated Financial Report September 30, 2015
 Consolidated Financial Report September 30, 2015 Contents Independent Auditor s Report on the Financial Statements 1 2 Financial Statements Consolidated balance sheets 3 4 Consolidated statements of operations
Consolidated Financial Report September 30, 2015 Contents Independent Auditor s Report on the Financial Statements 1 2 Financial Statements Consolidated balance sheets 3 4 Consolidated statements of operations
The Financial Effects of Critical Access Hospital Conversion
 The Financial Effects of Critical Access Hospital Conversion July 23, 2003 Richard Donkle, CPA Dale Gullickson, FHFMA Rural Wisconsin Health Cooperative INTRODUCTION The Balanced Budget Act of 1997 established
The Financial Effects of Critical Access Hospital Conversion July 23, 2003 Richard Donkle, CPA Dale Gullickson, FHFMA Rural Wisconsin Health Cooperative INTRODUCTION The Balanced Budget Act of 1997 established
Mount Sinai Medical Center of Florida, Inc. and Subsidiaries
 Mount Sinai Medical Center of Florida, Inc. and Subsidiaries Consolidated Financial Statements as of and for the Years Ended December 31, 2013 and 2012, Supplemental Information as of and for the Year
Mount Sinai Medical Center of Florida, Inc. and Subsidiaries Consolidated Financial Statements as of and for the Years Ended December 31, 2013 and 2012, Supplemental Information as of and for the Year
A. SCOPE: Rutland Regional Medical Services
 RUTLAND REGIONAL MEDICAL CENTER Page 1 of 11 DEPARTMENT: PATIENT FINANCIAL SERVICES TITLE: BILLING AND COLLECTIONS JOINT COMMISSION STANDARD: EFFECTIVE DATE: 08/18/15 PREPARED BY: ROXANNA FUCILE ENDORSED
RUTLAND REGIONAL MEDICAL CENTER Page 1 of 11 DEPARTMENT: PATIENT FINANCIAL SERVICES TITLE: BILLING AND COLLECTIONS JOINT COMMISSION STANDARD: EFFECTIVE DATE: 08/18/15 PREPARED BY: ROXANNA FUCILE ENDORSED
Best practices for migrating healthcare payments to ACH
 Best practices for migrating healthcare payments to ACH Member FDIC Member FDIC Matt Brodis, MBA, MHA Adventist Health System, Inc. June St. John, SVP, CTP Wells Fargo Treasury Management Member FDIC Healthcare
Best practices for migrating healthcare payments to ACH Member FDIC Member FDIC Matt Brodis, MBA, MHA Adventist Health System, Inc. June St. John, SVP, CTP Wells Fargo Treasury Management Member FDIC Healthcare
(Cont.) FORM CMS Line For cost reporting periods that overlap October 1, 2013 and subsequent years, enter the amount of the
 FORM CMS Line For cost reporting periods that overlap October 1, 2013 and subsequent years, enter the amount of the") 11-16 FORM CMS-2552-10 4030.1 4030. WORKSHEET E - CALCULATION OF REIMBURSEMENT SETTLEMENT Worksheet E, Parts A and B, calculate title XVIII settlement for inpatient hospital services under the inpatient
11-16 FORM CMS-2552-10 4030.1 4030. WORKSHEET E - CALCULATION OF REIMBURSEMENT SETTLEMENT Worksheet E, Parts A and B, calculate title XVIII settlement for inpatient hospital services under the inpatient